La performance du système de santé Belge. Rapport 2012 · 1. Donner une vue d’ensemble de la...
180
2013 www.kce.fgov.be KCE REPORT 196 B LA PERFORMANCE DU SYSTÈME DE SANTÉ BELGE RAPPORT 2012
Transcript of La performance du système de santé Belge. Rapport 2012 · 1. Donner une vue d’ensemble de la...

2013 www.kce.fgov.be
KCE REPORT 196 B
LA PERFORMANCE DU SYSTÈME DE SANTÉ BELGE RAPPORT 2012

Le Centre Fédéral d’Expertise des Soins de Santé Le Centre Fédéral d’Expertise des Soins de Santé est un parastatal, créé par la loi-programme (1) du
24 décembre 2002 (articles 259 à 281), sous tutelle du Ministre de la Santé publique et des Affaires sociales. Il est chargé de réaliser des études éclairant la décision politique dans le domaine des soins de santé et de l’assurance maladie.
Conseil d’Administration Membres effectifs Membres suppléants
Président Pierre Gillet Fonctionnaire dirigeant de l'INAMI (vice président) Jo De Cock Benoît Collin Président du SPF Santé publique (vice président) Dirk Cuypers Chris Decoster Président du SPF Sécurité sociale (vice président) Frank Van Massenhove Jan Bertels Administrateur général de l'AFMPS Xavier De Cuyper Greet Musch Représentants du ministre de la Santé publique Bernard Lange François Perl Marco Schetgen Annick Poncé Représentants du ministre des Affaires sociales Olivier de Stexhe Karel Vermeyen Ri De Ridder Lambert Stamatakis Représentants du Conseil des ministres Jean-Noël Godin Frédéric Lernoux Daniel Devos Bart Ooghe Agence intermutualiste Michiel Callens Frank De Smet Patrick Verertbruggen Yolande Husden Xavier Brenez Geert Messiaen
Organisations professionnelles représentatives des médecins
Marc Moens Jean-Pierre Baeyens
Roland Lemye Rita Cuypers
Organisations professionnelles représentatives des infirmiers
Michel Foulon Myriam Hubinon
Ludo Meyers Olivier Thonon
Fédérations hospitalières Johan Pauwels Katrien Kesteloot Jean-Claude Praet Pierre Smiets Partenaires sociaux Rita Thys Leo Neels Paul Palsterman Celien Van Moerkerke Chambre des Représentants Lieve Wierinck

Contrôle Commissaire du Gouvernement Yves Roger Direction Directeur Général
Raf Mertens
Directeurs du programme d'études Christian Léonard Kristel De Gauquier
Contact Centre Fédéral d’Expertise des Soins de Santé (KCE) Doorbuilding (10e étage) Boulevard du Jardin Botanique, 55 B-1000 Bruxelles Belgique T +32 [0]2 287 33 88 F +32 [0]2 287 33 85 [email protected] http://www.kce.fgov.be


2013 www.kce.fgov.be
KCE REPORT 196B HEALTH SERVICES RESEARCH
LA PERFORMANCE DU SYSTÈME DE SANTÉ BELGE RAPPORT 2012 FRANCE VRIJENS, FRANÇOISE RENARD, PASCALE JONCKHEER, KOEN VAN DEN HEEDE, ANJA DESOMER, CARINE VAN DE VOORDE, DENISE WALCKIERS, CÉCILE DUBOIS, CÉCILE CAMBERLIN, JOAN VLAYEN, HERMAN VAN OYEN, CHRISTIAN LÉONARD, PASCAL MEEUS

COLOPHON Titre : La performance du système de santé Belge. Rapport 2012
Auteurs : France Vrijens (KCE), Françoise Renard (ISP – WIV), Pascale Jonckheer (KCE), Koen Van den Heede (KCE), Anja Desomer (KCE), Carine Van de Voorde (KCE), Denise Walckiers (ISP – WIV), Cécile Dubois (KCE), Cécile Camberlin (KCE), Joan Vlayen (KCE), Herman Van Oyen (WIV - ISP), Christian Léonard (KCE), Pascal Meeus (INAMI – RIZIV)
Experts externes : Health Promotion Group : Luc Berghmans (Observatoire de la santé du Hainaut), Lien Braeckevelt (WVG Vlaanderen), Christian De Bock (CM), Léa Maes (UGent), Myriam De Spiegelaere (ULB – Observatoire de la santé Bruxelles), Stephan Van Den Broucke (UCL), Chantal Vandoorne (ULg), Alexander Witpas (WVG Vlaanderen) Mental Healthcare Group: Joël Boydens (CM), Robert Cools (CGG - De Pont), Raf De Rycke (Broeders van Liefde), Pol Gerits (FOD Volksgezondheid – SPF Santé Publique), Jean-Pierre Gorissen (FOD Volksgezondheid – SPF Santé Publique), Bernard Jacob (SPF Santé publique – FOD Volksgezondheid), Gert Peeters (UZ Leuven), Jean-Paul Roussaux (Cliniques Universitaires St-Luc) Continuity of Care and Patient Centeredness Group: Corinne Boüüaert (Maison Médicale Bautista Van Schowen), Xavier de Béthune (CM), Veerle Foulon (KU Leuven), Mirco Petrovic (UZ Gent), Luc Seuntjens (het Artsenhuis), Anne Spinewine (UCL de Mont-Godinne), Johan Van der Heyden (WIV - ISP), Annelies Van Linden (Domus Medica), Johan Wens (UA) Long term care Group: Daniel Crabbe (RIZIV – INAMI), Jan Delepeleire (KU Leuven), Johan Flaming (UZ Leuven), Margareta Lambert (UZ Brussel), Jean Macq (UCL), Alex Peltier (MC), Luc Van Gorp (Katholieke Hogeschool Limburg), Isabelle Vanderbrempt (SPF Santé publique – FOD Volksgezondheid ) End of Life Group: Joachim Cohen (VUB), Marianne Desmedt (UCL), Rita Goetschalckx (RIZIV – INAMI), Johan Menten (UZ Leuven), Kathleen Kleemans (VUB), Birgit Gielen (CM)
Remerciements : Greet Haelterman (FOD Volksgezondheid - SPF Santé publique), Willem Alvoet (FOD Volksgezondheid - SPF Santé publique), Marie-Noëlle Verhaegen (FOD Volksgezondheid - SPF Santé publique ), Hans Verrept (FOD Volksgezondheid - SPF Santé publique ), Isabelle Coune (SPF Santé publique - FOD Volksgezondheid), Luc Nicolas (SPF Santé publique – FOD Volksgezondheid), Dirk Moens (FOD Sociale Zekerheid – SPF Sécurité Sociale), Elke Van Hoof (Kankercentrum – Centre Cancer), Elisabeth Van Eycken (Stichting Kankerregister – Fondation Registre du Cancer), Xavier Ledent (INAMI – RIZIV), Pierre Bonte (INAMI – RIZIV), Olaf Moens (VIGeZ), Sadja Steenhuizen (VIGeZ), Stefaan Demarest (WIV – ISP), Béatrice Jans (ISP – WIV), Natacha Viseur (ISP – WIV), Viviane Van Casteren (WIV – ISP), Nathalie Bossuyt (WIV – ISP), Xavier de Béthune (MC), Johan Hellings (ICURO)
Validateurs externes : Ann-Lise Guisset (WHO), Irene Papanicolas (London School of Economics and Political Science), Niek Klazinga (Academisch Medisch Centrum – Universiteit van Amsterdam)

Stakeholders: Les administrations et organismes suivants ont été consultés tout au long du projet lors de réunions inter-administrations : au niveau fédéral (SPF Santé Publique, SPF Affaires Sociales, INAMI, ISP), et au niveau des entitées fédérées: Communauté et Région Flamande (Vlaams Agentschap Zorg en Gezondheid), Fédération Wallonie-Bruxelles (Direction générale de la Santé), Communauté Germanophone (DGOV Ministerium der Deutschsprachigen Gemeinschaft), Région Wallonne (Direction générale opérationnelle des Pouvoirs locaux, de l'Action sociale et de la Santé et observatoire wallon de la santé), Région Bruxelloise (Observatoire de la Santé)
Conflits d’intérêt : Toute relation directe ou indirecte avec un producteur, un distributeur ou une institution de soins qui pourrait entrainer un conflit d’intérêt : Gert Peeters (UZ Leuven – UPC) (Administratief manager van het UPC – UZ Leuven), Joël Boydens (MC ; Groep Emmaüs vzw – lid bestuurscomité)
Layout : Ine Verhulst, Sophie Vaes
Disclaimer : • Les experts externes ont été consultés sur une version (préliminaire) du rapport scientifique. Leurs remarques ont été discutées au cours des réunions. Ils ne sont pas co-auteurs du rapport scientifique et n’étaient pas nécessairement d’accord avec son contenu.
• Une version (finale) a ensuite été soumise aux validateurs. La validation du rapport résulte d’un consensus ou d’un vote majoritaire entre les validateurs. Les validateurs ne sont pas co-auteurs du rapport scientifique et ils n’étaient pas nécessairement tous les trois d’accord avec son contenu.
• Finalement, ce rapport a été approuvé à l'unanimité par le Conseil d’administration. • Le KCE reste seul responsable des erreurs ou omissions qui pourraient subsister de même que des
recommandations faites aux autorités publiques. Date de publication : 25 janvier 2013 Domaine : Health Services Research (HSR) MeSH : Delivery of Health Care, Health Promotion; Health Services Accessibility, Quality of Health Care, Efficiency,
Organizational, Healthcare Disparities, Social Justice; Benchmarking, Belgium Classification NLM : W84 Langue : français, anglais Format : Adobe® PDF™ (A4) Dépôt légal : D/2012/10.273/111 Copyright : Les rapports KCE sont publiés sous Licence Creative Commons « by/nc/nd »
http://kce.fgov.be/fr/content/a-propos-du-copyright-des-rapports-kce

Comment citer ce rapport ? Vrijens F, Renard F, Jonckheer P, Van den Heede K, Desomer A, Van de Voorde C, Walckiers D, Dubois C, Camberlin C, Vlayen J, Van Oyen H, Léonard C, Meeus P. La performance du système de santé Belge Rapport 2012. Health Services Research (HSR). Bruxelles: Centre Fédéral d’Expertise des Soins de Santé (KCE). 2012. KCE Report 196B. D/2012/10.273/111.
Ce document est disponible en téléchargement sur le site Web du Centre Fédéral d’Expertise des Soins de Santé.

KCE Report 196B Performance du système de santé i
PRÉFACE
Notre époque est souvent associée de manière péjorative au culte de la performance, toutefois, dans le domaine de la santé et des soins de santé, la recherche de la performance revêt un caractère quasiment indiscutable et même rassurant. Qui pourrait en effet se plaindre d’un système de soins de qualité, efficace, efficient, accessible et équitable ? Que pourrait-on reprocher à un système de promotion de la santé qui réduirait efficacement les inégalités de santé et permettrait aussi que ce niveau de santé s’améliore constamment ?
Le présent rapport vous propose une photographie de cette performance au travers de 74 indicateurs établis de manière rigoureuse par les chercheurs du KCE, de l’Institut Scientifique de Santé Publique et de l’INAMI. Leur travail a été facilité et enrichi par l’implication de dizaines d’experts du monde académique et de la société civile. Les membres de l’administration et du monde politique ont suivi activement toutes les étapes de l’élaboration de ce rapport. Nous remercions vivement chacune et chacun pour cette participation qui renforce la crédibilité du résultat et va en améliorer l’appropriation par toutes les parties concernées.
Nous vous laissons découvrir le détail des points forts de notre système, tels que l’état de santé perçu par nos concitoyens ou la couverture vaccinale des enfants, qui sont autant de raisons d’être satisfaits d’efforts qui ne peuvent toutefois être relâchés. Il faut aussi être conscient que des domaines tels que le dépistage insuffisant de certains cancers ou le report de soins pour raisons financières exigent une attention soutenue et accrue. Il nous faudra également veiller aux multiples manifestations des inégalités entre catégories socioéconomiques ou régionales.
Toutefois, malgré tout le soin et la rigueur dont chaque indicateur a fait l’objet, ce rapport doit être interprété avec une certaine prudence. En effet, les dernières données disponibles remontent parfois à quelques années, notamment celles fournies par les enquêtes. Il faut également tenir compte du temps nécessaire pour que les effets d’interventions de santé publique se traduisent dans les chiffres. En effet, l’administration et le monde politique ont pris des mesures susceptibles d’améliorer la situation dans les domaines de l’offre médicale, de l’adéquation des soins ou de l’équité. Il faudra donc remettre régulièrement l’ouvrage sur le métier afin d’évaluer si le rythme auquel nous progressons sur le chemin de la performance est suffisant. Très probablement, de nouvelles données devront être enregistrées, certains indicateurs devront être modifiés ou remplacés. En matière de santé et de soins de santé, comme dans d’autres domaines de l’activité humaine, il existe très peu d’acquis, l’efficience et l’équité seront toujours en devenir.
Raf MERTENS Directeur Général

ii Performance du système de santé KCE Report 196B
RÉSUMÉ INTRODUCTION L’évaluation de la performance du système de santé (Health System Performance Assessment - HSPA) est un processus qui permet d’offrir un bilan global, une évaluation holistique du système de santé. En se basant sur des indicateurs mesurables, cet outil établit un lien entre les résultats relatifs à la santé et les stratégies et fonctions du système de santé. L’HSPA est explicitement mentionnée dans la Charte de Tallinn, signée par tous les pays européens de l’Organisation Mondiale de la Santé (OMS) mais chaque HSPA est développée selon un cadre stratégique spécifique au pays. Une première évaluation de la performance du système belge de la santé a été publiée en juin 2010. Deux ans plus tard, le rapport HSPA 2012 vise à examiner l’accessibilité, la qualité, l’efficience, la durabilité et l’équité du système de santé belge. Il a également pour objectif d’être une source d’informations pour les décideurs compétents en matière de santé en Belgique.

KCE Report 196B Performance du système de santé iii
OBJECTIFS Objectifs stratégiques du processus d'évaluation de la performance 1. Donner une vue d’ensemble de la performance du système de santé
afin de faciliter la planification des politiques de santé ; 2. Rendre compte de la performance du système du système de santé
belge, conformément à l’engagement de transparence pris dans la Charte de Tallinn ;
3. À long terme, suivre les progrès de la performance du système de santé au fil du temps.
Objectif général du rapport 2012 Proposer et mesurer un ensemble d’indicateurs couvrant tous les domaines et certaines dimensions choisies du système de santé belge, tout en conservant un nombre d’indicateurs qui soit gérable (74 dans ce rapport).
Objectifs opérationnels du rapport 2012 1. Revoir et éventuellement adapter les 55 indicateurs du rapport
précédent, en se focalisant sur les 11 indicateurs qui n’avaient pas pu être mesurés en 2010 ;
2. Enrichir l’outil avec de nouveaux indicateurs relatifs aux domaines suivants : médecine générale, santé mentale, soins de longue durée, soins aux personnes en fin de vie, promotion de la santé ; ajouter des indicateurs relatifs à la continuité des soins et à l’approche centrée sur le patients (deux sous-dimensions de la qualité) ; enfin, proposer des indicateurs relatifs à l’équité dans le système de santé ;
3. Mesurer les indicateurs sélectionnés lorsque c'est possible, ou identifier les lacunes dans la disponibilité des données ;
4. Interpréter les résultats afin de fournir une évaluation globale de la performance du système belge de santé, au moyen de plusieurs critères, y compris une comparaison au niveau international.
MÉTHODES Un examen approfondi de la littérature indexée et de la littérature grise a été effectué pour trouver de nouveaux indicateurs dans les domaines et dimensions susmentionnés. Les indicateurs les plus pertinents ont été sélectionnés, en collaboration avec des experts externes dans chaque domaine. Au total, 74 indicateurs ont été sélectionnés et mesurés. Pour chaque indicateur, des analyses ont été menées au niveau national et régional (quand les données étaient disponibles à ce niveau), par statut sociodémographique (si possible). Les résultats ont aussi été comparés à ceux des 15 pays de l’Union Européenne (UE). Enfin, une évaluation globale a été effectuée.
Source des données L’étude a exploité au maximum les données disponibles en routine (p.ex. bases de données administratives, registres nationaux ou enquêtes récurrentes) : les données administratives de sortie des hôpitaux (RHM), l’échantillon permanent, les bases de données de l’INAMI (doc N, Pharmanet), le Registre Belge du Cancer, les données de surveillance des infections nosocomiales, l’enquête de santé par interview, les études de vaccination et la base de données de la “Direction générale Statistique et Information économique” (DGSIE).

iv Performance du système de santé KCE Report 196B
RÉSULTATS Etat de santé (4 indicateurs) Les quatre indicateurs relatifs à l’état de santé évoluent positivement au cours du temps. L’espérance de vie est légèrement inférieure à la moyenne des pays de l’UE-15, tandis que l’espérance de vie en bonne santé (c’est-à-dire le nombre d’années restant à vivre sans limitation des activités) et la mortalité infantile occupent des positions moyennes dans le classement. Le taux de personnes percevant leur santé comme (au moins) bonne est supérieur à la moyenne des pays de l'UE-15.
Accessibilité des soins (13 indicateurs) En ce qui concerne l’accessibilité financière, malgré la couverture universelle par l’assurance-maladie et l’existence de filets de sécurité sociaux (MAF, OMNIO, Fonds spécial de solidarité), certaines observations sont préoccupantes telles qu’un niveau élevé de dépenses à charge du patient, et un certain niveau de report des contacts avec les services des soins de santé pour des raisons financières. L’accessibilité des mesures de prévention montre des résultats divergents, avec un taux assez moyen de dépistage du cancer (avec des disparités sociales et parfois régionales), un taux de vaccination moyen contre la grippe chez les personnes âgées, mais un bon taux de vaccination chez les enfants. Un autre aspect de l'accessibilité concerne l’adéquation entre les forces de travail en soins de santé (médecins, infirmières) et les besoins de la population. Même si d’importants efforts ont été entrepris pour rendre disponibles les données relatives aux forces de travail, nous manquons toujours d'informations sur le nombre de professionnels de la santé nécessaires pour répondre aux besoins.
Qualité des soins : efficacité (7 indicateurs), adéquation (8), sécurité (6), continuité (7), approche centrée sur le patient (3) La qualité a été subdivisée en 5 sous-dimensions. Concernant l’efficacité, les résultats sont mitigés. Ils sont très bons quant au taux de survie après cancer, mais préoccupants dans le domaine de la santé mentale ; la Belgique présente en effet le second taux de suicide le plus élevé d'Europe (avec de très fortes disparités régionales) ainsi qu’un nombre de colocations en hôpital psychiatrique en augmentation. Pour décrire l’efficacité des soins dans le domaine de la santé mentale davantage d’indicateurs et de données sont nécessaires. L’adéquation des soins est assez décevante, avec des taux élevés et en augmentation de dépistage du cancer du sein en dehors des groupes cibles, un suivi modéré des recommandations (antibiotiques, patients diabétiques) et une augmentation des taux de césarienne, avec une grande variabilité entre les hôpitaux. La sécurité des soins présente des résultats encourageants, avec une tendance à la baisse concernant l‘exposition aux rayons ionisants médicaux, les infections nosocomiales et la mortalité hospitalière après une fracture de la hanche. Par ailleurs, l’incidence de la septicémie post-opératoire et la prescription d’antidépresseurs anticholinergiques aux personnes âgées présentent des niveaux stables. Cependant, l’incidence d'escarres est en hausse. La continuité et la coordination des soins présentent des résultats mitigés, avec une bonne continuité relationnelle avec le même praticien, un taux moyen et en augmentation de consultation multidisciplinaire pour les cas de cancer, mais un faible taux de couverture du dossier médical global et un taux élevé de réadmission dans les hôpitaux psychiatriques. L’approche centrée sur le patient n’a pu être évaluée que très partiellement. Le taux de satisfaction envers les services de santé est élevé, et on observe aussi une tendance à la hausse des décès au domicile. Mais il faut collecter davantage de données dans ce domaine.

KCE Report 196B Performance du système de santé v
Efficience du système de santé (3 indicateurs) L’efficience du système de santé présente des résultats moyens à bons, avec une augmentation de la prescription de médicaments « bon marché », de l’usage de la chirurgie de jour et une diminution de la durée du séjour pour un accouchement normal. Toutefois, ce message positif doit être tempéré par l’inadéquation, et donc le gaspillage de ressources, que montrent certains indicateurs, comme les mammographies en dehors du groupe cible évoquées ci-dessus.
Durabilité du système de santé (6 indicateurs) La durabilité du système de santé présente certains résultats interpellants concernant le manque de remplacement de la cohorte actuelle de médecins généralistes. Il faudrait aussi des données sur le besoin en personnel infirmier associées à des données sur l’évolution du nombre d’infirmiers.
Équité (analyses de tous les indicateurs en fonction du statut socioéconomique et de 2 indicateurs contextuels) La dimension de l’équité a été abordée de deux manières complémentaires. Tout d’abord, les inégalités ont été analysées en fonction du statut socioéconomique pour l’état de santé, les modes de vie et l’utilisation des soins de santé. De grandes inégalités ont été observées dans les indicateurs relatifs à la santé et au mode de vie. Des inégalités ont aussi été observées concernant le dépistage du cancer et le suivi des patients atteints de maladies chroniques. Toutefois, comme la plupart des indicateurs basés sur les hôpitaux n’ont pas pu être étudiés en fonction du statut social dans le cadre de ce projet, les conclusions concernant les inégalités en qualité des soins sont encore largement incomplètes. L’équité a également été abordée par le biais de deux indicateurs mettant en évidence ce problème au niveau macro. Le premier est la progressivité du financement des soins de santé. Il est en diminution, ce qui constitue une évolution vers moins d’équité. Le second est l’index Gini qui correspond au niveau d’inégalité dans la répartition globale des revenus, et qui est lié à un état de santé général moins bon. Cet indice est relativement peu élevé en Belgique, mais il augmente au fil du temps, ce qui indique une répartition moins égale des revenus dans notre pays.
Promotion de la santé (15 indicateurs) Enfin, la promotion de la santé a été principalement abordée au moyen d’indicateurs classiques sur la santé et le mode de vie, complétés par des indicateurs relatifs aux politiques de santé, aux milieux sains et aux aptitudes individuelles. En raison de la disponibilité très limitée d’indicateurs adéquats et de données en dehors des indicateurs classiques de la santé et du mode de vie, seul un aperçu fragmentaire a pu être fourni. La plupart des indicateurs de la santé et du mode de vie présentent un taux national intermédiaire par rapport aux 15 pays de l’UE, mais d’importantes disparités régionales et sociales ont été observées. Nous mettons en évidence le problème de l’obésité et du surpoids qui présente un niveau élevé et une tendance à la hausse, avec d’importantes disparités. La consommation de tabac diminue, mais avec de fortes disparités sociales et régionales. La consommation de fruits et de légumes est largement inférieure aux besoins quotidiens, mais est en hausse. Le manque de support social présente aussi d’importantes disparités sociales et régionales et est particulièrement préoccupant chez les personnes âgées. La Belgique se classe à un rang intermédiaire dans le classement international du Tobacco Control Scale. En outre, certains indices complexes visent à mesurer l’importance des politiques locales de promotion de la santé dans divers environnements (écoles, communes, entreprises) mais ne sont disponibles qu’en Flandre et sont difficiles à interpréter sans une analyse en profondeur.

vi Performance du système de santé KCE Report 196B
CONCLUSION ET DISCUSSION Au moyen de 74 indicateurs, ce rapport fournit une vue d’ensemble de la performance du système de santé belge, donne des signaux aux autorités de santé et pose des questions en vue du suivi ou de recherches ultérieures. Par rapport à la première évaluation du système de santé en Belgique, qui constituait principalement une étude de faisabilité, le rapport 2012 apporte une amélioration substantielle : il est plus complet et met à jour l'outil précédent des 55 indicateurs en intégrant des indicateurs plus pertinents. Il permet aussi de mesurer l’évolution de certains indicateurs. Certaines lacunes dans les données de routine ont été comblées, comme les taux de mortalité infantile, ou le taux de survie après cancer. Cependant, il ne couvre pas de la même manière tous les domaines des soins de santé ni tous les groupes de patients. Les indicateurs donnent des avertissements concernant l’état du système de santé en termes d'accessibilité, de qualité, d’efficience, de durabilité et d’équité. Dans certains cas, les décideurs politiques connaissent déjà les problèmes et ont déjà commandé des analyses supplémentaires pour savoir quelle action entreprendre. Dans d’autres cas, il s’agit de nouveaux signaux adressés aux décideurs politiques, ce qui nécessitera donc une analyse approfondie. La présentation des indicateurs de manière complète et structurée vise à faciliter la priorisation des actions nécessaires et/ou des études à mener. La Belgique n’est pas le premier pays à relever ce défi. Avec la signature en 2008 de la Charte de Tallinn, les États membres se sont officiellement engagés à suivre et à évaluer la performance de leur système de santé. Plusieurs pays voisins ayant des années d’expérience dans la mesure de la performance de leur système de santé ont servi d’exemple pour élaborer ce rapport, notamment les Pays-Bas. La faible disponibilité de données récentes est une des faiblesses entravant la mesure de la performance (comme l’indiquent aussi les rapports précédents sur la performance aux Pays-Bas). La mise à jour régulière des données administratives et la publication dynamique des résultats sur un site Internet seraient l’une des modalités à investiguer.
Avec la Directive européenne sur l’application des droits des patients dans les soins de santé transfrontaliers, cet engagement devient une question intéressant tous les États members.a Dès la transposition de la Directive dans la législation nationale en octobre 2013, les États membres devront faire en sorte que les patients issus d’un autre État membre puissent obtenir des informations pertinentes sur les normes de sécurité et de qualité, afin de choisir en connaissance de cause leurs soins de santé transfrontaliers. Dans ce contexte, le présent rapport établit non seulement la base d’une future évaluation systématique de la performance, mais il peut aussi être considéré comme une première étape dans l’engagement de la Belgique à assurer des soins de santé sûrs, de haute qualité, accessibles et efficients, tant pour les patients belges que pour les patients étrangers.
a Directive 2011/24/UE du Parlement européen et du conseil du 9 mars 2011
relative à l’application des droits des patients en matière de soins de santé transfrontaliers, JO L 88/45, 4 avril 2011

KCE Report 196B Performance du système de santé vii
RECOMMANDATIONSb
Recommandation d’ordre général aux responsables politiques Le concept de performance est implicitement lié à l’atteinte d’objectifs. Si le rapport actuel pose un «constat de la situation», sa principale utilité devrait s’orienter vers une fonction «d’amélioration de la situation». Dans ce but, il est recommandé que les décideurs politiques explicitent des objectifs mesurables et fixent des délais pour les réaliser en tenant compte des recommandations qui suivent.
Constats positifs (situation à maintenir) et constats négatifs (signaux d’attention) De manière générale, il est recommandé que les institutions et instances concernées s’appuient sur les constats qui suivent afin, soit de maintenir le cap dans les domaines pour lesquels des constats positifs ont pu être établis, soit d’améliorer la situation dans les domaines où des points d’attention sont signalés
Maintenir les constats positifs : • Etat de santé : l’état de santé ‘rapporté’ ou ‘perçu’ mesuré par les enquêtes santé (Institut
Scientifique de Santé publique) est meilleur que le niveau moyen européen. • Couverture de mesures préventives : le taux de vaccination des enfants est meilleur que le
niveau moyen européen. • Qualité des soins :
o Efficacité des soins curatifs : très bon résultats pour la survie à 5 ans après cancer du sein ou après cancer colorectal en comparaison des autres pays européens.
o Bonne continuité relationnelle avec le médecin généraliste et très grande satisfaction (au-dessus de 90%) des Belges lors de leurs contacts avec le système de santé.
• Efficience : l'augmentation des taux d’hospitalisation de jour et du taux d'utilisation des médicaments moins chers témoignent d'une amélioration de l'efficience.
Considérer les points d’attention pour orienter les futures politiques de santé : • État de santé :
o Les très hauts taux de suicide par rapport à la moyenne européenne sont interpellants.
b Le KCE reste seul responsable des recommandations adressées aux autorités publiques.

viii Performance du système de santé KCE Report 196B
o On observe une proportion croissante de personnes en surpoids ou obèses et par ailleurs un taux d’activité physique relativement bas, toujours par rapport à la moyenne européenne.
• Couverture de mesures préventives : Les taux de couverture de dépistage du cancer du sein et du col de l’utérus sont bas dans les groupes cibles en comparaison du niveau moyen européen. La couverture du dépistage organisé du cancer du sein est insuffisante pour être efficiente. Autre point d’attention, le dépistage en dehors des groupes cibles du dépistage organisé pour le cancer du sein est important et en augmentation pour les 40-49 et pour les 70-79 ans, ce qui est contreproductif en termes de santé publique et d’utilisation des ressources collectives.
• Équité/inégalités sociales : Les personnes avec un statut socioéconomique plus bas (mesuré par le niveau d’instruction ou par l’accès au remboursement préférentiel des soins de santé) présentent par rapport à la classe la plus élevée : un plus mauvais état de santé (espérance de vie, espérance de vie en bonne santé, mortalité infantile, obésité), des habitudes de vie moins saines (nutrition, tabac, activité physique), une moins bonne couverture de dépistage du cancer, un suivi moins bon pour les patients diabétiques, un support social moins présent et décèdent plus souvent à l’hôpital qu'à leur lieu de résidence habituel.
• Qualité des soins : o Soins (in)appropriés : plusieurs indicateurs montrent que la pratique médicale n'est
pas toujours appropriée. Ainsi : Le choix des antibiotiques prescrits en première intention ne correspond pas
suffisamment aux recommandations et ne montre pas d'amélioration à travers le temps (sauf chez les enfants).
Le pourcentage de patients diabétiques correctement suivis selon les recommandations est insuffisant.
Bien que le niveau soit un peu inférieur à la moyenne des autres pays européens, le taux de césarienne est élevé (20%) et on constate une grande variabilité des taux de césarienne entre hôpitaux pour des grossesses non compliquées.
o Sécurité des soins : le niveau d’irradiation d’origine médicale, bien qu'en légère diminution en 2011, reste très élevé par rapport à la moyenne européenne.

KCE Report 196B Performance du système de santé ix
o Continuité des soins : certains indicateurs montrent une faiblesse dans ce domaine. Ainsi :
Malgré une augmentation constante, le pourcentage de patients disposant d'un dossier médical global (DMG) reste encore trop faible.
Les taux de réadmission dans les hôpitaux psychiatriques sont relativement élevés par rapport à la moyenne européenne.
• Pérennité du système : Le système de santé s'appuie sur une première ligne de soins dont la médecine générale est un élément important. Or l'âge moyen des généralistes ne cesse d'augmenter, tandis que les quotas prévus par la commission de planification ne sont pas remplis depuis quelques années. A pratique constante, ceci pourrait poser des problèmes rapidement quant au fonctionnement de la première ligne de soins.
Recommandation d’amélioration des systèmes d’information de santé La qualité des données et la rapidité avec laquelle elles sont rendues disponibles sont des critères essentiels afin que les indicateurs qui en dépendent soient pertinents. • Délais de mise à disposition des données :
o Poursuivre les efforts afin de transmettre des mises à jour récentes aux organisations internationales (OECD, Eurostat, OMS) ;
o Accélérer la mise à disposition des bases de données administratives (Résumé Hospitalier Minimum).
• Données par domaine de soins : o Soins de santé mentale : réformer le Résumé Psychiatrique Minimum afin de l’adapter
aux standards internationaux (identifiant patient unique) et aux évolutions dans le secteur. Ceci demande une révision qui permette de suivre l’ensemble du trajet des soins des patients, y compris en dehors de l’hôpital.
o Soins de longue durée : s’assurer que les données collectées dans le cadre du projet BelRai seront bien disponibles à un niveau national pour permettre la mesure des différents indicateurs sélectionnés.
o Santé bucco-dentaire : sur-échantillonner le groupe des enfants de 12 ans dans l’enquête sur la santé bucco-dentaire afin de pouvoir calculer correctement les indicateurs internationaux.
o Soins aux personnes en fin de vie : améliorer l'exploitation des données existantes (Registre du Cancer et réseau des Médecins Vigies).

x Performance du système de santé KCE Report 196B
o Santé publique : compléter la banque de données de consommation des médicaments afin de disposer de données concernant l’ensemble des médicaments consommés, y compris ceux qui ne sont pas remboursés mais qui sont essentiels à étudier pour la santé publique ou la sécurité du patient ( benzodiazépines, certains anti-inflammatoires)
Recommandations sur la récolte de nouvelles données ou de nouvelle recherches Certaines données nécessaires à l’établissement des indicateurs sélectionnés doivent encore faire l’objet de récolte. • Inégalités socio-économiques : les bases de données administratives ne peuvent fournir
qu’une réponse partielle. Certaines données manquent complétement (par exemple, le statut socio-économique dans les données des Résumés hospitaliers ou l’origine ethnique), d’autres sont peu précises ou peu discriminantes (par exemple le statut BIM).
• Accessibilité financière : améliorer l'enquête sur le budget des ménages afin d'enregistrer toutes les charges financières des patients liées à leurs soins de santé et afin de permettre une analyse par niveau socio-économique.
• Expérience du patient : des données seront disponibles grâce à la prochaine enquête santé de l’ISP (elles concerneront les médecins généralistes et l’ensemble des spécialistes sans distinction). Il faudrait toutefois collecter des données par type de spécialité).
• Promotion de la santé : o Il n’y a pas de données sur la « litéracie de santé » (health litteracy) en Belgique. En
particulier, il est recommandé que la Belgique participe aux recherches européennes sur le développement d’outils pour mesurer la litéracie de santé et pour qu’elle s’inscrive dans une perspective de collecte de ces données.
o Promotion de la santé dans les milieux de vie : il existe des initiatives dans les différentes régions du pays, toutefois, toutes ces initiatives ne font pas l’objet d’un relevé statistique. En Flandre les données relatives à la promotion de la santé dans certains milieux de vie (écoles, communes, entreprises) sont collectées au moyen des enquêtes VIGeZ. Il est donc recommandé que les autres régions collectent plus systématiquement les données sur la promotion de la santé dans les milieux de vie en fonction de leurs besoins en information pour documenter et soutenir leurs politiques.
o Finalement, il est recommandé de vérifier la possibilité d’inclure des indicateurs de promotion de la santé spécifiquement dans le domaine des soins de santé dans le prochain rapport.

KCE Report 196B Performance du système de santé xi
Recommandations pour le prochain rapport performance (prévu pour décembre 2015) • A l’attention du SPF Santé Publique, de l’INAMI et de l’ISP
o Calculer les indicateurs pour lesquels les données ne sont pas encore disponibles, mais qui le seront d’ici le prochain rapport (projet sur les trajets de soins en ambulatoire, projet BelRAI, expérience des patients dans l’enquête santé, prévalence des infections nosocomiales, délai d’enregistrement des médicaments).
o A l’avenir à des fins de monitoring, il est souhaitable d’inclure les résultats les plus récents. Ces indicateurs devront de préférence être mesurés en routine par les institutions/ administrations, gestionnaires respectifs des banques de données administratives. Les résultats seront transmis aux équipes chargées de l'actualisation du rapport, selon un échéancier et un canevas à préciser.
o Suivre les évolutions internationales (OECD, OMS, Eurostat) afin d’adapter le set d’indicateurs en Belgique si nécessaire.
• A l’attention des équipes de recherche o Identifier de nouveaux indicateurs pour les thématiques peu documentées (question
des forces de travail en soins infirmiers, par exemple). o Actualiser l’évaluation de la performance sur base des données les plus récentes. o Analyser la cohérence globale (en particulier pour renforcer les dimensions relatives à
l’efficience et à la pérennité) et actualiser le set d’indicateurs, à la lumière de nouvelles preuves ou de nouvelles thématiques prioritaires.


