3 MedArt Case Trendelenburg - unispital-basel.ch · pathway activation is important in...
28
Marten Trendelenburg Stv. Chefarzt / Klinik Innere Medizin STURZABKLÄRUNG
Transcript of 3 MedArt Case Trendelenburg - unispital-basel.ch · pathway activation is important in...

MartenTrendelenburgStv.Chefarzt/KlinikInnereMedizin
STURZABKLÄRUNG

77jährigerPatient- Anamnese
¨ PatientkommtvonzuHause.¨ 17:30vonEhefrauaufFussboden vorgefunden(Sturzereigniss unklar).Patientberichtete,erhabezuHausebeihäuslichenTätigkeitendasGleichgewichtverlorenundseirückwärtsauf‘s KreuzunddenRückengefallen.KeinSchwindel,keineBewustlosigkeit.
¨ AllgemeinzustandsverschlechterungundKraftlosigkeitseiteinpaarTagen.
¨ HustenmitAuswurfseit2Tagen,amEintrittstagangeblichFieber.
¨ HäufigesWasserlösenmitHarndrangseit2Monaten.

77jährigerPatient- Vorgeschichte
¨ LeichtesdementiellesSyndrom¤ 1x/Woche(Eintrittstag)inTagesstättedesFelix-Platter-Spitals
¨ UnklareGangstörung¤ keinHinweisaufeineneurodegenerativeErkrankungimPET/CT10Monatevorher(AbklärungviaNeurologie)
¨ SubakuterNSTEMIbeikoronarer2-AstErkrankung2009
¨ ArteriellerHypertonus¨ St.n.Subarachnoidalblutung undKontusionsblutungennachSturzunklarerUrsache2003

77jährigerPatient- Medikamente
¨ Pantoprazol 40mgTbl.1-0-0¨ Amlodipin 5mgTbl.1-0-0¨ Simvastatin40mgTbl.0-0-1/2¨ Aspirincardio 100mgTbl.1-0-0¨ VitaminD3Tropfen(wieviel?)

77jährigerPatient- Status
¨ LeichtreduzierterAllgemeinzustand¨ Notfallstation:
¤ Temperatur38.0°C,Blutdruck164/85mmHg,Puls100/min,Sättigung95%ohneO2,GCS15,Atemfrequenz22/min
¤ LeichtezeitlicheundörtlicheDesorientiertheit¤ KörperlicheSchwäche; wirdoffensichtlichbeimAufsitzen/Aufstehen
¤ Gesichtleichtgerötet,leichteSchmerzensakralunduntereBWS
¤ Keinefokal-neurologischenAusfälle¤ InternistischerStatussonstunauffällig

77jährigerPatient- Diagnostik
¨ EKG:Grenzwertigtachykarder Sinusrhythmus¨ RöntgenThorax:KeineAuffälligkeiten¨ Labor:
¤ VenöseBlutgasanalyse:Unauffällig¤ Kreatinin,Elektrolyte,Leberwerte:Normwertig¤ CRP21.5mg/l(Normbis10)¤ LDH393U/l(Normbis225),CK436U/l(50-200)¤ Leukozyten:12.78x109/l(10.99Neutrophile),Lymphozyten0.831x109/l,Hämoglobin181g/l,Thrombozyten327x109/l
¤ Urinstatus:Unauffällig

1. Austritt(keineweiterenAbklärungen)
2. BeginnAntibiotikum(empirischbeiInfektzeichenohneklarenFokus,DDpulmonal)
3. Infusion(HydrierungbeiV.a.Exsikkose)
4. WeitereDiagnostik
5. Punkt2und3
20%
20%
20%
20%
20%
StandardWastun?
020 000

WeitereDiagnostik
¨ CTSchädel:KeineintrakranielleBlutung.Alte,demarkierteInfarktarealeinbeidenMediastromgebieten.FleckigeLeukenzephalopathie, amehestenvaskulärbedingt.
¨ RöntgenBeckenübersicht,Ossacrum,Brustwirbelsäule:KeinHinweisaufFraktur

1. Austritt
2. BeginnAntibiotikum(empirischbeiInfektzeichenohneklarenFokus)
3. Infusion(HydrierungbeiV.a.Exsikkose)
4. WeitereDiagnostik
5. Beobachten
20%
20%
20%
20%
20%
StandardWastun?
020 000

InfusionundstationäreAufnahmemitfolgendemAuftrag:
¨ ErneuteLaborkontrolle:BeierneutemFieber/CRP-Anstiegevtl.Antibiotikaevaluieren
¨ AnmeldungPhysiotherapie¨ JenachneurologischerEvaluation,weiteresProcederediskutieren
¨ ggf.DemenzabklärungimVerlauf

