Approaching Universal Health Coverage in Kenya – The ...
218
Aus dem Lehrstuhl für ABWL und Gesundheitsmanagement Univ.- Prof. Dr. rer. pol. Steffen Fleßa der Rechts- und Staatswissenschaftlichen Fakultät der Ernst-Moritz-Arndt-Universität Greifswald Approaching Universal Health Coverage in Kenya – The Potential of integrating Community Based Health Insurance Schemes into an Integrated National Social Health Insurance System Inaugural - Dissertation zur Erlangung des akademischen Grades Doktor der Wissenschaften in der Medizin (Dr. rer. med.) der Universitätsmedizin der Ernst-Moritz-Arndt-Universität Greifswald Juli 2016 vorgelegt von: Ouedraogo, Lisa-Marie geb. am: 11.03.1982 in: Berlin
Transcript of Approaching Universal Health Coverage in Kenya – The ...

Aus dem Lehrstuhl für ABWL und Gesundheitsmanagement
Univ.- Prof. Dr. rer. pol. Steffen Fleßa
der Rechts- und Staatswissenschaftlichen Fakultät der Ernst-Moritz-Arndt-Universität
Greifswald
Approaching Universal Health Coverage in Kenya – The Potential of integrating Community Based Health Insurance Schemes
into an Integrated National Social Health Insurance System
Inaugural - Dissertation
zur
Erlangung des akademischen
Grades
Doktor der Wissenschaften in der Medizin (Dr. rer. med.)
der
Universitätsmedizin
der
Ernst-Moritz-Arndt-Universität
Greifswald
Juli 2016
vorgelegt von: Ouedraogo, Lisa-Marie geb. am: 11.03.1982 in: Berlin

Dekan: Prof. Dr. rer. nat. Max P. Baur 1. Gutachter: Prof. Dr. Steffen Fle a
2. Gutachter: Prof. Dr. Manuela de Allegri (Universität Heidelberg)
Ort, Raum: Universitätsmedizin Greifswald
Fleischmannstr. 42, Seminarraum 4
Tag der Disputation: 24. März 2017

3

4

5
Figure 1: Cube of Universal Health Coverage……………………………………………… 16 Figure 2: Stage Model for Universal Health Coverage……………………………………... 17 Figure 3: WHO Health System Framework………………………………………………… 22 Figure 4: Sources of Social Protection in Health…………………………………………… 23 Figure 5: Models of Micro Health Insurance……………………………………………….. 28 Figure 6: The mutual model of Micro Health Insurance…………………………………… 30 Figure 7: Possible roles of community-based MHI schemes within a national SHI system 33 Figure 8: Expected interactions between different areas of public social health protection
in Kenya…………………………………………………………………………... 42
Figure 9: Health financing landscape in Tanzania………………………………………….. 46 Figure 10: CHF structure on national level after the governance reform from 2009………… 47 Figure 11: CHF Management Structure on District Level as per CHF Act from 2001……… 48 Figure 12: Funding of the CHF system………………………………………………………. 50 Figure 13: Rwandan SHI system……………………………………………………………... 52 Figure 14: The AMU in Burkina Faso……………………………………………………...... 57 Figure 15: Institutional Structure of the AMU……………………………………………….. 58 Figure 16: Funding of the AMU……………………………………………………………… 59 Figure 17: Organizational Structure of the NHIS…………………………………………….. 62 Figure 18: Cartoon about common critiques of CBHF schemes and supporting NGO
structures in West Africa…………………………………………………………. 106
Figure 19: Stakeholder Matrix national SHI System in Kenya……………………………… 114 Figure 20: Kenya and Rwanda located in the UHC Stage Model…………………………… 128 Figure 21: Proposed structure of national SHI system in Kenya…………………………….. 155 Figure 22: General Stage Model for Implementation of a national SHI system in a low-
income context……………………………………………………………………. 158
Figure 23: Crucial components and building blocks of integrative national SHI system………………………………………………………………………
162
Figure 24: Recommended funding of integrated SHI system…………………………… 163 Figure 25: Potential roles of CBHF schemes within a national SHI system………….. 164

6
Table 1: Comparison of Benefits of National Health Insurance Schemes and Community
Based Health Insurance Schemes………………………………………………… 32
Table 2: Ubudehe categories of Rwandan SHI system……………………………………. 54 Table 3: (Internal) strengths of Tanzanian SHI system……………………………………. 68 Table 4: (Internal) weaknesses of Tanzanian SHI system…………………………………. 69 Table 5: (External) opportunities of the Tanzanian SHI system…………………………… 69 Table 6: (External) threats of Tanzanian SHI system……………………………………… 70 Table 7: (Internal) strengths of Rwandan SHI system……………………………………... 73 Table 8: (Internal) weaknesses of Rwandan SHI system…………………………………... 74 Table 9: (External) opportunities of the Rwandan SHI system……………………………. 74
Table 10: (External) threats of Rwandan SHI system……………………………………….. 74 Table 11: (Internal) strengths of the envisaged SHI system in Burkina Faso……………….. 77 Table 12: (Internal) weaknesses of the envisaged SHI system in Burkina Faso…………….. 78 Table 13: (External) opportunities of the envisaged SHI system in Burkina Faso………….. 78 Table 14: (External) threats of the envisaged SHI system in Burkina Faso………………… 79 Table 15: (Internal) strengths of Ghanaian SHI system……………………………………... 82 Table 16: (Internal) weaknesses of Ghanaian SHI system…………………………………... 83 Table 17: (External) opportunities of Ghanaian SHI system………………………………... 84 Table 18: (External) threats of Ghanaian SHI system………………………………………. 84 Table 19: Categories generated from PICD tool…………………………………………….. 98 Table 20: Description of categories for Nyanza province, Kenya…………………………... 98 Table 21: CBHF products of STIPA………………………………………………………… 99 Table 22: Proposed combined product of CBHF/NHIF…………………………………….. 102
Table 23: Stakeholder matrix for national SHI system in Kenya…………………………… 112 Table 24: Stakeholder participation strategy matrix for national SHI system in Kenya……. 116 Table 25: (Internal) strengths of Kenyan health financing sector towards a national SHI
scheme………………………………………….………………………………… 123
Table 26: (Internal) weaknesses of Kenyan health financing sector towards a national SHI scheme…………………………………………………………………………….
124
Table 27: (External) opportunities of Kenyan health financing sector towards a national SHI scheme……………………………………………………………………….
125
Table 28: (External) opportunities of Kenyan health financing sector towards a national SHI scheme…………………………………………………………………………….
126
Table 29: Components of Design Stage of national SHI system in Kenya…………………. 139 Table 30: Components of Pilot Implementation Stage of national SHI system in Kenya….. 146 Table 31: Components of Evaluation and Amendment Stage of national SHI system in
Kenya…………………………………………………………………………….. 152
Table 32: Components of National Implementation Stage of national SHI system in Kenya 153

7
ADS
AMU
ART
ASAL
AYI
CARFO
CBHF
CBHI
Anglican Development Service
Assurance Maladie Universelle
Anti-Retroviral Therapy
Arid and Semi Arid Land
Afya Yetu Initiative
Caisse Autonome de Retraite des Fonctionnaires
Community Based Health Financing
Community Based Health Insurance
CBO
CCSAM
CGoK
CHAG
CHD
Community Based Organization
Cadre de Concertation des Structures d’Appui aux Mutuelles
Central Government of Kenya
Christian Health Association of Ghana
Community Health Directorate
CHEW Community Health Extension Worker
CHF
CHMT
Community Health Fund
Community Health Management Team
CHS Community Health Strategy
CHW
CNSS
CPA
Community Health Worker
Caisse Nationale de Sécurité Sociale
Complementary Package of Activities
CPHC
CRS
CSA
CSCS
CSPF
CSPS
CT-OVC
DANIDA
DRTSS
Comprehensive Primary Health Care
Catholic Relief Services
Case Study Approach
Community Saving and Credit Scheme
Central Social Protection Fund
Centre de Santé et de Promotion Sociale
Cash Transfer Programme for Orphans and Vulnerable Children
Danish International Development Agency
Department for Road Traffic and Safety Services
DSP
DWMHI
ERD
GDP
Donors Social Protection
District-wide Mutual Health Insurance
European Report for Development
Gross Domestic Product

8
GIZ Gesellschaft für Internationale Zusammenarbeit
GLUK
GNHIA
Great Lakes University of Kenya
Ghana National Health Insurance Authority
HDR
HIS
HIV/AIDS
HMIS
HSR
IGAs
Human Development Report
Health Information System
Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome
Health Management Information System
Health Sector Reform
Income Generating Activities
ILO
IMF
International Labour Organization
International Monetary Fund
IMIS Insurance Management Information System
IPD
KCBHFA
KCDH
KCHSSIP
In-Patient-Services
Kenya Community Based Health Financing Association
Kisumu County Directorate of Health
Kisumu County Health Sector Strategic and Investment Plan
KES Kenyan Shilling
KTDA
MDG
Kenyan Tea Development Agency
Millennium Development Goal
MFI
MHI
MoHSW
MoU
MPA
MTP
MWK
Micro Finance Institution
Micro Health Insurance
Ministry of Health and Social Welfare
Memorandum of Understanding
Minimum Package of Activities
Medium Term Plans
Malawi Kwacha
NGO
NHHP
NHIA
NHIF
NHIS
NHSSHP
NSAs
NSHIS
Non-Governmental Organization
Nsambya Hospital Healthcare Plan
National Health Insurance Act
National Hospital Insurance Fund
National Health Insurance Scheme
National Health Sector Strategic Health Plan
Non-State Actors
National Social Health Insurance Scheme

9
NSPC National Social Protection Council
NSPP
NSSF
OECD
National Social Protection Policy
National Social Security Fund
Organization for Economic Co-operation and Development
OI Opportunistic Infections
OOPP Out-of-Pocket-Payments
OPD
OST
OVCs
PICD
PLWHA
PNDS
PSPF
PWD/OP
RAMA
RHMIS
SCADD
SDG
Out-Patient-Services
Office de Santé des Travailleurs
Orphans and Vulnerable Children
Participatory Integrated Community Development
People living with HIV and AIDS
Plan Nationaux de Développement Sanitaire
Public Social Protection Funds
Persons with Disabilities/Older Persons
Rwandaise d’Assurance Maladie
Rwandan Health Management Information System
Stratégie Croissance Accélérée et du Développement Durable
Sustainable Development Goals
SFSA
SHI
SOPs
SPF
SSNIT
STIPA
SWAp
Swiss TPH
SWOT
TB
TC
TIKA
TLCs
Syngenta Foundation for Sustainable Agriculture
Social Health Insurance
Standard Operational Procedures
Social Protection Floor
Social Security and National Insurance Trust
Support for Tropical Initiatives in Poverty Alleviation
Sector Wide Approach
Swiss Tropical Institute for Public Health
Strengths Weaknesses Opportunities Threats
Tuberculosis
Target Communities
Tiba kwa Kadi
Technical Learning Conversations
TNHIF
ToRs
TZS
Tanzanian National Health Insurance Fund
Terms of Reference
Tanzanian Shilling

10
UHC
UMEOA
Universal Health Coverage
West African Economic and Monetary Union
UN
UNDP
United Nations
United Nations Development Fund
USD
VAT
VSL
WASH
US Dollar
Value Added Tax
Village Savings and Loans
Water, Sanitation and Hygiene
WHO
WHR
World Health Organization
World Health Report

11
Problem Statement
Decades after international guidelines to approach Universal Health Coverage and Access for
All to essential health care services have been formulated by the global community, social
protection in health remains a major global challenge. This implies the devastating situation of
having less than 15% of the global population benefiting of any kind of social protection in
health (Loewe 2009), while more than 70% of the world population lacks any type of social
protection coverage (WSPR 2010). 36 years after the famous and often-cited Alma-Ata
Declaration proclaimed that „the promotion and protection of the health of the people is
essential to sustained economic and social development and contributes to a better quality of life
and to world peace” (Alma Ata Declaration 1978:III), people of the informal sector – which
forms up to 90% of the population in many countries of sub-Saharan Africa – are still forced to
take out loans or sell their assets to settle their hospital bills and in the end fall into poverty
because of unbearable health care costs (MIN 2014, Deblon and Loewe 2012, Ouedraogo 2012).
While private health insurance schemes are mainly serving people living in urban areas
and offer products and services that are not tailored to the needs of people of low-income from
rural and/or remote areas, public social health insurance schemes are usually designed to serve
the formal sector or are exclusively catering for public servants (Huber et al 2005). At the same
time, social protection in health is increasingly regarded to be a guarantor for development and
economic growth of the national economy (Loewe 2009).
In this context, some authors are convinced that community-based health financing is to
be seen as a promising approach to insure parts of the population, which are normally excluded
from any type of social protection in health, against catastrophic health care costs (Atim 1998,
Criel 1998, Arhin-Tenkorang 2001, La Concertation 2004, Churchill 2006, Ouedraogo et al
2012). With a focus on low-income people, Community-based Health Financing (CBHF)
schemes offer products, processes and institutions that are tailored to the specific needs of their
low-income target group, usually situated in the informal sector (Arhin-Tenkorang 2001).
In the aim to meet international standards and comply with the global development
agenda, governments in sub-Saharan Africa are increasingly acknowledging the need to include
the informal sector and people of low-income into their public health financing systems. As a
result, innovative health systems evolved, which often comprise of hybrid sub-systems to cover
various target groups of the society (Coheur et al 2008). While some governments – such as the
governments of Rwanda, Ghana and Tanzania – have already implemented integrated national
Social Health Insurance (SHI) systems that consider CBHF schemes to cover the informal

12
sector (cf. to Ministry of Health Kigali 2004, Singleton 2006 and Ramadhani 2003), others are
aiming at implementing this innovative idea in the near future, e.g. Burkina Faso and Togo (cf.
Seynou 2009, République du Togo 2010).
Objectives
Given the above-illustrated situation, the overall research objective of this thesis is to explore
the potential contribution of CBHF schemes towards Universal Health Coverage (UHC) in low-
income countries of sub-Saharan Africa.
Furthermore, the specific research objectives are set as follows;
(1) To establish common lessons learnt from low-income countries in sub-Saharan Africa
which implemented integrative SHI systems by combining efforts of national SHI
schemes and CBHF schemes, or which are in an advanced stage of designing and
implementing the same.
(2) To comprehensively analyze the Kenyan health financing system and design adequate
interventions towards the design and implementation of an integrative national SHI
scheme in Kenya which is favoring UHC.
(3) To develop a standard model for implementing integrative SHI systems in low-income
countries of sub-Saharan Africa and the world.
Structure of the Thesis
This thesis will at first provide a comprehensive topical background containing evidence about
different relevant concepts such as Development, Universal Health Coverage, Social Protection,
Health Financing and Micro Health Insurance. On this basis, the potential of combining
community-based and national efforts towards tailored health care financing at national level
will be explored by analyzing strengths and weaknesses of both approaches and providing brief
insights from low-income countries of sub-Sahara Africa in this area. Furthermore, a
comprehensive background to common development initiatives as well as the social protection
and health care financing sectors in Kenya is provided to introduce the case study of chapter
four.
In the third chapter, common efforts of governments and other stakeholders involved in
health care financing in sub-Saharan African countries to integrate CBHI schemes into public
SHI schemes will be reviewed and analyzed. In the scope of this review, Tanzania, Rwanda,
Burkina Faso and Ghana will serve as practical country case examples. Based on this extensive

13
cross-country analysis, common lessons learnt regarding the complex process of designing
integrative SHI systems in low-income countries of sub-Saharan Africa will be presented.
In chapter four, through a comprehensive country case study, the Kenyan health and
health financing sector and its stakeholders will be analyzed regarding its potential towards
UHC, aiming at the development of most promising interventions towards the design and
implementation of an integrated SHI scheme in Kenya, considering CBHF schemes as one
building block of the system. A multi-stage model as well as a multi-level structure of a national
SHI system to approach UHC in Kenya will be outlined and presented.
The thesis will be concluded in chapter five by transferring the Kenyan experience to a
global level and suggesting a standard model for implementing integrated SHI schemes in
similar contexts as given in Kenya and the presented case examples. In the conclusion, common
opportunities and limitations of community-based approaches towards UHC are highlighted and
a way forward for the Kenyan context is suggested.

14
Development has been defined in different contexts and with different intentions. In 1987, the
Brundtland Commission defined Sustainable Development as a “Development that meets the
needs of the present without compromising the ability of future generations to meet their own
needs.” Human Development, a people-centered approach towards development, was initially
defined by the International Labour Organization (ILO) to formulate Basic Needs in the context
of the ILO World Employment Programme in 1976 (Ralf Bunch Institute for international
Studies 2009). While the Basic Needs-Agenda was neglected in times of structural adjustment
and economic-focused programmes of World Bank and the International Monetary Fund (IMF)
in the 1980ies, the human aspect of development was re-prioritized in 1990 with the publication
of the first Human Development Report (HDR) that defined Human Development as a process
of “(…) enlarging people’s choices. The most critical of these wide-ranging choices is to live a long and healthy life, to be educated and to have access to resources needed for a decent standard of living. Additional choices include political freedom, guaranteed human rights and personal self-respect.” (HDR, 1990)
During this era, many countries were focusing on people-centered strategies and global attention
was paid to the Human Development concept that “incorporates all aspects of well-being – from
their health status to their economic and political freedom” (World Bank 2000:7). In the concept
of Human Development, “economic growth and human development are supposed to be
mutually reinforcing” (UNDP 1996).
The concept of Sustainable Development, just as the Human Development concept, was
initially formulated in the late 1970ies and is considered to be more comprehensive than the
people-centered approach. The innovative element of this concept is the fact that ideally social,
economic and environmental objectives of development are to be combined, leading to the
overall objective of Sustainable Development (World Bank 2000).
In more recent guidelines and policies, both concepts of Sustainable and Human
Development are interlinked to each other, e.g. in the report of the United Nations Conference
on Sustainable Development from June 2012, emphasizing that “people are at the centre of
sustainable development” (UN 2012:2) and further recommending to “mainstream sustainable
development at all levels, integrating social, economical and environmental aspects and
recognizing their inter-linkages” (UN 2012:1f). Various conceptual frameworks, such as the
Millennium Development Goals (MDGs)1, the International Human Rights Declaration2 from
1 For further information, please refer to http://www.un.org/milleniumgoals/. 2 For further information, please refer to http://www.un.org/en/documents/udhr/#atop.

15
1948, as well as the Human Security3 framework from 1994, and the concept of Happiness,
which was manifested in the World Happiness Report of 2013,4 are complementing the
understanding of Development as illustrated above.
Most international development actors acknowledged the crucial role of health in
development. Following the often-cited guideline Good Health – Good Economics (Frenk and
de Ferranti 2012), the World Health Organization (WHO) formulated that “Good health is
essential to sustained economic and social development and poverty reduction.” 5 The
importance and close inter-linkage of health and development was initially acknowledged by the
global community in the Alma-Ata Declaration of 1978,6 which proclaimed access to health as a
basic right, which is significantly contributing to economic and social development. On the
basis of the Alma-Ata Declaration, several other international guidelines and policies, such as
the Bamako Initiative,7 were formulated to emphasize the importance of access to health care
and health financing as part of the development agenda in a global perspective. Furthermore,
health is a determining element of the MDGs. Explicit formulated in MDG 4, 5 and 6 on
Reduction of Child Mortality, Improving Maternal Health and Combating HIV/AIDS, Malaria
and other diseases, and also closely related to the achievement of MDG 1, aiming at
Eradicating extreme Hunger and Poverty, due to the close relation of health and poverty (Fleßa
2007).8 The WHO constitution states, “the enjoyment of the highest attainable standard of health
is one of the fundamental rights of every human being." (WHO 1946:1) In addition to this,
health is one of the seven interconnected elements of Human Security as formulated in the
Human Development Report from 1994. In the UN World Happiness Report of 2013, health is
considered to be closely interlinked to the concept of Happiness.9
Due to the crucial role health is playing in development, global health partnerships are
on the rise with more than 80 operational global partnerships, which are recognized by the
WHO (WHO 2007:9).
3 For further information, please refer to the Human Development Report from 1994: http://hdr.undp.org/sites/
default/files/reports/255/hdr_1994_en_complete_nostats.pdf. 4 For further information, please refer to http://unsdsn.org/wp-content/uploads/2014/02/WorldHappinessReport
2013_online.pdf. 5 For further information please refer to http://www.who.int/healthsystems/universal_health_coverage/en/. 6 For further information, please refer to http://www.who.int/publications/almaata_declaration_en.pdf. 7 For further information on the Bamako Initiative, please refer to http://www.unicef.org/sowc08/docs
/sowc08_panel_2_5.pdf. 8 For further information, please refer http://www.un.org/millenniumgoals/. 9 For further information, please refer to http://unsdsn.org/wp-content/uploads/2014/02/WorldHappinessReport
2013_online.pdf.

16
Since the crucial health component within Sustainable Development is uncontested as described
above, the concept of UHC became a major focus of the international development agenda. It is
against this background, that the overall goal of UHC was acknowledged by all member states
of the WHO in the scope of reforming health financing systems in a global perspective (cf. to
WHR 2010).
The WHO defines UHC as “ensuring that all people can use the promotive, preventive,
curative, rehabilitative and palliative health services they need, of sufficient quality to be
effective, while also ensuring that the use of these services does not expose the user to financial
hardship” (WHO 2010). The common WHO-definition of UHC further embodies three related
objectives, being Equity in Access to Health Services, Quality of Health Services and Financial
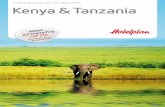
Risk Protection. As illustrated in Figure 1, the three dimensions of UHC were set to be (1) the
Population, with an objective to extend health services to the non-covered, (2) the Services, with
an objective to include other services, e.g. non-medical services, and (3) the Direct Costs, with
an objective to reduce common cost sharing and user fees:10
In 2010, the WHO published the annual World Health Report (WHR) with the title Health
System’s Financing: The Path to Universal Coverage. The WHR report marked the final turn of
international development actors towards UHC as a guarantor for effective and efficient health
10 For further information, please refer to http://www.who.int/health_financing/universal_ coverage_definition/en/.
Picture 1: Cube of UHC Dimensions, Source: WHO.
Figure 1: Cube of Universal Health Coverage, Source: WHO 2010.

17
systems in a global perspective (WHR 2010). Also stated by Jim Yong Kim, in his position as a
President of the World Bank Group, “achieving UHC and equity in health are central to
reaching the global goals to end extreme poverty by 2030 and boost shared prosperity.”11
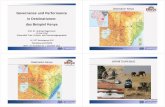
In the scope of implementing UHC, several stages can be observed as illustrated in Figure 2,
ranging from the Absence of any Financial Protection Measure (first stage), to an Intermediate
Stage of Coverage through a mix of community, cooperative and enterprise-based health
insurance schemes, other private insurance coverage as well as social health insurance coverage
for specific groups through (limited) tax-financing (second stage), to the ideal third stage of
Universal Health Coverage, through a mix of tax-based and social health insurance coverage
(cf. to Carrin et al 2005).
While most industrialized countries are to be located in stage three as a result of comprehensive
public and private social protection measures covering the majority of the population, most low-
income countries in sub-Saharan Africa are to be located between the first and second stages
and are hence to be considered to be in initial stages towards approaching UHC. It is important
to note, that it was acknowledged by the global community, that there is no universal solution
for implementing UHC, but each country has to find their own unique way. It is against this
11 Please refer to Kim’s speech on 6th December 2013, URL:
http://www.worldbank.org/en/news/speech/2013/12/06/speech-world-bank-group-president-jim-yong-kim-government-japan-conference-universal-health-coverage.
Figure 2: Stage Model for Universal Health Coverage,Source: Adjusted from Carrin and James 2005.

18
background, that several countries in sub-Saharan Africa have taken different steps to approach
UHC, based on different principles, rules and regulations (WHO 2014).
Social Protection has a long tradition in welfare states around the globe. Extensive measures
were designed and institutions were established to protect the citizens against main social risks,
such as unemployment, age, illness and disability. In recent years, social protection became a
crucial component of most agendas of global development actors and the importance of social
protection towards economic development and social equalization of the target population
became evident. The focus on people-centered approaches in international development
emphasizes the importance of efficient social protection measures once more.
The Overseas Development Institute defines Social Protection as “the public actions
taken in response to levels of vulnerability, risk and deprivation which are deemed socially
unacceptable within the given polity or society” (Norton et al 2001:7). In the European Report
on Development of 2010, Social Protection is further defined as “a kind of insurance policy
against poverty and a tool for delivering social justice, as well as a means of promoting
inclusive development. It is an expression of solidarity and cohesion between the haves and
have-nots, between governments and citizens, and even between nations.” (ERD 2010).
The two named definitions will serve as a basis for the understanding of Social
Protection in this thesis as they entail the two main elements of Social Protection being Social
Assistance and Social Insurance (Norton et al 2001). It is important to highlight the distinction
between Contributory Instruments of Social Protection – such as social health insurance – and
Non-contributory Instruments of Social Protection – such as social assistance, as well as other
instruments of Social Protection – such as targeted public social protection programmes (MIN
2013:8). While the main topic of this thesis – integrative approaches in social health insurance
in sub-Saharan Africa – can rather be located in the area of Social Insurance as a contributory
instrument of Social Protection, it is also relevant in the field of Social Assistance, as a
comprehensive social health insurance system – especially when aiming at UHC – is supposed
to both, deliver comprehensive contributory social health insurance measures to the target
population, as well as to entail proper non-contributory measures for vulnerable parts of the
society in terms of designing adequate indigents and waiving mechanisms. Furthermore, in most
low-income countries of sub-Saharan Africa, to fulfill the principle of Social Justice, a

19
comprehensive social protection system should cater for both Basic Needs as well as Economic
Security of the target group (Unni and Rani 2002).
In 2001, the Overseas Development Institute published the first comprehensive report on
concepts and approaches of social protection in international development. Norton et al stated in
the same year that social protection had been neglected in low-income countries, where
economic-focused approaches have been favored in the past (Norton et al 2001:7).
In times of Western Imperialism and Colonialism in sub-Sahara Africa, social protection
measures emerged according to the preferences of the colonialists, who usually transferred
European systems to the African context, aiming at catering for the European expatriates. The
African population had limited access to the provided services, which was mainly restricted to
industrial workers, with an aim to stabilize the general labor force and serve existing trade
unions. Nevertheless, various patterns of social protection practices can be observed during this
time, linked to different colonial backgrounds.
In Northern Africa, several pension schemes emerged in the 1950ies due to the European
influence. In some cases, even self-employed workers were covered with various benefits, such
as unemployment insurance. In opposition to this, in former British colonies of sub-Saharan
Africa, several employment injury schemes were established, which placed the main liability on
the employer, rather than developing contributory risk-pooling schemes. Most systems catered
for public servants and formally employed workers only and hence excluded the better part of
the societies. Emerging social protection schemes, e.g. national provident funds, contributed to
the creation of individual saving accounts. In some African countries, e.g. Sierra Leone, the
absence of public social protection measures resulted in a common dependency on private
provident funds and occupational pension schemes, which excluded the majority of the
population once more. In the French-occupied colonies, after a common prioritization of pure
employment injury schemes, other benefits, mostly family- and maternity-focused, were
introduced in the 1950ies. Furthermore, public pension schemes providing retirement benefits,
based on the length of service and the average salary earned over the years, were introduced in
most French-occupied colonies (Bailey 2004:3f.).
Even if – according to the overall responsibility in the areas of health and well-being of
the population – the government is supposed to play a major role in providing proper social
protection measures to its citizens, civil forms of social protection should not be neglected.
Amongst others, such measures could be observed in the United Kingdom, where the so-called
Friendly Societies evolved in the late 19th century to be the basis for a strong civil society

20
movement, which became significantly important during the 20th century while striking for
public health care measures affordable and accessible for all (Norton et al 2001:11). In sub-
Saharan Africa, due to a common failure of public institutions to establish proper social
protection measures for all (Huber et al 2005), most social protection measures in sub-Saharan
have been of civil or informal character. Social protection is therefore mainly provided through
community-based saving and credit cooperatives or other Community Based Organizations
(CBOs), e.g. as a common emergency or health fund for its members. Another common practice
in many countries of sub-Saharan Africa are the so-called tontines in Western Africa or marry-
go-round-clubs in East Africa, rotating investment schemes, which encourage its members to
regularly contribute a fixed amount to a common pool and benefit on a regular basis from a
larger amount, generated by the contributions of other members. Nevertheless, due to the
growing informal economy of most countries in sub-Saharan Africa, the essential need for
adequate social protection measures for informal sector employees’ measures became more
exigent in recent years.
Health risks are among the major risks that are tackled by social protection measures. Hence,
health financing and providing access to health care are playing unique roles in the provision
social protection. It has been proofed that social protection in health – besides serving as a main
tool to fight poverty – is leading to a continuous growth of the national economy and
comprehensive social health protection measures can support low- and middle- income
countries towards sustainable growth and development and favor the overall objective of UHC
(Hörmansdörfer 2009).
In the former French-occupied colonies, social protection measures in the area of health
were linked to social insurance principles of the established pension schemes for public
servants, while countries that were occupied by the British government focused on national
health insurance schemes, funded by common government revenues (Bailey 2004). Both
approaches excluded people working in the informal sector and/or agricultural workers. As
already mentioned, this resulted in the evolvement of civil and/or community-based social
protection mechanisms and the emergence of external interventions through international
organizations in the field of social protection in health in most countries of sub-Saharan Africa.
One of the first global programmes aiming at comprehensive social protection in health
was the ILO Step-Programme, which was implemented in several countries in a global
perspective – such as Burkina Faso, Portugal and Senegal. The ILO Step-Programme was
introduced as “a global programme for combating poverty and social exclusion in the

21
framework of the follow-up of major world social tool of the Global Campaign on Social
Security and Coverage for All“ (Bailey 2004:12).12 The ILO Step-Programme supported the
West African movement of mutual health organizations by supporting the regional network of
Mutuelles de Santé, called La Concertation. Other global stakeholders in international
development joined the ILO initiative and started prioritizing social protection measures in their
development efforts, e.g. GIZ, World Bank and WHO (cf. to Hörmansdörfer 2009). The global
community later adopted the ILO/UN lifecycle approach of establishing a comprehensive Social
Protection Floor (SPF). The SPF approach is a global social policy approach to ensure universal
access to common basic needs related to social protection, such as access to essential health
care, including maternity care; basic income security for children; basic income security for
persons in active age who are unable to work; persons with disabilities or the unemployed; as
well as basic income security for older persons.13
To achieve social health protection and approach UHC, effective health care financing measures
accessible for all, and efficient and comprehensive health systems, are indispensable. The WHO
framework for health system’s strengthening in a global perspective considers six “building
blocks and priorities” (WHO 2007:3), being Service Delivery, Health Workforce, Information,
Medical Products, Vaccinations and Technologies, Financing and Leadership. The building
blocks are supposed to use joint efforts to approach the set outcomes of Improved Health,
Responsiveness, Social and Financial Risk Protection, and Improved Efficiency. Common
indicators to achieve the named outcomes were agreed to be Coverage, Access, Quality and
Safety in regards to the different components, as illustrated in Figure 3 (WHO 2007:3).
12 For more information on the ILO STEP-Programme in different countries, please refer to
http://www.ilo.org/public/english/region/afpro/abidjan/publ/ilo8/social6.pdf. 13 Please refer to http://www.social-protection.org/gimi/gess/ShowTheme.action?th.themeId=1321.

22
Furthermore, the WHO stated, that an adequate health care financing system “raises adequate
funds for health, in ways that ensure people can use needed services and are protected from
financial catastrophe or impoverishment associated with having to pay for them.” (WHO
2007:3)
Health Care Financing as one of the six building blocks within a health system, can be defined
as “the function of a health system concerned with the mobilization, accumulation and allocation of money to cover the health needs of the people, individually and collectively, in the health system (…) the purpose of health financing is to make funding available, as well as to set the right financial incentives to providers, to ensure that all individuals have access to effective public health and personal health care” (WHO 2000)
From the presented definitions and frameworks, two main objectives of Health Care Financing
can be isolated, being (1) to raise funds for health and (2) to provide financial risk protection for
the target population (WHO 2008:2). This thesis is addressing components of the second
component of Financial Risk Protection. Various types of possible interventions in health care
financing to provide Financial Risk Protection to the respective target population can be
identified, such as Health Insurance, Conditional Social Cash Transfers to the Demand-Side,
User Fees/Out of Pocket Payments (OOPP), Pay for Performance to the Supply-Side, Provider
Financing Modalities as well as Sector Wide Approaches and Basket Funding (WHO 2009:46).
While in a global perspective, OOPP are still the most common way to cater for health care
costs, various other types of Health Care Financing evolved in recent times, such as social and
private health insurance schemes and tax-based health financing measures (Savedoff 2004).
Figure 3: WHO Health System Framework, Source: WHO 2007.

23
Health Care Financing can be either public or private financing, as illustrated in Figure 4,
which implies that either the market or the government is playing a major role in providing
efficient health financing measures (Jenson and Fernandez 2007). While the market in its private
measures is more flexible in developing a variety of products tailored to the needs of the target
population and can offer different option to different target groups (e.g. company packages,
family packages, student packages) as well as adapt their products to changing circumstances,
the government – usually through tax-financing – is in a position to implement public programs
for vulnerable parts of the society, which would otherwise not be able to afford any kind of
health financing measure. Furthermore, the government can set common rules and regulations
for a harmonized health financing landscape, while private health financing providers are often
duplicating each other and are facing a high level of competition. Nevertheless, the market
usually lacks sufficient measures to comprehensively cover the target population, often fearing
to include marginalized groups, such as low-income people, informally employed workers or the
unemployed in general.
The government usually uses tax payments to finance health protection measures for
taxpayers or identified vulnerable groups, which regularly excludes informal employed workers
and parts of the society that are not considered to be part of a specific identified group to benefit
from any targeted public measure (Jenson and Fernandez 2007). Most countries worldwide are
currently implementing a mixture of public and private measures in health financing. To
Figure 4: Sources of Social Protection in Health, Source: Author.

24
approach UHC and ensure access to health care for everyone, it is envisaged by many countries
to make use of the advantages both – public and private – measures provide.
In Social Health Insurance, mainly two systems are dominating in industrialized
countries, being the Bismarck and the Beveridge Models. While the Bismarck Model offers a
comprehensive social health insurance legislation dominated by “statuary social insurance
programs” and is based on contributions of three parties, being the employer, the employee and
the state, the Beveridge Model aims at providing “universal tax-financed flat-rate benefit
schemes, usually for all residents and for all kind of human risks” (Rösner 2012:23f.). Bismarck
systems rely on wages and salaries of the contributors, resulting in a reflection of the economic
status achieved during their work-life, while Beveridge systems are focused on a “Basic
Protection” securing a basic level of subsistence for everyone (Rösner 2012:24).
In addition to the two described models, two further models are worth to be mentioned,
namely the National Health Insurance Model and the Out-of-Pocket Model. The National
Health Insurance Model comprises of elements of both the Bismarck and the Beveridge Model,
as private sector health providers are contracted for the provision of health services, while the
payments are done through a public health insurance programme. The Out-of-Pocket Model
applies in absence of a proper health system combined with limited or no access to health
financing for the better part of the population, e.g. a national health insurance scheme for public
servants.
Within OECD countries, it was chosen to combine the Bismarck and the Beveridge
Model by combining compulsory social health insurance and budgetary subventions in several
areas such as unemployment, health and pension (Dimitrijevi and Obradovi 2005:54).
While SHI systems in industrialized countries reach coverage of up to 80% (Rösner 2012:24),
their impact remains limited in low- and middle-income countries, as OOPP are still catering for
most of the health care costs and either private nor public measures are yet able to cater for the
informal sector and people of low-income, which comprises up to 90% in many countries of
sub-Saharan Africa. Hence – if established at all – social health insurance systems are so far
implemented gradually only (Van Ginneken 2003). Most countries in sub-Saharan Africa are
benefitting of a large number of international donors that strongly support public health
activities. The revenue collection for health is thus done through a mixture of external and
domestic sources. Nevertheless, in most countries the overall funding for health is still
insufficient (WHO 2008:2)

25
In times of Western Imperialism and Colonialism in sub-Saharan Africa, most countries
benefitted of free or almost free health care provided through mission and/or faith-based
hospitals and health centers. Even if access to health care was ensured, most missionary
institutions linked the provision of health care to their widespread of missionary beliefs, often
leading to a certain level of dependency amongst the local population and the common
association of health care with colonial power and colonial intervention in general (Good
1991:2). Moreover, most public health institutions were established after the end of the First
World War, when colonial governments were trying to overtake the health sector of occupied
African territories. Even if a certain level of access to health care for the population was
provided during that era, it has to be stated that “a proper health status of the population served
as a means to economic and missionary goals rather than as an intrinsic by itself” (Leppert et al
2012:47). Furthermore, providing health care by Eurocentric colonialists was regarded as part
of their “civilizing mission”, rather than aiming at a general establishment of comprehensive and
sustainable health systems for the population (Good 1991:1, Worboys 2000: 211-213).
After regaining Independence, most governments in sub-Saharan Africa were aiming at
offering free or highly subsidized health care for everybody, based on the principles of the
Beveridge Model. The Alma-Ata Declaration of 1978 supported the aim of Universal Health
Coverage and Access for All to essential Health Services. Compulsory social health insurance
schemes were not yet on the agenda of post-Independence governments, and most health
facilities were based in urban centers of the countries, leaving the rural population without
access to health care. Rural areas were mainly served by missionary and/or faith-based health
care providers, which introduced user fees to provide high quality health care after
Independence (Criel 1998, Dror et al 2002, Atim 1998, Arhinful 2003).
Moreover, the limited tax base of most countries in sub-Saharan Africa resulted in
budgetary constraints and poor quality of provided health services, such as long waiting hours
and non-availability of drugs. At the same time, during public cost-recovery programmes in the
scope of structural adjustment policies of World Bank and IMF in the 1980ies, public spending
on health had to be reduced, aiming at a common recovery of the national economies and to
repay pending depts. The Bamako Initiative of 1987 brought the topics of access to essential
drugs and improved quality of health care back to the agenda of African governments. In order
to stabilize and strengthen health providers, common cost recovery measures were
recommended. In the early 1990ies, this resulted in the re-introduction of user fees and OOPP,
either in form of “cash and carry” or “fee for service”-systems, which overburdened the
populations – mainly consisted of low-income earners – with high health care expenses (Atim

26
1998). Furthermore, these approaches led into a common reduce of health care utilization and a
complete exclusion of people of low-income from any kind of health care service (Asfaw et al
2004, Lagarde and Palmer 2008).
After the turn of the millennium in the year 2000, the formulation of health-focused
Millennium Development Goals as well as an increased international demand for comprehensive
social protection in health for sustainable development, resulted in a common turn of many
governments in their health policies towards social protection and UHC. It is against this
background that – through the global emphasis on self-responsibility of local communities as
expressed in the Bamako Initiative as well as a common turn towards bottom-up approaches –
various types of community-based health financing mechanisms evolved (Mc Pake et al 1993).
MHI Schemes are health insurance schemes, operating on a micro level, and providing social
protection in health for the informal and low-income sector. While they are designed and
functioning similar to conventional insurance schemes, e.g. through the principle of risk pooling
and pre-payment, procedures and products are tailored to the needs of a low income target
group, mostly working in the informal sector (Fleßa 1998, Churchill 2006, McCord 2000,
Wiesmann and Jütting 2001). MHI schemes are usually not regulated under any public or
government law, which is re-emphasizing their micro perspective and role. The latter can be
beneficial to the MHI schemes avoiding registration costs and preserve their flexibility (Rösner
2012), but is having an adverse impact in terms of outreach and impact, as the scope of action
usually remains very limited.
Microinsurance schemes are part of the Microfinance Movement that comprises of
different approaches, aiming to improve access of low-income earners to financial services.
Besides providing access to insurance services, the Microfinance Sector comprises of
microleasing, microlending and microsaving components (Rösner 2012:22). All microservices
are generally characterized by the “comparatively limited regional outreach, the small scale of
their financial transactions and their orientation towards specific target groups” (Rösner
2012:21), such as low-income workers and/or famers from rural and remote areas. As main
objectives, microfinance services are aiming at strengthening the individual’s productivity level
as well as providing the target group with coping mechanisms to common risks, which might
occur in their daily contexts.

27
MHI is one type of microinsurance. Microinsurance was defined by Craig Churchhill as “the
protection of low-income people against specific perils in exchange for regular premium
payments proportionate to the likelihood and cost of the risk involved” (Churchill 2006:12). As
a special type of Microinsurance, MHI is an institution aiming at social protection in health
through compensation of enrolled members for illness-related losses (Ouedraogo et al 2012:5).
Different types of MHI schemes emerged in sub-Saharan Africa as a reaction to public cost-
recovery programmes and the introduction of extensive user fees in the 1990ies. MHI schemes
are usually embedded in different organizational forms and based on various principles and
objectives. Most popular suppliers and/or supporters of MHI schemes are commercial insurance
companies, Non-Governmental Organizations (NGOs), CBOs, faith-based organizations,
Microfinance Institutions (MFIs), cooperatives and health care providers (Roth et al 2007:20-
25).
Commercial insurance schemes can either implement the so-called Commercial Insurer
with direct sales Model – where MHI packages for low-income earners are sold to the clients
like conventional insurance policies – or the Partner-Agent-Model of MHI, where a commercial
insurance (the Partner) company is cooperating with an NGO or an CBO (the Agent) to provide
tailored MHI products to the target population. The Agent is acting as the link between the
insurance company and the target group and ensures a high level of trust, tailored products and
processes as well as targeted social marketing activities for the MHI product. In the Provider
Model, the MHI product is offered through the health provider itself as part of the services
offered at the respective health facility. By implementing this MHI model, health providers are
aiming at an increased level of utilization as well as their general income.
In the Benevolent Insurer Model, an NGO, MFI or faith-based organization is acting as a
link between the clients/members of the MHI scheme and the health provider, and offers
subsidized products to the target communities with the aim of increasing access to quality health
care.
The Mutual Model is the most common in sub-Saharan Africa and is based on a
cooperative approach, where members are equally owners and managers of the respective MHI
scheme. If implemented well, the mutual model is the most sustainable model, as it is purely
based on social capital in the target communities and does not depend on any external funding
and/or support (Leppert et al 2012:42-46).
The different organizational approaches in MHI can be classified according to their
profit or non-profit orientation as well as the risk-carrier, which is in most organizational models

28
transferred from the insured to the insurer, while solely the mutual model shows an identity of
insured and insurer resulting in one joint risk-carrier (Leppert et al 2012). The classification is
illustrated in Figure 5.
All described models of MHI are found in sub-Saharan Africa, while different models show
different geographical priorities. The Mutual Model of MHI has the most outstanding tradition,
especially in West African and bordering countries of Central Africa. In countries of the West
African Economic and Monetary Union (UMEOA), e.g. in Cameroon, Senegal and Burkina
Faso, MHI based on a mutual model approach have been well established since several decades.
The West African mutual MHI schemes are called Mutuelles de Santé, Assurances de Santé or
Mutual Health Organizations. In Kenya and Uganda, there are several MHI schemes found,
which can be classified as mutual MHI schemes, mostly known as Community-based Health
Insurance Schemes, Community-based Health Funds or Mutual Health Organizations. Even if
MHI schemes in West Africa are common, the outreach remains low with an overall coverage of
less than 1% of the population. This is a result of the fact that mutual MHI schemes are usually
small community based schemes, covering up to 100 households.
Provider Based Models evolved in many African countries, with a focus on East and
Central Africa, were mutual movements that favor mutual models of MHI are to be regarded not
as strong as in Western Africa. The most promising example of a provider-based MHI scheme is
the Bwamanda Hospital Insurance Scheme in DR Congo, which – founded in 1986 – managed
Figure 5: Models of Micro Health Insurance, Source: Author.

