Weiss Lecture
16
INT .J .RADIAT .BIOL .,1991,VOL .쓀9,NO .3, 쓀 9 쓀 -610 WeissLecture' Thedose-ratefactorinradiationbiology E .J .HALL CenterforRadiologicalResearch,CollegeofPhysicansandSurgeonsof ColumbiaUniversity,NewYork,NY,USA (Received1October1990 ;accepted22October1990) Thedose-rateeffecthasbeenthetopicofextensiveradiobiologicalstudiesand hasimportantimplicationsinradiationtherapyandinthefieldofradiation protection .Threeexampleswillbediscussed :twoinradiationtherapyandone inprotection.First,continuouslowdose-rateinterstitialbrachytherapymaybe replacedbypulsedbrachytherapy,usingasinglesourcemovingthroughthe cathetersoftheimplant .Thisstrategy,usingamoderncomputer-controlled afterloadingdevice,wouldallowbetterdoseoptimizationandresultina considerablecostsaving .Radiobiologicaldatahaveprovedusefulindefiningthe pulselengthandpulsefrequencythatisequivalenttocontinuouslowdose-rate . Second,intheintracavitarytreatmentofcarcinomaofthecervix,afewhigh dose-rate(HDR)fractionsonanoutpatientsbasiscanreplacethelowdose-rate (LDR)treatmentthatrequiresthepatienttobehospitalizedforseveraldays . RadiobiologicaldatacanbeusedtoestimatethedoselevelsatHDRthatare equivalenttoconventionalLDRprotocols .Third,itisusuallyassumedin radiationprotectionthatdosesaccumulatedoveraperiodoftimeatlowdose- ratearelesseffectivebiologicallythanthesamedosedeliveredinasingleacute exposure .WhilethismaybetrueforX-ory-rays,radiobiologicaldataindicate thatneutronsdeliveredatlowdoseorinaseriesoffractionsspreadoutovera periodoftimemayproducemoreoncogenictransformationthanasingleacute exposure .Thishasimportantimplicationsinradiationprotection . 1 .Introduction IfeelveryhonouredtoreceivetheWeissMedal,andgratefultothosewho thoughtmeworthyofit .Thereisacertainfeelingofdeja-vuformetoreturnto Oxfordforthisoccasion ;myfirstjobwashereattheChurchillHospital,anditwas atOxfordasagraduatestudentthatIwasfirstintroducedtoradiationphysicsand radiationbiology. Thebiologicaleffectsofionizingradiationcorrelatecloselywiththeenergy absorbedperunitmass(i .e .thedose) .Foragivendose,biologicaleffectsdepend, too,onthepatternofenergydepositionatthemicroscopiclevel,i .e .thequalityof theradiationexpressedintermsofthelinearenergytransfer(LET),andontherate ofenergydeposition,i .e .thedose-rate .Theselattertwofactorsarenotindependent variables,sincethedose-rateeffectvariesqualitativelyandquantitativelywith tGivenontheoccasionofthepresentationoftheWeissMedaltotheauthor,forhis contributionstotheadvancementofknowledgeinthefieldofradiobiology,attheAssoci- ationforRadiationResearchmeetingattheClarendonLaboratory,OxfordUniversity,UK 쓀April1990 . 0020-7616/91$3 .00©1991Taylor&FrancisLtd Int J Radiat Biol Downloaded from informahealthcare.com by University of Melbourne on 11/06/14 For personal use only.
Transcript of Weiss Lecture

INT . J . RADIAT . BIOL ., 1991, VOL . 쓀9, NO . 3, 쓀9쓀 -610
Weiss Lecture'
The dose-rate factor in radiation biology
E. J. HALLCenter for Radiological Research, College of Physicans and Surgeons ofColumbia University, New York, NY, USA
(Received 1 October 1990 ; accepted 22 October 1990)
The dose-rate effect has been the topic of extensive radiobiological studies andhas important implications in radiation therapy and in the field of radiationprotection . Three examples will be discussed : two in radiation therapy and onein protection. First, continuous low dose-rate interstitial brachytherapy may bereplaced by pulsed brachytherapy, using a single source moving through thecatheters of the implant . This strategy, using a modern computer-controlledafterloading device, would allow better dose optimization and result in aconsiderable cost saving . Radiobiological data have proved useful in defining thepulse length and pulse frequency that is equivalent to continuous low dose-rate .Second, in the intracavitary treatment of carcinoma of the cervix, a few highdose-rate (HDR) fractions on an outpatients basis can replace the low dose-rate(LDR) treatment that requires the patient to be hospitalized for several days .Radiobiological data can be used to estimate the dose levels at HDR that areequivalent to conventional LDR protocols. Third, it is usually assumed inradiation protection that doses accumulated over a period of time at low dose-rate are less effective biologically than the same dose delivered in a single acuteexposure . While this may be true for X- or y-rays, radiobiological data indicatethat neutrons delivered at low dose or in a series of fractions spread out over aperiod of time may produce more oncogenic transformation than a single acuteexposure . This has important implications in radiation protection .
1. IntroductionI feel very honoured to receive the Weiss Medal, and grateful to those who
thought me worthy of it . There is a certain feeling of deja-vu for me to return toOxford for this occasion ; my first job was here at the Churchill Hospital, and it wasat Oxford as a graduate student that I was first introduced to radiation physics andradiation biology.
The biological effects of ionizing radiation correlate closely with the energyabsorbed per unit mass (i .e. the dose) . For a given dose, biological effects depend,too, on the pattern of energy deposition at the microscopic level, i .e . the quality ofthe radiation expressed in terms of the linear energy transfer (LET), and on the rateof energy deposition, i .e . the dose-rate . These latter two factors are not independentvariables, since the dose-rate effect varies qualitatively and quantitatively with
tGiven on the occasion of the presentation of the Weiss Medal to the author, for hiscontributions to the advancement of knowledge in the field of radiobiology, at the Associ-ation for Radiation Research meeting at the Clarendon Laboratory, Oxford University, UK쓀 April 1990 .
0020-7616/91 $3 .00 © 1991 Taylor & Francis Ltd
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

