Diagnose und Therapie der exokrinen Pankreasinsuffizienz ... · Klinik für Kleintiermedizin...
32
Klinik für Kleintiermedizin Diagnose und Therapie der exokrinen Pankreasinsuffizienz bei Hund und Katze PD Dr. med. vet. Peter Hendrik Kook DACVIM, DECVIM Baden-Badener Fortbildungstage 2016
Transcript of Diagnose und Therapie der exokrinen Pankreasinsuffizienz ... · Klinik für Kleintiermedizin...
Klinik für Kleintiermedizin
Diagnose und Therapie der exokrinen Pankreasinsuffizienz bei Hund und Katze
PD Dr. med. vet. Peter Hendrik Kook DACVIM, DECVIM
Baden-Badener Fortbildungstage 2016

Klinik für Kleintiermedizin
Darlegung potentieller Interessenkonflikte
Der Referent versichert, dass keine Interessenkonflikte bestehen, die sich aus einem Beschäftigungsverhältnis, einer Beratertät igkeit oder Zuwendungen für Forschungsvorhaben, Vorträge oder andere Tätigkeiten ergeben.

Klinik für Kleintiermedizin
Exokrine Pankreasinsuffizienz (EPI) - Definition
Funktionelle Erkrankung des exokrinen Pankreas
Inadequate Enzymproduktion führt zu klinischen Zeichen einer Maldigestion
Klinische Zeichen erst bei Verlust von ca. 90% der sekretorischen Kapazität
Klinik für Kleintiermedizin
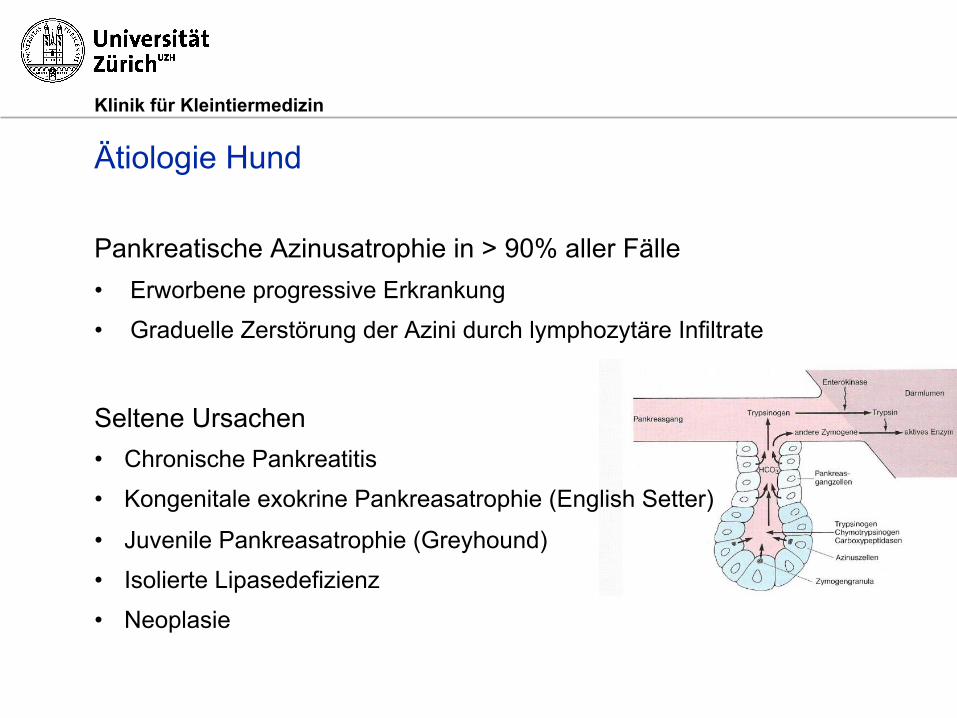
Ätiologie Hund
Pankreatische Azinusatrophie in > 90% aller Fälle • Erworbene progressive Erkrankung
• Graduelle Zerstörung der Azini durch lymphozytäre Infiltrate
Seltene Ursachen • Chronische Pankreatitis
• Kongenitale exokrine Pankreasatrophie (English Setter)
• Juvenile Pankreasatrophie (Greyhound)
• Isolierte Lipasedefizienz
• Neoplasie

