1920 airsicknessitsna00crucuoft

of 120
-
Upload
ulf-dunell -
Category
Documents
-
view
215 -
download
0
Transcript of 1920 airsicknessitsna00crucuoft
-
8/6/2019 1920 airsicknessitsna00crucuoft
1/120
AIR SICKNESS:Its Mature and. Treatment
C R U C H E TAND
IHGULINIER
-
8/6/2019 1920 airsicknessitsna00crucuoft
2/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
3/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
4/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
5/120
AIR SICKNESS:Its Nature and Treatment
-
8/6/2019 1920 airsicknessitsna00crucuoft
6/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
7/120
nrrc.
Bale's Medical Books and Journals
AIR SICKNESS:Its Nature and Treatment
BYRENE CROCHET,
Professor of Medicine in the University of BordeauxAND
RENE MOULINIER,Naval Surgeon ; sometime Professor of Naval Hygiene in the
University of Bordeaux
With a Preface to the French Edition by Dr. V. PACHON,Professot of Physiology in the University of Bordeaux.
And an Introduction to English Readers byWing-Commander MARTIN FLACK, M.B,
Translated from the French by J. ROSSLYN EARP, M.A., M.R.C.S,
LONDONJOHN BALE, SONS & DANIELSSON, LTD.
83-91. GREAT TITCHFIELD STREET, OXFORD STREET, W.19*0
-
8/6/2019 1920 airsicknessitsna00crucuoft
8/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
9/120
TABLE OF CONTENTS.PAGE
To ENGLISH READERS, by LT.-COL. MARTIN FLACK, C.B.E. viiPRKFACE, by PROFESSOR V. PACHON xFOREWORD xiii
CHAPTER I.THB PHYSIOLOGY OF FLYING BEFORE THE WAR.
Ascent 3Descent 5Landing ... ... ... ... ... ... 6Study in arterial tension... ... ... ... ... 8Pathogenesis IIDiscussion and Summary ... ... ... ... ... 12
CHAPTER II.THE PHVSIOLOGY OF FLYING SINCE THE WAR.
General impressions 16Physiological phenomena 18
Ascent ... ... ... ... ... 18Descent 24Landing 28
CHAPTER III.THE NATURE OF AIR SICKNESS.
Arterial hypertension ... ... ... ... ... ... 31Fatigue. Criteria of fitness 35Cold 53Mental strain 56Emotion 56Oto-rhino-pharyngeal lesions ... ... ... ... ... 58Speed 61Other factors 63Discussion and conclusions 64
-
8/6/2019 1920 airsicknessitsna00crucuoft
10/120
TABLE OF CONTENTSCHAPTER IV.
TRAINING AND OVERWORK IN THE AIRMAN. PAGEPhysical overstrain 73Cardiac asthenia ... ... ... ... ... ... ... 74Psychical overstrain ... 79Air neurosis 81
CHAPTER V.AIR HYGIENE.
The hygiene of the airman ... ... ... ... ... 86General advice 89
THE PRINCIPAL CONTRA-INDICATIONS TO FLIGHT.Cardio-vascular ... ... ... ... ... ... ... 9Pulmonary 91Auditory ... ... ... ... ... .. ... ... 93Digestive 93Neuro-psychic 94The place of the disabled in aviation 95
VI
-
8/6/2019 1920 airsicknessitsna00crucuoft
11/120
AN INTRODUCTION TOENGLISH READERS.By Wing Commander MARTIN FLACK,
C.B.E., M.A., M.B.Director of Medical Research, Royal Air Force.To a far greater extent than is generally realized,
a successful future for aviation depends upon themental aptitude and physical fitness of the personnelengaged in flying. Investigation has shown thatmany flying accidents are due to what may be calledthe human element. For this reason, it is impera-tive that special methods shall be employed in theselection and care of the airman. Not only mustthe candidate for aviation possess the necessarymental aptitude, but he must also have the potentialability to acquire the mechanics of flight. Further-more, he must also be endowed with resistance tothe fatigue, both bodily and mental, necessarilyassociated with learning to fly, with flights of longduration, and with flights at high altitudes.Given proper selection, the medical care of theflier is therefore largely preventive. It is the dutyof medical officers to watch over their flying per-sonnel, to see how pilots are withstanding the effectsof flying, and to take proper steps to combat at anearly stage the onset of flying stress, and to mitigateits effects. For this reason, periodic medicalexamination, as required by the InternationalAeronautical Convention, is a necessity. It is im-portant, therefore, that medical officers shall be
VII
-
8/6/2019 1920 airsicknessitsna00crucuoft
12/120
AN INTRODUCTION TO ENGLISH READERSthoroughly cognizant, not only of the methodsemployed in their own country, but also of thosein use in various other countries. They should alsobe acquainted with the progress of research intothe various medical aspects of aeronautics. On thisaccount, the publication of the valuable work of theirFrench colleagues is particularly opportune at thepresent time.There is still a wide field of investigation open tomedical officers interested in flying; such work willdo much, not only to further medical knowledge,but also to advance the success of aviation, bothmilitary and civil.Medical Department,
Air Ministry,March, 1920.
vm
-
8/6/2019 1920 airsicknessitsna00crucuoft
13/120
PREFACE.ALL progress is at a price ; man pays a ransom foreach of his adventures. The conquest of the air,besides its numerous dangers, is to-day resulting ina new disease, the disease we call air sickness.
Messrs. Cruchet and Moulinier gave to it aprecise definition in 1910-11. Aviation was at thattime making its first great debut, and credit is dueto these authors in the first place because they sawat once that, if there should happen to be disturb-ances peculiar to aviation, they would be bestdetected during these early flights and beforeassuetude should have had time to play its part.In this respect their work was the result of judg-ment rather than of opportunity. Through reasonthey foresaw and time has blessed their observation.In addition they spared no pains to analyseexperimentally those peculiar disturbances whichthey observed. Here again it seems likely that theiranalysis must remain as the foundation of thepathological physiology of the airman.Having directed their researches especially fromthe point of view of the changes observed inarterial tension and many observers seem to havecopied their example Cruchet and Moulinier werefrom the first struck by a remarkable phenomenonconstant in athletic individuals and quite charac-teristic after flights in high altitudes. This was anobservation on landing after flight : a condition ofarterial hypertension remarkable for the constantrise in minimal pressure, with no correspondingincrease of the maximum pressure. On the contrary,a distinct fall of systolic pressure is the general
ix
-
8/6/2019 1920 airsicknessitsna00crucuoft
14/120
PREFACErule. This constant rise of minimal arterialpressure appears therefore to be a vasomotorphenomenon. But what is the first cause of thisintense and general vasoconstriction ? Above allit is important to know whether this phenomenonshould be merely recorded along with others, orwhether it may not be of basic import, controllinga whole series of secondary extra-physiologicalreactions. Here indeed is the problem which liesat the heart of this little book, to the solution ofwhich the authors have brought a distinctly originalcontribution. It will be seen how Cruchet andMoulinier have been led to attribute to the questionof speed in the course of flight (speed in getting upand, above all, speed in the descent) not only animportant but a preponderating place in the genesisof various reactions. The perusal of their workwill also, I think, justify the belief that the stateof arterial hypertension, or better, of vasomotorhypertonia. normally observed in the airman, repre-sents something quite other than a simple pheno-menon to be added to a catalogue of observations.This increase of vasomotor tone constitutes inreality the fundamental phenomenon on whichdepend the multiple disturbances in the domain ofthe nervous centres. Dizziness, headache, drowsi-ness, the triad symptomatic of a profound cerebralvasoconstriction, are here its various expressions.
Certainly there arecases in which the arterial
hypertension is wanting, or to speak more correctly,it appears so to be, for Cruchet and Moulinier haveshown that this paradox is only apparent. Inreality the slightest lowering or raising of theminimal pressure expresses a particular thing: thefatigue of the airman. The pages of this book
-
8/6/2019 1920 airsicknessitsna00crucuoft
15/120
PREFACEdevoted to fatigue, and particularly to the means ofdetermining its presence in the airman, containmany very striking passages. We possess to-day inthe systematic study of the variations of arterialpressure resulting from measured output of energya true criterion of the training* and of the functionalvalue of an organism for the production of work.When the individual is "in training/' the methodicalstudy of his arterial pressure, taken at regular inter-vals in the course of work, shows the existence ofa work plateau, expressing the adaptation of thesubject. If the latter is not adapted, the fall ofpressure (and especially of the maximum pressure)is equivalent to a real danger sign, which indicatesthe cardio-vascular breaking point; that is to say,it constitutes a precise objective sign of fatigue,independent of any personal equation. Cruchet andMoulinier have shown by abundant evidence howsuch a criterion of "training" might be made useof with great profit for estimating fatigue both inthe case of the airman and in various sports. Asthey themselves say, the recent researches ofVillemin confirm their own in this respect.And finally, Messrs. Cruchet and Moulinier havedrawn from this scientific study a right conclusion :a code of practical applications, determining thehygiene of the airman and the centra-indications toindulgence in flight. Thus their work becomes prac-tical. It is apparent that physiological analysispursues the observations of facts, not only to under-stand them, but also and more especially to controlthem, or as Claude Bernard would have put it totranslate them into deeds.
