
Prähabilitation vor großen Operationen - dgem.de · Prähabilitation vor großen Operationen Ines...
53
Prähabilitation vor großen Operationen Ines Gockel Klinik und Poliklinik für Viszeral-, Transplantations-, Thorax- und Gefäßchirurgie DGEM – 22. Leipziger Fortbildungsveranstaltung: Ernährung und Bewegung in besonderen Krankheitssituationen 23.11.2018, Schloss Machern
Transcript of Prähabilitation vor großen Operationen - dgem.de · Prähabilitation vor großen Operationen Ines...

Prähabilitation vor großen Operationen
Ines Gockel
Klinik und Poliklinik für Viszeral-, Transplantations-, Thorax- und Gefäßchirurgie
DGEM – 22. Leipziger Fortbildungsveranstaltung: Ernährung und Bewegung in besonderen Krankheitssituationen
23.11.2018, Schloss Machern

Prähabilitation
„Functional Recovery“ entscheidend für das postoperative Ergebnis!
2
Pfirrmann D, Weimann A, Simon P, Gockel I, et al. Chirurg 2018
prä-OP post-OP
PRÄHAB ERAS
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Publikationen Prähabilitation (PubMed)
Entwicklung 2000-2017
3
Pfirrmann D, Weimann A, Simon P, Gockel I, et al. Chirurg 2018
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Risiko-Assessment & Prähabilitation
Morbidität &
Mortalität
chirur-gisches
Team
anästhesio-logisches
Team
Patienten-Performance
Status
Ausmaß chirurg.
Invasivität
4
Haga Y, et al. Surg Today 1999
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
-> Re-Allokation von Ressourcen

PRÄHAB vs. ERAS?
Der „High-Risk“-Patient
5
+ = ??
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Präkonditionierung
6
-> Kulturwandel
Carli F et al., Acta Oncologica 2017
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Gesamtkonzept – multimodale Prähabilitation
Optimierung der
funktionellen postoperativen
Resultate
körperliche Bewegung
Ernährung (Proteine!)
Rauch- Entwöh-
nung
psycholog. Angstre-duktion
Compliance-
Steigerung
gezieltes Atemtrai-
ning
7 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Evidenz Prähabilitation
8
Pfirrmann D, Weimann A, Simon P, Gockel I, et al. Chirurg 2018
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Interventionsgestaltung
9
Pfirrmann D, Weimann A, Simon P, Gockel I, et al. Chirurg 2018
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Präoperatives Work-up
kardiovaskuläre Anamnese, Nikotin, COPD-Evaluation
präoperatives funktionelles Work-up: FEV1 = Standard
Low technology-Belastungstest (z.B. Shuttle Walk-Test oder „Treppenstufen“-Test): Screening für pulmonale Risikopatienten
Kardiopulmonaler Belastungstest bei schlechten Resultaten des Screeings
maximaler O2-Verbrauch (VO2max) mit Werten < 10ml/kg/min bzw. 35%: hohes kardiopulm. Risiko, Mortalität
10
Brunelli A, J Thorac Dis 2016 Brunelli A et al., Chest 2013
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Optimierung des nutritiven Status vor OP
Proteine im Fokus!
„Post-Excercise“: stimulatorischer Effekt der Aminosäuren verstärkt
Protein-Einnahme nach Krafttraining stimuliert die myofibrilläre Protein-Synthese (Atemhilfsmuskulatur!)
Beispiel standardisierte Protein-Nahrung prä-OP:
11
Wolfe RR, Am J Clin Nutrit 2006 Biolo G et al., Am J Physiol 1997
Moore DR et al., J Physiol 2009 Carli F et al., Acta Oncologica 2017
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
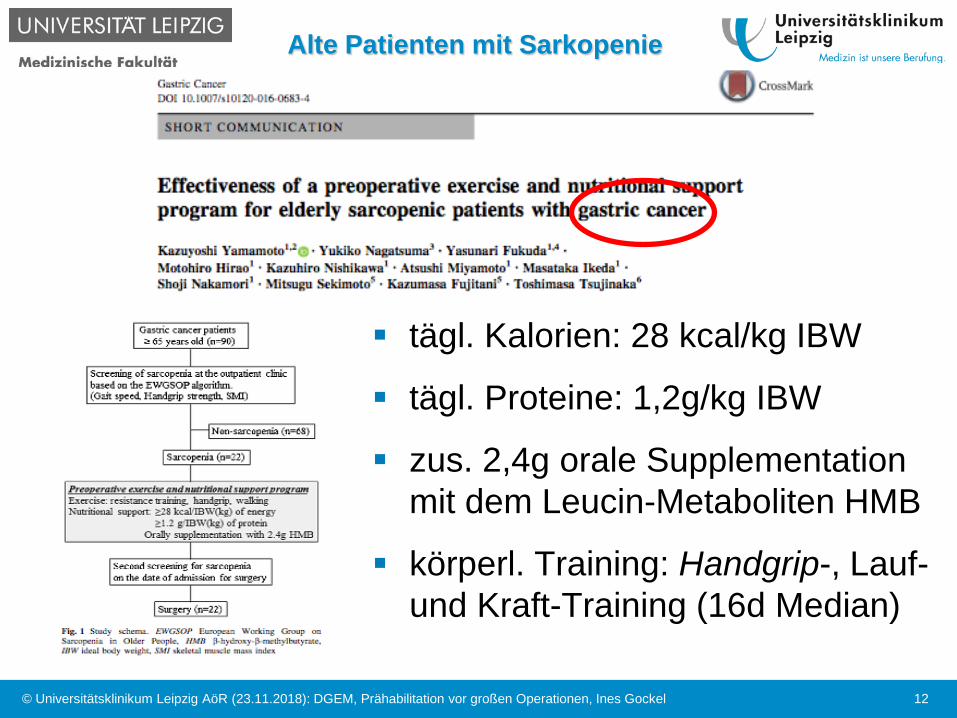
Alte Patienten mit Sarkopenie
12
tägl. Kalorien: 28 kcal/kg IBW
tägl. Proteine: 1,2g/kg IBW
zus. 2,4g orale Supplementation mit dem Leucin-Metaboliten HMB
körperl. Training: Handgrip-, Lauf- und Kraft-Training (16d Median)
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Körperliches Training / Atemtraining vor OP
Welche Dosisintensität?
Wie lange?
Wie oft?
Modalität, z.B. Intervalle / Intensitätssteigerung?
Ausdauer- vs. Krafttraining? Welches Atemtraining?
Simultane neoadjuvante (Radio-) Chemotherapie!
limitiertes Zeitintervall bis zur OP!
Balance = keine Überforderung des onkolog. Patienten
Training individuell an das „Fitness-Niveau“ angepasst
13 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

