Dr M Norberg Réadaptation en - Reha Schweiz · Réadaptation en cas d’altérations...
65
Réadaptation en cas d’altérations inflammatoires de l’appareil locomoteur : l’importance de l’activité physique Rehabilitation bei entzündlichen Veränderungen am Bewegungsapparat, Wichtigkeit der Bewegung“ Dr M Norberg
Transcript of Dr M Norberg Réadaptation en - Reha Schweiz · Réadaptation en cas d’altérations...
Réadaptation en
cas d’altérations
inflammatoires de
l’appareil
locomoteur :
l’importance de
l’activité physique Rehabilitation bei
entzündlichen Veränderungen
am Bewegungsapparat,
Wichtigkeit der Bewegung“
Dr M Norberg
2 2 2

MENU
• Refresh: basics in
inflammation
• Lumbar pain: Modic
and inflammation
• AR
– rehabilitation
• SPA
– rehabilitation
3

Frequency
Literature suggests that 26% of patients with
rheumatoid arthritis were referred for
physical therapy and/or occupational
therapy Li LC, Bombardier C.. Physiother Can 2003; 55:23–30
4
2004
Current Opinion in Rheumatology 2004, 16:130–131
5
2008
Mayoux-Benhamou, Joint Bone Spine 75 (2008) 3-4
6

2008
Current Opinion in Rheumatology 2008, 20:218–219
7
2016
F. Gérald ,P. StéveninLa revue du praticien 2016 (66) , 631-2
8

2017
Berdal et al, Disability and Rehabilitation, 2017 10.1080/09638288.2016.1275043
9

Part 1: Basics
Physiology effects of exercise
10

Exercise-induced cytokines in arthritis
model mice
•Exercise delayed the onset of arthritis and slowed
its progression
•Thickened articular cartilage
•↑the expression of IL-6, IL-10, IL-15,
•inhibited TNF-α expression.
•=>anti-inflammatory IL-6/IL-10, inhibited
the inflammatory activity of TNF-α
•=>delayed the onset of arthritis
•=>slowed its progression
11
Kito et al Okajimas Folia Anat Jp 2016
The cells
•The leucocytes ↑ during exercise and ↓ after long standing exercises
•But neutrophiles ↑ during and after an intense exercise:
•*The reason is that the recruited cells come from mature cells and not from steam cells on maturation.
•During exercise the proportion CD4/CD8 ↓
since the > ↑ of TCD8+.
•NK CD94+ / - ↑
Nemet D et al Br J Sports med 2004; 38: 154-8
12