This little book is a deed. VICTOR PACHON.XI
-
8/6/2019 1920 airsicknessitsna00crucuoft
16/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
17/120
FOREWORD.THE researches on the physiology of aviationwhich we undertook in 1910-1911 have roused a
certain amount of interest, 'both in France andabroad, since we made our communication on" Air Sickness " to the Academic des Sciences inApril, 191 1. 1Described in the first place by the present writers,air sickness has rapidly acquired a place in Frenchand foreign literature. It is commonly to be founddescribed in pre-war writings under the names ofEl Mai de los Aviadores, in Spanish-speakingcountries; La Malattia degli Aviatori or // Maledegli Aviatori or Di Pegaso, in Italy; Mai dosAviadores, in Portugal and Brazil; Aviation orAviator Sickness, in English-speaking countries;Die Fliegerkrankheit or Aviatiker Krankheit, inGermany.Since 1911 we have observed that the phenomenaof air sickness, considered under their most usualand least serious form, are physiological pheno-mena; that is to say, there is nothing morbid inthese changes which may be experienced by every
1 Cruchet and Moulinier : " Le mal des aviateurs "(Acad. des Sciences. April 24, IQII, and Journal de Physiol.et Pathol. Generate, pp. 388-395, May, IQII). The firstnotice of this communication appeared in the Journal demed. de Bordeaux on September 18, IQIO, and in theGazette Hebdom. des Sciences Med. de Bordeaux on Sep-tember 25, IQIO. See also articles by R. Cruchet in theJournal (Paris, April 25, IQII), the Journal Medical Fran-fats (August 15, IQII), the Revue Scientifique (December9, IQII).
xiii
-
8/6/2019 1920 airsicknessitsna00crucuoft
18/120
FOREWORDhealthy man who goes in for high flying. Theirexistence must not be interpreted by any means asa proof either of physical or intellectual degeneracy.On the contrary, they are most commonly foundamongst airmen of keen mentality, perspicacity andjudgment. It is not everyone who is aware ofthem, even when they exist, and since they arerarely or never all found in the same subject, itwill be understood that they may pass unnoticedin a rapid examination.What is important is not so much their existence,in itself of little moment and always transitory, butthe conditions under which the man is liable to findhimself at the time when they make their appear-ance. A momentary loss of consciousness, a slightgiddiness, a simple hesitancy in controlling theaeroplane, a buzzing in the ears, an instant ofsleepiness or of languor, are in themselves veryinsignificant, and do not suggest any real failure inthe functioning of the human mechanism, but at aHeight of 50 metres and a fortiori at a height ofseveral hundred metres above the earth, the con-sequences of even such slight disturbances as these
. are to be treated with very great respect. 1We shall recall in our first chapter those pheno-mena which we described originally before the war.In the second chapter we shall study the advancemade in the physiology of flight since the war, andwe shall show that experience has completely con-firmed our first observations.We shall try in the third chapter to unravel thereal cause of the phenomena which we havedescribed. After having pointed out the capital
1 R. Cruchet : Revue Scientifique, December g, igu,loc. cit.
-
8/6/2019 1920 airsicknessitsna00crucuoft
19/120
FOREWORDimportance of arterial hypertension, we shall dis-cuss the functional value of cold, fatigue, intellectualeffort, emotion, speed, and other factors of lessimportance.Our observations will lead us in the fourth chapterto treat of the questions of training and overworkand the physical and psychical accidents which mayresult from them .
Finally, in Chapter V we shall discuss generalhygiene and the elementary advice which should begiven to airmen, as well as the chief contra-indications to flying.
xv
-
8/6/2019 1920 airsicknessitsna00crucuoft
20/120
-
8/6/2019 1920 airsicknessitsna00crucuoft
21/120
AIR SICKNESS. 1ITS ORIGIN AND TREATMENT.
CHAPTER I.THE PHYSIOLOGY OF FLYING BEFORE THE WAR.FLYING requires a physical effort and a constantmental strain because it is carried out under con-
ditions to which the organism was not originallyadapted. Generally speaking, flights at high alti-tudes such as were carried out by airmen up tillthe year 1911 lasted for a maximum duration of45 minutes. A height of 2,000, 2,500, or 3,000metres is reached in from 30-40 minutes, and themachine rushes from this height to the earth infrom 5-7 minutes. Chavez, during his tragic flightacross the Simplon, rose from 880 metres (Brieg) to2,100 (Kulm) in 19 minutes. Morane at Le Havrereached 2,600 metres in 24 minutes, and returnedin 6 minutes. At Bordeaux the same flier rose in22 minutes to 1,500 metres and came down in 5.Legagneux at Pan rose to 3,200 mietres in the samespace of time. Chavez, Legagneux and Moranewhose feats we have quoted were flying mono-planes. On biplanes these high altitudes arereached more slowly and require a more prolongedeffort on the part of the airman. The descent is1 Cruchet et Moulinier : " Le Mai des Aviateurs," loc. cit.
I I
-
8/6/2019 1920 airsicknessitsna00crucuoft
22/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARmade with equal speed in either kind of machine,the rapidity depending on the method of returningto earth. 1 This method is known under the nameof vol-planing. It is used because it appears to beimpractical to effect a landing with the throttlepartly or completely open on a machine which"has no mechanical contrivance to enable a fastmachine to descend slowly " (Morane). 2 Moreover,if they made use of their motor in the descent theairmen would see their speed increased in that thedriving power of the propeller is added to theaction of gravity.A high speed in ascending, a vertiginous descent,such is the special mechanical condition peculiarto flight at high altitudes.
This condition gives quite a special character tothe biological effect of these ascents. It is a newand important factor added to the action of pres-sure variations (760 millimetres mercury on thelevel, 591 at 2,000 metres, 521 at 3,000 metres) andto the changes in the chemical composition ofthe air, and to the temperature variations (60-70degrees F. on the earth, 45 degrees F. at 3,000metres). These being the ordinary factors whichcondition physiological variations, and to which aliving organism is always subject at high altitudes.It is probably this new factor which gives itsspecial character to air sickness an illness whichwe have tried to study during the festival atBordeaux, which took place from September n-18, 1910, in the neighbourhood of Merignac. To
1 And sometimes on a breakdown of the motor while themachine is in the air.2 Note by Translator. Modern machines have a greaterrange of speed.
-
8/6/2019 1920 airsicknessitsna00crucuoft
23/120
THE ASCENTthis end we were able to follow every day of theweek the programme of the principal airmen. Inparticular, Naval Lieut. Byasson, Lieuts. Cammer-mann and Remy (biplanes), Messieurs Morane,Legagneux, Tyck (monoplanes), Bielovucic, Bregiand Juillierot (biplanes) were good enough to replyto our questions and submit themselves to ourexperiments. Here are the results of the inquirywhich constitute our first communication on thesubject.The Ascent. During the ascent respiration be-comes shorter at a height of about 1,500 metresthat is to say, at a less height than when rising ina balloon; the heart beats faster, but usually thereis no palpitation; there is, strictly speaking, nosensation of nausea or of abdominal distensionsuch as sometimes occurs in mountain climbing,but there is a slight discomfort which Moraneattributes to the mental inquietude which one ex-periences in so vast a solitude. At about 1,200metres difficulty in hearing makes its appearance;the hum of the motor becomes dimmed. Thisphenomenon, which is clear enough in dry weather,is even more noticeable when the weather is cloudyor misty. Buzzing in the ears, although notsevere, shows itself at a greater height abouti,800 metres (Morane). Legagneux has observedclickings in the ears at a lower altitude; it is truethat it was the first time he had risen to so greata height, and a passenger who rose in the sameway the first time to 300 or 400 metres on a biplaneexperienced the same phenomenon; the question ofassuetude must evidently be taken into account.Even considering it to occur at 1,800 metres, how-ever, this phenomenon makes its appearance at a
-
8/6/2019 1920 airsicknessitsna00crucuoft
24/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARlower altitude than that at which it has beenobserved in mountain climbing. No airman ex-perienced any dizziness.
' The view is always very clear," writes Morane,"though the rapidity with which objects pass intothe distance and diminish in size may give a contraryimpression/' Moreover, in fine weather and whenthere is a haze, the sun may be reflected from thesurface of the mist with such blinding effect as tointerfere considerably with the control of the mono-plane (Morane). 1 Another airman experienced truevisual hallucinations in the course of a long flight;every moment he seemed to see the spires of theCathedral of Notre-Dame appearing on his rightat the time when he was still several hundred milesfrom Paris.A slight temporal headache appears in experiencedairmen at a height of 1,500 metres; in beginnersit makes its appearance at a lesser altitude.Cold becomes rapidly painful above 2,000 metres;at Bordeaux this was particularly the case.
" At Bordeaux," writes Morane, " I was not cold up to1,500 metres; above this height the temperature fell veryrapidly and at 2,000 metres it was certainly in the regionof 15 C. 2 At the mouth of the Seine the phenomenonof falling temperature was much less marked. I can onlyexplain it in relation to the time of the year : it was thenmidsummer, and perhaps the warmth was more penetrat-ing and reached farther upwards through the atmosphericbelt."Above the height of 1,500 metres an insistent
desire to micturate made its appearance.1 The great difficulty with the monoplane is to avoid
giving it too sharp an angle of inclination either in risingor in descent (Morane).2 Airmen did not carry thermometers at this time.Morane's estimate is purely subjective and consequentlymust be accepted with caution.
-
8/6/2019 1920 airsicknessitsna00crucuoft
25/120
THE DESCENTAbove the height of 1,000 metres, and to a greaterextent above the height of 1,500 metres, voluntarymovement becomes more nervous, and irregular,
reflex movements have a greater amplitude (Morane).Cold, slight breathlessness which comes on at thistime, the more rapid action of the heart, the re-flection of the sun and the disturbances of hearing,to which must also be added the nervous tensionand fatigue all these suffice to explain the changesin the motor system.The Descent. In the descent the heart beats withgreater force, but without acceleration. The palpi-tations which are felt without delay increase inproportion to the rapidity of the descent. It isdifficult to take account of the respiratory changeson account of the rapidity of the speed of vol-planing in which 300 or 400 metres are coveed in aminute. The result is a kind of distress, com-parable to the sensation of emptiness which weexperience in a rapidly descending lift. The buzz-ing and whistling in the ears, the desire to micturate,tend to increase towards the end of the descent, butthe phenomena which dominate the situation andwhich increase as the earth is approached, are asfollows :
(1) A burning sensation; a flushing of the facewith a sensation of warmth. There is irritation ofthe eyes, which are injected; the nostrils are moist,though there is no epistaxis.(2) The headache.