PET: Ergebnisse aus der Thoraxchirurgie (SR)
PET = Preoperative Excercise Training
moderates – intensives Training hat positive Effekte auf die aerobe Kapazität, körperliche Fitness und die Lebensqualität
Reduktion postoperativer Komplikationen und des stationären Aufenthalts
Allerdings: heterogene Programme & Intensität / Dauer, AT und Outcome-Parameter; keine Angaben, ob Rauchentwöhnung obligat & erfolgreich
14
Pouwels S, Respir Med 2015
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Ambulantes / häusliches Training: vor Thoraxchirurgie
15
Coats V et al., Can Respir J 2013
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Veränderungen der funktionellen Kapazität perioperativ
6MWD = six-minutes walk distance
16
Minnella EM et al., Acta Oncologica 2017
n=185 Pat. mit onkologischer kolorektaler Chirurgie
-> keine Unterschiede hinsichtlich des postoperativen stationären
Aufenthalts bzw. der Komplikationen
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
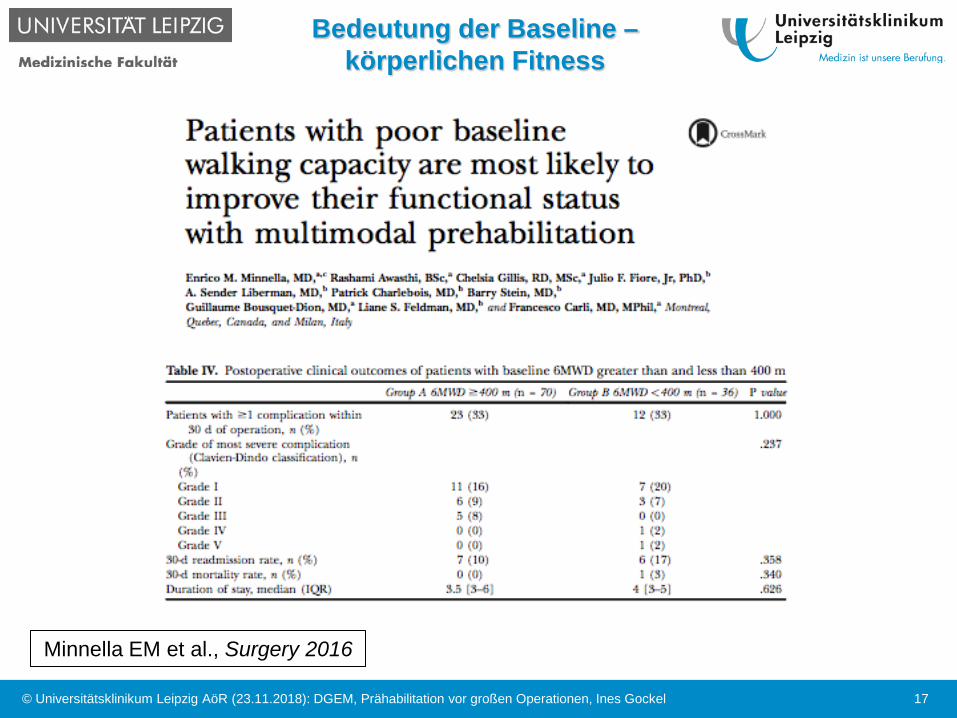
Bedeutung der Baseline – körperlichen Fitness
17
Minnella EM et al., Surgery 2016
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
Cave: Compliance!
RCT n=112 Pat. mit kolorektaler Chirurgie
Home-based-Programm: Sham Intervention (Kontroll-Gruppe mit Basis-Empfehlungen) vs. hoch-intensives Trainingsprogramm (Aerobic- und Krafttraining)
Kontrollgruppe signifikant besser, da Complicance nur 16% in der Interventionsgruppe!
-> alleinige Verordnung eines intensiven Trainingsprogramms nicht ausreichend! -> immer professionelles Monitoring, Erfolgskontrollen und weitere Faktoren der multimodalen Prähabilitation, wie Ernährungsprogramme etc. erforderlich!
18
Carli F et al., Br J Surg 2010
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Effekt des präoperativen inspiratorischen Muskeltrainings (SR)
Signifikante Reduktion postoperativer pulmonaler Komplikationen (nach abdominellen und herzchirurgischen OPs)
19
Valkenet K et al., Clin Rehabilitation 2011
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Beispiel: Ösophaguschirurgie - Zweihöhleneingriff
20
Gockel I et al., J Thorac Dis 2017
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