KCE Report 196
TABL
6
LE OF COONTENTLISTLISTLIST
11.11.2
1.3
22.12.22.32.4
2.52.62.72.8
Belgian
TS T OF FIGURES ..T OF TABLES ...T OF ABBREVIA
SYNTHÈSECONTEXTECONTEXTE .CADRE CONBELGE .........LES OBJECT1.3.1 Les o
sant1.3.2 Les oFORCES ETCOMMENT INÉTAT DE SAACCESSIBILQUALITÉ DE2.4.1 Effic2.4.2 Adéq2.4.3 Sécu2.4.5 Cont2.4.6 CentEFFICIENCEPÉRENNITÉPROMOTIONÉQUITÉ ET É2.8.1 Inég
n Health System
.........................
.........................ATIONS ............ ........................
E, CADRE CONC............................
NCEPTUEL D'ÉVA............................
TIFS DE CE RAPPobjectifs stratégiqé ..........................objectifs générauxT FAIBLESSESNTERPRÉTER LENTÉ .....................ITÉ ......................
ES SOINS .............acité ....................quation ................urité .....................tinuité des soins ..tralité du patient ..
E DU SYSTÈME D............................
N DE LA SANTÉ ..ÉGALITÉ ..............alités socio-écono
Performance
.........................
.........................
.........................
.........................CEPTUEL ET O............................ALUATION DE LA............................PORT ..................ques du processus............................x et opérationnelsDU SYSTÈME
ES TABLEAUX S................................................................................................................................................................................................................................
DE SANTÉ ...............................................................................................omiques ..............
.........................
.........................
.........................
.........................OBJECTIFS .......
............................A PERFORMANC........................................................s d'évaluation de ............................s du rapport 2012DE SANTÉ EN YNOPTIQUES PR............................................................................................................................................................................................................................................................................................................................................................................
.........................
.........................
.........................
.........................
.....................................................E DU SYSTÈME ........................................................la performance du.......................................................BELGIQUE .....
RÉSENTANT LES............................................................................................................................................................................................................................................................................................................................................................................
..........................
..........................
..........................
........................ 1
........................ 1.......................... 1DE SANTÉ .......................... 1.......................... 1u système de .......................... 1.......................... 1........................ 1S RÉSULTATS ?.......................... 1.......................... 1.......................... 2.......................... 2.......................... 2.......................... 2.......................... 2.......................... 2.......................... 3.......................... 3.......................... 3.......................... 3.......................... 3
1
. 5
. 7
. 9 12 12 12
13 15
15 15 16 16 18 19 22 22 24 26 27 29 30 31 32 36 36

2
2.93
3.1
3.23.3
4
11.1
1.21.3
1.41.522.12.22.333.13.2
Belgian
CONCLUSIOLE RAPPORLIMITATIONQUELLE ESTSANTÉ ? ......QUELLE ESTQUELLES SO3.3.1 La p3.3.2 Pren3.3.3 Une CONCLUSIOSCIENTIFICBACKGROUCONTEXT ....1.1.1 Inter1.1.2 NatioTHE BELGIAOBJECTIVES1.3.1 Strat1.3.2 OverMETHODS TTHE 2012 SEOVERALL HHOW DID WEFACTS AND KEY FINDINGACCESSIBIHOW DID WEFACTS AND
n Health System
ONS SUR LES FORT 2012 SUR LANS.....................T L'UTILITÉ D’UN............................
T LA VALEUR AJOONT LES LIMITATerformance, mais
ndre des décisionsvision plus globa
ON GÉNÉRALEC REPORT ........UND AND APPR............................
rnational context ..onal context .........N PERFORMANC
S OF THE PERFOtegic objectives ofrall and operationO REACH OPER
ET OF PERFORMHEALTH STATUE DESCRIBE THEFIGURES ...........
GS .......................ILITY OF CAREE EVALUATE THFIGURES ...........
Performance
ORCES ET FAIBLEA PERFORMAN......................... RAPPORT SUR ............................OUTÉE DE CE RTIONS DE CE RAs en fonction de qus sur base de donle, mais certaines
E ................................................ROACH ................................................................................................CE FRAMEWORKORMANCE PROJf the HSPA proceal objectives of th
RATIONAL OBJECMANCE INDICATOUS OF THE POPE OVERALL HEA........................................................
E ........................E ACCESSIBILIT............................
ESSES ................NCE : UTILITÉ, .........................LA PERFORMAN............................
RAPPORT COMPAAPPORT ? ...........uel objectif ?........
nnées obsolètes ?s lacunes subsiste...............................................................................................................................................................K AND DEFINITIOECT ....................
ess ........................he 2012 report .....CTIVES ................ORS AND STRUCPULATION .......
ALTH STATUS OF.................................................................................
TY OF HEALTHCA............................
............................VALEUR AJOU.........................NCE DU SYSTÈM............................ARÉE AU PRÉCÉ........................................................? ..........................ent ......................................................................................................................................................................................ONS ....................................................................................................................................
CTURE OF THIS R.........................
F THE POPULATI.................................................................................
ARE? ...............................................
KCE Report
.......................... 4UTÉE ET ........................ 4ME DE .......................... 4
ÉDENT? ............ 4.......................... 4.......................... 4.......................... 4.......................... 4........................ 4........................ 4........................ 4.......................... 4.......................... 4.......................... 4.......................... 4.......................... 5.......................... 5.......................... 5.......................... 5REPORT ........... 5........................ 5ION? ................. 5.......................... 5.......................... 6........................ 6.......................... 6.......................... 6
t 196
40
42
42 43 44 44 44 44 46 48 48 48 48 49 49 53 53 53 54 55 56 56 56 60 60 60 61

KCE Report 196
6
3.344.1
4.2
4.3
4.4
4.5
55.15.25.366.16.2
Belgian
KEY FINDINGQUALITY OEFFECTIVEN4.1.1 How4.1.2 Fact4.1.3 Key APPROPRIAT4.2.1 How4.2.2 Fact4.2.3 Key SAFETY OF C4.3.1 How4.3.2 Fact4.3.3 Key CONTINUITY4.4.1 How4.4.2 Fact4.4.3 Key PATIENT CE4.5.1 How4.5.2 Fact4.5.3 Key EFFICIENCYHOW DID WEFACTS AND KEY FINDINGSUSTAINABHOW DID WEFACTS AND
n Health System
GS .......................OF HEALTHCARNESS OF CARE ..w did we evaluate tts and figures .......findings ...............TENESS .............
w did we evaluate tts and figures .......findings ...............CARE ..................
w did we evaluate tts and figures .......findings ...............
Y OF CARE ..........w did we evaluate tts and figures .......findings ...............NTEREDNESS ...
w did we evaluate ts and figures .......findings ...............Y IN HEALTHCAE EVALUATE THFIGURES ...........
GS .......................BILITY OF THE E EVALUATE THFIGURES ...........
Performance
............................RE .................................................the effectiveness ....................................................................................the appropriatene....................................................................................the safety of care....................................................................................the continuity of c....................................................................................patient centeredn........................................................ARE .................E EFFICIENCY IN........................................................HEALTH SYST
E SUSTAINABILI............................
............................
.........................
............................of care? ..................................................................................................
ess of care? .............................................................................................? .............................................................................................................
care? ........................................................................................................
ness? .....................................................................................................N HEALTHCARE?........................................................
TEM ..................TY OF THE HEA............................
..............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................? ..........................................................................................................
ALTH SYSTEM? ..............................
.......................... 7........................ 7.......................... 7.......................... 7.......................... 7.......................... 7.......................... 7.......................... 7.......................... 7.......................... 8.......................... 8.......................... 8.......................... 8.......................... 8.......................... 8.......................... 8.......................... 9.......................... 9.......................... 9.......................... 9.......................... 9.......................... 9........................ 9.......................... 9.......................... 9.......................... 9...................... 10........................ 10........................ 10
3
70 71 71 71 72 77 78 78 78 84 84 84 85 89 89 89 90 93 93 93 94 95 96 96 96 99 00 00 00

4
6.377.17.2
7.388.18.2
8.3
9
10
APP
APPAPP
Belgian
KEY FINDINGPERFORMAHOW DID WEFACTS AND 7.2.1 Heal7.2.2 Inter7.2.3 HealKEY FINDINGEQUITY ANINTRODUCTSOCIO-ECON8.2.1 How8.2.2 Fact8.2.3 Key EQUITY OF T8.3.1 How8.3.2 Fact8.3.3 Key TOWARDS ASSESSMEGENERAL CAPPENDICE
ENDIX 1. LIST TIER OF TH
ENDIX 2. LISTENDIX 3. LIST
REFERENC
n Health System
GS .......................ANCE OF HEALE EVALUATE THFIGURES ...........lth outcomes .......rmediate health oulth Promotion outcGS .......................D EQUALITY ..ION .....................NOMIC INEQUAL
w did we evaluate sts and figures .......findings ...............
THE HEALTH SYw did we evaluate tts and figures .......findings ...............A MORE COMP
ENT: ADDRESSCONCLUSION .ES ....................T OF INDICATOHE HEALTH SYT OF CHANGEST OF INDICATO
CES ...................
Performance
............................LTH PROMOTIOE PERFORMANC........................................................utcomes ..............comes ..................................................................................................LITIES .................socio-economic in........................................................STEM AT A GLOthe equity of the h........................................................PREHENSIVE H
SING CURRENT..................................................
ORS MEASUREYSTEM, DOMAINS TO INDICATOORS MEASURA.........................
............................ON .....................CE OF HEALTH P.............................................................................................................................................................................................................................nequalities? .................................................................
OBAL LEVEL ........health system at a........................................................
HEALTH SYSTET SHORTCOMIN..................................................
ED IN THE 2012 N OF CARE AN
ORS COMPAREABLE IN A NEAR
.........................
.....................................................
PROMOTION? .................................................................................................................................................................................................................................................................................................................................................a global level? .............................................................EM PERFORMANGS ....................................................................REPORT, CLA
ND DIMENSIONED TO THE 2010R FUTURE ................................
KCE Report
........................ 10...................... 10........................ 10........................ 11........................ 11........................ 11........................ 11........................ 12...................... 12........................ 12........................ 12........................ 12........................ 12........................ 13........................ 13........................ 13........................ 13........................ 13
ANCE ...................... 13...................... 13...................... 13
ASSIFIED BY ..................... 130 REPORT ... 14...................... 14...................... 15
t 196
07 07 07 10 10 15 19 22 23 23 23 23 25 30 30 30 31 33
33 37 38
38 42 47 50

KCE Report 196
LIST OF F
6
FIGURES FigurFigurrégioFigurFigurFigurFigurFigurcompFiguroveraFigurFigurFigurcompFigurcompFigurFigurwith dFigurby yeFigurFigur(2004FigurFigurinternFigurFigurFigur
Belgian
re 1 – Cadre concre 2 – Indicateur dns ........................re 3 – The concepre 4 – Life expectare 5 – Infant mortare 6 – Number of pre 7 – Out-of-pockparison .................re 8 – Percentageall (b)) within the lare 9 – Breast cancre 10 – Percentagre 11 – 5-year relaparison (2004) .....re 12 – Suicide ratparison .................re 13 – Percentagre 14 – Employmedisability: internatire 15 – Mammogrear and region .....re 16 – C-sectionsre 17 – Defined da4-2010) and internre 18 – Chemothere 19 – Expositionnational comparisore 20 – Mean incidre 21 – Percentagre 22 – Percentag
n Health System
ceptuel d'évaluatiode l'équité: coeffic............................
ptual framework toancy at birth: interality rate: internatipractising physiciaket expenditures (............................ of women (aged ast two years, by cer and cervical cae of children cove
ative survival after............................tes (number per 1............................e of involuntary c
ent rates by healthional comparison am coverage of w............................
s per 1000 live birtaily dosage of antnational compariserapy near end-of-n to medical radiaton ........................dence of Healthcae of population we of hospitalisatio
Performance
on de la performanient de Gini après............................o evaluate the perrnational comparisonal comparison .ans (per 1000 popas a percentage o............................50-69) who had aregion (2006-201ancer screening: iered by main vaccr breast, cervix an............................100 000 populatio............................ommittals in psych condition, as a r(2002) ................
women aged 40-49............................ths: international idepressants per on (2000-2010) ..-life for patients wtion per inhabitant............................are Acquired MRSith a global medic
ons for the elderly
nce du système ds taxation et transf............................
rformance of the Bson (2000-2010) ..............................pulation): internatof total health exp............................a mammogram (w0) ........................international comcinations (2000-20nd colorectal canc............................n) per region (199............................
chiatric hospitals, batio of the employ............................9 years and of wo............................comparison .........1000 population p............................
with cancer, by plat (most 20 exams............................
SA, per 1000 admcal record (GMD –
(aged 65 and ove
de santé belge .....ferts, en Belgique............................Belgian health sys........................................................ional comparison
penditures): intern............................
within program (a) ............................parison (2000-20009): internationacer for females: int............................99-2008) and inte............................by region (2000-2yment rate of all p............................omen aged 70-79 ........................................................per day: by region............................ce of death ........., expressed in mS............................issions (1994-201
– DMG), by regioner) followed by a c
.......................... 1e et dans les .......................... 4
stem ................... 5.......................... 5.......................... 5.......................... 6ational .......................... 6or .......................... 610) ..................... 6l comparison ..... 6ternational .......................... 7rnational .......................... 7
2009) .................. 7people .......................... 7years, .......................... 7.......................... 8
n .......................... 8.......................... 8
Sv): .......................... 810) ..................... 8n (2006-2009) .... 9contact
5
14
40 50 58 59 62
64
66 67 68
74
75 76
77
79 81
82 83
85 87 90

6
with aFigurFigurFigurinternFigurFigurFigurFigurFigurFigurFigurpromFigurregioFigurFigurFigurconsu30 mFigurFigurand in
Belgian
a GP within 1 weere 23 – Degree of re 24 – Percentagre 25 – Percentagnational comparisore 26 – Average lere 27 – Age distribre 28 – Medical anre 29 – Acute carere 30 – Health expre 31 – Total healtre 32 – The Nutbeotion ...................
re 33 – Percentagn (1997-2008), anre 34 – Diagnosticre 35 – Rate of there 36 – Percentagumption, (c) consuin of physical activre 37 – Internationre 38 – Gini coefficnternational comp
n Health System
ek after dischargesatisfaction with he of low-cost mede of surgical one-on ........................ength of stay for abution of GPs (200nd nursing graduae bed days per capenditures in Belgth expenditures as
eam’s framework a............................e of the adult pop
nd international coc rate of HIV by ree new HIV diagnoe of the populatiouming at least 2 frvity per day, by re
nal comparisons ocient before and aparison .................
Performance
, by region (2003-healthcare servicedication delivered -day hospitalisatio............................
a normal delivery: 00-2004-2009) ....ates (per 100 000 pita, international
gium by main funcs a % of GDP: intand selected indic............................
pulation (aged 18 omparison (2000-egion, for all casesosis per 100 000 inon (a) smoking daruits and 200 vegegion (1997/2001-on the Tobacco Coafter taxation and ............................
-2009) .................es, by type of servin ambulatory set
ons on all surgical ............................international com............................pop): internationa comparison ........
ction in the Systemernational compacators to measure............................years or older) wi2008 ....................s (a) and for Belginhabitants: Internaily, (b) with probleetables daily, (d) -2008) ..................ontrol Scale in Eutransfers (1998-2............................
............................vice (2008) ..........tting (DDDs) (200 hospitalisations: ............................
mparison ...........................................al comparison (20............................
m of Health Accouarison ...................e performance of h............................th obesity (BMI ≥............................an cases only (b)ational compariso
ematic alcohol performing at leas............................
urope (2010) ........2010): Belgium ............................
KCE Report
.......................... 9
.......................... 900-2010) ............. 9 .......................... 9.......................... 9........................ 10
010) .................. 10........................ 10
unts (2010) ....... 10........................ 10health ........................ 10
≥30), by ........................ 11) (1985-2010) .. 11on ..................... 11
st ........................ 11........................ 12
........................ 13
t 196
91 94 97
98 99 00 02 03 05 06
09
11 13 14
16 21
32

KCE Report 196
LIST OF T
6
TABLES TableTableTableTableTableTableTableTableTableTableTableTableTableTable(/100TableTablepopuTableTableTableTableTableTablefollowTableTableTableTableTable
Belgian
eau 1 – Indicateureau 2 – Indicateureau 3 – Indicateureau 4 – Indicateureau 5 – Indicateure 6 – Indicateurs éeau 7 – Indicateureau 8 – Indicateureau 9 – Indicateureau 10 – Indicateueau 11 – Synthèseeau 12 – Indicateue 13 – Life expecte 14 – Number of 0 population) (20
e 15 – Out-of-pocke 16 – Number of lation 65 years an
e 17 – 5-year relate 18 – Exposition e 19 – Percentagee 20 – Evolution oe 21 – Mean age oe 22 – Progressionwing graduation ace 23 – Percentagee 24 – Total healthe 25 – Alcohol cone 26 – Offer of phye 27 – Life expect
n Health System
rs généraux de l'érs évaluant l'accesrs évaluant l'efficars de l'adéquationrs évaluant la sécuévaluant la continurs évaluant de la crs de l'efficience drs de la pérennité urs de la promotioe des inégalités sur de l'équité: progancy at birth (201practising physici10) .......................ket expenditures (accredited beds i
nd older, per regiotive survival by stato medical radiati
e of cancer patienof place of death oof practising GPs n between 1996 according to type oe of GPs using rech expenditures acnsumption habits fysical activity in seancy at 25 years
Performance
état de santé ........ssibilité aux soinsacité des soins ..... des soins ...........urité des soins ....uité et de la coordcentralité du patiedes soins .............
du système de saon de la santé ......ocio-économiquegressivité du finan0), and Healthy Lians, estimation o............................(2003-2010) ........n homes for the e
on, 2010 ..............age, period 2004-on per inhabitant ts who had a MO
over time in Flande(2000-2009) .......
and 2008 of graduof specialisation ...commended softwccording to the Syfor the populationecondary schoolsby sex and educa
............................ de santé .................................................................................................
dination des soinsnt dans le systèm............................anté .................................................s ..........................ncement public duLife Years at age 2of Full Time Equiva........................................................
elderly and nursing............................-2008: Belgium ....(expressed in nb C – COM, per regers and Brussels ............................
uates in medicine ............................
ware to maintain thstem of Health Ac
n (aged 15 or oldes in Flanders ........ational level, abso
............................
............................
............................
............................
............................s ...........................me de santé .........................................................................................................................u système de soin25 (2008), by sex alent, and density........................................................g homes per 100 ........................................................mSv): Belgium (2
gion, (2005-2008)(1998-2007) ...................................in the two years ............................heir patients’ medccounts (2003-20er) (1997-2008) ................................
olute difference to
.......................... 1
.......................... 2
.......................... 2
.......................... 2
.......................... 2
.......................... 2
.......................... 2
.......................... 3
.......................... 3
.......................... 3
.......................... 3ns de santé ........ 3
and region ........ 5y .......................... 6.......................... 6 .......................... 6.......................... 7
2004-2011) ........ 8 ......................... 9.......................... 9........................ 10
........................ 10dical records .... 1010) ................... 10........................ 11........................ 11
7
18 21 23 25 26 28 29 30 31 34 37 39 57
61 64
69 73 85 92 95 01
01 04 05 15 19

8
higheTablehigheTableTable
Belgian
est educational leve 28 – Health expeest educational leve 29 – Inequalitiese 30 – Progressivi
n Health System
vel and concentraectancy at 25 yeavel and concentras expressed with aity indicators of th
Performance
ation inequality indars by sex and eduation inequality indabsolute difference financing of the
dices (CII) (Belgiuucational level, abdices (Belgium 20ce, relative differen public healthcare
m 2001) ..............bsolute difference 04) ......................nce, and summare system (2005-20
KCE Report
........................ 12 to ........................ 12
ry measures ..... 12011) ................. 13
t 196
25
26 28 32

KCE Report 196
LIST OF A
6
ABBREVIAATIONS
Belgian
ABBREVIATIONADL ADQ AIDS BIM – RVV
BMI CAP CII CM – MC DDD DGSIE – ADSEI
DMFT DTP EARSS ECDC ECHIM EMA EPS ER EU EU – SILC FOBT FPS FTE GDP GMD – DMG GMR
n Health System
N DEFINITIActivities Average Acquired Bénéficia(verzekerBody MaCommunConcentrChristelijkDefined DDirection StatistiekDecayedDiphteriaEuropeanEuropeanEuropeanEuropeanEchantilloEmergenEuropeanEuropeanFaecal OFederal PFull TimeGross DoGlobaal MGlobal M
Performance
ION of Daily Living Daily Quantity Immunodeficienc
aire de l’Intervenrings)tegemoetkoss Index
nity Acquired Pneuration Index of Ineke Mutualiteiten –Daily Dose
générale Statistk en Economische, Missing, Filled T - Tetanos - Pertun Antimicrobial Ren Centre for Disean Community Hean Medical Agencyon Permanent – P
ncy Room n Union n Union Statistics
Occult Blood Test Public Service e Equivalent omestic Product Medisch Dossier –edical Record
cy Syndrome ntion Majorée –ming
umonia equalities – Mutualités Chrét
tique et Informate informatie Teeth ussis esistance Surveillaase Control and Palth Indicators Moy Permanente Steek
on Income and L
– Dossier Médica
Rechthebbende
tiennes – Christian
tion économique
ance System Prevention nitoring
kproef
Living Conditions
l Global
en op de Verho
n Sickness Funds
– Algemene Di
9
oogde
s
rectie

10
Belgian
GP HAI HBSC HCQI Hib HIS HIV HLY HSPA IMA – AIM IMR ISCED LE LOS MAB MMR MOC – COM MRPA – ROB MRS – RVT MRSA NSIH OECD ONE – KG OOP OR PA PAF PPP
n Health System
General PHealthcaHealth BeHealthCaHaemophHealth InHuman ImHealthy LHealth SyIntermutuInfant MoInternatioLife ExpeLength ofMaximumMeasles MultidisciMaisons Maison dMethicillinNational OrganisaOffice NaOut-of-PoOdds RaPhysical PopulatioPurchasin
Performance
Practitioner re Acquired Infectehaviour in Schooare Quality Indicathilus Influenzae Bterview Survey mmunodeficiency Life Years ystem Performancualistic Agency - Inortality Rate onal Standard Claectancy f Stay
m Billing System - Mumps - Rubelliplinair Oncologisde Repos pour Pe
de Repos et de Son-Resistant StaphSurveillance of In
ation for Economicational de l'Enfancocket tio Activity
on Attributable Frang Power Parities
tions ol-aged Childrentor
B
Virus
ce Assessment nterMutualistisch
assification of Edu
a h Consult – Consersonnes Agées -oins – Rust- en Vehylococcus Aureusfections in Hospit
c Co-operation ance – Kind en Gezi
action s
Agentschap – Ag
cation
ultation Multidisci- Rustoorden voorerzorgingstehuiss tals d Development (On
KCE Report
gence InterMutual
plinaire d'Oncologr Bejaarden
OESO – OCDE)
t 196
iste
gie

KCE Report 196
6
Belgian
PSI PYLL RAI RHM – MZG RIZIV – INAMI
RR SE SHA SP SPMA SSF THE UK UPC VIGeZ WHO WIV – ISP
n Health System
Patient SPotential Resident Résumé Rijksinstitmaladie-iRelative Socio-ecoSystem oSpecialisStandardSpecial STotal HeaUnited KiUsual ProVlaams InWorld HeWetenschof Public
Performance
Safety Indicator Years of Life LosAssessment InstHospitalier Minimtuut voor ziekte- invalidité- NationaRisk onomic
of Health Accountsst Physician dized Procedures Solidarity Fund alth Expendituresingdom ovider Index nstituut voor Gezoealth Organisationhappelijk InstituutHealth
st rument
mal - Minimale Zieken invaliditeitsver
al Institute for Hea
s
for Mortality Analy
ondheidspromotien t Volksgezondheid
kenhuisgegevensrzekering – Institualth and Disability
ysis
e en Ziektepreven
d – Institut de Sa
ut national d’assurInsurance
tie
anté Publique- Ins
11
rance
stitute

12
SYNTTHÈSE
Belgiann Health System
1
1LSjupdDsc
Q(LbscHq
ÀHudpgpppsLp
Performance
1 CONTEXOBJECT
1.1 ContexteLa première « ÉvaSystem Performanuin 2010.1 Ce prpremière définissad'approches adopDans la seconde sse sont révélés êcours du temps et
Qu'est-ce qu'uneHSPA) ?
L’HSPA est un probilan global, une ésur des indicateurscontribuer à la plaHSPA est élaboré question.2
À l'issue de la pubHSPA belge ont sune évaluation sysdemandé d’étoffeportant sur les dogénérale, la santpersonnes en fin dpatient et sur la coproposer des indisanté. Le présent Rappprésente le fruit de
XTE, CADRTIFS
aluation de la Pernce Assessment remier rapport coait un cadre conptées par d'autresection, 55 indicaêtre mesurables. points d’action en
e Évaluation de la
ocessus, spécifiquévaluation holistiqus chiffrés qui envonification stratégiqen fonction d'un c
blication de ce prouhaité la poursustématique du sys
er ce jeu d'indicamaines suivants :é mentale, les sde vie ; ajouter deontinuité des soinscateurs permetta
port sur la Perfoe ce travail.
RE CONCE
rformance des So- HSPA) en Belg
omportait deux seceptuel pour le
es pays, adaptéeateurs avaient été
Les forces, faibnvisagés ont été d
a Performance d
ue à chaque paysue du système deoient des « signauque du système dcadre stratégique
remier rapport, lesuite du projet, danstème de santé beateurs en y inté: la promotion de soins de longue es indicateurs ports (deux sous-dim
ant de mesurer l'
ormance du Syst
KCE Report
EPTUEL ET
ins de Santé » (Hgique a été publiéections principaleHSPA belge sur
es au contexte bé sélectionnés, doblesses, évolutiondiscutés.
u Système de Sa
, qui permet d’offre santé. En se basux », cet outil visede santé. Chaque e spécifique au pa
s commanditairesns le but de procéelge. Ils ont égale
égrant des indicala santé, la méddurée, les soins
tant sur la centralensions de la quaéquité du systèm
tème de Santé
t 196
T
Health ée en
es. La base
belge. ont 40 ns au
anté
rir un sant
e à
ys en
s de l' éder à ement ateurs ecine
s aux ité du alité) ; me de
2012

KCE Report 196
La Charte de Tmesurer la per
En juin 2008, le'Europe' de l'Or« 'Charte de Taprospérité ». Ceengagement posignataires s'encomptes au sujpublication de r
1.2 Cadre systèm
Le cadre conce
6
Tallinn (2008), unrformance des sy
es Ministres de la rganisation Mondiallinn sur les systèette Charte contieorte sur la performngagent à promouet de la performarésultats mesurab
conceptuel d'éme de santé beleptuel est présenté
n engagement intystèmes de sant
Santé des 53 payale de la Santé (O
èmes de santé poent sept engagemmance des systèmuvoir la transparennce des systèmes
bles ».3
évaluation de lalge é en Figure 1.
Belgian
ternational visanté en Europe
ys composant la rOMS) ont signé laur la santé et la ents. Le troisième
mes de santé : « lence et à rendre des de santé grâce l
a performance
n Health System
nt à
égion a
e es États es la
du
Performance 13

14
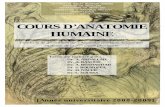
Figure 1 – Cad
Remarque : Ce ravie sont présenté
dre conceptuel d
rapport ne contient aés dans le chapitre c
'évaluation de la
aucun chapitre spécconsacré à la promo
Belgian
a performance du
cifiquement consacrotion de la santé.
n Health System
u système de san
ré aux indicateurs s
Performance
nté belge
sur les déterminantss non médicaux de lla santé. Les indica
KCE Report
teurs relatifs au mo
t 196
de de

KCE Report 196
1.3 Les objL'évaluation syun processus éobjectifs stratéterme de ce proobjectifs spécifrapport. 1.3.1 Les ob
perforLe processus H1. Informer le
pour les aid2. Rendre co
système dsignant la C
3. Suivre les temps.
1.3.2 Les obProposer et medes dimensionsque le nombre dQuatre objectifs1. Revoir les
attention pn'était disp
a Le nombr
maladie cguides dedents carcardiovascsurvie à 5l'utérus);
6
jectifs de ce raystématique de laévolutif, jalonné pgiques peuvent ocessus évolutif. fiques et des sou
bjectifs stratégiqrmance du systèHSPA poursuit troies autorités de la der à planifier les omptes, de manide santé belge, Charte de Tallinn.progrès de la pe
bjectifs générauesurer un jeu d'ins choisies du systd'indicateurs restes opérationnels ons 55 indicateurs articulière aux 11onible en 2010a.
re d'infirmières en chez les patients e bonne pratique criées, manquantes culaire chez les pe
5 ans après un diagla mortalité prém
apport performance de
par la publication être définis comCes derniers doiv
us-objectifs opéra
ques du processème de santé is objectifs stratégsanté quant à la politiques de sanère transparenteconformément à
. erformance du sy
ux et opérationnendicateurs couvraème de santé en e gérable (74 indint été fixés :
du rapport pré indicateurs pour
exercice; les coûtschroniques; les pr
clinique; le dépistagou obturées à l'âgersonnes âgées degnostic de cancer (dmaturée; l’incidence
Belgian
s systèmes de sdes rapports HS
mme les objectifsvent être différenctionnels de ce de
sus d'évaluation
giques : performance du s
nté. e, de la performaà l'engagement
ystème de santé a
els du rapport 20ant tous les domBelgique, en veillcateurs dans ce r
écédent, en portar lesquels aucune
s supplémentaires lrescriptions conforge du cancer colorge de 12 ans; le de 45 à 75 ans; ledu sein, du côlon, de des escarres d
n Health System
anté est SPA. Les s à long ciés des euxième
de la
système,
ance du pris en
au fil du
012 aines et lant à ce rapport).
ant une donnée
iées à la mes aux ectal; les dépistage e taux de du col de dans les
2
3
4
Lradsl'sp
Performance
2. Étoffer ce jeules domainesgénérale, la spersonnes encentralité du dimensions dmesurer l'équ
3. Mesurer les identifier les la
4. Interpréter lesde la performcritères, notam
Le rapport sur la apport de monitor
d'autres pays. A trsystème de santé efficacité, la pére
se veut une sourcepolitiques compéte
établissemenrisque.
u d'indicateurs en s suivants : la psanté mentale, lesn fin de vie ; a
patient et sur de la qualité) ; prité du système deindicateurs chois
acunes en terme ds résultats dans lance du systèmemment une compa
performance during national. La Bravers 74 indicatebelge s'efforce dennité/durabilité et e d'informations gents en matière de
nts de soins de lon
y intégrant des ipromotion de las soins de longue
ajouter des indicla continuité de
roposer des indice santé. sis, ou quand cde disponibilité dee but de fournir u de santé belge aaraison internatio
u système de sanBelgique y est noturs, le rapport sure mesurer l'accesl'équité du systèm
globale pour les die santé et de prom
ngue durée et au
indicateurs portana santé, la méde durée, les soinsateurs portant s
es soins (deux cateurs permetta
e n’est pas poses données. une évaluation glau moyen de diffénale.
nté belge est un amment comparér la performance dsibilité, la qualité,me de santé belgeifférents décideursmotion de la santé
sein de la popula
15
nt sur ecine s aux
sur la sous-nt de
ssible,
obale érents
ée à du e. Il s é.
tion à

16
2 FORCDE SA
2.1 Commeprésen
Les résultats synoptiques ci-est consacré à Ces tableaux sy• Un pictogr
indicateur. niveau natinternationasocio-éconpossible qu
• Dans la Belgique(benchmarcouleur.
• La colonnerésultats sdécideurs sur la baséchéant la
• L'évolutionprésentée l'importanc
• Les dernièrésultats p
b EU-15 fait
décembreEspagne, Portugal,
ES ET FAIANTÉ EN B
ent interpréter tant les résultades 74 indicatedessous, par domla promotion de laynoptiques contieamme illustre l'év
Cette évaluatiotional, par rappoaux ; l’évolution d
nomiques. Notonue pour certains incolonne « Belgiquest comparée
rking international
e suivante contienont disponibles. politiques, notam
se de données ocollecte d'informa générale au couensuite (augmen
ce es changementères colonnes par sous-groupes
t référence aux 15
e 2003, à savoir: Finlande, France,
Royaume-Uni et Su
BLESSESBELGIQUE
les tableaux syats ? eurs sont présemaine et/ou dimena santé.
ennent les informavaluation globale n résume diversort à d’éventuelsdans le temps ; lesns que cette éndicateurs. ue », la valeur
aux résultats l) et représentée
nt l'année la plus Cette informationment pour éviter bsolètes, ainsi qations plus récentrs des 5 dernière
ntation, diminutionts n'est pas illustréprésentent, quan: sexe, statut soc
États membres deAllemagne, Autri
Grèce, Irlande, Itauède.
Belgian
DU SYSTÈ
ynoptiques
ntés dans les tnsion. Un chapitre
ations suivantes : des résultats de
s critères : la vas objectifs nations disparités région
évaluation global
de l'indicateur des pays de au moyen d'un
récente pour laqn est importante de prendre des due pour favorisees.
es années disponn ou stabilité). Toée.
nd c’est possiblecio-économique (f
e l'Union européeniche, Belgique, Da
alie, Luxembourg, P
n Health System
ÈME
tableaux e distinct
chaque aleur au naux ou nales ou le n’est
pour la l'EU15b
code de
uelle les pour les
décisions r le cas
ibles est outefois,
e, des faible ou
ne au 31 anemark,
Pays-Bas,
•
SC(tol'PinS“
c
Performance
élevé)c et régpar sous-groul'ampleur desrégionale, il cRégion de Brud'une granderégions du paet ruraux.
Enfin, les dodoivent être m
Source des donnCe rapport utilise atelles que les bas
ou les enquêtes réÉchantillon perma
Pharmanet), le Renfections nosocomSurvey - HIS), les Direction générale
Selon la sou
par le niveadépenses de
gion (Wallonie, Flaupes, des couleurss différences. Poconvient de teniruxelles-Capitale. Ce agglomération ays se composen
omaines dans lemenées sont indiq
nées autant que possib
ses de données adécurrentes) : le Réanent (EPS), les b
egistre belge du Cmiales, l'enquête détudes de vaccine Statistique et In
rce des données, au d'études, soit p santé.
andre et Bruxelless aident le lecteurour ce qui concr compte du contCette région se courbaine, tandis t d'environnemen
esquels des étuués au moyen du
ble les données didministratives, lesésumé hospitalier bases de données
Cancer, les donnéede santé par interation et la base dformation économ
le statut socio-éconpar le droit au rem
KCE Report
s). Dans ces anar à mieux appréhecerne la compartexte spécifique ompose exclusiveque les deux a
nts urbains, subur
udes complémenu symbole .
sponibles en routs registres nationar minimal (RHM), s de l'INAMI (doc es de surveillancerview (Health Intere données de la
mique” (DGSIE).
nomique est mesurmboursement major
t 196
alyses ender raison de la
ement autres rbains
taires
tine aux
N, e des rview
ré soit ré des

KCE Report 196
Légende des t
Évaluation glob
Résumau
Résu
Résu
Bons
Très(tousrenc
Des comnéce
§ Les quintiles so£ Groupe de réféobtenu les meillegroupe socio-écodans le groupe so
6
ableaux synopti
bale
ultats trèvais
ultats mauvais
ultats moyens
s résultats
s bons résultats les critères son
contrés)
données/étudeplémentaires son
essaires
ont calculés sur la bérence : le statut soceurs résultats. Exemonomique élevé OUocio-économique él
ques
Comparaiso(EU-15) La Belgiqueles pays ob
s Les moins b
Des résultamoyenne
Des résulta
Des résultamoyenne
s nt
Les meilleu
s nt
base des résultats dcio-économique le p
mples fictifs : Deux foU moitié moins bons
levé.
Belgian
on internationale
e se situe§ parmibtenant :
bons résultats
ats inférieurs à la
ats moyens
ats supérieurs à la
urs résultats
de tous les pays. plus élevé, le genre ois plus mauvais : 2: 13% d'alimentatio
n Health System
i
Risques rela
Très grandemauvais ouréférence£
a Grandes diffmoins bons
Différences ou moins bo
a Différences bons de 20%
Paramètre n
Données no
(femmes/hommes)20% de fumeurs danon équilibrée dans le
Performance
atifs en fonction d
es différences entru moitié moins b
férences entre les
moyennes entre ons
ténues ou nulles % au maximum
non pertinent pour
on disponibles
) affichant les meillens le groupe socio-ée groupe socio-écon
u genre, du statut
re les groupes : leons dans le gro
s groupes : les ré
les groupes : les
entre les groupes
r cet indicateur
eurs résultats, la régéconomique faible pnomique faible par r
t socio-économiqu
es résultats sont aupe comparé qu
ésultats sont au m
résultats sont de
s : les résultats so
gion (Wallonie, Flanpar rapport à 10% drapport à 26% d'alim
ue et de la région
au moins deux foisue dans le group
moins 50% meilleu
e 20% à 50% mei
ont meilleurs ou m
ndre, Bruxelles) ayande fumeurs dans le mentation équilibrée
17
s plus pe de
urs ou
lleurs
moins
nt
e

18
2.2 État deQuatre indicaterésultats globala promotion dsanté. Pour ces quatrtemps (Tableamoyenne EU-1santé (définie fonctionnelle à
Tableau 1 – Ind
Indicateur
Espérance de v
Espérance de sannées)
Etat de santé p(% en bonne ou
Taux de mortal(nombre de dnés vivants) i L'espérance de ii La comparaisoniii Le code couleuautres indicateurs
e santé eurs généraux de aux et très distauxe la santé, à cô
re indicateurs, onu 1). L’espéranc5 (de 0,7 années
comme le nopartir d'un âge
dicateurs généra
vie (en années)
santé (à 25 ans, e
erçu u très bonne santé
ité infantile écès/1000 enfan
vie par statut socion internationale est bur utilisé pour les diffrs), mais sur l'ample
l'état de santé onx de l'efficacité duté de tous les a
n observe une éce de vie et légès). La mortalité inmbre d'années donné) se situen
aux de l'état de s
Global B
80
en 4
é) 76
nts 3.
o-économique est pbasée sur l'espéran
fférences sociodémoeur des différences a
Belgian
nt été choisis comu système de sanutres déterminan
volution positive èrement inférieurnfantile et l'espérde vie sans l
nt dans la moyen
santé
Belgique Dernièannée dispon
0.0 2010
1.0 ii 2008
6.8 2008
.5 2010
présentée ici à l’âgence de santé à la naographiques en termabsolues : jaune = 1
n Health System
mme des nté et de nts de la
dans le re à la rance de imitation nne des
résEOl’vamsm
ère
nible
Évolution
augmentat
augmentat
augmentat
diminution
e 25 ans. aissance. mes d'espérance de1 à 2 ans de différen
Performance
ésultats de l’EU-santé comme assEU-15. On observe de graespérance de vie
vivent plus longteavec des limitationmoins bonne. Tosocio-économiquemeilleurs en Fland
M F
tion 77.4 82.6
tion 41.3 41.2
tion 79.5 74.3
n 4.2 3.4
e vie et d'espérancence, orange = 2 à 6
15. Le pourcentasez bonne (ou trè
andes différencese, mais pas pomps que les homns fonctionnelles,us les paramètre
es plus faibles. Edre, hormis pour la
Socio faible
Socioélevé
M: 47.6i F: 54.0
M: 55F: 59
M: 27.7 F: 28.9
M: 46F: 47
57.4 85.7
e de santé n'est pas6 ans de différence,
age de personneès bonne) est su
s entre les femmeur l'espérance de
mmes, mais viven et elles considères sont moins bon termes de régioa mortalité infantil
o é
Flandre
5.0 .9
80.9
6.3 .1
M: 43.7 F: 42.3
78.6
4.0
s basé sur le risque rouge = plus de 6 a
KCE Report
s qui considèrenupérieur à la moy
es et les hommese santé : Les femnt davantage d'anrent leur santé coons pour les groons, les résultatse.
Wallonie Brux
78.5 80.0
M:37.4 F:39.1
M:38F:40
73.7 74.3
3.1 4.6
relatif (comme pourans de différence.
t 196
t leur yenne
s pour mmes nnées omme oupes s sont
xelles
8.5 .6
r les

KCE Report 196
2.3 AccessL'accessibilité peuvent avoir physique (répadisponibilité depréalable à la qTreize des sepde santé. Ils saccessibilité finaux soins de lode vie.
Disponibilité dDes efforts conpersonnel soignpreuve l'ajout dpas de résultaindicateurs ne est suffisant po
Accessibilité fMalgré la couvmultiples filets Spécial de Solidifférer certainsmédicaments, lfinancières. Ce 90. Par ailleurssanté en Belgmoyenne EU-15
6
sibilité est définie commrecours aux pr
artition géographie personnel qua
qualité et à l'efficietante-quatre indicsont regroupés p
nancière, couvertuongue durée et m
des soignants : mnsidérables ont étnant en Belgique de ces deux indicats complets dansuffisent pas à ur répondre aux b
financière verture par l'assude sécurité socidarité), 14% des s soins de santé lunettes/lentilles, pourcentage est , la contribution d
gique se monte 5, qui est de 15%
me la facilité avrestations de saique), de coût, dalifié.4 L'accessib
ence d'un systèmecateurs évaluent lpar thèmes : disure des mesures
moment de début
médecins et infirmté consentis pour (médecins et infi
cateurs, pour lesqns le précédent déterminer si l'ef
besoins de la pop
urance santé univaux (maximum àménages déclare(soins médicaux,soins de santé men augmentation
des patients à l'enà 19%, soit se
%.
Belgian
vec laquelle les nté, en termes de temps d’accèbilité est une ce de santé. l'accessibilité du ponibilité des sopréventives, accedes soins palliati
mières en activitquantifier les effe
rmières en activitquels nous ne disrapport. Cependaffectif soignant disulation.
verselle et l'existeà facturer, Omnioent avoir été contr intervention chiru
mentale) pour desn depuis la fin desnsemble des dépeensiblement plus
n Health System
patients d'accès
ès et de condition
système oignants, essibilité fs en fin
té ectifs du té). Pour sposions ant, ces sponible
ence de o, Fonds raints de urgicale,
s raisons s années enses de
que la
CLmLdadqdpmcnLpqEdleLe
Performance
Couverture des mLa Belgique peut mesures préventivLa couverture du deçà de la moyenans, malgré l’existdu sein. D’autre paqui peut susciter dépistage. La couprésente peu de moyenne EU-15, communément acnotable de cette coLa couverture duprésentée, car le que très récemmeEn termes de vacde l'OMS (75%) nentement. La Belgique obtienenfants.
mesures préventcertainement fai
ves. dépistage du ca
ne EU-15 (68.3%tence d'un prograart, les différencedes questions q
verture du dépistdisparités régionmais restent médcepté en Europe.ouverture.
u dépistage du cprogramme de la
ent. ccination contre la'est pas atteint et
nt en revanche de
tives ire mieux en term
ancer du sein (60). Ce pourcentage
amme organisé des entre les régionquant à l'efficientage du cancer duales. Les résultadiocres par rappo. On n’observe pa
cancer du côlon a Communauté fr
a grippe des perscette couverture
e bons résultats p
me de couverture
0%) est nettemee reste stable depe dépistage du ca
ns sont marquantece du programmu col de l'utérus (
ats sont proches ort à l'objectif de as non plus d’évo
ne peut encorerançaise n'a été
onnes âgées, l'obne progresse que
pour la vaccinatio
19
e des
nt en puis 5 ancer es, ce
me de (62%) de la 80%, lution
e être lancé
bjectif e très
n des

20
Accessibilité dLe nombre de évolué au coursâgées de 65 anélevé en WallonLes soignants les personnes (ACVQ) pendamaillon importapopulation âgéinformels varie 12,1% est lég(11,7%). Ce rémode de vie, spécifiques d'enAucune donnédisponible, cel'accessibilité de
Moment de déLe début des sretrouve en phproblèmes de tardive d'y avodans la semainleur mutuelle, cutile d’obtenir ptemps, différenc
des soins de longlits dans les éta
s de la dernière dns ou plus. Dans nie et à Bruxelles informels, qui sonâgées dans leurs
ant au moins unant des soins deée de 50 ans et
de 8% en Suèdèrement supérie
ésultat doit toutedes valeurs so
ncouragement à re relative aux b
es deux indicatees soins à long te
but des soins paoins palliatifs est ase terminale. Cdisponibilité des
oir recours. Dans ne de la demandece qui semble inplus de données ces régionales).
gue durée blissements de s
décennie, avec 70l'ensemble, ce noqu'en Flandre.
nt définis commes activités couranne heure par see longue durée.5
plus et faisant de à 16,2% en Itur à la moyennfois être contextociétales et de rester à la maisonesoins des patieeurs restent ins
erme.
alliatifs parfois différé jus
Ce délai peut êtresoins palliatifs, 20% des cas, le
e du forfait pour ndiquer une décis
sur cet indicateu
Belgian
soins résidentiels 0 lits par 1.000 peombre est nettem
'les personnes antes de la vie quoemaine', représen
5 Le pourcentagpartie de ces so
talie. Le chiffre bne des pays de ualisé, car il dépl'existence de m
n. ents n'étant actuesuffisants pour
squ’à ce que le pae la conséquence
soit d'une décises patients sont dsoins palliatifs au
sion trop tardive. ur (évolution au c
n Health System
n'a pas ersonnes ment plus
assistant otidienne ntent un e de la oignants belge de
l'OCDE pend du mesures
ellement évaluer
atient se e soit de sion trop décédés uprès de
Il serait cours du
Performance
KCE Reportt 196

