Dietfurter Natursteine - Dietfurt Natural Stones - Highlights

Aus der Klinik für Urologie
KRH Klinikum Siloah
Lehrkrankenhaus der Medizinischen Hochschule Hannover
Leiter: Prof. Dr. med. Christoph Wiesner
“Flexible ureterorenoscopy for treatment of kidney
stones: Establishment as primary standard therapy
in a tertiary stone center”
Dissertation
zur Erlangung des Doktorgrades der Medizin in der
Medizinischen Hochschule Hannover
vorgelegt von
Stephan Ising
aus Oldenburg
Hannover 2015

Angenommen vom Senat der Medizinischen Hochschule Hannover am
01.03.2016
Gedruckt mit Genehmigung der Medizinischen Hochschule Hannover
Präsident: Prof. Dr. med. Christopher Baum
Betreuer der Arbeit: Prof. Dr. med. Christoph Wiesner
Referent: PD Dr. med. Matthias Oelke
Korreferent: Prof. Dr. med. Michael Carsten Truß
Tag der mündlichen Prüfung: 01.03.2016
Promotionsausschussmitglieder:
Prof. Dr. med. Hermann Haller
Prof. Dr. med. vet. Klaus Otto
Prof. Dr. med. Martin Sauer

Inhaltsverzeichnis
1. Originalarbeit 1
Flexible Ureterorenoscopy for Treatment of Kidney Stones:
Establishment as Primary Standard Therapy in a Tertiary Stone Center.
Ising S, Labenski H, Baltes S, Khaffaf A, Thomas C, Wiesner C.
Urol Int. 2015 Sep 24. [Epub ahead of print]
2. Zusammenfassung 8
Einleitung 8
Diskussion 10
3. Literaturverzeichnis 15
4. Lebenslauf 16
5. Erklärung nach § 2 Abs. 2 Nr. 6 und 7 PromO 18

E-Mail [email protected]
Original Paper
Urol Int
DOI: 10.1159/000439574
Flexible Ureterorenoscopy for Treatment of Kidney Stones: Establishment as Primary Standard Therapy in a Tertiary Stone Center
Stephan Ising a Heike Labenski a Stefan Baltes a Aso Khaffaf a
Christian Thomas b Christoph Wiesner a
a Department of Urology, KRH Klinikum Region Hannover, Klinikum Siloah – Oststadt – Heidehaus, Hannover ,
b Department of Urology, Goethe-University, Frankfurt, Universitätsmedizin, Johannes Gutenberg-University,
Mainz, Germany
Introduction
Calculus formation in the upper urinary tract is one of the most common diseases among people in the western world. In Germany, approximately 750,000 cases of stone formation are diagnosed annually and a continuously in-creasing incidence has been observed in the last 10 years [1–3] . Current guidelines recommend extracorporeal shockwave lithotripsy (ESWL) as the first treatment op-tion for calculi located in the kidney or the upper ureter [1, 4] . However, since the development of ultrathin-sized flexible and rigid ureterorenoscopes, endoscopic tech-niques play an increasing role in stone treatment espe-cially for stones located in the ureter but also in the lower pole calyx of the kidney [5, 6] . The 2013 updated EAU Guidelines on urolithiasis state that flexible ureteroreno-scopy (fURS) is recommended as a valid alternative treat-ment option to ESWL for stones sized less than 1 cm in the renal pelvis and the upper pole and middle calix [7] . For lower pole calyceal stones, the treatment of choice is even considered primary fURS [7] .
Recently, Donaldson et al. [8] performed a systematic review and meta-analysis investigating the clinical effec-tiveness of ESWL, retrograde intrarenal surgery and percu-
Key Words
Kidney stones · Flexible ureterorenoscopy · Endoscopic
stone therapy
Abstract
Introduction: To analyze the primary stone free rate (pSFR)
of flexible ureterorenoscopy (fURS) in the treatment of re-
nal stones and to identify clinical predictors for the primary
freedom from renal stones. Materials and Methods: Two
hundred and seventy five patients, who underwent fURS for
kidney stones were analyzed. Results: Index stone size was
6 mm. The stone was located in the lower calyx in 48%. Ure-
teral access sheath was used in 97%. Operation time was 35
min and primary stone clearance was 83%. pSFR increased
from 74% in 2012 to 83% in 2013 and 90% in 2014 (p = 0.001).
Preoperative stenting, index stone size, cumulative stone
size, lithotripsy, ureteral access sheath and operation time
were significantly correlated with the pSFR by univariate
analysis. Multivariate regression analysis showed index
stone size, cumulative stone size, ureteral access sheath and
operation time as independent parameters for pSFR. Con-
clusions: fURS for kidney stones is safe with a high pSFR. Clin-
ical parameters for pSFR are stone size, use of ureteral access
sheath and operation time. In future, the effective use of
fURS for the removal of kidney stones needs to be checked
by prospective randomized trials. © 2015 S. Karger AG, Basel
Received: April 24, 2015
Accepted after revision: August 19, 2015
Published online: September 24, 2015 Internationalis
Urologia
Christoph Wiesner, MD Department of Urology KRH Klinikum Region Hannover, Klinikum Siloah – Oststadt – Heidehaus Stadionbrücke 4, DE–30459 Hannover (Germany) E-Mail christoph.wiesner @ krh.eu
© 2015 S. Karger AG, Basel0042–1138/15/0000–0000$39.50/0
www.karger.com/uin
C.T. and C.W. contributed equally for senior authorship.
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

