GIB 19552402

of 7
-
Upload
vandermarkra -
Category
Documents
-
view
223 -
download
0
Transcript of GIB 19552402
-
8/8/2019 GIB 19552402
1/7
Psychosocial Risk Factors for Adverse Outcomes in Patients witt> Nonvaivuiar AtriaiFibriiiation Receiving WarfarinDaniel P. Schauer, MD, MSc,^-^ Charles J. Moomaw, PhD,^ Mark Wess, MD,^-^Thomas Webb, MD,^'^ Mark H. Eckman, MD, MS^-^'Division of Gnerai internai iVledicine. ijniversity of Cincinnati iViedicai Center, Cincinnati, Oiiio. USA; ^institute for ihe Study of fHeaitin,university of C incinnati iViedicai Center, Cincinnati, Oinio, USA; Deportm ent of N euroiogy, university of Cincinn ati Me dica i C enter,Cincinnati , Oh io, USA.
OBJECTIVE; Our goal was to establish wh ether psychosocial r isk fac-tors for nonadherence, previously identified as negative predictors ofwarfarin prescribing, are predictors of adverse events for patients w ithnonvaivuiar atriai fibrillation receiving warfarin.DESIGN: Retrospective cohort an alysis.SETTING: Ohio Medicaid administrative database.PATIENTS: We studied Ohio Medicaid recipients with nonvaivuiar atri-ai fibrillation receiving warfarin to determine whether a history of sub-stance abuse, psychiatric illness, or social factors (identified asconditions perceived to be ba rriers to adherence) are predictors of ad-verse events, including stroke, intracranial hemorrhage, and gastroin-testinal bleeding. Multivariable risk ratios were calculated for each riskfactor using Cox proportional hazards models.RESULTS: 9,345 patients w ere identified as having nonvaivuiar atriaifibnllation and receiving 2 or more warfarin p rescr iption s betwee n1997 and 2002 . The event rates for the sam ple as a whole were 1.5strokes, 0.7 intracranial hemorrhages, and 4.3 gastrointestine bleedsper 100 person-ye ars of follow-up. Subjects with substan ce ab use hadthe highe st adjusted risk ratio . 2.4 (95% confidence interval [CI!: 1.4.4.0) for an intracranial hemorrhage while receiving warfarin, followedby subjects with psychiatric illness, adjusted risk ratio of 1.5 (95%CI: 1.04. 2.1). Subjects with psychiatric illness also had an adjustedrisk ra tio of 1.4 (95 % CI: 1.1, 1.7) for str ok e. Pa tie nts in all 3 idenUfiedrisk groups were at a significantly increased risk of gastrointestinalbleeding.CONCLUSION: PaUents with nonvaivuiar atriai fibrillation treated withwarfarin who have psychosocial r isk factors for nonad herenc e have anincreased risk of adverse eve nts.KEY WORDS: atriai fibrillation: warfarin: risk factors: psychosocial:stroke: hemorrhage.DOI: 10.1111 /J . 1525-1497.2005.0242.xJ GEN INTERN MED 2005: 20:1114-1119.