(3) A remarkable tendency to sleep. So compel-ling is this that the eyes will close from time totime, in spite of the most determined effort to keepthem open. Only quite recently there was reportedthe case of a young airman who was found fast
-
8/6/2019 1920 airsicknessitsna00crucuoft
26/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARasleep in his aeroplane in the open country; whenhe had been awakened he was unable to rememberin what way he had landed. 1We must add that in this dizzy descent as anexperienced airman has remarked the distress putsa strain on the strongest. Momentarily the airmanis even surprised by fear a fear which, happily, isnearly always very brief; but the thought and thepicture of death are never absent from his mind. 2Voluntary movement is slow and awkward, inmarked centra-distinction to the physical and mental
vivacity of the individual. Some airmen are awareof this numbing of the wits and of a dullness whichprevents them from carrying out the necessarymechanical actions as rapidly as they would wish.Others, on the contrary, are unaware of itsexistence.The Landing. When he lands the airman, how-ever energetic he may foe by nature, steps from hisaeroplane with a manifest heaviness; he moves offwith a firm step, though a little slowly, to hishangar a short distance away. But now the buzz-ings and whistlings in the ear become more intense
1 This may be compared with the experience of thosewho have come down mountain sides on the funicular rail-way. In the descent of the Jungfrau, for example, it iswell known that travellers who come down from 3,200 to2,000 metres (the little Scheidegg) go to sleep in theircompartments one after the other, though the journey takesno longer than 15 to 20 minutes. Practically everyoneexperiences some buzzing in the ears in the course of thisdescent.2 The airman Renaux, landing at Puy-de-D6me onMarch 7, 191 1, found himself confronted by these thoughts :" The sinister outline of the mountains rose up before me,"he said, " and in spite of myself I could not help thinkingof the hapless Chavez, who paid for his great victory withhis life."
-
8/6/2019 1920 airsicknessitsna00crucuoft
27/120
THE LANDINGthan they have ever been up to the present; ourhero is as though deafened, he hears indistinctlythose who speak to him, or the applause with whichhe is greeted; sometimes he is seized with giddiness,his head swims, and it once happened that an air-man fell almost into our arms as he was returningto his tent.The headache persists not only at the time oflanding, but for several hours afterwards; the sameis true of the sleepiness. One of the officials atthe Bordeaux Meeting attached to a young airman,who was flying at great heights for the first time,confessed to us that his ward was in the habit ofsleeping* for five or six hours after his excursions,that he gave no reply to those who spoke to him,but had a numbed and stupefied appearance, eatingnothing at meal-times, thinking only of sleep.These experiences are confirmed by Vedrines.The respiratory movements tend to recover theirnormal rhythm from the time of landing: it isotherwise with the circulatory mechanism, on whoseaction we shall lay special emphasis. Cyanosis isobserved in the extremities: the fingers are blue.Wynmalen, who reached a height of 2,870 metres,remarks that he could feel the blood running fromhis nails into his fur-lined gloves and the red dropsmoistening his lips. 1 Morane never noticed a likephenomenon, which, moreover, may be related tothe low temperature in the upper regions of theair which makes the speed of the aeroplane morenoticeable. This chilling is very painful, and allairmen complain of it. We have never seen epi-
1 P. Bassett-Rivet : "A tire d'aile " (Revue des DeuxMondes, February i, 191 1, p. 659).
-
8/6/2019 1920 airsicknessitsna00crucuoft
28/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARstaxis, but we have constantly observed hypersemiaof the conjunctiva. The eyes, however, may beefficiently protected by appropriate glasses.The pulse is slightly increased, the dicrotic im-pulse in the radial artery is not well marked. Theoscillations on the Pachon oscillometer are of smallamplitude. There is no palpitation.Study in Arterial Tension. Arterial pressure is
constantly increased at the time of landing after anyflight at altitudes of from 1,000 to 2,000 metres.Amongst the observations which we have made,the following are worthy of remark (they are takenat the wrist, using the Pachon oscillometer) :
AIRMAN Y.Before flying 5.30 p.m.
Minimum pressure 9 cm. Hg.Maximum pressure 18 ,, ,,Pulse-rate 70 per minute.
At 6 p.m., after a flight of 25 minutes, duringwhich on the 20th minute the height of 1,100 metreswas registered by the barometer, the followingobservations were made :Minimum pressure 12 cm. Hg.Maximum pressure 19 ,, ,,Pulse-rate 80 per minute.
After a flight of 27 minutes, with a maximumaltitude of 1,500 metres:
Minimum pressure 12 cm. Hg.Maximum pressure 19 ,, ,,Pulse-rate 75 per minute.
-
8/6/2019 1920 airsicknessitsna00crucuoft
29/120
STUDY IN ARTERIAL TENSION111 the case of another airman, after a first flight
attaining 1,100 metres, we observed:Minimum pressure ... ... Qi cm. Hg.Maximum pressure 16 ,, ,,.Pulse-rate 80 per minute,
and after another flight, reaching to 1,380 metres :Minimum pressure io cm. Hg.Maximum pressure ... ... i6 ,, ; ,Pulse-rate 84 per minute.
This hypertension, which we have very oftenobserved, is the more remarkable in that ourobservations were made upon athletes in perfecttraining, a condition which is essential if usefuldata are to be obtained. 1The increased pressure is less apparent in sub-jects who are suffering from great fatigue. These
latter experience severe palpitations and show a verymarked increase in the pulse-rate (108). This tire-some tachycardia, symptomatic of cardiac in-sufficiency, was noticed in a young airman who hadjust reached a height of 1,000 metres, after a risingflight of one hour's duration (see fig. i, p. 32).The increase of arterial pressure is peculiar toairmen descending from high altitudes. We havenever observed it in airmen who maintain a heightof 100 to 150 metres.Thus with Lieut. Z. at the time of departure:
Minimum pressure 9 cm. Hg.Maximum pressure 19 ,, ,,Pulse-rate 80 per minute.1 v. Pachon : " Education physique et criteres fonctipn-nels. Les variations de la pression arterielle, critered'entrainement " (Soc. de Biol., May 21 and 28, 1910,pp. 809 and 927).
-
8/6/2019 1920 airsicknessitsna00crucuoft
30/120
THE PHYSIOLOGY OF FLYING BEFORE THE WAROn landing after a flight of 55 minutes at an
average height of 100 metres :Minimum pressure Q$ cm. Hg.Maximum pressure i8i ,,Pulse-rate 100 per minute.
If we must formulate a hypothesis to account forthese changes in blood-pressure changes whichmay have a serious sequel in patients subjected toa very vigorous mental strain, or to a sustainedconcentration we should like to submit that anorganism falling in 20, 30 or 40 minutes from aheight of 1,000, 2,000 or 3,000 metres has not thetime necessary to adapt his circulatory system tothe variations of atmospheric pressure (521 mm. Hgat 3,000 metres, 591 mm. Hg at 2.000 metres,760 mm. Hg at o). The hypertension observed onlanding is the expression of a vasomotor reaction.The disturbances upon which we have remarkedoften show different forms in different individuals.In this respect air sickness resembles mountainsickness. Some, perhaps, are always free fromsickness, such as Janssen; some will be affected atrelatively low altitudes, as Martin de Moussy, whoexperienced " la puna "at 1,970 metres. " Many havetold me, and I have experienced it myself, thatthey were taken ill at altitudes of less than 2,000metres/' 1 The symptoms may be more or lessmarked, according to individual temperament, butspeaking generally it may be concluded that theymake their appearance at a lesser altitude than isthe case in mountain climbing or even in balloonascents.
1 H. Kronecker, Revue Scientifique, January 26, 1895,P. 98.
10
-
8/6/2019 1920 airsicknessitsna00crucuoft
31/120
PATHOGENESISPathogenesis. What is the pathogenesis of the
events which we have described?The numerous controversies 1 which gave origin
to the researches on mountain-sickness and on thesickness of high altitude do not enable us to formany conclusion on the disturbances which we haveobserved, and which in certain respects resemblethese former disorders. But we have been struckby the constancy and the importance of the varia-tions in arterial pressure which are evidenced byour measurements and by the fact that these varia-tions are especially marked after rapid ascent ordescent to or from high altitudes, whereas in flightsat moderate altitudes, undertaken by trained pilots,there is no clearly marked reaction.
In conclusion, it is to be noted that vasomotorreactions, accompanied by hypertension, dizziness,headache, sleepiness, appear particularly at sometime after landing. It is these phenomena which dis-tinguish " air sickness " from " mountain sickness,"and which give a quite special aspect to these dis-turbances. The origin of air sickness is in allprobability the rapidity with which the airmantravels in space, and we believe that it is the inter-vention of this factor which makes comparativelyslight changes in atmospheric pressure of seriousand even dangerous moment. We say compara-tively slight, for so they are, in relation to thechanges of pressure to which divers, for example,are subjected, and it is worth noting that the diver'stroubles (buzzings, dizziness, congestion, haemor-
1 See the " Remarques " by Zuntz and Loewy, and the* Reponse a ces remarques " by de J. Tissot, in Journalde Physiologic et Pathologic Generate _, January i, 1911,pp. i and 75.
II
-
8/6/2019 1920 airsicknessitsna00crucuoft
32/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARrhage, &c.) are in some respects analogous withthose which we have been considering in theairmen.Discussion and Summary. Certain objectionshave been raised since the publication of our com-munication, as a result of which we have had aseries of interesting interviews.Some of the airmen whom we have interrogatedstate that no such symptoms as described abovehave ever been experienced by them. But most ofthese had never taken part in high flight tests, andas a result their experience is not of great interest.The disturbances which we have observed werealways, even in their least severe forms, consequentupon ascents to a minimum altitude of 800 metresand a rapid descent therefrom. It was only, there-fore, such observations as had been made uponairmen coming down with great rapidity from thisheight that had any value : amongst those whounderwent these conditions there were very few whohad had no experience of symptoms.We do not attach the significance of originalityto those physiological phenomena which accom-panied the ascent : they are already classical, havingbeen known for a long time by climbers andballoonists. They do show in airmen, as we havepointed out, this special peculiarity that they maketheir appearance at much lower altitudes than is thecase either in mountaineering or in the balloon.But the aeroplane ascent is too slow and the heightattained less than 4,500 metres up to the timeof the war was not sufficient for any reallydisquieting symptoms to result.