29
to cover 100.000 beneficiaries (Criel and Kegels 1997, Shepard et al 1990, CDI Bwamanda
2011). Furthermore, in Kenya, Uganda and Tanzania, various MHI schemes were established
based on the initiative of private or public health facilities.
The Commercial Insurer with Direct Sales as well as the Partner Agent Model as more
market-oriented approaches are mostly found in East and Southern Africa. In general, their role
can be stated as minor within the context of MHI movement in sub-Saharan Africa. One
examples from Uganda showed moderate success though, namely the NHHP/FINCA Partner
Agent Model that reached out to 50.000 beneficiaries. Pure Commercial Insurer with Direct
Sales models are mostly found in countries with an increased level of ability to pay, e.g. in
middle-income countries of East and Southern Africa. In Botswana, one commercial insurer, the
Itekanele Health Scheme, is offering a product for low-income earners of the informal sector.
The Benevolent Insurer Model of MHI is not yet common in sub-Saharan Africa, but
especially stable and well-established MFIs show significant potential to implement MHI as part
of their products in future. Some efforts had been taken by the Kenyan Jamii Bora Trust, which
introduced a mandatory health insurance for their microloan takers (Leppert et al 2012).
Community-Based Health Financing (CBHF) is one model of MHI. While other MHI models
are based on partnerships with commercial insurance schemes or NGOs, or designed in a
provider-based manner, CBHF is a mutual model based on a cooperative approach. In CBHF,
members are equally owners and managers of the scheme and participate in all processes, as
illustrated in Figure 6 (Leppert et al 2012).
In sub-Saharan Africa, mutual MHI schemes are rooted in traditional risk-sharing
arrangements, e.g. in the Thiès Region of Senegal, mutual MHI schemes could be traced back
up to the 1950ies. In Rwanda, mutual MHI schemes have been well established for several
decades as well. In other countries, such as Kenya, Mali, Burkina Faso, and Ghana, mutual MHI
schemes evolved in the 1980ies and 1990ies as a result of initiatives of common mission
hospitals that offered health services at a low cost (Ndiaye et al 2007).
Mutual MHI schemes are based on trust, social control and close linkages to the target
community and the cooperating local health providers. The elements of trust as well as a high
level of social control ensure that premiums are paid and scheme officials are settling the
hospital bills. Due to the fact, that no external partner or funder is involved in the operations of
mutual MHI schemes, they have potential to contribute to a long-term community
empowerment, by ensuring that the community is successfully coping with existing health
financing needs.

30
In this thesis, the terms of Community-based Health Financing, Community-based Health
Insurance, Mutual Health Insurance as well as Community-based or Mutual MHI schemes will
be used equally to describe the above-illustrated mutual model of Micro Health Insurance.
Figure 6: The mutual model of Micro Health Insurance, Source: Author.

31
While the mutual approach of MHI is promising regarding sustainable community
empowerment and social protection in health, it’s so far impact in countries of sub-Saharan
Africa remains limited with coverage rates of as low as 1%. Recent research revealed that the
scaling-up of CBHF schemes towards the national level as part of national health insurance
systems is to be regarded as very promising. In this approach, advantages of both systems can be
combined towards the development of a most advantageous integrated social health insurance
system (cf. to Loewe 2006, Coheur 2008, Leatherman et al 2010, Deblon and Loewe 2012,
Ouedraogo 2012, MIN 2013).
In direct comparison, national SHI schemes provide strengths in the areas of regulation
on a national level as well as standardized processes and systems due to proper – external or tax-
based – funding. On the other hand, CBHF schemes – due to their community-based and -
owned character – show higher levels of ownership, trust and good governance. In terms of
coverage, national SHI schemes are showing potential to a wide coverage, e.g. through
compulsory and nation-wide health insurance. This higher level of coverage is automatically
leading to a larger risk pool that will allow the scheme to offer more attractive products,
specifically regarding ceilings of offered products and the general coverage of services.
CBHF schemes nevertheless show advantages in the area of inclusive and universal
access, as they are open for all groups of the society and implement indigents for vulnerable
parts of the society as part of their general mandate towards community empowerment. In terms
of product sensitivity, CBHF schemes show an increased potential as compared to national
health insurance schemes, as – through extensive community involvement and participation –
they are able to assess the needs and demands of the community members. This leads to more
flexibility of the CBHF products, which are not determined by national policies and can be
revised frequently through continuous community involvement and consultations. The
comparison of advantages of both national health insurance schemes and community-based
health insurance schemes is illustrated in Table 1.

32
National Social Health Insurance Schemes
Community Based Health Insurance
Schemes Level of Ownership
Level of Trust Good Governance
National Regulation Standard Procedures
Inclusive Access Coverage
Dimension of Risk Pool Product Sensitivity
Attractiveness of Products Flexibility of Products
Table 1: Comparison of Benefits of National Health Insurance Schemes and Community Based Health Insurance Schemes, Source: Author.
Due to the promising character of CBHF schemes, many governments in sub-Saharan Africa
started to implemented integrative national SHI schemes, which are either based on community-
based MHI schemes or make use of community-based MHI schemes to cover certain parts of
their target group, especially the informal sector.
Community-based MHI schemes can occupy various roles and responsibilities within a national
SHI scheme, as illustrated in Figure 7. In the case, where the respective government totally fails
to implement social protection measures in health, community-based MHI schemes can be seen
as a substitute for the same, while in case a national health insurance scheme is operating, but
considered to be irrelevant or not attractive to a certain target group, community-based MHI
schemes can serve as an alternative to public social protection measures.
In the case, where the national SHI scheme is attractive to the entire population,
community-based MHI schemes can establish linkages, and furthermore – specifically in cases

33
where the SHI is not providing comprehensive cover for relevant health risks – serve as an
attractive complement of the public SHI scheme. In all presented cases, community-based MHI
schemes can provide attractive supplementary coverage to the national SHI scheme (Deblon and
Loewe 2012, MIN 2013).
The National Health Insurance Authority (NHIA) of the Government of Ghana started
implementing a national SHI scheme, namely the National Health Insurance Scheme (NHIS) in
2003. The established system aimed at making use of existing community-based health
financing structures and based the entire national system on District-wide Mutual Health
Insurance Schemes (DMHIS). In this case, MHI schemes are serving as substitutes of the NHIS,
which is comprehensively based on the local schemes.
In Burkina Faso, the government with the assistance of the ILO Step-Programme,
initiated the establishment of a national SHI system, the Assurance Maladie Universelle (AMU)
in the years 2000 up to 2010. The system was initiated to provide universal coverage to the
Burkinabé population and existing local Mutuelles de Santé were supposed to be integrated into
the system to cover the informal sector. From 2011 on, the Partners for Health Network, in
cooperation with the WHO, made efforts in designing and implementing the AMU (Ministère de
la Fonction Publique, du Travail et de la Securité Sociale Ministère de la Fonction Publique, du
Figure 7: Possible roles of community-based MHI schemes within a national SHI system, Source: Adjusted from Deblon and Loewe 2012
and MIN 2013.

34
Travail et de la Securité Sociale 2013). The envisaged system in Burkina Faso is considered to
use MHI schemes as complementary institutions to the national SHI system.
The Ministry of Health of the Government of Tanzania initiated the integrative
TNHIF/Community Health Fund (CHF) system in Tanzania in 1996 as a voluntary pre-payment
scheme, containing exemption mechanisms for the poor (Mtei and Mulligan 2007). Prior to the
establishment of the CHF, only few established mutual health insurance schemes were to be
found in Tanzania. The aim of the government was to guarantee sustainable access to basic
health care for poor and vulnerable groups within the population. The Tanzanian CHF is closely
linked to the Tanzanian National Health Insurance Fund (TNHIF) and is complementing the
same. In 2009, the TNHIF started to overtake main managerial functions of the CHF. Hence, the
Tanzanian system is to be regarded as a closely interlinked system of community-based and
public approaches towards social protection in health.
In Rwanda, the Programme de développement des mutuelles de santé was established in
1999, while the tradition of mutual health insurance schemes has been in existence since the
1960s (Ministry of Health of Rwanda 2004). The number of mutual health insurance schemes
increased from six in 1998 to 76 in 2001 and to 226 in 2004. In 2005, the programme covered
about 2,101,034 people, representing 27% of the entire population of Rwanda (Mukabaranga
2005). By 2008, 85% of the population were benefiting from mutual health insurance.
Furthermore, a law, passed in April 2008, obliged every Rwandan to become a member of a
health insurance scheme (WHO 2008a). The program is supposed to be a national health care
financing program based on solidarity. Consisting of 294 mutual health insurance schemes
operating throughout the country, it complements national social security measures for the
formal sector, such as the Rwandaise d’Assurance Maladie (RAMA). The primary objective of
the program is to reach the informal sector of the country, which is not covered by the RAMA.
The system is financed by a national fund, the Fonds Nationale au Solidarité aux mutuelles de
santé. It also benefits from external funding from donors such as USAID (Ministry of Health of
Rwanda 2004). In Rwanda, MHI schemes are complementing the national system, but given the
fact that the RAMA does not cover the informal sector at all, the Rwandan system of Mutuelles
de Santé can be considered to be substitutive to the RAMA.
Observing the illustrated case examples, it becomes obvious that in sub-Saharan Africa,
MHI schemes – if part of a national system – are either to be considered as substitutes to the
national SHI system or closely interlinked to the same, and hence complementing the national
SHI system. Cases, where MHI schemes can be considered as strong alternatives to the national
SHI system, cannot be reported yet. Equally, supplementing MHI schemes are rare, and can

35
only be reported in very low numbers, e.g. for Kenya where CBHF schemes cater for OPD
services of informal sector employees and non-medical services, which are not considered by
the National Hospital Insurance Fund (NHIF).
Kenya – while considered as the largest economy of East Africa – is still classified as a low-
income country facing the devastating situation of 43.3% of the population living below the
poverty line (World Fact Book 2012). 76% of the population is living in rural areas, leading to a
total of 75% of work force in agriculture or agricultural related fields, which reveals the crucial
development need for rural development as well as professionalization and/or industrialization
of the agricultural sector.
In the area of health, the number of children underweight under the age of five stands at
16.4% (2009), while the Maternal Death Rate stands at 360 deaths/100,000 live births and the
Infant Mortality Rate stands at 40.71 deaths/1,000 live births. 0.18 physicians are found per
1,000 inhabitants and 1.4 hospital beds cater for 1,000 people. The HIV/AIDS prevalence rate
stands at 6.1% (2012 est.).14 These figures reveal the major challenges, Kenya’s health system is
facing, leading to a main focus of the government and external donors to strengthen the current
health system and the common objective of achieving better health outcomes in the near future.
In opposition to that, the Kenyan constitution states, “every person has the right to the highest
attainable standard of health which includes the right to health care services” (Constitution of
Kenya 2010).
Kenya revised the Community Health Strategy (CHS)15 in 2007, which was initially
designed to foster the implementation of the National Health Sector Strategic Health Plan II
(NHSSP II).16 The NHSSP II was implemented from 2005 to 2010. In the scope of the CHS,
6,000 community units were established. Each unit covers 1,000 households, and comprises one
Community Health Extension Worker (CHEW) and 50 Community Health Workers (CHW) to
support the respective community unit regarding their health needs in a community based
approach. Through the CHS, the Kenyan government is aiming at a close involvement of
14 For further information, please refer to https://www.cia.gov/library/publications/the-world-
factbook/geos/ke.html. 15 The CHS was set up by the Kenyan Ministry of Health with technical assistance of GLUK University to
strengthen the use of Comprehensive Primary Health Care (CPHC). For more information, please refer to Buong et al (2013): Uptake of Community Health Strategy on Service Delivery and Utilization in Kenya. In: European Scientific Journal. August 2013 – Edition, Volume 9, No. 23.
16 For more information on the NHSSP II, please refer to http://www.nacc.or.ke/attachments/ article/102/NHSSP%20II-2010.pdf.

36
community members and local leaders in development activities with a focus on providing
Comprehensive Primary Health Care (CPHC) on community level. CBHF can be considered as
one component of the CHS, given that one of its main objectives is to “empower Kenyan
households and communities to take charge of improving primary health care and their own
health” (Ministry of Health/UNICEF 2010:11).
In 2008, the Government of Kenya formulated the Vision 2030 “to create a globally
competitive and prosperous nation with a high quality of life by 2030”.17 Vision 2030 is to be
implemented based on 5-year Medium Term Plans (MTP) and is aiming at an “issue-based,
people-centered, result-oriented and accountable democratic political system.”18 Vision 2030
comprises three pillars and health is a strong component of the social pillar that was designed to
complement the economic and political pillars. The objective of the social pillar of Vision 2030
is the improvement of quality of life for all Kenyans through various human and social welfare
projects and programmes, specifically in the areas of Education and Training, Health,
Environment, Housing and Urbanisation, Gender, Children and Social Development, as well as
Youth and Sports, while the economic pillar of Vision 2030 seeks to improve the prosperity of
all regions of the country and all Kenyans by achieving a 10% Gross Domestic Product (GDP)
growth rate by 2012. The economic pillar considers various areas such as Infrastructure,
Tourism, Agriculture, Trade, Manufacturing, Business Process Off-Shoring and Information
Technology-enabled Services and Financial Services. The political pillar of Vision 2030 aims at
establishing a democratic system that is issue-based, people-centred, result-oriented and
accountable to the public. The political pillar is anchored on transformation of Kenya’s political
governance across five strategic areas, being The Rule of Law – the Kenya Constitution 2010,
Electoral and Political Processes, Democracy and Public Service Delivery, Transparency and
Accountability, Security, as well as Peace Building and Conflict Management.
Within the first MTP (2008-2012), in 2010, a new constitution was adapted, which
established the right of each Kenyan to access adequate health care and initiated the devolution
process, which is considered to be the “Heart of the New Constitution” (World Bank 2012).
Within the devolution process, Kenya was divided into 47 administrative divisions, the counties.
Each county is governed by a devolved county government structure, equipped with own
decision-making processes and authorities in various areas of public responsibilities. The county
governments are replacing the provincial, district and local government administration
governments that were formed after Kenya gained back its Independence in 1963. The transfer
of functions to the county governments was supposed to be carried out within three years
17 For further information, please refer to http://www.vision2030.go.ke/. 18 For further information, please refer to http://www.vision2030.go.ke/.

37
starting in 2010 (KPMG 2013). De facto, the 47 county governments were set up in March
2013. With the set-up of county-based Huduma Centers, basic service provision to the citizens
was devolved to the county governments.19
Within the devolution process of the Government of Kenya, the health component is
based on multi-faced orientations and objectives. Health financing is part of the policy
orientations, while the overall policy goal was set to be “Better Health – In a responsive
manner” (Ministry of Medical Services and Ministry of Public Health and Sanitation 2012:13).
Nevertheless, some development actors fear that the devolution process “could also fuel
inefficiencies, exacerbate existing inequities and precipitate policy and structural discord in the
sector” (Development Initiatives 2013).
The devolution of the Kenyan health sector – besides being an important step towards
decentralized democratic governance structures – in fact poses challenges in clarity and division
of roles of the national and the county government structures. While the Kenyan constitution is
supposed to provide clear guidelines on basic rights to be fulfilled, the concrete implementation
– e.g. the basic right to access to clean water or health services – remains vague. Some tasks,
e.g. the overall responsibility for development is supposed to be divided amongst the two
government entities on county and central level, while the coordination of the same is not
clearly described or further elaborated. Other responsibilities demanding national coordination,
e.g. the management of the Kenyan Health Information System (HIS), were completely
devolved to the county structures, threatening their sustainability, as this responsibility can
hardly be fulfilled in provided fund allocations to the counties. Other responsibilities were
divided in an arbitral way, which questions the overall accountability and transparency. In
addition, specific responsibilities – such as the running of provincial hospitals as well as the
undertaking of immunization campaigns and common drug procurement and supply – have not
been clearly divided amongst the two entities, so that the implementation of crucial tasks
remains uncertain (Lakin and Kinuthia 2013).
Due to the mentioned gap in clarity of roles and responsibilities, one of the immediate
results of the devolution process was a general shortage of drugs nationwide. By law, counties
are entitled to least 15% of the total national revenues collected. Despite some counties
currently receiving adequate funding, there is still a common demand of most counties for an
increase of budgetary allocations, and a common complaint about the central government being
reluctant to comply with the law was formulated. The low level of cooperation by the central
government is perceived as an attempt to compromise the effectiveness of the devolved county
19 For more information, please refer to http://www.hudumakenya.go.ke/services.

38
units. On a closer look, it becomes evident, that the currently established county governments do
not have the capacity to absorb more than the allocated 15% of the national government
revenues (Laibuta 2013).
In addition to those named challenges, the impact of extensive corruption is still
immense in Kenya, absorbing an estimated 30% of public funds (Hope 2012, Damdinjav et al
2013:5). While the new constitution and the set objectives of the devolution process are
addressing corruption and are suggesting common coping mechanisms, the need for clarifying
legislations and guidelines is obvious. To ensure a “sustained central coordination”, clear,
participatory and transparent information channels and flows have to be established as well as
an adequate intergovernmental communication has to be ensured (Damdinjav et al 2013).
The Kenyan National Social Protection Policy (NSPP) was passed through an Act of Parliament
in May 2012, and the Draft National Social Protection Bill was submitted to the Kenyan
parliament for discussion. An intermediate National Social Protection Secretariat was set up in
2012 (Ministry of Labour, Social Security and Services 2012:6). The NSPP is based on an
assessment of the ILO, which was undertaken in 2010 and revealed that Kenya’s overall
spending on social protection was less than 2% of the GDP and furthermore criticized an
overspending on pensions for former civil servants, while an absence of general social pensions
is given. ILO strongly recommended the development of an integrated social protection policy
to approach UHC (ILO 2010).
The NSPP entails components of social assistance, social security and health insurance.
Under the latter component, the reformation of NHIF to become a comprehensive and universal
social health insurance scheme for all Kenyans is named as one crucial objective. All three
components explicitly name the inclusion of the informal sector within the social protection
strategies, aiming at universal coverage of the Kenyan population with comprehensive social
protection measures (Ministry of Gender, Children and Social Development 2011:vi/vii). On
institutional level, the establishment of the National Social Protection Council (NSPC) – with
similar agencies on county level – as well as the effective collaboration between national,
county and sub-county structures is proclaimed. The NSPC is supposed to be composed by
government entities concerned with social protection as well as None State Actors (NSAs) from
the private and development sector to complement the committee. In the NSPP, the UN/ILO
Social Protection Floor Lifecycle Approach towards social protection is named as being the
basis for the implementation of a comprehensive social protection strategy in Kenya. In this
given context, the lifecycle approach comprises social protection measures in all stages of life –

39
such as access to education and health, income security, unemployment benefits, disability
benefits as well as income security in old age (Ministry of Gender, Children and Social
Development 2011:2).
Within the strategic plan of the Kenyan Ministry of Labour, Social Security and Services
for the period from 2013 to 2017, the establishment of a Consolidated Social Protection Fund
(CSPF) is part of the main programme activities. Under key result area 2 – Social Protection
and Services – the strategies entail (2.4) Strengthening of Community Participation and – in
cooperation with World Bank, the Government of Kenya and DFID – (2.9) the Establishment of
a Strategic Institutional and legal Framework to ensure Coordination and Harmonization of the
Social Protection Sector. In 2.9, the National Social Protection Council Act and the National
Social Protection Council are named as main outputs (Ministry of Labour, Social Security and
Services 2012:56-58).
As the mentioned new developments are still in initial stages, the National Social
Security Fund (NSSF) is currently the biggest social protection fund in Kenya. It was founded in
1965 and, as a national pension and provident scheme, is mainly designed for formally
employed workers. In January 2014, the NSSF rates were adjusted to 12% of the pensionable
wages, consisting of two equal portions of 6% from the employee and 6% from the employer,
subject to an upper limit of KES 2,160 (21.6 USD) for employees earning above KES 18,000
(180 USD).20 The NSSF provides relatively high levels of coverage among formal sector
employees. In 2009, 2,143,000 formal wage employees could be identified in Kenya, out of
which 1,182,552 were NSSF members. Conversely, the informal economy – comprising of
8,200,000 workers – only 40.218 (0.04%) of them were members of the NSSF. The total
national coverage rate of the NSSF is estimated to stand at 20%. In November 2009, the NSSF
coverage was extended to employers with one to four employees. In April 2010, 101,100
employers were registered within the NSSF. As of April 2010, the cumulative membership of
the scheme was set at 4,272,853 (ILO 2010).
The Government of Kenya started implementing a Social Cash Transfer Programme for
OVCs with focus on children affected by HIV/AIDS in 2007, namely the Kenya Cash Transfer
Program for Orphans and Vulnerable Children (CT-OVC). In 2010, 100,000 households and
230,000 OVCs were reported to benefit from the programme. Eligible households – ultra-poor
and containing OVCs – are receiving a flat monthly cash transfer of 1,500 KES, equal to 21
USD (The Transfer Project 2014).
20 For more information, please refer to http://www.nssf.or.ke/new-contribution-rates.

40
Other mentionable Social Protection Funds in Kenya are the Public Disability Fund, based on a
National Policy for Persons with Disabilities, the National Policy for Older Persons as well as
the Civil Service Pension Scheme and the Occupational Pension Scheme. Other external funded
Social Protection Programmes comprise various OVC supporting programmes, the Hunger
Safety Net Programme, the Arid and Semi Arid Land (ASAL) programme in the field of
infrastructure, productive sectors, health, education security and land tenure, the People with
Disabilities/Older Persons (PWD/OP) programme, as well as several Slum-Upgrading/Low-
cost housing programmes.
In the education sector, the Government of Kenya provides free primary education and
subsidized secondary school education, while in the health sector, several Hospital Fee Waver
Programmes for Children under Five as well as Malaria- and Tuberculosis-patients are being
implemented. In addition to this, the Government of Kenya is implementing certain Economic
and Social Empowerment Programmes as well as Constituency Based Funds (Government of
Kenya 2008).
The Kenyan population faces a high burden of health care costs. Though public measures are in
place, catering for 30% of health care costs, there is still a high percentage of 50% of health care
costs that are paid out of pocket. While external donors contribute 16% to the health expenses,
only 3% of costs are paid by private health insurance schemes. 20% of the population are
insured with the NHIF – most of them are formal sector employees (Wamai 2009).
In 2002, the government designed a national SHI scheme, which was supposed to cover
the entire population. Unfortunately, the president did not approve the national scheme in
December 2004, and as a result, the National Hospital Insurance Fund (NHIF) is the only
national SHI scheme in Kenya. The national NHIF coverage stands at 20% of the Kenyan
population. The NHIF was mainly designed for formal sector employees to access IPD services.
Civil servants benefit from IPD and OPD services through the NHIF since 2012. Recently, the
NHIF launched a new insurance cover for informal sector employees – it caters for IPD services
and targets 10 Million informal sector employees (Deloitte 2011).21 NHIF-rates to enroll
voluntary or as self-employed within the NHIF – which would apply for informal sector
employees also – were set at 160 KES, which equals to 1.7 USD. In 2014, NHIF announced a
general increment of NHIF rates and set the rate for informal sector employees at 500 KES per
month, which equals 5.5 USD. The new NHIF rates have not yet been confirmed, but they
21 Deloitte (2011). Strategic Review of the National Hospital Insurance Fund – Kenya; NHIF website:
www.nhif.co.ke.

41
would – once in place – exclude large parts of the Kenyan society, not being able to afford the
increased rates of the NHIF product. Although one of the main objectives of the NHIF is to
cover the informal sector, the NHIF coverage amongst the informal sector remains low with a
coverage rate of below 3%. Hence, comprehensive social protection in health is still a main
challenge for people of low-income working in the informal sector of Kenya.
There is a mentionable landscape of CBHF schemes, implementing the mutual model of
MHI in Kenya, covering about 1% of the Kenyan population. National NGO stakeholders and
development professionals, with support of foreign donors, initiated a number CBHF schemes
in the 1980ies and 1990ies.
Numerous NGOs are supporting CBHF schemes in Kenya, the most successful ones are
the Afya Yetu Initiative (AYI) in Nyeri, Central Kenya, the Jamii Bora Trust in Nairobi as well
as the Anglican Development Service (ADS) and Support for Tropical Initiatives in Poverty
Alleviation (STIPA), implementing CBHF programmes in Nyanza Province.22 The national
organization Kenya Community Based Health Financing Association (KCBHFA) is the
coordinating and networking body on national level.23
CBHF initiatives were acknowledged in the recently published health strategy – the
KHSPP 2012-2020 – but there is no formal partnership or collaboration between the national
system and community-based initiatives yet. In the common social protection review of ILO in
2010, CBHF schemes were classified as Social Assistance Schemes, but were stated to be “very
scattered” and in need of “substantial alignment” to harmonize benefits and optimize existing
costs (ILO 2010:52). Nevertheless, CBHF Schemes were acknowledged and recognized, and it
was recommended to integrate them into the new national system, above all to complement the
existing NHIF system (ILO 2010:65).
It is worth to mention that various organizations are recently initiating alternative models
of CBHF. After common failures of various NGOs in implementing the mutual model of CBHF,
many organizations are favoring to implement the Partner-Agent-Model, where the NGO is
collaborating with a for-profit MHI scheme to provide low-cost health insurance products to the
community members. One of the most popular amongst those new approaches is the Linda
Jamii (Kiswahili for Take Care of the Family) product, that – launched in November 2012 – is a
collaboration between the commercial health insurance scheme Britam, the microinsurance
provider Changamka Microinsurance Ltd. and the mobile networking company Safaricom, to
offer low-budget health insurance to the Kenyan society. Even if considered as a
22 The case example of STIPA and its partnering CBHF schemes will be further elaborated in chapter 4.3.1.1 of this
thesis. 23 For more information, please refer to www.kcbhfa.org.

42
Microinsurance scheme, the premiums of Linda Jamii cannot be considered as affordable to
most low- and/or middle-income people in Kenya, e.g. IPD coverage for an annual premium of
200,000 KES – equal to 2,181 USD – per family. 24 Britam also offers various other
Microinsurance products, such as the Afyatele (Kiswahili for Abundant Health) and the Kinga
ya Mkulima (Kiswahili for Protection for the Farmer) products. While the Afyatele product is a
family medical cover entailing funeral support in case of death of a beneficiary and has similar
rates as the Linda Jamii product, the Kinga ya Mkulima product was specifically designed for
small-scale Tea Farmers who are members of Kenyan Tea Development Agency (KTDA).
Several other pilot projects in Microinsurance through cooperation with commercial
insurance schemes were implemented in Kenya in recent years – such as the Kilimo Salama
(Kiswahili for Safe Agriculture) crop insurance of UAP insurance and Syngenta Foundation for
Sustainable Agriculture (SFSA) in 2011, a Partner-Agent-Model,25 or the Afya Card of AAR
Insurance and Adide Foundation, offering simplified saving for health and access to other
financial services at collaborating banks.26
24 For more information, please refer to http://lindajamii.co.ke/. 25 For more information, please refer to http://kilimosalama.wordpress.com/about/. 26 For more information, please refer to http://www.adidefoundation.org/afya-card.
Figure 8: Expected Interactions between different areas of public social healthprotection in Kenya, Source: Author.

43
Another approach is undertaken by various MFIs, offering a mandatory health insurance for
their loan takers – such as the Faula Afya product27 of Faula MFI or the Jamii Bora Trust health
insurance named Afya Bora (Kiswahili for Good/Better Health). In both cases, loan takers are
exposed to a compulsory health insurance to obtain a loan and access micro-saving services. In
the case of the Jamii Bora Trust, this approach let to coverage of 500,000 non-salaried members
of the Jamii Bora Trust nationwide in 2009. Figure 8 illustrates the expected interactions
between the several Kenyan public policies in social protection and how health financing is
supposed to be fitted in the same.
27 For more information, please refer to http://www.faulukenya.com/index.php?option=com_content
&view=category&layout=blog&id=56&Itemid=70.

44
The following analysis of several integrated national SHI systems from low-income countries in
sub-Saharan Africa will serve as a basis to generate common lessons learnt in the process of
designing and establishing integrated SHI systems in countries with similar pre-conditions –
such as classification as low-income country, high poverty levels, huge informal sector, history
of public and private failure in providing comprehensive social protection and SHI measures to
the society. Furthermore, the generated lessons learnt will be used as basic indicators for the
design of a standard model for an integrated SHI system in Kenya.
To review existing integrative SHI systems, four examples – two from Eastern and two from
Western Africa – were identified to illustrate different approaches and priorities set by the
respective governments and stakeholders. After the general characterization and description of
case examples, an adjusted SWOT analysis will be carried out, which will reveal common
strengths, weaknesses, opportunities and threats in the chosen systems. To lay the focus of
analysis on health insurance specific indicators, the four SWOT categories will be furthermore
divided into the following sub-categories: (1) Design, (2) Sales, (3) Servicing and (4)
Sustainability. A common conclusion combining the outcomes from the case example analysis
will be drawn.
The SWOT analysis will provide insights into internal strengths and weaknesses of the
analyzed health systems and will reveal external threats and opportunities. As a formal
definition, the SWOT analysis can be defined as “an examination of an organization’s internal
strengths and weaknesses, its opportunities for growth and improvement, and the threats the
external environment presents to its survival. Originally designed for use in other industries, it is
gained increased use in healthcare.” (Harrison 2010:92)
Within the SWOT analysis, several steps are taken to undertake an extensive analysis
of a specific system. In step one, relevant data is gathered depending on the main objective of
the SWOT analysis, while in step two, the data will be analyzed regarding the four given
categories of strengths, weaknesses, opportunities and threats. In the third step of the SWOT
analysis, a SWOT matrix is developed and finally, in step 4, the results from the SWOT matrix
are used to analyze the entire system.

45
In the following – after a common characterization and description of the four case examples – a
comparative SWOT analysis is executed for the four different SHI systems. This analysis will
be used to generate common lessons learnt for the successful implementation of integrative SHI
systems in sub-Saharan Africa.
In this section, the four chosen case examples will be examined using different analysis
categories, being Brief Background of Health Financing Landscape (1), Legal Context (2),
Benefit Package and Premiums (3), Exemptions and Indigents (4), Population Coverage (5),
Funding (6), Provider Involvement and Provider Payment Mechanisms (7), Insurance
Education and Social Marketing (8), Management Information System and M&E (9). These nine
categories are to be considered as crucial in the effective analysis of common strengths,
weaknesses, opportunities and threats, as they strongly determine the success of an integrated
SHI system.
Brief Background of Health Financing Landscape
In Tanzania, high OOPP are still a reality for most people, representing 83.4% of private
expenditures (Rogers-Witte et al 2009). Furthermore, OOPP are contributing a percentage of
47% to the overall health expenditures due to the introduction of user fees in 1993 (Mtei and
Mulligan 2007). Particularly women and children are suffering from the lack of adequate social
protection measures and access to essential health care. In 2006, the national infant mortality
rate was set at 68 per 1.000 live births, while the maternal mortality rate stood at 578 per
100,000 live births (WHO 2006). Furthermore, most common causes of death for children under
five years are preventable or treatable diseases, such as Malaria with 23% and Pneumonia with
21% (WHO 2006). As a result, a huge demand for adequate social protection measures in health
is given countrywide.
At present, several public SHI schemes are to be found in Tanzania, namely the
mandatory scheme for civil servants, the Tanzanian National Health Insurance Fund (TNHIF),
and a mandatory scheme for employees of the formal sector, the National Social Security Fund
(NSSF) (Humba 2005). The TNHIF covers a small percentage of the Tanzanian population
only. In 2003, the TNHIF membership was estimated to be at 5.4% (United Republic of
Tanzania 2003). Coverage through the NSSF was estimated to be even lower, as in 2005, only
9.000 NSSF members could be identified nationwide (GESS 2011). In addition to the named
SHI schemes, few private for profit health insurance schemes are available. Their products are

46
usually not affordable for the majority of the population, being informal workers or farmers. At
the same time, they are not tailored to the specific needs of low-income people, working
predominantly in the informal or rural sector. As a result, an adequate coverage of illness-related
risks amongst the population is not given. The ILO estimated the percentage of people
benefiting of social health protection at only 1% of the entire population including 6.5% of the
formal working population (GESS 2011).28
Due to this lack of social health protection measures for informal workers and people
with low and/or irregular income, district-based prepayment schemes were established to secure
better access to health care services. The Community Health Funds (CHF) evolved in 1996 as an
initiative of the Government of Tanzania and the World Bank. The CHF were part of the
national Health Sector Reform (HSR) that was initiated in 1993 by the Ministry of Health and
Social Welfare (MoHSW). The CHF Act from 2001 provides the legal context for local districts
to implement and manage their own district-based CHF schemes. In 1996, local CHF schemes
were initially introduced in few pilot districts (Mtei and Mulligan 2007). In addition, an urban
equivalent to the CHF was designed, the Tiba Kwa Kadi (TIKA) initiative. TIKA was
established in a similar way as the CHF and is aiming at covering the urban population of
Tanzania, while the CHF is concentrated on the rural population.29
28 This number differs from recent data gathered by the TNHIF showing that different CHF at least cover 7.9% at
national level. Nevertheless, the national coverage has to be regarded as low according to the public commitment of the government aiming at reaching at least 30% of the population.
29 Currently, TIKA is implemented in Dar-es-Salam with support of the TNCHF, please refer to TNCHF 2010.
Figure 9: Health financing landscape in Tanzania, Source: Author.

47
In 2006, 68 district councils with operating CHF comprising approximately half of the existing
districts in Tanzania could be identified (Kiwara et al 2006). Figure 9 illustrates the health
financing landscape in Tanzania.
Organizational and Institutional Structure
In 2009, a three-year plan was developed by the Government of Tanzania, which transferred
main management competencies of the CHF to the Tanzanian National Health Insurance Fund
(TNHIF). Prior to the reform, the CHF and the TNHIF were managed separately. The CHF was
managed under the HSR governance structures of Ministry of Health and Social Welfare, while
the TNHIF was a mandatory SHI scheme serving the formal sector, and equally reporting to the
Ministry of Health and Social Welfare. The common reform in 2009 to harmonize the
governance structures of both insurance schemes had the overall objective of approaching UHC
by extending the coverage of the CHF through an increased visibility, and to improve general
efficiency and supervision of both systems through the central government (Ifakara Health
Institute 2012). In a Memorandum of Understanding (MoU), which was signed by the CHF, the
TNHIF and the Prime Minister’s Office for Regional Administration and Local Government, it
was agreed to transfer main management responsibilities of the CHF to the TNHIF over a period
of three years. Figure 10 illustrates the reformed CHF governance structure.
Since 2011, an improvement in reporting systems and awareness about the national system was
observed, while the general top-down approach and challenges in the information and
communication flows were stated to be remaining challenges of the hybrid system.
Figure 10: CHF structure on national level after the governance reform from 2009, Source: Adjusted from Ifakara Health Institute 2012.

48
The management of the CHF on district level – which is mainly executed through CHF agents,
based in each contracted health facility, where they cooperate with the Health Facility
Governance Committees, as well as CHF promoters that are engaged in on-site community
mobilization – was not changed during the reform and remained as initially defined in the CHF
Act of 2001 and illustrated in Figure 11 (Ifakara Health Institute 2012).
Legal Context
The CHF is legally based on the Community Health Fund Act (2001), which has the following
objectives: (1) to mobilize financial resources from the community for provision of health care
services to its members, (2) to provide quality and affordable health care services through
sustainable financial mechanisms, and (3) to improve health care services management in the
communities through decentralization and by empowering the communities in making decisions
and by contributing on matters affecting their health. The Community Health Fund Act is
embedded in the wider context of the Tanzania National Health Policy with the common
objective of improving the wellbeing and health of all Tanzanians, especially focusing on risk-
exposed and vulnerable people and groups. The Tanzanian National Strategy for Growth and
Reduction of Poverty also serves as a basis for the CHF implementation, as its objective is to
create equity in the provision of health care and social services delivery (Mtei and Mulligan
2007).
Figure 11: CHF Management Structure on District Level as per CHF Act (2001), Source: Adjusted from TNCHF 2006.

49
Benefit Package and Premiums
The CHF membership is voluntary and each household is supposed to contribute an equal
amount of membership fee as agreed by the respective communities. In targeted studies about
the willingness to pay for the CHF, the premium rates ranged between 3,000 and 10,000 TZS
being an equal to 1.68 and 5.60 USD (Mtei and Mulligan 2007). Currently, members are paying
between 5,000 and 30,000 TZS being an equal to 2.80 and 16.80 USD (Ifakara Health Institute
2012).
Exemptions and Indigents
The CHF acknowledges vulnerable parts of the society and emphasizes the importance of
adequate identification of indigents who are supposed to access the CHF without a monetary
contribution. Each district is supposed to identify specific individuals and/or groups to be
exempted from premium payment towards the CHF. In practice, the applied waiving
mechanisms are considered as very complex and most community members are not able to
understand and fully embrace them, which led to the fact that many districts could not identify
vulnerable parts of their target community and hence could not design adequate waivers
(Ouedraogo 2012, Mtei and Mulligan 2007).
Population Coverage
In the first two years of the 2009 reform aiming at linking the governance structure of the CHF
and the TNHIF, the coverage of the CHF increased from 92 to 111 districts and from 2% to 5%
national coverage rate. The CHF coverage mainly increased in rural areas (Ifakara Health
Institute 2012). So far, amongst existing SHI schemes in Tanzania, solely the CHF reaches out
to informal workers and people of low income.
Funding
The CHF – besides receiving membership contributions in form of premiums – is funded by a
Public Matching Grant, through which the government is topping up all contributed premiums
by members in a percentage of 100%. 25% of this matching grant is supposed to support the
partnering health facilities in improving the quality of services of their facilities. Furthermore,
international donors and development partners are contributing to the funding of the CHF
system. The district council is meant to contribute to the CHF by funding specific pro-poor
measures of the CHF. Figure 12 illustrates the funding structure of the CHF system.

50
Provider Involvement and Provider Payment Mechanisms
As the CHF district structure is located within the partnering hospitals, health providers play a
major role in the CHF system. Hospitals as part of the CHF receive direct tax-based funding
through the government and can also access a minimum of 25% of the public matching grant
that is channeled through the local CHF accounts, which were established in each district.
Insurance Education and Social Marketing
Within the integrated TNHIF/CHF system, regional and district medical officers as well as other
local authorities are supposed to take lead in mobilizing the respective target communities and
sensitize them on the insurance concept as well as the integrated governance approach of the
TNHIF and the CHF. Besides this guideline, the CHF units are not receiving any training on
insurance education or social marketing. Campaigns on national level to promote the nationwide
system are rare.
Management Information System and M&E
A comprehensive Insurance Management Information System (IMIS) in certain piloting regions,
such as the Dodoma Region covering seven districts, was established with support of the Swiss
Tropical Institute for Public Health (Swiss TPH). The IMIS is meant to provide “a
comprehensive solution for data management, including membership enrolment through mobile
phone technology, contribution management, claims processing and payment, as well as
member feedback collection” (Swiss TPH 2013). Within the IMIS, locally recruited enrollment
officers persecute enrollment to the CHF. The enrollment officers capture the details of the
members and take their photos, using a low-cost mobile smartphone, and send this information
directly to the central database of the IMIS (MIA 2012).
Figure 12: Funding of the CHF system, Source: Adjusted from Hennig 2012.

51
The Swiss TPH developed innovative cards, which are part of the IMIS, which is IT-based and
operational online or offline. The card allows members to use their cards in all CHF partnering
health facilities, a main innovation that was added by the IMIS. Through a partnership with the
mobile network provider Vodacom, the CHFs are provided with free access to the Internet, as
well as to free text message communication between different enrolment officers of CHF
entities, the central IMIS database and the health facilities (Swiss TPH 2013). The IMIS is
providing a useful basis for data management and collection and is designed with appropriate
features to be rolled out nationwide. Nevertheless, at the end of the piloting phase in January
2015, further funding for maintaining and expansion of the IMIS remained uncertain. Moreover,
comprehensive measures for conducting comprehensive monitoring and evaluation measures
within the CHF system are neglected within the IMIS.
Brief Background of Health Financing Landscape
The Government of Rwanda followed the common guidelines from the Bamako Initiative
towards ensuring access to primary health care and community empowerment in 1988 by
decentralizing the health system to provincial and district levels. These efforts were interrupted
by the devastating Genocide of 1994, which badly affected the whole country on various levels,
including the health system. In post-Genocide-times, the government put efforts in restructuring
the health system and continued the decentralization process to provincial and district levels
aiming at increasing the utilization rates and improving the overall health status of the
Genocide-affected society. The public policy of Health for All was threatened by a common
under-supply of most essential resources – such as drugs, infrastructure and health personnel –
leading to an introduction of user fees in the same year of 1994. The user fees-oriented policy
led to an under-usage of health care services decreasing to 23%, while the prevalence rates of
HIV/AIDS and other infectious diseases rose up (Kayonga 2007).
In 2001, the Government of Rwanda decided to undertake a radical turn from the failed
user fees policy to a support of CBHF initiatives, which were established nationwide as a
reaction of the unbearable user fees in the 1990ies. Innovative elements of the new public health
policy in Rwanda were (1) the focus on public investment in preventive measures towards
preventable diseases – preventive measures were offered free of charge – (2) the focus on access
to curative care through community-based pre-payment schemes, and (3) the introduction of
performance-based financing of involved health care providers to ensure a high quality of care
(Kayonga 2007). The so-called Programme de Développement des Mutuelles de Santé is one
crucial element of the Rwandan health reform that considered CBHF schemes as main providers

52
of health insurance to the Rwandan society. The public supporting programme of Mutuelles de
Santé is complementing the national SHI scheme, namely the Rwandaise d’Assurance Maladie
(RAMA). As a result, the Government of Rwanda subsidizes preventive services, while curative
services are provided through CBHF schemes.
The government of Rwanda considers CBHF schemes as “a transitory path towards a unified,
public social health protection scheme”, while the Rwandan Social Security Board is acting as
an umbrella organization to the entire system. Existing private insurance schemes are covering
parts of the population, which are able to access higher income levels (MIN 2014). Since
September 2012, Rwanda was recognized as one of the nine countries in Africa and Asia
making significant progress to make UHC possible (Nyandekwe et al 2012).
Organizational and Institutional Structure
Under the stewardship of the Ministry of Health of Rwanda, the Mutuelles de Santé are
managed at the community level by elected community members. Each Rwandan sector is
covered by one Mutuelle de Santé and comprises of averagely 50,000 people. One district
entails up to five sectors and five Mutuelles de Santé (Kayonga 2007). The Mutuelles de Santé
are considered as “payers” within the SHI system of Rwanda, as they provide required fees for
services at the different levels of health providers.
As illustrated in Figure 13, besides the Mutuelles de Santé, other crucial actors and institutions
contributing to the fees within the Rwandan SHI system, namely the Rwandan Health Care
Figure 13: Rwandan SHI system, Source: Adjusted from Bump 2010.

53
Insurance, the Genocide Survivors Support Fund, the Military Health Insurance as well as
various commercial private health insurance schemes (Bump 2010).
Legal Context
Several legal documents, policies and guidelines are building the basis for the Rwandan SHI
system. The long-term strategy of the Government of Rwanda – Vision 2020 – has a clear focus
on strategic social protection through universal access to health care. It was established in 2000.
In 2004, the first legal document for a national regulation of Mutuelles de Santé came into force,
namely the Rwanda's Politique Nationale de Développement des Mutuelles. Furthermore, the
Law Nº 62/2007 of 30th December 2007, promulgated in March 2008, introduced the mandatory
element of the Rwandan SHI, based on Mutuelles de Santé, stating that each Rwandan resident
must be affiliated to a health insurance scheme that provides quality health care. Two other
policies followed in 2010, being the Rwanda Community Based Health Insurance Policy and the
Rwanda National Health Insurance Policy (Nyandekwe et al 2012).
Benefit Package and Premiums
As a result of financial constraints of public funds, the system in Rwanda offers a universal
minimum benefit package (MIN 2014). Each individual in Rwanda as part of a health insurance
scheme is entitled to access this Minimum Package of Activities (MPA), while it can be
complemented with the Complementary Package of Activities (CPA). The MPA covers services
and drugs provided at health centers including pre- and post-natal care, vaccinations, family
planning, minor surgical operations, and essential and generic drugs, while the CPA covers
certain services at the district hospitals, including IPD care, caesarian sections, minor and major
surgical operations, medical imaging, and diseases affecting children under the age of five years.
The premium ranges between 2,000 RWF and 7,000 RWF being an equivalent to 3.34 USD and
11.69 USD, dependent on the different Ubudehe categories, which will be further described in
the next paragraph.
Exemptions and Indigents
The Rwandan Health System considers vulnerable parts of the society as indigents and supports
them based on the principles of equity and inclusion. In the financial year of 2011/2012, 24.8%
of the population within the Rwandan SHI system was classified as indigents, which is
responding well to the general indication of 24.1% of the population living in extreme poverty
in Rwanda.

