Seltene Nierenerkrankungen bei Kinder und Erwachsenen · H.W. Seyberth, Zentrum für Kinder- und...
41
H.W. H.W. Seyberth Seyberth , , Zentrum f Zentrum für Kinder Kinder- und und Jugendmedizin Jugendmedizin , , Philipps Universit Philipps Universität Marburg Marburg und und Kommission Kommission für Arzneimittelsicherheit im Kindesalter Arzneimittelsicherheit im Kindesalter (KASK) (KASK) der der DGKJ DGKJ PMS PMS- Workshop: Workshop: Arzneimittel seltener Krakheiten Arzneimittel seltener Krakheiten – Herausforderungen Herausforderungen und und Chancen Chancen 25. 25. Januar Januar 2007 Berlin 2007 Berlin- Brandenburgische Akademie der Wissenschaften Brandenburgische Akademie der Wissenschaften Heriditäre Salzverlust-Tubulopathien mit sekundären Hyperaldosteronismus : Seltene Nierenerkrankungen bei Kinder und Erwachsenen Heriditäre Salzverlust-Tubulopathien mit sekundären Hyperaldosteronismus : Seltene Nierenerkrankungen bei Kinder und Erwachsenen
Transcript of Seltene Nierenerkrankungen bei Kinder und Erwachsenen · H.W. Seyberth, Zentrum für Kinder- und...

H.W. H.W. SeyberthSeyberth, , Zentrum fZentrum füürr KinderKinder-- und und JugendmedizinJugendmedizin, , Philipps UniversitPhilipps Universitäätt Marburg Marburg
undundKommissionKommission ffüürr Arzneimittelsicherheit im KindesalterArzneimittelsicherheit im Kindesalter (KASK) (KASK) der der DGKJDGKJ
PMSPMS--Workshop:Workshop:Arzneimittel seltener Krakheiten Arzneimittel seltener Krakheiten –– Herausforderungen Herausforderungen und und ChancenChancen
25. 25. Januar Januar 2007 Berlin2007 Berlin--Brandenburgische Akademie der WissenschaftenBrandenburgische Akademie der Wissenschaften