Quite otherwise is it with the descent, which isdangerous in proportion to its rapidity and to the
12
-
8/6/2019 1920 airsicknessitsna00crucuoft
33/120
DISCUSSION AND SUMMARYheight from which it commences. If in the case ofslow descents the phenomena experienced arelimited to a slight buzzing in the ears (Legagneux),to a slight oppression, some auditory disturbancesand excitement (Latham), to a sensation of stoppingof the ears (Garros), 1 these limitations do notapply when the descent is made at a high' speed.Take the case of Leon Morane, who came down atTrouville, his motor out of action as the result ofa break-down, from 2,585 metres in i minute and40 seconds, or at a speed of 57^ miles per hour.He acknowledged that he had felt faint, languorous,that he was extremely fatigued, and had a violentheadache. All of these symptoms became worse atthe time of landing when there were added to thembuzzings and whistlings of the ears which lasted forseveral hours afterwards. Similarly Vedrines con-fessed to us that when one day he was obliged tocome down at Varennes-sur-Allier from 3,000 metresin the space of about 3 minutes, or at a speed of37J miles per hour, his hands became purple, hisveins swollen and blue and he experienced a persis-tent headache for several days afterwards.Although one cannot ascertain definitely that itwas owing to such phenomena as these that Chavezmet his death, there are strong grounds for such apresumption; the same is true in the case of Hoxseywho, at Los Angeles in America, rose to a heightof 2,300 metres in half an hour, came down again
1 Garros, who arrived at Bordeaux on January 24, 1914,for an exhibition flight, volunteered readily to submit toan examination. On that day he flew scarcely higher than700 metres, remaining in the air on each occasion for10 to 15 minutes and descended gradually. His pressurewas the same on landing as at the departure : MX., 16^-17;Mn., 8i.13
-
8/6/2019 1920 airsicknessitsna00crucuoft
34/120
THE PHYSIOLOGY OF FLYING BEFORE THE WARin 2f minutes, or at a speed of about 31 miles perhour and was killed on the spot. No less authoritythan Latham who witnessed the accident, relatesthat 150 metres from the ground the machine wasseen to turn round and round without any efforton the pilot's part to recover himself. " Everythingpoints to the conclusion/* adds Latham, '7 thatHoxsey must have fainted/'There are others who have noticed that accidentsmay be due to the airman himself and are not alwaysthe result of failure in the machinery.
P. Rogers fell in California from a height ofsome 60 metres. He had the good fortune toescape alive and related that he had been seizedwith sleep at about 350 metres above the earth.He added that in spite of the clear consciousnessof danger, he had been quite unable to overcomethis somnolence which gradually encompassed him.He thought that this " aerial somnipathy " musthave resulted in the death of many airmen.The same newspaper article relates that CaptainMadiot met his death in 1910 through a fall atDouai which appeared to have resulted from anattack of syncope. 1
Vidart and Vedrines, after they had landed atthe aerodrome of Ans (near Liege) one Sunday atthe end of June, 1911, "could not disguise theirirresistible desire to sleep." The same phenomenawere observed in the case of Vedrines during theParis-Rome-Turin race.It is interesting to notice that immunity tomountain sickness confers no immunity to airsickness; thus Latham, who had never felt any
1 Popular Science Sittings, October 19, 1912, pp. 84-86.
-
8/6/2019 1920 airsicknessitsna00crucuoft
35/120
DISCUSSION AND SUMMARYsymptoms of mountain sickness despite numerousclimbs in high countries to a height above 2,500metres and balloon ascensions to 3,000 or 4,000metres, experienced those slight disturbances whichwe have described as air sickness, in coming downfrom a height of 1,500 metres in an aeroplane. Itis clear, therefore, that the two syndromes -are notidentical, and it is for this reason that we haveespecially insisted on the part played -by hyper-tension resulting from rapid descent.To resume briefly, we have always thought thatair sickness is due to the rapidity with which airmenregain the earth from great altitudes. When theyhave taken 20, 30, 40, 50 minutes (Captain Felix),i hour 54 minutes (Garros) to ascend, they comedown again vol-planing in 4, 5, 7, 8 (Felix), or 9minutes (Garros), that is at the rate of 300, 400, or500 metres a minute, a speed equivalent to from 12to 20 miles an hour. Prevost in December, 1911,rose to 3,000 metres in 58 minutes 30 seconds with apassenger, and came down again in 7 minutes, orat 15 miles an hour.The human organism, particularly as regards itsrespiratory apparatus, is not able to adapt itself inso short a time to the different conditions of atmo-spheric pressure, varying from 520 mm. of mercuryat 3,000 metres, or 591 mm. at 2,000 metres to760 mm. at sea level. Thus, from the time ofour earliest research it has seemed to us of thegreatest importance to draw attention to the result-ing rapid increase in arterial tension and particularlyin the minimal arterial pressure.
-
8/6/2019 1920 airsicknessitsna00crucuoft
36/120
THE PHYSIOLOGY OF FLYING SINCE THE WAR
CHAPTER II.THE PHYSIOLOGY OF FLYING SINCE THE WAR.WAR experience, as we shall now show, 1 hasconfirmed very closely our original work. Fromthe outset of this chapter it must be clearly under-stood that it is not with the influence of curiosityand emotion that we are now concerned, but onlywith the part played in the physiology of flying by
physiological reactions.GENERAL IMPRESSIONS.
The impressions of one's first flight are delicious,exhilarating, unforgettable. Here are the recordsmade by one of us (Cruchet) at Toul, on a Septem-ber evening of 1915, in a Maurice Farman :
I put on my hat, cross the fuselage, climb up and seatmyself behind the pilot. Round my waist I pass a belt,which is securely fastened to the seat behind me.The pilot raises his arm. The propeller is swung andwhirls round with an infernal noise; everything about usis flickering; a soldier's cap is blown away; the overallsof the mechanics who stand round flap in the strong windwhich we are making. The blades of grass are flattenedlike a field of corn after a thunderstorm.This for a moment only. Now we are off. We skim theearth for 100 yards or so, then abruptly we rise. Thesefew seconds occupied in leaving the earth are unspeakablydelicious. There is an exquisite surprise. The warm airlashes our faces. There is no shock, no hesitancy as ina motor-car; we glide on smoothly with no obstacle in ourpath.In spite of the fact that dizziness is said to be unknownin an aeroplane, one still hesitates to lean a little out of
1 Cruchet and Moulinier : " Le mal des aviateurs," Soc.de Biol. meeting of June 21, 1919, pp. 677-679, and Journ,de Medecine de Bordeaux, July 25, 1919.16
-
8/6/2019 1920 airsicknessitsna00crucuoft
37/120
GENERAL IMPRESSIONSone's seat and look beneath. There is a momentary senseof fear, and already the earth appears 300 or 400 metresdistant at the first timid glance. This view charms im-mediately, and it is quite true that there is no sense ofdizziness : confidence increases.Presently the country stretches out as far as the eye can
see. The earth is mottled with splashes of light greenthese are the, meadows and with stretches of dark green :the forests and woods. Elsewhere it is striped with greatbands of colour, brown or pale, according to the cropsthere under cultivation. Here is a rocky crest, surmountedby a fortress; there a village with houses of white stonesand red roofs. A few surrounding trees throw shadowslengthened by the sinking sun. In the valley is theMoselle, like some sinuous serpent, reflecting the lightfrom its silver scales. The white tracery of the roads liesover all. This might be a miniature sheep-fold, such aswe played with when we were children : people, houses,animals, leafy trees, we know them all again as we knewthem in those far-off festivals at Christmas and the NewYear. A delicious emotion moistens the eyelids with tearsof pure joy.Towards the horizon the distance melts into the infiniteblue : one longs to arrive there, always to go farther onthe way. The day-dream is only slightly disturbed by thedeafening hum of the motor and the cold which is begin-ning to get a grip. The sense of security is extraordinary,all fear, even anxiety, has disappeared. We seem to growlighter as if drinking air, only the wind whistling in thebracing wires tells the speed at which we are travelling,and still we seem to stand still. Actually we are movingat 50 or 60 miles an hour.Now we are lost in immensity ! Only with great diffi-culty can I make myself understood by the pilot on accountof the noise of the motor. From time to time I catch afew words that he is obliged to shout.
Presently the pilot makes a sign to me. I move my earto his lips. " See," he says, " how easy and supple is thehandling of an aeroplane," and he looses the controls,raising his two arms into the air. For some seconds heremains thus and then takes control again. A littlenervousness on my part does nothing to lessen my growingwonder and enthusiasm. We are more than 1,000 metreshigh, when suddenly he signals to me again. I draw near." Now look out," the pilot says ; " hold fast, we are goingto descend."
I sit solidly in the depth of my seat. The machinestarts sharply and turns upon its course. The wind seems
17
-
8/6/2019 1920 airsicknessitsna00crucuoft
38/120
THE PHYSIOLOGY OF FLYING SINCE THE WARsuddenly to have dropped and I have been transferred toa downward-travelling lift, a tightness gripping my heart.I want to see where I have got to, but the sky appearsbeneath me and the earth in the sky. I have no sense ofdizziness, strictly speaking, but I have lost all sense ofdirection. The silence is impressive; the pilot has shutdown his throttle and I have closed my eyes.When I open them, only a few seconds later, I lookover the fuselage and recognize the earth drawing rapidlynearer. Anxiety gives place again to enchantment. Weare planing with silent engine, so that there is not theslightest vibration. We can see the earth once more inrelief, things and creatures grow larger, the flying groundbecomes more distinct. And now we have arrived ; a bumpand we touch the earth, our journey at an end. It hastaken us fifteen to twenty minutes to reach 1,000 metres,and scarcely five minutes to return. I experienced no sortof physiological phenomenon, except the sensation of fall-ing as in a lift at the beginning of the descent; no dizzi-ness, not even a whistling in the ears, neither fatigue,nor sleepiness, nor headache.There is nothing strange in this, for the height reachedwas not great, and the speed both in rising and in descend-ing was slow, say, two miles an hour in the first case andseven miles an hour in the second.
