






Sprachen
Seiten
Rechtliche

Welche Donor-spezifischen HLA Antikörper sind schädlich?
Prof. Dr. med. Caner Süsal Transplantationsimmunologie
Institut für Immunologie Universität Heidelberg
Sensitization – Alloantibody Production
Before Transplantation Hyperacute rejection Accelerated humoral rejection Delayed graft function
After Transplantation (de novo)
“Chronic rejection”
Alloantibodies
Alloantibodies
HLA (A, B, C, DRB1/3/4/5, DQA1, DQB1, DPA1, DPB1) Non-HLA
Angiotensin II Typ 1 R MIC-A Endothelial antigens
Antibody Specification
CDC-PRA ELISA-PRA Luminex (PRA, Single Antigen)
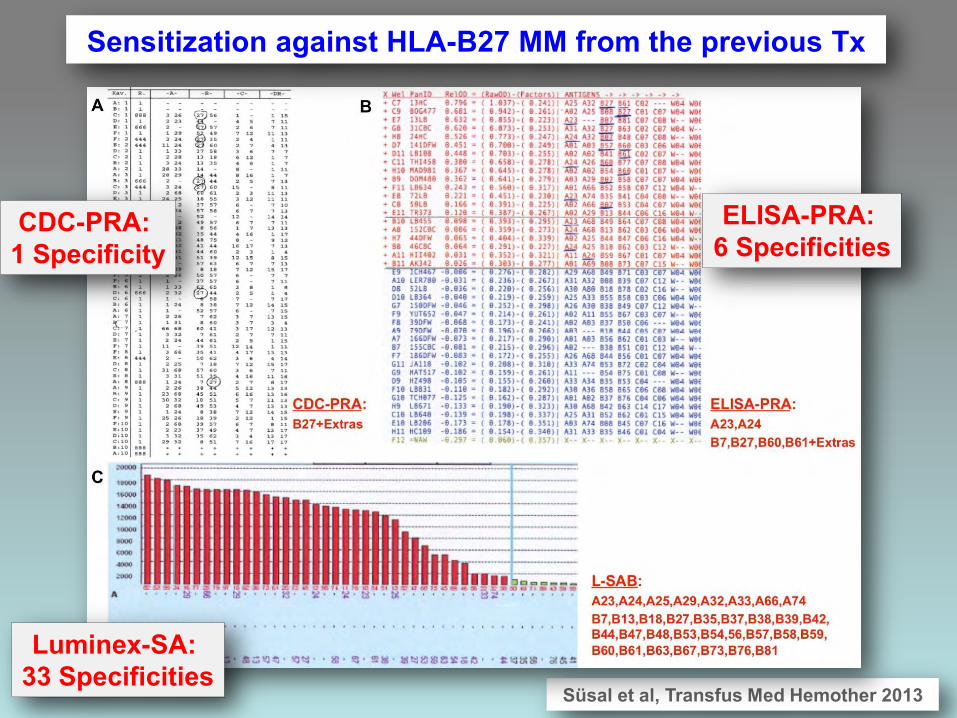
Süsal et al, Transfus Med Hemother 2013
Sensitization against HLA-B27 MM from the previous Tx
CDC-PRA: 1 Specificity
ELISA-PRA: 6 Specificities
Luminex-SA: 33 Specificities
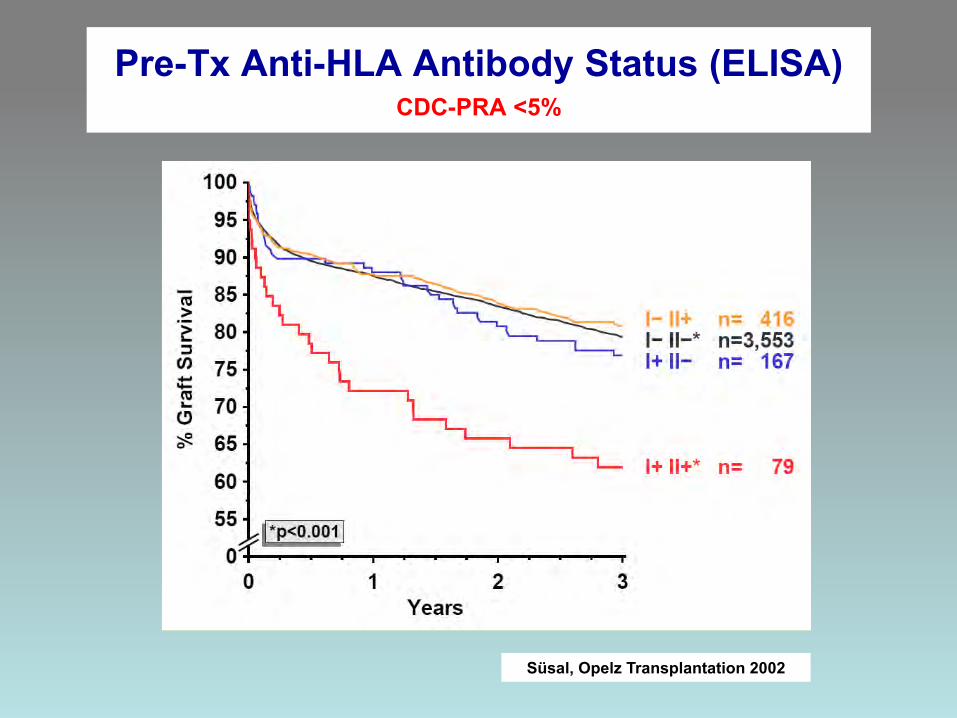
Süsal, Opelz Transplantation 2002