Heriditäre Salzverlust-Tubulopathien
mit sekundären Hyperaldosteronismus :
Seltene Nierenerkrankungen bei Kinder und Erwachsenen
Heriditäre Salzverlust-Tubulopathien
mit sekundären Hyperaldosteronismus :
Seltene Nierenerkrankungen bei Kinder und Erwachsenen
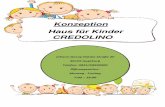
GIII/PII; current gestational age: 32 + 0 weeks, amniotic fluidGIII/PII; current gestational age: 32 + 0 weeks, amniotic fluid volume about 15 lvolume about 15 lPolyhydramniosPolyhydramnios started to develop in the 22nd week of gestationstarted to develop in the 22nd week of gestation


Bladder
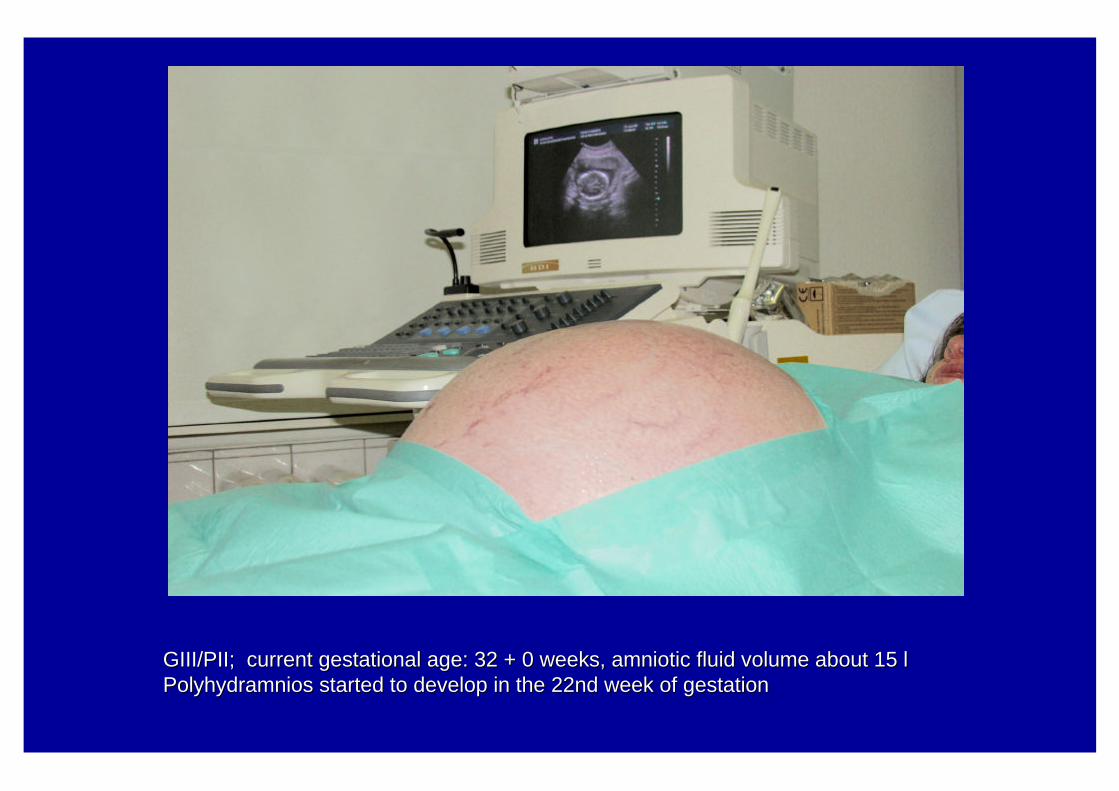
after amniocentesis with drainage of 3 L fluidafter amniocentesis with drainage of 3 L fluidChloride concentration 116 Chloride concentration 116 mM mM (normal up to 112 (normal up to 112 mMmM))

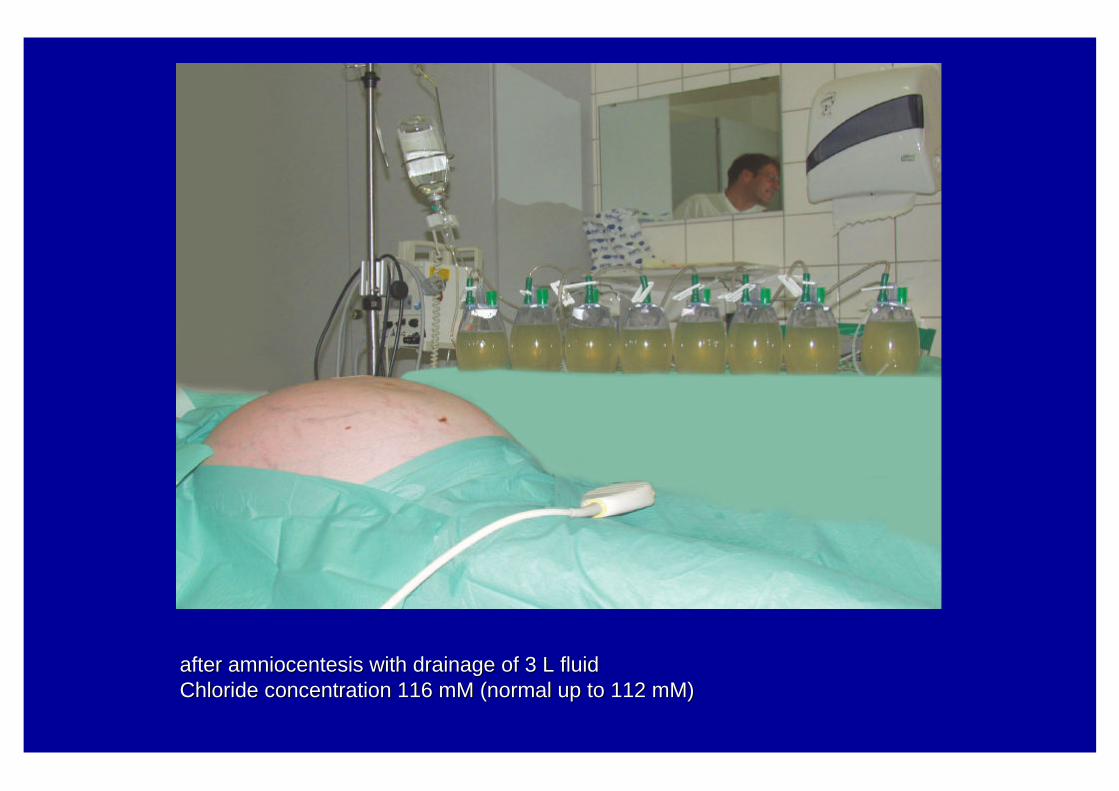
Diuresis [ml/kg/h]
IndomethacinIndomethacin reduces reduces polyuriapolyuria in in HyperprostaglandinHyperprostaglandin E SyndromeE Syndrome
0
10
20
30
40
50
48h 96h 120h
postnatal age
PGE2-excretion[ng/h/1,73 m2]
400
200
upper normallimit
Indomethacin 0.5 mg/kg/d
Komhoff et al, 2005, Acta Paed

Sodium-Potassium-Switch in HPS
0
40
80
120
160
Age [weeks]
Uri
ne
con
cen
trat
ion
[m
M]
0 1 2 3 4
K+
Na+
Reinalter et al. 1998, Pediatr Nephrol
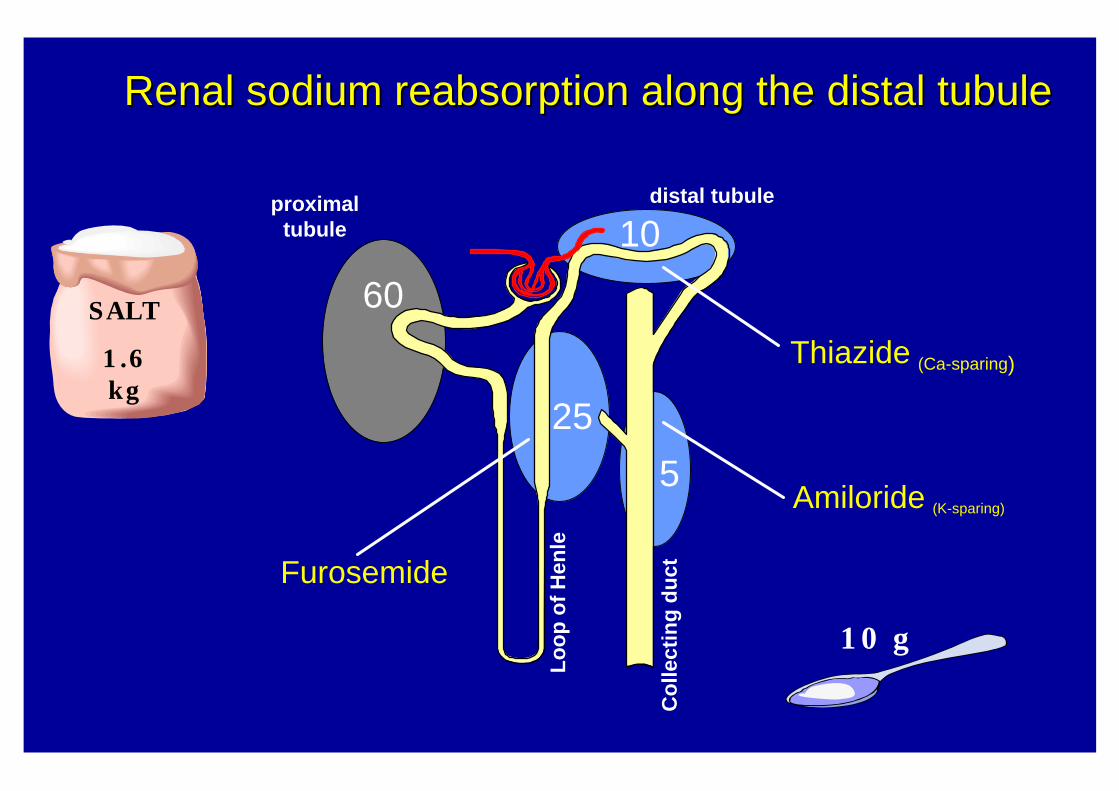
25
10
5
60
Co
llect
ing
du
ct
Lo
op
of
Hen
le
distal tubuleproximaltubule
Thiazide (Ca-sparing)
Amiloride (K-sparing)
Furosemide
Renal sodium Renal sodium reabsorptionreabsorption along the distal tubulealong the distal tubule
