MSN 2 2012 Knorpeltherapie zur Prävention von Arthrose im Sprunggelenk
Arthroskopie an Sprunggelenk und Fuß
Das Praxisbuch der Techniken und Indikationen
Mit einem Geleitwort von C. Niek van Dijk
Galla ß Walther
Mellany Galla Markus Walther
Arthroskopie an Sprunggelenk und Fuß

This page intentionally left blank
Arthroskopie an Sprunggelenk und FußDas Praxisbuch der Techniken und Indikationen
Herausgegeben vonMellany Galla und Markus Walther
Mit Beiträgen von
Boris AdamietzMoez BallalChristoph BecherJames D. F. CalderPeter A. J. de LeeuwFlorian DreyerManfred EppelMellany GallaChristoph Lampert
Sabina MalhotraChristian PlaaßMartin RöpkeAmol SaxenaHajo ThermannC. Niek van DijkMarkus WaltherImke WeyersRuben Zwiers
Mit einem Geleitwort von C. Niek van Dijk
Mit 400 Abbildungen und 9 Tabellen

IV
Ihre Meinung zu diesem Werk ist uns wichtig!Wir freuen uns auf Ihr Feedback unter www.schattauer.de/feedback oder direkt über QR-Code.
Bibliografische Information der Deutschen NationalbibliothekDie Deutsche Nationalbibliothek verzeichnet diese Publikation in der Deutschen National-bibliografie; detaillierte bibliografische Daten sind im Internet über http://dnb.d-nb.de abruf-bar.
Besonderer Hinweis:Die Medizin unterliegt einem fortwährenden Entwicklungsprozess, sodass alle Angaben, ins-besondere zu diagnostischen und therapeuti-schen Verfahren, immer nur dem Wissensstand zum Zeitpunkt der Drucklegung des Buches ent-sprechen können. Hinsichtlich der angegebenen Empfehlungen zur Therapie und der Auswahl sowie Dosierung von Medikamenten wurde die größtmögliche Sorgfalt beachtet. Gleichwohl werden die Benutzer aufgefordert, die Beipack-zettel und Fachinformationen der Hersteller zur Kontrolle heranzuziehen und im Zweifelsfall einen Spezialisten zu konsultieren. Fragliche Unstimmigkeiten sollten bitte im allgemeinen Interesse dem Verlag mitgeteilt werden. Der Benutzer selbst bleibt verantwortlich für jede diagnostische oder therapeutische Applikation, Medikation und Dosierung. In diesem Buch sind eingetragene Warenzei-chen (geschützte Warennamen) nicht besonders kenntlich gemacht. Es kann also aus dem Fehlen eines entsprechenden Hinweises nicht geschlos-
sen werden, dass es sich um einen freien Waren-namen handelt.Das Werk mit allen seinen Teilen ist urheber-rechtlich geschützt. Jede Verwertung außerhalb der Bestimmungen des Urheberrechtsgesetzes ist ohne schriftliche Zustimmung des Verlages unzulässig und strafbar. Kein Teil des Werkes darf in irgendeiner Form ohne schriftliche Ge-nehmigung des Verlages reproduziert werden.
© 2016 by Schattauer GmbH, Hölderlinstraße 3, 70174 Stuttgart, GermanyE-Mail: [email protected]: www.schattauer.dePrinted in Germany
Projektleitung: Dipl.-Biol. Sabine Poppe, Alina PiasnyLektorat: Dipl.-Biol. Martina Kunze, EhringshausenIllustrationen: Hans Jörg Schütze, Köln (www.schuetze-illustration.de)Satz: Fotosatz Buck, KumhausenDruck und Einband: Mayr Miesbach GmbH, Druck · Medien · Verlag, Miesbach
Auch als E-Book erhältlich:ISBN 978-3-7945-6790-4
ISBN 978-3-7945-2967-4

V
by-step instructions help surgeons to per-form the surgical procedures. In each chap-ter, pearls and pitfalls of each technique are highlighted. Beyond common indications for ankle arthroscopy, this book likewise addresses operative methods such as ten-doscopy, metatarsophalangeal arthroscopy and open techniques for treatment of os-teochondral lesions and chronic instability of the ankle joint.This excellent and richly illustrated text book by Mellany Galla and Markus Walther finally fills a gap in German orthopedic lit-erature. I can recommend it to all orthope-dic surgeons dealing with foot and ankle, or-thopedic sports medicine and traumatology.
Amsterdam, June 2016 Prof. Dr. C. Niek van Dijk
Foreword
Arthroscopy has become increasingly im-portant in foot and ankle surgery. Formerly used merely for diagnostics, it has developed into an important tool for treating a variety of pathologies of the foot and ankle. Besides the treatment of the ankle joint and the sub-talar joint, arthroscopy has become feasible to address small joints of the middle and forefoot and extraarticular compartments such as tendon sheaths and the Kager’s Tri-angle.An international group of authors has con-tributed their experience to cover the subject of arthroscopic treatment concepts in foot and ankle surgery. This comprehensive text book comprises anatomy, imaging and phys-ical examination for preoperative diagnosis as well as indications and contraindications for the different procedures. Illustrated step-

VI
Vorwort
„Das obere Sprunggelenk ist aufgrund der straffen knöchernen und ligamentären Füh-rung des Talus in der Malleolengabel und der hohen Gelenkkongruenz zweifellos ar-throskopisch nicht zugänglich“, berichtete Michael S. Burman 1931 nach experimen-tellen Kadaveruntersuchungen.Doch bereits 1939 beschrieb Kenji Tagaki erstmals eine systematische Zugangsweise und Untersuchungsmöglichkeit des Gelenk-raums.Zunächst fand diese Technik in Ermange-lung eines geeigneten Instrumentariums am Sprunggelenk wenig Beachtung. Erst in den 1970er-Jahren konnte sich das Verfahren stärker durchsetzen. Das stetig steigende Interesse an minimal-invasiven Operati-onsverfahren in den letzten Jahren hat vor dem Hintergrund der rasanten Entwicklung technischer Möglichkeiten in der arthros-kopischen Chirurgie dazu geführt, dass die Sprunggelenksarthroskopie aktuell zu den dritthäufigsten arthroskopischen Eingriffen neben der Knie- und Schulterarthroskopie gehört und aus dem Portfolio der Fuß- und Sprunggelenkchirurgie nicht mehr wegzu-denken ist.Nach anfänglicher Anwendung am ventra-len oberen Sprunggelenk gelten heute die dorsale Arthroskopie des Sprunggelenks so-wie die Arthroskopie des unteren Sprung-gelenks als etablierte Verfahren. Darüber hinaus werden seit Beginn der 1990er-Jahre die arthroskopischen Techniken nicht mehr ausschließlich für die Behandlung intraar-
tikulärer Läsionen angewendet. Der Einsatz des Arthroskops im extraartikulären Be-reich des Rückfußes ermöglicht die mini-mal-invasive Therapie von Pathologien am Sprunggelenk und Fuß, welche sich außer-halb des Gelenkkavums befinden.Wunsch der Herausgeber und Autoren war es, eine umfassende deutschsprachige, pra-xisorientierte Übersicht der Arthroskopie am Fuß und Sprunggelenk zu schaffen. Das Buch richtet sich an Ärzte, welche die Ba-sistechniken erlernen möchten, ebenso wie an erfahrene Operateure, die ihre Kenntnis-se insbesondere bei seltenen Indikationen vertiefen wollen. Neben den grundlegenden arthroskopischen OP-Techniken am oberen und unteren Sprunggelenk sowie am Rück-fuß werden die Behandlungsmöglichkeiten typischer Krankheitsbilder dargestellt.Unser Dank gilt allen Autoren, die dazu beigetragen haben, dieses Buch über die Arthroskopie am Sprunggelenk und Fuß zu verwirklichen, sowie Herrn Hans Jörg Schütze für die Erstellung der ausgezeich-neten Illustrationen. Den Mitarbeiterinnen des Schattauer Verlages Frau Sabine Pop-pe, Frau Alina Piasny sowie Frau Martina Kunze danken wir für die hervorragende Betreuung des Projekts.
