Sarkome und Lymphomerkrankungen des Kindes – Welche ... · 11. Bremer MR-Symposium - 02. bis 04 ....
90
11. Bremer MR-Symposium - 02. bis 04 . Oktober 2015 Sarkome und Lymphomerkrankungen des Kindes – Welche Schlüsselinformationen aus der Bildgebung benötigt der Kinderonkologe? Heribert Jürgens
Transcript of Sarkome und Lymphomerkrankungen des Kindes – Welche ... · 11. Bremer MR-Symposium - 02. bis 04 ....
11. Bremer MR-Symposium - 02. bis 04 . Oktober 2015
Sarkome und Lymphomerkrankungen des Kindes – Welche Schlüsselinformationen aus der Bildgebung benötigt der Kinderonkologe? Heribert Jürgens
2
3
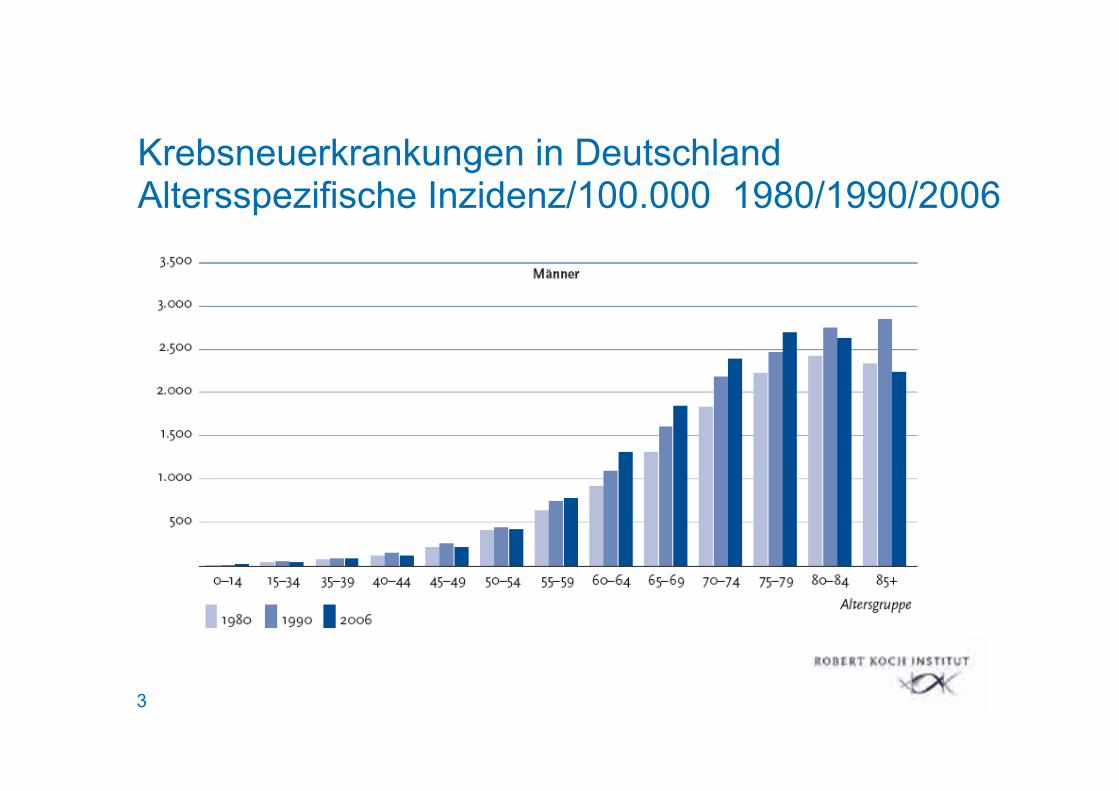
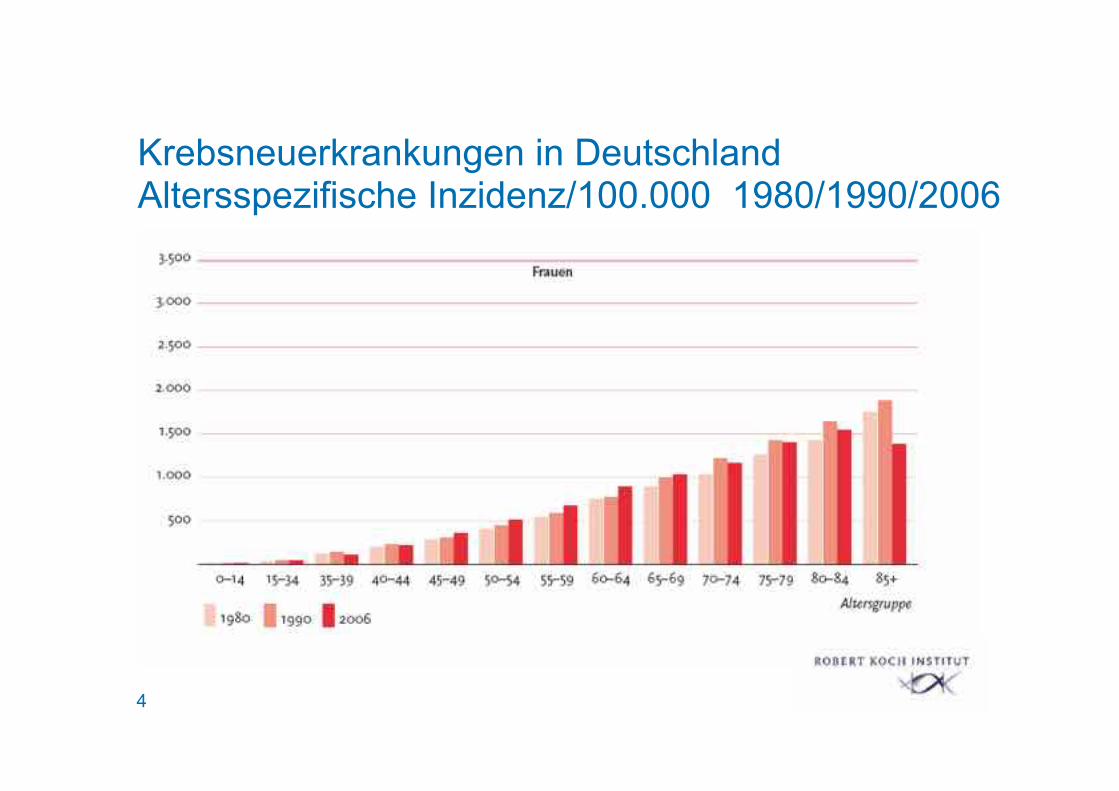
Krebsneuerkrankungen in Deutschland Altersspezifische Inzidenz/100.000 1980/1990/2006
4
Krebsneuerkrankungen in Deutschland Altersspezifische Inzidenz/100.000 1980/1990/2006
5
Krebs bei Kindern und Jugendlichen Inzidenz
~ 14 / 100.000 Kinder <15 J pro Jahr
~ 1800 Patienten <15 J pro Jahr in Deutschland
~ 2000 Patienten <18 J pro Jahr in Deutschland
≅ 25 Neuerkrankungen pro 1 Mio Einwohner
6
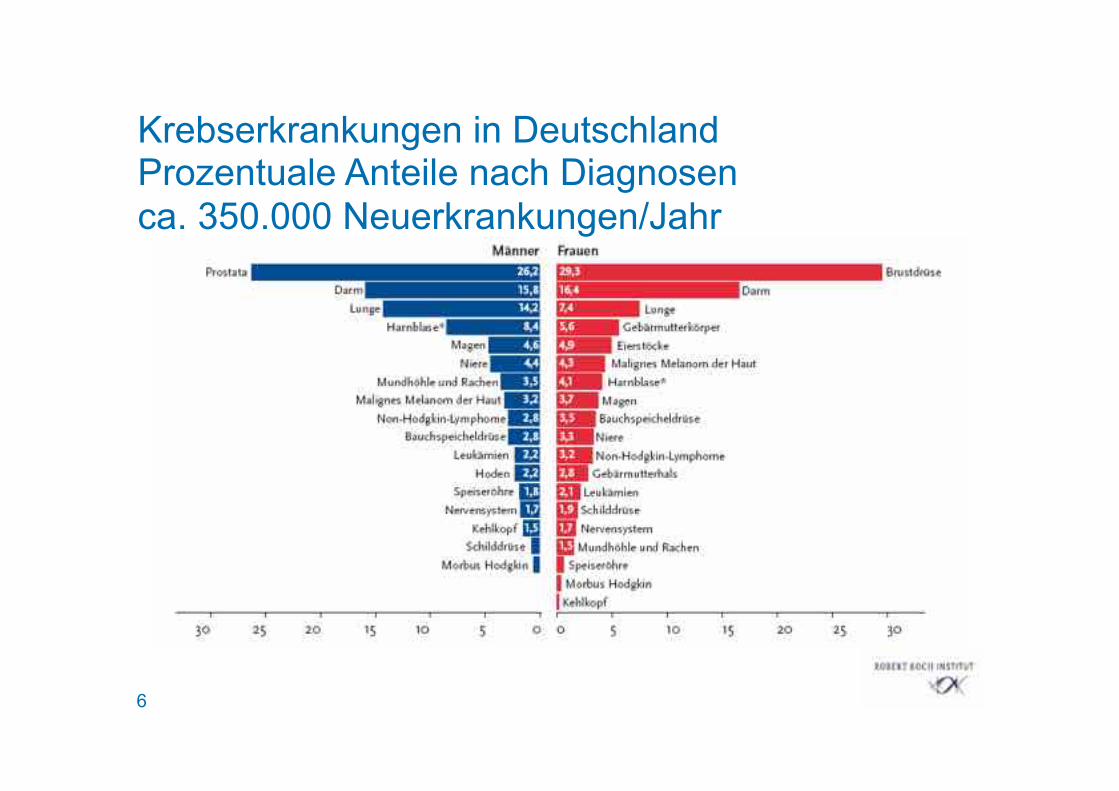
Krebserkrankungen in Deutschland Prozentuale Anteile nach Diagnosen ca. 350.000 Neuerkrankungen/Jahr
7
Krebs bei Kindern und Jugendlichen
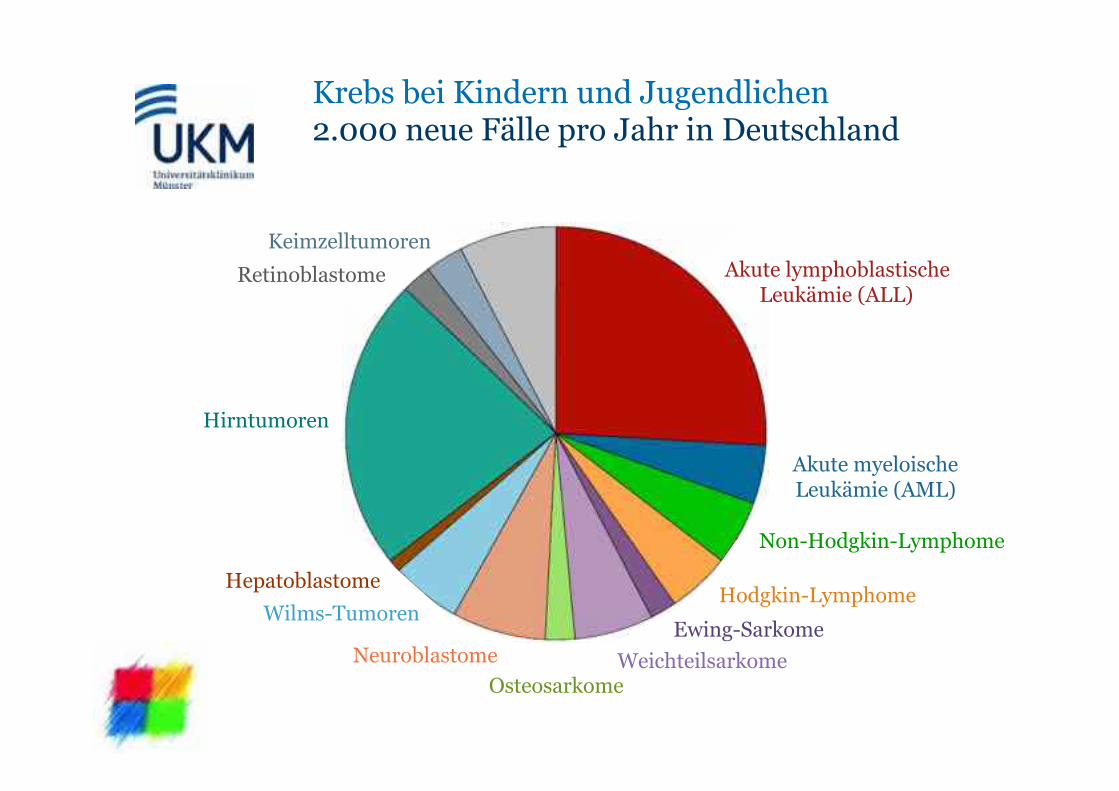
Hirntumoren
Retinoblastome
Hepatoblastome
Keimzelltumoren
Akute myeloische Leukämie (AML)
Non-Hodgkin-Lymphome
Hodgkin-Lymphome Ewing-Sarkome
Neuroblastome
Wilms-Tumoren
Osteosarkome Weichteilsarkome
Akute lymphoblastische Leukämie (ALL)
Krebs bei Kindern und Jugendlichen 2.000 neue Fälle pro Jahr in Deutschland
9
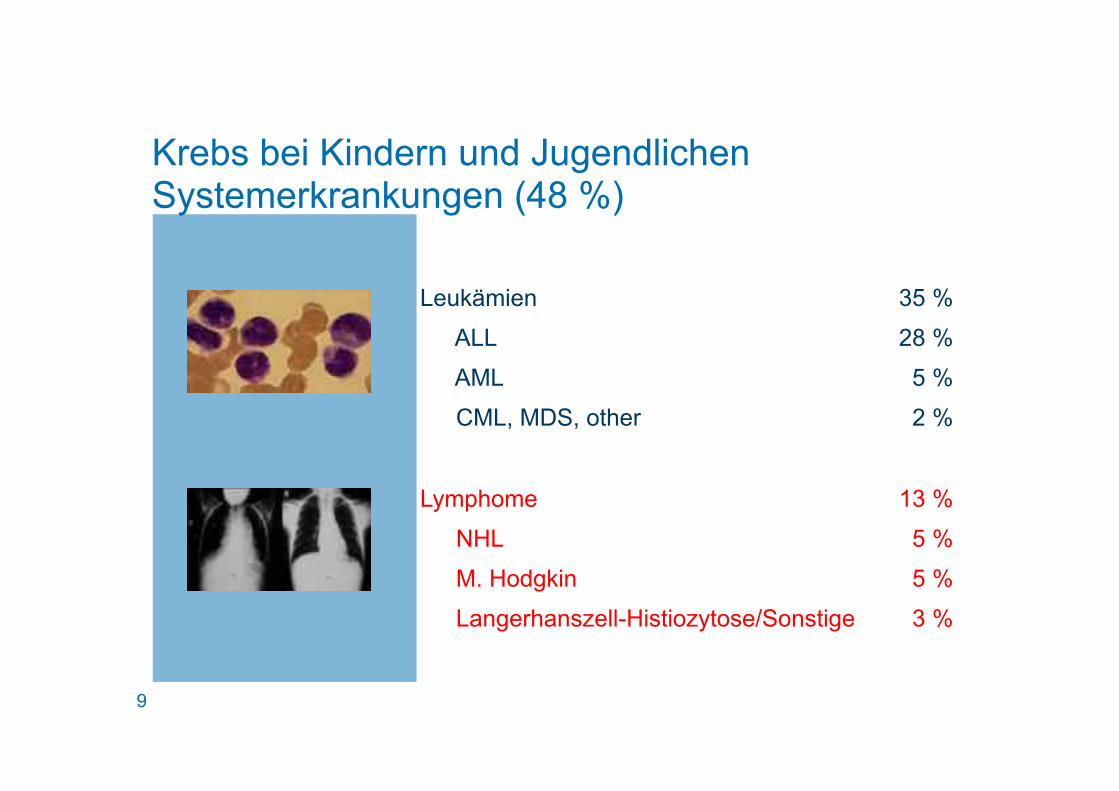
Krebs bei Kindern und Jugendlichen Systemerkrankungen (48 %)
Leukämien 35 %
ALL 28 %
AML 5 %
CML, MDS, other 2 %
Lymphome 13 %
NHL 5 %
M. Hodgkin 5 %
Langerhanszell-Histiozytose/Sonstige 3 %
10
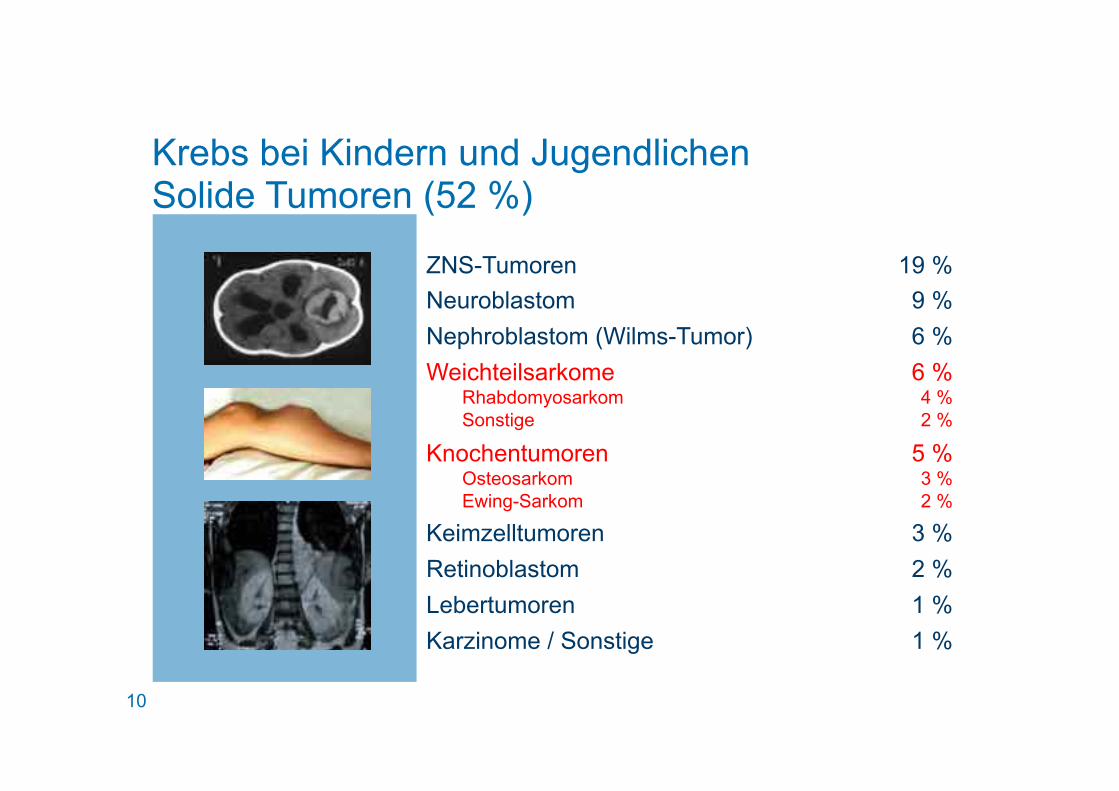
Krebs bei Kindern und Jugendlichen Solide Tumoren (52 %)
ZNS-Tumoren 19 % Neuroblastom 9 % Nephroblastom (Wilms-Tumor) 6 % Weichteilsarkome 6 %
Rhabdomyosarkom 4 % Sonstige 2 %
Knochentumoren 5 % Osteosarkom 3 % Ewing-Sarkom 2 %
Keimzelltumoren 3 % Retinoblastom 2 % Lebertumoren 1 % Karzinome / Sonstige 1 %
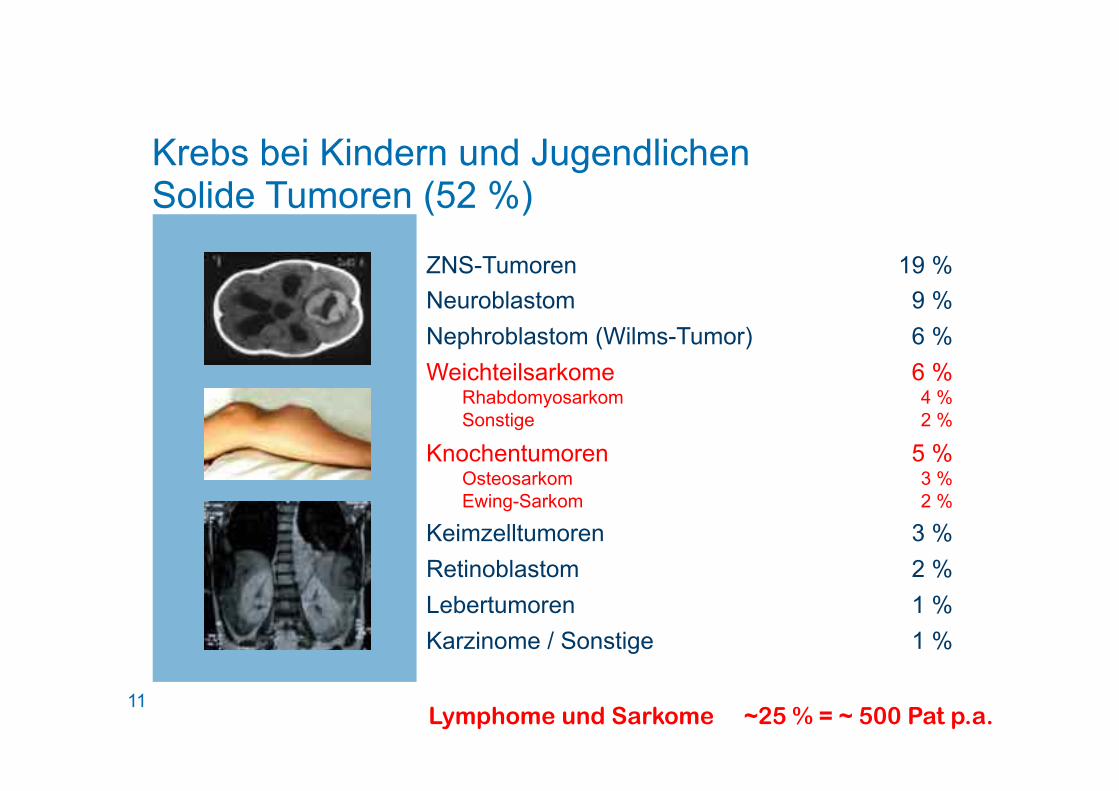
11 Lymphome und Sarkome ~25 % = ~ 500 Pat p.a.
Krebs bei Kindern und Jugendlichen Solide Tumoren (52 %)
ZNS-Tumoren 19 % Neuroblastom 9 % Nephroblastom (Wilms-Tumor) 6 % Weichteilsarkome 6 %
Rhabdomyosarkom 4 % Sonstige 2 %
Knochentumoren 5 % Osteosarkom 3 % Ewing-Sarkom 2 %
Keimzelltumoren 3 % Retinoblastom 2 % Lebertumoren 1 % Karzinome / Sonstige 1 %
12
% S
urvi
val a
fter 2
yea
rs
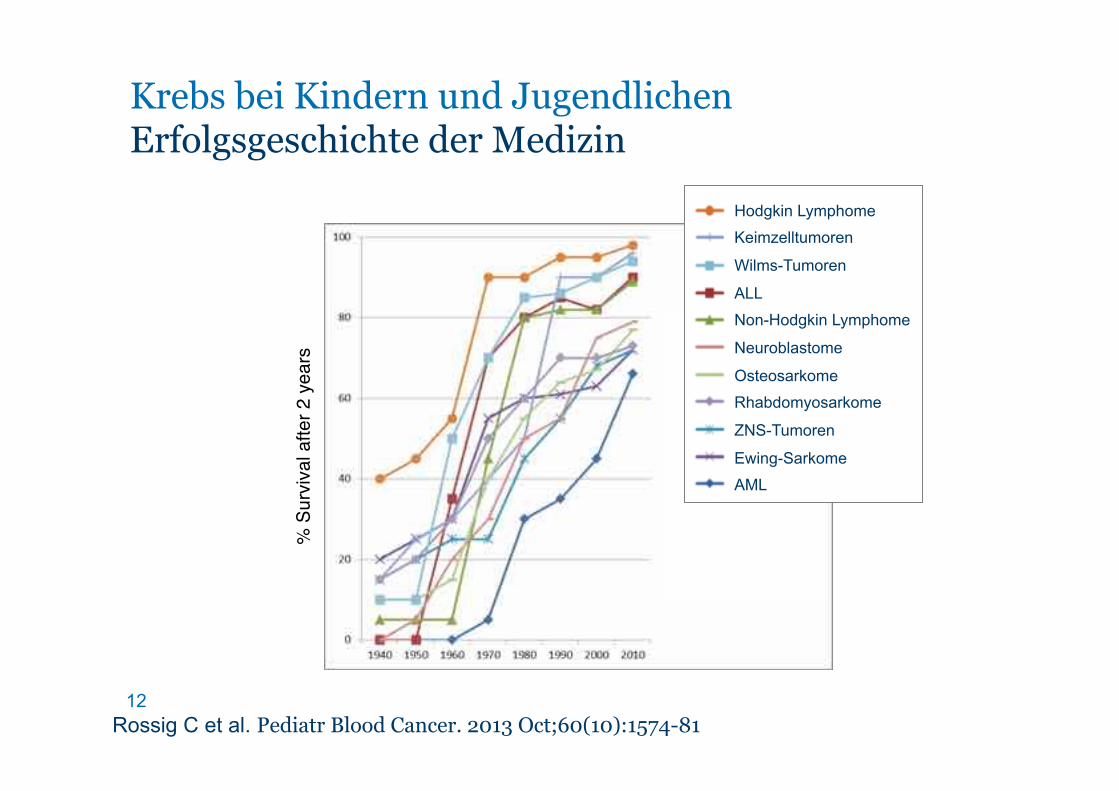
Rossig C et al. Pediatr Blood Cancer. 2013 Oct;60(10):1574-81
Krebs bei Kindern und Jugendlichen Erfolgsgeschichte der Medizin
Hodgkin Lymphome
Keimzelltumoren
Wilms-Tumoren
ALL
Non-Hodgkin Lymphome
Neuroblastome
Osteosarkome
Rhabdomyosarkome
ZNS-Tumoren
Ewing-Sarkome
AML
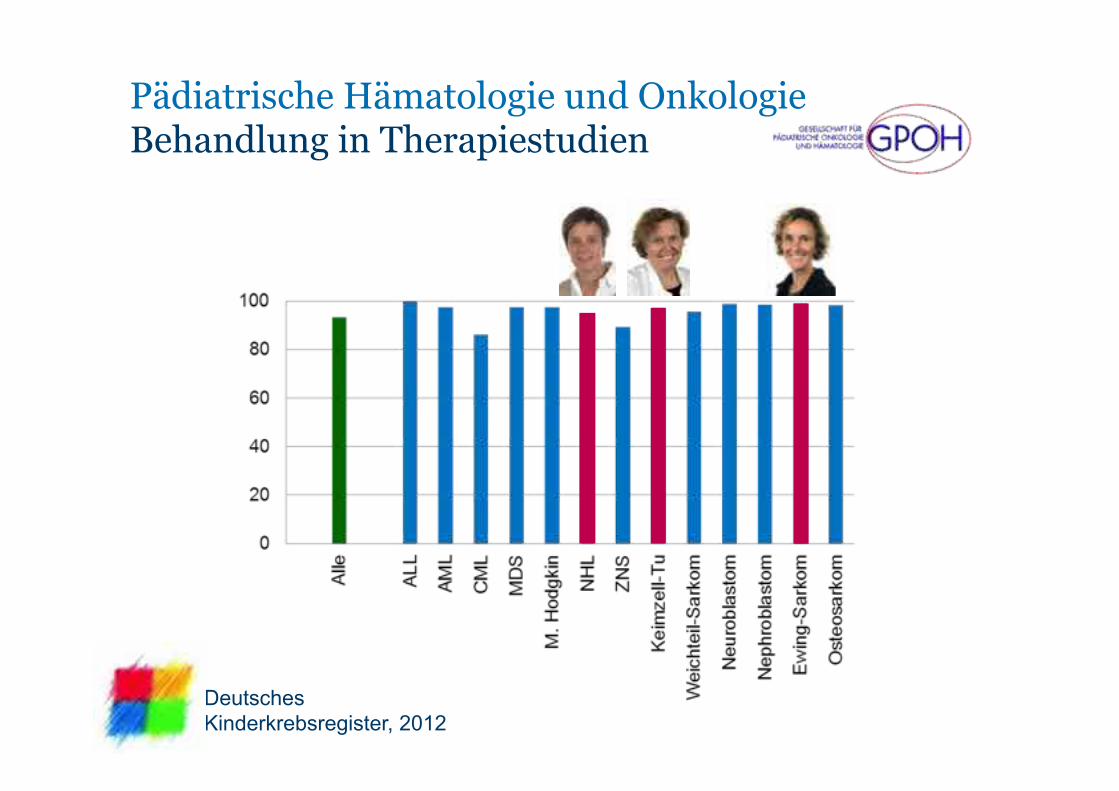
13 Deutsches Kinderkrebsregister, 2012
Pädiatrische Hämatologie und Onkologie Behandlung in Therapiestudien
14
Krebs bei Kindern und Jugendlichen Therapie

