Welche Targets, welche Substanzen bleiben nach … · Welche Targets, welche Substanzen bleiben...
22
Welche Targets, welche Substanzen bleiben nach GATSBY, RAINFALL & Co. für die Therapie fortgeschrittener, gastroösophagealer Tumoren? Prof. Salah-Eddin Al-Batran Krankenhaus Nordwest UCT- University Cancer Center Frankfurt
Transcript of Welche Targets, welche Substanzen bleiben nach … · Welche Targets, welche Substanzen bleiben...
Welche Targets, welche Substanzen bleiben nach
GATSBY, RAINFALL & Co. für die Therapie
fortgeschrittener, gastroösophagealer Tumoren?
Prof. Salah-Eddin Al-Batran
Krankenhaus Nordwest
UCT- University Cancer Center Frankfurt
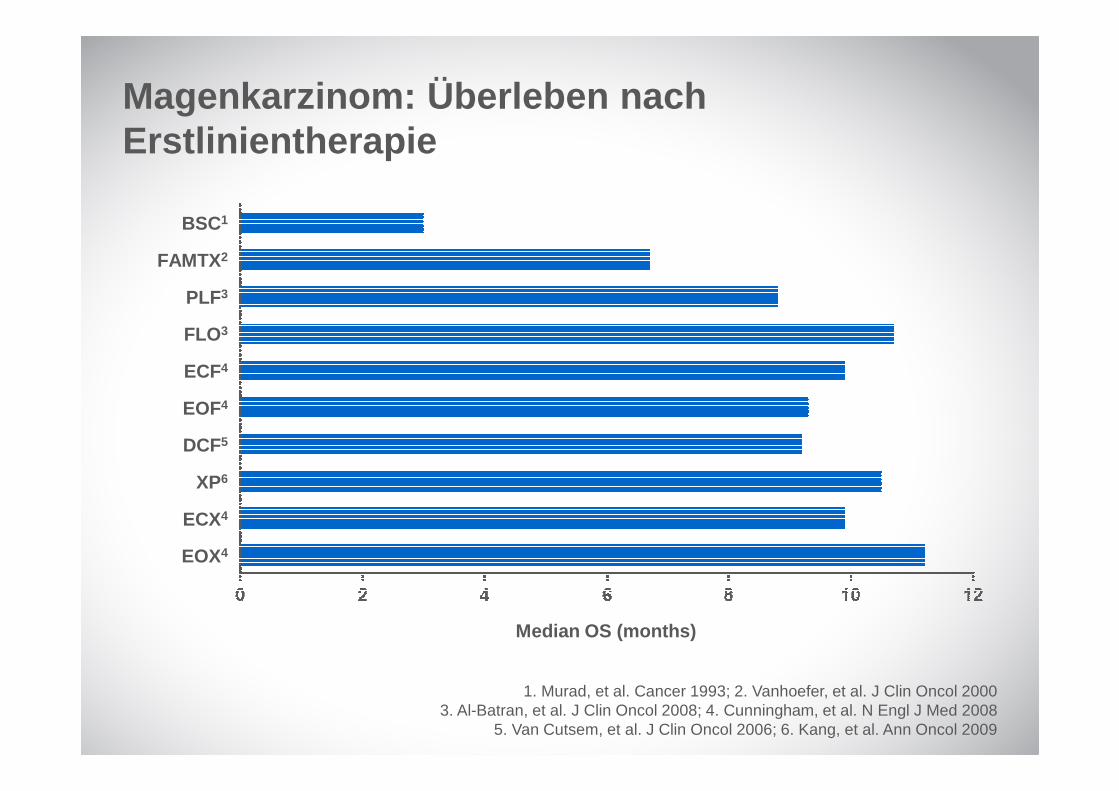
1. Murad, et al. Cancer 1993; 2. Vanhoefer, et al. J Clin Oncol 20003. Al-Batran, et al. J Clin Oncol 2008; 4. Cunningham, et al. N Engl J Med 2008
5. Van Cutsem, et al. J Clin Oncol 2006; 6. Kang, et al. Ann Oncol 2009
Magenkarzinom: Überleben nach Erstlinientherapie
BSC1
FAMTX2
PLF3
FLO3
ECF4
EOF4
DCF5
XP6
ECX4
EOX4
Median OS (months)
Lordick, Lorenzen et al Gastric Cancer 2014; 17(2):213-25
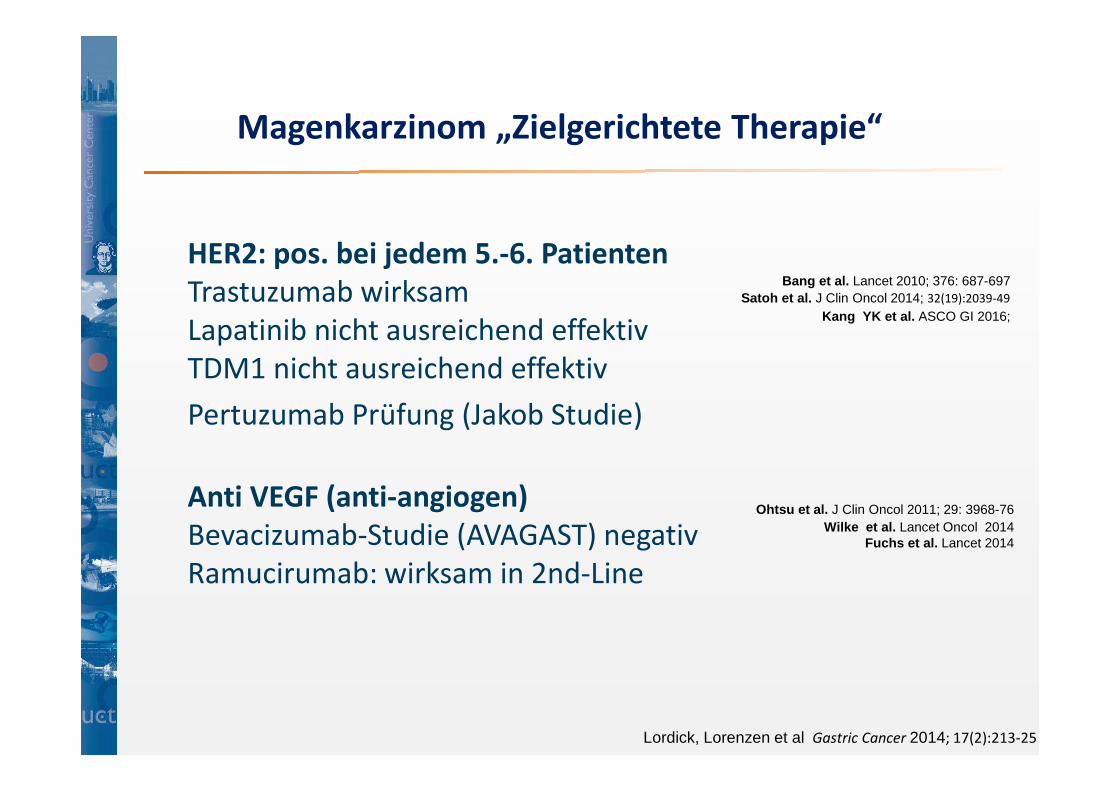
HER2: pos. bei jedem 5.-6. Patienten
Trastuzumab wirksam
Lapatinib nicht ausreichend effektiv
TDM1 nicht ausreichend effektiv
Pertuzumab Prüfung (Jakob Studie)
Anti VEGF (anti-angiogen)
Bevacizumab-Studie (AVAGAST) negativ
Ramucirumab: wirksam in 2nd-Line