Hildesheim und München, im Juni 2016
Mellany GallaMarkus Walther
VII
Anschriften
HerausgeberDr. med. Mellany GallaChirurgie im MedicinumGoslarsche Landstraße 1931135 [email protected]
Prof. Dr. med. Dr. med. habil. Markus WaltherSchön Klinik München HarlachingZentrum für Fuß- und Sprunggelenk-chirurgieHarlachinger Straße 5181547 Mü[email protected]
AutorenPD Dr. med. Boris AdamietzRadiologie am HerkomerplatzOberföhringer Straße 281679 Mü[email protected]
Dr. Moez Ballal, MD, FRCSConsultant Trauma & Orthopaedic SurgeonUniversity Hospital South ManchesterSouthmoor RoadWythenshawe Manchester M23 [email protected]
PD Dr. med. Christoph BecherHKF – Internationales Zentrum für Hüft-, Knie- und FußchirurgieATOS-Klinik HeidelbergBismarckstraße 9–1569115 [email protected]
Dr. James D. F. Calder, MD, FRCSConsultant Orthopaedic SurgeonFortius Clinic London17 Fitzhardinge StreetLondon W1H [email protected]
Dr. Peter A. J. de LeeuwDepartment of Orthopaedic SurgeryAcademic Medical CenterUniversity of AmsterdamP.O. Box 227001100 DE [email protected]
Dr. med. Florian DreyerSchön Klinik München HarlachingZentrum für Fuß- und Sprunggelenk-chirurgieHarlachinger Straße 5181547 Mü[email protected]
Dr. Manfred EppelUniversitätsklinik für Unfallchirurgie und SporttraumatologieParacelsus Medizinische PrivatuniversitätSalzburger LandesklinikenMüllner Hauptstraße 485020 SalzburgÖ[email protected]
VIII Anschriften
Prof. Dr. med. Hajo ThermannHKF – Internationales Zentrum für Hüft-, Knie- und FußchirurgieATOS-Klinik HeidelbergBismarckstraße 9–1569115 [email protected]
Prof. Dr. C. Niek van Dijk, MD, PhDDepartment of Orthopaedic SurgeryAcademic Medical CenterUniversity of AmsterdamP.O. Box 226601100 DD [email protected]
Prof. Dr. med. Dr. med. habil. Markus WaltherSchön Klinik München HarlachingZentrum für Fuß- und Sprunggelenk-chirurgieHarlachinger Straße 5181547 Mü[email protected]
Dr. med. Imke WeyersInstitut für AnatomieUniversität zu LübeckRatzeburger Allee 160, Geb. 6323362 Lü[email protected]
Ruben ZwiersDepartment of Orthopaedic SurgeryAcademic Medical CenterUniversity of AmsterdamP.O. Box 226601100 DD [email protected]
Dr. med. Mellany GallaChirurgie im MedicinumGoslarsche Landstraße 1931135 [email protected]
Dr. med. Christoph LampertOrthopädie RosenbergRorschacher Strasse 1509000 St. [email protected]
Dr. Sabina Malhotra, DPM, AACFASArthritis and Sports Orthopedics21475 Ridgetop CircleSuite 150Sterling, VA [email protected]
Dr. med. Christian PlaaßOrthopädische Klinik der Medizinischen Hochschule Hannover (MHH)Diakovere AnnastiftAnna-von-Borries-Straße 1–730625 [email protected]
Dr. med. Martin RöpkeUniversitätsklinikum Magdeburg A. ö. R.Orthopädische UniversitätsklinikLeipziger Straße 4439120 [email protected]
Dr. Amol Saxena, DPMPalo Alto Foundation Medical Group (PAFMG)Dept. of Sports Medicine795 El Camino RealPalo Alto, CA [email protected]
IX
Abkürzungsverzeichnis
A. ArteriaAMIC autologe matrixinduzierte Chondro-
geneseAOFAS American Orthopaedic Foot and
Ankle Societya.-p. anterior-posterior
BMI Body-Mass-IndexBV Bildverstärker
CPM Continuous Passive MotionCRPS Complex regional pain syndromeCT Computertomografie
DEGUM Deutsche Gesellschaft für Ultra-schall in der Medizin e. V.
dGEMRIC delayed Gadolinium- Enhanced Magnetic Resonance Imaging of Cartilage
d.-p. dorsoplantar
ESSR European Society of Skeletal Radiology
FFI Foot Function IndexFHL Flexor hallucis longusFOV Field of ViewFS fat saturated
HDTV High Definition TelevisionHF HochfrequenzHU Hounsfield Units
ICRS International Cartilage Repair Society
ISAKOS- Conference of the InternationalFIMS Society of Arthroscopy, Knee Sur-
gery and Orthopaedic Sports Medi-cine and International Federation of Sports Medicine
i. v. intravenös
KM Kontrastmittel
LCF Ligamentum calcaneofibulareLFC Ligamentum fibulocalcaneareLFTA Ligamentum fibulotalare anteriusLFTP Ligamentum fibulotalare posteriusLig. LigamentumLTFA Ligamentum talofibulare anteriusLTFP Ligamentum talofibulare posterius
M. MorbusM. MusculusMACT matrixassoziierte Knorpelzelltrans-
plantationmm. musculorumMRT Magnetresonanztomografie
N. NervusNSAR nichtsteroidale orale Antiphlogistika
OATS osteochondrale autologe Transplan-tation
OCL osteochondrale LäsionenOP OperationOSG oberes Sprunggelenk
p.-a. posterior-anteriorPD ProtonendichtePDS PolydioxanonPRP platelet-rich plasma, thrombo-
zytenreiches Plasma
X Abkürzungsverzeichnis
TEP Totalendoprothese
USG unteres SprunggelenkUSP United States Pharmacopeia
V. VenaV. a. Verdacht aufVAS visuelle Analogskala
Z. n. Zustand nach
R. RamusRr. Rami
SE Spin-EchoSPECT Single Photon EmissionSPECT-CT Single Photon Emission Computed
TomographySTIR Short Tau Inversion RecoverySYSADOA symptomatic slow acting drugs in
osteoarthritis
XI
Inhalt
1 Anatomie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Imke Weyers
1.1 Oberes Sprunggelenk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1.1 Knöcherne Strukturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1.2 Ligamentäre Strukturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.2 Unteres Sprunggelenk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1.2.1 Articulatio talocalcaneo navicularis (vorderes Gelenk, vordere Kammer) . . . . . . . . . . . . . . 10
1.2.2 Articulatio subtalaris (hinteres Gelenk, hintere Kammer) . . . . . . . . . . . . . . . . . . . . . . . . . . 11
1.3 Muskuläre und tendinöse Strukturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.3.1 Extensorengruppe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.3.2 Fibularisgruppe (Peroneusgruppe) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
1.3.3 Flexorengruppe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
1.4 Neurovaskuläre Strukturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.4.1 Arterien . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
1.4.2 Venen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
1.4.3 Nerven . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
1.5 Großzehengrundgelenk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
1.5.1 Knöcherner Aufbau, Bänder und Sehnen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
1.5.2 Neurovaskuläre Strukturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2 Klinische Untersuchung von Fuß und Sprunggelenk . . . . . . . . . . . . . . . 31
Manfred Eppel
2.1 Anamnese . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
2.2 Klinische Untersuchung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2.2.1 Inspektion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2.2.2 Palpation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
2.2.3 Messung des Bewegungs umfangs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
2.2.4 Bandstabilität am oberen und unteren Sprunggelenk . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
2.2.5 Impingementtests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
2.2.6 Gefäßstatus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
2.2.7 Neurologischer Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
XII Inhalt
3 Bildgebende Diagnostik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Boris Adamietz, Markus Walther
3.1 Konventionelle Röntgentechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
3.1.1 Untersuchungstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
3.1.2 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
3.2 Sonografie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
3.2.1 Untersuchungstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
3.2.2 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
3.3 Computertomografie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
3.3.1 Technische Voraussetzungen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
3.3.2 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
3.4 Magnetresonanztomografie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
3.4.1 Untersuchungstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
3.4.2 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
3.5 SPECT-CT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
3.5.1 Technik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
3.5.2 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
4 Arthroskopie des ventralen oberen Sprunggelenks . . . . . . . . . . . . . . . 81
Mellany Galla
4.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
4.1.1 Synovialitis und Weichteil impingement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
4.1.2 Arthrofibrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
4.1.3 Ventrales knöchernes Impingement durch Osteophyten . . . . . . . . . . . . . . . . . . . . . . . . . . 83
4.1.4 Gelenkkörper/Chondromatosen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
4.1.5 Arthrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
4.1.6 Chondrale und osteochondrale Flakefrakturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
4.1.7 Chronische chondrale und osteochondrale Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
4.1.8 Subchondrale zystische Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
4.1.9 Arthroskopisch gestützte Frakturversorgung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
4.1.10 Arthroskopische Gelenk stabilisierung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
4.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
4.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
4.4 Zugangswege und Untersuchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
4.4.1 Anteromediales Standardportal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
4.4.2 Anterolaterales Standardportal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
XIIIInhalt
4.4.3 Anterozentrales Portal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
4.4.4 Akzessorische Portale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
4.5 Operationstechniken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
4.5.1 Synovialitis und Weichteil impingement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
4.5.2 Arthrofibrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
4.5.3 Ventrales knöchernes Impingement durch Osteophyten . . . . . . . . . . . . . . . . . . . . . . . . . . 99
4.5.4 Gelenkkörper/Chondromatosen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
4.5.5 Arthrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
4.5.6 Chondrale und osteochondrale Flakefrakturen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
4.5.7 Chronische chondrale und osteochondrale Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
4.5.8 Subchondrale zystische Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
4.5.9 Arthroskopisch gestützte Fraktur versorgung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
4.5.10 Arthroskopische Gelenk stabilisierung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
4.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
4.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
5 Rückfußarthroskopie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Mellany Galla
5.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114
5.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
5.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
5.4 Zugangswege und Untersuchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
5.4.1 Hohe paraachilläre Portale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
5.4.2 Tiefe paraachilläre Portale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124
5.5 Operationstechniken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 127
5.5.1 Dorsales knöchernes Impingement am oberen und unteren Sprunggelenk . . . . . . . . . . . . 127
5.5.2 Dorsales Weichteilimpingement am oberen und unteren Sprunggelenk . . . . . . . . . . . . . . 131
5.5.3 Haglunddeformität und retro kalkaneare Bursitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 132
5.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135
5.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 136
6 Arthroskopie des unteren Sprunggelenks . . . . . . . . . . . . . . . . . . . . . . . . . 139
Martin Röpke
6.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
6.1.1 Synovialitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
XIV Inhalt
6.1.2 Arthrofibrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
