Thromboembolieprophylaxe beim Polytrauma · Polytrauma Epidemiologie •Häufigste Todesursache...
61
Thromboembolieprophylaxe beim Polytrauma 14. St.Galler IPS Symposium 12. Januar 2010 Dr. med. R. Lussmann
Transcript of Thromboembolieprophylaxe beim Polytrauma · Polytrauma Epidemiologie •Häufigste Todesursache...

Thromboembolieprophylaxebeim Polytrauma
14. St.Galler IPS Symposium
12. Januar 2010
Dr. med. R. Lussmann

Inhalt
• Begründung
• Problemstellung
• Risikofaktoren
• Prophylaxe-Möglichkeiten
• Vorschlag SOP
• Konklusionen
PolytraumaEpidemiologie
• Häufigste Todesursache zwischen 18. - 45. LJ–1/3 verbluten–1/3 SHT–1/3 cardiales
Versagen
Trunkey D: New Engl. J Med (1992)
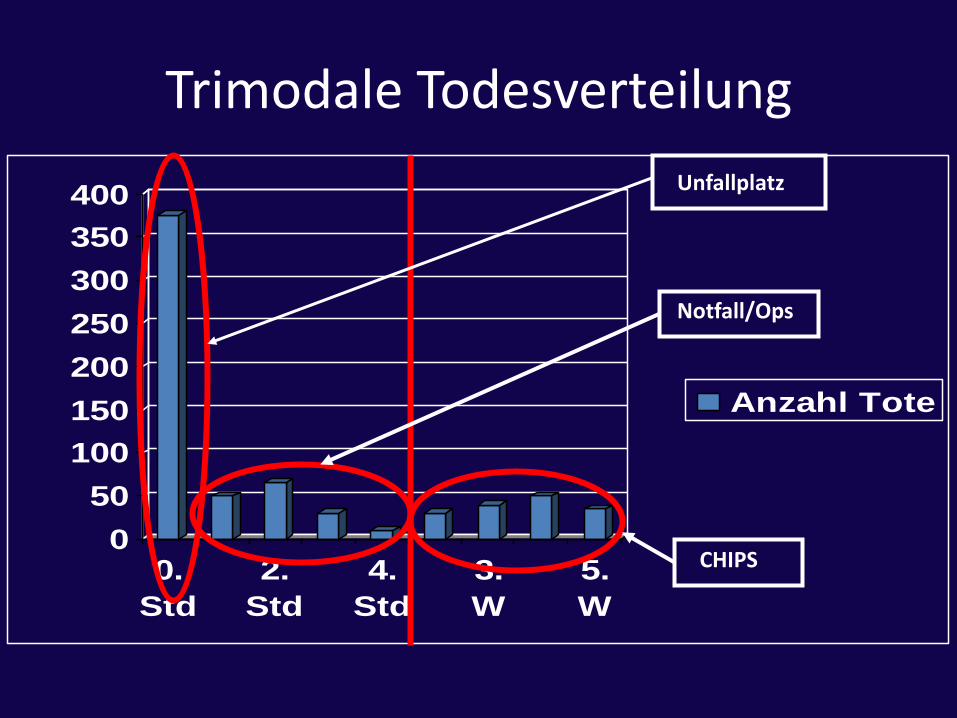
Trimodale Todesverteilung
0
50
100
150
200
250
300
350
400
0.
Std
2.
Std
4.
Std
3.
W
5.
W
Anzahl Tote
CHIPS
Notfall/Ops
Unfallplatz

Geerts WH et al.: Prevention of venousthromboembolism: the eight Conference on Antithrombotic and ThrombolyticTherapy. Chest 2008; 133: S381 – S453
Prevention of Venous Thromboembolism (VTE) –an example
• The American College of Chest Physicians published their first consensus conference on antithrombotic therapy in 1986
– In 2008 published their 8th edition of the evidence-based guideline
– Despite all of these published editions…..
VTE - the most common preventable cause of hospital death- 2/3 of all cases occur in recently hospitalized patients- up to 3/4 of all cases of PE death are a result of hospitalization

“The best estimates indicate that 350,000 to 600,000 Americans each year suffer from DVT and PE, and that at least 100,000 deaths may be directly or indirectly related to these diseases. This is far too many, since many of these deaths can be avoided. Because the disease disproportionately affects older Americans, we can expect more suffering and more deaths in the future as our population ages–unless we do something about it.”