54
The Rwandan system uses Ubudehe categories to identify the most-needy parts of the
population. Ubudehe can be translated to “mutual assistance”. In the Ubudehe approach, the
community is classified in six different categories. The categories are set through a participatory
process by the community members. The different categories and respective percentages of the
Rwandan population within the Rwandan SHI system are illustrated in the following Table 2:
Ubudehe Category Population Coverage Premium
Group 1: Very Poor
Category (Ubudehe
category 1 and 2)
24,8% RWF 2,000 (USD 3.34)
Group 2: Poor Category
(Ubudehe category 3 and 4)
68,8% RWF 3,000 (USD 5)
Group 3: Rich Category
(Ubudehe category 5 and 6)
2,17% RWF 7,000 (USD 11.69)
Table 2: Ubudehe categories of Rwandan SHI system, Source: Rwanda National CBHI Policy 2010.
Population Coverage
In 2014, the Rwandan SHI system covered 94.1% of the Rwandan population. The coverage
rate increased from 7% in 2003 to 74% in 2007 and to 94.1% in early 2014 (Nyandekwe et al
2012). The Mutuelles de Santé are responsible for increasing their respective membership base,
to maintain re-enrollment, carry out insurance education and social marketing activities as well
as to verify the number of active members in each household, and collect premiums. Common
outreach campaigns are usually done at the community level using church forums, and radio
broadcasts (Joint Learning Network on Universal Coverage 2014).
Funding
55% of the Rwandan SHI system is financed through member contributions, while other public
social insurance funds, external development partners, donors and/or NGOs and charitable
organizations fund the remaining percentage. MFIs are providing loans for those parts of the
population who cannot afford to pay the standard premium and were not classified as indigents
as per the first and second Ubudehe category. The contributions to the Mutuelles de Santé are
pooled on different levels – on community level for primary care, on district level for secondary
care, and on national level for tertiary care (Kayonga 2007).
Provider Involvement and Provider Payment Mechanisms
Partnering health facilities are private and public not-for-profit hospitals and health centers,
while for-profit health providers are not considered within the system. The principle of

55
performance-based payments of the health facilities was maintained within the compulsory SHI
system in Rwanda (Joint Learning Network on Universal Coverage 2014).
Insurance Education and Social Marketing
Within the Rwandan Policy of Supporting Mutuelles de Santé to approach UHC, the
responsibility to carry out comprehensive measures in the areas of insurance education and
social marketing is transferred to the Mutuelles de Santé at sector level. Due to several national
policies in place manifesting the mandatory element of the Rwandan SHI, the level of public
awareness of the system is very high.
Management Information System and M&E
The Health Management Information System (HMIS) of the Government of Rwanda was
upgraded to a web-based system in January 2012. Former assessments of the HMIS (e.g. by
USAID in 2006), revealed a low level of human capacities to operate the system, crucial
information limits within the HMIS as well as issues regarding the fitting-in of the HMIS into
the ongoing decentralization process (USAID 2006). The newly introduced Rwandan Health
Management Information System (R-HMIS) is based on open source software, namely the
DHIS-2. According to the Government of Rwanda, over 700 data managers and monitoring and
evaluation staff have been trained on the usage of the system, which is accessible online for
authorized users (Government of Rwanda 2012). The R-HMIS comprises an information system
for community health workers – the so-called SIScom – as well as reporting system for the
Mutuelles de Santé based on monthly indicators (Government of Rwanda 2012). The R-HMIS
has been in operation from February 2012 and connects over 700 health facilities as well as
collects data from the same. In 2013, also private clinics were joining the system. The system –
through certain modules – is supposed to monitor the overall performance of the Rwandan
Health sector, including the Mutuelles de Santé and is hence providing a basis for
comprehensive data management and collection (Management Sciences for Health 2013).
Brief Background of Health Financing Landscape
In Burkina Faso, less than 10% of the population had access to any measure of social protection
in health. Mutuelles de Santé traditionally provide access to health care financing for the
informal sector. The first Mutuelle de Santé in Burkina Faso was established in 1963 (Ministère
de la Fonction Publique, du Travail et de la Sécurité Sociale 2014). Public social protection and
SHI measures – e.g. through the Caisse Nationale de Sécurité Sociale (CNSS), the Caisse

56
Autonome de Retraite des Fonctionnaires (CARFO) and the Office de Santé de Travailleurs
(OST) – are designed to serve the formal sector (Ouedraogo 2012).
The number of community-based institutions for mutual help and social assistance,
namely the Mutuelles Sociales, emerged from 64 in 2000 to 205 in 2011. 63.9% out of the 205
institutions are Mutuelles de Santé, while others are simple cost-sharing or prepayment schemes
(Solidarité Socialiste 2011). The local NGO ASMADE supports 19 Mutuelles de Santé
nationwide, serving around 30,000 beneficiaries. The number of people that are aware about the
operations of mutual health schemes in Burkina Faso was estimated at 1,000,000.30
ASMADE is representing the mutual health schemes in the public committee developing
the Assurance Maladie Universelle (AMU), a comprehensive national SHI scheme, intending to
cover the entire population of Burkina Faso. The process of developing a national SHI scheme
was initiated in 2008 with a Comité du Pilotage, comprising different stakeholders, such as
government entities concerned with social protection in health, the Cadre de Concertation des
Structures d’Appui aux Mutuelles (CCSAM) – a support network to mutual health organizations
– and health providers. In the initial stage of the AMU, as part of the piloting committee, the
mutual health schemes occupied important roles, such as coordination of activities, providing
technical advice and availing relevant data from their practical field experiences.
The Partners in Health network, supported by the WHO, initiated the finalization
process of the AMU in 2013. A strategic document was published which illustrated major steps
to be taken until 2015, including the completion of the design of the system, the participation in
different exchange forums about the AMU implementation, the establishment of the overall
management body of the AMU, the design of appropriate piloting activities, the establishment
of an appropriate number of Mutuelles de Santé, as well as general capacity building measures
in institutional and systematic areas of the AMU (Ministère de la Fonction Publique, du Travail
et de la Securité Sociale 2013:6).
In October 2014, following a civil uprising of the society Burkinabè, the former
President, Blaise Compaoré, was removed from executing his power. Due to the emerging
political tension, the implementation of the AMU delayed and up to January 2015, no significant
step of AMU implementation could be observed.
Organizational and Institutional Structure
The general secretariat for implementation of the AMU was established in 2009. Mutuelles de
Santé supported the secretariat with technical inputs as well as the coordination and
30 For more information, please refer to http://www.ongasmade.org/index.php?option=com_content
&view=article&id=62:promotion-de-la-sante&catid=39:nos-domaines-dintervention&Itemid=90 .

57
management of potential and de-facto partners. Potential roles of the CBHF schemes were
agreed to be located in the areas of mobilization and member recruitment, premium collection,
management of effective risk coverage and social control (Solidarité Socialiste 2011).
While in the initial AMU development model from 2008, different target groups were to
contribute to different mutual structures – such as informal sector employees were to contribute
to mutual health organizations, while subsistence farmers and identified indigents were to
contribute to specialized structures supported by public social assistance programmes – a
revised model in 2011 considered to pool resources from the informal sector, subsistence
farmers and identified indigents together in a common pool of CBHF schemes, as illustrated in
Figure 14. The CBHF schemes are expected to pool resources at community level and further
contribute to a regional pooling with specific contributions. The formal sector would be covered
by the AMU through the CARFO and the CNSS (Solidarité Socialiste 2011). While the
membership in the AMU would be mandatory for the formal sector, the membership in one of
the Mutuelles de Santé as part of the AMU would be voluntary in the revised AMU model. The
CNAM is considered as the overall managing body of AMU as both, the mandatory and the
voluntary health insurance, will be pooled together at national level in the CNAM framework
(Solidarité Social 2011).
Further crucial actors within the envisioned structure of the AMU are the health providers,
responsible for the claims management, as well as the technical assistance platform comprising
development partners and national research institutions, as illustrated in Figure 15. The AMU
Figure 14: The AMU in Burkina Faso, Source: Author.

58
system is supposed to be connected by a comprehensive management information system on all
involved institutional levels.
Legal Context
There was no legal framework for the Mutuelles de Santé in Burkina Faso developed yet. Since
2008, several stakeholders, such as the Westafrican regional network of mutual health
organizations – La Concertation – with support of GIZ and the ILO – are aiming at establishing
a comprehensive law for Mutuelles Sociales for the UMEOA region, but so far their efforts were
futile. Envisioned is a general legal framework for Mutuelles Sociales, with a focus on
Mutuelles de Santé. Legally binding rules and regulations for the Mutuelles de Santé are to be
considered as crucial within the AMU system, as the coverage of the informal sector is solely
based on their efforts.
The development of the AMU was furthermore embedded in different strategic plans of
the Government of Burkina Faso, such as the Stratégie Croissance Accélérée et du
Développement Durable (SCADD), that was implemented from 2001 to 2015. Initial steps of
the AMU development were moreover based on certain components of the Plan Nationaux de
Développement Sanitaire (PNDS), which has been implemented in the years 2001 to 2011
(Ministère de la Fonction Publique, du Travail et de la Securité Sociale 2013).
Benefit Package and Premiums
The envisioned AMU benefit package is a universal basic package of benefits accessible. The
so-called Paquet de Base is supposed to cover essential health services and medication.
Figure 15: Institutional Structure of the AMU, Source: Author.

59
Exemptions and Indigents
Vulnerable parts of the society that are considered as indigents in the AMU are classified under
the informal sector as well as the agricultural, agro-pastoral and agro-forestry sector. These
sectors are supposed to be covered through the voluntary health insurance provided by
Mutuelles de Santé. There is no clear process yet to identify indigents within the AMU, and it is
not part of the strategy of the Partners for Health network and WHO support.
Population Coverage
The AMU is supposed to cover the whole population of Burkina Faso, with different institutions
covering different groups of the society. The overall objective is UHC using a multi-level
approach to meet different needs of different parts of the society. The two components of the
AMU – namely voluntary (1) and mandatory (2) health insurance – are aiming at meeting the
different needs of the informal (1) and formal sector (2) through adequate institutions, like the
Mutuelles de Santé (1) and the CNSS and CARFO (2). It is envisioned to cover 10% of the
population in 2015, 40% in 2020 and the final UHC rate of 100% in 2025 (Le Faso 2013).
Funding
As illustrated in Figure 16, the funding of the AMU will be managed on different levels,
according to the different institutions and entities involved. The collected premiums from the
Mutuelles de Santé would be pooled on community level for the individual Mutuelles, as well as
on regional level, before contributing to the national pooling under the umbrella of the CNAM,
the overall managing body of the AMU. The CNAM will receive funding from a consortium of
technical and financial partners, amongst them the WHO and the Partners for Health network,
that have been supporting the AMU implementation from 2011.
Figure 16: Funding of the AMU, Source: Author.

60
Provider Involvement and Provider Payment Mechanisms
Health facilities, ranging from the first level of Centres de Santé et de Promotion Sociale
(CSPS) and Centres Médicaux avec Antennes chirurgicales (CMA), the second level of Centres
Hospitaliers Régionals (CHR), and the third level of Centres Hospitaliers Universitaires
(CHU), are considered in the AMU as contracted providers of quality health care. As illustrated
in Figure 15, the health providers are invoicing the different institutional levels of the AMU
system, namely the CNAM at national level, the different institutions delivering voluntary and
mandatory health insurance on regional and community level, as well as the CNSS and CARFO,
who receive the pooled resources of the formally employed.
Insurance Education and Social Marketing
Within the envisaged AMU, Mutuelles de Santé are engaged in the areas of insurance education
and social marketing. So far, while many Mutuelles de Santé show adequate skills to implement
efficient measures in these two crucial areas of implementation of SHI, most Mutuelles de Santé
in Burkina Faso are considered as weak institutions suffering from low levels of visibility. This
is due to the fact that Mutuelles de Santé usually do not possess enough means to carry out large
marketing or awareness creation campaigns, while other stakeholders within the AMU do not
have the skills and capacity to provide efficient measures leading to an increased level of
insurance literacy. A general knowledge exchange and mutual support would be needed to
complement existing technical and financial capacities.
Management Information System and M&E
Within the envisaged AMU in Burkina Faso, a comprehensive Système d’Information (SI) will
be implemented. The SI would connect the different AMU stakeholders, such as the CNSS and
the CARFO as well as the Mutuelles Sociales. The SI will also be a crucial element in
connecting the voluntary and mandatory components of the AMU. The involved health facilities
will access the SI and all AMU stakeholders will access the central database that will be hosted
by the technical assistance platform. Besides connecting the various actors within the AMU to
each other, the SI is supposed to be used for common data collection, which will allow
measuring the performance of the system. The SI is hence combining aspects of data
management as well as M&E (Solidarité Social 2011).

61
Brief Background of Health Financing Landscape
In Ghana, community based mutual health organizations show a high level of historic tradition,
just as in the neighboring country of Burkina Faso. The CBHF schemes emerged as a reaction to
the “cash-and-carry”-system that was introduced in 1985 (Singleton 2006). This system was
initiated after a general failure of post-Independence welfare practices aiming at providing UHC
through a socialistic approach – the “Nkrumah Ideology” (Dietrich-O’Connor 2010). Through
the support of the Danish International Development Agency (DANIDA), the number of CBHF
schemes grew from 44 in 1997 to 44 in 2001 and 159 in 2002.
In the area of considering CBHF schemes as part of a national SHI system, Ghana – just
as the already illustrated examples of Tanzania and Rwanda – can be seen as a pioneer in the
context of sub-Saharan Africa. The Government of Ghana started implementing an integrative
SHI system in 2003 by passing the National Health Insurance Act (NHIA). Through the
establishment of the National Health Insurance Scheme (NHIS), the Government of Ghana
aimed at a comprehensive integration of existing CBHF schemes and furthermore at establishing
District-wide Mutual Health Insurance (DWMHI) schemes in all districts of Ghana. In this
process, 168 DWMHI schemes were established. CBHF schemes which did not meet certain
standards or which were not willing to be incorporated within the public NHIS structure of the
NHIS, have been in existence alongside to the newly established DWMHI schemes. To become
part of the NHIS structure, only one mutual health scheme was allowed per district, which had
to ensure a minimum membership of 2,000 members (Dietrich-O’Connor 2010), which most
existing CBHF schemes could not provide. Besides the DWMHI schemes, private mutual health
insurance schemes and private commercial health insurance schemes are acknowledged under
the NHIS, while the two latter ones only cover around 1% of the Ghanaian Population (Gajate-
Garido and Owusua 2013).
The Government of Ghana aimed at achieving UHC in 2008 through the NHIS – five
years after its establishment. Evidence has shown that – if current strategies will be continuously
followed – it would take up to 2076 to achieve the ultimate goal of UHC. Studies furthermore
revealed that administrational challenges, such as delays in settlements of bills or provision of
membership cards, resulted in a general mistrust amongst the population of Ghana towards the
NHIS. In this context, contracted NHIS health facilities started to reject NHIS members because
the NHIA delayed the claim settlement in an extensive manner. This resulted in (1) an increased
number of OOPP by the population including NHIS members, and (2) a higher frequency of
clients in those health facilities that are still accepting NHIS members. The latter resulted in

62
long waiting hours and a general shortage of drugs in the few health facilities that still accepted
NHIS members in early 2014. Nevertheless, significant impact of the NHIS on access to quality
of care and health care utilization in general was measured and acknowledged by recent studies
(Gajate-Garido and Owusua 2013).
Organizational and Institutional Structure
The NHIS is managed and controlled by the Ghanaian National Health Insurance Authority
(GNHIA) and the National Health Insurance Council (NHIC) who are in charge of national
overseeing and governance of the implementation of the national SHI policy. The NHIC is the
main implementer of the NHIS and is equally responsible for providing subsidies, reinsurance
and technical support to the system. The NHIC also manages the NHIS funds as well as
registers, licenses, regulates the DWMHI schemes and determines the premiums. Moreover, the
NHIC is responsible to accredit grants to health providers and promote health education.
As illustrated in Figure 17, the DWMHI schemes are directly reporting to the regional
offices of the central government and are not allowed to partner with any other health scheme or
entity on community level. Due to the centralized system, the DWMHI schemes do not possess
any flexibility in monetary terms.
Figure 17: Organizational Structure of the NHIS, Source: Adjusted from Boateng 2007.

63
Legal Context
The NHIS was introduced based on the NHIA from 2003. By passing the National Health
Insurance Bill in the same year of 2003, it was declared, that “each resident in Ghana belong to
the National Health Insurance Scheme.” While this statement can be considered as introducing a
mandatory element of the NHIS, national coverage still remains low and is currently estimated
below 50%. Some stakeholders even estimated the coverage as low as 18% (Oxfam
International 2011).
Benefit Package and Premiums
The basic benefit package of the NHIS is relatively comprehensive as compared to other
national schemes and it is supposed to cover about 95% of all health problems reported in local
health facilities. There is a significant emphasis on female reproductive health to be noted
within the benefit package as well.31 Not covered under the NHIS basic benefit package is
specialized care, such as dialysis and organ transplants. ARV treatment is supposed to be
covered by a separate government program targeting People living with HIV and AIDS (Joint
Learning Network on Universal Coverage 2014).
NHIS premiums are to be paid based on the income of the respective NHIS member and
the premium levels are ranging from 7.20 and 48 GHS being an equal of 2.22 and 14.8 USD.
People of low-income and/or working in the informal economy are not considered as indigents,
but are supposed to pay a standard annual premium between 8 to 12 GHS being an equivalent of
2.48 and 3.71 USD. De facto, only low-quality drugs are covered by the NHIS, which leads to
the fact that most NHIS members pay for high quality drugs out of pocket.
Exemptions and Indigents
The NHIS comprises exemption mechanisms for specific parts of the society. These
mechanisms comprise of formal sector employees contributing to the Social Security and
National Insurance Trust (SSNIT) and SSNIT pensioners, people under 18 and over 70 years
old, as well as pregnant women. Nevertheless, only 2% of the Ghanaian population was covered
under the NHIS indigent section in 2013, while an estimated 30% are living below the poverty
line (Gajate-Garido and Owusua 2013). The indigents are considered insufficient, which led to a
common exclusion of the poor and very poor population segments.
31 The maternity benefits include antenatal care, caesarean sections, and postnatal care for up to six months after
birth. Treatment for breast and cervical cancer are included in the package, while treatment for other cancers is not covered.

64
Population Coverage
The integrative NHIS system achieved national coverage of 50% in 2007 (Boateng 2007), and
increased its coverage rate to 67.5% in 2009. Assuming that the latter number was gathered in a
cumulative way, a significantly lower level of coverage rate of 33% was reported in 2011
(Gajate-Garido and Owusua 2013:1).
Funding
As illustrated in Figure 17, the funding of the NHIS system evolves from seven different
sources being a general Value Added Tax (VAT) levy of 2.5% (1) and a social security
contribution (2), while exemptions are funded by the Ministry of Finance through resources for
indigents (3). Furthermore, certain parliamentary allocations (4) are contributing to the NHIS, as
well as investment returns (5), voluntary grants, donations (6) and the common member
contributions (7), ranging from 7.20 and 48 GHS being an equal of 2.22 and 14.8 USD (WHO
2010).
Provider Involvement and Provider Payment Mechanisms
As of December 2009, 966 private and 1,368 public health providers as well as 163 health
providers established by the Christian Health Association of Ghana (CHAG) were contracted
within the NHIS. Due to the introduction of unified tariff lists through the GNHIA, there was an
enormous cost increase in 2009/2010. Nevertheless, contracted hospitals were observed to
benefit from the new tariff lists as they are increasingly campaigning to treat NHIS-covered
patients.
Insurance Education and Social Marketing
In the Ghanaian NHIS system, a close involvement of District Chief Executives (DCE) and
district assemblies within the operations of the DWMHI schemes can be observed. The same
stakeholders are involved in marketing measures concerning the NHIF. Standardized
educational materials about the NHIS are in place, which are distributed in the target
communities. Other strategies in the area of social marketing of the NHIS are door-to-door
campaigns, education sessions in churches and mosques, community durbars and social
gatherings, as well as the use of radio broadcasting and video shows on community level
(Asenso-Boadi and Agbeibor 2010).
Management Information System and M&E
The NHIF is centrally managed by the GNHIA in the capital city Accra. The GNHIA deployed
an IT-based infrastructure for the provision of insurance services to the nation. All NHIS

65
contracted healthcare providers are accessing a common ICT platform with standard protocols
for patient’s authentication and claims management (Achampong 2012). Efforts were taken
towards a further harmonization of tools used on the district level, resulting in a standard tool
for NHIS membership registration and renewal as well as a module for claim management,
containing standardized claim forms (Owusu-Asamoah 2012). Future plans of the GNHIA are
underway to deploy an online claims management system. Currently, the IT platform for the
NHIS does not support any shared services. It meets only the NHIS business processes and
needs.
Regarding a comprehensive Health Management Information System (HMIS) for
Ghana, various pilot projects were implemented without adequate coordination amongst each
other. As a result, two main applications of the developed HMIS are used for common
information management within the NHIS. The first application supports the management of
clinical business processes, while the other application supports the general data collection and
reporting within the NHIS (Achampong 2012).

66
In the following, a comprehensive SWOT analysis is presented, based on the above-described
social health financing approaches from Tanzania, Rwanda, Burkina Faso and Ghana.
The Tanzanian system of decentralized CHF units, which shows a clear objective of targeting
the informal sector, has various significant internal strengths to be mentioned. The
comprehensive coverage is ensured through the combined governance structure of the CHF and
the TNHIF, which targets members of the formal and informal sector and meets their specific
needs (Ifakara Health Institute 2012). In the area of sales, many local CHF units make use of
the decentralized structures of the government and involve regional and district medical officers
as well as local authorities and chiefs in the common marketing of the CHF (Swiss TPH 2012).
Through the commitment and support of these stakeholders in sensitization of the target
communities, the public good will and political commitment is visible.
The offered CHF product comprises of curative and preventive health services at health
providers of different levels and shows a high level of comprehensiveness (Ifakara Health
Institute 2012, Rogers and Witte 2009). The public matching grant ensures a certain level of
sustainability of the entire system, as it does not rely on external funding or premium
contributions only, but has a strong public financing component (Mtei and Mulligan 2007,
United Republic of Tanzania 2003, WHO 2006).
Internal weaknesses of the Tanzanian System can be observed in the area of standards
and harmonization, as the two systems of CHF and the TNHIF are not yet fully integrated and
interlinked which each other. The general approach of the Government of Tanzania is top-down
as the entire system is still supervised and controlled by the central government with only minor
decision-making authorities on district level, leading to a low level of community participation
and/or involvement. Due to the low level of experience in serving the informal sector of the
TNHIF, the overall coverage remains low with most districts not expanding 15% of coverage
through the CHF/TNHIF system (Ifakara Health Institute 2012, GESS 2011, TNCHF 2010). In
addition to this, there is an over-reliance on district structures and a non-existence of appropriate
community-based structures, resulting in a limited involvement of crucial stakeholders, e.g. the
communities themselves, but also NGOs or other private social support structures (Kiwara
2007). The identification of indigents within the Tanzanian TNHIF/CHF system was rated very
complex and not transparent and is not well understood and/or accepted amongst the target
communities. Furthermore, it results in a common exclusion of needy people to access indigents
within the system (Mtei and Mulligan 2007).

67
In terms of social marketing, the measures in place a very limited, which might be one reason
for the low coverage of the overall SHI system. The existing government structures are not
effective in social marketing and insurance education and at the same time, the level of
knowledge about how to cover the informal sector amongst the TNHIF is to be rated very low.
In addition, the managerial capacities amongst the district-based CHF units are not advanced,
which results in main weaknesses on various areas, e.g. financial management, claims
management, and membership management, affecting the overall performance of the respective
CHF unit (Swiss TPH 2012).
In terms of servicing, a general low level of quality of the provided health services at
contracted health providers could be observed (Ifakara Health Institute 2012, Ouedraogo 2012).
Moreover, there is a lack of qualified full-time staff serving the CHF/TNHIF system. In terms of
data management and M&E, there is no adequate nationwide MIS and/or M&E system in place,
which supports the CHF/TNHIF system in these crucial areas (MIA 2012). This results in a low
level of accountability and overall sustainability within the system, especially on CHF level.
The low level of community participation in processes and product design is another weakness
affecting the sustainability as processes and products in place may not meet the needs of the
actual target community.
External opportunities within the design of the Tanzanian SHI system are above all in the areas
of governance, where it is promising to create independent CHF units that are supported by the
TNHIF in certain areas only, e.g. in terms of standard procedures, funding, coordination (Swiss
TPH 2012, TNCHF 2010). Another opportunity for the existing Tanzanian system would be the
introduction of a compulsory SHI for all citizens. This would result in higher numbers and a
general public commitment towards the system. This overhaul of the system may also include
an intensive community involvement and community consultation to enable the system to
address certain needs of specific parts/groups of the population, e.g. the informal sector and
other marginalized and/or vulnerable groups. It is also a promising opportunity to extend island
or pilot projects, such as the IMIS project in Dodoma Region (Swiss TPH 2012), to other
regions or to scale it up to the national level.
In the area of sales, the approach of using local administrators as well as district medical
officers and regional medical officer for common sensitization and mobilization should be
expanded to all CHF districts.
Servicing within the hybrid TNHIF/CHF system could be improved by inclusion of a
comprehensive referral system to upper levels of health facilities of the Tanzanian health

68
system. This would avoid the recent limitation of beneficiaries that are mainly accessing
dispensaries and health centers. To guarantee sustainability of the system, the compulsory
element of the TNHIF/CHF system should be emphasized by a sound and understandable public
policy. In line with that, the common commitment of other public and private stakeholders in
the field of social protection in health can be increased towards a joint effort to improve the
current system. This can be achieved through a public visibility campaign. The close
involvement of the target communities in this process will lead to an increased level of
community ownership and insurance literacy.
External threats to the Tanzanian SHI system were observed regarding the low support on
national and international level, which may result in an inability to redesign the scheme
adequately. Common threats to SHI scheme may also threaten the Tanzanian system, e.g. moral
hazard, adverse selection or a common mistrust by members and/or non-members of the
schemes (Ouedraogo 2012). The already mentioned low quality of health care, predominantly
the regular shortages of drugs and supplies as well as the lack of well-skilled health personal,
could threaten the system significantly (MIA 2012). The low-rated impact of the entire system
as well as common issues related to corruption and in-transparency may also result in a low
future support of external donors, which might not be convinced about the positive long-term
impact of the system. Due to the low level of success of the Tanzanian SHI system, the
evolvement of alternative health financing schemes to suit specific needs of excluded parts of
the society is furthermore possible and should be expected in case no general overhaul of the
system is being implemented in the near future.
The results of the SWOT analysis of the Tanzanian system are furthermore illustrated and
summarized in the following Tables 3 to 6:
Table 3: (Internal) strengths of Tanzanian SHI system, Source: own SWOT analysis.
1. (Internal) Strengths
Design • Targeting and (partly) coverage of informal sector • Combined governance structure CHF/TNHIF (informal
and formal sector health insurance schemes) Sales • Involvement of Regional Medical Officer (RMO), District
Medical Officer (DMO) and local authorities in sensitization of local communities
Servicing • Comprehensive product of curative and preventive health services at dispensaries and health centers

69
Sustainability • Public matching grant
Table 4: (Internal) weaknesses of Tanzanian SHI system, Source: own SWOT analysis.
2. (Internal) Weaknesses
Design • CHF system is not yet fully harmonized with the TNHIF • Limited involvement of crucial stakeholders • Limited coverage (15% CHF and TNHIF) • Top-down approach • Low level of community participation and/or involvement • Very complex system for identification of indigents • Over-reliance on district structures • Lack of experience of TNHIF to serve the informal sector
Sales • Very limited social marketing measures • Existing government structures are not effective in social
marketing and insurance education • Low level of managerial capacities amongst the district-
based CHF units • Low level of knowledge about how to cover informal
sector amongst TNHIF Servicing • Low level of quality in provided health care
• Lack of qualified full-time staff serving the CHF • Lack of adequate and nationwide MIS and M&E system
Sustainability • Low level of community participation in processes and product design
• Low level of accountability on CHF level
Table 5: (External) opportunities of the Tanzanian SHI system, Source: own SWOT analysis.
3. (External) Opportunities
Design • To introduce a compulsory element of CHF, to design and implement a compulsory SHI for all citizens in Tanzania
• To create independent CHF units, supported by the TNHIF in certain areas
• Intensive community involvement • To address certain needs of specific parts/groups of the
population (e.g. the informal sector, marginalized groups) • To extend pilot projects of IMIS (e.g. in Dodoma Region)
to other regions and the national level Sales • To extend the approach of using local administrators as
well as DMOs/RMOs for sensitization and mobilization to all CHFs districts
• To apply comprehensive insurance education and social marketing measures on TNHIF, CHF and community level
Servicing • Inclusion of referral services to upper levels of the health system, rather than limiting the beneficiaries to dispensaries and health centers

70
Sustainability • To introduce a compulsory element of CHF, to design and implement a compulsory SHI for all citizens in Tanzania in line with a public visibility campaign about the system
• To involve all government entities and donors in the field of social protection to contribute to a common TNHIF/CHF system
• To increase the level of community ownership • To increase the level of insurance literacy amongst the
target population
Table 6: (External) threats of Tanzanian SHI system, Source: own SWOT analysis.
4. (External) Threats
Design • Low support on national and international level may lead to an inability to redesign the scheme
Sales • Moral Hazard, Adverse Selection, mistrust by members and non-members of the scheme
Servicing • Low quality of health care, shortage of drugs • Moving out of Health Providers due to delay of claims
settlement and general corruption of the CHF system Sustainability • Low support of external donors due to low impact and
issues linked to lack of transparency and corruption • Evolvement of alternative health financing schemes to
suit specific needs of excluded parts of the society
In Rwanda, internal strengths can mainly be identified in the area of design of the overall
system, which is designed with affordable premiums and indigent subsidies for the most
vulnerable parts of the society. The system is based on a bottom-up approach ensuring high
levels of community participation and involvement, which resulted in an increased enrolment
amongst the target community, a national scale up process as well as good governance of the
SHI scheme (Kayonga 2007, Bump 2010).
The Rwandan system is furthermore based on formally and legally acknowledged public
guidelines and policies, including a compulsory element, which led to a high level of public
commitment and awareness nationwide. The coverage amongst the informal sector is equally
high as compared to other countries in the region. The national coverage increased from 7% in
2003 to 91% in 2010 (Nyandekwe et al 2012).
The Rwandan system implemented an adequate sub-system of the Ubudehe categories to
identify vulnerable parts of the population, which are to be classified as indigents. The system in
Rwanda was implemented very promptly, without major delays (Government of Rwanda 2012;
Nyandekwe et al 2012).

71
Through the public acknowledgement, the Rwandan system shows main strengths in the area of
sales. This is a result of the establishment of a comprehensive supporting and strengthening
structure of public and private stakeholders, as well as financial and technical partners of the
system (Nyandekwe et al 2012).
In the area of servicing, the Rwandan system benefits from the performance-based
funding of health providers by the Government of Rwanda, which ensures a high quality of care,
and regular monitoring and evaluation of the same. Through the high level of community
participation in processes and decision-making, most crucial procedures are tailored to the target
group. Furthermore, the technical working groups according to different health clusters are
continuously improving the quality of care and the common insurance supply (Management
Sciences for Health 2013, Nyandekwe et al 2012).
In terms of sustainability, the Rwandan system reveals its strengths in the high level of
community participation and involvement, which – in combination with the political goodwill
and supporting public policies and guidelines – results in a more sustainable implementation of
the overall system. The compulsory element within the system furthermore ensures a long-term
commitment and enrolment of a larger part of the target population. Another guarantor of
sustainability of the Rwandan system is the result-driven approach of the Rwandan government,
which results in a continuous process of monitoring and evaluation of the Rwandan SHI system
(Nyandekwe et al 2012; Joint Learning Network on Universal Coverage 2014, MIN 2014).
Common internal weaknesses of the Rwandan system can be identified in the area of
community-based structures that are considered as main drivers of the SHI system, and are
equally supposed to serve as a transferring link to a comprehensive national SHI system. In the
current situation, it remains uncertain, how this final transfer will look like and how feasible the
transfer is. In terms of a comprehensive MIS, the currently system in place to serve the
Rwandan health system, the RHMIS, is not yet tailored to serve the system of Mutuelles de
Santé in the areas of a comprehensive MIS and M&E system (USAID 2006).
In addition, there is still not enough emphasis being laid on the implementation of
effective social marketing and insurance education campaigns within the Rwandan system, as
there is no standardized manual for the Mutuelles de Santé in place to carry out such activities
and the general awareness about the actual benefits and functioning of a health insurance is still
rated low amongst the target group (Bump 2010).
Regarding the sustainability of the Rwandan SHI system, the existing capacities of
Mutuelles des Santé in institutional and/or managerial regards as well as on health facility level

72
are still rated as low and there is need for a comprehensive capacity assessment and building
plan. The transfer of Mutuelles de Santé towards a national comprehensive SHI system is not
clear yet, which threatens the long-term success of the current system (Nyandekwe et al 2012).
An external opportunity for the Rwandan system could design an adequate transfer strategy on
how to set up a national comprehensive social protection system, after the potential of
community-based schemes is fully explored (Nyandekwe et al 2012). Another opportunity for
the Rwandan system would be to develop and implement an adequate and tailored insurance
education and social marketing campaign to strengthen the overall awareness about the system
as well as to increase the general level of insurance literacy amongst the target group. Other
important areas for capacity development include the areas of financial management and general
scheme management (Bump 2010). A further opportunity in the Rwandan context would be the
inclusion of enrolment within a Mutuelle de Santé into the districts performance contracts
between the local governments and the central Government of Rwanda (Nyandekwe et al 2012).
The strong government leadership and political goodwill and commitment can
furthermore be regarded as a basis for a variety of opportunities to further develop the Rwandan
system. New components and/or evolvements within the system should be developed on the
basis of the general existing culture of solidarity and mutual assistance and/or aid amongst the
target group, which forms an ideal basis for a sustainable and effective social protection system
in the long term.
External threats to the Rwandan system could be the inappropriate priority setting of the
Rwandan government who feels that they have too many tasks to fulfill in the health and social
protection sector (Nyandekwe et al 2012). Priorities should hence be identified and followed-up
accordingly. Another threat might occur once current financial and technical supporters of the
Rwandan system move out, assuming that their support to the SHI system is no longer needed,
given that the ultimate goal of UHC was already achieved (cf. to Nyandekwe et al 2012). While
the funding of the Rwandan system is balanced, the moving out of crucial partners might
threaten the entire system in a significant way.
The high poverty levels in Rwanda, showing 44.9% of the population living below the
poverty line and 24.1% living in extreme poverty, is still reason enough to question the overall
success of the Rwandan SHI system, as it is supposed to reduce poverty in a significant way.
The low levels of insurance literacy amongst the target population are also potential
threats to the system, because this situation may lead to an increased level of adverse selection,

73
moral hazard and fraud. The role of health facilities in a future transformation process towards a
national SHI system is not clear, given the current lack of involvement of health providers in
common decision making processes (MIN 2014).
With regards to sustainability, the weak financial risk sharing between the different
community-based schemes and other health insurance schemes may become a concern
(Nyandekwe et al 2012). Moreover, the external funding of up to 50% through external donors
creates a common dependency of the system on the same and threatens the long-term
sustainability of the system. Innovative exit strategies have to be designed, so that the funding of
the system can be well balanced without creating common dependencies.
The results of the SWOT analysis of the Rwandan system are furthermore illustrated and
summarized in the following Tables 7 to 10: Table 7: (Internal) strengths of Rwandan SHI system, Source: own SWOT analysis.
1. (Internal) Strengths
Design • Affordable premiums with indigent subsidies for most vulnerable parts of the society
• Bottom-up approach: High level of community participation and involvement led to large take up and scale-up as well as good governance of the scheme
• Based on formally and legally acknowledged public policies and guidelines
• Compulsory element • Huge coverage of informal sector (increased national
coverage from 7% in 2003 to 91% in 2010) • Adequate system of Ubudehe categories to identify the
parts of the population that are to be classified as indigents Prompt implementation process without major delays
Sales • Public acknowledgement and comprehensive support through government and relevant stakeholders
Servicing
• Performance-based funding of health providers ensures high level of quality of care
• High level of community participation in processes and decision-making
• Technical working groups according to different health clusters are continuously improving quality of care and insurance supply in general
Sustainability • Bottom-up approach: High level of community participation and involvement
• Political good will and supporting public policies and guidelines
• Compulsory element • Result-driven approach of the government

74
Table 8: (Internal) weaknesses of Rwandan SHI system, Source: own SWOT analysis.
2. (Internal) Weaknesses
Design • Community-based structures as transferring link to comprehensive SHI system: How will the final transfer look like? • RHMIS is not yet tailored to serve the system of Mutuelles de
Santé in the areas of MIS and M&E Sales • Gap/Lack in the areas of social marketing and insurance
education campaigns Servicing • Human resource constraints: Lack of skilled personal on
various levels Sustainability • Low institutional and managerial capacities
• Community-based structures as link to comprehensive SHI system: How will the final transfer look like?
Table 9: (External) opportunities of the Rwandan SHI system, Source: own SWOT analysis.
3. (External) Opportunities
Design • To design an adequate transfer strategy how to set up national Social Protection System after potential of community based schemes is explored
Sales • To set up an adequate and tailored Insurance Education and Social Marketing Campaign
• To train all involved actors on the Insurance Concept as well as Financial and Scheme Management
Servicing • Inclusion of Mutuelles de Santé enrolment in districts' performance contracts between local governments and the President of the Republic of Rwanda
Sustainability • Strong government leadership, political commitment • Synergy between reforms in health sector • Culture of solidarity and mutual assistance and/or aid
Table 10: (External) threats of Rwandan SHI system, Source: own SWOT analysis.
4. (External) Threats
Design • Priority-Setting of government • Moving out of donors and technical support units assuming
ultimate goal of UHC was achieved • High poverty levels of population of Rwanda (44.9% below
poverty line and 24.1% living in extreme poverty) Sales • Low level of insurance literacy amongst target population
• Adverse selection, moral hazard and fraud due to low level of insurance literacy amongst the target population
Servicing • Unclear role of health facilities in transformation process towards national SHI system due to low involvement in decision-making
Sustainability • Weak financial risk-sharing between CBHF schemes and

75
other health insurance schemes • External funding of system of up to 50%, dependency of
external donors and other stakeholders
In Burkina Faso, a significant internal strength towards the design of the envisaged SHI system
is the bottom-up-approach. This was insured through a close involvement of Mutuelles de Santé
from the initial stage of design and implementation of the system. In addition, a comprehensive
involvement of various institutions and relevant stakeholders was ensured, aiming at a common
incorporation of various needs and demands of the multifaceted society in the future SHI system
(Solidarité Socialiste 2012, Le Faso 2013, Ministère de la Fonction Publique, du Travail et de la
Sécurité Sociale 2014).
In terms of sales, the involved Mutuelles de Santé are supposed to play a major part in
sensitization, mobilization and training of the target communities and future members of the
SHI system. This engagement is supposed to be based on a standardized training and capacity
building curriculum that was developed during the previous ILO Step-Programme engagement
in Burkina Faso, which supported and developed various CBHF schemes (ASMADE 2014).
The envisaged close involvement of health providers in all stages and processes of
implementation of the AMU may positively affect the servicing component of the system in
Burkina Faso, as the involved health providers will be aware about the system and – once the
concept of health insurance and the role of health providers in the system are well embraced –
will guarantee a high quality of provided health services (Solidarité Socialiste 2012). Through
the comprehensive involvement of various stakeholders, a common ownership is ensured, which
will strengthen the overall operations of the system, and will contribute to its sustainability.
An internal weakness of the system in Burkina Faso is the identified over-reliance on Mutuelles
Sociales, which are not yet regulated by any public body in Burkina Faso. Furthermore, the
AMU is not yet linked to any comprehensive social protection strategy, which is already
established or planned to be implemented in the near future in Burkina Faso.
The fact that the AMU is supposed to be a voluntary health insurance scheme for the
informal sector (Solidarité Socialiste 2012), can be identified as a main weakness as well, as
people from the informal sector might not develop commitment towards the AMU and rather
rate the AMU as an offer they would not necessarily benefit from. It may also be challenging to
expect people of low income working in the informal sector to invest their limited income and
resources into a voluntary health insurance scheme.

76
Another significant weakness of the system in Burkina Faso is its major delay in
implementation. Keeping in mind that initial discussions about the AMU started as early as
2008, it is a main challenge that until the year 2015, the system was not yet moved towards its
initial piloting and/or implementation stage. In addition to this, there is not clear strategy on
design of adequate indigents and/or waiving mechanisms to serve the most vulnerable and
marginalized parts of the population. The design of the AMU hence lacks a number of essential
components, which will challenge the final success of implementation of the system.
In the area of sales, the system to be implemented in Burkina Faso shows weaknesses in
terms of a low level of managerial and technical capacities of involved Mutuelles de Santé and
Mutuelles Sociales in general. While there are manuals and capacity building tools available
through the ILO Step-Programme, the institutional expertise is still to be rated as very low and
insufficient, as most Mutuelles operate through volunteers and without a properly equipped
office, often without power supply and adequate stationary for simple membership and claims
management. In addition to this, the awareness about Mutuelles de Santé amongst the target
population is still low. On health provider level, there is still a low level of insurance literacy to
be noted.32
In addition, the lack of a legal framework for Mutuelles de Santé to operate as well as the
lack of a more comprehensive social protection strategy in place, significantly threatens the
overall sustainability of the envisaged AMU in Burkina Faso.
External opportunities within the AMU in Burkina Faso are closely related to the weaknesses
addressed and are above all to be identified in the area of a future contextualization of the AMU
within a broader national social protection strategy. In addition to this, the development of a
legal framework and common rules and regulations for Mutuelles de Santé and Mutuelles
Sociales in general would clarify their role and responsibilities in a future AMU. To
complement the strengthening of existing Mutuelles de Santé, a comprehensive IT-based MIS
and M&E system for Mutuelles de Santé and Mutuelles Sociales in general may be considered.
To support the overall sales component of the AMU, a broad campaign on insurance
education and social marketing to prepare the society as well as all involved stakeholders for the
roll out of the AMU, is a promising approach to consider. Health providers should be closely
involved in this public campaign to ensure ownership and a common understanding of the
system by all stakeholders. Moreover, an extensive assessment of quality of care should take
32 This became evident during different field research periods in Burkina Faso in 2008, 2009 and 2013.

