Percutaneous Trans-Radial Intervention for Acute Thrombosis ......Vascular Medicine Percutaneous...
6
Vascular Medicine Percutaneous Trans-Radial Intervention for Acute Thrombosis of Upper Arm Grafts: An Outpatient-Based, Effective, and Feasible Option Lung-Sheng Wu, 1 Yu-Shen Lin, 1 Chang-Min Chung, 2 Jen-Te Hsu, 2 Shih-Tai Chang, 2 Teng-Yao Yang, 2 Hui-Wen Chen, 2 Chi-Tai Kuo 1 and Pi-Chi Lin 2 Purpose: To evaluate the efficacy, safety, and feasibility of an outpatient-based trans-radial intervention for acute thrombosis of upper arm graft. Materials and methods: A total of 101 trans-radial balloon angioplasty was performed in 63 patients with acute thrombosis of upper arm graft (29 males, 34 females; age: 69 ± 10 years). Thrombus was macerated and pushed into the central circulation with a balloon catheter. Low-dose urokinase injection was given as an adjunctive therapy in 17 interventions. Procedure time, anatomical and clinical success, and complications were analyzed. Results: The procedural time was 56+/-29 minutes. Anatomic success (< 30% residual stenosis) was obtained in 87.2% of cases and clinical success in 79.2%. There was no major bleeding or symptomatic pulmonary embolism. Other complications were distal arterial embolism with or without clinical symptoms in 2% and 5.9% of cases, respectively. The complication rate of axillary extravasations was 3%. Conclusion: Trans-radial intervention for acute thrombosis of upper arm graft as an outpatient procedure had comparable success and complications compared to the results reported earlier. Therefore, outpatient-based trans- radial intervention should be considered a feasible therapy for acute thrombosis of upper arm graft. Key Words: Trans-radial approach · Angioplasty · Hemodialysis access INTRODUCTION Maintaining adequate patency of arterio-venous (AV) access is very important for patients on hemodialysis. AV access often gets occluded and contributes signifi- cantly to morbidity and hospitalization for such pa- tients. 1 Acute occlusion of an AV access in patients on hemodialysis necessitates immediate restoration of pa- tency. The treatment of an AV graft thrombosis has tradi- tionally been surgical, i.e. incision of the graft with Fogarty balloon, thrombectomy and revision as neces- sary. However, percutaneous methods are also an effec- tive alternative to surgical thrombectomy. 1-3 Transve- nous 4-7 or trans-brachial 8 approaches are common tech- niques in endovascular intervention for thrombosed ac- cess. Both trans-brachial and trans-venous approaches (crossed catheter technique) are commonly used to in- crease success rate. 5,9-12 The trans-radial approach is widely used for per- cutaneous coronary intervention because of fewer com- plications related to the puncture site, and early ambula- tion. 13 Recently, it has also been applied for non-coro- nary interventions such as renal artery stenting, mesen- teric artery stenting or cerebral artery stenting. 14-17 How- Acta Cardiol Sin 2008;24:86-91 86 Original Article Acta Cardiol Sin 2008;24:86-91 Received: October 29, 2007 Accepted: January 30, 2008 1 First Cardiovascular Division, Department of Internal Medicine, Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Taipei; 2 Section of Cardiology, Department of Medicine, Chang Gung Memorial Hospital at Chiayi, Chiayi, Taiwan. Address correspondence and reprint requests to: Dr. Pi-Chi Lin, Section of Cardiology, Department of Medicine, Chang Gung Memo- rial Hospital at Chiayi, No. 6, W. Sec., Jiapu Rd., Puzih City, Chiayi County 613, Taiwan. Tel: 886-5-362-1000 ext. 2854; Fax: 886- 5-362-3002; E-mail: [email protected].
Transcript of Percutaneous Trans-Radial Intervention for Acute Thrombosis ......Vascular Medicine Percutaneous...

Vascular Medicine
Percutaneous Trans-Radial Intervention for
Acute Thrombosis of Upper Arm Grafts: An
Outpatient-Based, Effective, and Feasible Option
Lung-Sheng Wu,1 Yu-Shen Lin,1 Chang-Min Chung,2 Jen-Te Hsu,2 Shih-Tai Chang,2
Teng-Yao Yang,2 Hui-Wen Chen,2 Chi-Tai Kuo1 and Pi-Chi Lin2
Purpose: To evaluate the efficacy, safety, and feasibility of an outpatient-based trans-radial intervention for acute
thrombosis of upper arm graft.