Klinik für Kleintiermedizin
Ätiologie Hund
DSH ! Langhaarcollie
Eurasier / Chow Chow
WHWT Prinzipiell jede Rasse

Klinik für Kleintiermedizin
Ätiologie Hund
Cavalier King Charles Spaniel (CKCS) • Chronische Pankreatitis als Ursache
• Medianes Alter bei Diagnose EPI 7 Jahre
Kent et al. JSAP 201

Klinik für Kleintiermedizin
Ätiologie Hund
Alter bei Diagnosestellung: • Median 3.5 Jahre
• Intervall: 3 Monate -17 Jahre
CKCS signifikant älter
• Median 7 Jahre
• Intervall: 2-13 Jahre
Batchelor et al. JVIM 2007

Klinik für Kleintiermedizin
Ätiologie Hund
Isolierte pankreatische Lipasedefizienz • Klinik einer EPI (Polyphagie, Gewichtsverlust, voluminöser Kot)
• Normale TLI-Resultate (> 5 µg/l)
• Exzellentes Ansprechen auf Enzymsupplementation
• Junge Hunde von „Risikorassen“ Viviano und Ziglioli, JVIM 2013
• Sibirischer Husky Xenoulis et al. JVIM 2007

Klinik für Kleintiermedizin
Ätiologie Katze
Keine Rasseprädisposition Medianes Alter ≈ 7J (4 Mon - 16J) Steiner et al. JVIM 2000, Thompson et al. JFMS 2009, Kook et al. Schweiz Arch Tierheilkd 2011, Xenoulis et al. ACVIM 2011
Pankreatische Azinusatrophie noch nicht beschrieben
Chronische Pankreatitis Hauptursache
EPI Katzenwelpen mit histologisch bestätigter chronischer Pankreatitis beschrieben Perry et al. JAAHA 1991

Klinik für Kleintiermedizin
Ätiologie Katze
Juvenile Pankreasatrophie • Endokrines + exokrines Pankreas (EPI + DM)

Klinik für Kleintiermedizin
Ätiologie Katze
Pankreatische lipomatöse Pseudohypertrophie • Pankreas mit normaler Grösse, weich, cremig-gelblich • Keine Entzündung
• Massive Fettinfiltration • Ursache unklar
Dobromylskyj und Dobromylskyj, JFMS 2015 Klinik: Polyphagie, Gewichtsverlust

Klinik für Kleintiermedizin
Klinische Zeichen Hund
Oft • Erhöhtes Stuhlvolumen und
-frequenz
• gelblicher, weicher Kot • zT schlecht verdauter Kot
• Flatulenz
• Polyphagie • Gewichtsverlust
Selten • Wässriger Durchfall
• Seborrhoe
• Koprophagie
• Nervosität, Aggressivität • Rasse ? (Schäferhund)

Klinik für Kleintiermedizin
Klinische Zeichen Katze
Gewichtsverlust Polyphagie ODER Anorexie
Apathie
Verdauung unterschiedlich • Weicher (geformter) Kot ⅔
• Wässriger Durchfall ⅓
Erbrechen Seborrhoe

Klinik für Kleintiermedizin
Diagnose
Routinelabor idR obB • Amylase und Lipase-Aktivität nicht hilfreich
TLI (cTLI / fTLI) = Test der Wahl • TLI = Trypsin-like Immunreactivity
Normalbereich: 5.7-45.2 µg/l
• cTLI < 2.5 µg/l diagnostisch für EPI
• cTLI zw. 2.5-5 µg/l selten mit Klinik einer EPI assoziiert (subklinische EPI)

Klinik für Kleintiermedizin
Diagnose via TLI Messung
Median 0.7µg/l (0.5-1.5) bei 25 Hunden mit EPI Median 10.7 µg/l (5-46) bei 74 gesunden Hunden
cPLI kein idealer Test für EPI
Gesunde Hunde oft mit tiefen cPLI Werten Steiner et al. AJVR 2006