Ising/Labenski/Baltes/Khaffaf/Thomas/Wiesner
Urol IntDOI: 10.1159/000439574
2
taneous nephrolithotomy for lower pole renal stones from 7 randomized controlled trials including 691 analyzed pa-tients. Retrograde intrarenal surgery and percutaneous therapy were superior to ESWL in clearing stone burden.
Effective ESWL is dependent on stone size and stone location. Calculi located in the renal pelvis are usually amenable to ESWL, with a documented stone-free rate of up to 90% [1, 7] . Larger stones in simple size, a huge stone burden or stones located in the lower pole calyx are main-ly associated with a decrease in primary stone free rates (pSFR) [9] . In addition, successful ESWL is dependent on skin-to-stone distance, resulting in poorer results in obese patients [10] . In contrast, no negative influence regarding body mass index (BMI) on the stone free rate was docu-mented for fURS [11] .
Ten years ago, a prospective randomized clinical trial comparing ESWL and fURS for treatment of up to 1 cm lower pole calyceal stones showed no significant differ-ence in pSFR. Since then, fURS had evolved dramatically including the ‘chip-on-the-tip’ camera technique in high definition visual quality, use of flexible access sheaths or intracorporeal lithotripsy devices suspecting further im-provement of endoscopic stone therapy today [12, 13] .
From an economic point of view, it was demonstrated that URS is favorable as compared to ESWL for distal ure-teral stones; this might not be true while using flexible ureterorenoscopes because of the high maintenance costs [14] .
Since 2012, fURS has been established as a standard therapy for the treatment of kidney stones in any location in our department. In this study, our aim was to evaluate the pSFR of fURS as well as to identify the clinical predic-tors for obtaining freedom from renal stones.
Material and Methods
With the acquisition of the newest generation ‘chip-on-the-tip’ digital flexible ureterorenoscopes (Olympus URF-V) in 2012, our patients were offered fURS as a primary therapy option for kidney stones of up to 2 cm in diameter. Pre-interventional elucidation included ESWL as an alternative option for stone treatment in all patients.
As a tertiary care center, the prospectively computerized files of 275 patients, who underwent fURS for renal calculi between 2012 and 2014, were reviewed. Low-dose non-contrast-enhanced computed tomography was the primary radiological investigation employed for the evaluation of stone burden and stone location. Preoperative urine check analysis was performed in all patients. Those who were found to have preoperative urinary tract infec-tions were treated with culture-specific antibiotics before therapy. The others received single-shot intraoperative cephalosporine an-tibiotics for prophylaxis.
fURS was performed under general anesthesia using an 8.3 Fr. digital flexible ureterorenoscope (URF-V, Olympus, Hamburg, Germany) on a fully digital radiological workstation (Uroskop Omnia, Siemens, Erlangen, Germany). Patients were placed in a lithotomy position. A ureteral access sheath (12 Fr access sheath ReTrace, Porges Coloplast GmbH – Hamburg, Germany) was used in 267 patients. A safety wire (Sensor flex, Boston Scientific, Natick, MA) was left alongside the ureteral access sheath. Stone extraction was performed using a zero tip nitinol basket (Boston Scientific, Natick, Mass., USA). Lithotripsy was performed using a Holmium YAG LASER (Medilas H20, 2.1 μm, 2,500 mJ, Dornier MedTech Europe GmbH, Wessling, Germany) with a 270 nm laser fiber at 4–8 Hz/800–2,500 mJ. Irrigation during fURS was pro-vided by an irrigation pressure pump (UROMAT E.A.S.I., KARL STORZ GmbH & Co., KG, Tuttlingen, Germany). At the end of the procedure, usually a 7 Fr ureteral MonoJ catheter (UROMED Kurt Drews KG, Oststeinbek) was used for stenting to prevent ob-struction secondary to tissue edema. The catheter was fixed to a transurethral CH 14 bladder catheter and both were removed after 24 to 48 h just before departure from hospital. In cases of compli-cations, such as ureteral perforation or residual stones, a double-J-tube was used.
Prestenting was generally performed under anesthesia and re-sulted from hydronephrosis due to initial ureter stones with intra-operative push back into the kidney as an emergency procedure or in cases when the access sheath could not be passed. Additionally, until end of 2013, we routinely performed prestenting to facilitate the placement of the ureteral access sheath in elective patients. Clearance from stone burden was checked directly at the end of the endoscopic procedure when stone treatment was completed. The presence of residual stones was optionally checked by plain X-ray or a urinary ultrasound taken on the day after intervention. How-ever, postoperative routine check by X-ray was not performed.
The pSFR was correlated with clinical parameters such as age, sex, BMI, DJ-stenting preoperatively, number of stones, index stone size (mm), cumulative stone size (sum of the diameters of all stones in one and the same patient, mm), stone location lower pole calyx, lithotripsy, ureteral access sheath and operating time (min) and taken from our prospective data base. Complications were classified using the Clavien-Dindo classification system [15] .
Statistical Analyses For statistical analysis, we used MedCalc (MedCalc Software,
Ostend, Belgium). Chi-square test was used to compare stone free rates in 2012, 2013 and 2014. Differences in operative time during the same time period were evaluated by the Mann–Whitney U test. The pSFR was correlated with the aforementioned clinical param-eters in uni- and multivariate logistic regression analyses (stepwise backward).
Results
A total of 275 patients underwent fURS for treatment of kidney stones between 2012 and 2014 in our depart-ment. Patient demographics are illustrated in table 1 . Pre-operative DJ stenting was performed in 249 patients (91%). The median index stone size was 6 mm (range
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