Materials and methods: A total of 101 trans-radial balloon angioplasty was performed in 63 patients with acute
thrombosis of upper arm graft (29 males, 34 females; age: 69 � 10 years). Thrombus was macerated and pushed into
the central circulation with a balloon catheter. Low-dose urokinase injection was given as an adjunctive therapy in
17 interventions. Procedure time, anatomical and clinical success, and complications were analyzed.
Results: The procedural time was 56+/-29 minutes. Anatomic success (< 30% residual stenosis) was obtained in
87.2% of cases and clinical success in 79.2%. There was no major bleeding or symptomatic pulmonary embolism.
Other complications were distal arterial embolism with or without clinical symptoms in 2% and 5.9% of cases,
respectively. The complication rate of axillary extravasations was 3%.
Conclusion: Trans-radial intervention for acute thrombosis of upper arm graft as an outpatient procedure had
comparable success and complications compared to the results reported earlier. Therefore, outpatient-based trans-
radial intervention should be considered a feasible therapy for acute thrombosis of upper arm graft.
Key Words: Trans-radial approach � Angioplasty � Hemodialysis access
INTRODUCTION
Maintaining adequate patency of arterio-venous (AV)
access is very important for patients on hemodialysis.
AV access often gets occluded and contributes signifi-
cantly to morbidity and hospitalization for such pa-
tients.1 Acute occlusion of an AV access in patients on
hemodialysis necessitates immediate restoration of pa-
tency. The treatment of an AV graft thrombosis has tradi-
tionally been surgical, i.e. incision of the graft with
Fogarty balloon, thrombectomy and revision as neces-
sary. However, percutaneous methods are also an effec-
tive alternative to surgical thrombectomy.1-3 Transve-
nous4-7 or trans-brachial8 approaches are common tech-
niques in endovascular intervention for thrombosed ac-
cess. Both trans-brachial and trans-venous approaches
(crossed catheter technique) are commonly used to in-
crease success rate.5,9-12
The trans-radial approach is widely used for per-
cutaneous coronary intervention because of fewer com-
plications related to the puncture site, and early ambula-
tion.13 Recently, it has also been applied for non-coro-
nary interventions such as renal artery stenting, mesen-
teric artery stenting or cerebral artery stenting.14-17 How-
Acta Cardiol Sin 2008;24:86�91 86
Original Article Acta Cardiol Sin 2008;24:86�91
Received: October 29, 2007 Accepted: January 30, 20081First Cardiovascular Division, Department of Internal Medicine,
Chang Gung Memorial Hospital, Chang Gung University College of
Medicine, Taipei; 2Section of Cardiology, Department of Medicine,
Chang Gung Memorial Hospital at Chiayi, Chiayi, Taiwan.
Address correspondence and reprint requests to: Dr. Pi-Chi Lin,
Section of Cardiology, Department of Medicine, Chang Gung Memo-
rial Hospital at Chiayi, No. 6, W. Sec., Jiapu Rd., Puzih City, Chiayi
County 613, Taiwan. Tel: 886-5-362-1000 ext. 2854; Fax: 886-
5-362-3002; E-mail: [email protected].

ever, there are very few studies on trans-radial interven-
tion for managing thrombosis of AV access in hemo-
dialysis patients; only two studies related to radio-ce-
phalic fistula18-19 have been reported.
This study was an analysis of a single center’s experi-
ence with endovascular intervention using trans-radial ap-
proach for acute thrombosis of upper arm grafts over a
three-year period. We sought to examine the feasibility, ef-
ficacy and complications of this outpatient-based approach.
METHOD
Patient population
This study was conducted in Chang Gung Memorial
Hospital, Chia Yi, Taiwan. All patients from January
2004 to July 2007 with acute occlusion of upper arm
graft due to thrombosis and normal Allen’s test that were
referred to the interventional cardiology department
were included in this study. They underwent treatment
within 72 hours of no palpable thrill. Grafts with evi-
dence of infection were excluded. All grafts were made
with polytetrafluoroethylene (Gore-Tex; W.L. Core, Elk-
ton, MD). Patients underwent treatment on an outpatient
basis and were hospitalized only if necessary for other
reasons. Written informed consent was obtained from all
patients prior to the procedure.