쓀96
E. J . Hall
LET. I propose to illustrate the practical importance of the dose-rate effect withtwo examples from radiation therapy and one from radiation protection .
2 . The dose-rate effect in radiotherapyIn this case the dose-rate effect involves a low-LET radiation, namely y-rays,
with the biological endpoint being cell killing . The mechanisms are well understoodas a result of almost 30 years of laboratory investigation and were summarized byHall (1972) . The principal change in our understanding of the dose-rate effect sincethis review was published results from the fact that cells of human origin have beenutilized increasingly (Hall et al . 1988, Steel et al . 1987) for which the dose-rateeffect is, in general, smaller in magnitude than for cells of rodent origin . We haverecently summarized the experimental data for 38 cell lines of human origin, of bothnormal tissues and tumours, exposed to a range of dose-rates . Since all of the cellswere treated in exponential growth they correspond in vivo to early-, as opposed tolate-responding tissues . These data were analyzed using the linear-quadraticmodel, with a factor to allow for dose-rate (Brenner and Hall 1990a) . Theexpression used to fit the data was
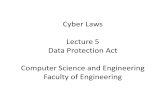
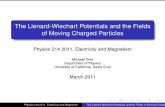
where S is the fraction of cells surviving a dose D, while a and fl are constants . G is afactor to allow for dose-rate or fractionation first proposed by Lea and Catcheside(19쓀2), which includes such factors as the half-life of sublethal damage repair, thedose-rate in the case of continuous low dose-rate, or the fractionation pattern . Theanalysis of the data is described in more detail in the paper by Brenner and Hall(1990a). The data show a large range of values for of f, the parameters of the acutedose-response relationship and for T,/2, the half-time of repair of sublethaldamage. The frequency distributions of these quantities are shown in Figures 1 and2. There are also some limited data in the literature for repair times for late-responding normal tissues in vivo, for the mouse and the human (Table 1) .
These in vitro data for cells of human origin, as well as the limited in vivo datafor late effects, have been used to address two areas of brachytherapy .
2.1 . Pulsed interstitial brachytherapyInterstitial brachytherapy is considered to be the treatment of choice for the
쓀-10% of patients in whom the tumour is accessible . A major revolution of the past
1쓀7
10
Frequency
쓀
S=e-'D -PGD (1)
0 -r- --0.1
10
100
a/(3/Gy
Figure 1 . Distribution of 38 values of a/(3, taken from the analysis of in vitro low dose-ratestudies on 38 cell lines of human origin, some from our own laboratory and some fromthe literature (redrawn from Brenner and Hall 1990a) .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

Dose-rate factor in radiation biology
0cmcdU-
10
e-
01
10
100
1000
Half Time for Repair l Min
쓀 97
Figure 2 . Distribution of 38 values of the half-time for sublethal damage repair, taken fromthe analysis of in vitro low dose-rate studies on 38 cell lines of human origin (redrawnfrom Brenner and Hall 1990a) .
decade has been the introduction of computer-controlled remote afterloadingdevices, which allow more complex source distributions and, as with all goodafterloading devices, essentially eliminate the radiation exposure of nursing andtechnical staff. An interstitial implant involves the use of a large number ofradioactive sources which are loaded into catheters previously implanted into thetumour. The essence of an afterloading system is that the catheters can beimplanted `cold' in the operating theatre, while the radioactive sources can beinserted later, after the patient has returned to his/her room, by means of a remote-controlled afterloading device .
A typical prescribed dose-rate would be about 0 . 쓀 Gy/h for a total exposure timeof about 60 h . This would correspond to a boost treatment to be added to externalbeam therapy. Commercially available afterloading devices are complex andexpensive because they must house multiple channels and an inventory of manyradioactive sources, to allow the use of small or large, single or multi-planeimplants . Iridium-192 is the radionuclide of choice, and sources must be replacedseveral times each year to allow for radioactive decay .
Table 1 . Values of a, fl, a/fl, T112 for late-responding tissues evaluated in vivo .
j' The slow and fast components of the repair were roughly equally important .
Endpoint Referencesa
fi(Gy-1 ) (Gy-2 )
a/fl(Gy)
T112(min)
Human skin (telangiectasia)Fast repairt Turesson and 0. 10
0.02쓀 쓀 . 1 2쓀Slow repair j' Thomas 1989 0 . 10
0.02쓀 쓀.1 210
Mouse lung Travis et al . 1987 0 . 31
0.072 쓀.1 39Late damage
Rat spinal cord Ang et al . 1987 0. 066
0.019 3 . 쓀 93Paralysis
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

쓀98 E. J. Hall
A possible strategy to simplify such machines would be the use of pulsed, ratherthan continuous, low dose-rate irradiation . An afterloading device based on thisprinciple could consist of a single high-activity radioactive source, that would stepthrough the catheters making up an implant, with a computer-controlled dwell timein each position to reflect the required differential loading of activity . This singlesource would replace the complex inventory of sources required in currentafterloaders for interstitial brachytherapy . A device of this sort would have threeadvantages :
1 . Better dose optimization because of the opportunity to infinitely vary computer-controlled dwell times .
2. A greatly simplified afterloading device, with a single channel, rather thanmultiple channels, which may therefore be less costly to build .
3 . A single radioactive source to be replaced at regular intervals in place of a wholeinventory of sources, leading to a considerable cost saving . Source replacementcould also be less frequent .
Continuous low dose-rate could obviously be simulated perfectly by an infinitenumber of infinitely small pulses. However, for a pulsed brachytherapy device to bepractical there is a limit to the number of pulses per unit time that can be used,otherwise the stress on the weld between the radioactive source and the flexiblecable used to drive it in and out of the implant becomes a problem . This weld isconsidered the limiting feature of remote afterloaders, and could be subject topotentially catastrophic breakage after 100000-200000 uses . In order to design aclinical unit with acceptable safety standards, it is essential that the replacement ofthe radioactive iridium source due to radioactive decay should occur long beforethere is a possiblity of such a mechanical failure . These considerations necessitatepulse repetition times to be as long as possible .
Brenner and Hall (1990a) used equation (1), with the radiobiological data forhuman cells summarized in Figures 1 and 2, to determine the combination ofradiation pulse widths (i .e . the length of pulse) and pulse frequency (i .e . the numberof pulses per hour) that would be equivalent to continuous irradiation . They usedeach of the 38 parameter sets (a, /3, T112 ) and calculated, for given values of the totaldose and irradiation time, what combinations of the pulse width and frequencywould be predicted to yield survivals equivalent to a continuous protocol . Onerepresentative result is shown in Figure 3 for a particular human cell line . Therepresentation in this figure is such that any combination of pulse width and periodthat is within the enclosed shaded region will yield a survival equivalent to thatpredicted for the continuous protocol .
The regions of interest are the upper boundaries of the shapes in Figure 3-because the longer the period between treatments the more practical the protocolbecomes. The maximum time between pulses is independent of the pulse width aslong as the pulse width is significantly shorter than the time constant of sublethaldamage repair . As the pulse width becomes longer, a longer period between pulsesbecomes acceptable .
The results for all 38 cell lines are summarized in Figure 쓀 . For a 10-min pulsethis figure shows the maximum time between pulses that would result in anacceptable equivalence to continuous low dose-rate . If it can be assumed that thesurvival curve characteristics, and more importantly the repair time characteristics,of the 38 cell lines of human origin are representative of those found in the target
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