Klinik für Kleintiermedizin
Diagnose bei der Katze
fTLI Referenzbereich: 12.0 - 82.0 µg/l Werte < 8 µg/l diagnostisch für EPI Steiner et al. JVIM 2000
Werten zw. 8 – 10 (12) µg/l ? • Wiederholtes Testen empfohlen
• Beginn Supplementation mit Enzymen
• Niereninsuffizienz ? (renale Exkretion Trypsinogen)
Klinik für Kleintiermedizin
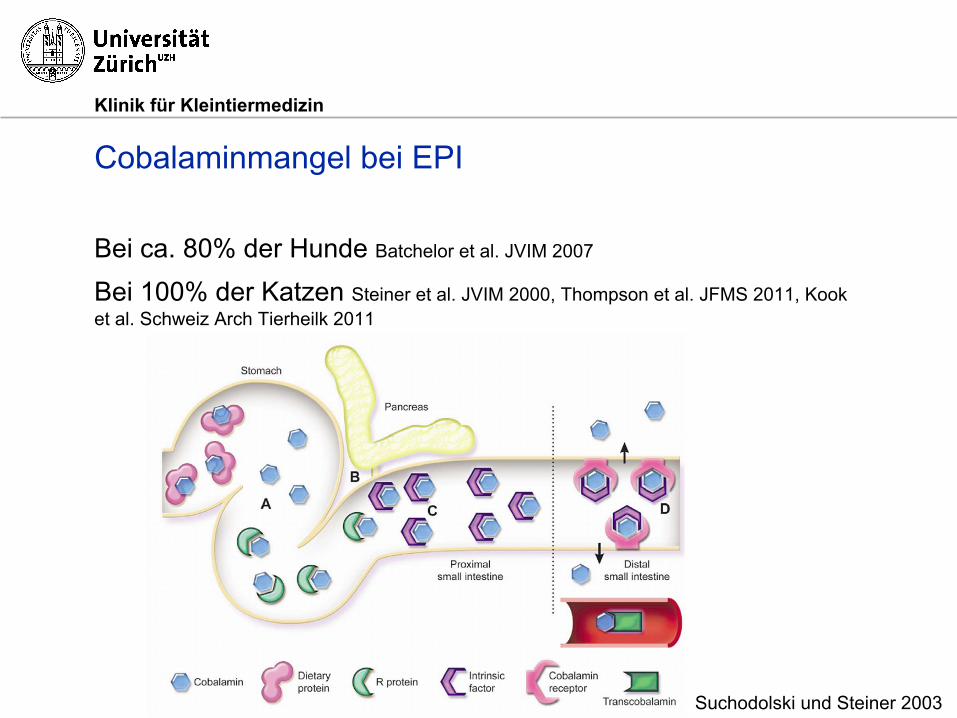
Cobalaminmangel bei EPI
Bei ca. 80% der Hunde Batchelor et al. JVIM 2007
Bei 100% der Katzen Steiner et al. JVIM 2000, Thompson et al. JFMS 2011, Kook et al. Schweiz Arch Tierheilk 2011
Suchodolski und Steiner 2003

Klinik für Kleintiermedizin
Cobalaminmangel bei EPI
h
Batchelor et al. JVIM 2007

Klinik für Kleintiermedizin
Therapie - Futter
Fettarm, faserreich, hoch-verdaulich...?
Weniger Flatulenz/Borborygmi, Kotvolumen und -frequenz mit fettreduzierter, faserarmer, hochverdaulicher Diät Westermarck et al. Acta Vet Scand 1990
Fettgehalt ohne Einfluss auf Klinik einer EPI Westermarck et al. 1995 AJVR

Klinik für Kleintiermedizin
Therapie - Futter
ä

Klinik für Kleintiermedizin
Therapie - Futter
Fazit: Fütterung wichtig im EPI- Management
Hohe interindividuelle Variation
⇒ Ideale Diät durch individuelles «trial and error» herausfinden