21
abdo
min
ell
thor
akal
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Risikofaktoren: SCC vs. ADC
22
Hongo M et al., J Gastroenterol Hepatol 2009
Risikofaktoren SCC ADC Nikotinkonsum +++ ++ Alkoholkonsum ++ ++ Barrett-Ösophagus n.s. +++ GERD-Symptome n.s. +++ Adipositas n.s. ++ Exzessiver Fettkonsum n.s. ++ Armut ++ n.s. niedriger Bildungsstand + n.s. Exzessive Zufuhr heißer Getränke (thermischer Schaden)
+ n.s.
H. pylori-Infektion protektiv protektiv
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Zylinderepithel infolge GERD
Plattenepithel
Karzinom
Barrett-Karzinom Norman Barrett (1903-1979)
23 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
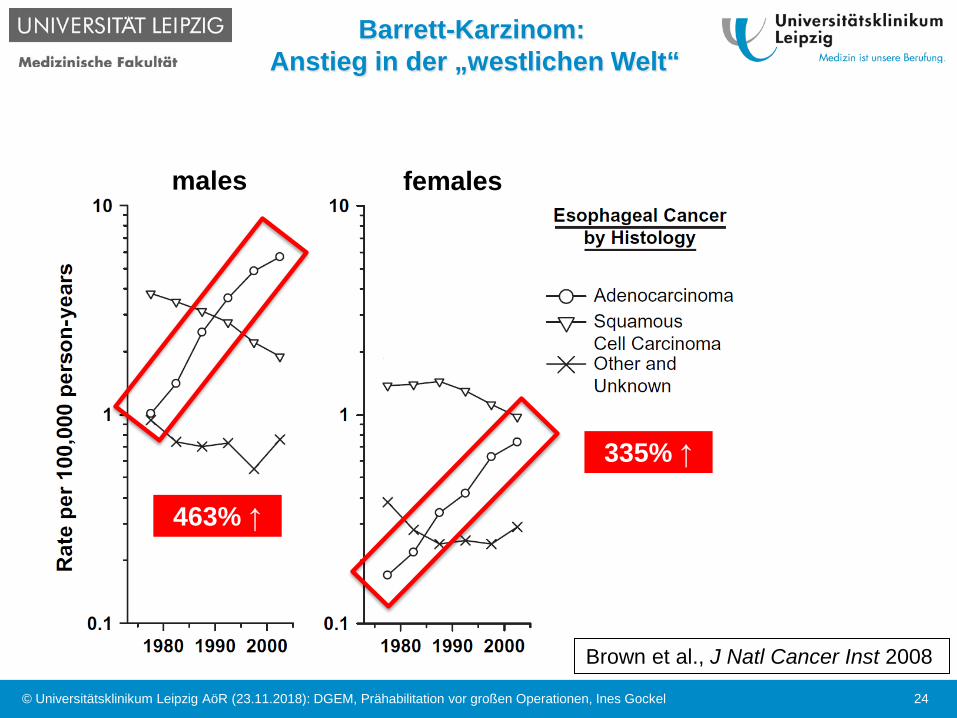
Brown et al., J Natl Cancer Inst 2008
463% ↑
335% ↑
Barrett-Karzinom: Anstieg in der „westlichen Welt“
males females
24 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
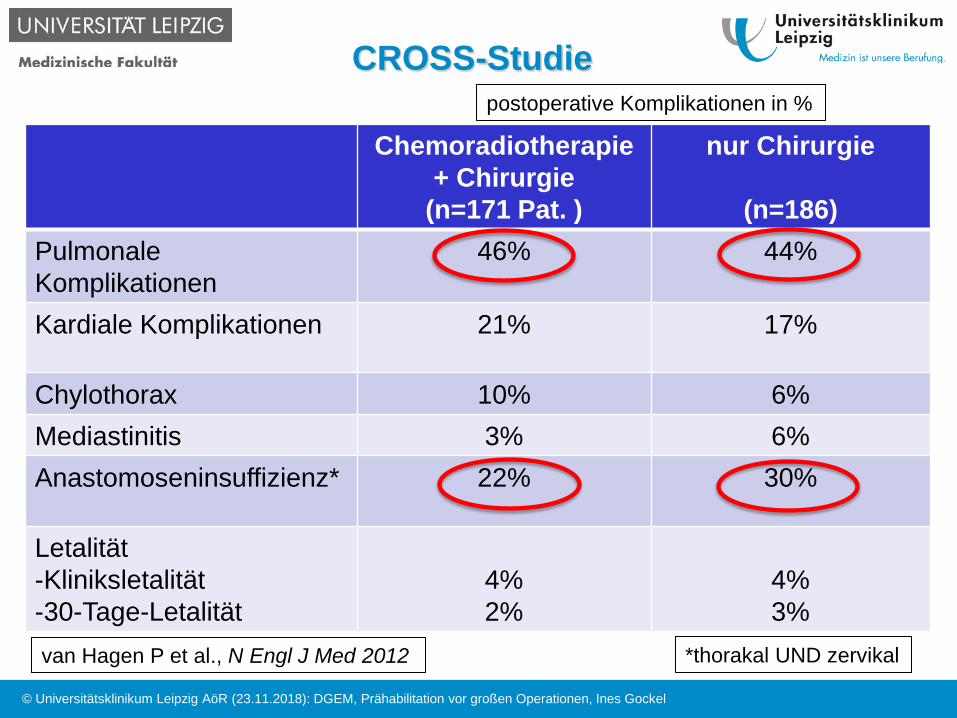
CROSS-Studie
Chemoradiotherapie + Chirurgie
(n=171 Pat. )
nur Chirurgie
(n=186) Pulmonale Komplikationen
46% 44%
Kardiale Komplikationen 21% 17%
Chylothorax 10% 6% Mediastinitis 3% 6% Anastomoseninsuffizienz* 22% 30%
Letalität -Kliniksletalität -30-Tage-Letalität
4% 2%
4% 3%
postoperative Komplikationen in %
van Hagen P et al., N Engl J Med 2012 *thorakal UND zervikal
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
Pulmonale Komplikationen nach Ösophagektomie
25-70% (unterschiedliche Definitionen!): Pneumonie, Atelektasen, Dystelektasen, Pleuraerguss, -empyem, ARDS, etc.
neoadjuvante (Radio-) Chemotherapie kann die Lungenfunktion weiter verschlechtern = strukturelle Lungenveränderungen – Re-Assessment !
26
Rivera MP et al., Chest 2009
Leo F et al., Ann Thorac Surg 2004
-> zusätzlicher Risikofaktor für postoperative respiratorische Komplikationen!
Takeda S et al., Ann Thorac Surg 2006
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