fURS for Treatment of Kidney Stones Urol IntDOI: 10.1159/000439574
3
1–11) and the median cumulative stone size was 7 mm (range 1–27). Lower calyceal stones were diagnosed in 132 patients (48%). Intraoperative ureteral access sheath was used in 267 patients (97%) for protection during fURS. In situ lithotripsy was performed in 159 patients
(58%). Postoperative DJ stenting was performed in 245 patients (89%). The median operation time was 35 min (range 4–118). Primary stone clearance, according to our definition was achieved in 228 patients (83%). The me-dian duration of hospital stay was 2 days (range 1–11).
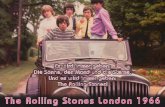
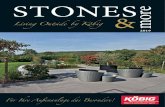
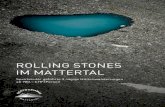
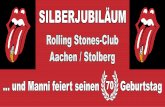
During the investigated time period, the median op-eration time continuously decreased from 45 min in 2012 to 37 min in 2013 and 27 min in 2014 (12 vs. 13, p = 0.03; 13 vs. 14, p = 0.003; fig. 1 ). Additionally, the pSFR in-creased from 74 in 2012 to 83 in 2013 and 90% in 2014 (12 vs. 14, p = 0.001; fig. 2 ). Uni- and multivariate logistic regression analyses for pSFR is shown in table 2 . Of the clinical parameters, preoperative stenting (yes vs. no: OR 3.6, 95% CI 1.55–8.42, p = 0.004), index stone size (>6 vs. ≤ 6 mm: OR 0.16, 95% CI 0.08–0.33, p < 0.0001), cumula-tive stone size (>7 vs. ≤ 7 mm: OR 0.16, 95% CI 0.08–0.34, p < 0.0001), lithotripsy (yes vs. no: OR 0.16, 95% CI 0.07–0.36, p < 0.0001), ureteral access sheath (yes vs. no: OR 20.3, 95% CI 1.76–32.91, p = 0.007) and operating time (>35 vs. ≤ 35 min: OR 0.21, 95% CI 0.11–0.43, p < 0.0001) were significantly associated with the pSFR by univariate analysis. By multivariate cox regression analysis, index stone size (OR 0.41, 95% CI 0.16–1.08, p = 0.04), cumula-tive stone size (OR 0.39, 95% CI 0.16–0.96, p = 0.04), ure-teral access sheath (OR 16.0, 95% CI 109–233, p = 0.005) and operation time (OR 0.39, 95% CI 0.17–0.89, p = 0.02) were found to be independent predictors for the pSFR.
Complications In a total of 24 patients (8.7%), complications (Cla-
vien-Dindo I–IIIb) were observed. In detail, Clavien Grade 1 complications including fever and urinary tract
0
20
40
60
80
100
2012 2013 2014
Year
Ston
e-fre
e ra
te (%
)
p = 0.001
68.8%
81.1%90.2%
p = 0.08p = 0.11
Fig. 1. A significant increase of the pSFR from 2012 to 2014 (p = 0.001) was ob-served.
Table 1. Patient characteristics (n = 275)
Age, years 53.0 (40.0–63.0)Gender
Male 188 (68.4)Female 87 (31.6)
BMI, kg/m2 27.0 (24.0–31.0)Stone burden
Left 115 (41.8)Right 160 (58.2)
Cumulative stone size 7 (5–10)Number of stones 1 (1–2)Index stone size, mm 6 (4–8)Stone lower calyx
Yes 132 (48.0)No 143 (52.0)
Hospitalization, days 2 (2–2)Re-intervention 47 (17.0)Number of re-interventions 1 (1–1)Lithotripsy 159 (57.8)Preoperative stent 249 (90.5)Postoperative stent 245 (89.1)Operation time, min 35 (24.0–52.0)Ureteral access sheath 267 (97.1)Stone free after 1 intervention 228 (82.9)One additional intervention 41 (14.9)Two additional interventions 6 (2.2)
Values are n (%) or median (interquartile range).
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

Ising/Labenski/Baltes/Khaffaf/Thomas/Wiesner
Urol IntDOI: 10.1159/000439574
4
infection were observed in 7 patients (2.5%). They were treated with iv. fluids, antibiotics and antipyretics for 5 days and the complications resolved thereafter. Cla-vien Grade 2 complications included prolonged hema-turia and were found in 11 patients (4%). In those pa-tients bladder irrigation through a hematuria transure-thral catheter was performed for 2 days. Clavien Grade 3b complications including ureteral perforation were recognized in 6 patients (2%). The perforation was man-aged by DJ stenting of the ureter for 2 weeks. No Clavien Grade 4 complications were observed and no major sur-gery had to be performed for complication manage-ment.
Discussion
fURS is a valid treatment option for patients with kid-ney stones of up to a size of 2 cm in diameter in the lower pole calyceal position [16] . However, its primary indica-tion in the upper/middle calyx or in the renal pelvis re-mains controversial [7] . Success is documented by the pSFR in the literature and it mainly depends on the esti-mated stone size ( ≤ 1 vs. >1 cm, ≤ 2 vs. >2 cm) and stone location (upper/middle calyx vs. lower pole calyx). Fur-thermore, the collecting system’s anatomy influences the success rate in the lower pole calyceal stone location [17] . Jessen et al. [17] investigated the infundibular length and
Table 2. Uni- and multivariate logistic regression analysis (stepwise backward; enter if p < 0.1; remove if p > 0.2) of predictors for pSFR
Variable Univariate Multivariate
coefficient OR 95% CI p value c oefficient OR 95% CI p value
Age >53 vs. ≤53 years –0.51 0.6 0.33–1.11 0.10Male vs. female 0.03 1.03 0.54–1.95 0.94Urethral access sheath yes vs. no 2.03 7.6 1.76–32.91 0.007 2.77 16.0 233–109.9 0.005Preoperative stent yes vs. no 1.28 3.6 1.55–8.42 0.004 0.95 2.6 0.95–7.02 0.062Lithotripsy yes vs. no –1.84 0.16 0.07–0.36 <0.0001 –0.89 0.41 0.16–1.08 0.072Number of stones >1 vs. ≤1 –0.13 0.87 0.45–1.69 0.69Index stone size >6 vs. ≤6 mm –1.84 0.16 0.08–0.33 <0.0001 –0.90 0.41 0.17–0.98 0.045Stone lower calyx yes vs. no –0.33 0.72 0.29–1.31 0.28BMI >27 vs. ≤27 –0.16 0.85 0.46–1.57 0.61Operation time >35 vs. ≤35 min –1.54 0.21 0.11–0.43 <0.0001 –0.94 0.39 0.17–0.89 0.025Cumulative stone size >7 vs. ≤7 mm –1.82 0.16 0.08–0.34 <0.0001 –0.93 0.39 0.16–0.96 0.041
0
20
40
60
80
100
120
2012 2013Year Year
45 min37 min
p = 0.033
0
20
40
60
80
100
120
2013 2014
Ope
rativ
e tim
e (m
in)
Ope
rativ
e tim
e (m
in)
37 min
27 min
p = 0.0003
a b
Fig. 2. Operation time significantly decreased from 2012 to 2014 (12 vs. 13, p = 0.033; 13 vs. 14, p = 0.0003).
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