1000
Time
100
Between
1Pulses / min
0 .1
Dose-rate factor in radiation biology
쓀99
a = 0.쓀30 G3 = 0.0783 T± = 0.쓀2 hrTotal Dose = 30 Gy equiv Radiation Time=60 hrSurvival Within a Factor of 7 .쓀 of 3 .1e - 08
10000
0.010 .01 0.1
1
10 100 1000 10000Pulse width/min
Figure 3 . Combination of pulse widths and periods between pulses that will yield anequivalent survival to a continuous low dose rate irradiation of 30 Gy in 60h .(Continuous and pulsed irradiation schemes are considered to be equivalent if theratio of survivals is less than a factor f at a survival of 10 -f.) Any combination of pulsewidth and period within the marked boundary is predicted to yield equivalent cellkilling. The figure shows representative data for one of the 38 cell lines analyzed(redrawn from Brenner and Hall 1990a) .
volume of human tumours in vivo, then a pulse width of several minutes, and a pulseinterval of about 1 h, would result in a close equivalence of cell killing by the pulsedirradiation scheme and a continuous low dose-rate scheme of 30 Gy in 60h(쓀0 cGy/h). This system would be very flexible since, as the iridium-192 sourcedecays, the pulse width could be adjusted to compensate, keeping the average dose-rate constant .
Although the results shown here are derived for the typical `boost' protocol of30 Gy in 60 h, similar results were obtained for other feasible total dose/total timecombinations, including 쓀0 Gy in 120 h or 36 Gy in 60 h .
In conclusion, for an average dose-rate of about 0 .6 Gy/h, a pulse width ofaround 10 min with a pulse period of about 1 h appears to be functionally equivalent
10
8-
6
Frequency쓀
2-
010
100
1000
Max Time Between Pulses/min
Figure 쓀 . Distribution of maximum times between 10-min pulses that would yieldequivalent survival to a continuous low dose-rate treatment of 30 Gy delivered in 60 h(redrawn from Brenner and Hall 1990a) .
10 min pulses
Melanomaa/R=6.8Gy
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

600
E. J. Hall
to a continuous irradiation protocol . This result might be inferred intuitively,without the analysis of any experimental data at all, on the following grounds . Thepulsed and continuous protocols involve the same overall dose in the same overalltime. In addition, the dose per hour is the same in both cases (60 cGy), but in thepulsed case it is delivered in 10 min of each hour, while in the continuous case it isspread out over the entire hour. A dose fraction as small as 60 cGy is on the initialpart of the survival curve where single-event (a) killing predominates, and there isunlikely to be detectable difference in the fraction of cells killed if the dose isdelivered in 60 min or 10 min .
It is hoped that these conclusions, based on the analysis of a large body ofexperimental data, will allow the development of a new generation of pulsed lowdose-rate afterloading devices that will combine better dose optimization withincreased simplicity. The development of such machines should allow the advan-tages of computer-controlled afterloaders for low dose-rate brachytherapy to bemore readily available to smaller clinics and hospitals in both developed anddeveloping countries .
2.2 . High dose-rate V . low dose-rate in the treatment of carcinoma of the cervixIntracavitary brachytherapy at low dose-rate (LDR), often with the addition of
external beam radiotherapy, has been the treatment of choice for carcinoma of thecervix for over half a century. Initially, radium tubes were used, replaced in morerecent years by caesium-137 or iridium-192 sources . A typical LDR regimen forcervical cancer involves two insertions, 1-3 three weeks apart, to a total dose topoint-A of 쓀쓀-70 Gy (plus an external whole-pelvic irradiation), or to a total of7쓀-80 Gy with no external treatment (Moss and Cox 1989, Perez and Brady 1987,Stout and Hunter 1989) . The LDR treatment is usually delivered at 0 . 쓀-0 . 6 Gy/h .Such lengthy irradiations, totalling 쓀-6 days, are based largely on historicalprecedent but, in retrospect, may be justified by the rationale that LDR schedulesdifferentially spare late-responding tissues compared with early-respondingtumour cells (see, for example, Withers et al . 1982) .
High dose-rate (HDR) treatment for cervical carcinoma was introduced about2쓀 years ago, motivated by the practical advantages to the patient, who mayundergo therapy on an outpatient basis . A number of different HDR fractionnumbers, from 2 to 1쓀, are currently in use . From the treatment standpoint, HDRunits such as the Cathetron (O'Connell et al . 196쓀) or the Selectron HDR (van'tHooft, 198쓀) provide accurate and flexible dosimetry, as well as increased patientthroughput . The practical advantages of HDR have recently been summarized byJoslin (1989) .
The radiobiological data for cells of human origin, summarized earlier in thispaper, may be used to estimate the equivalence of HDR fractionated schemes toLDR protocols. Equation (1) can be used to calculate the total dose, D FA in thefractionated scheme that would give equivalent early effects to the LDR treatment .Figure 쓀(a, b) shows, for various HDR fractionation schemes, the distribution ofpoint-A HDR doses predicted (based on the 38 parameter sets of Figures 1 and 2) toyield comparable acute effects to two fractions totalling 60 Gy, delivered at0 . 쓀 Gy/h . This latter is a typical LDR brachytherapy regime used in conjunctionwith external whole-pelvic irradiation . Figure 6 shows the corresponding means ofthese histograms, as a function of fraction number, and also presents a comparison
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