SALT
1.6 kg
10 g
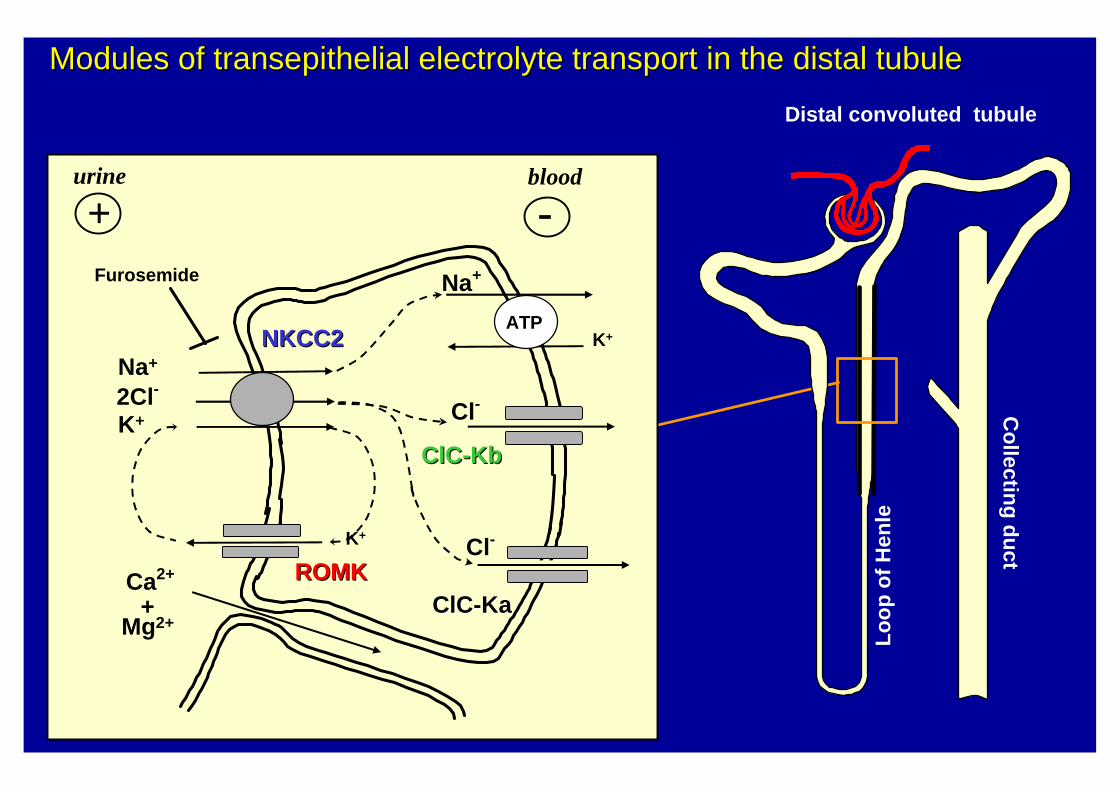
Distal convoluted tubule
urine blood
K+
Na+
ATP
Na+
2Cl-
Furosemide
K+
NKCC2NKCC2
K+
ROMKROMK
Cl-
ClCClC--KbKb
Cl-
ClCClC--KaKa
+ -
Modules of Modules of transepithelialtransepithelial electrolyte transport in the distal tubuleelectrolyte transport in the distal tubuleC
ollectin
g d
uct
Lo
op
of
Hen
le
Ca2+
+Mg2+
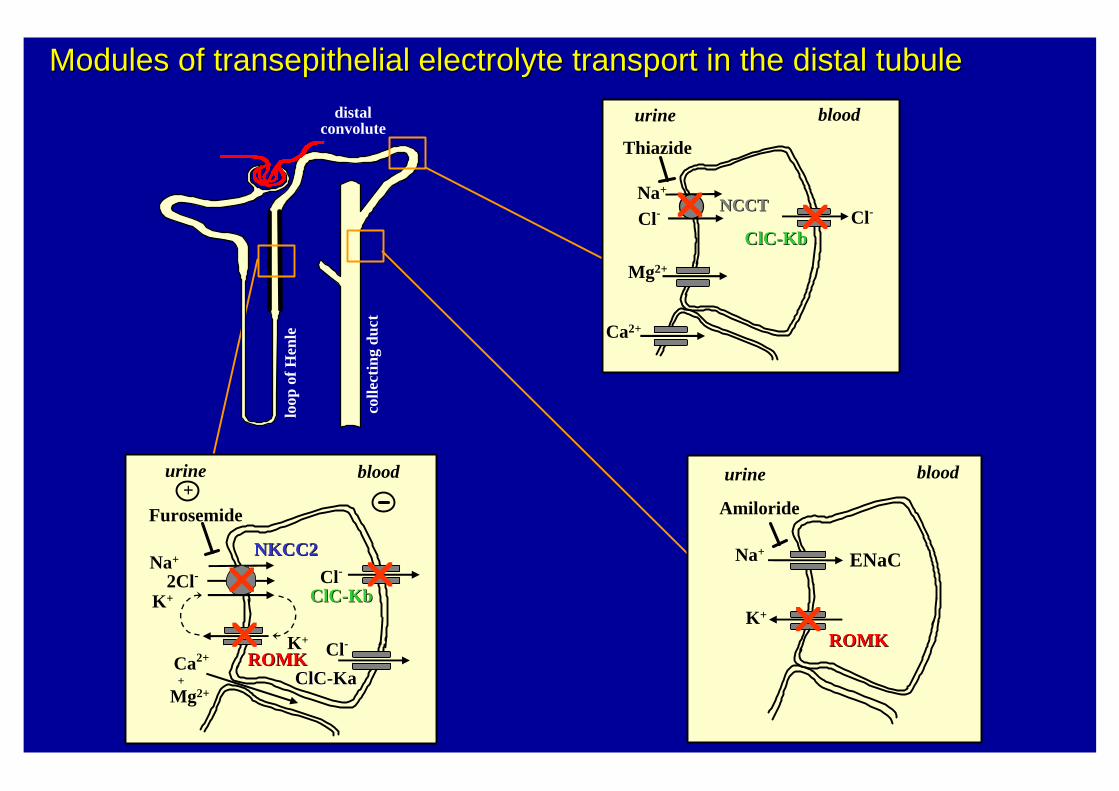
colle
ctin
g du
ct
loop
of H
enle
distalconvolute
K+
ROMKROMK
Na+
2Cl-
Furosemide
K+
Cl-
NKCC2NKCC2
Ca2+
+
ClCClC--KbKb
+urine blood
ClCClC--KaKa
Cl-
Na+
Cl- Cl-
ClCClC--KbKb
Thiazide
NCCTNCCT
urine blood
K+
ROMKROMK
Na+ ENaC
Amiloride
urine blood
Modules of Modules of transepithelialtransepithelial electrolyte transport in the distal tubuleelectrolyte transport in the distal tubule
r
rr
r r
r
Mg2+
Ca2+
Mg2+
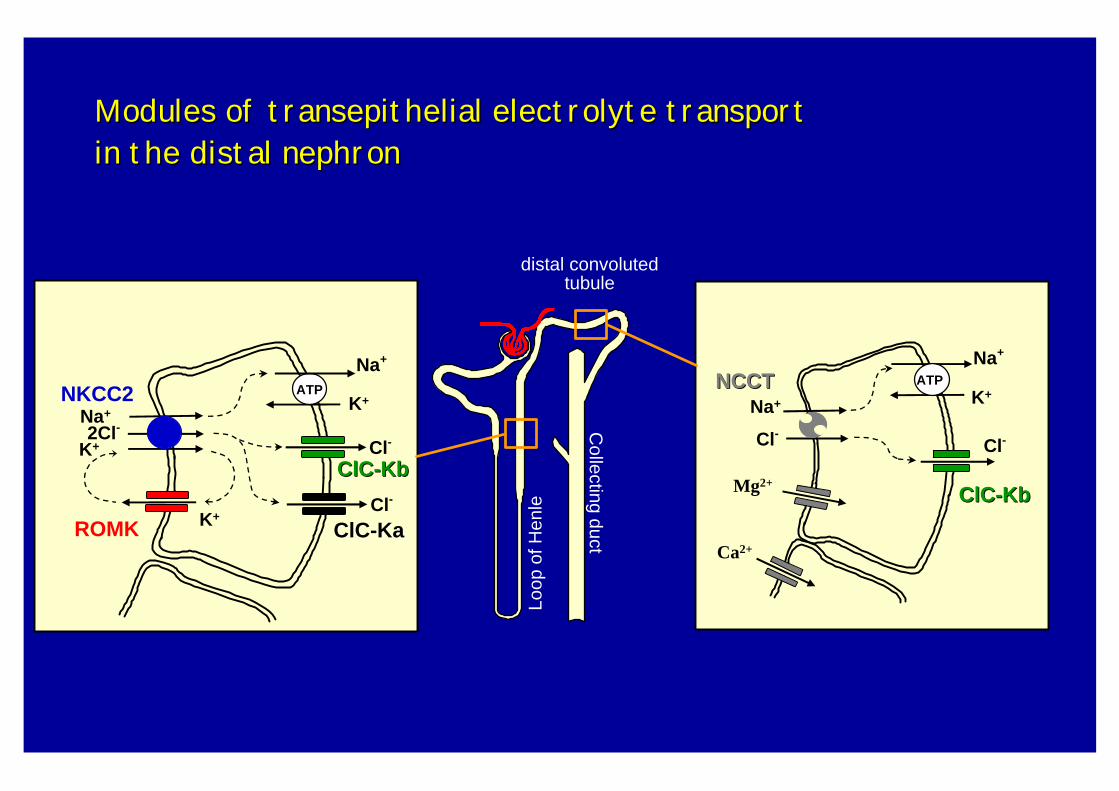
Fazit: Der Ausfall eines Moduls wird zwangsläufig auch Auswirkungen auf andere
Module entlang des Nierentubulus haben.
Frage: Warum ist diese genetische Salzverlust-Erkrankung besonders im frühen
Kindesalter so lebensbedrohlich?
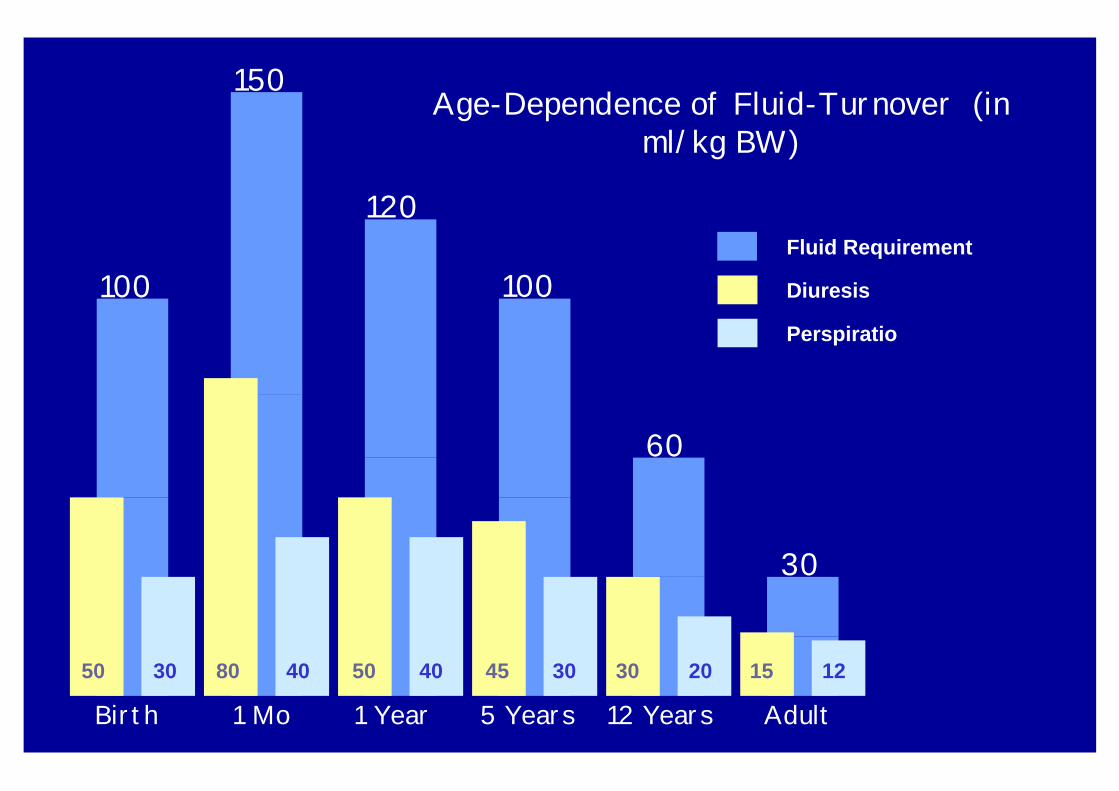
100
150
120
100
60
30
50 80 50 45 30 1530 40 40 30 20 12
Birth 1 Mo 1 Year 5 Years 12 Years Adult
Age-Dependence of Fluid-Turnover (in ml/kg BW)
Diuresis
Perspiratio
Fluid Requirement
M.Michael geb.04.05.1986
T. Maria geb.22.10.1982
R. Ranjit geb.11.09.1984
Foto März 1994
0
1
2
3
4
5
6
7
8
1 2 3
50
70
90
110
130
1 2 3
0
100
200
300
400
1 2 3
0
1
2
3
4
5
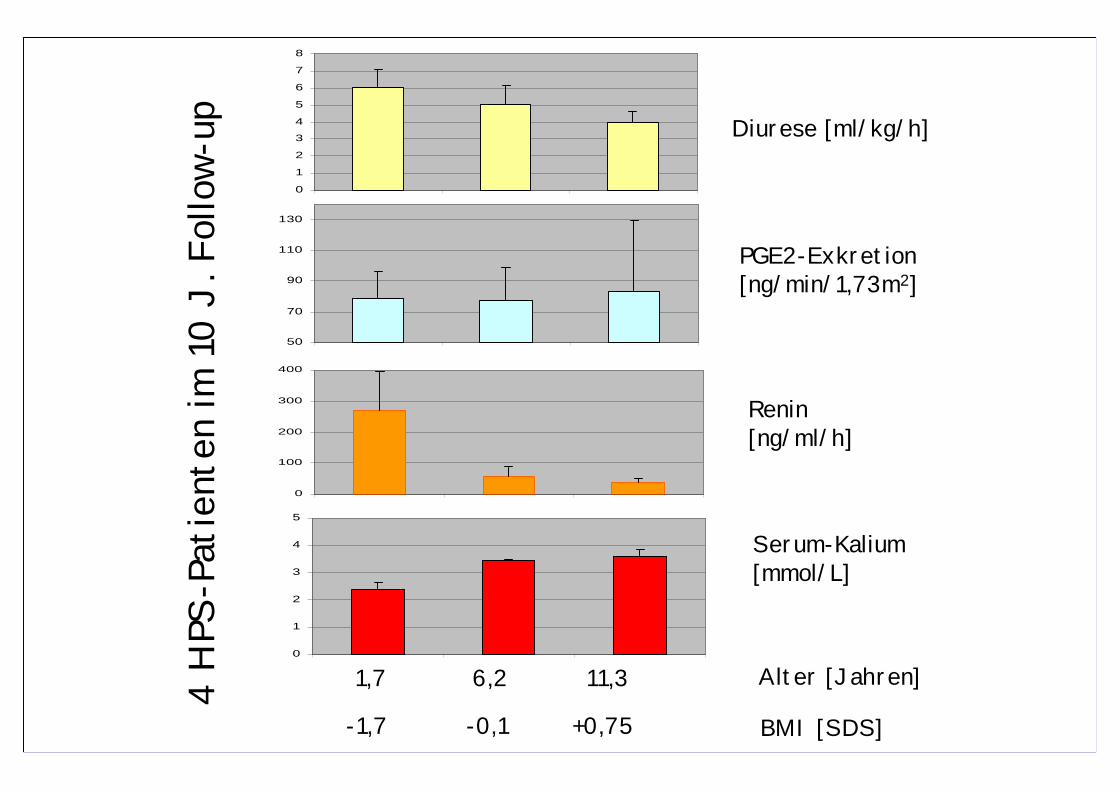
Diurese [ml/kg/h]