Laborkontrolle
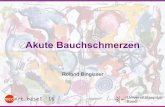
¨ Kreatinin,Elektrolyteunauffällig¨ CRP85.7mg/l(steigend)¨ CK830U/l(50-200),CK-MB-Masse5.4µg/l(<5.0),LDH366U/l(135-225)
¨ Leukozyten9.04x109/l¨ Hämoglobin186g/l,Hämatokrit0.57l/l,MCV101fl(Normbis95)
¨ Thrombozyten322x109/l¨ VitaminB12undErythrozyten-Folsäurenormwertig¨ RestimWesentlichenunauffällig,keineHypoxämie

1. Patienterneutanschauen(Volumenstatus?),Trink(Fremd-)anamnese
2. BeginnAntibiotikum(empirischbeiInfektzeichenohneklarenFokus)
3. Infusion(HydrierungbeiV.a.Exsikkose)
4. Aderlass(Hämatokrit57%)
5. Alles
20%
20%
20%
20%
20%
StandardWastun?
020 000

Alles,nurkeinAntibiotikum…
¨ Volumenstatus:Klinischeuvoläm¨ Fremdanamnese(Ehefrau):Patienttrinktsehrwenig(seitca.1Jahrca.0.5l/Tag),daherweitermitInfusion
¨ Isovolämer Aderlass(V.a.neurologischeVerschlechterungbeiHkt >55%ohneZeichenderHypoxämie)
¨ AbklärungPolyglobulie

DifferentialdiagnosederPolyglobulie
¨ Exsikkose/Diuretika¨ ChronischeHypoxämie(Lungenerkrankungen,rechts-linksShunt,Schlafapnoe,Adipositas-Hypoventilationssyndrom,grosseHöhe,…)
¨ Androgene,anaboleSteroide¨ Doping(Epo)¨ Erythropoietin-produzierendeNeoplasien (Nierenzell-,Hepatozelluläres Karzinom,…)
¨ Erythropoietin-produzierendeNierenläsionennachTransplantation
¨ Knochenmarkserkrankungen(PrimärePolyglobulie,z.B.Polycythämia vera)

Abklärungen
¨ KeineverdächtigenMedikamente/Dopingetc.¨ Polyglobulie persistierttrotzInfusion,Trinkaufforderung,klinischEuvolämie
¨ SauerstoffsättigungauchunterBelastunggut,UnauffälligearterielleBlutgasanalyse,Lungenfunktionunauffällig
¨ Ultraschall-Abdomen:KeineHepatosplenomegalie,Nierenunauffällig,keineRaumforderungen(guteUntersuchungsbedingungen)
¨ Erythropoietin:2.6U/l(Norm4.3- 29.0)

Verdachtsdiagnose
Myeloproliferative Neoplasie vomTypPolycythämia vera

Polycythämia vera
¨ HäufigsteprimärePolycythämie¨ TeilderPhiladelphia-Chromosomnegativenmyeloproliferativen Neoplasien
¨ Amhäufigsten(>90%)durchJAK2 V617FMutation(erworben)– führtzurErythropoietin-Unabhängigkeitbzw.Hypersensitivität
¨ SeltenandereMutationen(JAK2 exon 12Mutationen,andere)

UnserPatient
¨ FazialePlethora,Hypertension,V.a.gestörteMikrozirkulation(neurologischeSymptome)
Major(WHO2016)¨ Hämoglobin>165g/l,Hämatokrit>49%¨ TypischerKnochenmarksbefund¨ PositivfürJAK2 V617F(Exon 14)und JAK2 Exon 12Mutation
Minor¨ Serum-Erythropoietin 2.6IU/l(Norm4.3-29.0)

TherapieoptionenbeiPolycythämia vera
¨ Ziele:Symptomenkontrolle,Lebensverlängerung
¨ Ziel-Hämatokrit<45%,beiFrauenehernochtiefer
¨ DazuAderlässe(z.B.250-500ml)und/oder¨ Zytoreduktive TherapiebeiHochrisikopatienten(z.B.Hydroxyurea)
¨ NiedrigdosiertesAspirin(Thromboseprävention,aberauchhilfreichbeiJuckreizundErythromelalgie)

0 5 1 0 1 5
1 4 0
1 5 0
1 6 0
1 7 0
1 8 0
1 9 0
2 0 0
0 .4 0
0 .4 5
0 .5 0
0 .5 5
0 .6 0
T a g e
Hä
mo
glo
bin
in g
/l Hä
ma
tok
rit in l/l
H äm og lob in
H äm a tok rit
A d e r lä s s e
Verlauf

‘Takehome messages’
¨ AuchbeiälterenMenschenkanndieSturzabklärungselteneUrsachenhervorbringen.
(Problemderawareness)¨ RelevanzderklinischenBefundenichtunterschätzen(beiunseremPatienten:VolumenstatusundfazialePlethora,aberauchdie(Fremd-)Anamnese!)
¨ Erhobene(Labor-)Befundeansehen(VorteilversusRisikobeiunselektiven «Screenings»).
¨ NichtnurdieAnämie,sondernauch(seltener)diePolyglobulie kanneinProblemsein.


