
Gefäßheilung nach Koronarinterventionen was bringen neue ... · - Prasugrel und Ticagrelor -...
31
Gefäßheilung nach Koronarinterventionen – was bringen neue Plättchenhemmer und bioresorbierbare Stents Hans Theiss Medizinische Klinik und Poliklinik I Klinikum der Universität München
-
Upload
nguyenmien -
Category
Documents
-
view
215 -
download
0
Transcript of Gefäßheilung nach Koronarinterventionen was bringen neue ... · - Prasugrel und Ticagrelor -...

Gefäßheilung nach Koronarinterventionen – was bringen neue Plättchenhemmer und
bioresorbierbare Stents
Hans Theiss
Medizinische Klinik und Poliklinik I Klinikum der Universität München
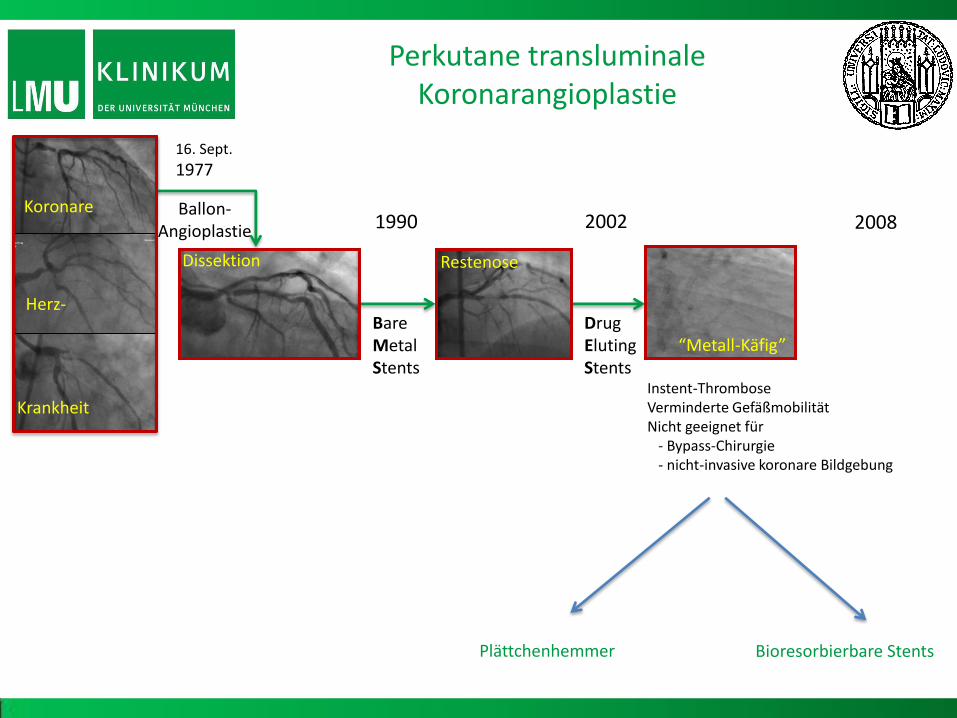
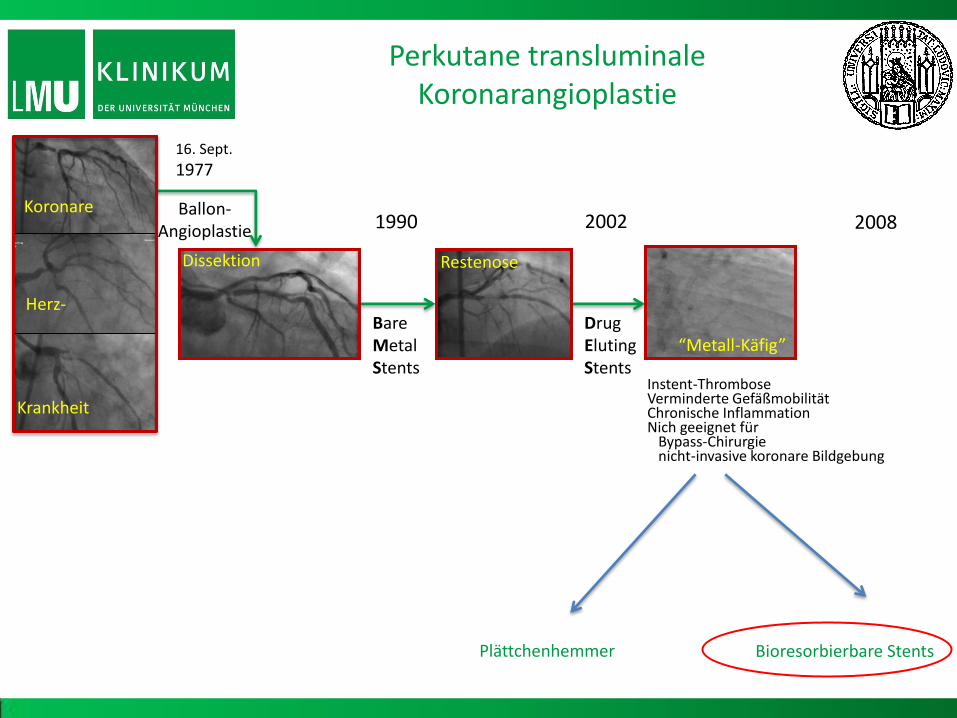
16. Sept.
1977
Ballon- Angioplastie 1990
Bare Metal Stents
2002
Drug Eluting Stents
2008
Bioresorbierbare Stents
Perkutane transluminale Koronarangioplastie
Krankheit
Koronare
Herz-
Dissektion Restenose
“Metall-Käfig”