Klinik für Kleintiermedizin
Therapie - Enzymsupplementation
= Therapie der Wahl Enzympulver (zB Kreon®, Pancrex®)
• 2 TL pro 20 kg KGW pro Mahlzeit
• Dosisreduktion möglich (idR mind 1 TL/Mahlzeit notwendig) • Blutung aus Maul als seltene Komplikation
Rohes Pankreas (Schwein) • ≈ 80-90 g / Mahlzeit (kann gefroren werden)
• Deutlich günstiger, evtl. schlechtere Akzeptanz

Klinik für Kleintiermedizin
Therapie
Problem ist der saure Magen….. • pH 1-2 in ≈ 90% der Zeit Kook et al. JVIM 2014
• Zerstörung von Amylase und Lipase bei pH < 3.5
Mensch • Enzyme in Mikrokugeln mit magensaftresistentem Überzug
Hund • Bisher widersprüchliche Resultate Hall et al. JSAP 1991, Batchelor et al.
JVIM 2007

Klinik für Kleintiermedizin
Therapie - Update
RESEARCH ARTICLE Open Access
A blinded randomised controlled trial todetermine the effect of enteric coating onenzyme treatment for canine exocrine pancreaticefficiencyAran Mas1†, Peter-John M Noble1†, Peter J Cripps1, Daniel J Batchelor1, Peter Graham2 and Alexander J German1*
Abstract
Background: Enzyme treatment is the mainstay for management of exocrine pancreatic insufficiency (EPI) in dogs.‘Enteric-coated’ preparations have been developed to protect the enzyme from degradation in the stomach, buttheir efficacy has not been critically evaluated. The hypothesis of the current study was that enteric coating wouldhave no effect on the efficacy of pancreatic enzyme treatment for dogs with EPI.Thirty-eight client-owned dogs with naturally occurring EPI were included in this multicentre, blinded, randomisedcontrolled trial. Dogs received either an enteric-coated enzyme preparation (test treatment) or an identicalpreparation without the enteric coating (control treatment) over a period of 56 days.
Results: There were no significant differences in either signalment or cobalamin status (where cobalamin deficientor not) between the dogs on the test and control treatments. Body weight and body condition score increased inboth groups during the trial (P<0.001) but the magnitude of increase was greater for the test treatment comparedwith the control treatment (P<0.001). By day 56, mean body weight increase was 17% (95% confidence interval11-23%) in the test treatment group and 9% (95% confidence interval 4-15%) in the control treatment group. Thedose of enzyme required increased over time (P<0.001) but there was no significant difference between treatmentsat any time point (P=0.225). Clinical disease severity score decreased over time for both groups (P=0.011) and nodifference was noted between groups (P=0.869). No significant adverse effects were reported, for either treatment,for the duration of the trial.
Conclusions: Enteric coating a pancreatic enzyme treatment improves response in canine EPI.
Keywords: Dog, Pancreas, Malabsorption, Diarrhoea, Lipase, Trypsin
BackgroundExocrine pancreatic insufficiency (EPI) is a commoncondition in dogs, resulting from inadequate functionalreserve of pancreatic acinar tissue [1]. The most com-mon cause of EPI is pancreatic acinar atrophy, althoughother causes have been reported, including chronic pan-creatitis, pancreatic neoplasia and (possibly) congenitalhypoplasia. Clinical signs only develop when a critical
mass (e.g. >90%) of exocrine tissue has been lost, andresult from maldigestion and subsequent malabsorption.Clinical management usually involves enzyme replace-
ment therapy with the addition of dietary modification(e.g. highly digestible diet) and ancillary therapies (e.g.antibacterials) if response to enzyme alone is poor [1].Most dried pancreatic extracts are given as a powderedformulation, although ‘enteric-coated’ preparations havebeen developed in which granules of enzyme powder arecoated in a lacquer that protects the enzymes from deg-radation in the stomach. However, whilst widely used,the effectiveness of enteric-coated preparation has beenquestioned, and one study found that such formulations
* Correspondence: [email protected]†Equal contributors1School of Veterinary Science, University of Liverpool, Neston, UnitedKingdomFull list of author information is available at the end of the article
© 2012 Mas et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.
Mas et al. BMC Veterinary Research 2012, 8:127http://www.biomedcentral.com/1746-6148/8/127

