Behandlungspfade „Interdisziplinäres Onkologisches Zentrum ... file• Anamnese und körperliche...
27
Behandlungspfade „Onkologisches Zentrum“ Klinikum Ernst von Bergmann Potsdam Mundhöhlenkarzinom Lippenkarzinom Stand Mai 2019 Autoren: Dr. Dr. Teltzrow, Dr. Laepple, Dr. Bertram 13.05.2019 Überprüft: Prof. Dr. Maschmeyer, PD Dr. Badakhshi 15.07.2019 Freigabe: Dr. Dr. Teltzrow, Prof. Dr. Maschmeyer 13.08.2019
Transcript of Behandlungspfade „Interdisziplinäres Onkologisches Zentrum ... file• Anamnese und körperliche...

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
MundhöhlenkarzinomLippenkarzinom
Stand Mai 2019
Autoren: Dr. Dr. Teltzrow, Dr. Laepple, Dr. Bertram13.05.2019
Überprüft: Prof. Dr. Maschmeyer, PD Dr. Badakhshi15.07.2019
Freigabe: Dr. Dr. Teltzrow, Prof. Dr. Maschmeyer13.08.2019

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
Quellen:NCCN vom 20.06.2018S3-Leitlinie von 12/2012SOP überarbeitet vom 02/2018 bei Stand 01.10.2016
2
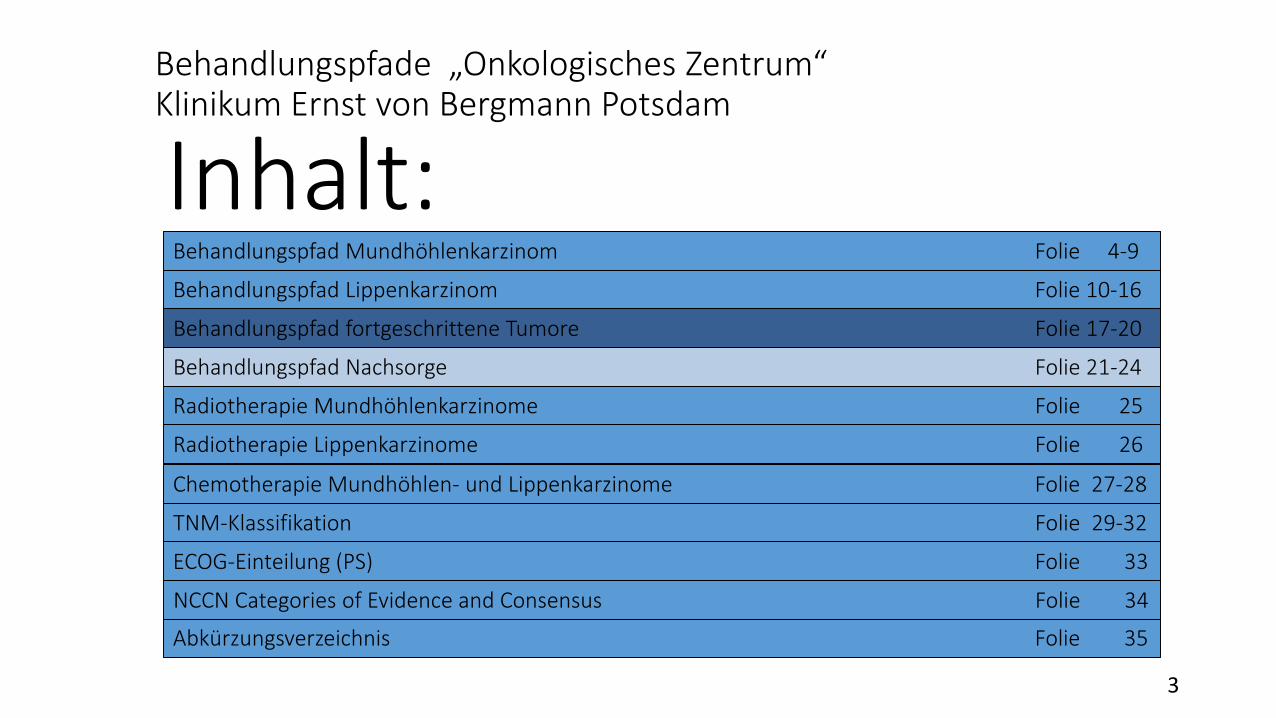
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
Inhalt:Behandlungspfad Lippenkarzinom Folie 10-16
3
Behandlungspfad fortgeschrittene Tumore Folie 17-20
Behandlungspfad Nachsorge Folie 21-24
Radiotherapie Mundhöhlenkarzinome Folie 25
Radiotherapie Lippenkarzinome Folie 26
TNM-Klassifikation Folie 29-32
Behandlungspfad Mundhöhlenkarzinom Folie 4-9
ECOG-Einteilung (PS) Folie 33
Abkürzungsverzeichnis Folie 35
Chemotherapie Mundhöhlen- und Lippenkarzinome Folie 27-28
NCCN Categories of Evidence and Consensus Folie 34