Instent-Thrombose Verminderte Gefäßmobilität Nicht geeignet für - Bypass-Chirurgie - nicht-invasive koronare Bildgebung
Plättchenhemmer

Ndrepepa, Mehilli et al., Cardiology 2009
Mortalität beim akuten Koronarsyndrom
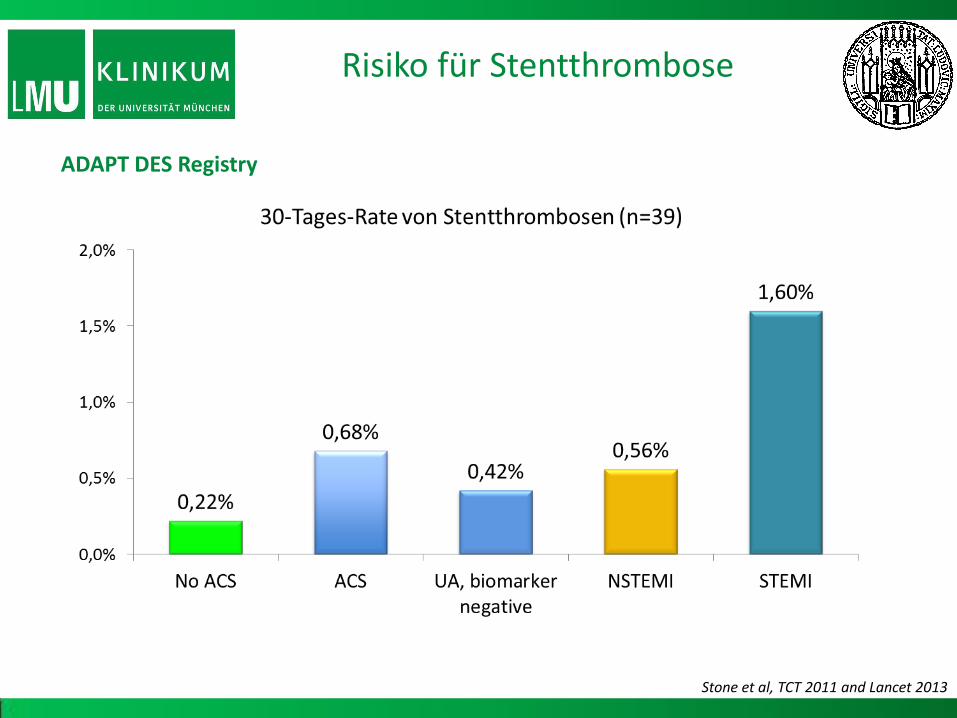
ADAPT DES Registry
Stone et al, TCT 2011 and Lancet 2013
Risiko für Stentthrombose
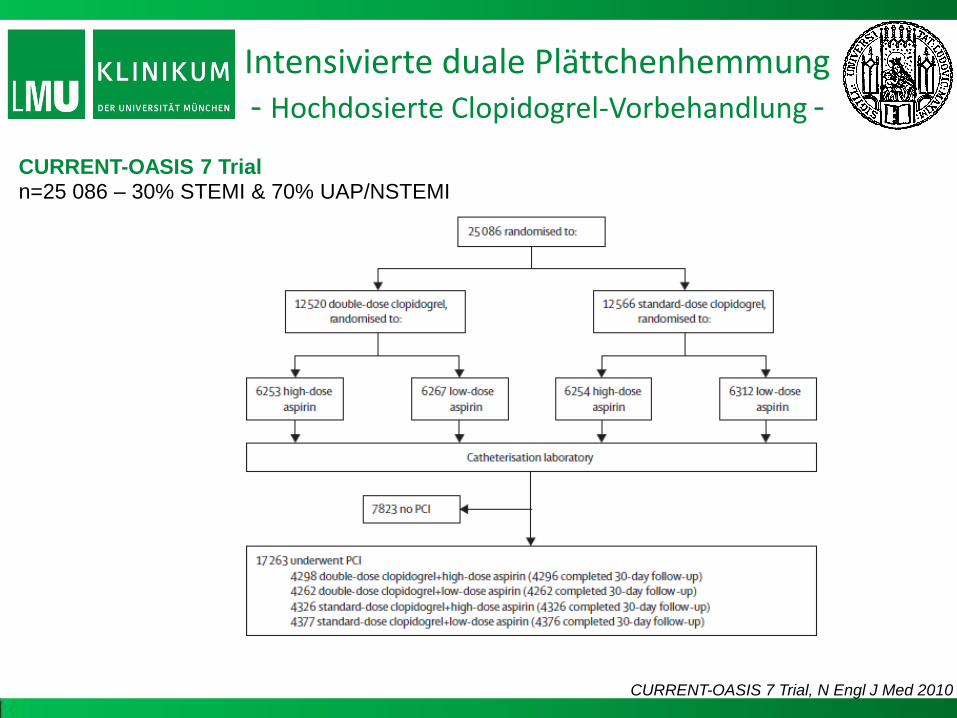
Intensivierte duale Plättchenhemmung - Hochdosierte Clopidogrel-Vorbehandlung -
CURRENT-OASIS 7 Trial, N Engl J Med 2010
CURRENT-OASIS 7 Trial n=25 086 – 30% STEMI & 70% UAP/NSTEMI

Primärer Endpunkt – Kardiovaskulärer Tod, AMI, Schlaganfall
Definitive/wahrscheinliche Stentthrombose
Mehta et al, Lancet 2010
CURRENT-OASIS 7 Trial PCI population
N=17263
Intensivierte duale Plättchenhemmung - Hochdosierte Clopidogrel-Vorbehandlung -
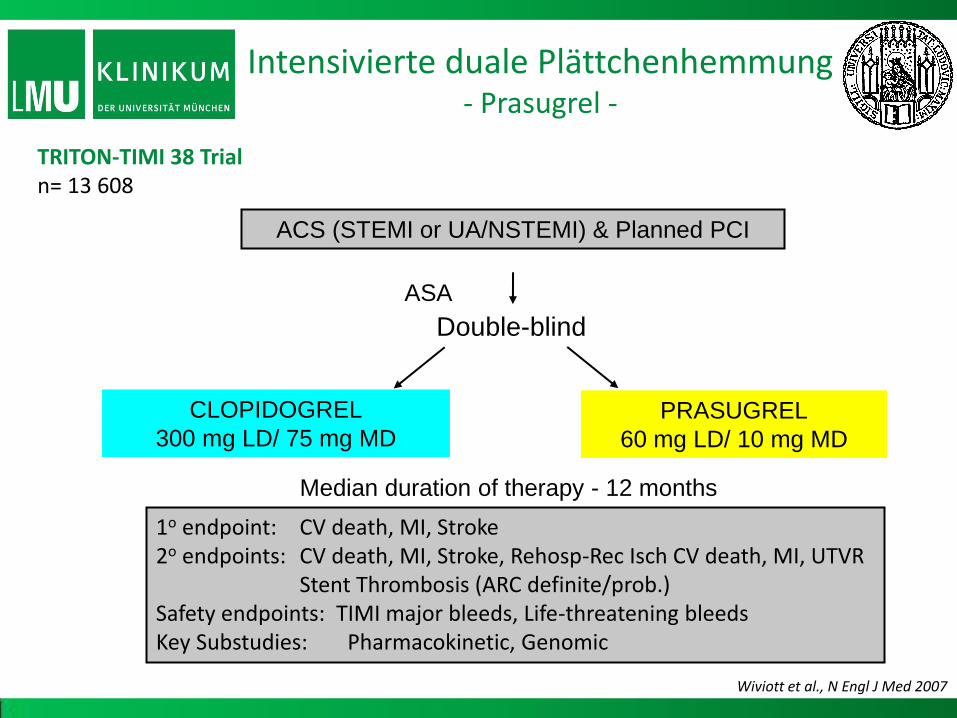
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCI
ASA
PRASUGREL
60 mg LD/ 10 mg MD
CLOPIDOGREL
300 mg LD/ 75 mg MD
1o endpoint: CV death, MI, Stroke 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic
Median duration of therapy - 12 months
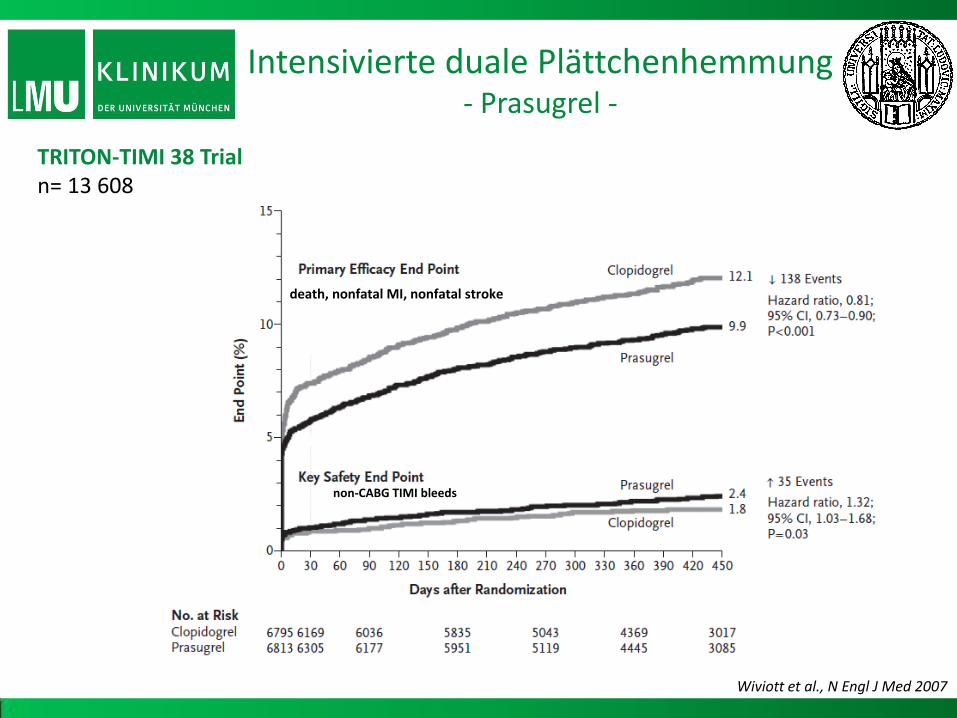
TRITON-TIMI 38 Trial n= 13 608
Wiviott et al., N Engl J Med 2007
Intensivierte duale Plättchenhemmung - Prasugrel -
Wiviott et al., N Engl J Med 2007
TRITON-TIMI 38 Trial n= 13 608
death, nonfatal MI, nonfatal stroke
non-CABG TIMI bleeds
Intensivierte duale Plättchenhemmung - Prasugrel -

+ 10
- 15
- 10
- 5
+ 5
0
- 20
- 25
Nu
mb
er
of
even
ts p
er
10
0 p
atie
nts
myocardial infarction
Non-CABG TIMI major bleeds
- 23
+ 6
TRITON-TIMI 38 Trial n= 13 608
Net clinical benefit Prasugrel vs. Clopidogrel
F.-J. Neumann, Eur Heart J Suppl 2009
Intensivierte duale Plättchenhemmung - Prasugrel -
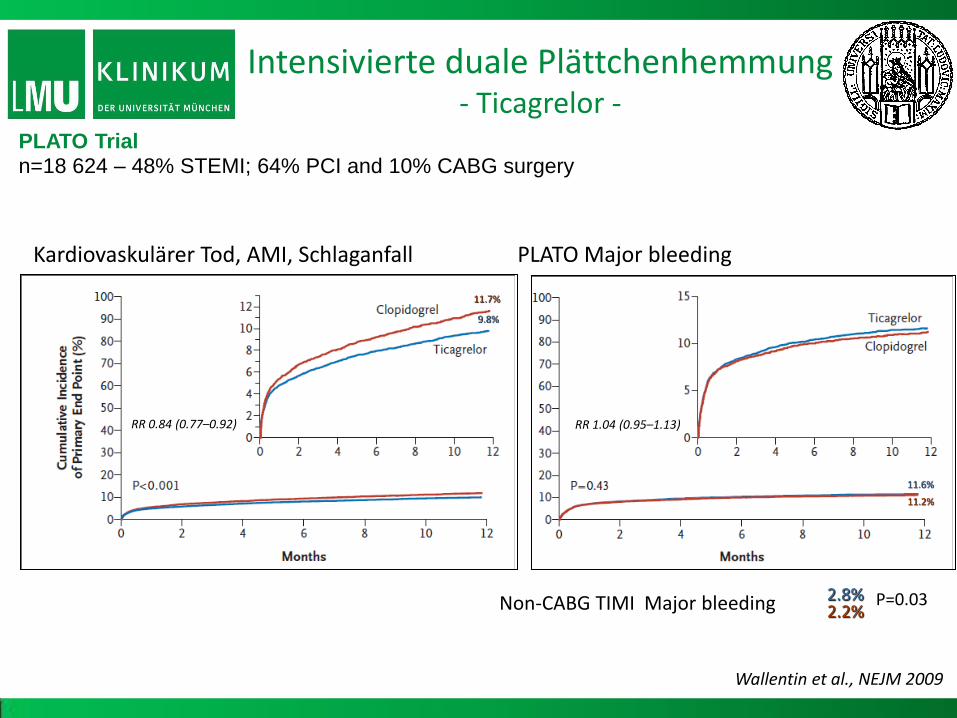
Kardiovaskulärer Tod, AMI, Schlaganfall PLATO Major bleeding
Wallentin et al., NEJM 2009
RR 0.84 (0.77–0.92)
9.8%
11.7%
11.6%
11.2%
RR 1.04 (0.95–1.13)
PLATO Trial n=18 624 – 48% STEMI; 64% PCI and 10% CABG surgery
2.8% 2.2% Non-CABG TIMI Major bleeding P=0.03