P atien ts with nonv aivuiar atriai fibrillation have a fivefoldincrease In the incidence of thromboembollc stroke.''^Several factors have been identified tha t increase the risk of anembolie event in patients with nonvaivuiar atriai flbrillauonincluding increasing age, prior transient ischmie event orstroke, hypertension, diabetes, and left ventricular dysfunc-tion.^'^ While anticoagulation with warfarin h as been show n to
reduce the incidence of embolie events,^ ^ there is a n increased risk of bleeding.A number of ciinical risk factors for bleeding while receiving anticoagulation have been identified, such as an international normalized ratio (INR) greater than 3, poorly controlledhypertension, history of gastrointestinal bleeding, and increasing age,^''* but no pub lished m odels have included psychosociai risk factors in addition to the known clinical riskfactors. Several clinical rea son s for an elevated INR have been
identified including drug-drug interactions, noneompliancwith drug or diet, worsened heart failure, and impaired livefunction.'^' Current alcohol abuse h as been shown to be associated with major bleeding and an elevated INR in severasmall studies ' ' ' ' ^ and in 1 large study ' while others have nshown such an association.''^ No studies have examined theffect of psychiatrie illness on bleeding risk .Despite the evidence supporting the benefits of antlcoagulating patients with nonvaivuiar atriai fibrillation, only 30%to 55% of patients v^thout contraindications are currently receiving warfarin. "^^ One of the po tential ba rriers to prescribing warfarin may be physician concern about psychosociafactors that may impair effectiveness and present barriers to
therapy . A reeent study of Ohio Medicaid patie nts identifiedseveral psyehosocial factors that were negative predictors owarfarin use in newly diagnosed cases of atriai fibrillation.^Johnston and colleagues demonstrated in this study that patients with substan ce abu se had an adjusted odds ratio of 0.5(95% confidence interval (CI) 0.35, 0.99) for receiving warfariat the time of diagnosis. Patients w ith other perceived ba rrierto compliance, including psychiatric illness and soeiai riskfactors, had an adjusted odds ratio of 0.84 (95% CI 0.730.97) for receiving warfarin. The social risk factors includedno earegiver for the patient, homelessness and previous documentation of noneomplianee. In this study psychiatric illneswas defined as schizophrenia, affective psychosis (includinmajor depressive disorder, m anic disorder, or bipolar affectivdisorder), paranoia or other nonorganic psychosis as determined by inte rnation al C lassification of Diseases , Ninth Revsion, Clinical ModificaUon codes (ICD-9-CM) as these werconsidered to be likely predictors of nonadherence. No othepsychiatric diagnoses were considered. It has yet to be determined whether these negative predietors of warfarin prescribing are risk factors for adverse outcomes in patients receivinwarfarin.
The authors have no conicts of interest to declare for this article orthis research.
Address correspondence and reprint requests to Dr. Schauer: D ivisionof General Internal Medicine. University of Cincinnati Medical Center.P.O. Box 670535. Cincinnati. OH 45267-0535 (e-mail: DanielSchaueruc.edu).
Received for publication July 8. 2005and in revised form July 3, 2005Accepted for publication July 21. 2005
-
8/8/2019 GIB 19552402
2/7
JGIM Schauer et al, Psyehosocial Risk Factors for Adverse Outcomes 1115The specific aim of this study is to identily and quantify thepsychosoeiai r isk factors leading to thromboembolic and hem-orrhagic complications in Ohio Medicaid patients who receivedwarfarin for nonvaiv uiar atriai f ibrillation. We hypothes ize tha tsubstance abuse, psychiatr ic disease, and the social factorsthat are perceived barr iers to adherence increase the r isk ofboth thromboembolie and hemorrhagic events in these pa-t ients .