It is by no means the same in flights at high alti-tudes, especially under conditions of high speed and rapidchanges of pressure, as was seen during the war. Theexperiences both of pilots and observers must be takeninto consideration.
PHYSIOLOGICAL PHENOMENA.The Ascent. In rising respiration becomes more
rapid at about 2,000 metres and markedly so at4,500 metres. This is the most distressing pheno-menon. Shortness of breath is constant. At 5,000metres one observer became out of breath withfaster and faster respiration on such small exertionas was demanded by the slightest movement. Theattempt to change his seat even resulted in a diffi-culty in getting his breath. Inspiration especially isinsufficient and the accessory muscles are called intoaction.
18
-
8/6/2019 1920 airsicknessitsna00crucuoft
39/120
THE ASCENTPalpitation and a rapid pulse are noticed above
2,000 metres. (In Lieut. D. a pulse-rate of 100 ascompared with 80 at the time of departure.)Congestion of the facial capillaries takes place
at about 4,000 metres. Formerly this phenomenonwas observed at from 1,500 to 2,000 metres, forin the early days the precautions taken against coldwere not sufficient. To-day the airman is muchbetter protected; he is sheltered, warmly clad, evenartificially heated.
Anorexia, nausea, and even vomiting, occurredfrequently amongst certain airmen who wereexamined by Ferry: a sensation of sea-sickness wasnoticed particularly in the eddies of warm air whichpress upwards upon the machine, or the eddies ofcold air which draw it towards the earth.
In addition to those whom we have treated forfrequent and persistent vomiting occurring in thecourse of each flight and after returning to earth, acertain number have told us that they sometimesexperience a true sea-sickness with distressing nauseawhen their speed in mounting was greater thanusual, or their machine was tossed about to anunusual extent. 1A sensation of dryness of the mouth makes itsappearance at about 1,500 metres.
Desire to micturate is occasionally so strong thatsome airmen carry a urinal.Hearing. One of the commonest sensations is
that of fullness in the ears the sensation of a corkplaced in the auditory meatus. There results fromit a certain degree of deafness, especially above2,000 metres.
1 J. G. Ferry : " Le Syndrome mal des aviateurs," Thesede Nancy, 1917, p. 47.19
-
8/6/2019 1920 airsicknessitsna00crucuoft
40/120
THE PHYSIOLOGY OF FLYING SINCE THE WARBuzzings in the ears are also a common pheno-menon appearing under 2,000 metres if the ascentis made too fast. They often occur as clickingswhich sound like ''rapid firing" (Ferry), and arenot affected by the movements of deglutition.There is never any dizziness. Thus Lieut. B., a
pilot who experienced dizziness on a doorway 20metres from the earth, was able to get out of hisseat 3,000 metres in the air, stand upright on thelanding carriage, and focus his camera without theslightest discomfort.
Sight. Disturbances of vision occur for the mostpart as psychic phenomena. The power of estimat-ing distances or the speed of another aeroplane isa faculty which must be educated. Novices some-times fail to see a German aeroplane passing attheir side on account of the speed at which it passes.But physical fatigue also affects the sight : thereflection of sunlight from the clouds is very hardto endure. It is the airman's aim to keep the sunas much as possible on his left and behind him.The Sense of Direction. It is chiefly in horizontalflight at altitudes of about 1,000 metres that youngairmen develop their skill and muscular endurance.The sense of equilibrium is one of the most difficultto acquire. In a fog the most skilful airman com-pletely loses his idea of the horizontal : he has nolonger any starting-off point.
In the course of a voyage in the mist, writes the lateDr. Emile Raymond, 1 I was a whole hour without seeingeither earth or sky, and therefore without any line of thehorizon.In such a case the pilot easily loses his sense of the
horizontal, particularly in the lateral direction; he doesnot notice that one wing is high and the other low, par-1 Bulletin Mtdical, November n, 191 1.
2O
-
8/6/2019 1920 airsicknessitsna00crucuoft
41/120
THE ASCENTticularly if he is so jolted as not to know which way heis sitting on his seat.
I observed that the earth was nearer on my right andtherefore that the right wing was lower, that the earthwas further off on my left, the left wing therefore beinghigher. In order to right my machine I had to carry myjoy-stick to the left. The fear of a mistake, which wouldhave been disastrous, caused me to work out this argumenttwice over before carrying out the necessary movements.Every airman has had the same experience; aftera passage through cloud or fog they often discoverthat one plane is lower, or that they are pointingdownwards or upwards, without ever being aware
of the change in direction. Bernard recalls howGraeme Anderson went up in an aeroplane with hiseyes bandaged intending to describe the move-ments of his machine to the pilot by telephone. Atfirst his description was accurate, but after a timehis conception of the aeroplane's movements and ofhis position in space lost their exactness.These facts tend to prove that our conception ofequilibrium is to a large extent a function of thesense of sight. I (Cruchet) had an opportunity ofdiscussing this question with Colonel Leclere, whohad also been struck with the loss of his sense ofdirection when flying through clouds. It appearsthat this sense is gained by a prolonged educationof the machinery of hearing. When we close oureyes in a motor-car or in a train, we have to bevery careful if we are not to be deceived about thegradient of our path, either when we are goinguphill or downhill, and the same thing applies alsoto our sense of transverse slope. Much more isthis the case in an aeroplane when the starting-pointof the earth's surface is wanting.Headache. A temporal headache is experiencedat a height above 2,000 metres, and more constantly
21
-
8/6/2019 1920 airsicknessitsna00crucuoft
42/120
THE PHYSIOLOGY OF FLYING SINCE THE WARabove 3,000 metres. Above 4,000 or 5,000 metresthe headache becomes very painful. At 5,200metres B. suffered so severely that he was obligedto descend: it is true that he had remained atthis height for more than an hour. On two otheroccasions, after being for more than five hours ata height of over 4,000 metres, the unbearable paincompelled him to come down again.Movement. Beyond 3,000 metres movementsbecome quick, jerky and nervous; reflexes are
sharper and the reactions produce movements ofgreater amplitude. Movement becomes more diffi-cult and requires greater effort, and a longer timeis necessary for the achievement of the same result.Signals as transmitted by the Morse code are givenout more slowly in proportion as the distance above3,000 metres is increased.Slowness of Ideation. A half-torpor, a sleepycontentment creeps over the airman. He feels itdifficult to concentrate his attention. His visualintelligence leaves much to be desired. Familiarobjects within reach of his hand appear blurred.He looks for a compass or the barometer and canno longer find them; the revolution counter appearsto be multiplied. A pilot with eighteen months'experience, flying at a height of 4,500 metres, sawseven or eight of these counters instead of a singleone, and was obliged to put his hand on it in orderto see it clearly.
"This is really it," he said, ashe touched it. He saw two or three oil gauges,
the map fluttered in its case, the latter grew to athing of immoderate dimensions. He dropped 500metres and all these phenomena disappeared.In proportion as one rises, gesture requires moreenergy, more time and greater effort. A simple
22
-
8/6/2019 1920 airsicknessitsna00crucuoft
43/120
THE ASCENTsum which can be calculated on the earth in twominutes requires twice that time at 5,000 metres.To rise to 6,000 metres and come down to 2,000metres, to rise again to 4,000 metres, is exhausting.To remain three hours in the air has almost thesame effect. 1The same anonymous author speaks of the suddendiscomfort which is experienced by the most expert
of pilots during the course of flight: "I do notknow what was the matter with me. I felt myselfgrowing weak/' There is a tendency to believethat these sensations are connected with dizzinessand disturbances of the ear, but this has by nomeans been proved to be the case.An Italian airman, Captain Ruffo, who has beenthrough many flights at high altitudes, says that at6,000 metres he experienced a heaviness of the head,a sleepiness, a mental and physical torpor. Thiscondition is very prejudicial to one's chances in air-fighting, for the combatant has need of all hisagility of movement and quickness of thought.Another pilot at 5,200 metres felt his hands andhis feet becoming numbed, their sensibility blunted,and the delicacy of touch considerably diminished,although he was not cold. When he withdrew hisfur gloves, being once more on land, his hands werestill livid, like the hands of a corpse, and all objectshad an abnormal sense of roughness to the touch;the right leg was still heavy and paralysed. Thesephenomena persisted until the next day.Lumbago. Lumbago is found chiefly among
beginners and is to be explained by the fact that thelumbar muscles are required to do most of the work,1 LIllustration, July 6, 1918, pp. 6 and 9.
23
-
8/6/2019 1920 airsicknessitsna00crucuoft
44/120
THE PHYSIOLOGY OF FLYING SINCE THE WARsince these correct the tendency of the head andshoulders to set themselves at right angles to thehorizontal plane of the machine.The Descent. In the descent emotional anxietyis experienced by novices and trained pilots who aresuffering from fatigue. The moment when thethrottle is closed must always be an impressive one.If the descent is made at a normal speed, say threeto four minutes for a thousand metres, i.e., 10 to12 m.p.h., nothing is noticed save some buzzingsin the ears with a sensation of fullness of theears which can be dispelled or diminished by degluti-tion. Occasionally when coming down in a closespiral those who are not accustomed to this methodexperience an unpleasant faintness of short dura-tion. On one occasion this occurred twice in thesame descent (Ferry).But should the descent be swift, the phenomenaalready remarked upon are accentuated : hearing isgreatly affected and becomes indistinct ; buzzings areincreasing and auricular pain becomes intolerable." The ears are forced open so that one might putone's fist in them/* so one observer has said;
" itis as though a speculum were being forced into thepassage and this were being torn to pieces"; it isa sensation of " scratching with a knife which stabsto the depth of the ear"; it is "a sharp prickingwith a thousand sharp needles "; a " shrill unbear-able whistling like the whistling of a steamengine " is heard. Even repeated deglutitionscarcely affects this sensation.In rapid descent the sense of distance is losttemporarily and the altmetre at this time gives noexact information. Thus airmen are recommendedto make a tour round the aerodrome before landing
24
-
8/6/2019 1920 airsicknessitsna00crucuoft
45/120
THE DESCENTin order the better to estimate their distance fromthe earth. This is what they call " getting to theearth into one's eye " (A. Castex).At the same time a painful constraint, sometimespassing into a veritable sensation of burning, thoughnot always very marked, affects the region of theheart. Palpitation appears and the tachycardia isincreased. Respiration also is interfered with,especially inspiration, on account of the speed ofthe descent. Blood rushes to the face which be-comes red and congested. Headache is more severein proportion as the speed increases.