Intensivierte duale Plättchenhemmung - Ticagrelor -
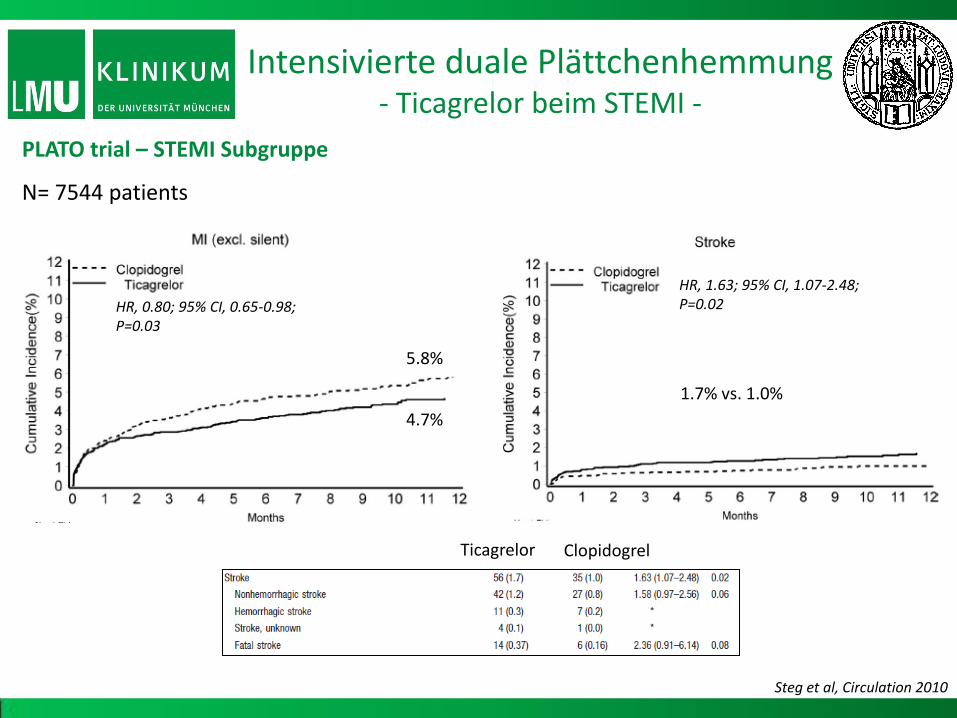
HR, 0.80; 95% CI, 0.65-0.98; P=0.03
Steg et al, Circulation 2010
5.8%
4.7%
HR, 1.63; 95% CI, 1.07-2.48; P=0.02
1.7% vs. 1.0%
PLATO trial – STEMI Subgruppe
N= 7544 patients
Ticagrelor Clopidogrel
Intensivierte duale Plättchenhemmung - Ticagrelor beim STEMI -
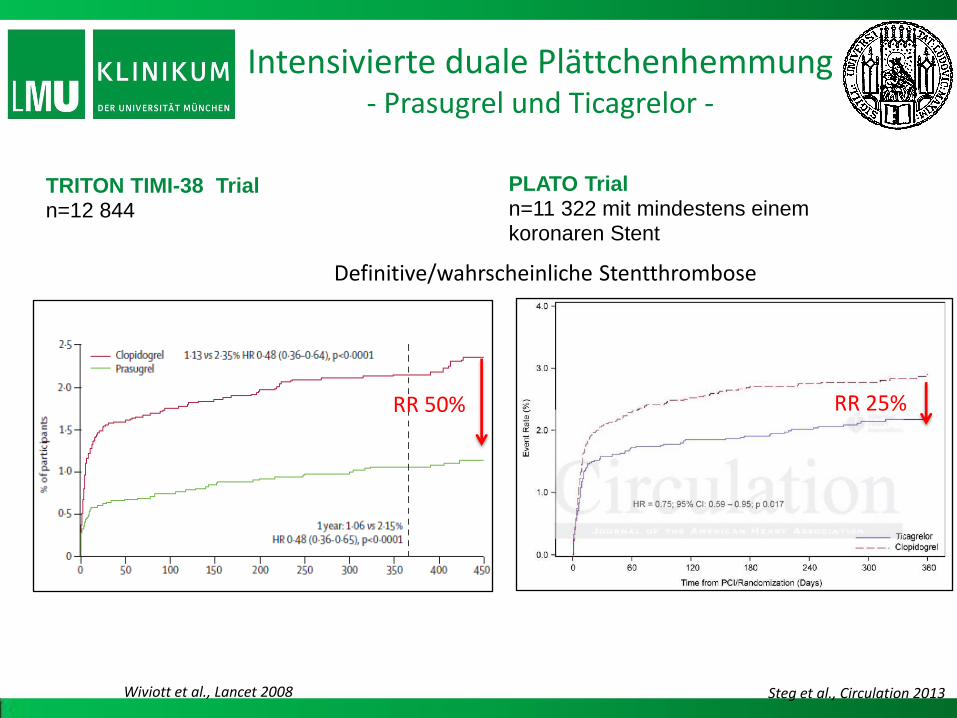
Definitive/wahrscheinliche Stentthrombose
Wiviott et al., Lancet 2008
RR 50%
PLATO Trial n=11 322 mit mindestens einem koronaren Stent
Steg et al., Circulation 2013
TRITON TIMI-38 Trial n=12 844
RR 25%
Intensivierte duale Plättchenhemmung - Prasugrel und Ticagrelor -
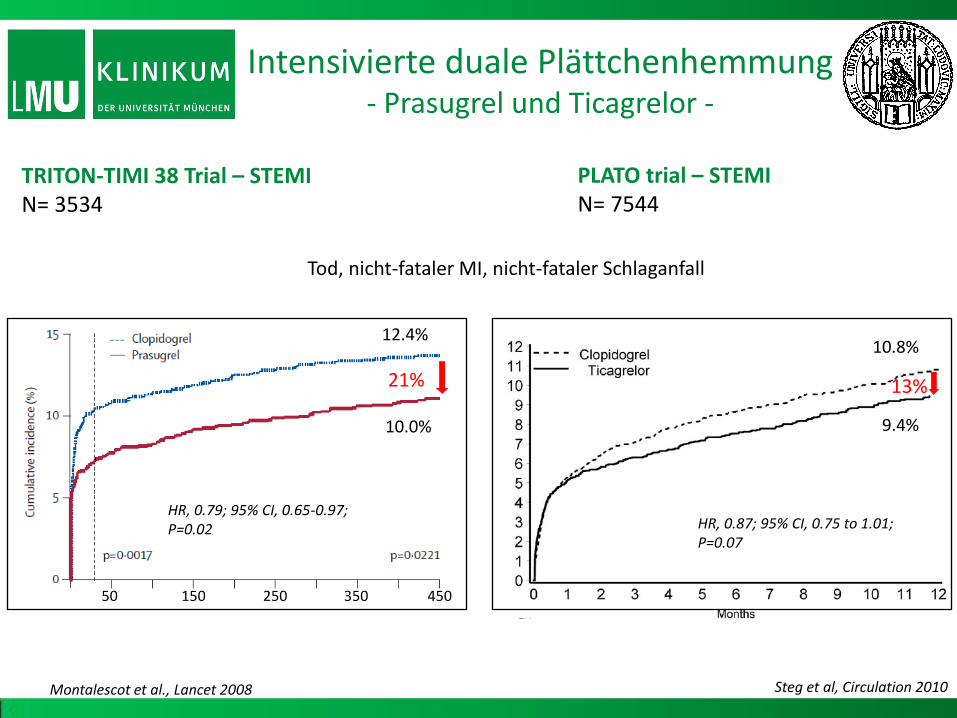
Steg et al, Circulation 2010
PLATO trial – STEMI N= 7544
HR, 0.87; 95% CI, 0.75 to 1.01; P=0.07
10.8%
9.4%
13%
Tod, nicht-fataler MI, nicht-fataler Schlaganfall
21%
HR, 0.79; 95% CI, 0.65-0.97; P=0.02
12.4%
10.0%
50 350 150 250 450
Montalescot et al., Lancet 2008
TRITON-TIMI 38 Trial – STEMI N= 3534