SUBJECTS AN D METHODSBasic Design and Data SourceWe performed a retrospective coh ort analy sis of Ohio Medicaidpatients f rom January 1, 997, through May 3i , 2002. Datawere collected from the Ohio Medicaid administrative claimsdatabase which has been well described elsewhere.^^"^^ Brief-ly, the database includes fee-for-serviee data from all institu-t ions , providers, and pharmacies that provide services to OhioMedicaid enroUees. The 2 Ohio Medicaid categories are peoplewho are Aged, Blind, or Disabled and Covered Families andChildren (CFC). All enrollees must meet income eligibility re-quirements: elder ly or disabled recipients must earn no morethan 64% of the federal poverty level. Recipient identificationnumbers link the data. The Institutional Review Board at theUniversity of Cineinnati approved the use of this database.Patient SelectionWe identified all subjects with 2 or more claims containing anICD-9-CM for atriai fibrillation (427.31) during the study pe-r iod of January i , 1997. through May 31, 2002. Two claimswere required for inclusion to ensure that we did not includesubjects with transient atriai f ibrillation. Exclusion criteria aredescribed in Figure 1.We used pharmacy claims data to determine when pa-tients filled prescriptions for warfarin, and we examined allwarfarin prescriptions filled. Searching for National DrugCodes eorresponding to warfarin and the ICD-9-CM codes in-dicating warfarin use identified warfarin prescriptions forthese patients. Patients were included in the study only if theyfilled 2 or more prescriptions for warfarin and if the averagetimebetween prescr ipt ion ref i l ls was less than 100 days. Wechose the 100-day window because some pa tients , on a s tabledose of anticoagulation, may receive up to a 3-month supplyper refill.Risi< FactorsWe identified the p syehosoc ial features of intere st from th e da -tabase using ICD-9-CM codes and then categorized them asbeing present or absent for each pat ient . Psychiatr ic i l lnesswas defined as schizophrenia (ICD-9-CM code 295.x), affectivepsychosis (296.x), paranoia (297.x), or other nonorganie psy-chosis (298.x). Affective psychosis includes major depressivedisorder, manie disorder, and bipolar affective disorder. Sub-stanee abuse was defined as aleohol dependence (303.x), drugdependence (304.x) , or nondependent abuse (305.x excluding305.1-tobacco use disorder). Social r isk factors included laekof housing (V60.0), inadequate housing (V60.1), inadequatematerial resources (V60.2), persons living alone (V60.3), noother household member able to render care (V60.4), or non-
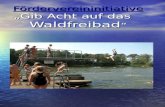
Excluded PatientsPatients with at least one ICD-9-CI\/lcode for atriai fibrillation:38,508
r2 or more codes for atriai fibrillation:25,200
rNo valvular heart disease:23,346
rAt least one warfarin prescription:11,395
r2 or more warfarin prescriptionsaveraging less than 100 days apart:9,885
rPatients included in the analysis:9,345
w
Only one code foratriai fibrillation:13,308
Valvular heart disease:1,854
No warfarinprescriptions:11,951
Only one warfarinprescription orintermittent:1,510
Prior stroke, intracranialhemorrhage orgastrointestinal bleed:540
FIGURE 1. Flow diagrann ot subjects. We ex clud ed all subjects with ohistory of volvular heart disease (2 or more claims w ith In ternationalClassification of Diseases, Ninth Revision, Clinical Modificationcodes tor mitral valve disease (394,x), aortic valve disease(395.x), mitral and aortic valve disease (396.x), heart valve trans-plant (V42.2), ar heart valve replacement (V43.3), or a procedurecode for mitral or aortic valve repair or replacement-(35.1Cfc35.14,35.20-35.28)). Subjects vi/ere excluded if fhey..had g previous-diag-nasis ot stroke (434.x, 438.x), intracranial hemorrhage (430.x. 431.x,'432.0, 432.1, 432.2, 432.9, 851-854), or gastrointestinai bleedihg(530.82, 531.2, 531.4, 531.6, 532.2, 532.4 532.6, 533.2, 533.4, 533.6,534.2, 534.4, 534.6, 535.xl, 537.83, 562.02, 562,03, 562.12, 562.13,569.3, 578.x) prior to starting wartarin therap y.