Bang et al. Lancet 2010; 376: 687-697Satoh et al. J Clin Oncol 2014; 32(19):2039-49
Ohtsu et al. J Clin Oncol 2011; 29: 3968-76
Magenkarzinom „Zielgerichtete Therapie“
Kang YK et al. ASCO GI 2016;
Wilke et al. Lancet Oncol 2014Fuchs et al. Lancet 2014
HER2
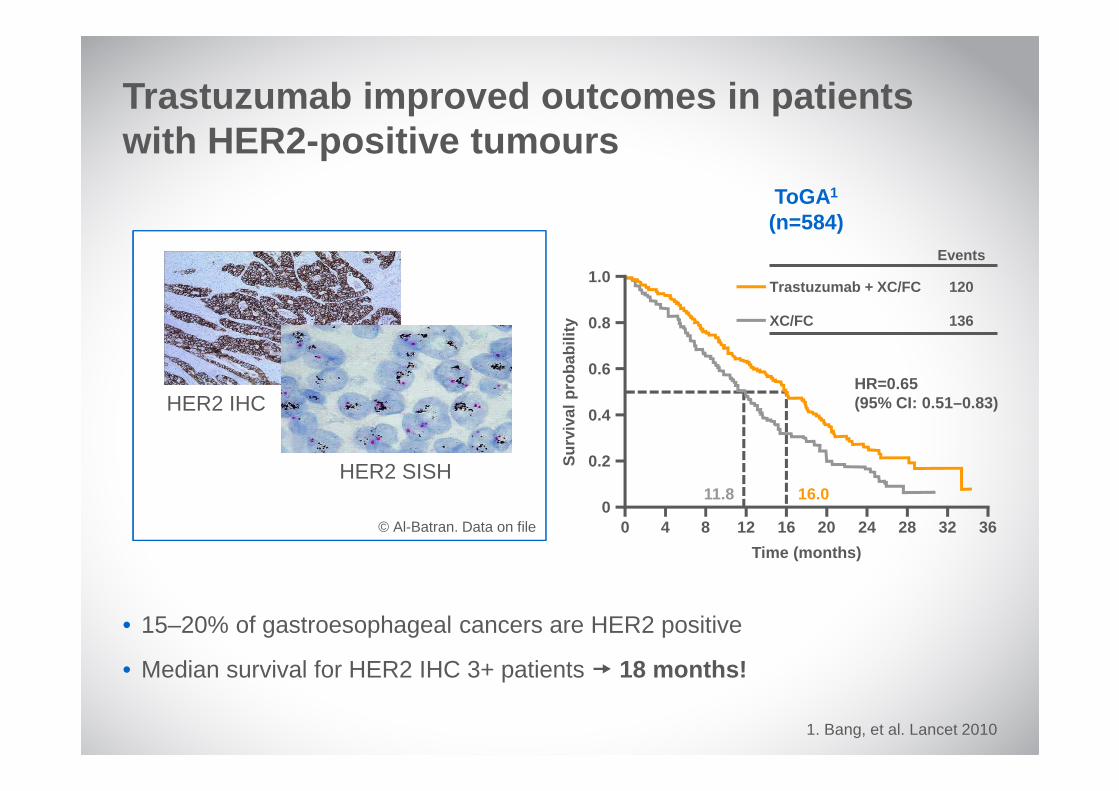
• 15–20% of gastroesophageal cancers are HER2 positive
• Median survival for HER2 IHC 3+ patients � 18 months!
1. Bang, et al. Lancet 2010
Trastuzumab improved outcomes in patients with HER2-positive tumours
ToGA1
(n=584)
© Al-Batran. Data on file0
0.2
0.4
0.6
0.8
1.0
Sur
viva
l pro
babi
lity
0 4 8 12 16 20 24 28 32 36
11.8 16.0
Time (months)
HR=0.65(95% CI: 0.51–0.83)
Events
Trastuzumab + XC/FC 120
XC/FC 136
HER2 IHC
HER2 SISH
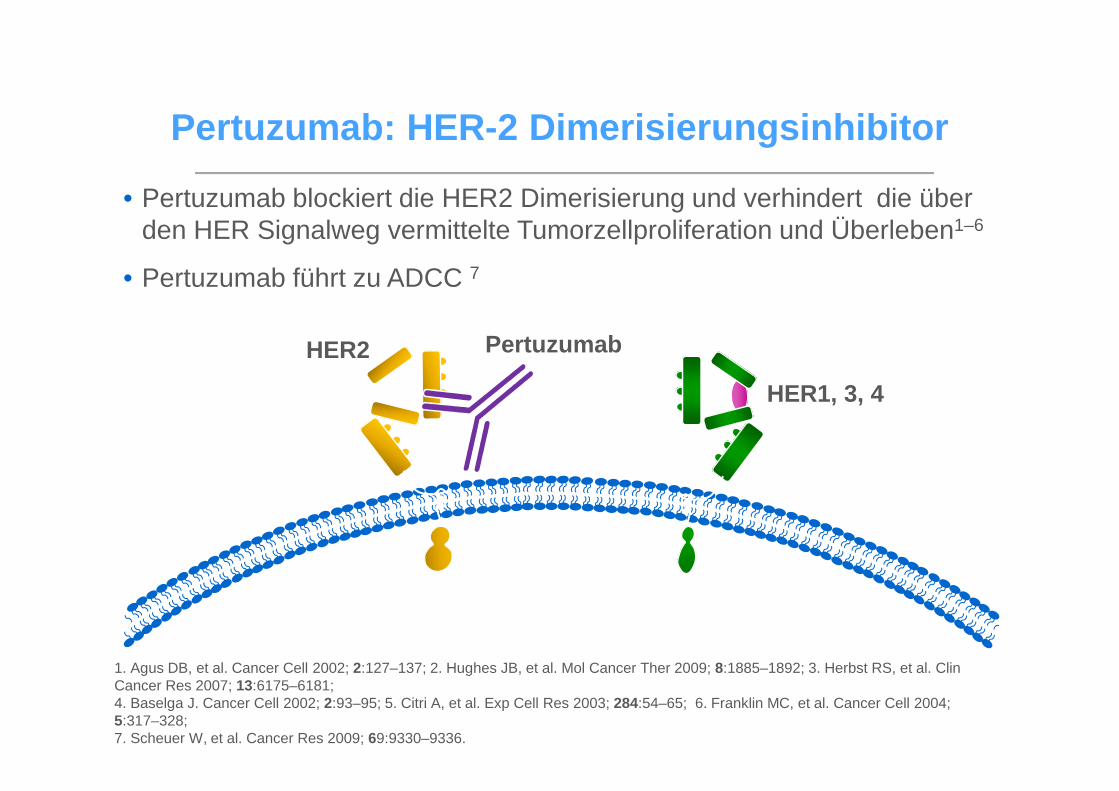
Pertuzumab : HER-2 Dimerisierungsinhibitor
HER2
HER1, 3, 4
Pertuzumab
• Pertuzumab blockiert die HER2 Dimerisierung und verhindert die über den HER Signalweg vermittelte Tumorzellproliferation und Überleben1–6
• Pertuzumab führt zu ADCC 7
1. Agus DB, et al. Cancer Cell 2002; 2:127–137; 2. Hughes JB, et al. Mol Cancer Ther 2009; 8:1885–1892; 3. Herbst RS, et al. Clin Cancer Res 2007; 13:6175–6181;4. Baselga J. Cancer Cell 2002; 2:93–95; 5. Citri A, et al. Exp Cell Res 2003; 284:54–65; 6. Franklin MC, et al. Cancer Cell 2004; 5:317–328; 7. Scheuer W, et al. Cancer Res 2009; 69:9330–9336.
