
Was ist in der Risikoadjustierung mittels administrativer ... · PubMed-ID: 19690309 Langan SM,...
24
Was ist in der Risikoadjustierung mittels administrativer Routinedaten gesichert? Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte e. V. Berlin, 13.02.2015
Transcript of Was ist in der Risikoadjustierung mittels administrativer ... · PubMed-ID: 19690309 Langan SM,...
Was ist in der Risikoadjustierung mittels administrativer Routinedaten gesichert?
Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte e. V.
Berlin, 13.02.2015

Vorbemerkungen
3
4
5
6
91 Leitsätze und Empfehlungen Einführung
Grundlagen
Modellentwicklung
Multiple logistische Regression
Bewertung der Prognosegüte
Modellvalidierung
Übertragbarkeit
Transparenz
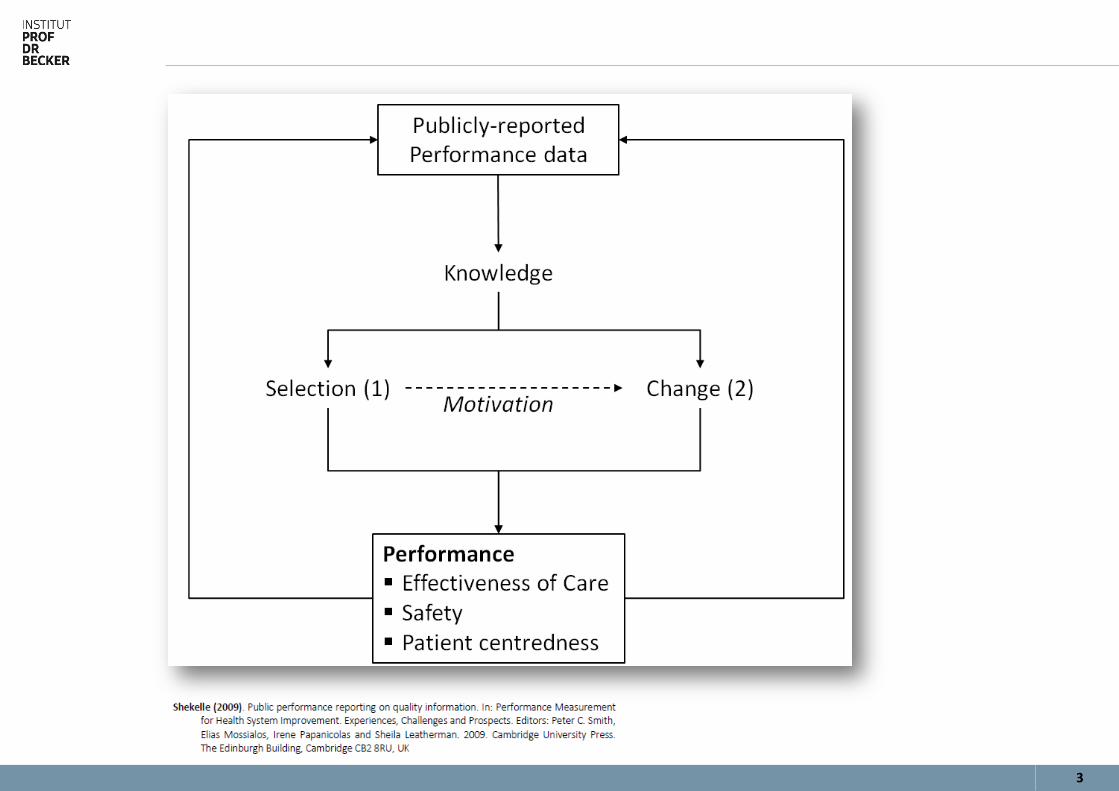
Public Reporting
Risikoadjustierung löst doch alle Probleme!?
8
Risiken der Risikoadjustierung Datenqualität (»Es gibt doch einheitliche Regelwerke«).
Definitionen (»Es gibt doch einheitliche Regelwerke«).
Sonderkodes in der ICD-10-GM für spezifische Komplikationen?
Fehlendes Kennzeichen »Present On Admission«.
CPR bei Aufnahme – Wie geht man mit diesen Fällen um?