Covariates. which, a priori, were believed to confer inde-pendent risks for the outcomes, were identified from the data-set using ICD-9 CM codes. Hypertension (401-405), diabetesmellitus (250.x), chronic heart failure (4O2.xl, 4O4.xl, 404.x3,428), l iver disease (070.2-6, 070.9, 570, 571.x, 572.2-4,572.8), and renal disease (584.x, 585.x, 586.x) were the po-tential confounders identified for each patient as being presentor absent. We also included a history of deep vein thrombosis(451.1) in the modeling proeess as another indication for war-far in therapy. Demographic data were used to obtain the age,sex, and race for each subject. Another potential covariate in-eluded in the analysis was frequency of warfarin refills,
-
8/8/2019 GIB 19552402
3/7
1116 Schauer et ai. Psychosocial Risk F actors for Adverse Outcomes JGIadherence was considered present if the average time betweenprescription refills for a subject was greater than 32 days (themedian prescription refill time) and ab sent if less than or equalto 32 days.OutcomesWe defined adverse events b ased on ICD-9-CM codes tha t wererecorded on inpatient hospitalization elaims. Inpatient hospi-talization codes were required to improve the reliability of theclaim and the diagn osis. The primary adverse events consider-ed were stroke (434.x), intracranial h emorrhage (430.x, 431.x,432.0, 432,1, 432.2, 432.9, 851-854), and gastrointestinalbleeding (530.82, 531.2, 531.4, 531.6, 532.2, 532.4 532.6,533.2, 533,4, 533.6, 534.2, 534.4, 534.6, 535,xl, 537.83,562.02, 562,03, 562.12, 562.13, 569.3, 578.x). For gastroin-testinal bleeding, we only considered major bleeding as definedas bleeding requiring hospitalization. Other studies using ad-ministrative data have used a similar approach.' Date ofdeath was used to adjust the time at risk for each patientand was considered a secondary end point, although cause ofdeath was no t available in the dataset.Time at RiskThe date of a patient's initial warfarin prescription claim wasused to define the s tart of the pa tient's at-risk period. A patientwas then considered to be at risk until an adverse eventoccurred. Patients without adverse outcomes were censoredat 30 days following their last prescription for warfarin, theirdate of disenroUment from Medicaid or on their date of death . A30-day window was chosen to allow patients to finish takingtheir last prescription refill.
AnalysisWe used descriptive statistics including the t-test and the xtest to characterize the study sample, stratified by risk factoEvent rates for each outcome (stroke, intracranial hemorrage, and gastrointestinal bleeding) were calculated for eaerisk factor group and for the cohort as a whole.Cox proportional hazards models were used to evaluathe univariate relationship between each risk group and thpotential confounders with each outcome. We then selectethe variables that were signifieant predietors at P
-
8/8/2019 GIB 19552402
4/7
JGIM Schauer et al. Psychosocial Risk F actors for Adverse Outcomes 1117
Adverse eventStrokeIntracranialhemorrhageGastrointestinal bleed
Total(n =9,345)
308 (3.3)158(1.7)864 (9.5)Event rates (/IOO person-years)
StrokeIntracranialhemorrhageGastrointestinal Bleed
1.50 . 74 . 3
Table 2 . Adver s eNo Risk Factors(n =4,994)
141 (2.8)68(1 .4)
397 (8.0)1.30 . 63 . 7
Events Across Risk Factor G roups*Substance Abuse( n= 435)
13 (3.0)16 (3.7)^
55 (12.6)t1.41.76 . 2
Psyctilotrlc Illness(n=2 ,108)
87(4 .1)49 (2.3)t
245 (11.6)1. 81.05 .2
Social Risi< Factors(n =2 ,619)
108 (4.1)t44(1 .7)
3 1 4 ( 1 2 . 0 ) '1.80 . 75 . 3
' Re s u l t s are presented as number (%) unless otherwise noted,' P< .05 when compared with no risk factor group using x^.