Most hospitalized patients have at least one additional risk factor for VTE
Risk Factors for VTE
• Surgery
• Trauma
• Immobility, paresis
• Cancer
• Cancer therapy
– hormonal therapy, chemotherapy or radiotherapy
• Venous compression
• Previous VTE
• Increasing age
• Pregnancy and post-partum period
• Estrogen-containing oral contraception or HRT
• SERM
• Erythropoiesis stimulating agents
• Acute medical illness
• Inflammatory bowel disease
• Nephrotic syndrome
• Myeloproliferative disorders
• Paroxysmal nocturnal Hb-uria
• Obesity
• Central venous catheterization
• Inherited or acquired thrombophilia
Geerts W et al. Chest. 2008;133:381S-453S.
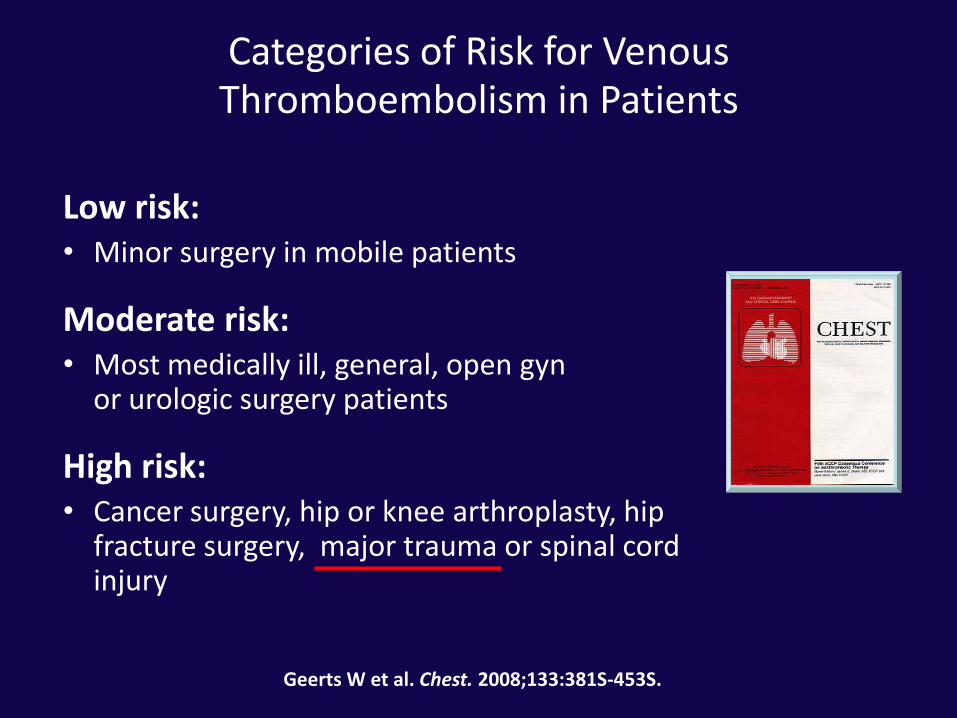
Categories of Risk for Venous Thromboembolism in Patients
Low risk:• Minor surgery in mobile patients
Moderate risk:• Most medically ill, general, open gyn
or urologic surgery patients
High risk:• Cancer surgery, hip or knee arthroplasty, hip
fracture surgery, major trauma or spinal cord injury
Geerts W et al. Chest. 2008;133:381S-453S.
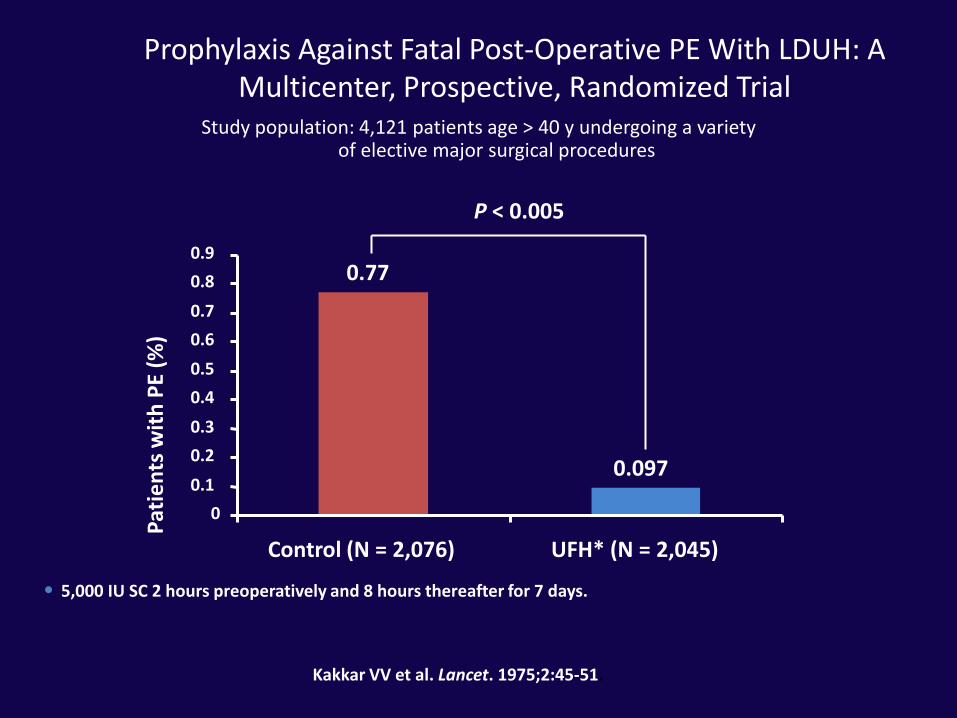
Prophylaxis Against Fatal Post-Operative PE With LDUH: A Multicenter, Prospective, Randomized Trial
Study population: 4,121 patients age > 40 y undergoing a variety of elective major surgical procedures
P < 0.005
• 5,000 IU SC 2 hours preoperatively and 8 hours thereafter for 7 days.
Pat
ien
ts w
ith
PE
(%)
Kakkar VV et al. Lancet. 1975;2:45-51.
0.77
0.097
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Control (N = 2,076) UFH* (N = 2,045)
Problem• Keine Prophylaxe: 7 - 58% TVT, 1% fatale LE (1)
• Abhängig von Demographie, Verletzungen, diagnostische Methoden, Art der Prävention
• LE innert 24 Std nach Eintritt in 6% (2,3)
• Innert 4 Tagen: 37% (4)
• Innert 1 Woche nach posttraumatischem Schock: 30% (5)
• 3. häufigste Todesursache beim Polytrauma, wenn die ersten Tage überlebt werden
1. Geerts WH et al.: a prospective study of venous thromboembolism after major trauma. NEJM 1994; 331: 1601 - 1606
2. O‘Malley KF et al.: Pulmonary embolism in major trauma patients. J Trauma 1990; 30: 748 - 7503. Owings JT et al.: Timing of the occurrence of pulmonary embolism after injury. Arch Surg 1997; 132: 862 -8674. Menaker J et al.: Incidence of early pulmonary embolism after injury. J Trauma 2007; 63: 620 - 6275. Nathens AB et al.: The practice of venous thromboembolism prophylaxis in the major trauma patient. J
Trauma 2007; 62: 557 - 563