15 DKKR 1997
Leitsymptom Knochenschmerz
• Knochentumor
• ALL
• NHL
• Neuroblastom

16
17 DKKR 1997
Erwartungen an die Bildgebung Die fünf W‘s
• Wo?
• Wie?
• Wo noch?
• Weg?
• Wieder da?
18
Non-Hodgkin Lymphom
19
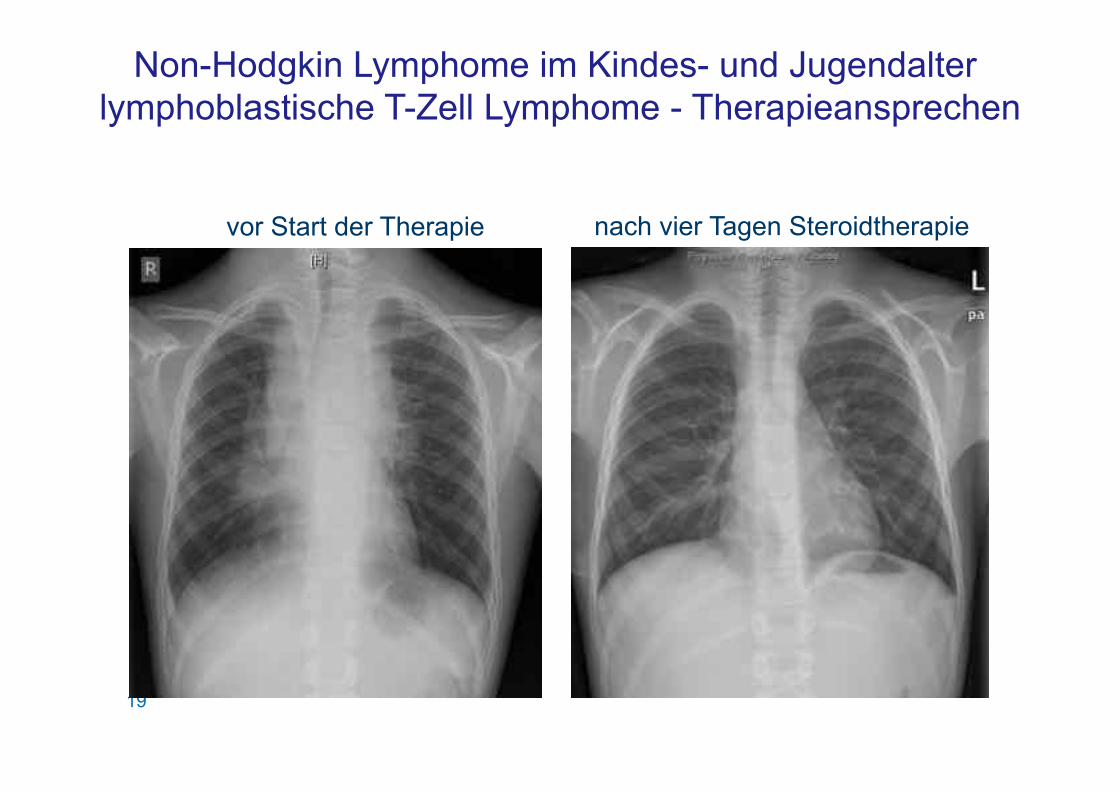
Non-Hodgkin Lymphome im Kindes- und Jugendalter lymphoblastische T-Zell Lymphome - Therapieansprechen
nach vier Tagen Steroidtherapie vor Start der Therapie
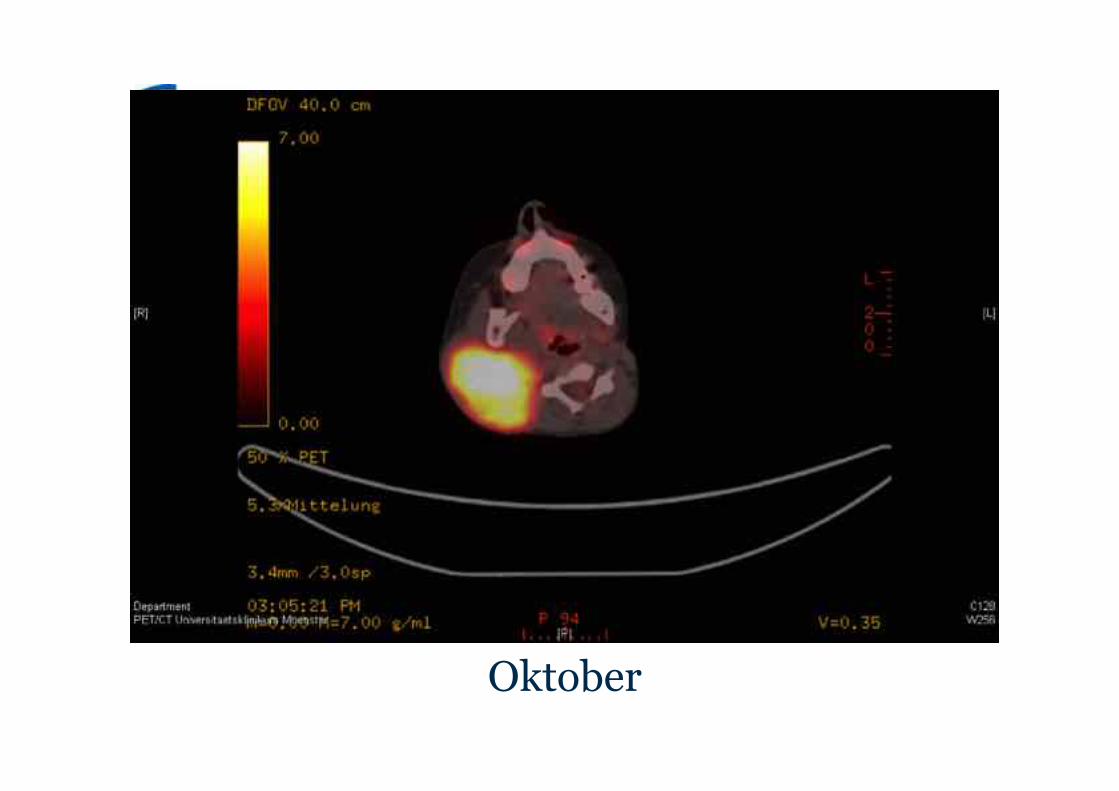
Oktober
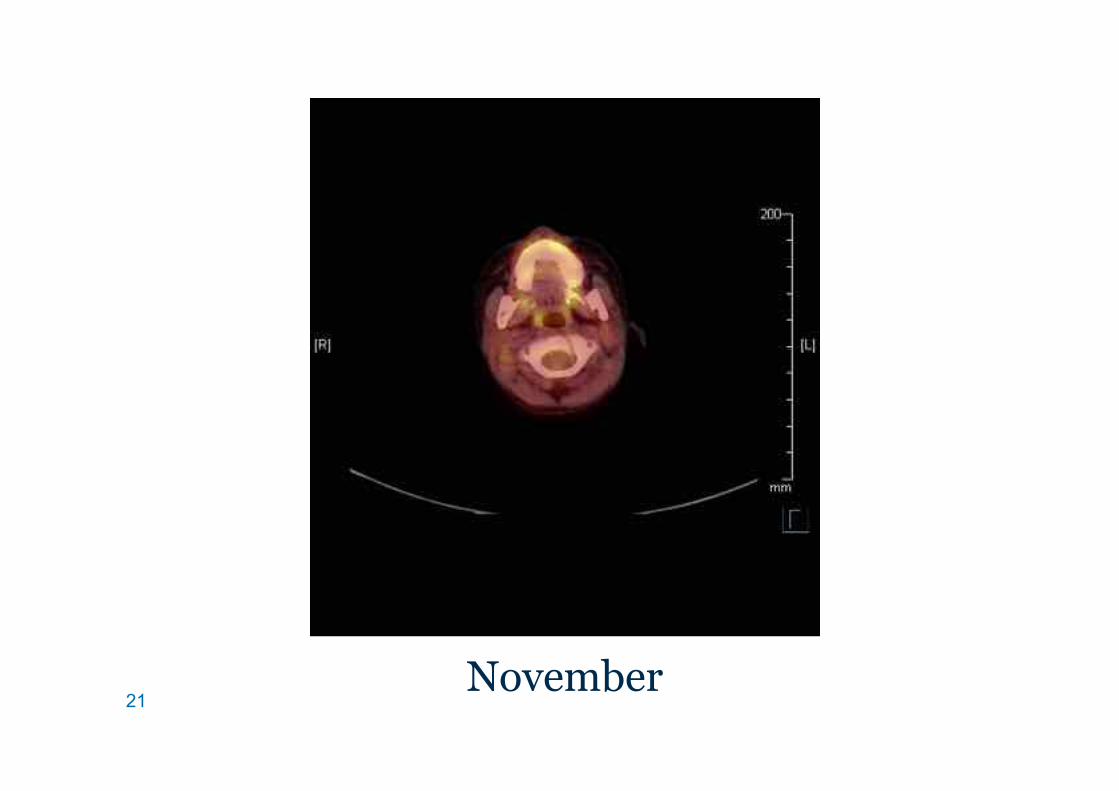
21 November
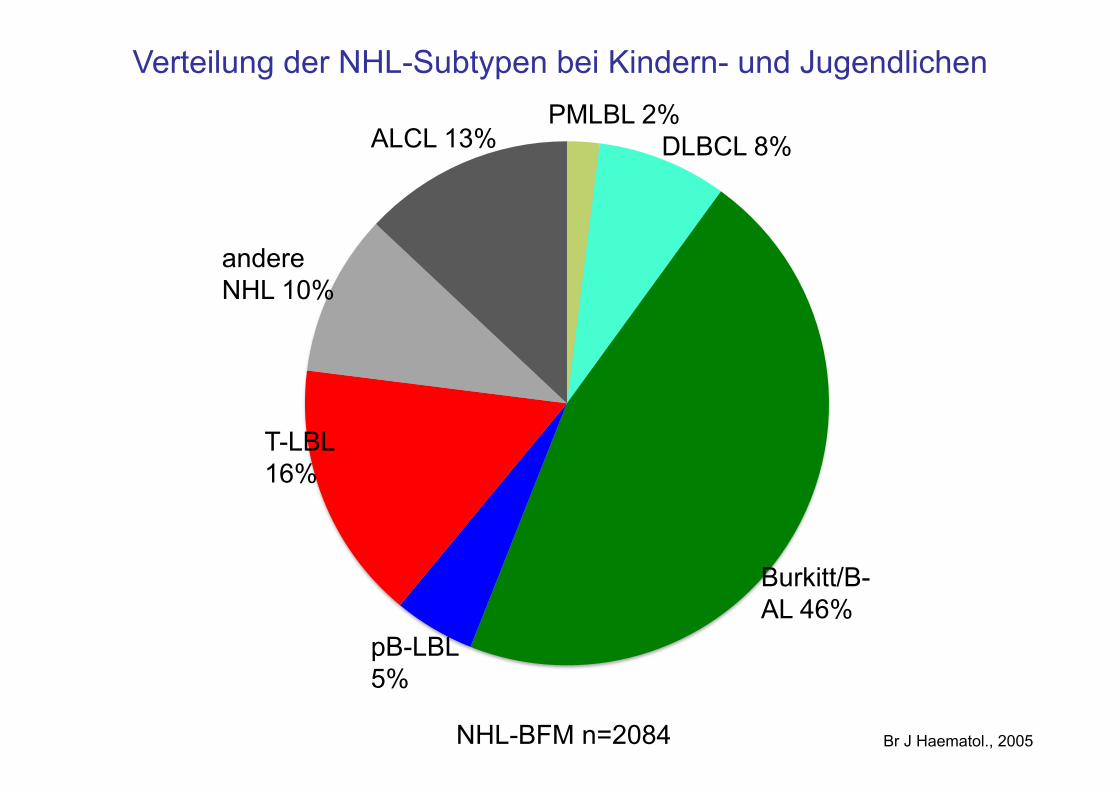
Verteilung der NHL-Subtypen bei Kindern- und Jugendlichen
Br J Haematol., 2005 NHL-BFM n=2084
Burkitt/B-AL 46%
DLBCL 8% PMLBL 2%
ALCL 13%
andere NHL 10%
T-LBL 16%
pB-LBL 5%
23
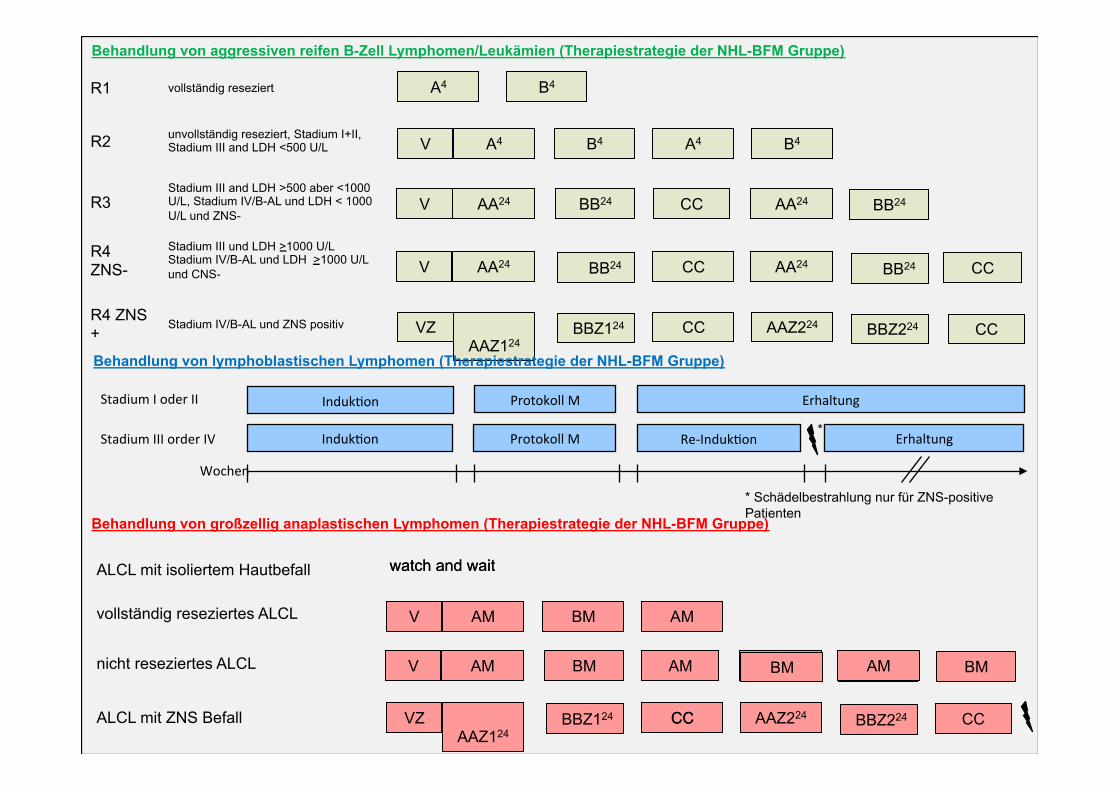
Behandlung von aggressiven reifen B-Zell Lymphomen/Leukämien (Therapiestrategie der NHL-BFM Gruppe)
R1 vollständig reseziert
R2 unvollständig reseziert, Stadium I+II, Stadium III and LDH <500 U/L
R3 Stadium III and LDH >500 aber <1000 U/L, Stadium IV/B-AL und LDH < 1000 U/L und ZNS-
R4 ZNS-
Stadium III und LDH >1000 U/L Stadium IV/B-AL und LDH >1000 U/L und CNS-
R4 ZNS+
Stadium IV/B-AL und ZNS positiv
A4
V
B4
A4 B4 A4 B4
V AA24 BB24 CC AA24
V AA24 BB24 CC AA24 CC
VZ AAZ124
BBZ124 CC AAZ224 CC
BB24
BB24
BBZ224
Behandlung von lymphoblastischen Lymphomen (Therapiestrategie der NHL-BFM Gruppe)
Protokoll'M' Erhaltung'
Wochen'
Induk4on'
Protokoll'M' Re6Induk4on' Erhaltung'Induk4on'
Stadium'I'oder'II'
Stadium'III'order'IV'*
V A4 B4 A4
V AA24 BB24 CC AA24
VZ AAZ1 BBZ124 CC AAZ224 CC
BB24
BBZ224
watch and wait
Behandlung von großzellig anaplastischen Lymphomen (Therapiestrategie der NHL-BFM Gruppe)
ALCL mit isoliertem Hautbefall
vollständig reseziertes ALCL
nicht reseziertes ALCL
ALCL mit ZNS Befall
V AM BM AM
V AM BM AM AM
VZ AAZ124
BBZ124 CC AAZ224 CC
BM
BBZ224
watch and wait
BM
* Schädelbestrahlung nur für ZNS-positive Patienten
24
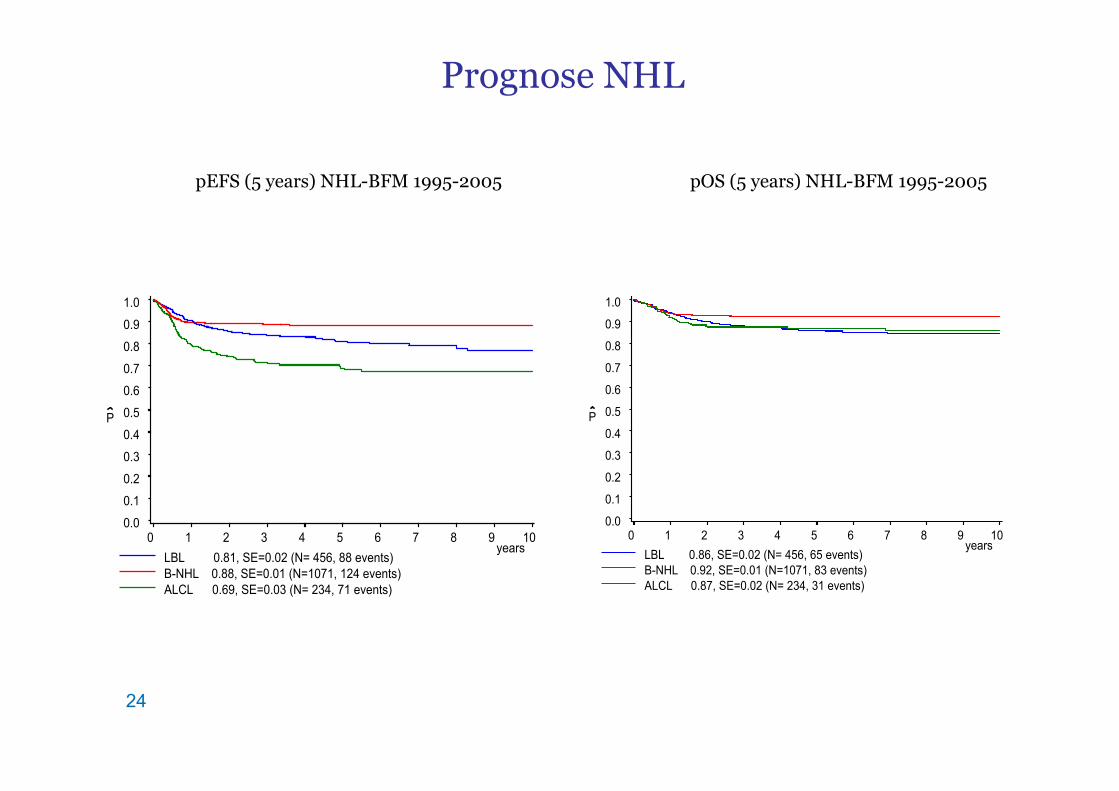
Prognose NHL
LBL 0.81, SE=0.02 (N= 456, 88 events) B-NHL 0.88, SE=0.01 (N=1071, 124 events) ALCL 0.69, SE=0.03 (N= 234, 71 events)
years
P
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10
pEFS (5 years) NHL-BFM 1995-2005
LBL 0.86, SE=0.02 (N= 456, 65 events) B-NHL 0.92, SE=0.01 (N=1071, 83 events) ALCL 0.87, SE=0.02 (N= 234, 31 events)
years
P
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10
pOS (5 years) NHL-BFM 1995-2005
25
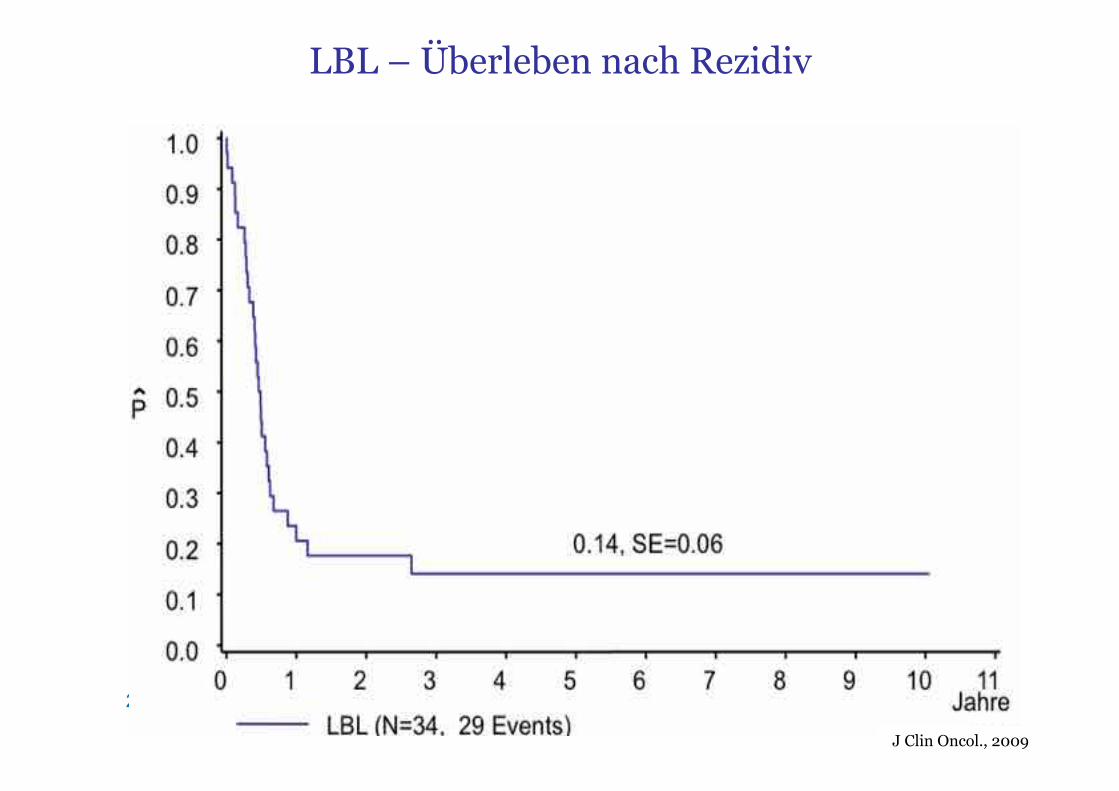
LBL – Überleben nach Rezidiv
J Clin Oncol., 2009
26
Morbus Hodgkin
27
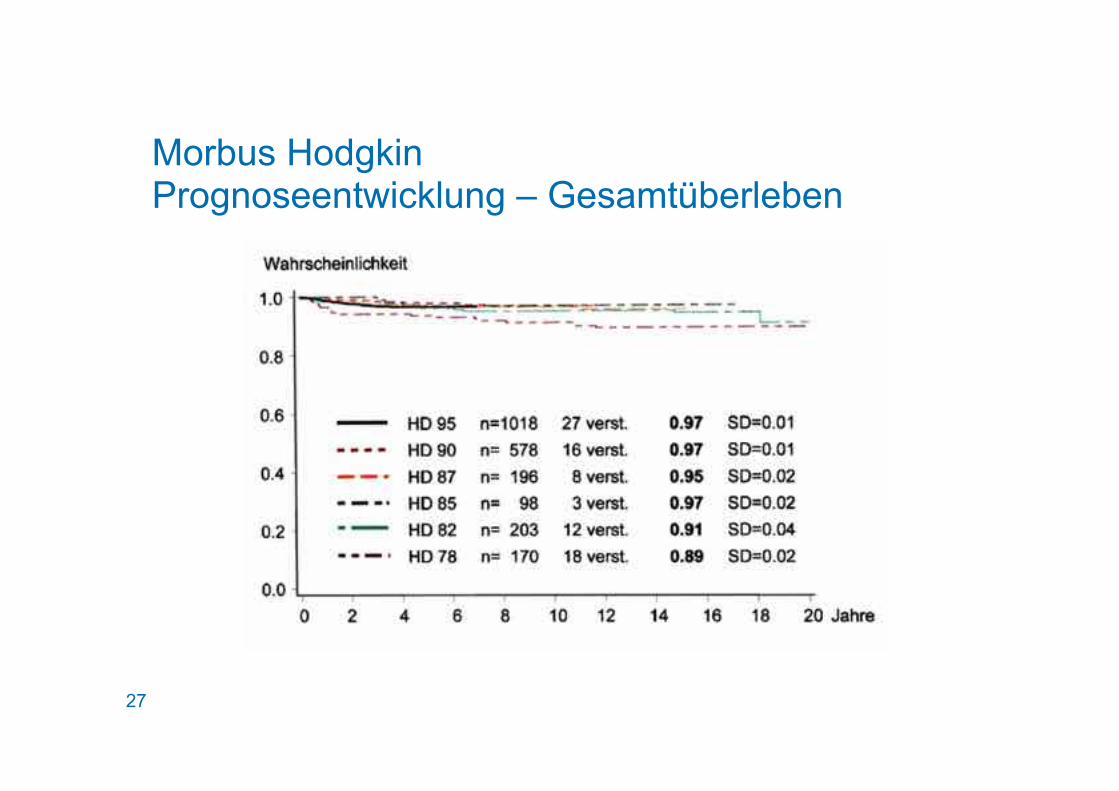
Morbus Hodgkin Prognoseentwicklung – Gesamtüberleben
28
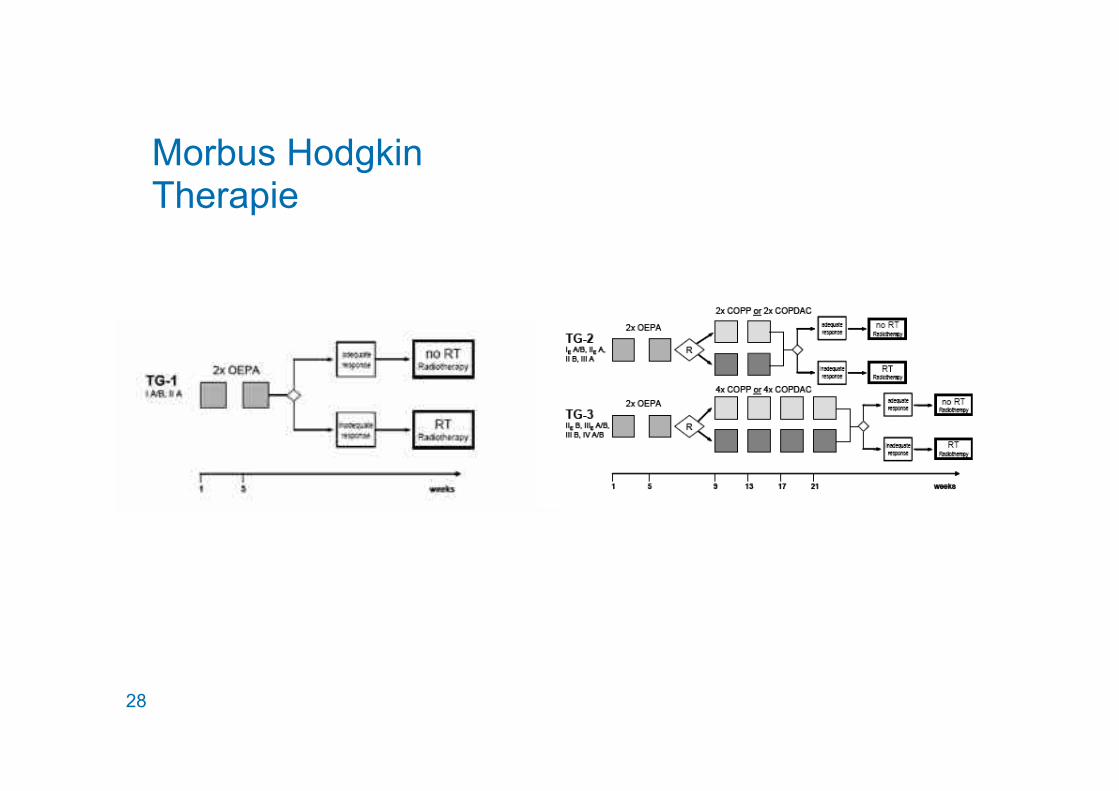
Morbus Hodgkin Therapie