fURS for Treatment of Kidney Stones Urol IntDOI: 10.1159/000439574
5
width and the infundibulopelvic angle in 111 fURS for lower pole stones. They found that a long infundibulum and acute infundibulopelvic angle <30° negatively affects the pSFR. An adequate evaluation of the SFR is manda-tory but its documentation is inconsistent in the litera-ture.
A randomized study investigated the outcome of fURS (n = 70 patients) with ESWL (n = 70 patients) for lower pole stones smaller than 1 cm [18] . The pSFR was signif-icantly higher for fURS (100%) as compared to ESWL (91%). Another analysis included 789 matched pair pa-tients with larger lower pole stones of 1–2 cm [19] . In this study, the pSFR was 92% for fURS but 40% for ESWL only (p < 0.0001). In both studies, complications were higher for fURS without being statistically different. From those data it could be concluded to consider fURS as an alterna-tive first treatment option at least for lower pole calyceal stones even when larger than 1 cm in diameter.
Cecen et al. [30] treated stones (1–2 cm in diameter) located in the upper/middle calyx in their retrospective study either by fURS (n = 66) or by ESWL (n = 108). The pSFR was lower for ESWL (87%) when compared to fURS (92%). However, the difference was not statistically sig-nificant (p = 0.27). In our series, 48% of the patients were treated for a lower pole calyceal index stone with a median stone size of 6 mm (range 2–15). The pSFR was 81% ( ≤ 1 cm: 84%; >1 cm: 64%). The others had upper/middle calyceal stones of 6 mm (range 1–17) with a pSFR of 85% ( ≤ 1 cm: 89%; >1 cm: 43%). The pSFR was not associated with stone location but was negatively correlated with cat-egorized index stone size (>6 vs. ≤ 6 mm: OR 0.16, p < 0.0001) in our univariate analysis. Additionally, the index stone size remained an independent parameter for the pSFR by our multivariate analysis (OR 0.41, p = 0.04). For the whole cohort, with any stone location in the kidney, we observed a learning curve regarding the pSFR from 69% in 2012 where we started the procedure to 90% in 2014 (p = 0.001). Being an educational hospital, we started a training program for our residents with guided surgery of an experienced endourologist in 2014. However, an ide-al training model for fURS prior to real live surgery is missing. Tunc et al. [20] reported an in vivo porcine mod-el that may help in practicing under realistic conditions.
Recently, numerous percutaneous transrenal micro techniques have emerged, especially as alternative proce-dures for lower pole stones between 1 and 2 cm in diameter. Sabnis et al. [21] report the outcome of 70 patients who were randomized to microperc or retrograde intrarenal surgery for kidney stones with a mean stone size of 1 cm. The overall stone clearance did not differ between the 2
groups (97.1 vs. 94.1%). The authors concluded micrope-rc as an alternative treatment option to URS. Similar re-sults were documented by Wilhelm et al. [22] (SFR 92 vs. 96%). However, the mean operating time was significantly longer in the microperc group (130 vs. 98 min, p = 0.002). Xu et al. [23] found that fURS using intrarenal holmium laser lithotripsy may serve as an alternative to mini percu-taneous procedures even in larger kidney stones (>2 cm diameter). The estimated pSFR was 65% in their study and increased to 89% 6 months after the first surgery.
The BMI is well known to correlate with the incidence of urolithiasis [24] . A high BMI additionally influenced the outcome of ESWL negatively due to difficult stone location and increased skin-to-stone distance with atten-uation of the application of shock wave energy [25] . Sari et al. [11] investigated the effect of the BMI on outcome of fURS. The average BMI was 26 with a distribution of normal weighted patients being 43%, overweight 32%, obese 22% and morbidly obese 3%. Clinical stone param-eters in between the groups were comparable. The pSFR was 61, 62, 74 and 62%, respectively (p = 0.08). In the pre-sented series, the median BMI was 27 (range 18–53). Ac-cording to the definition by Sari, a total of 99% of our patients were at least overweight and 35% were obese or morbidly obese. In our statistical analysis, the BMI had no influence on the clinical outcome. The conclusion could be that achieving higher pSFR by fURS is possible when compared to ESWL among the obese, who com-prise a majority of patients with renal stones. However, this hypothesis should be confirmed by a prospective ran-domized study.
Ureteral access sheath was introduced in 1974 and lauded for a means of passing the flexible ureteroreno-scope [26] . However, passage was sometimes difficult, es-pecially in ureters without preoperative stenting, resulting in an increased risk of ureteral injury during the place-ment [27] . Today, the newest generation of devices has impregnated wires and hydrophilic coating for easier and safer insertion. Therefore, the urgent need of a postopera-tive stenting is discussed controversially and may be as-sociated with patients’ discomfort. Torricelli et al. [28] compared the data of patients, who underwent fURS with the ureteral access sheath with or without postoperative stenting. Their indication for postoperative stenting in-cluded older patients, use of larger ureteral access sheaths and presence of greater stone burden. The postoperative-ly stented group had significantly lower pain scores as compared to the postoperatively unstented group. Inter-estingly, preoperative stenting resulted in lower pain scores in the postoperatively unstented group only con-
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