The cytokine pathway
Physical exercise produces: ↑ IL1 and IL6.
During a marathon
↑ TNFα and IL1β (2x),↑ IL6 (50x).
↑ of IL1 RA,
↑ soluble receptors of TNF and the IL10 with
anti-inflammatoiry effects.
IL8, CCL3 and CCL4 ↑ after a marathon.
Chemokine (C-C motif) = Macrophage inflammatory protein
13
But if too intense:
Temporary negative incidence on immune function.
The ↓ in the immune function after exercise is more important...
•..when the exercise is more intense, longer ( > 1.5 h),
•..if it is done with medium or high intensity (55 to 75 % of the aerobic capacity)
•..without eating
Gleeson, M et al Exerc. Sport Sci. Rev. 2013 41:148-153. 14
Effects of physical activity on
inflammation
9 weeks of resistance training
•beneficial effects on circulating IL-8, IL-6.
•↑ anti-inflammatory cytokines sTNFR1 and
IL-1RA.
•resistance training has anti-inflammatory
effects in healthy young persons
Forti et al Eur J Appl Physiol 2017
15
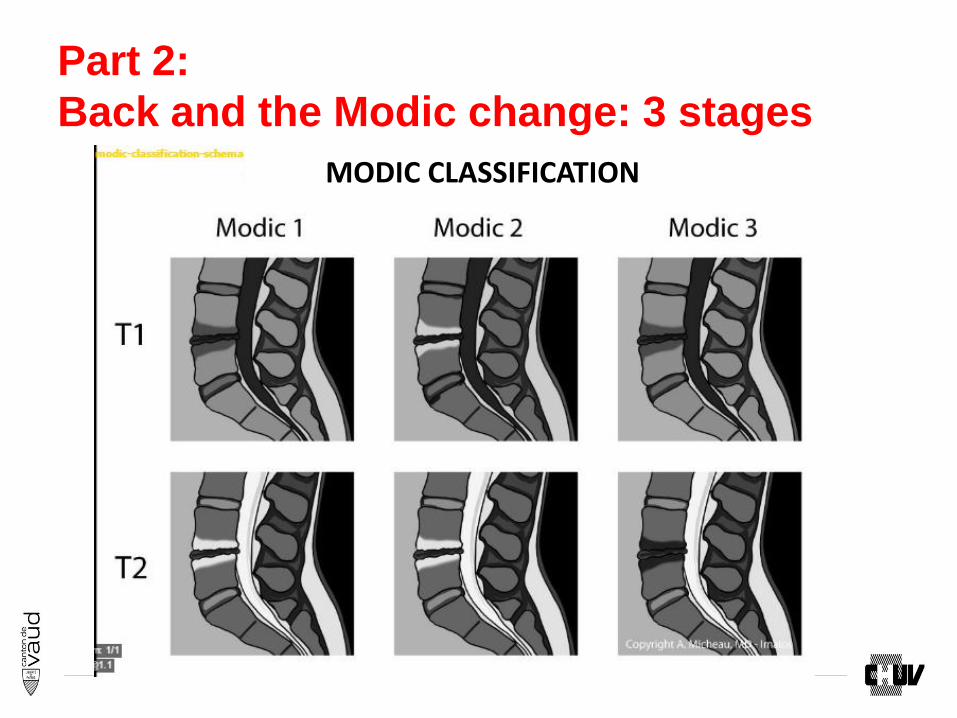
Part 2:
Back and the Modic change: 3 stages
MODIC CLASSIFICATION
16
Back anatomy: importance VSB
VSB integrity, rather than the degree
of disk deg, determines the extent of
damage during compression
VSB vessels ensure cartilage endplate and
avascular–intervertebral- disk nutrition by
diffusion of dissolved molecules through
marrow contact channels C. Nguyen et al Osteoporos Int (2012) 23 (Suppl 8):S857–S860
VSB: Vertebral subchondral bone
17

But…
• Not all patients with
disc/endplate damage
develop MC.
• => related to the
inflammatory potential
of the disc and the
capacity of the BM to
respond to the
inflammatory
stimulus.
18
Eur Spine J (2016) 25:3723–3734
Epidemiology of Modics
Prevalence is high in LBP : 43 % compared to 6 % in asymptomatic population.
• Jensen T et al Eur Spine J 2008,17:1407–1422.
MC1 more associated LBP than the others • Thompson KJ et al Radiology 2009 250:849–855
• Järvinen J et al BMC Musculoskelet Disord 2015; 16. 98
More prevalent and more severe at L4–S1 • Modic MT et al Radiology 1988 166:193–199
• Kuisma M et al Spine 2007 32:1116–1122 ,
More prevalent in the anterior third of vertebra • Chung CB et al Skeletal Radiol 2004 33:399–404
• Karchevsky et al Skeletal Radiol 2005 34:125–12913
Generally symmetric cephalad and caudad to a particular disc
• Kuisma M et al. Spine 2006 31:1714–1718
19
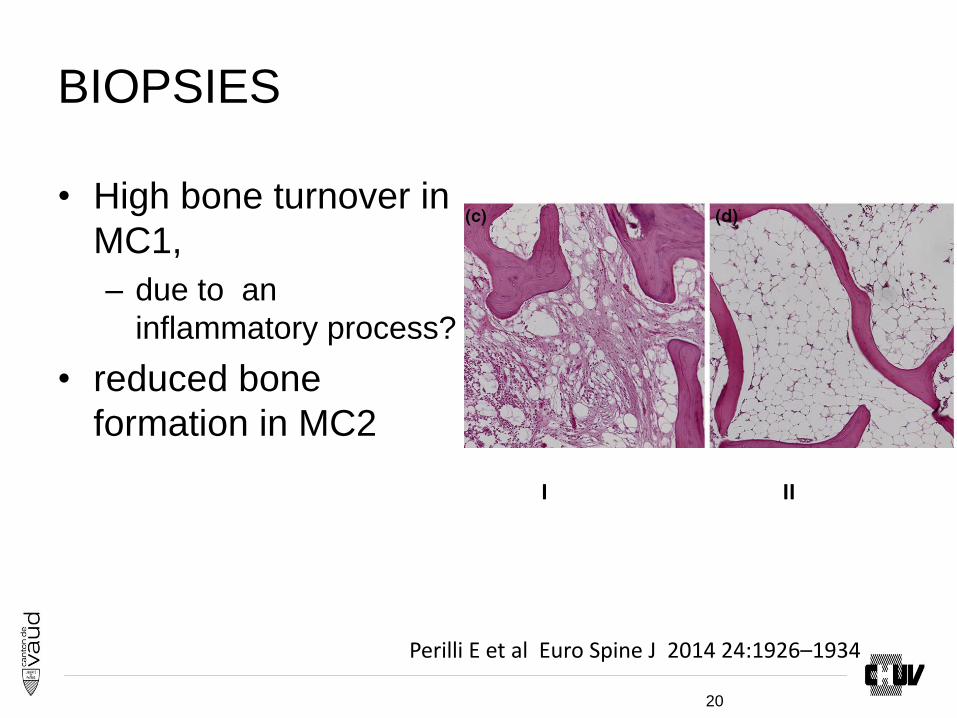
BIOPSIES
• High bone turnover in
MC1,
– due to an
inflammatory process?
• reduced bone
formation in MC2
I II
Perilli E et al Euro Spine J 2014 24:1926–1934
20