Polycythämia vera – häufigeBefunde
¨ Polyglobulie (Hämoglobin,Hämatokrit)¨ Evtl.Leukozytose,Thrombozytose¨ FazialePlethora¨ Juckreiz(evtl.verschlimmertdurch(warmes)Wasser)¨ Geschichtevonthromboembolischen Ereignissen¨ Gicht¨ Bluthochdruck¨ Splenomegalie¨ Sehstörungen,Kopfschmerzen,Schwindel,…

BegrenzterAderlass
¨ BeiSymptomeninfolgevonerhöhtemBlutvolumenund/oderHyperviskosität.
¨ CavebeiPatientenmitchronischerHypoxämie¨ Initial250ml(isovoläm),sonstbis500ml¨ 500mlsenkendenHämatokritumca.3%¨ TypischeIndikationen:Polycythämia vera,Hämochromatose,Porphyria cutanea tarda

JAK2MPLCALR
EssentialThrombocythemia (ET)
Platelets
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
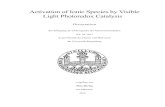
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Myelofibrosis (MF)Bonemarrowfibrosis
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Redbloodcells
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPD Activating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
Platelets Essentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
Eosinophils Chroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
R E V I E W S
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
PolycythemiaVera(PV)
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid progenitor
HSC
MPDActivating mutation
Chronic myeloidleukaemiaChronic myelomonocyticleukaemiaPrimarymyelofibrosis
Mast cell
Systemicmastocytosis
KITD816VFIP1L1–PDGFRA
Red blood cells
Polycythaemiavera
JAK2V617FJAK2 Exon 12
PlateletsEssentialthrombo-cythaemia
JAK2V617FMPLW515L/K
JAK2V617FMPLW515L/K
EosinophilsChroniceosinophilicleukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRBBCR–PDGFRATEL–JAK2other fusion TKs
LeucopaeniaLow white blood cell count.
ErythrocytosisIncreased red blood cell count.
In vitro studies demonstrate that the expression of JAK2V617F activates multiple downstream signalling pathways8,36, including the Stat family of transcription factors, the mitogen activated protein kinase (MAPK) signalling pathway, and the phosphotidylinositol 3-kinase (PI3K)–Akt signalling pathway (FIG. 2). Most activated tyrosine kinases that have been identified in human malignancies activate these same signalling cascades, and the role and requirement of the Stat, MAPK and PI3K–Akt signalling pathways in JAK2V617F-mediated transformation of haematopoietic cells has not been fully elucidated. However, several lines of evidence suggest that activation of the Stat family of transcription factors is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or its anti-apoptotic target gene BCL-XL in human haemat-opoietic progenitors results in EPO-independent colony formation37, a hallmark of human PV. Moreover, STAT3 activation and BCL-XL overexpression are observed in most PV patient samples38,39. These data imply that Stat pathway activation is important in JAK2V617F-mediated transformation, but do not indicate whether Stat pathway activation is necessary and/or sufficient for JAK2V617F-mediated transformation. Murine bone marrow trans-plantation (BMT) assays using Stat5a;Stat5b-deficient mice have been used to show that STAT5 is required for haematopoietic transformation by the constitutively active TEL–JAK2 fusion tyrosine kinase40, and future experiments will ultimately determine whether the same is true for JAK2V617F. In addition, the activation of sig-nalling by the JAK2V617F kinase might in part be due to escape from negative-feedback mechanisms important in attenuating JAK2 signalling. Jak activity is negatively regulated by the Socs family of proteins, which normally bind to the Jak kinases and result in their degradation. In particular, SOCS1 and SOCS3 have been shown to bind to JAK2 and inhibit JAK2 catalytic activity41,42, and over-expression of SOCS1 results in abrogation of in vitro and in vivo transformation by TEL–JAK2 (REF. 43). Although expression of SOCS1 results in JAK2 and JAK2V617F deg-radation and inhibition of kinase activity, the expression of SOCS3 paradoxically results in increased JAK2V617F protein stability, increased SOCS3 phosphorylation and increased JAK2V617F phosphorylation44. These data demonstrate that regulation of JAK2 kinase activity by SOCS3 is altered in the context of the V617F substitution, and suggest the possibility that therapeutic inhibition of SOCS3 might selectively attenuate JAK2V617F, but not wild-type JAK2 signalling.