Unspezifische Kodes (I21.9 Akuter Myokardinfarkt, nicht näher bezeichnet)
Warum kommen in meinem Modell aus Studien bekannte und aus klinischer Sicht plausible Risikofaktoren nicht vor?
Warum ist das OR eines Risikofaktors sehr hoch mit einem sehr weiten Konfidenzintervall?
Administrative Routinedaten verführen zum Ansatz »Die Statistiksoftware entwickelt das Modell«.
9
Paradoxe Variablen bzw. Effekte Kodierungsfehler.
Interaktionen der Einflussvariablen.
Multikollinearität.
Sehr unterschiedlicher Umgang damit in der Literatur.
Von Ignorieren bis zu »… der darunter liegende Mechanismus ist bisher unbekannt.«
10
11
12
13
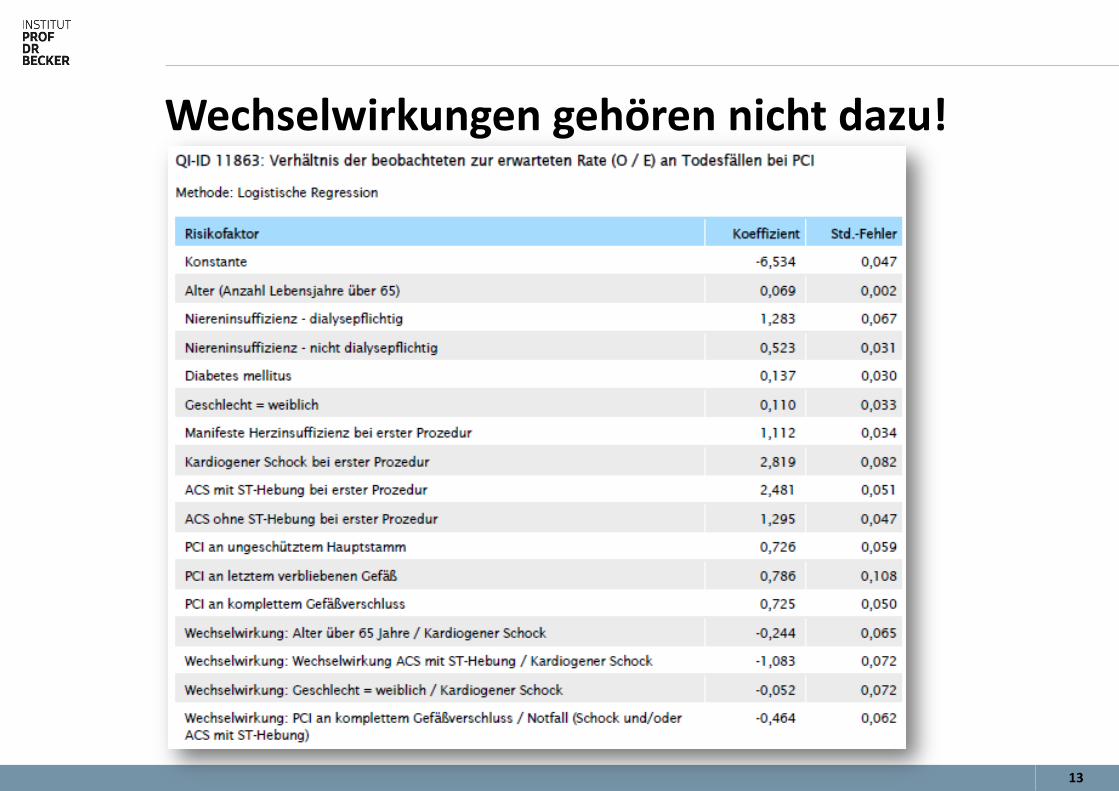
Wechselwirkungen gehören nicht dazu!
14
Manktelow BN, Evans TA, Draper ES (2014). Differences in case-mix can influence the comparison of standardised mortality ratios even with optimal risk adjustment: an analysis of data from paediatric intensive care. BMJ Qual Saf. 2014. PubMed-ID: 24840239
Doch noch ein Problem mit dem case-mix?