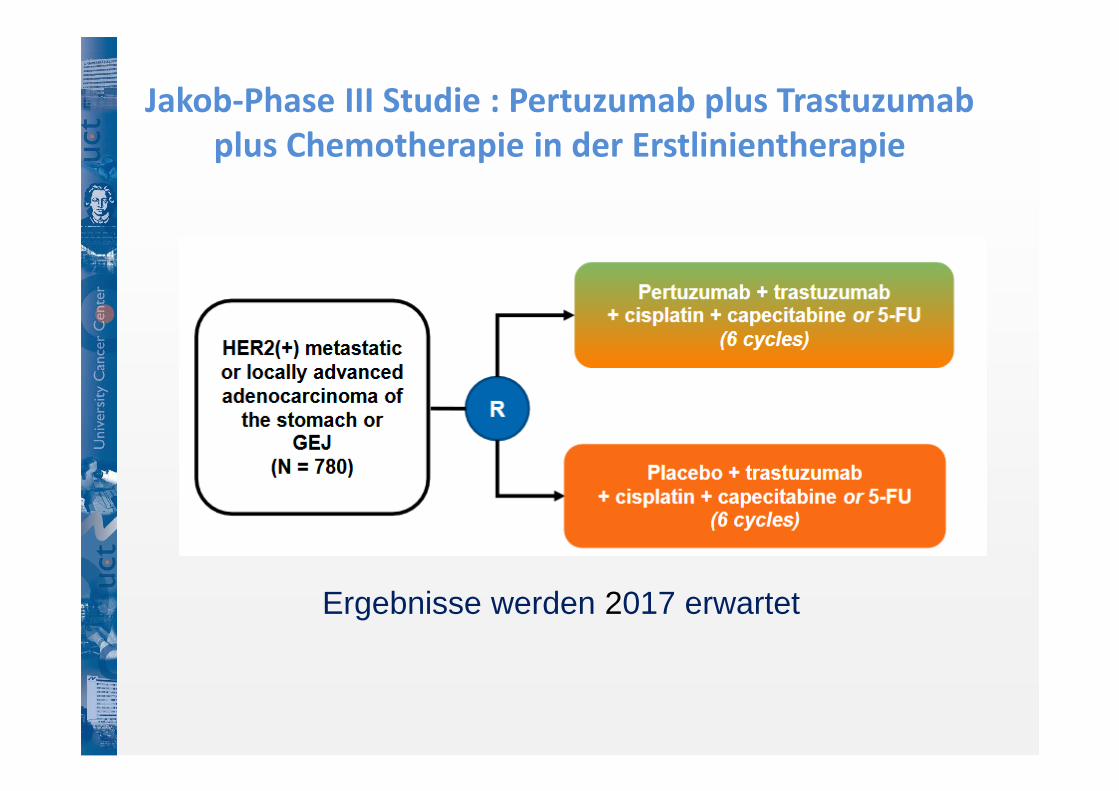
Jakob-Phase III Studie : Pertuzumab plus Trastuzumab
plus Chemotherapie in der Erstlinientherapie
Ergebnisse werden 2017 erwartet
VEGF/VEGFR
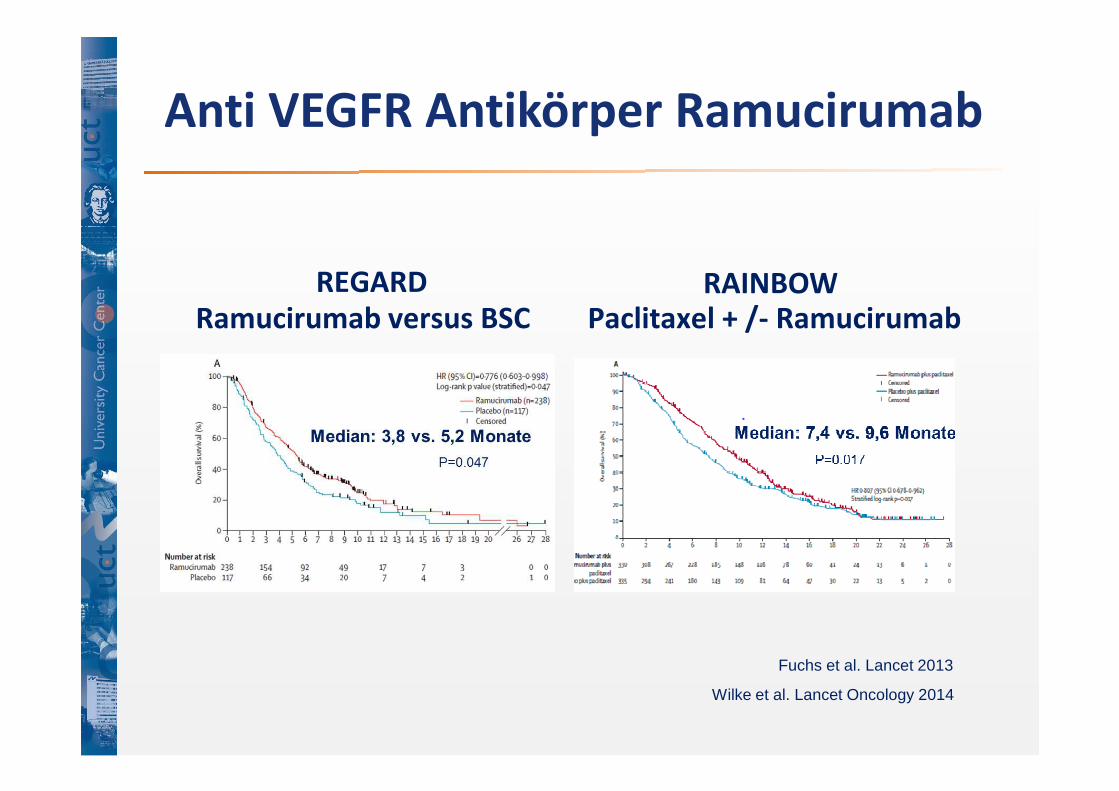
Anti VEGFR Antikörper Ramucirumab
Ramucirumab versus BSC Paclitaxel + /- Ramucirumab
REGARD RAINBOW
Fuchs et al. Lancet 2013
Wilke et al. Lancet Oncology 2014
FOLFIRI + Ramucirumab
Paclitaxel + Ramucirumab
R
2
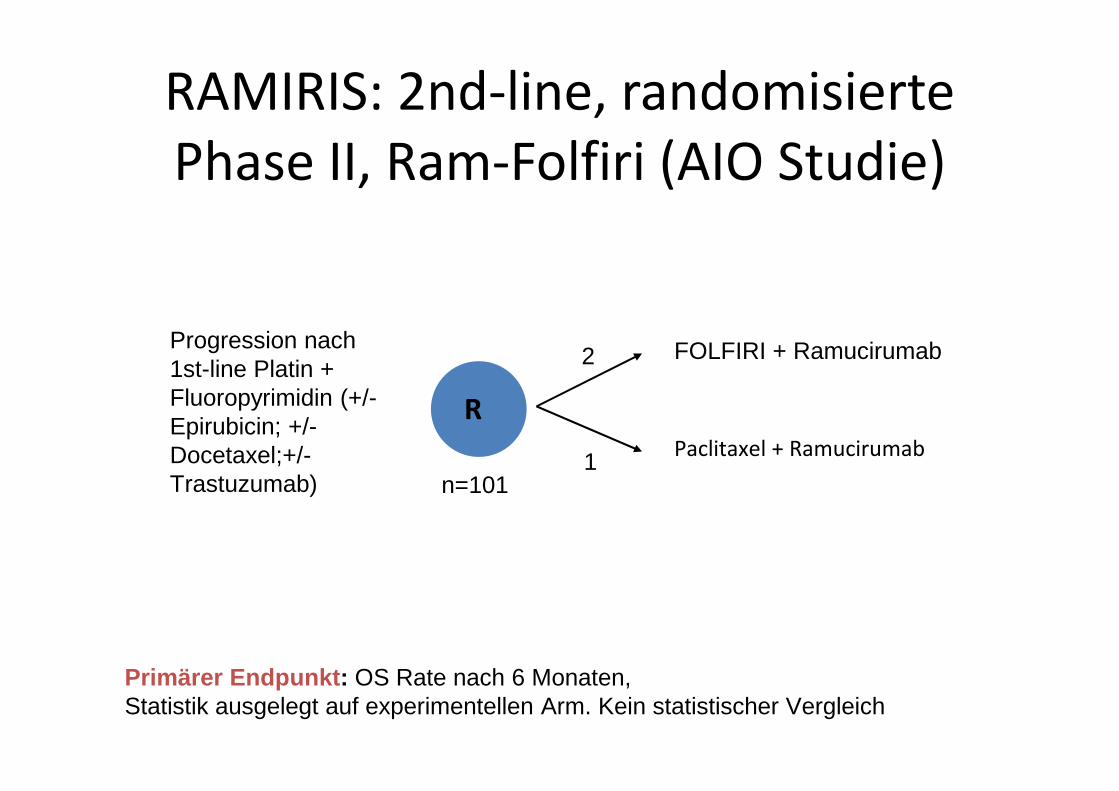
1n=101
Primärer Endpunkt : OS Rate nach 6 Monaten, Statistik ausgelegt auf experimentellen Arm. Kein statistischer Vergleich
Progression nach 1st-line Platin + Fluoropyrimidin (+/-Epirubicin; +/-Docetaxel;+/-Trastuzumab)
RAMIRIS: 2nd-line, randomisierte
Phase II, Ram-Folfiri (AIO Studie)
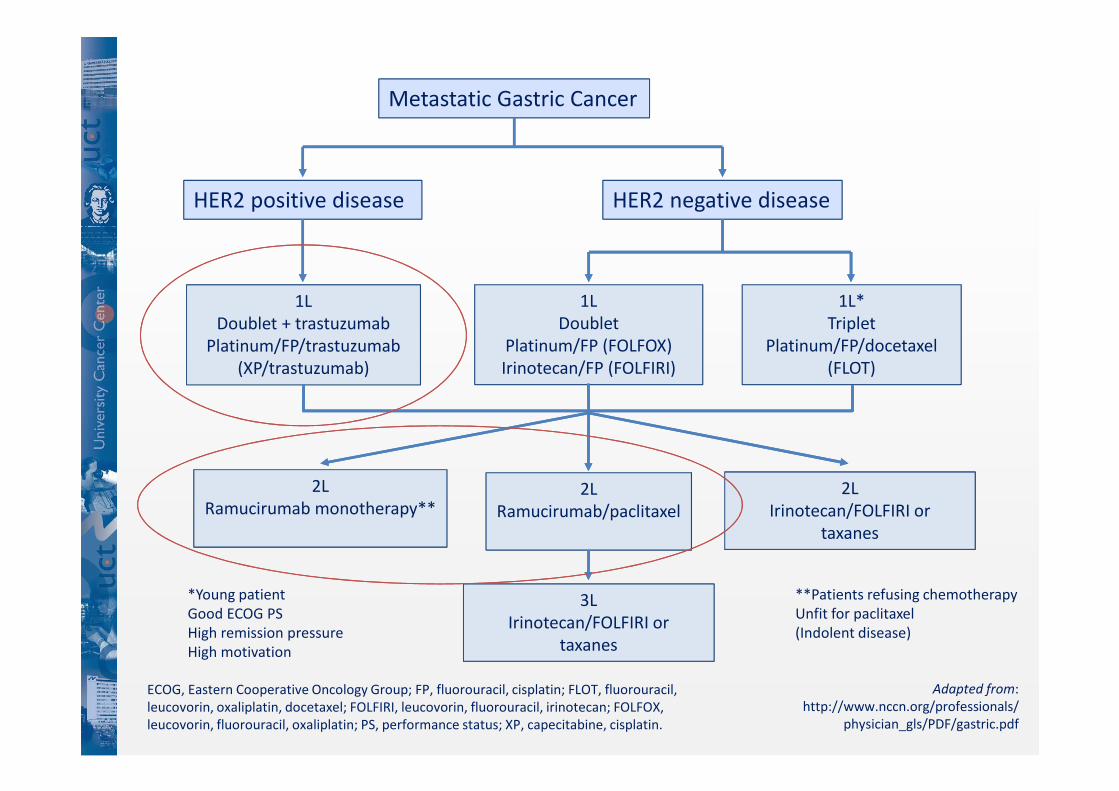
Metastatic Gastric Cancer
HER2 positive disease HER2 negative disease
1L
Doublet + trastuzumab
Platinum/FP/trastuzumab
(XP/trastuzumab)
1L*
Triplet
