Influencia de determinantes sociales en promoción y prevención de salud

of 12
-
Upload
psychforall -
Category
Documents
-
view
228 -
download
0
Transcript of Influencia de determinantes sociales en promoción y prevención de salud
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
1/12
The influence of social determinants on the use of
prevention and health promotion services: Results of a
systematic literature review
Der Einfluss sozialer Determinanten auf die Inanspruchnahme vonManahmen der Prvention und Gesundheitsfrderung in Deutschland:Ergebnisse einer systematischen Literaturrecherche
Abstract
Background: The following analysis aims to determine whether differ-ences in the use of prevention and health promotion services in Germany
Christian Janen1
Stefanie Sauter2
can be attributed to health inequality between different social statusChristoph Kowalski2groups measured by education, occupation and income and where
certain improvements can be made in health promotion and preventionefforts and research to reduce those differences. 1 Department of Applied Social
Sciences, Munich UniversityMethods: A systematic literature search was conducted using MedPilotto identify relevant articles published between 1998 and 2010 in the of Applied Sciences, Munich,
GermanyMedline, Medizinische Gesundheit, CC Med, Deutsches rzteblatt andSozialmedizin (SOMED) databases, the Hogrefe, Karger, Krause and 2 Institute for Medical
Sociology, Health ServicesPachermegg and Thieme publisher databases, the Cochrane Databaseof Systematic Reviews (CDSR), the Cochrane Database of Abstracts of Research and RehabilitationReviews of Effectiveness (DARE), and the Cochrane Central Register ofControlled Trials.
Science, Faculty of HumanScience and Faculty ofMedicine, University of
Cologne, Cologne, Germany
Results: A total of 23 empirical studies on the topic of prevention,
health prevention and social inequality met the criteria for inclusionin the review. 20 of the 23 reviewed studies provided relatively clearevidence of a significant association between higher social status andgreater use of prevention and health promotion services. According tothe reviewed studies, gender tends to have a greater effect on the useof prevention and health promotion services than characteristics ofvertical social inequality. No studies were found dealing with tertiaryprevention or using qualitative methods to explore their researchquestions.Conclusions: Overall, the review shows that there is sufficient evidencefor the relationship between social status and the use of preventionand health promotion services and that this association is both signifi-
cant and relevant. There are, however, a few blind spots in researchon this topic, such as a lack of studies on tertiary prevention, especiallywith regards to prevention and health promotion services use amongmen, as well as general studies on health promotion among men andwomen. There is also a lack of published intervention studies demon-strating how to better reach the socially disadvantaged.
Keywords: social determinants, education, occupation, income,prevention, health promotion, systematic review
Zusammenfassung
Hintergrund: Der vorliegende Beitrag untersucht den Einfluss sozialer
Determinanten auf die Inanspruchnahme prventiver und gesundheits-frderlicher Leistungen in Deutschland. Damit soll ein Beitrag zur Be-antwortung der Frage geliefert werden, warum Morbiditt und Mortalittso stark nach sozialen Statusmerkmalen (Bildung, Beruf und Einkom-
1/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Review ArticleOPEN ACCESSSpecial issue: Health care utilization in Germany: The NWInresearch network
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
2/12
men) eines Menschen differieren und wo im Bereich der Gesundheits-frderung und Prvention mgliche Verbesserungs- und notwendigeForschungspotentiale bestehen.Methoden: Hierzu wurde mittels Medpilot eine systematische Literatur-recherche fr den Zeitraum 19982010 in den Datenbanken Medline,
Medizinische Gesundheit, CC Med, Deutsches rzteblatt, Sozialmedizin
(SOMED), Hogrefe Verlag, Karger Verlag, Krause und PachermeggPublikations-Datenbank, Thieme Verlag, Cochrane Database of Syste-matic Rrviews (CDSR), Cochrane Database of Abstracts of Reviews ofEffectiveness (DARE), Cochrane Central Register of Controlled Trialsnach empirischen Untersuchungen zu dieser Thematik durchgefhrt.Ergebnisse: Zusammenfassend lsst sich sagen, dass 20 der 23 sogefundenen empirischen Untersuchungen eindeutig signifikante Effektehinsichtlich einer Zunahme der Inanspruchnahme prventiver odergesundheitsfrderlicher Leistungen mit zunehmendem sozialen Status,drei Studien zeigten keine eindeutigen Ergebnisse. Es zeigte sich, dassdas Geschlecht berwiegend grere Effektstrken hinsichtlich der In-anspruchnahme von Manahmen der Prvention und Gesundheitsfr-
derung zeigt als Merkmale der vertikalen sozialen Ungleichheit. Eswurden berwiegend Manahmen der Sekundrprvention untersuchtund es konnte keine Studie gefunden werden, welche sich mit Tertir-prvention beschftigt oder eine qualitative Methodik bei der Untersu-chung der Forschungsfrage angewandt hat.Diskussion: Insgesamt kann festgestellt werden, dass der Zusammen-hang zwischen einem eher niedrigerem sozialen Status und der ehergeringeren Inanspruchnahme gesundheitsfrderlicher und prventiverLeistungen als hinreichend belegt, signifikant und relevant angesehenwerden. Trotzdemgibt es noch einige blinde Flecken in der Forschungs-landschaft in diesem Gebiet: So fehlen Studien im Bereich der Tertir-Prvention, speziell fr den Bereich der Prvention und Gesundheitsfr-derung bei Mnnern sowie allgemein Studien im Bereich der Gesund-
heitsfrderung bei Mnnern und Frauen. Es fehlt zudem an publiziertenInterventionsstudien, die zeigen, wie sozial Benachteiligte besser erreichtwerden knnen.