In vivo data from murine BMT experiments have provided important insights into the role of JAK2 activa-tion in the pathogenesis of MPD. James et al. noted that the expression of JAK2V617F, but not wild-type JAK2, in a murine BMT assay results in significant erythrocytosis in recipient mice 28 days after transplantation8,9, and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different myeloproliferative disorders (MPD) can be classified by the predominant terminally differentiated myeloid cell involved in the disorder, and for each terminally differentiated myeloid cell there is a clinically distinct MPD. Different approaches have been used to identify the activating alleles that cause these disorders, and in all cases these alleles result in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature, terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition, although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal involvement of the different haematopoietic lineages111,112.
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia (CML) that arises as a consequence of the 9:22 translocation2, a causative agent for this disease, and recurrent translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B (PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3. The observation that KIT is highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5, and imatinib responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that gives rise to the FIP1L1–PDGFRA fusion4. Most recently, investigators have identified Janus kinase 2 (JAK2) and thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55.
REVIEWS
NATURE REVIEWS | CANCER VOLUME 7 | SEPTEMBER 2007 | 675
Nature Reviews |
Cancer
Neutrophils
Monocytes
Myeloid
progenitor
HSC
MPD
Activati
ng
mutation
Chronic myeloid
leukaemia
Chronic
myelomonocytic
leukaemia
Primary
myelofibrosis
Mast
cell
Systemic
mastocytosis
KITD816V
FIP1L1–
PDGFRA
Red
blood cells
Polyc
ythaemia
vera
JAK2V617F
JAK2 Exo
n 12
Platelets
Essentia
l
thrombo-
cythaemia
JAK2V617F
MPLW515
L/K
JAK2V617F
MPLW515
L/K
Eosin
ophils
Chronic
eosinophilic
leukemia
FIP1L1–
PDGFRA
BCR-ABL
TEL–PDGFRB
BCR–PDGFRA
TEL–JAK2
other fusio
n TKs
Leuco
paenia
Low white
blood cell c
ount.
Erythro
cytosi
s
Increase
d red blood ce
ll count.
In vitro stu
dies dem
onstrate t
hat the e
xpressio
n of
JAK2V617F activate
s multip
le downstre
am sig
nalling
pathways8,36, in
cluding th
e Stat
family of tr
anscriptio
n
factors,
the mito
gen activate
d protein kinase (
MAPK)
signalling path
way, and the p
hosphotidylinositol 3-kinase
(PI3K)–Akt signallin
g pathway (FIG
. 2). M
ost activ
ated
tyrosine kinases th
at have been id
entified in
human
malignancies a
ctivate th
ese sa
me signallin
g casca
des,
and the r
ole and re
quirement o
f the S
tat, M
APK and
PI3K–Akt signalli
ng pathways in
JAK2V617F-m
ediated
transfo
rmatio
n of haemato
poietic ce
lls has n
ot been fully
elucid
ated. H
owever, severa
l lines o
f evidence suggest
that activ
ation of th
e Stat
family of tr
anscription fac
tors
is importa
nt in JA
K2V617F-mediate
d transfo
rmatio
n.
First, ex
pressio
n of either c
onstitutively
active S
TAT5 or
its anti-a
poptotic tar
get gene B
CL-XL in human haem
at-
opoietic p
rogenitors resu
lts in EPO-in
dependent colony
formatio
n37, a
hallmark
of human PV. Moreo
ver, STAT3
activatio
n and BCL-XL
overexpres
sion are
observed in
most PV patie
nt samples
38,39. These data
imply that S
tat
pathway act
ivation is i
mportant in
JAK2V617F-m
ediated
transfo
rmatio
n, but do not indicat
e wheth
er Stat
pathway
activatio
n is nece
ssary an
d/or suffic
ient fo
r JAK2V617F-
mediated tra
nsform
ation. M
urine b
one marr
ow trans-
plantati
on (BMT) assa
ys usin
g Stat5a;Stat5b-deficien
t
mice have b
een used to sh
ow that S
TAT5 is require
d
for haem
atopoieti
c transfo
rmatio
n by the constit
utively
active TEL–JAK2 fu
sion tyrosin
e kinase
40, and future
experiments w
ill ultim
ately dete
rmine w
hether t
he same
is true fo
r JAK2V617F. I
n additio
n, the ac
tivation of si
g-
nalling by the JA
K2V617F kinase might in
part be d
ue to
escape fr
om negative-fe
edback mech
anisms im