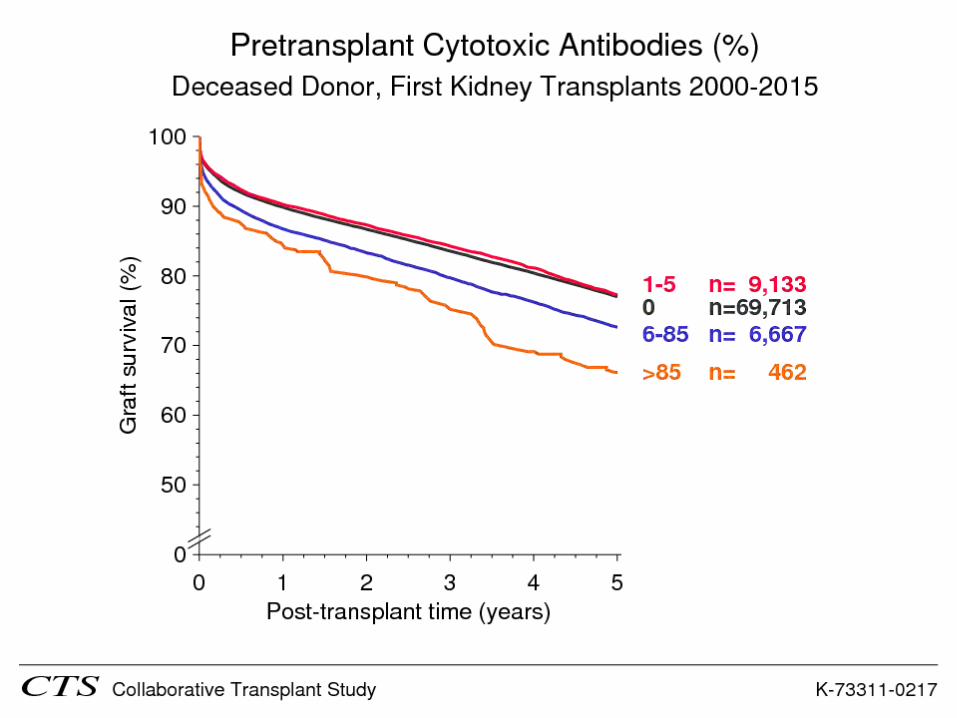
Pre-Tx Anti-HLA Antibody Status (ELISA) CDC-PRA <5%
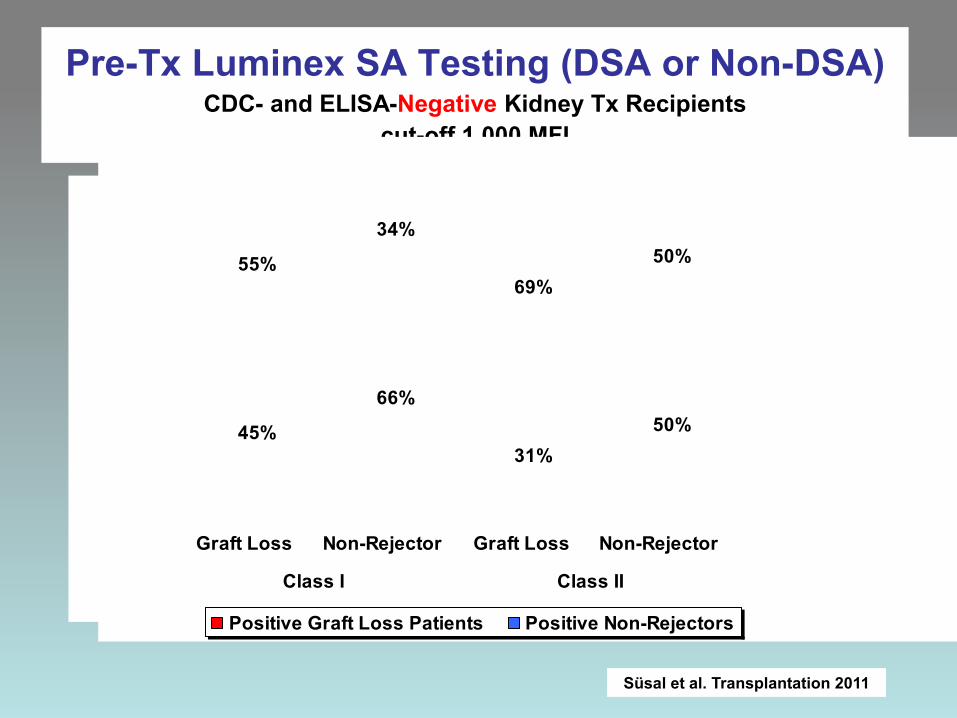
Pre-Tx Luminex SA Testing (DSA or Non-DSA) CDC- and ELISA-Negative Kidney Tx Recipients
cut-off 1,000 MFI
45%
66%
Graft Loss Non-Rejector
Class I
31%50%
Graft Loss Non-Rejector
Class II
45%
55%
66%
34%
31%
69%
50%
50%
Graft Loss Non-Rejector Graft Loss Non-Rejector
Class I Class II
Positive Graft Loss Patients Positive Non-Rejectors
Süsal et al. Transplantation 2011
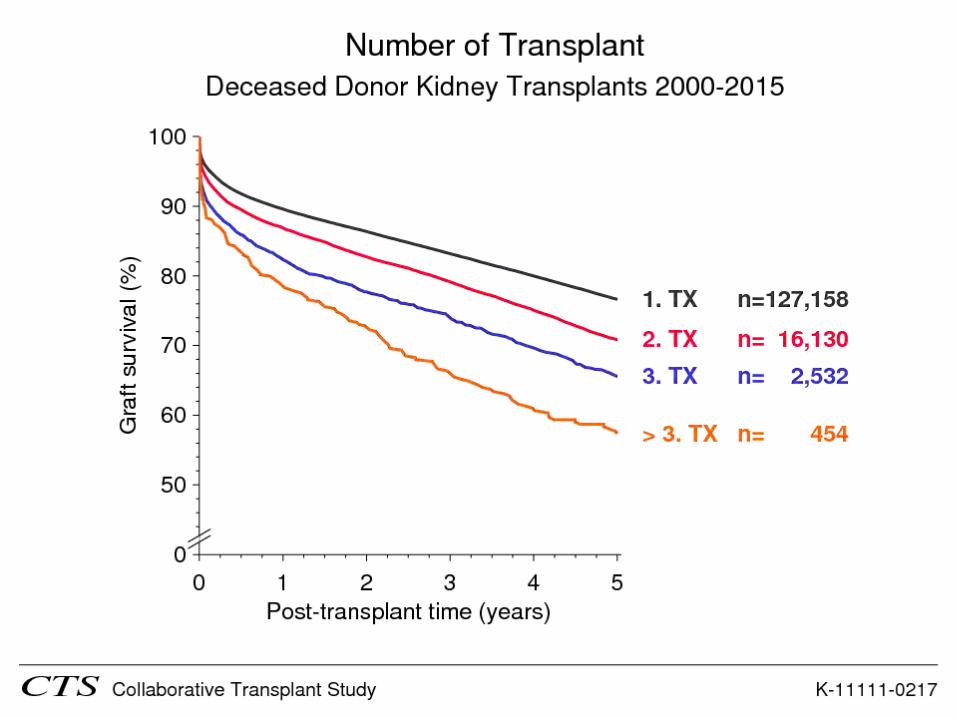
Disadvantages of Presensitization 1. Prolonged waiting time
2. Inferior graft survival
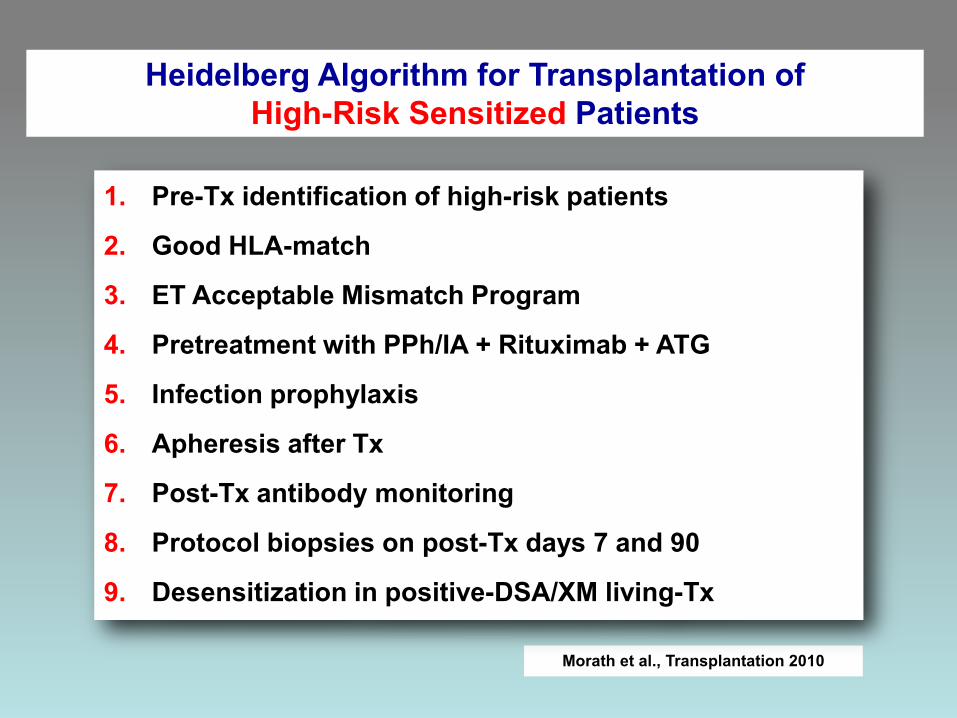
Morath et al., Transplantation 2010
1. Pre-Tx identification of high-risk patients
2. Good HLA-match
3. ET Acceptable Mismatch Program
4. Pretreatment with PPh/IA + Rituximab + ATG