Schlsselwrter: soziale Determinanten, Bildung, Beruf, Einkommen,Prvention, Gesundheitsfrderung, systematische Literaturrecherche
Introduction
This review investigates the impact of social factors onthe use of prevention and health promotion services inGermany and, in doing so, attempts to help answer the
questions as to why there are such strong differences inmorbidity and mortality based on individuals social statuscharacteristics (e. g. education, occupation, income) andwhere certain improvements can be made in health pro-motion and prevention efforts and research to reducethose differences.In social epidemiology research, social inequalityprimarily encompasses horizontal inequalities (age,gender, marital status, nationality) and vertical inequal-ities (occupation, education, income). This study focuseson vertical inequalities that is, on the differences in in-dividuals education, occupation and income character-
istics. (For in-depth studies analyzing horizontal inequality,see [6], [53], [38], [43]). These characteristics are alsoreferred to as socioeconomic characteristics and are oftencombined to an index in order to describe an individuals
social status [20], [36]. In this review, the terms socialstatus and social class are used synonymously since al-though the concept of social class differs in theoreticalmeaning from that of social status, it can also be seenas a categorized form of social status [18]. In addition to
the individual indicators education, occupation, and in-come, each with their various limitations and strengths(for an overview, see [14], [36]), this review also exploresgender-related differences in services use, since signifi-cant differences between women and men have beenfound in previous research.Social inequality leads to unequal distribution of healthchances in populations. For example, the mean differencein mortality between members of the upper and lowersocial classes can range from four to ten years [46].Already in the early 1970s in Great Britain, Marmotidentified a typical phenomenon of modern industrialized
countries: a social class gradient in health, such that thehigher the social position, the better the health of a per-son [35]. This gradient, which he termed a status syn-drome, means that not only the lowest social class is at
2/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
3/12
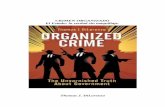
Figure 1: A complete recursive model of social and health inequality (based on [36] and modified by the authors)
a disadvantage or that the poorest of the poor is affected.Rather, it implies that the gradient in health, in the formof an inverse gradient, cuts across society as a whole[33], [34], [46].Other groundbreaking studies conducted by [4], [15], and[23] in the U.S. observed that the distribution of relevantchronic diseases and the risk for premature death followa social gradient as well: the higher the social status ofa population group, the lower the groups morbidity andmortality. Evidence for this gradient has been providedin all industrialized countries, in which such studies havebeen conducted [9], [31], [33], [46]. Even though the size
of the inequalities between classes may vary, internation-al research has shown that in all European countriespremature death rates become increasingly higher as wemove down the social status scale. The fact that thereare indications that these inequalities are increasing [32]shows just how relevant they are today. The finding thatthe mean difference in life expectancy between membersof the highest income group and lowest income group inGermany is 8.4 years for women and 10.8 years for men[27] clearly illustrates how relevant this issue is for healthpolicy and science in Germany in particular.Those most impacted by social status-based health in-
equalities are young children and middle-aged adults.Fewer inequalities are observed during adolescence andold age [26]. There are also differences between genders.Mens health seems to be more impacted by social status measured at least in terms of level of education, occu-pation and income than womens health [5]. Noticeabledifferences have also been observed in the magnitudeof social inequality in health between countries, evenwithin relatively homogeneous regions, such as Europeancountries [32]. For instance, whereas social disparitieshave been found to be lower in Southern Europeancountries, these disparities are greater in EasternEuropean countries. Disparities have also been foundwith regard to different diseases: Among low statusgroups, there are considerably higher (twice as high orhigher) risks for heart attack, stroke, chronic liver disease,
angina pectoris (in women), diabetes mellitus (in women),chronic bronchitis (in men) and osteoporosis (in men).These groups are also at a greater risk (i.e., have at leasta significantly increased likelihood) for: hypertension anddepression; high cholesterol, chronic bronchitis, bronchialasthma, arthrosis and osteoporosis (in women); andangina pectoris, heart failure, diabetes mellitus, chronicrenal failure and arthritis (in men). Less pronounced socialdisparities can be also observed for most types of cancer,gastrointestinal diseases and neurological disorders. Alimited number of diseases are more prevalent in higherthan in lower social classes. These include allergies and
breast cancer [46].In Germany, medical sociological research on this topicgot a late start because restrictive data regulations hadlimited the amount of available data and because thefield of medical sociology did not catch up with interna-tional developments until late. Since 2000, however, thetopic has been examined in more depth and detail in ex-tensive collective volumes of articles [17], [36], [40], [57].Although various sociological models can be drawn uponto explain social differences in morbidity and mortality[19], Mielcks model for explaining health inequality [36]is probably the most comprehensive (see Figure 1). Ac-
cording to the model, less knowledge (e.g., obtainedthrough schooling or professional training), less power(e.g., position in the occupational hierarchy or controlover the work content, intensity and processes of others),less prestige (e.g., how society regards the occupation)and less money (income and wealth) lead to greaterhealth burdens at ones place of residence or work, tofewer coping resources, to poorer medical care and toless healthy behavior. This, in turn, increases the risk forillness and premature death. At the same time, themodel identifies other direct pathways between socialand health inequality, such that illness can lead to a socialdowngrade and such that there are also direct relation-ships between physical and social characteristics (e.g.,the parameters of the immune system or blood pressure).Despite this, not all dimensions of social inequality are
3/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
4/12
of course influenced by dimensions of health inequalityand vice versa.This review aims to determine whether differences in theuse of prevention and health promotion services in Ger-many can be attributed to health inequality between dif-ferent social status groups. So far, no other systematic
reviews have been conducted to determine if any suchassociation exists despite the fact that there have beenmany complaints about the tendency of prevention effortsto focus on the middle class.In the following section, a brief description of the Germanhealth care system will be given. Only an overview of thesystem will be provided due to its complexity and espe-cially given that the system is subject to constant changeowing to current medical and economic developmentsas well as associated political decisions and legislativeamendments. Following the overview, the results of thesystematic review will be presented. The findings of the
reviewed empirical studies on socioeconomic differencesin the use of prevention and health promotion serviceswill be synopsized in tables and briefly analyzed in con-sideration of systematic viewpoints. The final section willdiscuss the reviews findings as well as the limitationsand strengths of the review methods.