4 H
PS-P
atie
nten
im 1
0 J.
Fol
low-
upPGE2-Exkretion [ng/min/1,73m2]
Renin[ng/ml/h]
Serum-Kalium[mmol/L]
Alter [Jahren]
BMI [SDS]
1,7 6,2 11,3
-1,7 -0,1 +0,75
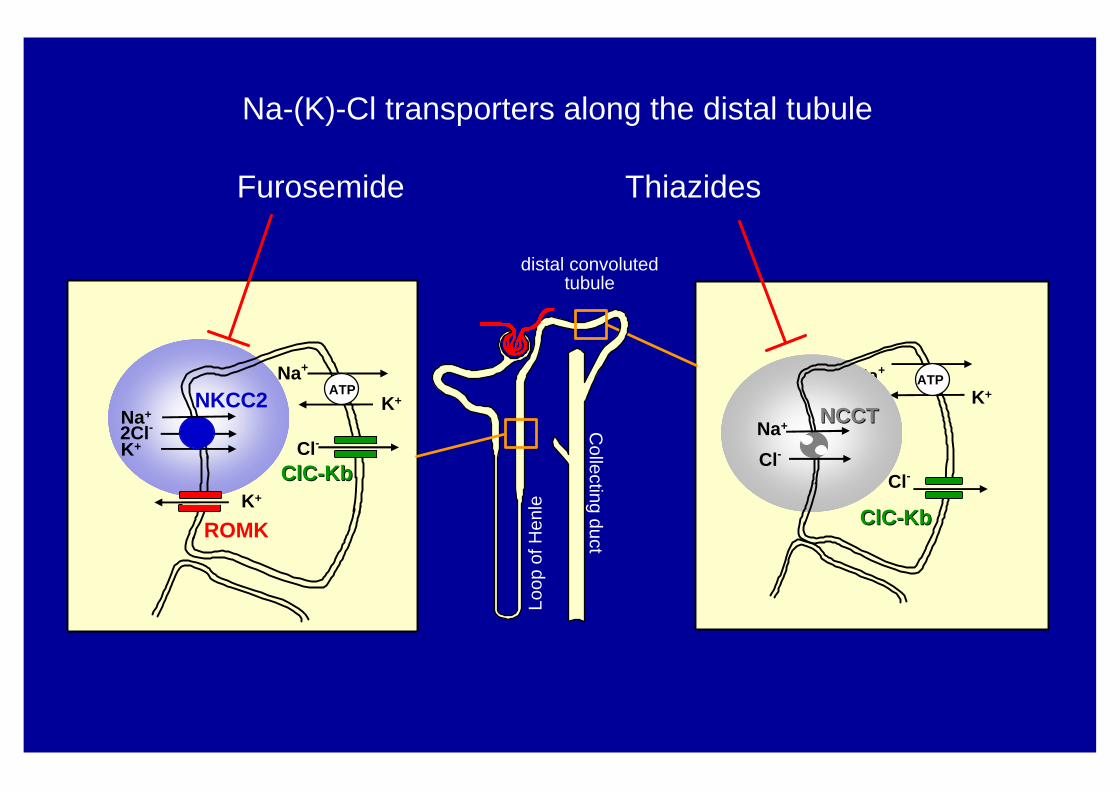
Loop
of H
enleK+
ROMK
Na+
K+Na+
ClCClC--KbKbCl-
K+
ClCClC--KbKb
Cl-
distal convoluted tubule
Collecting duct
Na+
2Cl-K+
ATPNKCC2
Na+
Cl-
ATP
NCCTNCCT
Furosemide Thiazides
Na-(K)-Cl transporters along the distal tubule
Hypothese: Beim heriditären Salzverlust mit Schleifen-Defekt entwickelt sich im weiteren
Verlauf der Erkrankung eine distaleConvolut(DC)-Kompensation bzw. der
Furosemid-Resistenz vergleichbarer Zustand.
Proof of Concept:Proof of Concept:
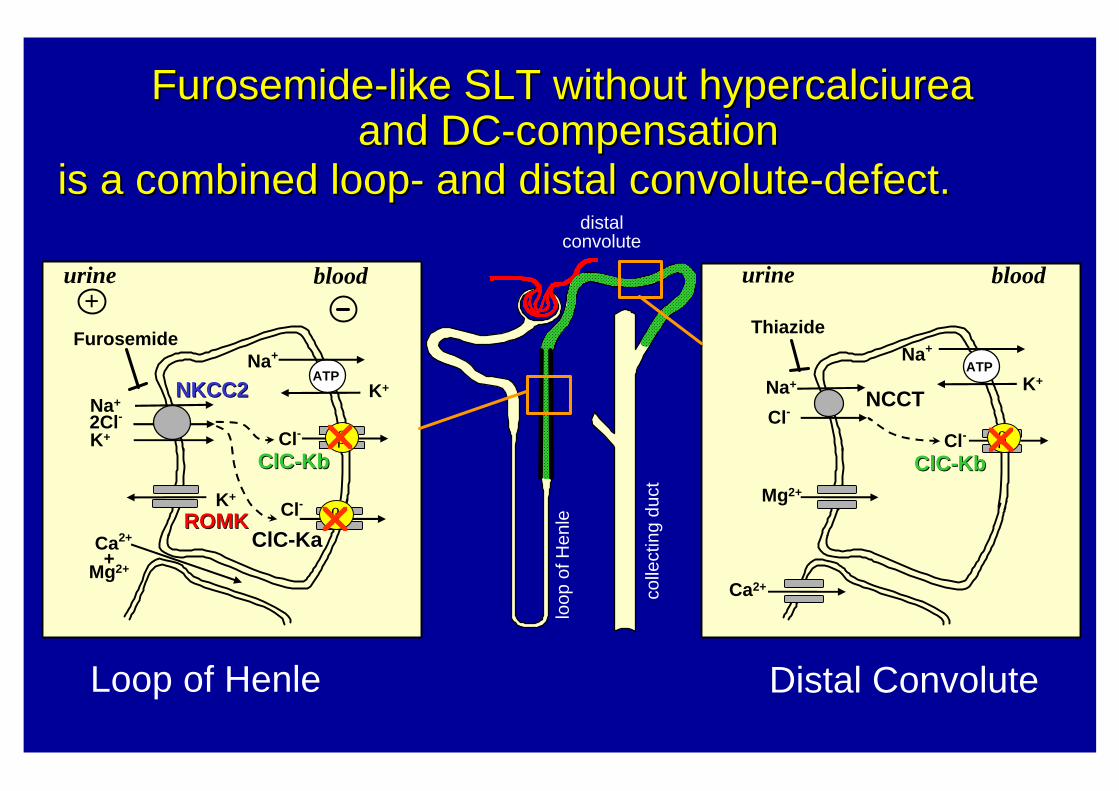
There is a special furosemide-like SLT (HPS)
without DC-compensation over time and
without hypercalciurea and nephrocalcinosis
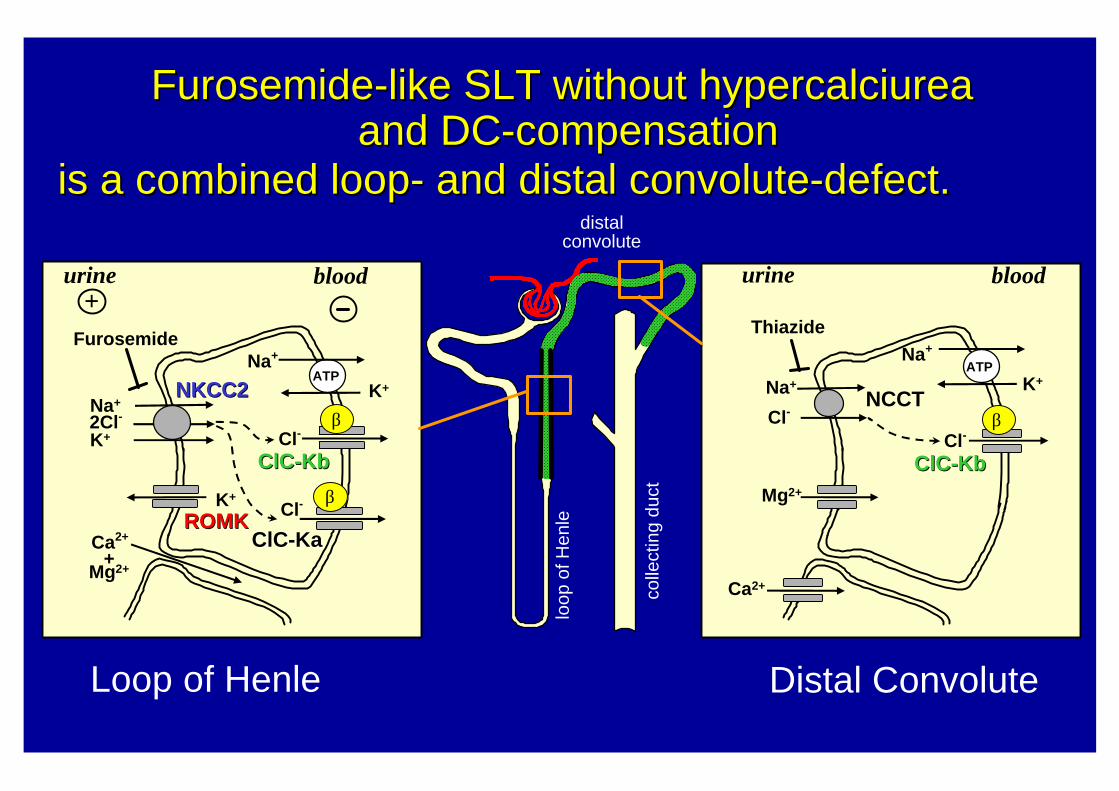
FurosemideFurosemide--like SLT without like SLT without hypercalciurea hypercalciurea and DCand DC--compensationcompensation
+Furosemide
Na+
Cl-
Thiazide
NCCTK+
Na+
ATP
Cl-
Mg2+K+
ROMKROMK
Cl-
Ca2+
ClCClC--KbKb
ClCClC--KaKa
Na+
K+
Na+
2Cl-K+
Cl-
ATPNKCC2NKCC2
ClCClC--KbKb
Distal ConvoluteLoop of Henle
urine blood urine blood
colle
ctin
g du
ct
loop
of H
enle
distalconvolute
is a combined loopis a combined loop-- and distal convoluteand distal convolute--defect.defect.