pertension than the other subgroups. The subjects with socialrisk factors for nonadherence tended to be older and weremore likely to have chronic heart failure, diabetes mellitus.and renal disease (Table 1).With regard to the average time between prescription re-fills (Table 1). subjects with substance abuse and with socialrisk factors averaged significantly more time between prescrip-tion refills thctn subjects without risk factors for nonadher-ence. However, subjects with psychiatric illness filledprescriptions more frequently than any other risk group ex-amined.The percentage of subjects with each outcome andthe baseline event rates are presented for each risk group inTable 2. Significantly more strokes occurred in the subjectswith psychiatric illness and in the subjects with social riskfactors for nonad herence. Significantly more intracranial hem-orrhages occurred in subjects with substance abuse and psy-chiatric illness. All 3 risk groups had significantly moregastrointestinal bleeding events than the group with no riskfactors.Risk RatiosIn the univariate analysis (Table 3), there were several signif-icant predictors of increased risk for stroke at the P< .05 levelincluding psychiatric illness, social risk factors for nona dher-
ence. hypertension, diabetes mellitus, renal d isease, and Afri-can-American race. Only 2 variables conferred an increase riskof intracranial hemorrhage at the P 3 2 dAge (per decade )Sex. maleRace, white
Stroi
-
8/8/2019 GIB 19552402
5/7
1118 Schauer et ai. Psychosocial Risk Factors for Adverse Outcomes JGIM8% had 2 risk factors, and 0.5% of the patients had all 3. Forthe outcome of gastro intestin al bleeding in the adjuste d mod-els, the risk ratio for having any 1 of the psyc hosocial risk fac-tors was 1.19(95% CI 1.02. 1.37). for having any 2 risk factorsthe risk ra tio was 1.57 (9 5% CI 1.26. 1.95). and for a patienthaving all 3 risk factors the risk ratio wa s 2.85 (95% CI 1.56.5.21). This trend was signiflcant with a P value less tha n .00 1.For the outcomes of s t roke and in tracranial hemorrhage thetrend s towards increa sing risk with increasing num ber of r iskfactors were signiflcant w ith P values of .02 for both, however,the individual risk ratios were not all signiflcant.
DISCUSSIONWe have shown in the Ohio Medicaid population that psycho-social risk factors for nonadherence. previously identied asnegative predictors of warfarin prescribing, are strong predic-tors of adverse events in patients with nonvalvular atrial flbril-lation receiving warfarin compared with patients without theserisk factors. Subjects with psychiatric illnesses had a 36% in-crease in the risk of stroke, a 46% increase in the risk of In-tracranial h emorrhage, and a 19% increase in the r isk ofgastro intes t inal b leeding. Sub stance a buse rs had a 13 5% in-crease in the r isk of in tracranial hemorrhage and a 41 % in-crease in the risk of gastrointestinal bleeding. Subjects withsocial risk factors for non adh ere nce h ad a 28% increa sed riskfor gastrointestinal bleeding.
Previous studies have identifled clinical predictors forbleeding in patients receiving wa rfari n.^ '^ '^ and risk fac torsfor embolie events from atrial flbrillation.^-^ Several of thesepreviously identifled pred ictors of adverse events were not sig-niflcant in our multivariable models but were signiflcant in theunivariate analyses. We can only speculate as to why some ofthe other known risk factors for stroke were not predictive inth is analysis . W ang et al.^*^ have described prior stroke orTIA,diabetes , and hypertension as predictors of s t roke. In our co-hort we have excluded patients with a prior stroke or TIA inorder to incre ase th e validity of our outcom es (so that they willnot be incorrectly coded as "prior stroke or TIA"). Our cohorthas a fairly high proportion of comorbid conditions and it islikely we no longer have the same discriminatory power forsome of the other predictors including hypertension. Our in-cidence rates for the outcomes of s t roke, in tracranial hem-orrhage, and gastro intes t inal b leeding are s imilar to whatothers have reported in the literature for patients receivingancoagulation for atrial flbrillaon. '4.27.28
McMahan et al . , ' ' ' demonstrated that alcohol abuse wasassocia ted with a 2.7-fold inc reased risk of major bleeding in as tudy of 579 veterans , and W hite et al . '^ demonstrated that anadmission for an alcohol-related diagnosis was associatedwith a 2.6-fold increased risk of major bleeding in a study ofover 21,000 pat ients . Our re sul ts are s imilar to these f indings,part icularly for in tracranial hemorrhage, where we haveshown pat ients have 2 .5 t imes the r isk for in tracranial hem-orrhage i f they are substance abusers , which includes drugabuse in addition to alcohol. To our knowledge, there are nopreviously reported studies examining the effect of psychiatricillness or the social risk factors we identifled on adverseevents .The validity of using the Ohio Medicaid administrativedatabase for the diagnosis of atrial fibrillation and the use of