Intensivierte duale Plättchenhemmung - Prasugrel und Ticagrelor -
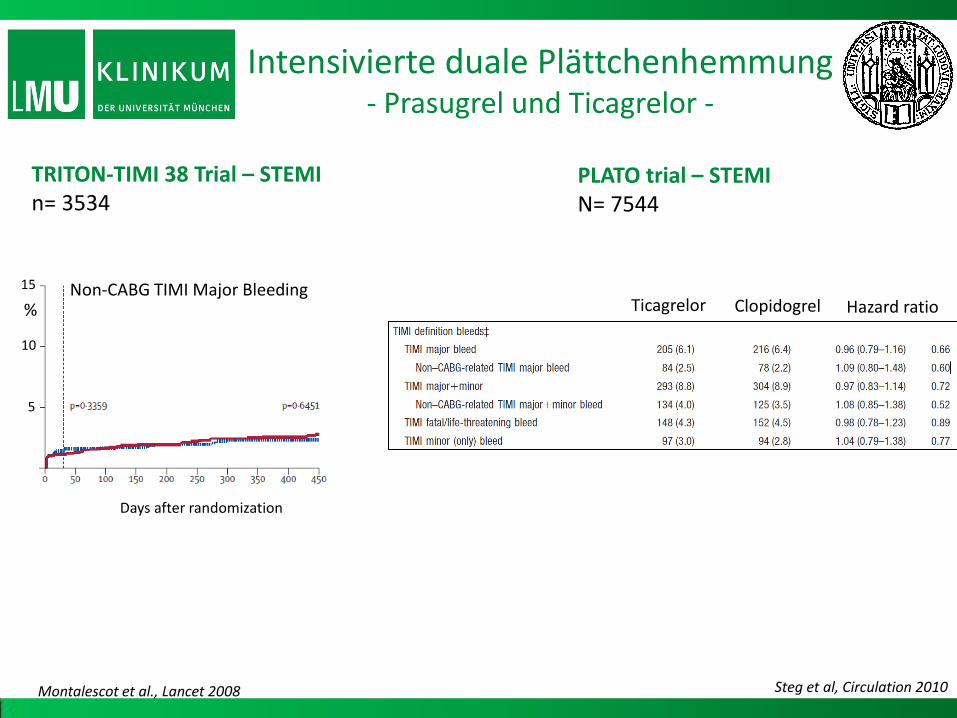
Days after randomization
Non-CABG TIMI Major Bleeding
Montalescot et al., Lancet 2008
TRITON-TIMI 38 Trial – STEMI n= 3534
Ticagrelor Clopidogrel Hazard ratio
Steg et al, Circulation 2010
PLATO trial – STEMI N= 7544
5
10
15
%
Intensivierte duale Plättchenhemmung - Prasugrel und Ticagrelor -

Wiviott et al., N Engl J Med 2007 F.-J. Neumann, Eur Heart J Suppl 2009
80%
16%
4%
Patienten ≥ 75 Jahre oder Gewicht < 60 kg
Patienten < 75 Jahre oder Gewicht > 60 kg ohne Schlaganfall/TIA in der Vorgeschichte
Früherer Schlaganfall/TIA
Intensivierte duale Plättchenhemmung - Prasugrel Net Clinical Benefit -

14%
10%
RR 0.72 (0.58–0.89)
James et al, Circulation 2010
PLATO Trial Reduziert die Mortalität bei Patienten mit eingeschränkter renaler Funktion
Kreatinin-Clearance <60 mL/min N =3237 Kreatinin-clearance ≥60mL/min N= 11 965
RR 0.77 (0.65–0.90)
RR 0.90 (0.79–1.02)
Intensivierte duale Plättchenhemmung - Ticagrelor bei chronischer Niereninsuffizienz-