portant
in attenuatin
g JAK2 sig
nalling. Ja
k activity is
negatively
regulate
d by the Socs f
amily of protein
s, which
normally
bind to the Jak kinase
s and res
ult in their
degradatio
n. In
particu
lar, SOCS1 an
d SOCS3 have been
shown to bind
to JAK2 an
d inhibit JAK2 cat
alytic
activity
41,42, and over-
expressio
n of SOCS1 results i
n abrogatio
n of in vitro
and
in vivo tra
nsform
ation by TEL–JAK2 (REF. 4
3). Although
expression of SOCS1 res
ults in JA
K2 and JA
K2V617F deg-
radatio
n and inhibitio
n of kinase act
ivity, the ex
pressio
n
of SOCS3 paradoxica
lly results
in increase
d JAK2V617F
protein sta
bility, in
crease
d SOCS3 phosphorylation an
d
increased JA
K2V617F phosphorylation44. T
hese data
demonstra
te that r
egulation of JA
K2 kinase ac
tivity by
SOCS3 is alter
ed in the contex
t of the V
617F substitution,
and suggest
the possib
ility that t
herapeutic
inhibition of
SOCS3 might selec
tively att
enuate JA
K2V617F, but n
ot
wild-type JA
K2 signalli
ng.
In vivo data fro
m murin
e BMT experiments h
ave
provided importa
nt insig
hts into the ro
le of JA
K2 activa-
tion in the path
ogenesis of M
PD. James e
t al. noted
that
the expres
sion of JA
K2V617F, but not w
ild-type JA
K2, in
a murin
e BMT ass
ay results
in signific
ant eryth
rocytosis
in recip
ient m
ice 28 days a
fter tra
nsplantation8
,9, and
Figure 1 | Classi
ficatio
n and molecular p
athogenesis of th
e MPD. The diffe
rent
myeloproliferativ
e disorders (
MPD) can be classified by th
e predominant term
inally
differentia
ted myeloid cell involved in th
e disorder, a
nd for each te
rminally diffe
rentiated
myeloid cell there is a
clinically distinct M
PD. Diffe
rent approaches have been used to
identify th
e activatin
g alleles that cause th
ese disorders,
and in all cases th
ese alleles result
in constitutiv
e tyrosine kinase sig
nalling. H
SC, haematopoietic ste
m cell; JAK2, Ja
nus
kinase 2; MPL, th
rombopoietin receptor; P
DGFR, platelet deriv
ed growth factor receptor.
Box 1 | Myeloprolife
rative dise
ases
Myeloproliferativ
e diseases (M
PD) are proliferativ
e syndromes th
at present w
ith increased numbers o
f functio
nal, mature,
terminally diffe
rentiated myeloid elements.
Thus, in contra
st to im
paired myeloid diffe
rentiatio
n that is
characteristic of
myelodysplastic sy
ndromes (MDS) and acute myeloid leukaemia (A
ML), patie
nts with
MPD ra
rely present with
infectious
complications re
lated to leu
copae
nia, or complicatio
ns related to
anaemia that a
re observed in MDS and AML. In
addition,
although th
ese MPD can be asso
ciated with bleeding te
ndencies (diatheses) t
hat are observed in M
DS and AML owing to
thrombocytosis and platelet d
ysfunctio
n, they are ofte
n associated with
specific
clinical se
quelae that in
clude thrombotic
diatheses that a
re not observed in M
DS or AML. H
owever, MDS and AML are th
ought to be ste
m cell diso
rders, based on
clonality analyses u
sing X-in
activatio
n-based assays in
females o
r cytogenetic
analyses that d
emonstrate th
e clonal
involvement of th
e different h
aematopoietic lin
eages111,112.
The first M
PD allele to
be identified and characteriz
ed was the BCR-ABL fu
sion oncogene in chronic myeloid leukaemia
(CML) that a
rises a
s a consequence of th
e 9:22 translo
cation2, a causativ
e agent for th
is dise
ase, and recurre
nt
translo
cations le
d to th
e discovery of d
ifferent fu
sion ty
rosine kinases, i
ncluding platelet deriv
ed growth factor receptor-B
(PDGFRB) fusio
ns in patie
nts with
chronic myelomonocytic leukaemia (C
MML) and other MPD
3. The observation th
at KIT is
highly expressed in mast c
ells led to
the disc
overy of the KITD816V alle
le in syste
mic mastocytosis
(SM)5, and imatin
ib
responses in patie
nts with
chronic eosinophilic
leukaemia (CEL) and SM led to
the disc
overy of an interstitia
l deletion th
at
gives rise to
the FIP1L1–PDGFRA fu
sion4. M
ost recently
, investig
ators have identifi
ed Janus kinase 2 (JA
K2) and
thrombopoietin re
ceptor mutatio
ns in polycythaemia vera (PV), e
ssentia
l thrombocythaemia (ET) and prim
ary
meylofibrosis
(PMF) that re
sult in th
e activatio
n of JAK2 sig
nalling8
–11,53,55.
REVIEW
S
NATURE REVIEWS | CANCER
VOLUME 7 | SEPTEMBER 2007 | 6
75
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid
progenitor
HSC
MPD
Activating
mutation
Chronic myeloid
leukaemia
Chronic
myelomonocytic
leukaemia
Primary
myelofibrosis
Mast
cell
Systemic
mastocytosis
KITD816V
FIP1L1–PDGFRA
Red
blood cells
Polycythaemia
vera
JAK2V617F
JAK2 Exon 12
Platelets
Essential
thrombo-
cythaemia
JAK2V617F
MPLW515L/K
JAK2V617F
MPLW515L/K
Eosinophils
Chronic
eosinophilic
leukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRB
BCR–PDGFRA
TEL–JAK2
other fusion TKs
Leucopaenia
Low white blood cell count.
Erythrocytosis
Increased red blood cell count.
In vitro studies demonstrate that the expression of
JAK2V617F activates multiple downstream signalling
pathways8,36 , including the Stat family of transcription
factors, the mitogen activated protein kinase (MAPK)
signalling pathway, and the phosphotidylinositol 3-kinase
(PI3K)–Akt signalling pathway (FIG. 2). Most activated
tyrosine kinases that have been identified in human
malignancies activate these same signalling cascades,
and the role and requirement of the Stat, MAPK and
PI3K–Akt signalling pathways in JAK2V617F-mediated
transformation of haematopoietic cells has not been fully
elucidated. However, several lines of evidence suggest
that activation of the Stat family of transcription factors
is important in JAK2V617F-mediated transformation.
First, expression of either constitutively active STAT5 or
its anti-apoptotic target gene BCL-X L in human haemat-
opoietic progenitors results in EPO-independent colony
formation37 , a hallmark of human PV. Moreover, STAT3
activation and BCL-X L overexpression are observed in
most PV patient samples38,39 . These data imply that Stat
pathway activation is important in JAK2V617F-mediated
transformation, but do not indicate whether Stat pathway
activation is necessary and/or sufficient for JAK2V617F-
mediated transformation. Murine bone marrow trans-
plantation (BMT) assays using Stat5a;Stat5b-deficient
mice have been used to show that STAT5 is required
for haematopoietic transformation by the constitutively
active TEL–JAK2 fusion tyrosine kinase40 , and future
experiments will ultimately determine whether the same
is true for JAK2V617F. In addition, the activation of sig-
nalling by the JAK2V617F kinase might in part be due to
escape from negative-feedback mechanisms important
in attenuating JAK2 signalling. Jak activity is negatively
regulated by the Socs family of proteins, which normally
bind to the Jak kinases and result in their degradation. In
particular, SOCS1 and SOCS3 have been shown to bind
to JAK2 and inhibit JAK2 catalytic activity41,42 , and over-
expression of SOCS1 results in abrogation of in vitro and
in vivo transformation by TEL–JAK2 (REF. 43). Although
expression of SOCS1 results in JAK2 and JAK2V617F deg-
radation and inhibition of kinase activity, the expression
of SOCS3 paradoxically results in increased JAK2V617F
protein stability, increased SOCS3 phosphorylation and
increased JAK2V617F phosphorylation44 . These data
demonstrate that regulation of JAK2 kinase activity by
SOCS3 is altered in the context of the V617F substitution,
and suggest the possibility that therapeutic inhibition of
SOCS3 might selectively attenuate JAK2V617F, but not
wild-type JAK2 signalling.
In vivo data from murine BMT experiments have
provided important insights into the role of JAK2 activa-
tion in the pathogenesis of MPD. James et al. noted that
the expression of JAK2V617F, but not wild-type JAK2, in
a murine BMT assay results in significant erythrocytosis
in recipient mice 28 days after transplantation8,9 , and
Figure 1 | Classification and molecular pathogenesis of the MPD. The different
myeloproliferative disorders (MPD) can be classified by the predominant terminally
differentiated myeloid cell involved in the disorder, and for each terminally differentiated
myeloid cell there is a clinically distinct MPD. Different approaches have been used to
identify the activating alleles that cause these disorders, and in all cases these alleles result
in constitutive tyrosine kinase signalling. HSC, haematopoietic stem cell; JAK2, Janus
kinase 2; MPL, thrombopoietin receptor; PDGFR, platelet derived growth factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (MPD) are proliferative syndromes that present with increased numbers of functional, mature,