et al.^^ have validated the use of administrative data in thVetera ns Administratio n for the diagnosis of atrial flbrillationThey demonstrated an observed agreement of 0 .98 betweechart review and adminis trat ive data-based algori thms wheonly 1 adm inistrativ e diagnosis wa s required. They report thbest strategy was to require 2 diagnoses over a period of aleast 2 years. In our analysis, we required 2 diagnostic codefor atrial flbrillation as well in an effort to increase the validity
Other studies have documented the reliability of Medicaiadministrative claims data when compared with medical recordiagnoses or experi cha rt review. Walkup et al..^ dem onstratea 100% concord ance rate for both psychiatric diagn oses ansecondary substan ce a bus e d iagnoses in the New York State 'Medicaid Management Information System compared with thmedical record. In a similar study. Lurie et al..^ ' demonstratethat the diagnosis of schizophrenia in Medicaid claims data actually agreed with an expert cha rt review by two psychia trists i87% of patients. In the Maryland Medicaid claims databaseboth the diagnosis and the date of service were shown to be iagreement with the medical record 82% of the time across broad range of patients.^^ Bright et al.,^^ demonstrated thaMedicaid pharmacy claims correspond to medical records 94%of the time, making them quite reliable.
Our stu dy h as several limitations. Prior studie s of atrial fbrillation have generally included fewer women and individualof higher socioeconomic status than in the current study. However, the results of this study are probably applicable to otheMedicaid populations. We are aware of no studies that examinthe validity of warfarin prescriptio ns in adm inistrative data . Amentioned above, while administrative billing data has reasonable reliability, chart review would enhance the accuracy of diagnoses and of warfarin use. There is likely a severity of illnesbias in using ICD-9-CM codes for diagnosing the psychosociarisk factors limiting the generalizability to only those patientwith diagnosed conditions. The results are not adjusted for patient compliance with warfarin use nor for the intensity of anticoagulation thera py be cau se of lack of laboratory r esults. If patient had prior events or conditions not documented duringthe study yea rs, our resu lts would not reflect this information obe adjusted accordingly. However, given the large cohort sizand length of foUow-up, this information is likely to have minimal effects on our conclusions.
While th is s tudy cannot address the quest ion of whetheor not patients with these risk factors should be antlcoagulated . these pat ients have an increased risk of adverse events an dif they are anticoagulated they should be monitored closely toensure that INRs remain with in the therapeutic range. Furthermore, as pat ients with psychiatric i l lness were at an increased risk of both thromboembolic and hemorrhag icomplications, it is reasonable to suspect that their level oancoagulat ion may al ternate between subtherapeutic andsupratherapeutic ranges . Another possib i l i ty is that these patient s are placed at an increase d risk of dru g interacti ons withwarfarin because of addi t ional ant ipsychotic medicat ionleading to fluctuations in the INR altho ugh this study doenot address this. Clearly, further evaluation needs to bperformed in order to determine whether these pat ients beneflt from ancoagulation or are only placed at increased risk oadverse outcomes.In conclusion, our study of Ohio Medicaid patients withnonva lvular atrial flbrillaon receiving warfarin dem ons tra te
-
8/8/2019 GIB 19552402
6/7
JGIM Schauer et al, Psychosocial Risk Fa ctors for Adverse Outcomes 1119negative predictors of warfarin prescribing are also risk factorsfor adverse events in patien ts receiving warfarin. Patients w ithpsychiatric illnesses had an increased risk of both thrombo-embolic and hemorrhagic complications, while substanceabusers and patients with social risk factors for nonadher-ence were at increased risk for hemorrhagic complications.Closer monitoring of these patients during anticoagulation isrequired to ensure the efficacy and safety of warfarin therapy.