Platinum/FP/docetaxel
(FLOT)
1L
Doublet
Platinum/FP (FOLFOX)
Irinotecan/FP (FOLFIRI)
**Patients refusing chemotherapy
Unfit for paclitaxel
(Indolent disease)
2L
Ramucirumab/paclitaxel
3L
Irinotecan/FOLFIRI or
taxanes
*Young patient
Good ECOG PS
High remission pressure
High motivation
2L
Irinotecan/FOLFIRI or
taxanes
2L
Ramucirumab monotherapy**
Adapted from:
http://www.nccn.org/professionals/
physician_gls/PDF/gastric.pdf
ECOG, Eastern Cooperative Oncology Group; FP, fluorouracil, cisplatin; FLOT, fluorouracil,
leucovorin, oxaliplatin, docetaxel; FOLFIRI, leucovorin, fluorouracil, irinotecan; FOLFOX,
leucovorin, fluorouracil, oxaliplatin; PS, performance status; XP, capecitabine, cisplatin.
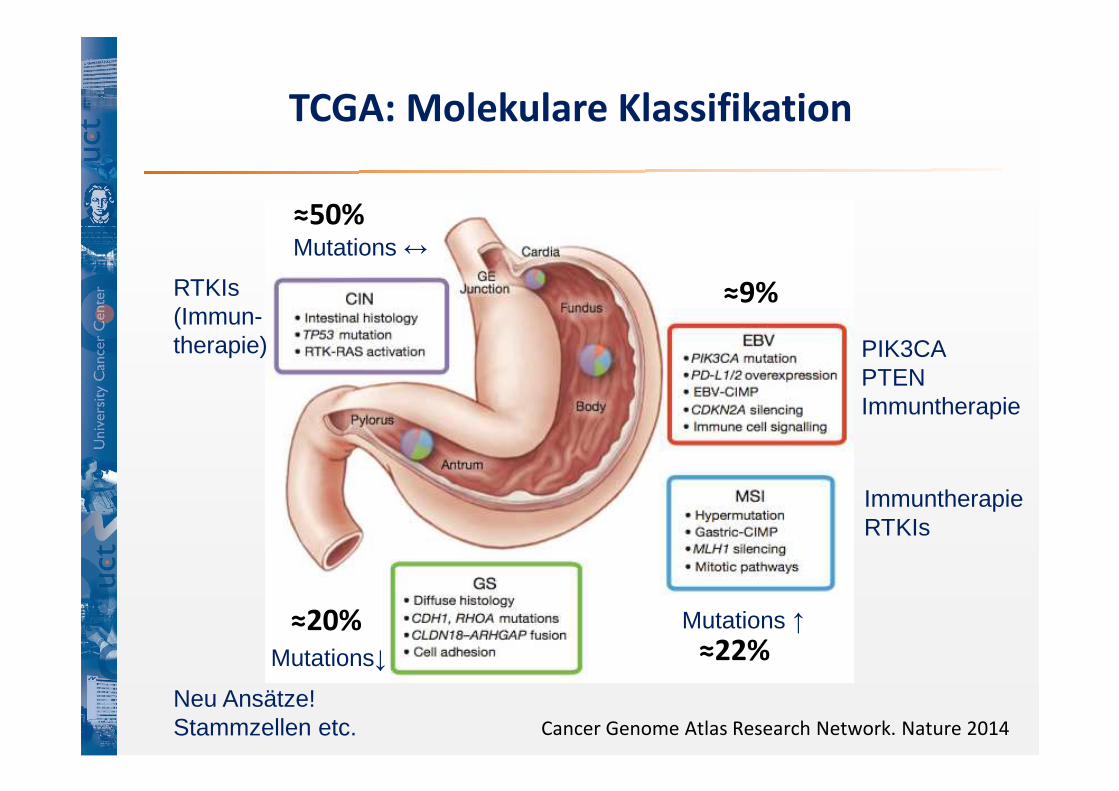
TCGA: Molekulare Klassifikation
Cancer Genome Atlas Research Network. Nature 2014
≈9%
≈22%≈20%
≈50%
Mutations ↑
Mutations↓
Mutations ↔
RTKIs(Immun-therapie) PIK3CA
PTENImmuntherapie
ImmuntherapieRTKIs
Neu Ansätze!Stammzellen etc.