77
place to agree with the involved health providers on certain minimum standards to be
implemented once they will be part of the AMU.
In terms of sustainability, the AMU planning committee might consider to link up with
other government departments that are engaged in social protection interventions as well as
common donors and stakeholders in this area to win them as strong supporters and drivers of the
future AMU as well as to ensure effective linkages and referral mechanisms to other social
protection measures for the AMU beneficiaries.
The AMU is exposed to specific external threats that above all can be identified in the unclear
role of the AMU in case of implementation of a national social protection system or strategy. In
addition to this, an increased level of competition of Mutuelles de Santé with private for-profit
health insurance schemes may arise due to the lack of clear rules and regulations of Mutuelles de
Santé in Burkina Faso.
In addition, the role of other actors within the landscape of health care provision in
Burkina Faso, such as private and faith-based health facilities remains unclear, as the envisioned
AMU only considers public health providers. This may cause challenges towards the smooth
servicing within the AMU. Regarding sustainability of the AMU, the transformation process
from the voluntary health insurance within the AMU for the informal sector towards UHC in
Burkina Faso remains unclear and was not yet discussed by the involved planning committees
(Solidarité Socialiste 2012).
The significant delay of implementation equally threatens the overall success of the
AMU in Burkina Faso, because major donors and technical partners may move out due to a
decreased level of trust and confidence in the system to be implemented in the near future.
The results of the SWOT analysis of the system in Burkina Faso are furthermore illustrated and
summarized in the following Tables 11 to 14: Table 11: (Internal) strengths of the envisaged SHI system in Burkina Faso, Source: own SWOT analysis.
1. (Internal) Strengths
Design • Bottom-up approach • Close involvement of Mutuelles de Santé from initial design
stage • Involvement of various institutions and stakeholders aiming
at meeting various needs and demands of a multifaceted society
Sales • Acknowledgement and involvement of Mutuelles de Santé in sensitization, mobilization and trainings of the target communities

78
• Standardized curriculum due to former ILO Step-Programme engagement
Servicing • Close involvement of contracted health providers from initial stage
Sustainability • Close involvement of all crucial stakeholders ensures ownership
Table 12: (Internal) weaknesses of the envisaged SHI system in Burkina Faso, Source: own SWOT analysis.
2. (Internal) Weaknesses
Design • Over-reliance on Mutuelles Sociales • No public regulation yet • No public social protection strategy developed that would be
linked up with AMU • Voluntary health insurance for informal sector • Major delays in implementation process • No clear strategy on design of indigents and waiving
mechanisms for the vulnerable parts of the society Sales • Low level of managerial and technical capacities of Mutuelles
de Santé • Low level of visibility of Mutuelles de Santé
Servicing • Low level of insurance literacy amongst health providers Sustainability • No legal framework for Mutuelles de Santé
• No public social protection strategy or framework
Table 13: (External) opportunities of the envisaged SHI system in Burkina Faso, Source: own SWOT analysis.
3. (External) Opportunities
Design • To contextualize the AMU within a broader national social protection strategy • To set up a legal framework for Mutuelles de Santé in
Burkina Faso to clarify their role and responsibilities within the AMU • To design and implement an IT-based MIS and M&E system
Sales • To develop a broad campaign on insurance education and social marketing to prepare the society for the roll out of the AMU
Servicing • To closely involve health providers in the public campaigns (insurance education, social marketing) • To assess level of quality of care before rolling out the AMU
and to agree on certain standards for contracted health providers within the new system of AMU
Sustainability • To link up with other government departments in charge of social protection as well as donors/stakeholders in the field of social protection

79
Table 14: (External) threats of the envisaged SHI system in Burkina Faso, Source: own SWOT analysis.
4. (External) Threats
Design • Unclear relevance of AMU system in case of implementation of national social protection system and/or strategy
Sales • High level of competition with private commercial health insurance schemes
Servicing • Unclear role of private and faith-based health facilities Sustainability • Unclear transformation process from voluntary health
insurance to UHC • Moving out of donors because of significant delay of
implementation process
In Ghana, main internal strengths can be identified in the area of exemption measures and
indigents for identified vulnerable parts of the society. In addition to this, the GNHIA put in
place a comprehensive marketing strategy with various tools and approaches, also involving
district chief executives and district assemblies, which is a favorable asset in terms of sales of the
NHIS (Achampong 2012; Asenso-Boadi and Agbeibor 2010). Moreover, the benefit package
offered under the NHIS is of comprehensive nature and does require only low co-payments by
the beneficiaries. A unique approach in Ghana under the NHIA is the inclusion of eye and dental
care as well as the focus on maternal services, so that main needs of the society are fully covered
by the NHIS (Boateng 2007; Gajate-Garido and Owusua 2013, Singleton 2006, Joint Learning
Network on Universal Coverage 2014). A significant success in Ghana is furthermore the
increased health care utilization by NHIS beneficiaries, which increased from 6,262,765 in 2005
to 17,603,216 in 2009 and strengthened the servicing component of the NHIS (Oxfam
International 2010).
In terms of sustainability, the NHIS is based on existing district structures and involves
local authorities and the target communities, which ensure its long-term effect and successful
operations. Furthermore, a high percentage of the NHIS system is tax-based, as 62.37% of the
overall funding is generated through public taxing. This avoids over-reliability or dependencies
on external donors and/or the beneficiaries (Dietrich-O’Connor 2010).
The NHIS faces several internal weaknesses that can mainly be located in its initial design. The
vertical NHIS control structures, which do not provide decision-making authority to the district-
based NHIS units, result in a lack of financial autonomy and/or flexibility on schemes level.

80
The NHIS units are furthermore multiply dependent on the hierarchal structures of the NHIS and
opportunities towards cost control are very limited on district level. The NHIS shows a general
low level of transparency, which – through the hierarchic structure – affects the entire NHIS
system.
In addition to this, it has to be noted, that while the general OOPP rates reduced slightly
to 22-37% in Ghana, they are still above the WHO recommended average rate of 15-20%. The
NHIS was furthermore designed with a pro-poor focus, but is de-facto mainly serving the
middle- and high-income sector, resulting in the fact that well-designed pro-poor measures are
de-facto not operational and/ not effectively implemented (Gajate-Garido and Owusua 2013;
Oxfam International 2010).
The designed exemption measures within the NHIS are so far not applying to informal
sector employees, excluding a larger part of the society from the national scheme. Children can
access the NHIS through their parents only, while child-headed households and OVCs are not
adequately considered within the scheme. This results in the overall observation that the
identification of indigents within the NHIS is imprecise and the existing indigents are
insufficiently designed. The overall NHIS coverage still remains below 50%, while the overall
progress is to be rated as slow (Oxfam International 2010). The MIS is to be rated as limited and
cannot generated crucial data for effective data management and M&E within the NHIS (Owusu-
Asamoah 2012).
In the area of sales, the NHIS lacks expertise in the fields of technical and managerial
capacities on schemes level as well as adequately implemented insurance education and social
marketing measures, while the servicing component is threatened by low quality of drugs and
major delays within the claim settlement process (WHO 2010). In most NHIS health facilities,
only low-quality drugs are covered by the NHIS, which results in a decreased level of trust of the
beneficiaries in the scheme and an increased level of co-payments, as most beneficiaries tend to
purchase high quality drugs externally. The common rejection of NHIS beneficiaries in certain
health facilities furthermore led to an over-usage of other facilities where patients faced long
waiting hours and shortages of drugs.
In addition to this, further gaps in the Ghanaian NHIS could be observed in the areas of
effective referral mechanisms as well as the existence of informal payments of NHIS members
that represent up to 40% of all OOPP. Moreover, there is a general gap of human resources in the
Ghanaian health sector to be noted. As a result, 56% of the NHIS DWMHI schemes are exposed
to under-staffed health facilities (WHO 2010). The introduction of unified tariff lists through the
NHIS led to an enormous cost increase at health provider level. As a result, health providers were

81
trying to gain profit out of the NHIS patients, which compromises the entire NHIS. There is a
tendency of contracted health providers to oversubscribe certain drugs due to the increased tariff
lists for drugs, leading to a de-facto system of incentives for over-subscription, threatening the
entire NHIS. Furthermore, most contracted health providers are located in the Greater Accra
region, while the better part of the NHIS beneficiaries live in rural areas and can hardly access
the contracted providers (WHO 2010).
Regarding the sustainability of the NHIS, it has to be stated that the offered NHIS
benefit package is very generous covering 95% of the disease burden, resulting in a high
financial burden to the national scheme. At the same time, the referral system is not well
developed and ineffective, while the M&E system is not operational. In addition, there is an
increasing politicization of the NHIS through GNHIA representatives leading to the common
perception amongst the target population of the NHIS being a political led scheme, rather than
being a universal health scheme for all Ghanaians (WHO 2010, Gajate-Garido and Owusua
2013).
Given these numerous weaknesses in the design of the NHIS, there are various external
opportunities to be noted to possibly address the same. The existing government funds for social
protection could be used to support the NHIS or to create linkages for NHIS beneficiaries to
other social protection measures. This should be done in a combined effort of all relevant line
ministries of the Government of Ghana. Furthermore, the needs of the informal sector should be
specifically acknowledged and targeted within the NHIS, so that currently excluded parts of the
society can gain access to the NHIS. Children should be decoupled from their parents, to ensure
proper access for child headed households and OVCs as well. In line with that, proper measures
to integrate vulnerable parts of the society into the NHIS system should be applied. To ensure a
more professional, transparent and accountable operation of the NHIS, an adequate IT-based
MIS should be developed.
With regards to the sales component of the NHIS, a standardized training curriculum for
scheme personnel and health facility staff, especially in the areas of insurance education and
social marketing, should be put in place. Furthermore, to ensure an increase in numbers, group
approach and/or mass community registration efforts should be considered.
To improve the servicing component of the overall NHIS, an IT-based claim-processing
center should be considered. This should be implemented in line with a functional and effective
M&E system as well as regular clinical audits (WHO 2010).

82
With regards to sustainability, a crucial opportunity would be to transfer more influence and
power to the district level and the communities to ensure a certain level of ownership of the
scheme on various levels.
External threats to the existing NHIS are parallel structures of CBHF schemes that could not be
absorbed by the NHIS (Ouedraogo 2012). Given the recent challenges of the national scheme,
the probability for the target group to consider alternatives to the NHIS can be rated as high.
In terms of sales, the low awareness about the scheme and the general low level of
embracement of the insurance concept amongst the target community can be rated as a main
threat to the NHIS. Due to the mentioned challenges, the trust level towards the NHIS amongst
the target population is to be rated as low (Ouedraogo 2012). Effective measures to build up trust
and confidence towards the system would be needed to successfully sell the NHIS concept to the
population.
In the area of servicing, the already mentioned low quality of drugs results in an
increased mistrust and dissatisfaction amongst NHIS beneficiaries as well as potential members
of the NHIS. Low quality paired with shortages of drugs also resulted in a high percentage of
OOPP for high quality drugs purchased at external health care providers. This opposes the main
objective of the NHIS to decrease OOPP amongst its beneficiaries. The external purchase of
drugs equally led to a high level of competition between external pharmacies and NHIS
contracted health care providers. This can be rated as an unhealthy competition, which
compromised the principles of common harmonization within the health sector towards best
quality service delivery to the patients.
In terms of sustainability, the NHIS stands at high risk to lose its long-term supporters,
as the mentioned challenges related to trust and transparency might be against common standards
of most international NGOs and/or donors and development partners.
The results of the SWOT analysis of the Ghanaian system are furthermore illustrated and
summarized in the following Tables 15 to 18: Table 15: (Internal) strengths of Ghanaian SHI system, Source: own SWOT analysis.
1. (Internal) Strengths
Design • Comprehensive exemption measures for identified indigents and specific groups
Sales • Comprehensive marketing strategy with various tools and approaches
• Involvement of district chief executives and district assemblies in marketing of the scheme

83
Servicing • Comprehensive benefit package, no or low co-payments, comprising eye and dental care and focus on maternal services
• Increased health care utilization (from 6,262,765 in 2005 to 17,603,216 in 2009)
Sustainability • Based on district structures and (even if limited) involvement of local authorities and target communities
• High percentage of system is tax-based (62.37%)
Table 16: (Internal) weaknesses of the Ghanaian SHI system, Source: own SWOT analysis.
2. (Internal) Weaknesses
Design • Vertical control structures • OOPP rates reduced slightly, but are still above the
recommended average rate as recommend by the WHO • Even if officially designed with a pro-poor focus, the NHIS
is de-facto serving mainly the middle- and high income sector • Inadequate and limited MIS • No exemptions mechanisms for informal sector employees • Access for children only through parents • Identification of indigents is imprecise/insufficiently
designed indigents • No autonomy and/or financial flexibility of DWMHI
schemes • Multiple dependency of schemes on external hierarchal
structures – no opportunity of cost control on DWMHI schemes level • OOPP rates reduced slightly, but are still above the
recommended average rate as recommend by the WHO • NHIA shows low transparency levels • Low coverage level • Slow process and progress
Sales • Low level of technical and managerial capacities on scheme level • Lack of adequate insurance education and social marketing
measures Servicing • Low quality of drugs
• Delay in claims settlements results in rejection of NHIS clients in certain facilities leading to an over-usage of other facilities facing long waiting hours and shortages of drugs
• Main gaps in health system and health care delivery system (e.g. in terms of referrals, informal payments for NHIS members: 40%)
• Inadequate human resources (56% of DWMHI schemes) • Enormous Cost increase due to unified tariff lists • Most contracted hospitals are located n Greater Accra
Region while most beneficiaries live in rural areas • Only low-quality drugs are covered by the scheme

84
(decreased level of trust of beneficiaries towards the scheme)
Sustainability • Provider incentives to oversubscribe • Generous benefit package covering 95% of the disease
burden • Ineffective referral system • Underdeveloped M&E system of the NHIS • Politicization of the NHIS
Table 17: (External) opportunities of the Ghanaian SHI system, Source: own SWOT analysis.
3. (External) Opportunities
Design • Use government social protection funds to support the NHIS (combined efforts of all ministries)
• Target and acknowledge needs of informal sector • Decoupling of children and parents • Apply proper measures to integrate vulnerable parts of the
society into the NHIS system • Implement an adequate IT-based MIS
Sales • Trainings of scheme personnel and health facility staff on insurance education and social marketing
• Group-approach/mass community registrations into the NHIS
Servicing • IT-based claims processing center • Clinical audits • Functional M&E system
Sustainability • Giving more influence and power to the district level and the communities would ensure ownership on various level
Table 18: (External) threats of the Ghanaian SHI system, Source: own SWOT analysis.
4. (External) Threats
Design • Parallel structures of mutual health organizations not absorbed by the NHIS
Sales • Low awareness about the scheme and low level of embracement of insurance concept
• Low level of trust among the target population Servicing • Low quality of drugs result in distrust of members in NHIS
and high percentage of OOPP for high quality drugs – high level of competition between external pharmacies and contracted NHIS health care provides
Sustainability • Moving out of long-term supporters and donors because of challenges in the areas of trust and transparency

85
Based on the comprehensive SWOT-Analysis, common lessons learnt towards the
implementation of an integrated national SHI system are presented in the following. The lessons
learnt will refer to low-income countries of sub-Saharan Africa, aiming at combining the four
illustrated examples from different regions. To comply with the health insurance framework, the
cumulated lessons learnt are divided into the sub-categories of Design (1), Sales (2), Servicing
(3) and Sustainability (4).
1. Many countries in sub-Saharan Africa introduced national insurance schemes that are
mandatory for formal sector employees and public servants, while the informal sector is
supposed to be covered by voluntary insurance. As most low-income countries in sub-
Saharan Africa comprise a large informal sector, it is advisable to target the same. In this
context, it is crucial to design simple processes and affordable premiums tailored to the
specific needs of this target group who will build the basis for the national scheme. Each
health insurance – either with a commercial or a social protection focus – is highly
determined by the number of members, clients or beneficiaries that are contributing to
the common risk pool. A low coverage will result in higher premiums, limited products
and benefits and low ceilings and is challenging the overall attractiveness of the health
insurance scheme.
2. A clear and transparent way to identify and implement indigents and waiving
mechanisms is indispensable to ensure that vulnerable parts of the society will also
benefit from the scheme, while their ability to pay for the same may be limited. If this is
not given, the scheme will exclude larger parts of the society, that could not been
properly identified under the defective system. To adequately identify vulnerable parts of
the society, a participatory approach to classify indigents should be used. Participatory
community development provides various approaches to empower the target
communities to identify their indigents and design adequate categories for tailored
premium payment. A low level of community participation in this area may negatively
impact the target population towards a low level of ownership and general acceptance of
the scheme.

86
3. Centralized scheme management applying a top-down orientation and vertical control
structures will result in the fact that the target communities will not own the local
structures of the national scheme. Local SHI scheme structures will equally not be
flexible in their operations, e.g. to design tailored products and processes. It is hence
advisable to opt for a bottom-up approach to ensure a high level of community
participation and ownership, which will lead to larger level of take-up and scale up as
well as an advanced level of good governance of the scheme. In this context, a close
involvement of existing community-based organizations as well as all other relevant
stakeholders during the scheme design is highly advisable to ensure that various needs
and demands are met within the process. To ensure a high level of community
ownership, the local units of the national SHI system should be self-dependent and
flexible in their decisions of handling funds and processes.
4. While the overall approach should be bottom-up-oriented, the implementation process of
a national SHI scheme should be embedded in clearly formulated, formally and legally
acknowledged policies and guidelines. In this context, a compulsory element for the
target population to become member of the scheme is to be considered as a main driver
of the scheme. Evidence in countries with a high coverage (e.g. Rwanda) reveals that a
compulsory element was necessary to convince the target population to join the scheme.
In addition, a national SHI scheme that is not closely linked to existing government
policies or programmes is unlikely to survive, because the level of public awareness and
acknowledgement will be low.
5. Once the government or certain government entities are closely involved in the design
and implementation of the national SHI system, the danger of politicization of the
scheme is given. In this scenario, clear guidelines have to be developed to delink the
system from political activities and in the same way show its independency clearly to the
public and the potential target group.
6. The implementation process of a SHI scheme should be prompt without delays, as a
bureaucratic and time-consuming implementation process may result in a low level of
confidence towards the scheme amongst the target population as well as common
supporters and funders of the scheme. In this context, it is advisable to allocate enough
time and resources for the pre-implementation phase, in which the design of the entire

87
implementation process of the scheme is agreed with all stakeholders. Neglect towards
the involvement of crucial stakeholders in the scheme implementation process may lead
to the failing of the scheme due to a low level of ownership and commitment. Once the
general support of the scheme on national and/or community level is low, the scheme in
its operations is seriously threatened as the multi-level support of it– especially in its
initial stages, but also in a long-term-perspective to ensure sustainability of the scheme –
is more than crucial.
7. On central level, it is advisable to have a national coordinating body, which sets
standards and provides tools and systems as well as exchange forums for the local units
of the system. In the long term, to achieve UHC, local structures of the system have to be
up-scaled to, linked to or embedded into national structures. To ensure this, an adequate
transfer mechanism as well as an adequate implementation plan and timeline should be
designed during the initial stage of the national SHI system.
8. Proper systems should be established within the national SHI system to support all
involved stakeholders to adequately fulfill their duties. For this purpose, a clear guideline
about roles and responsibilities of each stakeholder has to be developed during the initial
design stage of the SHI system. It is necessary to ensure a high level of professionalism,
accountability and check and balances.
9. If the national SHI system is purely based on one kind or type of institution or structure,
e.g. district structures or CBHF schemes, this structure has to be very stable and reliable,
because once the structure fails, the entire scheme system will the threatened to fall. It is
hence recommendable to design a system with various approaches and different
structures/institutions to serve different groups of the society.
10. A clear channel of communication as well as adequate systems for data gathering and
management are crucial in a national SHI scheme. Many systems neglect the named
components, resulting in conflicts between the different stakeholders because of poor
communication as well as an inability to measure success and failure due to a common
lack of data. Moreover, a low level of transparency is a potential threat to a national SHI
scheme on different levels. Internally, it will lead to a general doubting of most involved
stakeholders towards the system. Externally, the system will lack acknowledgement and

88
donor support once its level of transparency is questioned. Especially in initial stages,
national SHI schemes are in urgent need of public acknowledgement to cope with the
initial phase of implementation with an adequate level of external and internal support. A
serious threat to a national SHI system would be the potential moving out of donors
and/or technical support units. This might happen once the need for their support is no
longer seen (e.g. UHC was achieved or almost achieved) or the system is doubted in
terms of its accountability, legitimacy and/or transparency.
11. Especially during the initial stages of scheme design and implementation, a close
monitoring will be important to ensure a proper implementation of the national SHI
system within a long-term-perspective. A well-developed M&E system should be
established and accessible on all different levels of the system (e.g. community,
county/district and national level), and should be able to capture all crucial component
and indicators (e.g. regarding membership dynamics, financial and scheme
management). Ideally, it should be IT-based containing web and mobile phone
applications, to ensure and extensive use and it should also entail elements of a
comprehensive MIS.
12. Focus on extensive premium payments to finance the SHI scheme, rather than
considering a comprehensive tax-financing element as well as a generally flexible and
balanced funding of the system bares the danger of excluding large parts of the society
as well as creating financial dependencies of the system on the beneficiaries. In addition,
a successful SHI scheme is supposed to minimize OOPP. Once the OOPP are at a
medium or high level, the overall objective of Access for All and UHC cannot be met.
13. High poverty levels of the target group – the potential beneficiaries of the scheme – are
threatening the scheme, as their monetary contributions in forms of premiums are main
carriers of the scheme. In most existing schemes, tax- and/or donor funding alone was
not rated as able enough to sustain the scheme and without contributions of the
members, the main concept of pooling of risks and resources would be extensively
compromised.
14. In most countries of sub-Saharan Africa, different models and institutions of
community-based health insurance schemes are in existence. When implementing a SHI

89
scheme, it is possible that few structures cannot be absorbed by the system due to
institutional weaknesses, a low level of commitment of those schemes or other crucial
factors. The co-existence of local schemes and schemes part of the national scheme
moreover will result in a very heterogeneous landscape of local social health financing
institutions resulting in a common confusion and low commitment of the target
population towards the national SHI scheme.
1. The lack of effective and efficient social marketing and insurance education measures
within a national SHI scheme will result in a low level of public visibility of the national
scheme and an equally low level of support through the government and other crucial
stakeholders, e.g. donors and development partners as well as technical supporters of the
scheme. In this context, the close involvement of relevant government entities as well as
recognized local leaders and devolved government authorities in the areas of insurance
education and social marketing will ensure a smooth implementation process as well as a
high level of commitment towards the scheme. In addition, the involvement of
community-based structures and other local stakeholders, such as churches, in
sensitization, mobilization and trainings of the target communities is indispensable for
the overall success of the scheme. A remaining low level of insurance literacy amongst
the target population of the system can seriously threaten the scheme, as conflicts may
arise due to a misunderstanding of the overall principles of health insurance, e.g. people
would expect to get their premiums back once they did not fall sick after one year or
would expect people that fall sick more frequently to contribute higher premiums.
Furthermore, comprehensive insurance education and social marketing measures
amongst the target group are to be seen as guarantors of a sustainable SHI scheme. These
measures should be applied in an extensive way to cover all levels of the system. Ideally,
they should be standardized in a way that standard modules and a certain timeline are
provided to ensure proper implementation.
2. To ensure a successful implementation of the scheme, a standardized training curriculum
should be put in place. To ensure that the scheme is marketed in a professional way, a
high level marketing strategy with various tools should be designed and implemented.
For this purpose, technical assistance from commercial marketing professionals should
be considered.

90
3. The provision of a tailored and comprehensive benefit package within a national SHI
system is highly recommended. The package should cover curative and preventive
services, as well as involve only minimal co-payments, while a focus on maternal health
services and other crucial needs of the target society will result in a high level of
perceived attractiveness and relevance of the national scheme towards the target
population.
4. Inadequate management capacities among the key scheme staff of the national SHI
scheme on community level will result in a low level of trust amongst the targeted
communities, which will not be willing to trust and invest their limited resources in a
poorly managed scheme.
5. To ensure high enrolment into the scheme, existing group structures on community level
should be used. Introducing the scheme to an already organized group will result in a
high social commitment amongst the group members and a high number of absorption of
community members into the scheme. Following this approach may lead to a fast
coverage of huge parts of the targeted population.
6. Private commercial health insurance schemes that are not involved in the national SHI
scheme will be serious competitors of the contracted health providers, e.g. in terms of
offering better quality of services. Due to this potential threat, it is advisable to include
private health insurance schemes, e.g. in the area of technical advice and support
regarding actuarial specific of the system, such as an adequate premium calculation or
smooth claims procedures, into a national SHI scheme equally to public, private and
faith-based health providers.
1. The close involvement of health providers from the initial stages of implementation of
the national scheme will ensure that their needs, interests and demands are met and that a
high level of ownership is ensured. In addition, it is very important to ensure that health
providers are sensitized on the insurance concept as well as the implications of fraud for
all involved parties within the system. Health providers are crucial stakeholders that are
usually neglected when implementing a national SHI System. Besides their role as
service providers and guarantors of high quality services, they should also play a crucial

91
role in the marketing of the scheme as well as in general member recruitment for the
scheme.
2. Universal access to quality health care is one key objective of a national SHI scheme and
hence to ensure the same should not be neglected. To provide a high quality of services
includes avoiding high co-payments as well as “informal payments” of scheme members
to the health providers. In addition, the accessibility of accredited health providers as
well as a certain level of insurance literacy amongst the health personnel should be
insured. A low quality of care at contracted health care providers of the national scheme
will result in a common mistrust and dissatisfaction of members towards the scheme. To
avoid this, regular assessments and audits of the contracted health providers may support
the relevant government entities to ensure a high level of quality of care within the
national SHI system. The level of quality of care should be assessed during the initial
planning stages of the SHI system and equally be followed up regularly after the
successful establishment of the system. Regular clinical audits of contracted health
providers are one opportunity to serve this purpose. In addition, a compensation of
contracted health providers according to the delivered services (performance-based
contracts) will ensure a high level of quality of health care and a continuous review of
provided quality by the health facilities of relevant authorities of the SHI system.
Governments have developed specific agreements on district performance. To include
the level of enrolment into the health insurance scheme of the district population into
these contracts seems to be a motivating practice towards a common commitment of the
district authorities towards the scheme. The establishment of an independent entity on
national level, e.g. a technical working group comprising national and international
development partners and research institutions, which provides continuous technical
support and input can furthermore ensure a continuous improvement of quality of care
and health insurance supply to the target population.
3. Through a high level of involvement and participation of the targeted communities in
common processes and decision-making within the national scheme, the services
delivered will be tailored to their needs and the level of satisfaction will be increased.

92
4. The establishment of an effective referral system will result in a more cost-effective
national SHI system as occurring illnesses will be treated adequately and members will
not forego treatment because of a lack of access to higher-level facilities. The premium
should include the coverage of transport costs to referral health facilities.
5. A low level of managerial capacities at the local scheme level will result in the provision
of poor services, e.g. delays in claims settlement. In addition to the danger of inadequate
capacities amongst local scheme managers, the lack of capacities to reach the informal
sector with all its specific characteristics will result in a lack of ownership of the scheme
by the targeted communities. In addition, if main principles of good governance of the
health insurance are not maintained, the scheme will be threatened by a low level of
support by the contracted health providers that would rather move out of the entire
system than cover the depth of the national scheme.
1. Through a long-term financial commitment of the government, the national SHI scheme
is to be considered as more viable in terms of financial sustainability. A public matching
grant or a comprehensive tax-based element of the national scheme can fulfill this
purpose.
2. To achieve commitment amongst the target population, a strong political goodwill and
commitment is needed, that will also lead to sustainable operations of the scheme.
Common reforms of the respective public health sector are to be considered to contribute
to the overall success of the envisioned system. If relevant reforms are tailored to
support the new system, it will be carried by these reforms and support its sustainable
components in a crucial way. Public commitment and policy support through the
respective government, e.g. through the introduction of a compulsory element of the
scheme, will further lead to a higher level of acknowledgement and commitment
amongst the target population towards the scheme and will result in an increased level of
sustainability of the overall national SHI scheme.
3. A well-balanced funding of the national scheme through national and international,
public and private sources, will ensure financial sustainability, and protect the scheme
against dependency on a certain funding source or donor. An adequate tax-financed
element of a national SHI scheme will provide sustainability and the necessary back-up

93
funding once premium payment becomes unpredictable or unreliable. If a national SHI
system focuses on premium payment rather than on taxation, it is vulnerable, because
once the income levels of the target group decrease or the priorities of the target group
change, the main funding cannot be provided anymore and the system fails. An over-
dependency of more than 50% on external donor funding is seriously threatening the
long-term-operation of the scheme. It is therefore advisable to consider premium
payments as well as tax- and donor funding in a well-balanced way so that none out of
the three elements becomes main driver or carrier of the system.
4. Many governments in sub-Saharan Africa envisaged implementing a national SHI
system and/or strategy to fit in the global request and conviction of social protection as a
guarantor for development. In cases where the SHI scheme is not developed in line with
existing social protection strategies, a sidelining social protection system will threaten its
overall existence and sustainability.
5. Some countries in sub-Saharan Africa consider implementing national SHI schemes that
in its initial stages will cover the informal sector in forms of a voluntary insurance only.
As in the long term a transition to UHC is envisioned, a clear strategy on how the
voluntary insured beneficiaries will later be integrated into the mandatory national health
insurance is highly advisable to serve the purpose of sustainability.
6. A promising approach towards sustainability is to involve a high number of relevant
committed stakeholders, which will own the scheme and ensure its long-term operations.
To convince relevant stakeholders about the benefits and relevance of a national SHI
scheme is the biggest challenge in this regard. The common commitment of all
stakeholders is also needed to ensure adequate technical and financial inputs towards
scheme implementation as well as an extensive public visibility of the scheme in the
long-term.
7. Once the scheme is not designed in an inclusive way considering including all parts of
the society, the probability of alternative institutions to serve specific needs of specific
groups of the society can be rated as high. This fact would compromise the overall
objective to provide a transparent and harmonized system of social protection in health
for all citizens.

94
8. The involvement of existing public and community-based structures, e.g. to base the
scheme on existing district structures, will lead to more stableness of the scheme in a
long-term perspective.
9. Once the impact of the scheme is rated as too low or concerns related to corruption
become more evident amongst the national and international community around the
national scheme, the trust of external donors will decrease and a general decrease of
external support is expected. A delay of the implementation process or a general low
level of transparency will result in the same.

95
After the analysis of various case examples of integrative SHI systems in sub-Saharan Africa,
the focus of this chapter will be laid on the specific example of the Republic of Kenya and its
national challenges and opportunities in social protection in health. As described in the
comprehensive background provided in chapter 2.6,33 Kenya is currently implementing various
policies and strategies in this field. The following in-depth analysis – besides comprehensively
analyzing the case of Kenya – is aiming at transferring lessons learnt from chapter three to the
case of Kenya, to hence develop a standard model for implementation of an integrated SHI
system in Kenya.
Based on this model, a further standard model for implementing integrated SHI systems in low-
income countries will be developed. Thus, the case study is aiming at fulfilling the following
objectives:
(1) To analyze existing social health financing and social health protection measures and
implementing stakeholders on various levels of the Kenyan context, and to elaborate the
potential of fulfilling the ultimate goal of UHC;
(2) To apply and transfer lessons learnt from the chosen country case examples of the third
chapter (Tanzania, Rwanda, Burkina Faso and Ghana) to the case of Kenya and hence
develop tailored recommendations for the Kenyan context;
(3) To develop a standard system of an integrated SHI system in Kenya and – in a more
general perspective – for the context of low-income countries.
This chapter is based on the Case Study Approach (CSA) combining different methods of in-
depth analysis. A case study is “a research approach that is used to generate an in-depth, multi-
faceted understanding of a complex issue in its real-life context” (Crowe et al 2011:1). A case
study is hence “based on in-depth investigation of a single country” (ESS Edunet 2013). The
CSA contrasts any experimental approach that does not consider real life settings and the CSA
is expected to be of a “naturalistic” nature. Case studies are meant to have a conceptual structure
and furthermore within the given case, various perspectives and contexts are to be considered
(Crowe et al 2011).
33 Please refer to pages 35ff.

96
Following this approach, the first part of the presented case study will present the analysis of
qualitative data from various levels, including the micro level – an empiric analysis of CBHF
schemes in Kenya supported by STIPA, a national NGO, and data gained from interviews with
numerous stakeholders in this field34 – and the macro level – including data gained from
interviews with stakeholders from relevant government entities, e.g. the National Hospital
Insurance Fund and the Community Health Strategy35 (first step).
A comprehensive Stakeholder Analysis (SA) will complement the above-described data by
providing insights into the general context of a future SHI system in Kenya (second step). A
professional SA can be defined as “a methodology used to facilitate institutional and policy
reform processes by accounting for and often incorporating the needs of those who have a
‘stake’ or an interest in the reforms under consideration” (World Bank 2005). The SA will
hence assist in clarifying about crucial actors within the implementation process of the national
SHI scheme, as well as clarify how each stakeholder is expected to be part of the future system.
Therefore, it is important to identify the stakeholders and their main needs and demands, and
equally assess the respective levels of commitment and/or resistance (Schmeer 1999). Based on
this different dimensions, a comprehensive SA considers the following four steps: Identifying of
Stakeholders (1), Determining Stakeholders Interests (2), Determining Stakeholders Powers and
Influences (3), and – as a final step – Formulating a Stakeholder Participation Strategy (4). For
the first two steps, a stakeholder mapping will be developed, while the third step will be
illustrated in a stakeholder matrix. The final stakeholder participation strategy will be presented
based on the results from the mapping exercise and the matrix development.
In the third step, an adjusted SWOT analysis36 will be presented, that is based on an
extensive desk review as well as the outcomes of the first two steps of the qualitative data
analysis of the Kenyan case example. The Kenyan health financing system will be examined
and analyzed towards its potential regarding UHC using specific sub-categories from the
standardized WHO framework, which will form integral part of the SWOT analysis. The WHO
framework considers the three following factors when analyzing health systems towards its
potential regarding UHC: Coverage of Essential Health Services at Prevention and Treatment
Level (1), Coverage of Financial Protection (2), Equity in Coverage (3). For the analysis, it will
34 The interviews include two key informant interviews with the CBHF project coordinator of STIPA and one
CBHF scheme chairman as well as a qualitative survey undertaken amongst CBHF scheme officials of all existing 14 CBHF schemes STIPA is supporting. A total number of 32 scheme officials took part in the survey during a bi-annual stakeholder meeting in Kisumu city in November 2014.
35 The interviews include three interviews with members of the Kisumu county health management team as well as one interview with the Kisumu county community health strategy representative and two NHIF representatives for Kisumu County.
36 Please refer to chapter 3.2, pages 44ff. of this thesis.

97
be furthermore relevant to consider the three main components of UHC being reduced cost
sharing and user fees (4), include other services (5), and extend to the non-covered (6).37 Hence,
the named six sub-categories will be serving as guiding principles within the SWOT analysis of
step three of this data analysis.
Based on the three steps, a standard model of implementing an integrated SHI system in
Kenya will be developed. At this point, the generated lessons learnt from chapter three will
complement the collected data from the Kenyan context and hence a comparative cross-country
analysis will be applied including a comprehensive cross-country knowledge and lessons learnt
transfer. As a final step, the developed standard model will be transferred to a general level and
its relevance to most low-income countries in sub-Saharan Africa will be explored.
Background: The Community Level
Support for Tropical Initiatives in Poverty Alleviation (STIPA) is a national NGO based in
Kisumu city in the Western part of Kenya, registered in 1997. In its efforts towards participatory
community development, STIPA implements various programmes in the fields of health and
health financing, livelihoods, gender, HIV/AIDS as well as Water, Sanitation and Hygiene
(WASH) programmes.38 STIPA has been implementing the CBHF programme since 2006 and –
in its three different phases – established 14 CBHF schemes serving over 6,000 beneficiaries in
rural sites of Western Kenya. The STIPA CBHF programme also includes one special scheme
for People living with HIV and AIDS (PLWHA) and one safe motherhood pilot project, which is
incorporated in the CBHF programme. In addition, a community-based credit saving and loans
component is integrated into the STIPA CBHF programme.
STIPA facilitates the implementation of CBHF scheme in its partnering communities
through a participatory approach, using tools of Participatory Integrated Community
Development (PICD). PICD enables the community to set up their own structures, elect
community leaders and set priorities for future community development activities. As most
communities rate health and health financing as a core priority, CBHF is an adequate
programme to respond to this urgent need of rural communities in the Kenyan setting. Within
the PICD process, the community is enabled to identify vulnerable parts of the society, which
37 Please refer to chapter 2.21, Figure 1 shows the WHO cube of UHC (WHO 2010), page 16 of this thesis. 38 For more information, please refer to the STIPA website: www.stipakenya.org.

98
will be considered indigents within the future CBHF programme and benefit from premium
waiver mechanisms. In the following, the example of a PICD classification is presented, aiming
to design targeted development interventions for the different categories. The following
classification (Tables 19 and 20) was done for a STIPA target community in Nyanza province of
Kenya in 2014:
Category 1 The Rich: high income
Category 2 The Middle-Class: middle income
Category 3 The Poor: low- and/or irregular income
Category 4 The Very Poor: no or very low income
Table 19: Categories generated from PICD tool, Source: STIPA Kenya 2014.
Category 1 and 2 Category 3 and 4
• Access to primary, secondary, university and college education at quality facilities. • Steady income streams, and access to water and
sanitation services • Medical cover • Can afford a regular balanced diet • Rarely exposed to epidemics because they are
aware about the preventive measures • Have access to proper good sanitation
infrastructure and have high-quality drugs
• Hardly complete grade eight since they cannot access quality faculties • Exposed to epidemics because of low or no access to a
proper sanitation infrastructure and the use of sub-standard low-quality drugs • Cannot access health care and if they do, they get low-
quality health services, characterized by a common insufficiency of drugs and medical supply and delays in service provision at the accessed health facilities • Use herbs and traditional methods for cure
Table 20: Description of categories for Nyanza province, Kenya, Source: STIPA Kenya 2014.
The PICD classification is used to identify the target group of tailored development initiatives to
be implemented. The CBHF project mainly targets categories three (3) and four (4), while parts
of these categories can qualify to become indigents within the programme.
In addition to the participatory PICD tools, STIPA in cooperation with Freedom from
Hunger39 has developed specific participatory tools to implement CBHF. Technical Learning
Conversations (TLCs) 40 is a collection of training modules and sessions in which the
communities through participatory learning exercises learn about the concept of health
insurance and specific processes and products of CBHF.
Besides introducing the health insurance and CBHF concept to the target communities,
STIPA is supporting in the CBHF scheme management with a focus on financial management,
and also provides participatory trainings in the areas of leadership and good governance for the
established CBHF schemes. In addition, STIPA assists in assessing the involved health
providers to be contracted, and in calculating adequate premiums for local CBHF products.41
39 For more information about the learning modules, please visit the Freedom from Hunger website:
https://www.freedomfromhunger.org/education-modules. 40 Please see Annex I for the TLC manual that was adjusted to the STIPA context in 2014. 41 For more information about STIPA, please visit the STIPA website: www.stipakenya.org.

99
In the following – as illustrated in Table 21 – the products offered by established CBHF
schemes under the STIPA CBHF programme are presented (financial year of 2014). While
Product A provides benefits in OPD and IPD Services and Minor Surgeries, it also includes
Normal Delivery and Caesarean Section (C/S) for a premium of 2,000 KES, being an equivalent
of 21.50 USD.42 Product B provides the same services as Product A, with an addition of
Emergency Transport and Care Giver Allowance for a set premium of 2,400 KES, being an
equivalent of 25.80 USD. Product C is the most comprehensive product, offering the same
services as Product B, with an additional Funeral Support Benefit for a premium of 2,700 KES,
being an equivalent of 29 USD. Product D is supposed to be a complementary product for NHIF
cardholders, and is hence providing OPD Services and Funeral Support for a set premium of
1,200 KES, being an equivalent of 12.90 USD.
Product Premium (KES) Services Covered
A 2,000/= OPD + IPD + Minor Surgery + Normal
Delivery + C/S
B 2,400/= OPD + IPD + Minor Surgery + Normal
Delivery + C/S + Emergency Transport +
Care Giver Allowance
C 2,700/= OPD + IPD + Minor Surgery + Normal
Delivery + C/S + Emergency Transport +
Care Giver Allowance + Funeral Support
D 1,200/=
(NHIF card holders)
OPD + Funeral Support
Table 21: CBHF products of STIPA, Source: STIPA Kenya 2014.
The STIPA CBHF programme offers comprehensive products, including medical and non-
medical services, responding to the general aim of UHC to include other services beyond pure
medical services. Each CBHF scheme member pays 100 KES (an equal of 1 USD) of annual
registration fee to the CBHF scheme. Furthermore, specific ceiling amounts for each product
and health facility are calculated and set by STIPA to ensure that the respective scheme accesses
health services according to the scope of risk pool, size of membership and available reserves.
A common analysis from data collected in the years 2012 and 2013 provides the basis for the
following illustration of membership dynamics and general scheme performance of the STIPA
42 It is important to note that the stated premiums are standard annual amounts for a family of five.