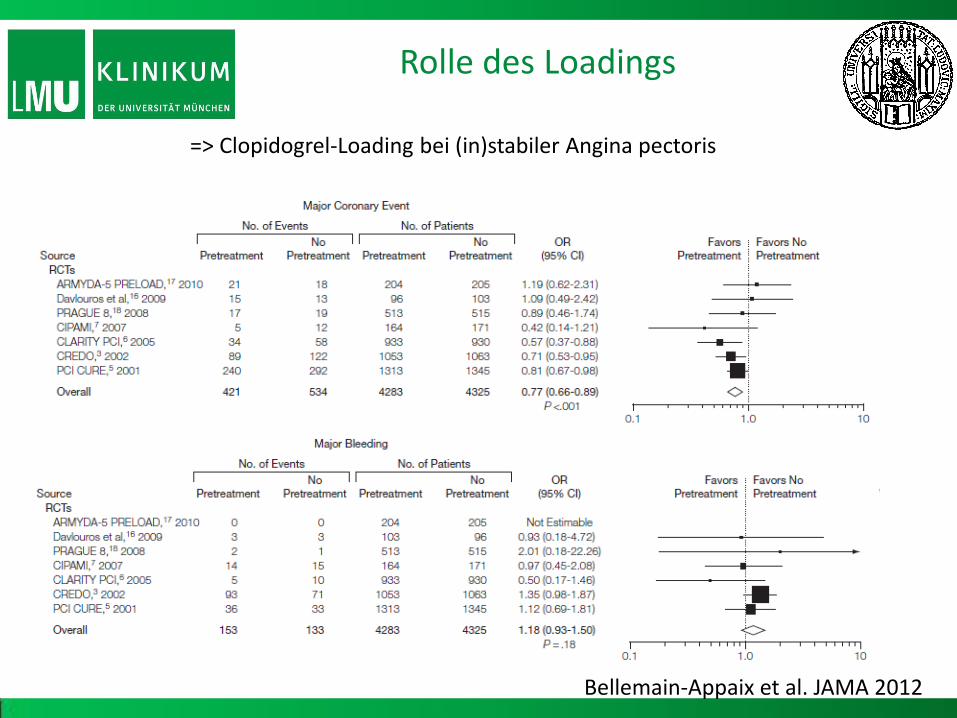
=> Clopidogrel-Loading bei (in)stabiler Angina pectoris
Bellemain-Appaix et al. JAMA 2012
Rolle des Loadings
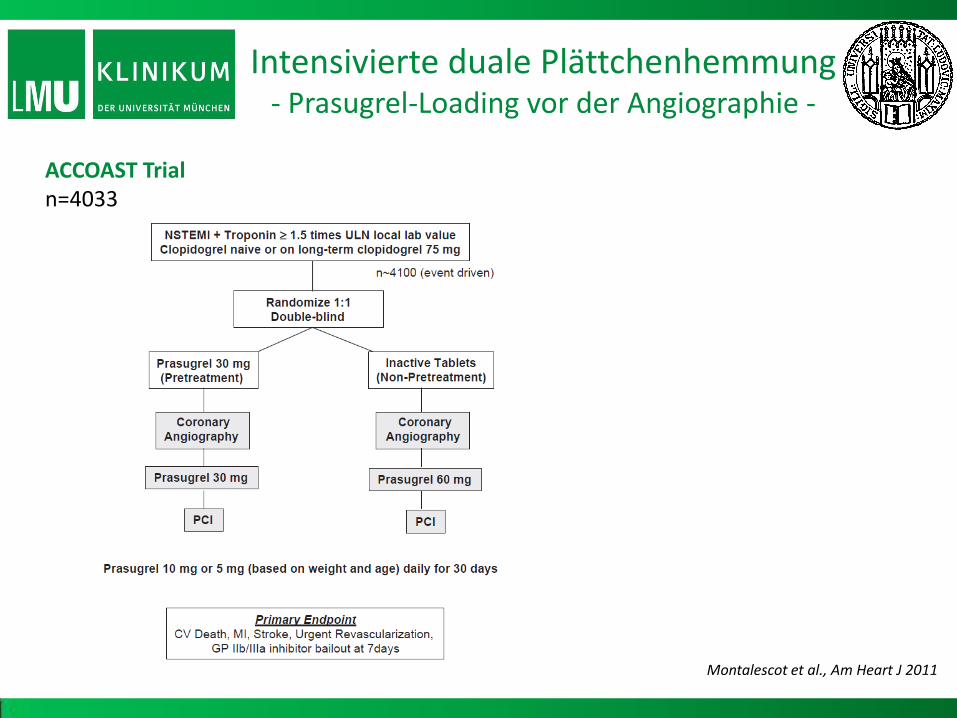
Intensivierte duale Plättchenhemmung - Prasugrel-Loading vor der Angiographie -
ACCOAST Trial n=4033
Montalescot et al., Am Heart J 2011
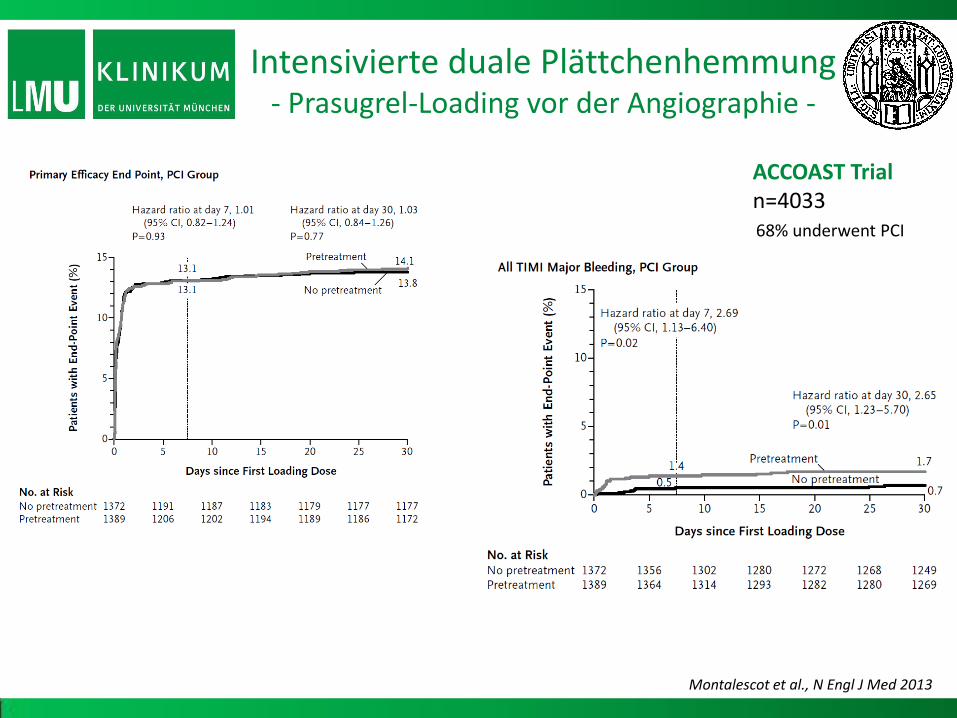
Montalescot et al., N Engl J Med 2013
68% underwent PCI
ACCOAST Trial n=4033
Intensivierte duale Plättchenhemmung - Prasugrel-Loading vor der Angiographie -

68% underwent PCI
ACCOAST Trial n=4033
Blutungsereignisse
Montalescot et al., N Engl J Med 2013
Intensivierte duale Plättchenhemmung - Prasugrel-Loading vor der Angiographie -

1. Stabile Angina pectoris 2. Stattgehabter
Schlaganfall/TIA 3. TAVI/ MitraClip 4. LAA/PFO Verschluss 5. STEMI + NSTEMI-ACS mit Kontraindikationen für Prasugrel/Ticagrelor
Clopidogrel 75mg/d
Prasugrel 10 mg/d (5 mg bei Gewicht < 60 kg
oder Alter > 75 a)