EuroNet-PHL Justus Liebig University of Giessen
EuroNet-PHL-C2
EuroNet-Paediatric Hodgkin’s Lymphoma Group Second International Inter-Group Study
for Classical Hodgkin’s Lymphoma in Children and Adolescents
EudraCT-Number: 2012-004053-88
Training material for site initiation and new staff members on site
Prof. Dr. Dieter Körholz and Prof. Dr. Christine Mauz-Körholz for the EuroNet-PHL study group
30
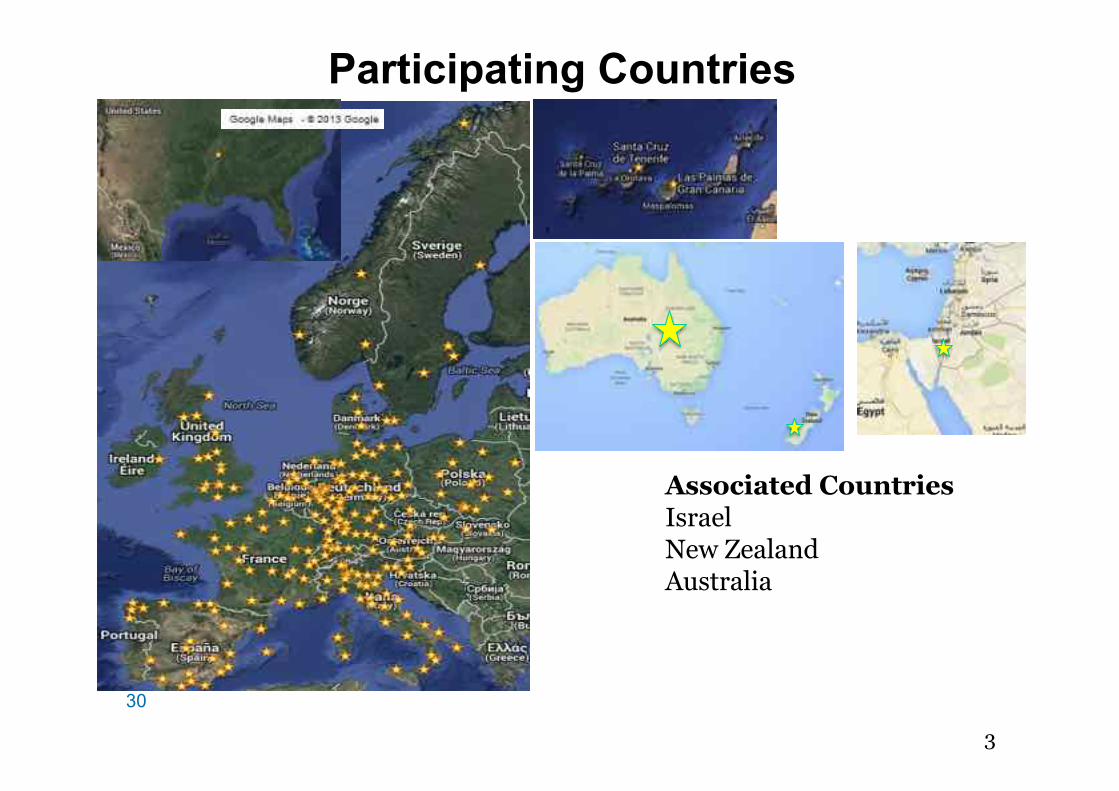
Participating Countries
Associated Countries Israel New Zealand Australia
30
31
Aims
Reduction of radiotherapy (RT) burden without compromising cure rates
Chemotherapy randomisation to compensate for
RT reduction
31
32
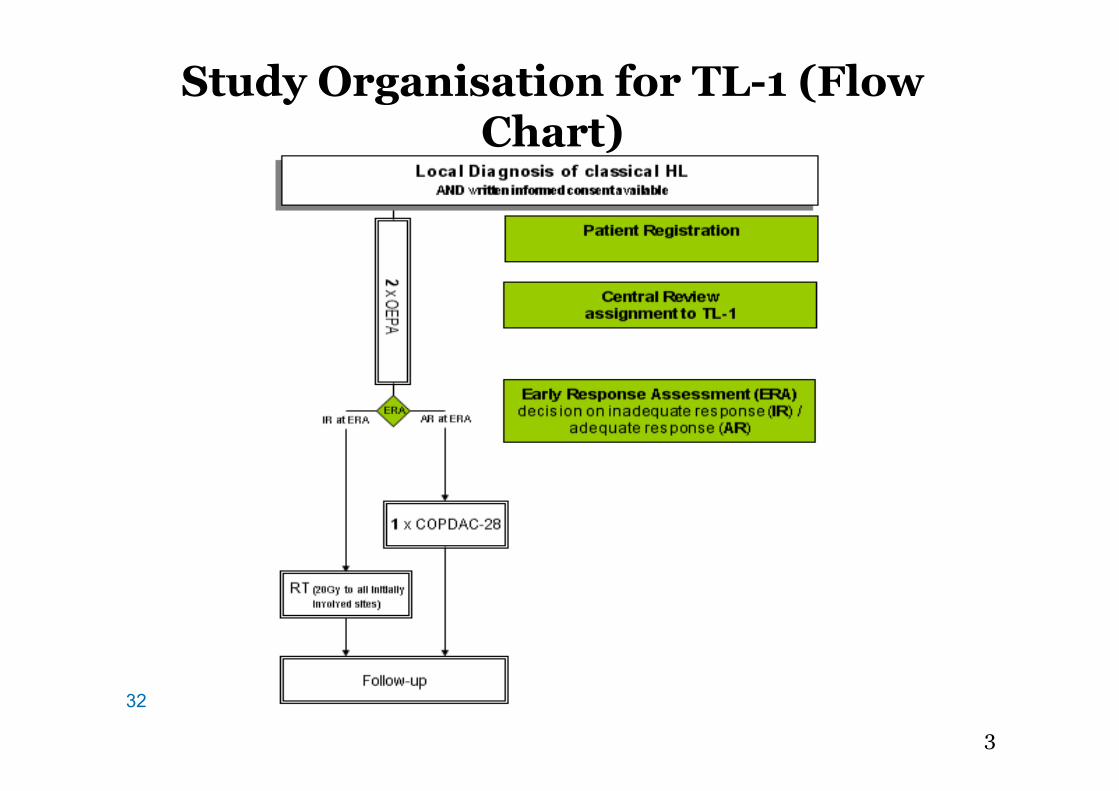
Study Organisation for TL-1 (Flow Chart)
32
33
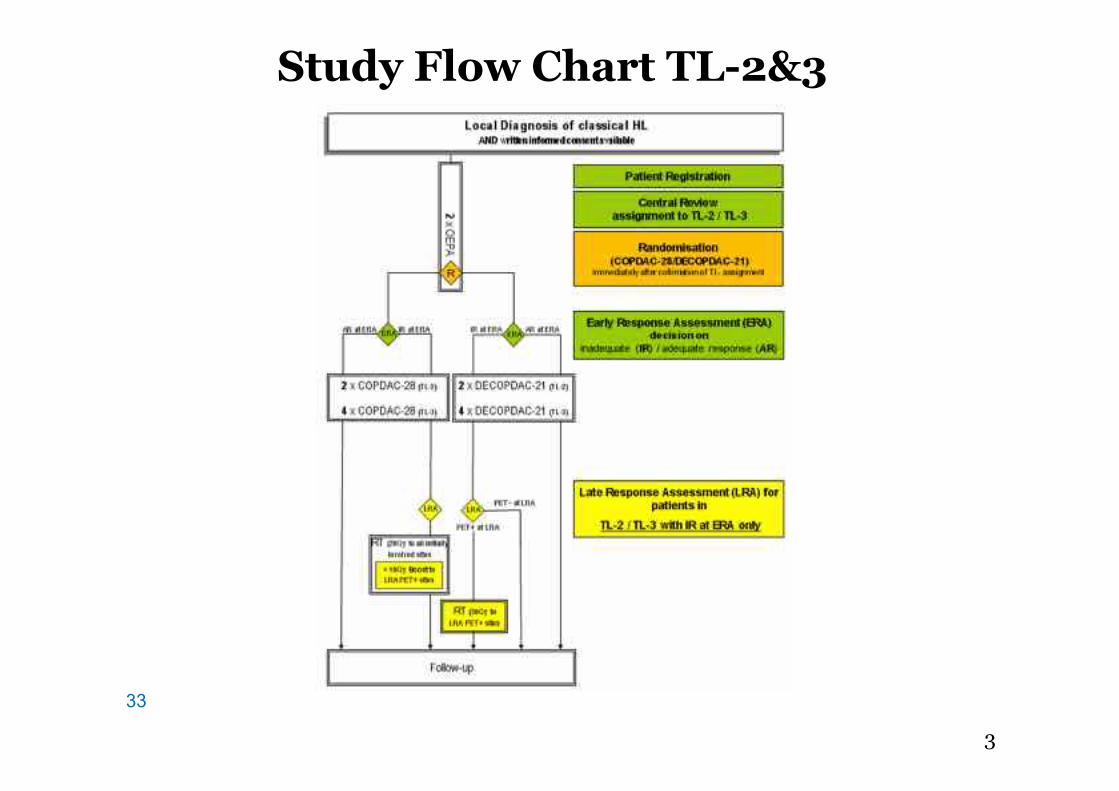
Study Flow Chart TL-2&3
33
34
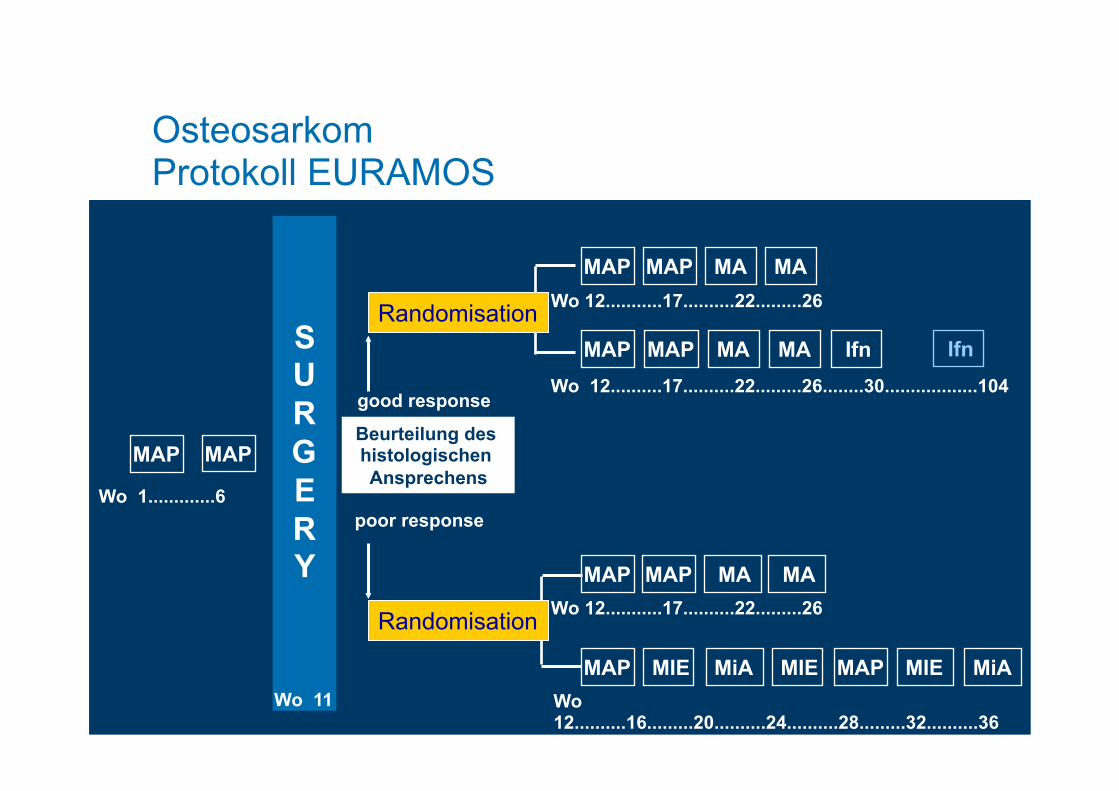
Osteosarkom
35
MAP
Randomisation
Randomisation
S U R G E R Y
Beurteilung des histologischen Ansprechens
Wo 12...........17..........22.........26
Wo 12..........17..........22.........26........30..................104
Wo 12..........16.........20..........24..........28.........32..........36
MAP
poor response
good response
MAP MAP MA MA
MAP MAP MA MA Ifn Ifn
MAP MAP MA MA Wo 12...........17..........22.........26
MAP MIE MiA MIE MAP MIE MiA
Wo 1.............6
Wo 11
Osteosarkom Protokoll EURAMOS
36
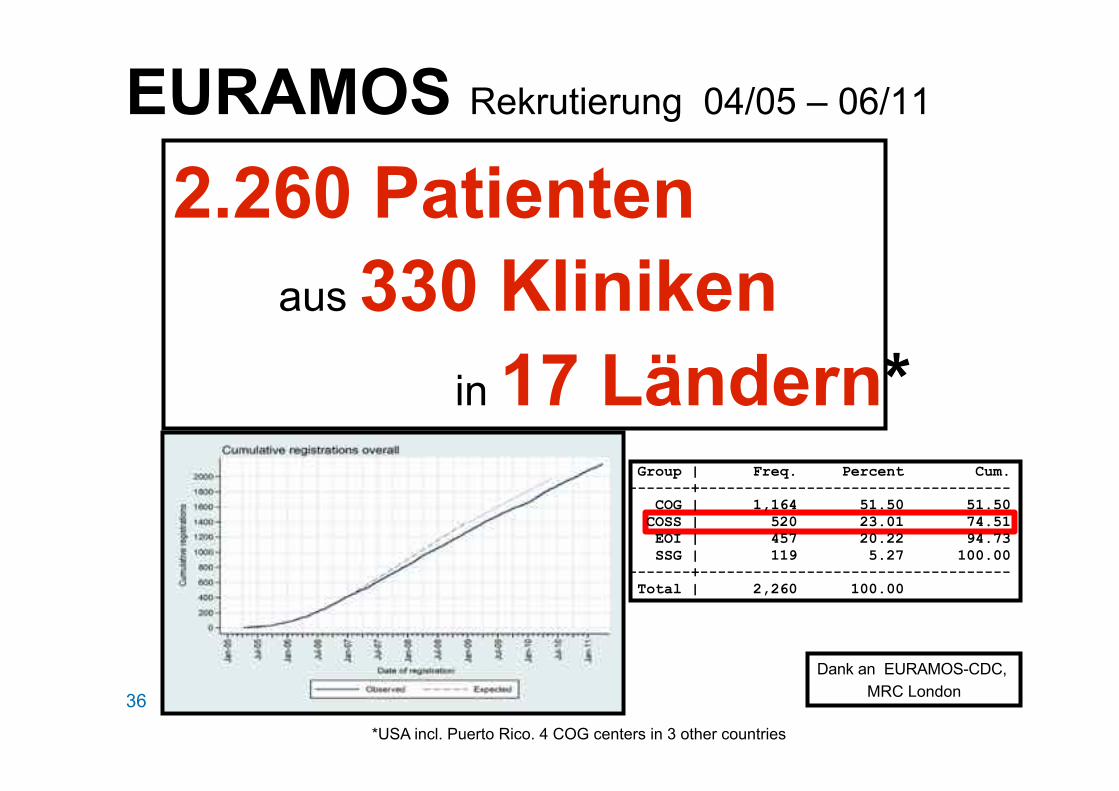
EURAMOS Rekrutierung 04/05 – 06/11
Dank an EURAMOS-CDC, MRC London
2.260 Patienten aus 330 Kliniken in 17 Ländern*
*USA incl. Puerto Rico. 4 COG centers in 3 other countries
Group | Freq. Percent Cum. ------------+----------------------------------- COG | 1,164 51.50 51.50 COSS | 520 23.01 74.51 EOI | 457 20.22 94.73 SSG | 119 5.27 100.00 ------------+----------------------------------- Total | 2,260 100.00