terminally differentiated myeloid elements. Thus, in contrast to impaired myeloid differentiation that is characteristic of
myelodysplastic syndromes (MDS) and acute myeloid leukaemia (AML), patients with MPD rarely present with infectious
complications related to leucopaenia, or complications related to anaemia that are observed in MDS and AML. In addition,
although these MPD can be associated with bleeding tendencies (diatheses) that are observed in MDS and AML owing to
thrombocytosis and platelet dysfunction, they are often associated with specific clinical sequelae that include thrombotic
diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem cell disorders, based on
clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that demonstrate the clonal
involvement of the different haematopoietic lineages111,112 .
The first MPD allele to be identified and characterized was the BCR-ABL fusion oncogene in chronic myeloid leukaemia
(CML) that arises as a consequence of the 9:22 translocation2 , a causative agent for this disease, and recurrent
translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B
(PDGFRB) fusions in patients with chronic myelomonocytic leukaemia (CMML) and other MPD3 . The observation that KIT is
highly expressed in mast cells led to the discovery of the KITD816V allele in systemic mastocytosis (SM)5 , and imatinib
responses in patients with chronic eosinophilic leukaemia (CEL) and SM led to the discovery of an interstitial deletion that
gives rise to the FIP1L1–PDGFRA fusion4 . Most recently, investigators have identified Janus kinase 2 (JAK2) and
thrombopoietin receptor mutations in polycythaemia vera (PV), essential thrombocythaemia (ET) and primary
meylofibrosis (PMF) that result in the activation of JAK2 signalling8–11,53,55 .
REVIEWS
NATURE REVIEWS | CANCER
VOLUME 7 | SEPTEM
BER 2007 | 675
Nature Reviews | Cancer
Neutrophils
Monocytes
Myeloid
progenitor
HSC
MPD
Activating
mutation
Chronic myeloid
leukaemia
Chronic
myelomonocytic
leukaemia
Primary
myelofibrosis
Mast
cell
Systemic
mastocytosis
KITD816V
FIP1L1–PDGFRA
Red
blood cells
Polycythaemia
vera
JAK2V617F
JAK2 Exon 12
Platelets
Essential
thrombo-
cythaemia
JAK2V617F
MPLW515L/K
JAK2V617F
MPLW515L/K
Eosinophils
Chronic
eosinophilic
leukemia
FIP1L1–PDGFRA
BCR-ABL
TEL–PDGFRB
BCR–PDGFRA
TEL–JAK2
other fusion TKs
Leucopaenia
Low white blood cell count.
Erythrocytosis
Increased red blood cell count.
In vitro studies demonstrate that the expression of
JAK2V617F activates m
ultiple downstream signalling
pathways
8,36 , including the Stat family of transcription
factors, the mitogen activated protein kinase (M
APK)
signalling pathway, and the phosphotidylinositol 3-kinase
(PI3K)–Akt signalling pathw
ay (FIG. 2). Most activated
tyrosine kinases that have been identified in human
malignancies activate these sam
e signalling cascades,
and the role and requirement of the Stat, M
APK and
PI3K–Akt signalling pathw
ays in JAK2V617F-mediated
transformation of haematopoietic cells has not been fully
elucidated. However, several lines of evidence suggest
that activation of the Stat family of transcription factors
is important in JAK2V617F-mediated transform
ation.
First, expression of either constitutively active STAT5 or
its anti-apoptotic target gene BCL-XL in human haemat-
opoietic progenitors results in EPO-independent colony
formation
37 , a hallmark of human PV. Moreover, STAT3
activation and BCL-XL overexpression are observed in
most PV patient samples38,39 . These data im
ply that Stat
pathway activation is important in JAK2V617F-mediated
transformation, but do not indicate w
hether Stat pathway
activation is necessary and/or sufficient for JAK2V617F-
mediated transform
ation. Murine bone marrow trans-
plantation (BMT) assays using Stat5a;Stat5b-deficient
mice have been used to show
that STAT5 is required
for haematopoietic transform
ation by the constitutively
active TEL–JAK2 fusion tyrosine kinase
40 , and future
experiments will ultimately determine whether the sam
e
is true for JAK2V617F. In addition, the activation of sig-
nalling by the JAK2V617F kinase might in part be due to
escape from negative-feedback m
echanisms important
in attenuating JAK2 signalling. Jak activity is negatively