1. STEMI 2. NSTEMI (positive
Biomarker positiv und GFR> 60ml/min) 1. Clopidogrel Resistenz
Ticagrelor 2x90mg/d
1. STEMI + KI für Prasugrel (Allergie)
2. NSTEMI-ACS und GFR< 60 ml/min
Zusammenfassung duale Plättchenhemmung
16. Sept.
1977
Ballon- Angioplastie 1990
Bare Metal Stents
2002
Drug Eluting Stents
2008
Bioresorbierbare Stents
Perkutane transluminale Koronarangioplastie
Krankheit
Koronare
Herz-
Dissektion Restenose
“Metall-Käfig”
Instent-Thrombose Verminderte Gefäßmobilität Chronische Inflammation Nich geeignet für Bypass-Chirurgie nicht-invasive koronare Bildgebung
Plättchenhemmer
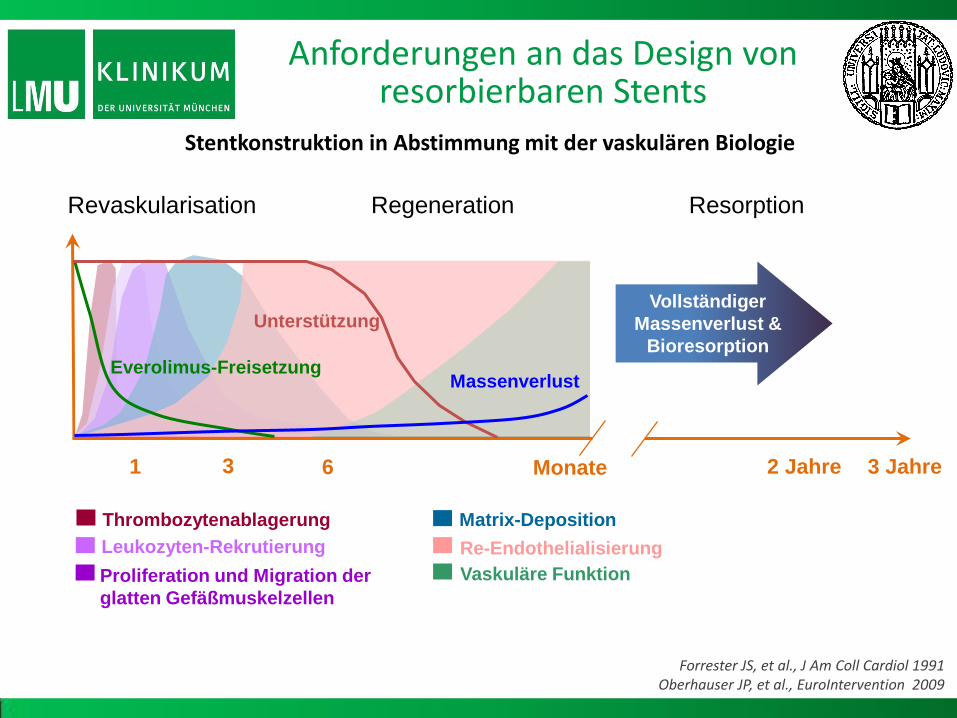
1 3 6 2 Jahre
Vollständiger
Massenverlust &
Bioresorption
Monate
Thrombozytenablagerung
Leukozyten-Rekrutierung
Proliferation und Migration der
glatten Gefäßmuskelzellen
Matrix-Deposition
Re-Endothelialisierung
Vaskuläre Funktion
Everolimus-Freisetzung
Unterstützung
Massenverlust
Revaskularisation Regeneration Resorption
Forrester JS, et al., J Am Coll Cardiol 1991 Oberhauser JP, et al., EuroIntervention 2009
3 Jahre
Anforderungen an das Design von resorbierbaren Stents
Stentkonstruktion in Abstimmung mit der vaskulären Biologie
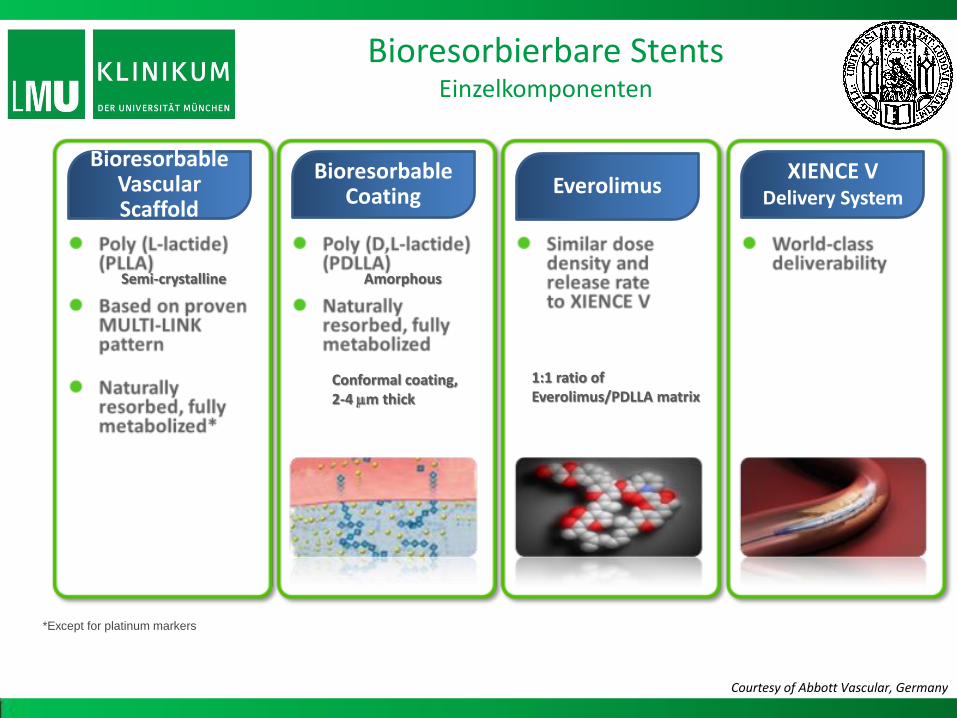
Bioresorbable Vascular Scaffold
Bioresorbable Coating Everolimus
XIENCE V Delivery System
*Except for platinum markers
Bioresorbierbare Stents Einzelkomponenten
Courtesy of Abbott Vascular, Germany
Semi-crystalline
1:1 ratio of Everolimus/PDLLA matrix
Amorphous
Conformal coating, 2-4 m thick

Cohort A
Cohort B
Uniforme Strutverteilung
Stärkere Stützung der Arterienwand
Geringerer “late scaffold area loss”
- Hält die Radialkraft für mind. 3 Monate aufrecht
Aufbewahrung bei Raumtemperatur
Verbesserte Device-Retention
Unverändert:
- Material, Beschichtung und Rückgrat
- Strutdicke
- Drug release-Profil
Optimierung der bioresorbier-baren Stents BVS 1.0 vs. BVS 1.1 -
Bioresorbierbare Stents Fallbeispiel