37
Therapiestrategie Bildgebung/Biopsie
neoadjuvante Chemotherapie
Operation
adjuvante Chemotherapie
38
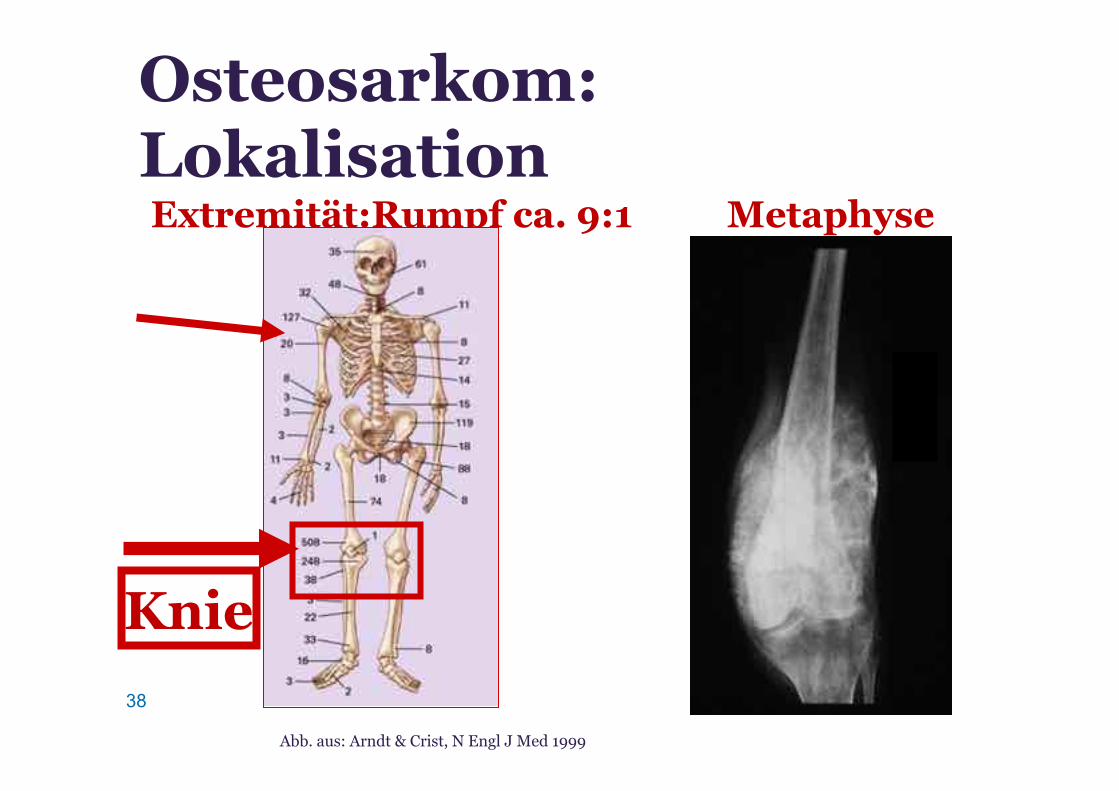
Abb. aus: Arndt & Crist, N Engl J Med 1999
Osteosarkom: Lokalisation Extremität:Rumpf ca. 9:1 Metaphyse
Knie

39
Osteosarkom Bildgebung: MRT
Methode der Wahl für • Weichteilkomponente • intramedulläre Ausdehnung • Beziehung zu Nerven und Gefäßen
40
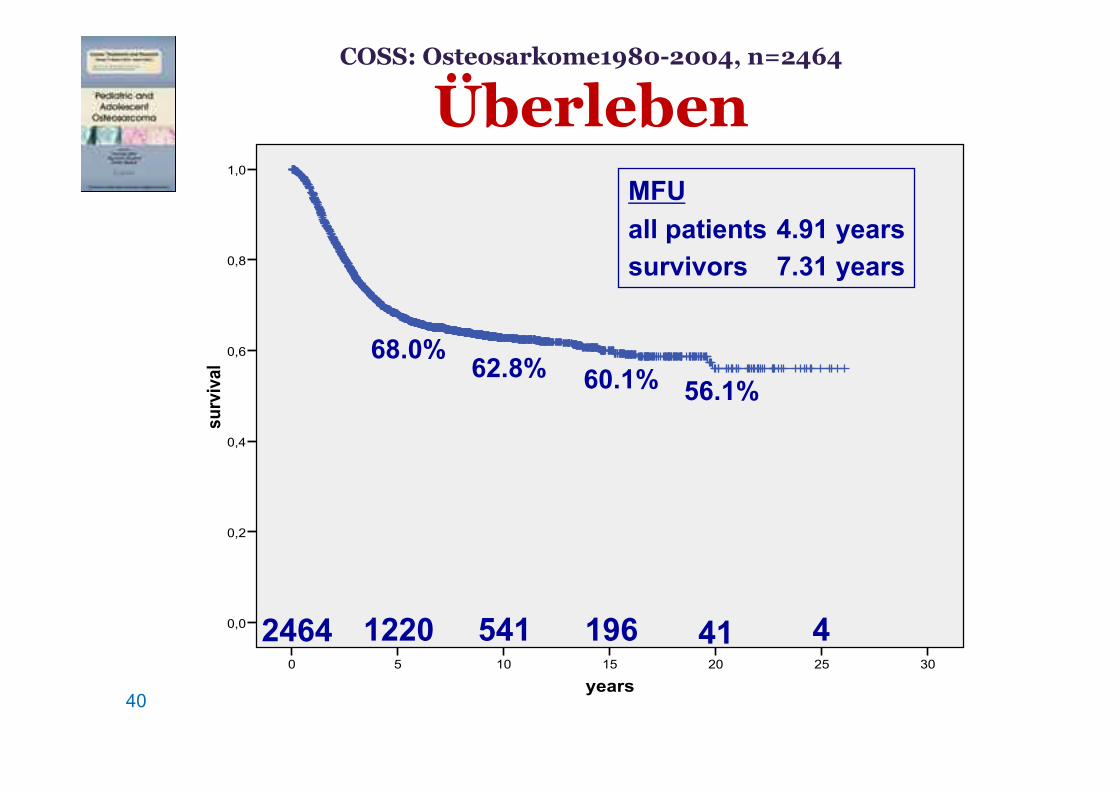
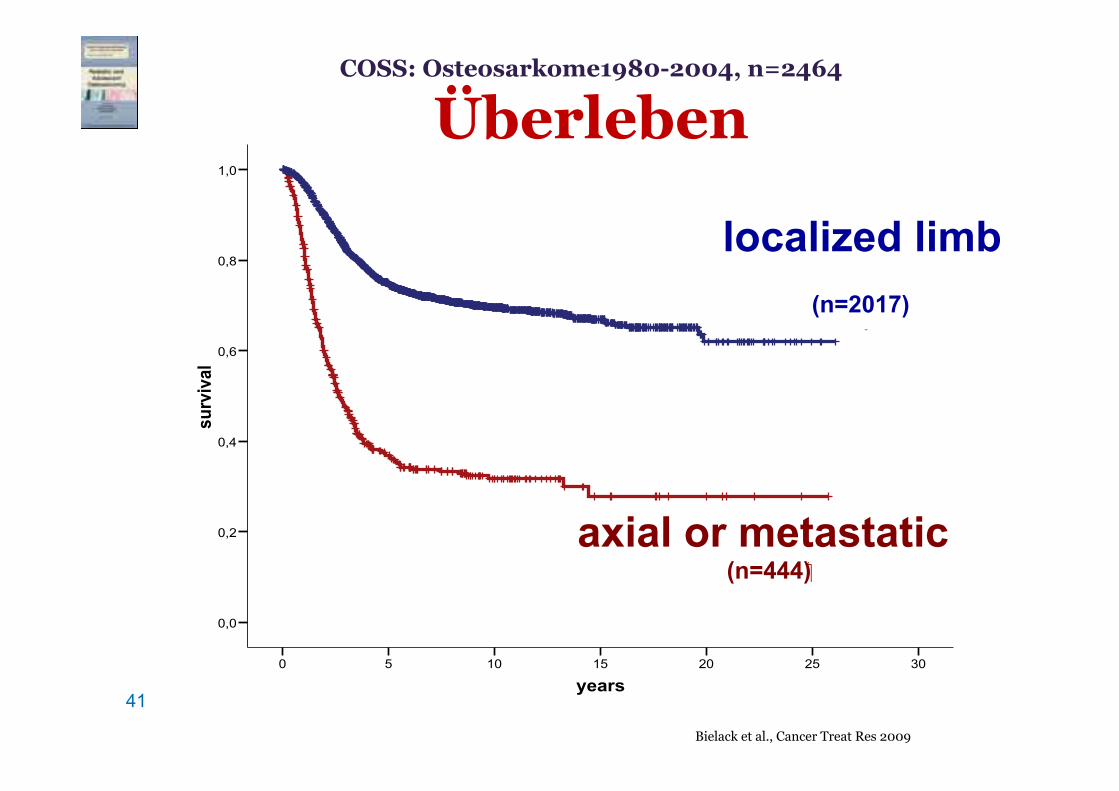
COSS: Osteosarkome1980-2004, n=2464
Überleben
years302520151050
survival
1,0
0,8
0,6
0,4
0,2
0,0
68.0% 62.8% 60.1% 56.1%
MFU all patients 4.91 years survivors 7.31 years
41 1220 541 196 4 2464
41 years
302520151050
survival
1,0
0,8
0,6
0,4
0,2
0,0
localized extremity
axial or / and primary metastatic
localized limb (n=2017)
axial or metastatic (n=444)
COSS: Osteosarkome1980-2004, n=2464
Überleben
Bielack et al., Cancer Treat Res 2009
42
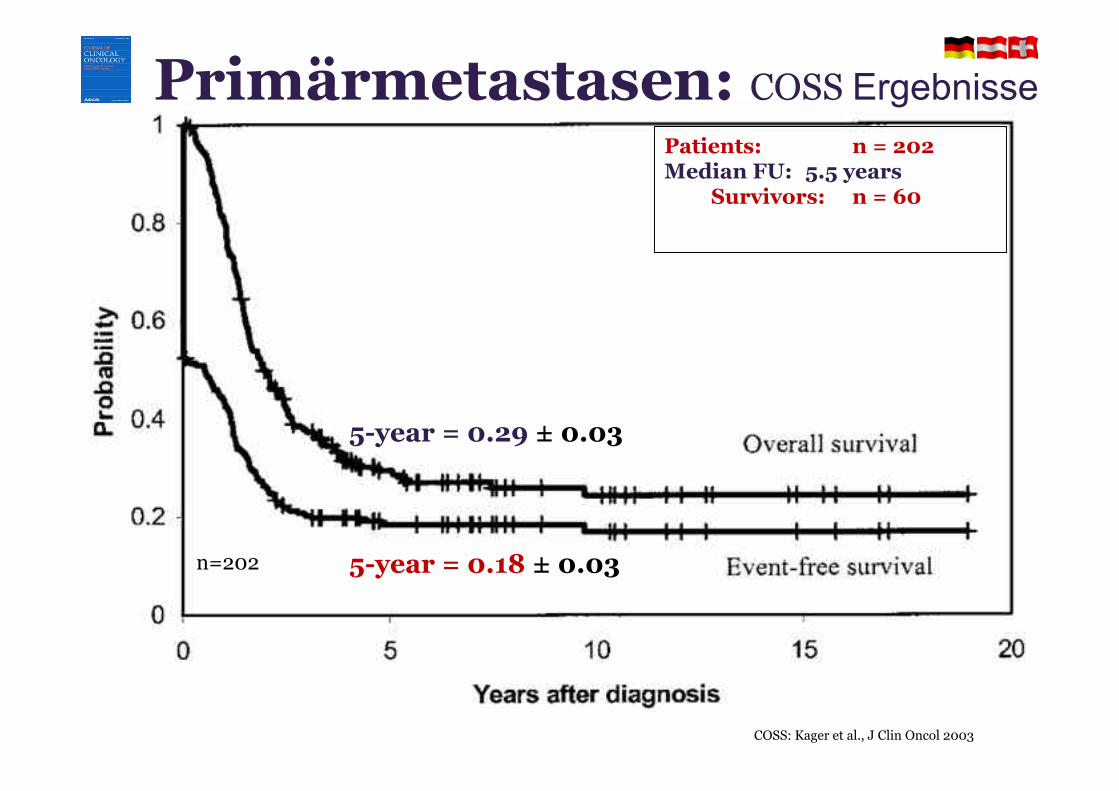
Patients: n = 202 Median FU: 5.5 years
Survivors: n = 60
5-year = 0.29 ± 0.03
5-year = 0.18 ± 0.03 n=202
Primärmetastasen: COSS Ergebnisse
COSS: Kager et al., J Clin Oncol 2003
43
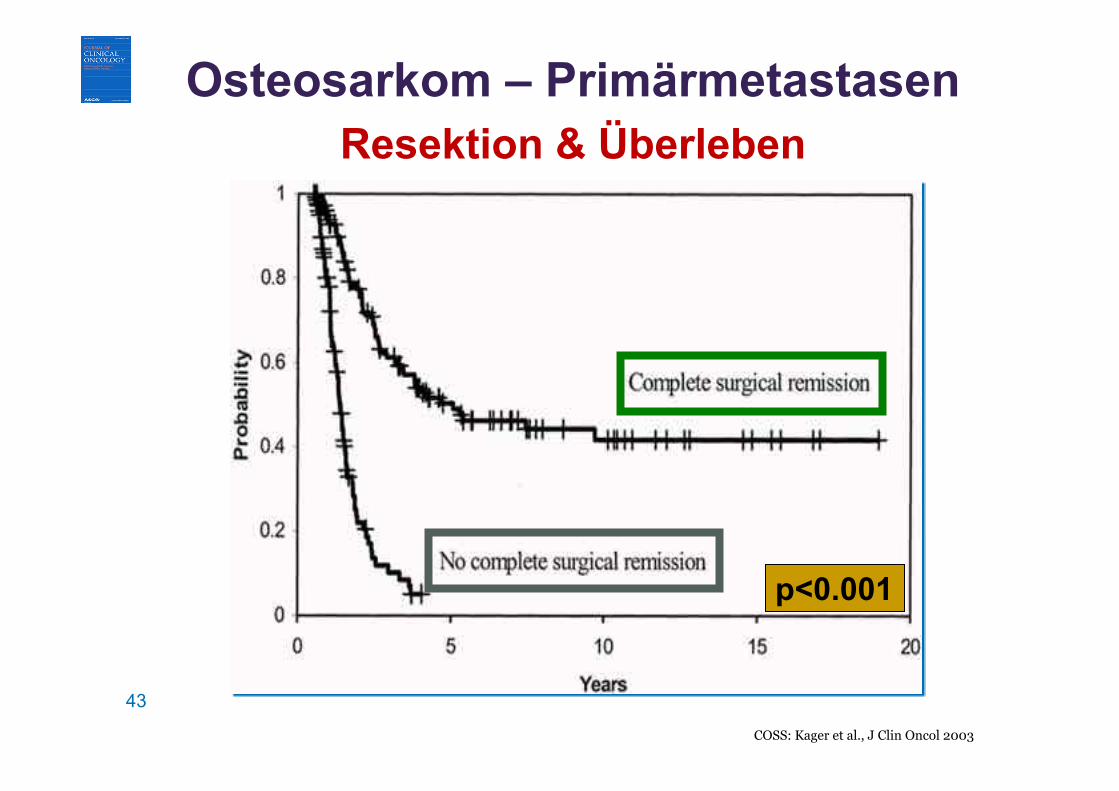
p<0.001
Osteosarkom – Primärmetastasen Resektion & Überleben
COSS: Kager et al., J Clin Oncol 2003
44
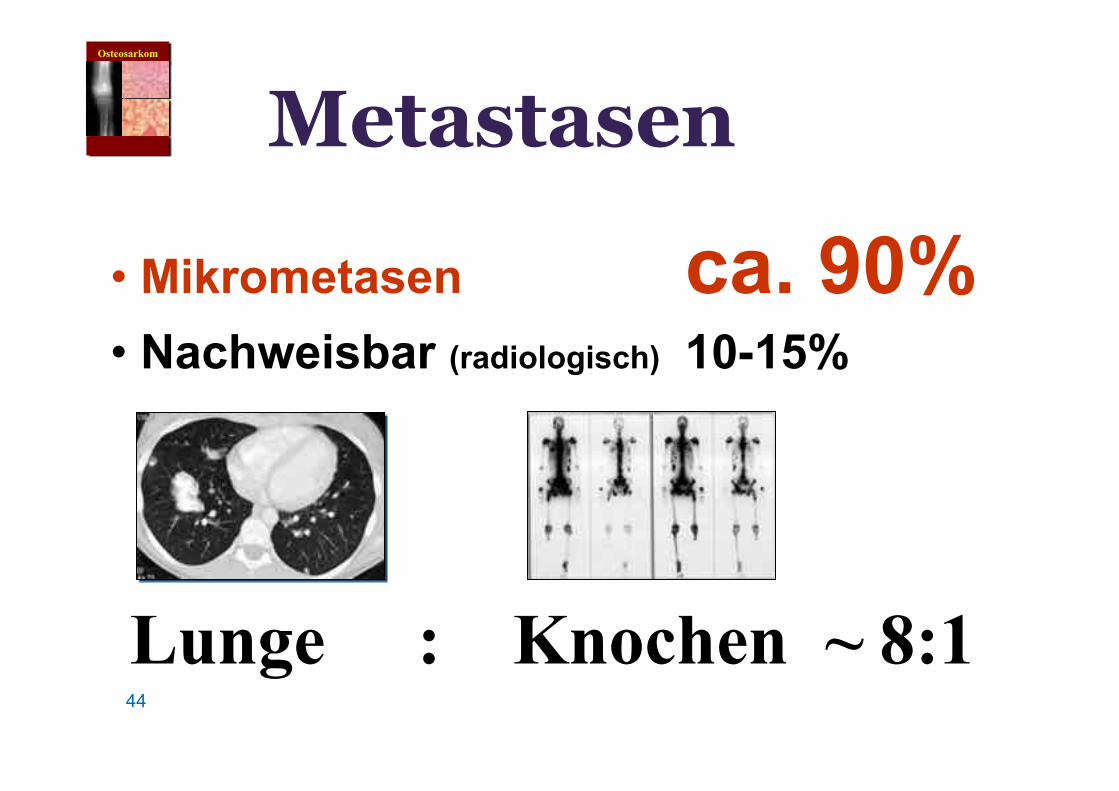
Metastasen
• Mikrometasen ca. 90% • Nachweisbar (radiologisch) 10-15%
Lunge : Knochen ~ 8:1
Osteosarkom