Pathophysiologie• Virchow‘sche Trias:
– Venenverletzung
– Venöse Stase
– Hyperkoagulabilität
• Erhöhte Prothrombinfragmente in 81% und D-Dimer Spiegel in 100% bei Polytrauma, persistieren für Monate, nicht prädiktiv für TVT und LE
• Hyperkoagulabilität benötigt zudem venöse Stase zur Bildung eines lokalen Thrombus (1)
1. Meissner MH et al.: Venous thromboembolism in trauma: a local manifestation of systemichypercoagulability? J Trauma 2003; 54: 224 - 231


Pathophysiologie• Systemische Hyperkoagulabilität: (1)
– Exzessive Aktivierung der Gerinnung
– Cytokin-vermittelte Reduktion der Gerinnungsinhibitoren
– Erhöhte Hemmung der Fibrinolyse
• Venöse Stase permissiver Faktor (2)
• Endothelschaden prothrombotisch Tc-Adhäsion Aktivierung der Gerinnungskaskade Thrombingeneration (3)
1. Meissner MH et al.: Venous thromboembolism in trauma: a local manifestation of systemichypercoagulability? J Trauma 2003; 54: 224 - 231
2. Meissner MH et al.: Acute venous disease: venous thrombosis and venous trauma. J Vasc Surg 2007; 46 SupplS: 25S – 53S
3. Knudson MM et al.: Venous thromboembolism after trauma. Curr Opin Crit Care 2004; 10: 539 - 548
Inzidenz – divergierende Daten
• Abhängig von Detektions Modalität und Häufigkeit
• LE in 30%, wenn mittels LE-CT gescreent (1), jedoch ACS NTDB: 0,18% (2)
1. Schultz DJ et al.: Incidence of asymptomatic pulmonary embolism in moderately to severely injured traumapatients. J Trauma 2004; 56: 727 - 733
2. Knudson MM et al.: Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann Surg 2004; 240: 490 - 498
Risikofaktoren• Greenfield: Risk assessment profile score (1):
– In 160 Patienten erprobt (2)
– Inzidenz TVT in 10% in high risk pts (trotz Prophylaxe) vs 0% in low risk pts ohne Prophylaxe
• (3) RM oder WS-Verletzungen höchstes Risiko
• Alter, ISS, Transfusionen erhöhen Risiko TVT
• Hingegen trad. RF wie # lange Röhrenknochen, Becken#, SHT nicht prädiktiv
1. Greenfield LJ et al.: Posttrauma thromboembolism prophylaxis. J Trauma 1997; 42: 100 - 1032. Gearhart MM et al.: The risk assessment profile score identifies trauma patients at risk for vein thrombosis.
Surgery 2000; 128: 631 - 640 3. Rogers FB et al.: Practice management guidelines for the prevention of venous thromboembolism in trauma
patients. The EAST practice guidelines work group. J Trauma 2002; 53: 142 - 164
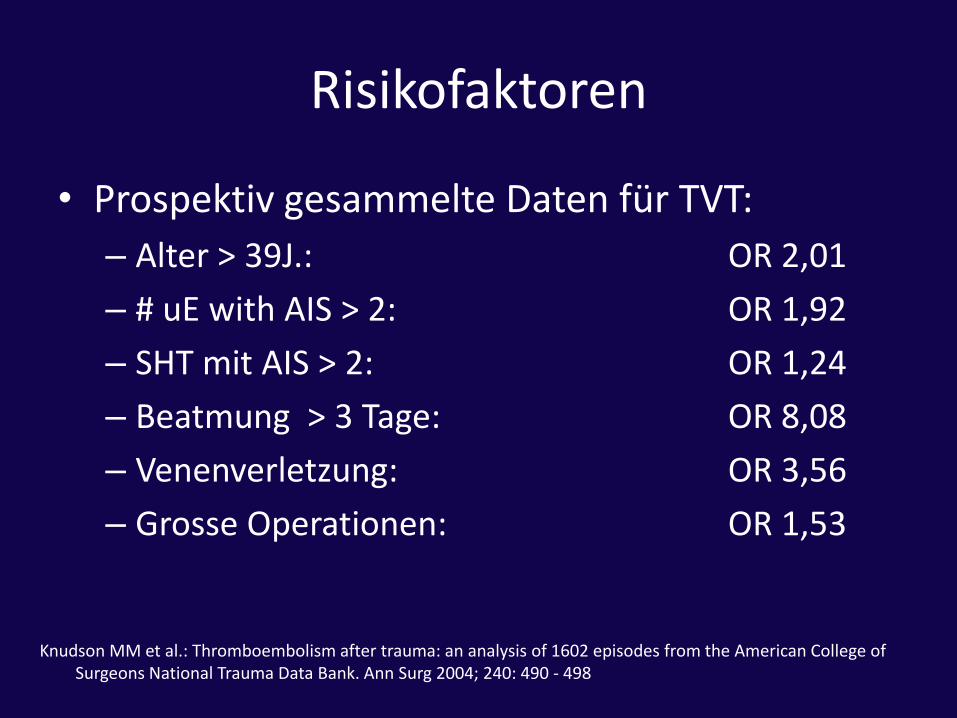
Risikofaktoren
• Prospektiv gesammelte Daten für TVT:
– Alter > 39J.: OR 2,01
– # uE with AIS > 2: OR 1,92
– SHT mit AIS > 2: OR 1,24
– Beatmung > 3 Tage: OR 8,08
– Venenverletzung: OR 3,56
– Grosse Operationen: OR 1,53
Knudson MM et al.: Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann Surg 2004; 240: 490 - 498
Balanceakt Thromboembolieprophylaxe beimPolytrauma
Blutung
Thrombose / Embolie
Yin und Yang
Yin und Yang unkontrollierte Blutung und TVT Prophylaxe
• Jede Substanz, die die venöse Gerinnung supprimiert, hat das entsprechende Potential, das Blutungsrisiko zu erhöhen
• Unkontrollierbare Blutungen: 30 – 40% der traumabedingtenTodesfälle, häufigste Todesursache der potentiell verhinderbaren frühzeitigen Todesfälle im Spital (1 -5)
• SHT und MOV, die durch schwere Blutungen verschlimmert werden, bedingen die anderen Todesursachen (6)
1. Spahn DR et al.: Task force for advanced bleeding care in trauma. Management of bleeding following majortrauma: a European guideline. Crit Care 2007; 11: R,17. Erratum in: Crit Care 2007; 11: 414
2. Chiara O et al.: Treatment of critical bleeding in trauma patients. Minerva Anestesiol 2006; 72: 383 – 3873. Spivey M et al.: Therapeutic approaches in trauma-induced coagulopathy. Minerva Anestesiol 2005; 71: 281 – 94. Sauaia A et al.: Epidemiology of trauma deaths: a reassessment. J Trauma 1995; 38: 185 – 1935. Nardi G et al.: Epidemiological study on high grade trauma. Friuli VG Major >Trauma Study Group. Minerva
Anestesiol 1999; 65: 348 – 3526. The Brain Trauma Foundation. The american association of neurological surgeons. The joint section on
neurotrauma and critical care. Hypotension. J Neurotrauma 2000; 17: 591 - 595