β
β
β
+Mg2+
Ca2+
FurosemideFurosemide--like SLT without like SLT without hypercalciurea hypercalciurea and DCand DC--compensationcompensation
+Furosemide
Na+
Cl-
Thiazide
NCCTK+
Na+
ATP
Cl-
Mg2+K+
ROMKROMK
Cl-
Ca2+
ClCClC--KbKb
ClCClC--KaKa
Na+
K+
Na+
2Cl-K+
Cl-
ATPNKCC2NKCC2
ClCClC--KbKb
Distal ConvoluteLoop of Henle
urine blood urine blood
colle
ctin
g du
ct
loop
of H
enle
distalconvolute
is a combined loopis a combined loop-- and distal convoluteand distal convolute--defect.defect.
β
β
βr
r
r
+Mg2+
Ca2+
Letzter therapeutischer Ausweg bei dem kombinierten Schleifen- und distaler Konvolut-Defekt ist die unilaterale Nephrektomie bzw.
Nierentransplantation.
Möglicher Nutzen von einer seltenen Krankheit:
Von einer extrem seltenen Salzverlust-Krankheit (<1:100 000) zu einer weit verbreiteten
Volkskrankheit (~30%) :der Salz-sensitiven arteriellen Hypertonie ?
Cl- Cl-
K+
H+
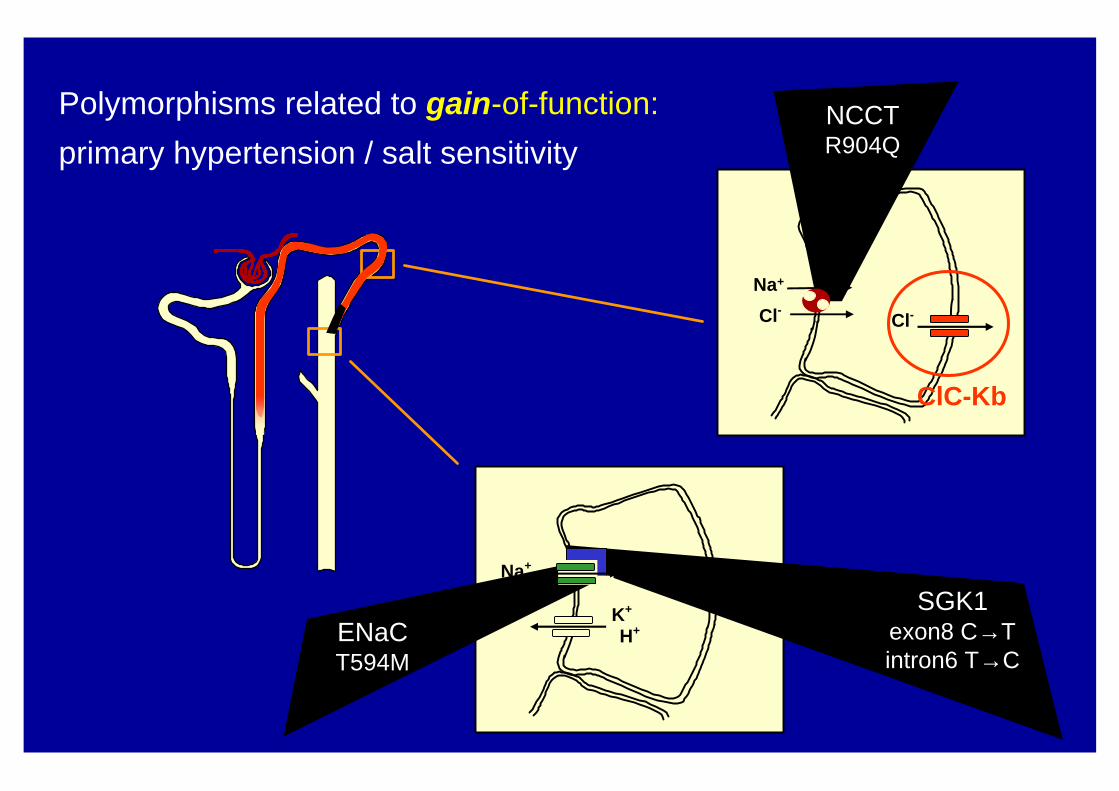
Polymorphisms related to gain-of-function:
primary hypertension / salt sensitivityNCCTR904Q
ENaCT594M
SGK1exon8 C→Tintron6 T→C
Na+
Na+
ClC-Kb
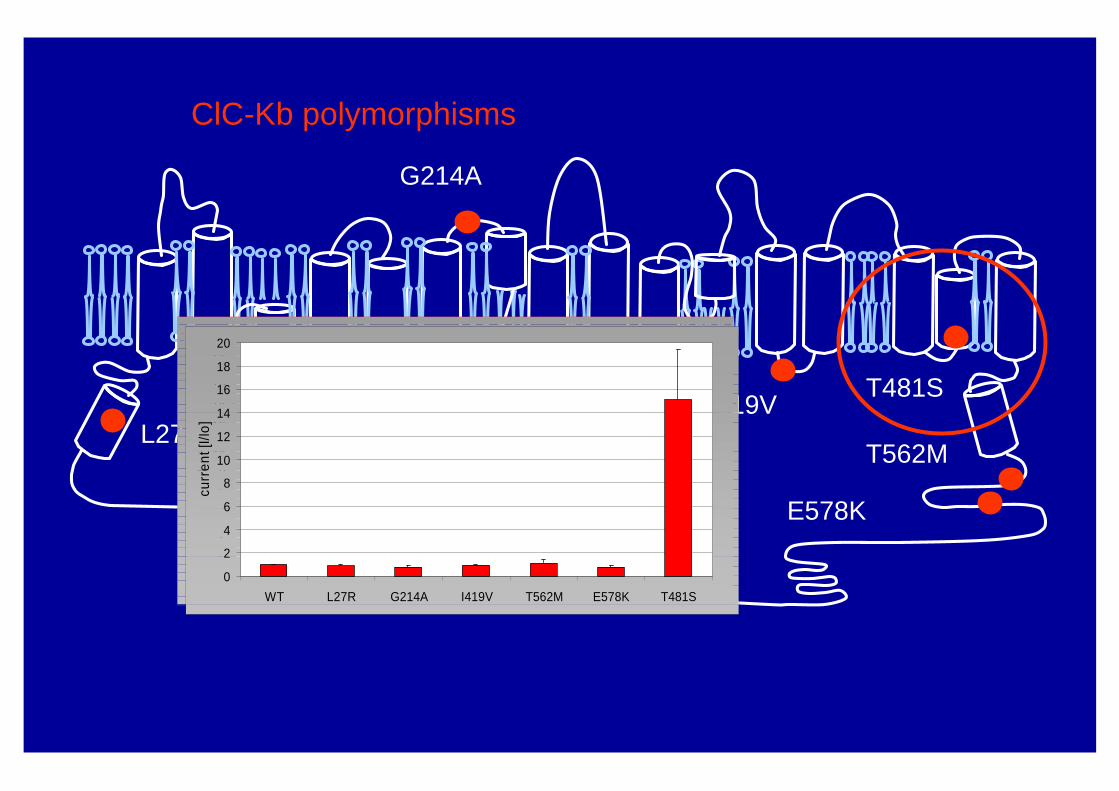
L27R
G214A
I419VT481S
T562M
E578K
ClC-Kb polymorphisms
02
46
81012
1416
1820
WT L27R G214A I419V T562M E578K T481S
curr
ent [
I/Io]