6.1.3 Sinus-tarsi-Syndrom . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
6.1.4 Freie Gelenkkörper . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142
6.1.5 Osteochondrale Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142
6.1.6 Arthrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142
6.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143
6.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
6.4 Zugangswege und Unter suchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145
6.4.1 Anterolaterale Portale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145
6.4.2 Posterolaterale Portale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
6.4.3 Untersuchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147
6.5 Operationstechniken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150
6.5.1 Synovialitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150
6.5.2 Arthrofibrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
6.5.3 Sinus-tarsi-Syndrom . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
6.5.4 Freie Gelenkkörper und Osteophyten . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
6.5.5 Chondrale und osteochondrale Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
6.5.6 Arthrose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
6.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
6.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
7 Arthroskopie des Großzehengrundgelenks . . . . . . . . . . . . . . . . . . . . . . . . 157
Markus Walther
7.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
7.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158
7.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
7.4 Zugangswege und Untersuchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 160
7.5 Operationstechniken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162
7.5.1 Synovialitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162
7.5.2 Osteophyten und degenerative Gelenkveränderungen . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
7.5.3 Freie Gelenkkörper . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
7.5.4 Osteochondrale Läsionen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
7.5.5 Weitere Einsatzgebiete . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 164
7.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165
7.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
XVInhalt
8 Arthroskopisch assistierte Arthrodese des oberen Sprunggelenks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
Florian Dreyer, Markus Walther
8.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
8.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
8.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173
8.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173
8.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 176
8.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 180
8.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182
9 Arthroskopisch assistierte Arthrodese des unteren Sprunggelenks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185
Christoph Lampert
9.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 186
9.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
9.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
9.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191
9.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 194
9.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198
9.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198
10 Tendoskopie . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201
Ruben Zwiers, Peter A. J. de Leeuw, C. Niek van Dijk
10.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202
10.1.1 Tibialis-posterior-Sehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202
10.1.2 Peronealsehnen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
10.1.3 Achillessehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 204
10.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206
10.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
10.4 Zugangswege und Untersuchungsgang . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 210
10.4.1 Tibialis-posterior-Sehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 210
XVI Inhalt
10.4.2 Peronealsehnen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212
10.4.3 Achillessehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 214
10.5 Operationstechniken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
10.5.1 Tibialis-posterior-Sehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216
10.5.2 Peronealsehnen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
10.5.3 Achillessehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
10.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
10.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
10.7.1 Tibialis-posterior-Sehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
10.7.2 Peronealsehnen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
10.7.3 Achillessehne . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
11 Endoskopische Gastrocnemiusverlängerung . . . . . . . . . . . . . . . . . . . . . . 225
Amol Saxena
11.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 226
11.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 226
11.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
11.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 228
11.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 233
11.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235
11.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 236
12 Endoskopisches Plantarfaszienrelease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
Amol Saxena, Sabina Malhotra
12.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
12.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
12.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
12.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241
12.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 244
12.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 246
12.7 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 246
XVIIInhalt
13 Operative Behandlung osteochondraler Läsionen am Talus . . . . . . . 249
Christoph Becher, Christian Plaaß, Hajo Thermann
13.1 Arthroskopische Mikrofrakturierung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252
13.1.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252
13.1.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253
13.1.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253
13.1.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253
13.1.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255
13.1.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 256
13.2 Autologe matrixassoziierte Chondrogenese (AMIC) . . . . . . . . . . . . . . . . . . . . . . . . . 257
13.2.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257
13.2.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258
13.2.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258
13.2.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 259
13.2.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 261
13.2.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
13.3 Transplantation von osteochondralen Zylindern (OATS, Mosaikplastik) . . . . . . . . 263
13.3.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
13.3.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263
13.3.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264
13.3.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264
13.3.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264
13.3.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
13.4 Weitere Verfahren: retro grade Anbohrung, retrograde Spongiosaauffüllung, autologe Knorpelzelltransplantation, juvenile allogene Knorpelpartikel, HemiCAP® . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
13.4.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 267
13.4.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268
13.4.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268
13.4.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 269
13.4.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 269
13.4.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272
13.5 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273
13.5.1 Arthroskopische Mikro frakturierung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273
13.5.2 Autologe matrixassoziierte Chondrogenese (AMIC) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 274
13.5.3 Transplantation von osteochondralen Zylindern (OATS, Mosaikplastik) . . . . . . . . . . . . . . . 275
13.5.4 Weitere Verfahren: retrograde Anbohrung und Spongiosaauffüllung, HemiCAP® . . . . . . . 276
InhaltXVIII
14 Operative Behandlung der chronischen lateralen Sprung gelenksinstabilität . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279
James D. F. Calder, Moez Ballal, Mellany Galla
14.1 Direkte Rekonstruktion nach Broström-Gould . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
14.1.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
14.1.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
14.1.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281
14.1.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281
14.1.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282
14.1.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285
14.2 Arthroskopische laterale Stabilisierung des Sprunggelenks (modifiziertes Broström-Gould-Verfahren) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
14.2.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
14.2.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 286
14.2.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
14.2.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
14.2.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
14.2.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295
14.3 Anatomische Rekonstruk tion mit autologem Sehnentransplantat . . . . . . . . . . . . . 296
14.3.1 Indikationen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
14.3.2 Lagerung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
14.3.3 Instrumentarium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
14.3.4 Zugangswege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297
14.3.5 Operationstechnik . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297
14.3.6 Nachbehandlung . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
14.4 Ergebnisse und Risiken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305
Sachverzeichnis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 309
1 AnatomieImke Weyers
1.1 Oberes Sprunggelenk
1.1.1 Knöcherne Strukturen
Das obere Sprunggelenk (Articulatio talocruralis, OSG) entsteht aus der Verbindung der Unterschenkelknochen, Tibia und Fibula, mit dem Talus. Die Tibia und die Fibula umschließen dabei den Talus als Malleolengabel. Die größte Artikulationsfläche bildet die Facies inferior der Tibia zusammen mit der Trochlea tali. Die Fibula liegt einer wesentlich kleineren lateralen Artikulationsfläche an, die als Facies malleolaris lateralis bezeichnet wird. Die Facies malleolaris medialis stellt die Verbindung zum Malleolus medialis der Tibia dar. Das OSG ist im Wesentlichen ein Scharniergelenk, als Bewegungen sind Dorsalextension und Plantarflexion möglich. Da die Talusrolle
vorne breiter ist als hinten, sind Tibia, Fibula und Talus bei Dorsalflexion wesentlich fester miteinander verzahnt als in Plantarflexion. In geringen Graden lässt das Gelenk auch Rotationsbewegungen des Talus in der Malleolengabel zu.Die knöchernen Strukturen sind bei der klinischen Untersuchung einfach zu identifizieren, da sie gut tastbar sind. Es ist wichtig zu wissen, dass die Malleolen auf unterschiedlicher Höhe liegen. Die Spitze des lateralen Malleolus befindet sich ca. 1 cm tiefer (distal) und ca. 2 cm hinter (posterior) der Spitze des medialen Malleolus. Die vordere Gelenklinie kann gut getastet werden, wenn man den Fuß passiv dorsalflektiert. Die hintere Gelenklinie wird durch die dichte Schicht aus Sehnen (Achilles und Flexorensehnen) und Fettgewebe bedeckt und kann daher nicht direkt palpiert werden.