Klinik für Kleintiermedizin
Therapie - Update
At this stage, the purpose of the trial was again dis-cussed with the owner and, assuming that they werehappy, they were asked to sign the study consent form.Thereafter, dogs were allocated a study number and thetreatment dispensed. The owners were instructed onhow to use the treatment and any specific questions thatthe owner had were answered at this stage.
Monitoring, treatment alterations and follow-upA summary of the study protocol is given in Figure 1.Throughout the trial, dogs returned on a weekly basisfor administration of subcutaneous cobalamin (seebelow). Detailed assessments were conducted on days14, 28 and 56. At each visit, a physical examination wasperformed, body weight was measured (using the sameelectronic scales as for the first visit), and a body condi-tion score was performed. In addition, clinical signs wereagain scored using the same questionnaire as for the ini-tial visit. Compliance with administration of the treat-ment was confirmed and, if necessary, dosage alterationswere made and additional therapy was added.In addition to the official re-evaluation visits, clients
contacted either the attending veterinarian or studyobservers using telephone calls and, occasionally, e-mailupdates.
Treatment alterations, use of additional therapy, and dietThe intention was that only the enzyme supplement andweekly cobalamin injections (see below) would be admi-nistered during the trial. However, in accordance withnormal clinical practice, alterations in enzyme dose andthe addition of other therapies were allowed if responseto therapy was poor. Primary care veterinarians made alltreatment changes, after discussing them with one of thestudy observers, and in accordance with a standardisedprotocol. In this regard if, at the first reassessment(14 days), clinical response was deemed to be insufficient(e.g. poor weight gain, lack of resolution of clinicalsigns), the dose of enzyme was doubled. A further en-zyme dosage increases were allowed on days 28 and 56,if necessary.Given that hypocobalaminaemia is a negative prognos-
tic indicator in canine EPI [3], and in order to ensure thatthis was not a confounding factor during the trial, weeklysubcutaneous injections of cobalamin (at 20 μg/kg) wereadministered to all dogs. This treatment was given irre-spective of whether hypocobalaminaemia was present inpre-trial serum biochemical results. No other treatmentwas initially allowed in any of the dogs. Additional ther-apies were avoided as far as possible but if, in the opinionof the attending veterinarian they were deemed to be ne-cessary, then they could be added from third visit (week
Figure 1 Summary of the trial design and inclusion of dogs. Forty dogs, with exocrine pancreatic insufficiency, were randomised to receiveone of two enzyme treatments (test e.g. coated and control e.g. uncoated), and were re-examined at 3 follow-up visits (day 14, day 28 and day56). Information in the lower part of the figure refers to the procedures conducted at each visit. BCS: body condition score; LTFU: lost to followup. Arrows indicate when doses of parenteral cobalamin were injected. Other than the timeline, all numbers refer to dogs recruited andremaining within the trial at the respective points.
Mas et al. BMC Veterinary Research 2012, 8:127 Page 4 of 11http://www.biomedcentral.com/1746-6148/8/127