12
10av 8c
6
N 쓀LLL
Dose-rate factor in radiation biology
2
0
12
10
v 8
6Q 쓀NLL 2
0
(b)
Figure 쓀 . Distribution of point-A HDR doses predicted (based on the 38 parameter sets) toyield comparable acute effects to two fractions totalling 60 Gy, delivered at 0 . 쓀 Gy/h,3 weeks apart : (a) 1, 2, and 3 HDR fractions ; (b) 쓀, 8, and 12 HDR fractions .
with the regimens reported in the literature as having been used for such HDRclinical trials .
While it is a simple matter in an analysis such as this to include HDRfractionation schemes down to two or even one fraction, there may be compellingreasons, unrelated to dose-rate considerations, to exclude so few fractions . Anobvious factor is the need to allow adequate reoxygenation of possible hypoxictumour cells . Prudence may dicatate a lower limit to the number of HDR fractionsof about five .
An overrriding consideration in any discussion of changing dose-rate orfractionation schemes in radiotherapy is the impact of the change on the possibility
0
101
101
Dose per fraction / Gy
2
쓀
6
a
10
12
1쓀
Number of Fractions
10
601
Figure 6 . Arithemetic means of the distributions shown in Figure 쓀 . The bars correspondto the standard deviations of the samples. The points represent HDR intracavitarybrachytherapy regimens reported in the literature to have been used in clinical trials .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

602
E. J. Hall
of late effects. Laboratory data and clinical experience over the past decade haveshown that late-responding tissues are more sensitive to changes of fractionationthan early-responding tissues (including tumours), which is consistent with thenotion that the dose-response relationship is more `curvy' for late- than for early-responding tissues, corresponding to a smaller value of a//J (Withers et al . 1982,Withers 198쓀) . It would be predicted on radiobiological grounds, and it is certainlyobserved in clinical practice, that if doses are matched for early effects, a protocolconsisting of a few large fractions will result in worse late effects than a protocolconsisting of many small fractions, or continuous low dose-rate . Strictly speaking,this is true only if the late-responding tissues receive the same total dose as theearly-responding tissues for which the different fractionation patterns werematched. If, in fact, the normal tissues at risk for late effects receive a dose lowerthan that at which early effects are matched, then it does not follow inevitably thatlate effects will be worse for the protocol involving the few small fractions . It can beshown mathematically (Brenner and Hall 1990b), that if the total doses in twoprotocols involving different fractionation patterns are matched for early effects,then late effects will be equal at a fraction of that dose which approximates to :
a//3 (late)
a//J (early)
For typical values of the published parameters of the dose-response curves forearly- and late-responding tissues, this may be 3 to 1 .
The principle derived above is based on sound defensible radiobiologicalprinciples. Whether it has any relevance to the treatment of carcinoma of the cervixby intracavitary brachytherapy is a more debatable point . Most papers in theliterature identify the normal tissues most at risk for developing late effects assequelae to treatment of carcinoma of the cervix to be the bladder, the rectum andsigmoid. Table 2 shows results of measurements and estimates of doses in theseorgans, which fall in the range 3 to of the point-A prescribed dose . To the extentthat this is correct, or at least representative, these data would lead one to predictthat five HDR intracavitary fractions would not produce noticeably worse lateeffects than LDR intracavitary treatments . On the other hand there are other datain the literature that suggest that critical normal tissues may often receive 7쓀-100%of the point-A dose, and then the HDR treatments may be at a serious disadvan-tage. This may be particularly true when a large tumour leads to distortions of thenormal anatomy .
An important factor that aids in making HDR techniques acceptable is thatapplicators that retract normal tissues away from the intracavitary radioactive
Table 2 . Percentage of point-A dose delivered during cervical intracavitary brachytherapyto normal tissues at risk for late effects .
OrganPercentageof point-A dose Reference
Rectum 쓀쓀±12 Bidmead and Staffurth (198쓀)쓀2 Joslin (1989)
Bladder 쓀2±20 Hunter et al. (1986)Sigmoid 28±7 Bidmead and Staffurth (198쓀)
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

Dose-rate factor in radiation biology 603
sources can be used for the short exposure times (a few minutes) characteristic ofHDR, while they would not be tolerable for the protracted exposures (days)necessary for LDR techniques .
In conclusion, low dose-rate data for cells of human origin, combined withradiobiolgical theory, can provide guidance for the choosing of doses at HDR thatmay produce equivalent early effects to LDR, and suggest situations in which lateeffects may not be worse for HDR treatments .
3 . The inverse dose-rate effect for radiations of intermediate LETIn the practical case of radiation protection, doses to personnel are usually
accumulated over a protracted period of time at low dose-rate, whereas cancer riskestimates, based on the experience of the survivors of Hiroshima and Nagasaki,relate to a single acute exposure . In the case of low-LET radiations, such as X- andy-rays, it is generally agreed that the biological effects of a given total dose arereduced when the dose is delivered over a protracted period of time at low dose-rate. This is the conventional dose-rate effect referred to in previous sections . Thisappears to be the case whether the biological effect of interest is cell killing mutationor cancer induction . The same is not true for more densely ionizing radiations, suchas neutrons, where a greater biological effect may result from a protracted exposurethan from the same total dose delivered in an acute exposure . This has come to beknown as the inverse dose-rate effect and is of special importance in radiationprotection . Some evidence for this inverse dose-rate effect for neutrons or otherhigh-LET radiations comes from life-shortening tumour induction and cataractinduction in laboratory animals (Ullrich 198쓀, Vogel et al ., 1982, Cross 1988, Littleet al . 198쓀, Muller et al . 1988, Worgul et al . 1989) .
There are also some epidemiological studies that are supportive of the animalstudies, though none are conclusive (Hornung and Meinhardt 1987, Lubin et al .1990, Darby and Doll 1990, Chemlevsky et al. 1988) .
However, the most comprehensive set of data for the inverse dose-rate effectrelate to studies with in vitro assays for oncogenic transformation .
Elkind and his colleagues first reported an inverse dose-rate effect for fissionspectrum neutrons in the induction of oncogenic transformation in C 3H1OTI/2cells (Hill et al. 1982) . They found that for a given low dose of neutrons (쓀-30 cGy),the transformation incidence was much higher if the radiation were delivered at lowdose-rate, or in a series of fractions over 쓀 days, than if delivered in a single highdose-rate exposure .
This is a topic of considerable importance since some 60 000 individuals whowork around nuclear reactors in the US, and comparable numbers in othercountries, are exposed to degraded fission spectrum neutrons, and in addition,manned long-term space missions should also involve low dose-rate irradiation ofthe crew with radiations of intermediate LET .
The bulk of the in vitro experimental data available involves oncogenictransformation with the C 3H10TI/2 assay. Limited data are also available forhamster embryo cells (Jones et al . 1989) and also for mutation assays (Kubota andHill 1989) but these data are too sparse for systematic analysis. Since the initialreport by Hill et al . (1982), 10 further publications have appeared reportingexperimental results that address the possible enhancement of transformation bydose protraction (i .e. by low dose-rate or fractionation). These measurements covera variety of radiations of intermediate to high LET including fission neutrons (Hill
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