Forc
eA
cces
sibi
lité
Cou
vert
ure
des
mes
ures
Soin
sde
Tise
KCE Report 196
Tableau 2 – Ind
Indicateu
Forc
e de
tr
avai
l Densité (p- médecin- infirmière
Acc
essi
bilit
é fin
anci
ère
Couvertursanté (%)Tickets patients(% des déReport depour raiso
Cou
vert
ure
des
mes
ures
pr
éven
tives
Dépistage- Sein (% - Col de l'64 ans) Couvertur- % DTP-H
- % ROR
Couvertur65 ans et
Soin
s de
lo
ngue
du
rée
Densité dsoins (pa65 ans) Soignantsde plus de
ming des soins emaine de soins p
6
dicateurs évalua
ur
par 1.000 habitantns en activité es en activité re de la populat) modérateurs et
épenses totales dee contacts avec leons financières (%e du cancer des femmes âgéeutérus (% des fem
re vaccinale infanHib (3)
(1)
re vaccinale contplus)
de lits en maisonr 1.000 personne
s informels (% dee 50 ans) palliatifs : décès
palliatifs (%)
ant l'accessibilité
ts) de :
tion par l'assuran
t contribution d
e santé) es services de sa
%)
es de 50 à 69 ansmmes âgées de 2
tile
tre la grippe (% d
ns de repos et es âgées de plus
e la population âg
s durant la premi
Belgian
é aux soins de sa
Global Begi
2.
9.nce 99
des 19
anté 14
s)
6025 à 61
97
94
des 65
de de
70
gée 12
ère (2
n Health System
anté
el-ique
Dernièreannée disponible
9 2010
9i 2009 9.0 2010
9.4 2010
4 2008
0.1 2010
1.8 2010
7.9 2009
4.5 2009
5.0ii 2009
0.3 iii 2011
2.1 2007
20.0) iv 2006
Performance
e
b
Évolution
M
stable
stable
stable
augmen-tation
stable
stable
augmen-tation
augmen-tation
augmen-tation
stable
M F Socio faible
Soél
27.0 4.
48.6 62
48.9 64
63.5 46
ocio evé
Flandre
0 11.0
2.9 64.9
4.2 61.0
98.3
96.8
6.3 65.8
58
Wallonie Br
14.0 26
55.3
51
64.6 63
96.9
98
92.4 91
60.9 59
83 10
21
ruxelles
6.0
1.9 3.6
8.6
1.1
9.2
01

22
i Les données deii Valeurs nationaiii Valeurs et compiv Données natioDTP-Hib (3) DiphROR (1) Rougeo
2.4 QualitéLa qualité est daux individus eeffets souhaitéconnaissances.dimensions : l'ela centralité du 2.4.1 EfficaL'efficacité est souhaités sont mais à l'exclusindicateurs d'effSept indicateursanté : le tauxcolorectal, le taindicateurs de habitants (ce qpopulation), le tmentale par rahandicaps (telsd'hospitalisationà l'ensemble de
e l'OCDE relatives aales basées sur la Hparaison internation
onales indisponibleshtérie-Tétanos-Coquole-Oreillons-Rubéol
é des soins définie comme 'laet aux populationés sur la sant.'6 La qualité deefficacité, l'adéquapatient. cité
définie comme atteints, pour toutsion de celles qfficacité sont doncrs ont été chois
x de survie aprèsaux d'hospitalisati
santé mentale qui est égalementaux d'emploi de apport au taux ds que musculo-sns psychiatriqueses hospitalisations
aux effectifs des infiHIS, disparités socionale basées sur dess. Valeur basée sur ueluche-Haemophille (première dose).
a capacité des ses d’augmenter laté, conformémenes soins est suation, la sécurité,
'la mesure selotes les personnesqui n'en tireraienc des indicateurs dis pour évaluer s cancer du seinon pour asthme, : le nombre de
nt un indicateur personnes souffr
d'emploi de perssquelettiques), ais non volontaires s psychiatriques.
Belgian
irmières ne sont paso-économiques basés données de 2010.une seule étude delus Influenzae B (tau
ervices de santé da probabilité d’obnt à l'état actu
ubdivisée en cinla continuité des
on laquelle les rs qui pourraient ennt aucun avantagde résultats. l'efficacité des sn, du col de l'utainsi que trois no
e suicides par de l'état de sant
rant d'un trouble donnes souffrant insi que le pour(colocations) par
n Health System
s comparables entreées sur l'EPS. s Mutualités Chrétieux de couverture po
destinés tenir les uel des q sous-soins et
résultats n profiter ge'. Les
soins de térus ou ouveaux 100.000 té de la de santé d'autres
rcentage r rapport
LaeLpePtaepl’inspplaqpimcré
Performance
e pays.
ennes. our la troisième dos
La survie après unaux autres pays encore disponible Les taux hospitaliprestations ambulaen terme d’efficaciPour les indicateuaux de suicide européens. Toutepersonnels et socefficacité des sondiquent qu'une suicide en Belgipersonnes souffrapersonnes atteintea nécessité de réqu’au cours des psychiatriques nomportant constatéces disparités poégional).
e) ;
n cancer du sein européens. L’évà ce jour. isations pour cauatoires – sont légité) que la moyen
urs d'efficacité en extrêmement é
fois, le taux de ciétaux, et n’est doins de santé me
action concertéeque. Le deuxièm
ant de troubles mes d'autres handicécolter d’autres d
dernières annéon volontaires (cé à Bruxelles doitourraient être lié
et du colon est bvolution des taux
use d'asthme – rgèrement plus élene EU-15. soins de santé m
élevé par rapposuicide dépend é
donc qu’un qu'unentale. Quoi qu'il e est requise pome indicateur, l
mentaux comparé caps, est difficile données. Le dernées, le pourcentcolocations) a at s’interpréter aveées à un phéno
KCE Report
bonne, en comparx de survie n’est
eflétant un échecevés (donc moins
mentale, on observort aux autres également de fac
n indicateur indireen soit, les rés
ur réduire le taue taux d’emploiaux taux d’empl
à interpréter et mnier indicateur mtage d'hospitalisaugmenté. Le % ec prudence (en omène urbain et
t 196
raison t pas
c des bons
ve un pays
cteurs ect de sultats ux de des loi de
montre montre ations
plus effet,
t non

KCE Report 196
Tableau 3 – Ind
Indicateur
Soin
s cu
ratif
s
Taux de su- Cancer du
- Cancer du
- Cancer du
Hospitalisa(/100 000 s
Sant
é m
enta
le
Taux de su(nombre/10
Taux d'esouffrant d
Hospitalisa(colocationhospitalisat
i Résultats pour leii Dernières donnéiii Le résultat tiré div Dernières donnv Rapport entre levi Résultats tirés d
6
dicateurs évalua
r
urvie relative à 5 au sein
u col de l'utérus
u côlon
ations pour asthmesujets 15+)
uicide 00 000 personnes
mploi des pate troubles mentau
ations forns) (en % de toutetions psychiatriqu
e cancer colorectal ées disponibles poudes Données de Sa
nées disponibles poe taux d'emploi des de la dernière éditio
ant l'efficacité de
Global Bq
ans 8
6
MF
e 4
s) 1
tients uxv
0
rcées es les ues)
8
dans les Données ur la Belgique dans anté de l'OCDE, aveur la Belgique danspersonnes souffran
on de l'Enquête sur
Belgian
s soins
Belgi-que
Dernièannéedispoble
88.0 2008 i
69.8 2008 i
M: 62.3 iF: 64.6
2008 i
48.4iii 2009 i
18.6 2008iv
0.7 2002vi
8 2009
de Santé de l'OCDEles Données de Sa
ec ajustement en fos les Données de Sant de troubles mentales Forces de Trava
n Health System
ère e ni-
Évolution
i
i i
i stable
v stable
Augmen-tation
E pour la Belgique ;anté de l'OCDE: 200nction de l'âge. Le tanté de l'OCDE : 20aux et celui de persail de l'Union Europ
Performance
n M F
62.3 64.6
28 52
28 10
; 04 (cette année a setaux belge non ajus005 (cette année a ssonnes atteintes d'apéenne.
Socio faible
Socioélevé
ervi de base à la costé est de 40/100 00servi de base à la cutres handicaps.
o Flandre W
87.6 8
70.6 6
M: 62.5 F: 64.5
MF
17 2
8 7
omparaison internati00 ; omparaison interna
Wallonie Brux
88.8 88.0
69.1 67.7
M: 62.5 F: 64.9
M: 59F: 64
24 14
7 14
ionale) ;
ationale) ;
23
xelles
9.9 .3

24
2.4.2 AdéquL'adéquation pesoins de santé des meilleures La relation entrles résultats et Huit indicateursgénéral, leurs rqui concerne lepopulation cibleles antibiotiquesLa proportion caractérise par Deux indicateud'antipsychotiquque cette consaugmentation.Enfin, un indicaa été utilisé (l’cancéreux), maréférence, com
uation eut être définie cdispensés sont apreuves disponibre l'efficacité et l'ales processus de s ont été choisis résultats sont plute dépistage non e) ou le respect des ou le suivi des pde naissances pune grande varia
urs portent sur ues par l'ensembsommation, déjà
ateur de l’agressivutilisation des ch
ais ses résultats sparaison à d’autre
comme étant 'la mdaptés aux besoiles'. adéquation est le soins. pour mesurer l'a
tôt mauvais, plusapproprié du ca
es guides de bonpatients diabétiqupar césarienne eabilité entre hôpita
la consommatioble de la populatsupérieure à la
vité des soins auxhimiothérapies ensont difficiles à ines pays, ou évolut
Belgian
mesure selon laquns cliniques, com
reflet de la relatio
adéquation des so particulièrement ncer du sein (hone pratique cliniqes).
est en progressioaux. on d'antidépresstion. Tous deux moyenne EU-15
x personnes en fin fin de vie des nterpréter sans notion au cours du t
n Health System
uelle les pte tenu
on entre
oins. En pour ce
ors de la ue (pour
on et se
seurs et révèlent , est en
n de vie patients
orme de temps.
Performance KCE Reportt 196

KCE Report 196
Tableau 4 – Ind
Indicateur
Mammographiegroupe cible (%- Femmes âgée
- Femmes âgée
Antibiotiques comparée à l‘aou associéeclavulanique.)
Suivi correct diabétiques (%)
Césariennes (naissances viva
Prescription journalière personnes)
- Antidépr
- Antipsyc
Patients souffrbénéficiant dedurant les 14 dleur vie (%) i Des patients déc*Patients diabétiq
6
dicateurs de l'ad
es en dehors du %) es de 40-49 ans
es de 71-79 ans
(% amoxicilline moxicilline seule
es à l‘acide
des patients )*
(par millier de antes)
de (quantité moyenne/1 000
resseurs
chotiques
rant du cancer chimiothérapie
derniers jours de
cédés à leur domiciques adultes se sou
déquation des so
Global Belgiq
35.5
20.8
44.9
54
193
68.4
10.5
(12%/23%)i
ile/à l'hôpital. Absenumettant régulièrem
Belgian
oins
que Dernière année disponible
2010
2010
2008
2008
2009
2010
2010
/ 2005
nce de données natment à des examens
n Health System
e
Évolution
stable
augmentation
stable
stable
augmentation
augmentation
augmentation
tionales. Valeurs tirés rétiniens et sangui
Performance
M F Sofa
28
16
46.4 51.1 44
54 55 48
43.1
92.8
10.8 10.3
ées d'une seule étuins (%)
ocio aible
Socio élevé
Fl
8.6 36.6 28
6.2 23.2 16
4.4 49.4 46
8 58 57
60
9.
de des Mutualités C
andre Wallonie
8.6 46.4
6.4 27.7
6.0 42.8
7 52
0.6 85.8
6 11.9
Chrétiennes.
e Bruxelles
47.7
31.2
47.1
48
57.1
11.7
25

26
2.4.3 SécurLa sécurité desystème ne porSix indicateursmoyens : l’expoavec un débu
Tableau 5 – Ind
Indicateur
Exposition de lradiations (MSv/capita)
Incidence du Mmillier d'admiss
Incidence dpostopératoire
Incidence despatients hospita
Mortalité intra-fracture de la ha
Prescription anticholinergiquprenant des antI OR Odds Ratio
rité s soins est définrte pas préjudice as évaluent la séosition aux radia
ut de diminution
dicateurs évalua
la population belgd’origine m
MRSA nosocomisions)
de la sept(/100 000 sorties)
s escarres chealisés (%)
-hospitalière aprèanche (%)
d’antidépreues (% des patientidépresseurs)
nie comme « la mau patient ». écurité des soinations médicales
en 2011), régr
ant la sécurité de
Global
ge aux édicale
al (par
ticémie )
ez les
ès une
esseurs nts 65+
Belgian
mesure selon laq
ns. Leurs résultareste trop élevé
ression importan
es soins
Belgique Deranndis
2.2 201
1.5 201
1224 200
16.8 200
6.3 200
14 201
n Health System
quelle le
ats sont ée (mais tes des
inmdpSa
rnière née ponible
Évolut
1 modesdiminut2011
0 diminut
07 stable
07 augme
07 diminut
0 stable
Performance
nfections nosocomméticilline) ; diminde la hanche ; et iprescription d’antiSeule l'incidence augmentation.
tion M F
te tion en
tion
entation
tion 1.84i
13 1
miales au MRSAution de la mortaincidence stable ddépresseurs antides escarres c
F Socio faible
Socéle
14
A (Staphylococcusalité intra-hospitalide la septicémie pcholinergiques auchez les patients
cio vé
Flandre
1.2
17
KCE Report
s aureus résistanère après une frapostopératoire et ux patients plus s hospitalisés es
Wallonie Brux
2.2 1
11 10
t 196
t à la acture de la âgés. st en
xelles

KCE Report 196
2.4.5 ContinLe concept de que la continuicontacts, l'aspecoordination enindicateurs pedimensions, cerapport précédeContrairement asur l'efficacité d’autres pays indicateurs sondossier médiconcologie (COMscientifique, teProvider of Carle mesurer. Un seul résultasupposer d’unehabituel. Des « contact avechospitalisation »observés en réadmissions efaire l'objet dspécifiquement
d L'indice U
proportionhabituel. Lmédecin gl'indice UPtrois quarhabituel.
6
nuité des soins continuité des soté de l'informatio
ect relationnel desntre les soignantsrmet de tirer d
e qui représente ent sur la performaux indicateurs codes soins, on peen matière de ct spécifiques à nocal global ou M). D'autres indicals que l'indice Ure)d, mais rares s
at, l'indice UPC, pee bonne qualité résultats moyen
c le médecin g» et « 'tenue d’utermes d'utilisat
en hôpital psychiad'une collecte dt la santé mentale
UPC (prestataire de n des contacts d'un Lorsque l'indice estgénéraliste. L'indicaPC est égal ou surts des contacts s
oins recouvre diffén entre les soigns contacts patients et les organisatdes conclusions une avancée sig
mance. ommunément utilieut difficilement coordination des otre système de s
la consultatioateurs sont bien
UPC (prestataire ont les pays disp
eut être considérérelationnelle ave
s sont enregistrgénéraliste endéaune COM ». Destion du dossier atrique. Ce derniede données par.
soins habituel – Uspatient qui a lieu avt de '1', le patient aateur exprime le popérieur à 0,75, c'ese sont faits avec
Belgian
érentes dimensionnants, la planificat/généraliste, ainstions. Le set actupour chacune
gnificative par rap
isés sur l'état de scomparer la Besoins. En effet,
soins de santé, teln multidisciplinadécrits dans la litde soins habituosant des donné
é comme positif, ec son médecinés dans les indans les 7 jourss résultats négat
médical globaler indicateur est lr l'OCDE ; il c
sual Provider of Cavec son médecin géa toujours consulté ourcentage de patieest-à-dire dont au mc leur médecin gé
n Health System
ns, telles ation des si que la uel de 7 de ces
pport au
santé ou lgique à certains ls que le aire en ttérature el-Usual
ées pour
et laisse traitant
dicateurs s après tifs sont et de e seul à
concerne
are) est la énéraliste le même
ents dont moins les énéraliste
Performance 27

28
Table 6 – Indic
Indicateur
Patients dispmédical global
Patients diagcancer et consultation multidisciplinair
Contact avec ldans la semal’hôpital (% des
Proportion demédecin géné(Indice UPC iii)
Réadmission dpsychiatrique, dsortie (%) - diagnostic de
- diagnostic de
Patients ayancontact avec ledurant leur der(%) i: Données belgesii 72% des persontirés d'une seule iii L'indice UPC (Ucontact avec le m3 contacts sur 4 a
cateurs évaluant
osant d'un do(%)
gnostiqués avecbénéficiant
oncolore (COM) (%)
e médecin généraine de la sortis sujets 65+)
e contacts avéraliste habituel
dans le même hdans les 30 jours
schizophrénie
trouble bipolaire
t eu au moinur médecin générrnière semaine d
s les plus récentes.nnes décédées à leétude des Mutualité
Usual Provider of Camême médecin généavec leur médecin g
la continuité et d
Global
ossier
c un d’une
ogique
raliste ie de
vec le (%)
hôpital de la
s un raliste de vie
Les données de l'Our domicile ont eu ués Chrétiennes) ; are) est la proportioéraliste. L'indicateurgénéraliste habituel)
Belgian
de la coordinatio
Belgique Dernannédisp
47 2010
68.8 2008
58.4 2009
71.4 2010
20.2
2009
15.6 2009
(72%) ii 2005
OCDE les plus réceun contact avec leur
on des contacts avecr utilisé présente le l).
n Health System
on des soins
nière ée onible
Évolutio
0 augmen
8 augmen
9 stable
0 stable
9i
augmen
9 i stable
5
entes pour la Belgiqur médecin généralis
c le médecin générapourcentage de pa
Performance
on M F
tation 42 50
tation
55.4 60
72.1 71
tation
ue datent de 2007 ;ste durant leur derni
raliste habituel d'un ptients dont l'indice U
Socio faible
Soéle
0 54 44
0.8 64.2 54.
.2 76.7 70.
; ière semaine de vie
patient. L'indice '1' iUPC est au moins d
cio evé
Flandre
58
73.8
6 60.6
5 70.8
25.2
19.7
e (données nationale
indique que le patiede 0,75 (ce qui signi
KCE Report
Wallonie Brux
32 29
62.7 55.7
57.8 42.5
74.4 65.9
17.2
10.2
13.4 7.1
es indisponibles, ch
ent a toujours été enifie qu'ils ont eu au
t 196
xelles
hiffres
n moins

KCE Report 196
2.4.6 CentraLa centralité duprestation de sodu patient ». Lcentralité du paa été entreprisprésentés. Ce données. En odes information
Tableau 7 – Ind
Indicateur
Satisfaction qusoins de san'satisfaits' ou 'tr
Douleur toujol'hospitalisation
Personnes déchabituel (% de i Données nationii Le degré de satsatisfaction n'est iii Résultats tirés div Fondé sur une
6
ralité du patient u patient est défioins respecte les
Le rapport précédatient. Une rechercse, à l'issue defaible nombre d'
outre, les rares inns parcellaires sur
dicateurs évalua
uant aux servicenté (% de parès satisfaits')
urs maîtrisée d (% de patients)
cédant à leur dopersonnes décéd
ales pas encore distisfaction est supérielégèrement inférieu
d'une seule étude, détude des Mutualité
inie comme « la besoins, valeurs e
dent ne contenaiche approfondie d
e laquelle trois i'indicateurs reflètndicateurs mesurar un sujet complex
ant de la centralit
Global
es de atients
durant
omicile ées)
sponibles. Les résuleur à 90% pour les ur (87%) que pour ledans le cadre du proés Chrétiennes et su
Belgian
mesure selon laqet préférences indt aucun indicateude données et indindicateurs peuvete une réelle careables ne fournissxe.
té du patient dan
Belgique Dad
>90% ii 2
(41.0) iii 2
(45.1)i 2
ltats pour la Flandrecontacts avec les mes hôpitaux, rojet RN4cast ; ur d'autres publicati
n Health System
quelle la dividuels ur de la dicateurs ent être ence en sent que
LdUqpdLnsé
ns le système de
Dernière année disponible
Évo
2008
2009
2007 augm
e et Bruxelles sont gmédecins généralist
ions.
Performance
Les résultats attesdifférents servicesUne seule étude question centrale performances de d'autres pays. L'indicateur relatifnombre de paties'assortit toutefois économique.
santé
olution M
Aucudiffér
mentation
groupés ; tes, les dentistes, le
stent d'une satisfas de soins de sant
a été en mesuqu'est la maîtrisela Belgique so
f à l'endroit du dents qui décèden
de différences co
F Socio faible
SH
ne rence
Aucune différence
iv
es spécialistes et les
action générale dté. ure de fournir dee de la douleur, ént relativement
décès révèle unent à l'hôpital esonsidérables en fo
Socio High
Flandre
Plus élevée
45.1i
s services de soins
des patients quan
es informations sétude dans laquelfaibles par rapp
évolution positivst en diminution)onction du statut s
Wallonie Brux
Plus faible
La faible
45.1
à domicile. Le degr
29
nt aux
sur la le les
port à
ve (le ), qui socio-
xelles
plus e
i
ré de

30
2.5 EfficienL'efficience est correcte de rl’ « input ») est que ces ressobénéfice ou lesTrois indicateursanté. À l'instarune utilisation confirmée par prescription deinterventions chséjour en hôpit
Tableau 8 – Ind
Indicateur
Proportion de c
Durée d'hospitun accoucheme
Prescription dmarché » (% dtotal, en ambula
Autres indicatesection « Adéqu
DDD = dose quo
nce du systèmedéfinie comme é
ressources (budginvestie dans le urces sont utilisé meilleurs résultatrs ont été retenur des autres pays plus efficiente del'évolution des tr
e médicaments «hirurgicales de jotal après un acc
dicateurs de l'eff
chirurgie de jour (%
talisation moyennent normal (en jou
de médicamentsde DDD par rapatoire)
eurs analysés uation des soins »
tidienne déterminée
e de santé étant 'la mesure sgets, temps et système (au niveées de manière ts possibles (l’«ous pour évaluer l'eeuropéens, la ten
es services de sorois indicateurs :« bon marché »,
our, ainsi que la rcouchement norm
ficience des soin
Globa
%) ne après urs)
s « bon pport au
dans la »
e (Defined Daily Dos
Belgian
selon laquelle la personnel, nota
eau macro), en s’aà en tirer le plu
utput»).'4, 7 efficience du systndance en Belgiqoins. Cette tendaune augmentatioune augmentat
réduction de la dmal (qui est un in
ns
al Belgique Dad
46.2 2
4.3 2
46.0 2
se)
n Health System
quantité amment, assurant
us grand
tème de que est à ance est on de la tion des durée du ndicateur
pdDinnnrélapvsl'c
Dernière année disponible
Évo
2008 aug
2008 dim
2010 aug
Performance
plus comparable dernière reste touD'autres indicateundications quant nombre de patiennature à réduire évèlent toutefois a moitié des déprogramme nationvariabilité inexpliqsigne de manquefficience. C'est l
césariennes.
olution M
mentation
inution
mentation
entre pays que lutefois supérieure urs analysés dans
à l'efficience dnts disposant d'ule nombre d'examdes tendances mpistages du cannal suscite des qquée des prestatiue d'adéquation, le cas par exemp
F Socio faible
Soél
la durée d'hospità la moyenne EU
s ce rapport fourndu système. Ainn dossier médicamens redondants
moins positives. Lencer du sein s'efquestions quant ions de soins pe
une dimensionple pour la grande
ocio evé
Flandre
46.2
KCE Report
alisation totale). U-15. nissent égalemensi, l'augmentatioal global peut êtrs. D'autres indicae fait par exempleffectue en dehorà son efficience.
eut également êtrn directement liée variabilité du tau
Wallonie Brux
45.9 45.3
t 196
Cette
nt des on du re de ateurs e que rs du Une re un ée à ux de
xelles

KCE Report 196
2.6 PérennLa pérennité (système à: • Offrir et m
exemple pl'équipeme
• Être innova• Répondre a• Rester finaDes indicateuréléments de ladépenses totalfinancière.
Tableau 9 – Ind
Indicateur
% de diplôgénéralistes Âge moyen desInfirmières diplô% des médecinmédical électroNombre de jouraigus (par habitProportion desproduit intérieuri Pour cette sérieii Cet indicateur diii Cet indicateur dPIB : produit intér
6
nité (ou durabilité) e
maintenir des inpar la formation ent ; ant ; aux besoins émer
ancé durablement rs spécifiques ona définition. Le des de santé) est
dicateurs de la p
més en méde
s médecins générômées (par 1 000ns généralistes utnique rnées d'hospitalistant)iii s dépenses de r brut (% du PIB)
e d'indicateurs, les ddoit être interprété cdoit être interprété crieur brut
st définie comm
frastructures comet l'enseignemen
rgents ; par des recettes
nt été choisis pdernier indicateurt un indicateur gé
pérennité du syst
ecine devenant
ralistes habitants)ii tilisant un dossier
ation en hôpitaux
santé dans le
données ne sont pasconjointement avec conjointement avec
Belgian
me étant la capa
mme du personnnt), des structure
collectives. pour chacun desr (% du PNB alloénérique de la p
tème de santé
Global Be
t 30.
51.41.
r 74.
x 1.2
e 10.
s disponibles par rél'indicateur de la de
c l'indicateur relatif a
n Health System
acité du
nel (par es et de
s quatre oué aux
pérennité
LladhminreEre2
lgique Deandis
1 20
4 207 200 20
2 20
5 20
égion, mais par langensité en infirmièresau pourcentage de c
Performance
Les résultats sont a cohorte de médde la retraite) et phôpitaux aigus pmédical électronndicateurs ne peelatives aux beso
En termes de poueprésentaient 10.
27,6 milliards en 2
ernière nnée sponible
Évolu
09 diminu
09 augme10 stable10 augme
09 stable
10 augme
gue (francophones os diplômées (dans lechirurgies de jour (d
parfois négatifs (decins généralisteparfois moyens (nar habitant ; utiliique par les
euvent pas être oins (infirmières dircentage du PIB, .5% en 2010. En
2003 et € 37.3 mill
ution Néerlai
ution 29.2
entation 51 e entation 83.7
e
entation
ou néerlandophonese chapitre consacrédans le chapitre con
(faible capacité dues qui vieillit et qunombre de journéisation encore inmédecins générinterprétés sans plômées). les dépenses totatermes absolus,
liards en 2010.
ndophones Fra
31
52 62
s) ; é à l'accessibilité) ;nsacré à l'efficience)
u système à rempui arrive bientôt à ées d'hospitalisationsuffisante du doralistes). Les adisposer de don
ales en soins de ce montant était
ancophonesi
.0
.5
).
31
placer l’âge
on en ossier autres nnées
santé t de €

32
2.7 PromotPour différentesdu présent rappromotion de la1. La promoti
conférer d'améliorerstratégiqueresponsabsoins de snombre dspécifique
2. La plupart promotion un travail adaptés au
3. Les donnée4. Les indicat
comportemvision rédudistaux, qud'autres favaleurs et politiques d
e Les cinq a - élaborer
santé d'int - créer des - développ - renforce - réoriente Les valeu
suivantes:multisecto
tion de la santés raisons, il n'a pa
pport un aperçu ca santé : on de la santé, daux patients dav
r leur santé', ees (définis dansilités situées ess
santé, et même a'indicateurs strucseraient nécessades indicateurs
de la santé ne sode développeme
u contexte belge/res disponibles soteurs convention
ments de santé, uctrice de la promui sont influencés acteurs. De nomb
d’un certain bede santé.
axes de la Charte d'r de politques publtégrer la santé danss environnements pper les aptitudes indr l'action communauer les services de sars et dimensions p: participation, auto
orialité.
é as été possible decomplet de la pe
définie comme 'le vantage de maîtest un concept s la Charte d'Osentiellement en au-delà du systèmcturés au sein ires. qui seraient néc
ont pas opérationent complémentairégional. nt rares. nnels de résultatsaisés à mesurer
motion de la santétant par la promo
breux autres indicnchmarking, son
'Ottawa sont les suiiques saines (il aps toutes les politiquepropices (cadres dedividuelles utaire anté rincipales de la pro
onomisation, équité,
Belgian
e présenter dans erformance en ter
processus qui cotrise sur leur sa
très large. SeOttawa) portent s
dehors du système de santée. U
d'un cadre con
cessaires pour évnnels. Certains reire, d'autres doiv
s liés à la santér mais représenté. Ce sont des rotion de la santé cateurs, assortis t requis pour pil
ivants: ppartient aux autorites) vie)
omotion de la santé, pérennité, multistr
n Health System
le cadre rmes de
onsiste à anté afin es axes sur des
ème des Un grand nceptuel
valuer la equièrent vent être
ou aux tent une résultats que par de leurs loter les
tés de la
é sont les ratégie et
EpfrPvrépeRinptandecstoaré«pLanpminpB
Performance
En conséquence, présentée dans leragmentaire, comPour la plupart devie, les chiffres naégionales et socia
propices à la santet au sein des catéRares sont les nternationale. Onprésente, en progabagisme reste néanmoins en régdisparités socialesest largement inféconsommation hesemble être en aoutefois être interau biais de désiraégionale pour l
« consommation pplus de « binge drLe taux de diagaugmentation depnette augmentatioprésentons pas demesure où les rénclure une propopertinent pour l'éBelgique.
la performance e présent rapport
mme illustré dans ls indicateurs clasationaux ont des ales sont observéé en Flandre (à l'égories socio-éco
indicateurs à n soulignera la pgression et caracttrop élevé (20%ression. Il se cara
s et régionales. Laérieure aux besoiebdomadaire d'alaugmentation. Le rprété avec prudeabilité sociale. Onl’indicateur, à l'problématique » (inking » chez les j
gnostic de l’infecpuis quelques anon parmi la populae comparaison inésultats obtenus ortion importantevaluation des po
en termes de pau moyen de 15
e Tableau 10. ssiques de statut d
valeurs intermédées, sous la formeexception de la c
onomiques plus élavoir fait l'objetroblématique de térisée par d'impo
% de fumeurs auactérise égalemena consommation dns quotidiens, mcool n'est pas tdegré de conso
ence, car il est pan observe peu deexception d'un tendance à l'assujeunes en Flandrection HIV en Bnées. Ce pource
ation homosexuelternationale pour pour la populatio
e de cas 'importéolitiques de prom
KCE Report
promotion de la 5 indicateurs n'es
de santé et de stydiaires Des dispe de modes de vieconsommation d'aevées. t d'une comparl'obésité, qui es
ortantes disparitéu quotidien) maint par de substantde fruits et de légais elle s'améliorrès élevée, mais
ommation d'alcoorticulièrement sene disparité sociataux plus élevé
uétude) à Bruxellee. elgique est en
entage est de plule masculine. Nocet indicateur, da
on non belge peés', ce qui n’est
motion de la sant
t 196
santé st que
yle de arités e plus alcool)
raison t très
és. Le s est tielles umes re. La s elle ol doit nsible ale ou é de es, et
lente us en us ne ans la uvent t pas té en

KCE Report 196
On observe audisparités sociaélevé parmi la pLa Belgique seScale (échelle les politiques consommation Les autres indpolitiques localede vie. Ils ne soCes données stendances obseamélioration détablissements bonne), et l'offdes politiques dœuvre dans de
6
ssi que le manquales et régionalespopulation âgée. e positionne dandes Politiques de
publiques de de tabac.
dicateurs sont dees de promotion dont disponibles qusont difficiles à inervées au gré d'éde la culture d
scolaires (la cfre d'activités phyde promotion de nombreuses com
ue de support socs. Ce niveau est
ns la moyenne de Lutte contre le T
différents pays
es indices visant de la santé menéeue pour la Flandrnterpréter sans aétudes successivede promotion dculture de particysiques est en ala santé ne sont
mmunes.
Belgian
cial montre d'impen outre nettem
dans la Tobacco Tabagisme), qui cs visant à réd
à mesurer l'impes dans différentsre (via les études analyse approfones semblent indiqde la santé dacipation est relatugmentation. Parpas idéalement m
n Health System
portantes ent plus
Control compare duire la
pact des s milieux VIGeZ). die. Les
quer une ans les tivement r contre, mises en
Performance 33

34
Tableau 10 – In
Indicateur
Adultes en surp
Adultes obèses
Dents cariées, l’âge de 12-14 a
Taux de diagpopulation belg
Fumeurs quotid
Consommation- Problématique
- Surconsomma
- Consommatio
Consommation200 g. de légum
Au moins 30 mpar jour (%)
Support social i
Échelle d’évalumesures anti-tScale)
Volume d'activit
ndicateurs de la
poids ou obèses (
s (%)
manquantes, obtans (moyenne)
nostic du VIH de (/100 000 hab)
diens (% 15+)
d'alcool (% 15+) ei
ationii
on ponctuelle imm
quotidienne minimes et 2 fruits (%)
inutes d'activité p
insuffisant (%)
uation de l’efficactabac (Tobacco
té physique à l'éc
promotion de la
Global
%)
turées à
dans la
odéréeiii
male de )
physique
cité des Control
cole
Belgian
santé
l Belgi- que
Deèreanndisnib
46.9 200
13.8 200
1.3 iv 201
3.9 201
20.5 200
10.2
200
7.9 200
8.1 200
26.0 200
38.1 200
15.5 200
50/100 201
200
n Health System
rnie née
spoble
Évolution
08 augmenta-tion
08 augmenta-tion
10
10 augmenta-tion
08 diminution
08 augmenta-tion
08 stable
08
08 augmenta-tion
08 stable
08
10
09 augmenta-
Performance
M F
53.7 40.4
13.1 14.4
6.9 0.7
23.6 17.7
13.1
7.3
10.1 5.9
12.8 3.7
23.4 28.5
48.7 28.3
15.1 16
Socio faible
Socioélevé
57.8 40
19.1 9.1
22.1 13.1
11.5
11
5.9 8.4
8.3 7.6
21.7 29.4
24.0 42.8
24.4 10.1
o
Flandre
47.1
13.6
3.8
18.6
9.5
7.9
8.9
30.0
45.1
12.4
5.5/10
KCE Report
Wallonie Brux
48.9 39.8
14.6 11.9
2.40 8.9
24 22.3
10.7
14.4
8.4 6.7
7 6.2
19.2 25.3
28.4 24.7
20.0 22.9
t 196
xelles
8
9
3
4
3
7
9

KCE Report 196
Politiques de dans les comm
% des établissd'une 'équipe sai: Calculé sur la b ii Femmes 15+ ; iii Consommation iv Certaines donnv Pour la Wallonievi Indicateurs tirés
6
promotion de launesVII
sements scolaireantéVII
base de la populatioHommes 22+ ; ponctuelle de nomb
nées sont disponiblee et Bruxelles ; s de VIGeZ, respec
a santé
es dotés
on des personnes co
breuses boissons aes, mais pour un nom
ctivement pour la pré
Belgian
200
200
onsommant de l'alco
alcoolisées (≥6 boismbre trop restreint d
évention du tabagis
n Health System
tion
09
09 augmenta-tion
ool (non abstinents)
ssons) au moins unede pays ;
sme, l'alimentation é
Performance
) et du cut-off CAGE
e fois par semaine ;
équilibrée et l'activité
E, 2+ ;
;
é physique (scores
37/36/50vi
42/64/54 vi
importés de VIGeZ)
40%v 40%
Z) ;
35
% v

36
2.8 Équité L'équité est unsystème de sajugement normd'approches etlittérature. Ellesintitulée « L'équsanté » (disponEn tenant compl'équité de dedocumenté les et de recours asocio-économiqEnsuite, nous donner un éclasanté (les résulL'équité en md'inégalités sysgroupes sociausociale ». En exclusivement (par exemple tableaux synopfiche détaillée drestreint la situniveau d'étuderemboursemenbases de donsociale, telles qn'ont pas été ét
et égalité n paramètre clé danté.1 C’est aussatif et et à une prt de définitions s sont présentéeuité dans l'évalua
nible sur notre sitepte de ce contexeux manières cinégalités en term
aux soins de sanque (les résultatavons proposé d
airage contextuel tats sont contenu
matière de santé tématiques dans
ux qui occupent dconséquence,
sur les inégalités en fonction du sptiques de chaqude chaque indicateuation socio-écones (pour les indt majoré (bénéficnées administrat
que le statut profetudiées dans ce ra
dans l'évaluation si une question rise de position pode l'équité ont
es dans l'Annexeation de la perfore Internet). xte, nous avons acomplémentaires.mes de santé, de té en Belgique ets sont contenusdes indicateurs gaux questions d'
us dans le Tableauest parfois déf
la santé/les déterdes positions diffé
le présent csocio-économiqu
sexe ou de la rue dimension, et eur (voir Annexe Snomique à une sdicateurs provenciaires de l’intervetives. D'autres dssionnel, les reveapport.
Belgian
de la performancontroversée, lié
olitique. Un large été formulées
e S2 au présent rmance des systè
approché la dimen D'abord, nousdéterminants de n fonction de la ss dans le Tableglobaux d’équité équité dans les su 12 et la Figure 2finie comme « l'arminants de la sanérentes dans la hichapitre se coues. Les autres inrégion) figurent d
sont évoquées S1). Nous avons seule caractéristi
nant de la HIS)ention majorée)
dimensions de l'enus ou l'origine e
n Health System
nce d'un ée à un éventail dans la rapport,
èmes de
nsion de s avons la santé situation
eau 11). afin de
soins de 2). absence nté entre iérarchie oncentre négalités dans les dans la en outre ique : le ) ou le pour les inégalité
ethnique,
2Dinécospdinnm
Performance
2.8.1 InégalitéD’importantes ndicateurs de saétat de santé perçchaîne des détermobservées dans dsanté » (tabagismphysique et suppodimension « accendicateurs des an’étaient pas dismesurées.
és socio-économinégalités socionté globaux (esp
çu). Ces résultats minants de la sade nombreux indime, surpoids, aort social). Des inéessibilité ». Malhautres dimensionsponibles, de so
miques -économiques s
pérance de vie etrévèlent l'existen
anté. Des inégaliticateurs du chapalimentation peuégalités ont aussi heureusement, pns, les donnéeorte que les iné
KCE Report
s’observent danst espérance de s
nce d'inégalités datés ont égalemenitre « Promotion u équilibrée, acété observées da
pour la plupart es socio-économégalités n'ont pu
t 196
s les santé, ans la nt été de la ctivité ans la
des iques être

KCE Report 196
Tableau 11 – S
État de santé gEspérance de v
Espérance de v
Espérance en s
Espérance en s
% de la popula'très bonne'iii
Accessibilité dReport du conraisons financiè
Dépistage du ca
Dépistage du c64 ans) v
Adéquation % des patientsappropriés (exréguliers) v
Promotion de % de la populat
% de la populinsuffisant iii
% de la populat
6
Synthèse des iné
général vie à 25 ans, hom
vie à 25 ans, femm
santé à 25 ans, ho
santé à 25 ans, fe
ation 15+ qui qual
des soins ntact avec les seères (% des ména
ancer du sein (%
cancer du col de l
s diabétiques adamens de la ré
la santé tion 15+ qui décla
lation 15+ qui fa
tion adulte consid
égalités socio-éc
mes, 2001 i; ii
mes, 2001 i; ii
ommes, 2001 i; ii
emmes, 2001 i; ii
lifie sa santé de '
ervices de santé ages) iv
des femmes 50-6
'utérus (% des fe
ultes bénéficiant tine et analyses
are fumer tous les
ait état d'un supp
dérée comme obè
Belgian
onomiques
Valeglob
51.38
57.09
40.47
40.42
bonne' ou 76.8%
pour des 14.0%
69 ans) v 60.1%
mmes 25- 61.8%
de soins de sang
54.0%
jours iii 20.5%
port social 15.5%
èse (IMC ≥ 13.8%
n Health System
ur bale (f)
Valeur le grsocial plus ba
8 47.56
9 53.98
7 27.75
2 28.92
% 57.4%
% 27.0%
% 48.6%
% 48.9%
% 48.0%
% 22.0%
% 24.4%
% 19.2%
Performance
dans roupe
le as (f)
Valeur le grosocial le élevé (f)
55.03
59.9
46.33
47.1
85.7%
4.0%
62.9%
64.2%
58.0%
13.1%
10.1%
9.1%
dans oupe plus
Différencabsolue
(le plus plus élev
-7.47
-5.92
-18.58
-18.18
-28.3%
23.0%
-14.3%
-15.3%
-10.0%
8.9%
14.3%
10.1%
ce
bas vs le vé)
Risqrelat
(le pvs élev
n.a.
n.a.
n.a.
n.a.
0.67
6.75
0.77
0.76
0.83
1.68
2.42
2.11
que tif
plus bas le plus é)
Mesusynth(CII ou
3.73%
1.43%
15.30%
16.56%
11.6%
-71.4%
4.7%
3.9%
7.4%
-36.1%
-34.8%
-34.1%
37
re de hèse u PAF)
%
%
%
%
%
%
%
%
%