thorakale Anastomoseninsuffizienz nach Ösophagektomie (ca. 6-30%)
Sepsis MOV
- Mediastinitis - Pleuraempyem - tracheobronchiale Läsion - septische Arrosionsblutung
Bartels H, Siewert JR. Chirurg 2008
-> Letalität bis 80%
Anastomoseninsiffuizienz nach Ösophagektomie
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Studienprotokoll Ösophaguschirurgie
Präoperatives inspiratorisches Muskeltraining
28
Valkenet K et al., Trials 2014
Ziel: n=248 Pat. mit Ösophagusresektion bei Karzinom; 30 Zyklen AT, 2x pro Tag bis zur OP über mind. 2 Wochen vs. Kontrolle (TAU);
Endpunkte: Pneumonieraten, post-OP LUFU, ICU, LOS
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

PREPARE-Study
Studiendesign
29
Valkenet K et al., Trials 2014
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Eigenes Studienkonzept
Internet-based Perioperative Exercise Program
iPEP – Study
30
-Pat. mit neoadjuvanter Therapie bei AEG Typ I-II
-Training über Online-Platform
-Kombination aus Ausdauer-, Kraft- und intensivem Atemtraining
-initialer Leistungstest (V02max + Laktatmessung) sowie individuelle
Trainingspläne (wöchentlich aktualisiert) über Sportwissenschaftler
-RCT, multizentrisch, D
Trial registration: NCT02478996
Pfirrmann D, ...Simon P, Gockel I, BMC Cancer 2017
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