15
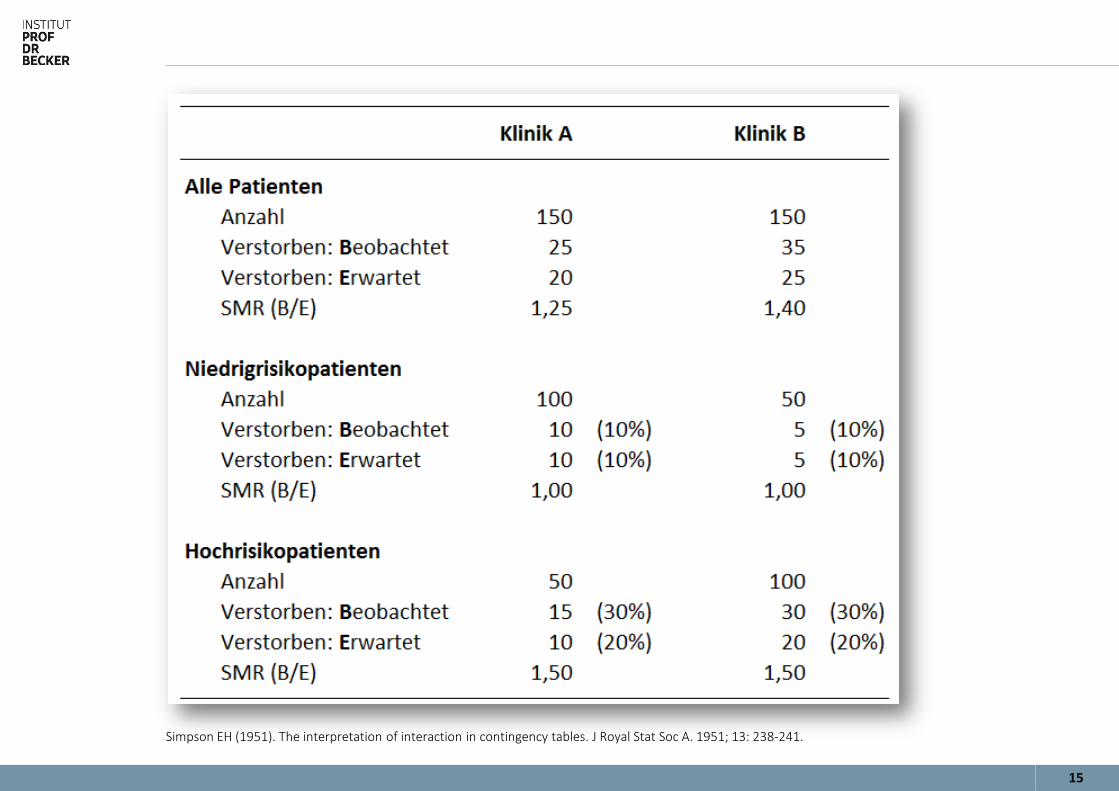
Simpson EH (1951). The interpretation of interaction in contingency tables. J Royal Stat Soc A. 1951; 13: 238-241.