2 1 Anatomie
Membranainterossea
Lig. tibiofibulareanterius (vorderesSyndesmosenband)
IntraartikulärerAnteil der vorderenSyndesmose
Lig. talofibulareanterius
Lig. calca-neonavi-culare
Lig. calca-naeocubo-ideum
Lig. bifur-catum
Ligg. calcaneo-cuboidea dorsalia
Lig. deltoideumPars tibiotalaris anteriorLig. talonavicularedorsale
Ligg. tarsidorsalia
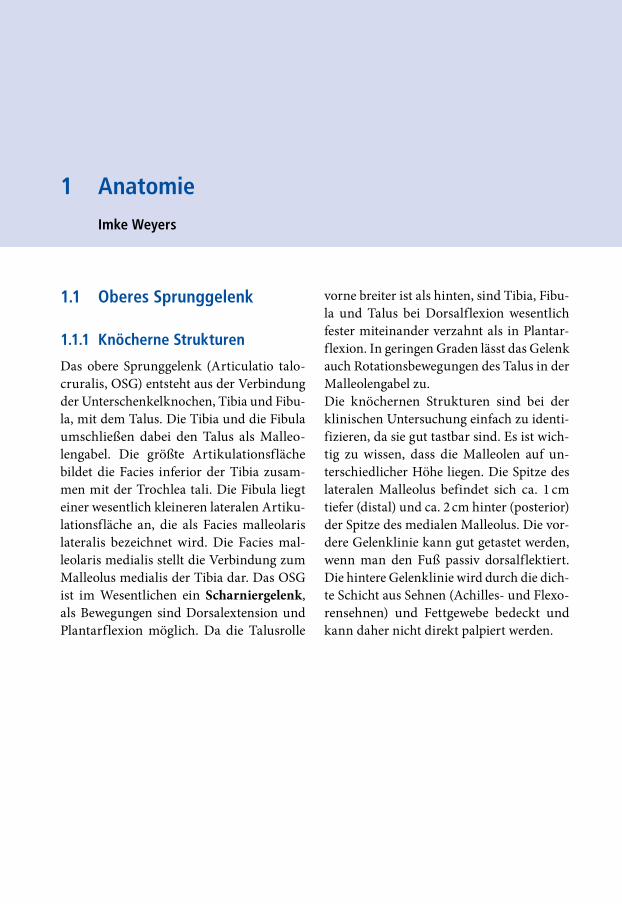
Abb. 1-1 Knochen und Bänder des Sprunggelenks und des Dorsum pedisa Darstellung am anatomischen Präparat
a
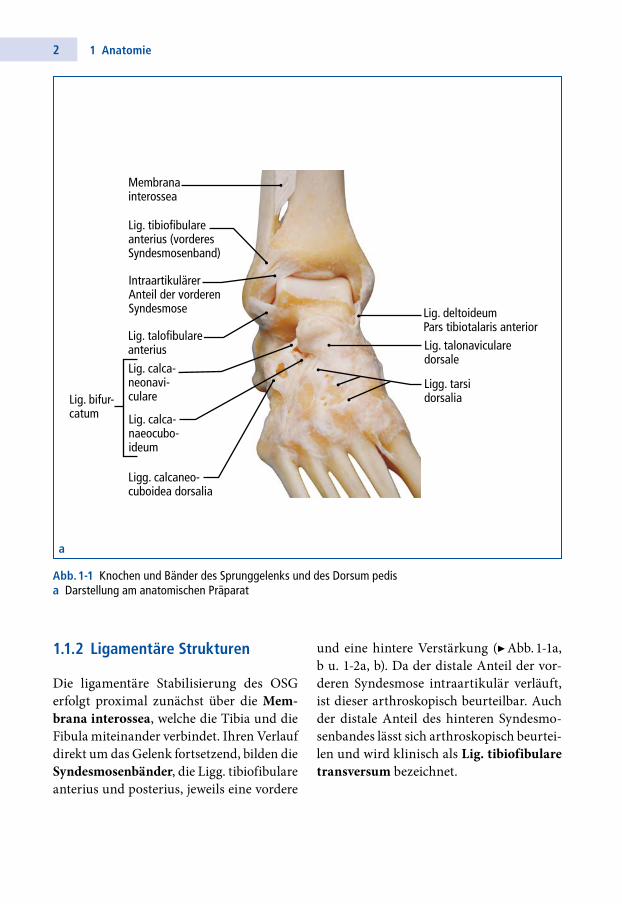
1.1.2 Ligamentäre Strukturen
Die ligamentäre Stabilisierung des OSG erfolgt proximal zunächst über die Mem-brana interossea, welche die Tibia und die Fibula miteinander verbindet. Ihren Verlauf direkt um das Gelenk fortsetzend, bilden die Syndesmosenbänder, die Ligg. tibiofibulare anterius und posterius, jeweils eine vordere
und eine hintere Verstärkung (▶ Abb. 11a, b u. 12a, b). Da der distale Anteil der vorderen Syndesmose intraartikulär verläuft, ist dieser arthroskopisch beurteilbar. Auch der distale Anteil des hinteren Syndesmosenbandes lässt sich arthroskopisch beurteilen und wird klinisch als Lig. tibiofibulare transversum bezeichnet.
31.1 Oberes Sprunggelenk
Membrana interossea
Lig. tibiofibulare anterius (vorderes Syndesmosen-band)
Intraartikulärer Anteil der vorderen Syndesmose
Lig. deltoideum, Pars tibiotalaris anterior
Lig. talofibulare anterius
Lig. talonaviculare dorsale
Ligg. tarsi dorsalia
Ligg. calcaneocuboidea dorsalia
Lig. calca-naeonavi-culare Lig. bifur-
catumLig. calca-naeocubo-ideum
Abb. 1-1 (Fortsetzung)b schematische Darstellung
b
4 1 Anatomie
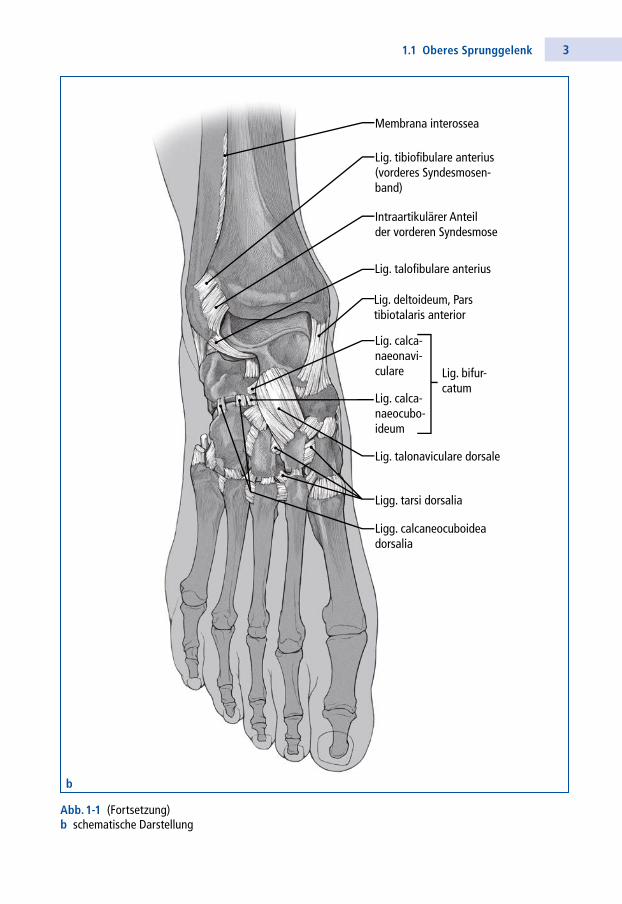
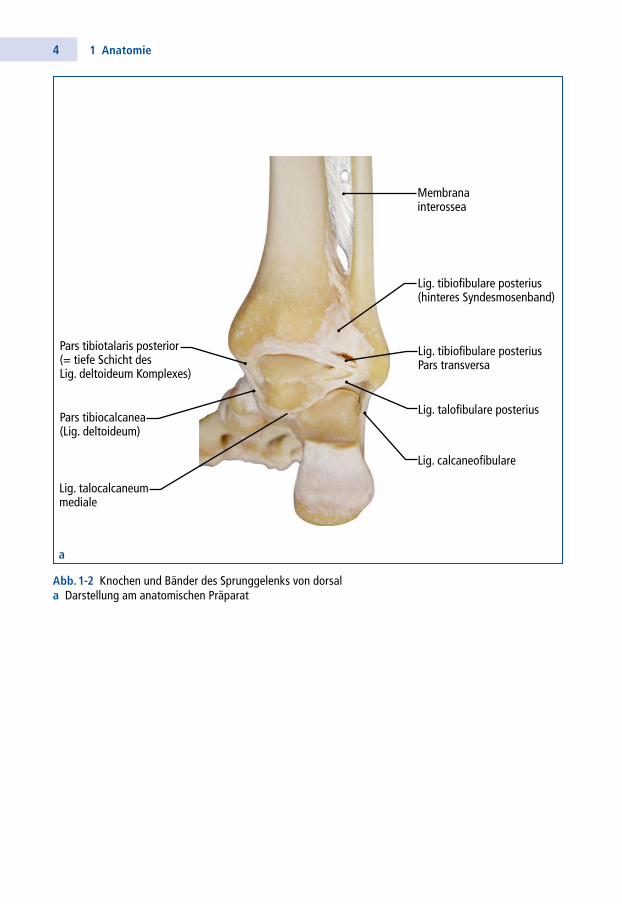
Abb. 1-2 Knochen und Bänder des Sprunggelenks von dorsala Darstellung am anatomischen Präparat
Membranainterossea
Pars tibiotalaris posterior(= tiefe Schicht desLig. deltoideum Komplexes)