iPEP-Study
31 31
Baseline
Web-based program
Pre-surgery phase
iProgram Social Community
Clinical examination Cognitive Testing
Questionnaires, QoL
Cardiology
Lung function
Spiroergometry NRS, BMI
Intervention endpoint
8-12 weeks surgery
Treatment as usual (TAU)
Web-based program
Post-surgery phase 12 weeks
iProgram Social Community
Clinical examination Cognitive Testing
Questionnaires, QoL
Cardiology
Lung function
Spiroergometry NRS, BMI
R
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
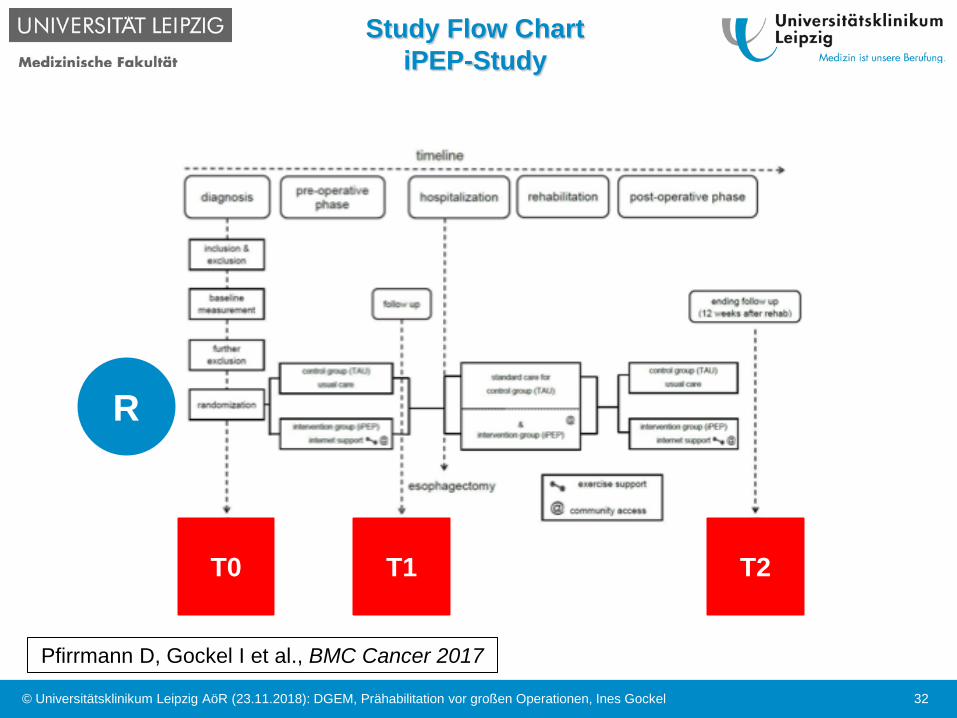
Study Flow Chart iPEP-Study
32
R
T0 T1 T2
Pfirrmann D, Gockel I et al., BMC Cancer 2017
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Primärer Endpunkt: Änderung max. O2-Verbrauch (VO2max)
33
VO2max
Spiroergometrie
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Modifizierte Borg-Scale
34
Borg-Scale = Level der subjektiven Erschöpfung nach dem Trainingsprogramm
Borg G, Scand J Rehabil Med 1970
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Sekundäre Endpunkte
Change in Forced Expiratory Volume in 1 second (FEV1) directly prior to surgery and at 12 weeks after surgery
Change in Forced Vital Capacity (FVC) directly prior to surgery and at 12 weeks after surgery
35 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Tertiäre Endpunkte
Pneumonia within 12 weeks after surgery
Anastomotic insufficiency within 12 weeks after surgery (according to Veeramootoo et al.), duration of mechanical ventilation, re-intubation rate, length of intensive care unit stay, postoperative in-hospital stay, feasibility of the internet-based exercise program, quality of life as assessed with the EORTC (European Organization for Research and Treatment of Cancer), QoLQ-C30 questionnaire with the esophagus-specific module OES-18, and social support of disease coping by means of the modified Berlin Social Support Scale
36 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
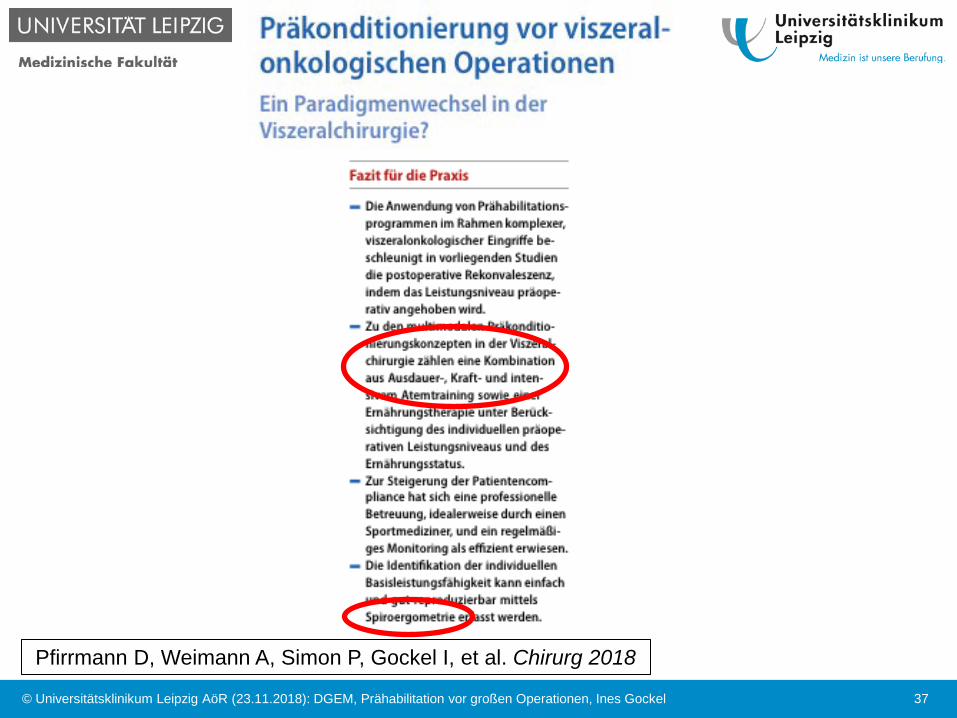
37
Pfirrmann D, Weimann A, Simon P, Gockel I, et al. Chirurg 2018
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
Fazit Prähabilitation vor großen Operationen
Nicht nur der „Risikopatient“, sondern JEDER Pat. vor großen Operationen, sollte präkonditioniert werden, um postoperative Komplikationen zu reduzieren
Multimodales Prähabilitationskonzept
Zeit der neoadjuvanten Therapie nutzen!
38 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Weiterer Faktor: Volumen-Outcome-Effekt
39 © Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

40
Vielen Dank für Ihre Aufmerksamkeit
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Mindestmengen – ein weiterer Beitrag zur Patientensicherheit!?
41
Nimptsch U et al., Gesundheitswesen 2016
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