Fundamental characteristics of theGerman health care system with afocus on health promotion andprevention
In Germany, the health care system forms the third pillarof the social welfare system alongside pension and un-employment insurance. The main tasks of the Germanhealth care system include health maintenance andpromotion as well as the prevention and treatment of ill-ness. The states job is to provide the proper regulatoryframework facilitating the exchange, negotiation and co-ordination processes needed for respective institutionsto allocate funds [45]. Compared to other countries,Germany has an above-average number of physicians,dentists, physical therapists, nursing staff and hospital
beds. Approximately 4.3 million people nearly 9% ofthe nations workforce were reportedly either directlyor indirectly employed in the German health care sector[1].Funding for the German health care system is primarilyprovided through insurance contributions. Nine out of tenGerman citizens approx. 70 million people are mem-bers of the countrys nearly 150 statutory health insur-ance funds. Only ten million are coveredby private healthinsurance funds. The cornerstone of the German statutoryhealth insurance system is the solidarity principle. Accord-ing to this principle, insurance contributions are basedon an insured individuals level of income rather than the
individuals gender, age or risk of illness. In the case ofprivate health insurance, premiums depend on thenumber of services covered by the particular insurance
policy and the overall health status, gender and age atentry of the policyholder [37].Inpatient care in Germany is delivered in preventive,curative and rehabilitation health facilities. Funding forboth hospitals and rehabilitation facilities is provided bypublic, private or non-profit sources. The increasing focus
of hospitals on economic efficiency is placing new de-mands on nursing staff, other therapeutic professionsand physicians. Although prevention strategies are be-coming just as important as health promotion strategies,overall expenditures for prevention, health promotion,health protection, health information and education,screening and health care services make up a mere0.53% of the nations health budget [55]. Preventionand health promotion are interventions that achievecompression of morbidity. In Germany, the main parti-cipants in these efforts are the Public Health Service, thestate business supervisory authorities, institutions
providing occupational accident insurance and those re-sponsible for occupational health and safety, as well asthe health insurance funds.According to the WHO [58], the term health promotionrefers to a set of strategies and methods implementedat different societal levels in an attempt to increasepeoples health resources and potentials. Types of healthpromotion measures include: 1) those aimed at modifyingand promoting individual health behavior and 2) thoseaimed at creating health-promoting environments (oftenreferred to as the "settings approach) through, for ex-ample, organizational development, community develop-ment, policy development or health-related education
measures. According to [50], prevention (Latinpraeveniere: to come before), unlike health promotion,involves activities aimed at avoiding, lessening the likeli-hood of or delaying harm to a persons health. Preventionmeasures can focus on the behavior of individuals orgroups (behavioral risk prevention) or can be geared to-ward modifying the biological, social or technical environ-ment (environmental risk prevention).As illustrated in Table 1 based on Leppin [29], preventionactivities can also take place on three different levels(primary, secondary, and tertiary) depending on the time,objective and target of the preventive intervention.
The terms prevention and health promotion oftenused to be used synonymously. Recently, however, a dif-ferentiated view has come to be taken. The fundamentaldistinctions made between health promotion measuresand prevention measures can be summarized as follows(Table 2): (Please note that this way of differentiatingbetween prevention and health promotion is an ideal typeand is, by all means, open to debate.) While health pro-motion measures tend to focus more on resources (e.g.,health loci of control or social support), preventionmeasures are geared toward health burdens (e.g., vaccin-ations against certain diseases such as measles, mumpsor rubella). Health promotion interventions tend to bedesigned and conducted by public health specialistswithout a specific problem, risk factor or disease in mind;that is, they usually promote health in general. Prevention
4/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
5/12
Table 1: The differences between primary, secondary, and tertiary prevention based on the time, goal and target of the intervention
(according to [29])
Table 2: Criteria for distinguishing health promotion from prevention
interventions, on the other hand, are performed by med-ical experts to counter specificdiseases (see, for instance,the vaccination example given in the previous sentence).Health promotion measures encourage patients and cit-izens to play an active role in their own health. In the caseof preventive measures, however, they play a morepassive role when being protected from diseases.