Klinik für Kleintiermedizin
Therapie - Update
As with any study, limitations must be consideredwhen interpreting findings. Firstly, group sizes weresmall, and study withdrawals reduced further the abilityto make comparisons. In addition to this, trial recruit-ment was slower than expected, requiring changes in therecruitment protocol (e.g. multi-centre vs. single-centrerecruitment) and the sacrifice of two batches of therapy(one test and one treatment) to verify that enzyme activ-ity was maintained. Despite these problems, differenceswere identified for the primary outcome measure, sug-gesting that the study power had been sufficient. Thatsaid, the use of larger group sizes might have enabledsubtle differences in the secondary outcome measures tobe identified. The switch from single-centre to multi-centre design was an added complication, and meantthat 5 cases were recruited from one centre, with inher-ent concerns of introducing unwanted influence or pos-sible bias. However, since these 5 cases were, more orless, evenly distributed between treatment groups, it isunlikely that this one centre had any undue influence.The cases from the only other practice to recruit morethan one case were randomly assigned to the same treat-ment group (e.g. test treatment) group. Although notideal, the effect of this small ‘cluster’ is not likely to have
had a major bearing on outcome. A third limitation wasthe fact that the study was short term and, arguably, alonger period of therapy would have helped to determinewhether the treatment advantage identified was main-tained, if the relative lack of efficacy of the control treat-ment could ultimately have been overcome by furtherdose increases, and if delayed side effects of the therap-ies developed. That said, initial response (e.g. the first2-3 months) has been shown to be critical in predictinglong-term response [3]. Longer term and larger scaletrials are now recommended, to enable a more completeunderstanding of the treatment advantage that entericcoating provides.A further study limitation was the fact that diet was
not standardised amongst study dogs, and details ofexact diets were not recorded as part of the study. Diet-ary management is recommended as adjunctive therapyin canine EPI, and the most important considerationappears to be in fat content with fat restriction recom-mended in some [10,11], but not all [12,13], studies. Fur-ther, prospective studies have not demonstrated a clearbenefit of any specific diet in the treatment of canineEPI [13-15]. In fact, different diet types (i.e. low fat, nor-mal fat high fibre) appeared to suit different dogs,
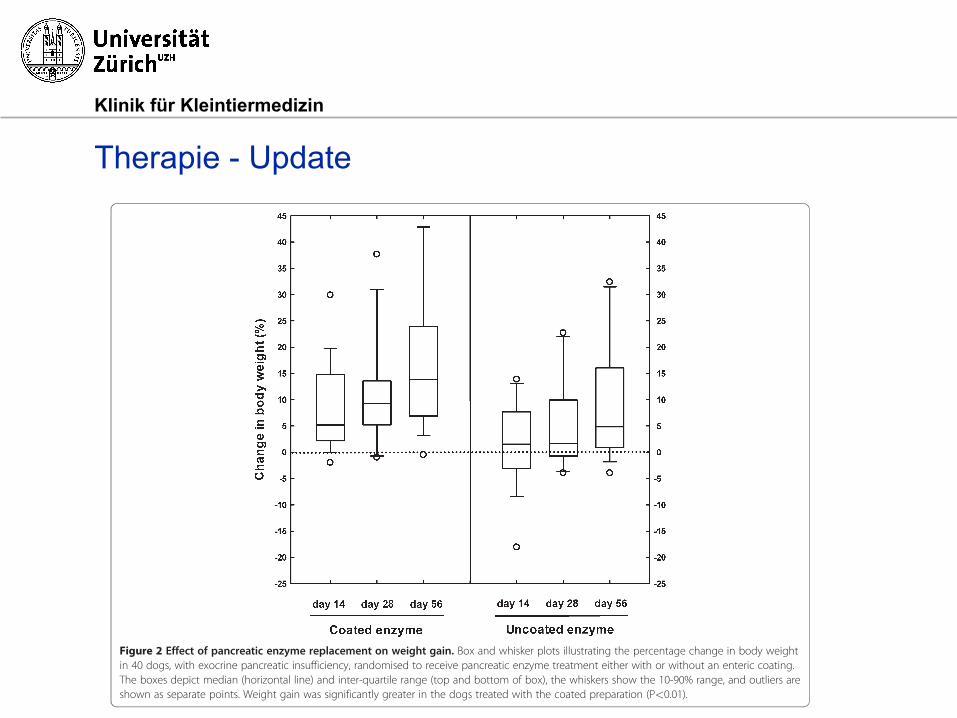
Figure 2 Effect of pancreatic enzyme replacement on weight gain. Box and whisker plots illustrating the percentage change in body weightin 40 dogs, with exocrine pancreatic insufficiency, randomised to receive pancreatic enzyme treatment either with or without an enteric coating.The boxes depict median (horizontal line) and inter-quartile range (top and bottom of box), the whiskers show the 10-90% range, and outliers areshown as separate points. Weight gain was significantly greater in the dogs treated with the coated preparation (P<0.01).
Mas et al. BMC Veterinary Research 2012, 8:127 Page 9 of 11http://www.biomedcentral.com/1746-6148/8/127