Yin und Yang• Hyperkoagulabler Zustand evolutionäre
Bedingung zum Überleben beim Polytrauma (1)
• Die andere Seite der Hyperkoagulabilität TVT und Lungenembolie
1. Velmahos GC: Posttraumatic thromboprophylaxis revisited: an argument against the current methods of DVT and PE prophylaxis after injury. World J Surg 2006; 30: 483 – 487
Yin und Yang• Optimale Prophylaxe nicht definiert oft adäquate
Prophylaxe nicht verordnet (1,2,3)
• V.a. SHT, RM-Verletzungen, grosse Organläsionen, komplexe Beckenfrakturen (4,5,6)
1. Improving the evidence base for trauma care: progress in the international CRASH-2 trial. PLoS Clin Trials 2006; 1:e30
2. Knudson MM et al.: Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann Surg 2004; 240: 490 - 498
3. Geerts WH et al.: Prevention of venous thromboembolism: the Seventh ACCP Conference on antithromboticand thrombolytic therapy. Chest 2004; 126 (3Suppl): 338S-400S
4. Geerts WH et al.: a prospective study of venous thromboembolism after major trauma. NEJM 1994; 331: 1601 – 1606
5. Geerts WH et al.: A comparison of low-dose heparin with low-molecular-weight heparin as prophylaxisagainst venous thromboembolism after major trauma. NEJM 1996; 335: 701 – 707
6. Cothren CC et al.: Utility of once-daily dose of low-molecular-weight heparin to prevent venousthromboembolism in multisystem trauma patients. World J Surg 2007; 31: 98 - 104
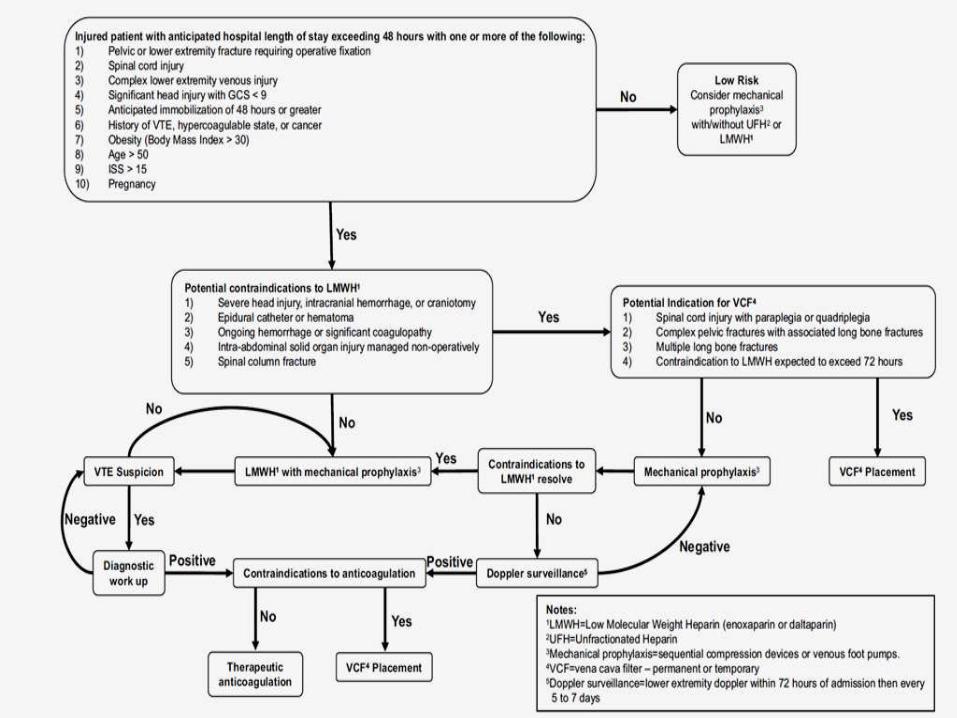
Prophylaxe
• Erste Manifestation einer TVT kann eine fatale LE sein
• Empfehlungen ACCP: alle Traumapatientensollten eine Prophylaxe erhalten
Geerts WH et al.: Prevention of venous thromboembolism: the eight Conference on Antithrombotic and Thrombolytic Therapy. Chest 2008; 133: S381 – S453
Möglichkeiten
• Mechanische Prophylaxe:
– ATS
– IPC oder SCD
• Medikamentöse Prophylaxe:
– LDUH
– LMWH: Dalteparin, Enoxaparin
– Pentasaccharide: Fondaparinux
• Vena Cava inferior Filter
Mechanische Prophylaxe• Vorteil:
– Keine Beeinträchtigung der Gerinnung, schnell, einfach
– Sinnvoll in Kombination mit LMWH in high risk Pat
– Ad interim oder Alternative zu LMWH bei Blutungsrisiko
• Kontraindikationen:– Gefässläsionen, Verbrennungen, Fasziotomien,
Gipsverbände, externe Fixationen, PAVK
– Morbide Adipositas nicht anpassbare devices
• Hauptproblem: – Ungenügende Anpassung
– Compliance: 19-56%
1. Rogers FB et al.: Practice management guidelines for the prevention of venous thromboembolism in traumapatients. The EAST practice guidelines work group. J Trauma 2002; 53: 142 – 164
2. Geerts WH et al.: Prevention of venous thromboembolism: the eight Conference on Antithrombotic andThrombolytic Therapy. Chest 2008; 133: S381 – S453