This project wos conducted under an interagency agreementwith the University of Cincinnati and the Ohio Department ofJobs an d Famiiy Services through the Ohio Medicaid TechnicoiAssistance Poiicy and Program (MEDTAPP). Resuits and opin-ions expressed do not necessariiy represent the o fficiai views ofthe Ohio Department of Jobs an d Famiiy Services.
R E F E R E N C E S1. Wolf PA, Abbott RD. Kannel WB. Atrial flbrillation as an Independentrisk factor for stroke: the Framingham Study. Stroke. 1991:22:983-8.2. Britton M,Gustafsson C. Non-rheum atic atrial flbrillation as a risk fac-tor for stroke. Stroke. 1985:16:182-8.3. Ezekowitz MD, Bridgers SL, Jam es KE, et al. Warfarin In the preven-tion of stroke associated with nonrheumatic atrial flbrillation. VeteransAffairs Stroke Prevention in Nonrheumatic Atrial Fibrillation Investiga-tors. N Engl J Med. 1992:327:1406-12.4. Stroke Preven tion in Atrial Fibrillation Study. Final results. Circula-tion. 1991:84:527-39.5. Connolly SJ, Laupacis A. Gent M, Roberts RS, Cairns JA, Joyner C.Canadian Atrial Fibrillation Anticoagulation (CAFA) Study. J Am CollCardiol. 1991:18:349-55.6. Petersen P. Boysen G. Godtfredsen J , Andersen ED. Andersen B. Pla-cebo-controlled, randomised trial of warfarin and aspirin for preventionof thromboembolic complications in chronic atrial fibrillation. The Co-
penhage n AFASAK study. Lancet. 1989:1:17 5-9.7. Tbe Bosto n Area Anticoagulation Trial for Atrial Fibrillation Inves-tigators. The effect of low-dose warfarin on the risk of stroke in p atientswith nonrheumatic atrial flbrillation. N Engl J Med. 1990:323:1505-11.8. Hylek EM, Heiman H, Skates SJ. Sheeba n MA. Singer DE, Acetami-nophen and other risk factors for excessive warfarin anticoagulation.JAMA. 1998:279:657-62.9. Landefeld CS. Goldman L. Major bleeding in outpatients treated withwarfarin: incidence and prediction by factors known at the start of out-patient therapy. Am J Med. 1989 :87:144-5 2.10. Landefeld CS. Cook EF, Flatley M, Weisberg M, Goldman L. Identifl-cation and preliminary validation of predictors of major bleeding in hos-pitalized patients starting anticoagulant therapy. Am J Med.1987:82:703-13.11. Landefeld CS, Rosenblatt MW, Goldman L. Bleeding in outpatientstreated with warfarin: relation to the prothrombin time and important
remediable lesions. Am J Med. i989:87:1 53-9.12. Man-Son-Hing M, Laupacis A. Anticoagulant-related bleeding in olderpersons with atrial flbrillation: physicians' fears often unfounded. ArchIntern Med. 2003:163:158 0-6.13. The Stroke Prevention in Atrial Fibrillation Investigators. Bleedingduring antithrombotic therapy in patients with atrial flbrillation. ArchIntern Med. 1996:156:409-16.