45
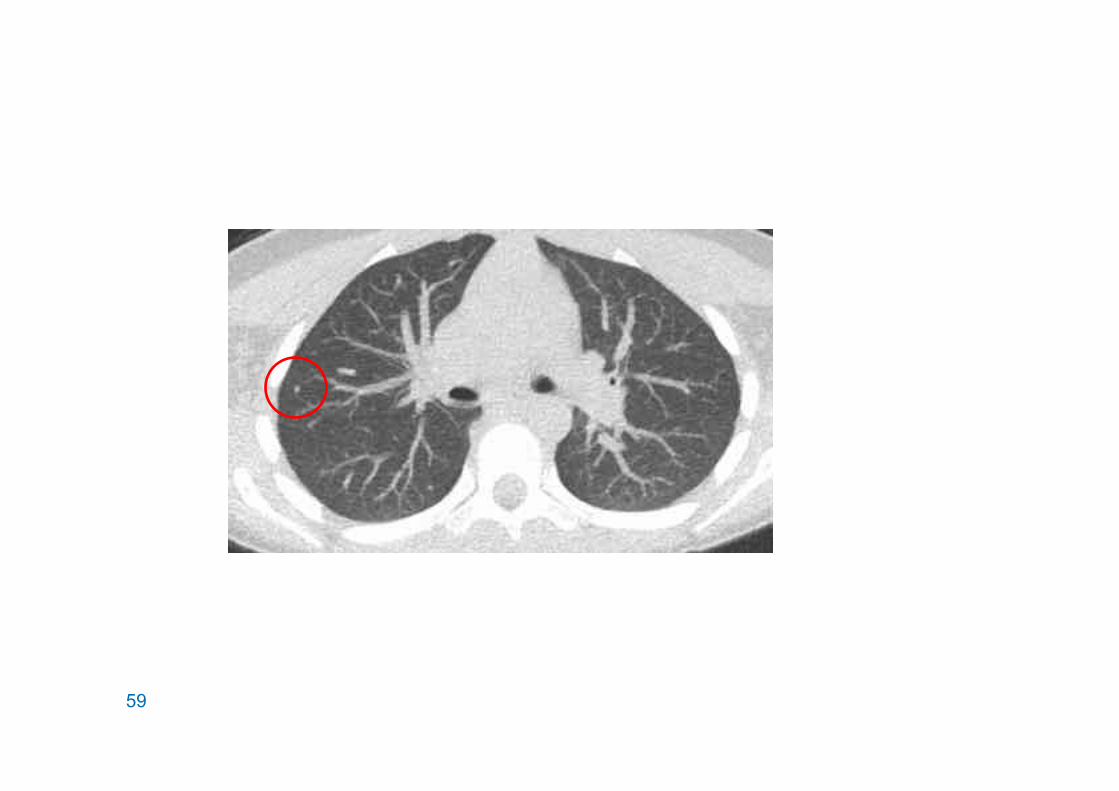
Sind CTs “perfekt”?
Osteosarkom: Lungenmetastasen
46
CT: 51 suspicion Thoracotomy: 39 metastatic
22 no mets
47
48
49
Schlussfolgerungen: • keine perfekte Methode • oft mehr als erwartet • bilateral denken!
Osteosarkom-Lungenmetastasen
Bildgebung

50 FDG PET CT Fusion FDG PET
Port
Primärtumor
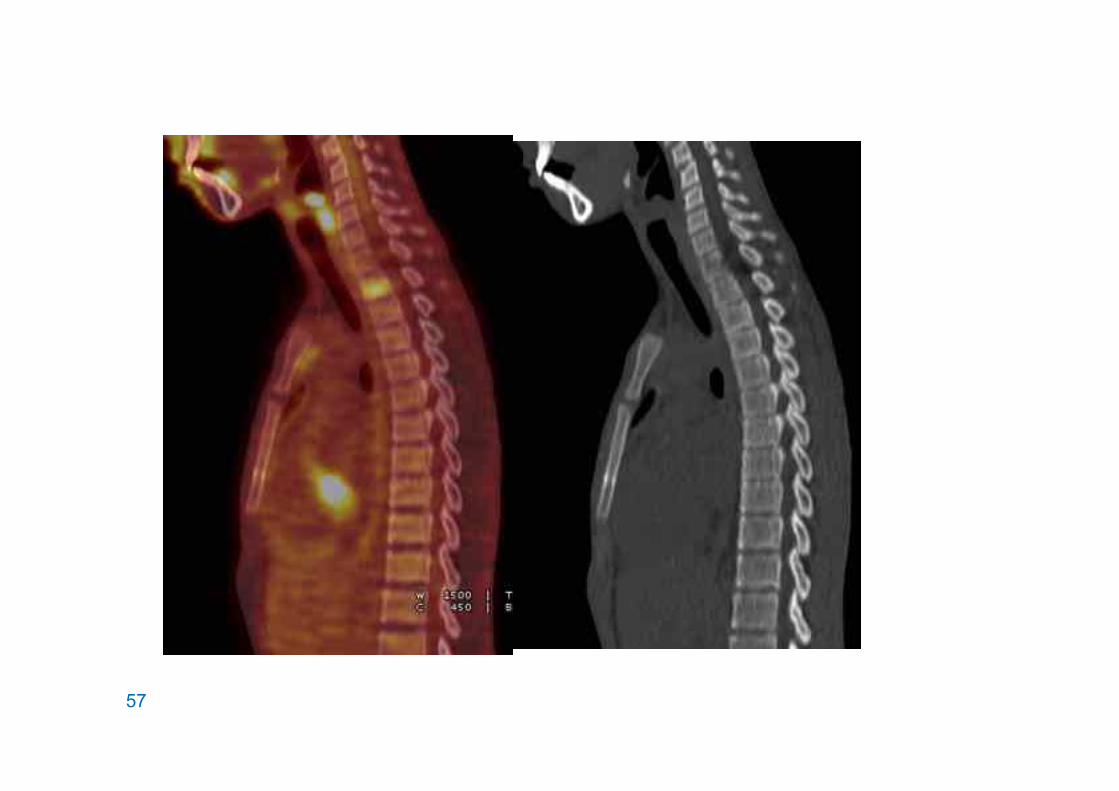
PET und PET-CT bei ossären Sarkomen – Osteosarkom Knochenmetastasen, FDG negativ

51
Ewing-Sarkom
Röntgen MRT
52
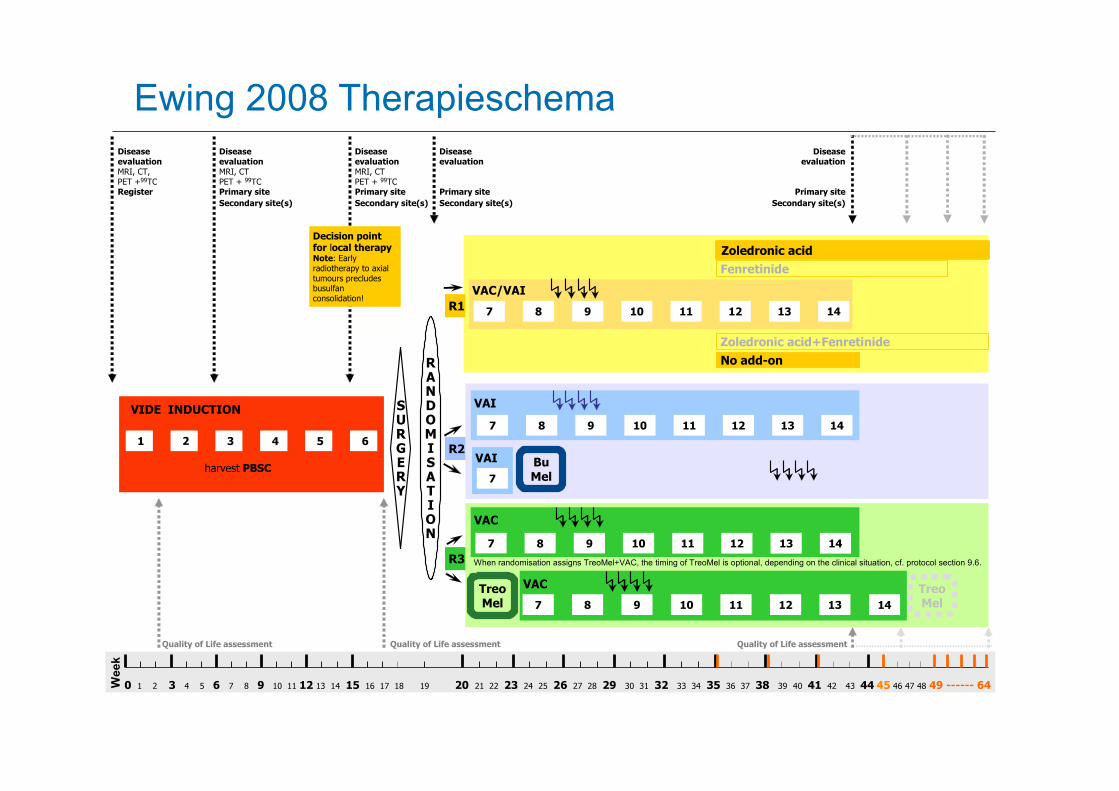
Ewing 2008 Therapieschema Ewing 2008 Treatment Schema
35 38 41
Quality of Life assessment Quality of Life assessment Quality of Life assessment .....................................................
VAC/VAI
VAI
VAC
VIDE INDUCTION
2 3 5 64
SURGERY
harvest PBSC
1 VAI
RANDOMISATION
R3
No add-onZoledronic acid+Fenretinide
FenretinideZoledronic acid
7 9 8 14 10 11 12 13
7
Decision point for local therapyNote: Early radiotherapy to axial tumours precludes busulfan consolidation!
7 9 8 14 10 11 12 13
7 9 8 14 10 11 12 13
R1
R2
VAC
7 9 8 14 10 11 12 13
Week
Disease Disease Disease Disease Diseaseevaluation evaluation evaluation evaluation evaluationMRI, CT, MRI, CT MRI, CTPET +99TC PET + 99TC PET + 99TC Register Primary site Primary site Primary site Primary site
Secondary site(s) Secondary site(s) Secondary site(s) Secondary site(s)
BuMel
TreoMel
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 ------ 64
When randomisation assigns TreoMel+VAC, the timing of TreoMel is optional, depending on the clinical situation, cf. protocol section 9.6.
TreoMel
53
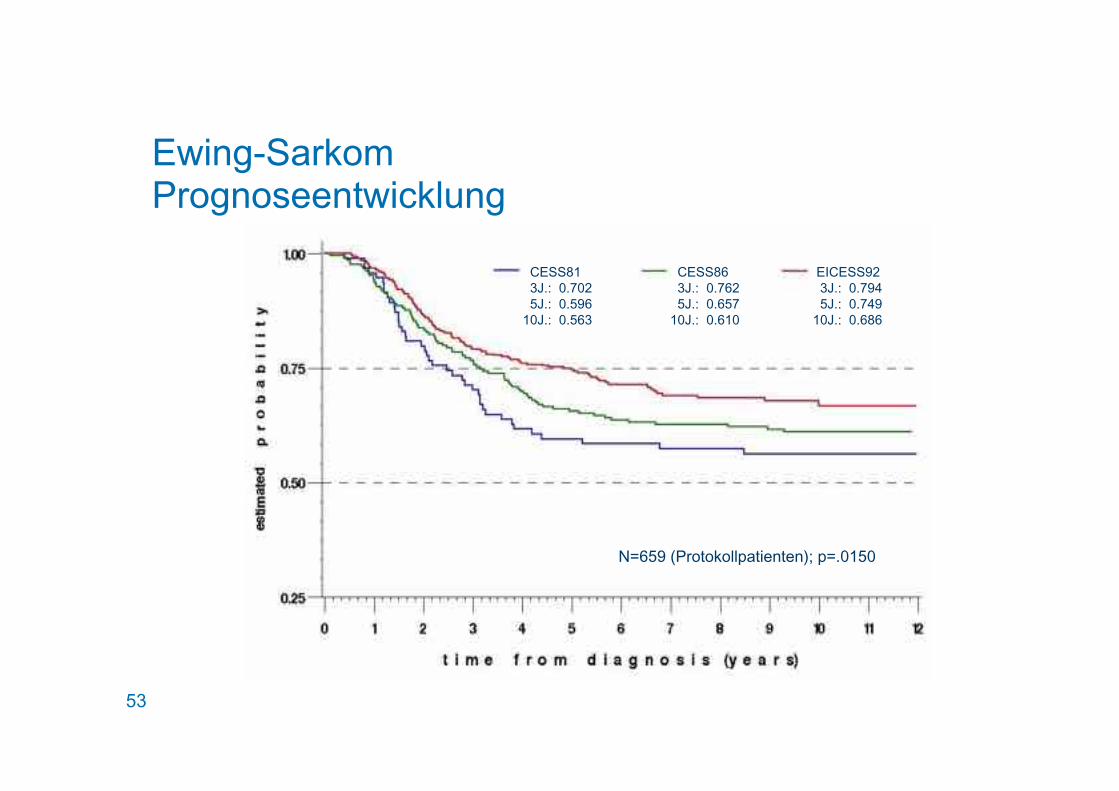
Ewing-Sarkom Prognoseentwicklung
7957 /(): 0 & /+: 0 & /&: 0 & .
57 .): 0 & (+: 0 & +&: 0 & &
57 .): 0 & &(+: 0 & +/&: 0 & + )
3 +/ OM MIMJJNC EL EL 1 N3 & +&
54 DKKR 1997
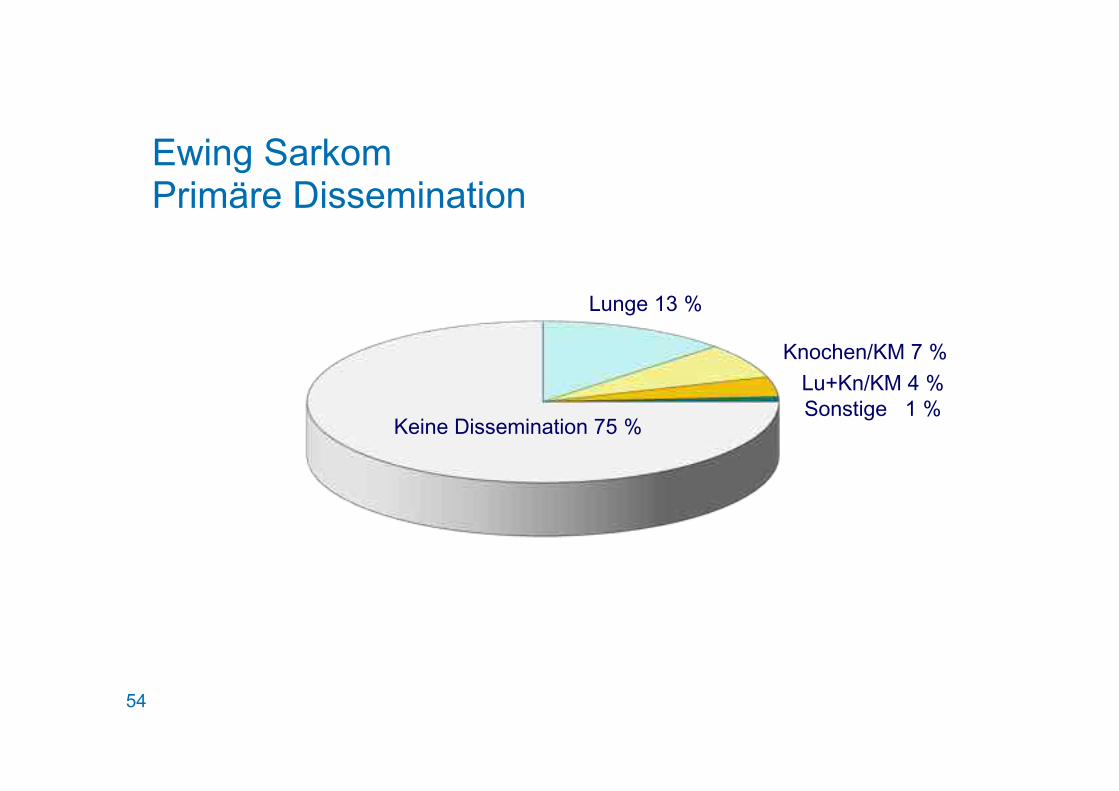
Ewing Sarkom Primäre Dissemination
<R ;L%;=MLP FE
;LMD EL%;=
<RLFE )
;E LE 6 PPEK LC ML +
55
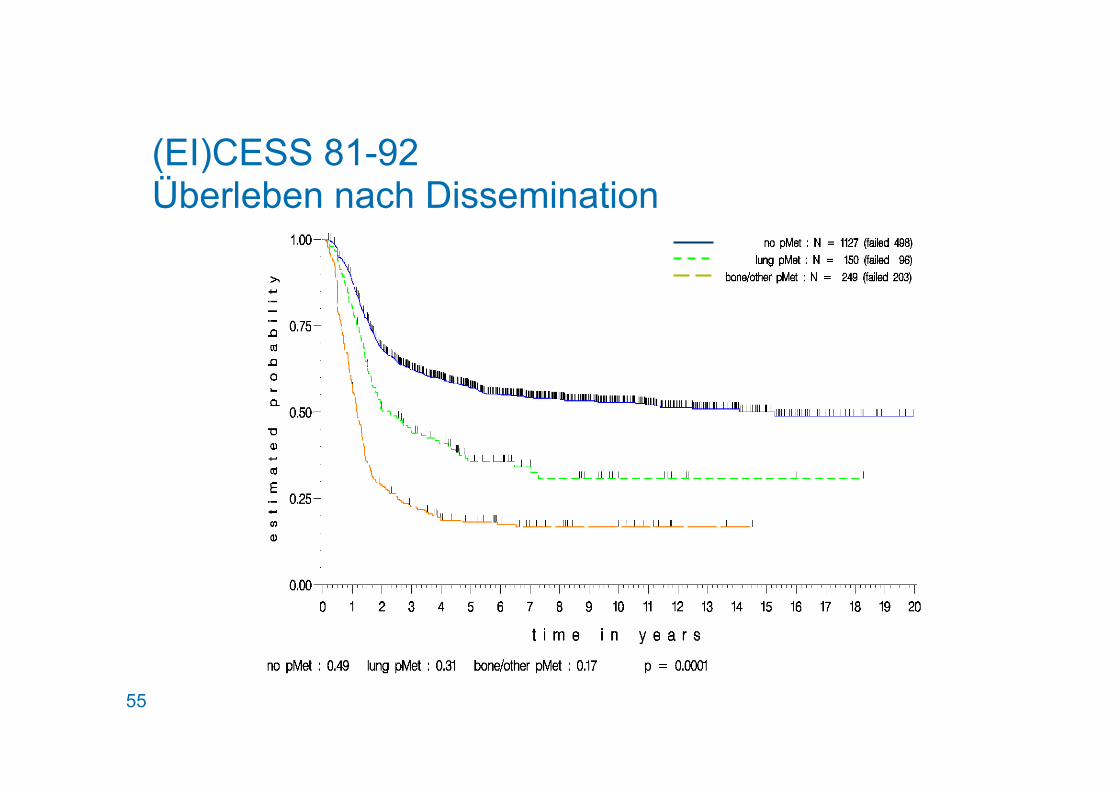
(EI)CESS 81-92 Überleben nach Dissemination