Pars tibiocalcanea(Lig. deltoideum)
Lig. talocalcaneummediale
Lig. tibiofibulare posteriusPars transversa
Lig. tibiofibulare posterius(hinteres Syndesmosenband)
Lig. talofibulare posterius
Lig. calcaneofibulare
a
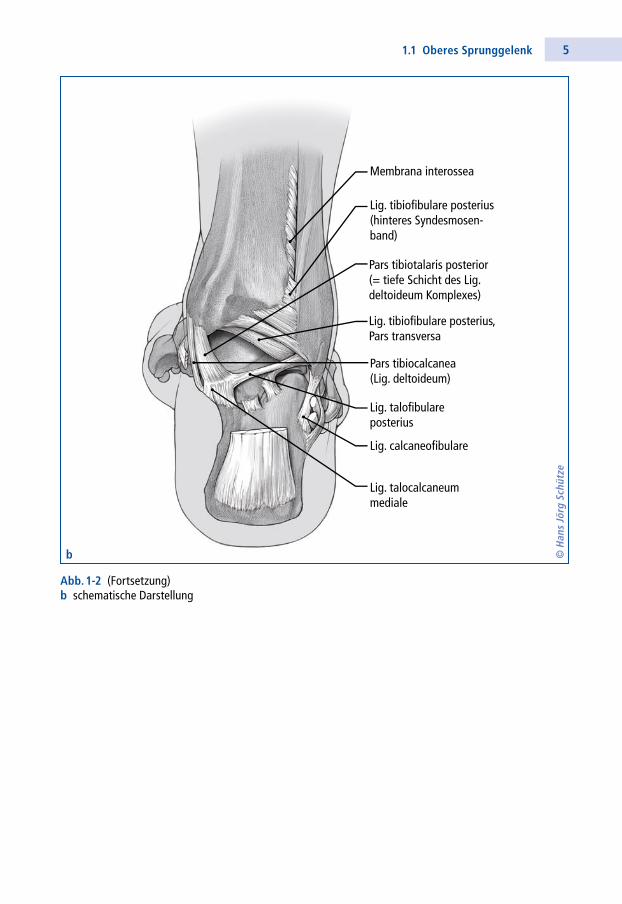
51.1 Oberes Sprunggelenk
Membrana interossea
Lig. tibiofibulare posterius (hinteres Syndesmosen-band)
Lig. tibiofibulare posterius, Pars transversa
Pars tibiotalaris posterior(= tiefe Schicht des Lig.deltoideum Komplexes)
Pars tibiocalcanea(Lig. deltoideum)
Lig. talocalcaneum mediale
Lig. talofibulareposterius
Lig. calcaneofibulare
© H
ans
Jörg
Sch
ütze
Abb. 1-2 (Fortsetzung)b schematische Darstellung
b
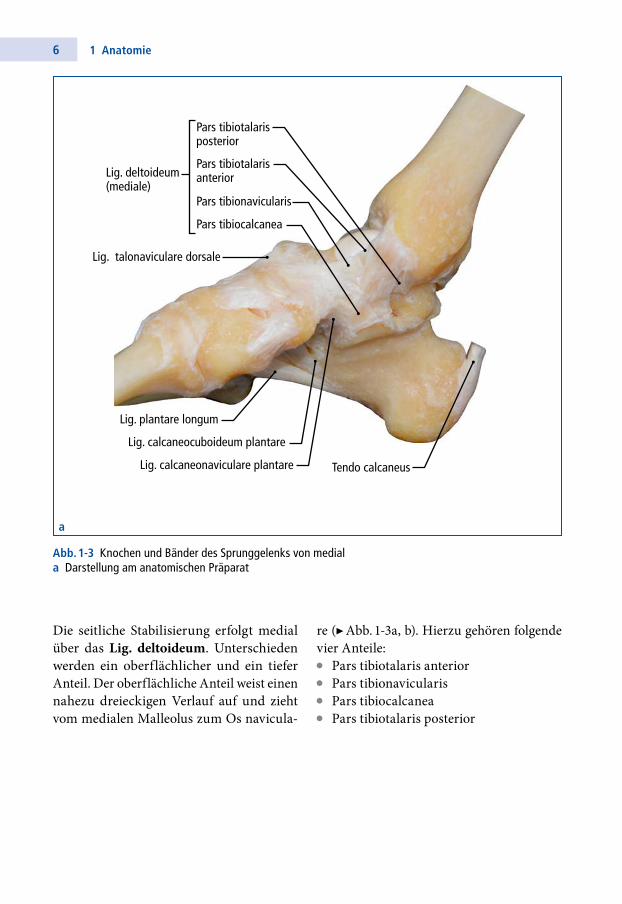
6 1 Anatomie
Die seitliche Stabilisierung erfolgt medial über das Lig. deltoideum. Unterschieden werden ein oberflächlicher und ein tiefer Anteil. Der oberflächliche Anteil weist einen nahezu dreieckigen Verlauf auf und zieht vom medialen Malleolus zum Os navicula
Lig. talonaviculare dorsale
Tendo calcaneus
Lig. deltoideum(mediale)
Lig. plantare longum
Lig. calcaneocuboideum plantare
Lig. calcaneonaviculare plantare
Pars tibiotalarisanterior
Pars tibiotalarisposterior
Pars tibionavicularis
Pars tibiocalcanea
Abb. 1-3 Knochen und Bänder des Sprunggelenks von mediala Darstellung am anatomischen Präparat
a
re (▶ Abb. 13a, b). Hierzu gehören folgende vier Anteile:• Pars tibiotalaris anterior• Pars tibionavicularis• Pars tibiocalcanea• Pars tibiotalaris posterior
71.1 Oberes Sprunggelenk
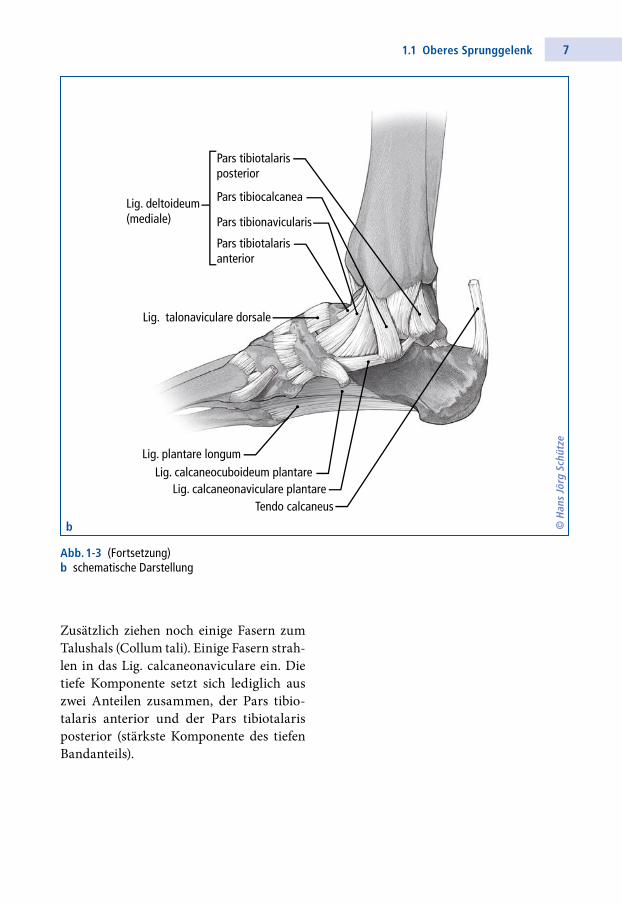
Zusätzlich ziehen noch einige Fasern zum Talushals (Collum tali). Einige Fasern strahlen in das Lig. calcaneonaviculare ein. Die tiefe Komponente setzt sich lediglich aus zwei Anteilen zusammen, der Pars tibiotalaris anterior und der Pars tibiotalaris posterior (stärkste Komponente des tiefen Bandanteils).