Risk factors for Modic I / II
M I
M I / II M I / II
21 Eur Spine J (2016) 25:3723–3734
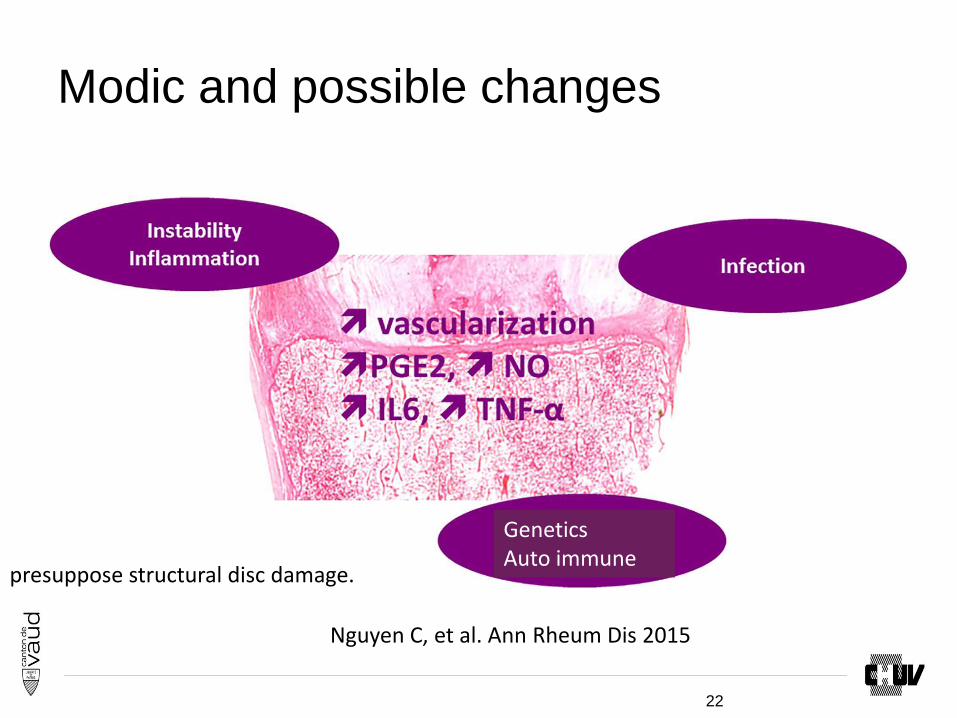
Modic and possible changes
Nguyen C, et al. Ann Rheum Dis 2015
Genetics Auto immune
presuppose structural disc damage.
22