Interventional procedure
The radial artery was punctured with a 30-mm 20-G
sheathed needle, under local anesthesia (2% lidocaine).
After successful access and free flow of blood, the nee-
dle was removed from the sheath and a 150-cm 0.025-in
angled hydrophilic guidewire (Terumo) was inserted
through the soft sheath. The wire was advanced until se-
cured, then the 20-G soft sheath was removed, leaving
the guidewire in place. A 6-Fr 10-cmsheath (Terumo)
was then introduced into the radial artery. Heparin
(3000IU) was given in all cases in order to prevent intra-
procedural thrombus formation. Midazolam (5 mg) was
administered intravenously for anxiolysis and amnesia as
needed. Nitroglycerin (0.2 mg) was administered intra-
arterially if brachial artery spasm occurred.
A diagnostic fistulogram was conducted through the
sheath. Upon fluoroscopy of a thrombosed upper arm
graft, in most of the cases, only a small stump was visu-
alized. A 6Fr right Judkins 4 (JR4) catheter (Boston Sci-
entific, Maple Grove, MN) was used for better support
to guide the hydrophilic guidewire. If the 0.025-in an-
gled hydrophilic guidewire was unable to pass through
the lesion, a 0.014-in coronary wire with a soft hydro-
philic coating on the tip was employed. After the guide-
wire was passed through the lesion or the entire graft,
the JR4 was withdrawn, and a 6-mm peripheral Wanda
balloon (Boston Scientific Ireland, Galway, Ireland) was
advanced over the wire. The balloon was inflated over
the stump and then withdrawn with the guidewire left in
place. The Wanda balloon was again advanced over the
wire and inflated over the identified lesions under re-
peated imaging. The inflation pressure was increased
gradually until no “waist” remained or the maximal rated
balloon pressure was reached. The balloon catheter size
was 6-7mm � 20 or 40 mm. The balloon was usually in-
flated to 8-16 atmospheres (atm) for 30-40 seconds at a
time. The balloon was inflated for up to 2 minutes as re-
coil was encountered. If the lesion revealed significant
stenosis after initial ballooning, a non-compliant Con-
quest balloon (Bard, Crawley, UK) with a 1:1 balloon-
vessel ratio was employed and inflated to 20-24 atm.
When significant residual thrombus was demonstrated in
the occluded segment, the same Wanda balloon was se-
quentially inflated downstream over the entire graft (6-8
atm) and for a shorter duration of inflation, usually 10- 15
seconds a time. If thrombus was persistent, 60,000~
120,000 U of urokinase was directly injected into the
graft from the peripheral Wanda balloon catheter placed
near the inflow anastomotic area. Contrast medium was
injected 10-15 minutes thereafter to evaluate the effect of
urokinase injection. Finally, the balloon was sequentially
inflated downstream over the entire graft again at a low
pressure of 6-8 atm and for a short duration of inflation to
macerate residual clot or the inflated balloon maintained
at 4-6 atm was used to push the residual clot into the cen-
tral venous system. The declotting procedure was consid-
ered complete when fluoroscopy revealed restored blood
flow and palpable thrill was detected (Figure 1).
At the end of the intervention, the sheath was removed
and the puncture site was manually compressed for approx-
imately 1~2 minutes before compression with gauze and
pressure bandage. The bandage was removed two hours
later. All procedures were performed on an outpatient basis
unless the patient was already admitted to hospital.
87 Acta Cardiol Sin 2008;24:86�91
Trans-Radial PTA for Thrombosed Graft

Study definitions
Procedural time was measured from the start of per-
cutaneous trans-radial puncture to completion of the en-
dovascular procedure. In our laboratory, the procedure
time also includes the time to achieve hemostasis of the
puncture site. Anatomic success for thrombosed lesion
was defined as restoration of flow with less than 30%
maximal residual stenosis. Clinical success was defined
as presence of palpable thrill and the ability to carry out
hemodialysis for at least one week via treated AV graft.