Diagnostik Klinisches Staging Entscheidung
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• Anamnese und körperliche Untersuchung
• Panendoskopie• Zahnärztliche
Untersuchung• Biopsie• Anästhesievorstellung• CT/MRT mit KM des
Primärtumors und des Halses (Dünnschicht mit KM)
• Thorax-CT konventionell
• Orthopantomogramm• Ggf. logopädische
Vorstellung (Ess-, Sprech-, Schluckanalyse)
• cT1-2, cN0
• cT3, cN0• cT1-3, cN1-3• cT4a, jedes cN
• cT4b, jedes cN, oder nicht R0-resezierbare lokale Lymphknoten-metastasen oder nicht operationstauglich
• cM1 Fernmetastasen
OR-2
Mundhöhlenkarzinom (OR-1) – NCCN + LL + SOP
OR-3
ADV-1(Neu
diagnostiziert)
ADV-2(initiale
Fernmetastase)
4
TUMOR-BOARD
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• R0-Resektion (präferiert)(Mit Schnellschnitt-diagnostik)
• Ggf. SLN im Rahmen einer Studie
• + Neck dissection(ipsi-/bilateral)
• Definitive Radiotherapie
Mundhöhlenkarzinom (OR-2) + LL + SOP
SLN-Identifikation
erfolgreich
SLN-Identifikation
nicht erfolgreich
SLN-pN0
SLN-pN+
Neck dissection
• N0• OHNE ungünstige
Faktoren
• ein positiver Lymphknoten
• OHNE ungünstige Faktoren
• Lymphknoten MIT ungünstigen Faktoren (Kapselüberschreitung, positive Randschnitte, N2/N3, perineuraleInvasion, vasculärerEmbolus, lymphatische Invasion)
Extranodale Ausbreitung+- positiver Randschnitt
positiver Randschnitt
Andere Risikofaktore
n
Follow-Up
Radiochemo-therapie
Kategorie 1
RadiochemotherapieKategorie 1
o.Re-Resektion, wenn durchführbar undggf. Radiotherapie
bei negativen Randschnitten
Radiotherapieo.
Radiochemotherapie
Radiotherapie(optional)
o.Follow-Up
Follow-Up
cT1 – cT2, cN0(OR-2)
5• Neck dissection Level I-III ggf. bds., bei positiver Lymphknoten-metastase -> Level I-V• Close Margin: Resektatrand zum Primärtumor am formalinfixierten Präparat mindestens 3-5 mm
(entspricht ca. 10 mm vom tastbaren Tumorrand)
TUMOR-BOARD
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• R0-Resektion
• Schnellschnitte
Oder
• Studien-einschluss
Mundhöhlenkarzinom (OR-3) – NCCN + LL + SOP
cN1,cN2a-b,
cN3
cN2c (bilateral)
Resektion des Primärtumors
+ bilateral neck dissection
Level I-III und auf der betroffenenSeite Level I-V
Resektion des Primärtumors
+ bilateral neck dissection
Level I-V
Extranodale Ausbreitung+- positiver Randschnitt
positiver Randschnitt
Andere Risikofaktore
n
Radiochemo-therapie
Kategorie 1
RadiochemotherapieKategorie 1
o.Re-Resektion, wenn durchführbar undggf. Radiotherapie
bei negativen Randschnitten
Radiotherapieo.
Radiochemotherapie
Radiotherapie(optional)
o.Follow-Up
Follow-Up
cT3, cN0; cT1-3, cN1-3; cT4a, jedes cN(OR-3)
6
cN0
Resektion des Primärtumors
+ bilateralneck dissection
Level I-III
TUMOR-BOARD
NCCNSOPLL• Close Margin: Resektatrand zum Primärtumor am formalinfixierten Präparat mindestens 3-5 mm
(entspricht ca. 10 mm vom tastbaren Tumorrand)
• N0• OHNE ungünstige
Faktoren
• ein positiver Lymphknoten
• OHNE ungünstige Faktoren
• Lymphknoten MIT ungünstigen Faktoren (Kapselüberschreitung, positive Randschnitte, N2/N3, perineuraleInvasion, vasculärerEmbolus, lymphatische Invasion)