Methods used in the systematicreview
Already in 2009, a systematic literature review was con-ducted to determine the extent to which social statuscharacteristics are associated with the use of serviceswithin the entire German health care system [18].32 studies were identified as having been publishedbetween 2000 and 2008. According to the results ofthese studies, the overall level of health care provided toall social status groups in Germany is relatively high, andhardly any differences were found in the curative or re-habilitative care received across status groups. Therewere, however, marked differences with regard to thegroups use of prevention and health promotion services,
suggesting that prevention and health promotion pro-grams aimed at influencing individuals use of such ser-vices, providing them with relevant health and diseaseinformation and impacting the way this information is
used must be tailored to less privileged social statusgroups in order to be at least somewhat better able toreduce existing health inequalities in the future. After all,a socially equitable health care system should be able toclaim, in future, that it continues to contribute to the re-duction of health inequality [18]. The findings of the 2009review indicate that certain changes need be made tothe German health care system. However, when makingthese changes, care should be taken to ensure that thesame level of high-quality care continues to be providedto all social groups.In light of the findings of the previous review, the present
review only focuses on the use of prevention and healthpromotion services using search terms only in regard tothe mentioned topics while the first review and its searchterms were in regard to the medical system in general.On March 22, 2011, a new literature search was conduct-ed using MedPilot to identify relevant articles publishedbetween 1998 and 2010 in the Medline, Medizinische
Gesundheit, CC Med, Deutsches rzteblatt and Sozialme-dizin (SOMED) databases, the Hogrefe, Karger, Krauseand Pachermegg and Thieme publisher databases, theCochrane Database of Systematic Reviews (CDSR), theCochrane Database of Abstracts of Reviews of Effective-
ness (DARE), and the Cochrane Central Register of Con-trolled Trials. The following combinations of search termswere used:
5/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
6/12
gesundheit* AND deutsch* AND (einkommen* ORbildung* OR beruf* OR geschlecht*) AND (prvent* ORscreening* OR vorsorge* OR gesundheitsfrderung* ORfrherkennung*) AND (inanspruchnahme* OR nutzung*OR besuch*)OR
health* AND german* AND (income* OR education* ORprofession* OR occupation* OR gender* OR sex*) AND(prevent* OR "early detect*" OR "health promotion" ORscreening*) AND (utili?ation* OR use* OR usage*)
Retrieved papers met the inclusion criteria if they werepublished in English or German and reported empiricalfindings.
Results
After excluding duplicate hits, a total of 1,303 articleswere independently screened by two of the authors. Fol-lowing the same procedure used in the 2009 review, thearticles were screened to identify empirical studies pub-lished in either English or German. In the end, a total of23 empirical studies on the topic of prevention, healthprevention and social inequality met the criteria for in-clusion in the review. Table 3 presents the results of thesystematic review. Only study findings pertaining to edu-cation, occupation, income and gender are listed. In manyof the studies, additional factors were also found to beassociated with prevention and health promotion servicesuse.
As evidenced by the findings presented in Table 3, 20 ofthe 23 reviewed studies provided relatively clear evidenceof a significant association between higher social statusand greater use of prevention and health promotion ser-vices. (The results of the other three studies were not asconclusive as the others.) Evidence of this associationwas provided for almost the whole of Germany. Whereasonly one study was conducted exclusively with men, threewere conducted only with women. The majority of thestudies examined secondary prevention measures. Nostudies were found dealing with tertiary prevention orusing qualitative methods to explore their research
questions.
Discussion
The aim of this study was to examine social inequality inprevention and health promotion in Germany through asystematic review of literature. The choice of search termsplayed a major role in the review process. On the onehand, they had to be broad enough in order to identify allstudies on the reviews topic; on the other hand, they hadto be narrow enough to distinguish between relevant andirrelevant studies. Nevertheless, it is possible that some
studies (e.g., unpublished studies) may not have beenincluded. This should be taken into consideration wheninterpreting the reviews results.
Overall, the review shows that there is sufficient evidencefor the relationship between social status and the use ofprevention and health promotion services and that thisassociation is both significant and relevant. There are,however, a few blind spots in research on this topic,such as a lack of studies on tertiary prevention, especially
with regards to prevention and health promotion servicesuse among men, as well as general studies on healthpromotion among men and women. There is also a lackof published intervention studies demonstrating how tobetter reach the socially disadvantaged. Recently, how-ever, there have been concerted efforts in this area (e.g.,by the German Federal Ministry of Education and Re-search). Studies on tertiary prevention measures may nothave been identified due to the terms chosen for the lit-erature search. It is possible that these types of measuresare subsumed under the term rehabilitation. Accordingto the reviewed studies, gender tends to have a greater
effect on the use of prevention and health promotionservices than characteristics of vertical social inequality.This is in part due to the greater public awareness ofpreventive measures for women (e.g., breast vs. prostatecancer early detection) and does not take into considera-tion the degree to which the offered measures are neces-sary and under which circumstances they were used.According to the Andersen model, all of the determinantsof services use examined in this review (i.e., education,occupation, income and gender) may be categorized asindividual factors [2], [3]. Contextual factors have onlybeen examined in a few studies, the reason for this mostoften being that specific data on individual characteristics
are not available. For this reason, studies such as thatof [44] use data on average income in individual regionsand not on individual or household income. This particulartype of ecological analysis makes it difficult to derivecausal inferences, particularly since the individual char-acteristic is not (cannot be) controlled for. Though in someStudies (e.g. [11]) some inividual characteristics arecontrolled for (eg. school type attended) but other relevantvariables (e.g. class size or financial resources of theschool), are not. Although "type of school attended is anindividual characteristic for which data is collected fromindividual people, it must be assumed that schools con-