38
30) iii
% de la populaou obèse (IMC
% de la populaet 200 gramme
% de la populatpendant au moi en années ; ii 5 nles taux ne sont p(Fraction attribuaSource : Health IIndicateurs conte
Nous avons retde la progressindicateur de laratios calculés financement réles taxes indirecitoyens acquconsommation proportion plus des taxes indireà mesure que lel'interprétation prévisionnels etEnsuite, commedes revenus aude Gini depuistraduit un surccroissante en Bque dans les au
ation adulte consi≥ 25) iii
ation affirmant cons de légumes par
tion affirmant pratins 30 minutes paniveaux d'études ; iipas ajustés en fonc
able à la Population)Interview Survey et extuels de l'équité
tenu deux indicatsivité du financea répartition du redans le Tableau gressif (taxes in
ectes sont régresittent le mêmeet services, deélevée de leurs
ectes (le montant e revenu augmende la des donnét pas de comptes e l'état de santé pu sein d'un pays, 1988 en Belgiqucroît d'inégalité
Belgique, ainsi qu'utres régions.
idérée comme en
nsommer au moir jour iii
tiquer une activitéar jour iii ii 4 niveaux d'étudestion de l'âge ; mesu) pour tous les autreEPS (calculs du KC
teurs contextuels ement public desevenu national. P12 indiquent que
ndirectes) a augmssives parce que taux d'imposit
e sorte que les revenus. En consdes taxes divisé
nte. Il convient touées 2010-2011, définitifs.
peut être influencénous présentons
ue. L’augmentatiodes revenus, on'un degré d'inégal
Belgian
n surpoids 46.9%
ns 2 fruits 26.0%
é physique 38.1%
s ; iv 5 catégories deures de synthèse = Ies indicateurs. CE et de l’ISP (instit
de l'équité: un ins soins de santéPremière observae la part des sou
menté. En règle gtoutes les catég
tion sur les binantis conserve
séquence, le taux par les revenus) tefois d'être prudecar il s’agit de
é par le niveau d's l'évolution du coon du coefficient n observe une lité plus élevé à B
n Health System
% 57.8%
% 21.7%
% 24.0%
e revenus ; v 2 catégICI (Indice de Conc
tut de santé publiqu
ndicateur é et un
ation, les urces de générale, ories de ens de ent une x moyen diminue
ent dans budgets
inégalité oefficient
de Gini inégalité
Bruxelles
Performance
40.0%
29.4%
42.8%
gories de rembourscentration des Inéga
ue)
17.8%
-7.7%
-18.8%
ement ; alités) portant sur l'e
1.45
0.74
0.56
espérance de vie et
KCE Report
-14.7%
13.1%
12.3%
de bonne santé, FA
t 196
%
%
%
AP

KCE Report 196
Tableau 12 – In
Indicateurs de
Ratio rentréetotales
Ratio rentrtotales
Ratio rentrées
Total
Source : Vade m
6
ndicateur de l'éq
e progressivité
es proportionn
rées progress
régressives/ren
ecum de la sécurité
quité: progressiv
nelles/rentrées
sives/rentrées
ntrées totales
é sociale, INAMI, ca
Belgian
vité du financeme
2005 (comptes définitifs)
20(cdé
71.1% 71
18.9% 19
10.0% 10
100.0% 10
alculs du KCE
n Health System
ent public du sys
006 comptes éfinitifs)
200(codéf
1.0% 72.0
9.0% 18.0
0.0% 10.0
00.0% 100
Performance
stème de soins d
07 mptes
finitifs)
2008(comprov
0% 70.6%
0% 17.3%
0% 12.1%
0.0% 100.0
de santé
mptes
isoires)
200(copro
% 69.4
% 17.2
% 13.4
0% 100
09 mptes
ovisoires)
201(bu
4% 64.
2% 19.
4% 15.
0.0% 100
10 udget)
2011 (budg
.8% 61.4%
.4% 18.4%
.8% 20.2%
0.0% 100.0%
39
get)
%
%
%
%

40
Figure 2 – Inditransferts, en B
Source : DGSIE Note : le coefficiepopulation. Lorsqrevenus), le coeffpossède tous lesfaible, plus la distégale.
cateur de l'équitBelgique et dans
(Belgique) ent de Gini exprime que l'égalité est parffficient est '0'. Lorsqs revenus), le coeffictribution des revenu
té: coefficient des les régions
l'inégalité entre les faite (toutes les persue l'inégalité est totcient est '1'. Plus le us au sein de la pop
Belgian
e Gini après taxat
revenus au sein d'usonnes ont les mêmtale (une seule perscoefficient de Gini e
pulation en question
n Health System
tion et
une mes sonne est n est
2ÉLcmsacbAEusocsLadcvUtrpdtonQaLlecBdc
Performance
2.9 ConclusioÉtat de santé Les quatre indicatcours du temps. moyenne des paysanté (c’est-à-direactivités) et la morclassement. Le taubonne est supérieAccessibilité desEn ce qui concuniverselle par l’asociaux (MAF, observations sont charge du patientservices des soinsL’accessibilité desavec un taux redisparités socialescontre la grippe vaccination chez leUn autre aspect deravail en soins dpopulation. Mêmedisponibles les dooujours d'informanécessaires pour rQualité des soapproche centréeLa qualité a été ses résultats sont cancer, mais préBelgique présented'Europe (avec decolocations en h
ons sur les forc
teurs relatifs à l’éL’espérance de
ys de l’UE-15, tae le nombre d’annrtalité infantile occux de personnes ur à la moyenne d
s soins cerne l’accessibiassurance-maladOmnio, Fonds préoccupantes te
t, et un certain ns de santé pour des mesures de prévelativement bas s et parfois régio
chez les persoes enfants. e l'accessibilité code santé (médece si d’importants onnées relatives ations sur le norépondre aux besins : efficacitée sur le patient ubdivisée en 5 somitigés. Ils sont toccupants dans e en effet le see très fortes dispahôpital psychiatri
ces et faiblesse
état de santé évoe vie est légèrendis que l’espéranées restant à vivcupent des positiopercevant leur sades pays de l'UE-
lité financière, mie et l’existence
Spécial de elles qu’un niveauniveau de report des raisons financièvention montre de
de dépistage donales), un taux onnes âgées, m
oncerne l’adéquatcins, infirmières)
efforts ont été aux forces de tra
ombre de professoins. é, adéquation,
ous-dimensions. Crès bons quant ale domaine de
econd taux de sarités régionales) ique en augme
KCE Report
es
oluent positivemeement inférieure ance de vie en bvre sans limitationons moyennes da
anté comme (au m15.
malgré la couvede filets de sé
Solidarité), certu élevé de dépendes contacts aveères. es résultats divergdu cancer (avecde vaccination m
mais un bon tau
tion entre les forcet les besoins entrepris pour reavail, nous manqsionnels de la
sécurité, contin
Concernant l’efficu taux de survie ala santé mentalesuicide le plus ainsi qu’un nombntation. Pour dé
t 196
ent au à la
bonne n des ans le
moins)
erture curité taines ses à
ec les
gents, c des moyen ux de
es de de la endre quons santé
nuité,
cacité, après e ; la élevé
bre de écrire

KCE Report 196
l’efficacité des d’indicateurs etL’adéquation deaugmentation dcibles, un suivdiabétiques) etgrande variabiliLa sécurité detendance à lamédicaux, les une fracture depost-opératoirepersonnes âgéd'escarres est eLa continuité etavec une bonnmoyen et en ade cancer, maiun taux élevé dL’approche cepartiellement. Lélevé, et on odomicile. Mais i
Efficience du s
L’efficience du avec une augmarché », de l’du séjour pourdoit être tempéque montrent cdu groupe cible
6
soins dans le dt de données sontes soins est assedu dépistage du vi modéré des rt une augmentatté entre les hôpita
es soins présentea baisse concerinfections nosoco la hanche. Par a et la prescriptiones présentent deen hausse. t la coordination d
ne continuité relatugmentation de cs un faible taux de réadmission da
entrée sur le pLe taux de satisfobserve aussi unil faut collecter da
système de santé
système de santgmentation de usage de la chirur un accouchemeéré par l’inadéquacertains indicateure évoquées ci-des
domaine de la st nécessaires. ez décevante, av
cancer du sein recommandationstion des taux deaux. e des résultats ernant l‘expositionomiales et la moilleurs, l’incidencen d’antidépresseues niveaux stables
des soins présenttionnelle avec le consultation multide couverture du ans les hôpitaux ppatient n’a pu faction envers le
ne tendance à laavantage de donné
é
té présente des rla prescription
urgie de jour et unent normal. Touteation, et donc le grs, comme les ma
ssus.
Belgian
anté mentale da
ec des taux élevéen dehors des
s (antibiotiques, e césarienne, av
encourageants, avn aux rayons iortalité hospitalière de la septicémieurs anticholinergiqs. Cependant, l’in
tent des résultats même praticien, disciplinaire pourdossier médical gsychiatriques. être évaluée q
es services de saa hausse des déées dans ce doma
résultats moyens de médicamentsne diminution de efois, ce messaggaspillage de ressammographies en
n Health System
avantage
és et en groupes patients
vec une
vec une onisants re après e ques aux ncidence
mitigés, un taux
r les cas global et
ue très anté est écès au aine.
à bons, s « bon la durée e positif sources, n dehors
PLcmpd
ÉsLcdséDelaecinLeducereq
Performance
Pérennité du sysLa pérennité du syconcernant le remédecins généralpersonnel infirmied’infirmiers.
Équité (analysessocioéconomiqueLa dimension complémentaires. décrivant l’état desanté en fonction été observées danDes inégalités ontet le suivi des pata plupart des indien fonction du staconcernant les inncomplètes. L’équité a égalemen évidence ce prdu financement deune évolution vecorrespond au nivet qui est lié à elativement peu é
qui indique une ré
tème de santé ystème de santé
enouvellement inslistes. Il faudrait
er associées à de
s de tous les e et 2 indicateursde l’équité a
Tout d’abord, e santé, les mod
du statut socioéns les indicateurst aussi été observients atteints de mcateurs basés suatut social dans négalités en qua
ent été abordée problème au niveaues soins de santéers moins d’équveau d’inégalité dun état de santélevé en Belgiquepartition plus inég
présente certainssuffisant de laaussi des données données sur
indicateurs en s contextuels)
été abordée les inégalités o
des de vie et l’utéconomique. De gs relatifs à la sanvées concernant lmaladies chroniquur les hôpitaux n’o
le cadre de ce plité des soins so
par le biais de deu macro. Le premé. Il est en dimin
uité. Le second dans la répartitionté général moinse, mais il augmengale des revenus d
s résultats interpe cohorte actuelles sur les besoinl’évolution du no
fonction du s
de deux mannt été analyséetilisation des soingrandes inégalité
nté et au mode dee dépistage du caues. Toutefois, coont pas pu être étprojet, les concluont encore large
eux indicateurs memier est la progres
ution, ce qui conest l’index Gin
n globale des revs bon. Cet indicente au fil du tempdans notre pays.
41
ellants e de ns en ombre
statut
nières es en ns de és ont e vie. ancer omme tudiés usions ement
ettant ssivité stitue
ni qui enus, e est ps, ce

42
Promotion de Enfin, la promod’indicateurs claindicateurs relaaptitudes indivd’indicateurs aclassiques de lpu être fourni. La plupart des taux national d’importantes dmettons en évidun niveau éledisparités. La disparités sociaest largement imanque de supet régionales âgées. La Belgique sinternational dcomplexes vispromotion de lentreprises) mainterpréter sans
De plus amplePour chacun depeut être consuSupplement S1informations tecalcul, présentinternationales interprétations,
la santé otion de la santéassiques sur la saatifs aux politiquviduelles. En raadéquats et dea santé et du mo
indicateurs de laintermédiaire pa
disparités régionadence le problèm
evé et une tendconsommation d
ales et régionalesinférieure aux bepport social préseet est particulièr
se classe à un du Tobacco Consent à mesurer a santé dans divais ne sont disps une analyse en
es informations ses indicateurs décultée sur le site In1. Cette fiche motechniques sur leste les résultats
et analyses ainsi que les réfé
a été principaleanté et le mode d
ues de santé, auaison de la d données en
ode de vie, seul u
a santé et du moar rapport aux 1ales et sociales o
me de l’obésité et dance à la hausde tabac diminu. La consommatiosoins quotidiens,
ente aussi d’imporrement préoccup
rang intermédiantrol Scale. En
l’importance devers environnemeonibles qu’en Flaprofondeur.
sont disponibles crits ci-dessus, unnternet du KCE, dtive le choix de l'is sources de do
chiffrés, y compar sous-grou
érences bibliograp
Belgian
ment abordée aude vie, complétés ux milieux sains
disponibilité très dehors des indun aperçu fragme
ode de vie présen15 pays de l’UEont été observéedu surpoids qui psse, avec d’impe, mais avec d
on de fruits et de l mais est en hau
rtantes disparités ant chez les pe
aire dans le clasoutre, certains
s politiques locents (écoles, comandre et sont dif
sur notre site Inne fiche de documdans le documenindicateur et cont
onnées et les mompris les compaupes, les limitephiques.
n Health System
u moyen par des et aux limitée
dicateurs entaire a
ntent un E, mais
es. Nous présente portantes e fortes légumes usse. Le sociales
ersonnes
ssement indices
ales de mmunes, fficiles à
nternet! mentation nt intitulé tient des odes de araisons es des
3
3
LpsincéddecCddladcàdQp
Performance
3 LE RAPPERFORAJOUTÉ
3.1 Quelle essystème d
La finalité du syspossible, afin de csanté des persnformations présecas échéant, la également aider lde santé publiqud’objectifs est un en effet, les futcomparaison entreCe rapport esquissde santé à traversde signaux d'avera pérennité et l'décideurs politiqucommandité des aà prendre. Dans décideurs politiqueQuoiqu’il en soit, lpour ambition d’or
PORT 201RMANCE :ÉE ET LIMIst l'utilité d’un rade santé ? stème de santé contribuer au mieonnes vivant eentées dans ce rperformance du
es décideurs poliue aux niveauxmaillon importantures évaluationse résultats observse un tour d’horizs le prisme de 74rtissement quant équité du systèmes étaient déjà c
analyses complémd'autres cas, c
es et requièrent da présentation ex
rienter le choix de
2 SUR LA UTILITÉ, VITATIONSapport sur la pe
belge est d'être eux au maintien een Belgique. Erapport devraientu système de sitiques à formulefédéral et régiot dans l'évaluatios pourront ains
vés et objectifs à aon de la performa
4 indicateurs. Cesà l’'accessibilité, me de santé. Dconscients des p
mentaires visant àces signaux sondès lors une ana
xhaustive et structes priorités d’actio
KCE Report
VALEUR
erformance du
aussi performantt à l'amélioration n conséquence,t servir à optimissanté. Elles devrr des objectifs ch
onaux. La formuon de la performai s’appuyer sur
atteindre. ance du système s indicateurs font la qualité, l’'efficians certains cas
problèmes et ontà identifier les ment nouveaux poualyse plus approfoturée des indicateons et de recherch
t 196
t que de la
, les er, le raient hiffrés lation
ance : une
belge office ence, s, les t déjà sures
ur les ondie. eurs a hes

KCE Report 196
3.2 Quelle précéde
Le rapport préPerformance', éétait que, en Bgrâce notammesecond rappoperformance du
Meilleure dispo
La disponibilité données sont mortalité infantnationales de m
Un éventail d'ipanoramique d
Comme indiquéétoffé pour co(suffisamment) indicateurs ontmentale, des sdans une moindsoins de longueDeux indicateules indicateurs statut socioécosont disponibles
6
est la valeur ajent? écédent, intitulé était avant tout u
Belgique, il est poent à la bonne crt présente la
u système belge d
onibilité des don
des données a édésormais dispo
tile. D'autre partmortalité a été nota
ndicateurs plus du système
é dans les objectiouvrir les domapris en compte
t été ajoutés à soins aux personndre mesure, danse durée, la centrars contextuels deont fait l'objet d'
onomique (lorsqus).
joutée de ce ra
'Un premier Pasune étude pilote. ossible de procédecollaboration entre
première évalude santé. Ses atou
nnées
été améliorée de monibles pour la t, le délai de diablement réduit.
complet, pour u
ifs opérationnels, aines et dimensdans le rapport l'éventail dans lnes âgées, de la
s les soins aux pealité du patient et e l'équité ont été une analyse syst
ue les données p
Belgian
apport comparé
s vers la MesurSa principale coer à une telle évae les administratiuation complète uts sont les suivan
manière significatsurvie au cance
isponibilité des d
ne vision plus
le jeu d'indicateusions qui n'étaieprécédent. De nole domaine de la continuité des sersonnes en fin de
la promotion de lajoutés, tandis q
tématique en fonpermettant cette
n Health System
ée au
re de la nclusion aluation, ons. Ce
de la nts :
ive : des er et la données
urs a été ent pas ouveaux la santé soins et, e vie, les la santé. que tous ction du analyse
SmLSins'Iace'pn
SLpdc
R
Uqle( pPedcte
AEédd
Performance
Simplification demeilleure lisibilitéLa structure du jeSeuls les indicatendicateurs pour lsont évoqués danIndicateurs en capproche favorisechangements en ten matière de principaux' et 'secne jouait aucun rô
Systématisation L'analyse des donprésentés selon ldans le temps parcomparaison inter
Recours aux info
Une utilisation maque celles qui sones registres et lesHIS), Résumé hopermanente steePharmanet), les denquêtes de vaccdonnées disponibcollecte additionneemps.
Amélioration de lEnfin, des tableauélaborés pour perde leur interprétatdes indicateurs.
la structure de lé de l'analyse eu d'indicateurs aeurs mesurés onlesquels nous n'ans la section 'Doours de dévelop
e la compréhensermes de disponi
données. L'ancondaires' a aussile dans leur interp
de l'analyse des nnées a été systéa même structur
r région, analyse pnationale.
ormations déjà di
aximale a été faitnt contenues danss enquêtes récurrospitalier minimalekproef), bases onnées de survecination, Registreles de manière roel, facilite l'analys
la communicatioux synoptiques armettre une présetion. Ces tableau
l'éventail d'indica
a été simplifiée ànt été gardés daavons pas pu raonnées disponiblppement' (voir susion du jeu d'indbilité des donnéescienne distinctio été supprimée, cprétation.
données matisée et les ind
re : évolution danpar sous-groupes
isponibles
te des données ds les bases de dorentes : l’enquête l (RHM), EPS (é
de données illance des infectie belge du cancoutinière, qui n'indse de l'évolution
on des résultatsagrémentés de coentation claire et x favorisent égale
ateurs, pour une
à de multiples égaans le jeu actuelssembler de dones prochainemenupplément S1).
dicateurs, souligns ainsi que les lacon entre indicacar il s'est avéré q
dicateurs sont touns le temps, évo
socio-économiqu
déjà disponibles, onnées administra
de santé par intechantillon permande l'INAMI (doions nosocomiale
cer. Le recours àduisent aucun code l'indicateur da
odes couleurs onlisible des résultaement la compar
43
e
ards : . Les
nnées nt' ou Cette e les cunes ateurs qu'elle
ujours lution
ues et
telles atives, erview nent -c N, s, les
à des oût de ans le
nt été ats et raison

44
3.3 Quelles3.3.1 La peMalheureusemeau système de existent, la valel'objectif. Dans externes (tels qavec des résulont été comparde positionner pas pour autanCertains résultatout en étant l'interprétation ddébat8, en raisque les variativalidité des com
Plusieurs organd'autres pays dl'OMS dans sonbisannuel 'Panocollaboration enindicateurs ECHConsumer IndeConsumer Pow
3.3.2 PrendCertaines donndatent de 2010administratives internationales,2005! Dans de politiques, de b
s sont les limitarformance, maisent, très peu d’osanté ont été dé
eur de l'indicateules autres cas, l'a
que les objectifs ltats d'autres payrés à la moyenne la Belgique par r
nt à la question « ats peuvent en efmauvais par ra
des comparaisonon des multiples ions méthodolog
mparaisons.
nisations internatio'Europe en matièn Rapport 2000 suorama de la Santéntre l'OCDE et l'UHI supporté par l'Uex13 publié par l'orwerhouse.
dre des décisionées sont manifes. Ce délai est inhéet à des registres nous avons parfonombreux cas, il aser leurs décisio
ations de ce ras en fonction de bjectifs spécifique
éfinis en Belgique.r a été évaluée pappréciation s'estfixés par l'OMS)
ys. Quand c’étaitdes pays EU-15.
rapport à ses voisNos résultats sonffet être meilleurspport aux objects de performancelimitations liées
iques et context
onales comparentre de santé et de ur la Santé dans lé en Europe'10,11 qnion EuropéenneUnion Européennerganisation privée
s sur base de dotement obsolètesérent au recours às. Pour procéder àois dû nous baserserait difficile, pou
ons sur de telles in
Belgian
apport ? quel objectif ? es et mesurables. Lorsque de tels par rapport à la vt fondée sur des ou sur une comppossible, les indCette approche a
sins, mais elle nent-ils bons ou mas que ceux d'autretifs définis. Par e entre pays fait à cette démarch
tuelles, qui nuise
t déjà la Belgique soins de santé. Ce Monde”9, le rapqui est le fruit de l, le site Internet de12, et l'Euro Healsuédoise Health
onnées obsolète et les plus récent
à des données à des comparaisor sur des donnéesur les décideurs nformations. Pour
n Health System
s relatifs objectifs aleur de objectifs paraison dicateurs a permis e répond uvais? » es pays, ailleurs, toujours
he, telles ent à la
à Citons port a
des lth
es ? tes
ons s de
r ce qui
cap
3Ll'in1
2
3
Performance
concerne les indicactuelles devraienperformance, dans
3.3.3 Une visioLes lacunes ont gabsence de donnndicateur ou des i. Statut santé
dans la mortaDans le rappo'années potenutilisée commprématurée pamortalité évitaservices de sa
2. AccessibilitéPour optimiseindispensableambulatoires savoir le pourassurance, à
3. Accessibilitémesurer l'équdes dépensesremboursemeintervention déconomique. disposer de patients.
cateurs dérivés dent être contenues ds la mesure où un
on plus globale, généralement traitnées (actuelles), einformations plus
é général : étudialité prématuréeort précédent, la mntielles de vie perd
me indicateur du star groupe de causable, pourrait ajouanté. é financière : uneer les politiques d'ae d'avoir une visionainsi que des ass
rcentage de persoquel coût, pour qu
é financière et équité du système es privées (contribuents nets par lesdu maximum à
Pour calculer ctoutes les donné
e la HIS, des donndans le prochain r
n nouveau HIS se
mais certaines t à l'absence d'inet à la nécessité détaillées. ier la part de m
e mortalité prématurdues' jusqu’à l'âgetatut santé. L’étudse, et éventuellemter un éclairage in
e vision plus globaccessibilité finann plus globale des
surances hospitalionnes couvertes puelles couverturesquité : une maniè
est de prendre enution individuelle os compagnies d'afacturer) en fonc
cette distribution, ées de revenus
KCE Report
nées parfaitement rapport de ra mené en 2013
lacunes subsistdicateurs pertinende trouver un me
mortalité « évita
rée (exprimée en e de 70 ans) était de de la mortalité ment aussi de la ntéressant sur les
bale est nécessancière, il est s suppléments sation privées (à
par une telle s précisément). ère plus exhaustiv compte la distribofficielle, supplémassurances privéction du statut s
il est nécessairet de dépenses
t 196
.
tent nts, à eilleur
able »
s
aire.
ve de bution ments,
es et socio-re de s des

KCE Report 196
4. Force de disponiblesdemande. envisagée l'offre et desont incoToutefois, besoins. Dseulement d'organisatsoins prima
5. Santé mechangemeplus récenéquilibré aL'objectif pen charge recourant ambulatoirenouveaux i(tels que dossier, ouet le budgepas encordisponibles
6. Continuitérelatives adisponiblesnouveaux chronique dans la pmanque epertinents, coordinatio'santé' du p
6
travail : de mes, mais il manquUne planificationdans le cadre d
es besoins des pontestablement
ce rapport ne cD'autre part, l'ef
des besoins tion du système aires et des soinsentale : les indnts intervenus ré
nte a pour but d'axé sur les 'réseaprincipal de cette de proximité à chplus aux servic
es ne répondentindicateurs ont étle pourcentage d
u encore le rapporet total des soinsre pu être mesus. é et coordinatioux nouveaux tras, mais des lactrajets pour le dsont en cours d'
prochaine éditionencore des don
tels que les reon des soins ou lapatient.
eilleures donnéesue encore des in efficace de l'effed'une politique glpatients. Les donnaméliorées dep
contient aucun inffectif soignant médicaux, maisdes soins de s
hospitaliers. icateurs actuels
écemment dans c'instaurer un moaux de soins' (intréforme est de m
haque fois que la cces hospitaliers t plus aux besoié proposés pour de patients bénért entre les dépens de santé mentaurés en raison d
on des soins :ajets de soins amcunes subsistentiabète de type 2'évaluation. Ces n du rapport pennées relatives etours d'expérien
a disponibilité perm
Belgian
s relatives à l'offormations relativ
ectif soignant devlobale tenant comnées relatives à lpuis quelques ndicateur portant nécessaire dépes aussi des manté, et notamm
s ne reflètent pce secteur. La réfdèle de soins intitulé 'projet Artic
mettre l'accent surchose est possiblque lorsque le
ns du patient. Psuperviser ces év
éficiant d'une gesses en soins de ple). Ces indicateu
des limites des d
de nouvelles dmbulatoires seron. Les résultats
2 ou l’insuffisanceéléments seront
erformance. Toutaux autres ind
nce des patientsmanente des infor
n Health System
ffre sont ves à la vrait être mpte de 'offre se années. sur les
end non modalités ment des
pas les forme la tégré et le 107'). r la prise e, en ne
es soins Plusieurs volutions stion de proximité urs n'ont données
données t bientôt de ces
e rénale intégrés
tefois, il dicateurs s sur la rmations
7
8
9
Performance
7. Centralité dules données intrinsèquemecar elle exprimattentes spécPour nous pprochaine val'expérience d(généralistes internationalel'OCDE.14 Leambulatoires rapport.
8. Soins de lonévaluer la quâgés : la prévâgés soumis l'incidence deindicateurs nmanque de prochainemeninstrument a éâgées bénéfic
9. Soins aux pesont disponibLes quelquesrapport portensur la populatCes deux gpopulation élcarence en dnationale n'a en fin de vie. fin de vie n'edes organisat
u patient : de nomsont rares. La c
ent difficile à mesume la capacité ducifiques du patientpermettre de miegue de la HIS cdu patient en ma
ou spécialistes, ces questions s
es expériences seront donc inté
ngue durée : Plualité des soins devalence de la mà une contentions escarres et la p'ont pas encore données dans
nt des données été mis au point pciant de soins à doersonnes en fin bles en Belgique, s indicateurs relant sur la populatiotion de patients broupes ne couvigible aux soins données. Jusqu’àété publiée sur l'aEn comparaison
st pas ou peu retions international
mbreuses initiativecentralité du patiurer sur base de u système à répot ou à favoriser l'eux appréhendercontiendra une satière de soins d). Pour permettseront fondées sdes patients e
grées dans la pr
sieurs indicateurse longue durée dalnutrition, le pon physique, la pr
problématique de pu être mesuréce domaine. L’pour certains ind
pour évaluer les bomicile ou en instde vie : de nombmais très peu de
atifs à ce paramèon de patients dé
bénéficiant de soinvrent pourtant p
palliatifs, ce quà présent, aucunaccessibilité ou s avec les autres
eprésentée dans les.
es ont été prises, ent est un paramdonnées quantita
ondre efficacemen'implication du par cette dimensioérie de question
de santé ambulatre une comparur le questionnai
en matière de rochaine édition d
s ont été choisis dispensés aux paurcentage de parévalence des chla polymédicationés, ce qui attest’outil BelRAI foudicateurs retenusbesoins des persotitution. breuses études loe données nationètre présents danécédés d'un cancns palliatifs à dom
pas l'ensemble dui atteste d'une ne donnée de psur la qualité des domaines de soiles bases de don
45
mais mètre
atives, nt aux atient. on, la s sur toires
raison re de soins de ce
pour atients atients hutes, n. Ces te du urnira
s. Cet onnes
ocales nales. ns ce cer ou micile. de la réelle
portée soins ns, la nnées

46
10. Promotiondonnées sinformationlittéracie ecomme un comme lesles facteursaux individpromotion 2008-2013l’étude eurpour certai
11. Une plus le prochaine peut indicateurspropose divinputs et intéressant
12. Inégalitésindicateursdonnée somutuelles, brutes et a
n de la santé : nur la littéracie en
ns sont disponiben santé est un
paramètre clé das aptitudes individs qui déterminent dus de faire de
de cette littéraci3 de la stratégie opéenne sur la Hns pays. grande attentionin rapport. Manifêtre valablemen
s contenus dans verses mesures dles outputs.7,15
t potentiel d'étude: les inégalités n
s car, dans certaiocio-économique les informations pproximatives.
nous ne dispososanté (health lite
bles dans d'autconcept relativem
ans la gestion de lduelles requises p
sa propre santé. meilleurs choix eie a été définie de l'Union Europ
Health Literacy son
n devrait être pofestement, l'efficie
nt évaluée sur ce rapport. La
de l'efficience fondCe point recèle
e. n'ont pas pu êtreines sources de n'est disponible.sur le statut socio
Belgian
ns pas, en Belgieracy), alors que dres pays d'Euro
ment nouveau, coa santé. Il peut êt
pour comprendre Ces aptitudes pe
en matière de sacomme action p
péenne. Les résunt disponibles dep
ortée à l'efficiencence des soins dla base des qlittérature intern
dées explicitemene incontestablem
e étudiées pour données (RHM), Dans les donnéo-économique son
n Health System
ique, de de telles ope. La onsidéré tre défini et gérer rmettent anté. La
prioritaire ultats de puis peu
ce dans de santé quelques nationale nt sur les ment un
tous les aucune
ées des nt assez
4CpfacdpreCppteécLempppl'c(édlad
Performance
4 CONCLUCe rapport contieperformance du saisabilité préalabchiffrées, ce rappode la performancepolitiques sur certecherches comp
Ce rapport marquprécédent, grâce pertinents. Dans cemps. Des lacuneété comblées depcause ou le taux dLa Belgique n'est en 2008 la Charmembres se sonperformance de possèdent plusieperformance des élaboration de ce
clés d'une évaluaégalement soulig
données récentesa publication dyndes modalités à in
USION GÉnt les résultats dsystème belge deble. En présentaort a pour ambitioe du système de tains points et delémentaires. e une avancée s à un éventail
certains cas, il pees importantes duis la dernière éd
de survie au cancepas le premier parte de Tallinn st formellement eleur système de
eurs années d'esystèmes de s
e rapport, par exeation efficace de née dans les rapp. La mise à jour réamique des résu
nvestiguer.
ÉNÉRALE 'une première éve santé, faisant snt 74 indicateurs
on de brosser un santé, d'attirer l'ae suggérer des p
ubstantielle en cod'indicateurs pl
rmet de mesurer dans les donnéesdition, telles que leer. ays à avoir relevéur les systèmes
engagés à supere santé. Plusieuexpérience danssanté, ont servi
emple les Pays-Bala performance
ports néerlandaiségulière des donn
ultats sur un site
KCE Report
valuation globale suite à 'une étuds assortis de vatour d’horizon co
attention des décidpistes d’actions o
omparaison au raus complets et des 'évolution da
s de base ont en e taux de mortalit
é ce défi. En paras de santé, les rviser et à évaluurs pays voisinss la mesure d d'exemples loras. Une des conddu système de ) est la disponibilnées administrativInternet seraient
t 196
de la de de aleurs mplet deurs ou de
apport plus
ans le outre
té par
phant États
uer la s, qui de la rs de ditions santé ité de ves et
l’une

KCE Report 196
Avec la directivsoins transfropréoccupation directive aura é2013, les États autre État mepertinentes surpermettre de rapport jette nsystématique dcomme une presponsabilités soins sûrs, de h
f Directive 2
relative àtransfronta
6
ve européenne suontaliers, l’engag
partagée par toété transposée damembres devron
embre sont en r les normes de sprendre une décnon seulement de la performancepremière étape p
et de dispenser haute qualité, acc
2011/24/UE du Parl’application des draliers, JO L 88/45, 4
ur les droits des pgement pris àous les États mans les législation
nt s'assurer que lemesure de rec
sécurité et de quacision informée. les fondements e, mais il peut é
permettant à la tant aux patientsessibles et efficie
rlement européen eroits des patients e4 avril 2011
Belgian
atients dans le ca Tallinn devie
membres.f Lorsquns nationales, en es patients provencevoir des inforalité des soins, pDans cette optid'une future év
également être coBelgique d'assum
s belges qu'étrangnts.
t du conseil du 9 mn matière de soins
n Health System
adre des ent une ue cette
octobre nant d'un rmations pour leur que, ce
valuation onsidéré mer ses gers des
mars 2011 de santé
Performance 47

48
SCIENTIFIC RREPORT
Belgian
T
n Health System
111TInthTopspbrefuhadtoecsfosaTthfi
F
BEhthe
Performance
1 BACKG1.1 Context 1.1.1 InternatiThe Tallinn Chartn June 2008, thehe European regiTallinn Charter onobjective of the Tpeople’s health byseven commitmeperformance: “(thebe accountable foesults”. The ratiounctioning health health systems neacknowledged thadisease preventiono address health extensively develocommitments in tsolidarity, equity ostering investmesystems more resand ensure that heThe last commitmhe Tallinn Confeinancial crisis.
From values to a
By signing the TEuropean region highest attainable his common valuequitable basis,
ROUND A
ional context ter in 2008 e 53 Ministers of on of the World H
n Health SystemsTallinn Charter is y strengthening t
ents signed, thee member states or health systemnale of that commsystems are esse
eed to demonstratat health systemsn, health promotioconcerns in their
oped by the WHOhe Tallinn Charteand participatin
ent across sectorponsive to peopleealth systems are
ment proved afterwrence the world
ctions, from Tall
Tallinn Charter, areinforced that tstandard of healt
ue a set of goacontribute to so
ND APPRO
Health from the Health Organisatios for Health and
to commit memtheir respective he third is relate
commit) to proms performance to
mitment is given eential to improvingte good performa
s are more than hon and efforts to ir policies, an apprO in its “Health iner include promo
ng, investing in rs that influence e‘s needs, preferee prepared and abwards to be visiowas struck by a
linn to Health 202
all member statesthey share the cth as a fundamen
als were listed: iocial well-being a
KCE Report
OACH
countries belongion (WHO) signedWealth”. The pr
mber states to imhealth systems. Oed to health symote transparencyo achieve measuearlier in the text:g health, and thernce”. The Chartehealthcare and ininfluence other seroach that was alrn All Policies”.17 Ooting shared valu
health systems health, making h
ences and expectable to respond to conary, as no long
global economic
20
s of the WHO incommon value ontal human right. mprove health oand cohesivenes
t 196
ing to “The imary prove
Of the ystem y and urable “well refore r also clude
ectors ready Other es of
and health ations crisis. after c and
n the of the From
on an ss by

KCE Report 196
distributing the and aim at efficinterim report omember statesparallel, the Wpolicy, Health 2policy framewopast decades decreasing fertaccelerating tincreasing accefour policy prior(1) Investing inpeople, demonbenefits of heal(2) Tackling Euthe burden of activity, HIV/AID(3) Strengtheniand preparedne(4) Creating a h1.1.2 Nation2010, publicatiAssessment Two years afteron Health SysJune 2010.1 Thperformance oprudence of thesystem (a muchof this prudenc
6
burden of fundingciency by makingon the implemen
s have made opeWHO European re
2020.19 It aims to ork in light of the
in Europe: chanility), globalisationtechnological iness to informationrities focus on: n health through nstrating the impth promotion,
urope’s major heanon-communicab
DS, antibiotic resising people-centreess for emergencihealthy and supponal context ion of the report
r the signature of stem Performancehe title of this repof the Belgian he authors: healthch broader scope),
ce lie in the amou
g fairly accordingg the best use of ntation of the Talerational these vaegion has launche
provide a coheretrends that have
nges in demogran and migration (inovation (includn for patients and
a life-course apportance for the
alth challenges (able diseases, tobstance),
ed health systemies and ortive environmen
on Belgian Heal
the Tallinn Charte Assessment (Hport “A first step thealthcare systemcare system is me, and it is the first
unt of work neede
Belgian
to people’s abilitavailable resourc
llinn Charter detaarious commitmeed in 2010 a newnt evidence-basebecome salient o
aphy (increasing ncluding health w
ding genetics), d the general pub
pproach and empWHO of the e
among which recobacco, diet and
s, public health
t.19
lth System Perfo
er, the first BelgiaHSPA) was publtowards measurinm” is illustrativeentioned instead ot step only… The ed for this first eva
n Health System
ty to pay ces.3 An ails how
ents.18 In w health ed health over the ageing,
workers), rapidly
blic. The
powering expected
ognising physical
capacity
ormance
an report ished in
ng of the of the of health reasons aluation:
nleTHtasrewAHereswcps(toa
1T(staTwnocdE
Performance
new collaborationevels had to be The report was aHSPA framework ailored to the Beselected, and 40 oesults, strengths,
were discussed. After the publicatiHSPA requested evaluation of theequested to enric
such as mental hwere insufficientlycommunities requepromotion by enlsystem to a full evi.e. continuity of co be insufficientlyassess these dime
1.2 The BelgThe Belgian perfosee Figure 3) inailored to the BelgThe conceptual fwhich do not reprnon-medical deterof 5 domains: heacare and end-of-ldifferent dimensioEquity has been d
s between admiinitiated, and sta
articulated aroundwas constructed
elgian context. Seof them could be weaknesses, ev
on of the first repthe project to b
e Belgian Healtch the set of indicaealthcare, long-te
y covered in this fested new indicatarging the set fvaluation of the hcare, patient cent
y represented, andensions.
ian performancormance report mnspired by the Dgian health systemframework is comresent a hierarchyrminants of healthalth promotion, prife care. Each ons: their quality, aefined as an over
nistrations of theakeholders were d two main sectiod based upon inteecond, a core sete measured. Baseolution over time
port, the commisbe continued, aith System. The ators with indicatoerm care and endfirst report. In addtors to assess thefrom the evaluathealth system. Lateredness and eqd new indicators
ce framework amakes use of a Dutch and Canadm. mposed of threey. The three tiersh and the health sreventive care, cuf these domains accessibility, efficrarching dimensio
e federal and regconsulted extens
ons. First, the Beernational experiet of 55 indicators
ed on these indicaand proposed ac
sioners of the Beming at a syste
commissioners ors in specific domd-of-life care, as tdition, the regions performance of hion of the healt
astly, three dimenquity) were considhad to be propos
and definitions conceptual framedian frameworks
e interconnected s include health system itself, consurative care, long
can be evaluateciency or sustainaon.
49
gional sively. elgian ences s was ators, ctions
elgian matic
also mains those s and health hcare
nsions dered sed to
ework ,20, 21
tiers, tatus,
sisting g-term ed on ability.

50
Figure 3 – The
e conceptual frammework to evalua
Belgian
ate the performa
n Health System
nce of the Belgia
Performance
an health systemm
KCE Reportt 196

KCE Report 196
Definitions useThese definition(2006)4, VlayeCommittee (200
Health statusThis tier addresBelgium?”, covdisease, disordfunctions (altera[activity limitatibeing (physical
Non-medical dThis tier encomon if, when anbehaviour/lifestand working c(e.g. air, water,waste disposal)
Health systemWithin the politsystem is the eand resources system encompactivities to inflthe social, envir
Domains of theThe health syscurative care, lgoes far beyond• Preventive
disease (pi.e. taking
6
ed in the concepns are based on en (2006)6, Au01)22 and the Otta
sses the questionvering several dimder, injury, traumations to body, stion] and particip, mental, and soc
determinants of hmpasses the deternd how we use tyle (e.g. smokingonditions, person, food and soil qu).
tical and institutio
ensemble of all pumandated to im
passes both persuence the policieronmental and ec
e health system stem has been glong-term care ad the boundaries
care: healthcareprimary prevention
medication to p
ptual framework the following sou
ustralian Nationaawa Charter23.
“How healthy is mensions, such a
ma or other healttructure or functioation [restrictionsial well-being), an
health rminants that havcare. These dete
g, physical activitnal resources, anuality resulting fro
onal framework oublic and private prove, maintain osonal and populaes and actions of conomic determina
and health promgrouped into 4 dond end-of-life carof the health syste aiming to prevn, i.e. vaccinationprevent myocardi
Belgian
rces: WHO (2008al Health Perfo
the population reas health (prevah-related states),on [impairment], as in participationnd death.
e an effect on heerminants includety), genetic factornd environmental
om chemical pollu
of each country, aorganizations, insor restore healthation services as other sectors to
ants of health.
motion omains: preventivre. The health prem.
vent the occurrenn; secondary preal infarction afte
n Health System
8)3, Arah ormance
siding in lence of , human activities
n]), well-
ealth and e health rs, living l factors tion and
a health stitutions . Health well as
address
ve care, romotion
nce of a evention, r a first
•
•
•
g
Performance
episode) or ttesting, screeproblems earl
Curative carepromote recov
Long-term caorganisation aare limited inover an extecomponents operiod, and sprogram acromain populatilong-term careLong-term carhome nursing
End-of-life caclear that thecare includes elements of ca
Home nursin
daily living (Aprovided by example woucare (mainly In the residepersonnes âgvoor bejaardefacilities to opersons whopermanent hrepos et de costs and cohealth insura
to detect health ening for diseasesy before they mane: healthcare thvery. are: The term “loand delivery of s their ability to fu
ended period of of this definition: fsecond, the careoss service compons: first, long-tee for persons withre for older perso care, homes for tre: the care of a p
e person is in a ppalliative care bu
are relevant to the
ng care is availableADL) and/or cognitiv
home nurses incund dressing and ahygienic care in pat
ential sector, homgées”, MRPA /”wooen” ROB) provide nolder persons with o are strongly deospital treatment arsoins” MRS/”rust-
osts of care in residnce, board and lodg
problems befores, and other servnifest symptoms).at tends to ove
ong-term care seservices and assiunction independ
time. There arefirst, the care conte is usually proviponents.24 This rrm care for older
h mental disorder.ons include the folthe elderly and nuperson from the mprogressive state ut also broader soe end of the life.
e for persons with lve limitations, irrespcludes technical nuadministering medictients with ADL dysf
mes for the elderlyonzorgcentra”, prevnursing and personmainly low to mo
ependent on care re admitted to nursen verzorgingstehudential care facilitieging costs are to be
e they occur (reices that detect h. ercome disease,
ervices” refers tostance to peopleently on a daily e two complemetinues over a longided as an integreport focuses on
persons, and se llowing major servursing homes.g moment it has be
of decline. End-ocial, legal and sp
ow to severe activitpective of their ageursing interventioncation) and basic nfunction).
y (“maison de reposviously called “rustonal care as well asoderate limitations.
but who do not sing homes (“maisuis” RVT). While mes are covered by e paid by the residen
51
egular health
and
o the e who basis
entary g time grated n two cond,
vices:
come of-life
piritual
ties of . Care s (for ursing
s pour oorden living Older need
son de medical
public nt.