16
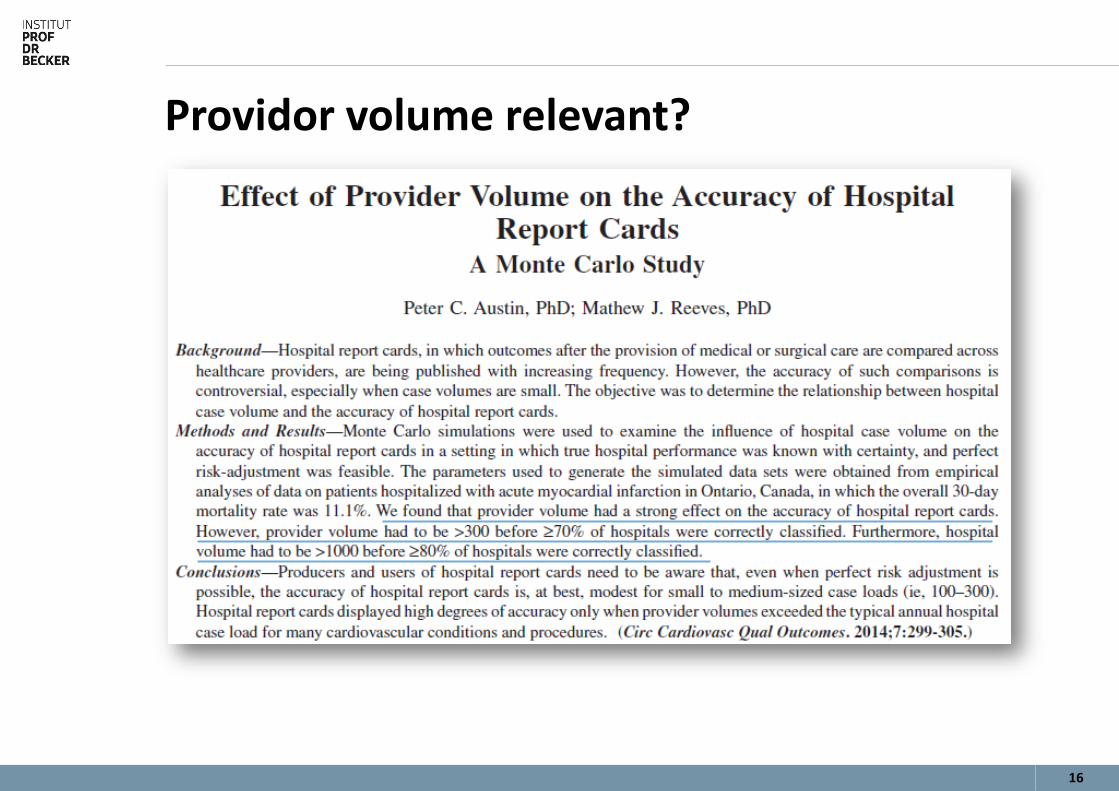
Providor volume relevant?

17
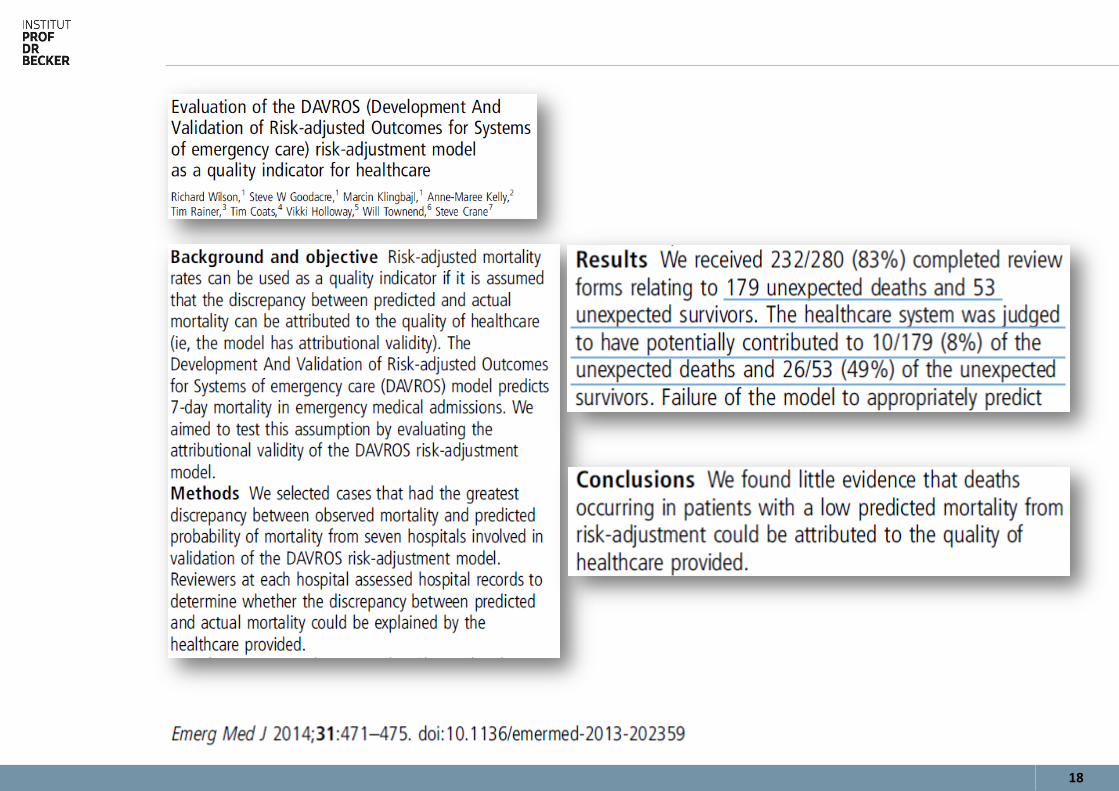
Träume von Rankings?
