Thyroid Abscess Due to Staphylococcus Epidermidis6. Jacobs A, Gros DC, Gradon JD. Thyroid Abscess...
3
Bombay Hospital Journal, Vol. 54, No. 2, 2012 Thyroid Abscess Due to Staphylococcus Epidermidis K. Shanmuga Priya*, G. Prabhu*, N. Sindhumathi*, M. V. Reddy**, M. # ## Chandrasekaran , K. Jagadeesan *Post Graduate Student, **Practicing Rural Surgeon, # ## Endocrine Surgeon, Surgeon, Chairman and Director, K. J. Hospital Research and Postgraduate Centre, Chennai - 600084. Abstract Acute suppurative thyroiditis - infection of the thyroid gland is uncommon constituting only 0.1-0.7% of the surgical thyroid pathologies. Many such cases have been reviewed and reported on. Here we review a male patient with history of hypothyroidism for two years now presenting with abscess in thyroid. Introduction hyroid abscess is a rare entity. It Tusually occurs in patients with a pre existing thyroid pathology. The organisms commonly associated with thyroid abscess are staph aureus, streptococcus etc. We present a case of thyroid abscess in a 41 year old male due to staphylococcus epidermidis. Case Report A 41 year old male patient came with complaints of swelling in front of neck for 2 years. It gradually increased in size and he had difficulty in swallowing, pain and fever for 4 days. He had history suggestive of hypothyroidism and was under treatment with 150 μg thyroxine. He is a known epileptic for past 15 years on regular treatment with eptoin, carbamazepine and sodium valproate. On examination patient was febrile with a single swelling over the front of neck of about 12 x 6 cm, prominent on right side, moves with deglutition. The plane of swelling was deep to deep fascia. On palpation it was warm and tender. Surface was smooth with no nodularity. Lower border was visible. Blood investigations showed an Hb of 13 g% with total WBC-9, 100/ cu.mm with a rise in polymorphs to 77%, ESR 42 mm at ½ hr and 128 mm at one hour. Renal and liver function parameters were normal. Urine culture sensitivity showed the presence of E.coli. T3 - 64ng/dl [60-200ng/dl], T4 - 10.10μg/dl[4.5 - 12 μg/dl], TSH - 0.15μIU/ml [0.30- 5.5 μIU/ml]. HIV testing showed him to be negative. X-ray AP and lateral view of neck showed a soft tissue swelling on the right side over thyroid and displacing trachea to left. USG showed a cystic mass with homogenous echo pattern of 8.0 x 4.8 x 2.0 cm (Fig. 1) Bilateral submandibular nodes enlarged with normal appearing left lobe and isthmus. Thyroidectomy was planned but difficulty was encountered while introducing endotracheal tube due to shift of trachea with reduced lumen. Under local anaesthesia incision and drainage was done. 300 ml of seropurulent fluid was obtained and sent for microbiological examination. It showed gram positive cocci which on culture were staphylococcus epidermidis susceptible to norfloxacin, cephazolin and tetracycline. The swelling reduced in size Fig. 1: USG showing a cystic mass with homogenous echo pattern 297
Transcript of Thyroid Abscess Due to Staphylococcus Epidermidis6. Jacobs A, Gros DC, Gradon JD. Thyroid Abscess...

Bombay Hospital Journal, Vol. 54, No. 2, 2012
Thyroid Abscess Due to Staphylococcus Epidermidis
K. Shanmuga Priya*, G. Prabhu*, N. Sindhumathi*, M. V. Reddy**, M. # ##Chandrasekaran , K. Jagadeesan
*Post Graduate Student, **Practicing Rural Surgeon, # ##Endocrine Surgeon, Surgeon, Chairman and
Director, K. J. Hospital Research and Postgraduate
Centre, Chennai - 600084.
Abstract
Acute suppurative thyroiditis - infection of the thyroid gland is uncommon
constituting only 0.1-0.7% of the surgical thyroid pathologies. Many such cases have
been reviewed and reported on. Here we review a male patient with history of
hypothyroidism for two years now presenting with abscess in thyroid.