Major complications included symptomatic distal arte-
rial embolization, remote site hematoma or bleeding,
vascular perforation or rupture, death, symptomatic pul-
monary embolism and puncture site complication.33 Mi-
nor complications included additional drug therapy or
short hospital stay for observation.28
RESULTS
From January 2004 to July 2007, 101 interventions
of trans-radial balloon angioplasty were performed in 63
patients with normal Allen test (29 males, 34 females;
age range: 20-90 years; average: 69 � 10 years). The re-
sults of procedural time, anatomical and clinical success,
and complications are shown in Table 1. Anatomic suc-
cess was achieved in 88 of 101 interventions (87.2%).
One intervention failed because of inaccessibility due to
tortuosity of the radial artery. No trans-radial approach
was hindered by unrelievable radial artery spasm. Twelve
interventions failed due to residual stenosis exceeding
Acta Cardiol Sin 2008;24:86�91 88
Lung-Sheng Wu et al.
Table 1.
Intervention N = 101
Procedural time (min) 56+/-29
Anatomic success rate 88/101 (87.2%)
Clinical success rate 80/101 (79.2%)
Major complications
Symptomatic distal arterial embolism 2/101 (2.0%)
Minor complications
Asymptomatic distal arterial embolism 6/101 (5.9%)
Axillary vein focal dissection or extravasation 3/101 (3.0%)
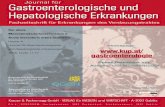
Figure 1. a. This fistulogram was taken trans-radial approach before percutaneous transluminal angioplasty (PTA) and revealed total occlusion
near the ostium of the brachio-axillary graft. b. After the guidewire passed through the thrombosed graft, the first ballooning at the stump of
thrombosed graft was performed. c. Sequential ballooning the entire graft was performed and the figure showed the last ballooning at the graft-ve-
nous junction. d. This fistulogram was taken after the PTA and revealed a successful result.

30% with excessive persistent thrombus. In 9 of the 12
failed interventions, PTA was done more than two days
after onset. In 8 patients re-thrombosis occurred within 7
days of the intervention. All of them had lesions both at
the venous and arterial junctions. Clinical success was
achieved in 79.2% of interventions (80 of 101). Adjunc-
tive therapy with urokinase (Abbokinase; Abbott La-
boratories, North Chicago, IL) at doses ranging from
60,000 U to 120,000 U was used in 17 of 101 interven-
tions at the discretion of the operating physician. The av-
erage procedure time was 56 � 29 minutes.
Complications occurred in 10.5% of procedures.
The major complications were two episodes of distal
embolism in the ulnar artery with pain and coldness. Mi-
nor complication included six episodes of smaller distal
arterial embolism without clinical symptoms, one epi-
sode of axillary vein focal dissection, two episodes of
axillary vein extravasations, and no patient experienced
bleeding complications or clinically detectable pulmo-
nary embolism.
DISCUSSION
Trans-radial percutaneous transluminal angioplasty
with or without urokinase restore the function of throm-
bosed upper arm graft, with acceptable anatomic (87.2%),
clinical (79.2%) success rates. Previous studies related
to salvaging thrombosed AV fistulae or grafts for hemo-
dialysis access, including surgical thrombectomy and
endovascular thrombectomy by various devices coupled
with or without thrombolytic agents, have reported suc-
cess ranging from 71~95%.1,5,7,10,12,21-23 In our series of
patients, the major anatomic failure was resulted from
massive residual thrombus even after performance of
several courses of angioplasty with higher pressure, lar-
ger balloon size, longer inflation time, non-compliant
balloon or low-dose urokinase injection. The potential
factors contributing to the persistence of thrombosis af-
ter PTA include venous limb stenosis,34 clotting disorder,
compromised arterial inflow35 and the age of thrombus.
In 9 of 13 cases with anatomical failure, PTA was done
more than two days after onset. Organization of the rela-
tively old thrombus might hamper effective fragmenta-
tion of the thrombus by PTA. Early intervention after on-
set may increase the success rate. In this study, only one
patient had tortuous radial artery and resulted in a failed
trans-radial intervention.