Ising/Labenski/Baltes/Khaffaf/Thomas/Wiesner
Urol IntDOI: 10.1159/000439574
6
cluding that prestenting may result in a more dilated ure-ter and easier passage of the ureteral access sheath during fURS. The authors concluded that patients with large stones and large sheaths should be treated with postop-erative stenting to decrease postoperative pain. In this study, a great majority of our patients (90%) were rou-tinely stented preoperatively to facilitate ureteral access sheath placement. Ureteral access sheaths were used in 267 out of 275 patients. In our statistical analysis, pre-stenting and ureteral access sheath were significantly as-sociated with our pSFR. Additionally, the use of ureteral access sheath was an independent prognosticator for the pSFR. For prevention of postoperative ureteral obstruc-tion due to mucosal swelling, almost 90% of our patients were stented postoperatively. The median operative time and median index stone size was lower in our postopera-tively non-stented as compared to the stented patients (in-dex stone size: 4 vs. 6 mm; operative time: 18 vs. 37 min). To overcome patients’ discomfort, we changed our initial concept of postoperative DJ stenting for 7 days to MonoJ stenting for 24–48 h following stent removal just before discharge from hospital. With this concept, no severe ure-teral injury from the access sheath was documented.
In this study, some of the patients had an initial ure-teral stone that moved into the kidney during retrograde urography and preoperative stenting, which changed the stone treatment from rigid to flexible. Seklehner et al. [29] found that retrograde pyelography prior to ureteroscopy for ureteral stones was associated with a significantly in-ferior stone-free-rate (87 vs. 73%) by changing the stone location from more distally to the proximal ureter.
This study has several limitations. First, the investi-gated collective is very heterogeneous concerning the number of treated stones, stone size and stone location. We therefore concentrated on the index stone size and
additionally evaluated the cumulative stone size. Sec-ond, the vast majority of our patients was stented preop-eratively and treated by the ureteral access sheath. This leads to a bias when to compare the pSFR with unstent-ed patients. Third, the pSFR was not routinely checked by radiographic evaluation postoperatively. However, we think that a careful reflection of the collecting system at the end of each endoscopic procedure leads to a meaning-ful estimation of significant residual stone masses.
In conclusion, fURS for kidney stones is a safe proce-dure. In this study, it was found that the operation time decreased significantly with increasing experience, sug-gesting that fURS is a procedure that can be easily learned. pSFR is associated with stone size, use of ureteral access sheath and operation time. In future, the effective use of fURS as compared to ESWL or microperc procedures for kidney stones as first treatment option has to be checked by prospective randomized trials.
Disclosure Statement
The authors declare no conflict of interest.
Authors Contribution
S.I. has collected the data of the patients and has made intel-lectual contribution to the design of the study and has written the manuscript; H.L., S.B. and A.K. have made intellectual contribu-tion to design the study and to the manuscript; C.T. has made in-tellectual contribution to the design of the study and performed the statistical analysis; C.W. has made intellectual contribution to the design of the study and to the manuscript and has approved the final version of the manuscript; All authors have read and ap-proved the final manuscript; The study was conducted in compli-ance with the Declaration of Helsinki.
References
1 Arbeitskreis Harnsteine der Akademie der Deutschen U, Arbeitskreis Endourologie und Steinerkrankung der Osterreichischen Ge-sellschaft für Urologie, Knoll T: [S2 guidelines on diagnostic , therapy and metaphylaxis of urolithiasis: part 1: diagnostic and therapy]. Urologe A 2009; 48: 917–924.
2 Turney BW, Reynard JM, Noble JG, Ke-oghane SR: Trends in urological stone disease. BJU Int 2012; 109: 1082–1087.
3 Nowfar S, Palazzi-Churas K, Chang DC, Sur RL: The relationship of obesity and gender prevalence changes in United States inpatient nephrolithiasis. Urology 2011; 78: 1029–1033.
4 Preminger GM, Assimos DG, Lingeman JE, Nakada SY, Pearle MS, Wolf JS Jr; AUA Nephrolithiasis Guideline Panel: Chapter 1: AUA guideline on management of staghorn calculi: diagnosis and treatment recommen-dations. J Urol 2005; 173: 1991–2000.
5 Johnson GB, Portela D, Grasso M: Advanced ureteroscopy: wireless and sheathless. J En-dourol 2006; 20: 552–555.
6 Breda A, Ogunyemi O, Leppert JT, Schulam PG: Flexible ureteroscopy and laser lithotrip-sy for multiple unilateral intrarenal stones. Eur Urol 2009; 55: 1190–1196.
7 Türk C KT, Petrik A, Sarica K, Seitz C, Skolarikos A, Straub M: Guidelines on Urol-thiasis (update march 2013). EAU Guide-lines, 25th EAU Annual Congress, Barcelona 2010, ISBN 978-90-79754-70-0. Arnhem, The Netherlands, EAU Guidelines Office, 2013, pp 293–326.
8 Donaldson JF, Lardas M, Scrimgeour D, Stewart F, MacLennan S, Lam TB, McClinton S: Systematic review and meta-analysis of the clinical effectiveness of shock wave lithotrip-sy, retrograde intrarenal surgery, and percu-taneous nephrolithotomy for lower-pole re-nal stones. Eur Urol 2015; 67: 612–616.
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

fURS for Treatment of Kidney Stones Urol IntDOI: 10.1159/000439574
7
9 Zehnder P, Roth B, Birkhäuser F, Schneider S, Schmutz R, Thalmann GN, Studer UE: A prospective randomised trial comparing the modified HM3 with the MODULITH ® SLX-F2 lithotripter. Eur Urol 2011; 59: 637–644.
10 Pareek G, Hedican SP, Lee FT Jr, Nakada SY: Shock wave lithotripsy success determined by skin-to-stone distance on computed to-mography. Urology 2005; 66: 941–944.
11 Sari E, Tepeler A, Yuruk E, Resorlu B, Akman T, Binbay M, Armagan A, Unsal A, Muslum-anoglu AY: Effect of the body mass index on outcomes of flexible ureterorenoscopy. Uro-lithiasis 2013; 41: 499–504.
12 Beiko DT, Denstedt JD: Advances in uretero-renoscopy. Urol Clin North Am 2007; 34: 397–408.
13 Pearle MS, Lingeman JE, Leveillee R, Kuo R, Preminger GM, Nadler RB, Macaluso J, Mon-ga M, Kumar U, Dushinski J, Albala DM, Wolf JS Jr, Assimos D, Fabrizio M, Munch LC, Na-kada SY, Auge B, Honey J, Ogan K, Pattaras J, McDougall EM, Averch TD, Turk T, Pietrow P, Watkins S: Prospective, randomized trial comparing shock wave lithotripsy and ure-teroscopy for lower pole caliceal calculi 1 cm or less. J Urol 2005; 173: 2005–2009.
14 Matlaga BR, Jansen JP, Meckley LM, Byrne TW, Lingeman JE: Economic outcomes of treat-ment for ureteral and renal stones: a systematic literature review. J Urol 2012; 188: 449–454.
15 Dindo D, Demartines N, Clavien PA: Classi-fication of surgical complications: a new pro-posal with evaluation in a cohort of 6336 pa-tients and results of a survey. Ann Surg 2004; 240: 205–213.
16 Srisubat A, Potisat S, Lojanapiwat B, Settha-wong V, Laopaiboon M: Extracorporeal shock wave lithotripsy (ESWL) versus percu-
taneous nephrolithotomy (PCNL) or retro-grade intrarenal surgery (RIRS) for kidney stones. Cochrane Database Syst Rev 2009; 4:CD007044.
17 Jessen JP, Honeck P, Knoll T, Wendt-Nordahl G: Flexible ureterorenoscopy for lower pole stones: influence of the collecting system’s anatomy. J Endourol 2014; 28: 146–151.
18 Sener NC, Imamoglu MA, Bas O, Ozturk U, Goktug HN, Tuygun C, Bakirtas H: Prospec-tive randomized trial comparing shock wave lithotripsy and flexible ureterorenoscopy for lower pole stones smaller than 1 cm. Uroli-thiasis 2014; 42: 127–131.
19 El-Nahas AR, Ibrahim HM, Youssef RF, Sheir KZ: Flexible ureterorenoscopy versus extra-corporeal shock wave lithotripsy for treat-ment of lower pole stones of 10–20 mm. BJU Int 2012; 110: 898–902.
20 Tunc L, Resorlu B, Unsal A, Oguz U, Diri A, Gozen AS, Bedir S, Ozgok Y: In vivo porcine model for practicing retrograde intrarenal surgery. Urol Int 2014; 92: 64–67.
21 Sabnis RB, Ganesamoni R, Doshi A, Ganpule AP, Jagtap J, Desai MR: Micropercutaneous nephrolithotomy (microperc) vs retrograde intrarenal surgery for the management of small renal calculi: a randomized controlled trial. BJU Int 2013; 112: 355–361.
22 Wilhelm K, Hein S, Adams F, Schlager D, Mi-ernik A, Schoenthaler M: Ultra-mini PCNL versus flexible ureteroscopy: a matched analy-sis of analgesic consumption and treatment-related patient satisfaction in patients with re-nal stones 10–35 mm. World J Urol 2015, Epub ahead of print.
23 Xu C, Song RJ, Jiang MJ, Qin C, Wang XL, Zhang W: Flexible ureteroscopy with hol-mium laser lithotripsy: a new choice for in-
trarenal stone patients. Urol Int 2015; 94: 93–98.
24 Semins MJ, Shore AD, Makary MA, Magnu-son T, Johns R, Matlaga BR: The association of increasing body mass index and kidney stone disease. J Urol 2010; 183: 571–575.
25 Delorme G, Huu YN, Lillaz J, Bernardini S, Chabannes E, Guichard G, Bittard H, Klein-clauss F: Ureterorenoscopy with holmium-yttrium-aluminum-garnet fragmentation is a safe and efficient technique for stone treat-ment in patients with a body mass index su-perior to 30 kg/m2. J Endourol 2012; 26: 239–243.
26 Takayasu H, Aso Y: Recent development for pyeloureteroscopy: guide tube method for its introduction into the ureter. J Urol 1974; 112: 176–178.
27 Traxer O, Thomas A: Prospective evaluation and classification of ureteral wall injuries re-sulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol 2013; 189: 580–584.
28 Torricelli FC, De S, Hinck B, Noble M, Monga M: Flexible ureteroscopy with a ureteral ac-cess sheath: when to stent? Urology 2014; 83: 278–281.
29 Seklehner S, Heißler O, Engelhardt PF, Riedl C: Does a retrograde pyelography prior to ureteroscopy influence stone-free rates and complication rates in ureteral calculi? Urol Int 2015; 94: 166–172.
30 Cecen K, Karadag MA, Demir A, Bagcioglu M, Kocaaslan R, Sofikerim M: Flexible ure-terorenoscopy versus extracorporeal shock wave lithotripsy for the treatment of upper/middle calyx kidney stones of 10-20 mm: A retrospective analysis of 174 patients. Spring-erplus 2014;3:557.
Dow
nlo
aded b
y:
Verlag S
. K
AR
GE
R A
G,
BA
SE
L
172.1
6.7
.29 -
10/7
/2015
4:5
3:3
4 P
M