stitute important contexts of influence on the use of pre-vention andhealth promotion services and that the typeof school attended variable along with other variables,such as class size, financial resources, teachers qualifi-cations is just a relevant characteristic of these con-texts.A noteworthy outcome of this review is the wide range ofstudies identified through the selected search strategy.Not only did the strategy identify studies on cancerscreening and vaccination prevalence; it also identifiedone on the use of sunscreen. A (survey) study focusingonly on physical activity was also found (and not excluded)[7]. A different search strategy probably would haveidentified numerous other studies exploring physicalactivity, though not explicitly within context of prevention
6/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
7/12
Table 3: A breakdown of the reviewed studies by area of interest, target population, region of study, and findings
7/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
8/12
(Continued)Table 3: A breakdown of the reviewed studies by area of interest, target population, region of study, and findings
8/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
9/12
(Continued)Table 3: A breakdown of the reviewed studies by area of interest, target population, region of study, and findings
9/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
-
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
10/12
and health promotion. This example reveals one problemwith the methods used in this review.Another main limitation of the selected review methods,according to the authors, involves publication bias; thatis, only significant results tend to be published. This maymean that studies finding no differences by social status
were not published and therefore not identified duringthis review. As another form of publication bias, manypublishers tend to prefer quantitative methods overqualitative methods. As a result, this review tends tocapture only quantitative results. In addition, the searchterms used in this review may have been too narrow,which means that papers which cover aspects of (tertiary)prevention, such as patient self-help groups or rehabilita-tion, but did not use one of the terms in our searchstrategy, were not identified. Another important limitationto this review is the time lag involved in empirical studiesobserving changes occurring in real life. Often, the time
between planning a study and publishing its results canbe months or even years. The question then needs to beraised as to the extent to which the methods in this reviewprovide an accurate picture of the current state of healthcare in Germany. The review provides an update of themore general review from 2009 [18], confirming its find-ings. Including a number of additional study results, thereis now a convincing body of literature that shows an as-sociation between social status and prevention/healthpromotion.Despite its limitations, the review also has certainstrengths. The analysis and discussion have a clear em-pirical basis. The design of the methods used in the re-
view is also clear, understandable and for the most partobjective. The results of the review could also serve as abaseline measurement for future comparison. In tenyears, for example, a follow-up study could be conductedto determine whether health careinequalities have grown,remained the same or even been reduced.Health care expenditures will continue to rise in Germanyin the future. The countrys aging population, coupledwith its declining birth rate, is throwing the solidaritysystem more and more out of balance as older peopleoften create higher expenditures yet contribute less tothe health insurance system. The result is increasing
health care costs that will have to be borne by a decreas-ing number of employed citizens unless extensive struc-tural reforms are implemented. In light of the expectedincrease in the number of elderly and dependent citizensover the coming years, one of Germanys main tasks willbe to expand existing prevention and outpatient struc-tures. Additionally, health promotion and prevention ser-vices for the elderly will gain in importance alongside careand rehabilitation. A socially equitable health care systemshould be able to claim, in future, that it continues tocontribute to the reduction of health inequality [18].
Notes
Acknowledgements
The writing of this article was carried out as part of thescientific network project Utilization of health-related
services in Germany theoretical approaches, methodsand empirical results in medical sociology (NWIN). Theproject is funded by the Deutsche Forschungsgemein-schaft (German Research Foundation, grant no.: JA1849/1-1).
Competing interests
The authors declare that they have no competing in-terests.
References1. Afentakis A, Bhm K. Beschftigteim Gesundheitswesen. Berlin:
RKI; 2009. (Gesundheitsberichterstattung des Bundes; 46).Available from: http://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=12049&p_sprache=D
2. Andersen RM,Davidson PL.Improvingaccess to care in America:individual and contextual indicators. In: Andersen RM, Rice TH,Kominski GF, eds. Changing the U.S. health care system: keyissues in health services, policy, and management. SanFrancisco, CA: Jossey-Bass; 2001. p. 3-30.
3. Andersen RM.Nationalhealth surveys andthe behavioral modelof health services use. Med Care. 2008 Jul;46(7):647-53. DOI:10.1097/MLR.0b013e31817a835d
4. Antonovsky A. Social class, life expectancy and overall mortality.Milbank Mem Fund Q. 1967 Apr;45(2):31-73. DOI:10.2307/3348839
5. Arber S, Thomas H. From women's health to a gender analysisof health. In: Cockerham WC, ed. The Blackwell companion tomedical sociology. Oxford: Blackwell; 2001. DOI:10.1002/9780470996447.ch5
6. Babitsch B. Soziale Ungleichheit, Geschlecht und Gesundheit.Bern: Huber; 2005.
7. Becker S, Huy C, Brinkhoff KP, Gomolinsky U, Klein T, Thiel A,Zimmermann-Stenzel M. "Ein aktives Leben leben" - Sport,Bewegung und Gesundheit im mittleren und hherenErwachsenenalter. Konzeption, Datenerhebung und erste
Ergebnisse eines reprsentativen Basis-Survey fr die 50- bis70-jhrige Baden-Wrttembergische Wohnbevlkerung ["Livingan active life"--sports, exercise and health in middle-aged andolder adults. An empirical database on physical activity, healthbehavior and lifestyle in the 50- to 70-year-old residentialpopulation of Baden-Wuerttemberg]. Gesundheitswesen. 2007Jul;69(7):401-7. DOI: 10.1055/s-2007-985127
8. Bergmann E, Kalcklsch M, Tiemann F. Inanspruchnahme desGesundheitswesens. Erste Ergebnisse des telefonischenGesundheitssurveys 2003 [Public health care utilisation. Initialresults of the Telephone Health Survey 2003].Bundesgesundheitsblatt GesundheitsforschungGesundheitsschutz. 2005 Dec;48(12):1365-73. DOI:10.1007/s00103-005-1167-6