The inflammatory potential of the disc
• Discs adjacent to MC produce more:
• cytokines – (IL-6, IL-8, TNF-a)
• osteoclastic factors – (RANKL, M-CSF,
NFATc1, RUNX1, OSCAR)
• than discs of the same degeneration degree without MC
23
Eur Spine J (2016) 25:3723–3734

Hyp infection
* disc’s anaerobic: ↑potential for disc tissue damage,
↓ capacity for repair. =>low virulent skin microorganisms such as P. acnes
• Stirling A et al (2001) Lancet 357:2024–2025
Disc cells : ↑ IL-6, IL-8, PGE-2 after stimulation =>The persistent efflux of cytokines and bacterial metabolites cause inflammation of the adjacent BM .
• Wedderkopp N et al (2009). Acta Radiol 50:65–70.
C-reactive protein ↑ • Rannou F, et al (2007) Arthritis Rheum 57:1311–1315
Antibiotic treatment • Albert et al Eur Spine J (2013) 22:697–707
24
7.5.2013
25

Results
VAS
0
1
2
3
4
5
6
7
8
AB back pain
AB leg pain
Placebo back pain
Placebo leg pain
Roland-Morris
0
2
4
6
8
10
12
14
16
AB
Placebo
26

Hyp: auto-immunity
•Nucleus pulposus (NP) no contact with the systemic circulation: no leucocytes contact.
• NP cells express Fas ligand, => apoptosis in infiltrating lymphocytes .
• Kaneyama S et al J Orthop Sci 2008 13:130–135.
•Endplate damage co-locates NP with BM leukocytes.
•↑ levels of Fas receptor in MC endplates, =>adaptive response to higher levels of Fas ligand, possibly from colocated NP .
• Wang F et al Injury 2011 42:790–795
•Peripheral disc damage expose the NP to the
immune system, => recognized as ‘‘foreign’’ and triggers an autoimmune response
• Dudli et al Eur Spine J (2016) 25:3723–3734
27

Ann Intern Med. doi:10.7326/M16-1700_ 21.3.2017
28

Results in VAS in Modic I patients
BUT…. 29
Secondary outcomes
And at 1/ 3/12 month after the intervention:
•No differences in
•QBPDS
•SF12
•HADS
•Analgesics / NSIAD
•work
30

Part 3: AR and SPA
31

Get moving! Dynamic exercise therapy
for rheumatoid arthritis
1) Getting our patients to move
2) Educating healthcare professionals
3) Educating rheumatoid arthritis patients
Mayoux-Benhamou, Revue du Rhumatisme 75 (2008) 5–7
32
Aim rehab
↓pain
Prevent and treat deformations
Recover and stabilise articular mobility and
stability
Continuous muscular training ( aerobic
capacity)
Functional adaptations and capacity
Quality of life
33
Pleasure and exercices
• enjoyment important
in motivating people
with arthritis to
exercise.
• advice regarding
feasible and
enjoyable exercise.
Kibblewhite et al Musculoskeletal Care 2016
34
Therapeutic education
On a 3 days education programme
(sessions of education, individual and group
physiotherapy, exchanges) to obtain an
improvement in the patients personal
knowledge.
Sudre A et al. Joint Bone Spine 2012;79: 99–100
35