18
19
»Wahrheit ist ein brauchbarer Irrtum.«
Zitiert nach Hans Vaihinger, Philosophie des Als Ob., 1911 Prof. Dr. Theo Wehner, ETH Zürich, Institut für Arbeits- und Organisationspsychologie Vortrag »Qualität und Patientensicherheit: beides verlangt Verantwortung, beides erzeugt Verantwortungsdiffusion« 11. ZQ-Forum Patientensicherheit und Risikomanagement, Hannover, 11.10.2014
20
Andersen KK, Olsen TS (2015). The obesity paradox in stroke: lower mortality and lower risk of readmission for recurrent stroke in obese stroke patients. Int J Stroke. 2015; 10 (1): 99-104. PubMed-ID: 25635277
Becker A (2012). Present-On-Admission-Kennzeichen (POA) für administrative Routinedaten in Krankenhäusern. Literaturübersicht und Handlungsempfehlungen. Eine Ausarbeitung für die Gesellschaft für Qualitätsma-nagement in der Gesundheitsversorgung e.V. (GQMG). Quelle: http://www.i-pdb.de/files/48-poa-vollversion-stand-2012-03-12.pdf
Benchimol EI, Langan S, Guttmann A (2013). Call to RECORD: the need for complete reporting of research using routinely collected health data. J Clin Epidemiol. 2013; 66 (7): 703-705. PubMed-ID: 23186992
Gurevich Y, McFarlane A, Morris K, Jokovic A, Peterson GM, Webster GK (2010). Estimating the number of coronary artery bypass graft and percutaneous coronary intervention procedures in Canada: a comparison of cardiac registry and Canadian Institute for Health Information data sources. Can J Cardiol. 2010; 26 (7): e249-53. PubMed-ID: 20847972
Heller G (2008). Zur Messung und Darstellung von medizinischer Ergebnisqualität mit administrativen Routinedaten in Deutschland. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2008; 51 (10): 1173-1182. PubMed-ID: 18985411
Heller G, Babitsch B, Günster C, Möckel M (2008). Mortality following myocardial infarction in women and men: an analysis of insurance claims data from inpatient hospitalizations. Dtsch Arztebl Int. 2008; 105 (15): 279-285. PubMed-ID: 19629233
Hess CN, Rao SV, McCoy LA, Neely ML, Singh M, Spertus JA, Krone RJ, Weaver WD, Peterson ED (2015). Identification of hospital outliers in bleeding complications after percutaneous coronary intervention. Circ Cardiovasc Qual Outcomes. 2015; 8 (1): 15-22. PubMed-ID: 25424242
Hotchkiss JW, Davies CA, Dundas R, Hawkins N, Jhund PS, Scholes S, Bajekal M, O'Flaherty M, Critchley J, Leyland AH, Capewell S (2014). Explaining trends in Scottish coronary heart disease mortality between 2000 and 2010 using IMPACTSEC model: retrospective analysis using routine data. BMJ. 2014; 348 (): g1088. PubMed-ID: 24503058
Ausgewählte Literatur
21
Jarman B, Pieter D, van der Veen A, Kool RB, Aylin P, Bottle A, Westert GP, Jones S (2010). The hospital standardised mortality ratio: a powerful tool for Dutch hospitals to assess their quality of care? Qual Saf Health Care. 2010; 19 (1): 9-13. PubMed-ID: 20172876