100
supported CBHF schemes. STIPA initiated six new schemes in 2014, while in 2012 and 2013,
STIPA supported eight (8) schemes, including one special scheme for PLWHA. The schemes
showed relatively high registration rates with 1,488 households in 2012 and 1,371 households in
2013, while the completions were only at 863 households in 2012 and 570 households in 2013.
The general completion rate was hence at only 42% (2012) and 36% (2013) (USAID/SHOPS
Project 2014). In 2014, the number of completed members could be raised to 1,758 households
and 6,500 beneficiaries (STIPA 2014). STIPA envisages having 8,000 beneficiaries in 2015 as
well as up to 20,000 beneficiaries in 2018 (STIPA 2015a). Evidence shows, that while the
interest and willingness to register with the CBHF scheme of potential CBHF beneficiaries is
usually gained, it is a main challenge of all STIPA supported schemes to achieve a high
completion rate, as most registered people do not pay the full amount of premium of their
chosen product.
One measure, that STIPA established to support the CBHF communities towards a smooth
premium payment as well as to increase their general productivity level, is the Village Saving
and Loans (VSL) approach, a village-based microfinance activity. VSL aims at encouraging the
community towards governance of their own saving and credit scheme. While other – NGO or
Microfinance Institution (MFI) governed – microfinance schemes in the recent past failed or
faced challenges due to high levels of loan defaults, the approach of VSL solely uses own funds
and resources of the community members, resulting in an increased level of ownership amongst
the beneficiaries. Within the VSL approach, the savings or shares of the members serve as the
basis for loans to be provided. The loans are repaid with an interest rate of 10%. The gained
interest will be shared out to the members on an annual basis, according to their savings
contributed during the year. After initiating the VSL approach in late 2013, one of the STIPA
supported schemes, Ogera CBHF Scheme, located near Oyugis town in South Nyanza, in 2014
was able to provide loans worth 2,084,500 KES to its CBHF members, being an equivalent of
22,370 USD, which generated an interest of 200,450 KES, being an equivalent of 2,236 USD.
The interest that was shared out back to the members was used to facilitate smooth premium
payment of the CBHF premiums for the consecutive year (STIPA 2015b). Furthermore, as a
result of the VSL approach, the scheme members started small businesses or were able to
improve existing businesses in their agricultural environment. STIPA provided trainings in the
areas of social and commercial entrepreneurship to support the emerging agribusiness
engagements amongst the CBHF scheme members.
Realizing the need for a tailored scheme for PLWHA, the TAI CBHF Scheme was formed
in 2011 during the second phase of the STIPA CBHF project. TAI CBHF Scheme has been

101
supported by STIPA from its initial stage with technical support and general capacity building
and was meant to be an innovative pilot project aiming at providing access to quality health care
to PLWHA. PLWHA in Kenya are usually organized and supported according to specific
support groups funded by national or international donors and/or other crucial health
stakeholders. In this arrangement, the latter are providing essential and long-term Anti-
Retroviral Therapy (ART) and usually cover larger parts of OPD costs related with
Opportunistic Infections (OI) of PLWHA participating in their programs. TAI CBHF Scheme is
receiving support by the Catholic Relief Service (CRS), who provides comprehensive ART,
caters for OPD services and certain drugs, as well as regular counseling sessions. The CRS
project staff had been facing serious challenges regarding client’s conditions, which could not
be managed at the out-patient-clinic and patients had to be admitted in the ward for further
management. It is against this background, that TAI CBHF Scheme is catering for IPD services,
transport allowances and additional drugs, so that the provided CRS services can be
complemented in an adequate way. In addition, STIPA in close cooperation with the scheme
leaders, provide preventive health trainings, health education, and HIV/AIDS awareness
measures for the TAI CBHF Scheme members.
Perceived Role of NHIF
NHIF as the national SHI scheme in Kenya is well known by most CBHF members, as product
D was specifically designed for NHIF cardholders to provide complementary OPD and funeral
support services. The CBHF scheme officials and members perceive NHIF positively. “We are
not competing CBHF”; states Henry Ajwang, Chairperson of GAWU CBHF Scheme,
emphasizing the positive attitude of his scheme members towards the national SHI scheme.
Nevertheless, NHIF is still perceived to serve the needs of public servants and formally
employed community members only: “Some of our members are retired civil servants, so they are automatically NHIF members, others are still serving as civil servants and are covered by NHIF, so they see CBHF as a complementary product to NHIF.” (Henry Ajwang, CBHF Scheme Leader GAWU CBHF Scheme, Nyakach Area, Kisumu county)
In addition, the CBHF project did not enter into any formal relationship with NHIF yet, as stated
by Merab Okwara, project coordinator of the STIPA CBHF project: “NHIF is complementing
CBHF, but I cannot say that we have a formal partnership”. The challenge of entering into a
formal NHIF partnership – according to STIPA staff – is caused by the centralized governance
structure of the NHIF, which leaves main decision-making competences to the national level of
the NHIF head office in Nairobi, while local NHIF offices are serving the central body without
own authorities or decision-making competences. STIPA approached the local NHIF office in

102
the year 2013 in Kisumu and won the local NHIF representative as a strong supporter of CBHF
in that area. Joint mobilization activities were successfully executed in 2013 and 2014, and
STIPA would go to the field with the NHIF representative and CBHF and NHIF products were
marketed concurrently.
In addition, a qualitative survey amongst the scheme leaders of the existing 14 CBHF
schemes revealed high demand for a formal partnership between CBHF and NHIF. 96% of the
officials that participated in the survey answered the question if they wish to integrate NHIF
products into the existing CBHF products with “yes”, while only 4% stated “no”. Reasons for
favoring the partnership were above all the wish for “comprehensive treatment” (50%), as well
as “to be treated nationwide” (15%). A reason for not favoring the partnership was the fear of a
“common failure of CBHF once the NHIF system collapses” (4%).
One of the STIPA supported schemes, Ogera CBHF Scheme, implements an innovative
approach of integrating NHIF products and services within the CBHF system. In the recruitment
process for 2015, the scheme requested members that were willing to access Product D for OPD
Services and the Funeral Support Benefit to register with the NHIF prior to their enrollment
within the CBHF scheme. The NHIF membership became a mandatory precondition to access
Product D. As a result of the introduction of the mandatory element of Product D, 20% of the
Ogera CBHF Scheme members in the NHIF within a period of three months.
After a comprehensive research undertaken by STIPA in 2014, a new series of CBHF
products was developed, aiming at an integration of the NHIF as the main provider of IPD
services, which would enable the scheme members to access IPD services without a set ceiling.
The products were designed by STIPA as illustrated in Table 22. The products suggest a
comprehensive Product A, covering OPD and IPD Services, while the latter will be provided
through the NHIF. In addition, Product A covers Minor Surgery, Normal Delivery and
Caesarian Sections. The premium for Product A was calculated at 3,000 KES (22.48 USD) and
is hence slightly higher than the former comprehensive CBHF Product C for 2,700 KES (29
USD), which only covered limited IPD services, while it covered non-medical services, such as
Emergency Transport and Care Giver Allowances and Funeral Support.
Product Premium (KES) Services Covered
A 3,000/= OPD + IPD (through NHIF without
ceilings) + Minor Surgery + Normal
Delivery + C/S

103
B 2,400 /= OPD + IPD (through NHIF without
ceilings) + Minor Surgery
C 2,700/= OPD + IPD (through CBHF with ceilings)
+ Minor Surgery + Normal Delivery + C/S
+ Emergency Transport + Care Giver
Allowance + Funeral Support
D 2,000/= OPD + IPD (through CBHF with ceilings)
+ Minor Surgery
E 1,200/= OPD + Funeral Support
Table 22: Proposed combined product of CBHF/NHIF, Source: STIPA Kenya 2014.
Product B covers OPD and IPD Services through the NHIF as well as Minor Surgery for a
premium of 2,400 KES (25.80 USD). Product C is equal to the former Product C and covers
OPD and IPD Services through the CBHF scheme, Minor Surgery, Normal Delivery, Caesarian
Sections, Emergency Transport and Care Giver Allowances as well as Funeral Support for
2,700 KES (29 USD). Product D is covering OPD and IPD Services through the CBHF scheme
as well as Minor Surgery for 2,000 KES (21.50 USD), while Product E intends to cover OPD
Services and Funeral Support for 1,200 KES (12.90 USD). The proposed integrated
CBHF/NHIF products were presented to the CBHF scheme leaders in April 2014, and 88% of
the group voted for Product A, due to its comprehensive nature and wide range of benefits for a
fair price. Due to administrative challenges and funding constraints, the new products could not
yet be implemented within the STIPA supported CBHF schemes, but the need for an integrated
CBHF/NHIF product became obvious.
Besides the named approaches by CBHF schemes and supporters towards integrating
NHIF products within the CBHF system, the NHIF encourages organizations and institutions
supporting the national SHI scheme in the area of member recruitment by providing a certain
allowance for newly recruited NHIF members. The Agent-Approach has benefitted one of the
KCBHFA members, the Nyeri-based NGO Afya Yetu Initiative (AYI), who achieved a 40%
increase of NHIF membership in their target areas. The NHIF is granting a 5% premium
discount for organizations registering groups with a minimum membership of 500 households
into the NHIF. AYI established two CBHF networks covering Kirinyaga and Nyeri County, and
the gained benefit provided by the NHIF is used to cater for the administrative costs of the
CBHF networks.43
43 This information was gathered during a two-week visit of the author to AYI in Nyeri to document common
institutional memory in July 2013.

104
Perceived Strengths and Weaknesses of CBHF and NHIF
Common strengths and weaknesses have been clearly stated by the CBHF scheme officials
during the qualitative survey undertaken by STIPA in December 2014. While perceived
strengths of CBHF were stated to be “early treatment” (50%), “affordable packages to choose
from” (47%), and the fact that CBHF “unites and empowers the community” (33%); other
positive elements of CBHF named were the “community ownership and management” (27%) of
CBHF, the “coverage of non-medical services” (17%) as well as the “coverage of polygamous
families” (13%). This strongly emphasizes the strengths of CBHF schemes, which were already
assumed in chapter 2.5.1,44 namely the high level of ownership and trust of CBHF schemes, the
good governance as well as the flexibility and sensitivity of products within the CBHF
framework.
Regarding common weaknesses of CBHF schemes, the CBHF scheme officials proclaimed the
“restriction on certain facilities” (40%), the “low ceilings” (40%) and the fact that the “CBHF
concept is not easy to sell to low-income communities” (20%) as the biggest challenges within
the CBHF structure. This was already assumed in Table 1, where CBHF scored low in terms of
attractiveness of products, coverage and dimension of risk pool.
Common strengths of the NHIF as stated by the CBHF scheme officials were the
“coverage of most hospitals of the nation” (40%) and the “coverage of higher charges” (30%),
as well as the “non-existence of ceilings” (23%) within the NHIF. Negatively perceived were
the “high penalties on default” (60%) as well as the “exclusion of OPD services” (27%) within
the NHIF. Another negative element of NHIF was the “centralized and unknown leadership”
(13%), as stated by the officials. The analysis of Table 1 revealed this evidence by rating the
main advantages of national schemes in the areas of national regulation and standard procedures
as well as the attractiveness of products, the coverage and the dimension of risk pool.
Lessons Learnt
1. CBHF ensures a high level of insurance literacy, as the community-based schemes are
initiated through participatory processes and comprehensive capacity building measures on
how insurance works. Communities are hence enabled to understand how insurance works
and learn about their potential benefits. As a result, the risks of fraud and adverse selection in
the future CBHF scheme can be lowered significantly. In addition, CBHF schemes are able
to carry out tailored social marketing measures to ensure outreach to their target groups.
These measures include the close cooperation with local administrators and churches as well
44 Please refer to Table 1 on page 32 of this thesis.

105
as organized groups and community structures. Once key stakeholders are reached and are
promoting local CBHF schemes, the entire community will favor it, based on the existing
support of relevant stakeholders of the community. Most national SHI schemes lack the
general understanding of the insurance concept on various levels (communities/target groups,
health providers, government officials), which is in many cases the reason for the failure of
the scheme. In opposition to this, once comprehensive insurance education measures are
provided based on a bottom-up approach, the entire SHI system can benefit from informed
stakeholders.
2. CBHF schemes – if built on strong existing structures of social capital, e.g. established CBOs
– are very powerful institutions of the civil society and they are showing a high level of
social cohesion and are hence in a good position to identify needs and demands of the target
population. A national SHI system – partly or comprehensively – built on strong community
based structures shows high probability to succeed in terms of sustainability, targeting and
good governance.
3. CBHF officials and members rated a future integration into the NHIF as positive given the
potential increase of their benefits. The analysis emphasized a high level of awareness
amongst the CBHF scheme officials about common strengths and weaknesses of both the
CBHF schemes and the NHIF, and hence the potential synergies of an integrated approach
became obvious. The observed low level of trust and dissatisfaction with administrative
structures and procedures of the NHIF amongst CBHF members should be cushioned by an
integrated governance structure of CBHF and NHIF officials when establishing an integrated
CBHF/NHIF structure.
4. The support of CBHF schemes should rather focus on empowerment and long-term self-
reliance of the scheme, than depending on the supporting NGO structure for more than three
to five years. A recent analysis of the SHOPS project, which assessed the CBHF project on
behalf of USAID, revealed the immense resources STIPA is investing in the CBHF schemes,
while considering themselves as a provider of technical support and capacity building. An
average cost of 82,604 KES, being an equal to 789 USD, is invested in each CBHF scheme
on a monthly basis.45 Hence, the dependency ratio of the CBHF schemes on STIPA is still
high. It is advisable to reduce the support to the CBHF schemes gradually to ensure
45 Please see Annex 2 of this thesis for a comprehensive table showing the SHOPS analysis of monthly monetary support of the CBHF schemes through STIPA.

106
sustainability, ownership and long term community empowerment. This can be done through
the gradually increment of community contributions, e.g. through contribution of local
resources, such as providing community funded meals during trainings, or encouraging the
schemes to use the collected premiums for administrational expenses, e.g. for stationaries,
transport, communication, rather than relying on external support of an NGO. In addition to
this, some researchers have recently opposed CBHF schemes (e.g. Queuille and Ridde 2015),
claiming their low impact and limited coverage. In addition, as illustrated in Figure 18,
critiques are regretfully stating that CBHF supporting NGOs in sub-Saharan Africa are often
showing self-interest and creating dependencies of CBHF schemes on the supporting NGOs,
rather than empowering the communities to access adequate measures of health financing.
5. To establish effective and efficient CBHF schemes, it is important to provide adequate
structures and systems. This should be ensured during the initial stages of the scheme and
will foster the smooth take off of schemes’ operations. Adequate structures and systems
entail suitable M&E tools, which are user friendly and can be used easily in the rural
environment, e.g. paper based rather than digital or web-based tools, as well as an adequate
MIS of the scheme, that should be operational at schemes and health facility level, ideally on
the basis of an IT-system that can also translate paper-based tools into a digital database.
While during the first two years, the supporting NGO can still provide assistance in terms of
financial audits and a general monitoring and evaluation of the schemes’ operations, CBHF
scheme leaders should be trained and empowered to overtake these duties and manage the
scheme independently after a certain time of support through an external NGO.
Figure 18: Cartoon about common critiques of CBHF schemes and supporting NGO structures in West Africa, Source: Equité Santé 2015.

107
6. The integration of the VSL approach into the CBHF scheme activities has shown significant
success regarding a smooth premium payment as well as a general empowerment of the
target group, especially in terms of an increased productivity and general engagement in
small business activities in the agribusiness sector.
7. CBHF schemes show a high level of inclusion, as PLWHA are members of their schemes
through effective cooperation with supporting groups. This opposes the general view of
researchers about PLWHA as a high-risk group, which cannot be insured through health
insurance.
Background: The County Level
The current interventions in the area of health in Kisumu County are based on the Kisumu
County Health Sector Strategic and Investment Plan (KCHSSIP) for 2013 to 2017. Embedded
in the Vision 2030 of the Kenyan government, which aims at achieving a “Globally Competitive
and Prosperous Nation”, the county is envisaging attaining the “highest standards of health, in a
manner responsive to the needs of the population” (Kisumu County 2013:foreword). The
Kisumu County Directorate of Health (KCDH) defined six service delivery outcomes, namely to
Eliminate Communicable Conditions (1), to Halt and Reverse the rising Burden of non-
communicable Conditions (2), to Reduce the Burden of Violence and Injuries (3), to Provide
essential Health Services (4), to Minimize exposure to health risk factors (5), and to Strengthen
Collaboration with Health related Sectors (6). Social protection in health and specifically health
financing can be classified under outcomes 4 and 5 and is hence part of the main agenda of the
KCDH. Health financing is furthermore one of the seven infrastructure investment areas that the
KCDH has identified (Kisumu County 2013).46
The NHIF47 coverage in March 2015 in Kisumu County stands at 513,032, with 179,737
principal members and 333,295 dependents.48 The public sector represents 40,485 (22.5%) of
the NHIF beneficiaries, while the informal sector represents 62,081 (34.5%) and the private
sector represents 63,115 (35.1%). 6,057 members (3.3%) are sponsored by special programmes,
46 Further identified investment areas are Organization of Service Delivery, Human Resources for Health, Health
Infrastructure, Health Products and Technologies, Health Information and Health Leadership and Governance (Kisumu County 2013:10).
47 For a detailed description oft he NHIF scheme and its benefits, please refer to chapter 2.6.3, pp. 38 f. of this thesis.
48 The given numbers represent the status of 2nd March 2015, as provided by Eddah Nyapola in her position as NHIF representative for Kisumu County.

108
which are subsidizing or completely funding their NHIF contributions (Eddah Nyapola, NHIF
Representative Kisumu County: March 2015).
Perceived Role of CBHF
Health financing – as stated above – is one of the core areas the devolved county health
directorates are engaged in. While the county staff seems to be aware of the existing CBHF
schemes in the country – all three key informants that were interviewed49 were aware of the
NHIF and CBHF schemes as main providers of health financing in Kisumu county – the
potential benefit CBHF schemes may bring to the target communities are not yet perceived or
acknowledged.
The Community Health Management Team (CHMT) of Kisumu seems to lack knowledge
about the CBHF approach, as one of the interview partners stated that “I know about CBHF, but
I do not know about any specific one (…) and I am not familiar with the detailed operations”
(Nelly Rangara, CHMT Kisumu). Others seem to know about CBHF due to IEC materials that
were provided to the CHMT. The common vision towards social protection in health was stated
by one of the informants as an “Affordable and Equitable Health Care Scheme for All” (Collins
Omondi Onyango, CHMT Kisumu), which illustrates a clear connection to the general
orientation towards UHC. One informant described CBHF as “a community-structured way of
pooling together to raise remittance for a group health financing cover” (Kilinda Kilei, CHMT
Kisumu). In addition, there are several on-going discussions of the county with for-profit
medical schemes, such as PharmAccess,50 to be noted, which reveals an orientation towards for-
profit health financing.
Perceived Role of NHIF
A formal partnership between the NHIF and the devolved county directorates of health could
not yet been established, but the NHIF aims at engaging the counties in designing and
implementing adequate waiving mechanisms for vulnerable parts of the society, to cover them
under the NHIF (Kilian Mboya, NHIF Kisumu). As the NHIF is currently discussing new rates
for a combined IPD and OPD product through the NHIF, a partnership with the county
governments will be indispensable, as the NHIF is aiming at monthly rates as high as 500 KES
(5.4 USD), resulting in an annual premium of 6,000 KES (64.5 USD) for informal sector
employees, which is far above the estimated and assessed ability to pay of low-income people
49 The interviews were undertaken via structured qualitative questionnaires filled by three members of the Kisumu
County Health Management Team. 50 For more information, please refer to http://www.pharmaccess.org.

109
and the most vulnerable parts of the society. There is a common fear amongst NHIF
representatives to enter into a formal partnership with the county, as this might limit them to
contract government facilities, which are known to deliver low-quality health services. The
NHIF usually prefers to work with private and faith-based health providers due to the high level
of quality of care (Kilian Mboya/NHIF).
The NHIF did not yet establish a formal partnership with the Community Health Strategy
(CHS) structure as well, but one of the CHMT informants mentioned the operational plan of the
CHS, “which gives appropriate guidance on how CHWs can be capacitated to unbundle NHIF at
the community level” (Kilinda Kilei, CHMT Kisumu).
Integration of NHIF and CBHF on County Level
The NHIF Kisumu County Office aims at covering the informal sector and each of the seven
compliance officers is supposed to enroll 300 new households into the NHIF per month. One of
the NHIF representatives for Kisumu region was willing to partner with STIPA in its efforts to
support CBHF initiatives and combine it with selling NHIF to the informal sector. This
partnership started in late 2013 and the NHIF representative attended all CBHF stakeholder
meetings and joined the CBHF officials in social marketing and mobilization activities. As the
NHIF has set ambitious targets to reach the informal sector, such partnerships are indispensable.
A common challenge named by community members, the NHIF and STIPA staff, is the
lack of commitment of the NHIF to enter the community level and show their presence. The
main strategy of the NHIF is furthermore to wait for potential members to register at the NHIF
offices, a strategy, which is not very adequate, especially for people in rural areas, which may
not be aware of the NHIF procedures and may fear to approach administrative structures of the
NHIF. Evidence has shown that once NHIF staff is facilitated to enter the communities, e.g. in
terms of joint sensitization meetings with CBHF schemes, the registration rate amongst the
informal sector can be increased. This was proved in Ogera CBHF scheme, where NHIF
registration increased significantly through the introduction of a mandatory NHIF membership
to access the low-cost CBHF product covering OPD services and funeral support.
Lessons learnt
1. While public policies on county level are favoring future cooperation with the NHIF and
CBHF initiatives, e.g. through the focus on health financing, this has not yet been explored
through the county health directorates. This is a result of the limited visibility of CBHF

110
initiatives on county level and the general public, while the overall objective of providing
quality health care to the informal sector is similar for both stakeholders.
2. The current focus of the county health directorate seems to be on for-profit MHI schemes, as
the international NGOs supporting such initiatives seem to be more aggressive and successful
in creation of visibility and marketing of their interventions, while their coverage amongst
the informal sector is lower and their approach less sustainable than the CBHF initiative.
3. Evidence has shown that to successfully enter the informal sector and tailor processes to the
needs of this specific target group, the NHIF would need technical and administrative support
from community-based organizations experienced in working with this target group, e.g.
CBHF schemes. So far – besides island projects in specific areas through individual
commitment of NHIF staff – no efforts were taken by the NHIF to further support existing
efforts of CBHF initiatives towards a successful CBHF/NHIF integration.
4. The approach of NHIF to seek support at county level for identification of indigents for the
national SHI scheme was not yet explored, while it would be crucial in the scope of the
planned reform of the NHIF. The hesitance of NHIF towards cooperating with the
government structures is based on a common fear to be limited on public health facilities,
which might compromise the delivered quality of care, as private and faith-based providers
are generally considered as quality health care providers in opposition to public health
providers.
5. The NHIF or the county health directorates do not yet consider the CHS structure as a helpful
structure towards promoting UHC on community and county level, while the operational plan
of the CHS shows a clear guidance on integration of promoting the NHIF on community
level.
Table 23 illustrates different groups of relevant stakeholders within the Kenyan social protection
and health financing sector and its potential impact towards the implementation of an integrated
SHI scheme in Kenya. It is important to note that the relevant stakeholders have been clustered
in groups to avoid a high level of heterogeneity during the analysis. For a more detailed

111
description of the different stakeholder groups, please confer to chapter 2.6.3, page 38ff of this
thesis.
In the stakeholder mapping, one of the most crucial stakeholders is the Government of
Kenya, which has an interest to implement a comprehensive social protection strategy involving
a comprehensive reform of the NHIF. This strategy was already formulated, but is yet to be
implemented. The expected impact is rated as high (A). Another significant stakeholder in the
Kenyan landscape of social protection and health financing is the NHIF, as the currently
operating national SHI scheme, whose interest is focused at a comprehensive national SHI
scheme by extending the current coverage to the informal sector and other currently excluded
parts of the society, e.g. vulnerable and marginalized groups. The expected impact is rated as
high (A). As the government already engaged the communities by setting up a system of
community units countrywide in the scope of the CHS, representatives and main drivers of the
CHS are to be considered as key stakeholders within a future national SHI scheme in Kenya.
The expected impact is rated as high (A). The devolved county health directories are a result of
the devolution process implemented in Kenya from 2013. Each of the 47 counties has an
operating county health directorate, which is responsible for coordinating health interventions
on county level and closely monitors and supervises the respective public health providers. The
interest of the county health directorates in a future national SHI scheme is to ensure access to
quality health care for a wider range of their target population. Given their crucial role, also
towards a smooth communication flow from central government to county and community
levels, their impact is rated as high (A). Health providers are main players and drivers of a
future SHI scheme, as they will significantly determine the satisfaction rate amongst the
beneficiaries. Health providers have a specific interest in not only providing high quality of care
as well as transparent and accountable processes, but also to maintain and improve their facility
through a wider reliant client and patient base. Their impact is hence rated as high (A). CBHF
schemes, as they are to be seen as the main linkages to the informal sector, are to be rated as
very influential and crucial in the implementation process of the national SHI scheme. Their aim
is to empower communities of the informal and low-income sector to pool their resources
together to access quality health care. Their impact is hence rated as high (A). External Donors
in Social Protection (DSP) have an interest in funding or providing technical advice to
sustainable social protection programmes. While so far, most DSP focus on specific target
groups, their interest is usually a wider and/or universal coverage, which can be enhanced
through a national SHI scheme. Their impact is rated as high (A), because of their high
relevance to the feasibility of a national SHI scheme, especially regarding the provision of funds

112
and technical support to the same. The actual Target Communities (TCs) of the national SHI
scheme to be implemented are crucial parts of the stakeholders as they determine the success or
failure of the scheme. Their interest is to access affordable, but high quality health care through
simple and understandable processes and relevant products. The TC are also interested in being
involved in the targeting process of indigents as well as the design of processes and products of
the future system. Because of their multiple roles and their high relevance in general, their
impact is rated as high (A).
Another crucial group of stakeholders within the Kenyan social protection and health
financing landscape are representatives of Public Social Protection Funds (PSPF) that are
already operating in Kenya. They have the prior interest to extend social protection to
vulnerable parts of the society in form of social assistance as well as to provide universal safety
nets for the entire population in form of social insurance. As most of them currently have their
fixed target groups, e.g. OVCs, their impact has to be rated as medium (B), even if their
contribution towards a national SHI system is crucial. The National Social Security Fund
(NSSF) is currently in charge of providing a basic pension scheme to formally employed
Kenyans, and they have an interest in extending their services to the informal sector to ensure
wider and/or universal coverage as well as a wider range of benefits. Given their current focus
on pension systems as well as the formal sector, the impact of the NSSF is rated as medium (B).
Profit-oriented MHI schemes are offering health insurance products on a micro level and should
be integral part of a future SHI scheme in Kenya, as their interest is to provide access to quality
health care through affordable and tailored health insurance and to gain a certain benefit from
their clients and members. Their impact is assessed as medium (B), due to their low impact and
low coverage so far in Kenya as well as due to their uncertain role in a future SHI scheme.
Table 23: Stakeholder matrix for national SHI system in Kenya, Source: Author adjusted from WHO 2008b.
Stakeholder Stakeholder Interests in the Project Assessment of Impact (A, B, C)*
Central Government of
Kenya (CGoK)
To implement a comprehensive Social Protection
Strategy involving an extensive reform of the NHIF
A
NHIF Extend coverage of the NHIF to the informal sector
and people of low-income
A
Community Health
Strategy (CHS)
To empower the communities to take care of their
health and establish their own structures for (financial
and de-facto) access to health care
A
County Health
Directories (CHD)
To adequately coordinate health activities on county
level, to ensure high quality of health care and
A

113
*Impact will assessed according to A=high impact, B=moderate impact and C=low impact.
Figure 19 emphasizes the different levels of interest and power, which apply to each of the
identified stakeholders of relevance towards the development of a national SHI system. The
illustrated matrix reveals that the interest of most stakeholders is high, while power levels vary.
While public bodies – including the central government of Kenya, the county health directorates
as well as the CHS and the NHIF – are rated as powerful and influential, entities like the TC, the
CBHF schemes and the health providers are rated as less powerful, as they are not yet involved
within a larger scale-up process towards a national SHI system. Government entities concerned
with provision of social protection measures for specific target groups (e.g. the NSSF and the
PSPF in general) are rated as moderately interested and moderately powerful. The for-profit
MHI schemes are rated as interested but less powerful, as their coverage is still low and their
role within a national SHI system is not obvious yet.
(financial and de-facto) access to health services, to
ensure transparent information and communication
flow to the national level and the central government
Health Providers (H/P) To provide high quality of health care to the patients,
to provide high level of transparency and low level of
corruption and financial mismanagement, to win
enough patients to maintain the facility
A
CBHF Schemes To empower low-income communities of the
informal sector to access quality health care through
adequate health care financing measures
A
External Donors in
Social Protection and/or
Health Financing (DSP)
To give (technical and/or financial) inputs towards
provision of social protection to certain groups and/or
the entire society and ensure sustainable social
protection measures on a wide scale
A
Target Communities
(TC)
To access affordable high quality health care and
participate in the establishment of categories to
identify indigents as well as to participate in
development of adequate products and processes
A
Public Social Protection
Funds (PSPF)
To extend social protection measures to vulnerable
parts of the society and/or the entire society
B
NSSF To provide social protection to the formal sector with
possible extension to the informal sector
B
For profit MHI Schemes
(MHI)
To provide access to low-budget health insurance
products for people of low-income
B

114
The matrix illustrates the high complexity level of the envisaged SHI system, as the
heterogeneous landscape of stakeholders needs effective coordination and harmonization of
various needs and priorities. The fact that most stakeholders would need close management
highlights once more the required efforts to initiate and maintain the new national SHI system.
Each presented stakeholders will show own and unique interests and priorities within a future
SHI system. Thus, there is need for a clear definition of their roles and responsibilities within the
same. In the following, possible roles and responsibilities of various stakeholders within a future
national SHI system in Kenya are suggested.
The NHIF should be involved closely in the design and implementation of the new
system, as the Government of Kenya – in the scope of the NSPP – considers the NHIF as the
basis for a reformed national SHI scheme. Hence, the already existing administrational structure
of the NHIF, e.g. local offices, branches in urban and sub-urban areas, the MIS and M&E
system, should be used and strengthened as well as adjusted to the needs of the new system.
The Government of Kenya should play a leading role, as the new system is supposed to be
administered by one of the line ministries or a consortium of relevant line ministries (e.g.
Ministry of Health, Ministry of Gender, Children and Social Development as well as Ministry of
Figure 19: Stakeholder Matrix of national SHI System in Kenya, Source: Author.

115
Labour, Social Security and Services). The respective ministries should be involved in the overall
design and implementation of the system and will be responsible to create and spread the
political goodwill about the envisaged system. In addition, government authorities should be
engaged in advocacy measures to win a multifaceted group of stakeholders and achieve
commitment towards the national SHI scheme on different stakeholder levels.
Representatives of the CHS should use established community structures, e.g.
community units, and explore the linkages to community leaders towards the new system. The
scaling up of relevant activities implemented in the scope of the CHS should be initiated and
supported in this context.
The PSPF should be moderately involved in the design and implementation of the new
SHI system. Existing social protection measures should be reviewed and tailored towards a more
holistic approach of social protection in health and UHC. A committee consisting of high-impact
stakeholders should do the initial design. This could be realized in the scope of the planned
NSPC, which will be established on national level to prepare the launch of the NSPP.
The NSSF should be moderately involved within the design and implementation of the
new SHI system. Specifically, it should be considered to scale up tailored social protection
measures for formal employees towards the informal sector as well as to specify the role of the
NSSF within a national SHI system.
The county health directorates have a crucial role to play in the design and
implementation process of the national SHI system, as they are serving as coordinating bodies of
the central government on county level. Their relevance is hence given in the area of
coordination of the new SHI system on county level as well as in the area of creation of linkages
to relevant stakeholders on county level. They should also serve as a connecting link between the
districts levels to the national level of the central government and hence a guarantor of a smooth
information and communication flow.
As the main service providers within a national SHI system, health providers will be closely
involved in the design and implementation of the same. Specific emphasis should be laid on the
needs of health providers within a national SHI system, as well as on specific measures to
involve them in targeted marketing measures. In addition, to ensure high commitment from the
involved health providers and a high quality of health care, binding and performance-based
contracts have to be developed and signed during the design stage of the system.
The CBHF schemes are integral part of the envisaged national SHI system, and should
be closely involved in the design and implementation of the national scheme. The CBHF
schemes should play a crucial role towards the general involvement of the informal sector. Due

116
to their expertise, CBHF schemes and their supporting NGO structures should be mainly
considered to ensure participatory processes and comprehensive community participation during
all stages of design and implementation of the new SHI system. Products and processes can
hence be developed tailored to specific needs of the different target groups of a national system.
Another important function of the CBHF schemes would be to lead the process of identification
of indigents. Established CBHF schemes are in a good position to facilitate participatory
category setting and identification of the most vulnerable parts of the target group at community
level.
Existing for-profit MHI schemes should be involved moderately within the design and
implementation of a national SHI system. They are capable to built useful linkages to
commercial insurance schemes and assess the relevance of products and processes for specific
target groups, e.g. the low- and middle-income sector, which usually forms the client-base for
profit-oriented MHI schemes.
External DSP should play a crucial role within the design and implementation of the
national SHI system, due to their role in providing essential resources and technical inputs
towards the same. The existing focal areas of DSP on various areas of social protection should be
used as an entry point to sensitize DSP on a holistic approach towards social protection and
universal benefits of the same. As a result, the respective donors would be in a position to
support a universal and holistic approach towards social protection and to integrate certain
components and/or measures in their specific focal areas, e.g. OVC support or support of
PLWHA.
Target Communities of the national SHI system should be closely involved in the design
and implementation of the future system, as they will be the main drivers and supporters of the
same. Existing social capital, e.g. organized groups on community level, and high levels of social
cohesion should be used to build strong community structures, which will support the future SHI
system. These structures will result in an enhanced support of the scheme at grass-root level and
an increased level of awareness, commitment and trust towards the scheme. Table 24 provides an
overview of the different roles of relevant stakeholders as described above.
Stakeholder Potential Strategy for obtaining support and reducing
obstacles
NHIF Close involvement in design and implementation of the national SHI
system, use of administrative structures where applicable (e.g. local
office structure, MIS, M&E)
Central Government of Close involvement in design and implementation of the national SHI

117
Kenya (CGoK) system, advocacy work towards the achievement of commitment and
political goodwill towards the national SHI scheme
Community Health
Strategy
Close involvement in design and implementation of the national SHI
system, use of established community structures (community units) and
close involvement of community leaders, scale up of existing structures
and measures to the national level
Public Social Protection
Funds (PSPF)
Moderate involvement in design and implementation of the national SHI
system, scale up of tailored measures towards a holistic approach of
social protection and Universal Coverage, involvement of NSPC as a
representative committee towards design and implementation of the
national SHI system
NSSF Moderate involvement in design and implementation of the national SHI
system, scale up of tailored measures for formal employees towards a
holistic approach of Universal Coverage
County Health Directories
(CHD)
Close involvement in design and implementation of the national SHI
system, emphasis on coordination and creation of linkages to relevant
stakeholders on county level and to the national level/the central
government
Health Providers Close involvement in design and implementation of the national SHI
system, emphasis on considering their needs and involvement in
marketing of the national scheme, development of binding and
performance-based contracts for provision of high quality health care
within the national system
CBHF Schemes and
supporting NGOs
Close involvement in design and implementation of the national SHI
system, use of participatory developed processes, products and
categories to identify indigents within the national system
For profit MHI Schemes Moderate involvement in design and implementation of the national SHI
system, assessment of relevance of products and involvement of
commercial health insurance providers
External Donors in Social
Protection and/or Health
Financing (DSP)
Close involvement in design and implementation of the national SHI
system, use of existing focus on social protection to win support towards
holistic system with specific components for tailored measures for
vulnerable groups
Target Communities
(TC)
Close involvement in design and implementation of the national SHI
system, use of existing social capital and high levels of social cohesion
to reach out to the grass-root-level and increase the general awareness
and commitment towards the national scheme
Table 24: Stakeholder participation strategy matrix for national SHI system in Kenya, Source: Author.

118
After the analysis of relevant stakeholders and their possible roles within a national SHI system
in Kenya, the following section presents an adjusted SWOT analysis of the Kenyan health and
health financing sector regarding its potential towards UHC and a national SHI scheme. This
analysis will provide crucial information for the final design of lessons learnt and
recommendations towards a national SHI system in the Kenyan context.
Through the CHS, a various preventive services are delivered through the community to the
community on community level, which can be considered as a common internal strength of the
Kenyan system in the area of coverage of essential health services on prevention level. While
the named services may be limited to restricted capacities of volunteering CHWs – and the
services may differ depending on the skills of the available CHW – the community can access
certain services, even in remote and/or rural areas. Available services may include, family
planning sensitization, HIV/AIDS awareness and sensitization, as well as maternal and newborn
sensitization (Wamai 2009). In addition to this, clinical officers of public health facilities are
supposed to train the communities on preventive health care through trainings, awareness
measures and sensitization campaigns on community level. On the same note, existing CBHF
schemes – often in cooperation with local CHWs – are regularly providing capacity building
measures in the area of preventive health and health education through the CBHF scheme
members (Karanja et al 2012). Other Non-State Actors (NSA), such as the Kenya Red Cross, are
equally involved in preventive and home management services on community level (Kenya Red
Cross 2010).
On treatment level, the coverage of essential health services is effectively addressed in
the free provision of maternity services at public health facilities, although the implementation
of this policy shows main gaps, e.g. non-availability of essential equipment and drugs and
under-staffing. The Sector Wide Approach (SWAp), which is implemented by the Government
of Kenya in cooperation with main donors and technical partners in the area of health, e.g. GIZ,
World Bank and Gates Foundation, aims at a combined effort of all relevant stakeholders
towards a prioritization of provision of high quality health services (Wamai 2009). In addition, a
general improvement of quality of provided health services could be noted through the
implementation of several SHI programmes in public health facilities, such as the NHIF,
different CBHF-based programmes, and products offered by MHI schemes.51
51 This information was gathered during qualitative interviews with STIPA staff and CBHF beneficiaries in
December 2014.

119
In the area of coverage of financial protection, the NHIF contributed to provide financial
protection to a limited part of the society, while the members’ base of the NHIF is mainly
consisting of formal employees. To complement the NHIF products, various CBHF schemes
and programmes are operating nationwide, aiming at providing financial protection in health to
the informal sector. The impact of CBHF schemes is very limited though, as the existing CBHF
schemes are small schemes, comprising an average of 100 households. In addition, various MHI
schemes are offering health insurance products at low rates to the low-income population of
Kenya through cooperating with commercial health insurance schemes. The impact of MHI
schemes has to be rated as low due to the low client base. Furthermore, various commercial
health insurance schemes are operating in Kenya, aiming to serve the middle and high-income
sector. Various donor supported health insurance subsidy programmes, e.g. by World Bank and
the Bill and Melinda Gates Foundation, are in place to address the needs of vulnerable parts of
the society, such as OVCs, PLWHA and the informal sector in general. The externally funded
subsidy programmes are still in initial piloting stages, so that the impact has to be rated as
minimal, due to small island pilot projects that were not yet up-scaled to the national level or a
representative number of counties.52
In the area of equity in coverage, it has to be noted that the NHIF is designed to serve the
formal and informal sector – even if so far the informal sector only forms a minimal part of the
NHIF member base. In addition to this, the existence of CBHF schemes and MHI schemes
provides further opportunities for the informal sector to be covered through health financing
measures. Some CBHF schemes included targeted measures for specific vulnerable groups
within their health insurance products, such as specific products for PLWHA or the integration
into the CBHF scheme of OVCs benefitting from the national social cash transfer programme.
This further contributes to a certain level of equity in coverage.53
The Kenyan government introduced and proclaimed free maternal health services in July
2014, which can be regarded as a common internal strength in the area of reduced cost sharing
and user fees. Furthermore, a hospital waiving mechanism was established to waive costs for
IPD services for children under five. For NHIF members, copayments at contracted health
facilities are at a low level, ranging from 10 to 20 KES, equal to 0.10 to 0.20 USD. In addition,
several public subsidy programmes are in place, aiming to support specific target groups, such
as Tuberculosis (TBC) patients, PLWHA or malaria patients (Wamai 2009, ILO 2010).
52 This information was gathered in December 2014 during qualitative interviews with STIPA staff and
representatives of various health insurance schemes, such as CBHF schemes and the NHIF, as well as commercial health insurance schemes.
53 This information was gathered during qualitative interviews with STIPA staff and CBHF beneficiaries in December 2014.

120
In the area of common internal strengths of the Kenyan health financing system towards
including other services than health-related services, it is important to acknowledge that CBHF
and some for-profit MHI schemes are offering non-medical services, such as transport and care
giver allowances as well as funeral support as part of their products. With regards to common
strengths in extending services to the non-covered, as already stated, the NHIF was reformed to
also serve the informal sector. In addition, CBHF and MHI schemes are providing services for
the usually excluded parts of the society, people of low income working in the informal sector.54
Regarding internal weaknesses of the Kenyan health financing system on preventive level, it has
to be stated that the NHIF does not cover any preventive care or services. In addition, clinical
officers and CHWs, which are supposed to implement preventive health measures and health
education on community level, are often not skilled and/or trained to fulfill this duty accordingly
(Karanja et al 2012).55 On treatment level, evidence shows that the provided health services are
often poor in terms of quality, resulting in long waiting hours, a lack of skilled health
professional and regular shortages of drugs. Moreover, most public health providers are located
in urban or semi-urban areas, while in remote rural areas access to health providers remains a
challenge (Wamai 2009). In the area of coverage of financial protection, the Kenyan health
financing system shows main weaknesses, as there is a low coverage of existing SHI schemes to
be noted. While the NHIF covers 20% of the population, commercial health insurance schemes
are reaching only 3%. CBHF schemes are reaching 2%, while profit-oriented MHI schemes are
reaching below 1% of the population (ILO 2010). In addition, administrative weaknesses of
existing SHI schemes, e.g. in the areas of card processing and/or claims administration, have to
be noted.
Regarding equity in coverage, it is important to mention that the focus of the NHIF is on
the formal sector, while efforts towards an expansion to the informal sector and people of low
income in general are limited. The outreach of targeted schemes for excluded groups, such as
CBHF and MHI schemes is equally limited to a small percentage of the envisioned target
group.56
In regards to the objective of reduced OOPP, one main weakness of the Kenyan health financing
system is the high level of OOPP, which stands at 53.1%, which causes a huge burden on low-
54 This information was gathered during qualitative interviews with STIPA staff and representatives of CBHF
schemes and the NHIF in December 2014. 55 This information was gathered during qualitative interviews with STIPA staff and representatives of CBHF
schemes and the NHIF in December 2014. 56 This information was gathered during qualitative interviews with STIPA staff and representatives of CBHF
schemes and the NHIF in December 2014.

121
income households. Considering the possible inclusion of other non-health-related services, it
has to be stated that there is no inclusion of non-medical services within the NHIF yet.
Furthermore, the provision of non-medical services through CBHF schemes is very limited,
especially in terms of coverage – due to the low membership – and the actual benefit – due to
the low ceilings and the limited benefit package. In the area of a possible extension of social
health financing services to the excluded, as already mentioned, the overall coverage of existing
SHI schemes is low, with one quarter of the Kenyan society having access to any kind of SHI
scheme (ILO 2010).57
On the basis of the named internal strengths and weaknesses, there are various external
opportunities to mention, which may lead to an improved and efficient national SHI system in
Kenya. The planned National Social Protection Policy (NSSP)58 which considers an overhaul
and reformation of the NHIF towards UHC is a unique opportunity to address common needs of
the population towards social protection in health and also to reform the NHIF towards wider
coverage and tailored services and processes to serve the the informal sector. The planned
establishment of the Consolidated Social Protection Fund (CSPF) will furthermore provide a
potential financial basis for the implementation of a comprehensive SHI system in Kenya, while
the NSPC will support the same with technical support (ILO 2010).
In terms of coverage of essential services, opportunities to implement extensive
preventive measures through the already existing community health strategy structures should
be explored. This could be realized in cooperation with local CBHF schemes and devolved
county health structures as well as respective health providers, clinical officers and CHWs. On
treatment level, an opportunity to ensure high quality services would be the introduction of
performance-based contracts between the Government of Kenya and the health providers. This
process should be formalized and standardized to ensure a high level of implementation in
different counties. The different levels of health care should be furthermore linked to each other
through an effective and efficient referral system. With regards to a future national SHI system,
to ensure the relevance of provided services, the target communities should be involved in
prioritization of relevant health care services, which might differ depending on the county.59
Furthermore, in a future SHI system, to strengthen and extend the national coverage of financial
protection, linkages of existing CBHF and NHIF structures to established CHS structures should
57 This information was gathered during qualitative interviews with STIPA staff as well as with CBHF schemes and
the NHIF in December 2014. 58 Please refer to chapter 2.6.2 for more comprehensive information about the NSPP. 59 This information was gathered during qualitative interviews with STIPA staff as well as CBHF beneficiaries in
December 2014.

122
be strengthened and created to ensure coverage of the informal and/or rural sector through the
national system. In addition, existing social protection programmes and/or funds as well as
existing (public and private) SHI schemes should be integrated to form part of the future
national SHI system. To ensure an increased level of equity in coverage, the existing public
social protection schemes, such as the NSSF and the NHIF, should be opened to all citizens and
appropriate waiving mechanisms for vulnerable parts of the society should be designed, e.g.
through the setting up of categories based on a participatory approach comparable to the
Rwandan Ubudehe categories, using a participatory approach, as used within PICD.
Existing OOPP and user fees should be reduced through comprehensive and mandatory
coverage of the population through the new SHI scheme with appropriate waivers for ultra-poor
and/or labor-constraint households. To approach the objective of inclusion of other services
within the new SHI scheme, a comprehensive SHI benefit package should be designed,
considering non-medical services, based on the assessed needs of the communities. The product
development can be done in collaboration with established CBHF and MHI schemes, which are
offering alternative services to their health benefits. To efficiently extend the offered health
financing services to the non-covered parts of the Kenyan society, public social protection
schemes should be made accessible to all parts of the society. In addition to this, CBHF and
profit-oriented MHI initiatives should be scaled up through a long-term partnership with the
NHIF and the CHS on county and national level of the central government.60
A weak political goodwill and low level of public commitment towards UHC and the provision
of high quality health care and proper prioritization of health services are possible external
threats to the Kenyan health financing sector regarding the coverage of essential health services
on prevention and treatment level. A further threat to the coverage of financial protection is the
existing high level of heterogeneity of social insurance and social assistance schemes, resulting
in a high level of competition and a lack of clarity amongst potential partners and/or supporters
as well as the target population of a national SHI system. Moreover, the perceived high level of
financial mismanagement of the NHIF is resulting in a general low level of trust amongst de-
facto and potential members of national scheme. In the area of equity of coverage, the focus of
external supporters on specific target groups, such as PLWHA and OVCs, rather than
considering a holistic approach of social protection and UHC threatens the current social health
financing system in Kenya and might hamper the development of a national SHI system.
60 This information was gathered during qualitative interviews in December 2014 with STIPA staff as well as
representatives of various health insurance schemes, such as CBHF schemes and the NHIF.