Immuntherapie
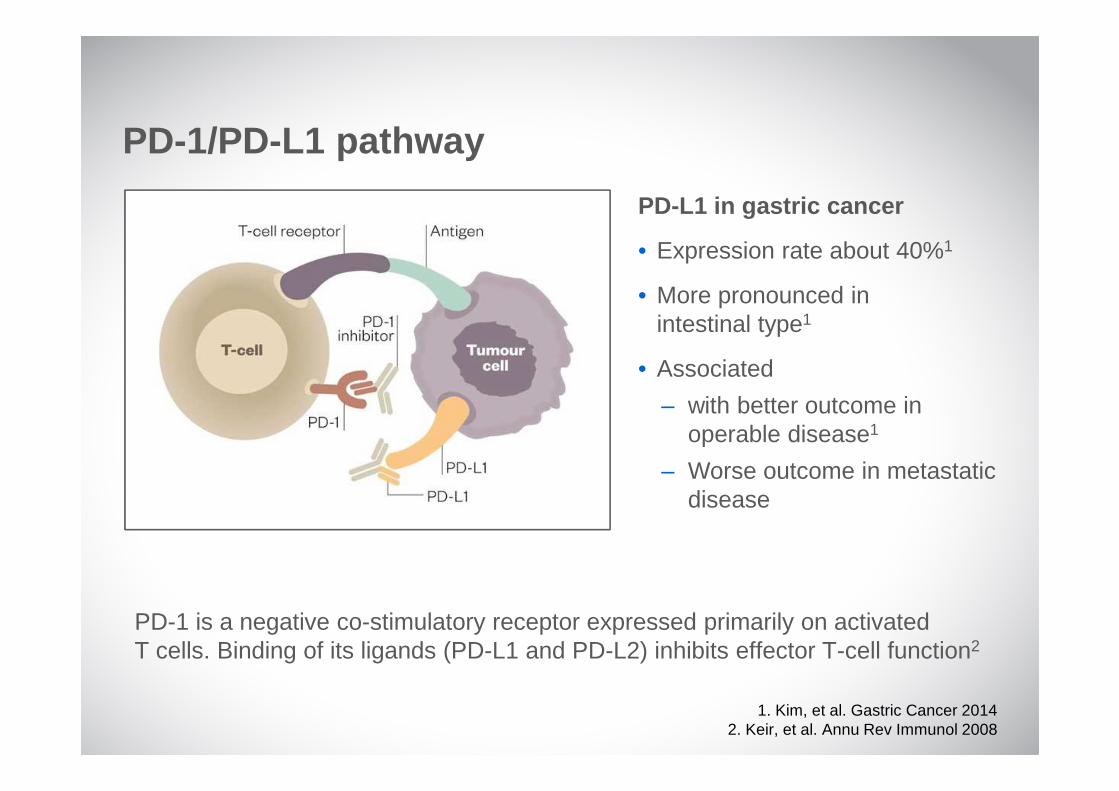
PD-L1 in gastric cancer
• Expression rate about 40%1
• More pronounced in intestinal type1
• Associated
– with better outcome in operable disease1
– Worse outcome in metastatic disease
PD-1/PD-L1 pathway
PD-1 is a negative co-stimulatory receptor expressed primarily on activated T cells. Binding of its ligands (PD-L1 and PD-L2) inhibits effector T-cell function2
1. Kim, et al. Gastric Cancer 20142. Keir, et al. Annu Rev Immunol 2008
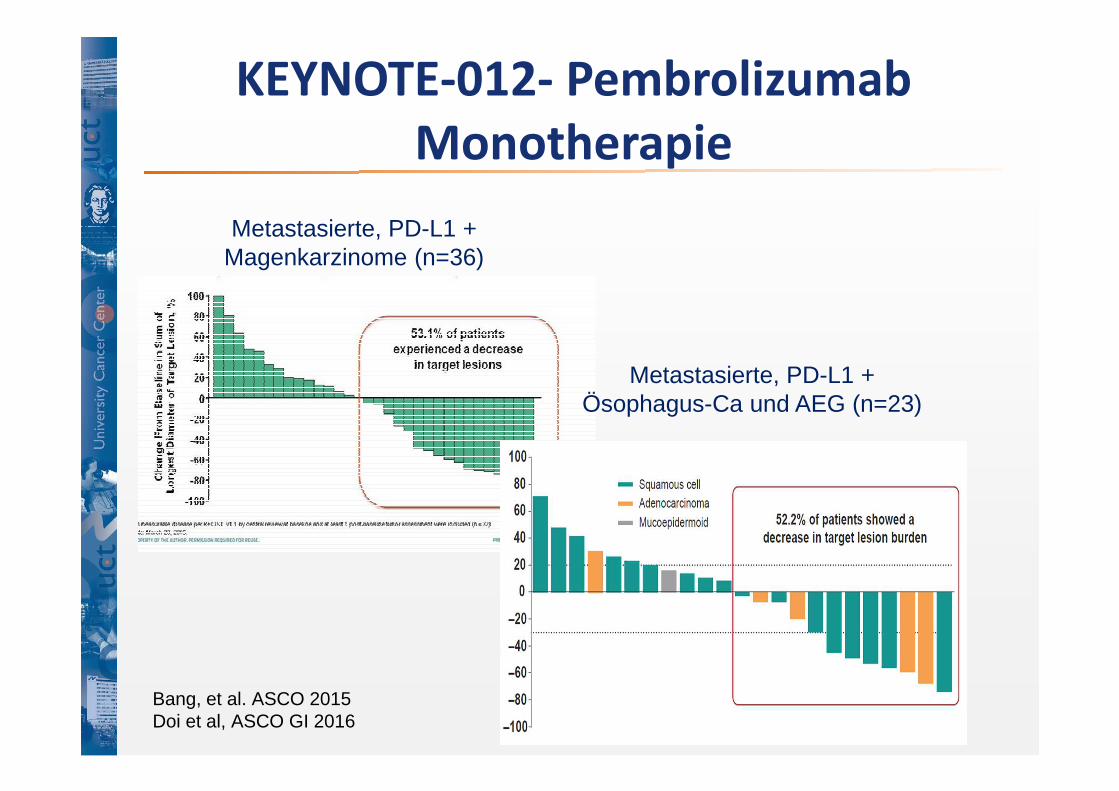
KEYNOTE-012- Pembrolizumab
Monotherapie
Metastasierte, PD-L1 + Ösophagus-Ca und AEG (n=23)
Metastasierte, PD-L1 + Magenkarzinome (n=36)
Bang, et al. ASCO 2015Doi et al, ASCO GI 2016
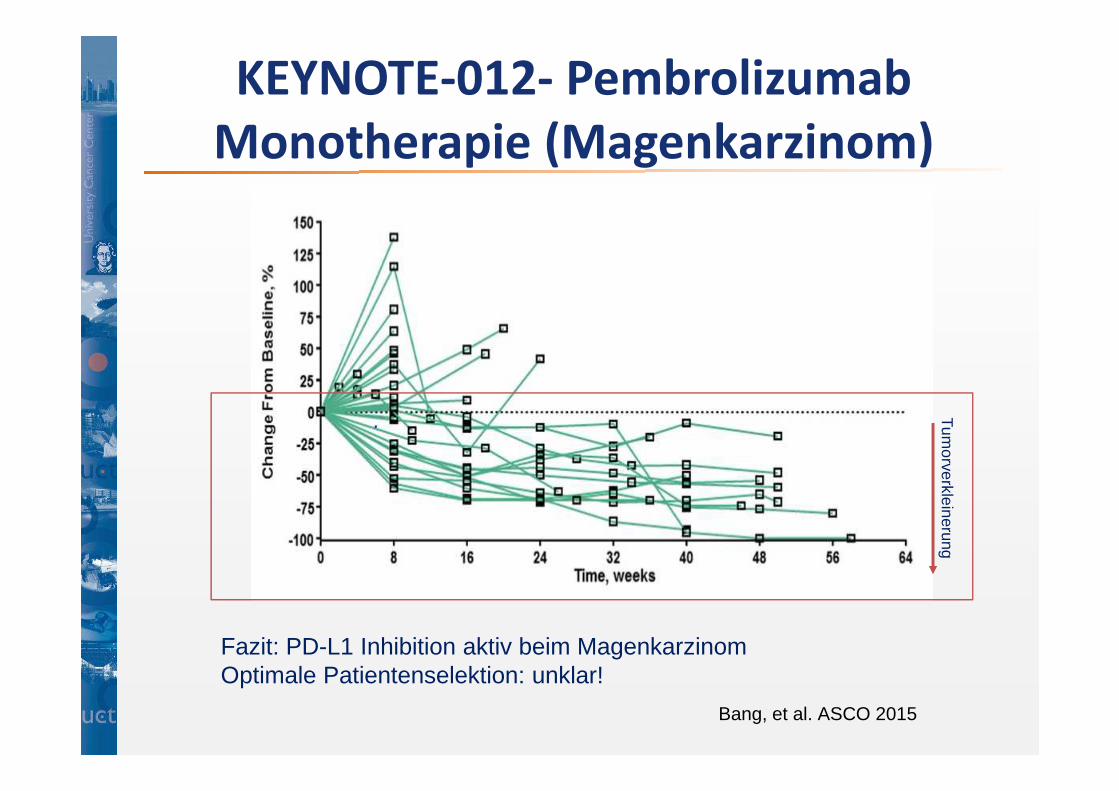
KEYNOTE-012- Pembrolizumab
Monotherapie (Magenkarzinom)T
umorverkleinerung
Bang, et al. ASCO 2015
Fazit: PD-L1 Inhibition aktiv beim MagenkarzinomOptimale Patientenselektion: unklar!
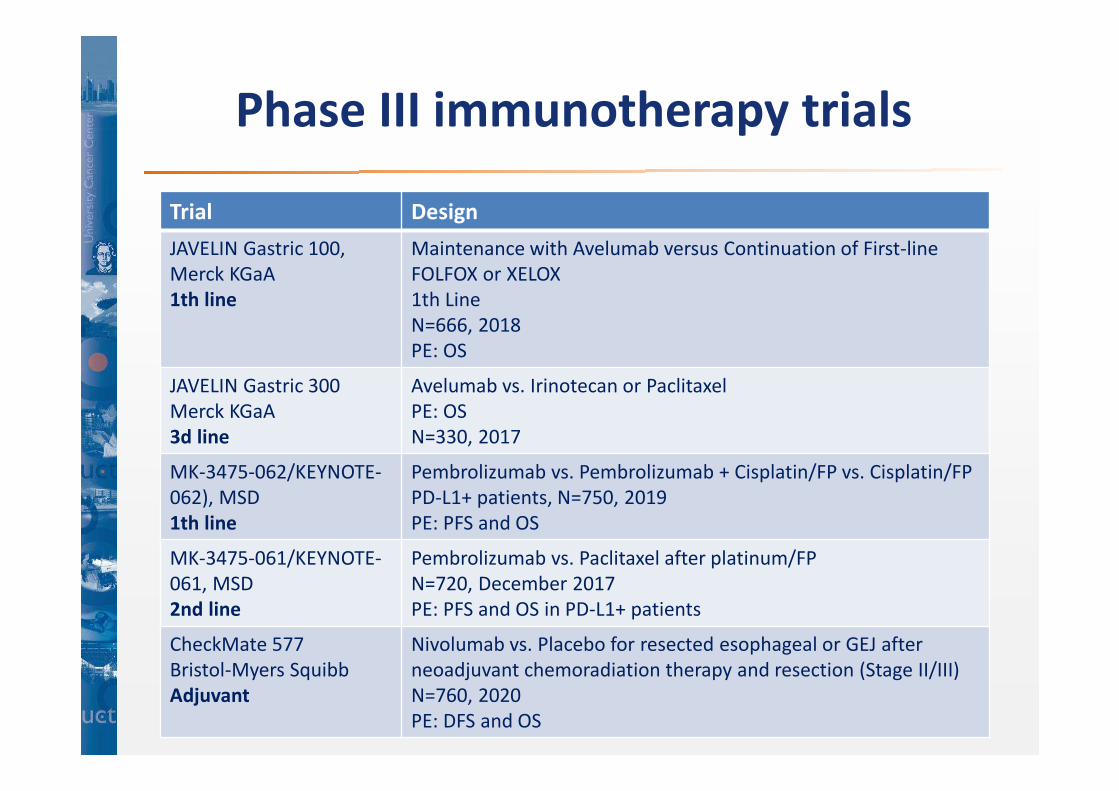
Trial Design
JAVELIN Gastric 100,
Merck KGaA
1th line
Maintenance with Avelumab versus Continuation of First-line
FOLFOX or XELOX
1th Line
N=666, 2018
PE: OS
JAVELIN Gastric 300
Merck KGaA
3d line