Lig. talonaviculare dorsale
Tendo calcaneus
Lig. deltoideum(mediale)
Lig. plantare longumLig. calcaneocuboideum plantare
Lig. calcaneonaviculare plantare
Pars tibiotalarisanterior
Pars tibiotalarisposterior
Pars tibionavicularis
Pars tibiocalcanea
Abb. 1-3 (Fortsetzung)b schematische Darstellung
b © H
ans
Jörg
Sch
ütze
8 1 Anatomie
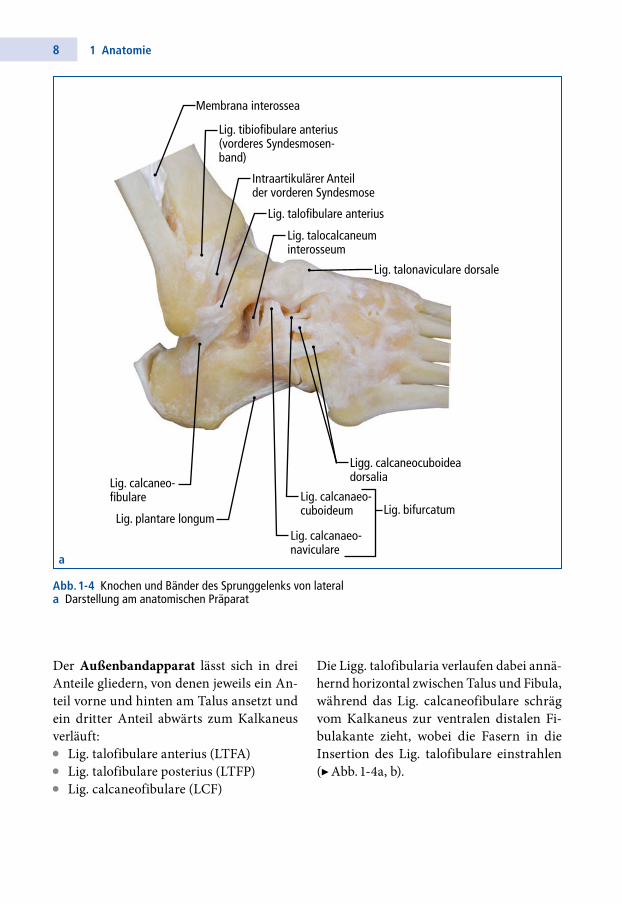
Die Ligg. talofibularia verlaufen dabei annähernd horizontal zwischen Talus und Fibula, während das Lig. calcaneofibulare schräg vom Kalkaneus zur ventralen distalen Fibulakante zieht, wobei die Fasern in die Insertion des Lig. talofibulare einstrahlen (▶ Abb. 14a, b).
Der Außenbandapparat lässt sich in drei Anteile gliedern, von denen jeweils ein Anteil vorne und hinten am Talus ansetzt und ein dritter Anteil abwärts zum Kalkaneus verläuft:• Lig. talofibulare anterius (LTFA)• Lig. talofibulare posterius (LTFP)• Lig. calcaneofibulare (LCF)
Membrana interossea
Lig. tibiofibulare anterius (vorderes Syndesmosen-band)
Intraartikulärer Anteil der vorderen Syndesmose
Lig. talofibulare anterius
Lig. plantare longum
Lig. talocalcaneum interosseum
Ligg. calcaneocuboidea dorsalia
Lig. talonaviculare dorsale
Lig. calcaneo-fibulare
Lig. calcanaeo-naviculare
Lig. bifurcatumLig. calcanaeo-cuboideum
Abb. 1-4 Knochen und Bänder des Sprunggelenks von laterala Darstellung am anatomischen Präparat
a
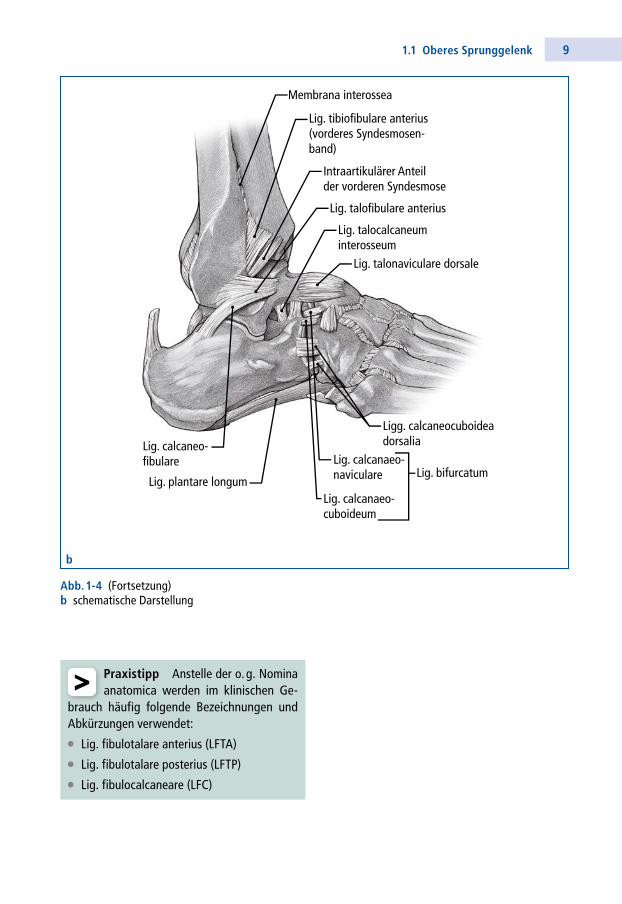
91.1 Oberes Sprunggelenk
Membrana interossea
Lig. tibiofibulare anterius (vorderes Syndesmosen-band)
Intraartikulärer Anteil der vorderen Syndesmose
Lig. talofibulare anterius
Lig. plantare longum
Lig. talocalcaneum interosseum
Ligg. calcaneocuboidea dorsalia
Lig. talonaviculare dorsale
Lig. calcaneo-fibulare
Lig. calcanaeo-cuboideum
Lig. bifurcatumLig. calcanaeo-naviculare
Abb. 1-4b
Abb. 1-4 (Fortsetzung)b schematische Darstellung
b
> Praxistipp Anstelle der o. g. Nomina anatomica werden im klinischen Ge-
brauch häufig folgende Bezeichnungen und Abkürzungen verwendet:
• Lig. fibulotalare anterius (LFTA)
• Lig. fibulotalare posterius (LFTP)
• Lig. fibulocalcaneare (LFC)
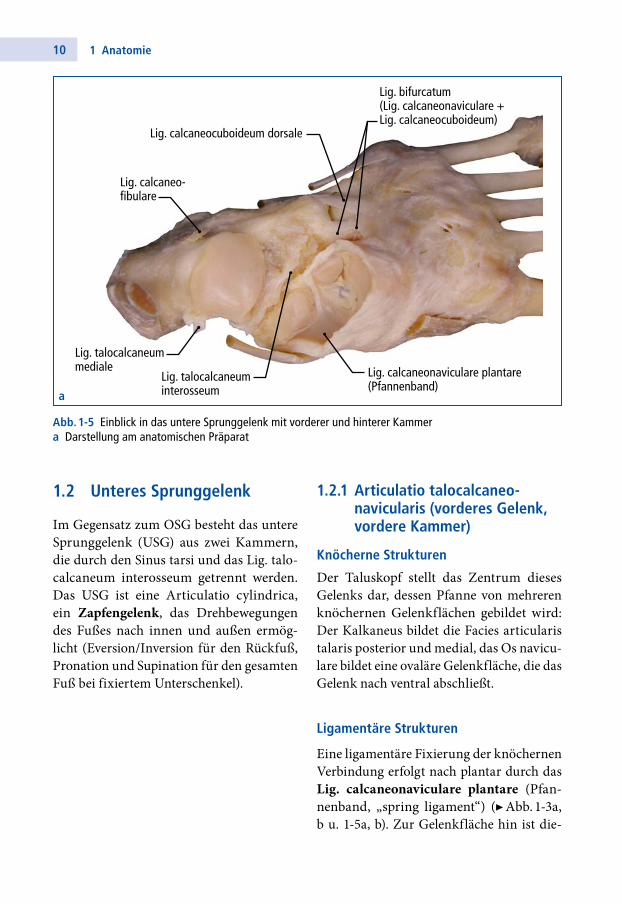
10 1 Anatomie
Lig. talocalcaneum mediale
Lig. talocalcaneum interosseum
Lig. calcaneonaviculare plantare (Pfannenband)
Lig. calcaneocuboideum dorsale
Lig. calcaneo-fibulare
Lig. bifurcatum(Lig. calcaneonaviculare +Lig. calcaneocuboideum)
1.2.1 Articulatio talocalcaneo-navicularis (vorderes Gelenk, vordere Kammer)
Knöcherne Strukturen
Der Taluskopf stellt das Zentrum dieses Gelenks dar, dessen Pfanne von mehreren knöchernen Gelenkflächen gebildet wird: Der Kalkaneus bildet die Facies articularis talaris posterior und medial, das Os naviculare bildet eine ovaläre Gelenkfläche, die das Gelenk nach ventral abschließt.