123
Reduced cost sharing and user fees are currently threatening factors to the Kenyan health
financing system, as the high occurrence of financial mismanagement, corruption and informal
payments at health facility level may lead to increased OOPP and a reduced level of trust
amongst the target population. In the area of including other services, a main threat is the low
level of commitment of the Kenyan government and external donors towards the participatory
prioritization of services to be included within a national SHI system, which may lead to
challenges towards the inclusion of adequate alternative services. Regarding the extension of
services to the non-covered, the low level of commitment and political goodwill as well as
external donor support may result in a low uptake and/or commitment of the target population
towards a national SHI system.61
The comprehensive SWOT analysis of the Kenyan health financing sector is illustrated in the
following Tables 25 to 28. Table 25: (Internal) strengths of Kenyan health financing sector towards a national SHI Scheme,
Source: own SWOT analysis.
1. (Internal) Strengths
Coverage of Essential Health Services (Relevance, Quality, Availability)
Prevention Level: - (Limited) provision of preventive services through CHW / CHS Structure - Participation of clinical officers in preventive health care - (Limited) provision of preventive services/health education through CBHF schemes - (Limited) provision of preventive and home management services through NSA (e.g. Kenya Red Cross) Treatment Level: - Free maternity services in public health facilities - SWAp to prioritize and harmonize provided health services and programmes - Improved quality of health care through existing SHI programmes (NHIF, CBHF, MHI)
Coverage of Financial Protection
• National Hospital Insurance Fund (NHIF) aiming at national coverage • Various CBHF schemes/programmes nationwide • Various MHI schemes nationwide • Various commercial health insurance schemes • Various donor-supported health insurance subsidy
programmes (e.g. World Bank and Bill and Melinda Gates Foundation)
Equity in Coverage • NHIF is open for formal and informal sector • CBHF aims to cover the informal sector
61 This information was gathered during qualitative interviews with STIPA staff and representatives of various
health insurance schemes, such as CBHF schemes and the NHIF, as well as officials of the Kenyan government in December 2014.

124
• CBHF aims to cover PLWHA in certain areas Reduced cost sharing and User fees
• Government is implementing policy of free maternity services • Government provides hospital waivers for children under
five • Low co-payments within the NHIF (10 to 20 KES) • Several public subsidy programmes in the area of TBC,
HIV/AIDS and Malaria Inclusion of other services
• Non-medical services provided by CBHF and MHI schemes, e.g. transport and care-giver allowances and funeral support
Extension to the non-covered • CBHF aims to cover informal sector • NHIF is targeting informal sector
Table 26: (Internal) weaknesses of Kenyan health financing sector towards a national SHI scheme,
Source: own SWOT analysis.
2. (Internal) Weaknesses
Coverage of Essential Health Services (Relevance, Quality, Availability)
• Prevention Level: NHIF does not cover preventive services Clinical officers and CHWs are not sufficiently
trained on preventive care and health education • Treatment Level:
Quality of services is often poor (lack of drugs, materials, long waiting hours)
- Health Providers are not accessible to rural population staying in remote areas
Coverage of Financial Protection
• Low coverage of existing SHI schemes (NHIF: 20%, commercial health insurance schemes: 3%, CBHF: 2%, MHI: <1%) • Administrative weaknesses existing SHI schemes (e.g.
delays in card processing or claims administration) Equity in Coverage • Focus of NHIF and other public social protection
schemes on formal sector • Limited outreach of CBHF and MHI schemes
Reduced cost sharing and user fees
• OOPP remain high (53.1%) and poses a significant burden on low-income households
Inclusion of other services
• No inclusion of non-medical services within the NHIF • Provision of non-medical services through CBHF is
limited in terms of coverage (low membership) and actual benefit (low ceilings)
Extend to the non-covered
• Low coverage of existing SHI schemes (NHIF: 20%, commercial health insurance: 3%, CBHF: 2%, for-profit MHI: <1%)

125
Table 27: (External) opportunities of Kenyan health financing sector towards a national SHI scheme, Source: own SWOT analysis.
3. (External) Opportunities
Coverage of Essential Health Services (Relevance, Quality, Availability)
• Prevention Level: Extensive preventive measures through CHS
structures in cooperation with CBHF schemes, devolved county structures as well as health providers and clinical officers
• Treatment Level: To ensure high quality of services through
performance-based contracts with health providers To contract health facilities at all levels to ensure
comprehensive accessibility and set up effective and efficient referral system
To ensure relevance by involving communities in prioritization of health care services
Coverage of Financial Protection
• NSPP which considers reforming the NHIF towards UHC, establishment of Consolidated Social Protection Fund (CSPF) to fund the NSSP, establishment of NSPC to support implementation of NSSP • To create linkages of the CBHF and the NHIF to the
CHS structures to reach the rural and/or informal sector • To integrate existing social protection funds and
programmes as well as existing (public and private) SHI schemes into national SHI scheme to ensure comprehensive coverage, funding and support
Equity in Coverage
• To open public social protection schemes to all citizens and design appropriate waving mechanisms for vulnerable parts of the society (e.g. through setting up categories based on a participatory approach comparable to the Ubudehe Categories in Rwanda/the PIC approach)
Reduced cost sharing and user fees
• To reduce OOPP/user fees through comprehensive and mandatory coverage of the population through a national SHI system
Include other services
• To design a comprehensive national SHI benefit package considering non-medical services, based on the needs of the communities, e.g. transport and care giver allowances and funeral support, with the support of existing CBHF and MHI structures
Extend to the non-covered
• To open public social protection schemes to all citizens and design appropriate waving mechanisms for vulnerable parts of the society • To scale-up CBHF and for-profit MHI initiatives through
long-term linkages with the NHIF and CHS structures on county and national level

126
Table 28: (External) threats of Kenyan health financing sector towards a national SHI scheme, Source: own SWOT analysis.
4. (External) Threats
Coverage of Essential Health Services (Relevance, Quality, Availability)
• Prevention Level: Low level of political goodwill and commitment
towards UHC, quality of care and prioritization of health services
• Treatment Level: Low level of political goodwill and commitment towards UHC, quality of care and prioritization of health services
Coverage of Financial Protection
• High level of heterogeneity of social insurance and social assistance schemes, resulting in a high level of competition and lack of clarity amongst potential partners and/or supporters and the target population • High level of financial mismanagement of the NHIF
resulting in a low level of trust amongst (potential) members
Equity in Coverage
• Focus of external supporters and donors on specific groups (e.g. PLWHA, OVCs), rather than considering a holistic approach of social protection and UHC
Reduced cost sharing and user fees
• Financial mismanagement/corruption/informal payments at health facility level may result in increased OOPP and reduced level of trust amongst the target population
Include other services
• Low level of commitment of government and external donors towards participatory prioritization of services to be included within a national SHI system may lead to challenges towards the inclusion of adequate alternative services
Extend to the non-covered
• Low level of commitment and political goodwill as well as external donor support may result in a low uptake and/or commitment of the target population

127
The presented case study analysis reveals that Kenya is still in the initial stage of developing a
national SHI scheme. While current policies and existing public structures, e.g. the devolved
county structures and the CHS, as well as the national commitment towards the NSPP,
involving a general reform of the NHIF, seem to be favoring the implementation of a national
SHI scheme, the commitment of crucial stakeholders on public and private levels remains low.
Reasons for this can be found in a lack of information and exchange amongst the relevant
stakeholders in the field of social protection in health in Kenya. The landscape of social health
protection in Kenya is multifaceted and there is an urgent need for harmonization and exchange
about the development of a common effort towards providing UHC in Kenya. It became
obvious, that currently all stakeholders are working on their own agendas. It is against this
background, that the NHIF is trying to fulfill the objective of covering the informal sector
without seeking support from the county health structures and/or community-based initiatives,
while the efforts of CBHF initiatives are rarely acknowledged.
Referring to the stage model of UHC that was introduced in the first part of this thesis62
and is furthermore presented in Figure 20, it becomes evident, that Kenya is to be located in
stage one, where OOPP are a daily burden to the society as well as the absence of a
comprehensive national SHI is given. Rwanda – always considered to be the Best Practice in
reaching UHC through a community based approach, as illustrated in Figure 20, can be located
in between stage two and three, given the remaining challenges in financing and sustainability
the Rwandan system faces.
62 Please refer to chapter 2.2.2, Figure 2 on page 17 of this thesis.

128
Figure 20: Kenya and Rwanda located in the UHC Stage Model, Source: Adjusted from Carrin and James 2005.

129
From the undertaken data analysis, the following recommendations towards implementing a
national integrated SHI in Kenya can be generated. In addition, generated lessons learnt from
chapter three63 will serve as a basis for the development of tailored recommendations for the
Kenyan context.
Design
1. To fulfill the objective of designing and implementing a national SHI, the efforts of various
public and private stakeholders towards social protection in health have to be harmonized
and tailored to the common goal of a holistic system that can serve various needs of different
target groups within the country. Given the fact that Kenya is currently implementing an
extensive devolution process, the different levels of decision-making and authorities to
execute certain measures must not be neglected. Crucial stakeholders to harmonize their
efforts towards social health financing are the central and county government structures and
its relevant county directories, the relevant representatives of the CHS, the NHIF as well as
the different MHI and CBHF initiatives and their supporting NGO structures. The envisaged
committee to be established within the implementation process of the NSPP, the NSPC, will
provide an opportunity for relevant stakeholders to approach a common harmonization of
approaches and programmes. Within the NSPC, relevant donors and supporters of a national
SHI scheme should be closely involved and their importance emphasized. This will be
important to avoid a moving out of donors and supporters due to a perceived shift of
priorities of the government. In addition, besides CBHF representatives, relevant
community-based institutions and structures, e.g. CBOs and MFIs, should be part of the
NSPC to avoid replication or parallel structures besides the national system on community
level.
2. The Kenyan SHI system should be based on a formal social protection strategic document,
entailing clear and binding rules and regulations to implement the envisioned strategy. This
will emphasize the commitment of public and private stakeholders and will initiate further
support of external actors. It will also ensure a high level of visibility among the target
society. The NSPC will provide an adequate forum to develop this strategic document, as it
will be composed of all relevant stakeholders engaged in the area of social protection in
health in Kenya. The strategic document should entail a detailed timeline for implementation
63 For more information, please refer to chapter 3.5, pages 85ff., of this thesis.

130
of the national system to ensure a smooth and prompt implementation of the system without
delays.
3. The existing SWAp structure of the Kenyan government, which unites relevant stakeholders
engaged in health-related programmes and policies, should be used to involve common
health stakeholders within the design and implementation of the national SHI system. As the
SWAp is already based on a certain level of consensus, the envisaged harmonization process
should be built on existing structures involving crucial stakeholders.
4. Health providers, as crucial and key players in a national SHI system, should be involved
during the initial design stage. They should be trained on the concept of health insurance and
on general social marketing measures, to enable them to be integral part in the marketing of
the national SHI system.
5. The future national SHI system should be based on a clear and sound national policy and
coordination, while decentralized components of the system on county and community levels
should possibly possess a certain level of flexibility and authority towards decision making in
their contexts. This will be important to avoid a centralized system, which cannot be adjusted
to certain circumstances in specific areas. This flexibility is crucial towards product design,
identification of indigents as well as calculation of premiums.
6. The national SHI system should not be delinked from the envisaged NSPP, but be integral
part of the same. Ideally, the first mandate of the NSPC would be to design and implement
the planned reform of the NHIF, which is integral part of the NSPP. The NHIF reform could
hence provide the basis for a holistic SHI system in the Kenyan context.
7. While the design and implementation of the national SHI system should be closely
embedded within national policies and guidelines, such as the NSPP, it should be clearly
delinked from political activities, campaigns and any political party, e.g. in the scope of the
commencing election campaign for the general elections in 2018.
8. The design and implementation process of the national SHI system should be well structured
and comprise different stages, such as the design and the implementation stages. Roles of
involved line ministries in the area of administration and supervision of the system should be

131
clear during the initial design stage of the national system. For this purpose, the NSPC should
develop Terms of Reference (ToRs) for each involved stakeholder to clarify roles and
responsibilities within the process. The ToRs will also ensure an increased level of
accountability and transparency of the national system, as they will introduce common
checks and balances between the different stakeholders.
9. An extensive sensitization of public bodies of the Kenyan government (county and national
level) and the NHIF about the need for cooperating with CBOs and community-based
initiatives and the informal sector to reach the common aim of UHC will be indispensable. In
this context, it will be necessary to illustrate and elaborate common examples from other
countries (e.g. Tanzania, Rwanda) and to commonly agree on a strategy to formalize
partnerships on different levels of the country. The conducted stakeholder analysis of chapter
4.3.2 provides a guideline on how relevant stakeholders can be involved adequately. The
sensitization process can be initiated through the NSPC, but should also be extended to other
relevant line ministries and ideally involve the Office of the President to ensure a high level
of visibility and commitment in a national perspective.
10. Comprehensive awareness creation measures about CBHF schemes and their supporting
NGO structures should be coordinated and implemented through the NSPC to oppose the
common perception of self-interest of national NGOs amongst the international donor
community. For this purpose, common success stories from NGO supported CBHF schemes
in the areas of insuring PLWHA, provision of VSL or CBHF/NHIF integration should be
illustrated and communicated to the relevant stakeholders.
11. The Kenyan SHI system should consider and/or envision a mandatory element to ensure a
high level of coverage and commitment amongst all relevant stakeholders. The design of the
mandatory element should be coordinated through the NSPC and should entail specifics
about the implementation of the same in the informal sector. It should be considered to
transfer the responsibility of ensuring the compliance of the informal sector with the
mandatory SHI policy of the government to the involved CBHF schemes and other
community-based structures and institutions, such as the CHS. On county level, this process
should be coordinated through the County Health Directorates.

132
12. To apply a common bottom-up approach, the future SHI system should be based on strong
partnerships on community level. This should entail a formal partnership between the NHIF
and CBHF schemes. The existing CBHF products should be adjusted towards the provision
of IPD services through the NHIF, while the CBHF system should provide additional OPD
and non-medical services. Once the number of NHIF registrations increases amongst the
informal sector through the CBHF partnership, the NHIF leadership should be convinced to
enter into a formal partnership with the CBHF initiatives. As a further step, the integrated
CBHF/NHIF schemes should be enabled to enter into a formal partnership with the CHS and
the County Health Directorates and hence approach UHC on county level. This approach
should be extended to the national level, after pilots on county level proved its efficiency.
13. A crucial element of the national SHI system should be the use of participatory approaches
where possible. Specifically, approved participatory methodologies, such as PICD, should be
used to prioritize health services, categorize the target communities to design indigents as
well as design and implement proper processes and systems of the national SHI system in
Kenya.
14. The NSPC, besides providing the legal basis for the implementing committee for the national
SHI system, should serve as a technical advisory board during the design and implementation
phases of the system. Due to the involvement of all relevant stakeholders in the area of health
and social protection within the NSPC, multifaceted technical expertise on various levels will
be available.
15. The national SHI system should consider to design specific components for specific groups
through the integration of existing support measures into the national system. Social
assistance programmes, such as the CT-OVC programme, which provides cash transfers to
identified OVCs can be considered by enrolling the beneficiaries as indigents into the
national system. In the area of inclusion of and PLWHA, the cooperation with established
supporting groups might result in a further consideration of members of the supporting
groups as indigents within the national system. Institutions, programmes and organizations,
which are sponsoring NHIF membership to certain vulnerable groups should furthermore
encouraged to extend their support towards the national SHI system.

133
Sales
1. To ensure an embracement of the health insurance concept and its potential towards social
protection in health, comprehensive insurance education and social marketing measures
should be implemented on all institutional levels. This should include public bodies, the
NHIF, community-based initiatives, health providers and other financial or technical
supporters of the future national SHI system. As CBHF schemes have a wide range of
expertise in these areas, they should be closely involved in this area and provide tailored
training materials.
2. The visibility of the national SHI system – once designed and ready to be implemented –
should be enhanced through a professional marketing campaign. The design of this
nationwide campaign should be supported by marketing professionals, who will be able to
design adequate messages and decide on suitable communication channels, such as radio or
TV shows or spots, national events and production of adequate IEC materials for different
target groups of the national SHI system.
3. A professional training curriculum should be developed through the NSPC and additional
external technical expertise, e.g. from Rwanda or Ghana, to ensure comprehensive capacity
building measures on all institutional levels of the future system. The focus of the trainings
should be on institutional and managerial capacity building as well as financial management.
Based on an initial capacity assessment during the design stage of the national SHI system, a
comprehensive capacity development plan should be developed, which will provide the
framework for successful implementation of the training curriculum.
4. Regarding the development of tailored products, the NSPC should seek advice from
established CBHF and for-profit MHI schemes to ensure that the needs of the informal sector
are met. The NHIF and the commercial health insurance schemes should also be consulted to
design suitable products for the formal sector. It is recommendable to closely involve
commercial health insurance schemes, to avoid a potential competitor-ship between the
national scheme and co-existing commercial health insurance scheme. In addition,
commercial health insurance schemes show potential to be part of a national SHI scheme as
service providers and technical advisors.

134
5. To ensure a high coverage of the national SHI scheme, it should be considered to standardize
the approach of mass registrations of existing groups and/or institutions within the national
SHI scheme. This will lead to a stable membership base in a relatively short period of time as
well as to an enhanced level of public visibility and acknowledgement.
6. The offered products should clearly respond to the needs of the target group and should be as
comprehensive as possible, while the affordability of the products has to be guaranteed to the
scheme and the beneficiaries. The initial needs assessment on community level should entail
a comprehensive Willingness and Ability to Pay Study as well as a general assessment of
needs and demands of the target group.
Servicing
1. Within the NSPC – as the common planning committee of a national SHI system –
considered health providers, possibly public, private and faith-based facilities, should be
closely involved to ensure ownership of the system on health provider level and hence
guarantee a high level of quality of provided health care services. The NSPC is furthermore
an able body to provide technical input towards the maintaining of high level of quality of
care in a long-term-perspective.
2. The ToRs developed by the NSPC should determine the development and use of
Memorandums of Understanding (MoUs) between the national SHI system and the involved
health providers. The MoUs will clearly indicate the services to deliver and the amounts to be
charged to the system. This will avoid copayments and reduce fraud on health provider level
against the SHI system. To ensure a high level of quality of health care provided through
contracted health providers in the future SHI system, after a comprehensive assessment of
suitable health providers, their contracts should be designed based on certain levels of
performance they have to provide to the beneficiaries of the SHI system.
3. The future national SHI system should be based on adequate systems to ensure a smooth
implementation as well as clear information and communication channels. This entails the
design and establishment of a comprehensive MIS on all levels as well as adequate and
comprehensive M&E tools and measures. Standard manuals and procedures in this area
should be developed with support of the technical supporting committee represented through

135
the NSPC. In addition, a communication strategy should be developed to ensure a smooth
communication and information flow amongst various stakeholders of the system.
4. Regarding a preventive health component of a national SHI system, the different community-
based structures, such as the CHS, CBHF initiatives and the county health directorates should
support existing NHIF structures in the provision of adequate health education and
preventive health measures through behavior change-focused trainings on community level.
5. To ensure a smooth implementation of a national SHI system, partly based on community-
based initiatives, existing administrative weaknesses of CBHF schemes should be addressed
through the respective supporting NGO structures, so that the national system can be based
on strong building blocks. For this purpose, smooth claims settlement processes, as well as
good governance and advanced managerial skills at CBHF schemes level have to be ensured
through tailored capacity building measures in the scope of the implementation of the
capacity development plan.
6. A consistent and functional referral system should be established within the national SHI
system. This will enable the national SHI scheme to refer its beneficiaries from health
providers at the community level to the county and national level health facilities. The
referral system is part of the quality orientation of the national system and will ensure that
sincere cases of illness as well as emergencies can be managed at a higher level.
Sustainability
1. A general harmonization of interventions within the Kenyan health, health financing and
social protection sectors will build an adequate basis for a joint effort towards a national SHI
system. This should be once more emphasized through the clear demonstration of political
goodwill through the national and county governments, and the creation of sufficient
visibility of the scheme and its purpose on national level. The relevance of the scheme should
become obvious for different parts of the society, namely the informal and formal sector, as
well as involved institutional stakeholders.
2. The national SHI should be implemented in line with public reforms of the Government of
Kenya. The national SHI system should form integral part of the envisaged NSPP, while it
should be considered in the context of other planned reforms in the areas of health and social

136
protection as well. This is crucial to ensure that no public measure will be implemented that
has potential to threaten or sideline the national SHI system. To guarantee this, regular
consultations of the NSPC with relevant line ministries are considered as indispensable
within the implementation process of the national SHI system.
3. A national financial commitment, e.g. through the public commitment towards the Central
Social Protection Fund (CSPF), will significantly support the sustainability of a national SHI
system in Kenya. Public commitment will strengthen the common trust and confidence
towards the system and hence result in an increased level of commitment amongst the target
group. In addition to this, a mandatory element for all sectors of the Kenyan society – formal
and informal sector employees as well as vulnerable parts of the society through efficient
waiving mechanisms – will lead to a nationwide commitment and ownership of the national
scheme.
4. To ensure that the challenge of low-income levels of the primary target group of informal
sector employees is addressed adequately, the creation of linkages to income generating
measures as well as access to financial and other social services of low-income beneficiaries
of the national SHI system should be ensured. In this context, interventions and capacity
building measures in the areas of VSL, social entrepreneurship and financial management in
the target communities should be part of the capacity development plan. This will increase
the general level of community productivity as well as strengthen the emergence of small
agribusiness initiatives amongst the same. The creation of linkages to other essential social
services, such as nutrition, health or education, will result in an improved living standard and
an improved well-being of the specific target group of informal sector employees, and hence
an increased ability to pay for the premiums for the national SHI system.
5. The final transfer and scale up of county-based pilots of the national SHI system should be
clearly communicated to all stakeholders and furthermore determined by the strategic
document, which should entail a comprehensive section about this stage of implementation of
the national system.
6. The funding of the Kenyan national SHI system should be well balanced, considering a tax-
based element as well as premium payments from the beneficiaries and waivers for specific
groups through external donor support and the existing NSPF. The CSPF should play a

137
leading role in centralizing, pooling and distributing the funding of the national system. In
addition, during the initial phase, the Government of Kenya should consider to accept kick-
off funding and subsidies towards the administrative costs of the national system from
relevant donors.
7. The design and implementation of the national SHI system should be based on an inclusive
approach and should possibly involve a high number of relevant stakeholders from different
institutional and sectorial areas. As the NSPC will aim at building a common consensus of all
involved stakeholders, a long-term commitment of all NSPC members towards the national
SHI system will be ensured. A high profiled and multifaceted NSPC will furthermore
increase the level of visibility and perceived transparency of the entire system.
8. The implementers of the national SHI system in Kenya should ensure a measurable impact of
the system within the first three years to achieve long-term support of external donors and
technical advisors. The impact should be measured through comprehensive longitudinal
research, e.g. in form of a comprehensive impact evaluation, which should be coordinated
through the NSPC. The initial baseline study should be part of the general research phase,
which should form part of the design stage of the national system.
9. Technical support to NGOs should be provided through the NSPC towards a an increased
level of sustainability in the context of supporting CBHF schemes, including a common exit
strategy and standardized short-term support to avoid dependency and further create
independent and self- reliable CBHF schemes on community level. This tailored capacity
building measures to the CBHF schemes should be part of the capacity development plan.

138
Based on the given recommendations in chapter 4.4.2, the following section illustrates the
different design and implementation stages of a national SHI system in Kenya.
Stage 1: Design Stage
The initial stage will be the Design Stage, where the different components of the system will be
designed and the pilot phase will be prepared. The main approach is to establish a planning
committee for the national SHI system under the NSPC. The different components will
furthermore be designed and coordinated by different sub-committees of the NSPC planning
committee.
Crucial NSPC sub-committees will be established in the following areas:
Strategic Document Development
Scheme Structure and Design
Research and Knowledge Creation
Mandatory Element Design
Communication and Knowledge Exchange
Indigent Design
Social Marketing and Insurance Education
Capacity Building and Curriculum Development
Product Development
PICD Implementation
County Partnership Development
Quality of Care
Funding and Resource Mobilization
Linkages and Referral System Design
It is important to consider seeking additional technical support in the chosen focal areas to
ensure a high level of expertise and proficiency. During this phase, the sub-committee for
funding and resource mobilization has to ensure sufficient funds for the pilot stage as well as
plan forward for the national implementation of the SHI system. The envisaged timeline of the
Design Stage should be one to two years. Table 29 further illustrates the different components of
the Design Stage.

139
•
•
•
•
•
• •
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
• • •
•

140
•
•
•
• •
•
•
•
•
• •
•
•
•
•
•
•
• • •

141
•
•
•
•
• •
•
•
•
•
•
•
•
•
•
•
•
•
•
•

142
•
•
•
•
•
• •
•
•
•
•
•
•
•
•
•
•
•
•
•

143
•
•
•
•
•
•
•
•
•
•
•
•
•
• •
•
•
•
•
•
•

144
•
•
•
•
•
•
•
•
• •
•
•
• •
•
•
•
•
• • •

145
•
•
•
•
•
•
•
•
•
•
•
•
•
• •
• • •
•

146
•
Table 29: Components of Design Stage of national SHI system in Kenya, Source: Author.
Stage 2: Pilot Implementation Stage
The second stage of the design and implementation process of a national SHI system in Kenya
will be the Pilot Implementation Stage in chosen pilot counties. The number of counties should
not exceed five (5) and it is advisable to choose counties, where the NHIF and CBHF initiatives
already reached a certain percentage of the population and the level of awareness about health
insurance can be rated as relatively high as compared to other counties. In addition, there should
be a regional, cultural and religious balance between the chosen pilot districts, so that different
structures of the Kenyan society can successfully be captured during the pilot stage. The
established NSPC sub-committees will be responsible for the successful implementation of the
Pilot Implementation Stage of the national SHI system. The envisaged timeline should be one
year. Table 30 illustrates this stage and its different components.
• • •
•
•
•
•
•
•
•
•
•

147
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
• •
•

148
•
•
•
•
•
•
•
•
•
•
• •
•
• • •
•

149
•
•
•
•
•
•
•
•
•
•
• •
•
•
•
•
•
•
•
•

150
•
•
•
•
• •
•
•
•
•
•
•
•
•
•
•
•
•
•
•
• • •

151
•
•
•
•
•
• •
•
•
•
•
•
•
•
•
•
•
• •
•
•
•
•
•
•
•

152
• •
•
•
• •
•
Table 30: Components of Pilot Implementation Stage of national SHI system in Kenya, Source: Author.
Stage 3: Evaluation and Amendment Stage
After the successful completion of the Pilot Implementation Stage of the national SHI, a
comprehensive evaluation of the same will be necessary. On the basis of the results of the
evaluation, specific amendments to the scheme will be done to ensure a maximum impact and
success of the national system. The Evaluation and Amendment Stage – besides reviewing the
pilot – aims at generating lessons learnt which would support the design of standard manuals as
well as Standard Operational Procedures (SOPs). In addition, this phase entails the crucial
component of fund raising and resource mobilization for the national scale up of the SHI
system. The envisaged timeline for the evaluating and amending of the SHI system is six to
twelve months. Table 31 illustrates different components of the Evaluation and Amendment
Stage.
•
•
•
•
•
•
•
• • •

153
•
•
•
• •
•
•
•
• •
•
• •
•
•
Table 31: Components of Evaluation and Amendment Stage of national SHI system in Kenya, Source: Author.
Stage 4: National Implementation Stage
After the successful review and amendment of the national SHI system, the national scale-up
should be launched through a national campaign. The scale-up should progress in phases of
covering three (3) additional counties every month and hence aim at a national coverage of the
SHI system after 14 months. The envisaged timeline of the entire scale up and National
Implementation Stage is two (2) years. Table 32 furthermore illustrates the different components
of the National Implementation Stage.
•
• •
•
•
•
•
•

154
•
•
•
•
•
•
•
• •
•
•
•
•
• •
•
•
•
• • •
• •
•
•
•
• •
•
•
Table 32: Components of National Implementation Stage of national SHI system in Kenya, Source: Author.

155
Proposed Structure
Based on the illustrated development stages of the national SHI system, the proposed structure
for the integrated national SHI scheme in Kenya can be divided into three levels, namely the
national level, the county level and the community level. As illustrated in Figure 21, the central
coordination body of the SHI would be placed on national level, located within one of the
relevant line ministries. The overall supervision of the national system would be located in a
further line ministry, possibly in a development related section of the Ministry of Finance.
On county level, devolved SHI units would be placed within the county government structure
and would work in close collaboration with the county health directorates as well as with the
county-based structures of the NHIF. The county-based SHI units would be acting as a
coordinating body of community-based interventions in the scope of the SHI. On community
level, SHI units would be represented through a hybrid structure of CBHF and NHIF
representatives, closely linked to the public CHS structure.
On the basis of the Kenya-specific model presented in chapter 4.4.3.1, a general model can be
developed, which will apply in contexts showing similar pre-conditions as Kenya, e.g. a low-
income context, a high percentage of informal sector employees as well as a large rural sector
and economy and an existing landscape of community-based health financing schemes.
Figure 21: Proposed structure of national SHI system in Kenya, Source: Author.

156
Four stages have to be considered while implementing a national SHI system in a low-income
context, namely the Design Stage (1), the Pilot Implementation Stage (2), the Evaluation and
Amendment Stage (3) and the National Implementation Stage (4).
During the Design Stage, the main focus should be on harmonization of approaches as well as
on establishing basic structures and networks for the future national SHI system. The detailed
design of all relevant components of the national system should be the initial mandate of the
established planning committee structure. Technical inputs from external consultant as well as
experts from other countries, which already implemented a national SHI system, will
complement the multifaceted stakeholder committees. In addition, evidence creation and
assessments should form a crucial part of the Design Stage. While initial assessments and
feasibility studies on various levels will be crucial to determine and design an adequate national
system, a system which is based on a professional research framework, such as a longitudinal
impact evaluation, shows high potential to receive national and international recognition and
acknowledgement. The baseline survey for this study should be undertaken during the Design
Stage, which should take one to two years.
The Pilot Implementation Stage will be initiated through a general commitment of SHI
stakeholders, which – as part of the planning committees – will sign tailored ToRs towards their
roles and responsibilities within the future SHI system. Furthermore, the pilot stage will serve as
a testing period to confirm the relevance and feasibility of designed strategies, tools and
structures of the national SHI system. The pilot should be implemented in a limited number of
decentralized units, such as counties or districts. The choice should be representative in terms of
demographic characteristics, which are to be found around the country. All relevant components
of the future national system should be pre-tested and the impact should be evaluated through
the midline survey of the longitudinal impact evaluation, which will be undertaken at the end of
the one-year pilot stage.
During the Evaluation and Amendment Stage, the piloted components of the system as well as
the general structure and design of the same will be comprehensively evaluated and the joint
SHI stakeholder consortium will do necessary adjustments. A further crucial part of the third
stage is the fundraising and resource mobilization for the national scale up. Developed lessons
learnt and standard manuals as well as operating procedures will serve as an adequate evidence
base for fundraising at public and private level. The evaluation stage should take one to two

157
years, as an adequate knowledge creation as well as extensive resource mobilization would
require a sufficient timeframe.
The National Implementation System comprises the actual launch of the national SHI system.
While the public bodies will be responsible to show commitment and relevance of the system to
the general public, the SHI implementers will be engaged in a step-by-step scale up all
components of the SHI pilot projects to a nationwide coverage. In line with the national scale
up, the endline survey of the impact evaluation should be undertaken. The implementation stage
should take one to two years.
It has to be noted, that the provided model is considering social assistance and social insurance
measures. Because of its focus on SHI, the social insurance component is more obvious and
dominant, but it has crucial social assistance components in it, being the identification of
indigents and adequate support of the same within the system.

158
* The various components to be considered within a national SHI system are Strategic Document Development, Scheme Structure and Design, Research and Knowledge Creation, Mandatory Element Design, Communication and Knowledge Exchange, Indigent Design, Social Marketing and Insurance Education, Capacity Building and Curriculum Development, Product Development, PICD Implementation, Partnership Development on devolved administrative division level (County or District), Quality of Care, Funding and Resource Mobilization, and Linkages and Referral System Design.
Figure 22: General Stage Model for Implementation of a national SHI system in a low-income context,
Source: Author.

159
“Every country should be well-positioned by 2030 to ensure universal health coverage for all citizens at every stage of life, with particular emphasis on the provision of comprehensive and affordable primary health services” – excerpt from description of proposed SDG 5, UNSDSN 2015.
The relevance of a functional, effective and efficient SHI system was re-emphasized in the
scope of the recent development of the Sustainable Development Goals (SDG), as the proposed
SDG 564 is focusing on UHC and its close relation to general well-being and higher productivity
levels. While the crucial role of social health protection measures towards development in low-
income countries seems to be uncontested amongst the global community and common
international development actors, approaching UHC in most low-income countries in sub-
Saharan Africa remains rather a dream than a reality. As most public measures in the area of
social protection and health are known to exclude the informal sector, alternative approaches
emerged to substitute, supplement and/or complement public SHI schemes. CBHF initiatives are
established institutions in most low-income countries of sub-Saharan Africa. While their
services are tailor-made to the needs and demands of the informal sector and people of low-
income, their cooperative structure is a guarantor for good governance and a high level of trust
of members into the scheme. Realizing the potential of these micro level institutions, some
governments of low-income countries in sub-Saharan Africa designed and implemented
innovative SHI systems, partly or completely based on community-based health financing
schemes.
This thesis aimed at analyzing the potential of an integration of CBHF schemes into a
national SHI system by reviewing existing integrative systems in sub-Saharan Africa and
developing common lessons learnt from the cross-country case studies. Furthermore, this study
aimed at an in-depth analysis of the Kenyan health financing and social protection sector and the
development of a standard model of an integrative SHI system to be implemented in Kenya and
similar contexts of low-income countries of sub-Saharan Africa and the world.
During the comprehensive analysis of the four country case examples from Tanzania,
Rwanda, Burkina Faso and Ghana, it was illustrated, that each of the analyzed low-income
countries of sub-Saharan Africa – while showing similar preconditions – chose a unique path
towards approaching UHC. In the different processes of designing and implementing an
integrative SHI system, various stakeholders were involved, showing potential and commitment
to contribute to the ultimate goal of UHC. The reviewed national SHI systems and models in
this thesis emphasize diverse approaches based on various institutions and structures of public
64 For further information, please refer to http://unsdsn.org/resources/goals-and-targets/goal-5-achieve-health-and-wellbeing-at-all-ages/.

160
and private nature. The common element of the elaborated examples is the consideration of
community-based approaches to supplement or complement public efforts to provide UHC to
the target population.
On the basis of the analysis of the four country case examples, several factors of success
of a national SHI could be identified in the areas of Design, Sales, Servicing and Sustainability
of an integrated national SHI system. Besides the focus on the informal sector, the adequate
design of indigents through participatory category setting at community level, a general bottom-
up approach, and clear public guidelines and policies, including a mandatory element, proved to
be factors of success of an integrative national SHI system implemented in a low-income
context of sub-Saharan Africa. A prompt implementation process as well as a clear structure of
the system on central and devolved administrative divisions level are further guarantors of
success of an integrated national SHI system, while adequate systems and clear channels of
communication and information should not be neglected as well. The funding of the system
should be flexible and equally be based on premium payments as well as on a tax-based element
and monetary contributions from public social protection funds and external donors. This will
ensure a balanced funding, which reduces the level of OOPP, as well as avoids dependencies of
the system on one funding source.
In the area of sales, comprehensive measures in social marketing and insurance
education should be implemented on all institutional levels as well as amongst the largest target
group of the informal sector. In addition, capacities of all involved stakeholders have to be built,
specifically in the areas of financial and general scheme management. A national SHI system
that is designed in an inclusive and participatory way, e.g. by involving representatives from
public social protection funds or supporting structures for vulnerable groups as well as public
and private health providers and various types of health insurance, has high potential to become
a stable system, built on a joint and harmonized effort of the named stakeholders. To ensure a
smooth enrolment process amongst the informal sector, existing group structures and the
approach of mass registrations of entire groups and/or companies should be used. Another
crucial element within a successful integrative is the provision of high quality of care at
contracted health providers, which can be ensured through close monitoring of the health
providers as well as performance-based contracts. Health providers should also not be seen as
pure service providers, but also as implementers and building blocks of the integrative SHI
system. Hence, the close involvement of health providers within the marketing of the national
SHI scheme is indispensible. An effective referral system is a further component, which can be
associated with a high level of quality of delivered health care within a national SHI system.

161
The benefit package should be tailored to the needs of the target population, and the expertise of
CBHF schemes in participatory and community-based product design can be used to ensure the
same. In terms of sustainability of the analyzed schemes, the study revealed that a long-term
financial commitment of the government would lead to a long-term commitment amongst the
target population as well. A strong political good will would always strengthen the general
acceptance and take up of a national scheme.
The in-depth analysis of the Kenyan system showed that Kenya has still a long way to go
to effectively approach UHC. While public structures and policies – such as the devolved
county structure of the government, the established CBHF landscape, the NHIF as an existing
national SHI scheme targeting the informal sector, as well as the fact that the government is in
the initial stage of implementing a national social protection strategy – seem to favor the
implementation of an integrative national SHI system, the main hindrances could be identified
in the areas of harmonization of approaches of relevant stakeholders as well as a low level of
communication and information exchange amongst the same. The latter would be indispensable
to approach the common goal of UHC. The microanalysis of a significant part of the CBHF
landscape in Kenya emphasized the commitment of existing CBHF schemes towards an
integrative approach, e.g. regarding the successful integration of NHIF and CBHF products.
Besides main advantages of CBHF schemes, such as participatory approaches towards insurance
education, process and product development as well as indigent design, the microanalysis also
revealed main weaknesses of CBHF schemes in the area of coverage as well as technical and
financial capacities.
While Kenya is still in its initial stage of the design and implementation of an integrated
national SHI system, the in-depth analysis revealed a possible path to follow. The
comprehensive stakeholder analysis as well as the SWOT exercise emphasized that the initial
harmonization of approaches of various stakeholders in the areas of social protection and health
financing on national level would be the first step towards the design and implementation of an
integrated national SHI system. Furthermore, the effective establishment of already initiated
partnerships on community and county level would be a significant move towards building the
basis of the integrated national SHI scheme.
The comprehensive multi-level analysis revealed that – besides the named preconditions
– there is no unique guarantor for success of an integrated national SHI scheme, but the
efficiency and general success of the same can be fostered through the effective integration of
identified crucial components of the system, namely in the areas of Strategic Document
Development (1), Scheme Structure and Design (2), Research and Knowledge Creation (3),

162
Mandatory Element Design (4), Communication and Knowledge Exchange (5), Indigent Design
(6), Social Marketing and Insurance Education (7), Capacity Building and Curriculum
Development (8), Product Development (9), and PICD Implementation (10). The areas of
Quality of Care, Indigent Design and an effective design and implementation of a Mandatory
Element have to be considered as crucial, due to their high relevance towards the overall success
of a national SHI system. The named ten components should be furthermore guided by the main
principles of Public and Private Commitment (1), Participation, Communication and Inclusion
(2) as well as a general Step-by-Step Approach (3). Regarding the latter, it has to be stated, that a
timeline of five to seven years is to be regarded as realistic for a feasible design and
implementation of a national SHI system, given that the recommended design and
implementation period comprises of four different stages, namely the Design Stage, the Pilot
Implementation Stage, the Evaluation and Amendment Stage as well as the National
Implementation Stage. Figure 23 illustrates the interlinked structure of components and building
blocks of the recommended standard model of an integrative SHI scheme in a low-income
context of sub-Saharan Africa.
The analysis of the four country case examples as well as the in-depth analysis of the Kenyan
case revealed that – as a result of the high number of different stakeholders involved –
implementers have to cope with a high complexity level when implementing an integrative
national SHI system. In this context, CBHF schemes are to be considered as one of many crucial
Figure 23: Crucial components and building blocks of integrative national SHI system, Source: Author.

163
stakeholders of an integrated national SHI system, which determines a close mutual cooperation,
specifically with public structures and bodies, as indispensable. To benefit from the named
advantages of CBHF schemes in the context of a national SHI system, their capacities have to
be strengthened adequately. In addition, the micro level institutions require to be contextualized
into a nationally coordinated and governed system, and hence they have to be based on clear and
sound national policies, so that they can be enabled to supplement and complement a national
SHI scheme.
On the basis of the extensive analysis, the recommended standard model of an integrative SHI
system which considers CBHF schemes, is based on the National Health Insurance Model as
presented in chapter 2.4.1, a mixture of the Beveridge and the Bismarck model, with a clear
bottom-up orientation and focus on community-based initiatives as potential building blocks.
The funding of this integrative national SHI system, as illustrated in Figure 24, should be
flexible by applying contributory and non-contributory elements through premiums as well as
public and private funds.
Elements of social assistance and social insurance will be integrated into this integrative system,
by providing social insurance to the larger part of the population and adequate social assistance
to vulnerable parts of the population through tailored indigents and waiving mechanisms.
Based on the evidence gathered in the five analyzed countries, it has to be stated, that
CBHF and/or community-based MHI schemes should be considered as supplements or
complements, but not substitutes, of a national SHI system. In addition, due to identified
weaknesses in the area of institutional management, financial sustainability and general
Figure 24: Recommended funding of integrated SHI system, Source: Author.

164
outreach, CBHF schemes should not be considered as stand-alone-guarantors of social health
protection for the informal sector, but as crucial components within a national system based on a
holistic approach towards universal social protection in health.
Specific roles of CBHF schemes within a national SHI system in the areas of
participatory and inclusive approaches, indigent design – through participatory category setting
– and the general bottom-up/community based approach – through their cooperative and
community-based nature – as well as the monitoring of quality of care – through their close and
trustful relationship to local health providers and the existing high level of trust – are
highlighted in Figure 25. The model developed is to be rated as a recommended standard model,
which needs to be embedded in the respective context of each country and adjusted accordingly.
This thesis and its presented results are limited by different factors, which are described in the
following.
(1) The empiric data analysis of thesis considered a certain period of time and hence
captured specific evolvement and/or development stages of the different systems, which
comprised the years of 2009 to 2014.
(2) The in-depth analysis of CBHF schemes in Kenya was focused on one CBHF-supporting
structure, the national NGO STIPA, which may not be representative for other CBHF
Figure 25: Potential roles of CBHF schemes within a national SHI system, Source: Author.

165
supporting organizations, because of unique approaches and a limited scope of work,
which is currently limited to Nyanza Province of the Western Part of Kenya.
(3) The analysis was restricted to sub-Saharan African countries and neglected approaches
towards integrative national SHI systems implemented in other geographic contexts.
(4) A further fact that has been neglected in this thesis is the proofed evidence that (social)
health insurance usually faces difficulties in being accepted by and sold to the target
group, because of its nature of being an insurance for a risk that people are trying to
avoid and are usually not willing to spend their limited resources on. In some cultures, to
pay for health in advance can be translated to call for illnesses or bad luck in general,
which is another hindering factor for selling health insurance in a certain context.
Nevertheless, the recommended social marketing and insurance education measures are
one opportunity to cope with the named assumptions.
(5) The analysis presented cannot be rated as comprehensive, as further research would be
needed to exhaust the topic. In this area, a longitudinal impact evaluation of the analyzed
country case examples is recommendable to measure the de-facto impact of the
implemented systems towards UHC. Furthermore, integrative SHI system in other
geographical contexts, such as South and/or Latin America, should be analyzed to
measure their potential relevance for the low-income context of sub-Saharan Africa. In
addition to this, several quantitative ad qualitative studies are recommended for the
Kenyan context, based on the recommendations for feasibility studies and assessments
from chapter 4.4.3.1. These studies are necessary to further determine the design and
implementation of an integrated SHI system in Kenya.
The presented results oppose the view of some researchers rating the potential of CBHF as low,
while focusing on their institutional and technical weaknesses. Furthermore, this thesis aimed to
emphasize their advantages that can be strengthened through adequate measures in the areas of
capacity building and contextualization of the micro level institutions in a national framework.
For the Kenyan context, the results of this thesis reveal the crucial need for establishing a
common consensus and commitment of relevant stakeholders towards the implementation of a
national SHI scheme in Kenya. Besides the long-term recommendations presented in chapter

166
4.4.2, the following ad-hoc measures for different stakeholders within the process, are highly
recommended.
The Government of Kenya should mobilize relevant stakeholders to develop a joint
strategy paper towards the implementation of the envisioned national SHI scheme to hence
identify existing hindrances and suggest possible coping mechanisms. In addition, it is
considered as crucial to create a general understanding amongst the Kenyan population about
the importance and relevance of a national SHI scheme for people of all income levels. This
could be realized through a public show case event, e.g. key politicians joining and committing
to health insurance schemes and communicating the benefits in public. Public stakeholders of
the Kenyan government should also make use of the opportunity to learn from best practice
cases in the region, such as Rwanda and Ghana, through study tours and/or regular exchange
and dialogue between the relevant government officials. The Government of Kenya should also
ensure an adequate involvement of public and private health providers. Specific support to
public facilities should be provided through the government to strengthen their roles as main
building blocks of a future national SHI system. To build the basis for a successful kick-off of
the envisaged NSPP, the government should initiate the ad-hoc set up of the NSPC and the
CSPF. In this context, the establishment of a national SHI Planning Committee to be integrated
into the NSPC structure is indispensable.
The devolved county government structures should immediately start promoting the
relevance of a national SHI system on county level and involve relevant stakeholders within an
extensive dialogue towards a feasible implementation of the system on county level.
Furthermore, the county governments should establish a partnership with existing community-
based structures within their counties towards a joint effort in providing comprehensive SHI
measures to the population. This will foster the creation of synergies and building on existing
structures, and discourage the establishment of parallel structures. Public and private health
providers on county level should be adequately involved and supported in this process to
strengthen their roles as main building blocks of a future national SHI system. Furthermore, the
county governments should initiate an effective dialogue with the NHIF on county level and
explore the feasibility of a future cooperation within a national SHI system.
The NHIF should consider CBHF schemes and community-based government structures,
such as the CHS, as main supporters and drivers of their own agenda. In this sense, the NHIF
should work towards establishing a common consensus amongst relevant stakeholders, aiming
at building the future national SHI on existing well-established NHIF structures and standards.