56
57
59
60
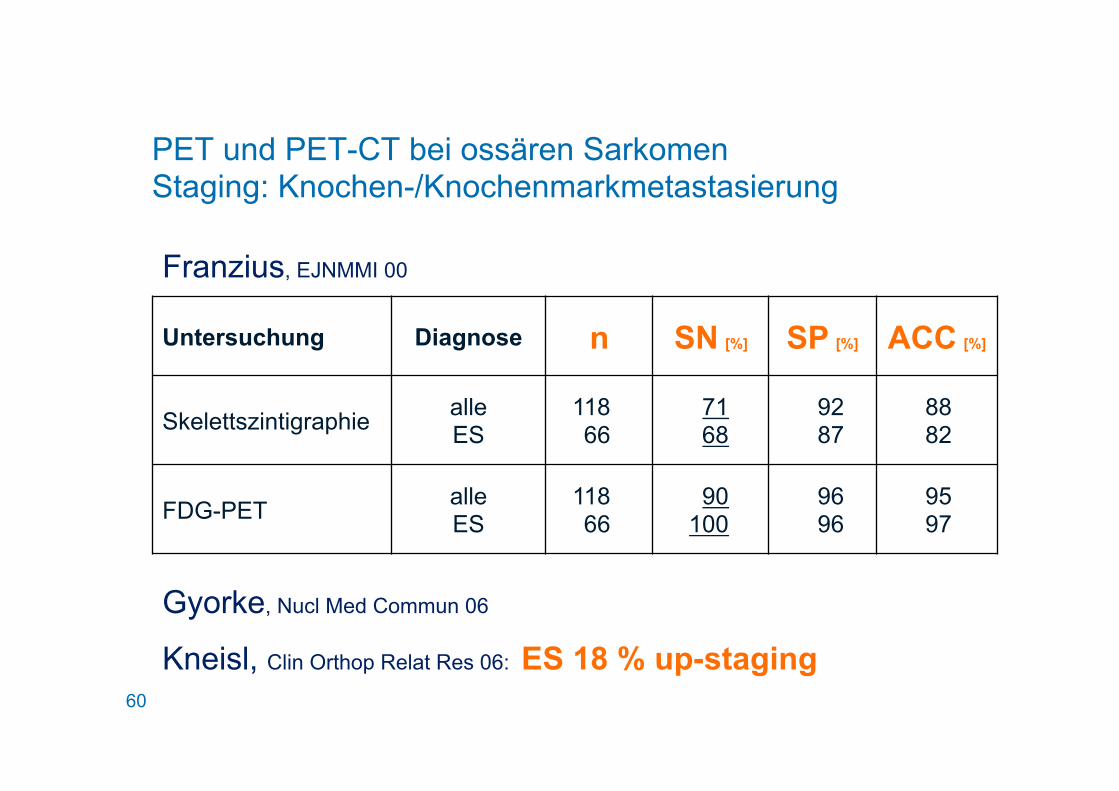
Franzius, EJNMMI 00
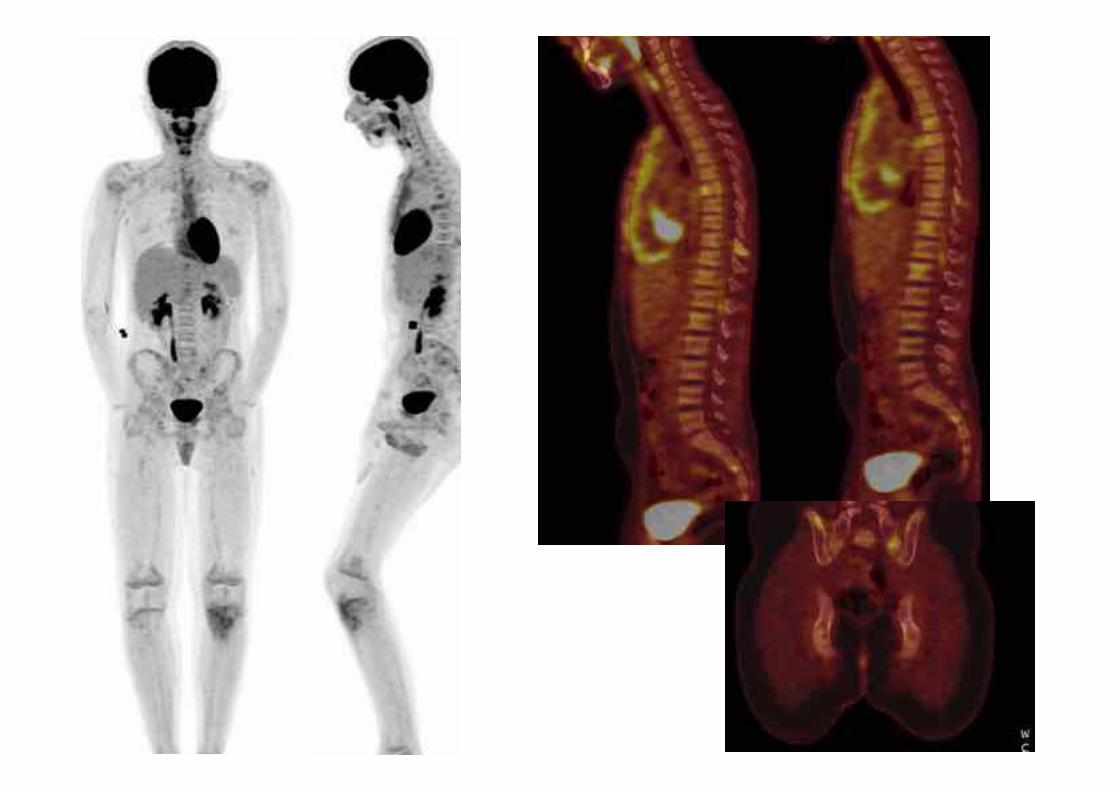
PET und PET-CT bei ossären Sarkomen Staging: Knochen-/Knochenmarkmetastasierung
Untersuchung Diagnose n SN [%] SP [%] ACC [%]
Skelettszintigraphie alle ES
118 66
71 68
92 87
88 82
FDG-PET alle ES
118 66
90 100
96 96
95 97
Gyorke, Nucl Med Commun 06
Kneisl, Clin Orthop Relat Res 06: ES 18 % up-staging
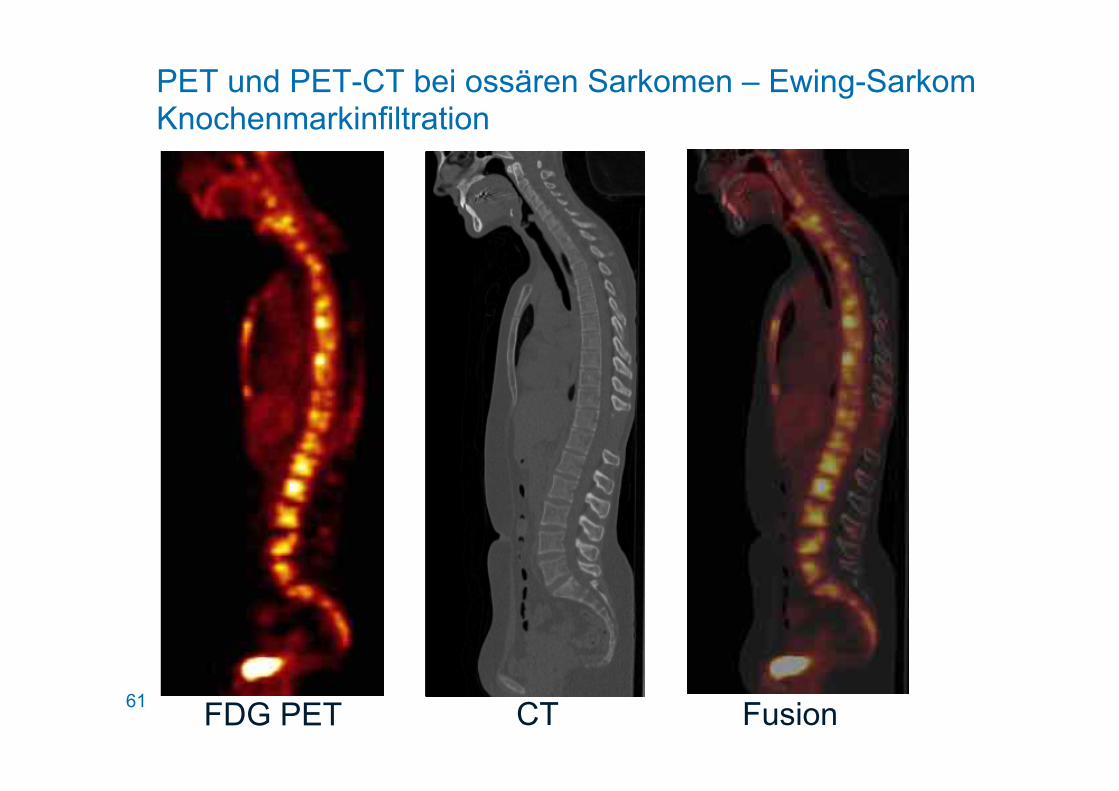
61 FDG PET CT Fusion
PET und PET-CT bei ossären Sarkomen – Ewing-Sarkom Knochenmarkinfiltration
62
Ewing Sarkom Operation oder Bestrahlung
63
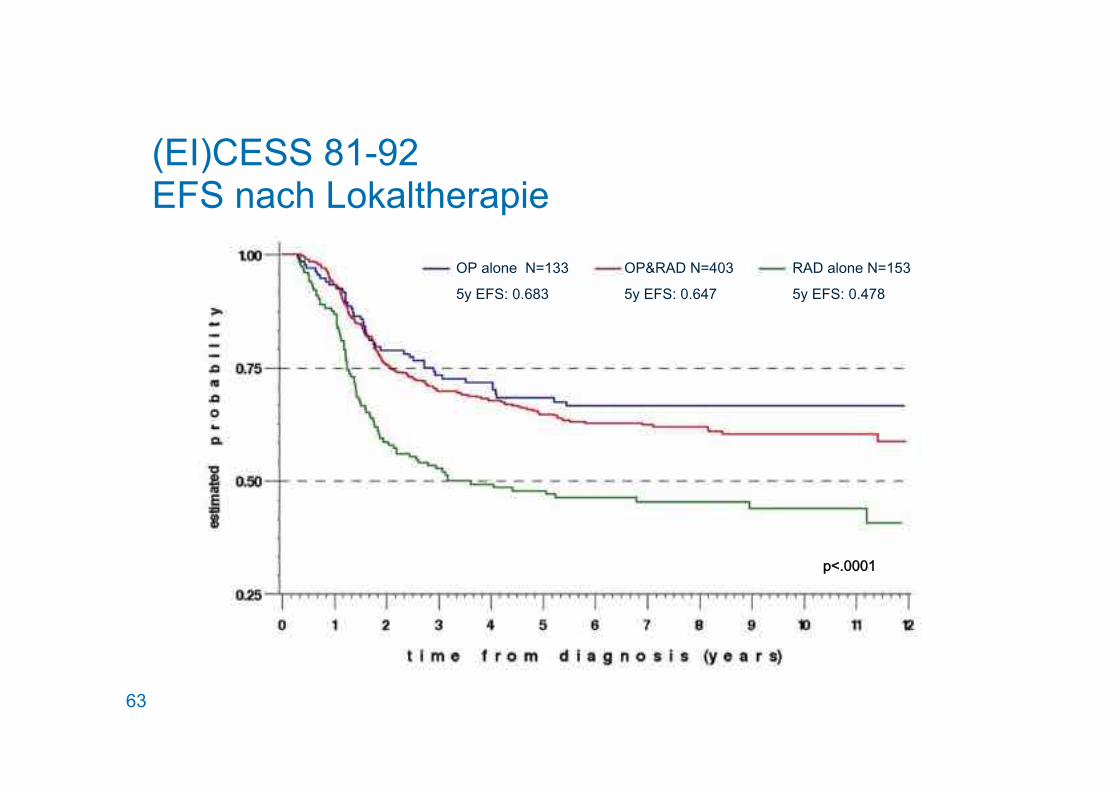
CJMLE 3 ))
+S 78 0 & .)
A46 3 &)
+S 78 0 &
A46 CJMLE 3 +)
+S 78 0 & .
N2 &&&
(EI)CESS 81-92 EFS nach Lokaltherapie
64
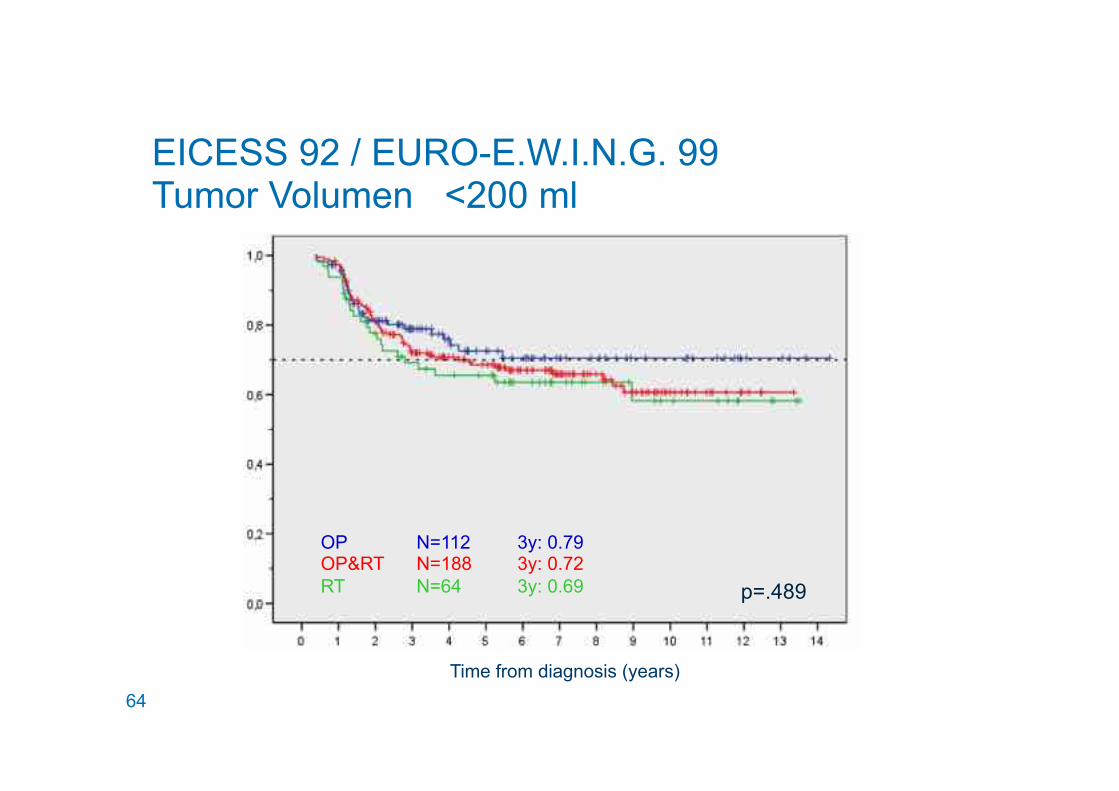
p=.489
OP N=112 3y: 0.79 OP&RT N=188 3y: 0.72 RT N=64 3y: 0.69
Time from diagnosis (years)
EICESS 92 / EURO-E.W.I.N.G. 99 Tumor Volumen <200 ml
65
p<.001
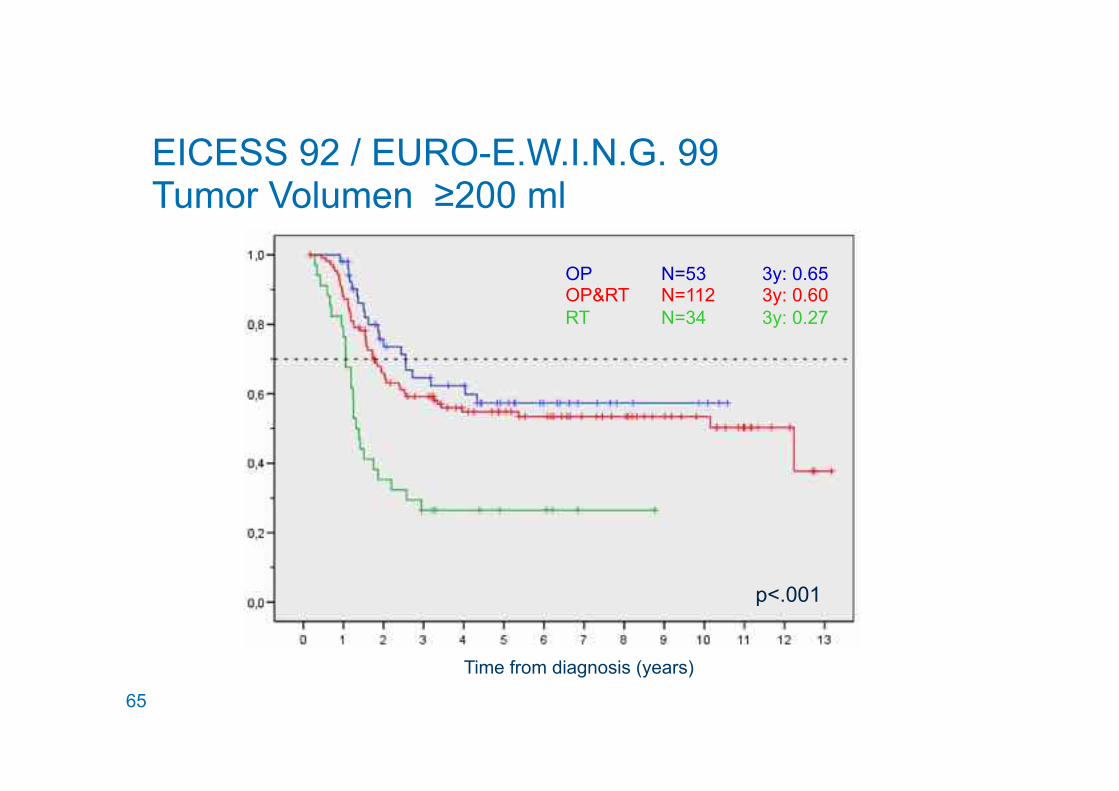
OP N=53 3y: 0.65 OP&RT N=112 3y: 0.60 RT N=34 3y: 0.27
Time from diagnosis (years)
EICESS 92 / EURO-E.W.I.N.G. 99 Tumor Volumen ≥200 ml
66
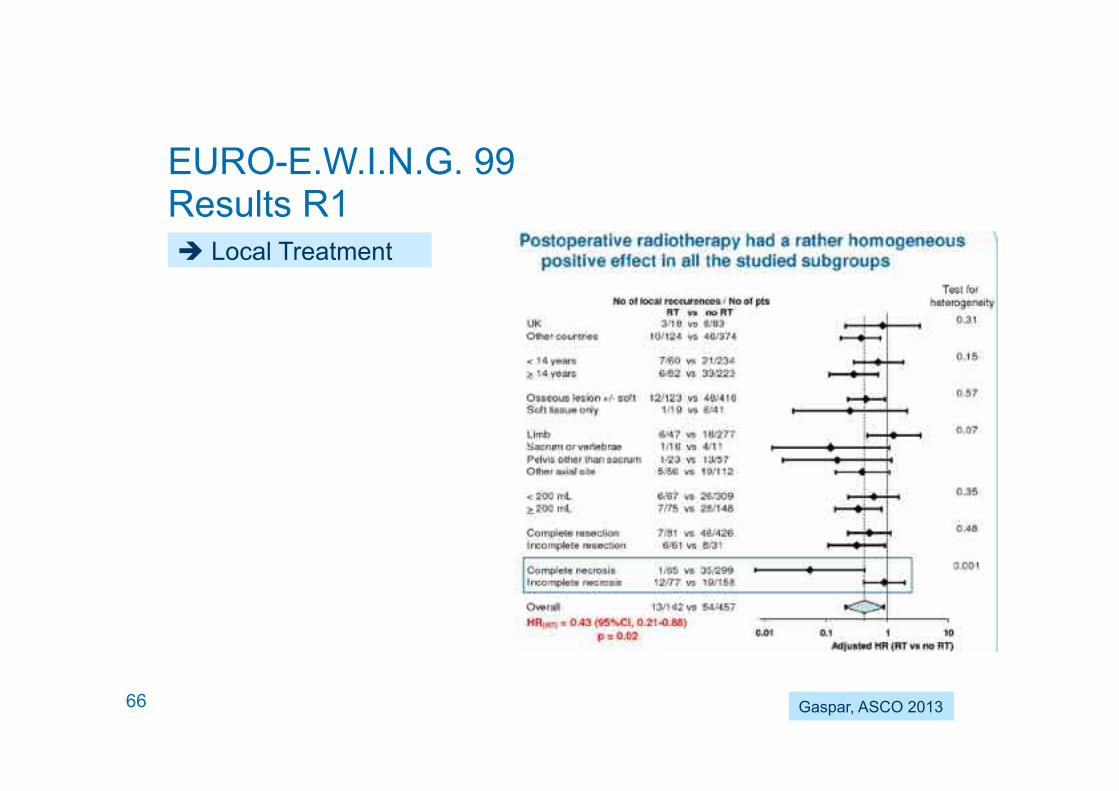
EURO-E.W.I.N.G. 99 Results R1 ! Local Treatment
Gaspar, ASCO 2013
67
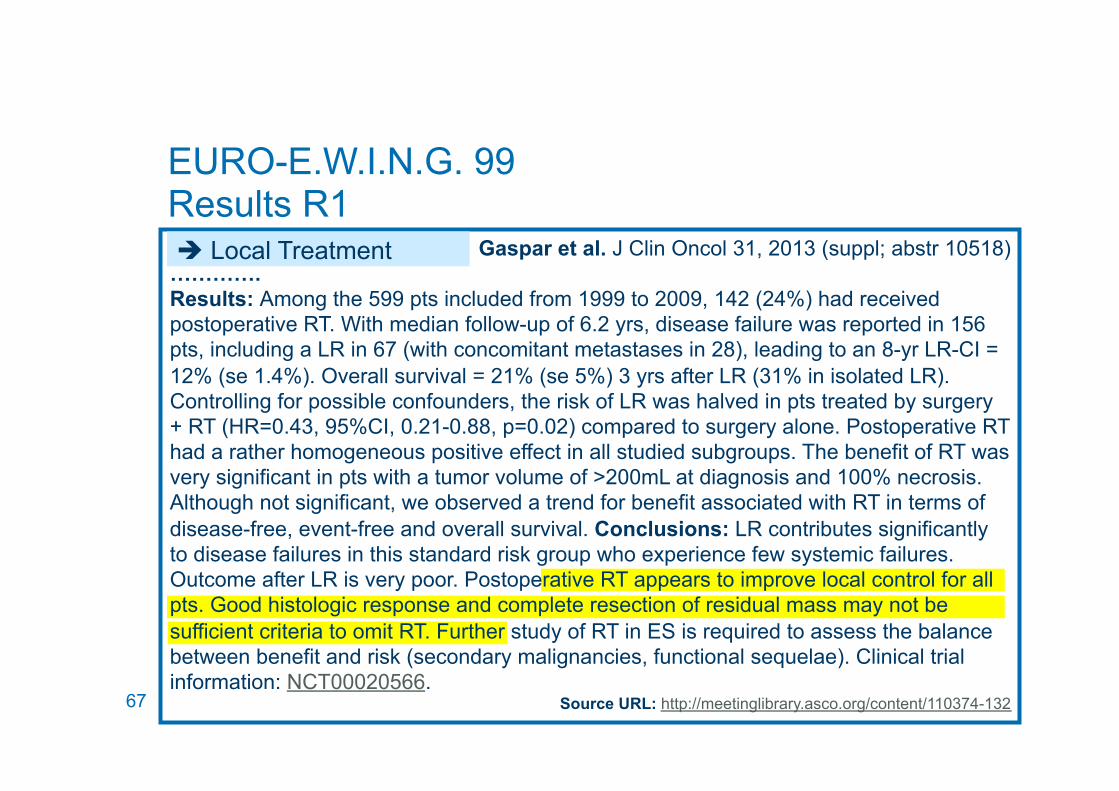
Gaspar et al. J Clin Oncol 31, 2013 (suppl; abstr 10518) …………. Results: Among the 599 pts included from 1999 to 2009, 142 (24%) had received postoperative RT. With median follow-up of 6.2 yrs, disease failure was reported in 156 pts, including a LR in 67 (with concomitant metastases in 28), leading to an 8-yr LR-CI = 12% (se 1.4%). Overall survival = 21% (se 5%) 3 yrs after LR (31% in isolated LR). Controlling for possible confounders, the risk of LR was halved in pts treated by surgery + RT (HR=0.43, 95%CI, 0.21-0.88, p=0.02) compared to surgery alone. Postoperative RT had a rather homogeneous positive effect in all studied subgroups. The benefit of RT was very significant in pts with a tumor volume of >200mL at diagnosis and 100% necrosis. Although not significant, we observed a trend for benefit associated with RT in terms of disease-free, event-free and overall survival. Conclusions: LR contributes significantly to disease failures in this standard risk group who experience few systemic failures. Outcome after LR is very poor. Postoperative RT appears to improve local control for all pts. Good histologic response and complete resection of residual mass may not be sufficient criteria to omit RT. Further study of RT in ES is required to assess the balance between benefit and risk (secondary malignancies, functional sequelae). Clinical trial information: NCT00020566.
Source URL: http://meetinglibrary.asco.org/content/110374-132
EURO-E.W.I.N.G. 99 Results R1 ! Local Treatment