Mindestmengenregelungen (MM) aktuell
Lebertransplantation (MM: 20)
Nierentransplantation (MM: 25)
Komplexe Eingriffe am Organsystem Ösophagus (MM: 10)
Komplexe Eingriffe am Organsystem Pankreas (MM: 10)
Kniegelenk-Totalendoprothesen (MM: 50)
Stammzelltransplantation (MM: 25)
Versorgung von Früh- und Neugeborenen (seit 2010)
42
§ 137 Abs. 3 Satz 1 Nr. 2 SGB V für nach § 108 SGB V zugelassene Krankenhäuser
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel
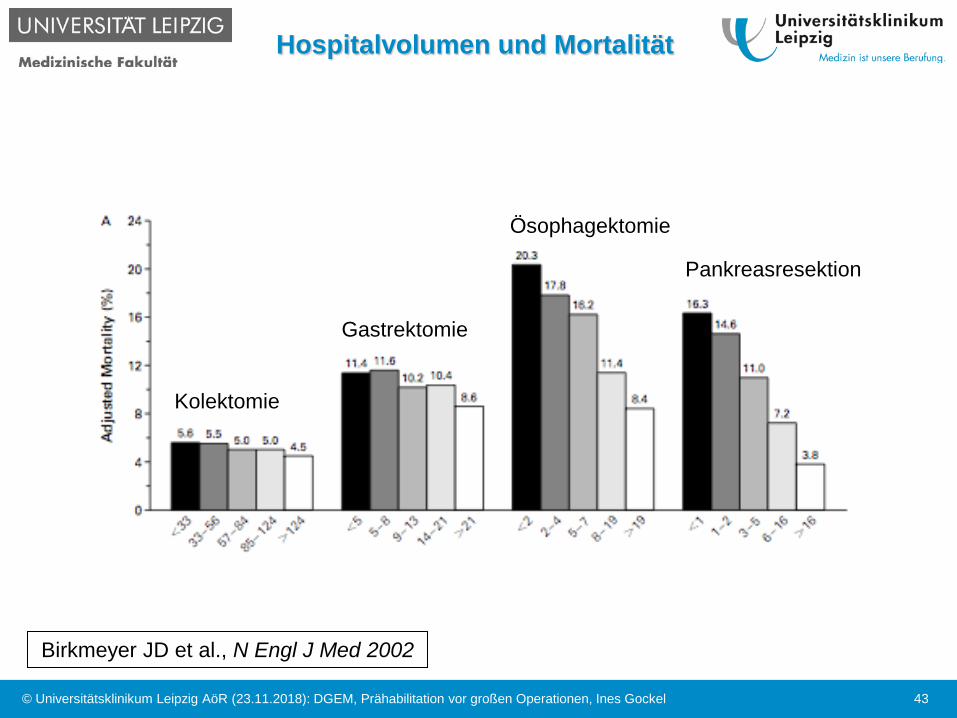
Hospitalvolumen und Mortalität
43
Birkmeyer JD et al., N Engl J Med 2002
Kolektomie
Gastrektomie
Ösophagektomie
Pankreasresektion
© Universitätsklinikum Leipzig AöR (23.11.2018): DGEM, Prähabilitation vor großen Operationen, Ines Gockel

„Failure to rescue“
44
Klinikvolumen – Mortalität – „Failure to rescue“ für 3 onkologische Hochrisiko-Operationen kombiniert*
Ghaferi AA, Birkmeyer JD et al., Med Care 2011
*Gastrektomie, Ösophagektomie und
Pankreasresektion
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel
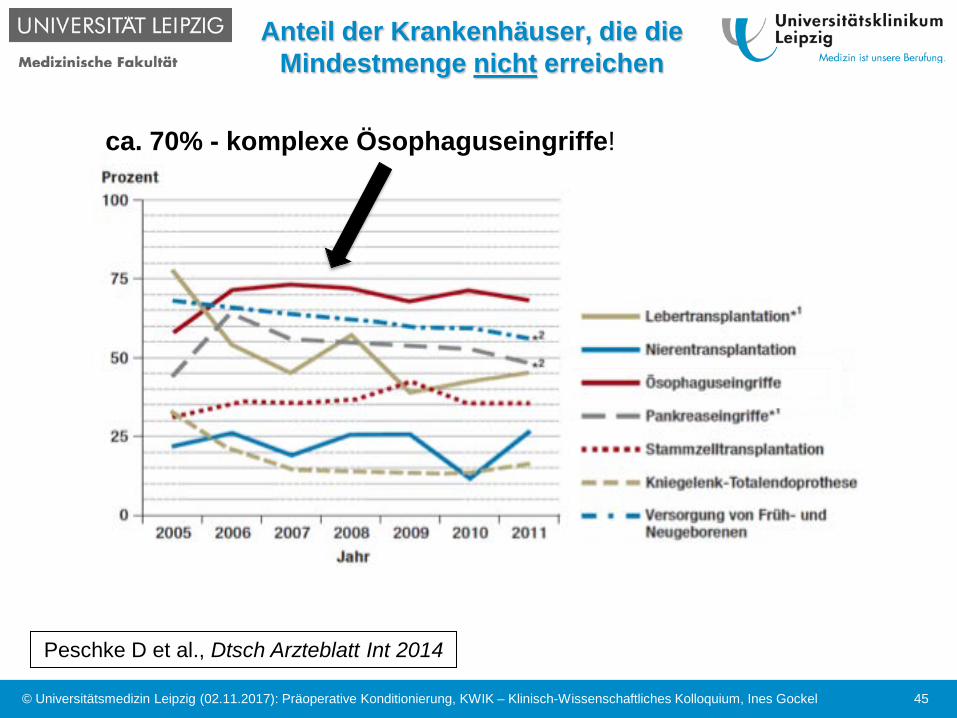
45
ca. 70% - komplexe Ösophaguseingriffe!
Peschke D et al., Dtsch Arzteblatt Int 2014
Anteil der Krankenhäuser, die die Mindestmenge nicht erreichen
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