52
• Health proenabling pdeterminangoes far bemeans of policy thathousing, foThe other settings, inindividuals
Health systemThis is a muchthan healthcardeterminants, picture of popul
Dimensions ofHealth system health system dquality, efficienequity. Accessibility reached”. It recfinancial, culturthat health servQuality is definand populationsconsistent withinto five sub-dipatient-centered• Effectivene
outcomes, services to
• It is therefoas “the deg
omotion has beenpeople to incrents, and thereby imeyond the boundahealth promotiont addresses the ood security, emp
axes defined inncrease the role o, reorientation of t
performance h broader concepre system perfohealthcare and lation health.
f Health System performance, wh
domain, is groupency and sustaina
is defined as “thcovers physical (ral, psychologicavices are a priori aned as “the degres increase the like
h current professimensions, includidness and continu
ess is defined given the correc
o all who could benore closely relatedgree to which pro
n defined by the ase control ovemprove their healaries of the health n occur through d
prerequisites of ployment, and qu the Ottawa Cha
of the community,the health service
ptual approach tormance by explcontextual inform
Performance hich is presenteded into four main ability, and the o
he ease with wh(geographical disl dimensions of
available. ee to which healtelihood of desiredional knowledge”ing effectiveness,uity. as “the degree ct provision of evnefit but not thosed to appropriateneovided healthcare
Belgian
WHO as “the proer their healthth". The health prsector: indeed on
developing healthhealth such as
uality working coarter are: create increase the skil
es.23
o measuring perfoicitly using non-
mation to give a
d and analysed fdimensions: acce
overarching dimen
hich health servistribution), organizaccess. Access
th services for indhealth outcomes. It is further su, appropriateness
of achieving dvidence-based hee who would not bess, which can be is relevant to the
n Health System
ocess of and its
romotion ne of the hy public
income, nditions. healthy
ls of the
ormance -medical clearer
for each essibility, nsion of
ices are zational, requires
dividuals and are bdivided
s, safety,
desirable ealthcare benefit”. e defined e clinical
•
•
•
E(ereSinfanthEadpmo
Performance
needs, given tThe link betwbetween outco
Safety can bestructures, reharm to the usenvironment i
Patient-centerand responsivand ensuring
Finally, contispecified useproviders, instrajectory is corganisation ato be part of c
Efficiency is defini.e. money, time a
ensuring that theesults (i.e. allocat
Sustainability isnfrastructure sucacilities and equineeds. Important fhe health personnEquity is a transvall three tiers of thdistribution of hepayment for healtmedical determinaoverlaps with the d
the current best eween effectivenesomes and proces
e defined as “the dnders services, aser, provider, or en this definition exredness is definedve to individual pthat patient valuenuity addresses rs, over time, is
stitutions and regcovered. This alsoacross providers, continuity. ned as “the degreand personnel) is se resources aretive efficiency)”. s the system’s h as workforce ipment, and be ifactors for the manel’s satisfaction aversal dimension, e framework. Equ
ealthcare across thcare. Above thants of health andimension of acce
evidence and the ps and appropriateses.
degree to which thand attains resultsenvironment”. Inclxtends the dimensd as “providing ca
patient preferencees guide all clinica
“the extent to smoothly organisions”, and to wh
o means that ‘coo institutions and
ee to which the rfound for the sys
e used to yield
capacity to p(e.g. through ednnovative and re
aintenance of the and working condbeing considereduity is concerned wpopulations andis, “equity” can bnd for health staessibility.
KCE Report
provider’s experieeness reflects the
he system has thes in ways that pruding the providesion beyond qualiare that is respectes, needs, and val decisions”. which healthcar
sed within and aich the entire dis
ordination’ (i.e. smregions) is consid
right level of resostem (macro-levelmaximum benef
rovide and maducation and trainesponsive to emeworkforce also initions. and presented awith the fairness o with the fairnebe estimated for atus. There are
t 196
ence”. e link
e right event
er and ity. tful of alues,
re for cross
sease mooth dered
urces l) and fits or
intain ning), erging clude
cross of the ss of non-
many

KCE Report 196
Assessment oOnly a partial amade into the Performance of• Outcomes
Nutbeam’sinto outcomhealth outoutcomes,
• The main participatiointervention
Health systemThis includes thspecific to theinterpreting thein a broad wainfluence the framework, finaThis also mea(federal, regionsystem influenperformance itwhich has an im
Health in all poThis is a dimehealth system. related strate(http://www.eurpolicies” is to improve healthother than healt
6
of the Health promassessment of thscope of this wo
f health promotionof the health pro
s framework in Chmes very distal to tcomes (like adocalled “health pro
values and pon, empowermens, sustainability.
design and conhe important desige Belgian health health system peay, encompassinhealth system (
ancing) and the inans that the articnal, local) is consncing its perforself. An addition
mportant influence
olicies ension linking no
It can be defineegy contributingro.who.int/docume
examine determ, but which are mth.
motion he health promotioork. More detailsn. omotion can be
hapter 7 Performaaction (like health
opting healthy lifeomotion outcomesrinciples of the
ent, equity, m
ntext gn and contextua system, and werformance. Cont
ng both the loca(e.g. federal vs. nternational conteculation between idered to be a chrmance, rather
nal contextual face on ethical questi
on-medical determed as a horizontag to improve
ent/E89260.pdf). Tminants of healthmainly controlled
Belgian
on performance cs are given in Ch
categorized (seeance of health proh outcomes), interestyle), and mors” (like health litera
health promotimultistrategic/multi
al information thatwhich are necesstext should be intal (national) fact
regional contexext factors (e.g. E
the different auharacteristic of th
than a dimenctor is the local ions.
minants of healthal, complementaryed population The core of “hea that can be altby the policies of
n Health System
could be hapter 7
e further, omotion) rmediate re direct acy). on are: sectorial
t may be sary for erpreted ors that xt, legal Europe). uthorities e health sion of culture,
h to the y policy-
health lth in all tered to f sectors
1SpStoo1T1
2
31OTcndpaF1
2
3
Performance
1.3 ObjectiveSystematic evaluprocess, with puStrategic objectiveo be differentiatedoperational sub-ob1.3.1 StrategicThe HSPA proces
. To inform thesystem and to
2. To provide a system perforTallinn Charte
3. On the long-te1.3.2 Overall aOverall objective: To propose and chosen dimensionnumber of indicadomains would beprofusion of resultaimed at a set of aFour operational o
. To review thespecial focus 2010;
2. To enrich thehealth promoend-of-life cacontinuity of propose indica
3. To measure tin the availabi
es of the perforation of health
ublication of HSes, defined as the d from the specificbjectives. c objectives of ths pursues three se health authorito be a support for transparent and
rmance, in accorder; erm, to monitor thand operational
measure a set ons of our healthators. With a tooe missed. But a toots would dilute mabout 80 indicatorobjectives have bee core set of 55 i
on the 11 indic
e core set with iotion, general meare; to add indi
care (two sub-dators on equity in he selected indicaility of data;
mance project system perform
PA reports as objective of the o
c objective of the
he HSPA processtrategic objectiveties of the perfopolicy planning;accountable view
dance with the co
e health system pobjectives of the
of indicators cove system, while ko small set, impo large set is difficain messages. Fo
rs. een defined: ndicators of the pators for which t
indicators from thedicine, mental hicators on patiedimensions of qthe health system
ators, when possi
ance is an on-important milest
on-going process, present report, a
ss s: rmance of the h
w of the Belgian hmmitment made
performance over e 2012 report
ering all domainskeeping a reasoportant dimensioncult to manage anor the 2012 repor
previous report, wthere were no da
he following domhealth, long-term nt centerednessuality); and fina
m; ible, or to identify
53
going ones. have nd its
health
health in the
time.
s and nable ns or nd the rt, we
with a ata in
mains: care, and lly to
gaps

54
4. To interpreperformancincluding a
1.4 MethodOperational objspecial focus onThe update of tbetween the reFederal Public SOperational objthe following dolong-term care,and continuity introduce indicaThe strategy fodimensions conThe indexed litsearch for Heathe grey literatreport) or inteHealth for All Ddimension studprocess occurrand panels of escoring allowedmany criteria (potential for acconsensus amoIndicators on threcent RIZIV –Indicators on tliterature. A spethe performancreport.
et the results in oce of the Belgian
an international be
ds to reach opebjective 1: To revn the 11 indicatorthe former 55 indesearch team anService (FPS) Pujective 2: To enriomains: health pr end-of-life care; of care (two sub
ators on equity-iner the selection of
nsisted of the folloterature was sea
alth Services Studture, mainly repo
ernational organizDatabase, Eurostdied). This resultered on an iterativexpert specific fod to select the mo(relevance, contection). In the othong experts. he performance oINAMI project usithe equity of theecific working papce of health system
order to provide ahealth system by
enchmarking when
erational objectview the core setrs for which there icators was made
nd a specialist inblic Health.
rich the core set wromotion, general to add indicators
b-dimensions of thequality in health/new indicators in
owing: arched using usudies.25 Many indicorts of national (zations (e.g. OEtat, and reports sed in long lists of ve way, involving or each topics. In ore appropriate inent validity, reliaer cases, the se
of general medicing the same meth
e system were dper “The place of ms can be found
Belgian
a global evaluatioy mean of severaln appropriate.
tives t of 55 indicatorswere no data in 2e in a consensus health indicators
with indicators illul medicine, mentas on patient centehe quality); and f/health system. a variety of doma
al standards of lcators were also (e.g. Dutch perfo
ECD Health Dataspecific to the doindicators. The sboth the researcsome cases, a t
ndicators, with rebility, interpretab
election was base
ine were selectedhodology.26 erived from interequity in assessmin Supplement S
n Health System
on of the l criteria,
s, with a 2010.
meeting s of the
ustrating al health, eredness finally to
ains and
iterature found in ormance a, WHO omain or selection ch team two step gards to ility and ed on a
d from a
rnational ments of
S2 of this
TaOoAgwwwlabdFwOeWadrereaTgfo
Performance
The whole set of avoid redundancieOperational objectobjective 2, and toAfter the setting gathered the data were classified intwithin the next twwhom these indicack of relevant dbeing relevant, development”. For each measurwritten with detaileOperational objectevaluation of the pWhen the data wanalysis at nationademographic and ecent results coesults were discu
and identify shortcThe documentatiogathered in Supplor all indicators us
indicators was thes in indicators antive 3: To measur
o identify gaps in tup of an updatedto measure them
to two categorieswo years, and thoscators should be data, these indicaand were kept
rable indicator, aed results, includintive 4: To interpreperformance of thewere available, thal and regional lesocioeconomic fampared to Europussed with the ecoming and areas on sheets and thlement 1. A synosing colour-coded
hen reviewed by nd enhance the core the indicators sthe available datad set of indicato
m. Indicators withos: those for whichse for which it is collected. Nevertators were select
under a secti
a complete docung international coet the results in ore Belgian health she following analyevel (with trends oactors, and finally pean Union (EU
expert groups to for further develo
e detailed resultsoptic table summad cells.
KCE Report
the research teaonsistency of the sselected in opera. rs, the research out (yet) availableh data will be ava
not clear how antheless, in spite oted by the experon “indicators u
umentation sheetomparisons. rder to provide a gsystem. yses were perforover time), analysbenchmarking of )-15 countries. Tfacilitate interpret
opment. s of the indicatorarises the main re
t 196
am to set.
ational
team e data ailable nd by of the rts as under
t was
global
rmed: sis by f most These tation
rs are esults

KCE Report 196
1.5 The 20this rep
The selected 7domain and byresults (valuesfollowing chapteChapters 2 to indicators illusconsists of thre1. First, we e
to a motiva2. The “facts
indicator wfor the thperspectivealso availa(available o
3. At the endanalysis in
The following cdiscussed in Cinequalities andat the beginningIndicators for widentify gaps recommendatioThe result of recan be found i2010, 5 indicatoeither removed soon. Another because they wdata were outda
6
012 set of perfoport 74 indicators whiy performance dim) of the indicatorers of this report. 6 have the sam
strating one dime parts:
explain how the dation of the selecti
and figures” sectwe present the ma
ree regions ‘(whe with internationable in each docon the website). d of each sectionkey findings – mo
chapters illustrate Chapter 7 and Chd equity. The concg of this documenwhich there are c
in availability ons to policy makeeviewing the 2010n Appendix 2. Frors could be meafrom the set, eith12 indicators h
were deemed as ated.
ormance indica
ich could be memension in Appenrs are summarize
me structure. Eacension (e.g. qu
imension was evaon of the indicatotion is the core o
ain results of the dhere possible) aal results and tre
cumentation shee
n, we summarizeostly one key findsome specific iss
hapter 8 discusseclusion and discunt. currently no data of data in Be
ers in Chapter 9.0 set of indicatorsrom the 11 indicaasured in this repoher moved to the ihave been remov
not being releva
Belgian
ators and struct
easured are classndix A of this reped and discussed
ch chapter discusality, sustainabili
aluated which boors. of each chapter. Fdata analysis for Bnd put these re
ends. Detailed reset in the Supplem
e the results of ting per indicator. sues: health promes the aspects ossion are in the s
have been discuelgium, and to
s (operational objeators with data mort. The others handicators to be mved from the 20ant anymore, or b
n Health System
ture of
sified by port. The d in the
sses the ity) and
ils down
For each Belgium, esults in sults are ment S1
the data
motion is of health ynthesis
ussed to provide
ective 1) issing in
ave been measured 010 set, because
InwinliM•
•
•
Performance
n addition to thesewithin a two-year ncluded in the nexsted in Appendix
More documents a In Supplemen
presented, stechnical infointerpretation,A list of indicbut for which presented in discussed to provide recomdetails in Cha
In Supplemeperformance opaper on equperformed in B
In Supplemenselection of indicators inidomains: HeaPatient centeof-life care.
e 74 indicators, 1timeframe have
xt edition of the p3.
are available on thnt S1: one documummarising the rmation on data s, and the bibliograators that were dno initiatives arethis Suppleme
identify gaps in mmendations to apter 9. nt S2: “The plaof health systemsuity, indicators foBelgium. nt S3: All techniindicators (MESHtially selected, salth promotion / redness / Long-te
1 indicators for whbeen selected.
erformance repor
he KCE website: mentation sheet p
rationale for chsources and com
aphical referencesdeemed pertinent e currently taken nt S1. These iavailability of dapolicy makers w
ace of equity in s” (author: Christiaor equity and rev
ical details of litH terms, databascoring of expe
Mental health /erm care and car
hich data are expProbably, they wrt. These indicator
per indicator has hoosing the indic
mputation, limitatios.
by the expert grto collect data, isndicators have
ata in Belgium, ahich are discuss
assessments oan Léonard): a spview of available
erature searchesases searched, lrts) for the follo/ Continuity of cre of the elderly /
55
ected will be rs are
been cator,
ons in
roups, s also been nd to ed in
of the pecific
work
s and ist of owing care /
End-

56
2 OVERAPOPU
2.1 How dipopula
The objective assessment of anyway 4 globageneral outcomwell as a reflecindicators are:1. Life expect2. Health exp3. Percentage4. Infant mortFour other heamatter of fact, individuals andspecific domain• Suicide rat
care) • Overweigh
social outc• Rate of ne
social outc• Mean num
in the secti
ALL HEALLATION d we describe tion?
of this performthe health status
al health status inmes of the health ction of the global
tancy pectancy e of population petality rate lth status indicatowhile those four societal actors,
n or dimensions. Tte (described in se
t and obesity rateomes) ew HIV diagnosisomes) ber of decayed, mon 7.2.1, health a
LTH STATU
the overall hea
mance report ws of the Belgian dicators. Those csystem/health prdevelopmental le
erceiving their hea
ors were describeparticular indicatothey make part o
Those four indicatection 4.1.1, effec
es (described in
s (described in s
missing, filled teethand social outcom
Belgian
US OF THE
alth status of th
was not to perfpopulation. We d
can be seen as veomotion interventevel of a society.
alth as good or ve
ed in other sectionors can be influe
of the evaluation ors are:
ctiveness of menta
section 7.2.1, he
section 7.2.1, hea
hes in children (demes)
n Health System
E
he
form an describe ery distal tions, as Those 4
ry good
ns. As a enced by of some
al health
alth and
alth and
escribed
2
Tfow
LLereaimsL2msHaineycbHliliinfo
h
Performance
2.2 Facts and
This section is a sor each indicatorwebsite).
Life expectancy aLife expectancy (Lexpectancy has reductions in mort
attributed to a nmproved lifestyleservices.5 LE was 5.3 years 2010 and is highemen and 1.8 yearslightly lower than Health expectancyage without long-ndicator named ‘Hexpectancy to moyears lived. HLY consistent with prebut data for many HLY at 25 in Belgve thus about 5 ved in activity limn women. The HLor both sexes (Ta
SPMA: https:
isp.be/SASSt%2FHealth+E
d figures
hort summary of tr in the Supplem
and Health expecLE) at birth in Beremarkably incretality rates at all number of facto, better education
higher in women er in Flanders thars in women) (Tathe average of th
y represents the -term activity limiHealthy Life Yearsorbidity and disab
can be computevious published other reference a
gium was 41 yearyears longer tha
mitation. HLY increLY at 25 is highe
able 13).
://stats.wiv-toredProcess/guestExpectancy+Statisti
the detailed resultent S1 of this re
ctancy elgium was 80 yeeased since deca
ages. These gainors, including risn and greater ac
(82.6 years) thanan in Wallonia (dable 13). Life exphe EU-15, 80.7 yeremaining years tation. This is ths’ (HLY).28 It extebility in order to ted for several work, we presen
ages can be founds in men and wo
an men, but thoseases slowly in m
er in Flanders tha
t?_program=%2FEhics&_action=proper
KCE Report
ts which are preseeport (available o
ears as of 2010.2ades, reflecting sns in longevity casing living standccess to quality h
in men (77.4 yeaifference of 3 yea
pectancy in Belgiuars in 2010 (Figulived from a parte structural Euro
ends the concept assess the qual
ages. In order tt the HLY at 25 y
d. men in 2008h. Woe additional year
men but remains sn in the other reg
hleis%2FStored+Prorties
t 196
ented n the
7 Life sharp an be dards, health
ars) in ars in um is re 4). ticular opean of life lity of to be years,
omen rs are stable gions,
ocess

KCE Report 196
For internationBelgium is situ62.6 years versEU-15.
Table 13 – Lifeage 25 (2008),
Male Life ExpectancyHealthy life yeaFemale Life ExpectancyHealthy life yeaSource: * DGSIE
i https://sta
isp.be/SA%2FHealt
6
nal comparisons, ated close to thesus 63.0 years in
e expectancy atby sex and regio
Belgiu
y at birth* 77.4
ars at 25** 41.3
y at birth* 82.6 ars at 25** 41.2 E, data 2010; ** SPM
ts.wiv-SStoredProcess/guth+Expectancy+Sta
Eurostat compue average of EU-n EU-15, and for
t birth (2010), anon
um Brussels F
76.9 738.5 4 82.8 840.6 4
MA i, data 2008
uest?_program=%2Ftistics&_action=pro
Belgian
utes the HLY at-15 countries: formen 64.0 versus
nd Healthy Life Y
Flanders Wallon
78.5 75.5 43.7 37.4
83.3 81.5 42.3 39.1
FEhleis%2FStored+perties
n Health System
t birth.29 r women s 63.1 in
Years at
nia
+Process
Performance 57

58
Figure 4 – Life
Source: OECD H
74
75
76
77
78
79
80
81
82
2000
Life
exp
ecta
ncy
at b
irth
(yea
rs)
Bel
Net
EU-
e expectancy at b
Health Data 2012
0 2001 2002 2003
gium
therlands
-15
birth: internation
2004 2005 2006 20
France
United Kingdom
Belgian
al comparison (2
007 2008 2009 201
Germany
United States
n Health System
2000-2010)
0
DenPorFi
BeGer
GrUnited King
EA
LuxembNether
IrFr
SwS
Performance
77 78
nmarkrtugalnlandlgiummanyreecegdom
EU-15ustriabourgrlandselandrance
wedenSpain
Life
79.379.8
80.280.3
8088888
79 80 8
e expectancy at birt
30.580.680.680.780.780.780.8
81.081.3
81.582.2
81 82 83
th (2010)
KCE Report
t 196

KCE Report 196
Self-perceivedSelf-perceived and as highly pIn 2008, 77% ogood or very subjective appreven after adjuregions. Two databasesOECD Health Dthe European Usurvey. The for
Figure 5 – Infa
Source: OECD H
2
3
4
5
6
7
8
20
Dea
ths
per 1
000
live
birt
hs(in
fant
mor
talit
y)
Bel
Net
EU
6
d health health has been predictive of mortaof the people agegood. This rate
raisal of health stausting for age. It
s provide informaData (in which daUnion Statistics onrmer database wa
ant mortality rate
Health Data 2012
000 2001 2002 200
lgium
therlands
-15
proven as a reliabality. ed 15 years or o
e has slightly incatus was slightly lewas higher in Fl
ation for the interata from Belgium n Income and Livas chosen for its
: international co
03 2004 2005 2006
France
United Kingdom
Belgian
ble reflection of m
lder rated their hcreased over timess favourable in landers than in th
rnational compariscome from the Hing Conditions (Ecomparability with
omparison
6 2007 2008 2009
Germany
United States
n Health System
morbidity,
ealth as me. The women,
he other
son: the HIS) and EU-SILC) h results
a7
In
TqoEto3rath
2010
s
PS
DeGe
LuxemB
Neth
United K
Performance
above. Belgium co71.7%).
nfant mortality ra
The infant mortalitquality of health cof development. TEU countries, sucho 3.5/1000 live b3.4/1000 live birthates in the three rhan for female inf
0.0
FinlandPortugalSweden
SpainEU-15
enmarkermany
ItalymbourgBelgiumFranceGreeceIrelanderlandsAustriaingdom
Num
ompares very wel
ate
ty rate (IMR) is a bare services, and
The IMR has regulh as in Belgium (abirths in 2010, w
hs (Figure 5). Datregions. Rates arefants (3.4/1000).
1.0 2.0
mber of deaths per
l with other EU-15
basic indicator ford is highly correlatlarly decreased ovaround 5 deaths/1which is within tta per region (froe also higher for m
2.32.52.5
3.23.43.43.43.43.43.53.6
333
3.0 4.
r 1 000 live births
5 countries (avera
r population healthted to a country'sver the last decad1000 live births in he EU-15 averag
om 2008) show smale infants (4.2/1
3.83.83.83.9
4.2
.0 5.0
(2010)
59
age of
h and s level des in 2000
ge of similar 1000)

60
2.3 Key fin• Life expec
increasingFlanders. average of
• Although wlonger in greported) aranking w
• 77% of thegood in 20women, another EU-1
• Infant morThe figure1000 live bclose to thneighbour
dings ctancy at birth in g over time, and Life expectancy f the EU-15 (80.7women live longgood health sincactivity limitationithin the averagee population repo008. This proportnd drops with ag15 countries (avertality has decreaes are similar in tbirths in 2010. Inhe average EU-15ring countries.
Belgium was 80is higher for womin Belgium is sli
7 years in 2010).ger than men, thece the number ofn is higher in woe as compared worted their healthtion is higher for
ge. Belgium comerage of 71.7%).ased regularly ovthe three regionsfant mortality rat5 rates, and bette
Belgian
0 years as of 201men. It is higher ightly lower than
ey do not live muf years with (self-omen. Belgium iswith the EU-15. h to be good to vr men as comparpares very good
ver the last decas and are close totes in Belgium aer than in the
n Health System
0. It is in
n the
uch -s
very red to
d with
ades. o 4 for re
33AinapInawupreposW12F345
C6789Ac1
Performance
3 ACCESS3.1 How did wAccessibility is defn terms of physicavailability of quaprerequisite of a qn this report, waccessibility of theworkforce, addresused to determinepocket payments easons. Another
preventive policiesone indicator relaservices. Workforce
. Number of pra2. Number of praFinancial accessib3. Coverage of t4. Amount of co-5. Percentage o
because of finCoverage of preve6. Breast cancer7. Cervix cancer8. Coverage of v9. Coverage of iAccessibility of locarers)
0. Number of beand older
SIBILITY Owe evaluate thefined as the easecal access (geog
alified personnel.4ualitative and effic
we have definede healthcare systssing the availabie financial accessand delaying cogroup of indicat
s such as canceates to the timing
actising physicianactising nurses pebility the population in t-payments and ouof consumers whnancial reasons entive measures r screening (womer screening (womevaccination for younfluenza vaccinat
ong-term care (re
eds in residential
OF CARE e accessibility with which health
graphical distribut4 Accessibility of cient health systed twelve indicatem. Some indicality of healthcare s, focusing on insntacts with healttors measures thr screenings and
g (or timeliness) o
ns per 100 000 poer 100 000 popula
terms of health insut-of-pocket paymho delay contact
en aged 50-69 yeen aged 25-64 yeung children tion for the elderlyesidential care fo
care facilities pe
KCE Report
of healthcare?h services are reation), costs, timea health systemm. tors to evaluate
ators are related tpersonnel, other
surance status, ohcare due to finahe coverage rated vaccinations. Fiof access to pall
pulation ation
surance ments t with health ser
ears) ars)
y (65 years and olr elderly and info
er population 65
t 196
? ached , and
m is a
e the to the rs are out-of-ancial es for inally, liative
rvices
der) ormal
years

KCE Report 196
11. Percentagecarer
Accessibility of 12. Start of pal
3.2 Facts a
This section is afor each indicawebsite).
Workforce The number of currently activeaccessibility of The number of31 815 in 2010these, 38.4% wpsychiatrist spethe RIZIV – population (TabFew EU-15 Eurto the OECD. Ball registered pway of countinwhich was oneon data older thphysicians, givBelgium. Compof practising phbut is slightly hi
j For intern
RIZIV – Iservice du
6
e of population ov
end-of life-care: tlliative care very c
and figures
a short summary ator in the Supple
care providers ge in the healthcthe healthcare syf practising physi0, corresponding were GPs and 6ecialists. ExpresseINAMI since 20ble 14). ropean countries Before 2009, Belghysicians at the R
ng resulted in a p of the highest inhan 2009) the deving a better picpared to other OEhysicians, the dengher than in the U
national comparisoNAMI as those whuring a year.
ver 50 years old re
timeliness of start close to death
of the detailed resement S1 of this
gives information ocare sector, andystem. iciansj increased to a density of 2
6.07% psychiatrised in full-time equ09), this density
report the numbegian data on practRIZIV – INAMI (pophysician density
n Europe.1 Since 2nsity is based oncture of the ‘usCD countries whi
nsity in Belgium isUK (in 2009) (Figu
ns, the practising
ho provided more th
Belgian
eporting to be an
of palliative care
sults which are pr report (available
on the medical wd thus indirectly
from 28 999 in 2.91/1000 popula
sts and 56% wheuivalents (as calcuy reduces to 1.
er of practising phtising physicians otentially practisiny of 4.03/1000 po2009 (and retrosp the number of peful’ medical dech also report thes lower than in Gure 6).
physicians are dehan one reimburse
n Health System
informal
resented e on the
workforce on the
2000 to ation. Of ere non-ulated by 99/1000
hysicians included ng). This opulation pectively ractising
ensity in e density
Germany,
efined by ed clinical
TE
P
M
SNre
Performance
Table 14 – NumbEquivalent, and d
Profession
Medical doctorsGPs Psychiatr
Source: RIZIV – INANote: Practising phyeimbursed clinical s
ber of practisingdensity (/1000 po
Totpractisin
31 8112 22
rists 1 93AMI ysicians are defined service during a yea
g physicians, estopulation) (2010)
tal ng
Density
15 2.9228 1.1232 0.18
as those who proviar.
timation of Full
Total FTE
De
21 6918 6461 260
ided more than one
61
Time
ensity
1.99 0.79 0.12
e

62
Figure 6 – Num
Source: OECD H
Nurses are geoutnumbering pnumber of pracnumber of prapayroll of hospiof them. Only INAMI databaslarge survey to showed that onin the healthcafor older person
0
0.5
1
1.5
2
2.5
3
3.5
4
2
Num
ber o
f pra
ctis
ing
phys
icia
ns p
er 1
000
popu
latio
n
Belg
Uni
mber of practisin
Health Data 2012
enerally the mostphysicians in almctising nurses is ectising medical ditals or nursing honurses outside th
ses. For that reameasure the num
n the 152 376 nursre sector (39% inns or in nursing h
2000 2001 2002 200
gium F
ted Kingdom U
ng physicians (pe
t numerous healmost all OECD ceven more challendoctors; indeed, momes, and there ihe hospitals are son, the FPS Pumber of practisingses included in th
n hospitals, and thhome care). This
3 2004 2005 2006 20
France
United States
Belgian
er 1000 populatio
lth professionals,countries.5 Estimanging than evaluamany nurses areis no centralized cregistered in the ublic Health orgag nurses in 2009.he study, 70% werhe rest in residencorresponds to a
007 2008 2009 2010
Germany
EU-15
n Health System
on): internationa
, greatly ating the ating the e on the counting RIZIV –
anized a Results re active
ntial care a density
okInmd
United King
Luxemb
Belg
EU
Germ
S
Au
Performance
al comparison
of practising nursknow the number nternational commeaningless, as Bdiploma, and not o
0 1
dom
ourg
gium
U-15
many
Spain
ustria
Number practis
ses of 9.9/1000 pof corresponding
mparison based Belgian data still reon their working st
2.7
2.8
2.9
3.4
3.
3
2 3 4
sing physicians per (2010)
population.30 HowFTE. on OECD Hea
epresent all nursetatus in healthcare
.7
3.8
4.8
5 6
1 000 population
KCE Report
wever, we still do
lth Data is cures (on the basis ofe).
t 196
o not
rently f their

KCE Report 196
Financial acceA prerequisite fA compulsory hcitizens living iasylum seekersand hence are they have no expenses are c CPAS), and nHealth Data re99.5% in 2009(with many coucoverage, both level of accesscovered and thacross countrieof complementcurrently availaLow out-of-pocaccessibility toexpenditures bocover the (fullpayments (tickmedications anBetween 2003€7.25 billion, bremained const2010). Co-paymin 2010. Expretotal of €665 in
6
essibility for financial acceshealth insurance, in Belgium. In prs) may not fulfil ad
not affiliated to aright to necess
covered by the pot by the sicknesport a constant p. Other Europeanntries reporting 1public and privat
sibility across thee degree of cost-
es. Another indicattary health insurble in Belgium. cket (OOP) payo the healthcareorne directly by a) cost of the heket modérateur nd other expendit and 2010, the ut compared to ttant during the saments representeessed per inhabit2010.
ssibility is coverain principle, coverractice, some cadministrative and/a sickness fund. sary medical caublic municipal wss funds. The da
percentage of 99%n countries repor00%). Neverthelete, is an imperfecte countries, sincsharing applied totor of financial accrance (usually pr
yments are anote system. Out-oa patient where health good or se
/ remgeld), cotures paid directly
OOP expendituthe total health eame time period (ed 26.7% of all outant, out-of-pocke
Belgian
ge with health insrs the whole poputegories of citize
/or financial requirThis does not mere, but their he
welfare centres (Oata for Belgium in% insured personrt similarly high cess, total health int indicator to com
ce the range of o those services ccessibility is the crivate), but no d
ther condition foof-pocket paymehealth insurance dervice. They inclosts of over-they by private hous
ures rose from €expenditures, the(20.0% in 2003, 1ut-of-pocket expeet payments repr
n Health System
surance. ulation of ens (e.g. rements, ean that
ealthcare OCMW –n OECD ns, up to coverage nsurance pare the services can vary
coverage data are
or good ents are does not ude co--counter seholds. €5.33 to eir share 19.4% in enditures resent a
CoEeeaUdc
Performance
Comparison of heon the System of Eurostat, WHO anexpenditures at expenditures in Bare at the higher eUK lying below 10detailed scrutiny calculation of their
ealth expendituresHealth Accounts
nd OECD, is a coa national levelelgium (expresseend, with countrie0% (Figure 7). Aga
of all expenses r System of Health
s across Europea (SHA). The SHAmmon way to rep. The comparis
ed as a % of totaes such as Franceain, this statemen
included or noth Accounts.
an countries are bA, developed joinport and classify hon shows that
al health expendite, the Netherlandsnt should require at by countries in
63
based tly by
health OOP
tures) s and a very n the

64
Table 15 – Out
Year
All out-of-pockeBillion € % expenditure o€/capita Co-payments oBillion € % of all out-of-pSource: - Out-of-pocket e- Co-payments (t
Figure 7 – Out
Source: OECD H
t-of-pocket expen
et expenditures
on health
only
pocket expenditur
expenditures: Systemtickets modérateurs/
-of-pocket expen
Health Data 2012
nditures (2003-2
2003
5.5337420.0 533.31
res
m of Health Accoun/remgeld):RIZIV – I
nditures (as a pe
Belgian
010)
2004 20
4 5.53049 5.
18.8 18530.70 54
nts (SHA), OECD HeNAMI
ercentage of tota
n Health System
005 2006
68334 6.270448.6 20.5 42.37 594.47
ealth Data 2012
l health expendit
Performance
2007 20
4 6.73778 7.0
20.9 20634.10 65 1.8 26
tures): internatio
008 2009
02868 6.859820.3 18.9 56.27 635.38
85261 1.966206.4 28.7
onal comparison
2010
2 7.25518
19.4 665.88
0 1.93881 26.7
n
KCE Reportt 196

KCE Report 196
To guarantee fhave introducehouseholds wiexpenses agaithese social capostpone healtmental healthcreaches 26% o1997, this perceIt is difficult to bneeds are availdue to waiting tThe five followmeasures are e
Coverage of scThese two inmodalities: orgopportunistic scthe colorectal c
k Only to ci
co-paymeimplemen
l For coloreregional aBrussels),years, peroccult blohigh risk.3program, Flanders,
6
financial accessibed several “sociith low financialnst catastrophic
are nets, 14% of thcare (medical care) for financiaf the households entage was belowbenchmark these lable in OECD Hetimes or distanceswing indicators meffectively accessi
creening for breanterventions currganized nationalcreening for the cancer screening p
ite some of them: t
ents (introduced in ted in 2002) and theectal cancer, there approaches co-exis, a screening progrrsons aged 50-74 y
ood test), or directly31 There has beenbut it is still too pilot projects were
bility of healthcaral care nets”, wl means or withealthcare expethe households dcare, surgery, dr
al reasons. In B(14% in Wallonia
w 10%. data: indeed, dat
ealth Data, but thos.
measure in which ible and used by t
ast and cervical rently run with program for t
cervix cancer. It isprogram.l
the entitlement to i
1963), the Maxime OMNIO status (inis no national pro
st: in the French ramme was startedyears old are invitey a colonoscopy fon a preliminary ev
early to evaluatealso started.33
Belgian
re in Belgium, legwhich aim is to h very high hensesk. However, declared that theyrugs, glasses or russels, this per and 11% in Flan
a on global unmeose also include p
way specific prthe population.
cancer different organ
the breast cancs still too early to e
increased reimbursmum Billing Systemtroduced in 2007).gram in place, butCommunity (Wallo
d in March 2009. Eed to perform a FOr individuals at higaluation of the sta
e the global cover
n Health System
gislators protect
ealthcare despite
y had to lenses,
rcentage ders). In
et clinical problems
eventive
izational cer and evaluate
sement of m (MAB,
t different onia and
Every two BT (fecal h or very
art of the rage.32 In
•
•
m
Performance
For breast caFlanders and years. The latperformed ouare called hemammogramsResult: In 2060%, far belo75% target scoverage occthe “mammotwith regard toonly 11% in Bpartially due opportunistic the program.3
Cervical cancprognosis, catest (or Pap twomen agedessentially opResult: The caround 62% b2000, the coEuropean cou61% in 2008, Finland (70%)
m It is not poss
done for oppo
ncer, a national s2002 in Wallonia
tter co-exists with tside of the progrreafter “mammotes (opportunistic sc10, the total cov
ow the EU-15 aveset by the EU.5 curred within the ptests” in 2010). Do the coverage witBrussels and 7%
to the persistescreening in Wa
34 cer, a cancer with an be largely detetest).35 This test 25-64 years. Curr
pportunistic. cervical cancer scbetween 2007 anoverage rate wasuntries, Belgium but is still far from
) (Figure 9).
sible to distinguish iortunistic screening
screening programa and Brussels) fopportunistic scr
ram). Mammogramests”, to be distincreening or diagn
verage of breast erage of 68%, an(Figure 9) Moreoprogram (30% sc
Differences betweethin the program: 4in Wallonia. (Figu
ence of pre-exisallonia and Brusse
a low incidence ected in a curablis recommended rently, the screen
creening coveraged 2010. In a prevs already 59%.3caught up with tm some countries
n the nomenclature from mammogram
m exists (since 20for women aged 5reening (mammogms within this pro
nguished from all ostic test)m. cancer screeningnd even further oover, only half ocreening coverageen regions are st46% in Flanders, ure 8) This is prosting higher leveels before the st
and a medium toe stage by the severy three yea
ing for cervix can
e has remained svious study from 16 Compared to the EU-15 averas such as UK (80
e between mammogs done for a diagno
65
001 in 50-69 grams ogram other
g was of the of this e with triking while
obably els of art of
o poor smear rs for cer is
stable 1998-other ge of %) or
grams ostic.