regulated by the Socs family of proteins, w
hich normally
bind to the Jak kinases and result in their degradation. In
particular, SOCS1 and SOCS3 have been show
n to bind
to JAK2 and inhibit JA
K2 catalytic activity41,42 , and over-
expression of SOCS1 results in abrogation of in vitro and
in vivo transformation by TEL–JA
K2 (REF. 43). Although
expression of SOCS1 results in JAK2 and JAK2V
617F deg-
radation and inhibition of kinase activity, the expression
of SOCS3 paradoxically results in increased JA
K2V617F
protein stability, increased SOCS3 phosphorylation and
increased JAK2V617F phosphorylation
44 . These data
demonstrate that regulation of JA
K2 kinase activity by
SOCS3 is altered in the context of the V
617F substitution,
and suggest the possibility that therapeutic inhibition of
SOCS3 might selectively attenuate JA
K2V617F, but not
wild-type JAK2 signalling.
In vivo data from murine BMT experiments have
provided important insights into the role of JA
K2 activa-
tion in the pathogenesis of MPD. James et al. noted that
the expression of JAK2V617F, but not w
ild-type JAK2, in
a murine BMT assay results in significant erythrocytosis
in recipient mice 28 days after transplantation
8,9 , and
Figure 1 | Classification and m
olecular pathogenesis of the MPD. The different
myeloproliferative disorders (M
PD) can be classified by the predom
inant terminally
differentiated myeloid cell involved in the disorder, and for each term
inally differentiated
myeloid cell there is a clinically distinct M
PD. Different approaches have been used to
identify the activating alleles that cause these disorders, and in all cases these alleles result
in constitutive tyrosine kinase signalling. HSC, haematopoietic stem
cell; JAK2, Janus
kinase 2; MPL, thrombopoietin receptor; PD
GFR, platelet derived grow
th factor receptor.
Box 1 | Myeloproliferative diseases
Myeloproliferative diseases (M
PD) are proliferative syndrom
es that present with increased num
bers of functional, mature,
terminally differentiated m
yeloid elements. Thus, in contrast to im
paired myeloid differentiation that is characteristic of
myelodysplastic syndrom
es (MDS) and acute m
yeloid leukaemia (AML), patients with MPD rarely present w
ith infectious
complications related to leucopaenia, or com
plications related to anaemia that are observed in M
DS and AML. In addition,
although these MPD can be associated w
ith bleeding tendencies (diatheses) that are observed in MDS and AML owing to
thrombocytosis and platelet dysfunction, they are often associated w
ith specific clinical sequelae that include thrombotic
diatheses that are not observed in MDS or AML. However, MDS and AML are thought to be stem
cell disorders, based on
clonality analyses using X-inactivation-based assays in females or cytogenetic analyses that dem
onstrate the clonal
involvement of the different haem
atopoietic lineages111,112 .
The first MPD allele to be identified and characterized w
as the BCR-ABL fusion oncogene in chronic m
yeloid leukaemia
(CML) that arises as a consequence of the 9:22 translocation
2 , a causative agent for this disease, and recurrent
translocations led to the discovery of different fusion tyrosine kinases, including platelet derived growth factor receptor-B
(PDGFRB) fusions in patients w
ith chronic myelomonocytic leukaem
ia (CMML) and other M
PD3 . The observation that KIT is
highly expressed in mast cells led to the discovery of the KITD
816V allele in systemic mastocytosis (SM
)5 , and imatinib
responses in patients with chronic eosinophilic leukaem
ia (CEL) and SM led to the discovery of an interstitial deletion that
gives rise to the FIP1L1–PDGFRA fusion4 . M
ost recently, investigators have identified Janus kinase 2 (JAK2) and
thrombopoietin receptor m
utations in polycythaemia vera (PV), essential throm
bocythaemia (ET) and prim
ary
meylofibrosis (PM
F) that result in the activation of JAK2 signalling8–11,53,55 .
REVIEWS
NATURE REVIEWS | CANCER
VOLUME 7 | SEPTEMBER 2007 | 675
Myeloproliferativeneoplasms:JAK2gain of functionmutationas common oncogene
Pikman etal,PLoS Med2006;Klampfl etal/Nangalia etal,NEJM2013

modifiedfromMeyerSCetal,Clin CancerRes2014Rampal Retal,Blood2014
Myeloproliferativeneoplasms arealldriven by increased JAK2signaling activity
MPL