8
Zusammenfassung
Einleitung
Die Urolithiasis ist eine der häufigsten urologischen Erkrankungen in
Deutschland mit einer kontinuierlich steigenden Prävalenz in den letzten 10
Jahren [1, 2]. Die aktuellen Leitlinien sehen zur Behandlung von Kelchsteinen
und hohen Harnleitersteinen die Extrakorporale Stosswellenlithotripsie (ESWL)
als Therapie der ersten Wahl vor [1, 3]. Aufgrund des technischen Fortschrittes
bei der Entwicklung immer dünnerer flexibler und rigider Ureterorenoskope bei
gleichzeitiger Verbesserung der optischen Qualität gewinnen die
endoskopischen Techniken zunehmend an Bedeutung [4, 5]. In der 2013
aktualisierten Fassung der Leitlinien der EAU zur Urolithiasis wird die
Ureterorenoskopie als Alternative zur ESWL bei Steinen bis 20 mm mit
Ausnahme der unteren Kelchsteine empfohlen, hier wird die endoskopische
Therapie sogar favorisiert [6].
Eine effektive ESWL ist abhängig von der Steingröße und -lokalisation, dem
Body Mass Index (BMI) sowie dem Abstand zwischen Haut und Stein [6, 7].
Während Steine im Nierenbecken mit dokumentierten primären
Steinfreiheitsraten (pSFR) bis zu 90% durch eine ESWL therapiert werden
können, sinkt die Steinfreiheitsrate mit zunehmender Steinlast, bei Vorliegen
multipler Steine sowie einer Steinlokalisation in der unteren Kelchgruppe [7].

9
Der BMI hat dagegen bei der flexiblen Ureterorenoskopie (fURS) keinen
Einfluss auf die pSFR[8].
Eine prospektive randomisierte Studie hatte vor 10 Jahren bei Steinen bis 10 mm
und einer Lokalisation in der unteren Kelchgruppe keinen Vorteil bezüglich der
pSFR für die fURS verglichen mit der ESWL gezeigt [9]. Seitdem hat sich die
Technik verändert, es stehen jetzt Geräte mit „chip-on-the-tip“-Technik und
hochauflösendem Videosignal zur Verfügung. Darüber hinaus konnte die pSFR
mit Hilfe von Ureterschleusen und der intrakorporalen Laserlithotripsie weiter
verbessert und die intraoperative Komplikationsrate gesenkt werden [10].
Seit 2012 haben wir die flexible Ureterorenokopsie als Standardtherapie für
Nierensteine bis 20 mm Größe in unserer Klink etabliert. Ziel der Untersuchung
war die Evaluierung der pSFR und Identifikation klinischer Prädiktoren.