167
In addition, the NHIF should develop tailored products for people of all income levels to ensure
a wide coverage of the population through the future SHI scheme.
CBHF schemes should focus on phasing out existing island projects, and rather aim at a
joint effort of all operating CBHF schemes nationwide. This joint effort should also involve the
NHIF, public government structures on community and county level, health providers as well as
private health insurance schemes. This will guarantee a large impact and possible future scale-
up of joint efforts to the national level within a national SHI system. Furthermore, CBHF
schemes should work towards an increased level of proficiency to cope with possible
requirements within a future national SHI scheme.
Private health insurance schemes should initiate and/or join a common dialogue with
relevant SHI stakeholders towards an increased outreach and the development of tailored
products for all income levels of the possible target group of a national SHI system in Kenya. In
addition, private health insurance schemes should share common lessons learnt and actuary
practices from commercial insurance practices with relevant government and NHIF stakeholders
as well as CBHF schemes, to hence ensure a high level of proficiency within the future national
SHI system.
On the basis of the successful implementation of the named ad-hoc interventions and activities,
the recommended stage model from chapter 4.4.3.1 has high probability to be successfully
adjusted and implemented.
In Malawi, the government recently introduced a new traffic information system, and made it
mandatory to register as a driver and/or owner of a vehicle.65 After the public announcement of
the new policy was spread through relevant radio and TV channels, the Office of Road Traffic
and Safety Services was swept with people and kilometer-long queues for weeks and months.
People of all income classes were found to queue and paid amounts as high as 36 USD (18,000
MWK) to renew their licenses, because they rated the lacking of a license as a relevant threat to
their lives. This is also a result of the gap of a national registration and identification system in
Malawi, which led to the situation, that a majority of people aimed at using the issued traffic
registration cards as a source of identification – As a final recommendation of this thesis,
governments of low-income countries with a high number of informal sector employees in sub-
Saharan Africa should consider this as an example and make the vision of people queuing for
getting registered for a national SHI membership card a reality in their country. It is possible,
65 The Department of Road Traffic and Safety Services (DRTSS) introduced the Malawi Traffic Information System in July 2015.

168
but the feasibility arises with national commitment and a common consensus of crucial
stakeholders on all levels about the relevance of a national SHI for their daily living contexts.

169
Achampong, E. K. (2012): The State of Information and Communication Technology and Health Informatics in Ghana. In: Online Journal of Public Health Informatics, Volume 4(2)/2012. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3615810/ (accessed 16th January 2015).
Arhinful, D.K. (2003): The solidarity of self-interest: Social and cultural feasibility of rural insurance in Ghana.
African Studies Centre – Research Report, N° 71/2003, Enschede. Arhin-Tenkorang, D. (2001). Health Insurance for the Informal Sector in Africa: Design Features, Risk Protection,
and Resource Mobilization, in: HNP Discussion Papers. The World Bank, Washington DC. Asenso-Boadi, F. M.; Agbeibor, W. (2010): Scaling Up National Health Insurance Schemes. Forum on Health
Financing in Tanzania. Blue Pearl Hotel, Dar-el-Salaam, 6th September 2010. URL: http://www.tzdpg.or.tz/fileadmin/documents/dpg_internal/dpg_working_groups_clusters/cluster_2/health/JAHSR-2010/8_NHIA_Ghana_-_Scaling_up_national_health_insurance_scheme__.pdf (accessed 11th December 2014).
Asfaw, A.; von Braun, J.; Klasen, S. (2004): How big is the Crowding-Out Effect of User Fees in the Rural Areas
of Ethiopia? Implications for Equity and Resource Mobilization. In: World Development, Vol. 32, N° 12, pp. 2065-2081.
ASMADE (2014): ONG ASMADE – 20 ans: Promotion de la Santé. URL:
http://www.ongasmade.org/index.php?option=com_content &view=article&id=62:promotion-de-la-sante&catid=39:nos-domaines-dintervention&Itemid=90 (accessed 16th January 2015).
Atim, C. (1998): The Contribution of Mutual Health Organizations to Financing, Delivering and Access to Health
Care: Synthesis of Research in Nine West and Central African Countries, Technical Report. Partnership for Health Reform. Bethesda, MD. URL: http://pdf.usaid.gov/pdf_docs/PNACH273.pdf (accessed 6th November 2014).
Bailey, C. (2004): Extending Social Security Coverage in Africa. Social Security Policy (SOC/POL), Geneva.
URL: http://www.ilo.int/public/english/protection/socsec/pol/campagne/files/addispaper.pdf (accessed 7th November 2014).
Buong, B. J. A.; Adhiambo, G. C.; Kaseje, D. O.; Mumbo, H. M.; Odera, O.; Ayugi, M. E. (2013): Uptake of
Community Health Strategy on Service Delivery and Utilization in Kenya. In: European Scientific Journal. August 2013 – Edition, Volume 9, No. 23.
Bump, J. B. (2010): The long road to universal health coverage: a century of lessons for development strategy. The
Rockefeller Foundation. URL: http://www.paho.org/forocoberturagt2014/wp-content/uploads/2014/08/DIM-The-Long-Road-to-UHC.pdf (accessed 5th February 2015).
Boateng, R. (2007): Mobilizing the private sector to develop sustainable healthcare economy in Africa. URL:
http://www.hifund.org/library/documents/HIFCO_RAS%BOATENG.pdf (accessed 14th November 2014). Carrin, G.; James, C. (2005): Social health insurance: Key factors affecting the transition towards universal
coverage. World Health Organization, Geneva. URL: http://www.who.int/health_financing/documents/shi_key_factors.pdf (accessed 15th August 2015).
CDI Bwamanda (2011): Health Insurance. CDI Bwamanda Website. URL:
http://www.cdibwamanda.com/website/main/en/?mid=Healthcare&sid=HealthInsurance (accessed 6th November 2014).
Churchill, C. (2006): Protecting the Poor – A Microinsurance Compendium. International Labour Organization and
Munich Re Foundation: Munich. Criel, B. (1998): District-Based Health Insurance in sub-Saharan Africa. Studies in Health Services Organization &
Policy, N° 9, Antwerp, Belgium.

170
Criel, B.; Kegels, G. (1997): A health insurance scheme for hospital care in Bwamanda District, Zaire: lessons and questions after 10 years of functioning. In: Tropical Medicine and International Health, Vol. 2, N° 7, pp. 654-672.
Crowe, S.; Cresswell, K.; Robertson, A.; Huby, G.; Avery, A.; Sheikh, A. (2011): The case Study Approach. BMC
Medical Research Methodology, 2011, 11:100. URL: http://www.biomedcentral.com/content/pdf/1471-2288-11-100.pdf (accessed 5th May 2015).
Damdinjav, M.; Garcia, I.; Lawson, E.; Margolis, D.; Nemeth, B. (2013): Institutional Failure in Kenya and Way
Forward. Journal of Political Inquiry at New York University, Spring Issue 2013. URL: http://www.jpinyu.com/uploads/2/5/7/5/25757258/institutional_failure_in_kenya_and_a_way_forward.pdf (accessed 20th November 2014).
Declaration of Alma-Ata (1978). International Conference on Primary Health Care, Alma-Ata, USSR, 6-12
September 1978 URL: http://www.who.int/publications/almaata_declaration_en.pdf (accessed 6th November 2014).
Deblon, Y.; Loewe, M. (2012): The Potential of Microinsurance for Social Protection. In: Churchill, C.; Matul, M.
(2012) (eds.): Protecting the Poor: A Microinsurance Compendium Vol. II, Geneva: International Labour Office and Munich Re Foundation.
Deloitte (2011): Strategic Review of the National Hospital Insurance Fund – Kenya. URL:
https://www.wbginvestmentclimate.org/advisory-services/health/upload/Strategic-review-of-the-NHIF-final.pdf (accessed 13th November 2014).
Dimitrijevi , M; Obradovi , G. (2005): Funding Social Insurance: Theoretical Aspect. In: FACTA UNIVERSITAT
– Series Law and Politics, Vol. 3, N°1, pp. 53-61. Dietrich-O’Connor, F. (2010): An Evaluation of the National Health Insurance Scheme in Ghana. University of
Guelph. URL: https://www.academia.edu/1873350/An_Evaluation_of_the_National_Health _Insurance_Scheme_in_Ghana (accessed 9th December 2014).
Dror, D.M.; Preker, A.S., Jakab, M. (2002): The Roles of Communities in Combating Social Exclusion. In: Dror,
D.M.; Preker, A.S. (Eds.): Social Reinsurance – A new Approach to Sustainable Community Health Financing. Washington D.C., pp.37-56.
Equité Santé (2015): Health Care Financing and Access in West Africa: Empirical and satirical! URL:
http://www.equitesante.org/wp-content/uploads/2015/01/Album_HFAccess_HELP-CHUM_2014_En_Screen.pdf (accessed 6th February 2015).
ESS Edunet (2013). The Case Study Approach. URL: http://essedunet.nsd.uib.no/cms/topics/family/1/1.html
(accessed 5th May 2015). European Report for Development – ERD (2010): What is Social Protection? URL: http://www.erd-
report.eu/erd/report_2010/documents/volA/factsheets/1-what_social_protection_en.pdf (accessed 6th November 2014).
Fleßa, S. (1998): Krankenversicherungen in Afrika: ein Strohhalm für das Gesundheitswesen‘, Das
Gesundheitswesen, 1/98, 60. Jahrgang, pp. 52-57. Fleßa, S. (2007): Investing in health. Overcoming the poverty trap by effective and efficient health care, Journal of
Public Health, Vol. 15, S. 415-421. Frenk, J.; de Ferranti, D. (2012): Universal health coverage: good health, good economics. In: The Lancet, Sep 8;
380 (9845): pp. 862-4. Gajate-Garrido, G.; Owusua, G. (2013): The National Health Insurance Scheme in Ghana: Implementation
Challenges and Proposed Solutions. IFPRI Discussion Paper 01309. Development Strategy and Governance Division. International Food Policy Research Institute (IFPRI). URL: http://www.ifpri.org/sites/default/files/publications/ifpridp01309.pdf (accessed 9th December 2014).

171
Global Extension of Social Security – GESS (2011). Global Extension of Social Security – Regions and Countries: Tanzania. URL: http://www.ilo.org/gimi/gess/ShowCountryProfile.do?cid=215&aid=2 (accessed 14th November 2014).
Government of Kenya (2008): Vision 2030. URL: http://www.vision2030.go.ke/ (accessed 4th November 2014). Good, C. M. (1991): Pioneer medical missions in colonial Africa. In: Social Sciences & Medicine, Vol. 32, No. 1,
pp. 1-10. Government of Kenya (2008): National Social Protection and Promotion in Kenya. Presentation during the Brazil
Study Tour for African Countries, 25th to 29th August 2008. URL: http://www.ipc-undp.org/doc_africa_brazil/KenyaI.pdf (accessed 21st November 2014).
Government of Rwanda (2012): Ministry of Health: About DHMIS. URL:
http://www.moh.gov.rw/index.php?id=129 (accessed 15th January 2015). Harrison, J. P. (2010): Strategic Planning and SWOT Analysis (Chapter 5). In: Harrison, J. P. (2010): Essentials of
Strategic Planning in Health Care. Health Administration Press. Hennig, J. (2012): The Community Health Fund (CHF) in Tanzania: Problems and solutions via collaboration with
microfinance institutions. In: Rösner, H. J.; Leppert, G.; Degens, P., Ouedraogo, L.-M. (Eds.): Handbook of Micro Health Insurance in Africa. LIT-Verlag, Münster, pp. 145-170.
Huber, G.; Hohmann, J.; Reinhard, K. (2005): Mutual Health Insurance (MHO) – Five Years’ Experience in West
Africa – Concerns, Controversies and Proposed Solutions. Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ). Division 4320 Health and Population, Eschborn.
Humba, E. (2005): Social Health Insurance – Implementing social security health care. The experience of the
National Health Insurance Fund. Hörmansdörfer, Cindy (2009). Health and Social Protection. In: OECD (Ed.). Promotion Pro-Poor Growth: Social
Protection. URL: http://www.oecd.org/dac/povertyreduction/ 43280818.pdf (accessed 6th November 2014). Hope, K. R. (2010): The Political Economy of Development in Kenya. Bloomsbury Academic, NIPPOD edition. International Labour Organization - ILO (2010): Kenya – Developing an integrated national social protection
policy. Social Security Department, International Labour Office, Geneva. URL: http://www.ilo.org/secsoc/information-resources/publications-and-tools/TCreports/WCMS_SECSOC _19224/lang--en/index.htm (accessed 19th November 2014).
Ifakara Health Institute (2012): Lessons from Community Health Fund Reform: Review of the past three years. In:
Spotlight, Volume 15. URL: http://ihi.eprints.org/1800/1/Sportlight_issue_-15_final.pdf (accessed 20th November 2014).
Jenson, J.; Fernandez, B. (2007): Health Insurance Basics: Roles for the Market and the Government in Providing,
Financing, and Regulating Private Insurance Coverage. ILR School – Cornwell University. URL: http://digitalcommons.ilr.cornell.edu/cgi/viewcontent.cgi? article=1480&context=key_workplace (accessed 5th November 2014).
Joint Learning Network on Universal Coverage (2014). Compare Reforms. URL:
http://programs.jointlearningnetwork.org/programs/compare (accessed 9th December 2014). Karanja, L. M.; Kakai, R.; Onyango, R. O. (2012): Participation of Clinical Officers in Preventive Health Care at
Rural Facilities in Kenya. In: African Journal of Health Sciences, Volume 21, N° 3-4. URL: Error! Hyperlink reference not valid. (accessed 3rd February 2015).
Kayonga, C. (2007): Towards Universal Health Coverage in Rwanda – Summary Notes from Briefing. The
Brookings Institution. URL: http://www.brookings.edu/~/media/events/ 2007/10/22%20rwanda/1022_rwanda.pdf (accessed 21st November 2014).

172
Kenya Red Cross (2010): Beyond Prevention: Home Management of Malaria in Kenya – Advocacy Report of Health Department. URL: https://ifrc.org/Global/Publications/Health/Beyond_Prevention_HMM%20Malaria-EN.pdf (accessed 3rd February 2015).
Kisumu County (2013): Health Sector Strategic and Investment Plan, 2013-2017. Republic of Kenya. Kiwara, A. D. (2007): Group Premiums in Micro Health Insurance – Experiences from Tanzania. In: East African
Journal for Public Health, Volume 4, Number 1, 2007. KPMG (2013). Devolution of Health Care Services in Kenya – Lessons learnt from other countries. URL:
https://www.kpmg.com/Africa/en/IssuesAndInsights/ArticlesPublications/Documents/Devolution%20of%20HC%20Services%20in%20Kenya.pdf (accessed 4th November 2014).
Lakin, J.; Kinuthia, J. (2013): First Do No Harm: Is Government Minding Our Health As it Devolves? Budget Brief
N°16. IBP – International Budget Partnership. URL: http://internationalbudget.org/wp-content/uploads/brief16.pdf (accessed 20th November 2014).
La Concertation (2004): Inventaire des mutuelles de santé en Afrique – Synthèse de travaux de recherché dan 11
pays. URL: http://www.social-protection.org/gimi/gess/RessourcePDF.action;jsessionid= e666a8b86c230b4b9938e219905ce25bcc3df494bf37ace973cbbaeab5fbf671.e3aTbhuLbNmSe34MchaRah8TbNn0?ressource.ressourceId=82 (accessed 12th November 2014).
Laibuta, M. (2013): Implementing devolution in Kenya: challenges and opportunities two months on. URL:
http://www.constitutionnet.org/news/implementing-devolution-kenya-challenges-and-opportunities-two-months (accessed 21st November 2014).
Lagarde, M.; Palmer, N. (2008): the impact of User Fees on health service utilization in low- and middle-income
countries: how strong is the evidence? In: Bulletin of the World Health Organization, Vol. 86, N° 11, pp. 839-848.
Leatherman, S.; Christensen, L.J.; Holtz, J. (2010): Innovations and Barriers in Health Microinsurance.
International Labour Office. Geneva: ILO. URL: http://www.ilo.org/public/english/employment/mifacility/ download/mpaper6_health_en.pdf (accessed 18th November 2014).
Le Faso (2013). Assurance maladie universelle au Burkina Faso: Le processus est en bonne voie. URL:
http://www.lefaso.net/spip.php?article53423 (accessed 11th December 2014). Leppert, G.; Degens, P., Ouedraogo, L.-M. (2012): Emergence of micro health insurance in sub-Saharan Africa. In:
Rösner, H. J.; Leppert, G.; Degens, P., Ouedraogo, L.-M. (Eds.): Handbook of Micro Health Insurance in Africa. LIT-Verlag, Münster, pp. 37-58.
Loewe, M. (2006): Downscaling upgrading or linking? Ways to realize Microinsurance. In: International Social
Security Review 59 (2), pp. 37-59. URL: http://onlinelibrary.wiley.com/doi/10.1111/j.1468-246X.2006.00238.x/pdf (accessed 18th November 2014).
Loewe, M. (2009): Soziale Sicherung, informeller Sektor und das Potential von Kleinstversicherungen. In:
Entwicklunsgtheorie und Entwicklungspolitik, Band 4, Baden-Baden. Management Sciences for Health – MSH (2013): New Information System increasing access to health data in
Rwanda. URL: https://www.msh.org/news-events/stories/new-information-system-increasing-access-to-health-data-in-rwanda (accessed 15th January 2015).
McCord, M. (2000): A synthesis of case stories from four health financing programs in Uganda, Tanzania, India
and Cambodia. Micro-Save Africa. McPake, B.; Hanson, K.; Mills, A. (1993): Community financing of health care in Africa: An evaluation of the
Bamako Initiative. In: Social Sciences & Medicine, Vol. 36, N° 11, pp.1383-1395. Micro Insurance Academy – MIA (2012): Reforming the Community Health Funds of Dodoma Region under the
Health Promotion and System Strengthening Project. URL: http://www.microinsuranceacademy.org/project/dodoma-tanzania/ (accessed 15th January 2015).

173
Microinsurance Network – MIN (2013): Microinsurance and Social Protection. Discussion Paper N°3. URL:
http://www.microinsurancenetwork.org/sites/default/files/Microinsurance_and_Social_Protection_FINAL_0.pdf (accessed 14th November 2014).
Microinsurance Network – MIN (2014): Situating Microinsurance in Social Protection: Lessons from six countries.
URL: http://www.microinsurancenetwork.org/sites/default/files/SituatingMicroinsurancein SocialProtection.pdf (accessed 9th December 2014).
Ministère de la Fonction Publique, du Travail et de la Sécurité Sociale (2014): Les mutuelles sociales au Burkina
Faso : Une passerelle pour l’assurance maladie universelle. URL: http://www.lefaso.net/spip.php?article57994 (accessed 9th December 2014).
Ministère de la Fonction Publique, du Travail et de la Securité Sociale (2013): Processus de mis en place d’un
système assurance maladie universelle: Document de Plaidoyer pour un accompagnement technique et financier du reseaux Providing for Health. URL: http://p4h-network.net/wp-content/uploads/2013/08/2013_06_14_MFPTSS_Burkina-Requete_appui_reseau_P4H.pdf (accessed 1st December 2014).
Ministry of Gender, Children and Social Development (2011): Kenya National Social Protection Strategy. URL:
http://www.africanchildforum.org/clr/policy%20per%20country/kenya/kenya_socialprot_2011_en.pdf (accessed 20th November 2014).
Ministry of Health; UNICEF (2010): Evaluation Report of the Community Health Strategy in Kenya. URL:
http://www.unicef.org/evaldatabase/files/14_2010_HE_002_Community_Strategy_Evaluation_report_ October_2010.pdf (accessed 4th November 2014).
Ministry of Health of Rwanda (2004). Mutual Health Insurance Policy in Rwanda, Kigali. Ministry of Medical Services and Ministry of Public Health and Sanitation (2012): Kenya Health Policy 2012 –
2030. URL: http://countryoffice.unfpa.org/ kenya/drive/FinalKenya HealthPolicyBook.pdf (accessed on 4th November 2014).
Ministry of Labour, Social Security and Services (2012): Strategic Plan 2013-2017. URL:
http://www.labour.go.ke/downloads/Ministry%20of%20Labour%20Strategic%20Plan%20201-2014.pdf (accessed 20th November 2014).
Mtei, G.; Muligan, J. A. (2007): Community Health Funds in Tanzania: A literature review. Ifakara Health
Research and Development Centre. Mukabaranga, R. (2005): Mutual health insurance in Rwanda. Presentation on the 25th of June 2005. Ndiaye, P.; Soors, W.; Criel, B. (2007): A view from beneath: Community health insurance in Africa. In: Tropical
Medicine and International Health, Vol. 12, N°2, pp.157-161. Norton, A.; Conway, T.; Foster, M. (2001): Social Protection Concepts and Approaches: Implications for Policy
and Practice in International Development. Centre for Aid and Public Expenditure – Overseas Development Institute.
Nyandekwe, M.; Nzayirambaho, M.; Kakoma, J.B. (2012): Universal health coverage in Rwanda: dream or reality?
URL: http://www.panafrican-med-journal.com/content/article/17/232/full/ (accessed 1st December 2014). Ouedraogo, L.-M. (2012): “Access for all” and “Reaching the poor”? Integration of mutual health insurance units
into public social security arrangements – benefits and risks for mutual schemes. In: Rösner, H. J.; Leppert, G.; Degens, P., Ouedraogo, L.-M. (Eds.): Handbook of Micro Health Insurance in Africa. LIT-Verlag, Münster, pp. 429-457.
Ouedraogo, L.-M.; Degens, P.; Leppert, G. (2012): Introduction: Social Protection in Health through Micro Health
Insurance in sub-Saharan Africa. In: Rösner, H. J.; Leppert, G.; Degens, P., Ouedraogo, L.-M. (Eds.): Handbook of Micro Health Insurance in Africa. LIT-Verlag, Münster, pp. 3-18.

174
Owusu-Asamoah, K. (2012): Modeling an information management system for the National Health Insurance Scheme in Ghana. Loughborough University - Institutional Repository. URL: https://dspace.lboro.ac.uk/dspace-jspui/bitstream/2134/16415/4/Thesis-2014-Owusu-Asamoah.pdf (accessed 15th January 2015).
Oxfam International (2011): Achieving a shared Goal: Free Universal Health Coverage in Ghana. URL:
http://www.oxfam.org/sites/www.oxfam.org/files/rr-achieving-shared-goal-healthcare-ghana-090311-en.pdf (accessed 11th December 2014).
Ralf Bunch Institute for international Studies (2009): The UN and Human Development. UN Intellectual History
Project – Briefing Note Nr. 8 – July 2009. URL: http://www.unhistory.org/briefing/ 8HumDev.pdf (accessed 29th October 2014).
République du Togo (2010): Programme Pays de Promotion du Travail Décent au Togo. 2010-2015. Rogers-Witte, B.; Guedenet, C.; Stellini, C.; Marienau, S. (2009): Improving Access to Health Care for Vulnerable
Children in Tanzania: An Evaluation of Pact’s Community Health Fund Insurance Card Implementation. URL: http://elliott.gwu.edu/assets/docs/acad/ids/capstone/c09_Tanzania_br_cg_cs_sm.pdf (accessed 28th November 2014).
Rösner, H. J. (2012): Micro Health Insurance in different institutional settings. In: Rösner, H. J.; Leppert, G.;
Degens, P., Ouedraogo, L.-M. (Eds.): Handbook of Micro Health Insurance in Africa. LIT-Verlag, Münster, pp. 21-36.
Roth, J.; McCord, M.; Liber, D. (2007): The Landscape of Microinsurance in the World’s 100 Poorest Countries.
Microinsurance Centre. URL: http://www.munichre-foundation.org/dms/MRS/Documents/Microinsurance/2012MILandscape/2007Landscape100poorestcountries_E.pdf (accessed 7th November 2014).
Savedoff, W. (2004): Tax-Based Financing for Health Systems: Options and Experiences. World Health
Organization. URL: http://www.who.int/health_financing/taxed_based_financing_dp_04_4.pdf (accessed on 4th November 2014).
Schmeer, Kemmi (1999): Guidelines for Conduction a Stakeholder Analysis. Bethesda, MD: Partnerships for
Health Reform, Abt Associates Inc. URL: http://www.who.int/management/partnerships/overall/GuidelinesConductingStakeholderAnalysis.pdf (accessed 3rd February 2015).
Seynou, Saibou (2009): Améliorer le financement de la santé au Burkina Faso à travers la mise en place d’un
Système National d’Assurance Maladie. Presentation at MunichRe International Microinsurance Conference (IMC) in Dakar, October 2009.
Shepard, D.S.; Vian, T.; Kleinau, E.F. (1990): Health Insurance in Zaire. Vol. 1. Policy Research and External
Affairs Working Paper, N°489. Washington, DC. URL: http://www-wds.worldbank.org/external/default/WDSContentServer/IW3P/IB/1990/08/01/000009265_3960929185712/Rendered/PDF/multi0page.pdf (Accessed 6th November 2014).
Singleton, J. L. (2006): Negotiating Change: An Analysis of the origins of Ghana’s National Health Insurance Act.
URL: http://digitalcommons.macalester.edu/cgi/viewcontent.cgi?article=1001&context=soci_honors (accessed 9th December 2014).
Solidarité Socialiste (2011): Le rôle de la société civil – Les mutuelles de santé au Burkina Faso. Presented on 15th
December 2011 in Brussels. URL: http://www.be-causehealth.be/media/14706/Be%20cause%20health%20-%202%20Le%20role%20de%20la%20societe %20civile_WS-SolSoc.pdf (accessed 9th December 2014).
Support for Tropical Initiatives in Poverty Alleviation – STIPA (2014): Bi-Annual Report, covering April-
September 2014. Prepared to be submitted to Bread for the World, Germany. Support for Tropical Initiatives in Poverty Alleviation – STIPA (2015a): Community Based Health Financing –
New Phase Proposal: 2015-2018. Prepared to be submitted to Bread for the World, Germany.

175
Support for Tropical Initiatives in Poverty Alleviation – STIPA (2015b): Ogera CBHF Scheme. VSL Financial Report. Prepared for Annual Sharing Out, 5th February 2015.
Swiss Tropical Institute of Public Health – Swiss TPH (2013): Launch of the Re-designed Community Health
Funds in Dodoma Region – 26.03.2013. URL: http://www.swisstph.ch/en/news/news/launch-of-the-re-designed-community-health-funds-in-dodoma-region.html (accessed 15th January 2015).
Tanzania Network of Community Health Funds – TNCHF (2006). Operations manual for implementation and
management of the Community Health Fund in Tanga Region – A Manual for Practitioners. URL: http://www.tgpsh.or.tz/uploads/media/Tanga_CHF_ Cook_Book_January_01.pdf (accessed 5th November 2014).
Tanzania Network of Community Health Funds – TNCHF (2010). TNCHF – Tanzanian Network of Community
Health Funds. CEO PROGRESS REPORT, Reporting Period: 2010. Prepared by: Sr. Rita Toutant/CEO TNCHF. URL: http://www.tnchf.or.tz/uploads/media/TNCHF_CEO_Progress__Report.docx (accessed 5th November 2014).
The Transfer Project (2014). The Kenya Cash Transfer Program for Orphans and Vulnerable Children (CT-OVC). URL: http://www.cpc.unc.edu/projects/transfer/countries/kenya.
The World Bank Group (2000): Beyond Economic Growth: Chapter 1: What is Development? URL:
http://www.worldbank.org/depweb/beyond/global/ chapter1.html (accessed 29th October 2014). United Nations Development Programme – UNDP (1990): Human Development Report 1990. United Nations Development Programme – UNDP (1996): Human Development Report 1996. New York/Oxford,
Oxford University Press: 1996. United Nations – UN (2000): Millennium Development Goals. URL: http://www.un.org/millenniumgoals/
(accessed 4th November 2014). United Nations – UN (2012): Report of the United Nations Conference on Sustainable Development – Rio de
Janeiro, Brazil, 20-22 June 2012. URL: Error! Hyperlink reference not valid. (accessed 29th October 2014).
United Republic of Tanzania (2003): The National Social Security Policy. URL:
http://www.tanzania.go.tz/pdf/policy%20framework%20final%20social%20security.pdf (accessed 12th November 2014).
Unni, J.; Rani, U (2002): Insecurities of Informal Workers in Gujarat, India, SES Papers 30, International Labour
Organization, Geneva. USAID (2006): Rwanda HMIS Assessment Report. Prepared by RTI International. URL:
http://pdf.usaid.gov/pdf_docs/PNADG504.pdf (accessed 16th January 2015). USAID/SHOPS Project (2014): Assessing the Feasibility of merging community based health financing schemes in
Kenya. Van Ginneken, W. (2003): Extending Social Security: Policies for Developing Countries. In: ESS Paper Series, N°
13, ILO, Geneva. Wamai, Richard (2009): The Kenya Health System – Analysis of the situation and enduring challenges. URL:
https://www.med.or.jp/english/journal/pdf/2009_02/134_140.pdf (accessed 13th November 2014). Wiesmann, D., Jütting, J. P. (2001): Determinants of viable health insurance schemes in rural Sub-Sahara Africa.
URL: http://www.zef.de/fileadmin/webfiles/downloads/articles/juetting-determinants-health-insurance.PDF (accessed 4th November 2014).
Worboys, M. (2000): The Colonial World as Mission and Mandate: Leprosy and Empire, 1900-1940, In: Osiris,
Vol. 15, pp. 207-218

176
World Bank (2005): What is Stakeholder Analysis? URL: http://www1.worldbank.org/publicsector/anticorrupt/PoliticalEconomy/PDFVersion.pdf (accessed 3rd February 2015).
World Bank (2012): Devolution without Disruption – Pathways to a successful new Kenya: Executive Summary.
Australia AID and Worldbank – Kenya Fiscal Decentralizaion Knowledge Programme. URL: http://www.tisa.or.ke/uploads/Devolution-Without-Disruption-by-The-World-Bank.pdf (accessed 20th November 2014).
World Health Organization – WHO (1946): Constitution of the World Health Organization. URL:
http://apps.who.int/gb/DGNP/pdf_files/constitution-en.pdf (accessed 4th November 2014). World Health Organization – WHO (2000): The World Health Report 2000 – Health Systems: Improving
Performance. URL: http://www.who.int/whr/2000/en/ whr00_en.pdf (accessed on 4th November 2014). World Health Organization - WHO (2006): National Health Accounts: Tanzania. URL:
http://www.who.int/nha/country/tza/tanzania-nha-_2002-2003_and_2005-2006.pdf (accessed 28th November 2014).
World Health Organization – WHO (2007): Everybody’s Business – Strengthening Health Systems to improve
Health Outcomes – The WHO Framework for Action. URL: http://www.who.int/healthsystems/strategy/everybodys_business.pdf (accessed 4th November 2014).
World Health Organization – WHO (2008a): Sharing the burden of sickness: Mutual health insurance in Rwanda.
Bulletin of World Health Organization, Vol. 86, No. 11. World Health Organization – WHO (2008b): How to conduct a Stakeholder Analysis. Transforming Health
Priorities into Projects – Health Action in Crisis. URL: http://www.who.int/hac/techguidance/training/stakeholder%20analysis%20ppt.pdf (accessed 2nd February 2015).
World Health Organization – WHO (2009): Systems Thinking for Health System’s Strengthening. Alliance for
Health Policy and System Research. URL: http://www.who.int/alliance-hpsr/resources/9789241563895/en/ (accessed 7th November 2014).
World Health Organization – WHO (2010): Obstacles in the process of establishing a sustainable National Health
Insurance Scheme: Insights from Ghana. Technical Brief for Policy Makers. URL: http://www.who.int/health_financing/pb_e_10_01-ghana-nhis.pdf (accessed 9th December 2014).
World Health Organization – WHO (2014): Monitoring and Progress towards Universal Health Coverage at
Country and Global Levels. Framework, Measures and Targets. URL: http://apps.who.int/iris/bitstream/10665/112824/1/WHO_HIS_HIA_14.1_eng.pdf (accessed 12th November 2014).
World Social Protection Report (2010): URL: http://www.ilo.org/wcmsp5/groups/public/---dgreports/---
dcomm/documents/publication/wcms_245201.pdf (accessed 7th November 2014).

177

1 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 1: Costs and Risks of Illness
Objectives
By the end of this Technical Learning Conversation, participants will have:
Calculated the costs and risks of an illness.
Preparation
1 green bottle cap, 1 yellow or orange bottle cap and 1 red bottle cap. If you do not have bottle caps, you can use 3 pieces of different colored paper (green, yellow, red) or other different colored tokens.
Bag or box 20 stones Pictures 1 and 2
Time
75 minutes
Steps
1. Introduce the topic of health insurance – 20 minutes
Illnesses can negatively affect you and your family’s health and finances. Today and during the
next 5 Technical Learning Conversations, we are going to learn about preparing to use health
insurance to face illness.
Put the red, yellow and green bottle caps in a bag or box. Then say:
Before we start today’s Technical Learning Conversation, let us play a game. I need 3
volunteers.
After identifying 3 volunteers, say:
I have 3 bottle caps inside this bag. I am going to ask the 3 volunteers to close their eyes and take
1 bottle cap from this bag. Each bottle cap represents their health:
. Green bottle cap represents a healthy family,
. Yellow bottle cap represents a person who needs to get tests and buy medicine
. Red bottle cap represents a person who needs to be hospitalized

2 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
The person who takes the green bottle cap represents a healthy family and wins the game.
After each volunteer takes a bottle cap from the bag, ask the volunteers to face the rest of the
group. Then ask the volunteer who has the green bottle cap:
How did you feel when you found out you were healthy?
[Relieved and happy. I know I do not have to spend money, I do not have to go to the
hospital.]
Then ask the volunteer who has the yellow bottle cap:
How did you feel when you found out you have to get tests and buy medicine?
[Worried, I know I have to spend money on the tests and medicines, I might even have to go
to the hospital if it is something bad.]
Then ask the volunteer who has the red bottle cap:
How did you feel when you found out you have to be hospitalized?
[Very worried and sad. I know I have to spend a lot of money on hospital bills.]
Real life is very much like this game. Sometimes we are lucky and stay healthy. We feel happy
and relaxed during those times. Many times, we are not so lucky and we get sick and feel
worried and sad. But we never know when illness is going to strike and we need to prepare for it.
The Technical Learning Conversations we are starting today are going to help you prepare for
illnesses.
Specifically, we are going to look at the services of the Community Based Health Financing Scheme so called CBHF in your area. These services can help you to manage the costs and risks of illness. These services can help you prepare for illness before it strikes.
What questions or comments do you have about this topic?
Respond to questions.
2. Tell a story to identify costs and risks of illness – 20 minutes
Now, I am going to tell you the story of Caroline’s illness. You are going to help calculate the cost
of Caroline’s illness using these stones.

3 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Place 10 stones in the middle of the group. Then say:
Each stone represents 200 KSh. Let us count 1000 right now. Please count with me.
Place stones on a flat surface where everyone can see—one by one. Have participants count with
you— 200, 400, 600, 800, 1000 KSh.
Show Picture 1 and say:
Every time Caroline spends money to treat her illness, I am going to ask a volunteer from the group
to come forward and put the appropriate number of stones on top of this picture.
Place the picture on a flat surface where everyone can see. Note that refer to the number of
stones that should be placed on the picture.
Caroline’s Illness
Caroline a has a stand in the market where she sells fruits and vegetables. Caroline has been suffering from body pain, fevers and chills for more than a week. One day the pain was so strong that she had to go to the hospital.
Caroline’s Illness
Picture 1: Costs of Illness Transportation
Caroline paid 600 KSh for the bus and a taxi to travel to and from the hospital.
Ask a volunteer from the group to put the correct amount of stones (2) on top of the
picture of the bus. Ask the group to count (“2”).
Picture 1: Costs of Illness Hospital
In the hospital, they found that Caroline had a serious case of malaria and needed to be hospitalized. She paid 1000 KSh for 5 days in the hospital.
Ask a volunteer from the group to put the correct amount of stones (5) on top of the
picture of the bed. Ask the group to count
(“200, 400, 600, 800, 1000”).
Picture 1: Costs of Illness Tests
Before leaving the hospital, the doctors ran some tests. Caroline paid 800 KSh for the tests.
Ask a volunteer from the group to put the

4 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
correct amount of stones (2) on top of the
picture of the needle. Ask the group to
count (“200, 400”).
Picture 1: Costs of Illness Medicines
When Caroline was released from the hospital, she bought medicine to finish treating her illness. She spent 600 KSh on the medicine.
Ask a volunteer from the group to put the correct amount of stones (2) on top of the
picture of the medicine bottle. Ask the group to count (“200, 400, 600”).
That is the first part of Caroline’s story. I want a volunteer to use the stones to count all of the
money she spends on her illness.
Ask a volunteer to use the stones to count all of the money Caroline spent on her illness—200, 400, 600, 800, 1000, 1200, 1400, 1600, 1800, 2000, 2200, 2400, 2600, 2800, 3000. Thank the volunteer and say:
How much money did Caroline spend to treat her illness?
[3000 KSh]
Thank the volunteer and then continue to tell the story as you show participants Picture 2.
We just calculated the money that Caroline actually spent treating her illness. When she is sick and
cannot be at her business, she does not earn money. Now let us calculate the money that Caroline
was not able to earn because she was sick. .
Picture 2: Lost Time at Work When Caroline went to the hospital
Caroline could not work. She lost 5 precious days of work. During those days, she would have made a total of 1000 KSh. Place the picture on the floor. Ask the group to count (“200, 400, 600, 800, 1000”) as each stone is placed on the picture.
How much money did Caroline lose the opportunity to make because she was in the hospital and not at work?
[1000 KSh]
What is the sum of money Caroline spent to treat her illness plus the money she was never able to make because of her illness?
[4000 KSh]
Yes, the total cost of Caroline’s illness is 4000 KSh —all of the expenses she had to pay, such as

5 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
transportation, hospital, tests and medicine, plus the money she could not earn because she was
sick.
Leave pictures 1 and 2 on the ground for the entire Technical Learning Conversation.
Let us continue Caroline’s story.
To pay the costs of her illness, Caroline had to sell her best clothing. She also had to borrow money
from a moneylender who charges a lot in interest. Caroline is worried because she is not sure she
has enough money to pay back the loan and feed her family. And she does not have her clothing
to fall back on.
What did Caroline do to get money to cover her illness?
[She sold her best clothing and borrowed money from a moneylender.]
Why is Caroline worried?
[She is not sure she has enough money to pay the loan and feed her family. And she does not
have her clothing to fall back on.]
These are the risks of Caroline’s illness—not having enough money to pay her loan and feed her
family and not having her clothing to fall back on.
What questions do you have about the costs and risks of illness?
Respond to questions.
3. Have small groups calculate the costs and risks of an illness – 30 minutes
Now you are going to work in groups to calculate the costs and risks of a serious illness that you
or any family member has suffered.
Form 4 groups.
Each group must choose a serious illness that a group member or a family member suffered in
the past. Examples of major illnesses include health conditions requiring surgery, problems
during childbirth, malaria, typhoid fever or injuries from traffic accidents.
In your group, calculate the costs of the illness that your group chose. Use the pictures to identify
and calculate the costs. You have 15 minutes.

6 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Visit each group and help them calculate the costs of illness. Remind groups to calculate the
money they did not earn because they were sick. After 15 minutes, ask:
How much do you spend to treat the illness?
[Total number of KSh for transportation, hospital stay, tests and medication.]
How much money were you not able to earn because you were sick?
[Count the number of days sick and then add together the amount of money that would have
been earned each day.]
What did you do to pay for this illness?
[Take out a loan, sell your best clothing or use all of the family’s savings.]
After all groups contribute to at least 1 of the above questions, thank them for sharing and
congratulate them for their work. Then say:
It is important to remember these costs because we are going to talk about them again later.
4. Invite participants to commit to talking to their family about the costs and risks of
illness– 5 minutes
Remember that all illnesses have costs and risks.
Some costs are the actual money spent in treating the illness. Other costs relate to the money that you are not able to make because of having the illness.
Some risks of illness include spending all of our income or savings, selling clothing, cooking utensils or things that help us earn money, or taking out a loan to treat the illness.
You can protect your family from these costs and risks of illness with health insurance. In the
next Technical Learning Conversation, we are going to learn about how health insurance works.
If you commit to talking to your family about the costs and risks of illness before the next
Technical Learning Conversation, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

7 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 2: How Health Insurance Works
Objectives
By the end of this Technical Learning Conversation, participants will have:
1. Compared the costs of treating illness with and without health insurance.
2. Practiced telling someone about how health insurance works.
Preparation
1 green bottle cap and 2 red bottle caps. If you do not have bottle caps, you can use pieces of different colored paper (green, red) or other tokens.
150 stones (organize stones into piles (see Step 2) before beginning the Technical Learning Conversation)
Pictures 1 and 2
Time
60 minutes
Steps
1. Review the costs and risks of illness– 10 minutes
Last time we discussed the costs and risks of illness. And you committed to talking to someone
about the costs and risks of illness. Let us review now.
Show and review pictures 1 and 2 as participants answer these questions.
What are some of the costs of illness?
[Transportation, hospital, tests, medicines, lost time at work.]
What are some of the risks of illness?
[Spending all of our income or savings; selling clothing, cooking utensils or things that help
us earn money; or taking out a loan to treat the illness.]
Thank them. Then ask:
Who would like to learn about 1 way to manage the costs and risks of illnesses?
We are going to talk about a service that can help you manage the costs and risks of serious
illnesses. We cannot know who in our family might get sick or have an accident or when it might
happen. But we can take steps to help us cover the costs and get the health services that we need.

8 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
2. Play a game to show how health insurance works – 25 minutes
The service that can help protect you and your family if you get sick is called health insurance.
Health insurance helps to pay for the costs of treating an illness. You can get health insurance
from Community Based Health Financing (CBHF) which is a community based health insurance.
Let us play a game to help you understand how health insurance works. I need 2 volunteers.
After identifying 2 volunteers, say:
___________ (insert the name of Volunteer 1) is a representative from CBHF.
___________ (insert the name of Volunteer 2) is a representative from the local hospital or health provider.
The rest of the participants are going to form 3 groups or families.
Form 3 groups and distribute 20 stones to each group and say:
Each group represents 1 family. Each family just received 20 stones. Remember that each stone
equals 200 KSh. Therefore, in total, you have 4000 KSh. This is money you earned that you use to
cover your expenses. At the end of the game, the group with more money wins.
All but 1 family is going to buy health insurance through CBHF. If you are a family that buys health insurance,
you must pay ________________ (insert the name of Volunteer 1) 2000 KSh or 10 stones.
Remember that ___________ (insert the name of Volunteer 1) is a representative from CBHF.
Which family would like to be the one that does NOT buy health insurance and saves 2000 KSh?
After 1 group volunteers to be the one that does not buy health insurance, say:
Now __________________ (insert the name of Volunteer 1) is going to collect 2000 KSh for the
insurance payment from the families that decided to buy health insurance. The family makes this
2000 KSh payment only one time which gives the family the right to have CBHF pay for some of
the costs of treating illness, for one year.
Ask Volunteer 1 to collect the 2000 KSh or 10 stones from each family with health insurance—20
stones total. Have the volunteer put the money in a pile on a flat surface on which everyone can
see.