68
WP7 Ewing Sarcoma Trials Multidisciplinary Tumour Board
69
Weichteilsarkome
70
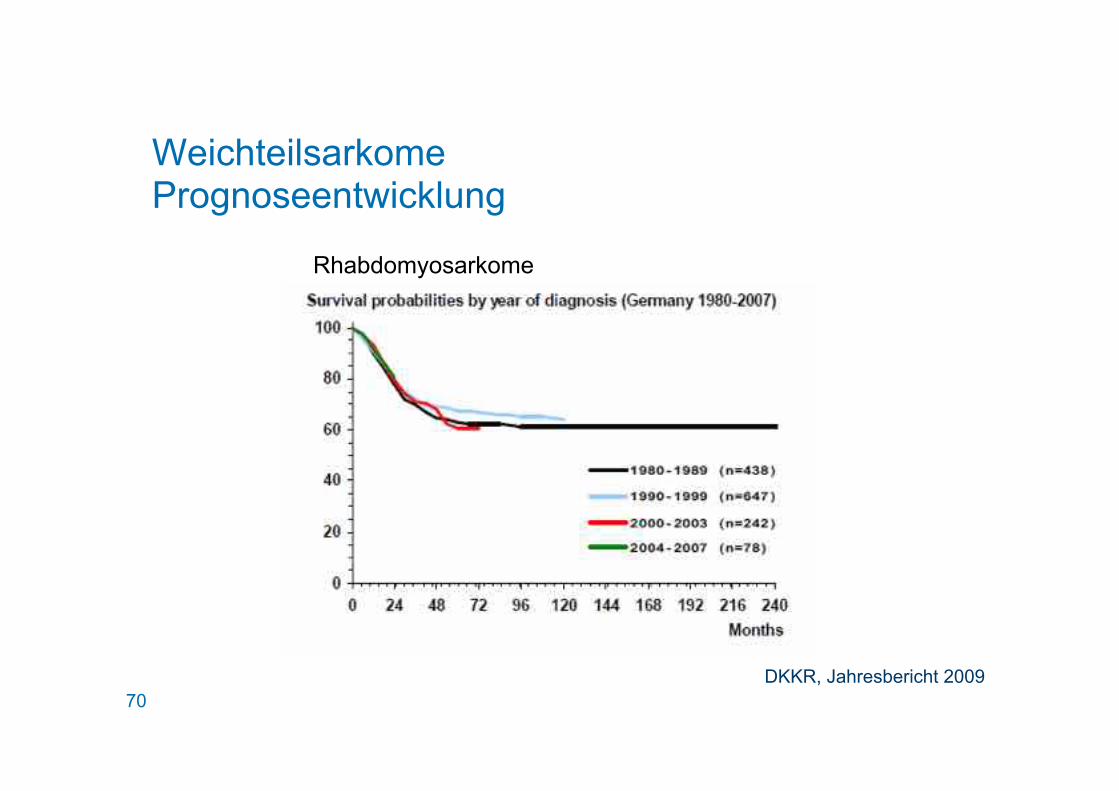
Weichteilsarkome Prognoseentwicklung
Rhabdomyosarkome
DKKR, Jahresbericht 2009
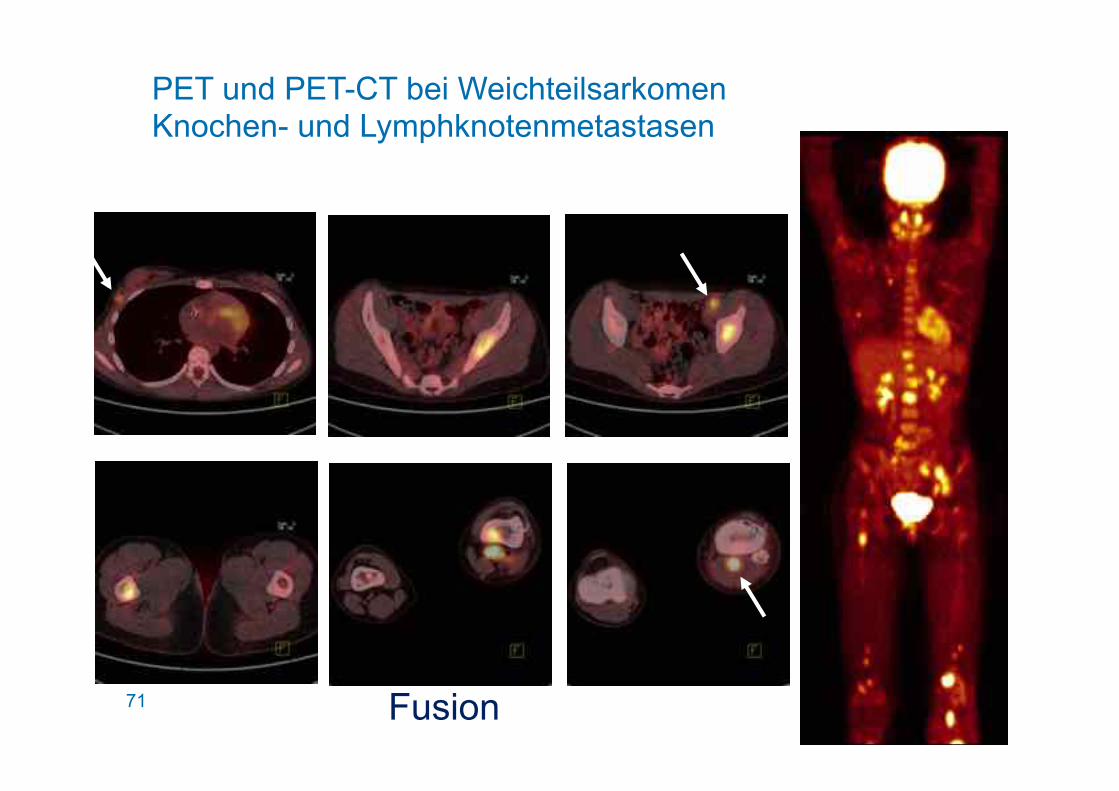
71 Fusion
PET und PET-CT bei Weichteilsarkomen Knochen- und Lymphknotenmetastasen
72
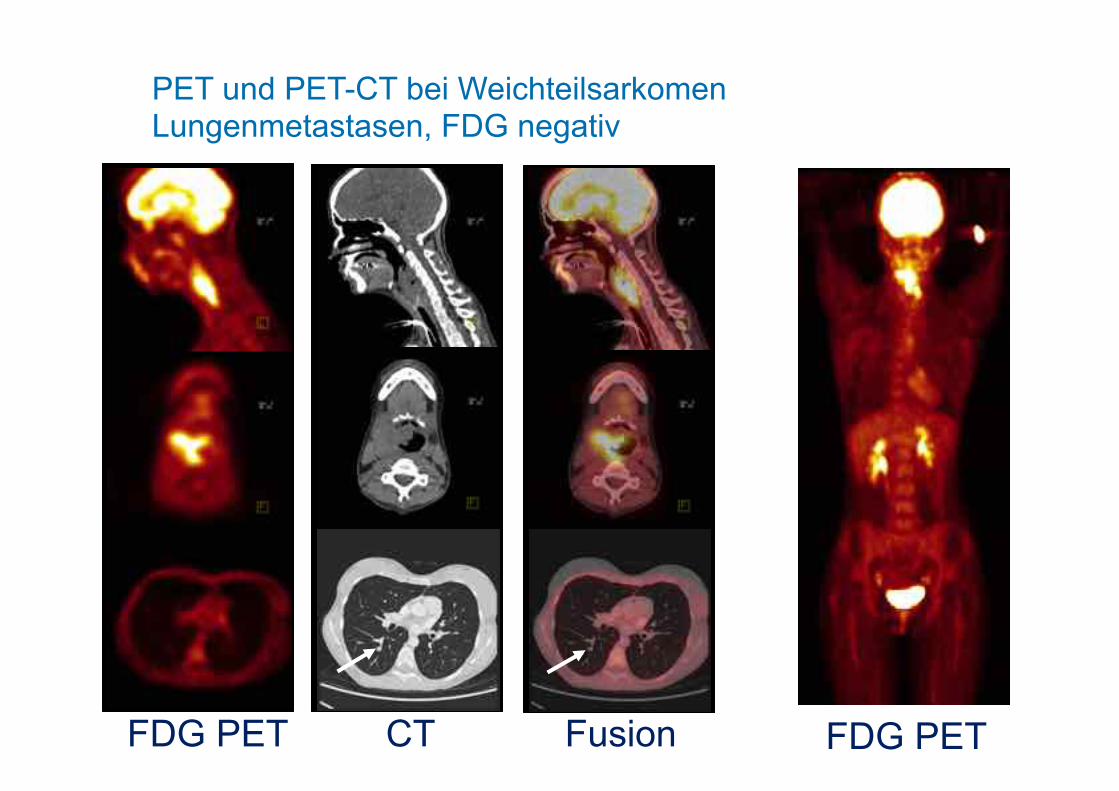
FDG PET CT Fusion FDG PET
PET und PET-CT bei Weichteilsarkomen Lungenmetastasen, FDG negativ
73
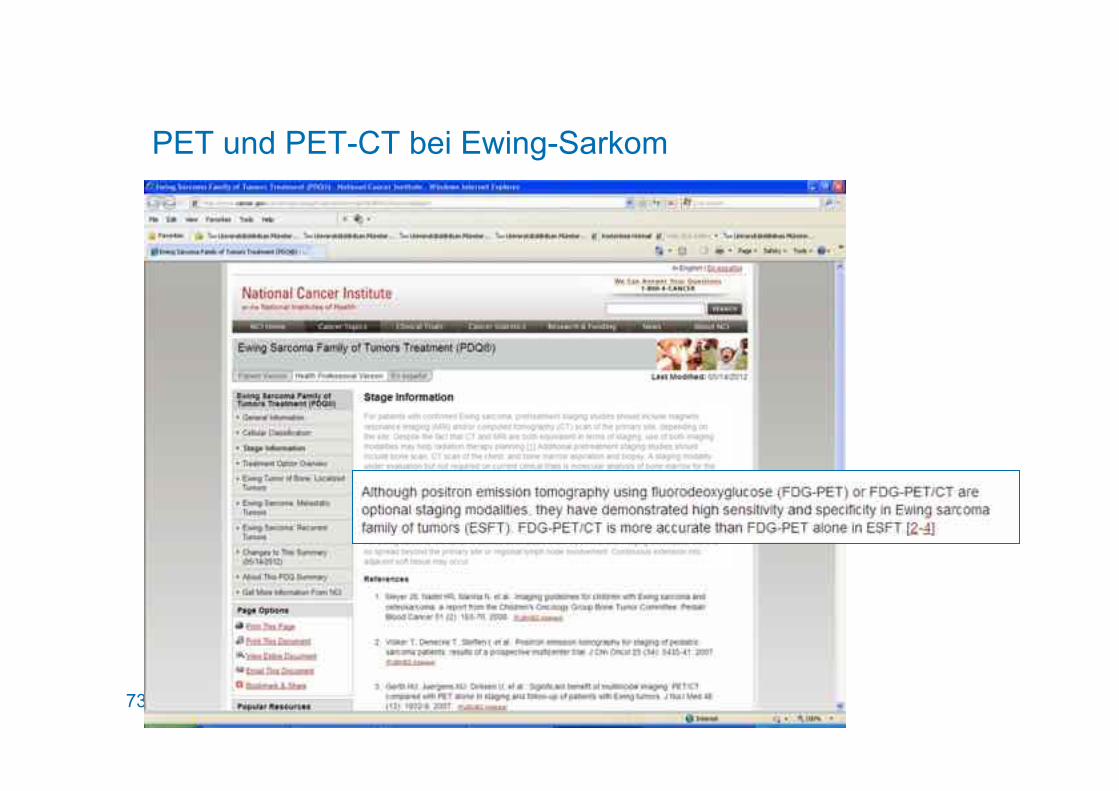
PET und PET-CT bei Ewing-Sarkom
74
Osteosarcoma
Whole body MDP bone scintigraphy, FDG-PET Recommended
Ewing Sarcoma
Whole body MDP bone scintigraphy, FDG-PET Recommended
"..
.."

75
PET und PET-CT bei Knochen- und Weichteilsarkomen Zusammenfassung
Ewing-Sarkom
• Standard der Initial- und Verlaufsdiagnostik
Osteosarkom
• Wenig Evidenz für zusätzlichen Informationsgewinn
• Unter Umständen Vorteile in der Verlaufsdiagnostik und bei Dissemination
Weichteilsarkom
• Stellenwert in der Diagnostik bei Lymphknoten- und Skelettmetastasierung
76
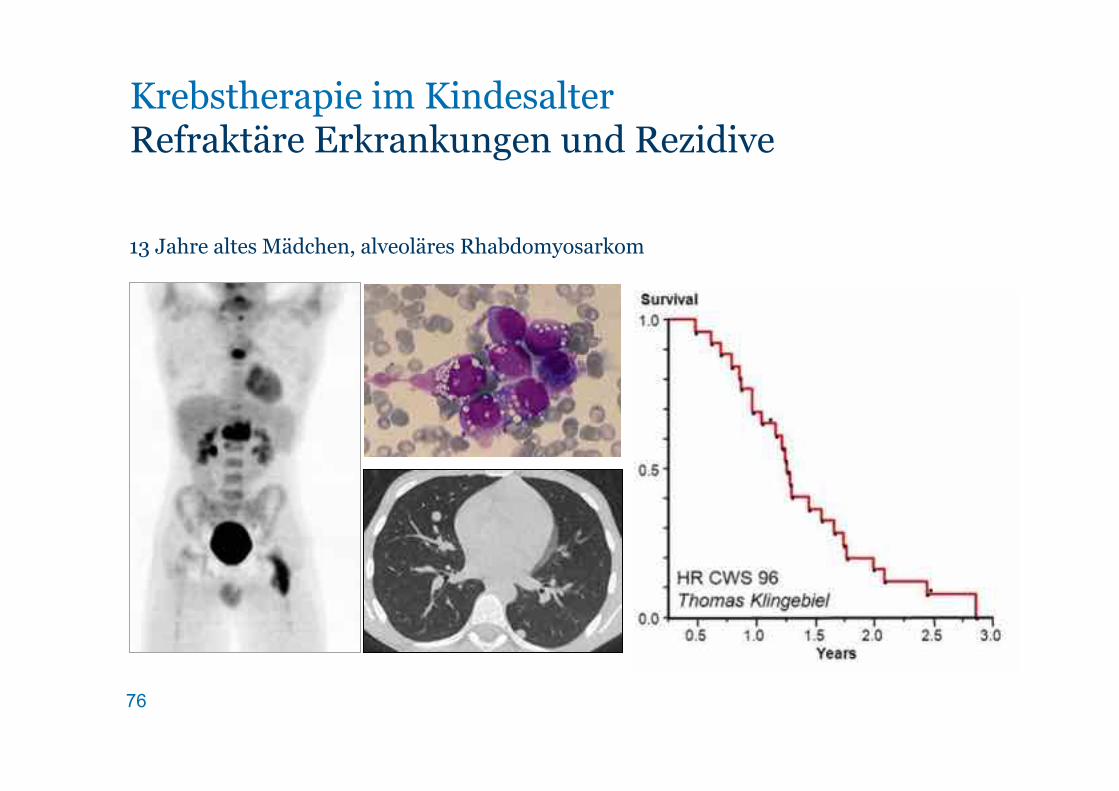
13 Jahre altes Mädchen, alveoläres Rhabdomyosarkom
Krebstherapie im Kindesalter Refraktäre Erkrankungen und Rezidive