ATS
• Benefit nur in low-risk Patienten bei Allgemeinchirurgie (Risikoreduktion der TE-Komplikationen) sowie einigen Patienten mit mässigem Risiko
• Keine Daten bei Polytraumapatienten

IPC (SCD)
• IPC der Füsse sowie verzögertes LMWH (5 Tage) in 200 Patienten, prospektiv, bei nicht penetrierendem Trauma in Komb mit # der langen Röhrenknochen vs früher Einsatz von LMWH (48 Std.) kein Unterschied (1)
1. Stannard JP et al.: Prophylaxis against deep-vein thrombosis following trauma: a prospective, randomizedcomparison of mechanical and pharmacological prophylaxis. J Bone Joint Surg Am 2006; 88: 261 – 266
IPC (SCD)
• 442 high risk Patienten: IPC vs LMWH, wöchentlicher Duplex: kein signifikanter Unterschied in TVT-Inzidenz (2,7 vs 0,5%; p = 0,122) (1)
• 120 Patienten mit SHT oder spinaler Verletzung: IPC vs LMWH: 6,6 vs 5,0 %; p=0,04 (2)
1. Ginzburg E et al.: Randomized clinical trial of intermittent pneumatic compression and low molecular weight heparin in trauma. Br J Surg 2003; 90: 1338 – 1344
2. Kurtoglu M et al.: Venous thromboembolism prophylaxis after head and spine trauma: intermittentpneumatic compression devices versus low molecular weight heparin. World J Surg 2004; 28: 807 - 811

Medikamentöse Prophylaxe• Indikation
– LMWH Standard of care in EAST/APPC Guidelines beim Polytrauma
1. Rogers FB et al.: Practice management guidelines for the prevention of venous thromboembolism in traumapatients. The EAST practice guidelines work group. J Trauma 2002; 53: 142 – 164
2. Geerts WH et al.: Prevention of venous thromboembolism: the eight Conference on Antithrombotic andThrombolytic Therapy. Chest 2008; 133: S381 – S453