66
Figure 8 – Per2010)
Note: mammotes
rcentage of wom
st = organised scree
en (aged 50-69)
ening program, mam
Belgian
who had a mam
mmogram = organiz
n Health System
mogram (within
zed + opportunistic s
Performance
program (a) or o
screening + diagnos
overall (b)) within
stic test; Source: IM
n the last two ye
MA-EPS, KCE calcul
KCE Report
ears, by region (2
lation
t 196
2006-

KCE Report 196
Figure 9 – Brea
Source: OECD H
Coverage of vaImmunisation iprimary prevenbased on the Indicators Moniregional healthregional level, athe three regionThe WHO-recofor Diphteria-Te
0
10
20
30
40
50
60
70
80
90
2000
%fe
mal
es 5
0-69
year
s sc
reen
ed fo
r bre
ast c
ance
r
Be
Ne
6
ast cancer and c
Health Data 2012, ex
accination s one of the m
ntion. The choice international indicitoring (ECHIM) ah competence, tand a national ranal rates. ommended target etanos-Pertussis
0 2001 2002 2003
lgium
therlands
cervical cancer s
xcept IMA-EPS for B
ost powerful andof the vaccinatio
cators from Euroand OECD. In Belthe vaccination
ate is computed a
rate for a collect(DTP) and 95 %
2004 2005 2006
France
United Kingdom
Belgian
screening: intern
Belgium 2008-2010
d cost-effective fons included in ouopean Communitylgium, as vaccinarates are meas
as a weighted ave
tive immunisation for measles. In
2007 2008 2009 2
Germany
EU-15
n Health System
ational comparis
0 (KCE calculation)
forms of ur set is y Health ation is a sured at erage of
n is 90% general,
thcBesolaCDcre
20100
10
20
30
40
50
60
70
80
90
%fe
mal
es 2
0-69
year
s sc
reen
ed fo
r cer
vica
l can
cer
Performance
son (2000-2010)
he recommendedcoverage of DiphtB (Hib), poliomyeexceeds 95%. Onstill just below 95%outbreaks of measarge outbreak of mCompared with oDTP3 coverage, pcoverage ranks ecommended lev
2000 2001 2002
Belgium
United Kingdom
d coverage rates teria-Tetanos-Pertelitis (Polio3), hely for Measles-Mu% in 2009. It mussles have occurremeasles occurredther European c
particularly since 2good, has muchel.
2003 2004 2005 2
Germany
EU-15
are reached in Btussis (DTP3), Haepatitis B (Hep3umps-Rubella (MMst be noticed thated in recent year
d in 2011.37 ountries, Belgium
2003. For measlesh improved and
2006 2007 2008 20
Netherla
elgium. The 3rd daemophilus Influe
3) has increasedMR) the coveraget some small epidrs, in all regions a
m ranks very goos (1st dose), the g reaches almos
009 2010
ands
67
dose-enzae d and e was demic and a
od for global st the

68
Figure 10 – Pe
Source: OECD H
In Belgium, seagroups of perpersons aged >professionals; risks like obestarget vaccinatAgency (IMA) rthe vaccination 2008-2009)40, eother countriesNetherlands (b(63%).
75
80
85
90
95
100
2000 2001
%ch
ildre
n va
ccin
ated
aga
inst
DTP
Belgium
Netherla
EU-15
ercentage of child
Health data 2012
asonal influenza vrsons defined as>65 years and apregnant womenity; chicken and ion rate of 75% eport which covercoverage of elde
except for elderly , coverage in Beletween 70% and
2002 2003 2004 2005 20
France
ands United Kingdo
dren covered by
vaccination is curs being of influell persons living
n; persons aged pig farmers).38 Tfor the elderly.39
rs the winters 07-rly does not reachresiding in institutlgium is lower tha
d 80%), and simil
006 2007 2008 2009 2010
Germany
om United States
Belgian
main vaccinatio
rrently recommenenza complicatioin institutions; he50-64 years with
The WHO recommThe last Intermu
08 and 08-09, shoh the WHO targettions (83%). Coman in France, UK ar to the EU-15
075
80
85
90
95
100
2000 200
%ch
ild
ren
vaccin
ate
d a
gain
st m
easle
s
n Health System
ons (2000-2009):
ded in 5 ons (like ealthcare h health mends a utualistic ows that t (63% in pared to and the average
AinRfapsinn6reinBbbh
1 2002 2003 2004 2005
Belgium France
Netherlands United Kin
EU-15
Performance
international com
Accessibility of nformal carers)Relative to the 6acilities has remapersons of 65 andsector: the numben the last decade,number of beds in65 000 over the segions. In 2010, nhabitants of 65 yBrussels than in beds does not divbeds in residentiahigher in Wallonia
2006 2007 2008 2009
Germany
gdom United States
mparison
long-term care
5+ population, thained constant ov over in 2010.41 T
er of beds in home, from around 88 0n nursing homes same period. Thethe number of b
years and older wFlanders (Table
verge much betweal facilities in rela
and Brussels tha
2010 0
10
20
30
40
50
60
70
80
90
100
20
%ch
ildre
n va
ccin
ated
aga
inst
hep
atiti
s
B
U
e (residential c
he number of bever the past decaThis stable figure hes for the elderly h000 in 2000 to 64almost doubled, fere are also largebeds in homes fowas considerably 16) while the deeen the regions. Oation to the elderan in Flanders.
000 2001 2002 2003 2004 2
Belgium Franc
United States EU-15
KCE Report
care for elderly
eds in residential de, at 7 beds pehides large shifts has decreased ste 000 in 2011, whifrom around 33 0e differences betor the elderly pehigher in Walloniansity of nursing Overall, the numbrly population is
2005 2006 2007 2008 200
e Germany
5
t 196
and
care er 100 in the eadily le the
000 to tween r 100 a and home ber of much
9 2010

KCE Report 196
Table 16 – Num
Number of beds/100 inhabitants
Source: RIZIV – I
Data are availarecipient of lonbetween 6% anbetween 4% aavailable for recInformal carersactivities of daimportant cominformal carers of declining fadisabilities and The average p16.2% in Italy. and older is slig(11.7%).5 Other results aavailable on theof care, distribuleave from worelated to informAs there are custill insufficient
6
mber of accredite
Bed
Wal
s s 65 +
4.9
INAMI 2011
ble internationallyng-term care (LTCnd 7%, Belgium and 5%), and scipients of home cs, defined as p
aily living (ADL) ponent in the lois estimated to demily size, changrising participatio
proportion of inforThe Belgian ave
ghtly higher than t
are available in the web) and includution of care recipork, flexible workmal care giving. urrently no data oto evaluate the ac
ed beds in home
ds in homes for t
lonia
y for the proportioC) in residential is higher than the
similar to the Necare. people providingfor at least one
ong-term care precrease in the comes in residential n rates of women
rmal carers variederage of 12.1% othe overall averag
he documentationde data on share
pients, employmenk schedule, and
on patient needs,ccessibility of long
Belgian
es for the elderly
he elderly
Flanders
2.5
ns of population ocare. With a pere EU-15 averageetherlands. No d
g assistance withour per week,
rocess.5 The numing decades, as
patterns of peon in the labour mard from 8% in Swf the population age of the OECD-c
n sheets (Supplemof women, week
nt rate and hours mental health p
these two indicag-term care.
n Health System
y and nursing hom
Brussels
6.3
over 65+ rcentage e (that is data are
h basic are an mber of
s a result ple with rket.
weden to aged 50
countries
ment S1 kly hours of work,
problems
ators are
ATpTthcspFsda
n
Performance
mes per 100 pop
Beds i
Wallon
3.4
Accessibility of eThe last indicator palliative care is sThis can denote ehat the decision currently very littlestarted, but the tpatient can providFunds (2006) givesum occurred for death. In 20% application.42,43 Mo
n Patients who
months can babolition of physiotherap8 504 lump s
pulation 65 years
in nursing homes
nia Fl
3.
end-of-life care: tof accessibility issometimes delayeeither problems o
to start palliative information on ttime when the pde some indicationes some indication
half of the patieof the cases,
ore data are need
o stay at home andbenefit from a “palliapatient co-paymenist. The use of palum in 2004 to 20 17
s and older, per r
s
anders
3
timeliness to sta specific to end-oed until patients
of accessibility of ve care was takethe real moment w
palliative lump sun.n A study from tns: the applicationents in less than
patients died ded on this indicat
d have a life expecative statute”. It invont for nursing, GP lliative lump sums70 in 2010 (source:
region, 2010
Brussels
3.8
art palliative careof-life care. The stare in terminal pend-of-life care, een too late. Thewhen palliative ca
um is requested the Christian Sick
n for the palliative a month beforewithin the weeor.
ctancy of less than olves a lump sum an
visits and visits oat home increasedRIZIV – INAMI).
69
e tart of hase. either ere is are is for a
kness lump their
ek of
three nd the of the d from

70
3.3 Key finWorkforce • The densit
than one r/1000 popuExpressed1.95 /1000
• The densit10/1000 pothe healthcare for olnot availab
Financial acce• The cover
(99.5%), du• Between 2
rose from expenditu20.0% in 2amountedcountries total healtcountries Kingdom l
• In 2008, 14postpone glasses orfinancial a
dings
ty of practising preimbursed cliniculation in 2000 tod in full-time equ population. ty of practising nopulation in 2009care sector (37%lder persons or ible in the previo
essibility rage of populatioue to compulsor2003 and 2010, th€5.33 to €7.25 bres remained co
2003 and 19.4% in to €665 in 2010.shows that OOPh expenditures) such as France, lying below 10%4% of the househsome of their her lenses, mental accessibility. In 1
physicians (thoscal act) increaseo 2.91/1000 popu
uivalents, medica
nurses in the hea9. On 100% nurse
% in hospitals, ann nursing home us report.
on by health insury affiliation to a he out-of-pocket illion. Their shar
onstant during thn 2010. OOP exp. Comparison wit
P expenditures (ein Belgium are a the Netherlands. holds declared thealthcare (medicahealthcare) due
1997, this percen
Belgian
se who performedd slightly from 2
ulation in 2010. al density decrea
althcare sector wes, 68% were act
nd the rest in rescare). This resu
urance is very higsickness fund. (OOP) expenditu
re in total health e same time per
penditures per cath other Europea
expressed as a %at the higher ends and the United
hat they had to al care, surgery, to problems of
ntage was below
n Health System
d more 2.83
ased to
was tive in
sidential lt was
gh
ures
riod: apita an % of d, with
drugs,
10%.
C•
•
•
•
Performance
Coverage of prev During the la
cancer screeparticipation Wallonia: 7%stabilized aro
Coverage of and 2010 (62annually waschanges in rethe EU-15 av
In general, thvaccination adiphtheria-teincreased ancoverage wa
The WHO-recinfluenza is ntarget. Vaccihigher (82%)
ventive measuresast five years, theening stagnates a between region
%). Overall coveraound 60%, whichcervical cancer s%-63%), while th
s divided by 2 beeimbursement ruerage (63%) but
he WHO-recommare reached in Beetanus-pertussis,nd are now aboves still just belowcommended covnot met: 63% in tnation rates for e.
s e coverage of orgaround 30%, withs (Brussels: 12%age, including alh is far below thescreening was s
he number of tesetween 2008 and ules. Coverage inlower than in the
mended coverageelgium. The cove, poliomyelitis, he 95%. Only for m
w 95% in 2009. verage of elderly the winter 2008-2elderly residing
KCE Report
ganized breast h huge differenc
%, Flanders: 46%l mammograms,
e EU-15 target (7stable between 20sts performed
2010, due to n Belgium is withe UK (around 80
e rates of childreerage rates of
hepatitis B have measles the
vaccination aga2009 against a 75in an institution
t 196
es in %, , 5%). 007
hin %). n
ainst 5% are

KCE Report 196
Accessibility informal carers• Relative to
care facilitdecade, fr2000 to 70care, Belg5%, and isusers are
• Informal cbasic activweek, are The Belgiareporting toverall ave
Timeliness to s• There is c
palliative sSickness Ffor the palless than aweek of apinternation
6
of long-term cs) o the 65+ populaties has remainerom 71 beds per 0 beds in 2010. Wium is higher tha
s similar to the Navailable for inte
carers, defined asvities of daily livan important co
an average of 12to be an informaerage of the OECstart palliative caurrently little infostatus is requestFunds (2006) givlliative lump suma month before dpplication. More nal comparison)
care (residential
tion, the numbered more or less c1000 persons of
With 6%-7% of 65an the EU-15 aveetherlands. No d
ernational compas people providining (ADL) for at lmponent in the l.1% of the popul
al carer is slightlyCD-countries (11are ormation about tted. A study fromves some indicatm occurred for hadeath. In 20%, padata are neededon this indicato
Belgian
care for elde
r of beds in residconstant over thef 65 years and ov+ residing in res
erage, between 4data on home caarison. ng assistance wleast one hour pong-term care plation aged 50 any higher than the.7%).
the moment whem the Christian tions: the applicaalf of the patientsatients died withd (trend over timer.
n Health System
rly and
dential e past ver in sidential 4% and re
ith er rocess. nd older e
en a
ation s in in the e,
4Qacinc
44Egwth4Naoinpm4FcapC123C4
Performance
4 QUALITQuality is defined and populations inconsistent with cunto 5 sub-dimenscare and patient c
4.1 Effectiven4.1.1 How did Effectiveness is dgiven the correct who could benefit hus outcome (res4.1.1.1 PreveNo indicator provias updating this soperational objectnclude: declines programme, shiftsmortality of epidem4.1.1.2 CuratiFour indicators hacare: three indicaand one indicatorpatients with a chrCancer Care
. 5-year relative2. 5-year relative3. 5-year relativeChronic care 4. Avoidable hos
TY OF HEAas “the degree t
ncrease the likelihurrent professionaions: effectivenesenteredness.
ness of care d we evaluate the
efined as “the deprovision of evidbut not those wh
ults) indicators. ntive care des information o
set of indicators fotives of this 2012in mortality for c
s in staging at dmics for which vacive care ave been selectedtors related to thr on the effectiveronic condition (in
e survival after bree survival after cee survival after co
spital admissions
ALTHCAREto which health sood of desired heal knowledge”.6 Itss, appropriatenes
e effectiveness oegree of achievindence-based heaho would not ben
on the effectiveneor preventive care2 report. Exampcancer for whichdiagnosis of canccination exits.
d to assess the efhe survival after aeness of ambulathis case: asthma
east cancer, by strvical cancer, by slon cancer, by sta
for asthma
E services for indiviealth outcomes ant is further subdiss, safety, continu
of care? g desirable outco
althcare services nefit”. All indicator
ess of preventive e did not belong tles of such indic there is a scre
ncer and incidenc
ffectiveness of cua diagnosis of caatory services to a).
tage stage age
71
duals nd are vided
uity of
omes, to all
rs are
care, to the cators ening ce or
rative ancer,
treat

72
4.1.1.3 LonThree indicatohealthcare: 1. Suicide rat2. Rate of inv3. Participatio
employmenWith regard to are currently aprovide data soelderly being in4.1.1.4 EndSome indicatorpercentage of instance) have data available f4.1.2 Facts
This section is afor each indicawebsite).
o The Resi
assess thextended Belgium aimplemenfor long-tethe Belgia
p This indicPerformanproposed
ng-term care rs are selected
e voluntary committaon rates by peopnt the effectiveness
available at a noon on a selected residential care fd-of-life care rs have been propalliative patientbeen assessed
for this indicator. and figures
a short summary ator in the Supple
dent Assessment
he care needs of twith instruments f
a national pilot proted in all care settinerm care facilities aan situation (details cator is already meance Report 20103,2
by the OECD work
to assess the
als as a percentagple with mental i
s of long-term carational level. Hoindicator: the pre
facility or receiving
oposed by the exs for which physand controlled, b
of the detailed resement S1 of this
Instrument (RAI)44
the elderly in institfor different care oject (the BelRAI) ngs: the assessmenand acute care havin Appendix C). asured in the Neth20) and also beloning group on long-te
Belgian
effectiveness of
ge of all hospitalizllness of working
re for the elderly, owever, the BelRevalence of malnug home care (BMI
pert groups, suchsical symptoms (but there are curr
sults which are pr report (available
4 is originally devetutions, and has lasettings and subgris ongoing, but is
nt instruments for hove already been ad
erlands (Dutch Heangs to the set of ierm care quality ind
n Health System
f mental
zations g age in
no data RAIo will utrition in I<19)p.
h as the (pain for rently no
resented e on the
eloped to ater been roups. In s not yet ome care, dapted to
alth Care ndicators
dicators.45
4SepcnninecTc2bcTdreaArereuwfoc(Othbrein
q
Performance
4.1.2.1 SurvivSurvival rates aeffectiveness of thprogress in treatincancer was detecnational 5-year reno evolution of renternational compexpressed as “relacorrected for the aThe 5-year breascountries5 and has2009. In Belgiumbetween 2004 acompared to otherThe 5-year cervicdiagnosed betweeelative survival r
average (Figure 1All countries haveelative survival ovelative survival
usually higher for fwith colon cancer or males and 64colorectal cancerq
Figure 11). Only for breast cahan Belgium (datbe able to distingelative survival rnformation which
Survival rates
available in th
val after a cancefter cancer are he healthcare sysng disease over
cted, and the effeelative survival daelative survival caparisons, data refeative 5-year survivage-specific expecst cancer relatives improved in all cm, the 5-year rend 2008 was 8r European countrcal cancer relativen 2004 and 2008rates of patients 1). e also shown imver the years. Thbetween gender females.5 In Belgibetween 2004 an4.6% for female
q are very good c
ancer and colon cta shown in documuish the effect of
rates should be is not yet availabl
s after colorectal cahe OECD Health Da
er one of the k
stem and are cotime. They reflectiveness of the t
ata became availaan be given alreaer to the incidenceval years”, meanincted mortality. e survival rate iscountries betweenelative survival o88%.46 Survivalries (Figure 11). e survival rate w8. Compared to odiagnosed in 20
provement in 5-yere are difference
across countrieum, on the cohort
nd 2008, the relaties. Again, relativcompared to othe
cancer, the US hamentation sheet if early screeningcompared acrosle at international
ancer, and not specata 2012.
KCE Report
key indicators ofmmonly used to ct both how earltreatment.5 In Beable only recentlyady in this reporte year 2004. Rateng that they have
80% in most On 1997-2002 and 2of women diagnrates are very
was 69.8% for woother EU-15 coun
004 are within th
year colorectal caes in colorectal caes: survival ratest of patients diagnive survival was 6e survival rates er European cou
as higher survival in Supplement S1 from the actual s countries by slevel.
cifically colon cance
t 196
f the track y the lgium y and t. For
es are been
OECD 2004-nosed good
omen ntries, e EU
ancer ancer s are nosed 62.3%
after ntries
rates 1). To care,
stage,
er, are

KCE Report 196
Table 17 – 5Belgium
Cancer type
Female breastcancer Cervical cancer Colon cancer:males Colon cancer:females Source: Belgian C
6
5-year relative
All patients
I
t 88.0% 99
69.8% 92
: 62.3% 91
: 64.6% 96
Cancer Registry an
survival by sta
II I
.8% 93.3% 7
.2% 63.6% 5
.6% 86.1% 6
.3% 86.1% 6
d Evaluation of Can
Belgian
age, period 200
Stage
III IV
73.8% 29.2%
54.5% 17.0%
61.7% 14.5%
62.1% 16.0%
ncer Plan (Cancer C
n Health System
04-2008:
missing
73.4%
64.6%
54.5%
55.5%
Centre)46
Performance 73

74
Figure 11 – 5-y
Source: OECD HNote: results for c
Effectiveness Asthma, a chrooutpatient basiProper managexacerbation aasthma commoadmission ratescare coordinatio(healthcare quaAcross OECDadmission rateasthma admiss
year relative surv
Health Data 2012 colorectal cancer m
of ambulatory caonic condition, is s through proper
gement of asthmnd costly hospita
only serves as a ps may indicate poon or continuity.5 ality indicator) of th countries, ther
e for asthma. Fesions compared to
vival after breast
males give similar res
are for a chroniceither preventab
r prevention or pma in primary calisations. The hoproxy for primary oor effectiveness This indicator be
he OECD. re is an 11-foldmales have conso males (on avera
Belgian
t, cervix and colo
sults for Belgium
c condition ble or manageablprimary care intercare setting can ospital admission care quality. Henof primary care,
elongs to the set
d difference in sistently higher rage 85% higher).
n Health System
orectal cancer fo
e on an rvention.
reduce rate for
nce, high or poor
of HCQI
hospital rates for 5 This is
awraamc
Eph
Performance
or females: intern
also the case in Bwas 52/100 000 inates in the OECD
are slightly abovemight highlight thecare setting.
Effectiveness ofpopulation, invhospitalization an
national compari
Belgium: in 2009,nhabitants and 28D Health data (20e the EU-15 avee need for more
f mental healthvoluntary comnd working statu
ison (2004)
the asthma adm8/100 000 inhabita007) show that 48erage (47.2/100 0
effective and tar
hcare: suicide mmittals withinus of persons wit
KCE Report
ission rate for femants for males. Be8.4/100 000 inhab000 inhabitants). rgeted care in pr
rate in the gen the psychth mental illness
t 196
males elgian bitants
This imary
eneral iatric
s

KCE Report 196
Suicide rate
Despite a slig18.75/100 000 general populacountries. For tWallonia than iwithin regions highest suicideinhabitants) whFlanders (21.4/men than for years).
Figure 12 – Su
Source: DGSIE (
6
ht decrease (froinhabitants in 20ation is considethe time period ofn Flanders and Bwere also found
e rates are foundhile in Flanders /100 000 inhabitawomen, and hig
uicide rates (num
(Belgium) and OECD
m 20.05/100 000008) the number erably higher thf the analysis, su
Brussels (Figure 1d in previous resd in the province
the highest rateants).47 The suicidgher for middle-a
mber per 100 000
D Health Data 2012
Belgian
0 inhabitants in of suicide death
han in other Eicides rates are h
12). Important diffsearch. In Walloof Namur (25.4/
es are observed de rate is also hiaged adults (age
population) per
2 (international, data
n Health System
1998 to s in the uropean higher in ferences
onia, the /100 000 in East
igher for d 40-64
region (1999-200
a for Belgium only a
Performance
08) and internatio
available in 2004-20
onal comparison
005)
n
75

76
Involuntary com
The percentaobservation”; “probation”; “obetween 2000hospitalizationscompared to tWallonia 7.2%7 719 involunta(n=1 579 or 2alcohol abuse share of invol36.31%); schiconditions (n=11998) showed compared to confirmed in an
mmittal in psychiat
age of involun“internment”;
ther judicial con0 and 2009 fros (Figure 13). Tthe two other re
%). The three ary committals r20.46%); psychot
(n=723 or 9.37%luntary committazophrenia (n=1
1 270/5 747 or 22that rates of invoother European
nalyses of involunt
tric hospitals
ntary psychiatric”prolongation i
nditions”;) in Belom 5.8% to 8
The rate in Bruegions (Brussels most common
registered in 20tic conditions (n=%). The three coals in 2009 wer
579/6 274 or 22.10%). Results oluntary committan countries. Thetary committal pop
Belgian
c hospitalizationinvoluntary admgium steadily in
8.2% of all psussels is twice
14.2%, Flanderconditions amo
009 were schizo=1 270 or 16.45
onditions with thee paraphilia (5725.17%) and pbased on old dal are very low in ese results havpulation rates.
n Health System
ns (”for mission”; ncreased ychiatric as high
rs 7.7%, ong the ophrenia 5%) and e largest 7/157 or psychotic ata (year Belgium
ve been
Fh
S
Pe
Teeb(s
Performance
Figure 13 – Pehospitals, by reg
Source: FPS Public
Participation rateemployment
The last EU Laboemployment rate oemployment rate obut is ranked loweFigure 14). An up
soon.
0
2
4
6
8
10
12
14
16
2000 20
Invo
lunt
ary
adm
issi
on ra
te (
%)
Belgiu
rcentage of invion (2000-2009)
Health, Minimum P
by people wit
our Force Surveyof people with meof people with other than Norway, t
pdate of this study
001 2002 2003
um Flander
voluntary comm
Psychiatric data (RP
th mental illness
y performed in 2ental disabilities isher disabilities.29
the Netherlands, y (year 2011) is ex
2004 2005 20
rs Brussels
KCE Report
mittals in psych
PM – MPG)
s of working ag
2002 showed thas low compared tBelgium performsSweden and Por
xpected to be rele
006 2007 2008
s Wallonia
t 196
iatric
ge in
at the to the s well rtugal eased
2009

KCE Report 196
Figure 14 – Ememployment comparison (2
Source: Europea
6
mployment ratesrate of all p
2002)
an Labour Force Stu
s by health conpeople with d
udy 2002
Belgian
dition, as a ratiodisability: intern
n Health System
o of the national
4•
•
•
•
•
Performance
4.1.3 Key findi The relative s
cervix cance(62% for menrelative survicolon cancerEU-15 averag
Hospital adm2009), and Be
The suicide rEuropean cobetween 1998for women, aFor the perioFlanders and
The percentaBelgium stea8.2% of all pstwice as highFlanders 7.7%(year 1998). Tvery low in B
The last EU lperforms weemployment recent data a
dings survival 5 years r and colon canc
n, 65% for womeival rate in Europr, but the cervicage.
mission rates for elgium is just abrate is considera
ountries, even if i8 and 2008. The
and higher for miod analysed, the d Brussels. age of involuntaradily increased bsychiatric hospith as in the two ot% and Wallonia 7They showed tha
Belgium compareabour survey (inll compared to Erate of people w
are lacking.
after a diagnosiscer is respectiven). Belgium has pe for female breal cancer surviva
asthma are stabbove the EU-15 avably high compart decreased sligsuicide rate is hiddle-aged adultsrate is higher in
ry psychiatric hobetween 2000 andtalisations. The rther regions (Bru7.2%). Results arat rates of involued to other Europn 2002) showed tEU countries conwith mental disab
s of breast cancely 88%, 70% andthe highest 5-ye
east cancer, and al is lower than th
ble over time (200verage. red to other htly in Belgium igher for men ths (aged 40-64 yeWallonia than in
ospitalizations ind 2009 from 5.8%rate in Brussels iussels 14.2%, re based on old d
untary committal pean countries. that Belgium ncerning the bilities, but more
77
er, d 63% ear
he
04-
an ears). n
% to is
data are

78
4.2 Approp4.2.1 How dAppropriateneshealthcare is evidence”. The link between ouSeven indicatorScreening out o1. Breast can
(aged 40-42. Breast can
71-79) Application of g3. Follow-up o4. PrescriptioGeographic var5. GeographicMental Health 6. Average
(antidepresAggressiveness7. Proportion
days of the
priateness did we evaluate ss can be defin
relevant to the link between effe
utcomes and procrs were selected tof the target groupncer screening fo49) ncer screening for
guidelines of diabetic patientn of antibiotics acriation in surgical cal variation in ca
daily quantity ssants / antipsychs of care at the enof cancer patien
eir life
the appropriatenned as “the deg
clinical needs, ectiveness and apcesses. to measure the apps or women younge
r women older tha
ts (blood and eye ccording to guideliinterventions
aesarean sections
(ADQ) of hotics / hypnotics and-of-life nts receiving chem
Belgian
ness of care? gree to which pgiven the curre
ppropriateness ref
ppropriateness of
er than target ag
an target age grou
exams) nes
per 1000 live birt
medication preand anxiolytics)
motherapy in the
n Health System
provided ent best lects the
care:
ge group
up (aged
ths
escribed
e last 14
4
Tfow
MTtathctoTladloathpm
r
Performance
4.2.2 Facts an
This section is a sor each indicatorwebsite).
Mammograms coThe national breasargets women aghe extension of categories (70-79)o which the screeThe percentage ofast 2 years was differences acrossower (21% in 201and Wallonia (Fighose mammograpossible to distinmammograms, ba
This include
diagnosis
nd figures
hort summary of tr in the Supplem
overage outside st cancer screenied 50-69. Two re
this target grou) in Belgium.48, 49
ening is performedf women aged 40stable around 35s regions. For w0), but increasing
gure 15). It shouams are performguish between o
ased on the reimbu
es all mammogram
the detailed resultent S1 of this re
of the target groing programme se
ecent guidelines hup to younger Those two indica
d outside of the ta-49 who received
5% between 2006women 71-79 yeag, and also with hld be noted that
med for diagnostopportunistic screursement codes).
ms, for opportuni
KCE Report
ts which are preseeport (available o
oups et up since 2001-ave not recomme(40-49) or olderators reflect the erget group. a mammogramr
6 and 2010, with ars old, the ratesigher rates in Brua small proporti
tic reasons47(it iseening and diagn
stic screening an
t 196
ented n the
-2002 ended r age extent
in the large s are
ussels on of s not nostic
nd for

KCE Report 196
Figure 15 – Ma
Source: IMA-EPS
0%
10%
20%
30%
40%
50%
% fem
ales
40-49
yea
rs s
cree
ned
B
6
ammogram cove
S, KCE calculation
2006 200
Belgium Bru
rage of women a
07 2008
ussels Fland
Belgian
aged 40-49 years
2009 2
ders Wallon
n Health System
s and of women a
2010
nia
Performance
aged 70-79 years
0%
10%
20%
30%
40%
50%
2006
% fem
ales
70-79
yea
rs s
cree
ned
Belgium
s, by year and re
6 2007
m Brussels
egion
2008 200
Flanders
09 2010
Wallonia
79

80
Application of and prescriptioSeveral situatiochronic patienmanagement orecommend thmonitored prefmonths. It is alsfundus examicomplications. Oreceived a bloalbumin check.over a period consultation. Tregard to glycadiabetic patienconsultation apanalyses showthan 75 years aThe appropriateof the prescript2000s, the authphysicians concbe prescribed opreferably tenamoxicillin shou
guidelines: folloon of antibioticsons permit evalunts, in particulaof diabetic patienhat glycated haeferably once a yeso recommended nation every yOver a 15-month
ood sugar check. In the last 12 mof three years,
The recommendaated haemoglobints who are not
ppears to be an ied that guideline
and for patients in eness of therapetion of antibioticshorities have beencerning the issueonly where they ad towards first-uld be prescribed
ow up of diabetic (acute care)
uation of the quaar the integratents. For diabetic emoglobin, albumear, and never lethat an ophthalmear in order tperiod, 95% of in
k, 93% a creatinmonths 57% had
20% of patientsations are relativn. The situation is
treated with insussue for one thirs are less well foresidential care.2
utic prescription is according to gun raising awarene of antibiotic resis
are really necessa-line antibiotics. in first intention w
Belgian
c patients (chron
ality of the monited and multidis
patients, the gumin and creatiness often than e
mologist performs ato early detect nsulin-dependent nine check and
undergone a ches had no ophthavely well observs less satisfactoryulin. The ophthard of diabetics. Sollowed for patien26 is evaluated on thuidelines. Since tess among the pustance. Antibioticsary and the choice
For most indwithout clavulanic
n Health System
nic care)
toring of ciplinary uidelines nine are every 15 a dilated
ocular patients 56% an eck and, lmologic
ved with y among lmologic ubgroup
nts older
he basis he early
ublic and s should e should ications, acid.
4aTwfivwhisTamp
GinRinbth1crethfrthatw
Performance
43% of patients wantibiotics during tThe number of dawith 21.2 in 2006)irst-line. For examvery often prescrwould suffice (thehigher rate of press observed in comThere are no interantibiotics prescribmore than twice apop/day versus the
Geographic varnappropriate carResults from intern the majority of Ebirths in 2009. Behan the EU-15 a93/1000 live birth
continuously increevealed a very highe national rate wrom 2004-2007) ahis average.50 Gealso been shown wo procedures fo
who consult a Gthe year. This – hays of treatment ). Furthermore, thmple, a combinatiribed even thoug 45% has been s
scriptions to patienmparison with the rnational data for tbed per capita reas much as the e Netherlands, 11
iation in surgire: the case of canational comparisEuropean countrieelgium has a C-seaverage. In 2009hs. Despite this seasing. Moreover,gh variability betw
was 13.7% (basedand relative differeeographic variabilin Belgium for h
r which Belgium r
P receive at leasigh – figure has bis increasing (23
he antibiotics presion of amoxicillin gh a prescriptionstable since 2006nts over the age oover-75s in generthis specific indica
eveals that BelgiuNetherlands (Bel
1.4 DDD/1000 pop
ical interventionaesarian sectionson show that C-ses, with EU-15 avection rate similar9, the C-section somehow reassu, an analysis of t
ween hospitals; in d on a selection oences ranged frolity for elective suip replacement a
ranks in the top of
KCE Report
st one prescriptioeen stable since 23.9 in 2008 compscribed are not aland clavulanic a for amoxicillin
6). In addition, a of 75 in residentiaral.26 ator, but comparism is in the top 5lgium, 27.5 DDD/p/day).5
ns as evidenc
sections are increverage at 251/100r to France, and rate in Belgium
ring result, the rathe FPS Public Hthe period 2004-2
of low-risk pregnam 61% to 70% arurgical proceduresand knee replacef EU-15 countries.
t 196
on for 2006. pared lways cid is alone much l care
son of 5, and /1000
ce of
asing 00 live lower
m was ate is
Health 2007,
ancies round s has ment, .5, 51

KCE Report 196
Figure 16 – C-s
Source: OECD H
Appropriateneantidepressan
Average daily q(DDD) per 1000The prescriptioper 1000 popPrescription of
6
sections per 100
Health data 2012, ex
ess of prests
quantity of antide0 population) n of the averagepulation increasef antidepressant
00 live births: inte
xcept for Belgium 20
scriptions in
epressants prescri
daily quantity aned from 51.4 (
drugs are high
Belgian
ernational comp
009 (FPS Public He
mental hea
ribed (Defined Da
ntidepressants pre(2004) to 68.4 hest in Wallonia
n Health System
arison
ealth)
althcare:
ily Dose
escribed (2010).
a (85.9,
chInacNindm
Performance
compared to 57.1higher for femalesnternational comantidepressant coconclude from thNevertheless, thenternational contedrugs (e.g. over-monitored.
1 in Brussels and (92.8) compared
mparison shows tonsumption (seeese figures if Be
e large differenceext) pinpoint that - and undercon
d 60.7 in Flande to males (43.1).that Belgium ran
e documentationselgium is performes (between sex
the appropriatensumption) needs
ers). It is conside
nks high in terms sheet). We caming better or wxes; between regness of antidepres to be studied
81
erably
ms of annot
worse. gions; essant and

82
Figure 17 – De
Source: Pharman
Average daily per day) The prescriptio1000 populatiobetween regionAggressivenesspatients Receiving (or incancer patients
0102030405060708090
100D
aily
con
sum
ptio
n of
ant
idep
ress
ant
per 1
000
popu
latio
n
efined daily dosa
net (RIZIV – INAMI,
quantity of antips
n of antipsychoticon) to 2010 (10.5ns (higher in Brusss of care at th
nitiating) a sessios is considered un
Belgium B
Flanders W
age of antidepres
for Belgium) and O
sychotics prescrib
c medication incre5 per 1000 popusels and Walloniahe end-of-life: ch
on of chemotherapnappropriate agg
Brussels
Wallonia
Belgian
ssants per 1000 p
OECD Health Data 2
bed (per 1000 po
eased from 2004 ulation), with diff than in Flanders)hemotherapy for
py near the end-oressiveness of tre
0
10
20
30
40
50
60
70
80
DD
D p
er 1
000
pop
ulat
ion
per d
ay
Belgi
Germ
Unite
n Health System
population per d
2012 for internationa
opulation
(8.0 per ferences ). r cancer
of-life for eatment.
TisFthcwpp
um Fr
many Ne
ed Kingdom EU
Performance
ay: by region (20
al comparison
The percentage ofs an internationaFunds on end-of-lhe highest use of cancer patients wwas 12.1% for ppalliative care unitpatients who died
rance
etherlands
U-15
004-2010) and in
f people receivingally used indicatoife care for cance
f chemotherapy duwho died in hospipatients dying at ts. The lowest usin residential care
0.0 10.0
Italy
Netherlands
Luxembourg
Germany
Spain
EU-15
United Kingdom
Belgium
Finland
Sweden
Portugal
Denmark
DDD
ternational comp
g chemotherapy nor. A study of ther patients (data uring last month otal (23.1%). The home and 11.5
se of chemotherape for elderly (3.4%
40.0
40.6
44
4
20.0 30.0 40.0 5D per 1 000 population per da
KCE Report
parison (2000-20
ear the end of thehe Christian Sick2005)43,42 showed
of life was observeuse of chemothe
5% for those dyipy was seen in ca
%).
4.6
46.7
61.2
61.3
65.9
68.7
68.8
75.8
78.
0.0 60.0 70.0 80.0ay - Antidepressant (2010)
t 196
010)
eir life kness d that ed for erapy ng in ancer
.7
83.8
90.0

KCE Report 196
Figure 18 – Ch
Source: Results f
Residential ca
Palliative care un
6
hemotherapy nea
from study “De CM
0
Home
Hospital
re for elderly
nit in hospital
Last week 1m
ar end-of-life for
neemt het levensei
5 10 15%of pe
month ‐ 1 week 3
Belgian
patients with can
inde onder de loep:
20 25 30eople
3‐1 months
n Health System
ncer, by place of
de cijfers” 43
35
Performance
f death
83

84
4.2.3 Key fi• Breast can
years. Howscreened Brussels, time showoften a mamammogrand Fland18% in 200
• Over a 15-received aan albumitest and, oophthalmo
• The perceto amoxic(Brussels:very high there are cDefined Dasize exist
• CaesareanBelgium 1births), buSeveral stcaesarean
• The presc2010, withthan in Brthat Belgiu
indings ncer screening iswever, there is a before that age (46% in Wallonia
ws no real decliniammography: 21raphy in the last ers 16%). Evolut06). -month period, 9a blood sugar chn check. In the laover a period of tological consultantage of prescripillin and clavulan: 43%, Flanders: internationally inconcerns about caily Doses (DDDbetween countrin rates in Belgium93/1000 live birth
ut increasing, as udies on Belgian
n rates between hription of antide large differenceussels and Flandum ranks high in
s recommended large group of w
(36% in Belgium and 39% in Flaning trend. Older w% of 71-79 yearstwo years (Brusstion over time sh
5% of insulin-deeck, 93% a creatast 12 months 57three years, 20%ation. ption with amoxinic acid) is stable46%, Wallonia: 4
n terms of antibiocomparability of
D), especially if dies. m are lower thanhs in 2009, EU-1in the majority o
n data have showhospitals. pressants also in
es between regioders). Internationn terms of antide
Belgian
for women agedwomen who are
overall, 48% in nders). Evolutionwomen undergos old women hadsels 31%, Wallon
hows rising trend
ependent patientstinine check and7% had undergo
% of patients had
icillin alone (come, around 45% 41%). Belgium raotic prescription
f results in total oifferences in pac
n the EU-15 avera5 average 251/10
of European counwn a large variab
ncreased from 2ons (higher in Wanal comparison sepressant consum
n Health System
d 50-69
n over o less d a nia 28% ds (from
s 56% ne a no
mpared
anks n but of ckage
age (in 000 live ntries.
bility in
004 to allonia shows mption.
•
44SstoeSA1H23
O4
5P6
Fafo
Performance
The use of chdying from cThere are cufrom the Chrobserved forlowest for painterpret thisover time, reg
4.3 Safety of 4.3.1 How did Safety can be defstructures, renderso the user, proenvironment in thisSix indicators to evA generic indicato
. Medical radiatHealthcare Acquir2. Incidence of M3. Incidence of
calculated on Other safety indica4. Incidence of p
calculated on 5. In-hospital moPrescription of ant6. Percentage
antidepressanFour other indicatoare not yet measuor the next perform
hemotherapy duancer is an indicrrently no nation
ristian Sickness Fr cancer patientsatients who died s indicator correcgional difference
care d we evaluate the
fined as “the degs services, and atovider, or enviros definition extendvaluate the safetyr tion exposure of ted Infections
MRSA in hospital post-operative s
hospital dischargators in hospital pressure ulcer in hospital discharg
ortality after hip fratidepressants to eof persons age
nts using an antichors related to saferable, but data fromance report (det
ring the last daycator of the aggrenal data on this inFunds, the highe
s who died in hosin residential ca
ctly, more data aes and internatio
e safety of care?gree to which thettains results in w
onment”.4 Includids the dimension y of healthcare hav
the Belgian popula
sepsis (Patient S
ge databases)
hospitals (Patientge databases) acture
elderly ed 65 years aholinergic antidepety of long-term com the BelRAI wiltails on those indi
KCE Report
ys of life for patieessiveness of candicator. In a stuest use was spital (23.1%) andare (3.4%). To are needed on treonal comparabilit
? e system has theways that prevent ng the providerbeyond quality. ve been studied:
ation
Safety Indicator,
t Safety Indicator
and older prescpressant care for elderly pal probably be avacators in Append
t 196
ents are. udy
d the
ends ty.
e right harm
r and
PSI,
, PSI,
cribed
tients ailable ix C).