Spondyloarthropathies (SpA)
36

ACR 2015: SPA active
strongly recommend treatment with
physical therapy over no treatment with
physical therapy
conditionally recommend active physical
therapy interventions (supervised exercise)
over passive physical therapy interventions
conditionally recommend land-based
physical therapy interventions over aquatic
therapy interventions
Ward et al:ARTHRITIS & RHEUMATOLOGY 2016, 68, 2, 282–298
37
ACR 2015: SPA stable
In adults with stable AS, it is strongly
recommend to treat with physical therapy
over no treatment
Ward et al:ARTHRITIS & RHEUMATOLOGY 2016, 68, 2, 282–298
38
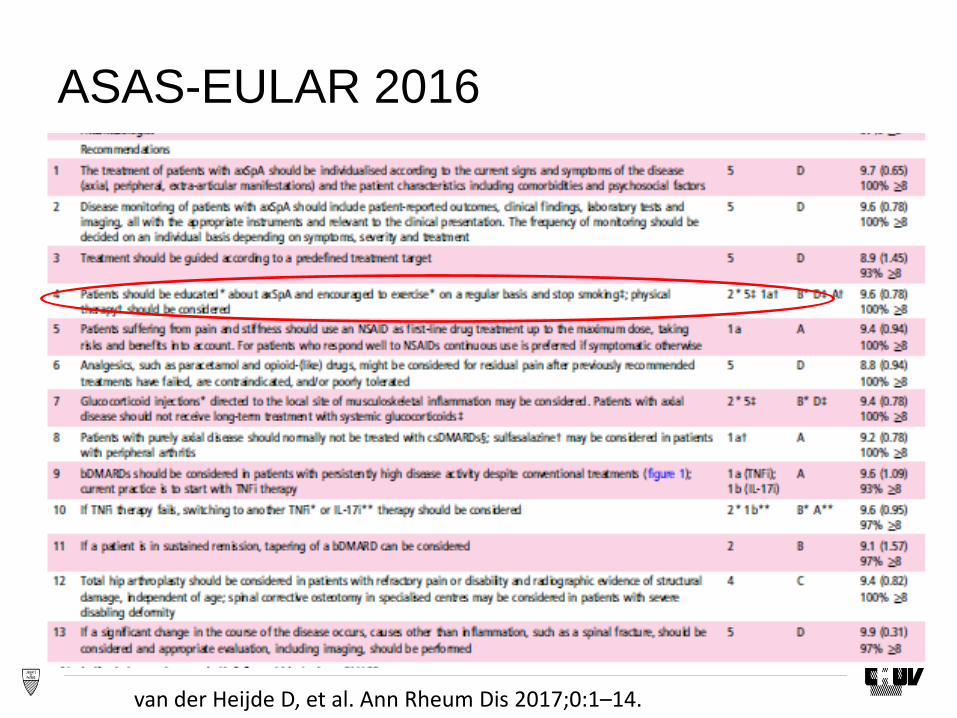
ASAS-EULAR 2016
van der Heijde D, et al. Ann Rheum Dis 2017;0:1–14. 39

Exercices
*Home exercises are efficacious and these
are therefore recommended to patients
*Physical therapy is proven to be
More efficacious than home exercises,
But more expensive and less feasible than
home exercises
May be required in some patients.
Dagfinrud H et al. Cochrane Database Syst Rev 2008
40
Exercices in SPA
• Several studies have showed that supervised group exercise provides superior results compared to an unsupervised HEP – Hidding A, et al. Arthritis
Care Res 1993
– Analay Y, et al. Clin Rehabil 2003
– Silva EM et al. Rheumatol Int 2012
41

Ex and SPA
42
Which exercices?
to maintain mobility and strength, as eccentric work of the erector spine muscle, the posterior muscle chain in the pelvic region, and the anterior chain of the scapular girdle
relieve symptoms,
prevent or limit spinal deformity,
long-term cardiopulmonary health,
improve quality of life.
behavioral interventions ↑ disease knowledge
↑ motivation for compliance
Millner et al.Sem Arthritis Rheum 2016
43

Exercise and SPA: anti-inflammatory
effects? What is known?
the antiinflammatory effects of exercise have
attracted attention over the last decade • C. Kasapiset al J. Am. Coll. Cardiol. 45 (2005)
1563-1569.
• I.J. Kullo, et al , J. Appl. Physiol. 102 (2007) 1374-
1379.
contractile dysfunction in muscles is related
to TNF-a • M.B. Reid, Am. J. Respir. Crit. Care Med. 166
(2002) 479-484.
44
SpA: Ex and IL-6
exercise induced IL-6 release from the
muscle tissue has an anti-inflammatory role
and inhibits TNF-a with a different receptor
pathway • R. Schindler et al, Blood 75 (1990) 40-47.
45