9. Berkman LF, Kawachi I. Social epidemiology. New York: OxfordUniversity Press; 2000.
10/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
http://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=12049&p_sprache=Dhttp://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=12049&p_sprache=Dhttp://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=12049&p_sprache=Dhttp://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=12049&p_sprache=D -
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
11/12
10. Born G, Baumeister SE, Sauer S, Hensel E, Kocher T, John U.Merkmale von Risikogruppen einer unzureichendenInanspruchnahme zahnmedizinischer Leistungen Ergebnisseder Study of Health in Pomerania (SHIP) [Characteristics of riskgroups with an insufficient demand for dental services - resultsof the study of health in Pomerania (SHIP)]. Gesundheitswesen.2006 Apr;68(4):257-64. DOI: 10.1055/s-2006-926723
11. Fridrici M, Beyer A, Lohaus A. Sind Jugendliche online besserzu erreichen? Zur Internetnutzung beiStressprventionsmanahmen fr Jugendliche [Getting throughto adolescents "online". The use of web-based programs forstress-prevention in youth]. Prax Kinderpsychol Kinderpsychiatr.2008;57(1):39-59.
12. Friedrichs M, Friedel H, Bdeker W. Teilnehmerstruktur undkonomischer Nutzen prventiver Bonusprogramme in derbetrieblichen Krankenversicherung [Participant structure andeconomic benefit of prevention bonus programmes in companyhealth insurance funds]. Gesundheitswesen. 2009Oct;71(10):623-7. DOI: 10.1055/s-0029-1239571
13. Garbe C, Buettner PG. Predictors of the use of sunscreen indermatological patients in Central Europe. Prev Med. 2000
Aug;31(2 Pt 1):134-9. DOI: 10.1006/pmed.2000.068114. Geyer S. Research on socialdeterminantsand health: what sorts
of data do we need? Int J Public Health. 2010 Feb;55(1):1-3.DOI: 10.1007/s00038-009-0066-2
15. Hinkle LE Jr, Whitney LH, Lehman EW, Dunn J, Benjamin B, KingR, Plakun A, Flehinger B. Occupation, education, and coronaryheart disease. Risk is influenced more by education andbackgroundthan by occupational experiences, in the Bell System.Science. 1968 Jul 19;161(3838):238-46. DOI:10.1126/science.161.3838.238
16. Horch K, WirzJ. Nutzungvon Gesundheitsinformationen [People'sinterest in health information]. BundesgesundheitsblattGesundheitsforschung Gesundheitsschutz. 2005Nov;48(11):1250-5. DOI: 10.1007/s00103-005-1153-z
17. Janen C, Borgetto B, Heller G, eds. MedizinischeVersorgungsforschung: Theoretische Anstze, Methoden,Instrumente und empirische Befunde. Weinheim, Mnchen:Juventa Verlag; 2007.
18. JanenC, Grosse Frie K, Dinger H, Schiffmann L, Ommen O. DerEinfluss von sozialer Ungleichheit auf die medizinische undgesundheitsbezogeneVersorgung in Deutschland. In: Richter M,Hurrelmann K, eds. Gesundheitliche Ungleichheit: Grundlagen,Probleme, Perspektiven. 2., aktual. Aufl. Wiesbaden: VS Verlagfr Sozialwissenschaften; 2009. p. 149-65. DOI: 10.1007/978-3-531-91643-9_8
19. Janen C, Pfaff H. Psychosocial environments. In: Kerr J,Weitkunat R, Moretti M, eds. ABC of Behavior Change: A Guideto Successful Disease Prevention and Health Promotion.
Edinburgh , New York: Elsevier Churchill Livingstone; 2005. p.153-265.
20. Jckel KH, et al. Messung und Quantifizierung soziographischerMerkmale in epidemiologischen Studien. In: Ahrens W, BellachBM, Jckel KH, eds. Messung soziodemographischer Merkmalein der Epidemiologie. Mnchen: MMV; 1998. p. 7-38.
21. Kahl H, Hlling H, Kamtsiuris P. Inanspruchnahme vonFrherkennungsuntersuchungen und Manahmen zurGesundheitsfrderung [Utilization of health screening studiesand measures for health promotion]. Gesundheitswesen. 1999Dec;61 Spec No:S163-8.
22. Kamtsiuris P, Bergmann E, Rattay P, Schlaud M.Inanspruchnahme medizinischer Leistungen. Ergebnisse desKinder-und Jugendgesundheitssurveys [Useof medical services.Results of theGerman HealthInterview and Examination Surveyfor Children and Adolescents (KiGGS)]. BundesgesundheitsblattGesundheitsforschung Gesundheitsschutz. 2007May-Jun;50(5-6):836-50. DOI: 10.1007/s00103-007-0247-1
23. Kitagawa EM, Hauser PM. Differential Mortality in the UnitedStates. A Study in Socioeconomic Epidemiology. Cambridge:Harvard University Press; 1973.