Finally, there is the tendency towards sleep witha relatively frequent state of syncope. This happensespecially with young airmen who go in for acro-batic performances and with experienced pilots whoare tired out by overlong flights.One of the airmen whom I have examined wasseized at about 3,000 metres on two occasions witha sensation of torpor and weakness during hisdescent; he lost consciousness for the space ofabout one minute, and meanwhile his machine setitself in a spin. Fortunately he awoke in time toland safely with his passenger.These phenomena, and particularly the last, arereported by all who have inquired into the cause ofair accidents since the war.
In the descent, writes Castex, airmen are especiallydisturbed by the rapid transit from one altitude to another.One of them has told me that at least an hour is necessaryin order to come down from 3,000 metres without experi-encing any discomfort. As they get nearer to the earthit appears that there are prickings in the ears, a sensationof moving liquid within them and of buzzings with head-ache. All these disturbances disappear when the airmanlands and become considerably more serious if the machinedives, that is to say, during a sudden descent. They ex-
-
8/6/2019 1920 airsicknessitsna00crucuoft
46/120
THE PHYSIOLOGY OF FLYING SINCE THE WARperience under these circumstances a stupor which greatlyhinders their control of the machine (Gezes). 1
Panter is convinced that a large proportion ofunexplained accidents are due to " loss of conscious-ness " of the pilot. He quotes four cases at leastin which consciousness was lost in the air. 2 Ander-son, examining at the same time the cause of fifty-eight accidents which occurred in the course of fivethousand flights, ascribes four to cerebral fatigue,stupor or lethargy. If such accidents are rare inflying schools where the descent is usually made ata reasonable speed, it is by no means the same inthe course of air-fights when it is sometimes ofnecessity faster than one would wish. 3
Lieut. B., who was obliged to drop direct from1,200 metres to the earth as the result of an accident(his machine was on fire), occupied one minute onlyin doing so, a vertical speed of 56 m.p.h. On an-other occasion, in order to avoid a German attack,he dropped full speed ahead from 4,200 to 3,000metres in twenty seconds, or at 124^ m.p.h. He isvery clear in his description of the above-mentionedphenomena during these experiences.Another officer was wont to amuse himself bydropping in a spin from 2,000 metres which enabledhim to pass through 1,000 metres in half a minute,tRat is to say, at 74 m.p.h. One day the phenomenaabove mentioned were so marked particularly thesensation of cardiac constriction that he becamethenceforth more prudent.
1 A. Castex : " Troubles auriculaires chez les aviateursmilitaires," Archives de med. et de -pharm. militaires,July i, 1918, pp. 73-76.2 Panter, Journal of the Royal Naval Medical Service }January, iQi8.3 H. Graeme, British Medical Journal, January, igi8.
26
-
8/6/2019 1920 airsicknessitsna00crucuoft
47/120
THE DESCENTThe same observations result from the experiments
of Messrs. Marchoux and Nepper who were enclosedin a Paul Bert bell-jar at the Sorbonne. Althoughthose who showed reactions experienced head-ache and pain in the ears during the progressivedecompression to a point corresponding -with thepressure normally found at 6,000 metres, it was therecompression (descent) which was least successfullyborne by all, and particularly the last 1,000 metres.Frequently it was necessary to interrupt the recom-pression to enable them to recover from the distress-ing symptoms to which they were subject. Head-ache, auricular pain, neuralgia, sometimes dizzinessand even nausea, also threatened syncope, compelledthe authors to decrease the speed of recompressionto 12 m.p.h. during the last 1,500 or 2,000 metres. 1To recapitulate, all airmen experience phenomenaduring rapid descent, especially in diving with thethrottle open at a speed of no m.p.h. Thesephenomena are increased in proportion to the heightfrom which the descent is made. For this reasonairmen usually fall by successive stages so as todiminish distressing symptoms and in this way areable to reach the earth without suffering any seriousharm.There is still another phenomenon of which wemust take account; it is that of "the attraction of
the earth/' which Garros in particular pointed outto us in January, 1914, and which is fairly common-place in the experience of airmen who are accus-tomed to remain a certain space of time in the air.When they begin to descend they feel themselvesseized with an " irrational," imperious impulse to
1 Marchoux and Nepper, Societe de Biologie, June 21,1919, pp. 668-673.
27
-
8/6/2019 1920 airsicknessitsna00crucuoft
48/120
THE PHYSIOLOGY OF FLYING SINCE THE WARreturn with the greatest possible speed to the earth.A great amount of self-control is required to preventthem from coming down faster than is actually neces-sary. Often when they are a little tired they havenot the strength of will to overcome this impulse,although their reason tells them that to yield is bothuseless and dangerous.The Landing. When the airman has safely landedthere is often observed a fibrillary tremor of theextremities; the pulse is quickened, there is hyper-tension, especially of the minimum pressure, diminu-tion in the amplitude of oscillation, congestion ofthe face, all to a greater or lesser extent. Buzzingsin the ears and deafness persist, but the auricularpain decreases in intensity. There is no nystagmus.Sometimes there is a heaviness in jumping downfrom the machine, staggering gait is seen after longraids. The headache continues. There is a strongdesire to micturate, sleepiness and exaggeratedsensibility of the nerves.In the case of experienced airmen who have beena long time in the air, or who have made a too rapiddescent, the call to sleep is urgent. Most of themrealize that they are very irritable and highly strungduring the descent and the hours which immediatelyfollow it. Even the most stolid and amiableamongst them admit themselves to be bad-temperedon such occasions.Sometimes they go to sleep on the first benchwhich comes in their way, and it is a deep sleepwhich may last for an hour or more. It is a com-
mon-place of the aerodromes for pupils who havebeen up to perhaps 2,000 metres for not more thanhalf an hour as observers, hastily to seek their beds,where they swiftly fall asleep.
-
8/6/2019 1920 airsicknessitsna00crucuoft
49/120
THE LANDINGThese phenomena are accentuated by rapid
descent, nose-dives, or spins. The headache ispersistent, as are also the buzzings and the deafness ;fatigue is extreme, drowsiness overwhelming. Thesetroubles diminish within twelve to twenty-four hours,But they have a tendency to reappear with greaterreadiness if the airman does not take sufficient rest.The flying men do not seek amusement when they come
back to port. They sleep the sleep of the exhausted.Nothing can waken them. There will be a saying afterthe war: "To sleep like an airman." 1Dh. . . , one of our aces, in the spring of 1918,with 1,500 hours' flight to his credit and a record ofseven successful duels, described to us as follows
the dizziness and sleepiness which he experiencedafter shooting down an enemy aeroplane at 6,000metres; he followed it in its descent. On landing,as he came out of his machine he staggered as ifdrunk and was obliged to stand still. Staggering isa common experience to him after sudden descent.Since that time he has had dizziness which formerlynever troubled him. Often drowsiness assails himwhile he is flying; sometimes he falls asleep in hismachine. It happened recently that he passedunwittingly over our lines on his return. He tellsus that he has never experienced either palpitationsor dyspnoea on exertion. But now the least effortmakes him feel extremely tired.
It is our opinion that the craving for alcohol withwhich airmen have been so much reproached isreally due to the necessity of fighting against theinvasion of this lethargy, which so often maintainsits hold after the flight is over. Furthermore, the
1 LIllustration, July 6, 1918.29
-
8/6/2019 1920 airsicknessitsna00crucuoft
50/120
THE PHYSIOLOGY OF FLYING SINCE THE WARpersistent thirst which is met with after long,repeated and exhausting raids, may also have some-thing to do with this.Contrary to the general belief, the sex instincttends to decrease in force in proportion as the hoursof flight are prolonged. This has been confided tous by many airmen. Some have even asserted thatthey were subject to a transitory impotence. 1A loss of muscular power has also been describedafter flight, both by pilot, observer and passen-gers. Also a decrease of cutaneous sensibility,exaggeration of the tendon reflexes (Juarros), 2 anda slight hyperglycsemia (0*15 to 0*18 instead of0*09 to O'i2). 3 But these facts, which are encoun-tered in most people who have been recentlyoccupied with physical exercises, do not appear tooffer any peculiar interest by their appearance inairmen. The hyperglobulia of high altitudes whichwas discovered by Viault (of Bordeaux) was alsoobserved by Gemelli in airmen in the year 1917.Amongst the phenomena observed on landing, themost important in our opinion is that of arterialhypertension. We have shown how ever since 1910our attention has been particularly directed towardsit. For this reason it is of great importance thatwe should closely examine this question into whichundeniable errors have crept through the wronginterpretation of many factors.
1 This impotence has even been observed as a sequelto repeated diving-bell experiments, during which thepressure had been lowered to that which corresponds toan altitude of from 5.000 to 7,000 metres. In one case itlasted for three months.2 Societe de Biologic de Paris, June 21, 1919, p. 692.3 G. Maranon : Societt de Biologie, June 14, 1919,P. 631.
30
-
8/6/2019 1920 airsicknessitsna00crucuoft
51/120
ARTERIAL HYPERTENSION
CHAPTER III.THE ETIOLOGY OF AIR SICKNESS,
Arterial Hypertension. Since 1910, when we firstundertook our researches, we have insisted uponthe importance of those changes of arterial pressurewhich are noticed in airmen during the course offlight. We have remarked that the minimal tensionis constantly increased after descent from highaltitudes; the maximum tension also shows an in-crease, but the latter is of scarcely any significancein comparison with that of the minimal. The maxi-mum pressure indeed was slightly lowered in courseof flight at low altitude.