Avelumab vs. Irinotecan or Paclitaxel
PE: OS
N=330, 2017
MK-3475-062/KEYNOTE-
062), MSD
1th line
Pembrolizumab vs. Pembrolizumab + Cisplatin/FP vs. Cisplatin/FP
PD-L1+ patients, N=750, 2019
PE: PFS and OS
MK-3475-061/KEYNOTE-
061, MSD
2nd line
Pembrolizumab vs. Paclitaxel after platinum/FP
N=720, December 2017
PE: PFS and OS in PD-L1+ patients
CheckMate 577
Bristol-Myers Squibb
Adjuvant
Nivolumab vs. Placebo for resected esophageal or GEJ after
neoadjuvant chemoradiation therapy and resection (Stage II/III)
N=760, 2020
PE: DFS and OS
Phase III immunotherapy trials
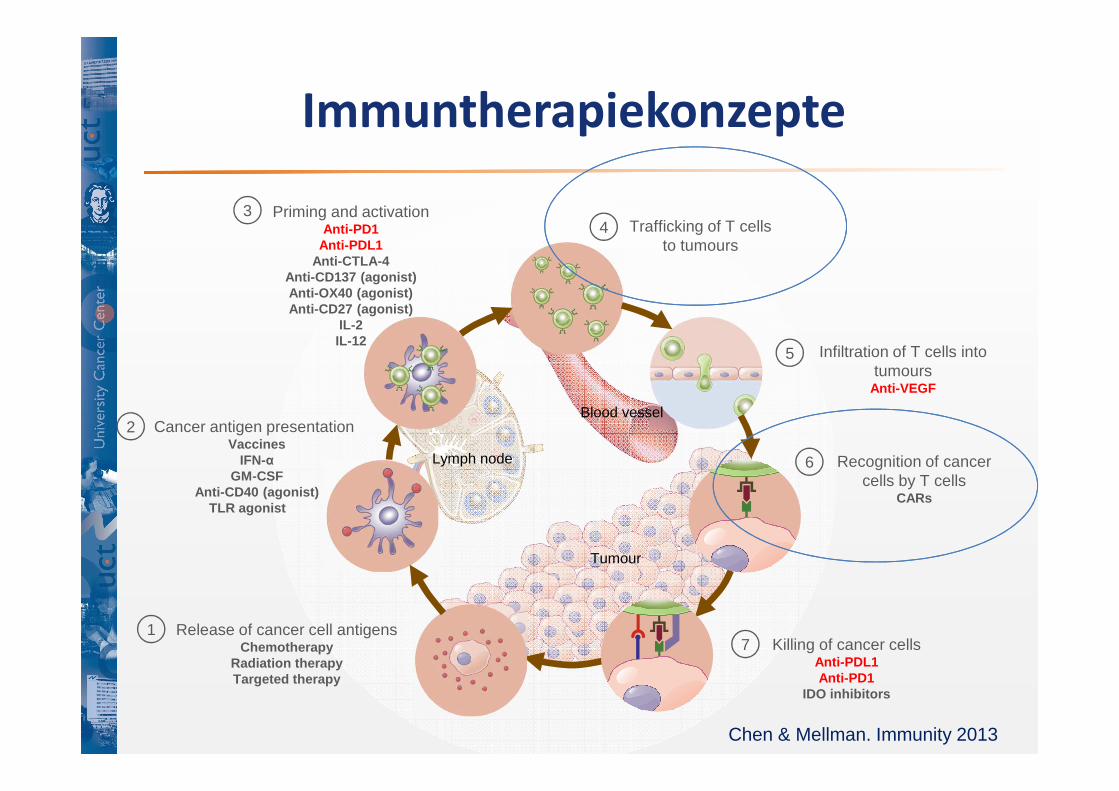
Immuntherapiekonzepte
Tumour
Lymph node
Blood vessel
Chen & Mellman. Immunity 2013
Release of cancer cell antigensChemotherapy
Radiation therapyTargeted therapy
1
Cancer antigen presentationVaccines
IFN-αGM-CSF
Anti-CD40 (agonist)TLR agonist
2
Priming and activationAnti-PD1
Anti-PDL1Anti-CTLA-4
Anti-CD137 (agonist)Anti-OX40 (agonist)Anti-CD27 (agonist)
IL-2IL-12
3
Infiltration of T cells into tumours
Anti-VEGF
5
Recognition of cancercells by T cells
CARs
6
Killing of cancer cellsAnti-PDL1Anti-PD1
IDO inhibitors
7
Trafficking of T cellsto tumours
4