10
Diskussion
Während die fURS eine etablierte Behandlungsmethode für Nierensteine bis 20
mm Größe in der unteren Kelchgruppe ist [11], wird die primäre Indikation bei
Konkrementen in der mittleren/oberen Kelchgruppe und im Nierenbecken
weiterhin kontrovers diskutiert [6]. Der Behandlungserfolg wird durch die pSFR
dokumentiert, die maßgeblich von der Steingröße und -lokalisation abhängig ist
sowie von der Anatomie des Hohlsystems [12].
In einer randomisierten Studie wurden die Ergebnisse bei der Behandlung
unterer Kelchsteine < 10 mm per ESWL (n=70) und fURS (n=70) verglichen
[13]. Hierbei war die pSFR bei der fURS (100 %) signifikant höher als bei der
ESWL (91%). Eine weitere Studie hat 789 matched-pair-Patienten mit größeren
Steinen in der unteren Kelchgruppe (10-20 mm) verglichen [14]. In dieser
Arbeit war die pSFR 92 % für die fURS und 40% für die ESWL (p<0.0001). In
beiden Studien war die Komplikationsrate der fURS höher, jedoch nicht
statistisch signifikant.
Aus diesen Daten könnte geschlossen werden, dass die fURS als
Behandlungsmethode der ersten Wahl zumindest für untere Kelchsteine in
Betracht gezogen werden sollte, auch wenn diese größer als 10 mm sind.
Die korrekte Evaluierung der SFR ist entscheidend, wird jedoch in der Literatur
unterschiedlich gehandhabt.

11
In unserer Studie wurden 48% der Patienten an einem unteren Kelchstein mit
einer medianen Größe von 6 mm (range 2-15) behandelt. Die pSFR war 81 %
(≤1 cm: 84%; >1cm 64%). Die übrigen Patienten hatten Nierensteine an anderen
Lokalisationen, hier betrug die mediane Steingröße ebenfalls 6 mm (range 1-17)
mit einer pSFR von 85 % (≤1cm: 89%; >1cm: 43%). Die pSFR war nicht mit
der Steinlokalisation korreliert, es zeigte sich jedoch eine negative Korrelation
mit der Indexsteingröße (>6 vs. ≤6 mm: OR 0.16, p < 0.0001) in der univariaten
Analyse. Die Indexsteingröße blieb auch in der multivariaten Analyse ein
unabhängiger Parameter für die pSFR (OR 0.41m p=0.04).
Für das gesamte Patientenkollektiv konnte unabhängig von der Steingröße eine
Lernkurve bezüglich der pSFR identifiziert werden, beginnend 2012 mit 69%
bis 90% in 2014 (p=0.001).
Der BMI korreliert mit dem Auftreten einer Urolithiasis [15], ein hoher BMI
wirkt sich aufgrund des erhöhten Haut-Stein-Abstandes jedoch negativ auf die
SFR bei der ESWL aus. Sari et al. [8] untersuchten die Auswirkung des BMI bei
Patienten, die sich einer fURS unterzogen. Der durchschnittliche BMI war 26,
mit 43 % normalgewichtigen, 32 % übergewichtigen, 22 % fettleibigen und 3 %
krankhaft übergewichtigen Patienten. Die klinischen Steindaten waren in allen
Gruppen vergleichbar. Die pSFR war 61, 62, 74 und 62% (p=0.08). In unserer
Serie war der mediane BMI 27 (range 18-53). Nach der Definition von Sari
waren 99 % unserer Patienten zumindest übergewichtig mit 35 % Fettleibigkeit

12
bzw. krankhaftem Übergewicht. In unserer statistischen Analyse hatte der BMI
keinen Einfluss auf die pSFR. Hieraus wäre zu schließen, dass durch die fURS
bei übergewichtigen Patienten, die einen Großteil der Steinpatienten darstellen,
höhere pSFR verglichen mit der ESWL erreicht werden können. Diese
Hypothese sollte jedoch in einer prospektiven randomisierten Studie überprüft
werden.
Ureterschleusen dienen der Erleichterung beim Einführen flexibler
Ureterorenoskope und wurden erstmal 1974 vorgestellt [16]. Besonders bei
primär nicht geschienten Ureteren war die korrekte Platzierung häufig schwierig
und ging mit einer erhöhten Gefahr von Ureterverletzungen einher [17]. Die
neueste Generation von Schleusen lässt sich aufgrund imprägnierter Drähte und
hydrophiler Beschichtungen einfacher und sicherer einführen. Die
Notwendigkeit einer postoperativen passageren DJ-Versorgung wird seitdem
kontrovers diskutiert. Torricelli et al. haben die Daten von Patienten mit und
ohne postoperativer DJ-Schiene verglichen, die eine fURS mit Ureterschleuse
erhalten haben [18]. Die Indikation für ein postoperatives Stenting waren ältere
Patienten, die Verwendung größerer Schleusen oder eine größere Steinlast. Die
postoperativ geschiente Gruppe hatte signifikant niedrigere Schmerz-Scores im
Vergleich zur nicht geschienten Gruppe. Interessanter Weise hatten präoperativ
DJ-versorgte Patienten weniger Schmerzen in der postoperativ nicht geschienten
Gruppe. Durch die präoperative DJ-Versorgung wird eine Ureterdilatation
erzielt, die intraoperativ eine einfachere Passage der Ureterschleuse ermöglicht.

13
Die Autoren schlussfolgerten, dass Patienten mit großen Steinen oder bei der
Verwendung größerer Schleusen postoperativ eine DJ-Schiene erhalten sollten.
In unserer Studie waren 90 % der Patienten präoperativ mit einer DJ-Schiene
versorgt worden, um eine problemlose und atraumatische Einlage einer Schleuse
zu ermöglichen. Bei 267 von 275 Patienten wurde eine Schleuse bei dem
Eingriff verwendet. Statistisch waren sowohl das Pre-Stenting sowie die
Verwendung einer Schleuse signifikant mit der pSFR korreliert. Die Benutzung
einer Schleuse war außerdem ein unabhängiger Prognostikator für die pSFR.
Um eine postoperative schwellungsbedingte Ureterobstruktion zu vermeiden,
wurden fast 90 % unserer Patienten postoperativ mit einer Schiene versorgt. Die
mediane OP-Dauer und die mediane Indexsteingröße waren in der postoperativ
nicht DJ-versorgten Gruppe kleiner als in der ungestenteten Gruppe
(Indexsteingröße: 4 vs. 6 mm; OP-Dauer: 18 vs. 37 min.). Um einen höheren
Patientenkomfort zu erlangen, haben wir das initiale Konzept der DJ-
Versorgung für 7 Tage verlassen und postoperativ eine Mono-J-Schiene für
24-48 Stunden eingelegt, die vor Entlassung aus der Klinik entfernt wurde.
Mit unserem Konzept wurden keine ernsthaften Ureterverletzungen durch eine
Ureterschleuse dokumentiert.
Die präsentierte Studie hat mehrere Limitationen. Zum einen ist das Kollektiv
sehr inhomogen, was die Anzahl der behandelten Steine, die Steingröße und