There were 8 episodes of early re-thrombosis. Hy-
percoaguloability, hypotension, and significant residual
stenosis were the assumed causes of early thrombosis.36
Reviewing the fistulograms of these cases, all of them
had lesions both at the venous and arterial junctions. Re-
coil after PTA at venous junction was noted in three pa-
tients. However, as early recoil occurs commonly in le-
sion at the graft junction, the anatomical locations of
these lesions suggest that recoil after PTA with insuffi-
cient flow may have contributed to the early rethrom-
bosis in these cases. None of them was treated with
low-dose urokinase. However, it was beyond this study
to answer whether routinely using low-dose urokinase
could achieve lower re-thrombosis rate or not.
In some cases with large thrombus burden, inflated
balloons were used at low-pressure status to push the re-
sidual clot to the central venous system after administer-
ing Urokinase injection for 10~15 minutes. We used
lower dose of urokinase (60,000~120,000 U) instead of
the full dose (250,000~500,000 U) as reported in some
reports.11,26 Fifteen out of 17 times, urokinase injection
helped the balloon angioplasty get optimal results. No
bleeding complication occurred in this subgroup of pa-
tients. Low-dose urokinase injection could be an effec-
tive adjunctive therapy in patients with large thrombus
burden. Further study is necessary to prove the benefit-
risk ratio of routine usage of this pharmacological ad-
junctive therapy for all lesions.
The trans-radial approach overcomes several limita-
tions of the traditional approach. First, the lesions can be
clearly visualized by antegrade contrast medium injec-
tion. Second, operators can be protected from exposure
to the X-ray generator throughout the procedure. Third,
one sheath is sufficient to treat all lesions from brachial
artery to the central vein, including thrombosed grafts.
The average procedural time for endovascular ma-
nagement of thrombosed hemodialysis access reported
previously was around 1 hour.5,7,21 In addition, more
than 10 minutes were required to achieve hemostasis in
the traditional approach, and often more if a thrombo-
lytic agent was used. Thus, the average time was more
than 1 hour in the traditional approach5,24 compared to
this study, where it was 56 � 29 minutes, which was in-
clusive of time required for hemostasis. In this study,
89 Acta Cardiol Sin 2008;24:86�91
Trans-Radial PTA for Thrombosed Graft

hemostasis was achieved in less than five minutes, whi-
ch minimized the burden on nursing and medical staff.
The possible complications of the trans-radial ap-
proach include radial artery occlusion, radial artery dis-
section and extravasation. Stella PR reported persistent
radial artery occlusion in less than 3% of patients, and
none had clinical symptoms at the time of trans-radial ar-
tery coronary angioplasty with 6-Fr guiding sheath.25 In
this study, 6-Fr guiding sheath was used in all patients,
and no patient complained of cold sensations or numb-
ness in the hand following the procedure, even those who
underwent several interventions.
The overall complication rates in endovascular ma-
nagement for thrombosed lesions as reported earlier
(4~15%)7,10,31,32 are comparable to our results (10.5% in-
cluding 5.9% asymptomatic arterial embolism). The in-
cidence of occurrence of a peripheral artery embolism
was reported to be as high as 6%.31 In several stud-
ies,3,5,31,32 the reported incidence actually reflected the
incidence of ‘symptomatic’ distal embolism. The sug-
gested threshold (%) of symptomatic distal arterial em-
bolization was 2%.33 Early in our experience, two epi-
sodes of symptomatic distal arterial embolism (2%) oc-
curred during vigorous contrast injection after balloon-
ing the thrombosed stump. Subsequently, these two cases
underwent successful surgical thrombectomy. There were
six episodes of asymptomatic distal arterial embolism.
All were related to smaller thrombus. Additionally, three
complications of the axillary vein were treated with local
compression successfully. Another concern with our
technique (clot maceration without removal) was the
possibility of pulmonary embolism. In this study, no pa-
tient had clinical symptoms of pulmonary embolism,
which was consistent with previous studies.3,28,29
Thus, in all aspects, including success rate, compli-
cations and procedural time, the reported result of this
study are not only equal but better in some ways to the
traditional surgical techniques or those reported by pre-
vious authors.