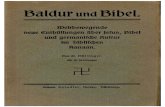
It was then the hypertension of the minimalpressure which we found particularly striking. Wetook care that our experiments were only carriedout upon " athletes in perfect training," for, aswe have pointed out, this hypertension may bediminished or even converted to hypotension inthe case of those who are fatigued or who aresuffering from cardiac insufficiency.Diagram i, which appeared in the Salon of
aeronautics at Paris in 1912, illustrates this pointextremely well. To it we have simply added overthe letters M and P some observations made byCrouzon which were published about the sametime. Though they record MX. pressure only, theystrictly confirm our own observations (fig. i).
Fatigue modifies considerably the vaso-motor
-
8/6/2019 1920 airsicknessitsna00crucuoft
52/120
THE AETIOLOGY OF AIR SICKNESSObservations made upon airmen (b) before and
(a) after flight.
120noIOO90807060
ofHJLz\2019IS17161514J312II1098765432I
At moderate a/t/'iuctesf/,2OO to 2,5OO metres)
L M N M P
At /owa/titudes /SOto 4OOmetres
By C 6rPulse rate. **+ Pulse rate (b)assumedWb Arteria/ pressure in Cm ofHg (Mtnfsn*)CD "/ " " (Maxima)
FIG. I.This diagram shows clearly (#) the increase of Mn.
pressure on landing. These figures were taken in Sep-tember, 1910, at Bordeaux on the following well-knownairmen : Legagneux (L), Leon Morane (M and N), NavalLieut. Byasson (By), Lieut. Cammermann (C), Juilleret(J), Bre*gi (Br). In the case of the latter only Mn. pres-sure is decreased as a result of an attack of faintness.The figures for Mahieu (M) and Paumier (P), recordedin March, 1912, by Dr. Crouzon, are only concerned withthe MX. pressure, which was markedly increased.
-
8/6/2019 1920 airsicknessitsna00crucuoft
53/120
ARTERIAL HYPERTENSIONreactions, the mechanical conditions of the circu-lation and the contracting power of the myocar-dium. The conclusions of certain authors areopen to criticism in that normal subjects have beencompared with fatigued and the MX. pressure onlyhas been considered, the value of the Mn. pressurebeing omitted from the observation. It 'is inter-esting to take up again the study of this hyper-tension considered in the light of literature whichhas appeared since the war.
Since 1913 we have had the assistance of M.Ferry, a resident physician of Nancy Hospital, atthat time auxiliary physician to the aviation centreof Epinal. At our request he took up our re-search, confirmed our observations, and was ableto measure changes of pressure during the courseof flight so as to have a complete record. M. Ferryset to work and we give below the extremely in-teresting results which he obtained at that timeand which he has been able to confirm during thewar. 1
In order that these results may be compared withour own diagrams, we have tabulated them in thesame v/ay. We thus obtain fig. 2.In comparing this figure with our own results{fig. i), we observe that the latter are amply con-firmed. We find that the changes in MX. pressureare of little importance and that at low altitudesthis even tends to be lowered.But the hypertension of the Mn. pressure whichalone indicates the true state of the heart, is of1 J. G. Ferry : " Le syndrome mal des aviateurs,"Presse medicate, February 14, 1916, pp. 65-67. See alsoanother article by the same author on the same subject,These Nancy, J. B. Bailliere et Fils, 1917.
33
-
8/6/2019 1920 airsicknessitsna00crucuoft
54/120
THE AETIOLOGY OF AIR SICKNESSfar greater importance. In this respect Ferry'sobservations confirm our own.Observations made upon F. (b) before, (d) during and
(a) after flight.
120no0090807060
Ata/tittscresf2,OOOto 2,5OOmetres)
Ata/titucfes f60Oto 1,250metres.
JF.3 FUIi
11
r.n
W& Arter/'af pressure in CmFIG. 2.
This diagram shows the pressure changes MX. and Mn.not only before (b) and after flight on landing (
-
8/6/2019 1920 airsicknessitsna00crucuoft
55/120
FATIGUEIf we compare the pressure before flight (b) with
that after (a), the hypertension is clearly shown.If we compare the pressure during flight (d) withthe pressure on landing (a), hypertension is stillmore marked.This hypertension during rapid descent is in our
opinion of the greatest importance.Our diagram of Br (fainting attack) is strictlycomparable to that of Ferry, who had two faintingattacks in the course of a rapid spiral descent.In this case there is hypotension both of MX. andMn. MX. in the case of Ferry shows a tendencyto recover if the point (d) be compared with point(a). But actually at (a) it shows a decrease incomparison with (b).We therefore conclude that arterial hypertension,particularly of the Mn. pressure, during rapiddescent and following upon a hypotension of thesame pressure during the ascent, is a normalreaction in the airman.We must now discuss this factor in relation toothers, amongst which the most important arefatigue, cold, mental strain, emotion and speed.
Fatigue. There are those who believe that thefactor of fatigue, mental as well as physical, is offundamental importance. They liken disturbancesoccurring in airmen to those experienced byathletes in the course of various tests of endurance,such as horse-riding, motor-racing, cycling andflat-racing.At times when fighting was severe, pilots were seen
returning in rough weather to the landing ground, havingfinished their work, and a few seconds afterwards theyappeared incapable of the effort necessary to land theirmachines, which were broken in the shock of contact with
35
-
8/6/2019 1920 airsicknessitsna00crucuoft
56/120
THE .ETIOLOGY OF AIR SICKNESSthe earth. Air "sickness has nothing to do with these cases.It is simply a question of many being tired out by too hardwork. lDoubtless fatigue makes it possible for disturb-ances to appear at much lower altitudes than theydo in climbing or balloon ascents; it cannot, how-ever, explain the arterial hypertension which hasbeen observed; in fact experiments of this kindcarried out on athletes result in an arterial hypo-tension at the first sign of fatigue. This fact, whichcontroverts the statements attributed to Bleriot andDr. Bregi, has been demonstrated by Pachon andis clearly shown in the case of footballers, as wefound during the winter 1910-1911 in the course ofsome hitherto unpublished researches. In the caseof airmen hypertension at least of the minima hasbeen our invariable observation.Let us in the first place determine precisely bywhat means we are able to recognize fatigue. 2Criteria of Fitness. It is less simple than one
might think to estimate fatigue. Many people whocomplain of being tired are less exhausted thanthey say, and on the other hand, there are otherswho in reality are more fatigued than they think.In fact fatigue is largely a subjective sensationa sensation which we try to express in phraseswhich are neither precise nor capable of com-parison. The same thing is true of fatigue as of
1 UIllustration, loc. cit. The author is quite right insaying that air-sickness and fatigue are not the samething. But how can he prove that fatigue alone is inquestion in the cases which he reports? Fatigue by itselfcoming on a few seconds before landing, is a far lesssatisfactory explanation of the fall than is a suddenphysiological disturbance which carries away the reservestrength, the last remaining resource of the airman.2 See the Petite Gironde, May 19, 1914.
36
-
8/6/2019 1920 airsicknessitsna00crucuoft
57/120
FATIGUEpain, that it is a quality which varies with eachindividual, and that so long as we confine ourattention to the information provided by the sub-ject himself, we cannot measure doses of fatiguein mathematical terms. One will answer us that heis completely knocked up, when a careful physio-logical examination shows that he is very far fromcollapse. Another and this happens daily amongmany of our modern athletes will pretend that ahard game of football and a long cycle ride leavehim at the end as fresh as he was at the beginning,whereas his heart-sounds, his pulse-rate and therecord of his arterial pressure enable us to diagnoseindisputable fatigue.
It is therefore necessary to resort to scientificmethods in which the personal element is not in-volved. Thus we have turned successively toexaminations of the cardiac muscle and its pulsa-tions, and to the minute study of the results ofurine analysis. But the information derived fromthese studies was not sufficient to enable us toassign to each individual under consideration thequantity of work which he might accomplishwithout overtiring himself.
In his 1910 memoir Pachon solved this difficultproblem in the following way. 1 It is known, hesays, that the distress of an organism in bad train-ing is due to reactions associated with the heart andthat it is in this quarter that pathological resultsare likely to follow an ill-considered strain. Thequestion then is how to track the origin of this
1 Societe de Biologie, May, 1910. See also : AntoineLe*ger, " Contribution a Petude du critere oscillometriqueconside're comme critere d'entrainement en educationphysique," These de Bordeaux. March 27, 1014.
37
-
8/6/2019 1920 airsicknessitsna00crucuoft
58/120
THE ETIOLOGY OF AIR SICKNESSreaction of cardiac distress. With this end in viewour eminent colleague selected two subjects, theone in training for a life of physical activity, theother untrained and accustomed to a sedentaryexistence. He made them go through the sameexercise for three minutes and observed in the case
1
-
8/6/2019 1920 airsicknessitsna00crucuoft
59/120
FATIGUEoscillometric test which enables us to estimate thepower of adaptation of any individual to a givenexercise.This may be seen in the graph shown in fig. 3.The figures were obtained from a subject in train-
ing well adapted to the work which he carriedthrough; and the pressures, especially the maxima,are seen to rise under the influence of muscularexertion. This is what Pachon calls the workingvalue, which expresses the work done by the heartin response to the demands made upon it by thecalling into action of large groups of muscles. Forsome time the pressures remain at this same height,constituting the work plateau, that is to say, thecondition of adaptation to exercise of the individual.In the example illustrated by this figure, the plateauis maintained throughout the duration of musculareffort, thereby proving the absence of fatigue andthe perfect training of the subject whose pressurevalues return almost to their previous position.Let us now see what happens in the untrainedindividual when fatigue makes itself felt. Thesame result will follow when he is overtrained orwhen he has continued his exertions beyond thelimits of his physiological endurance (see fig. 4).