SpA: Ex and cytokines
• Muscle derived IL-6
inhibits TNF-a by
activating TNF-a
receptor pathway: IL-
6 anti-inflammatory
during exercise.
• study:
• levels IL-6 stable,
• TNF-a levels ↓ during
the follow-up
46

Physical activity (PA)
PA may be
decreased (Swinnen et al PLoS ONE 2014 9(2))
no different (Plasqui G et al (Arthritis Care Res 2012) 4(1))
In the AS subtype, participants with high disease activity reported engaging in significantly less PA than respondents with low disease activity ( Fongen Clin Rheumatol 2013 32(12)), (Brophy et al Semin
Arthritis Rheu 2013 42(6)).
PA scores related to disease activity, physical function, and quality of life;
47

Compliance with PA
recommendations to achieve health-related
benefits vary across studies from
17 % (O’Dwyer T et al Rheumatology 2014, 53(10)) to
71 % (Manning et al J Clin Rheumatol Pract Rep Rheumat Musculoskelet Dis 2012 18(8))
48

AR
49

RA:Pathways activating macrophages
• RA synovitis :
• promoting cytokine
release:
– IL-6 , TNF
– probably GM-CSF,
• central importance :
clear therapeutic
benefits achieved
upon their inhibition.
Firestein, Immunity 46, February 21, 2017 50
Point of view of the physiotherapist
Musculoskeletal Care 2016
51

PTs reported:
•Lower degree of confidence and fewer roles
in managing RA compared with OA.
•good adherence to the national guidelines
for almost all the treatment modalities listed.
•a need for education, in chronic
inflammatory arthritis care.
Musculoskeletal Care 2016
52
Cochrane Database of Systematic Reviews
2009
53
Dynamic exercise therapy
Aerobic exercise and muscle strength training on land probably improve pain and physical function slightly in the short term.
It means activities with enough intensity, duration, and frequency to improve stamina or muscle strength. Exercise can be any activity that enhances physical fitness as aerobic exercise.
moderate evidence for a positive effect on aerobic capacity
functional ability and aerobic capacity
Cochrane Database of Systematic Reviews 2009 54

Balneotherapy
Cochrane Database of Systematic Reviews 2015, Issue 4. Art. No.: CD000518
55
Effects
•Improved both pain and functional
impairments after 3 and 6 months.
•↓medication consumption.
•If patient education program delivered
during spa treatment: better in alleviating
fears and deleterious beliefs compared to
simple patient information
Forestier R. et al Joint Bone Spine 84 (2017) 9–13
56

But…
• Evidence insufficient
to show that
balneotherapy is
more effective than
no treatment, that one
type of bath is more
effective than another
or that one type of
bath is more effective
than mudpacks,
exercise or relaxation
therapy. Verhagen et al Cochrane Database of Systematic Reviews 2015,
57

AR
*benefits of exercise and physical activity
programmes regarding RA-related outcomes
is demonstrated
*enhancing the effectiveness of self-
management
-Duration at least 6 weeks;
-Explicit use of cognitive behavioural
approaches
Curr Opin Rheumatol 2011 23:259–264 58
AR and hand
• Appropriately hand
physiotherapy in
women with RA
contributed to the
improvement of its
function by:
– pain reduction,
– improved value and
quality of grip,
– increased
manipulative ability
59
Reumatologia 2016; 54, 6: 285–290

Results
• Team-rehabilitation in
a warm climate
resulted in clinically
meaningful
improvements in body
function, activities and
well-being, and
promoted physical
activity for up to one
year.
J Rehab 2016
61

Succes rehabilitation
“I need a doctor who will take care of my whole person not ‘just my painful joint’. “
Successful rehabilitation programs in rheumatic diseases require a working partnership:
the patient,
the rheumatologist, ev rehab MD
other health professionals.
Multidisciplinary care teams
Ton Nghiem,Donohue: Curr Op Rheumat, 2008, 20:218–219
62

Take home meassage
• Exercise is important:
movement more.
• Mobility stimulate
immune system: anti-
inflammatory effects,
IL 6, TNF
• No danger to move
• Supervised more
stimulating
www.mon-sport.ch
www.mein-sport.ch
63
Questions?
64
Thank you for your attention: Go on training.
65