Diagnostik Klinisches Staging Entscheidung
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• Anamnese und körperliche Untersuchung
• Zahnärztliche Untersuchung
• Biopsie• Anästhesievorstellung• Dünnschicht-CT (ggf.
MRT) mit KM des Primärtumors und des Halses
• Thorax-CT konventionell
• Panendoskopie• Ggf. logopädische
Vorstellung (Ess-, Sprech-, Schluckanalyse)
• je nach Indikation multidisziplinäre Vorstellung
• cT1-2, cN0
• cT3, cN0• cT1-3, cN1-3• cT4a, jedes cN
• cT4b, jedes cN, oder nicht R0-resezierbare lokale Lymphknoten-metastasen oder nicht operationstauglich
• M1 Fernmetastasen
LIP-2
Lippenkarzinom (LIP-1) – NCCN + SOP
LIP-3
ADV-1(Neu
diagnostiziert)
ADV-2(initiale
Fernmetastase)
Pat. operations-
tauglich
nicht operations-
tauglich
7
TUMOR-BOARD
NCCNSOPLL
• Lippenkarzinom: Karzinom, welches vom Lippenrot ausgeht

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• R0-Resektion (präfe-riert)
Oder
• Defini-tiveRadio-thera-pie
Lippenkarzinom (LIP-2) – NCCN + SOP
Re-Resektion, wenn möglich
oderRadiotherapie
Radiotherapie(optional)
oderFollow-Up
Follow-Up
cT1 – cT2, cN0(LIP-2)
LIP-4 8
Low-Risk(G1 und DOI < 5mm,
≥ G2 und DOI < 2,5mm),
(Exzisions-biopsie oder Probe)
High-Risk(G1 und DOI > 5mm,
≥ G2 und DOI> 2,5mm),
(Exzisions-biopsie oder Probe)
cN+
cN0
cN0
cN+
TUMOR-BOARD
Tumorresektion mit Schnellschnitt
Tumorresektion mit Schnellschnitt + Neck dissectionLevel I-III oder aggressives Follow-Up-Monitoring
Tumorresektion mit Schnellschnitt + Neck dissectionLevel I-III
R1
R0
R0, N1Erweiterte Neck dissection Level IV und V
R1
R0, pN0
R0, pN1Neck dissectionLevel IV und V
TUMOR-BOARD
Re-Resektion, wenn möglich
oderRadiotherapie
Radiotherapie(optional)
oderFollow-Up
NCCNSOPLL
Vorführender
Präsentationsnotizen
Wermker et al. 2015 (Prediction model for lymph node metastasis and recommendations for elective neck dissection) Altmyollar et al. 2002 (Is suprahyoid dissection a diagnostic operation in lower lip carcinoma?) Bucur et al. 2004 (Management of patients with sqamous cell carcinoma of the lower lip and N0-neck) Gooris et al. 2002 (Supraomohyoid neck dissection in the management of cervical lymph node metastases of squamous cell carcinoma of the lower lip)