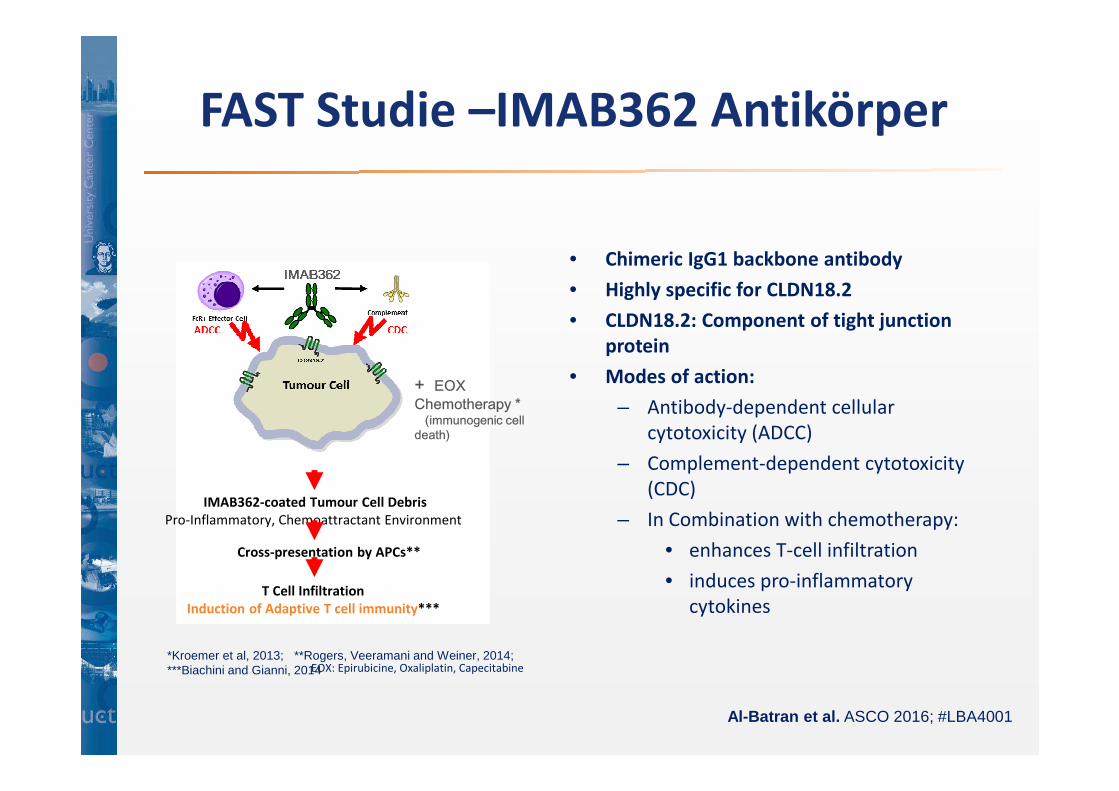
+ EOX Chemotherapy *
(immunogenic cell death)
T Cell Infiltration
Induction of Adaptive T cell immunity***
IMAB362-coated Tumour Cell Debris
Pro-Inflammatory, Chemoattractant Environment
Cross-presentation by APCs**
*Kroemer et al, 2013; **Rogers, Veeramani and Weiner, 2014; ***Biachini and Gianni, 2014EOX: Epirubicine, Oxaliplatin, Capecitabine
• Chimeric IgG1 backbone antibody
• Highly specific for CLDN18.2
• CLDN18.2: Component of tight junction
protein
• Modes of action:
– Antibody-dependent cellular
cytotoxicity (ADCC)
– Complement-dependent cytotoxicity
(CDC)
– In Combination with chemotherapy:
• enhances T-cell infiltration
• induces pro-inflammatory
cytokines
Al-Batran et al. ASCO 2016; #LBA4001
FAST Studie –IMAB362 Antikörper
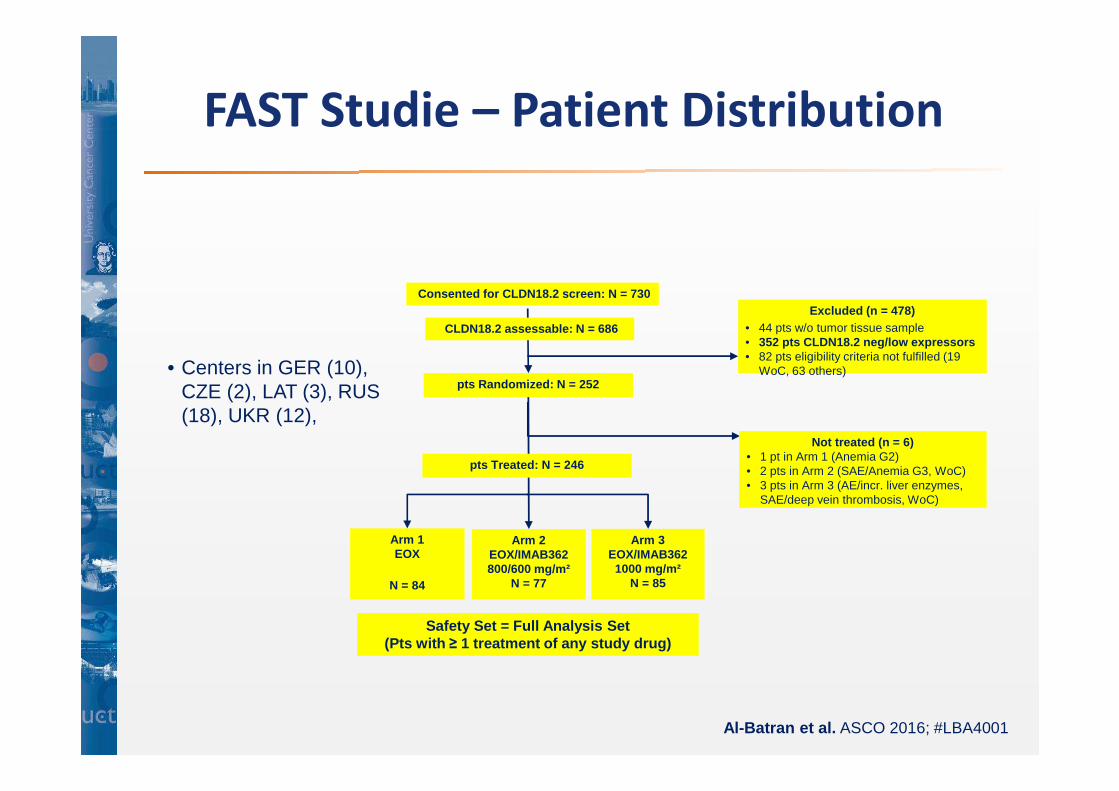
• Centers in GER (10), CZE (2), LAT (3), RUS (18), UKR (12),
pts Randomized: N = 252
Arm 1EOX
N = 84
Arm 2EOX/IMAB362 800/600 mg/m²
N = 77
Arm 3EOX/IMAB362 1000 mg/m²
N = 85
Excluded (n = 478)• 44 pts w/o tumor tissue sample• 352 pts CLDN18.2 neg/low expressors• 82 pts eligibility criteria not fulfilled (19
WoC, 63 others)