FAZ, Sept. 2015
46 © Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel
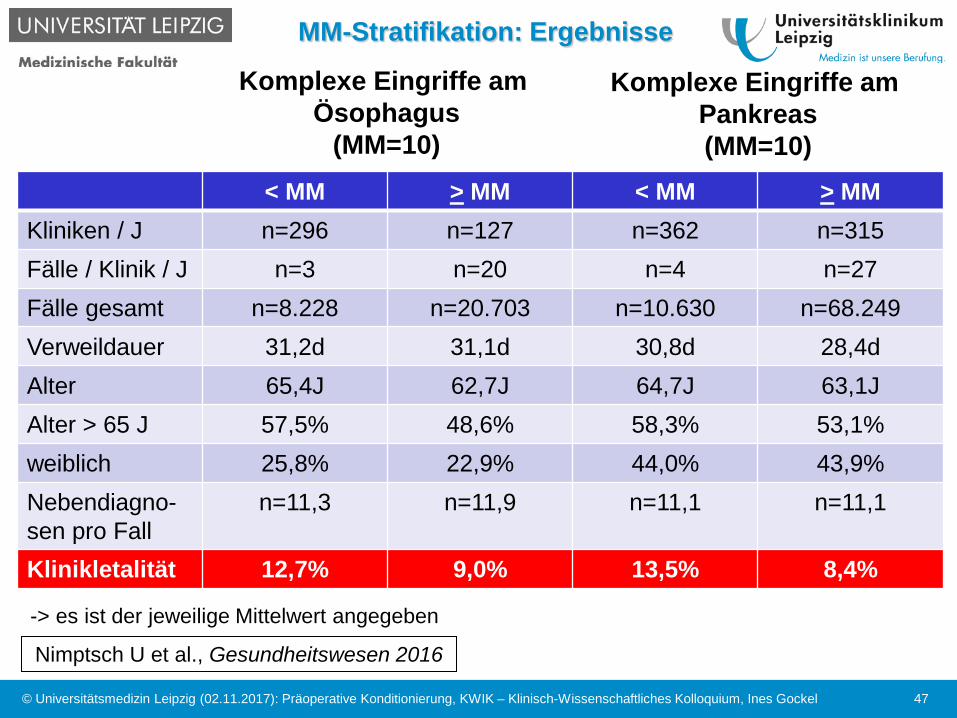
< MM > MM < MM > MM Kliniken / J n=296 n=127 n=362 n=315 Fälle / Klinik / J n=3 n=20 n=4 n=27 Fälle gesamt n=8.228 n=20.703 n=10.630 n=68.249 Verweildauer 31,2d 31,1d 30,8d 28,4d Alter 65,4J 62,7J 64,7J 63,1J Alter > 65 J 57,5% 48,6% 58,3% 53,1% weiblich 25,8% 22,9% 44,0% 43,9% Nebendiagno-sen pro Fall
n=11,3 n=11,9 n=11,1 n=11,1
Klinikletalität 12,7% 9,0% 13,5% 8,4%
47
-> es ist der jeweilige Mittelwert angegeben
Nimptsch U et al., Gesundheitswesen 2016
Komplexe Eingriffe am Ösophagus
(MM=10)
Komplexe Eingriffe am Pankreas (MM=10)
MM-Stratifikation: Ergebnisse
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

Elektive komplexe Viszeralchirurgie - Klinikletalität
© Universitätsmedizin Leipzig (2017): präoperative Konditionierung beim Ösophaguskarzinom, Ines Gockel, 23.03.2017 48
Nimptsch U, Mansky T, BMJ 2017
komplexe große Ösophaguschirurgie bei Karzinom (n=18.208 Pat. )
Pankreasresektion bei Karzinom (n=34.555 Pat. )
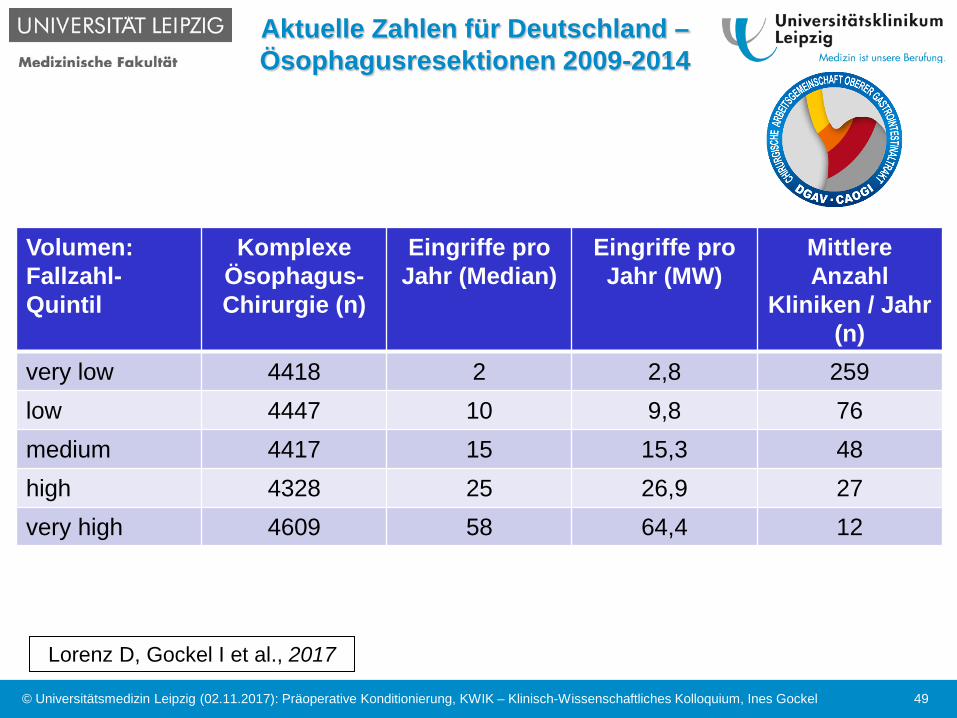
Aktuelle Zahlen für Deutschland – Ösophagusresektionen 2009-2014
Volumen: Fallzahl-Quintil
Komplexe Ösophagus-Chirurgie (n)
Eingriffe pro Jahr (Median)
Eingriffe pro Jahr (MW)
Mittlere Anzahl
Kliniken / Jahr (n)
very low 4418 2 2,8 259 low 4447 10 9,8 76 medium 4417 15 15,3 48 high 4328 25 26,9 27 very high 4609 58 64,4 12
49
Lorenz D, Gockel I et al., 2017
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