60쓀
E. J. Hall
et al. 1982, 198쓀, 198쓀, Balcer-Kubiczek et al . 1988), high-energy therapy neutrons(Hill 1989), monoenergetic neutrons (Miller et al . 1988, 1989), as well as chargedparticles (Miller et al . 1989, Hieber et al . 1987, Yang et al . 1987, Bettega et al . 1989) .A variety of doses, dose-rates, and fractionation schemes were utilized . Although atfirst sight the data appear to be confusing and conflicting, in fact a pattern doesemerge. The largest enhancement was observed for fission neutrons at dose-ratesbelow about 0 . 쓀 cGy/min, while little or no enhancement is apparent for allradiations at dose-rates above 0 . 쓀 cGy/min . It is apparent, too, that monoenergeticneutrons produce a significantly smaller enhancement than that produced by fissionneutrons, while charged particles having LET above 120 keV/µm produce little orno enhancement. In addition, the inverse dose-rate effect appears most prominentat doses around 0 .2 Gy, with less evidence of enhancement at doses much above orbelow this region .
Over the years a number of suggestions have been published to account for theenhancement of transformation by dose protraction (Hill et al . 198쓀, Barendsen198쓀, Burch and Chesters 1986, Elkind and Hill 1986, Rossi and Kellerer 1986,Dennis and Dennis 1988, Sykes and Watt 1989) . The simplest and most crediblemodel is based on an idea by Oftedal (1968) and subsequently formalized by Rossiand Kellerer (1986) . This model postulates that, for the biological endpoint ofinterest, cells at some period of their cell cycle are more sensitive to radiation than atother times-i .e . there is a `window' of increased sensitivity . A further postulate isthat an acute high-LET exposure of cycling cells results in some fraction of thesesensitive cells receiving very large depositions of energy-much greater than thatrequired to produce oncogenic transformation . On the other hand, if the exposure isprotracted or fractionated a larger proportion of sensitive cells will be exposed,though to smaller numbers of energy depositions ; however, since high-LETradiations are involved it is postulated that the total specific energy deposited in thesensitive cells by this smaller number of energy depositions will still be largeenough to produce transformation . To the extent that this latter postulate may nothold at low LET, the inverse dose-rate effect would not be expected to apply tosuch radiations .
The development of this model, and the methods used to fit the experimentaldata, have been described in detail by Brenner and Hall (1990c) ; only the generalconclusions will be discussed here . Figure 7 shows the transformation enhancementratio as a function of dose for three types of neutrons ; 6-MeV neutrons (y F=1쓀 .7 keV/µm), fission neutrons (y F =1 keV/µm) and cyclotron produced higher-energy neutrons used for radiotherapy (y F =쓀. 쓀 keV/ltm) . The predictions of themodel are also shown, assuming a window of sensitivity of 1 h .
It is apparent that the predictions are in reasonable accord with the data for thevarious different radiations. In particular, although 6-MeV neutrons and fissionneutrons have comparable values of YD, their markedly differing values of yF resultin a much larger enhancement from fission neutrons at low dose-rates . For all theradiations the predicted enhancements at dose-rates above 0 . 쓀 cGy/min are smallenough to be experimentally undetectable, again in agreement with experiment .Figure 8 shows the experimental data together with the corresponding predictionsfrom the model for higher LET charged particle radiations (1쓀0-200 keV/µm) ; thepredicted enhancements are very small, and are consistent with the lack of asignificant effect seen experimentally .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

WdC
10d7tS^
.~•7
C VO .acc d
E C0•
Ly O•
CLL
0.2
Dose-rate factor in radiation biology
60쓀
0 .03 0.1
1
Dose Rate/cGy/min .
Figure 7 . Published data with 9쓀% confidence limits for enhancement of oncogenictransformation of C 3H10T1/2 cells by low doses (20-30cGy) of `medium'-LETradiation (y p=60-70 keV/µm) in a 1 ym site . (0) 6-MeV neutrons (Miller et al . 1989) ;(A) fission neutrons (Hill et al . 1982, 198쓀); (D) fission neutrons (Balcer-Kubicek etal . 1988) (O), p(30)-Be and V p(쓀6) Be neutrons (쓀0 cGy), Hill (1989) (redrawn fromthe data of Brenner and Hall 1990c) . Predictions of model . Full curve ; y F =1 keV/µm ;30 cGy of fission neutrons, refers to (A, V) . Long dash : y F =1쓀 .7 keV/µm; 30 cGy of6-MeV neutrons, refers to (0) . Short dash : yF =쓀.쓀 keV/pm; 쓀0cGy of p-Beneutrons, refers to Fl .
0 .03
0.1
1
10Dose Rate/cGy/min .
Figure 8 . Published data with 9쓀% confidence limits for enhancement of oncogenictransformation of C 3H1OT1/2 cells by low doses (쓀0-100cGy) of high-LET chargedparticles . (A) 1쓀0 keV/µm (Hieber et al. 1987); (0) 1쓀0keV/µm (Yang et al . 1987) ;(0) 200 keV/pm (Yang et al. 1987) . Predictions of model . The predicted enhance-ments for 1쓀0, 1쓀0 and 200 keV/µm are virtually identical, and cannot be resolvedexperimentally from no enhancement (redrawn from the data of Brenner and Hall1990c) .
10
aac
10 -aCU2
o mIDE g
0
atPrediction1쓀0keV/µm
for 100 cGy
a O 1d
F
OCaO
--------------- v
0.2 t i n i i
i
i
i
i
i
i i i I i i i -
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