Not treated (n = 6)• 1 pt in Arm 1 (Anemia G2)• 2 pts in Arm 2 (SAE/Anemia G3, WoC)• 3 pts in Arm 3 (AE/incr. liver enzymes,
SAE/deep vein thrombosis, WoC)
Safety Set = Full Analysis Set (Pts with ≥ 1 treatment of any study drug)
CLDN18.2 assessable: N = 686
pts Treated: N = 246
Consented for CLDN18.2 screen: N = 730
Al-Batran et al. ASCO 2016; #LBA4001
FAST Studie – Patient Distribution
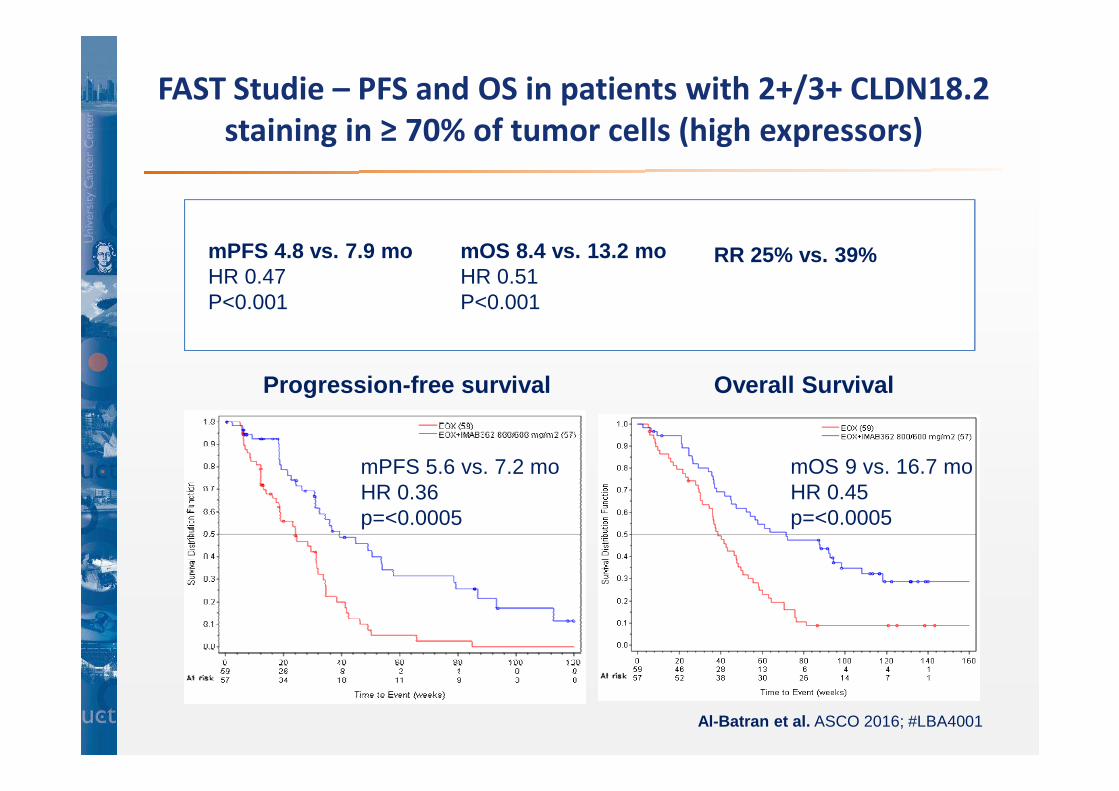
mPFS 5.6 vs. 7.2 moHR 0.36p=<0.0005
mOS 9 vs. 16.7 moHR 0.45p=<0.0005
Overall SurvivalProgression-free survival
Al-Batran et al. ASCO 2016; #LBA4001
FAST Studie – PFS and OS in patients with 2+/3+ CLDN18.2
staining in ≥ 70% of tumor cells (high expressors)
mPFS 4.8 vs. 7.9 moHR 0.47P<0.001
mOS 8.4 vs. 13.2 moHR 0.51P<0.001
RR 25% vs. 39%
Zusammenfassung
• Her2+ Magenkarzinom:– Pertuzumab/Trastuzumab/Cx vs. Trastuzumab/Cx
– Her2-Blockade + Immuntherapie (phase1/2)
• Immuntherapie
– PD-1/PD-L1 AK in Phase III, 1.-3. Linie + adjuvant
• Wirksam? Mit oder ohne Cx?
• Kombinationen: CTLA-4 AK + PD1/PD-L1 AK (ohne Cx) und
VEGF/VEGR AK + PD1/PD-L1 AK
– Neue Ansätze Z.B. IMAB362 (Phase 2)
• Sonstiges
– Weiterentwicklung Ramucirumab, MMP-9, Multitarget
TKIs, STAT Inhibitor