KCE Report 196
4.3.2 Facts
This section is afor each indicawebsite).
Medical radiatMedical ionisingto a large use level is measuradiation by in(2.29 mSv/pop)exposed are cabove 45 yearimaging is morinternational coare particularly
Figure 19 – Ex
Source: Europea
6
and figures
a short summary ator in the Supple
ion g radiation is parof scanner and m
ured in millisieverhabitant increase) and decreased ichronic patients, rs old. Children are frequent and omparisons show high in Belgium (
xposition to medi
an Population Dose
of the detailed resement S1 of this
rticularly high in Bmedical imaging inrts (mSv). The a
ed from 2004 to n 2011 (2.22 mSvpatients in reside
are less exposedmore intense in that average dos
Figure 19).
ical radiation per
from Radiodiagnos
Belgian
sults which are pr report (available
Belgium, in particn general. The irraverage level of 2009, stabilized
v/pop). The patienential care, and . Prescription of Wallonia.26 Resuses of medical irr
r inhabitant (mos
tic Procedures – Re
n Health System
resented e on the
ular due radiation medical in 2010
nts more persons medical
ults from radiation
Tin
nm
Ey
S
st 20 exams, exp
esults of Dose Data
Performance
Table 18 – Exposn nb mSv): Belgi
20
nb mSv/inhab.
2.0
Evolution year (X+1)/X
Source: RIZIV – INA
pressed in mSv):
med 2 (http://ddme
sition to medicaium (2004-2011)
004 2005 2006
00 2.01 2.11
0.4% 4.6%
AMI
international co
d.eu/_media/results
al radiation per in
6 2007 2008
2.18 2.25
% 3.6% 3.4%
omparison
s:ddm2_results_irpa
nhabitant (expre
2009 2010 2
2.29 2.29 2
1.6% 0.1% -2
a13v2.pdf)
85
essed
2011
2.22
2.9%

86
Healthcare-acqHealthcare-acqAccording to th(ECDC, www.ethe EU and abinfection. The urinary tract gastrointestinalthe acute hospiwere infected bavailable at thethe ECDC. In Belgium, su ISP, and is oInfections in Hacute care hosepsis, belongsIncidence of MRA decreasing incases/1000 adreaching 4.3 instatistically signacute care hoduring the secohospitals particdecrease of -0.decrease was application of tactually in revrationalization oNevertheless, tscreening prachospitals.53
quired infectionsuired infections he European Cecdc.europa.eu) ea
bout 37 000 of thmost frequent ty
infections, pne infections. In Beitals occurred in 2by a HAI.52 New e end of 2012, ba
rveillance of HAIsorganized by theospitals). For MR
ospitals (since 20s to the set of safeRSA ncidence was foudmissions), after n 2003. Since 2nificant decrease spitals, finally reond semester of ipating at least at29 new cases/10most impressivehe recommendatvision), the natioof the use of antithe interpretation ctices which vary
s (HAI) occur after e
entre for Diseaseach year 4 million
hem die as the dypes of HAIs areeumonia, bloodlgium, the last pre
2007, and showedresults of preval
ased on a commo
s is under the ree NSIH group (RSA, the surveilla007). The third ety indicators from
nd between 1994r which the inc2003, we measur
of the incidenceeaching 1.5 new 2010 (test for lin
t 5 surveillance pe000 admissions, p in the Brussels ions for the contr
onal hand hygiebiotics influencedof the indicator r
y in coverage rat
Belgian
exposure to hea Control and Pre
n patients acquire irect consequenc
e surgical site infstream infectionevalence survey id that 6.2% of the ence are expecteon protocol devel
esponsibility of thNational Surveillance is mandatoindicator, post-o
m the OECD.
4 and 1999 (from idence again inre a slow, const of nosocomial Mcases/1000 adm
near trend for a ceriods since 2003p<0.001) (Figure 2
hospitals. Probarol of MRSA (sincne campaigns, a
d positively this evemains influencedte and intensity b
n Health System
althcare. evention a HAI in
ce of the fections, ns and n half of patients
ed to be oped by
e WIV –ance of
ory in all operative
4.1 to 2 ncreased tant and MRSA in missions cohort of 3: annual 20). This ably, the ce 2003, and the volution. d by the between
NdSo
Performance
No international odifficult. An excSurveillance Systeon nosocomial acq
rganisations incluception is the em (EARSS), but quisition.
ude data on MRSEuropean Antithis European pr
KCE Report
A, making compamicrobial Resisrogram does not
t 196
arison tance focus

KCE Report 196
Figure 20 – Me
Source: National
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
5
nosocomial M
RSA/10
00 adm
issions
Source
6
ean incidence of
Surveillance of Infe
in
4,1
3,23,4
2,6
2
1994
/2
1995
/1
1995
/2
1996
/1
e: National surveilla
Healthcare Acqu
ections in Hospitals
MRcidence of nos
2,2
32,7
2,9
2,1
1996
/2
1997
/1
1997
/2
1998
/119
98/2
ance, B. Jans
Belgian
uired MRSA, per
(NSIH), WIV – ISP
RSA in Belgisocomial MRS
1 2
2,4 2,42,2
2
1999
/1
1999
/2
2000
/1
2000
/2
n Health System
r 1000 admission
an acute caSA (clinical sam
2,6 2,6
3,5
44,3
2001
/1
2001
/2
2002
/1
2002
/220
03/1
Surveil lance pe
Performance
ns (1994-2010)
are hospitalsmples) per 100
3
3,74
33,3
2
2003
/2
2004
/1
2004
/2
2005
/1
200
/2
eriods
s: 00 admissions
2,7
3,4
2,52,8 2,7
2005
/2
2006
/1
2006
/220
07/1
2007
/2
72,4
2,2 2,1 2,2
1
2008
/1
2008
/2
2009
/1
2009
/2
2010
/1
1,81,5
2010
/1
2010
/2
87

88
Patient Safety Incidence of poIncidence of posafety in hospitthe basis of hoon Belgian dataBetween 2000 around 8 casesother Europeanbut it is unclearin coding of secIncidence of preThe occurrencenegative impachospital stay. Pcare.58, 59 This ibe calculated bon the accuracyThe global rate2000 and reachfor both surgicavailable on theOther data thaestimate prevaorganised for tAdvisory Panepressure ulcersincluded 19 96observed. Conmeasurements,incontinence apressure ulcers
Indicators (PSI) ost-operative sepsost-operative septal (Patient Safetyospital discharge da, although with a and 2007, the inc
s per 1000 admissn countries which r whether this is dcondary diagnoseessure ulcer e of a pressure ulct on the individuPressure ulcers cndicator also belo
based on dischary of the coding pra
e of pressure ulcehed 17/1000 staysal and medical he OECD Health Dan administrativelence of pressurethe first time, foll guidelines (spes). This study wa64 patients. A pntrary to previo, no distinction w
associated dermas was 7%.60
sis psis is an internaty Indicator, PSI)54,
data. This indicatslightly different m
cidence of post-opsions. However, w
provided data, Bdue to higher incids.
lcer in a hospitalisual’s health57 andcan be prevented ongs to the set of ge data, but its aactices in hospita
ers in acute hospits in 2007, with inchospitalisations. Nata for Belgium.
e discharge datae ulcers. In 2008lowing the last E
ecific for registratas organized in 8ressure ulcer pr
ous Belgian prewas made betweeatitis. The preva
Belgian
tional indicator of 55, which is moni
tor has also beenmethodology.56 perative sepsis wawhen compared toBelgium ranks rathdence rates or diff
sed patient has ad often leads to a
with appropriatesafety indicators
accuracy largely dls. tals was 12/1000 creasing trends oNo more recent d
abases are avaia prevalence stu
European Pressution and classific
84 hospitals in 20evalence of 12.1
essure ulcer preen a pressure ul
alence of grade
n Health System
f patient tored on
n studied
as stable o the few her high, ferences
a serious a longer nursing that can depends
stays in over time data are
lable to udy was re Ulcer
cation of 008, and 1% was evalence lcer and 2 to 4
InHwfrtesin2hPaWmpaaeUecasgDapWcoeainpd
Performance
n-hospital mortaHip fractures are fwith an importantracture gives direechnical quality osafety, and seconn-hospital mortalit2004 and 2007. Thhospitals.50 Patients aged 65an anticholinergiWhile elderly indimedications, they physiological chanantidepressants wamitriptyline and delderly as they canUse of these ageeffects, including considerable influappropriateness osystem can be inguidelines.61, 62 During the last 5 yanticholinergic sidpercentages are Wallonia (11%) ancomparisons are hof consensus aboeffects.63,64,65 Nevantidepressants wnvestigation. Propsychopharmacolodocumented befor
ality after hip fracfrequent causes ot mortality risk. Bect information abof care, it is first cndly as an indicatty rate after a hiphere was also a h
5 years and oldec antidepressanividuals can be are at greater ris
nges associated with strong antidoxepin) are not n cause orthostatents has been afalls, among eld
ence over this inof prescribing behcreased through
years the prescripde-effects for eld
consistently hignd Brussels (10%hampered by absout what is an anvertheless, the
with (potential) antblems with the aogical drugs in re66 and should be
cture of disability in eldeBecause in-hospbout outcomes anconsidered as an tor of quality-effec fracture was 6.3
high variability in m
er prescribed ant drug (%) treated effectivel
sk of adverse druwith the aging cholinergic effecrecommended fo
tic hypotension, seassociated with hderly patients. Thndicator, as it is haviours by cliniceducation and tr
ption of antidepreerly (≥65 years) her in Flanders
%). It should be nsence of availablentidepressant witrelatively high
ticholinergic side appropriateness
the elderly poe a continuous are
KCE Report
erly and are assocital mortality aftend indirectly abouindicator of in-ho
ctiveness of care% in Belgium bet
mortality rates bet
ntidepressants u
ly with antidepreg reactions due tprocess. In particts (e.g., imipraor ongoing use iedation and confuhigh rates of adhe health systemtreatment-based
cians within the hraining and the u
essants known foris stable (14%).(17%) compare
noted that internae data but also byh anticholinergic prescription rateeffects warrant fuof the prescriptioopulation have ea of attention.
t 196
ciated er hip ut the ospital . The tween tween
using
essant to the cular, mine, n the usion. verse
m has . The health use of
r their . The ed to
ational y lack side-
es of urther on of been

KCE Report 196
4.3.3 Key fi• The averag
2009, stab(2.22 mSv/patients inChildren amore frequinternationradiation a
• A decreasobserved increased decrease odecrease w
• Incidence patient safdischarge operative Belgium racountries,practices
• Incidence pressure ureached 17for both su
• The in-hosBelgium bhospitals. data are av
• During thefor their anstable (13-compared
6
indings ge level of medic
bilized in 2010 (2./pop). The patienn residential careare less exposeduent and more innal comparisonsare particulary hsing incidence in between 1994 anin 2003. Since 2
of the incidence was most impresof post-operativfety (PSI) which data. Between 2
sepsis was stabanks high in com but this might bbetween countriof pressure ulce
ulcers in acute h7/1000 stays in 2urgical and medspital mortality rabetween 2004 and
More data are nvailable for bence last 5 years thenticholinergic sid-14%). The perce to Wallonia (13-
cal irradiation inc.29 mSv/pop) andnts more at risk ae, and persons a. Prescription of
ntense in Wallons show that averaigh in Belgium. healthcare-acqund 1999, after wh2003, we measure
of MRSA in acutssive in the Brus
ve sepsis is an inis monitored on
2000 and 2007, thle around 8 case
mparison with otbe due to large des. er is another PSIospitals was 12/
2007, with increaical hospitalisatiate after a hip frad 2007, with largeeded on trends
chmarking at intee prescription of de-effects for eldentages are high-14%) and Bruss
Belgian
creased from 20d decreased in 2are chronic patiebove 45 years ol
f medical imagingia. Results from age doses of me
uired MRSA was hich the incidence a slow and conte care hospitalsssels hospitals.nternational indic
the basis of hoshe incidence of pes per 1000 admiher European ifferences in cod
. The incidence r/1000 stays in 20asing trends overions. acture was 6.3% e variability betw
s over time, and fernational level.antidepressants
derly (≥65 years)er in Flanders (1els (10%).
n Health System
04 to 2011 ents, ld. g is
edical
ce again nstant s. This
cator of spital post-issions.
ding
rate of 000 and r time
in ween few
s known is 6-17%)
44CoaSths
IndtoMmohRmeCp
SaIn1
M2
R3
Performance
4.4 Continuity4.4.1 How didContinuity addressover time, is smoand regions”4, andSeveral aspects ohat continuity is skills, and good co
nformational conduring current pato another and fromManagement contmost commonly worganisational bouhealth problem)69;Relational continumore providers thevents68; Coordination: the professionals or be
Six indicators thatare presented: nformational cont. Percentage o
DMG) Management cont2. Percentage o
within a 6-weeRelational Continu3. Proportion of
most frequent
y of care d we evaluate the
ses “the extent toothly organised w
d to which the entiof continuity havethe result of goo
oordination of care
tinuity: availabilitient encounters; im one health evetinuity: coherent dwhether follow-upundaries (often fo
ity: an ongoing rehat connects care
integration, coordetween provider o
t assess the four
inuity of persons who h
tinuity of hospital discheks period for senuity
encounters that tly: Usual Provide
e continuity of cao which healthcawithin and acrossre disease traject
e been distinguishod information floe.67-72
y and use of danformation links cnt to another70;
delivery of care frop visits are madocus on care pla
elationship betweee over time and
dination and shareorganisations.70
above-mentioned
have a global m
arge followed wnior patients (65+)
were conducted r Continuity (UPC
are? re for specified u
s providers, institutory is covered.1 hed, based on theow, good interper
ata from prior ecare from one pro
om different prove when care cro
an for specific, ch
en patients and obridges discontin
ed information bet
d aspects of cont
edical record (G
ith a GP’s enco)
by the GP consC) index.
89
users, utions
e fact rsonal
events ovider
iders, osses hronic
one or nuous
tween
tinuity
MD –
ounter
sulted

90
Coordination 4. Proportion
meeting 5. Number of
schizophre6. Number of
the 3 last m4.4.2 Facts
This section is afor each indicawebsite).
Informational cSince 2001, thentrust a GP wGMD – DMG inlarge differenceBrussels 28%).(78% coveragreimbursement
of cancer pati
f re-admissions penia or (b) bipolar f contacts betweemonths of his/her
and figures
a short summary ator in the Supple
continuity he global medicalwith the task of mncreases progreses between regi The coverage by
ge for the 75+(entitled 54% ver
ients discussed
per 100 patients disorder
en the GP and thelife
of the detailed resement S1 of this
l record (GMD –managing their me
sively and reacheons (Flanders 5y the GMD – DMG
+), and personsrsus not entitled 4
Belgian
at the multidis
with a diagnosis
e palliative patien
sults which are pr report (available
DMG) allows patedical data. The ued 46% in 2009 8%, Wallonia 31G is higher for thes entitled to in44%).
n Health System
ciplinary
s of (a )
nt during
resented e on the
tients to use of a but with
1%, and e elderly ncreased
F(
S
M
LApthrewreckfr
Performance
Figure 21 – PercGMD – DMG), by
Source: RIZIV – INA
Management con
Link Hospital-GPsAs hospitalisation person, a GP’s enhe U.K.73 We haelevant in Belgium
with a GP in the wegion, this perce
continuity of care bknow if the GP’s erom the patient’s o
centage of popuy region (2006-20
AMI
ntinuity
s discharge is a p
ncounter in the 6 wave adapted the m. A majority of eweek after a dischentage is lower (4between the hospencounter followeown initiative.
ulation with a gl009)
pivotal moment inweeks following ddefinition to one elderly (58%) havharge from the ho42.5%). This res
pitals and the first ed a discharge pla
KCE Report
lobal medical re
n the care of an discharge is advis
week, which is ve at least one coospital. In the Brusult is an indicati
line, even if we dan from the hospi
t 196
ecord
older sed in more
ontact ussels on of
do not ital or

KCE Report 196
Figure 22 – Pand over) foldischarge, by
Source: IMA – EP
Link GPs-speciSince 2007, preimbursement are referred bycertain specialimeasure aims tand to stimulateare free to go specialist consincreased reimspecialists). Thproportion of re
6
Percentage of holowed by a coregion (2003-200
PS, KCE calculation
ialists patients with a of health expend
y a GP. The meaists and to one cto improve the spe a first encountedirectly to the s
ultations identifiebursement is veryis result does not
eferrals between G
ospitalisations fontact with a G
09)
n
GMD – DMG aditures for a spec
asure is limited in consultation per
pecialist-general per with a GP becasecond line. Howd as prescribed y small (around 2t allow drawing aGPs and specialis
Belgian
or the elderly (aP within 1 wee
re entitled to acialist consultation
scope: it appliesyear per special
practitioner’s collaause in Belgium,
wever, the percenby a GP and lea
2% of all consultany conclusion on sts. However, it dr
n Health System
aged 65 ek after
a larger n if they s only to ist. This
aboration patients
ntage of ading to ations at the real
raws the
abph
R
AtocsfolooinIntwo2mthresFTpcre
CMmpisgms
Performance
attention to a reimbetween GPs apercentage found heavy administrati
Relational contin
A longitudinal relao encourage compliance, and bservices and decror patients with ongitudinal continof the most commnterpretation. n the population owo years, aroundout-of-hours conta2009. It reaches 5meet the less strinhe time (UPC ≥ 0egions, with a gr
same GP at leastFlanders (71%) anThese results alsprovider of care iscoverage rates ofelational continuit
Coordination: MuMultidisciplinary temany countries aspatients receive tis evidence-basedguidelines develomultidisciplinary dstaging and treat
bursement measuand specialists.
in the data are ive burden.
nuity
ationship betweencommunication,
behavioural problerease hospitalisat
chronic diseasenuity with the Usuaon index used. Th
of patients who hd 44% have seenacts). This perce55% for patients ngent criteria of ha0.75). Some differreater proportion t in 75% of the cnd a smaller proposo show that ths good and stablef the GMD – DMGty with the GP.
ultidisciplinary teeam meetings (Ms the predominantmely diagnosis ad, and that thereoped by the Kiscussion is recoment plan of can
ure aimed at facilPossible explaa lack of knowle
physician and paimprove sati
ems, and stimulattions and emergee.74 There are al Provider of Cahe advantage of t
ad at least 3 conn the same GP (nentage was stableaged 65-84 years
aving seen the sarences are observof patients havin
cases (UPC ≥ 0.7ortion in Brussels he relational cone over time. It alsoG in Wallonia do
eam for cancer pOC – COM) havet model of cancernd treatment, tha
e is continuity ofKCE and the Commended to decncer patients. Sin
itating the coordinnations for the edge by GPs or
atient is acknowleisfaction, medicte receipt of preveency department several measurere (UPC) index ashis indicator is its
tacts with a GP dnot taking into ace in the period 2s. 72% of the pame GP at least 75ved between the
ng encounters wit75) in Wallonia (7(66%).
ntinuity with the o shows that the not implicate a w
patients e been implementr care to ensure that patient managef care.75 In all caCollege of Oncocide on the diagnnce its introducti
91
nation low
a too
edged cation entive visits
es of s one easy
during count 2003-tients 5% of three
th the 74%),
main lower worse
ted in hat all ement ancer ology, nostic, on in

92
2003, a clear discussions abOverall, about 6in 2008, with labreast cancer pan increasing ufrequently discfollowed by Wa
Table 19 – Perregion, (2005-2
Source: Belgian CNote: all tumours
0%
10%
20%
30%
40%
50%
60%
70%
80%
%M
OC-
COm
Bel
increase of its bout how to bette69% of cancer paarge variations bpatients, 74% lunguse is noticed for acussed at the MOallonia (63% in 200
rcentage of canc2008)
Cancer Registry ans excl. non-melanom
2005 2
gium Bruss
use is noticed fer involve GPs
atients were discuetween types of g cancer, 59% proall three regions, OC – COM in F08) and Brussels
cer patients who
d evaluation of Canma
006 200
els Flanders
Belgian
for all cancer typare currently con
ussed at the MOCcancer (in 2008:
ostate cancer).46 Acancer patients a
Flanders (74% in(56% in 2008).
had a MOC – CO
ncer Plan46
07 2008
s Wallonia
n Health System
pes and nducted.
C – COM 84% of
Although are more n 2008),
OM, per
CAhainaHcdpcuTdaara17(eab
CW(ancGfrshoh
8
Performance
Coordination: MeAlthough unforesehealth, mental heaan indicator of poon receiving data, ravailable for this reHospital readmisscomplications follodisorders since thplanning: follow-ucoordinated beforeup visits after discThe re-admissiondisorders within taround the OECDand 15.6% for bipates are the high9.7%) and lowes
7.1%). For schizoespecially in Flan
an increasing trenbipolar disorders a
Coordination: EnWith the regulationat home or in a
needed for the ccontinuity of care. GPs during end-orom different stushows that 72% ohad a contact withof contacts betwehigher in the Nethe
ental health careeen and unavoidalth related emergor coordination of results on the EReport. They will be
sion rates are alsoowing an inpatienthey indicate premup care and sue discharge) or laharge). n rates for patithe 30-days of
D-average of EU-polar disorders). hest in Flanders (st in Brussels (s
ophrenia, there is nders and Wallonnd in Flanders. Tare decreasing in
nd-of-life of pallian of palliative careresidential setting
coordination of sThere are currenf-life of palliative
udies. A study onof the palliative pah a GP during theeen palliative paterlands than in Be
dable emergenciegency room (ER)care and service
R use for mental he analysed for theo widely used as t stay for psychiatature discharge (upport have no
ack of continuity o
ents with schizothe initial hospit
-15 countries (20For both conditio
(schizophrenia 25schizophrenia 10.
an overall increania). For bipolar dThe re-admission
Wallonia.
ative patients e services in the rg) a more prominservices. This is tly no national dapatients but somn Christian Sicknatients who died e last week of theients and their Gelgium.76
KCE Report
es do arise in m) admission is usefailures. Due to dealth problems ar
e next update. proxies for relap
tric and substance(sub-optimal dischot been approprof services (e.g. fo
ophrenia and btalisation are situ
0.2% for schizophons these readmi5.2%; bipolar diso.2%; bipolar disoasing trend in Bedisorders, there isrates for patients
esidence of the pnent role of the G
thus an indicatta on the contactse results can be ness Funds memat home in 2005-ir life.42, 43 The nu
GP appeared how
t 196
mental ed as
delays re not
pse or e use harge riately ollow-
ipolar uated
hrenia ission orders orders lgium
s only s with
atient GP is tor of s with given
mbers -2006
umber wever

KCE Report 196
4.4.3 Key fi• The contin
stimulatedin Belgiumshows an particularlpersons eimproved,
• The managinterestinghospitalisahave at leaBrussels c
• The relatioparticularl
• The coordmultidiscipatients, wbreast can
• The coordservices (ecommunitpatients waround theFlanders.
• The coordshould be lacking anpalliative psituation t
6
indings nuity of medical d since 2001 by tm. Since its introd
increasing trendly reaches the vuntitled to increas especially in Brgement continuig indicator, overaation discharge, ast one contact wcompared to the onal continuity wly in the age grou
dination of care foplinary oncology
with large variationcer), and betweedination of mentae.g. assertive coty. The re-admiss
with schizophrene OECD-average
dination of palliatat the level of th
nd some studies patients and theito the Netherland
information manthe global medicduction, the used. Moreover, the ulnerable populased reimbursemerussels and in Wty between hospall for elderly. W a majority of eldwith a GP. Resultwo other region
with the same GPup 65-84 years aor cancer patieny meetings for abons between typen regions. al health care reqommunity care; fosion rate within tia and bipolar di
e, with higher and
tive care at homehe GP. However, showed less conir GP when they ds.
Belgian
naged by GPs is al record (GMD –of the GMD – DMGMD – DMG
ation (elderly andent) but it could allonia.
pital and GPs is aWithin one week a
derly patients (58ts are however lns. P is good in Belgand in Wallonia. ts is organised bbout 69% of canc
pes of cancer (89
quires a broad arollow-up by GPsthe same hospitasorders are situad increasing rate
e or in nursing hnational data ar
ntacts between compared the B
n Health System
– DMG) MG
d be
a after a 8%) ower in
ium,
by cer
9%
rray of s) in the al for ated es in
omes re
Belgian
44PreeAin•
•
•
T1
2
3
Performance
4.5 Patient C4.5.1 How did Patient-centeredneesponsive to ind
ensuring that patieAccording to this ndicators: Acknowledge
right; patientsspiritual suppaspects; comf
Providers skipatients carecourtesy/respto relieve feapoor commun
Patients and care and to mpatients/carersupport; patiepatients involvdecision or sh
Three indicators re. Percentage o
satisfied with 2. Percentage o
controlled 3. Percentage o
or institution)
Centeredness d we evaluate pa
ess is defined as dividual patient pent values guide a
definition, sever
ment of patientss’ needs; preferenport; cultural neefort; social supporll of communicatefully; providersect; spent enough
ar and anxiety; lnication.
carers involvememake informed ders information; ents/carers involvevement in quality
hared decision-maelated to centeredof population abhealthcare servicef adult inpatients
of patients dying i
atient centeredne“providing care thpreferences, neeall clinical decisionral categories are
s needs, wants, nce of care; pain eds; patients’ strrt. tion: providers ab
s ability to exh time to their patianguage; global
ent (enabling patecisions about thinformed conse
ement in services y improvement; paaking. dness are availablbove 15 years oes who reported ho
n their usual plac
ess? hat is respectful oeds, and values,ns”.6 e used to classif
preference: patmanagement; pri
rengths; psycho-s
bility to listen to xplain things client; emotional sucommunication
tients to manageeir treatment opt
ent; self-manageand delivery plan
atients’ participati
le: old who report t
w often their pain
ce of residence (h
93
of and , and
fy the
tients’ ivacy; social
their early;
upport skills;
their ions):
ement nning; ion in
to be
n was
home

94
4.5.2 Facts
This section is afor each indicawebsite).
Patients’ satisPatients have healthcare provthese issues. Apatient’s experused measure iBelgian citizenstheir contact w90% for contacOnly for hospitaDifferences berespect to agebetween socioeLarge differenclocation of the rural areas. Alsalways higher observed in Bru
and figures
a short summary ator in the Supple
faction often other ex
viders and their Although patients’ rience with the hin evaluating paties reported in the
with the healthcarcts with GP, dentals the satisfactionetween men and e are limited. Teconomic groups. ces are however patient: satisfacti
so, large differencein Flanders than ussels.
of the detailed resement S1 of this
xpectations, wishsatisfaction depsatisfaction is onealthcare systements’ care experieHIS that they are
re system: the satists, specialists an level is lower (87
women are negThe satisfaction l
observed with reon is systematicaes exist between in Wallonia. Low
Belgian
sults which are pr report (available
hes and prioritieends of the ans
nly one limited aspm, it is still a veryence.77, 78 e in general satisfatisfaction level iand home care s7%). gligible. Differenclevel also hardly
egard to the geogally lower in citiesregions, as satisf
west satisfaction ra
n Health System
resented e on the
es than swers to pect of a y widely
fied with s above services.
ces with y differs
graphical s than in faction is ates are
Fs
S(
PPTcth6dwascmcp
Performance
Figure 23 – Degreservice (2008)
Source: Results fromWIV – ISP)
Pain control Pain control or paThe RN4CAST-prcountries) of nurshe patient survey68%.79 Results shduring their hospiwas always well caverage of 54% fostudy show that 4controlled. Less thmajority of patientcould to help thempatients).
ee of satisfaction
m Health Interview S
ain assessment isroject included a ses and patients. y, with 2 623 patihowed that 69% tal stay and amo
controlled. This plaor the 8 countries47% of the patienhan 2% said thets considered tha
m with their pain (
n with healthcare
Survey, Scientific In
s paramount in aone-off internatioSixty Belgian ho
ients surveyed anof patients need
ong them 41% deaces Belgium vers who participatednts said that their ir pain was neve
at the hospital staalways 71% of pa
KCE Report
e services, by ty
nstitute of Public Hea
a patients’ perspeonal survey (Euroospitals participatnd a response raded medicine foreclared that theirry low compared td. Other data frompain was usually
er controlled. Theaff did everythingatients; usually 23
t 196
ype of
alth
ective. opean ted in ate of r pain r pain to the m the y well e vast g they 3% of

KCE Report 196
Place of deathPlace of death care. A surveyexpressed a pnational data palliative care certificates (pal(2007) on thes(55.1% of all de(18.3% in 1998remained stableof deaths in nresidential beds
Table 20 – EvBrussels (1998
Period
1998 2007 Source: A study o
There are largedeath of patienhome is very lohigher in the Ne
6
is considered an
y showed that in preference for dypublished on the
in Belgium. Dlliative or not) in
se death certificateaths in 1998 to 58 to 22.6% in 20e.81 The decline inursing homes cs by skilled nursin
volution of plac8-2007)
Home H
23.0% 522.5% 5
on death certificates
e differences betwnts with cancer. Tow in Norway (1etherlands (45%).
n important indicaFlanders, 71.6%
ying at home.80
e place of deathata are howeveFlanders and in tes showed a sh51.7% in 2007) to007). The percenn hospital beds acan be explainedng beds in care ho
ce of death over
Hospital NuHo
5.1% 181.7% 22s in Flanders and B
ween countries wThe percentage of
3%), higher in Fl
Belgian
ator of quality of p% of persons inte
There are curreh of patients eliger available fromBrussels. A rece
hift from dying in o dying in a nursinntage of deaths aand the increased d by the substit
omes.
r time in Flande
ursing ome
Oth
8.3% 3.6%2.6% 3.1%Brussels 81
with regard to the f cancer patients landers (28%) an
n Health System
palliative erviewed ently no gible for m death ent study
hospital ng home at home number
tution of
ers and
her
% %
place of dying at
nd much
4•
•
•
•
Performance
4.5.3 Key findi There is curr
The few meainformation o
Belgian patiethe healthcaravailable in t
One survey ipain. The vasstaff does ev(always 71%
A recent studshowed a shThe percentalarge differendeath for patdying at hom(28%) and mu
dings rently a real lack surable indicatoof a complex subents are in generre system. Data ohe new wave of n hospitals showst majority of patverything they ca
of patients; usudy on death certiift from dying in
age of deaths at nces between cotients with cance
me is very low in uch higher in the
of data on patieors only providedbject. ral satisfied with of the patients’ ethe Health Interv
wed a relatively gtients considere
an to help them wally 23% of patieificates in Flandehospital to dyinhome remained
ountries with regaer. The percentagNorway (13%), he Netherlands (4
nts’ centerednesd fragmented
their contact witexperience will bview Survey. good managemed that the hospit
with their pain ents). ers and Brusselsg in a nursing hostable. There areard to the place ge of cancer patihigher in Flander5%).
95
ss.
th be
ent of tal
s ome. e of ients rs

96
5 EFFIC5.1 How diEfficiency is de(i.e. money, tim(macro-level) amaximum beneThree indicatosystem: 1. Percentage2. Rates of on3. Length of hOther indicatorefficiency of theoutside target g
5.2 Facts a
This section is afor each indicawebsite).
Utilisation of leThe price of geof the original which a generretail price to thpaid by the prescription ofexpenditures, bon their speciacertain minimuintroduced in 20
IENCY IN Hd we evaluate
efined as “the degme and personnand ensuring th
efits or results (calrs measure spe
e of prescription one-day hospitalisahospitalisation for rs already mentioe health system (fgroups for breast c
and figures
a short summary ator in the Supple
ess costly drugseneric drugs is midrug. Low-cost d
ric alternative exihe reimbursementpatient; (2) genf low-costs drugboth for the third-palty, physicians aum percentage o006 and revised (
HEALTHCAthe efficiency gree to which theel, called input)
hat these resourlled output)”.4, 8 cifically the effic
of low-cost drugs iations for surgery a normal delivery
oned above can afor instance the cocancer screening)
of the detailed resement S1 of this
s in ambulatory cnimally 31% less
drugs are definedsts and which ht basis so that theneric drugs and s is thus a goparty payer and foand dentists are f low-cost drugshigher) in Decem
Belgian
ARE in healthcare? e right level of reis found for the
rces are used
ciency of the he
n ambulatory sett
y also help to illustoverage of mamm).
sults which are pr report (available
care expensive than t as (1) original dave lowered there is no suppleme
copies. Promotood way to limitor the patient. Derequired to pres
, the so-called “ber 2010.
n Health System
esources
system to yield
ealthcare
ting
trate the mograms
resented e on the
the price drugs for ir public ent to be ting the t health
epending scribe a “quotas”,
Bap4w
Performance
Between 2000 aambulatory settingperiod, the propo46.0% in 2010 (2which lowered the
and 2010, the g increased from rtion of low-cost
27.1% from geneir price).
total number of2.76 billion to 4.7DDD continuous
ric drugs and 18
KCE Report
f DDD prescribe7 billion. On the sly increased to r8.9% as original d
t 196
ed in same reach drugs

KCE Report 196
Figure 24 –ambulatory se
Note: DDD DefinSource: RIZIV – I
Utilisation of hospitalisationCarrying out elcircumstances etc.) saves moconsidered as aThe Belgian su2008. The coincreasing trend25).
6
Percentage oetting (DDDs) (20
ed Daily Doses INAMI, Pharmanet
less costly infn) lective procedure(e.g. inguinal her
oney on bed occan indicator of effiurgical day-case rmparison with ods, with Belgium
of low-cost me00-2010)
frastructures (on
es as day cases rnia repair, circumcupancy and nursciency.
rate grew from 42other European higher than the E
Belgian
edication delive
ne day versus
when allowed bymcision, cataract sing care. It is t
2.1% in 2004 to 4countries shows
European average
n Health System
ered in
classic
y clinical surgery, herefore
46.2% in s similar e (Figure
Performance 97

98
Figure 25 – Pe
Source: OECD H
Utilisation ofhospitalisationThe length of sorganisation acharacteristics to benchmark thIn Belgium, thedecreased from1.5 day above t
0
10
20
30
40
50
60
70
2000
surg
ical
day
cas
e ra
teercentage of surg
Health data 2010 82,
f less costly ns) tay after a norma
and care providonly (e.g. severityhe efficiency of the duration of hos
m 5 days in 2000 the EU-15 averag
0 2001 2002
Belgium
Netherlands
EU 15 - Average
gical one-day hos
except KCE calcula
infrastructures
al delivery is deterder characteristicy of illness). It is t
he healthcare systspitalization for ato 4.3 days in 20
ge of 2.9 days (Fig
2003 2004 200
France
United Kingdom
Belgian
spitalisations on
ation for Belgium 20
s (shortening
rmined more by facs than clinical therefore a good item. a normal delivery008. This is approgure 26).
05 2006 2007
Germany
United States
n Health System
n all surgical hos
008
classic
actors of patient
indicator
y slightly ximately
2008
United
Performance
spitalisations: int
0% 10
Germany
Spain
Finland
Ireland
EU-15
Belgium
Denmark
Kingdom
ternational comp
25%
0% 20% 30Surgical
parison
%
36%
39%
41%
42%
46
0% 40% 5 day care rate (2008)
KCE Report
6%
50%
58%
0% 60% 7
t 196
70%

KCE Report 196
Figure 26 – Av
Source: OECD H
5.3 Key fin• The perce
increased • The perce
in one-dayThese incris situated
• The duratidecreasedapproxima
0
1
2
3
4
5
6
2000
aver
age
leng
th o
f sta
ys in
day
s
6
verage length of s
Health Data 2012
dings ntage of low-cosfrom 7% in 2001ntage of surgicay hospital grew freasing trends a
d above the EU-1ion of hospitalizad from 5 days in 2ately 1.5 day abo
2001 2002 2003
BelgiumNetherlands
stay for a norma
st drugs in ambu1 to 46% in 2010.al hospitalisationfrom 42.1% in 200re observed ove5 average.
ation for a norma2000 to 4.3 days
ove the EU-15 ave
2004 2005 2006
FranceUnited King
Belgian
al delivery: intern
ulatory setting
ns that were perfo04 to 46.2% in 20
erall in Europe. B
al delivery slight in 2008. This is erage of 2.9 days
6 2007 2008 2009
Germgdom Unite
n Health System
national compari
ormed 008.
Belgium
tly
s.
9 2010
manyed States
Performance
son
0
United KingdomNetherlands
IrelandSweden
SpainDenmarkPortugal
EU-15Finland
GermanyItaly
LuxembourgAustriaFrance
Belgium
Single spon1
ntaneous delivery -(20
1.81.9
2.12.42.5
2.72.7
3.13.23.2
3
2 3average length of
009)
3.54.04.1
4.34.5
4 5stay in days
99

100
6 SUSTASYSTE
6.1 How disystem
Sustainability is• To provide
education a• To be inno• To stay du• To be respFor all four eleThe last indicafinancial sustainMaintenance of1. Evolution o2. Medical gra3. Nursing graMaintenance of4. Acute careInnovation 5. Number of Financial Susta6. Health exp
(Total, repa
AINABILITEM d we evaluate
m? s defined as the sy and maintain infrand training, facilivative; rably financed by
ponsive to emerginements of the deator, total healthnability. f workforce over time of the maduates becomingaduates f facilities
e bed days (numbe
GPs using an eleainability penditures accordartition, % gross d
Y OF THE
the sustainabi
ystem’s capacity: rastructure such aties and equipme
collective receiptsng needs. efinition, specific ih expenditures, is
ean age of practisg GPs
er per capita)
ectronic medical fi
ding to the Systdomestic product
Belgian
HEALTH
lity of the healt
as workforce (e.g.ent;
s;
indicators were ss a generic indi
sing GPs
le
tem of Health A(GDP), per capita
n Health System
th
through
selected. cator of
Accounts a)
6
Tfow
M
Ta2mpin
F
NS
Performance
6.2 Facts and
This section is a sor each indicatorwebsite).
Maintenance of w
The cohort of activage, as shown by2009 of physicianmeasuring this chpractising. The avn 2009, while it wa
Figure 27 – Age d
Note: only GPs with Source: Performanc
d figures
hort summary of tr in the Supplem
workforce: GPs
ve GPs is changiny the lines superis with over 1 250
hange is to calcuverage age of full as 47.3 years in 2
distribution of GP
more than 1 250 coce of general medici
the detailed resultent S1 of this re
ng: it is very fast aimposed for the y0 contacts (Figurlate the average time equivalents
2000.
Ps (2000-2004-20
ontacts /year ine in Belgium, a ch
KCE Report
ts which are preseeport (available o
approaching retireyears 2000, 2004re 27). Another w
age of GPs cur(FTE) was 51.4
009)
heck up (RIZIV – INA
t 196
ented n the
ement 4 and
way of rrently years
AMI)26

KCE Report 196
Table 21 – Mea
Number of GPsmoothed FTEMean age Source: Performa
One of the reasnew GPs. As arelated to the nand, of these, tof newly-gradugraduates entearea in the twoyear study cyc34% in 1996.26
Table 22 – Pro
Graduates afte
number of phyphysicians wit% physicians wphysicians witspecialists (SPgeneralists (G%GP compareSource: RIZIV – I
Compared to ograduates (all) the 11.5/100 00
6
an age of practis
2000
P E
8 515
47.3 ance of general med
sons for this agein matter of fact, th
numbers of new pthe percentage eated generalists ring general med
o years following gle). This percenta
ogression betwee
er 2 years
ysicians (after 7 ythout specialisatwithout specialisth a specialisatioP) P)
ed to GP +SP INAMI
ther European coof 9 medical grad
00 pop EU-15 ave
sing GPs (2000-2
2004 2
8 472 8
49.2 5dicine in Belgium, a
ng of GPs is the pe non-replaceme
physicians enterinntering general mis calculated by c
dicine to all gradugraduation (upon age currently stan
en 1996 and 2008
years) tion sation on (GP+SP)
ountries, Belgium duates per 100 00erage (Figure 28).
Belgian
009)
2008 2009
8 336 8 28
51.3 51.4a check up (RIZIV –
problematic recruint of older GPs is
ng the medical promedicine. The percomparing the nuates entering a scompletion of the
nds at 30%, whil
8 of graduates in
1
has a number of 00 pop, slightly low
n Health System
9
83
4 INAMI)26
tment of s directly ofession rcentage umber of specialist e seven-e it was
n medicine in the
1996 1998
1 105 1 2193 17%
912 988600312
34%
medical wer than
Performance
e two years follow
8 2000
35 1 172 247 220% 1
8 970 628 6360 3
36% 35
wing graduation
2002
1 180 202 2117% 18%
969 632 684338 2855% 29%
according to typ
2004 20
1 142 811810%
1 024 7756268
26%
pe of specialisat
006 2008
814 941 11014%
704 781 493211
30%
101
ion
160 17%
554 227
29%

102
Workforce: nuThere is currenon workforce complemented example of micworkforce studyhospitals nursecompared to ot
Figure 28 – Me
Source: OECD H
0
Netherlands
Spain
Belgium
United Kingdom
Finland
Italy
EU-15
Portugal
Germany
Denmark
Ireland
rsing ntly no indicator at
in nursing. Hwith data that re
cro-level data is y based on surves have, on avher EU countries.
edical and nursin
Health data 2012
2 4 6Medical gra
t the macro level tHowever, macro-eflect the situatiothe recent largeey data. It was i
verage, to take 79
ng graduates (pe
8
8
9
9.3
11
11
11.5
12
1
8 10 12duates per 100 000 pop
Belgian
to document the q-level data sho
on at the micro le-scale European llustrated that in care for more
er 100 000 pop): i
5
2
12
16
18
14 16 18pulation (2010)
n Health System
question ould be evel. An nursing Belgian patients
CthsEthn
international com
20
Lu
Unite
N
Performance
Contrary to the GPhe education sidstudents every yeaEU-15 average ofhis figure, as alsonot work in Belgium
mparison (2010)
0.0 1
Italy
uxembourg
Spain
Germany
EU-15
ed Kingdom
France
Portugal
Ireland
Netherlands
Belgium
Finland
Number of Nurs
Ps, the source of de, as Belgium far, where the numf 31.3. A word of o foreign studentm.
16.2
19.9
20.9
2
10.0 20.0 30.0ing graduates per
this problem doeforms a very higmber for 100 000 i
caution is necests are counted, a
8.2
33.2
33.2
34.4
34.8
36.7
40.1
41.7
0 40.0 50.0100 000 population
KCE Report
es not seem to begh number of nuis 41.7, high abovsary when interprnd those will pro
58.7
60.0 70.0n (2010)
t 196
e from ursing ve the reting
obably

KCE Report 196
Maintenance oThe number opopulation’s neinfrastructure. TIn 2009, there hospitalisation acute care bedand stable sin1 day/inhabitanhigher utilisatio
Figure 29 – Ac
Source: OECD H
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
2000
Num
ber o
f acu
te c
are
bed
days
per
cap
ita
6
of facilities: numof acute care beeed for acute cThis indicator indicwere 13 million donly, excluding o
d days. This figurnce 2003. The t. Of the neighbn of acute care ho
cute care bed day
Health data 2012
0 2001 2002 200
Belgium
Netherlands
EU-15
ber of acute beded days per cacare beds, and cates how this nedays spent in acuone day). Per care is decreasing bEU-15 average bouring countriesospitals per inhab
ys per capita, int
3 2004 2005 200
France
United Kingdom
Belgian
d days pita is indicativethus about the ed is met.
ute care hospitals apita, this represebetween 2000 anis a bit lower,
s, only Germanyitant.
ternational comp
06 2007 2008 200
Germany
United States
n Health System
e of the needed
(classic ents 1.2 nd 2003,
around y has a
parison
09 2010
s
Un
Performance
0.0
FinlandNetherlands
SpainIreland
ItalyPortugal
nited KingdomFranceEU-15
BelgiumLuxembourg
AustriaGermany
0.5Number of a
1.0acute care bed da
1.5 2.0ays (2009)
103
0