606
E. J. Hall
The model outlined here, and described in detail by Brenner and Hall (1990c)appears to be consistent with all the data currently available in the C 3H10TI/2system for the enhancement of transformation by dose protraction of intermediate-and high-LET radiations . Whether or not enhancement of transformation is seen asa consequence of dose protraction is a complex function resulting from the interplayof several factors, including dose, dose-rate and the LET of the radiation . Oneunequivocal prediction is that no enhancement would be expected for high-LETradiations such as HZE particles encountered in interplanetary spacecraft, or fora-particles produced by radon-daughter decay . However, it could well be thattrapped protons, to which astronauts on a space station would be exposed, wouldexhibit an enhancement, since the yF for these particles has a value of about IkeV/µm (Kliauga et al. 1978). For intermediate-LET radiations such as fissionneutrons the effect would be confined to intermediate doses, as the model predictsthat the acute and continuous transformation rates will have the same initial slope atlimiting low doses .
To assess the possible implications of the inverse dose-rate effect to the field ofradiation protection in general, the model has been extrapolated to the wide rangeof very low dose-rates encountered in radiation protection involving fissionspectrum neutrons, or other radiations of intermediate LET . The results are shownin Figure 9, which should not be taken too seriously since it does involve manyassumptions and large extrapolations . It is evident from Figure 9 that for doses lessthan 0 . 1 cGy (corresponding to non-occupational annual effective dose limits), theenhancement would be insignificant at any dose-rate . The annual occupationaleffective dose-equivalent limit is 쓀 cSv, corresponding (assuming a quality factor of10) to 0 . 쓀 cGy of fission neutrons ; if this dose were delivered continuously over ayear at a dose-rate of 10 -쓀 cGy/min, then an enhancement of about 2 might beexpected . Larger enhancements could theoretically be possible for astronautsreceiving bigger doses of protons at very low dose-rates . For example, NCRPreport 98 recommends that the effective dose equivalent for space missions in theshuttle be 0 . 쓀 Sv/year or 1-1 .쓀 Sv in a lifetime ; if the model can be believed, theenhancement ratio may then be as high as 쓀0 .
쓀 . ConclusionThe above examples of the dose-rate effect cover the areas of radiobiology
applied to radiation therapy and to the field of radiation protection . With cell killingas an endpoint, which is relevant to radiation therapy, the dose-rate effect is wellunderstood. For low-LET radiations, such as X- and y-rays, reducing the dose-rateand extending the time over which a given dose is delivered, results almost alwaysin a sparing effect and a reduction in cell killing due to repair of sublethal damage .Data for cells of human origin show a smaller-dose-rate effect than that previouslyreported for cells of rodent origin, but the effect is nevertheless substantial .Radiobiological data can be useful in predicting the equivalence of HDR and LDRtreatments for carcinoma of the cervix as illustrated, and also for obtaining theotpimum parameters for new pulsed brachytherapy devices .
In the field of radiation protection the biological endpoint of interest is surelynot cell killing but rather carcinogenesis, which has an in vitro counterpart inoncogenic transformation . In this case the dose-rate effect can be a complicatedfunction of several variables including dose, dose-rate and the LET of the radiation
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

Dose-rate factor in radiation biology
607
Nm
쓀0VCd7
m
fl ho0o
1
S
0.01
0.1
1
10M
Dose / cGy
Figure 9 . Predicted effect of dose fractionation of fission neutrons as a function of dose for awide range of dose-rates relevant to radiation protection .
involved. For radiations of intermediate LET, including fission spectrum neutronsand protons of certain energies, a protracted low dose-rate exposure can result inmore oncogenic transformations than the same dose delivered in an acute exposure .A model has been developed which accounts for the experimental observations ofan inverse dose-rate effect, which does not, of course, prove that the model iscorrect. However, if the model is extrapolated to very low dose-rates there aresituations where the inverse dose-rate effect may have important implications inradiation protection. One would be long-term space missions in the shuttle ataltitudes of about 100 nautical miles, if the dose limit were raised to 30 cSv . Anotherwould be workers in the nuclear industry exposed long-term to substantial doses ofdegraded fission-spectrum neutrons .
In the broader arena of risk estimates for radiation-induced cancer in thehuman, both the BEIR V and UNSCEAR committees based their estimates on thedata from the Japanese survivors-so that risk estimates are quoted for acuteexposures of Low-LET radiation. In the practical situation of radiation protection,radiation doses are accumulated over an extended period of time at low dose-rate,and some allowance must be made for the reduced biological effect that is usuallythe consequence of a low dose-rate, as opposed to high dose-rate exposure . TheBEIR III committee derived a Dose-Rate Effectiveness Factor (DREF) of 2 .2쓀from the a/fl value for leukaemia, but BEIR V preferred a linear fit for all solidtumours, which has no dose-rate effect implied . Both BEIR V and UNSCEAR 88played it safe and quoted a range of values for the DREF of 2 to 10, based on animaldata referring back to NCRP 1980. This assumes that a given dose delivered at lowdose-rate is less effective, which may be true for low-LET radiations but is notnecessarily true for all types of radiation . The transformation data in vitro, as well assome animal data, highlight the possibility that there may be an inverse dose-rateeffect for radiations of higher LET such as neutrons-so that low dose-rate is moreeffective .
AcknowledgementsThis paper would not have been possible without help from my colleagues at
Columbia. Much of the experimental data used were obtained by Drs RichardMiller and Michael Marchese . The analyses of the data, and particularly the
100
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