14
-lokalisation angeht. Wir haben uns daher auf die Indexsteingröße konzentriert
und zusätzlich die kumulative Steingröße erfasst. Zum anderen war der Großteil
unserer Patienten präoperativ mit einer DJ-Schiene versorgt und wurde unter
Verwendung einer Ureterschleuse operiert. Dies führt zu einem Bias im
Vergleich der pSFR bei nicht gestenteten Patienten.
Die pSFR wurde postoperativ nicht routinemäßig radiologisch evaluiert, sondern
lediglich eine sorgfältige endoskopische Evaluation der Hohlsystems am Ende
des Eingriffs durchgeführt um eine pSFR anzunehmen.
Zusammenfassend lässt sich schlussfolgern, dass die fURS ein sicheres
Verfahren zur Behandlung von Nierensteinen ist. In der präsentierten Serie kam
es mit der Zeit zu einer signifikanten Verbesserung der OP-Dauer. Die pSFR ist
abhängig von der Steingröße, der Verwendung einer Ureterschleuse und der OP-
Dauer.
Zukünftig gilt es, die fURS mit der ESWL als Therapie der ersten Wahl bei
Nierensteinen in prospektiven randomisierten Studien zu vergleichen.

15
Literaturverzeichnis
1. Arbeitskreis Harnsteine der Akademie der Deutschen, U., U. Arbeitskreis Endourologie und Steinerkrankung der Osterreichischen Gesellschaft fur, and T. Knoll, [S2 guidelines on
diagnostic, therapy and metaphylaxis of urolithiasis : Part 1: Diagnostic and therapy]. Urologe A, 2009. 48(8): p. 917-24.
2. Turney, B.W., et al., Trends in urological stone disease. BJU Int, 2012. 109(7): p. 1082-7. 3. Preminger, G.M., et al., Chapter 1: AUA guideline on management of staghorn calculi:
diagnosis and treatment recommendations. J Urol, 2005. 173(6): p. 1991-2000. 4. Johnson, G.B., D. Portela, and M. Grasso, Advanced ureteroscopy: wireless and sheathless. J
Endourol, 2006. 20(8): p. 552-5. 5. Breda, A., et al., Flexible ureteroscopy and laser lithotripsy for multiple unilateral intrarenal
stones. Eur Urol, 2009. 55(5): p. 1190-6. 6. Türk C, K.T., Petrik A, Sarica K, Seitz C, Skolarikos A, Straub M. , Guidelines on Urolthiasis
(Update March 2013). EAU Guidelines, edition presented at the 25th EAU Annual Congress, Barcelona 2010.ISBN 978-90-79754-70-0. EAU Guidelines Office, Arnhem, The Netherlands. 2013:293-326., 2013.
7. Zehnder, P., et al., A prospective randomised trial comparing the modified HM3 with the
MODULITH(R) SLX-F2 lithotripter. Eur Urol, 2011. 59(4): p. 637-44. 8. Sari, E., et al., Effect of the body mass index on outcomes of flexible ureterorenoscopy.
Urolithiasis, 2013. 41(6): p. 499-504. 9. Pearle, M.S., et al., Prospective, randomized trial comparing shock wave lithotripsy and
ureteroscopy for lower pole caliceal calculi 1 cm or less. J Urol, 2005. 173(6): p. 2005-9. 10. Beiko, D.T. and J.D. Denstedt, Advances in ureterorenoscopy. Urol Clin North Am, 2007.
34(3): p. 397-408. 11. Srisubat, A., et al., Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous
nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones. Cochrane Database Syst Rev, 2014. 11: p. CD007044.
12. Jessen, J.P., et al., Flexible ureterorenoscopy for lower pole stones: influence of the collecting
system's anatomy. J Endourol, 2014. 28(2): p. 146-51. 13. Sener, N.C., et al., Prospective randomized trial comparing shock wave lithotripsy and
flexible ureterorenoscopy for lower pole stones smaller than 1 cm. Urolithiasis, 2014. 42(2): p. 127-31.
14. El-Nahas, A.R., et al., Flexible ureterorenoscopy versus extracorporeal shock wave lithotripsy
for treatment of lower pole stones of 10-20 mm. BJU Int, 2012. 110(6): p. 898-902. 15. Semins, M.J., et al., The association of increasing body mass index and kidney stone disease. J
Urol, 2010. 183(2): p. 571-5. 16. Takayasu, H. and Y. Aso, Recent development for pyeloureteroscopy: guide tube method for
its introduction into the ureter. J Urol, 1974. 112(2): p. 176-8. 17. Traxer, O. and A. Thomas, Prospective evaluation and classification of ureteral wall injuries
resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol, 2013. 189(2): p. 580-4.
18. Torricelli, F.C., et al., Flexible ureteroscopy with a ureteral access sheath: when to stent? Urology, 2014. 83(2): p. 278-81.

18
Erklärung nach § 2 Abs. 2 Nr. 6 und 7 PromO
Ich erkläre, dass ich die der Medizinischen Hochschule Hannover zur Promotion
eingereichte Dissertation mit dem Titel „Flexible Ureterorenoscopy for
Treatment of Kidney Stones: Establishment as Primary Standard Therapy in a
Tertiary Stone Center“ im KRH Klinikum Siloah, Klinik für Urologie, unter
Betreuung von Prof. Christoph Wiesner ohne sonstige Hilfe durchgeführt und
bei der Abfassung der Dissertation keine anderen als die dort aufgeführten
Hilfsmittel benutzt habe.
Die Gelegenheit zum vorliegenden Promotionsverfahren ist mir nicht
kommerziell vermittelt worden.
Insbesondere habe ich keine Organisation eingeschaltet, die gegen Entgelt
Betreuerinnen und Betreuer für die Anfertigung von Dissertationen sucht oder
die mir obliegenden Pflichten hinsichtlich der Prüfungsleistungen für mich ganz
oder teilweise erledigt.
Ich habe diese Dissertation bisher an keiner in- oder ausländischen Hochschule
zur Promotion eingereicht. Weiterhin versichere ich, dass ich den beantragten
Titel bisher noch nicht erworben habe.
Ergebnisse der Dissertation wurden in folgendem Publikationsorgan „Urologia
Internationales“ veröffentlicht.
Hannover, den 21.10.2015
___________________________________
(Stephan Ising)