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
• R0-Resektion (präferiert)
oder
• Definitive Radio-therapie
Oder• Radio-
chemo-therapie
Lippenkarzinom (LIP-3) – NCCN + SOP
Resektion des Primärtumors mit
Schnellschnitt bilaterale neck
dissectionLevel I-III
OperabelcT3, cN0; cT1-3, cN1-3; cT4a, jedes cN(LIP-3)
Resektion des Primärtumors mit
Schnellschnitt +bilaterale neck
dissectionLevel I-III und auf der
betroffenen Seite Level I-V
Resektion des Primärtumors mit
Schnellschnitt +bilateral neck
dissectionLevel I-V
Follow-Up
LIP-4
cN0
cN1,cN2a-b,
cN3
cN2c (bilateral)
Extranodale Ausbreitung
u. o.positiver
Randschnitt
Radiotherapie(optional)
oderFollow-Up
Radiochemotherapie(präferiert) Kategorie 1
oderRe-Resektion, wenn
durchführbar (nur bei positivem Randschnitt)
oderRadiotherapie
Radiotherapieoderggf.
Radiochemo-therapie
Andere Risiko-
faktoren
9
TUMOR-BOARD
NCCNSOPLL
• N0• OHNE ungünstige
Faktoren
• ein positiver Lymphknoten
• OHNE ungünstige Faktoren
• Lymphknoten MIT ungünstigen Faktoren (Kapselüberschreitung, positive Randschnitte, N2/N3, perineuraleInvasion, vasculärerEmbolus, lymphatische Invasion)
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
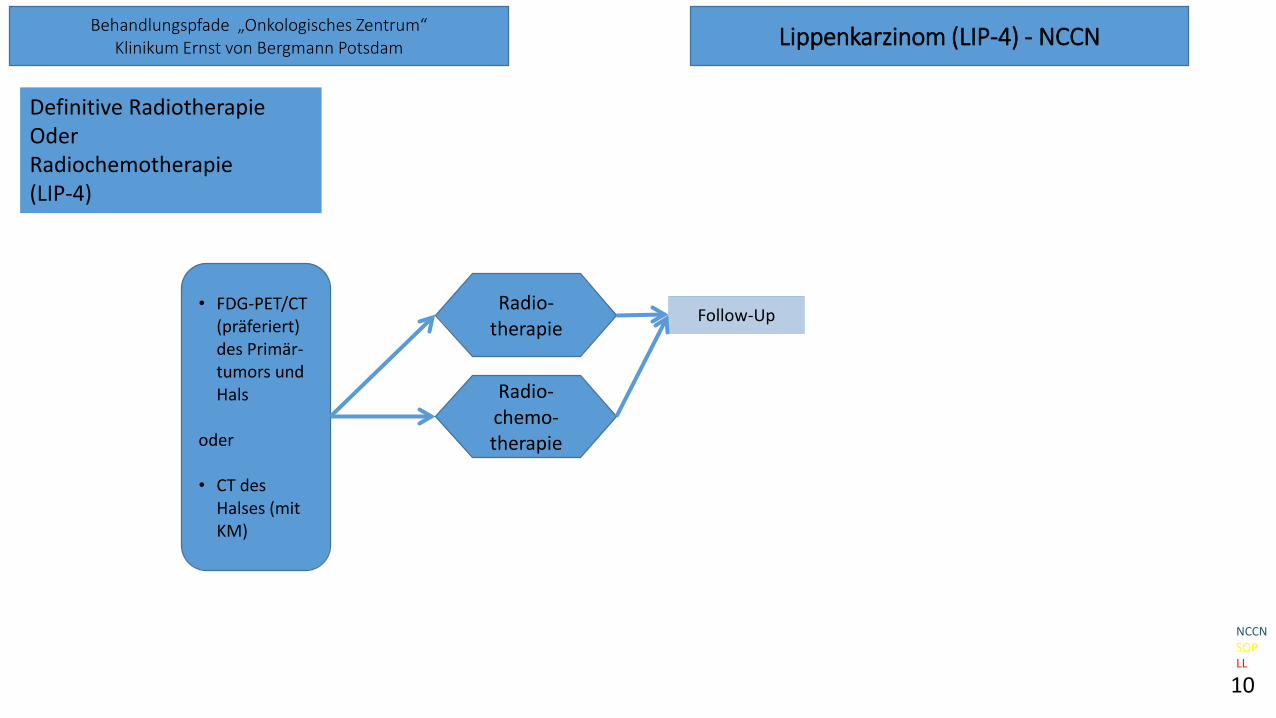
• FDG-PET/CT (präferiert) des Primär-tumors und Hals
oder
• CT des Halses (mit KM)
Lippenkarzinom (LIP-4) - NCCN
Radio-therapie
Definitive RadiotherapieOder Radiochemotherapie(LIP-4)
Radio-chemo-therapie
Follow-Up
10
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Fortgeschrittene Tumore (ADV-1) - NCCN
Neu diagnostizierte Erkrankung (ADV-1)
• Studien-einschluss
• PS 0-1
• PS 2
• PS 3
BSC
Follow-Up
Definitive Radiotherapie+- kombinierte Systemtherapie
Palliative Radiotherapie
Systemische Monotherapie
• cT4b, jedes cN
• nicht R0-resektable Lymphknotenmetastase
• nicht operationstauglich
• FernmetastaseADV-2
(initialeFernmetastase)
ADV-3(Residualtumor
oder Rezidiv)
11
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Fortgeschrittene Tumore (ADV-2) - NCCN
Initial metastasierter Tumor (ADV-2)
• Studien-einschluss
• PS 0-1
• PS 2
• PS 3
kombinierte Systemtherapie
BSC
Best SupportiveCare
Minimalinvasive Chirurgie
Radiotherapie(bei oligo-
metastasiert)
Systemische Monotherapie
Systemische Monotherapie
BSC
BSC
Systemische Therapie
BSC
Studieneinschluss(präferiert)
BSC
Studien-einschluss(präferiert)
operative Therapie Primarius und lokoregionäreLymphknoten
nur Fernmetastase
12
NCCNSOPLL
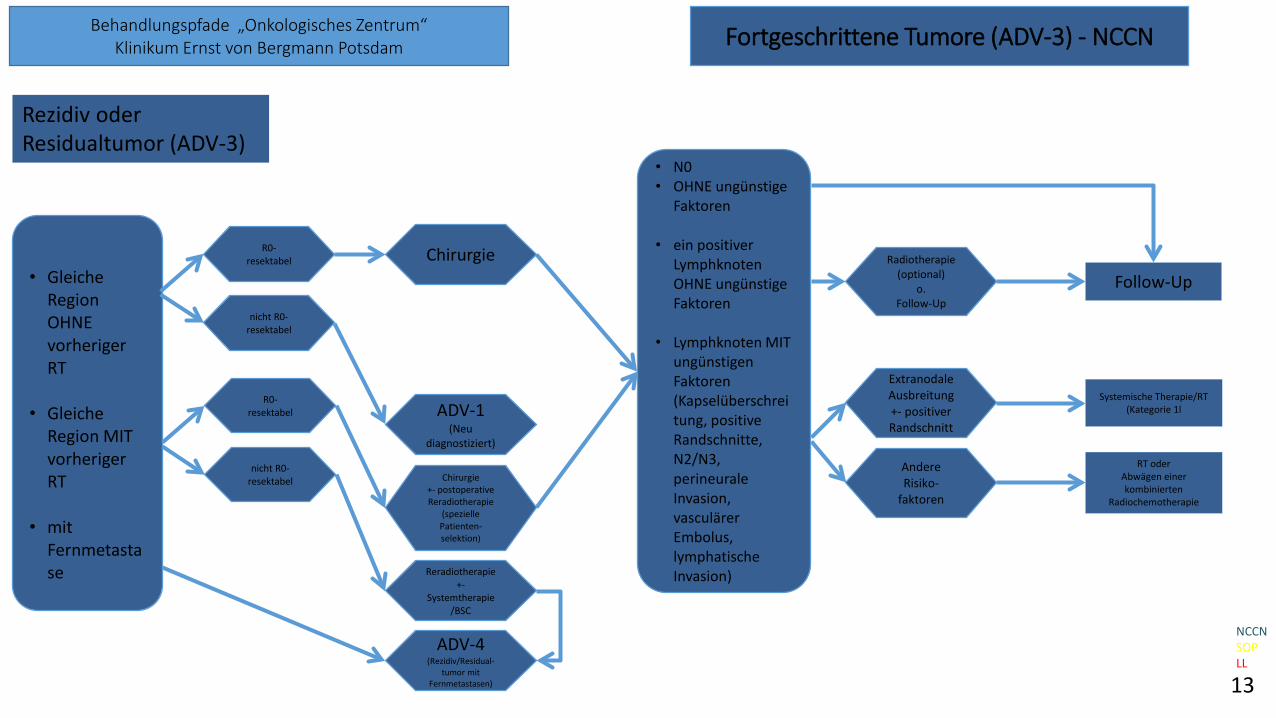
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Fortgeschrittene Tumore (ADV-3) - NCCN
Rezidiv oderResidualtumor (ADV-3)
• Gleiche Region OHNE vorheriger RT
• Gleiche Region MIT vorheriger RT
• mit Fernmetastase
R0-resektabel
nicht R0-resektabel
Reradiotherapie+-
Systemtherapie/BSC
Follow-Up
Systemische Therapie/RT(Kategorie 1l
R0-resektabel
nicht R0-resektabel
ADV-1(Neu
diagnostiziert)
Chirurgie+- postoperative Reradiotherapie
(spezielle Patienten-selektion)
ADV-4(Rezidiv/Residual-
tumor mit Fernmetastasen)
Extranodale Ausbreitung+- positiver Randschnitt
Andere Risiko-
faktoren
RT oder Abwägen einer kombinierten
Radiochemotherapie
13
NCCNSOPLL
Chirurgie
• N0• OHNE ungünstige
Faktoren
• ein positiver Lymphknoten OHNE ungünstige Faktoren
• Lymphknoten MIT ungünstigen Faktoren (Kapselüberschreitung, positive Randschnitte, N2/N3, perineuraleInvasion, vasculärerEmbolus, lymphatische Invasion)
Radiotherapie(optional)
o.Follow-Up