14. McMaban DA. Smit h DM, Carey MA. Zhou XH. Risk of major hem orrh-age for outpatients treated with warfarin. J Gen Intern Med. 1998:13:311-6.15. Penning-van Bcest FJ, van Meegen E, Rosendaal FR, Strieker BH.Characteristics of anticoagulant therapy and comorbidity related tooveranticoagulation. Thromb Haemost. 2001:86:569-74.16. Penning-van Becst FJ, Gclcijnse JM, van Meegen E, Vermeer C,Rosendaal FR, Strieker BH. Lifestyle and diet as risk factors for over-anticoagulation. J Clin Epidemiol. 2002:55:411-7.17. Brigden ML, Kay C, LeA, Graydon C, McLeod B. Audit ofthe frequencyand ciinicai response to excessive oral anticoagulation in an out-patientpopulation. Am J Hematol. 1998:59:22-7.18. White RH, Beytb RJ, Zhou H, Romano PS. Major bleeding afterhospitalization for deep-venous th rombo sis. Am J Med. 1999:107:414-24.19. Gitter MJ, Jaeger TM, Petterson TM, Gersh BJ, Silverstcin MD.Bleeding and thromboembolism during anticoagulant therapy: a popu-lation-based study in Rochester, Minnesota. Mayo Clin Proc. 1995:70:725-33.20 . Stafford RS. Singer DE. Recent national patterns of warfarin use inatrial flbrillation. Circulation. 1998:97:1231-3.21 . Go AS, Hylck EM, Borowsky LH, PhiUips KA, Selby JV, Singer DE,Warfarin use among ambulatory patients with nonvalvular atrial fibril-
lation: the anticoagulation and risk factors in atrial flbrillation (ATRIA)study. Ann Intern Med. 1999:131:927-34.22 . Fang MC, Stafford RS, Ruskin JN, Singer DE. National trends in an-tiarrhythmic and antithrombotic medication use in atrial flbrillation.Arch Intern Med. 2004:164:55-60.23 . John ston JA, Cluxton RJ Jr., Heaton PC, Guo JJ, Moomaw CJ, Eck-man MH. Predictors of warfarin u se am ong Ohio medicaid patie nts withnew-onset nonvalvular atrial flbrillation. Arch Intern Med. 2003:163:1705-10.24 . Koroukian SM, Cooper GS, RimmAA. Ability of Medicaid claims d ata toidentify incide nt case s of breas t cance r in the Ohio Medicaid p opulation.Health Serv Res. 2003:38 :947-60.25 . Shireman TI. Olson BM, Dewan NA. Patterns of antidepressantuse among children and ad olescents. Psychiatr Serv. 2002:53:144 4-50.26 . Wang TJ, Massaro JM, Levy D, et al, Ariskscore for predicting stroke ordeath in individuals with new-onset atrial flbrillation in the comm tmity:
the Framingham Heart Study. JAMA. 2003:290:1049-56 .27 . Fihn SD. Callahan CM, M artin DC, MeDonell MB, Henikoff JG, WhiteRH. The risk for and severity of bleeding complications in elderly patie ntstreated with warfarin. The National Consortium of Anticoagulation Clin-ics. Ann Intern Med. 1996:124:970-9.28 . Go AS, Hylek EM, Chang Y, et al. Anticoagulation therapy for strokeprevention in atrial fibrillation: how well do randomized trials tra nslateinto clinical practice? JAMA. 2003:290:2685-92.29 . Borzecki AM, WongAT, Hickey EC, Ash AS, Berlowitz DR. identifyinghypertension-related comorbidities from administrative data: what's theoptimal approach? Am J Med Qual. 200 4:19:201-6.30 . Walkup JT, Boyer CA, Kellermann SL. Reliabiliij- of Medicaid claimsfiles for use in psychiatric diagnoses and service delivery. Admin PolicyMent Health. 2000:27:12 9-39.31 . Lurie N, Popkin M, Dysken M, Moscovice I, Finch M. Accuracy of di-agnoses of schizophrenia in Medicaid claims. Hosp Community Psych-
iatr. 1992:43:69 -71.32 . Steinwachs DM, Stuart ME, Seholle S, Starfield B, Fox MH, WeinerJP. A comparison of ambulatory Medicaid claims to medical records: areliabiliiy assessment. Am J Med Qual. 1998:13:63-9.33 . Bright RA. Avom J, Everitt DE. Medicaid data as a resource i'orepidemiologic studies: strengths and limitations. J Clin Epidemiol.1989:42:937-45.
-
8/8/2019 GIB 19552402
7/7