Serruys PW, ABSORB Cohort B 3Year Data, Rotterdam EuroPCR Focus on BVS 2013
ABSORB Cohort B vs. Xience - Historische Kontrolle -
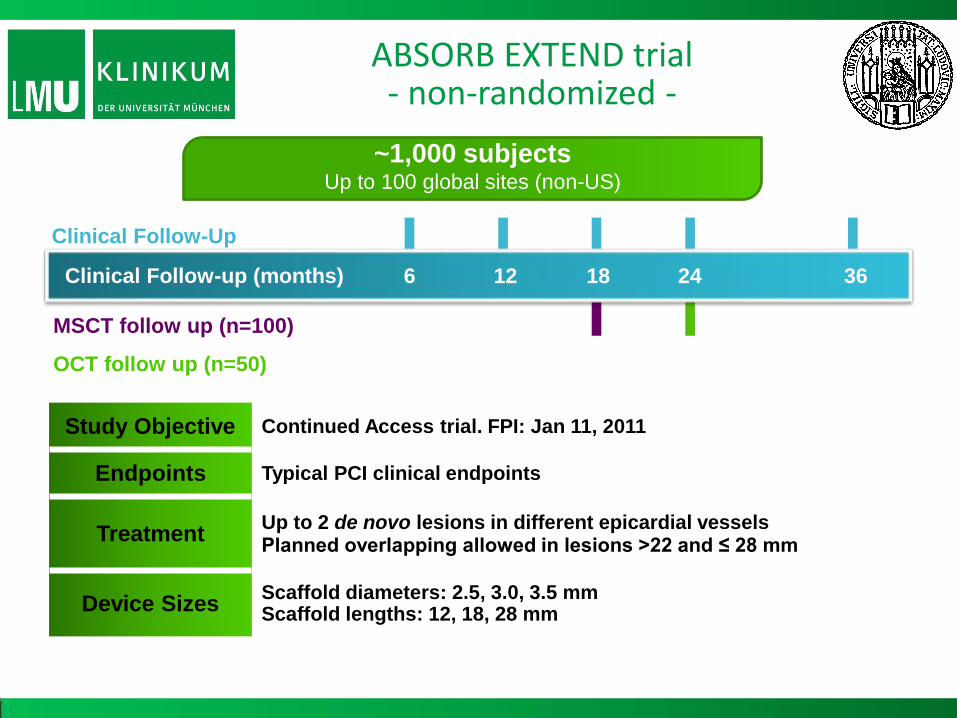
Study Objective Continued Access trial. FPI: Jan 11, 2011
Endpoints Typical PCI clinical endpoints
Treatment Up to 2 de novo lesions in different epicardial vessels Planned overlapping allowed in lesions >22 and ≤ 28 mm
Device Sizes Scaffold diameters: 2.5, 3.0, 3.5 mm Scaffold lengths: 12, 18, 28 mm
Clinical Follow-up (months)
~1,000 subjects Up to 100 global sites (non-US)
Clinical Follow-Up
MSCT follow up (n=100)
OCT follow up (n=50)
24 12 6 18 36
ABSORB EXTEND trial - non-randomized -

MACE: cardiac death, MI, ischemia-driven TLR *Reflects an interim snapshot with only cleaned data as of the cut-off date of 03 December 2012.
**No Absorb BVS was implanted in the target lesion
Non-Hierarchical
Cardiac Death % (n)
Myocardial Infarction % (n)
Q-wave MI
Non Q-wave MI
Ischemia Driven TLR % (n)
PCI
CABG
Hierarchical MACE % (n)
6 Months*
n = 450
0.2 (1)**
0.7 (3)
2.0 (9)
2.7 (12)
0.4 (2)
0.4 (2)
0.0 (0)
2.9 (13)
12 Months*
n = 450
0.2 (1)**
0.9 (4)
2.0 (9)
2.9 (13)
1.8 (8)
1.6 (7)
0.2 (1)
4.2 (19)
Scaffold Thrombosis
(ARC Def/Prob) % (n) 0.7 (3) 0.9 (4)
Chevalier, ABSORB EXTEND 12-month outcomes in the first 450 patient enrolled, Rotterdam EuroPCR Focus on BVS 2013
ABSORB EXTEND trial Intent to Treat; Interim Snapshot
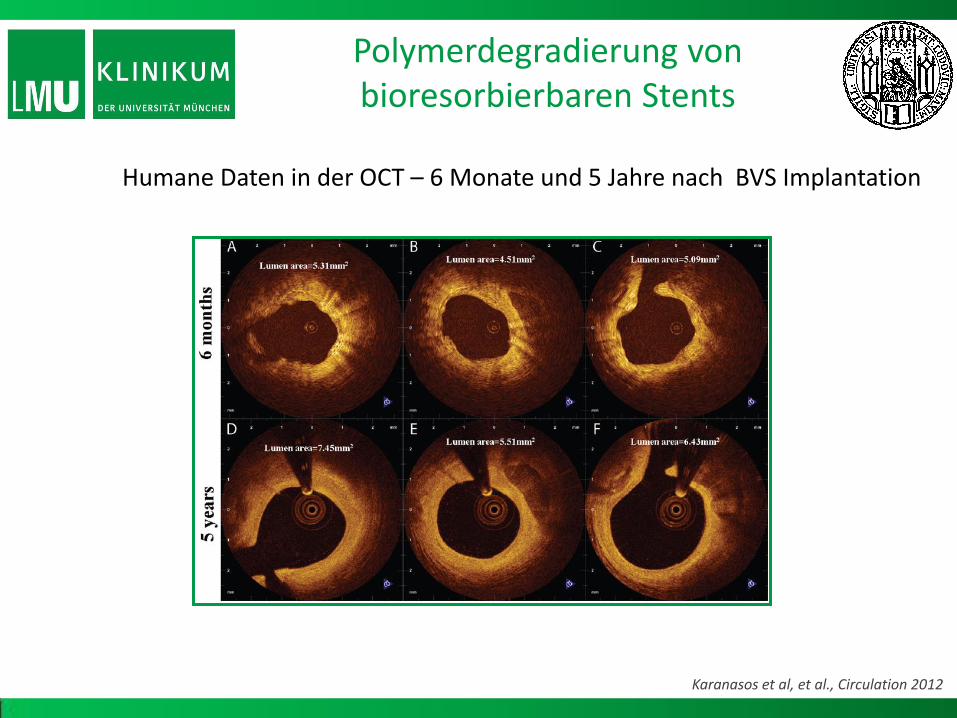
Polymerdegradierung von bioresorbierbaren Stents
Humane Daten in der OCT – 6 Monate und 5 Jahre nach BVS Implantation
Karanasos et al, et al., Circulation 2012

Vielen Dank!








![Technische Analyse - Münchner Verlagsgruppe · xà ÆÏÏÃj aÆÆÏj j =ØxC j Ï Ã? j ¦ ç ?ÃÏx à ?Ï j ]8 W j Ø a ?ÏÆØ j ... j8 W j -j j ÖÖç](https://static.fdokument.com/doc/165x107/5bee32b909d3f2f51e8c9993/technische-analyse-muenchner-verlagsgruppe-xa-aiiaj-aaaij-j-oxc.jpg)