24. Knopf H, Rieck A, Schenk L. Mundhygiene. Daten des KiGGSzum Karies-prventiven Verhalten. [Oral hygiene. KIGGS data oncaries preventative behaviour]. BundesgesundheitsblattGesundheitsforschung Gesundheitsschutz. 2008
Nov;51(11):1314-20. DOI: 10.1007/s00103-008-0700-9
25. Koller D, Lack N, Mielck A. Soziale Unterschiede bei derInanspruchnahme der Schwangerschafts-Vorsorgeuntersuchungen, beim Rauchen der Mutter whrendder Schwangerschaft und beim Geburtsgewicht desNeugeborenen. Empirische Analyse auf Basis der BayrischenPerinatal-Studie. [Social differences in the utilisation of prenatalscreening, smoking during pregnancyand birth weight--empiricalanalysis of data from the Perinatal Study in Bavaria (Germany)].Gesundheitswesen. 2009 Jan;71(1):10-8. DOI: 10.1055/s-0028-1082310
26. Kuh D, Ben-Shlomo Y. A life course approach to chronic diseaseepidemiology. 2nd ed. Oxford: Oxford University Press; 2004.DOI: 10.1093/acprof:oso/9780198578154.003.0011
27. Lampert T, Kroll LE, Dunkelberg A. Soziale Ungleichheit derLebenserwartung in Deutschland. AusPolitik und Zeitgeschichte.2007;42:11-8. Available from: http://www.bpb.de/apuz/30179/soziale-ungleichheit-der-lebenserwartung-in-deutschland
28. Lampert T, Kurth BM. Sozialer Status und Gesundheit vonKindern und Jugendlichen: Ergebnisse des kinder- undJugendgesundheitssurveys (KiGGS). Dtsch rztebl.2007;104(43): A-2944-9.
29. Leppin A. Konzepte und Strategien der Krankheitsprvention.In: Hurrelmann K, Klotz T, Haisch J, eds. Lehrbuch Prventionund Gesundheitsfrderung. Bern, Seattle : Huber; 2004. p. 31-40.
30. Leyk D, Rther T, Wunderlich M, Sievert AP, Erley OM, Lllgen H.Inanspruchnahme und Durchfhrung von sportrztlichenVorsorgeuntersuchungen. Befragung von mehr als 10.000Langstreckenlufern. Dtsch rztebl. 2008;105(36):609-14. DOI:10.3238/arztebl.2008.0609
31. Mackenbach JP, Backer M. Reducing inequalities in health: aEuropean perspective. London: Routledge; 2002.
32. Mackenbach JP. Socio-economic inequalitiesin health in WesternEurope: from description to explanation to intervention. In:Siegrist J, Marmot M, eds. Social Inequalities In Health. NewEvidence And Policy Implications. Oxford, New York: OxfordUniversity Press; 2006. p. 223-250. DOI:10.1093/acprof:oso/9780198568162.003.00010
33. Marmot M, Wilkinson RG. Social Determinants of Health. 2nded. New York: Oxford University Press; 2006.
34. Marmot M. Health in an unequal world. Lancet. 2006 Dec9;368(9552):2081-94. DOI: 10.1016/S0140-6736(06)69746-8
35. Marmot MG,Rose G, Shipley M, Hamilton PJ. Employment gradeand coronary heart disease in British civil servants. J EpidemiolCommunity Health. 1978 Dec;32(4):244-9. DOI:10.1136/jech.32.4.244
36. Mielck A. Soziale Ungleichheit und Gesundheit. EmpirischeErgebnisse, Erklrungsanstze, Interventionsmglichkeiten.Bern: Huber; 2000.
37. Nagel E. Das Gesundheitswesen in Deutschland. Struktur,Leistungen, Weiterentwicklung. Kln: Deutscher rzte-Verlag;2007.
38. Razum O, et al. Migration und Gesundheit. Schwerpunktberichtder Gesundheitsberichterstattung des Bundes.Berlin: RKI; 2008.
11/12GMS Psycho-Social-Medicine 2012, Vol. 9, ISSN 1860-5214
Janen et al.: The influence of social determinants on the use of ...
http://www.bpb.de/apuz/30179/soziale-ungleichheit-der-lebenserwartung-in-deutschlandhttp://www.bpb.de/apuz/30179/soziale-ungleichheit-der-lebenserwartung-in-deutschlandhttp://www.bpb.de/apuz/30179/soziale-ungleichheit-der-lebenserwartung-in-deutschlandhttp://www.bpb.de/apuz/30179/soziale-ungleichheit-der-lebenserwartung-in-deutschland -
7/29/2019 Influencia de determinantes sociales en promocin y prevencin de salud
12/12
39. Richter M, Brand H, Rssler G. Soziokonomische Unterschiedein der Inanspruchnahme von Frherkennungsuntersuchungenund Manahmen der Gesundheitsfrderung in NRW [Socio-economic differences in the utilisation of screening programmesand health promotion measures in North Rhine-Westphalia,Germany]. Gesundheitswesen. 2002 Jul;64(7):417-23.
40. Richter M, Hurrelmann K. Gesundheitliche Ungleichheit:
Grundlagen, ProblemePerspektiven. Wiesbaden: VS; 2009. DOI:10.1055/s-2002-32814
41. RichterM. Gesundheitund Gesundheitsverhaltenim Jugendalter.Der EinflusssozialerUngleichheit. Wiessbaden: VS Verlag; 2005.DOI: 10.1055/s-2005-858652
42. Rieger C, Walter M, Wolf B, Kstner K. Inanspruchnahmezahnrztlicher Dienste Ergebnisse einerMundgesundheitsstudiein Sachsen [Utilization of dental services--results of an oral hygiene study in Saxony]. Gesundheitswesen.1999 Dec;61(12):620-7.