5. Infection prophylaxis
6. Apheresis after Tx
7. Post-Tx antibody monitoring
8. Protocol biopsies on post-Tx days 7 and 90
9. Desensitization in positive-DSA/XM living-Tx
Heidelberg Algorithm for Transplantation of High-Risk Sensitized Patients

Four High Risk Groups
DSA- and XM-Positive Patients
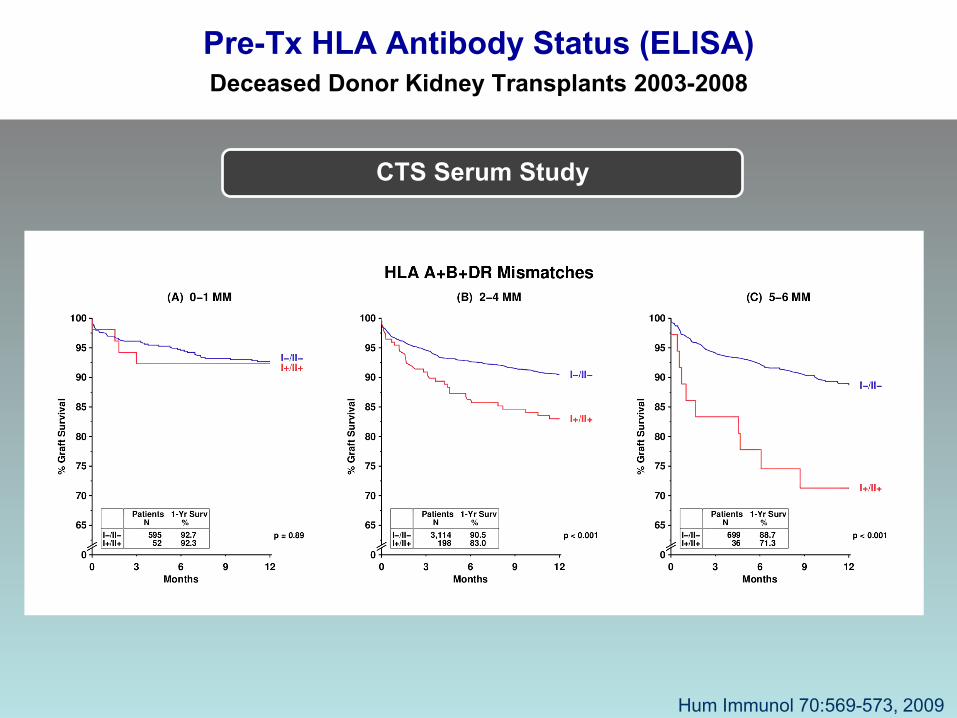
Pre-Tx HLA Antibody Status (ELISA) Deceased Donor Kidney Transplants 2003-2008
CTS Serum Study
Hum Immunol 70:569-573, 2009
Morath… Süsal, Transplantation 2010
1. Pre-Tx identification of high-risk patients
2. Good HLA-match
3. ET Acceptable Mismatch Program
4. Pretreatment with PPh/IA + Rituximab + ATG
5. Infection prophylaxis
6. Apheresis after Tx
7. Post-Tx antibody monitoring
8. Protocol biopsies on post-Tx days 7 and 90
9. Desensitization in positive-DSA/XM living-Tx
Heidelberg Algorithm for Transplantation of High-Risk Sensitized Patients