Limitation of study
This was an observational study and did not com-
pare head-to-head with traditional surgical methods. Pe-
ripheral duplex for radial artery before and after a trans-
radial intervention would had shown a better additional
index of success. This was not done in all patients. Pri-
mary and secondary patency rates or complications could
not be evaluated in this study because not all patients
were regularly followed up in this hospital.
CONCLUSION
This study showed that the success rate, procedural
time and complication rate of trans-radial intervention
for acute thrombosis of upper arm graft were comparable
to those reported in previous studies. This study clearly
demonstrated the overall safety, efficacy and feasibility
of outpatient-based trans-radial intervention for acute
thrombosis of upper arm graft.
REFERENCES
1. NKF-K/DOQI Clinical Practice Guidelines for Vascular Access:
update 2000. Am J Kidney Dis 2001;37:S137-8
2. Cohen MAH, Kumpe DA, Durham JD, et al. Improved treatment
of thrombosed hemodialysis access sites with thrombolysis and
angioplasty. Kidney Int 1994;46:1375-80.
3. Schwartz CI, McBrayer CV, Sloan JH, et al. Thrombosed dialysis
grafts: comparison of treatment with transluminal angioplasty and
surgical revision. Radiology 1995;194:337-41.
4. Beathard GA. Angioplasty for arteriovenous grafts and fistulae.
Semin Nephrol 2002;22:202-10.
5. Trerotola SO, Lund GB, Scheel PJ, et al. Thrombosed dialysis ac-
cess grafts: percutaneous mechanical declotting without uroki-
nase. Radiology 1994;191:721-6.
6. Surowiec SM, Fegley AJ, Tanski WJ, et al. Endovascular man-
agement of central venous stenoses in the hemodialysis patient:
results of percutaneous therapy. Vasc Endovascular Surg 2004;
38:349-54.
7. Overbosch EH, Pattynama PM, Aarts HJ, et al. Occluded hemo-
dialysis shunts: Dutch multicenter experience with the hydrolyser
catheter. Radiology 1996;201:485-8.
8. Manninen HI, Kaukanen ET, Ikaheimo R, et al. Brachial arterial
access: endovascular treatment of failing Brescia-Cimino hemo-
dialysis fistulas: initial success and long-term results. Radiology
2001;218:711-8.
9. Miyayama S, Matsui O, Taki K, et al. Occluded Brescia-cimino
hemodialysis fistulas: endovascular treatment with both brachial
arterial and venous access using the pull-through technique. Car-
diovasc Intervent Radiol 2005;28:806-12.
10. Sahni V, Kaniyur S, Malhotra A, et al. Mechanical thrombectomy
of occluded hemodialysis native fistulas and grafts using a hydro-
dynamic thrombectomy catheter: preliminary experience. Car-
diovasc Intervent Radiol 2005;28:714-21.
Acta Cardiol Sin 2008;24:86�91 90
Lung-Sheng Wu et al.

11. Schon D, Mishler R. Salvage of occluded autologous arteri-
ovenous fistulae. Am J Kidney Dis 2000;36:804-10.
12. Marston WA, Criado E, Jaques PF, et al. Prospective randomized
comparison of surgical versus endovascular management of
thrombosed dialysis access grafts. J Vasc Surg 1997;26:373-80.
13. Kiemeneij F, Laarman GJ, Odekerken D, et al. A randomized
comparison of percutaneous transluminal coronary angioplasty
by the radial, brachial and femoral approaches: the ACCESS
study. J Am Coll Cardiol 1997;29:1269-75.
14. Sharma GL, Louvard Y, Morice MC, et al. Noncoronary trans-
radial angioplasty with coronary equipment: a less invasive tech-
nique. Catheter Cardiovasc Interv 2002;55:197-205.
15. Nohara AM, Kallmes DF. Transradial cerebral angiography: tech-
nique and outcomes. Am J Neuroradiol 2003;24:1247-50.
16. Braunlich S, Ludwig J, Scheinert D. Transradial renal artery
angioplasty and stenting. J Invasive Cardiol 2002;14:147-9.
17. Raghu C, Louvard Y. Transradial approach for percutaneous
transluminal angioplasty and stenting in the treatment of chronic
mesenteric ischemia. Catheter Cardiovasc Interv 2004;61:450-4.