Klinik für Kleintiermedizin
Therapie - Update
Gewichtszuwachs 17 % (11-23) mit Magensaftschutz Gewichtszuwachs 9 % (4-15) ohne Magensaftschutz • 30 kg Hund: 2.7 versus 5.1 kg

Klinik für Kleintiermedizin
Therapie - Antibiotika
EPI führt zu bakterieller Überwucherung im Dünndarm Keine Normalisierung mit Enzymsupplementation Westermarck et al. Pancreas 1993
Tylosin (Tylan®) Dosis ≈ 15 mg/kg BID
Reduktion auf bis zu 5 mg/kg SID möglich
Metronidazol
Dosis 10-15 mg/kg SID oder BID

Klinik für Kleintiermedizin
Therapie – Probiotika
Sivoy® als Alternative ? • 1 Beutel 1 x tgl.
• Mehrere Bakterienstämme
Dauergabe von Antibiotika problematisch
Längere Zeit bis zur günstigen Modulation des Mikrobiom ?
Klinik für Kleintiermedizin
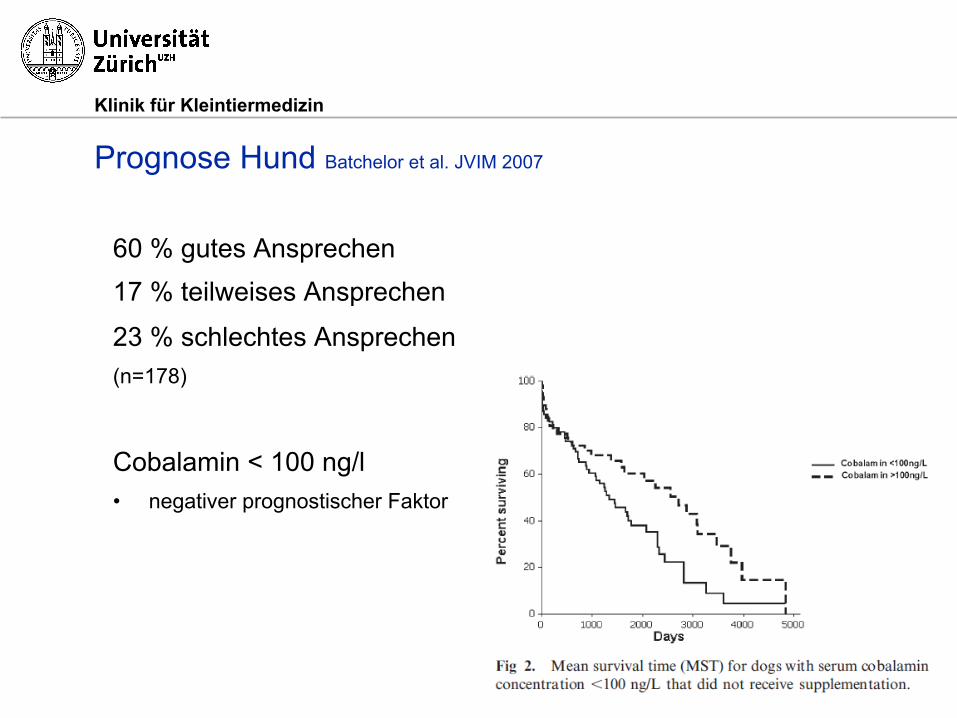
Prognose Hund Batchelor et al. JVIM 2007
60 % gutes Ansprechen 17 % teilweises Ansprechen
23 % schlechtes Ansprechen (n=178)
Cobalamin < 100 ng/l • negativer prognostischer Faktor

Klinik für Kleintiermedizin
Prognose Katze Xenoulis et al. ACVIM 2011
66 % gutes Ansprechen 24 % teilweises Ansprechen
10 % schlechtes Ansprechen (n=102)
Cobalaminkonzentration als Faktor bisher nicht untersucht

![Aus der Klinik für Allgemeine Chirurgie und ... · zweithäufigsten Tumoren des Pankreas [4]. Etwa 95% der Pankreastumoren haben ihren Ursprung im exokrinen Pankreas und sind zu](https://static.fdokument.com/doc/165x107/5e1bcb468ca13c07cc5e7e22/aus-der-klinik-fr-allgemeine-chirurgie-und-zweithufigsten-tumoren-des-pankreas.jpg)