Klakow-Franck R (2014). Perspektive: Rolle der Qualitätsmessung aus Sicht des Gemeinsamen Bundesausschusses. Z Evid Fortbild Qual Gesundhwes. 2014; 108 (8-9): 456-464. PubMed-ID: 25523843
Koek HL, Kardaun, Jan W P F, Gevers E, Bruin A de, Reitsma JB, Grobbee DE, Bots ML (2007). Acute myocardial infarction incidence and hospital mortality: routinely collected national data versus linkage of national registers. Eur. J. Epidemiol. 2007; 22 (11): 755-762. PubMed-ID: 17828438
Krumholz HM, Brindis RG, Brush JE, Cohen DJ, Epstein AJ, Furie K, Howard G, Peterson ED, Rathore SS, Smith SC, Spertus JA, Wang Y, Normand ST (2006). Standards for statistical models used for public reporting of health outcomes: an American Heart Association Scientific Statement from the Quality of Care and Outcomes Research Interdisciplinary Writing Group: cosponsored by the Council on Epidemiology and Prevention and the Stroke Council. Endorsed by the American College of Cardiology Foundation. Circulation. 2006; 113 (3): 456-462. PubMed-ID: 16365198
Krumholz HM, Normand ST (2008). Public reporting of 30-day mortality for patients hospitalized with acute myocardial infarction and heart failure. Circulation. 2008; 118 (13): 1394-1397. PubMed-ID: 18725492
Krumholz HM, Normand ST, Spertus JA, Shahian DM, Bradley EH (2007). Measuring performance for treating heart attacks and heart failure: the case for outcomes measurement. Health Aff (Millwood). 2007; 26 (1): 75-85. PubMed-ID: 17211016
Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, Roman S, Normand ST (2006). An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with heart failure. Circulation. 2006; 113 (13): 1693-1701. PubMed-ID: 16549636
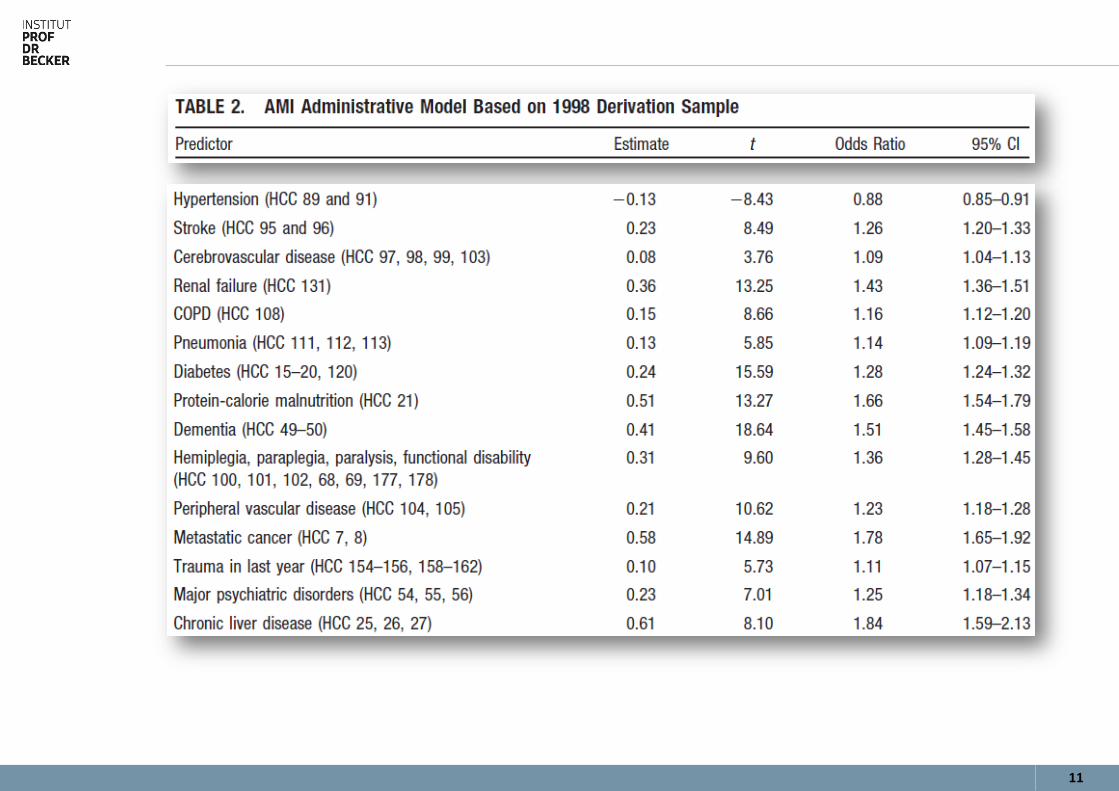
Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, Roman S, Normand ST (2006). An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with an acute myocardial infarction. Circulation. 2006; 113 (13): 1683-1692. PubMed-ID: 16549637
Ausgewählte Literatur
22
Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, Roman S, Normand ST (2006). An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with an acute myocardial infarction. Circulation. 2006; 113 (13): 1683-1692. PubMed-ID: 16549637
Krumholz HM, Wang Y, Chen J, Drye EE, Spertus JA, Ross JS, Curtis JP, Nallamothu BK, Lichtman JH, Havranek EP, Masoudi FA, Radford MJ, Han LF, Rapp MT, Straube BM, Normand ST (2009). Reduction in acute myocardial infarction mortality in the United States: risk-standardized mortality rates from 1995-2006. JAMA. 2009; 302 (7): 767-773. PubMed-ID: 19690309