Introduction
hyroid abscess is a rare entity. It Tusually occurs in patients with a pre
existing thyroid pathology. The organisms
commonly associated with thyroid abscess
are staph aureus, streptococcus etc. We
present a case of thyroid abscess in a 41
year old male due to staphylococcus
epidermidis.
Case Report
A 41 year old male patient came with complaints
of swelling in front of neck for 2 years. It gradually
increased in size and he had difficulty in swallowing,
pain and fever for 4 days. He had history suggestive of
hypothyroidism and was under treatment with
150 µg thyroxine. He is a known epileptic for past 15
years on regular treatment with eptoin,
carbamazepine and sodium valproate. On
examination patient was febrile with a single swelling
over the front of neck of about 12 x 6 cm, prominent
on right side, moves with deglutition. The plane of
swelling was deep to deep fascia. On palpation it was
warm and tender. Surface was smooth with no
nodularity. Lower border was visible. Blood
investigations showed an Hb of 13 g% with total
WBC-9, 100/ cu.mm with a rise in polymorphs to
77%, ESR 42 mm at ½ hr and 128 mm at one hour.
Renal and liver function parameters were normal.
Urine culture sensitivity showed the presence of
E.coli. T3 - 64ng/dl [60-200ng/dl], T4 -
10.10µg/dl[4.5 - 12 µg/dl], TSH - 0.15µIU/ml [0.30-
5.5 µIU/ml]. HIV testing showed him to be negative.
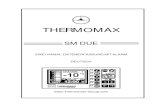
X-ray AP and lateral view of neck showed a soft
tissue swelling on the right side over thyroid and
displacing trachea to left. USG showed a cystic mass
with homogenous echo pattern of 8.0 x 4.8 x 2.0 cm
(Fig. 1)
Bilateral submandibular nodes enlarged with normal
appearing left lobe and isthmus. Thyroidectomy was
planned but difficulty was encountered while
introducing endotracheal tube due to shift of trachea
with reduced lumen. Under local anaesthesia
incision and drainage was done. 300 ml of
seropurulent fluid was obtained and sent for
microbiological examination. It showed gram positive
cocci which on culture were staphylococcus
epidermidis susceptible to norfloxacin, cephazolin
and tetracycline. The swelling reduced in size
Fig. 1: USG showing a cystic mass with homogenous echo pattern
297

Bombay Hospital Journal, Vol. 54, No. 2, 2012
following the procedure. Surgery was postponed and
in the meantime the patient was put on antibiotics
and thyroxine. Soft tissue X-ray neck taken after a
few days showed a dramatic reduction of soft tissue
on the right side of neck. Surgery was planned under
GA. Through a skin crease collar incision the thyroid
gland was exposed. It showed a mass in right lobe.
Classical right hemithyroidectomy was done and the
specimen sent for HPE. It showed thyroid follicles of
varying sizes filled with colloid and a cyst containing
haemorrhage (Fig. 2 and 3) with thickened cyst wall
due to fibrosis along with cholesterol clefts. No
evidence of malignancy seen.
Discussion
Thyroid abscess or acute suppurative
thyroiditis (AST) is uncommon. It is an
acute inflammatory condition due to
infection of thyroid gland. The most
common organisms are staphylococcus
and streptococcus. However rarely
o r g a n i s m s l i k e A c i n e t o b a c t e r
c a l c o a c e t i c u s , F u s o b a c t e r i u m
morteiferum., Salmonella, Eikennella
corrodens, Nocardia has been implicated.
Mycobacteria, Rhodococcus equi,
Anaerobes are common pathogens in HIV
patients.
Thyroid gland has inherent resistance
to infections owing to its high iodine
content, tough capsule, good blood supply
and lymphatic drainage, anatomic
isolation. The common predisposing
factors are pre existing thyroid pathologies
like a cyst or nodule, congenital pyriform
sinus fistula, following Fine needle
aspiration cytology (FNAC), direct trauma,
immuno compromised state. It can also
occur following a respiratory or urinary
tract infection and rarely through
haematogenous spread.
AST is a painful condition and should
be differentiated from other painful
conditions of thyroid like de quervain
thyroiditis, rapidly progressive carcinoma
and haemorrhage into a cyst.