9 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
How much money does each family have?
[2 families have 2000 KSh or 10 stones and 1 family still has 4000 KSh or 20 stones.]
Who is the winner so far?
[The ones who did not buy the insurance.]
Just as some of you decided to buy insurance, there are families in other communities that also
decided to buy insurance. Therefore, we are going to add their payments to CBHF’s pool of
money. The CBHF’s pool of money can pay for any big expense that might come along. Also add more stones representing other families that paid health insurance.
Now it is time for us to face illness with or without health insurance. I need 1 volunteer from each family to step forward.
After 1 person from each family steps forward, say:
I am now going to ask the volunteers to close their eyes. I am going to give each of you a red or
green bottle cap. The green bottle cap means that you are healthy. The red bottle cap means that
you are sick and have to be hospitalized.
Give 1 bottle cap to each person. Make sure you give 1 of the red bottle caps to the family that
did not buy insurance. After you distribute the bottle caps, say:
The unlucky ones who got the red bottle caps have to go to the hospital. The person who does
not have health insurance has to pay 4000 KSH to___________________ (insert the name of
Volunteer 2). Remember that _______________ (insert the name of Volunteer 2) is a
representative from the hospital. The person who does have health insurance does not have to
pay anything because CBHF pays the hospital directly.
Ask Volunteer 1 (the representative from CBHF) to take the 4000 KSh or 20 Stones from CBHF’s pile
of stones and give them to Volunteer 2 (the hospital).
Which family did not get insurance, but got sick? How much money do you have?
[no money is left.]
Which family got insurance and got sick? How much money do you have?
[2000 KSh or 10 stones]

10 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Which families got insurance, but did not get sick? How much money do you have?
[2000 KSh or 10 stones]
Who are the winners in this game? Why?
[Those who bought health insurance because they did not have to worry about paying for
illness and they had peace of mind.]
Then say:
This is how health insurance works. You pay CBHF for health insurance. In turn, the money
collected is used by CBHF to cover some of the costs for you and those unfortunate people who
get sick or are injured in an accident. CBHF still pays for the health services that are covered by
the health insurance even if the costs are more than the amount you paid to CBHF.
What questions do you have about how health insurance works?
Respond to questions, but do not discuss the details of the health insurance available to them.
This will be done in a later Technical Learning Conversation.
3. Ask participants to role-play talking with their family about how insurance works –
20 minutes
Form groups of 2.
Before making a decision about whether to get health insurance, it is important for your
husbands or others who make decisions in your family to understand how health insurance
works.
Now you are going to practice a role-play in groups of 2. One person will play the role of the
husband and the other will play the role of the wife. You have 2 minutes to describe how health
insurance works to your partner.
After 2 minutes, invite groups to change roles.
You are now going to change roles. You have 2 minutes to describe how health insurance works
to your partner.

11 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
After another 2 minutes, invite participants to come together again as a large group. Then say:
Now I invite members of 1 group to do their role-play for all of us.
After the role-play, thank the volunteers and clarify any misunderstandings participants have
about health insurance.
4. Invite participants to commit to telling others how health insurance works – 5 minutes
Remember that when you buy health insurance, you pay a set amount of money to CBHF. In turn,
the money collected is used by the CBHF to cover some of the costs for you and those
unfortunate people who got sick or were injured in an accident.
In the next Technical Learning Conversation, we are going to discuss some of the advantages of
health insurance.
If you commit to telling your family about how health insurance works before the next Technical
Learning Conversation, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

12 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 3: Advantages of Health Insurance
Objectives
By the end of this Technical Learning Conversation, participants will have:
Named the advantages of getting early access to health services by having health insurance.
Preparation
50 stones
Time
65 minutes
Steps
1. Review how health insurance works – 10 minutes
Last time we discussed how health insurance works. You committed to telling your family about
how health insurance works.
What did you tell them about how health insurance works?
[You pay a set amount of money to CBHF. In turn, the money collected is used by the CBHF to
cover some of the costs for you and those unfortunate people who got sick or were injured in
an accident.]
Thank participants. Then say:
I encourage everyone to tell other people how health insurance works.
Now imagine that your young child is in danger of being burned from a flame in the kitchen.
What would you do to keep your child from being hurt?
After participants share, say:
When 1 of our children is in danger of being burned, we would do everything to prevent it. We
would think ahead by making sure the flame is out of reach of our child or watch our child
closely. We would also act fast by pulling our child away from a flame if they got too close to it.

13 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Just as we protect our children from being burned, we can protect our families from the costs and
risks of future illness if we think ahead and act fast before it is too late. Today we are going to
talk about how health insurance can help us get needed health services to avoid more serious and
costly illnesses.
2. Tell 2 stories about accessing health services – 30 minutes
I am going to tell you the story of Akinyi and Onyango. They both have different ways to face illness.
Let us first listen to the story of Akinyi.
How Akinyi faces Illness
Akinyi started feeling very sick with body pain, a fever and chills. She wanted to go to the clinic,
but she was worried that she could not afford the cost of transport, the doctor visit, tests and
medicine. So she decided to take some medicines a friend recommended and hoped that she
would feel better. However, instead of getting better, Akinyi began to feel worse. She finally went
to the clinic when the pain got really bad. The doctor hospitalized her for one week. She had to
sell two chickens and one goat to help pay the hospital bill. The doctor released Akinyi from the hospital, but told her she has to spend 1 month in bed to recover. Between the week that she was in the hospital and the month she needs to spend in bed, she estimates that she is losing the opportunity to make 7000 KSh in her business. Now she is very worried and does
not know how she is going to take care of her business and provide for her family during the
coming month.
What happened to Akinyi?
[She got sick, waited until the pain was very bad to go to the doctor, was hospitalized for 1
week and now needs to spend 1 month in bed.]
What did Akinyi have to do to pay the hospital bill?
[She had to sell her best clothing and cooking utensils to help pay the hospital bill.]
How did Akinyi lose 7000 KSh?
[She had to spend 1week in the hospital and 1 month in bed and she was not able to work
and make money during that time.]

14 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Now listen to the story of Onyango.
How Onyango faces Illness
Onyango is a Boda Boda Driver. He started feeling very sick with body pain, a fever and chills. Because he has health
insurance, he decided to go right away to the clinic. He had malaria. Fortunately, the doctor
was able to treat his malaria before it was too serious. Onyango was disappointed because he could
have made 400 KSh in his business that day. However, Onyango was able to go back to work right
away and take care of his family. He was very relieved and happy because his health insurance
paid for the cost of malaria. Planning ahead by getting health insurance and acting fast helped
her to avoid more serious health and money problems.
How is Onyango’s story similar to Akinyi’s story?
[They both got sick.]
How is Onyango’s story different from Akinyi’s story?
[Onyango has health insurance. He went to the hospital right away and the hospital treated him.
He had to stay in the hospital only 1 day instead of 1 week. He was able to go back to work right away. Onyango’s illness cost much less and he did not have to worry about how to pay the
costs.]
Thank participants.
If you treat illnesses early, you can often reduce their total costs including the cost of health
services and the time lost at work. Planning ahead by getting health insurance can help you to act
fast to avoid serious illnesses and serious money problems.
3. Ask participants to name the advantages of health insurance – 20 minutes
Form 2 groups. Then say:
Each team has 2 minutes to discuss all of the advantages of health insurance.
In a couple of minutes, we are going to play a game. Each team is going to name the advantages

15 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
of health insurance—one by one. For each new advantage your team names, you win 1 stone.
The team with the most stones is the winner.
After 2 minutes, invite each team to name advantages—one by one. Only give the teams a stone if
they name a new advantage. You can write them down in your notebook to help you remember
the advantages that were named. After participants name all of the advantages they can, have
them count the stones. Then say:
Congratulations! Both teams named many important advantages of health insurance.
Mention the following points if participants have not done so already:
Advantages of Health Insurance
You do not have to borrow money from family, friends or moneylenders to pay for health emergencies. You can have peace of mind. If you access health services quickly, your illness does not get worse. You may not be sick as long, so you can continue to take care of your family and business. If you get treatment for your illness right away, it might not spread to other family members.
4. Invite participants to commit to telling others the advantages of health insurance – 5
minutes
Remember that there are many advantages of health insurance. Health insurance can give you
early access to treatment and can help you protect you and your family’s health and money.
In the next Technical Learning Conversation, we are going to talk about the health insurance
available to you.
If you commit to telling your family about the advantages of health insurance before the next
Technical Learning Conversation, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

16 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 4: Health Insurance Available to You
Objectives
By the end of this Technical Learning Conversation, participants will have:
1. Identified the Covered Services available to them.
2. Calculated the total Yearly Payment for family members who would be enrolled in health
insurance.
Preparation
Before facilitating the Technical Learning Conversation, insert the appropriate information about the health insurance that is available to participants [Yearly Payment, Eligibility, Covered Services].
Before facilitating the Technical Learning Conversation, make sure that STIPA has reviewed and made the appropriate changes on the Description of the Health Insurance handout. Make copies for each participant. Or, if available, distribute CBHF brochures with similar information.
Obtain information about the location of the nearest CBHF office and the name of a representative at the office.
100 stones Pictures 3–5 Product descriptions CBHF brochures
Time
65 minutes
Steps
1. Review the advantages of health insurance – 10 minutes
Last time we discussed the advantages of health insurance. Now let us review.
What are the advantages of health insurance?
[Encourage participants to share what they remember. Mention the following points if
participants have not done so already:
You do not have to borrow money from family, friends or moneylenders to pay for health emergencies.
You can have peace of mind.

17 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
You do not have to sell chickens, goats or assets to pay for treatment If you access health services quickly, your illness does not get worse. You may not be sick as long, so you can continue to take care of your family and
business. If you get treatment for your illness right away, it might not spread to other family
members.]
Thank participants. Then say:
I encourage everyone to tell other people about the advantages of having health insurance and
the ways health insurance can protect your family’s health and money!
Now please close your eyes.
Without opening your eyes, who can tell me how many children are here?
Note: If there are no children around, ask for something else that they can count. For example,
the number of trees around the meeting place.
After some volunteers make a guess, say:
Now open your eyes. Sometimes there are things that you do not notice even though they are
there. The same could happen when you agree to buy health insurance. There could be
information about health insurance that we are not aware of even though it is right in front of us.
Today we are going to talk about the basic terms and words that describe health insurance so that
before you commit to buying it, you understand everything about it.
2. Use pictures to explain the health insurance available – 30 minutes
I need 3 volunteers to help me hold the pictures.
After identifying 3 volunteers, have them stand in a line in front of the group. With the remaining
participants, form 2 groups.
I am going to tell you the story of Janet. Janet is learning about the CBHF of Nyanza Provinze in Kenya, the same health insurance that is available to you. As I tell you the story, I am going to
ask you some questions. The group that answers the question first gets a point.
Show and explain Pictures 3, 4 and 5, one at a time. After you explain each picture, hand it to

18 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
the volunteer in the line. Then ask the questions located below the box.
Health Insurance Available to Janet and You
Picture 3: Yearly Payment
Janet learns that health insurance is available to her from the CBHF scheme. The Yearly Payment is the money she has to pay to CBHF to have one year of health insurance for five members of her family. The Yearly Payment depends on the product Janet had chosen. There are different products as presented in these pictures (show CBHF product descriptions of Product A to D)
The yearly payment for Product A is 2000 KSh for a family of five.
The yearly payment for Product B is 2400 KSh for a family of five.
The yearly payment for Product C is 2700 KSh for a family of five.
The yearly payment for Product D is 1200 KSh for a family of five. This product is only for people that are also insured by the NHIF. NHIF is also a health insurance. But it is managed by the government and it only takes care of inpatient costs of your illnesses. It is called the National Health Insurance Fund. If you want to know about their rates, we can explain you where the next NHIF office is.
Janet also learns that she must ask whether there are any additional fees she has to pay with her Yearly Payment.
What is the Yearly Payment for health insurance for a family of five?
[It depends on the product chosen and ranges between 1200 and 2700 KSh.]
How often do you have to pay for health insurance?
[Once per year.]
Give points to the groups that answer the questions correctly. Then continue the story:
Picture 4: Eligibility
Janet learns that Eligibility means who can be covered by the health insurance. Janet learns that
her family members can be covered by health insurance if she pays their Yearly Payment. The premium is for five members of a family. But additional members of the family can be insured by paying a small top up.

19 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Who is eligible for health insurance?
[Everyone who pays the Yearly Payment.]
If Janet wants to get health insurance for herself, her husband, her 2 children and her grandmother, what is her payment contribution?
[Depending on the product, she has to pay the annual premium ranging from 1200 to 2700 KSh, because the product is for five members of a family].
Give points to the groups that answer the questions correctly. Then continue the story:
Picture 5: Covered Services
Janet learns that Covered Services are the health services that the health insurance pays for if you are sick or have an accident. Janet now knows that Covered Services from her CBHF include some medicines, doctor’s visits and tests, surgeries, childbirth, emergencies and more. These covered Services are available to Janet once she has been registered with CBHF and completed her premium. The registration fee for CBHF is 100 KSh. Janet also learned that the insurance does not pay for all services, but for everything which is included in the product package she has chosen before. For example, funeral support is only given in Products C and D.
What are the Covered Services available to Janet through CBHF in Product A?
[OPD + IPD + Minor Surgery + Normal Delivery + C/S ]
What are the Covered Services available to Janet through CBHF in Product B?
[OPD + IPD + Minor Surgery + Normal Delivery + C/S +Emergency Transport]
What are the Covered Services available to Janet through CBHF in Product C?
[OPD + IPD + Minor Surgery + Normal Delivery + C/S +Emergency Transport + Care giver Allowance + funeral support]
What are the Covered Services available to Janet through CBHF in Product D?
[Product D is only for NHIF card holders, it covers for OPD and funeral support]
How long does Janet have to wait before she can access the Covered Services?
[Until she paid the registration fee and completed her premium]
What are some things that health insurance does not pay for?
[Everything which is not named in the product description, e.g. Transport in Product A, Funeral Support in Product B.]

20 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Give points to the groups that answer the questions correctly. Then add the points for each
group. Congratulate the winning group.
3. Ask participants to calculate the total Yearly Payment for family members who would
be enrolled in health insurance – 20 minutes
Imagine that you decide to get the health insurance from CBHF. Turn to the person next to you
and discuss how to answer the following questions for 3 minutes:
Who in the family should get the health insurance? Which product would be suitable for you and your family? How much is the Yearly Payment for your family?
Visit each group and help participants calculate the amount of the Yearly Payment for their
family. After 3 minutes, encourage 2 or 3 participants to share their answers.
Then say: You will remember that earlier we calculated the costs of illness. The costs of illness include transportation, hospital stay, tests, medicine and time lost at work.
How do the costs of illness compare to the Yearly Payment for your family?
Encourage 2 or 3 participants to share.
Think about the advantages of having health insurance and the ways health insurance benefits
your family.
Thank participants.
What questions do you have about the health insurance available to you?
If you would like more information or if you have questions or complaints about CBHF you may
visit the nearest office, located _________________ or talk to _________________, your local CBHF chairman. You may also talk to me or STIPA if you have questions or concerns.
Respond to questions. Distribute a CBHF brochure and Product Description to each participant, if available. Then say: This is a Description of the Health Insurance available to you. It describes all of the information that we just discussed and has important information about the nearest CBHF office.
The nearest CBHF office is located __________. You may take this home to share with your family.

21 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
4. Invite participants to commit to telling others about the health insurance available to
them – 5 minutes
Remember the important information about the health insurance available to you. Knowing what
the Yearly Payment, Eligibility and Covered Services will help you understand the important
information about the health insurance available to you.
In the next Technical Learning Conversation, we are going to talk about how to use health
insurance.
If you commit to telling your family about the health insurance available to you before the next
Technical Learning Conversation, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

22 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 5: Using Your Health Insurance
Objectives
By the end of this Technical Learning Conversation, participants will have:
Practiced explaining how to use health insurance to their husband or other family member.
Preparation
Before facilitating the Technical Learning Conversation, insert the appropriate information about the health insurance that is available to participants [Yearly Payment, Eligibility, Covered Services].
Health provider profile (1 per participant) Description of the CBHF scheme that is available to participants (3 copies) An example of an authority letter of the CBHF scheme An example of a CBHF membership card or a picture of a CBHF membership card Information about the location of the nearest CBHF office and the name of a representative
at the office.
Time
65 minutes
Steps
1. Review key features of health insurance – 15 minutes
Last time we discussed the health insurance that is available to you and your family. Now let us
review.
What is the Yearly Payment for a family of five members to get health insurance?
[It is depending on the product and ranging from 1200 to 2700 KSh]
What are some of the Covered Services available to you through health insurance?
[It is depending on the product, ranging from OPD, IPD, funeral support, C/S, normal delivery, transport.]
Who is eligible for health insurance?
[Everyone who makes a yearly payment. The premium is for a family of five members. Additional members will pay a small top up amount]
Encourage 2 or 3 participants to share. Thank them.

23 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
2. Present steps for using health services with health insurance – 20 minutes
Imagine you decided to buy health insurance for everyone in your family and that you have
already paid the Yearly Payment. There are 3 steps to think about when you use health insurance for the first time. I am going to show you a cheer to help you remember these 3 steps:
Wait, Go, Show.
Ask everyone to please stand up.
Now you are going to learn the cheer. I am going to do each step and then you are going to do it
with me.
Wait until premium is paid (clap 3 times)
Invite participants to do it with you.
Go to the chairman, get an authority letter and go to a covered clinic (stomp your feet 3 times)
Invite participants to do it with you.
Show your membership card (wave a pretend card in front of you 3 times as though you are
showing it)
Invite participants to do it with you.
Now we are going to do the entire cheer together. We are all going to say each of the 3 steps
while doing the body movements at the same time.
Wait 3 months
Participants clap their hands 3 times.
Go to the chairman, get an authority letter and go to a covered clinic
Participants stomp their feet 3 times.
Show your membership card and the authority letter
Each participant waves a pretend card in front of her 3 times as though she is showing it.
Do the cheer 1 more time and then thank everyone and ask the participants to sit down.
When we stomp our feet, we say, Go to a covered clinic. I have a list of the local hospitals,

24 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
clinics and pharmacies that are covered by your health insurance, the CBHF. First, I would like you to tell me which clinics, hospitals and pharmacies you go to and know about. Then I am going to check to see whether they are on this list.
Have the health provider profile and tell participants whether the clinics and hospitals that they name are on the list. Explain to them that if they are on the list, then they can get Covered Services.
Remember, if you go to a clinic or hospital that is not on this list for a health service, your health insurance is not going to pay it.
From our cheer, you know that you need to show your membership card and a authority letter from the CBHF chairman. This is what a membership card and the authority letter look like. Hold up a copy of the CBHF membership card or a picture of it and then pass it around for everyone to see.
When you present your membership card, the CBHF pays the clinic or hospital later.
You will also need a signed letter from the chairman of the CBHF scheme that will authorize you to go to the clinic.
What questions do you have about the steps for using health services with health insurance?
Respond to questions.
If you forget or do not understand 1 of these steps, or you have a problem, you may visit the
nearest CBHF office, located ____________________ or talk to __________________, your
CBHF chairman. You can also ask me if you have any questions or concerns.
3. Ask participants to role-play talking about health insurance, how it works and how to use it
– 20 minutes
You have learned a lot about health insurance. Before you decide whether you are going to buy
health insurance, you may need to discuss with your husband or other family members. We are
going to practice talking about it now.
Form groups of 2.
One person in your group is going to play the role of the husband or other family member who is
helping to decide whether to buy health insurance. You must explain it to him and answer his
questions. Be sure to tell him the 3 steps for using health insurance—wait, go, show. After 3

25 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
minutes, you are going to change roles.
After 3 minutes, ask the participants to changes roles. After 3 more minutes, say:
Now I invite 1 group to volunteer to come up to practice the group’s role-play in front us.
Clarify if there is any confusion and thank the participants.
4. Invite participants to commit to telling others about health insurance – 10 minutes
During our next meeting, we are going to review all that we have learned about health insurance.
We are also going to share our thoughts about enrolling in health insurance. A representative from the CBHF will be at our meeting to enroll those who would like health insurance. It is important to share the information about health insurance with your husband or other adult members of your family, as you did in the role-play.
If you would like to enroll in health insurance during our next meeting, you will need to bring the following:
Identification card or birth certificate for each person who would like to enroll in health insurance
The registration fee of 100 KSh Your partly premium or the full amount of premium if you already decided for a product
In the next Technical Learning Conversation, we are going to talk about how to enroll in health insurance. If you commit to telling your family, as we did in the role-play today, about health insurance, how it works, the advantages of it, and how to use it before the next Technical Learning Conversation, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

26 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 6: Deciding to Enroll
Objectives
By the end of this Technical Learning Conversation, participants will have:
1. Reviewed technical information about health insurance.
2. Demonstrated their intention to enroll in health insurance or enrolled in health insurance.
Preparation
Bring the CBHF brochure, product descriptions and health provider profiles as a reference for participants. If possible, arrange for a representative from the CBHF to attend this meeting to assist participants with registering for the CBHF. If possible, bring the registration book of the CBHF scheme.
Time
50 minutes
Steps
1. Review the steps for getting health services with health insurance – 10 minutes
Last time we discussed the steps for using health insurance. We learned a cheer to remember. Let
us review now.
What are the steps for using health services with health insurance?
[There are 3 steps for getting health services with health insurance:
1. Wait until premium is paid (clap hands 3 times)
2. Go to the chairman and proceed to a covered clinic (stomp 3 times)
3. Show the authority letter and your membership card (wave a pretend card in front of you 3 times as though you are showing it)]
Thank participants. Then say:
I encourage you to use these steps for using health services with the CBHF!
Today is our last meeting about health insurance. Today you can plan ahead and take action by
registering for CBHF.

27 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
2. Play a game to review technical information about health insurance – 15 minutes
I am going to read statements about health insurance. For each statement I read, you are going to
indicate whether you think it is true or false. If you think it is true, stand up. If you think it is
false, stay seated.
Let us start with some practice statements. I am going to read each statement twice.
Read the first practice statement in the box below twice, then say “One, Two, Three, Go!” Make
sure the participants give the correct answer. Before reading the next statement, make sure
participants are seated. Do the same for the remaining practice statements.
Practice Statements
1. Today is _________ (absolutely incorrect weather—for example,
sunny or rainy). False
2. My name is _______ (your correct name). True
Then say:
Now let us do the same with statements about health insurance.
Read the first statement in the statement box below twice, then say, “One, Two, Three, Go!” If
all participants give the correct answer, congratulate them. If some participants think the
statement is true and others think it is false, ask someone who answered correctly to explain her
answer, tell the group the correct answer and finally clarify any questions. If all participants
give the wrong answer, lead a discussion to explain the correct answer. Do the same for the
remaining statements.
Health Insurance Game Statements:
CBHF gives you money back if you do NOT get sick.
FALSE (stay seated)

28 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
When you buy health insurance, you pay for protection against an illness that may or may not
happen.
TRUE (stand up)
A person saves a lot of money if she does not buy health insurance.
FALSE (stay seated)
The cost of illness can be very high. One person could even end up spending all her income or savings
treating an illness.
TRUE (stand up)
After you registered, you must wait until your premium is fully paid to get access treatment.
TRUE (stand up)
CBHF costs always 2000 KSh for five members of a family.
FALSE (stay seated)
The Yearly Payment for CBHF depends on the product you have chosen.
TRUE (stand up)
You can go to any clinic or hospital you want to use your CBHF card.
FALSE (stay seated)
Thank participants for their participation.

29 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
3. Invite participants to decide whether they would like to enroll in health insurance –
30 minutes
Let us get an idea of your thoughts about enrolling in health insurance. Pleases stand up. I am
going to read 3 options. Which 1 best fits with your thoughts about CBHF:
I have not yet decided I would like to register but I do not have money to pay for it right now I would like to register and I can pay for it right now
I am going to read these options again. Please walk to the corner of the room that best fits with
your thoughts about health insurance:
I have not yet decided
Walk to one corner of the meeting place as you read the statement.
I would like to register but I do not have money to pay for it right now
Walk to another corner of the meeting place as you read the statement.
I would like health insurance and can pay for it right now
Walk the third corner of the meeting place as you read the statement.
While participants are standing in the 3 corners, ask:
Who wants to share why they are standing where they are?
Let us hear from anyone who wants to talk.
Those of you who would like insurance, but cannot pay for it right now, what are some
ways you might be able to save money so that you can pay for health insurance?
Thank participants for their honesty and answer any questions they may have about health
insurance available to them.
If the insurance agent is at the meeting, say:
If you want to register today, please come forward and _______
(name of CBHF chairman) is going to help you.
Help participants complete the health insurance applications.

30 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
4. Invite participants to commit to thinking about the value of insurance or commit to
using it – 5 minutes
After interested participants complete the application, say:
Those of you who are still thinking about registering please discuss the advantages and value of it with your family members. Remember, you can always register at a later date. If you commit to using health insurance to help protect yourself and your family against the costs and risks of illness, or commit to thinking about the value of signing up for CBHF, please stand.
Now let us all join hands and say together, “Together, we prepare to face illness.”

31 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Health Insurance—Preparing to Face Illness Technical Learning Conversations
Technical Learning Conversation 7: Re-enrolling in Health Insurance
Note: Facilitate Technical Learning Conversation 7 one year after Technical Learning
Conversation 6 or when it is time for participants to re-enroll in health insurance.
Objectives
By the end of this Technical Learning Conversation, participants will have:
1. Shared their experiences with using health insurance over the past year.
2. Demonstrated their intention to re-enroll in health insurance.
Preparation
Before facilitating the Technical Learning Conversation, insert the appropriate information about the health insurance that is available to participants [Yearly Payment, Eligibility, Covered Services].
Bring the CBHF brochure, product descriptions and health provider profiles If possible, arrange for an representative of the CBHF to attend this meeting to assist
participants with registering for CBHF Bring the registration book and premium payment follow up book Pictures 3–5
Time
85 minutes
Steps
1. Review technical information about health insurance – 15 minutes
How does health insurance work?
[You pay a set amount of money to CBHF. In turn, the money collected is used by the CBHF to
cover some of the costs for you and other CBHF members who got sick or injured in an
accident.]
Show Picture 3 while you ask the following question:
What is the Yearly Payment for a family of five members to get health insurance?
[Depending on the product you have chosen the price is ranging between 1200 and 2700 KSh]

32 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Show Picture 4 while you ask the following question:
Who is eligible for health insurance?
[Everyone who makes a yearly payment.The premium is set for a family of five members.]
Show Picture 5 while you ask the following question:
What are some of the Covered Services available to you through health insurance?
[Depending on the product you have chosen it ranges between OPD, IPD, C/S, normal delivery, transport, minor surgery and funeral support]
2. Tell two stories about health insurance and discuss personal experiences – 45 minutes
I am going to tell you the story of Adhiambo and Otieno. They both had different experiences with
CBHF. Let us first listen to the story of Adhiambo.
Adhiambo Experience with Health Insurance
One year ago Adhiambo decided to register with CBHF. Adhiambo is very happy and relieved that she decided to buy health insurance. In the past year, her son got sick with malaria and her husband got a bad cough. They were able to see a doctor right away, get tests and receive medicine. CBHF paid for everything. Adhiambo felt thankful because her husband returned to work and her son went back to school. Adhiambo decided to re-enroll in CBHF. She feels that the health insurance is of good value and she feels peace of mind knowing that her family is covered. She was happy that her family already had CBHF membership cards, so re-enrolling was easier. Also, this time she did not have to wait so long to access treatment because she saved money in the scope of the year to pay the annual premium. She knew that to re-enroll she had to pay the Yearly Payment and registration fee again. The Yearly Payment was 2700 KSh for her, her husband and their three children. She chose product C because it covered all needed services and also transport and funeral costs as well as caregiver allowances.
What did Adhiambo use her health insurance for?
[When her son had malaria and her husband had a cough.]
How does Adhiambo feel about having health insurance?
[Happy, thankful, relieved.]

33 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Why did Adhiambo think that re-enrolling was easier?
[Her family members already have their membership cards and because she saved money for the premium, she could pay the premium easily and access treatment without waiting.]
Now listen to the story of Otieno.
Otieno’s Experience with Health Insurance
Otieno also decided to buy health insurance one year ago. He is happy because he has peace of mind knowing his family members are covered when they become sick. However, no one in Otieno’s family fell sick in the last year and so no one used the health insurance. Otieno feels very lucky that his family has been healthy this past year, but he is wondering whether he should reenroll. His wife thinks that the total Yearly Payment for the family is a lot of money and is not sure it is the best decision to re-enroll, especially because they did not use it during the previous year. Otieno tells his wife there are advantages of health insurance even if it is not used. He says that if they re-enroll, they can use the money they saved during the year to re-enroll. He also says that if a family member becomes sick, they will not need to use money from their business or sell assets because they will be covered with health insurance.
Why did Otieno’s family not use their health insurance?
[Her family was lucky and no one became sick during the past year.]
Why is Otieno’s wife is not sure the family should re-enroll in health insurance?
[The total Yearly Payment for the family seems like a lot of money and they did not use
health insurance during the previous year.]
What are advantages of health insurance even if it is not used?
[Peace of mind, use of savings for premium, they will not need to use money from the business when a family member becomes sick.]
Thank participants.
Now we are going to learn from those of you who decided to enroll in health insurance. We want
to hear about your experiences. First, please raise your hand if you enrolled in CBHF.
Form 3 groups. Make sure there is 1 person who has experience with using health insurance in
each group.

34 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
In your groups, I would like you to discuss your experiences with using health insurance.
After 3 minutes, bring the participants together again. Discuss personal experiences with health
insurance. Ask the following questions:
What did you like best about having health insurance? How did you use your health insurance?
After several participants have answered the questions and shared their experiences with health
insurance, thank everyone.
3. Deciding whether to re-enroll in health insurance – 20 minutes
Imagine that you are deciding to re-enroll in CBHF. Turn to the person next to you and discuss how to answer the following questions for 3 minutes:
How much is the Yearly Payment for your family? Which product will you chose? Does this health insurance provide good value for the money? Why?
Visit each group and help participants calculate the amount of the Yearly Payment for their
family. After 3 minutes, say:
Now I invite you to share what you discussed.
Encourage 2 or 3 participants to share. Thank the participants.
Some of you would like to re-enroll in health insurance but are worried about how you are going
to pay for it.
What are some ways you can save money so that you can re-enroll in health insurance?
Thank participants for their honesty and answer any questions they may have about health
insurance available to them.
If appropriate, say:
During our next meeting, a representative from the CBHF will visit us. This will give you the
opportunity to ask the representative questions and voice concerns. If you decide to re-enroll or
enroll in health insurance during our next meeting, you will need to bring the following:

35 Technical Learning Conversations – Preparing to face illness: adapted to CBHF in Kenya
Identification card or birth certificate for each person who would like to enroll in health insurance.
The annual registration fee of 100 KSh Your membership card, if you were already enrolled last year Premium Payment
4. Invite participants to commit to re-enrolling or enrolling in health insurance – 5 minutes
Those of you thinking about re-enrolling or enrolling in health insurance, please discuss the value of it with your family members. If you commit to thinking about re-enrolling or enrolling in health insurance to protect yourself and your family against the costs and risks of illness, please stand. Now let us all join hands and say together, “Together, we prepare to face illness.”

Subs
idy
thro
ugh
STIP
A
Kad
awa
Sche
me
Kam
rong
o Sc
hem
e G
AW
U
Sche
me
Mir
anga
Sc
hem
e M
asen
o Sc
hem
e O
gera
Sc
hem
e T
AI S
chem
e K
AST
EP
Sche
me
Eas
t Kar
achu
onyo
Sc
hem
e A
VE
RA
GE
A
MO
UN
T in
KE
S
Staf
f 41
,509
42
,779
46
,288
37
,206
13
,692
83
,468
58
,494
44
,453
67
,213
48
,345
Fuel
6,
500
3,50
0 34
,000
7,
000
3,50
0 36
,000
24
,000
12
,000
14
,000
15
,611
Stat
iona
ry
1,25
3 1,
253
3,00
0 1,
253
--
3,89
4 5,
033
4,20
0 5,
077
3,12
0
Prin
ting
6,00
0 6,
000
6,00
0 6,
000
6,00
0 6,
000
6,00
0 6,
000
6,00
0 6,
000
Com
mun
i-cat
ion
3,00
0 3,
000
3,00
0 3,
000
3,00
0 3,
000
3,00
0 3,
000
3,00
0 3,
000
Car
d C
osts
2,
500
2,50
0 2,
500
2,50
0 2,
500
2,50
0 2,
500
2,50
0 2,
500
2,50
0
Bro
chur
es
2,00
0 2,
000
2,00
0 2,
000
2,00
0 2,
000
2,00
0 2,
000
2,00
0 2,
000
Phot
o C
ards
2,
105
2,10
5 2,
105
2,10
5 2,
105
2,10
5 2,
105
2,10
5 2,
105
2,10
5
TO
TA
L in
KE
S 64
,867
63
,137
98
,893
61
,064
28
,692
14
3,34
7 10
7,51
2 75
,135
10
0,79
0 82
,604

Lisa-Marie Ouedraogo: Approaching Universal Health Coverage in Kenya - The Potential of integrating Community Based Health Insurance Schemes into an Integrated National Social Health Insurance System (Juli 2016)
Zusammenfassung (Deutsch) Selbst Jahrzehnte nach der erfolgreichen Formulierung von internationalen Richtlinien im Bereich der Universal Health Coverage (UHC) und dem Access for All zu essentiellen Gesundheitsleistungen durch die globale Gemeinschaft bleibt die soziale Absicherung im Krankheitsfall eine der globalen Grundherausforderungen. In diesem Zusammenhang ist zu beklagen, dass derzeit weniger als 15% der gesamten Weltbevölkerung von sozialen Sicherungsmaßnahmen im Gesundheitsbereich profitieren und zudem mehr als 70% der globalen Bevölkerung keinerlei Zugang zu sozialen Sicherheitsmaßnahmen haben. 36 Jahre nach der Formulierung der oft zitierten Alma Ata Declaration, welche die Förderung und den Schutz der menschlichen Gesundheit als essentiell bezüglich nachhaltiger wirtschaftlicher und sozialer Entwicklung festsetzte, sehen sich Angehörige des informellen Sektors in sub-Sahara Afrika – welcher oft bis zu 90% der Gesamtbevölkerung ausmacht – weiterhin regelmäßig gezwungen, im Krankheitsfall hohe Kredite aufzunehmen oder essentielle Gebrauchsgegenstände zu verkaufen, um die horrenden Krankheitskosten zu begleichen. Diese Situation bedingt einen oftmals irreversiblen Kreislauf aus existenzbedrohender Armut und Krankheit innerhalb des informellen Sektors. Private Krankenversicherungen im Kontext sub-Sahara Afrikas bieten in der Regel ihre Produkte vorrangig in den urbanen Zentren an. Zugleich sind private Krankenversicherungsprodukte zumeist nicht auf die besonderen Bedürfnisse des informellen oder ländlichen Sektors zugeschnitten. Staatliche Krankenversicherungen sind zudem üblicherweise vorrangig für den formellen Sektor ausgestaltet oder bieten lediglich Leistungen für Staatsbedienstete an. Dennoch wird soziale Sicherung im Krankheitsfall seitens der globalen Gemeinschaft zunehmend als vielversprechender Garant bezüglich Entwicklung und Wirtschaftswachstum in Niedrigeinkommensländern angesehen. In diesem Zusammenhang sind einige ForscherInnen davon überzeugt, dass gemeindebasierte Gesundheitsfinanzierung als eine vielversprechende Möglichkeit angesehen werden kann, welche die sonst ausgeschlossenen Bevölkerungsanteile mit sozialen Sicherungsmaßnahmen im Gesundheitsbereich versorgt. Gemeindebasierte Krankenversicherungen, sogenannte Community Based Health Insurance (CBHF) Institutionen, richten sich dabei mit ihren maßgeschneiderten Produkten und Prozessen in einem kooperativen und genossenschaftlichen Ansatz vor allen an NiedrigverdienerInnen des informellen Sektors.
Um den globalen Standards der UHC gerecht zu werden, ist CBHF Institutionen in den letzten Jahren zunehmend globale Aufmerksamkeit geschenkt worden und viele afrikanische Regierungen ziehen es infolgedessen in Erwägung, den informellen Sektor durch gemeindebasierte Krankenversicherungen in die öffentlichen Sozialversicherungssysteme zu integrieren und diese somit von sozialen Sicherungsmaßnahmen im Krankheitsfall profitieren zu lassen. Infolgedessen sind in einigen Ländern bereits innovative integrierte soziale Sicherungssysteme entstanden, die darauf abzielen, die verschiedenen existenten Bevölkerungsgruppen bedarfsgerecht mit sozialer Sicherung im Krankheitsfall zu versorgen. Während einige Staaten diese integrierten Systeme bereits implementiert haben – so etwa Ruanda, Ghana und Tansania – befinden sich andere Staaten in der konkreten Planung eines derartigen Vorhabens, so etwa Burkina Faso und Togo.

Lisa-Marie Ouedraogo: Approaching Universal Health Coverage in Kenya - The Potential of integrating Community Based Health Insurance Schemes into an Integrated National Social Health Insurance System (Juli 2016)
In Anbetracht der soeben dargestellten Situation, befasst sich die vorliegende Dissertationsschrift mit den folgenden Themenbereichen:
1. Auf Basis einer ausführlichen SWOT-Analyse von integrierten Sozialversicherungssystemen in vier Niedrigeinkommensländern sub-Sahara Afrikas (Ghana, Burkina Faso, Tansania und Ruanda) werden weitreichende Schlussfolgerungen/lessons learned entwickelt, die als grundlegend bezüglich der Implementierung integrierter Systeme sozialer Sicherung in Niedrigeinkommensländern sub-Sahara Afrikas zu betrachten sind.
2. Am Fallbeispiel des existenten sozialen Krankenversicherungssystems im ostafrikanischen Kenia wird das Potential der Implementierung eines integrierten sozialen Krankenversicherungssystems in einem Niedrigeinkommensland und dessen möglicher Beitrag zur UHC untersucht.
3. Auf Grundlage der oben erwähnten vergleichenden Länderanalyse und der Kenia-
Fallstudie wird ein Standardmodell für die Implementierung integrierter sozialer Krankenversicherungssysteme in Niedrigeinkommensländern entwickelt, welches in seinen Grundzügen globale Relevanz und universelles Anwendungspotential aufweist.
Die vorliegende Dissertationsschrift bietet zunächst eine ausführliche thematische Einleitung (Kapitel II), in der relevante Grundbegriffe erläutert und konzeptualisiert werden. Wichtige Terminologien, wie etwa Development, Universal Health Coverage, Social Protection, Health Financing und Micro Health Insurance werden dabei kontextspezifisch erkläutert. Im Weiteren wird auf theoretischer Basis das grundsätzliche Potential untersucht, gemeindebasierte Krankenversicherungen in öffentliche Systeme der sozialen Sicherung in Niedrigeinkommensländern in sub-Sahara Afrika zu integrieren. Dies geschieht mit Hilfe einer Analyse von grundsätzlichen Stärken, Schwächen und Synergien beider Ansätze. Die Kenia-Fallstudie des vierten Kapitels wird im einleitenden zweiten Kapitel durch eine ausführliche Einführung in den generellen Kontext Kenias vorbereitet. Dabei werden bestehende Entwicklungsinitiativen und der generelle Kontext hiesiger sozialer Sicherung und Gesundheitsfinanzierung erläutert. Im dritten Kapitel wird eine angepasste SWOT-Analyse verschiedener afrikanischer Länder (Ghana, Burkina Faso, Tansania und Ruanda) vorgenommen, in der grundsätzliche Stärken, Schwächen, Möglichkeiten und Bedrohungen der bestehenden integrierten Systeme der sozialen Sicherung in den ausgewählten Ländern identifiziert und analysiert werden. Auf Grundlage dieser ländervergleichenden Analyse werden grundlegende Schlussfolgerungen gezogen, welche die Implementierung integrierter Sozialversicherungssysteme in Niedrigeinkommensländern sub-Sahara Afrikas essentiell beeinflussen und deren Erfolg bestimmen. Kapitel 4 befasst sich mit der bereits erwähnten Kenia-Länderstudie, in der bestehende Strukturen der Gesundheitsfinanzierung und sozialen Sicherung bezüglich ihres potentiellen Beitrags zur UHC analysiert werden. Dieses Kapitel zielt darauf ab, effektive und effiziente Maßnahmen zu identifizieren, welche im Rahmen einer möglichen Implementierung eines integrierten Systems in Kenia als maßgeblich zu betrachten sind. In diesem Kontext werden CBHF Institutionen als eine Grundstruktur des innovativen sozialen

Lisa-Marie Ouedraogo: Approaching Universal Health Coverage in Kenya - The Potential of integrating Community Based Health Insurance Schemes into an Integrated National Social Health Insurance System (Juli 2016)
Krankenversicherungssystems angesehen. Auf dieser Grundlage wird ein Multi-Ebenen-Modell entwickelt, welches sich schrittweise der UHC-Agenda annähert. Im abschließenden Kapitel 5 werden die präsentierten Erkenntnisse aus dem kenianischen Kontext auf eine globale Ebene übertragen und auf dessen Grundlage wird ein Standardmodel für die Implementierung integrierter Sozialversicherungssysteme entwickelt und präsentiert. In der Schlussbetrachtung werden grundsätzliche Möglichkeiten und Grenzen gemeindebasierter Ansätze bezüglich UHC aufgezeigt, sowie ein möglicher Ausblick bezüglich des kenianischen Fallbeispiels präsentiert.


Vote of Thanks Was lange währt, wird endlich gut. – I would like to thank all people who supported me since 2009 to materialize my vast research ideas towards a robust thesis and research piece. Starting with the Department for Cooperative Studies at University of Cologne, I would like to acknowledge the extraordinary support I received from Prof. Hans-Jürgen Rösner and my colleagues, Dr. Gerald Leppert and Philip Degens, who shaped my initial research ideas in the area of integrated Social Protection in sub-Saharan Africa and who gave me the opportunity to be part of the “Pro MHI Africa” project for several years. Let me also thank the entire “Pro MHI Africa” team, who supported me in obtaining my first qualitative data over the period of 2009 to 2011. To all my precious Kenyan colleagues at STIPA in Kisumu: thank you so much for having me for all this while and sharing your experiences and expertise. I value this a lot and your input determined and influenced this thesis in a significant manner. To my wonderful supervisor at the Department of Health Care Management at University of Greifswald, Prof. Steffen Flessa: I cannot imagine a better support than the support you have been providing to me since 2011. I value this a lot and appreciate your efforts, time and extraordinary commitment you showed to help me in completing this long-term research. On a personal and emotional note, I want to greatly appreciate my family, who always supported me to the highest extend. I will forever be grateful to my sister Kristina Rohrdantz, my mother Ingeborg Rohrdantz, my father Dieter Rohrdantz, my grandmother Hildegard Roemer and my uncle Robert Roemer. Not to forget the great emotional support I received from family Roemer-Bockermann and my beloved friends Christina Loeber, Brigitta Moll, Miriam Nybo, Luise Ossenbach-Albalkhi, Wibke Pecksen, Christine Vesper, Nina Waibel, Anne Walkowiak, Katja Weber and Katrin Wenz. I am also very grateful to my two precious children, Maximilian Adama and Greta Serafine, who agreed to release their mum during the weekends – which usually belong to them – to work on her thesis and support her aim to become “a doctor”. To all my other great friends and colleagues in Cologne, Berlin, Frankfurt, Kisumu, Lilongwe and all over the world: you know you are amazing and you know who you are: Thank you so very much. I am more than blessed to have this supportive environment. And you alone made the completion of this thesis possible. T H A N K Y O U.