Here, as in the previous case, the pressures areseen to rise in the first instance up to the levelof the work plateau, but in this case the plateaumaintains its level for a short time only. After aninterval of about five minutes (this interval naturallyvaries in different cases) a fall of pressure chieflyin the maxima indicates the failing of a heartinadapted to exertion. It is this diminution ofarterial pressure which Prof. Pachon has describedby the expressive phrase of danger signal. It is
39
-
8/6/2019 1920 airsicknessitsna00crucuoft
60/120
THE AETIOLOGY OF AIR SICKNESSthe indication for stopping exercise, for it immedi-ately precedes the moment when fatigue is shownin an objective manner, whether or not it isperceived subjectively.
If in spite of this danger signal the individualpersists in his ex-ertions, he overworks his heart
1
-
8/6/2019 1920 airsicknessitsna00crucuoft
61/120
FATIGUEgraph in fig. 4 that twenty-five minutes after ceasingexercise the arterial pressure still remains abnormal.Let us now apply this oscillometric test oftraining, which consists in the systematic study ofarterial pressure variations and the results of whichcan be expressed diagrammatically, and in the firstplace let us consider the results obtained from aseries of Swedish exercises (fig. 5).The values expressed diagrammaticaliy over theletter N are the same as those which are repre-
sented graphically in fig. 3, and similarly thediagram P corresponds to the graph in fig. 4. N istrained. P is fatigued.The same results appear in the bicycle race.L shows adaptation throughout a race of 36 milesof good road, the MX. pressure increasing with theeffort necessary to climb two hills (d and d1).
S, aged 23, shows failure of adaptation. Over20 miles of hilly road between Bordeaux andLibourne both MX. and Mn. pressure show atendency to fall. Even during a period of exertionthey fall (at d) below the original pressure (b) andgive way to a still greater extent after the race (a).At the same time the oscillations show a diminutionof amplitude.The same results appear again in the exercise ofcarrying wood upstairs. (The subject of this experi-ment went up sixty-four steps in three stages.)L shows temporary adaptation, followed by lossof adaptation, the MX. and Mn. pressures (at r) hav-
ing fallen below their original value (at b). Theoscillations are small.
Strictly analogous were the results obtained fromflat races (fig. 6).On May 12, 1912, the celebrated athlete Bouin,
-
8/6/2019 1920 airsicknessitsna00crucuoft
62/120
THE AETIOLOGY OF AIR SICKNESSObservations made (b) before, (d, d') during, (a) after and
(r) at rest in the course of Swedish exercises, bicyclerace and climbing stairs with a load of wood.
\ZQ
10090807060
CmofSL22212019181716i51413\ZI I
509Q7e5432I
dd'
s 4
tycte
ateWM Arteri&J pressure in Cm of Hg (Mj'n/ma)C3 " " (May/ma)FIG. 5. (After Leger.)In Swedish exercises N is in perfect training since
pressure MX. and Mn. increase during exercise (d, d1 ), andreturn after exercise (at a and r} to their original value (b).P shows failure of adaptation, pressures at d' and a beingbelow that of b.Bicycle race. L shows adaptation, whilst S showsfailure of adaptation.Climbing stairs with weight. L shows temporary adapta-
tion only. 42
-
8/6/2019 1920 airsicknessitsna00crucuoft
63/120
Observations made (b) before, (d, d') during and (a, a')after a flat race and gymnastic exercises.
1140130120I 10too90807060
of Flat race
A, n6 ''
Bo Bon l\ Lf
Gymnastic exercise
L1 L2 13Pulse rateEH Arterial pressure in Cm of rig (Minima)
{~~} /> v (Maxima)FIG. 6.
. The failure of adaptation in this diagrambetrays a very evident fatigue. Bo represents the cele-brated flat racer Bouin, whom we examined at Bordeauxon May 12, 1912. He was at that time engaged in a raceover 5i miles with three competitors running in relays.It is worthy of remark that Bouin, who won the race in28' 37 4-5", is no more fatigued than his competitors. Heis even less fatigued than Lafue (Lf).Gymnastic exercises. Dr. Leger (Bordeaux Thesis,1914) shows adaptation to the strain in Li, since the pres-sures, particularly the Mn., return after a to their valueat b. Failure of adaptation is shown in L2 (d1 ), and isstill more clearly manifest in L$ (d1 and particularly a}.It is also shown in S.
43
-
8/6/2019 1920 airsicknessitsna00crucuoft
64/120
THE AETIOLOGY OF AIR SICKNESSracing at the Bordelais University Athletic Club,ran over 5^ miles against a team of three in relays.H-e ended a good first from a magnificent spurtagainst a fourth runner who had only the last lapto run against him. Each of the previous threerunners were also beaten in succession.
This diagram is the more remarkable in that itshows Bouin to be in the best condition at thefinish, despite the effort which he had furnished.There is, nevertheless, a slight diminution of pres-sure.The 5J miles (8'8 kil.) were covered in 28' 37 4-5",
the last J mile in 61 seconds. Bouin was 23\ years,his competitors were as follows : Bonnafond, 38years; Lacombe, 27 years; Lafue, 22 years.Each of the last three runners show markedfailure of adaptation. The heart volume was in-
creased, the pulse compressible, the first heart soundprolonged. Undoubtedly the heart was fatigued ineach of these cases.Again the same observations were made in gym-
nastic exercises (fig. 6).L marched 660 yards au pas gymnastique 1 onehour after the evening meal in cold, fine weather.The ground was level, except for the last 100 yardswhich was steeply inclined. The time taken was15 minutes. The first diagram shows adaptation.Oscillations 3 4 3. In the second case 3,500 yardswere covered in 20 minutes in two stages of 10minutes each. The limit of adaptation reached,oscillations are weaker: 2 3 2\. In the third case3,300 yards were stepped in 30 minutes six stagesof 5 minutes each. This case shows definite failure
1 At the double with knees raised.44
-
8/6/2019 1920 airsicknessitsna00crucuoft
65/120
UP!
FATIGUEof adaptation and even weaker oscillations :2 2j ij.S also shows failure of adaptation. He coveredi,800 yards in 10 minutes and then after 10 minutesof rest 330 yards farther.
Similar observations were made on a Rugbyfootball team. We made more than 100 observa-tions, nearly all during the season 1910-1911, whenone of us (R. Cruchet) was a member of the RugbyCommittee of the Bordelais University AthleticClub, and regularly observed the players. Theywere kept in perfect training up to the last matchwhich they won and with it the championship ofFrance. That was the year of what was called the
' Virgin Team," for they did not sustain a singledefeat.We have selected for our diagrams the mostcharacteristic results.
In the first place we give examples of untrainedindividuals (fig. 7).
(1) Referees. H represents Hutchinson, theofficial referee, aged 40. His curve, taken onNovember 10, 1910, shows a complete absence oftraining. Williams is a celebrated English refereewho came to Bordeaux for the famous game againstthe South Africans on January n, 1913. There isevident want of training in this case also, thoughit is less pronounced than in the former case.
(2) Players. An examination was held at thebeginning of the football season (1910) when lackof training was obvious. The observations weremade on Brachet (age 24), Canton (age 24), Laffitte(age 27), Monier, Martin, Droz (age 29), Jameton(age 25). In the case of Martin the examination
45
-
8/6/2019 1920 airsicknessitsna00crucuoft
66/120
THE .ETIOLOGY OF AIR SICKNESSObservations made on footballers (b) before and (a) aftera game.
-
8/6/2019 1920 airsicknessitsna00crucuoft
67/120
FATIGUEwas made after a hard game and one of the firstin which he had played.
(3) Captains. Leuvielle was the French captainand Millar captain of the South Africans in thematch of January n, 1913. Both players showslight hypotension. The game had been hardlycontested and both were beginning to feel fatigued.
Fig. 8 shows training in progress. Fig. 9 theteam of the Bordeaux Club already referred to onthe day (April 9, 1911) on which they won theChampionship of France.The same reactions were observed in the courseof swimming races (fig. 10). In the speed race thetemperature of the water was 17 C. Pierre T.swam the 100 metres in i ; 40". The increasedpressure occurred only in the course of the effortor immediately after coming out of the water.One hour after the race the pressure had returnedto normal.Four days later the same swimmer covered
the same distance in i' 32". Immediate!/ afterthe race the pressure had risen from 16 to 22.One hour afterwards it was 21, two hours after-wards 19, three hours afterwards 17, five hoursafterwards it returned to normal. In this caseadaptation is perfect.Lecam swam 400 metres on October 4, 1910.The temperature of the water was then 9 C.He covered the distance in 7' 29". The MX.pressure rose from 18 to 23 during the race andreturned to 18 four hours afterwards. Lecamstates 1 that at a temperature of 22 to 25 C. onecan stand immersion for a considerable time. At
1 Lecam : " De la natation au point de vue medical,"(These de Bordeaux, July, 191 1).47
-
8/6/2019 1920 airsicknessitsna00crucuoft
68/120
THE ETIOLOGY OF AIR SICKNESSObservations made on the same footballers (b) before and
(a) after a game, showing the effect of training andovertraining.
1201 1010090807060
/ // nihf3hfy 2V ^untrained in training trained overtrained
iBo I II HI Bey I II III CI II IIIe Pu/se rateW3h Arter/'&J pressure in Cmm' r> v >'
P J II IV
(Minims)
FIG. 8.Three members of the team reached the end of the
season in good condition. One (Perrens) was overtrained.Observations were taken on the following dates :Boyau Dec. 4, 1910 March 12, 1911 Ap*il 9, 1911De Beyssac Dec, 11, 1910 Jan. 14, ion April 9, 1911Canton Dec. 4, 1910 Feb. 19, 1911 April 9, 1911(Boyau is the celebrated airman who disappeared in thecourse of the war. Conilh de Beyssac, also a well-known
sportsman, was killed on his tank in action in 1918.)
-
8/6/2019 1920 airsicknessitsna00crucuoft
69/120
FATIGUE ""'^Observations made on footballers (b) before and (a) aftera Rugby Football Championship Final. The resultsshow the fine condition of the players.
j:120110100do6070