Ligamentäre Strukturen
Eine ligamentäre Fixierung der knöchernen Verbindung erfolgt nach plantar durch das Lig. calcaneonaviculare plantare (Pfannenband, „spring ligament“) (▶ Abb. 13a, b u. 15a, b). Zur Gelenkfläche hin ist die
1.2 Unteres Sprunggelenk
Im Gegensatz zum OSG besteht das untere Sprunggelenk (USG) aus zwei Kammern, die durch den Sinus tarsi und das Lig. talocalcaneum interosseum getrennt werden. Das USG ist eine Articulatio cylindrica, ein Zapfengelenk, das Drehbewegungen des Fußes nach innen und außen ermöglicht (Ever sion/ Inversion für den Rückfuß, Prona tion und Supination für den gesamten Fuß bei fixiertem Unterschenkel).
a
Abb. 1-5 Einblick in das untere Sprunggelenk mit vorderer und hinterer Kammera Darstellung am anatomischen Präparat
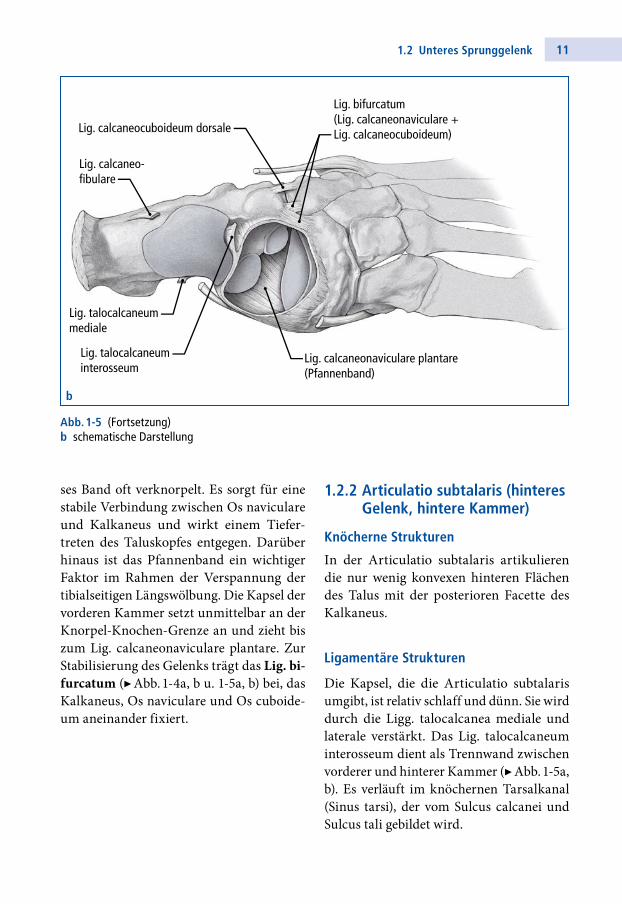
111.2 Unteres Sprunggelenk
Lig. talocalcaneum mediale
Lig. talocalcaneum interosseum
Lig. calcaneonaviculare plantare (Pfannenband)
Lig. calcaneocuboideum dorsale
Lig. calcaneo-fibulare
Lig. bifurcatum(Lig. calcaneonaviculare +Lig. calcaneocuboideum)
b
Abb. 1-5 (Fortsetzung)b schematische Darstellung
ses Band oft verknorpelt. Es sorgt für eine stabile Verbindung zwischen Os naviculare und Kalkaneus und wirkt einem Tiefertreten des Taluskopfes entgegen. Darüber hinaus ist das Pfannenband ein wichtiger Faktor im Rahmen der Verspannung der tibialseitigen Längswölbung. Die Kapsel der vorderen Kammer setzt unmittelbar an der KnorpelKnochenGrenze an und zieht bis zum Lig. calcaneonaviculare plantare. Zur Stabilisierung des Gelenks trägt das Lig. bi-furcatum (▶ Abb. 14a, b u. 15a, b) bei, das Kalkane us, Os naviculare und Os cuboideum aneinander fixiert.
1.2.2 Articulatio subtalaris (hinteres Gelenk, hintere Kammer)
Knöcherne Strukturen
In der Articulatio subtalaris artikulieren die nur wenig konvexen hinteren Flächen des Talus mit der posterioren Facette des Kalkaneus.
Ligamentäre Strukturen
Die Kapsel, die die Articulatio subtalaris umgibt, ist relativ schlaff und dünn. Sie wird durch die Ligg. talocalcanea mediale und laterale verstärkt. Das Lig. talocalcaneum interosseum dient als Trennwand zwischen vorderer und hinterer Kammer (▶ Abb. 15a, b). Es verläuft im knöchernen Tarsalkanal (Sinus tarsi), der vom Sulcus calcanei und Sulcus tali gebildet wird.
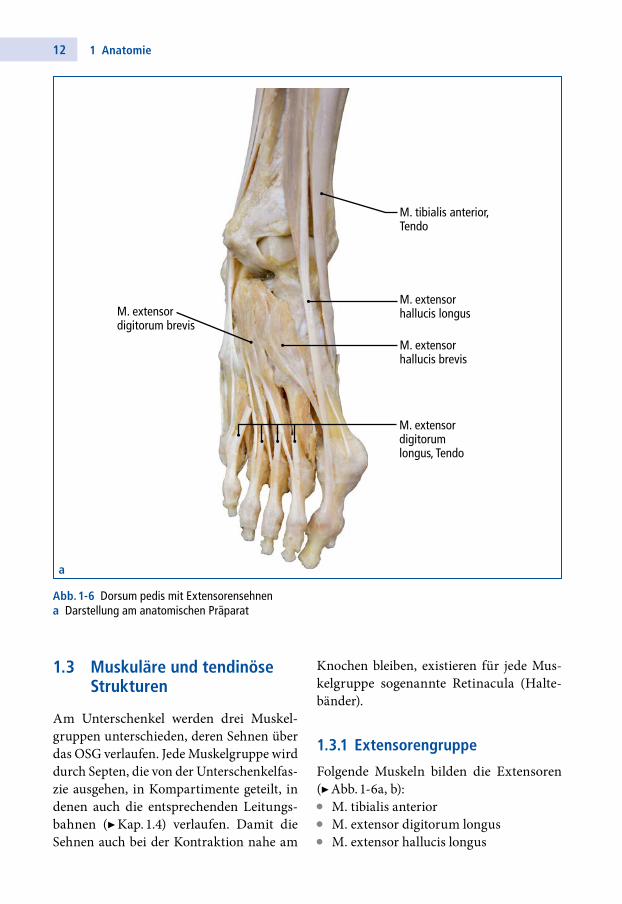
12 1 Anatomie
Knochen bleiben, existieren für jede Muskelgruppe sogenannte Retinacula (Haltebänder).