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Fortgeschrittene Tumore (ADV-4) - NCCN
Rezidiv oderResidualtumor mit Fernmetastasen (ADV-4)
Studien-einschluss(präferiert)
Palliative chirurgische Maßnahmen
nur Fernmetastase
• Studien-einschluss
• PS 0-1
• PS 2
• PS 3
kombinierte Systemtherapie
Radiochemotherapie (für spezielle
Patientenselektion mit wenig Metastasen)
BSC
Chirurgie
Radiotherapie
Systemische Monotherapie
Systemische Monotherapie
BSC
BSC
Systemische Therapie
BSC
Studieneinschluss(präferiert)
BSC
14
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Follow-Up – NCCN + LL
Anamnese und klinische Untersuchung inklusive zahnärztlicher Untersuchung:- Jahr 1 und 2: alle 3 Monate- Jahr 3-5: alle 6 Monate- >5 Jahre: alle 12 Monate
(darin enthalten sind: sorgfältige und systematische Untersuchung der gesamten Mundhöhle, des Oropharynx und des Halses; Frage nach Schmerzen und Gewichtsverlust)
Bildgebung:- Ultraschalluntersuchung des Halses zu jedem Termin- Jahr 1 und 2: CT Kopf und Hals oder MRT alle 6 Monate- Jahr 3-5: alle 12 Monate- ggf. CT-Thorax bei Raucheranamnese oder PET-CT bei V.a. lokoregionäres Rezidiv, Fernmetastase, Zweittumor (PE
erst nach Bildgebung)-> Bei Auffälligkeiten dann Tumorboard
Labor:- TSH-Kontrolle alle 6-12 Monate, wenn Hals mitbestrahlt
Supportive Therapie:- Logopädievorstellung (ggf. Schluck-, Sprechanalyse / -training)- Höranalyse / -Training- Evaluation der Ernährungssituation- psychologische Vorstellung (Depressionsevaluation)- Suchtberatung- SAPV- Lymphdrainage bei Bedarf- Kaufunktionelle Therapie
15
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Radiotherapie Mundhöhlenkarzinom - NCCN
DEFINITIVE:RT Alone
• Planning target volume (PTV)
− High risk: Primary tumor and involved lymph nodes (this includes possible local subclinical infiltration at the primary site and at the high-risk level lymph node(s))
Fractionation:- 66 Gy (2.2 Gy/fraction) to 70 Gy (2.0 Gy/fraction); daily Monday–Friday in 6–7 weeks- Concomitant boost accelerated RT:
- 72 Gy/6 weeks (1,8 Gy/fraction, large field; 1,5 Gy boost as second daily fraction during last 12 treatment days)- 66-70 Gy (2,0 Gy/fraction; 6 fractions/wk accelerated
- Hyperfraction: 81,6 Gy/7 weeks (1,2 Gy/fraction, twice daily)
- Low to intermediate risk: Sites of suspected subclinical spread- 44–50 Gy (2.0 Gy/fraction) to 54–63 Gy (1.6–1.8 Gy/fraction)
• Brachytherapy- Interstitial brachytherapy is considered for selected cases.
- Low dose-rate (LDR) brachytherapy (0.4–0.5 Gy per hour): - Consider LDR boost 20–35 Gy if combined with 50 Gy EBRT or 60–70 Gy over
several days if using LDR as sole therapy- High dose-rate (HDR) brachytherapy:
- Consider HDR boost 21 Gy at 3 Gy/fraction if combined with 40–50 Gy EBRT or 45–60 Gy at 3–6 Gy/fraction if using HDR as sole therapy.
POSTOPERATIVERT• Preferred interval between resection and postoperative RT is ≤6 weeks. • PTV- High risk: Adverse features such as positive margins (see footnote j on OR-3)
- 60–66 Gy (2.0 Gy/fraction) daily Monday–Friday in 6–6.5 weeks
- Low to intermediate risk: Sites of suspected subclinical spread- 44–50 Gy (2.0 Gy/fraction) to 54–63 Gy (1.6–1.8 Gy/fraction)
16
Rücksprache nach Bestrahlungsplanung zur regionalen Risikostratifizierung unter zahnärztlichen Aspekten gewünscht
(Auch von HNO-Tumoren)
NCCNSOPLL