Medikamentöse Prophylaxe
• Kontraindikation
– Erhöhtes Blutungsrisiko 1-3% (1,2)
– Akzept. KI: intraokkuläre oder intracerebraleBlutungen, inkomplett. RM-Läsion bei paraspinalem Hämatom, persistierende Blutung oder nicht korrigierte Koagulopathie (1,2)
– Verzögerter Einsatz bei SHT, Massivtransfusionen, oder bei Fehlen von Komborbiditäten (3)
1. Rogers FB et al.: Practice management guidelines for the prevention of venous thromboembolism in traumapatients. The EAST practice guidelines work group. J Trauma 2002; 53: 142 – 164
2. Geerts WH et al.: Prevention of venous thromboembolism: the eight Conference on Antithrombotic andThrombolytic Therapy. Chest 2008; 133: S381 – S453
3. Nathens AB et al.: The practice of venous thromboembolism prophylaxis in the major trauma patient. J Trauma 2007; 62: 557 - 563
Erhöhtes Blutungsrisiko?• 106 Patienten mit ICB: Enoxaparin innert 24 h;
Progression der Blutung in 4% (1)
• 120 SHT oder RM-Trauma: IPC vs IPC und Enoxaparin (keine kont. Blutung im CT nach 24 Std. post Trauma) je 1 Exacerbation der ICB/Gruppe (2)
• 743 Patienten (277 SHT/RM) high risk: Dalteparin 0 Pat mit unerwarteter Blutung (3)
1. Norwood SH et al.: A potentially expanded role for enoxaparin in preventing venous thromboembolism in highrisk blunt trauma patients. J Am Coll Surg 2001; 192: 161 - 167
2. Kurtoglu M et al.: Venous thromboembolism prophylaxis after head and spine trauma: intermittent pneumaticcompression devices versus low molecular weight heparin. World J Surg 2004; 28: 807 – 811
3. Cothren CC et al.: Utility of once-daily dose of low-molecular-weight heparin to prevent venousthromboembolism in multisystem trauma patients. World J Surg 2007; 31: 98 - 104
Beginn und Dauer
• Alle Traumapatienten sollten innert 36 Std nach Blutungskontrolle LMWH erhalten (1)
• verzögert nach 4 Tagen vs früher Beginn (5% TVT-Risiko nach hämorrhagischem Schock) erhöht das Risiko um das 3-fache für eine TVT (2)
• Bis Spitalentlassung und vollständige Mobilisation (1)
1. Geerts WH et al.: Prevention of venous thromboembolism: the eight Conference on Antithrombotic andThrombolytic Therapy. Chest 2008; 133: S381 – S453
2. Nathens AB et al.: The practice of venous thromboembolism prophylaxis in the major trauma patient. J Trauma 2007; 62: 557 - 563
LDUH
• Kein Benefit bei s.c. Gabe
• EAST Guidelines: extensive Meta-Analyse: kein Benefit durch LDUH
• Rolle in Komb mit SCD nur bei Patienten mit hohem Blutungsrisiko, falls Option der vollen Protaminantagonisierung im Falle einer Blutung eine Option ist (1)
1. Spinal cord injury thromboprophylaxis investigators. Prevention of venous thromboembolism in the acutetreatment phase after after spinal cord injury: a randomized, multicenter trial comparing low-dose heparinplus intermittent pneumatic compression with enoxaparin. J Trauma 2003; 54: 1116 - 1126
LMWH
• Einfach in der Anwendung
• Bessere Effizienz
• Erhöhte Spezifität als UFH
• Kein Monitoring notwendig
• Deutlich kleinere Inzidenz für HIT (3-5% vs 0-0,9%) (1)
1. Arepally GM et al.: Clinical practice. Heparin-induced thrombocytopenia. NEJM 2006; 355: 809 - 817
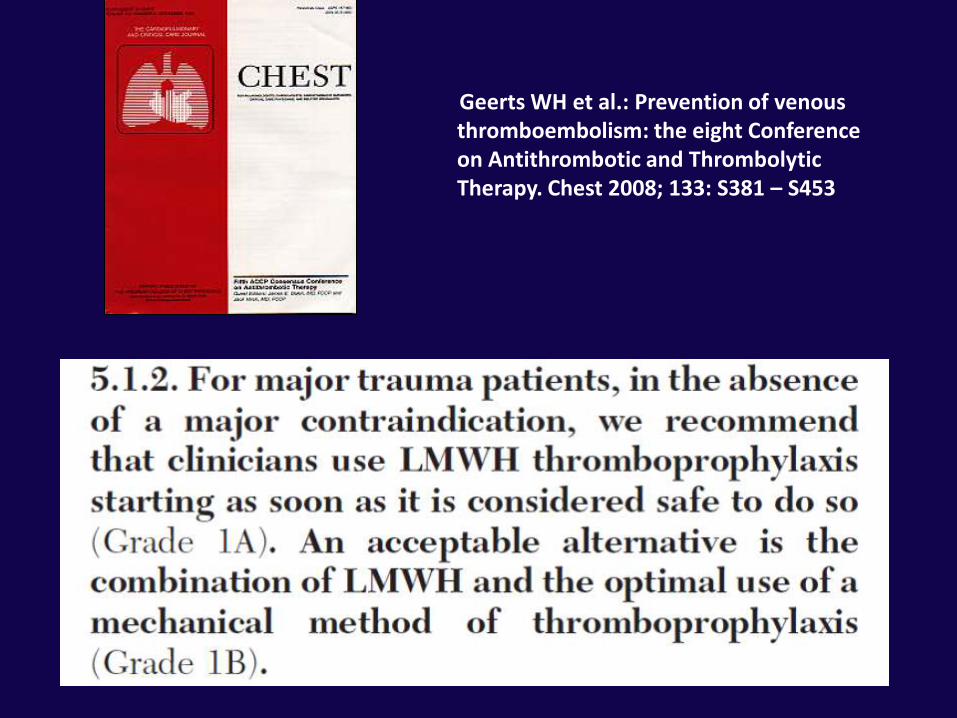
Geerts WH et al.: Prevention of venousthromboembolism: the eight Conference on Antithrombotic and ThrombolyticTherapy. Chest 2008; 133: S381 – S453

Enoxaparin (Clexane©)
• 344 Traumapatienten, DBRCT
– 31 vs 44% totaler TVT, proximale TVT 6 vs 15% 2 x 30 mg (nicht gewichtsadaptiert) vs LDUH (1)
– 1 x 40 mg in ödematösen Patienten leicht erhöhte Anti-FXa Spiegel (2)
1. Geerts WH et al.: A comparison of low-dose heparin with low-molecular-weight heparin as prophylaxisagainst venous thromboembolism after major trauma. NEJM 1996; 335: 701 – 707
2. Haas CE et al.: Pharmacokinetics and pharmacodynamics of enoxaparin in multiple trauma patient. J Trauma 2005; 59: 1336 - 1344

Dalteparin (Fragmin©)• 1x/Tag nicht gewichtsadaptiert in high risk
Traumapatienten 4% TVT bei DFCI und symptomatische nicht fatale LE in < 1% (1)
• Keine chirurgische Blutung oder intrakranielle Blutungen
• Retrospektive Analyse Dalteparin (3000 IE/die) vs Enoxaparin (2 x 30 mg): keine Unterschiede in TVT und LE (2)
1. Cothren CC et al.: Utility of once-daily dose of low-molecular-weight heparin to prevent venousthromboembolism in multisystem trauma patients. World J Surg 2007; 31: 98 - 104
2. Slavik RS et al.: Dalteparin versus enoxaparin for venous thromboembolism prophylaxis in acute spinal cordinjury and major orthopedic trauma patients: „DETECT„ trial. J Trauma 2007; 62; 1075 - 1081

Fondaparinux (Arixtra©)
• Pentasaccharid, selektiver FXa-Hemmer
• Gute Resultate bei orthopädischen und Patienten mit Abdominalchirurgie
• In Traumapatienten Studie am Laufen