608
E. J. Hall
mathematical models and concepts, were developed in collaboration with Dr DavidBrenner, to whom I offer special thanks . Based on research supported by grantnumber DE-FG02-88ER60631 from the Department of Energy and GrantsCA2쓀232 and CA12쓀36 from the National Cancer Institute .
ReferencesANG, K . K., THAMES, H . D., VAN DER KOGEL, A . J . and VAN DER SCHUEREN, E ., 1987, Is the rate
of repair of radiation-induced sublethal damage in rat spinal cord dependent on the sizeof dose per fraction? International Journal of Radiation Oncology, Biology, Physics, 13,쓀쓀7-쓀62 .
BALCER-KUBICZEK, E . K., HARRISON, G. H., ZEMAN, G . H., MATTSON, P . J . and KUNSKA, A.,1988, Lack of inverse dose-rate effect on fission neutron induced transformation ofC 3H/lOT1/2 cells . International Journal of Radiation Biology, 쓀쓀, 쓀31-쓀36 .
BARENDSEN, G . W., 198쓀, Do fast neutrons at low dose rate enhance cell transformation invitro? A basic problem of microdosimetry and interpretation . International Journal ofRadiation Biology, 쓀7, 731-73쓀 .
BETTEGA, D ., CALZOLARI, P., OTTOLENGHI, A . and TALLONE LOMBARDI, L ., 1989, Transfor-mation of C3H1OT1/2 with "Cm alpha particle at low and high dose rates . CellTransformation and Radiation-induced cancer, edited by K . H. Chadwick, C. Seymourand B. Barnhart (Adam Hilger, Bristol), pp . 333-3쓀0 .
BIDMEAD, M . and STAFFURTH, J . F ., 198쓀, Calculation and measurement of dose to the rectumand sigmoid . Brachytherapy, 198쓀, edited by R . F. Mould (Nucleotron, The Nether-lands), pp . 7쓀-79 .
BRENNER, D. J. and HALL, E . J., 1990a, Conditions for the Equivalence of continuous topulsed low dose-rate brachytherapy . International Journal of Radiation Oncology,Biology, Physics (In press) .
BRENNER, D. J. and HALL, E . J ., 1990b, Intracavitary brachytherapy for cervical carcinoma ;fractionated high dose-rate versus low dose-rate regimens . British Journal of Radiology(In press) .
BRENNER, D . J . and HALL, E . J ., 1990c, The inverse dose-rate effect for oncogenictransformation by neutrons and charged particles : a plausible interpretation consistentwith published data . International Journal of Radiation Biology (In press) .
BURCH, P . R . J. and CHESTERS, M. S ., 1986, Neoplastic transformation of cells in vitro at lowand high dose rates of fission neutrons : an interpretation . International Journal ofRadiation Biology, 쓀9, 쓀9쓀-쓀00 .
CHMELEVSKY, D., KELLERER, A. M., LAND, C. E., MAYS, C. W. and SPIESS, H ., 1988, Timeand dose dependency of bone sarcomas in patients injected with radium-22쓀 . Radiationand Environmental Biophysics, 23, 103-11쓀 .
CROSS, F . T., 1988, Evidence of lung cancer from animal studies in radon and its decayproducts in indoor air . Radon and its Decay Products in Indoor Air, edited by W. W .Nazaroff and A. V. Nero (John Wiley and Sons, New York), pp . 373-쓀0쓀 .
DARBY, S. C. and DOLL, R ., 1990, Radiation and exposure rate (Letter), Nature, 3쓀쓀, 82쓀 .DENNIS, J. A. and DENNIS, L. A., 1988, Neutron dose effect relationships at low doses .
Radiation and Environmental Biophysics, 27, 91-101 .ELKIND, M. M. and HILL, C . K ., 1986 . Age-dependent variations in cellular susceptibility to
neoplastic transformation reply to Letter to the Editor, by H . H. Rossi and A. M .Kellerer (1986) . International Journal of Radiation Biology, 쓀0, 1117-1122 .
HALL, E. J., 1972, Radiation dose-rate : a factor of importance in radiobiology andradiotherapy. British Journal of Radiobiology, 쓀쓀, 81-97 .
HALL, E. J., MARCHESE, M ., HEI, T. K. and ZAIDER, M ., 1988, Radiation responsecharacteristics of human cells in vitro . Radiation Research, 11쓀, 쓀1쓀-쓀2쓀 .
HIEBER, L ., PONSEL, G., Roos, H ., FENN, S ., FROMKE, E. and KELLERER, A. M., 1987,Absence of a dose-rate effect in the transformation of C3HIOT1/2 cells by a-particles .International Journal of Radiation Biology, 쓀2, 8쓀9-869 .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