77
Neue Therapien Stellenwert und Kombination
78
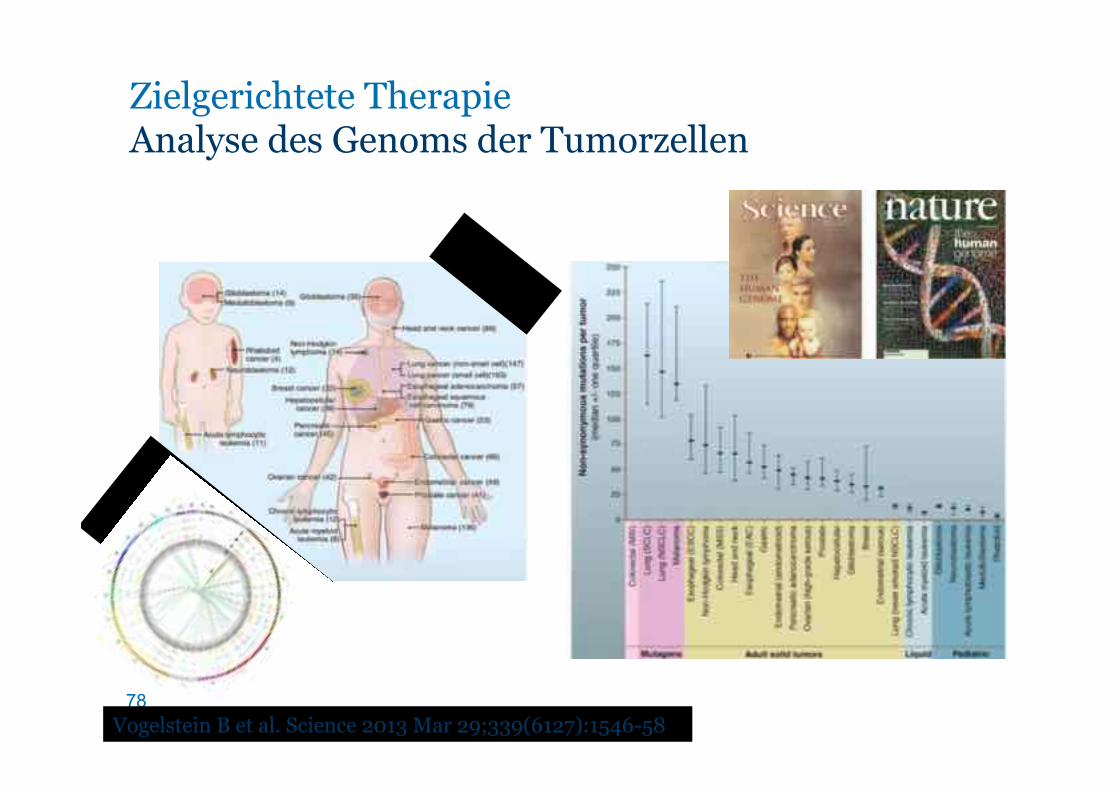
Zielgerichtete Therapie Analyse des Genoms der Tumorzellen
Vogelstein B et al. Science 2013 Mar 29;339(6127):1546-58
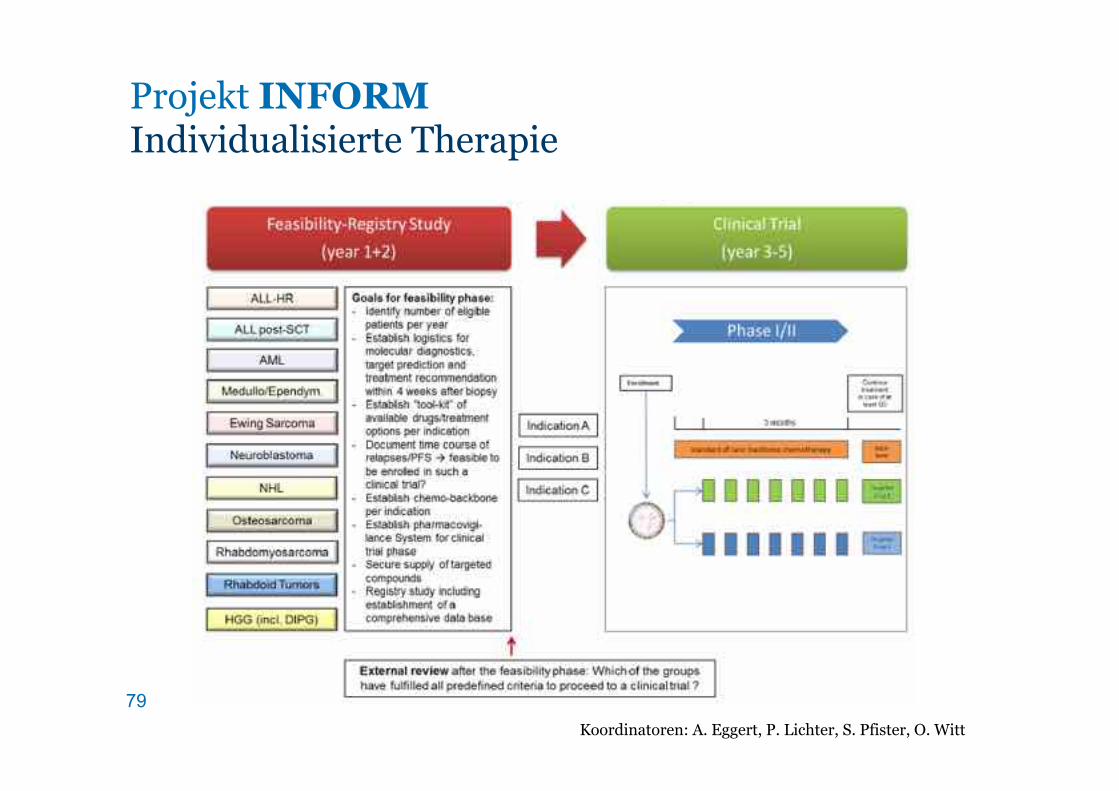
79 Koordinatoren: A. Eggert, P. Lichter, S. Pfister, O. Witt
Projekt INFORM Individualisierte Therapie
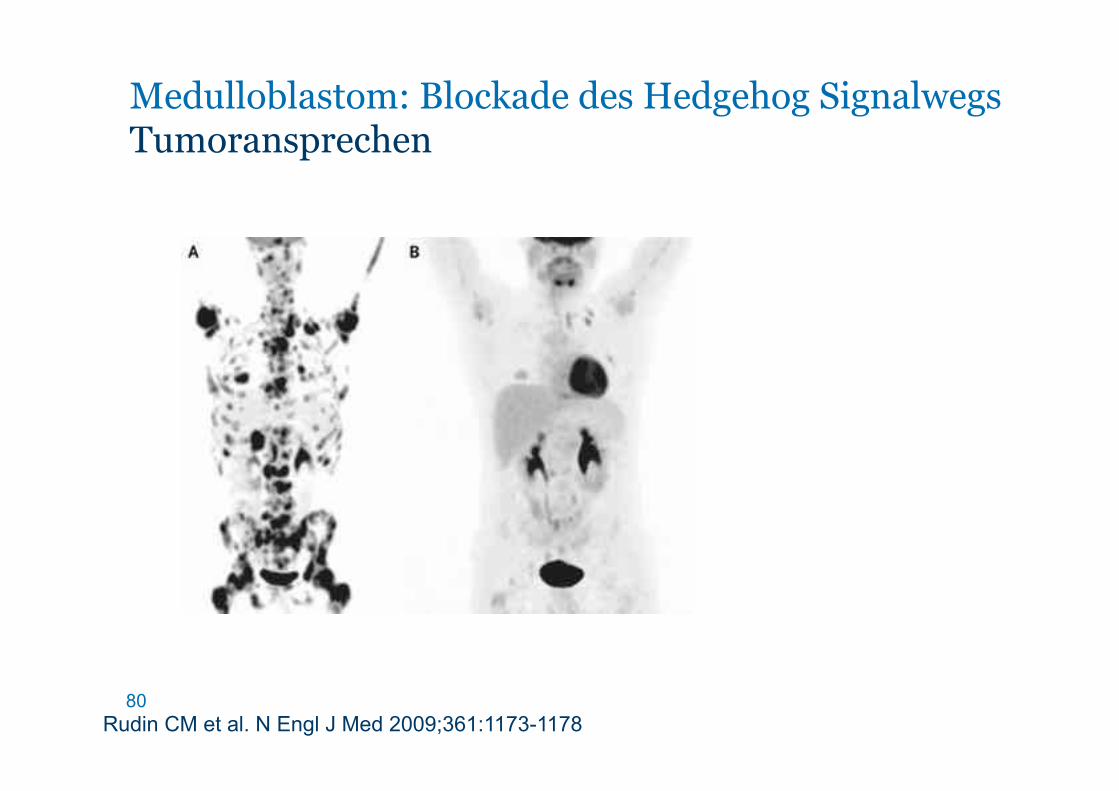
80 Rudin CM et al. N Engl J Med 2009;361:1173-1178
Medulloblastom: Blockade des Hedgehog Signalwegs Tumoransprechen
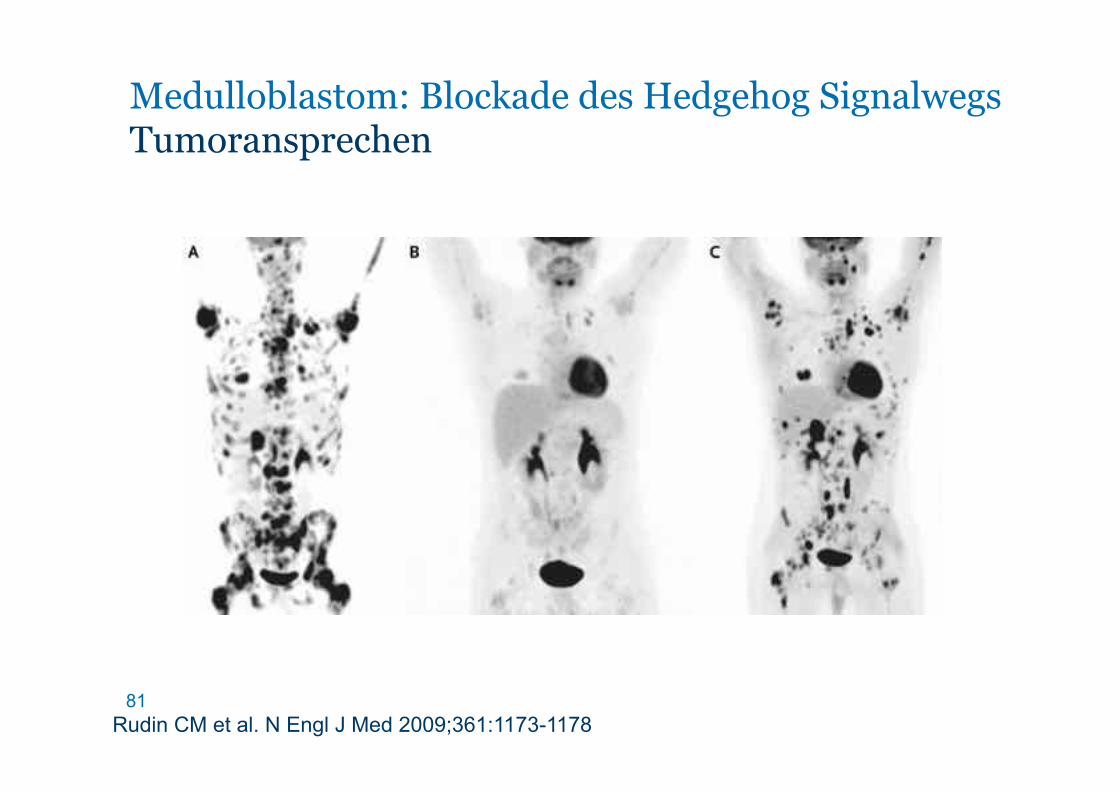
81
Medulloblastom: Blockade des Hedgehog Signalwegs Tumoransprechen
Rudin CM et al. N Engl J Med 2009;361:1173-1178

Tolcher AW et al. ASCO 2007
Zielgerichtete Therapie IGFR-1 Antikörper bei Ewing-Sarkomen
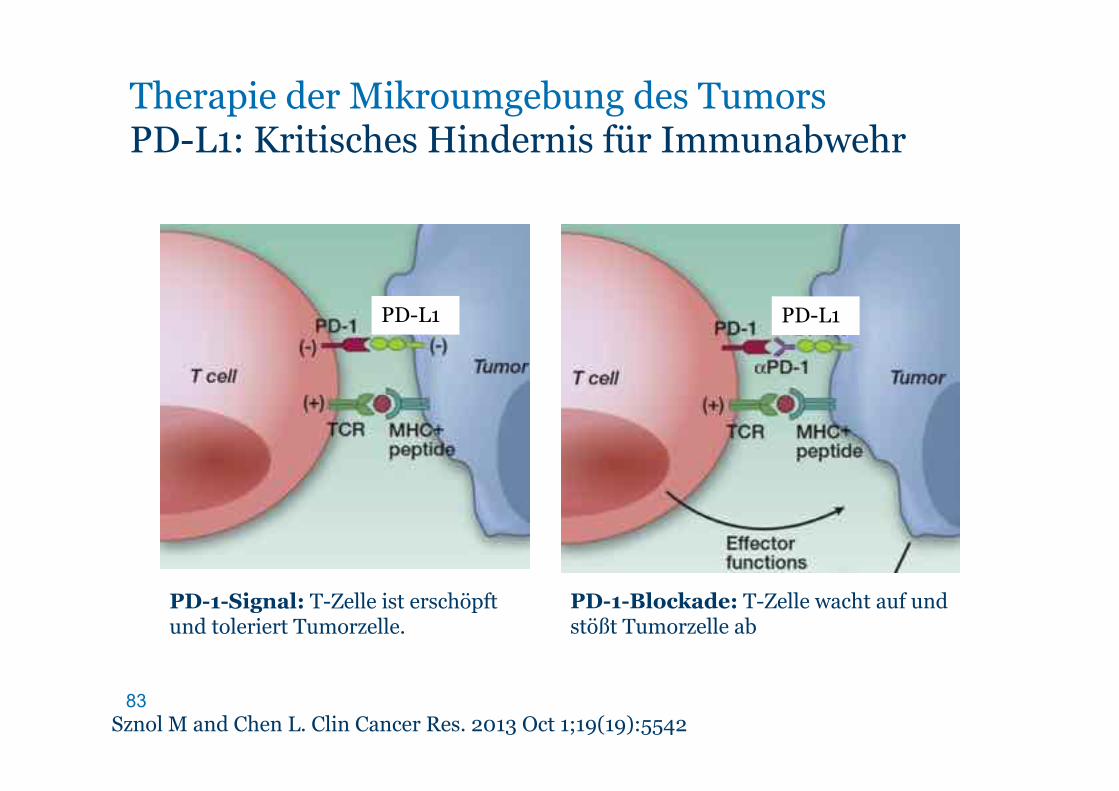
83 Sznol M and Chen L. Clin Cancer Res. 2013 Oct 1;19(19):5542
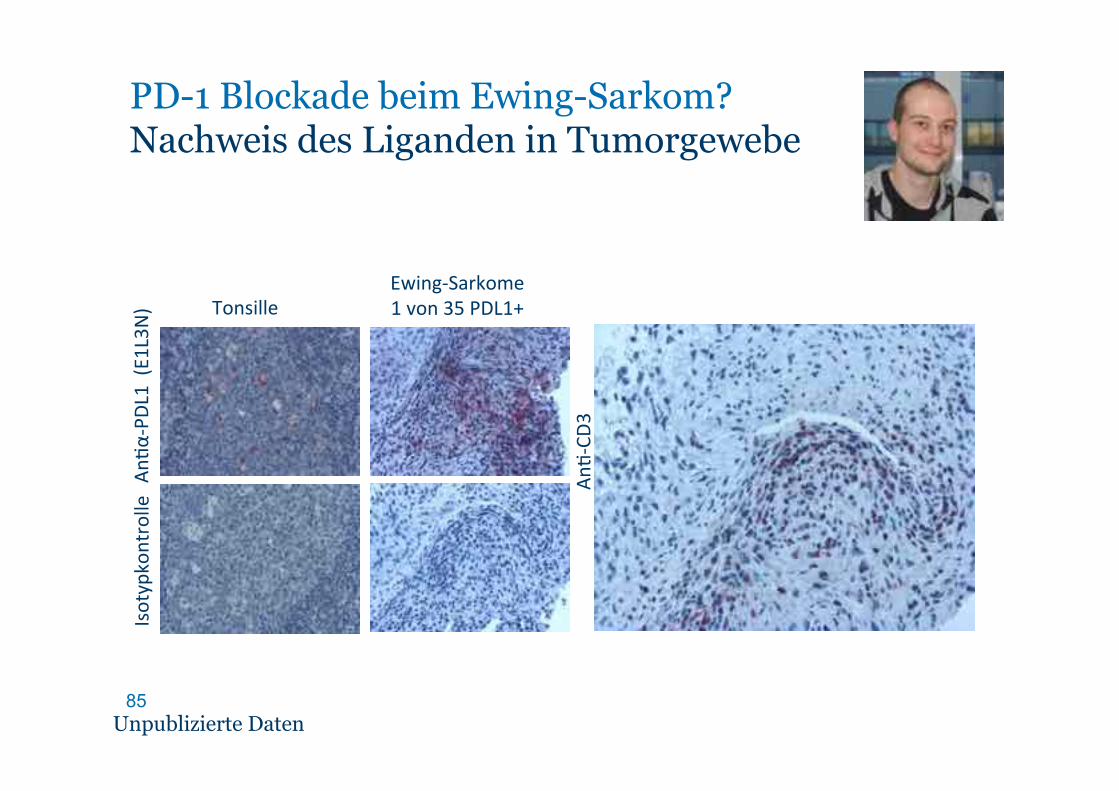
Therapie der Mikroumgebung des Tumors PD-L1: Kritisches Hindernis für Immunabwehr
PD-1-Signal: T-Zelle ist erschöpft und toleriert Tumorzelle.
PD-1-Blockade: T-Zelle wacht auf und stößt Tumorzelle ab
PD-L1 PD-L1
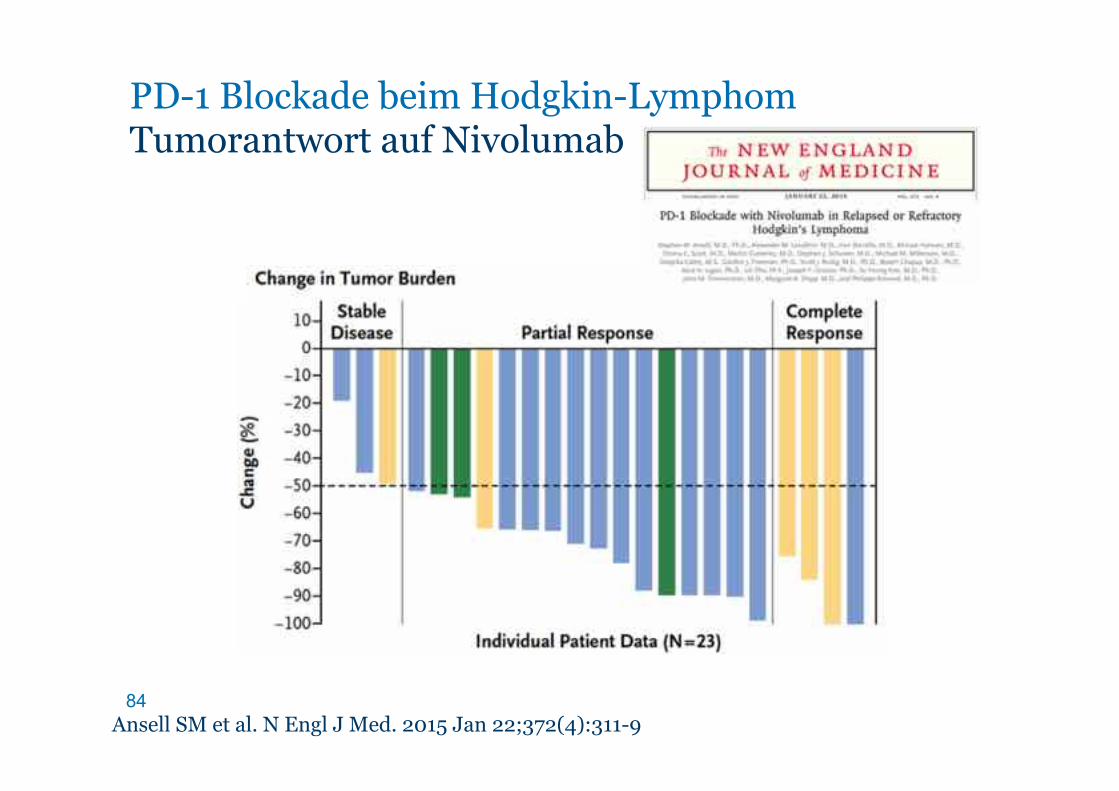
84 Ansell SM et al. N Engl J Med. 2015 Jan 22;372(4):311-9
PD-1 Blockade beim Hodgkin-Lymphom Tumorantwort auf Nivolumab
85
Tonsille Ewing6Sarkome'1'von'35'PDL1+'
An4α
6PDL
1''(E
1L3N
) Isotypkontrolle
An46CD
3
Unpublizierte Daten
PD-1 Blockade beim Ewing-Sarkom? Nachweis des Liganden in Tumorgewebe
86
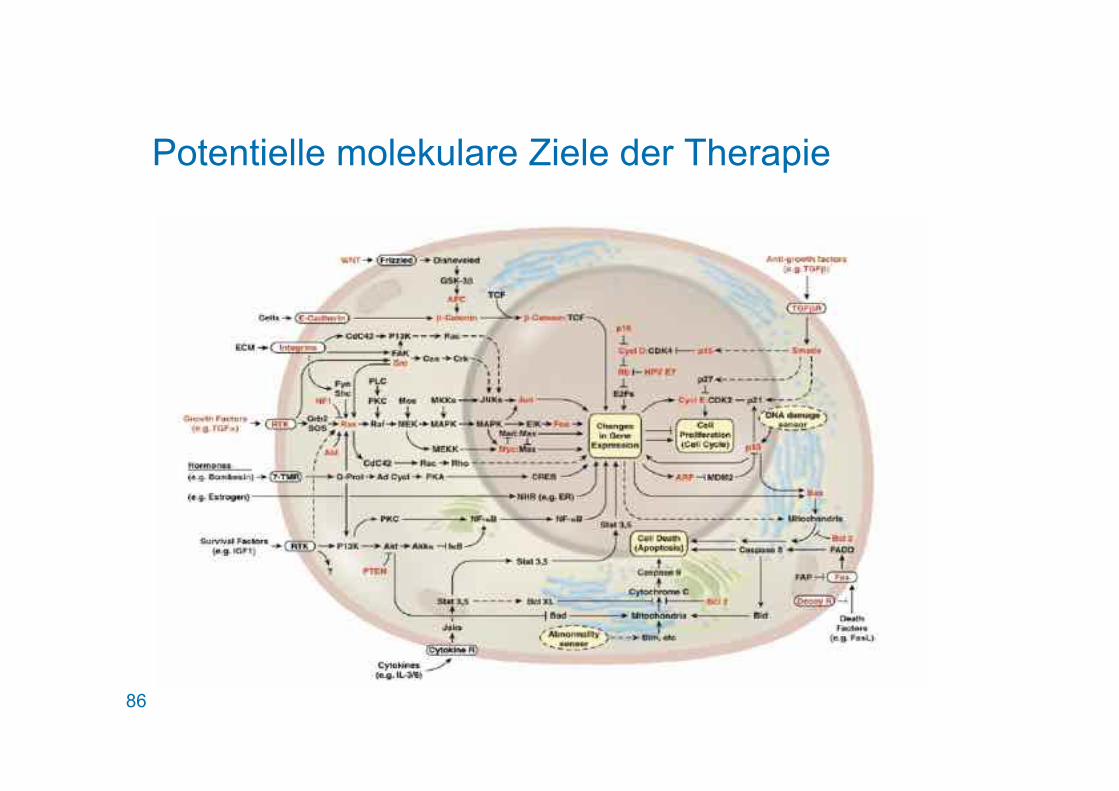
Potentielle molekulare Ziele der Therapie
Blockade tumorassoziierter Signalwege Resistenz
88
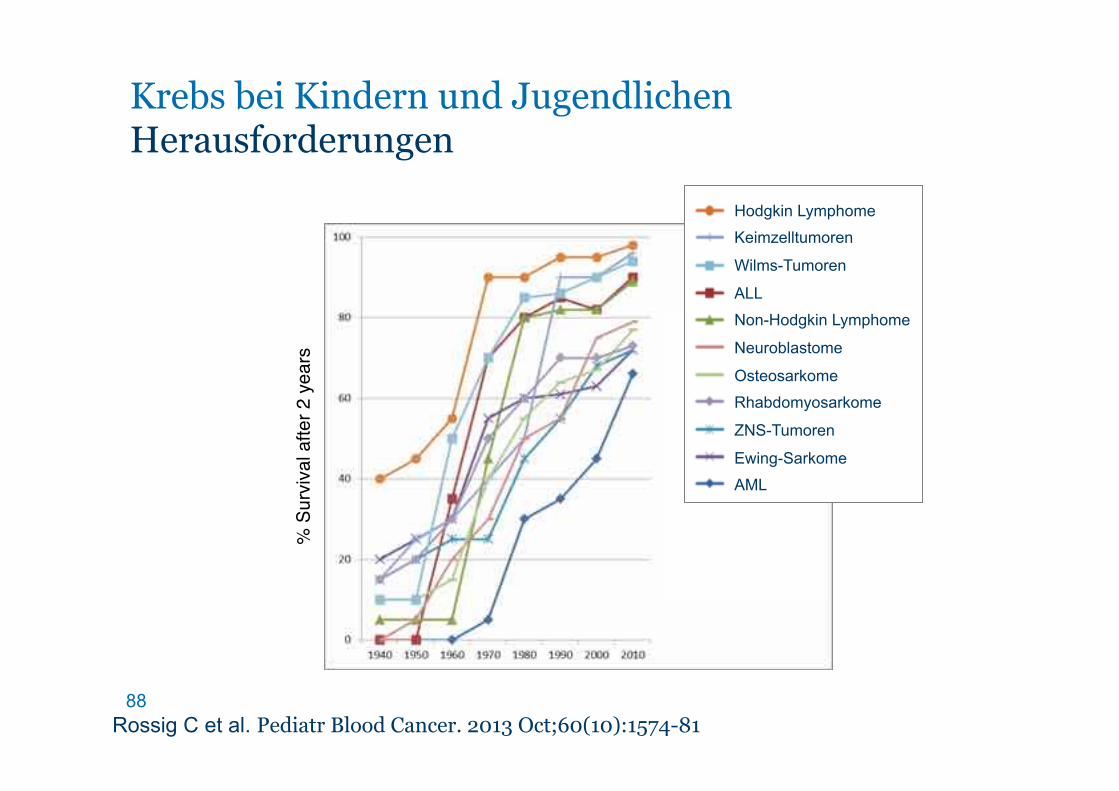
% S
urvi
val a
fter 2
yea
rs
Rossig C et al. Pediatr Blood Cancer. 2013 Oct;60(10):1574-81
Krebs bei Kindern und Jugendlichen Herausforderungen
Hodgkin Lymphome
Keimzelltumoren
Wilms-Tumoren
ALL
Non-Hodgkin Lymphome
Neuroblastome
Osteosarkome
Rhabdomyosarkome
ZNS-Tumoren
Ewing-Sarkome
AML

89

90