1.3.1 Extensorengruppe
Folgende Muskeln bilden die Extensoren (▶ Abb. 16a, b):• M. tibialis anterior• M. extensor digitorum longus• M. extensor hallucis longus
1.3 Muskuläre und tendinöse Strukturen
Am Unterschenkel werden drei Muskelgruppen unterschieden, deren Sehnen über das OSG verlaufen. Jede Muskelgruppe wird durch Septen, die von der Unterschenkelfaszie ausgehen, in Kompartimente geteilt, in denen auch die entsprechenden Leitungsbahnen (▶ Kap. 1.4) verlaufen. Damit die Sehnen auch bei der Kontraktion nahe am
M. tibialis anterior,Tendo
M. extensor hallucis longusM. extensor
digitorum brevis
M. extensorhallucis brevis
M. extensor digitorum longus, Tendo
Abb. 1-6 Dorsum pedis mit Extensorensehnena Darstellung am anatomischen Präparat
a
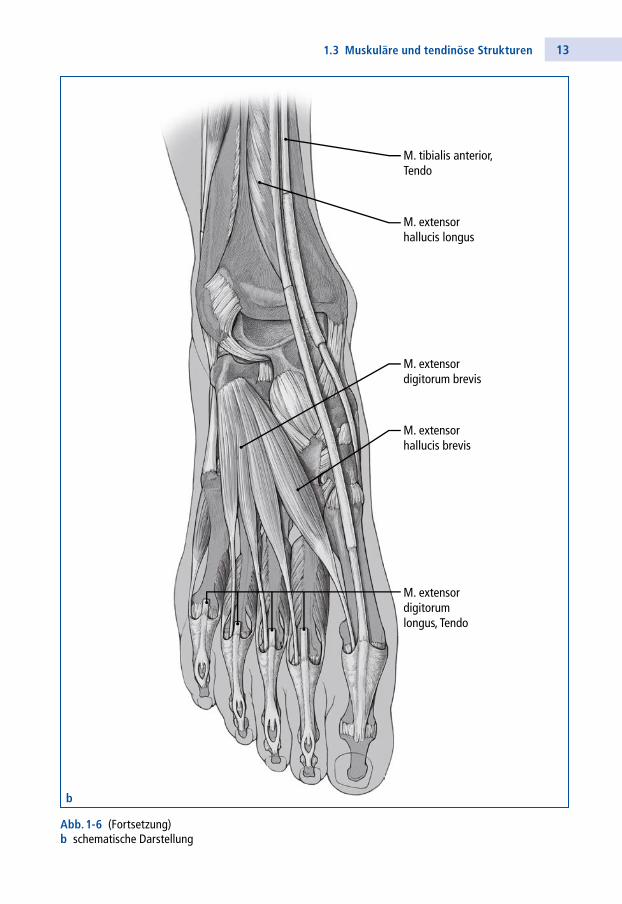
131.3 Muskuläre und tendinöse Strukturen
M. tibialis anterior,Tendo
M. extensor hallucis longus
M. extensor digitorum longus, Tendo
M. extensor hallucis brevis
M. extensor digitorum brevis
Abb. 1-6 (Fortsetzung)b schematische Darstellung
b
14 1 Anatomie
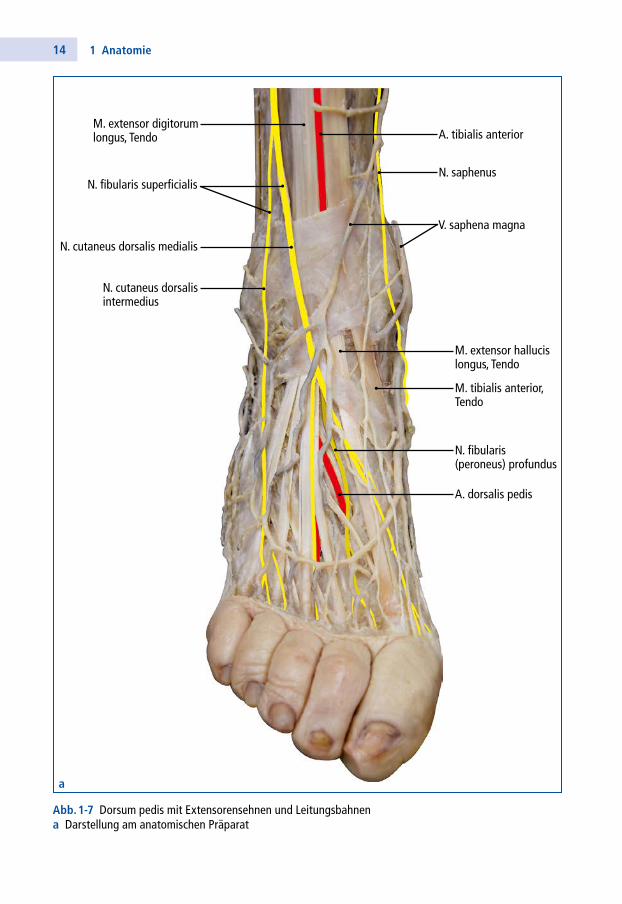
N. fibularis superficialisN. saphenus
A. tibialis anterior
A. dorsalis pedis
N. fibularis (peroneus) profundus
V. saphena magna
N. cutaneus dorsalis medialis
N. cutaneus dorsalis intermedius
M. extensor digitorum longus, Tendo
M. extensor hallucis longus, Tendo
M. tibialis anterior, Tendo
Abb. 1-7 Dorsum pedis mit Extensorensehnen und Leitungsbahnena Darstellung am anatomischen Präparat
a
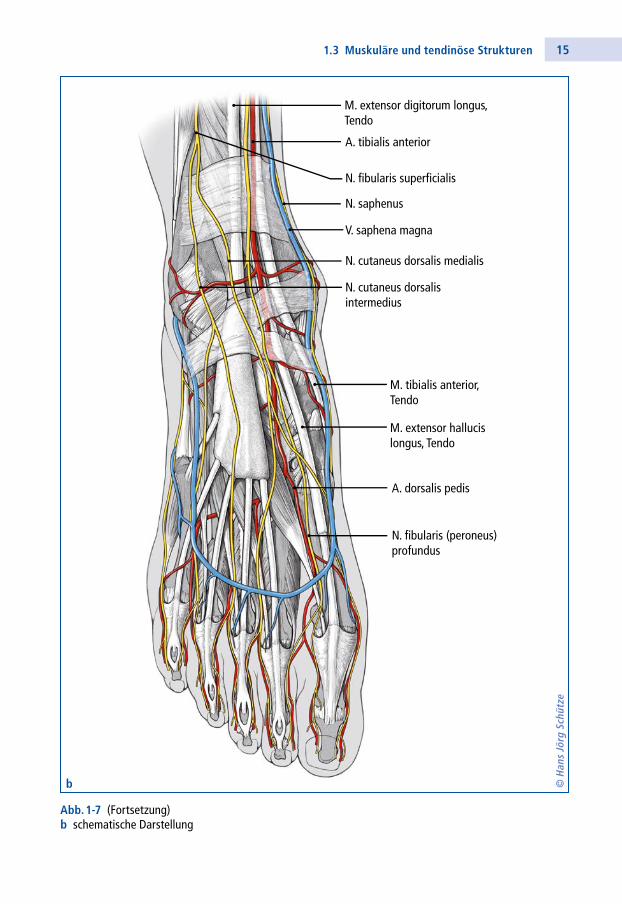
151.3 Muskuläre und tendinöse Strukturen
N. fibularis superficialis
N. saphenus
A. tibialis anterior
A. dorsalis pedis
N. fibularis (peroneus)profundus
V. saphena magna
N. cutaneus dorsalis medialis
N. cutaneus dorsalis intermedius
M. extensor digitorum longus,Tendo
M. extensor hallucis longus, Tendo
M. tibialis anterior, Tendo
Abb. 1-7bAbb. 1-7 (Fortsetzung)b schematische Darstellung
© H
ans
Jörg
Sch
ütze
b
16 1 Anatomie
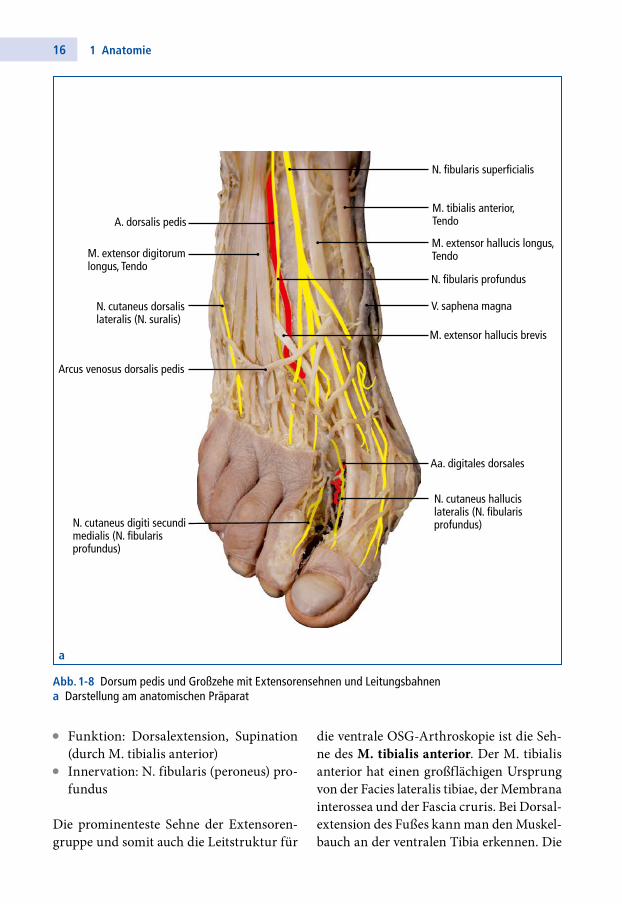
N. fibularis superficialis
V. saphena magna
M. extensor hallucis longus,Tendo
M. extensor hallucis brevis
Arcus venosus dorsalis pedis
Aa. digitales dorsales
M. tibialis anterior,TendoA. dorsalis pedis
N. cutaneus dorsalis lateralis (N. suralis)
N. cutaneus hallucislateralis (N. fibularis profundus)N. cutaneus digiti secundi
medialis (N. fibularis profundus)
N. fibularis profundus
M. extensor digitorumlongus, Tendo
Abb. 1-8 Dorsum pedis und Großzehe mit Extensorensehnen und Leitungsbahnena Darstellung am anatomischen Präparat
• Funktion: Dorsalextension, Supination (durch M. tibialis anterior)
• Innervation: N. fibularis (peroneus) profundus
Die prominenteste Sehne der Extensorengruppe und somit auch die Leitstruktur für
die ventrale OSGArthroskopie ist die Sehne des M. tibialis anterior. Der M. tibialis anterior hat einen großflächigen Ursprung von der Facies lateralis tibiae, der Membrana interossea und der Fascia cruris. Bei Dorsalextension des Fußes kann man den Muskelbauch an der ventralen Tibia erkennen. Die
a