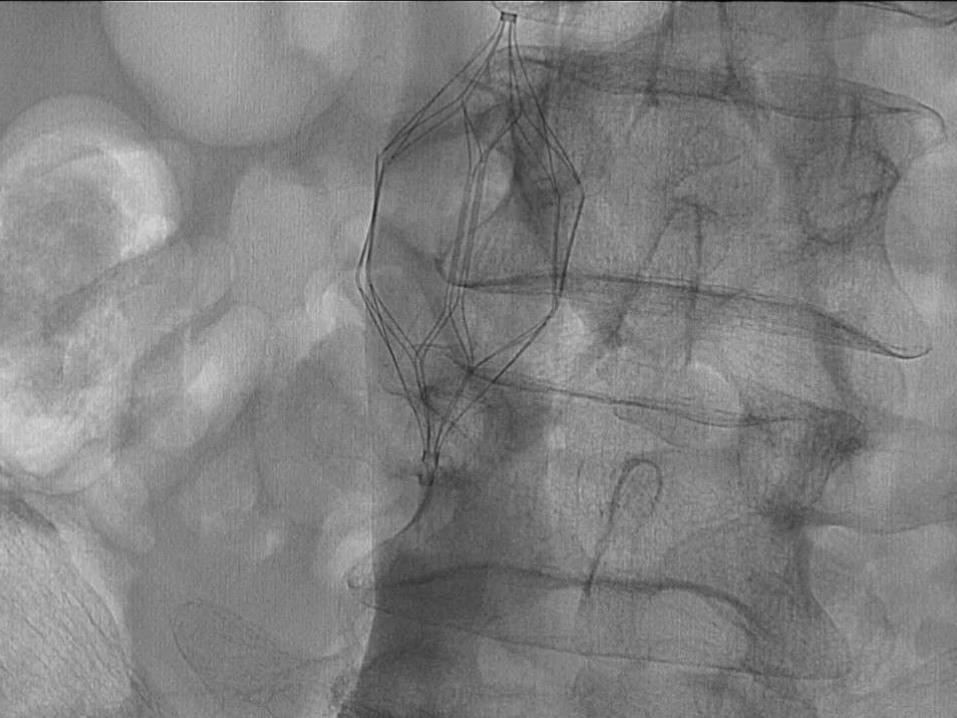
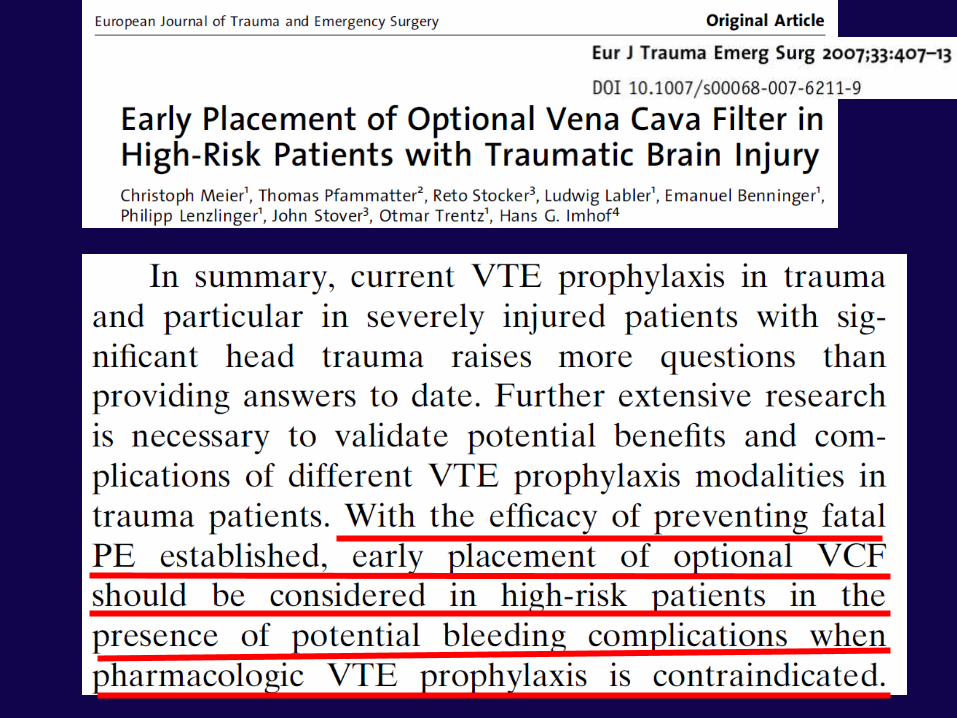
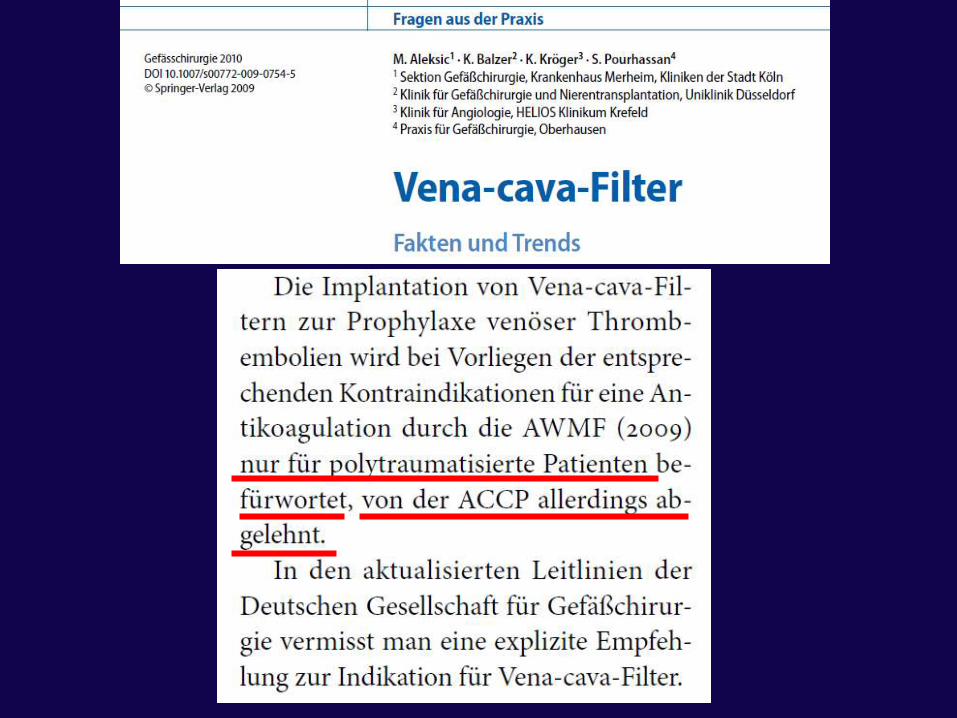
Vena cava filter
• Indikationen
• Komplikationen
• Timing und Dauer