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam Radiotherapie Lippenkarzinom - NCCN
DEFINITIVE:RT Alone
• Planning target volume (PTV)
High risk: Primary tumor and involved lymph nodes (this includes possible local subclinical infiltration at the primary site andat the high-risk level lymph node(s)) - 66 Gy (2.2 Gy/fraction) to 70 Gy (2.0 Gy/fraction); daily Monday–Friday in 6–7 weeksLow to intermediate risk: Sites of suspected subclinical spread- 44–50 Gy (2.0 Gy/fraction) to 54–63 Gy (1.6–1.8 Gy/fraction)- External beam RT (EBRT) ± brachytherapy- Brachytherapy
- Interstitial brachytherapy is considered for selected cases.- Low dose-rate (LDR) brachytherapy (0.4–0.5 Gy per hour):
- Consider LDR boost 20–35 Gy if combined with 50 Gy EBRT or 60–70 Gy overseveral days if using LDR as sole therapy
- High dose-rate (HDR) brachytherapy: - Consider HDR boost 21 Gy at 3 Gy/fraction if combined with 40–50 Gy EBRT or
45–60 Gy at 3–6 Gy/fraction if using HDR as sole therapy.
POSTOPERATIVERT• Preferred interval between resection and postoperative RT is ≤6 weeks. • PTV- High risk: Adverse features such as positive margins (see footnote j on LIP-3)
- 60–66 Gy (2.0 Gy/fraction) daily Monday–Friday in 6–6.5 weeks
17

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
Chemotherapie Mundhöhlen- und Lippenkarzinom – NCCN 1/2
PRINCIPLES OF SYSTEMIC THERAPYThe choice of systemic therapy should be individualized based on patient characteristics (PS, goals oftherapy).
• The preferred chemoradiotherapy approach for fit patients with locally advanced disease remainsconcurrent cisplatin and radiotherapy.
Squamous Cell Cancers(Lip, Oral Cavity, Oropharynx, Hypopharynx, Glottic Larynx, Supraglottic Larynx, Ethmoid Sinus, MaxillarySinus, Occult Primary)
• Primary systemic therapy + concurrent RT(category 1 if induction is chosen)
- High-dose cisplatin- Cetuximab (category 1 for oropharynx, hypopharynx, or larynx; category 2B for lip, oral cavity, ethmoidsinus, maxillary sinus, occult primary)- Carboplatin/infusional 5-FU (category 1)- Cisplatin/paclitaxel- Cisplatin/infusional 5-FU- Carboplatin/paclitaxel (category 2B)- Weekly cisplatin 40 mg/m (category 2B)
• Postoperative chemoradiation- Cisplatin (category 1 for high-risk non-oropharyngeal cancers)
18