18. Wang HJ, Yang YF. Percutaneous treatment of dysfunctional
Brescia-Cimino fistulae through a radial arterial approach. Am J
Kidney Dis 2006;48:652-8.
19. Kawarada O, Yokoi Y, Nakata S, et al. Transradial intervention
for native fistula failure. Catheter Cardiovasc Interv 2006;68:
513-20.
20. Gray RJ, Sacks D, Martin LG, et al. Society of Interventional Ra-
diology Technology Assessment Committee. Reporting standards
for percutaneous interventions in dialysis access. J Vasc Interv
Radiol 2003;14:S433-42.
21. McCutcheon B, Weatherford D, Maxwell G, et al. A preliminary
investigation of balloon angioplasty versus surgical treatment of
thrombosed dialysis access grafts. Am Surg 2003;69:663-7.
22. Vesely, Thomas M. MD. Management of Thrombosed Dialysis
Grafts. J Vasc Interv Radiol. 1998;9:124-9.
23. Karim Valji, Joseph J. Bookstein, Roberts AC, Davis GB. Phar-
macomechanical thrombolysis and angioplasty in the manage-
ment of clotted hemodialysis grafts: early and late clinical results.
Radiology 1991;178:243-7.
24. Barzel E. Use of a simple compression dressing to obtain hemo-
stasis after pharmacologic thrombolysis of dialysis grafts. J Vasc
Interv Radiol 1999;10:1039-42.
25. Stella PR, Kiemeneij F, Laarman GJ, et al. Incidence and outcome
of radial artery occlusion following transradial artery coronary
angioplasty. Cathet Cardiovasc Diagn 1997;40:156-8.
26. Ponikvar R. Surgical salvage of thrombosed arteriovenous fistu-
las and grafts. Ther Apher Dial 2005;9:245-9.
27. Duszak R Jr, Sacks D. Dialysis graft declotting with very low
dose urokinase: Is it feasible to use “less and wait?” J Vasc Interv
Radiol 1999;10:123-8.
28. Aruny JE, Lewis CA, Cardella JF, et al. Society of Interventional
Radiology Standards of Practice Committee. Quality improve-
ment guidelines for percutaneous management of the thrombosed
or dysfunctional dialysis access. J Vasc Interv Radiol 2003;14:
S247-5.
29. Zeit RM. Arterial and venous embolization: declotting of dialysis
shunts by direct injection of streptokinase. Radiology 1986;159:
639-41.
30. Davis GB, Dowd CF, Bookstein JJ, et al. Thrombosed dialysis
grafts: efficacy of intrathrombic deposition of concentrated
urokinase, clot maceration, and angioplasty. AJR 1987;149:
177-81.
31. Lazzaro CR, Trerotola SO, Shah H, et al. Modified use of the
arrow-trerotola percutaneous thrombolytic device for the treat-
ment of thrombosed hemodialysis acess grafts. J Vasc Interv
Radiol 1999;10:1025-31.
32. Smits HF, Smits JH, Wust AF, et al. Percutaneous thrombolysis of
thrombosed hemodialysis grafts: comparison of three mechanical
devices. Nephrol Dial Transplant 2002;17:467-73.
33. Aruny JE, Lewis CA, Cardella JF, et al. Quality improvement
guidelines for percutaneous management of thrombosed or dys-
functional Dialysis Access. J Vasc Interv Radiol 2003;14:
S247-53.
34. Schwab S, Raymond J, Safed M, et al. Prevention of hemodialysis
fistula thrombosis: Early detection of venous stenoses. Kidney Int
1989;36:707-11.
35. Vorwerk D, Schurmann K, Muller-Leisse C, et al. Hydrodynemic
thrombectomy of hemodialysis grafts and fistulae: Results of 51
procedures. Nephrol Dial Transplant 1996;11:1058-64.
36. Patrick Haage, Dierk Vorerk, Joachim E, et al. Percutaneous
treatment of thrombosed primary arteriovenous hemodialyis ac-
cess fistulae. Kidney Interventional 2000;57:1169-75.
91 Acta Cardiol Sin 2008;24:86�91
Trans-Radial PTA for Thrombosed Graft