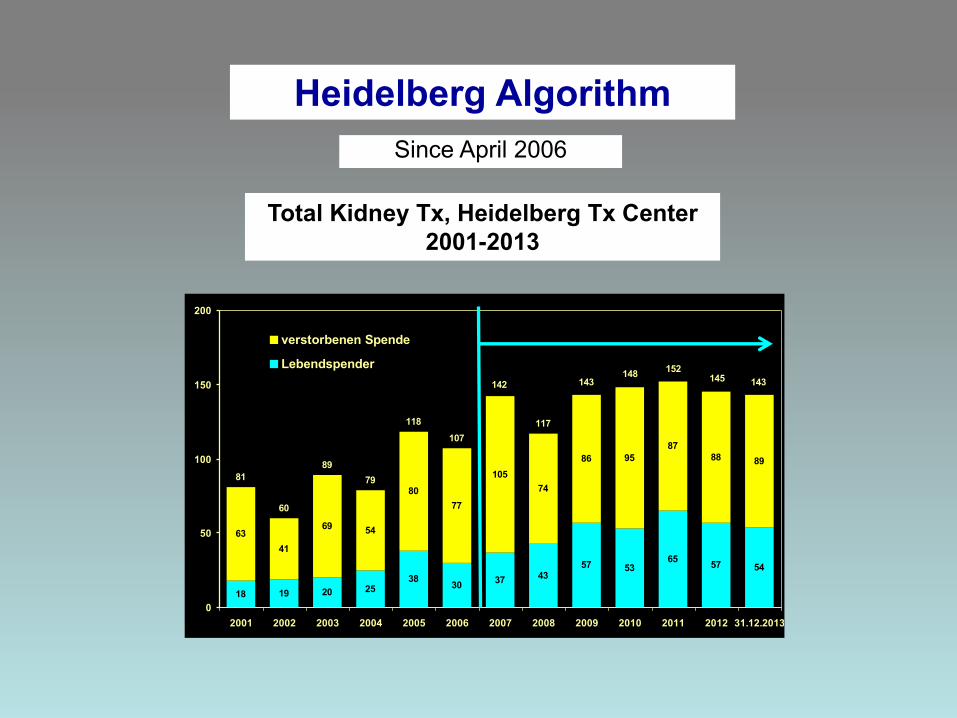
Total Kidney Tx, Heidelberg Tx Center 2001-2013
18 19 20 2538 30 37 43
57 5365 57 54
6341
69 54
8077
10574
86 9587
88 8981
60
8979
118107
117
142 143148 152
145
0
50
100
150
200
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 31.12.2013
verstorbenen Spende
Lebendspender143
Heidelberg Algorithm Since April 2006
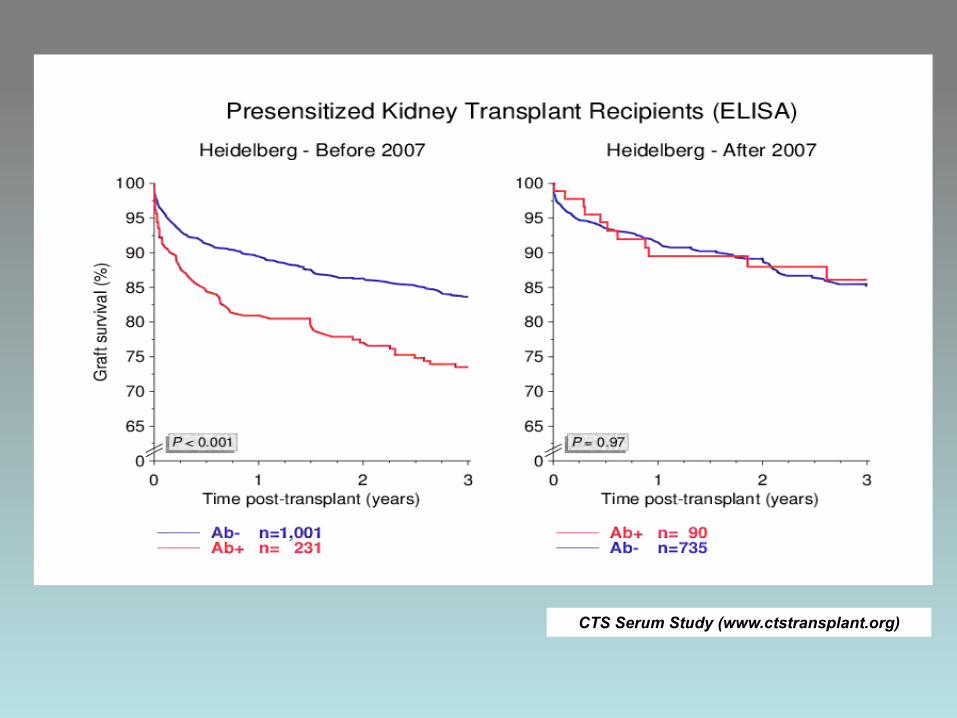
CTS Serum Study (www.ctstransplant.org)
1. Pre-existing DSA
2. Loss of pre-existing DSA 3. Persistence of pre-existing DSA 4. Reappearance of pre-existing DSA 5. de novo development of DSA 6. C1q-/C3d-DSA
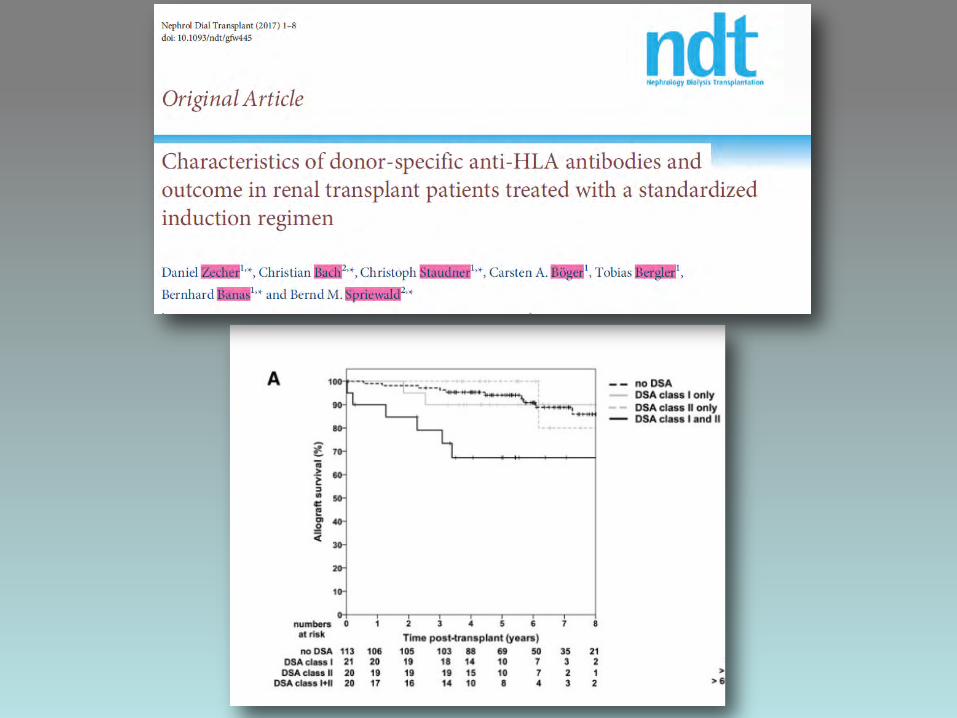
Donor-Specific HLA Alloantibodies (DSA)
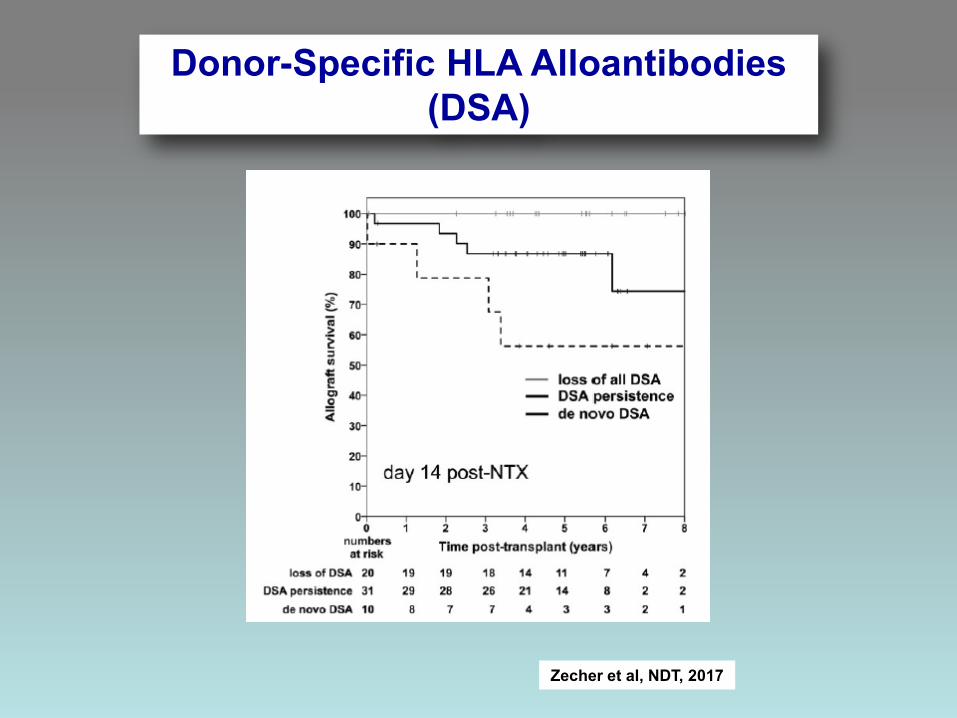
Donor-Specific HLA Alloantibodies (DSA)
Zecher et al, NDT, 2017
Morath… Süsal, Transplantation 2010
1. Pre-Tx identification of high-risk patients