Dose-rate factor in radiation biology
609
HILL, C. K., 1989, Is the induction of neoplastic transformation by radiation dependent uponthe quality and dose rate? Scientific Papers of the Institute of Physical and ChemicalResearch, 83, 31-3쓀 .
HILL, C . K., BUONOGURO, F. J ., MYERS, C . P., HAN, A. and ELKIND, M . M., 1982, Fission-spectrum neutrons at reduced dose rate enhance neoplastic transformation . Nature,298,67-68 .
HILL, C. K., HAN, A. and ELKIND, M . M., 198쓀, Fission-spectrum neutrons at low dose rateenhance neoplastic transformation in the linear, low-dose region (0-10 cGy) . Inter-national Journal of Radiation Biology, 쓀6, 11-1쓀 .
HILL, C . K., CARNES, B . A., HAN, A . and ELKIND, M . M., 198쓀, Neoplastic transformation isenhanced by multiple low doses of fission-spectrum neutrons . Radiation Research, 102,쓀0쓀-쓀10.
HORNUNG, R. W. and MEINHARDT, T. J ., 1987, Quantitative risk assessment of lung cancer inUS uranium miners . Health Physics, 쓀2, 쓀17-쓀30 .
HUNTER, R . D., WONG, F., MOORE, C ., NOTLEY, H . M. and WILKINSON, J ., 1986, Bladderdosage in patients undergoing intracavitary therapy . Radiotherapy and Oncology, 7,189-197 .
JONES, C . A ., SEDITA, B . A ., HILL, C . K . and ELKIND, M. M., 1989, Influence of dose rate onthe transformation of Syrian hamster embryo cells by fission-spectrum neutrons . LowDose Radiation : Biological Bases of Risk Assessment, edited by K . F. Baverstock andJ. W. Stather, (Taylor & Francis, London), pp . 쓀39-쓀쓀6 .
JOSLIN, C . A . F ., 1989, High-activity source afterloading in gynecological cancer and its futureprospects . Endocurietherapy/Hyperthermia Oncology, 쓀, 69-81 .
KLIAUGA, P. J ., COLVETT, R . D., LAM, Y. P. and Rossi, H . H ., 1978, The relative biologicaleffectiveness of 160 MeV protons . I. Microdosimetry. International Journal ofRadiation Oncology, Biology, Physics, 쓀, 1001-1008 .
KUBOTA, N. and HILL, C . K ., 1989, Dose rate effect of fission-spectrum neutrons on mutationinduction in Chinese hamster cells and human diploid fibroblasts . Scientific Papers ofthe Institute of Physical and Chemical Research, 83, 2쓀-30 .
LEA, D. E. and CATCHESIDE, D . G., 19쓀2, The mechanism of the induction by radiation ofchromosome aberrations in Tradescantia. Journal of Genetics, 쓀쓀, 216-2쓀쓀 .
LITTLE, J. B., KENNEDY, A . R. and MCGANDY, R . B ., 198쓀, Effect of dose rate on the inductionof experimental lung cancer in hamsters by y-radiation . Radiation Research, 103,293-299 .
LUBIN, J. H., QIAO, Y. L., TAYLOR, P . R., YAO, S . X., SCHATZKIN, A., MAO, B . L., RAO,J . Y., XUAN, X. Z . and Li, J . Y ., 1990, A quantitative evaluation of the radon and lungcancer association in a case control study of Chinese tin miners . Cancer Research, 쓀0,17쓀-180 .
MILLER, R . C., BRENNER, D . J ., GEARD, C . R., KOMATSU, K ., MARINO, S. A. and HALL, E . J .,1988, Oncogenic transformation by fractionated doses of neutrons . RadiationResearch, 11쓀, 쓀89-쓀98 .
MILLER, R. C., BRENNER, D . J., RANDERS-PEHRSON, G., MARINO, S. A. and HALL, E . J .,1990, The effects of the temporal distribution of dose on oncogenic transform-ation by neutrons and charged particles of intermediate LET . Radiation Research,12쓀,쓀62-쓀68 .
Moss, W. T. and Cox, J. D., 1989, Radiation Oncology, Rationale, Technique, Results (C . V .Mosby, St Louis, MO) .
MULLER, W. A., LINZNER, U . and Luz, A., 1988, Early induction of leukemia (malignantlymphoma) in mice by protracted low y-doses . Health Physics, 쓀쓀, 쓀61-쓀63 .
NCRP Report 98, 1989, Guidance on Radiation Received in Space Activities . National Councilon Radiation Protection and Measurements, Bethesda, MD .
O'CONNELL, D ., HOWARD, N ., JOSLIN, C. A . F ., RAMSEY, N . W. and LIVERSAGE, W. E ., 196쓀,A new remotely controlled unit for the treatment of uterine carcinoma . Lancet, ii,쓀70-쓀71 .
OFTEDAL, P ., 1968, A theoretical study of mutant yield and cell killing after treatment ofheterogeneous cell populations . Hereditas, 60, 177-210 .
PEREz, C. A. and BRADY, L. W., 1987, Principles and Practice of Radiation Oncology(J. B . Lippincott, Philadelphia, PA) .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.

610
Dose-rate factor in radiation biology
Rossi, H. H . and KELLERER, A. M., 1986, The dose rate dependence of oncogenictransformation by neutrons may be due to variation of response during the cell cycle .International Journal of Radiation Biology, 쓀0, 3쓀3-361 .
STEEL, G . G ., DEACON, J . M., DUCHESNE, G. M ., HARWICH, A., KELLARD, L. R . and PEACOCK,J. H ., 1987, The dose-rate effect in human tumor cells . Radiotherapy and Oncology, 9,299-310 .
STOUT, R. and HUNTER, R. D., 1989, Clinical trials of changing dose-rate in intracavitary lowdose-rate therapy. Brachytherapy, Vol . 2, edited by R . F. Mould (Nucleotron, TheNetherlands) .
SYKES, C. E . and WATT, D. E., 1989, Interpretation on the increase in efficiency of neoplastictransformation observed for some ionizing radiations at low dose rate . InternationalJournal of Radiation Biology, 쓀쓀, 92쓀-9쓀2 .
TRAVIS, E . L., THAMES, H. D ., WATKINS, T . L. and Kiss, I ., 1987, The kinetics of repair inmouse lung after fractionated irradiation . International Journal of Radiation Biology,쓀2,903-919 .
TURESSON, I . and THAMES, H . D ., 1989, Repair capacity and kinetics of human skin duringfractionated radiotherapy: erythema, desquamation, and telangiectasia after 3 and쓀 year's follow-up . Radiotherapy and Oncology, 1쓀, 169-188 .
ULLRICH, R. L., 198쓀, Tumor induction in BALB/c mice after fractionated or protractedexposures to fission-spectrum neutrons . Radiation Research, 97, 쓀87-쓀97 .
VAN'T HOOFT, E., 198쓀, The Selectron HDR : philosophy and design . Brachytherapy, 198쓀,edited by R . F. Mould (Nucleotron, The Netherlands) .
VOGEL, H. H. and DICKSON, H. W., 1982, Mammary neoplasia in Sprague-Dawley ratsfollowing acute and protracted irradiation . Proceedings of the European Seminar onNeutron Cardiogenesis, edited by J . J . Broerse and G . W. Gerber (CEC, Luxembourg),pp . 8쓀-90 .
WITHERS, H. R., 198쓀, Biologic basis for altered fractionation schemes . Cancer, 쓀쓀, 2086 .WITHERS, H. R., THAMES, H . D. and PETERS, L. J ., 1982, Differences in the fractionation
response of acutely and late-responding tissues . Progress in Radio-Oncology, Vol . II,edited by K . H . Karcher, H . D. Kogelnik and G. Reinartz (Raven Press, New York),pp. 287-296 .
WORGUL, B. V ., MERRIAM, JR, G. R ., MEDVEDOVSKY, C. and BRENNER, D. J ., 1989, Acceleratedheavy particles and the lens . III. Cataract enhancement by dose fractionation .Radiation Research, 118, 93-100 .
YANG, T . C ., CRAISE, L. M ., MEI, M. T. and TOBIAS, C. A., 1987, Dose protraction studieswith low- and high-LET radiations on neoplastic cell transformation in vitro . Advancesin Space Research, 6, 137-1쓀7 .
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mel
bour
ne o
n 11
/06/
14Fo
r pe
rson
al u
se o
nly.