Aktuelle Zahlen für Deutschland – Ösophagusresektionen 2009-2014
50
Lorenz D, Gockel I et al., 2017
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

Mindestmengenregelung – besseres Outcome, zusätzlich zur
Präkonditionierung?
Komplexe Eingriffe benötigen eine hohe Strukturqualität, die sich nur durch das ständige Training ALLER erreichen lässt
Bei diesen Eingriffen ist eine Fallzahl – Behandlungsergebnis – Beziehung (Ergebnisqualität) wissenschaftlich belegt
Diese geht mit einer erhöhten Patientensicherheit (reduzierte Klinikletalität) einher
Allerdings.....sind bisher keine wissenschaftlich belastbaren Absolutzahlen der Mindestmengengrenzen (je Zentrum / je Operateur) definiert, ab n=50 Pat. / Jahr ist die Qualität gut
51 © Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

52
Vielen Dank für Ihre Aufmerksamkeit
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel

Literatur Präkonditionierung
53
Benzo R, Wigle D, Novotny P, et al. Lung Cancer. 2011 Dec;74(3):441-5.
Burgio KL, Goode PS, Urban DA, et al. J Urol. 2006 Jan;175(1):196-201.
Burke SM, Brunet J, Sabiston CM, et al. Support Care Cancer. 2013 Dec;21(12):3345-53.
Carli F, Charlebois P, Stein B, et al. Br J Surg. 2010 Aug;97(8):1187-97.
Cho H, Yoshikawa T, Oba MS, et al. Ann Surg Oncol. 2014 Jun;21(6):2044-50.
Coats V, Maltais F, Simard S, et al. Can Respir J.2013 Mar-Apr;20(2):e10-6.
Dettling DS, Van der Schaaf M, Blom RL, et al. Physiother Res Int. 2013 Mar;18(1):16-26.
Divisi D, Di Francesco C, Di Leonardo G, et al. Eur J Cardiothorac Surg. 2013 Feb;43(2):293-6.
Gillis C, Li C, Lee L, et al. Anesthesiology. 2014 Nov;121(5):937-47.
Jones LW, Peddle CJ, Eves ND, et al. Cancer. 2007 Aug 1;110(3):590-8.
Kaibori M, Ishizaki M, Matsui K, et al. BMC Gastroenterology 2013, 13:119
Kasikcioglua E, Toker A, Tanjub S, et al. Lung Cancer 66 (2009) 85-88.
Li C, Carli F, Charlebois P, et al. Surg Endosc. 2013 Apr;27(4):1072-82.
Moyes L, McCaffer C, Carter R, et al. Ann R Coll Surg Engl 2013; 95: 125-130.
Older P & Hall, A Critical Care 2004, 8:369-372.
Patel MI, Yao J, Hirschhorn AD, et al. Int J Urol.2013 Oct;20(10):986-92.
Pehlivan E, Turna A, Gurses A, et al. Ann Thorac Cardiovasc Surg. 2011;17(5):461-8.
Van Adrichem EJ, Meulenbroek RL, Plukker JT et al. Ann Surg Oncol. 2014 Jul;21(7):2353-60.
West MA, Loughney L, Lythgoe D, et al. Br J Anaesth. 2015 Feb;114(2):244-51.
© Universitätsmedizin Leipzig (02.11.2017): Präoperative Konditionierung, KWIK – Klinisch-Wissenschaftliches Kolloquium, Ines Gockel







![Datenbankanfragen und -operationen mittels SQLsobe/InfoMB_Jg13/Vo/3_Datenbanken_… · SQL-Operationen: Projektion und Selektion SELECT merkmale FROM tabelle [WHERE bedingung] Projektion](https://static.fdokument.com/doc/165x107/5b16f49e7f8b9a4e6b8b8bea/datenbankanfragen-und-operationen-mittels-sql-sobeinfombjg13vo3datenbanken.jpg)