2. Good HLA-match
3. ET Acceptable Mismatch Program
4. Pretreatment with PPh/IA + Rituximab + ATG
5. Infection prophylaxis
6. Apheresis after Tx
7. Post-Tx antibody monitoring
8. Protocol biopsies on post-Tx days 7 and 90
9. Desensitization in positive-DSA/XM living-Tx
Heidelberg Algorithm for Transplantation of High-Risk Sensitized Patients
1. International CTS Serum Project
2. Heidelberg Pediatric Cohort
3. Heidelberg High-Risk Population
Clinical Relevance of Post-Tx DSA Monitoring
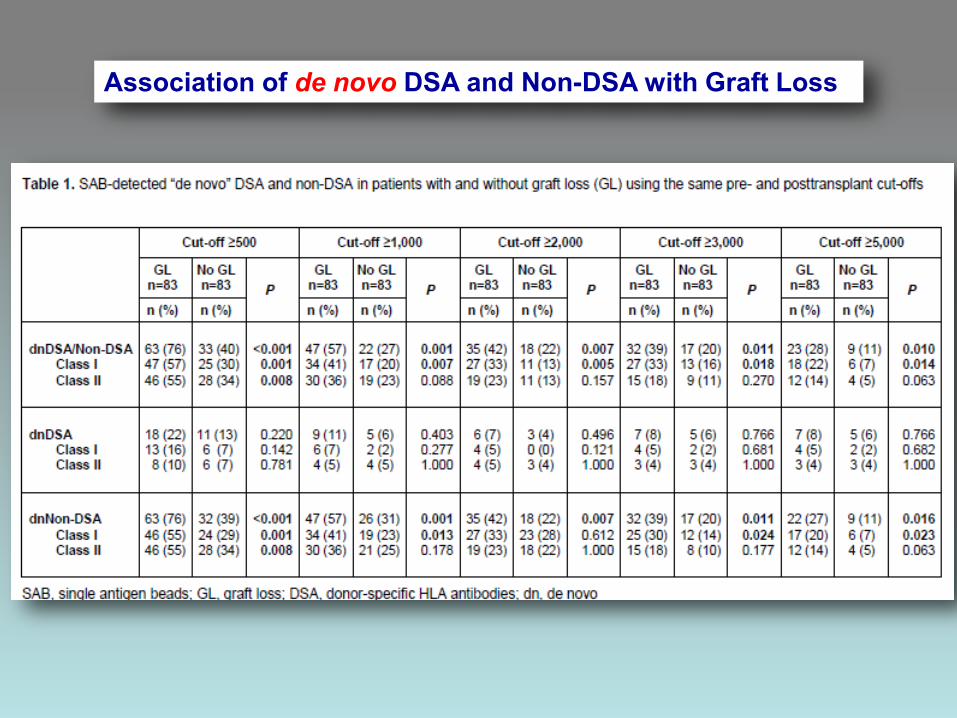
Association of de novo DSA and Non-DSA with Graft Loss
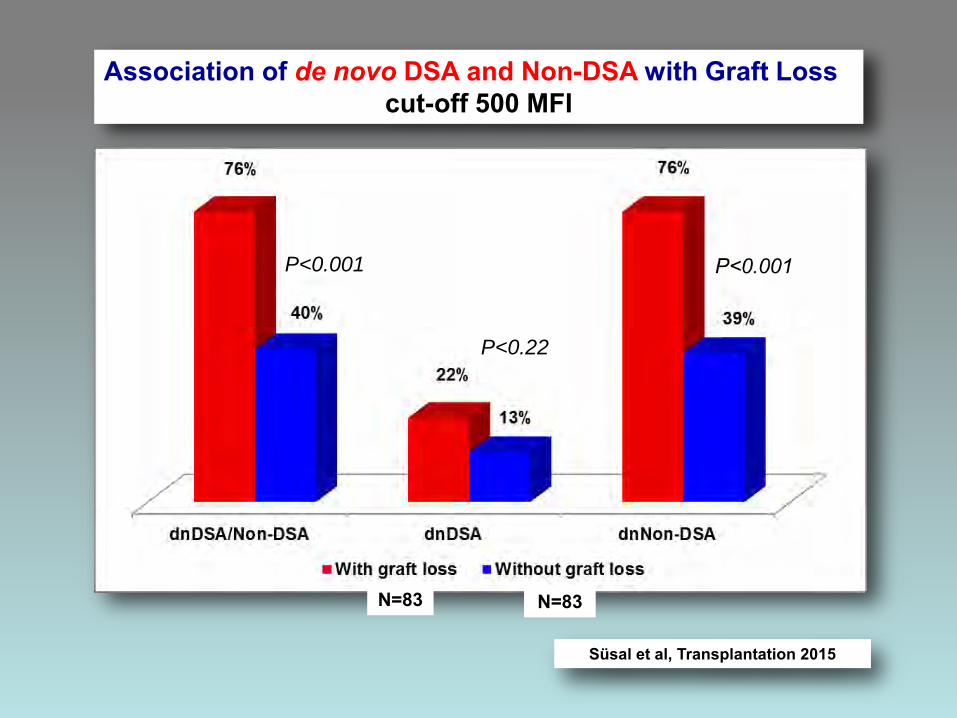
Association of de novo DSA and Non-DSA with Graft Loss cut-off 500 MFI
P<0.001
P<0.22
Süsal et al, Transplantation 2015
N=83 N=83
P<0.001
P<0.22
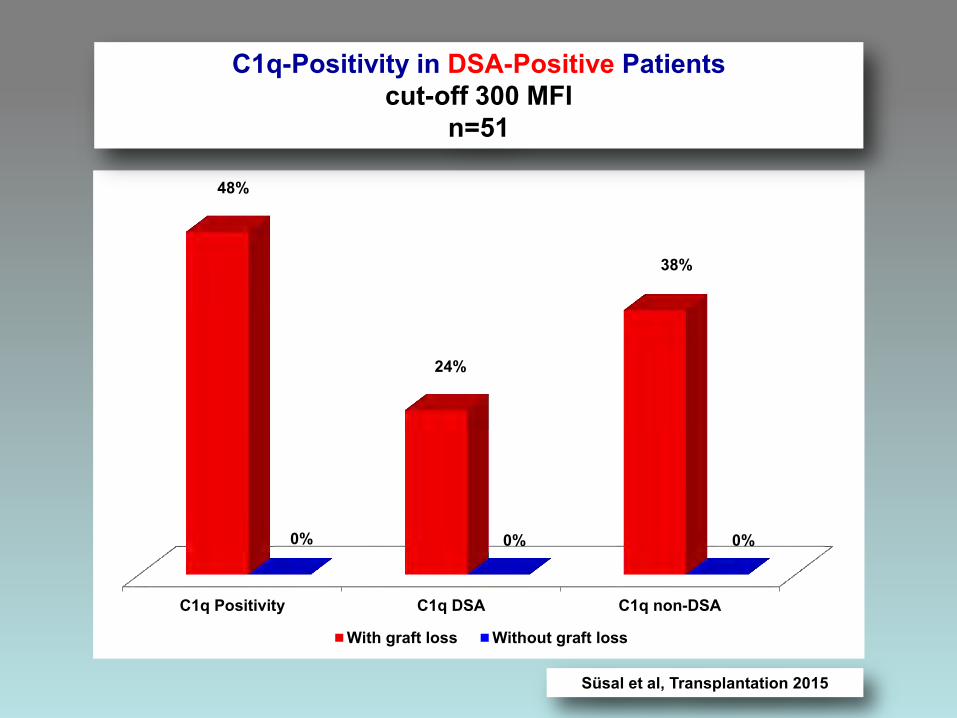
C1q Positivity C1q DSA C1q non-DSA
48%
24%
38%
0% 0% 0%