Indikationen
• Klasse III in EAST bei sehr Hochrisikopatienten (GCS < 8, WS-Verletzungen, komplexe Beckenfrakturen, # lange Röhrenknochen) mit zusätzlichem Blutungsrisiko (ICB, Läsionen grosser Organe, Gerinnungsstörungen) (1)
• 0,8% in USA, 80% prophylaktisch, fehlendes TVT-Risiko in 10% (2)
1. Rogers FB et al.: Practice management guidelines for the prevention of venous thromboembolism in traumapatients. The EAST practice guidelines work group. J Trauma 2002; 53: 142 - 164
2. Knudson MM et al.: Thromboembolism after trauma: an analysis of 1602 episodes from the American College of Surgeons National Trauma Data Bank. Ann Surg 2004; 240: 490 - 498
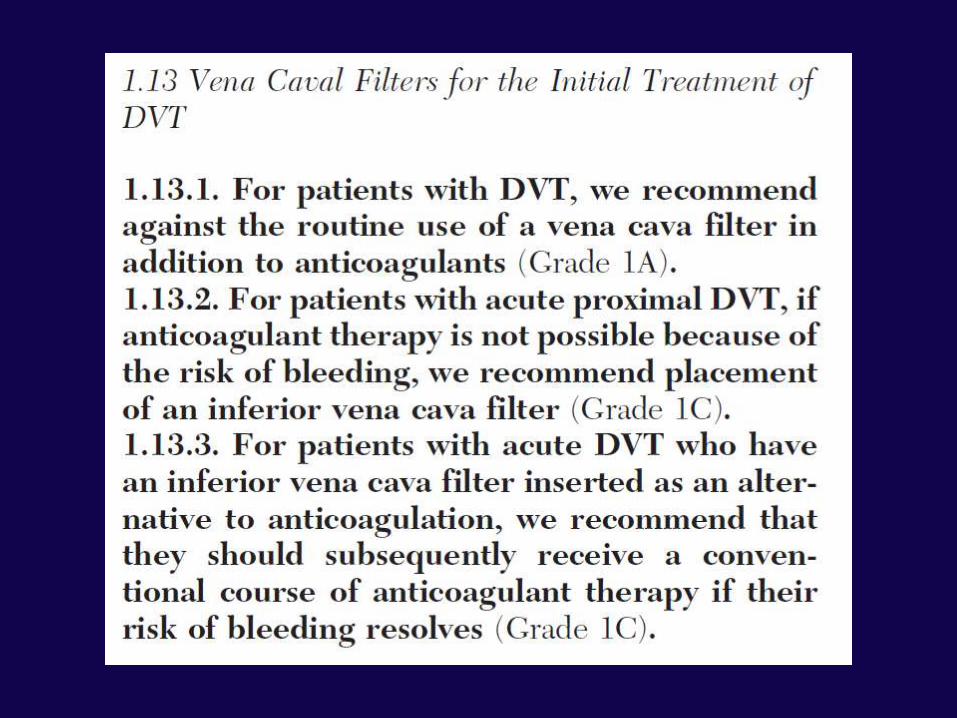
Indikationen
• Keine Indikation gemäss APPC-Richtlinien
• Keine RCT bezüglich Typ und Einlagetechnik
• 80% wieder entfernbar (1), bedside bevorzugt (2)
1. Karmy-Jones R et al.: Practice patterns and outcomes of retrievable vena cava filters in trauma patients: a AAST multi-center study. J Trauma 2007; 62: 17 - 25
2. Spaniolas K et al.: Bedside placement of removable vena cava filters guided by intravascular ultrasound in the critically injured. World J Surg 2008; 32: 1438 - 1443
Komplikationen
• Inzidenz LE 5% (1)
• Vena cava Thrombose mit Cavaverschluss 0-11% (2,3)
• Dislokationen bis rechter Ventrikel (4)
• Wiederentfernbar bis zu > 40% (5)
1. Young T et al.: Vena caval filters for the prevention of pulmonary embolism. Cochrane Database Syst Rev2007: CD006212
2. Karmy-Jones R et al.: Practice patterns and outcomes of retrievable vena cava filters in trauma patients: a AAST multi-center study. J Trauma 2007; 62: 17 - 25
3. Kinney TB: Update on inferior vena cava filters. J Vasc Interv Radiol 2003; 14: 425 - 4404. Adair JD et al.: Inferior vena cava filter migration to right ventricle with destruction of tricuspid valve: a case
report. J Trauma 2008; 64: 509 - 5115. Hermsen JL et al.: Retrievable inferior vena cava filters in high-risk trauma and surgical patients: factors
influencing successful removal. World J Surg 2008; 32: 1444 - 1449

Zeitpunkt und Dauer
• 446 Einlagen in 6 +/-8 Tage (1)
• Idealerweise innert 48 h
• 11% erleiden LE bis nach 22 Tage Entfernung erst danach (2)
• Entfernbarkeit unabhängig von Liegedauer (3)
1. Karmy-Jones R et al.: Practice patterns and outcomes of retrievable vena cava filters in trauma patients: a AAST multi-center study. J Trauma 2007; 62: 17 - 25
2. Sing RF et al.: Timing of pulmonary emboli after trauma: implications for retrievable vena cava filters. J Trauma 2006; 60: 732 - 735
3. Hermsen JL et al.: Retrievable inferior vena cava filters in high-risk trauma and surgical patients: factorsinfluencing successful removal. World J Surg 2008; 32: 1444 - 1449

Konklusionen
• Jeder Traumapatient sollte eine Thromboembolieprophylaxe erhalten
• Jede IS sollte Richtlinien für die Thromboembolieprophylaxe beim Polytrauma haben
• Mechanische Devices und LMWH sind die erste Wahl
• Starte frühzeitig (innert 36 Std.)