43. Rckl-Wiedmann I, Meyer N, Fischer R, Laubereau B, WeitkunatR, Uberla K. Schichtspezifische Inanspruchnahme medizinischerLeistungen und Vorsorgeverhalten in Bayern: Ergebnisse einerreprsentativen Bevlkerungsbefragung. [The use of medical
services and the utilization rate in screening programs in relationtosocialclass: results of a representativesurvey in Bavaria]. SozPraventivmed. 2002;47(5):307-17. DOI: 10.1007/PL00012641
44. Rckinger S, von Kries R, Pauli S, Munte A, Mielck A. DieKrebsfrherkennungsuntersuchung fr Frauen wirdin Regionenmit niedrigerem Haushaltseinkommen seltener in Anspruchgenommen Analyse von Daten der KassenrztlichenVereinigung Bayerns [Cancer screening for women is lessfrequently visited in regions with lower householdincomeanalysis of data from health insurances in Bavaria].Gesundheitswesen.2008 Jul;70(7):393-7. DOI: 10.1055/s-0028-1082075
45. Schwartz FW, et al., eds. Das Public-Health-Buch. Mnchen:Urban & Fischer Verlag; 2003.
46. Siegrist J, Marmot M. Introduction. In: Siegrist J, MarmotM, eds.Social Inequalities In Health. New Evidence And PolicyImplications. Oxford, New York: Oxford University Press; 2006.p. 1-25. DOI: 10.1093/acprof:oso/9780198568162.003.0001
47. Sieverding M, MatterneU, Ciccarello L, Haug U. Colonoscopy usein a country with a long-standing colorectal cancer screeningprogramme: evidence from a large German survey. ZGastroenterol. 2010 Dec;48(12):1351-7. DOI: 10.1055/s-0029-1245611
48. Sieverding M, Matterne U, Ciccarello L, Luboldt HJ.Prostatakarzinomfrherkennung in Deutschland. Untersuchungeiner reprsentativen Bevlkerungsstichprobe. Urologe.2008;47(9):1233-8. DOI: 10.1007/s00120-008-1695-4
49. Sieverding M, Matterne U, Ciccarello L. Gender differences inFOBT use:evidence from a large German survey. Z Gastroenterol.2008 Apr;46 Suppl 1:S47-51. DOI: 10.1055/s-2007-963489
50. Simoes E, Kunz S, Schmahl F. Inanspruchnahmegradienten inder Schwangerenvorsorge fordern zur Weiterentwicklung desPrventionskonzepts auf [Utilisation gradients in prenatal careprompt further development of the prevention concept].Gesundheitswesen. 2009 Jul;71(7):385-90. DOI: 10.1055/s-0029-1214401
51. Stock C, Brenner H. Utilization of lower gastrointestinalendoscopyand fecal occult blood test in 11 European countries: evidencefrom the Survey of Health, Aging and Retirement in Europe(SHARE). Endoscopy. 2010 Jul;42(7):546-56. DOI: 10.1055/s-0029-1244127
52. von dem Knesebeck O, Mielck A. Soziale Ungleichheit undgesundheitliche Versorgung im hheren Lebensalter [Social
inequality and health care among the aged]. Z Gerontol Geriatr.2009 Feb;42(1):39-46. DOI: 10.1007/s00391-008-0522-2
53. von dem Knesebeck O. Soziale Einflsse auf die Gesundheitalter Menschen. Bern: Huber; 2005.
54. Walter U, Drupp M, Schwartz FW, eds. Prvention durchKrankenkassen. Zielgruppen, Zugangswege, Wirksamkeit undWirtschaftlichkeit. Weinheim und Mnchen: Juventa; 2002.
55. Walter U, Schwartz FW. Prvention. In: Schwartz FW, et al., eds.DasPublic-Health-Buch. Mnchen: Urban & Fischer Verlag; 2003.p . 189-215.
56. Wanek V, Born J, Novak P, Reime B. Einstellungen undGesundheitsstatus als Bestimmungsfaktor einer Beteiligung anManahmen verhaltensorientierter Gesundheitsfrderung
[Attitudes and health status as determinants of participation inindividually oriented healthpromotion].Gesundheitswesen. 1999Jul;61(7):346-52.
57. WendtC, Wolf C. Soziologie derGesundheit. Wiesbaden: VS, Verl.fr Sozialwiss.; 2006. (Klner Zeitschrift fr Soziologie undSozialpsychologie : Sonderheft ; 46)
58. WorldHealth Organization. Ottawa Charter for HealthPromotion.Geneva: Health Promotion WHO; 1986.
Corresponding author:
Prof. Dr. Christian Janen, M.A.
Department of Applied Social Sciences, Munich Universityof Applied Sciences, Am Stadtpark 20, 81243 Munich,[email protected]
Please cite as
Janen C, Sauter S, Kowalski C. The influence of social determinants
on the use of prevention and health promotion services: Results of a
systematic literature review. GMS Psychosoc Med. 2012;9:Doc07.
DOI: 10.3205/psm000085, URN: urn:nbn:de:0183-psm0000850
This article is freely available from
http://www.egms.de/en/journals/psm/2012-9/psm000085.shtml
Published:2012-10-25
Copyright
2012 Janen et al. This is an Open Access article distributed under
the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by-nc-nd/3.0/deed.en). You
are free: to Share to copy, distribute and transmit the work, provided
the original author and source are credited.
Janen et al.: The influence of social determinants on the use of ...