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
Chemotherapie Mundhöhlen- und Lippenkarzinom – NCCN 2/2
PRINCIPLES OF SYSTEMIC THERAPYThe choice of systemic therapy should be individualized based on patient characteristics (PS, goals of therapy).Unless otherwise specied, regimens listed below can be used for either nasopharyngeal or non-nasopharyngeal cancer.
Recurrent, Unresectable, or Metastatic (with no surgery or RT option)• First-Line Combination Therapy Options:- Cisplatin or carboplatin/5-FU/cetuximab (non-nasopharyngeal) (category 1)- Cisplatin or carboplatin/docetaxel or paclitaxel- Cisplatin/cetuximab (non-nasopharyngeal)- Cisplatin/5-FU- Cisplatin or carboplatin/docetaxel/cetuximab (non-nasopharyngeal)- Cisplatin or carboplatin/paclitaxel/cetuximab (non-nasopharyngeal) - Cisplatin/gemcitabine (category 1) (nasopharyngeal) - Carboplatin/cetuximab (nasopharyngeal)
• First-Line Single-Agent Options:- Cisplatin- Carboplatin- Paclitaxel- Docetaxel- 5-FU- Cetuximab (non-nasopharyngeal) - Gemcitabine (nasopharyngeal)- Capecitabine
• Second-Line Therapy or Subsequent Therapy Options:- Combination therapy options listed above- Single-agent options listed above- Nivolumab (non-nasopharyngeal, if disease progression on or after platinum-containing chemotherapy) (category 1) - Pembrolizumab
- Non-nasopharyngeal: if disease progression on or after platinum-containing chemotherapy- Nasopharyngeal: if previously treated, PD-L1-positive recurrent or metastatic disease (category 2B)
19

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam TNM-Klassifikation – NCCN
TX: Primärtumor kann nicht beurteilt werden
Tis: Karzinoma in situ
T1: Tumor <= 2 cm mit DOI (depth of invasion) <= 5 mm
T2: Tumor <= 2 cm mit DOI > 5 mm oder Tumor > 2 cm und <= 4 cm mit DOI <= 10 mm
T3: Tumor > 2 cm und <= 4 cm mit DOI > 10 mm oder Tumor > 4 cm mit DOI <= 10 mm
T4: Moderat fortgeschrittener Tumor oder sehr fortgeschrittener Tumor
T4a: Moderat fortgeschrittener lokaler Tumor Tumor > 4 cm mit DOI > 10 mmoderTumor infiltriert nur angrenzende Strukturen (bspw. Knocheninfiltration der Mandibula / Maxilla oder infiltriert den Sinus maxillaris oder die Gesichtshaut(Wichtig: superfizielle Erosion von Knochen oder Zahnfach durch einen gingivalen Tumor reicht nicht aus, um diesen als T4 einzustufen.)
T4b: sehr fortgeschrittener lokaler TumorTumor infiltriert Masseterloge, die pterygoidalen Knochen, Schädelbasis und oder umschließt die A. Carotis interna.
WICHTIG: DOI bedeutet „Depth of invasion“ oder „Tiefe der Infiltration“ und NICHT Tumordicke!
Suffix:m: mehrere Primärtumore in einem Organ
20

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam TNM-Klassifikation – NCCN
Clinical N (cN)
4.2.1Clinical N (cN)
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Metastasis in a single ipsilateral lymph node, 3 cm or smaller in greatest dimension ENE {-}
N2 Metastasis in a single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension ENE {-}ormetastases in multiple ipsilateral lymph nodes, none larger than 6 cm in greatest dimension ENE {-}orin bilateral or contralateral lymph nodes, none larger than 6 cm in greatest dimension ENE {-}
N2a Metastasis in a single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension ENE {-}N2b Metastases in multiple ipsilateral nodes, none larger than 6 cm in greatest dimension, and ENE {-}N2c Metastases in bilateral or contralateral lymph nodes, none larger than 6 cm in greatest dimension, and ENE {-}
N3 Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE {-} ormetastasis in any node(s) and clinically overt ENE(+)
N3a Metastasis in a lymph node larger than 6 cm in greatest dimension ENE {-}N3b Metastasis in any node(s) and clinically overt ENE(+)
Note: A designation of “U” or “L” may be used for any N category to indicate metastasis above the lower border of the cricoid (U) or below thethe lower border of the cricoid (L). Similarly, clinical and pathological ENE should be recorded as ENE {-} or ENE {+}.
Suffix:(sn): Select if regional lymph node metastasis identified by SLN biopsy only.(f): Select if regional lymph node metastasis identified by FNA or core needle biopsy only.U: Metastasis above the lower border of the cricoidL: Metastasis below the lower border of the cricoid
21