With graft loss Without graft loss
C1q-Positivity in DSA-Positive Patients cut-off 300 MFI
n=51
Süsal et al, Transplantation 2015
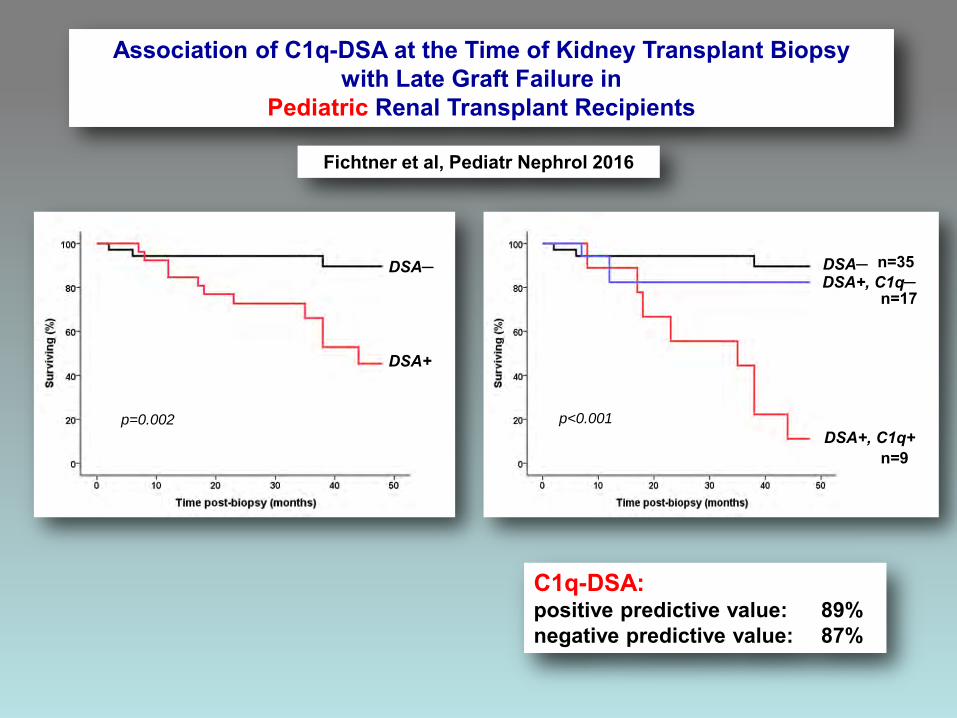
Association of C1q-DSA at the Time of Kidney Transplant Biopsy with Late Graft Failure in
Pediatric Renal Transplant Recipients
DSA─
DSA+
p=0.002
DSA─ DSA+, C1q─
DSA+, C1q+ p<0.001
Fichtner et al, Pediatr Nephrol 2016
n=35
n=17
n=9
C1q-DSA: positive predictive value: 89% negative predictive value: 87%
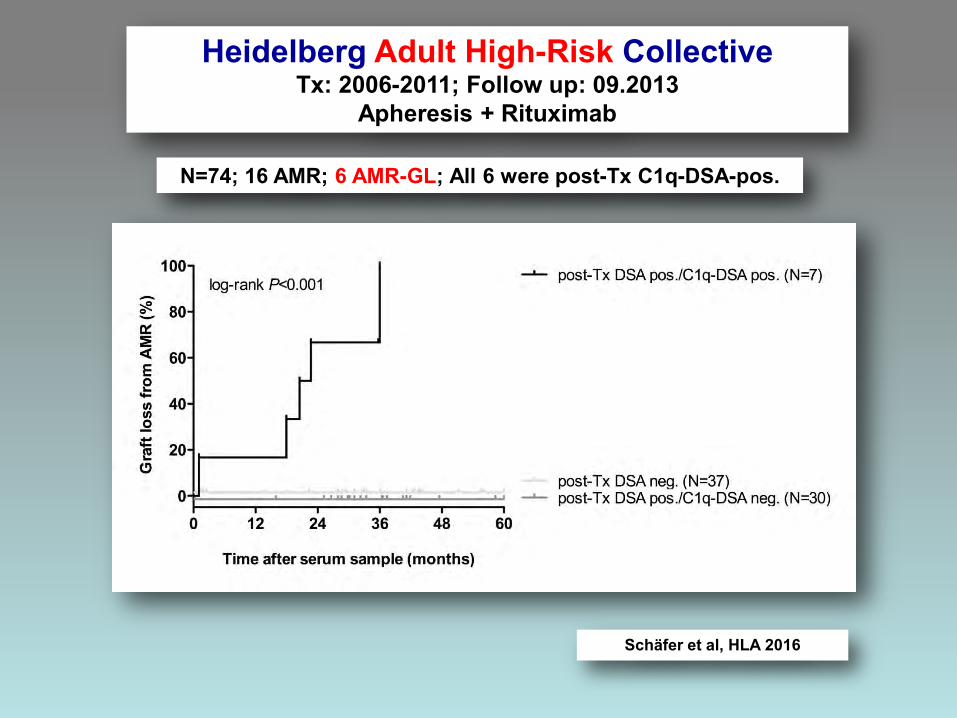
Heidelberg Adult High-Risk Collective Tx: 2006-2011; Follow up: 09.2013
Apheresis + Rituximab
Schäfer et al, HLA 2016
N=74; 16 AMR; 6 AMR-GL; All 6 were post-Tx C1q-DSA-pos.
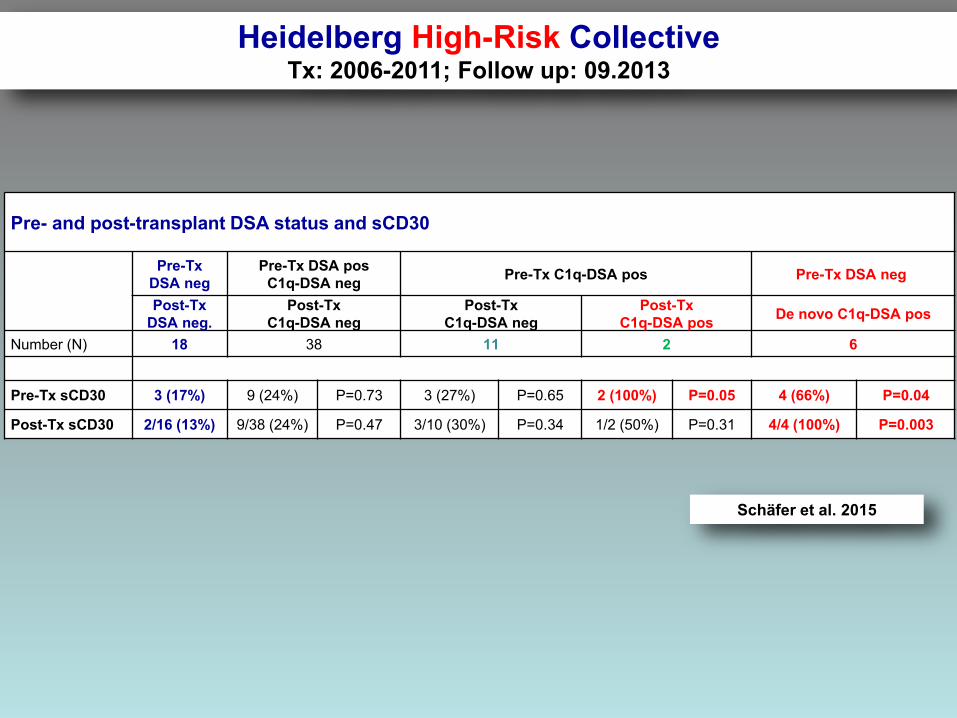
Pre- and post-transplant DSA status and sCD30
Pre-Tx DSA neg
Pre-Tx DSA pos C1q-DSA neg Pre-Tx C1q-DSA pos Pre-Tx DSA neg
Post-Tx DSA neg.