0
2
4
6
8
10
12
14
16
18
20
WT L27R G214A I419V T562M E578K T481S
curr
ent [
I/Io]
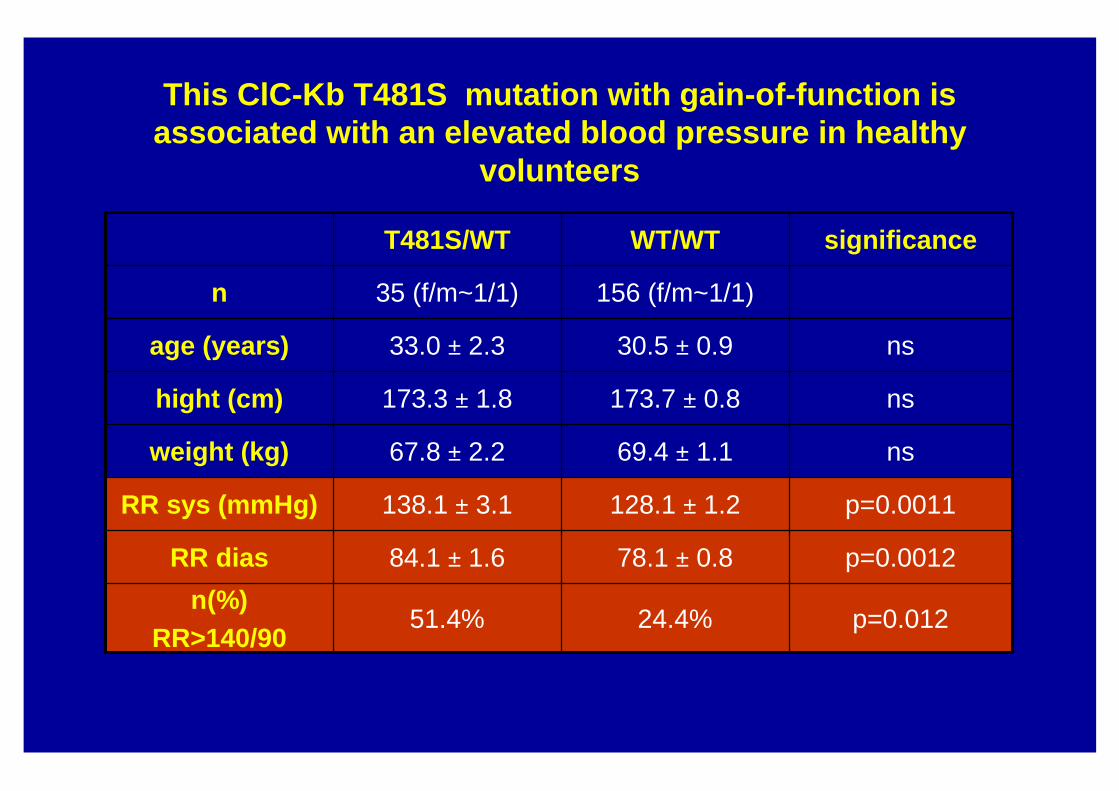
This ClC-Kb T481S mutation with gain-of-function isassociated with an elevated blood pressure in healthy
volunteers
p=0.01224.4%51.4%n(%)
RR>140/90
p=0.001278.1 ± 0.884.1 ± 1.6RR dias
p=0.0011128.1 ± 1.2138.1 ± 3.1RR sys (mmHg)
ns69.4 ± 1.167.8 ± 2.2weight (kg)
ns173.7 ± 0.8173.3 ± 1.8hight (cm)
ns30.5 ± 0.933.0 ± 2.3age (years)
156 (f/m~1/1)35 (f/m~1/1)n
significanceWT/WTT481S/WT
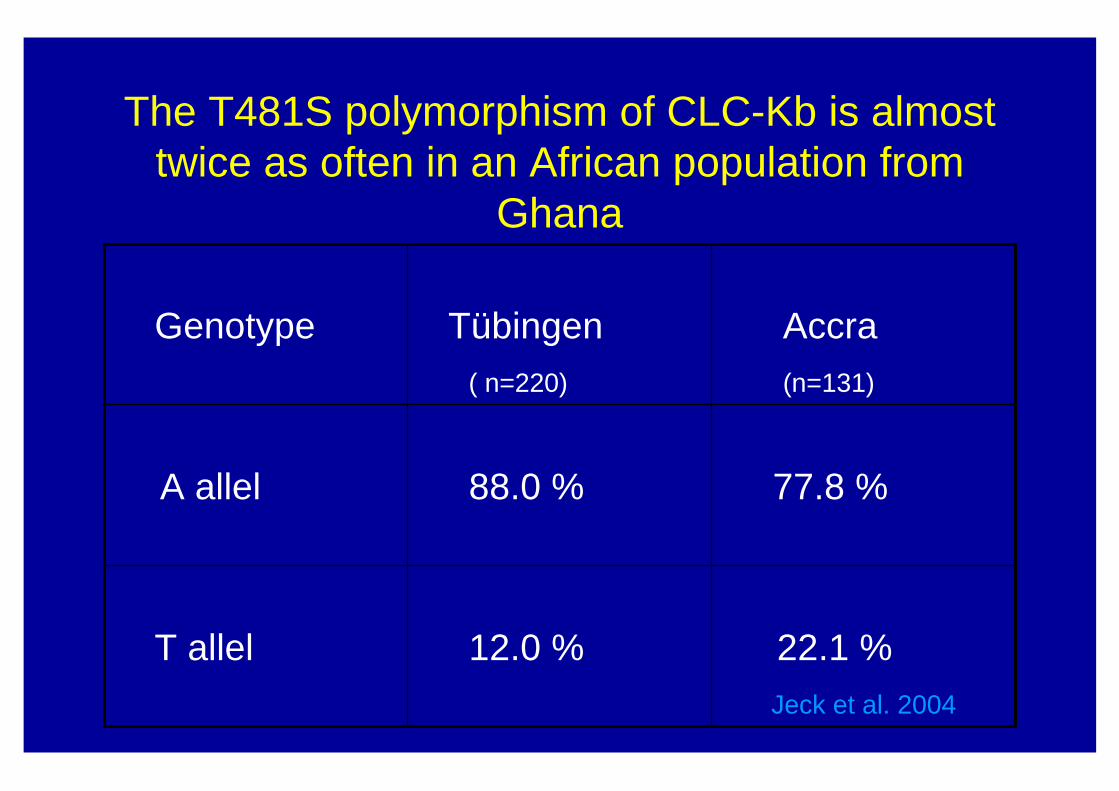
The T481S polymorphism of CLC-Kb is almost twice as often in an African population from
Ghana
22.1 %Jeck et al. 2004
12.0 %T allel
77.8 %88.0 %A allel
Accra(n=131)
Tübingen( n=220)
Genotype
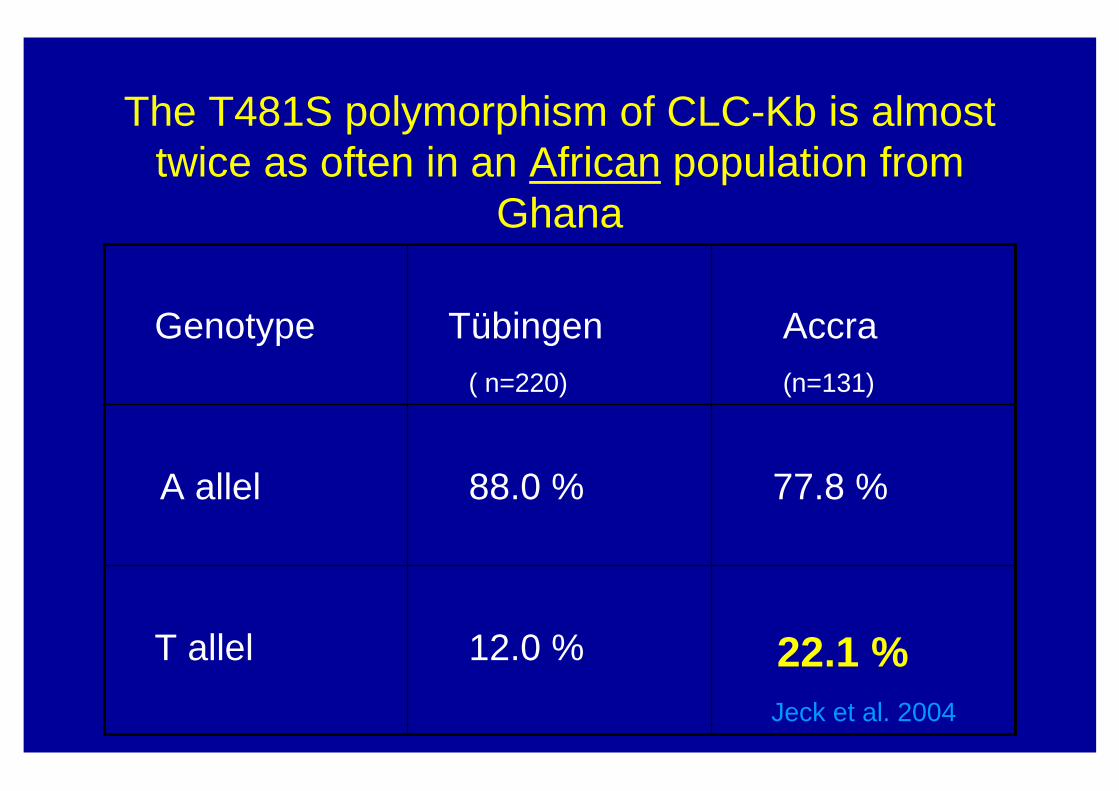
The T481S polymorphism of CLC-Kb is almost twice as often in an African population from
Ghana
22.1 %Jeck et al. 2004
12.0 %T allel
77.8 %88.0 %A allel
Accra(n=131)
Tübingen( n=220)
Genotype
Schußfolgerungen
• Für die Volkskrankheit: Dem ClCK b-Kanal kommt bei dem transepithelialen Salztransport eine zentrale Stellung zu und bieten sich als „Target“ für die Entwicklung neuartiger Diuretica, z.B. für die Behandlung der Kochsalz-senitivenHypertonie an.