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam TNM-Klassifikation – NCCN
Pathological N (pN)
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Metastasis in a single ipsilateral lymph node, 3 cm or smaller in greatest dimension ENE {-}
N2 Metastasis in a single ipsilateral node, 3 cm or smaller in greatest dimension ENE {-}orMetastasis larger than 3 cm but not larger than 6 cm in greatest dimension ENE {-}ormetastases in multiple ipsilateral lymph nodes, none larger than 6 cm in greatest dimension ENE {-}orin bilateral or contralateral lymph nodes, none larger than 6 cm in greatest dimension ENE {-}
N2a Metastasis in a single ipsilateral node 3 cm or smaller in greatest dimension ENE {+}ora single ipsilateral node larger than 3 cm but not larger than 6 cm in greatest dimension ENE {-}N2b Metastases in multiple ipsilateral nodes, none larger than 6 cm in greatest dimension, and ENE {-}N2c Metastases in bilateral or contralateral lymph nodes, none larger than 6 cm in greatest dimension, and ENE {-}
N3 Metastasis in a lymph node larger than 6 cm in greatest dimension and ENE {-} orMetastasis in a single ipsilateral node larger than 3 cm in greatest dimension and ENE {+}ormultiple ipsilateral, contralateral, or bilateral nodes, any with ENE {+}ora single contralateral node of any size and ENE {+}
N3a Metastasis in a lymph node larger than 6 cm in greatest dimension ENE {-}N3b Metastasis in a single ipsilateral node larger than 3 cm in greatest dimension and ENE {+}ormultiple ipsilateral, contralateral, or bilateral nodes, any with ENE {+}ora single contralateral node of any size and ENE {+}
Note: A designation of “U” or “L” may be used for any N category to indicate metastasis above the lower border of the cricoid (U) or below the the lower borderof the cricoid (L). Similarly, clinical and pathological ENE should be recorded as ENE {-} or ENE {+}.
Suffix:(sn): Select if regional lymph node metastasis identified by SLN biopsy only.(f): Select if regional lymph node metastasis identified by FNA or core needle biopsy only.U: Metastasis above the lower border of the cricoidL: Metastasis below the lower border of the cricoid
22

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam TNM-Klassifikation – NCCN
Distant metastasis
cM0: No distant metastasiscM1: distant metastasispM1: distant metastasis, microscopically confirmed
23

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam ECOG (PS)
ECOG Status (Performance Status / PS)
Grad Aktivitätsstatus0 Normale uneingeschränkte Aktivität wie vor der Erkrankung.
1 Einschränkung bei körperlicher Anstrengung, aber gehfähig; leichtekörperliche Arbeit bzw. Arbeit im Sitzen (z.B. leichte Hausarbeit oder Büroarbeit) möglich.
2 Gehfähig, Selbstversorgung möglich, aber nicht arbeitsfähig; kann mehrals 50% der Wachzeit aufstehen.
3 Nur begrenzte Selbstversorgung möglich; 50% oder mehr der Wachzeit an Bett oder Stuhl gebunden.
4 Völlig pflegebedürftig, keinerlei Selbstversorgung möglich; völlig an Bett oder Stuhl gebunden.
5 Tod
24

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam NCCN Categories of Evidence and Consensus
NCCN Categories of Evidence and Consensus
Category Explanation1 Based upon high-level evidence, there is uniform NCCN consensus that
the intervention is appropriate
2A Based upon lower-level evidence, there is uniform NCCN consensus thatthe intervention is appropriate
2B Based upon lower-level evidence, there is NCCN consensus thatthe intervention is appropriate
3 Based upon any level of evidence, there is mayor NCCN disagreement thatthe intervention is appropriate
All recommendations are category 2A unless otherwise indicated.
25

Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
Abkürzungsverzeichnis:
26
Abkürzung ErklärungBSC Best Supportive Care (Begleitende Therapie)ECE Extrakapsuläre Wachstum
ggf. GegebenenfallsLL LeitlinieNCCN National Comprehensive Cancer NetworkPS Performance Status (ECOG)o. OderSLN Sentinel Lymph NodeSOP Standard Operating Procedureu. und
Behandlungspfade „Onkologisches Zentrum“Klinikum Ernst von Bergmann Potsdam
MundhöhlenkarzinomLippenkarzinom
Stand Mai 2019
Autoren: Dr. Dr. Teltzrow, Dr. Laepple, Dr. Bertram13.05.2019
Überprüft: Prof. Dr. Maschmeyer, PD Dr. Badakhshi15.07.2019
Freigabe: Dr. Dr. Teltzrow, Prof. Dr. Maschmeyer13.08.2019