Post-Tx C1q-DSA neg
Post-Tx C1q-DSA neg
Post-Tx C1q-DSA pos De novo C1q-DSA pos
Number (N) 18 38 11 2 6
Pre-Tx sCD30 3 (17%) 9 (24%) P=0.73 3 (27%) P=0.65 2 (100%) P=0.05 4 (66%) P=0.04
Post-Tx sCD30 2/16 (13%) 9/38 (24%) P=0.47 3/10 (30%) P=0.34 1/2 (50%) P=0.31 4/4 (100%) P=0.003
Heidelberg High-Risk Collective Tx: 2006-2011; Follow up: 09.2013
Schäfer et al. 2015
Donor-specific antibodies require preactivated immune system to harm renal transplant
Caner Süsal1, Bernd Döhler1, Andrea Ruhenstroth1, Christian Morath2, Antonij Slavcev3, Thomas
Fehr4, Eric Wagner5, Bernd Krüger6, Margaret Rees7, Sanja Balen8, Stela Živčić-Ćosić8, Douglas
J. Norman9, Dirk Kuypers10, Marie-Paule Emonds11, Przemyslaw Pisarski12, Claudia
Bösmüller13, Rolf Weimer14, Joannis Mytilineos15 Sabine Scherer1, Thuong H. Tran1, Petra
Gombos1, Peter Schemmer16, Martin Zeier2, and Gerhard Opelz1
A Collaborative Transplant Study Report
EBioMedicine 2016
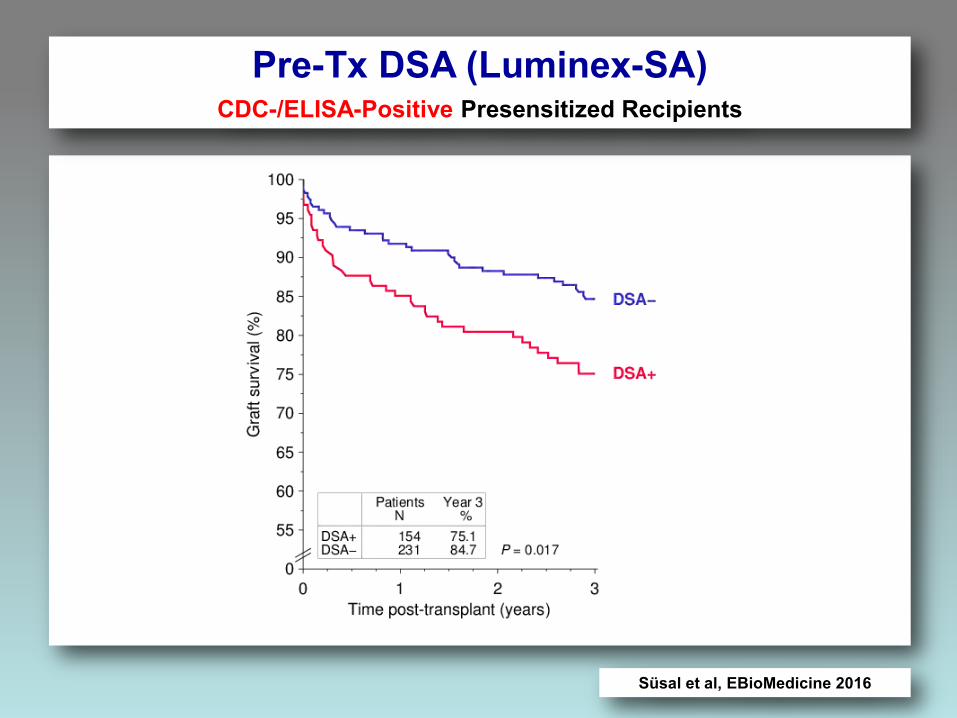