Schußfolgerungen
• Für die Volkskrankheit: Dem ClCK b-Kanal kommt bei dem transepithelialen Salztransport eine zentrale Stellung zu und bieten sich als „Target“ für die Entwicklung neuartiger Diuretica, z.B. für die Behandlung der Kochsalz-senitivenHypertonie an;
weniger für den seltenen renalen Salzverlust,wie dem Hyperprostaglandin E-Syndrom (HPS)
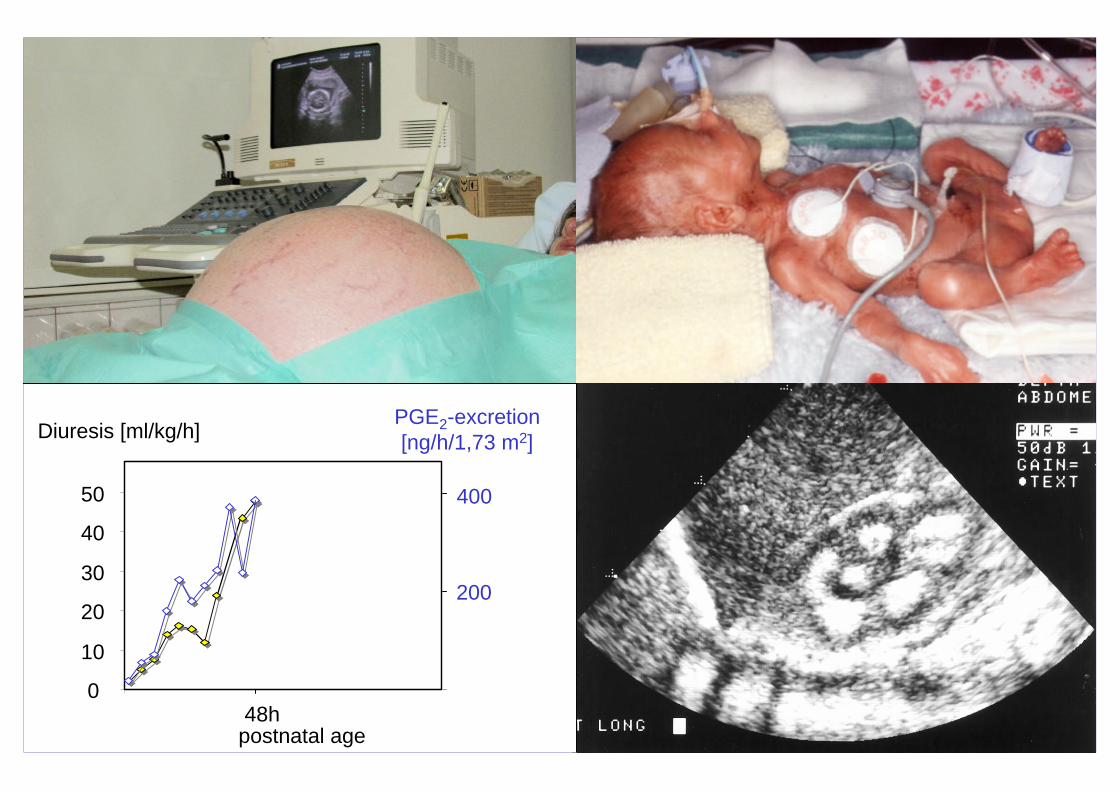
Polyhydramnion
Frühgeburt
NephrokalzinosePolyurieDiuresis [ml/kg/h]
0
10
20
30
40
50
48hpostnatal age
PGE2-excretion[ng/h/1,73 m2]
400
200
2 Cl-
K+Na+
2 Cl-
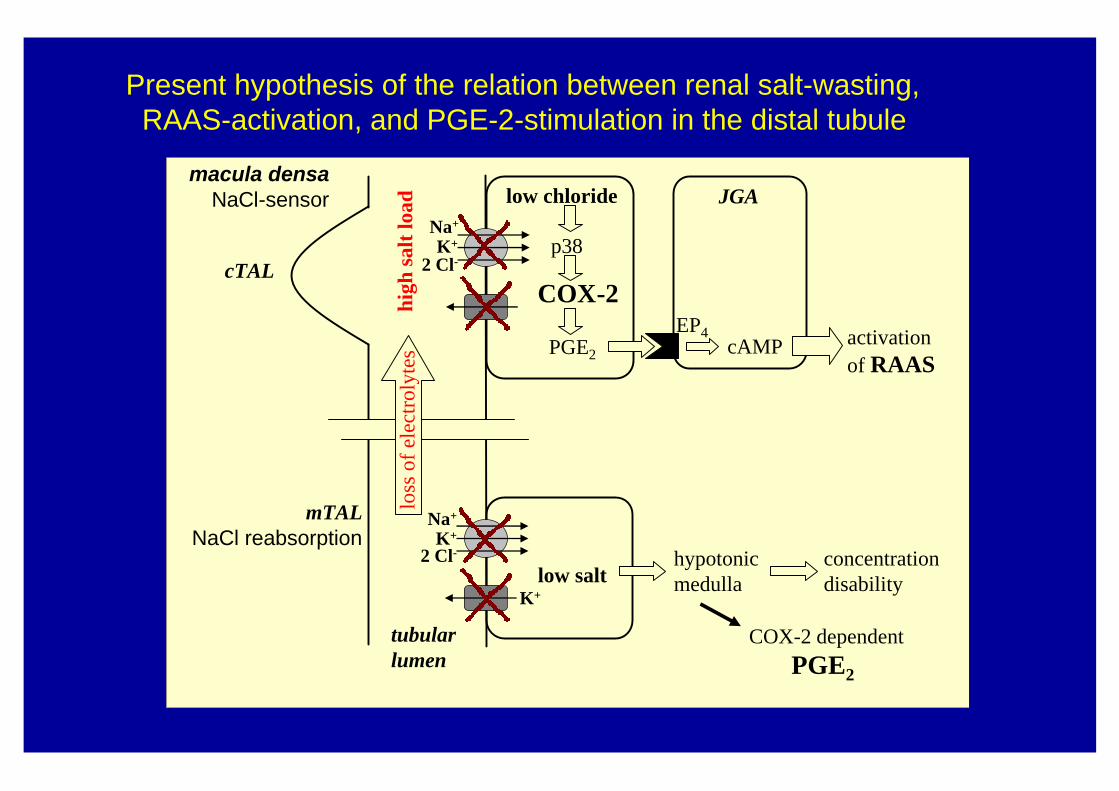
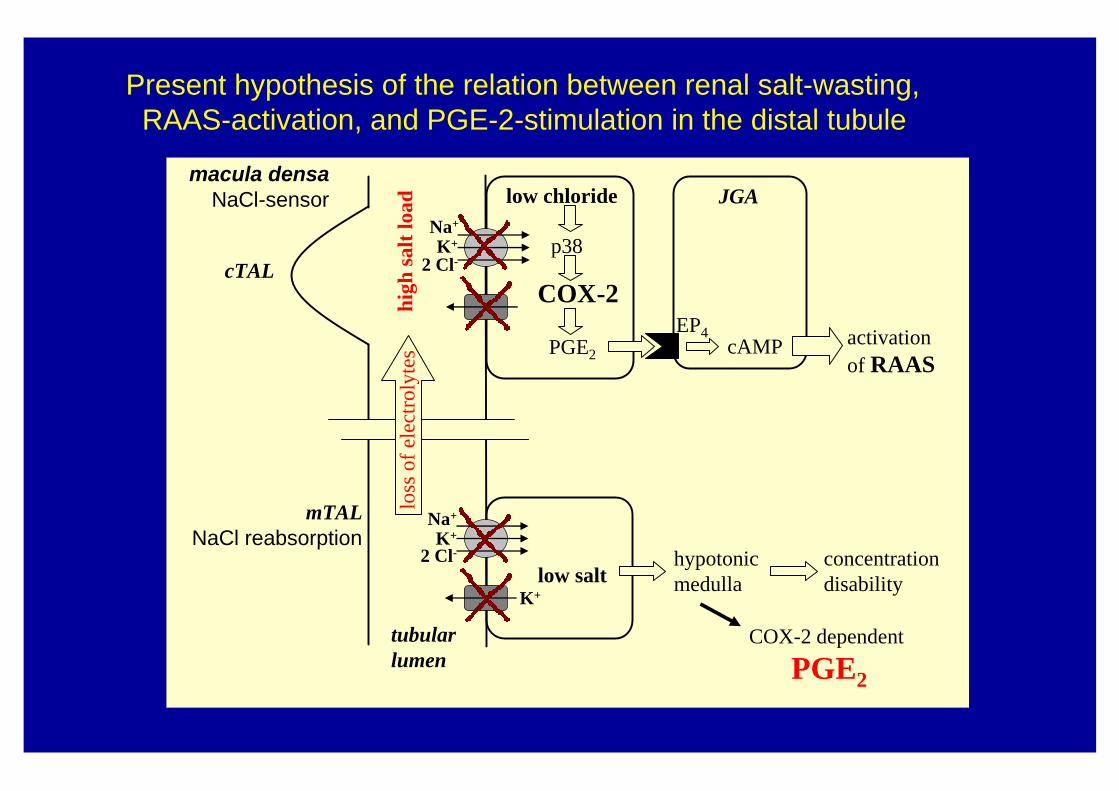
low chloride
COX-2
JGA
cAMP
cTAL
macula densaNaCl-sensor
mTALNaCl reabsorption K+
activationof RAAS
tubularlumen
loss
of e
lect
roly
tes
low salthypotonic medulla
concentrationdisability
EP4
Na+
p38
PGE2
K+
high
sal
tlo
ss o
f ele
ctro
lyte
s
COX-2 dependentPGE2
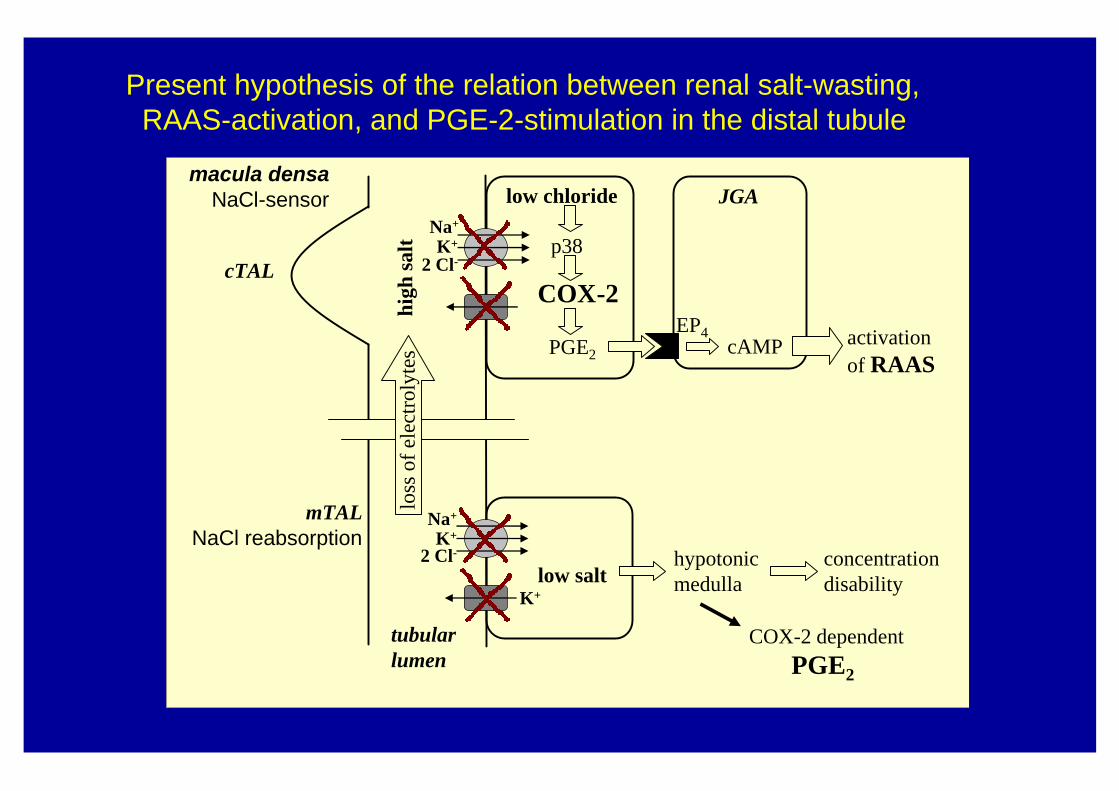
Present hypothesis of the relation between renal salt-wasting,RAAS-activation, and PGE-2-stimulation in the distal tubule
2 Cl-
K+Na+
2 Cl-
low chloride
COX-2
JGA
cAMP
cTAL
macula densaNaCl-sensor
mTALNaCl reabsorption K+
activationof RAAS
tubularlumen
loss
of e
lect
roly
tes
low salthypotonic medulla
concentrationdisability
EP4
Na+
p38
PGE2
K+
high
sal
t loa
dlo
ss o
f ele
ctro
lyte
s
COX-2 dependentPGE2
Present hypothesis of the relation between renal salt-wasting,RAAS-activation, and PGE-2-stimulation in the distal tubule
2 Cl-
K+Na+
2 Cl-
low chloride
COX-2
JGA
cAMP
cTAL
macula densaNaCl-sensor
mTALNaCl reabsorption K+
activationof RAAS
tubularlumen
loss
of e
lect
roly
tes
low salthypotonic medulla
concentrationdisability
EP4
Na+
p38
PGE2
K+
high
sal
t loa
dlo
ss o
f ele
ctro
lyte
s
COX-2 dependent
PGE2
Present hypothesis of the relation between renal salt-wasting,RAAS-activation, and PGE-2-stimulation in the distal tubule
Schußfolgerungen
• Für die Volkskrankheit: Dem ClCK b-Kanal kommt bei dem transepithelialen Salztransport eine zentrale Stellung zu und bieten sich als „Target“ für die Entwicklung neuartiger Diuretica, z.B. für die Behandlung der Kochsalz-senitivenHypertonie an.
• Für die seltene Erkrankung (HPS): Cox 2 und PGE2 sind integraler Teil der Signalverarbeitung im transepithelialen Salz-Transport in der Henle`schen Schleife und bieten sich als neues therapeutisches „Target“ an.