Langan SM, Benchimol EI, Guttmann A, Moher D, Petersen I, Smeeth L, Sørensen HT, Stanley F, Elm E von (2013). Setting the RECORD straight: developing a guideline for the REporting of studies Conducted using Observational Routinely collected Data. Clin Epidemiol. 2013; 5 (): 29-31. PubMed-ID: 23413321
Lusignan S de, Sun B, Pearce C, Farmer C, Steven P, Jones S (2014). Coding errors in an analysis of the impact of pay-for-performance on the care for long-term cardiovascular disease: a case study. Inform Prim Care. 2014; 21 (2): 92-101. PubMed-ID: 24841410
Normand ST, Glickman ME, Sharma RG, McNeil BJ (1996). Using admission characteristics to predict short-term mortality from myocardial infarction in elderly patients. Results from the Cooperative Cardiovascular Project. JAMA. 1996; 275 (17): 1322-1328. PubMed-ID: 8614117
Rath T, Büscher G, Schwartze D, Drabik A, Bokern E, Lüngen M (2010). Analyse von Mortalitäten und Konzentrationstendenzen in der stationären Versorgung von Schlaganfall und Myokardinfarkt. Herz. 2010; 35 (6): 389-396. PubMed-ID: 20814655
Renzi C, Asta F, Fusco D, Agabiti N, Davoli M, Perucci CA (2014). Does public reporting improve the quality of hospital care for acute myocardial infarction? Results from a regional outcome evaluation program in Italy. Int J Qual Health Care. 2014; 26 (3): 223-230. PubMed-ID: 24737832
Ross JS, Chen J, Lin Z, Bueno H, Curtis JP, Keenan PS, Normand ST, Schreiner G, Spertus JA, Vidán MT, Wang Y, Wang Y, Krumholz HM (2010). Recent national trends in readmission rates after heart failure hospitalization. Circ Heart Fail. 2010; 3 (1): 97-103. PubMed-ID: 19903931
Ausgewählte Literatur
23
Ross JS, Maynard C, Krumholz HM, Sun H, Rumsfeld JS, Normand ST, Wang Y, Fihn SD (2010). Use of administrative claims models to assess 30-day mortality among Veterans Health Administration hospitals. Med Care. 2010; 48 (7): 652-658. PubMed-ID: 20548253
Ross JS, Normand ST, Wang Y, Nallamothu BK, Lichtman JH, Krumholz HM (2008). Hospital remoteness and thirty-day mortality from three serious conditions. Health Aff (Millwood). 2008; 27 (6): 1707-1717. PubMed-ID: 18997230
So L, Evans D, Quan H (2006). ICD-10 coding algorithms for defining comorbidities of acute myocardial infarction. BMC Health Serv Res. 2006; 6 (): 161. PubMed-ID: 17173686
Swart E, Schmitt J (2014). STandardized Reporting Of Secondary data Analyses (STROSA) - Vorschlag für ein Berichtsformat für Sekundärdatenanalysen. Z Evid Fortbild Qual Gesundhwes. 2014; 108 (8-9): 511-516. PubMed-ID: 25523850
van Walraven C, Austin P (2012). Administrative database research has unique characteristics that can risk biased results. J Clin Epidemiol. 2012; 65 (2): 126-131. PubMed-ID: 22075111
Ausgewählte Literatur
Vielen Dank! T +49 2205 920 460 F +49 2205 920 462 M +49 172 29 88 040 E [email protected] W www.i-pdb.de Institut Prof. Dr. Becker Nonnenweg 120a 51503 Rösrath