Pre-Tx DSA (Luminex-SA) CDC-/ELISA-Positive Presensitized Recipients
Süsal et al, EBioMedicine 2016
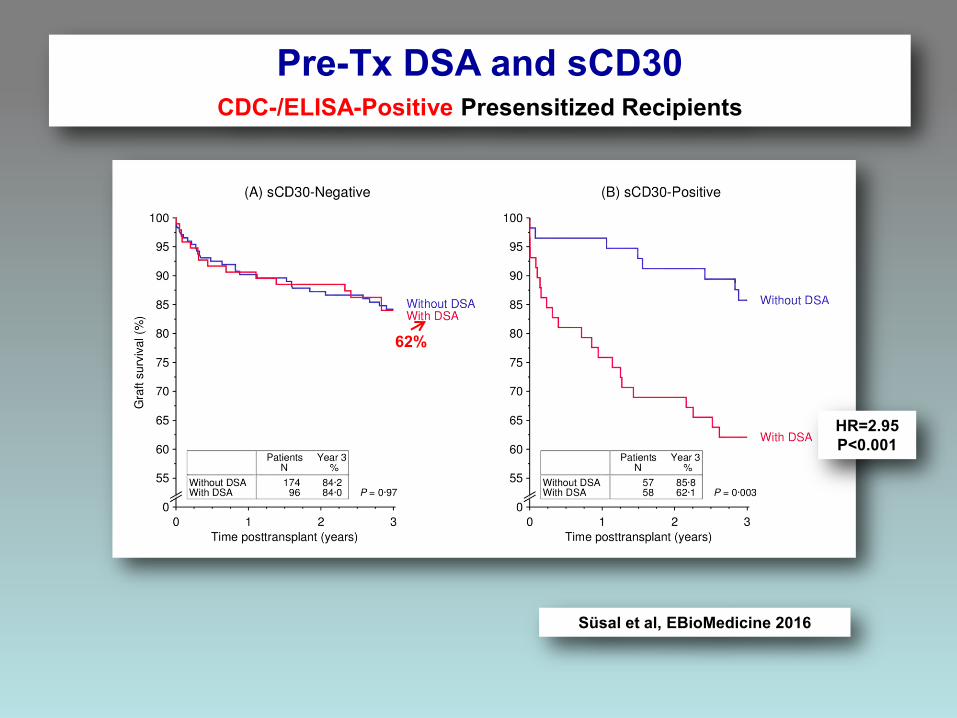
HR=2.95 P<0.001
62%
Süsal et al, EBioMedicine 2016
Pre-Tx DSA and sCD30 CDC-/ELISA-Positive Presensitized Recipients
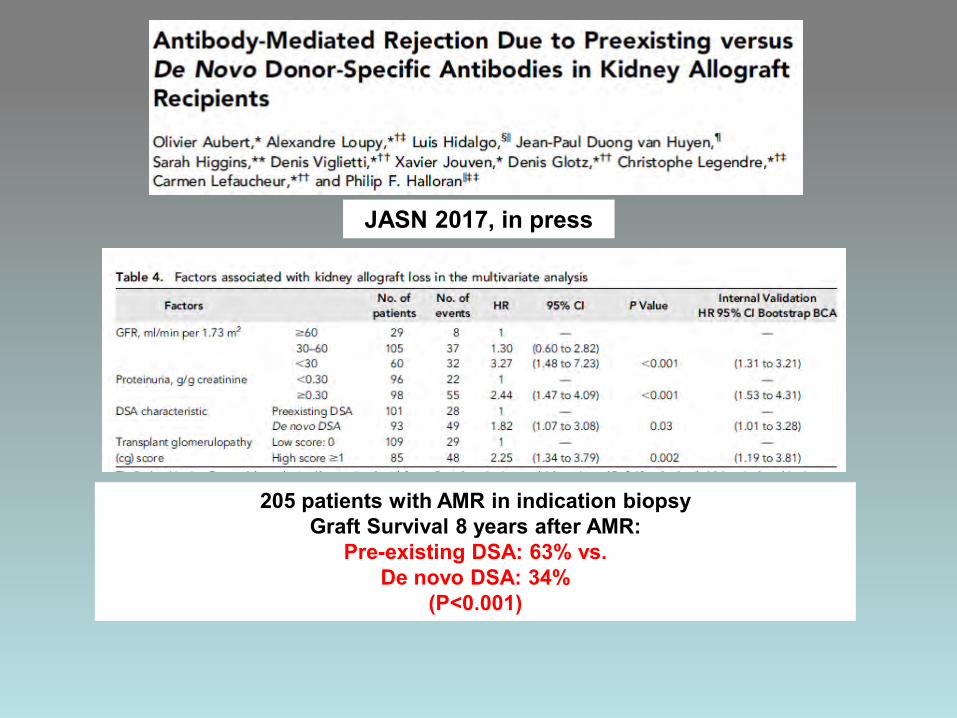
205 patients with AMR in indication biopsy Graft Survival 8 years after AMR:
Pre-existing DSA: 63% vs. De novo DSA: 34%
(P<0.001)
JASN 2017, in press

www.efi2017.org
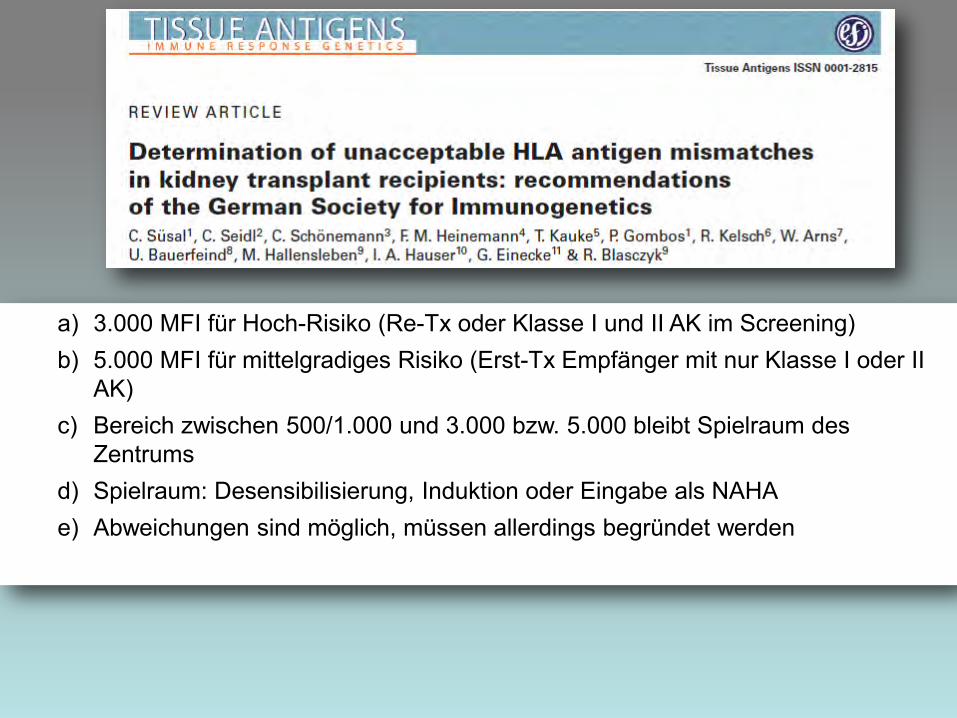
a) 3.000 MFI für Hoch-Risiko (Re-Tx oder Klasse I und II AK im Screening) b) 5.000 MFI für mittelgradiges Risiko (Erst-Tx Empfänger mit nur Klasse I oder II
AK) c) Bereich zwischen 500/1.000 und 3.000 bzw. 5.000 bleibt Spielraum des
Zentrums d) Spielraum: Desensibilisierung, Induktion oder Eingabe als NAHA e) Abweichungen sind möglich, müssen allerdings begründet werden
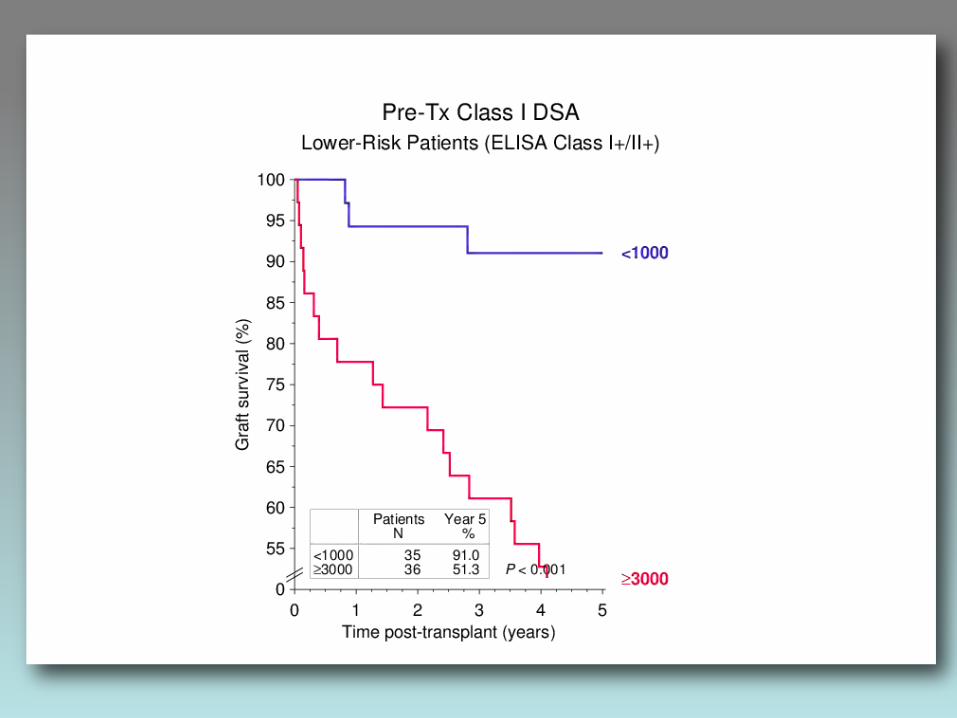
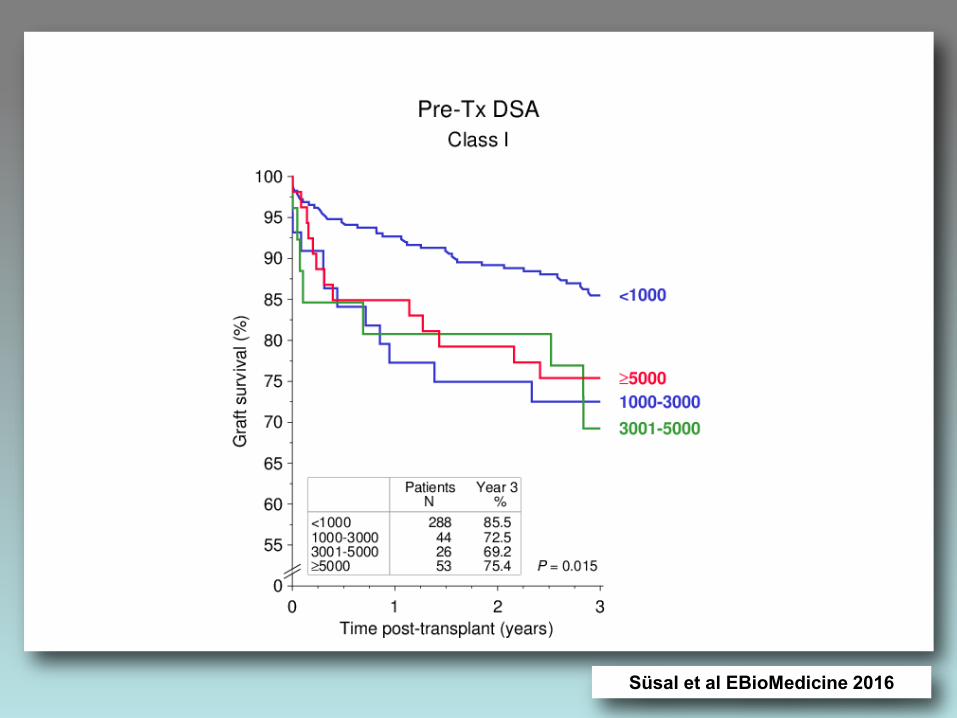
Süsal et al EBioMedicine 2016
Top Related