The The PediatricPediatric Research Team at our DepartmentResearch Team at our Departmentin in MarburgMarburg, Germany, Germany
Neonatology/NephrologyNeonatology/Nephrology
Andreas Andreas LeonhardtLeonhardtGünther Günther KlausKlaus
GeneticsGenetics
Nicola Nicola JeckJeckPiet SchlingmannPiet Schlingmann
PhysiologyPhysiology
Petra Petra WaldeggerWaldeggerSiegfried WaldeggerSiegfried Waldegger
PharmacologyPharmacology
Martin Martin KömhoffKömhoffStephan Stephan ReinalterReinalter
MassMass--SpectrometrySpectrometry
Horst Horst SchweerSchweerBernhard Bernhard WatzerWatzer
Reservedias
Conclusions
• ClC-K chloride channels participate in a critical way in chloride reabsorption along the distal nephron.
• Loss-of-function mutations in ClC-Ka and ClC-Kbcause a combined loop- and distal convolute-defect associated with severe renal salt wasting
• Gain-of-function mutations of ClC-Kb predisposesto renal salt retention and elevated blood pressure.
Conclusions
• ClC-K chloride channels participate in a critical way in chloride reabsorption along the distal nephron.
• Loss-of-function mutations in ClC-Ka and ClC-Kbcause a combined loop- and distal convolute-defect associated with severe renal salt wasting
• Gain-of-function mutations of ClC-Kb predisposesto renal salt retention and elevated blood pressure.
• A thiazide ought be the ideal antihypertensive target drug for this subpopulation, which is about 20% of the total caucasian population.
The second General Conclusion :
Orphan diseases, which are some kindof human knock-out models and can teach us general principles in normal and pathological physiology, are best
studied in ealy life - even prenatally.
Loop
of H
enle
Na+
Na+
2Cl-
NKCC2
K+
K+ATP
distal convoluted tubule
Collecting duct
ClCClC--KbKbCl-
ClCClC--KaKaCl-
K+ROMK
K+
Na+
Na+
Cl-
ATP
ClCClC--KbKb
Cl-
NCCTNCCT
Ca2+
Mg2+
Modules of Modules of transepithelialtransepithelial electrolyte transportelectrolyte transportin the distal in the distal nephronnephron

![Skript mit Aufgaben fur Funktionalanalysis · Literaturverzeichnis [1]H.W. Alt, Lineare Funktionalanalysis, Springer, 6. Auf-lage, Heidelberg, 2011. [2]A. Bressan, Lecture notes on](https://static.fdokument.com/doc/165x107/5f13a1df193c71498b2c219b/skript-mit-aufgaben-fur-f-literaturverzeichnis-1hw-alt-lineare-funktionalanalysis.jpg)