AST presents with fever, pain,
dysphagia and tachycardia. AST may
present as pulsatile swelling. But it may
sometimes follow an insidious course like
the index case with minimal signs and
symptoms of inflammation. Two cases of
vocal cord paralysis have been reported.
FNAC can be done to determine the type of
organism and its antibiotic susceptibility.
Untreated thyroid abscess may go in
for complications like jugular vein
Fig. 2 Cut section of thyroid gland showing thyroid follicle with abscess cavity and areas of haemorrhage
Fig. 3: Histopathology section showing colloid filled follicles with cholesterol cleft
298

Bombay Hospital Journal, Vol. 54, No. 2, 2012
thrombosis, sepsis, rupture, destruction
of thyroid and parathyroid glands and
formation of sinus or fistula. Abscess in
long standing goitre is an acute
emergency.
Different modalities of treatment have
been tried with varying results.
Ultrasonographic drainage or incision and
drainage followed by treatment with
susceptible antibiotics or surgical removal
of the abscess cavity along with part of
gland can be done.
Conclusion
We are reporting this in view of the
rarity of the case. The anaesthetic problem
where the intubation became critical. The
draining of the abscess of about 300 ml of
seropurulent material relieved the
obstruction of the airway, thereafter
intubation was made possible. It is noted
within a short period of 24 hours, the fluid
reaccumulated to the tune of about
100 ml. surgical resection was challenging
because of the adhesions around the
surrounding tissues. Extreme degree of
care was taken to save the neurological
structures and parathyroid. Post operative
period was uneventful. Patient's voice and
vocal cord functions remain normal. In
such situation where intubation become
difficult, on the spot tapping and
intubation or tracheostomy could be
attempted.
References
1. Rohondia O S, Koti R S, Majumdar P P,
Vijaykumar T, Bapat R D, Thyroid abscess. J
Postgrad Med. 1995;41:52-54.
2. Nishihara E, Miyauchi A, Matsuzuka F, Sasaki I,
Ohye H, Kubota S, Fukata S, Amino N,Kuma K.
Acute suppurative thyroiditis after fine-needle
aspiration causing thyrotoxicosis. Thyroid.
2005;15:1183-1187.
3. Nikolaos P. Stavreas, Constantina D.
Amanatidou, Emmanuel G. Hatzimanolis et al.
Thyroid Abscess Due to a Mixed Anaerobic
Infection with Fusobacteriummortiferum.
4. Menegaux, F., G. Biro, C. Schatz, and J. P.
Chigot. Thyroid abscess. Apropos of 5 cases,
Ann. Med. Interne (Paris). 1991;142:99-102.
5. Schneider, U, R. Birnbacher, S. Schick, W.
Ponhold, and E. Schober. Recurrent
suppurative thyroiditis due to pyriform sinus
fistula: Eur. J. Pediatr 1995;154:640-642
6. Jacobs A, Gros DC, Gradon JD. Thyroid Abscess
Due to Acinetobacter calcoaceticus: Case Report
and Review of the Causes of and Current
Management Strategies for Thyroid Abscesses
Southern Medical Associat ion. 2003
Mar;96(3):300-307.
7. Thyroid abscess caused by Eikenella corrodens.
Cheng AF, Man DW, French GL. Department of
Microbiology, Chinese University of Hong Kong.
8. Gram-negative thyroid abscess resulting from
fine-needle aspiration in animmunosuppressed
patient Wang. Yu-Chun | Yeh, Ta-Sen | Lin,
Jen-Der Clinical Infectious Diseases [CLIN.
INFECT. DIS]. 1997; Vol. 25, No.3, pp. 745-746.,
Sep.
9. Barton, Gary M. Shoup, William B. Bennett,
William G. Williams, James B. Vesely, David L.
Combined Escherichia Coli and Staphylococcus
Aureus Thyroid Abscess in an Asymptomatic
Man.
Antiretroviral Therapy in TB and HIV Coinfection
In this study from Cambodia, giving antiretrovirals 2 weeks after the start of TB therapy was superior to therapy begun at 8 weeks, with a decrease in mortality.
N ENGL J MED 2011; 1470365;16;
299