104
Innovation: thetheir patients’ The percentagsoftware to ma2004 to 74% in
Table 23 – Pmaintain their
% of GPs who received a lump sum for using an electronic medical records. Source: RIZIV – I
Total healthcsustainabilityTrends in healtthus sustainainternational deOECD’s Systemat measuring coHealth Accounexpenditures inPer capita, this€3430/inhabitandata are also eFinally, the shadomestic produin 2003.
e percentage of medical records
ge of GPs usingintain their patien2010.
Percentage of Gpatients’ medica
2004
61%
INAMI
care expenditu
h expenditure areability. For inteefinitions for healm of Health Accouonsumption of heants are only comncreased from €27s represents an int in 2010. To alloexpressed in 200are of Total Heauct (GDP) accoun
GPs using an els g an electronic nt’s medical recor
GPs using recoal records
2008 20
72% 75
ures as an i
e an important indernational compthcare and healtunts (SHA) are clalth and long-termmparable since 7.6 billion in 2003ncrease from €26ow comparisons
05 US$ Purchasinalth Expendituresnts for 10.5% of G
Belgian
ectronic file to m
file with recomrd increased from
ommended softw
009 2010
5% 74%
ndicator of f
icator of affordabparisons, the shcare expenditurassically used. SH
m care services. 2003. The tota
3 to €37.3 billion 660/inhabitant in between countrieng Power Parities (THE) in Belgia
GDP, compared to
n Health System
maintain
mmended m 61% in
ware to
0
%
inancial
ility, and standard re of the HA aims
l health in 2010. 2003 to
es, these s (PPP). an gross o 10.0%
Performance KCE Reportt 196

KCE Report 196
Table 24 – Tota
Absolute amou
Per capita
Per capita (US$
% GDP
Source: OECD H
More than half care (HC.1) or contributors arecomponent, no(mainly pharma
s Roughly s
performingsocial cardaily livingLTC into iprovided tensure cocare, the O
6
al health expend
nts (in billions €)
$ PPP)
Health Data 2012
of the total healtrehabilitation caree services for lonot the social comaceuticals product
speaking, one couldg activities of dailyre as care helping ig (IADLs) (e.g. shoits health and sociato LTC recipients h
omparability of the SOECD issued speci
ditures according
2003 27.6023
2660.18
3026.8
10.0
h expenditures (5e (HC.2). The follong-term care (LTC
mponent, HC.3, 20ts, HC.5, 17%).
d define healthcarey living (ADLs) (e.individuals perform
opping, laundry, …)al components is chhave both a healthSystem of Health Aific guidelines.24
Belgian
g to the System o
2004 200529.4811 30.60
2828.97 2920
3155.5 3246
10.1 10.1
53%) is spent for owing two most imC) (specifically th0%)s and medica
e as care helping ing. dressing, eatinging instrumental ac). In practice, the dhallenging as manyh and social compoAccounts (SHA) for l
n Health System
of Health Accoun
5 2006 064 30.5214
0.84 2893.59
6.8 3277.6
9.6
curative mportant e health
al goods
ndividuals g…), and ctivities of division of y services onent. To long-term
FS
S
E1eh
Performance
nts (2003-2010)
2007 200832.2427 34.59
3034.41 3230
3423.3 3698
9.6 10
Figure 30 – HealSystem of Health
Source: OECD Heal
Expressed as a p5 average. But
expenditures, as healthcare expend
2009 992 36.303
.56 3362.48
.4 3911.4
10.7
lth expendituresh Accounts (2010
lth Data 2012
ercentage of the caution is need
the better and thditures, the higher
2010 37.3737
3430.17
3968.8
10.5
s in Belgium by 0)
GDP, Belgium isded when compahe more exhaustr the level of these
main function in
s very close to thearing total healthtive the registratie expenditures.
105
n the
e EU-hcare on of

106
Figure 31 – To
Source: OECD H
02468
101214161820
200
Tota
l hea
lth e
xpen
ditu
re a
s %
GDP
Be
Ne
EU
otal health expen
Health data 2012
00 2001 2002 200
elgium
etherlands
U-15
ditures as a % o
03 2004 2005 200
France
United Kingdom
Belgian
f GDP: internatio
06 2007 2008 20
Germany
m United St
n Health System
onal comparison
009 2010
y
tates
Un
Performance
n
0%
FinlandIreland
ItalySweden
nited KingdomGreeceEU-15
BelgiumPortugal
AustriaDenmarkGermany
FranceNetherlands
E2% 4%
Expenditure Healt
9%99
6% 8% 1th care - % gross
(2010)
KCE Report
%9%9%10%10%
10%10%11%11%11%11%
12%12%
12%
0% 12% 14%s domestic produ
t 196
%uct

KCE Report 196
6.3 Key fin• Concernin
challenginis currentlsince 2000ageing of number ofin anotherpercentagand is actu
• The numbhigh in Bepopulationpopulationwill proba
• The analyshigh utilisthere werehospitalisarepresentsEU-15 ave
• The innovthe percenpatient’s m2004 to 74
• Concerninexpendituin 2010. Pe€2 660/inhhealth expaccounts fclose to th
6
dings ng the Belgian heng since GPs arely 51.4 years. Th0, when it was 47GPs is the problf graduates who r specialty was 7e of graduates inually (2008) 29%
ber of nursing graelgium comparedn compared to thn but the foreignbly not work in Bsis of the mainteation of acute cae 13 million daysation only, exclus 1.2 acute care
erage (1 bed day/ative perspectiventage of GPs usimedical record. T4% in 2010. ng the financial sres increased froer capita, this re
habitant to €3 430penditures in Belfor 10.5%, comphe EU-15 average
ealthcare workfoe aging. The averis average age h7.3 years. One ofematic recruitemspecialize either
781 in 2008. Amon general medici. aduates per 100 d to other EU-15 he average EU-15 students are co
Belgium. enance of the facare hospitals pers spent in acute cuding one day). Pbed days in 2009/inhabitant). e of the health syng an electronic
This percentage
sustainability, theom €27.6 billion presents an incr0/inhabitant in 20lgian gross domeared to 10.0% in e.
Belgian
orce, some resultrage age of FTEshas risen very rapf the reasons of tment of new GPsr in general medng these graduaine was 34% in 1
000 population icountries: 41.7/15 of 31.3 /100 000
ounted although
cilities shows a rr inhabitant. In 20care hospitals (cPer capita, this 9, a bit higher tha
ystem is measurc file to maintain
increased from 6
e total health in 2003 to €37.3
rease from 010. The share oestic product (G2003, which is v
n Health System
ts are s of GPs pidly this
s. The icine or
ates, the 996
s very 100 000 0 they
relative 009,
classic
an the
red by their 61% in
billion
f total DP)
very
7
7
AepewinisT••••••
t
Performance
7 PERFORPROMO
7.1 How did wpromotion
According to the enabling people toprocess of health efforts that a sociewhole range ofnterventions), situs also largely situaThe guiding princip Participation Empowermen Sustainability Multistrategic Equity Multisectorial
In Belgium, t
depending onCommunities
RMANCE OOTION
we evaluate then? Ottawa charter23
o increase controlpromotion is com
ety does to promof interventions
uated for a considated outside the sples of health pro
nt
the “health promotin the Health Admins.
OF HEALT
e performance
3, “health promotl over, and to imp
mplex and can beote the health of t
(e.g., policies, erable part outsid
so-called “health pmotion are the fol
on sector” is reprenistrations and Minis
H
e of health
tion is the proceprove their health”e understood as ahe citizens. It cov
law, environmde the health systepromotion sector”t
llowing:
esented by the strustries of the Region
107
ess of ”. The all the vers a mental em. It t.
ctures ns and

108
Several framewindicators. Nutpromotion indicindicators (hea(health literacyoutcomes (heato final health mortality, and sadopted the Ncorresponds laCharter.23 In the context evaluation of hcomplete studyof a limited set we illustrated smost distal frolifestyles are epresent resultshealth promotio
works have beenbeam83 has propcators in 4 broalth promotion acty, social influenlthy lifestyle, effecand social outco
social health likeutbeam’s framew
argely to the bro
of this project, itealth promotion i
y in itself. With regof indicators and
some categories oom action outco
easier to documes for more proxion outcomes).
n proposed to cposed a framewoad classes rankions), through hence and policiective health servicomes (physical h
e well-being and work to classify thoad axes and p
t has not been pin Belgium since gard to the limitatunavailability of d
of the Nutbeam’s omes like health nt, we also tried imal indicators (
Belgian
classify health prork that classifiesing from most p
ealth promotion oues), intermediateces and healthy shealth like morbidequity). In this whe indicators, beprinciples of the
possible to perforthis would neces
tions we faced (codata for many indframework. Althooutcomes and
to define indicatas healthy envir
n Health System
romotion s health proximal utcomes
e health settings), dity and
work, we cause it Ottawa
rm a full ssitate a onstraint dicators), ough the
healthy tors and ronment,
Performance KCE Reportt 196

KCE Report 196
Figure 32 – ThThe Nutbeam’s
Source: adapted “Health promotion
6
e Nutbeam’s fras framework
from the Nutbeam n actions”, the last c
mework and sele
framework83 category in the Nutb
Belgian
ected indicators
beam’s framework,
n Health System
to measure perfIn
H•••
InH••••H•••
H•••
is not represented h
Performance
formance of healndicators selected
Health and SocialOverweight anDental health:Incidence of H
ntermediate HealHealthy Lifestyles
Daily smokersAlcohol consuPhysical activiNutrition (fruits
Healthy EnvironmeComposite indPercentage ofOffer of physic
Health PromotionHealth LiteracSocial influencHealthy publiPolicies Scale
here
lth promotion d and classified w
l outcomes nd obesity decayed, missing
HIV
lth outcomes
s umption ity s and vegetables)ent dex of health promf schools with a pacal activity at seco
n outcomes cy: health literacy lce and action: pooc policy and or
e
ithin the Nutbeam
g, filled teeth at ag
)
motion policies in tarticipative healthondary school
level (not measuror social supportrganisation pract
m framework
ge 12
the municipalities promotion team
ed)
tice: Tobacco Co
109
ontrol

110
7.2 Facts a
This section is afor each indicawebsite).
7.2.1 HealthFour important described abovexpectancy, heas they are less
Overweight an
Adult populationIn 2008, 47% considered as and almost 14%on the reportedthan in womenwomen. Although the oaverage EU-ratfor age, the rateregions, but theAs for other indlack of physical
and figures
a short summary ator in the Supple
h outcomes indicators of ge
ve in the chapter ealth expectancy, s specific to health
nd obesity
n (aged 18 years of the Belgian pbeing overweight
% was consideredd weight and hei. For obesity, no
obesity and overte, they gradually e of obese peoplee difference tendsdicators related to activity, a strong
of the detailed resement S1 of this
eneral health outcon the health staself-perceived he
h promotion.
or older) population (aged t or obese (Bodyd as obese (BMIight. Overweight differences were
rweight rates areincreased over ti
e is higher in Walls to have decreaso overweight, like social gradient is
Belgian
sults which are pr report (available
come have alreadatus of the populaealth and infant m
18 years or oldy Mass Index (BM≥30). Results aris more frequentfound between m
e slightly lower time. After standaronia than in the tw
sed over time (Figpoor nutritional h
s observed.
n Health System
resented e on the
dy been ation: life mortality,
der) was MI) ≥25), re based t in men men and
than the rdization wo other gure 33). habits or
Performance KCE Reportt 196

KCE Report 196
Figure 33 – Pe(2000-2008
Source: Health In
Overweight andThe HIS surveoverweight andisp.be/epidemiooverall 18% ofoverweighed abetween gende
Dental health: DMFT is an intof dental cariesprevalence and
6
ercentage of the
nterview Survey, Sc
d obesity in childreey provides inford obesity in youno/epifr/CROSPFRf the young peond 5% was foun
ers.
decayed, missinternational index s in an individuald is obtained by
adult population
cientific Institute of P
en and adolescenrmation about thng people (2-17
R/HISFR/his08fr/9.ople (aged 2-17 nd to be obese. T
ng, filled teeth (Ddescribing the aml. DMFT numericacalculating the
Belgian
n (aged 18 years
Public Health (WIV –
nts he overall preval
years) (https://w.etat%20nutritionnyears) are foun
There was no di
DMFT) at age 12mount – the prevaally expresses thnumber of Decay
n Health System
or older) with ob
– ISP), and OECD H
ence of www.wiv-nel.pdf): d to be ifference
alence – e caries yed (D),
MmIns(inpyaTM
Performance
besity (BMI ≥30),
Health Data for inte
Missing (M), Fillemaximum mean Dn a national survesample of 30 child1.0) from a previon 2001. Neverthelpermanent teeth. year-olds (n=95). analysis by sex, reThe number of stuMoreover, the sco
, by region (1997
rnational compariso
ed (F) teeth (T). DMFT score belowey performed in 2dren aged 12 waous study based oless, 43% of theseThe mean DMFTThe very small
egion or by socioeudies performed pe is often limited
7-2008), and inter
on
WHO goals set w 1.0 for 12-year-o2009-201084, the mas 0.9 (± 1.37). Ton a large sample e children had sigT score was 1.3
sample does noeconomic status.in Belgium to dat
d to small selected
rnational compa
for the year 20olds. mean DMFT scorehis confirms the performed in Flan
gn(s) of dental car(± 1.82) for the 1ot allow any stra
te still remains limd areas.85
111
rison
010 a
e in a result nders ries in 12-14 atified
mited.

112
Incidence of HHIV is an imporserious morbidand shortened since the transmsex, safe injectindicator of the In Belgium, thediagnostic ratelong after the inThe diagnostic100 000 inhabitproportion of nobeing a mix of non-Belgian ca(such as Sub-Snon-Belgian caas a failure oexplanation foranalysis is nee3-4 per 100 000Figure 34 (a aregion from 19rates in Flandeincrease is obsmuch higher thaof a large city, whigh HIV-rate isrates in the twsemi-urban andFor Belgian phomosexual co
HIV rtant communicabity, high costs oflife expectancy.
mission is largelytion). Therefore, isuccess/failure of true incidence ra. This is an appr
nfection (the HIV-ic rate in Belgtants. Belgium on-Belgian casesresident and non
ases originate fromSaharan African ses are imported of health promor the large numbeeded. For Belgian 0 inhabitants. nd b) show the e85 to 2010, for a
ers and Wallonia served in Flandean in the other regwith the socio-culs a usual phenom
wo other regions rd urban contexts. patients, the mosntact (see Supple
ble disease in Eurf treatment and cIt is also a perf
y avoidable by beits incidence in af health promotion
ate is not known, aroximation since nfection remaininium for all cashas the particu
s (60% of cases w-resident people.
m countries with acountries). Partscases, and as sution in Belgium.er of imported ca cases only, the
evolution of the dall cases and for are quite comparrs since 1997. Tgions. The Brussetural characteristi
menon observed represent an ave st frequent way
ement S1).86
Belgian
rope. It is associacare, significant mfectly avoidable inhavioural measurdefined populatio
n. and is approachethe diagnostic cag long asymptomses is around larity to have with a known natA large proportio
a high prevalence of this large nuuch cannot be int. There is no cases in Belgium. rate is fluctuating
diagnostic rate ofBelgian cases o
rable. However, aThe rates in Brusels region mainly ics of an urban coin large towns. T
erage of rates fro
of infection wa
n Health System
ated with mortality nfection, res (safe on is an
ed by the an occur atic). 10 per a large ionality),
on of the e of HIV
umber of erpreted clear-cut
Further g around
f HIV by nly. The a steady sels are consists
ontext. A The HIV-om rural,
as male
Performance KCE Reportt 196

KCE Report 196
Figure 34 – Dia
Source:Scientific
6
agnostic rate of
Institute of Public H
HIV by region, fo
Health (WIV – ISP)
Belgian
or all cases (a) an
86
n Health System
nd for Belgian ca
Performance
ases only (b) (1985-2010)
113

114
Figure 35 – Ra
Source: OECD H
ate of the new HIV
Health Data 2012
V diagnosis per
Belgian
100 000 inhabita
n Health System
ants: Internationa
Performance
al comparison
KCE Report
t 196

KCE Report 196
7.2.2 Interm7.2.2.1 HeaDaily smokersThe percentagewhich is slightlysince 10 years,from 31% in 19remained stablefound in highlyas high as for tthe data in this 21 and 24 yearsThe comparisoin Flanders than
Alcohol consuThe consumptio• Percentage
excessive men and 1
• Percentagereporting aaddiction b
• Percentagerisky single
The percentagearound 8%. Hbehaviour (tendconsumption bedrinking is highe
6
mediate health oalthy Lifestyle
s e of daily smokey lower than the E, mostly in men, 997 to 23.7% in e until 2004. The -educated peoplethe rest of the popage group reveals, a priority targetn between regionn in the other regi
umption on of alcohol is ase of men and woalcohol consumpt4 glasses/140g a e of the non-abst
a problematic alcobased on CAGE sce of the populatioe-occasion drinkine of excessive a
However, the radency to addictionehaviour is more est in the 15-24 a
utcomes
ers was around 2EU average. It hain whom the rate2008. The rate idecrease in the
e. The rate of smpulation. Howevels that smoking prt for prevention. ns shows that theions.
ssessed on the bamen aged 15 yeation (more than 2week in women);inent population (
ohol consumption cale, 2+ cut off);87
on (aged 15 yeang (≥ 6 drinks) at lealcohol consumptte of people w
n) is increasing, mtypically masculin
age group.
Belgian
20% in Belgium as significantly de
of daily smokingn women is lowerate of smoking is
moking in young pr, a closer examinrevalence peaks b
e rate of smoking
asis of three indicaars and over repo1 glasses/210g a ; (aged 15 years a(defined as a tend7 ars and over) repeast once a weektion has remaine
with problematic mostly in Brussels.ne. Risky single-o
n Health System
in 2008, ecreased g passed er, but it s mainly
people is nation of between
is lower
ators: orting an week in
nd over) dency to
porting a k. d stable drinking
. Alcohol occasion
To
D
Ebq
Dsw
S
Performance
Table 25 – Alcoholder) (1997-2008
Drinks alcohol in
Exhibits problembehaviour (CAGEquestionnaire)
Drinks 6 or more single occasion aweakly
Source: Health Inter
ol consumption 8)
excess
matic drinking E
drinks in a at least
rview Survey, Scien
habits for the po
1997 2001
7% 9%
7%
tific Institute of Pub
opulation (aged
2004 200
9% 8%
8% 10%
8%
lic Health (WIV – IS
115
15 or
08
%
SP)

116
Figure 36 – Pevegetables dai
Source: Health In
0%
5%
10%
15%
20%
25%
30%
Adjus
ted %
of pe
ople
eatin
g 2 fr
uits &
200g
ve
getab
les da
ilyercentage of theily, (d) performin
nterview Survey 200
2004
Belgium Bruss
e population (a)ng at least 30 min
08, Scientific Institut
sels Flanders
Belgian
smoking daily, n of physical act
te of Public Health (
2008
Wallonia
n Health System
(b) with problemivity per day, by
(WIV – ISP)
Performance
matic alcohol coregion (1997/200
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Age-a
djuste
d % of
peop
le pr
actis
ing at
leas
t 30 m
in of
phys
ical a
ctivit
y per
day
Belg
onsumption, (c)01-2008)
2001
ium Brussels
consuming at le
2004
Flanders
KCE Report
east 2 fruits and
2008
Wallonia
t 196
d 200

KCE Report 196
Consumption The consumptcomplementary• Percentage• Percentage• Percentage
and 2 fruitsThe daily conshas progressevegetables. Altconsumed is fa200g vegetablerecommendatioaccording to thfruits or vegetaPlan90).
Physical activiStrong evidencmore active pedisease, high bcolon and breasactivity is difficuindicators raisechanged in thecurrently availaon physical actiThe global percminutes of any There is a lotmoderate) physwomen. There practising (at leWallonia (27%)
6
of fruits and vegtion of fruits a
y indicators: e of the populatione of the populatione of the populatios per day. umption of fruits d over time, anthough this is aar too low. Only 2es and 2 fruits dons (which are “he “Actieve Voedables, according t
ity ce demonstrates ople have lower rlood pressure, strst cancers, and dult to measure. Thed many questione next (E)-HIS. Mble. This being saivity in Belgium. centage of peopletype of (at least m
t of room for imsical activity rate
are important reeast moderate) p) or Brussels (22%
getables nd vegetables
n reporting to eat n reporting to eat n reporting to eat
and vegetables nd reaches 65% n encouraging p25% of the peopdaily, which is a“300g vegetables
dingsdriehoek”,88
to the WHO89 an
that compared torates of all-causeroke, type 2 diabeepression.91, 92 Buhe questionnaires
ns and criticism. TMoreover, very feaid, we present th
e (15 years or momoderate) physica
mproving this glois almost twice a
egional differencephysical activity in%).
Belgian
is expressed b
fruits daily; vegetables daily;
t at least 200g veg
(in the whole popfor fruits and 8
progression, the ple reports to eat a proxy of the nus and 2 fruits por five portions o
nd the Belgian Nu
o less active ind mortality, corona
etes, metabolic syut the quantity of s and the developThe questionnaireew international dhe currently availa
ore) practising at al activity per day
obal level. The (as higher in menes with a highern Flanders (45%)
n Health System
by three
getables
pulation) 84% for quantity at least
utritional per day” of either utritional
dividuals, ary heart yndrome,
physical pment of e will be data are able data
least 30 y is 38%. (at least n than in r rate of ) than in
7Ind"SoIt••Tpsdmosa
InTaRwpemhssimv
Performance
7.2.2.2 Healthn Flanders, the Vdeveloped a set ofhealth promotion"
Such indicators fopposed to the ust is in line with two Developing he Developing he
Three specific thphysical activity. Tseen globally as dimensions. Theymunicipalities, whover time can alschools, results caaged Children (HB
ndex of health pThe municipalitiesauthority. Results are only weighted sum ofpromotion policieseating and physmunicipalities scohealthy eating (gloscore=50%). The some municipalitiemportant to furthvariability, in order
hy Environment Vlaams Instituut vf global indices ai" in several settinfocus on public ual measures of ho axes of the Ottaealthy public policealthy environmenhemes were anaThose indicators a summary resul
y can be used asich can comparelso be followed an also be obtaineBSC) studies in W
romotion policies represent the m
available for Flaf “good” answerss at municipality-sical activity), r
ore low for tobaccobal score=36%),average scores
es doing nothing,er analyse the rer to intervene effic
voor Gezondheidsming to measure ngs (schools, wor
health authoritiehealth behaviour).awa charter:23 cies nt alysed: smoking,of health promotlt, or can be decs an (auto)-evalue themselves to t
(with caution). Fed from the Health
Wallonia and Bruss
es in the municipmost close-to-the-
anders. The scores to questions -level (in the fielrange between co prevention (gl, a bit better for phide a large disp, and others perfeason for those
ciently.
spromotie (VIGeZthe level of intens
rk, and municipales responsibilities.
, healthy eatingtion in settings cacomposed into spuation indicator fothe others. The trFor the indicatorh Behaviour in Scsels.
palities -citizen level of p
es, that represenrelated to the hd of tobacco, he0 and 100%.
lobal score=37%)physical activity (gpersion of scoresforming very welllow rates and fo
117
Z) has sity of ities). s (as
and an be pecific or the rends rs on chool-
public
nt the health ealthy
The ) and global s with . It is
or the

118
Percentage of The percentagcalculated sepaphysical activitpromotion as aHowever, the seFor Flanders, report:93 • The existe
the secondeating andgroup are “the health
• Whatever tcomposed team as su
• However, feedback oand parentin the decsuggestion
From the VIGepromotion is imparents are selexist. The authimplemented. In Wallonia and(HBSC) studycollaboration wyoung people'scontext. A parenvironmental directors.
schools with a hges of schools arately for 3 themety. The existencea whole cannot eparate indicatorsthe following res
nce of such a wodary schools (42%d 54% for physic“to give advice topromotion policiesthe theme, in themostly of teacher
uch. other participatio
of the discussionsts. In almost half
cisions. In 38% tns. eZ report we can mplemented in a ldom part of thos
hors conclude tha
d Brussels, the Hy is a cross-nawith WHO-Europe.s health, well-bert of the survey context of the s
health promotionwith activities ines: smoking prevee of a working gdirectly be dedu
s are a good proxysults are extracte
orking group is rat% for smoking preal activity; the m
o the Direction” ors of the schools”.
e majority of schors; parents and st
on mechanisms es of the working gof the schools, thhey only can giv
conclude that a majority of scho
se groups, other pat the participatio
Health Behaviour ational research. The HBSC aims
eing, health behais devoted to th
school, and is a
Belgian
n working groupn health promotention, healthy eagroup working onuced from those y of the situation.
ed from the VIGe
ther good implemevention, 64% for
main roles of the r “taking part in se
ools, the working tudents are not pa
exist for the studgroup is given to she students can tve their opinion o
working group foools. While studeparticipation mec
on culture is quite
in School-aged h survey condus to gain new insaviours, and thehe health strateganswered by the
n Health System
tion are ating and n health
results.
eZ 2009
mented in r healthy working
etting up
group is art of the
dents: a students ake part or make
or health ents and hanisms e largely
Children cted in
sight into ir social
gies and e school
In2hreAHspTisd
O
PSpth
Performance
n the French spe2010, 44 secondhealth related proetained as perform
Almost half of the However, it seemstudents are onlyparticipation are mThis point could bes an essential dimension should
Offer of physical
Physical activity inSchools can offephysical activitieshe VIGeZ 2009 re
eaking part of Bedary schools direojects conducted mance indicators schools report th
ms that the particiy implied in 7.7%maybe present, be explored more pdimension in thbe further improv
activity at secon
n young people iser many opportu. For Flanders, theport93.
elgium (Wallonia ectors were interin the school. Socould be extracteey have a permaipation of student
% of the cases. but were not partprofoundly in the e success of h
ved.
ndary school
s an important heanities to young he following resu
KCE Report
and Brussels) srviewed regardingome indicators thaed from the report.nent health cell (4ts is quite poor, Other mechanismt of this questionfuture. As particip
health promotion,
alth-enhancing acpeople to engag
ults are extracted
t 196
urvey g the at we . 40%). since
ms of naire. pation , this
ctivity. ge in from

KCE Report 196
Table 26 – Offe
Education
Supply
Reglementatio
Participation
Networking
Total
Note: The table ppromotion dimenresulting from thescore of “supply”score of the physpercent), represeof physical activitand 100, and shohealth promotion Source: VIGeZ re
In summary, wphysical activityare generally inthe dimension Nearly 100% oinsufficient spacmore problema2006, the acces
6
er of physical ac
N Minim
416 .00
416 .00
on 416 1.21
416 .00
416 .00
416 8.74
provides an overviewsions. Those partiale weighted sum of “gis one of those par
sical activity policy inents a global intensity, in all respondentould be interpreted apolicy).
eport93
we can conclude y in Flemish schontegrated in a glo
“supply” revealsof schools have ce available. Howatic. Although thessibility of facilities
ctivity in seconda
mum Maximum
10.00
8.59
10.00
10.00
10.00
84.27
w of the partial scorl scores are calcula
“good” answers to artial scores. The globn the secondary schity of the health promt schools. The globaas a “percentage” o
that health promools are in progreobal school policys that infrastruct(access to) a g
wever, the availabe range of activits could improve.
Belgian
ary schools in Fl
m Mean StdDe
6.0643 2.0
5.4758 1.2
6.9500 1.7
5.3100 2.3
4.7332 3.4
56.3475 14
res for several healtated as a 0-10 index long questionnairebal score, called “Tohools” (calculated amotion policies on thal score ranges betwof a perfect score (in
motion policies reess, score quite gy. A separate anature scores quitegym but with somility of a swimmingties has increase
n Health System
anders
d. eviation
08702
29252
74638
31019
41978
4.46473
th x . The otal s a he theme ween 0 n terms of
elated to ood and alysis of e good. metimes g pool is ed since
DTssDthWre77HItinrereUto7SShmosFsoalolo
Performance
Data for BrusselsThis report showssport facilities, anschools, the childrData on the availahe physical activWallonia and Brecommendations
7.2.3 Health P7.2.3.1 HealthHealth literacy is ot can be defined nformation relatedelated to the “eepresentative asp
Unfortunately, noo adequately mea7.2.3.2 SocialSocial support Social support is ahelps individuals tmodalities, like emof social support somatic illnesses aFifteen percent ofsocial support in 2of social support association with eowest educationaower in Flanders t
s and Wallonia as that 20% of thend that another ren are going to anability of (extra) phvity in the globarussels in order.
Promotion outcomh Literacy one of the most im
as “the individuad to health, healtempowerment” dpects of health prodata exist in Belg
asure health literal influence and a
a protective factoto deal with the d
motional support, have been link
and mortality. f the population 2008. There is nois gradually incre
educational level al level versus 1than in the other r
are extracted frome responding scho10% had no spnother place to hahysical activity anl school-policy sr to conclude a
mes
mportant indicatoral skills to understh determinants, imension, which omotion.95 gium yet. At interncy are still under v
action
r in times of stresdifficulties of life material aid, info
ked to increased
aged 15 years oo significant gendeeasing with age. T(age-adjusted rat0% in the higheregions, especially
m the HBSC survools had no adeqort facilities. In ave the sport lessnd on the integrathould be collectand eventually
rs for health promstand and managand health care”is one of the
national level, the validation.96, 97
ss. It is a resource(according to diffrmation…). Low l
rates of depres
or older reported er difference. TheThere is also a ste equals 22% ost). The rate is y in Brussels.
119
vey.94 quate those ons. ion of ed in make
otion. ge the . It is most
tools
e that ferent levels ssion,
poor e lack strong n the much

120
7.2.3.3 HeaThe Tobacco C
The concept policies arose policy initiative“Tobacco Contrcomparable levcomposed of th• Price incre
products; • Bans/restri• Better cons
media cove• Comprehe
products, lo• Large, dire
tobacco pro• Treatment
access to mBelgium is situ50/100. The sc(Greece) and golden opportuthe parliament The new law stsmoking is stilstrict rules. Dat2010 do not reother side, Belgwarnings in 20packs in 2011”.
althy Public PoliControl Policies of multi-prongedfrom governmen
es during the 90rol Policies Scalevel of the Toba
he following elemeeases through hig
ctions on smokingsumer informationerage, and publicinsive bans on theogos and brand nect health warninoducts; to help depende
medications. uated on the 10thcores of the more77 (UK). The au
unity to adopt commodified legislat
till permits smokinl allowed in somta from the Minis
espect the weak rgium was the firs06 and to print th
icy Scale
d and “comprehnts’ and non-gov0s. The interest e” is to provide a cco Control Pol
ents98: her taxes on ciga
g in public and won, including publiising research finde advertising andames; ng labels on cig
ent-smokers stopp
h place out of 32e extreme countruthors conclude mprehensive smoion in December ng in bars, discoth
me public places try of Health shorestrictions whichst EU country to he number of the
Belgian
ensive” tobacco vernmental organ
of the compositglobal and internicies in a count
arettes and other
ork places; c information camdings; promotion of all
garette boxes an
ping, including in
2, with a global sries were respectthat “Belgium m
oke-free legislatio2009 (articles 4
heques and casinin smoking-roomw that half of the applied to them.introduce pictoria
e quit line on all c
n Health System
control nisations’ te index ationally
try. It is
tobacco
mpaigns,
tobacco
nd other
ncreased
score of tively 32
missed a on when
and 5). nos. Also ms under e bars in . On the al health cigarette
Performance KCE Reportt 196

KCE Report 196
Figure 37 – Int
Source: A survey
6
ternational comp
y of tobacco control
parisons on the T
activity in 31 Europ
Belgian
Tobacco Control
pean countries in 20
n Health System
Scale in Europe
01098
Performance
e (2010)
121

122
7.3 Key fin• In 2008, 47
obese. Theoverweigh65, and areobesity rathe highersmall.
• The numbpopulationIn a 2009-2missing, fgoals set f1.0 for 12-samples.
• The rate oEuropean diagnosis imported cthose of ththe other rhomosexuBelgian catransmissby other w
• The perce2008. It hamen than decreasingbelow the
dings 7% of the populaese percentages
ht and obesity ince strongly assocte in the lowest er educational lev
ber of studies pern is scarce and a2010 study, the milled teeth) scorefor the year 2010year-olds). Howe
of new HIV diagno(EU-15) mean. Aare made in non
cases, with diffehe Belgian casesregions, represeual transmission ases. The numbeion way is increa
ways is not diminntage of daily sm
as significantly din women, in all g in men than in EU-15 average r
ation was in overs are increasing ocrease sharply wciated with educaeducational leveels. Differences
rformed in Belgiuare often limited mean DMFT (dene was 0.9. This sc0 (maximum meaever, more data a
osis in Belgium A large proportion-Belgian peoplerent patterns of ts. The rate in Brunting an urban p is the main way
er of cases resultasing; the numbenishing either. mokers was arouecreased since 1age groups. How women. The Berate.
Belgian
rweight, and 14%over time. Both
with age until theational level. The
el is twice as highbetween regions
um on oral healtto small selected
ntal health: decaycore meets the W
an DMFT score bare needed on la
is a bit higher thn of those new
e. Those are probtransmission thaussels is higher tphenomenon. Thy of transmissionting from this er of cases trans
und 20% in Belgi10 years. It is higwever, the rate islgian rate is slig
n Health System
% was
e age of e h as in s are
h of the d areas. yed, WHO below arger
an the
bably an than in e male
n for the
smitted
um in gher in s more htly
•
•
•
•
Performance
In 2008, 8% oalcohol over-common in ydifferences apeople reporregions. The dependency)Brussels. Thglasses) amo
In 2008, almowhich is an iconsumptiononly 26% of twith even low
The global peany type of pwomen. It is regions, and surprisingly
When assessthe Global Toposition.
of the population-consumption. O
young people (agare observed in trting over-consuproblematic alco
) seems to increae regular risky song young peoplost two-third of tmprovement com
n was still higherthe people ate 2 wer rates in Wallercentage of peo
physical activity much higher in Fis especially lowdeclining in Walsing the global pobacco Scale, Be
n was consideredOver-consumptioged 15-24 years).his age group, wmption in Flandeohol consumptioase in all regions
single-occasion dle is of concern.he population atmpared to 2004. r than that of fruifruits and 200g vonia (F: 28.5%, B
ople practising aper day is low, aFlanders (45%) tw in Brussels. Thlonia.
public policy on telgium is ranking
KCE Report
d to have a weekon is already . Regional
with more young ers than in the oton (trends to s and mostly in drinking (more th
te fruit every dayThe daily vegetaits (84%). Howevvegetables dailyB: 24.6%, W: 18.2t least 30 minute
at 38%. It is lowerhan in the two othe rate is also
tobacco control wg at an intermed
t 196
kly
ther
han 5
y, ables ver, , 2%). es of r in ther
with iate

KCE Report 196
8 EQUIT8.1 IntroduEquity is a keysystem.1 It is aand political pobeen proposed“The place ofsystems.” Being aware ofwith two comple1. In a first subthe inequalitiesBelgium acrossoperationalisatiequity in healthdeterminants ba social hierarc2. In a secondcan highlight ispurpose of thesystem at a glo
8.2 Socio-e8.2.1 How dSocio-economicstatus/health ddisfavour of thposition on theis consistent inequalities haslevel priority taProgramme104
reducing social
6
TY AND EQuction y feature in the ealso a controversiosition. A broad rad, and are discusf equity in asse
f this feature, we ementary ways: chapter, called “S
s in health, healths the socioeconoon and measure
h as “the absenceetween social grohy”. subchapter, we
ssues of equity ine second part of bal level”.
economic ineqdid we evaluate c health inequdeterminants/utilizhe social groups social scale. Theand has long bs long been a prioarget at Europeaand in the US
l inequalities in h
QUALITY
evaluation of the al normative issuange of perspect
ssed in the Suppessments of the
have approached
Socio-economic in determinants an
omic position. Indments, Braveman
e of systematic ineoups who have di
have proposed cn healthcare at athe chapter, cal
ualities socio-economic
ualities refer tozation of health
that are alreadye presence of sobeen recognizedority for the WHOan level, with thSA.105 To assesshealth, it is impor
Belgian
performance of ue, referring to judtives and definitiolement S2 of this
performance of
d the dimension o
nequalities“, we dod healthcare utiliz
deed, for the purn99, 100 suggests equalities in healtifferent social pos
contextual indicata global level. Thled “Equity of the
c inequalities? o disparities in
services, most y disadvantaged cio-economic ine
d.101, 102 TacklingO.103 It has becom
e DG Sanco 2ds the progress rtant to measure
n Health System
a health dgement ons have s report: f health
of equity
ocument zation in rpose of defining
th/health sitions in
tors that is is the e health
health often in by their qualities
g health e a high
d Health towards them100,
amT••
CTinesSeFethpclawEsascwFgFRp
Performance
and to monitor measurements). The measurement a characterist one or more
indicator(s).
Characteristics uThe social groups ndividual or eveeducational level, some of those varSocial groups’ deeconomic variableFor the indicators economic (SE) vahe highest educapartner was choseconsidered to be argely available, lwas coded accoEducation (ISCEDschool diploma), land higher educaservices for financhosen as proxy when explaining pFor the indicators grouped into 5 groFor the indicatorsRIZIV – INAMI, thproxy for the SE
if they chang
t of health inequaltic defining the soce synthetic inequ
used to define thecan be defined b
en geographical the occupation, aiables. finition varies acc
es in the different dissued from the H
ariables are availaational level attainen to define the sothe most compa
less sensitive andording to the InD) summarized as lower secondary ation. For the in
ncial reasons”, thfor the SE level.urely financial barof Life and Health
oups (no educations calculated fromhe status of increE level. Two soc
ge over time
lities requires chocial groups uality measures
e social groupsby different charac
levels: the hoa deprivation inde
cording to the avdata sources we uHealth Interview Sable. For most ined by the referenocial position. Ind
arable and robustd prone to bias thternational Standlower education education, higher
ndicator “delayed e income level o. Indeed, this chorriers. h Expectancy, then and primary lev
m the Permanenteased reimbursecial categories w
(by repeating
oosing:
in the health-re
cteristics at houseusehold income
ex, or a combinati
vailability of the sused. Survey, different sdicators of this re
nce person and heed, this informatt choice, becausehan the income levdard Classificatio(no diploma or prr secondary educ contacts with hof the householdoice is more per
e educational leveel were split). t Sample or from
ement was chosewere defined with
123
those
elated
ehold, , the ion of
socio-
socio-eport, is/her tion is e it is vel. It on of rimary cation health d was tinent
el was
m the en as h this

124
variable, the Bpeople with a lo
Measurement In a first step, wfor all the indicacan be found inIn a second steindices, allowinsummary indicenature (absolupairwise measuonly two groupspublic health pgroups are moinequality on thThe following in• For the Life
o The ahighes
o The Rconcenbetweeby the
• For the indo The a
levels)o The ab
• The Populahealth (or healtlevel if all the g
u BIM: Bén
reimburse
BIMu (increased ow income level) a
of inequalities
we showed the disators for which dan the documentatioep, we summariz
ng quantifying thees can be used.1te versus relativ
ures (like the rates are easy to comperspective, moreore useful sincee population heal
nequality indices ae/Health Expectanabsolute differencst educational groelative Concentrantration index is ten each group ansize of each grouicators issued fro
age-adjusted rate ) bsolute differenceation Attributable th determinant) r
groups experience
néficiaire à Interv
ement); BO: Bénéfic
reimbursement, and BO (normal re
sparities across thata were availableon sheets in the Szed the detailed ie size of the inequ106 They differ byve), their scope e difference, or thempute and to undee complex meas
e they measure th.107
are described in thncy: ce in years betwups
ation Inequality Indhe sum of the diffnd the highest edup, and divided bym the Health Interatio (between
e in age-adjusted rFraction (PAF): t
rate that would beed the rate of the
vention Majorée
ciaire Ordinaire
Belgian
mostly corresponeimbursement).
he socio-economice (this detailed infoSupplement S1).nformation by coualities. A wide vy several properti
and complexity:e relative risk) coerstand. Howeversures involving a
the total impact
his chapter:
ween the lowest
dices (CII rel): theference in life expducational level, wy the life expectanrview Survey the extreme edu
rates (idem) this is the relativee expected at po
e more advantage
(beneficiary of i
n Health System
nding to
c groups ormation
omputing variety of es: their : simple
omparing r, from a
all social t of the
and the
e relative pectancy weighted ncy
ucational
e gain in opulation ed social
ncreased
gpoInre
L
TdTSththnFalesrephthWininsa
Performance
group. It is comppopulation and thoverall rate in the n this chapter, welative risk (RR) a
Limitations
The inequalities codata on social posTherefore, our conSome issues knowhis work (like thehe topics specificnext report. For the indicators available. It is diffevel with the BIM status for financepresenting less
preferential reimbhandicap but no fhe next survey. We did not performn the indicators.nequalities relatescope of this workanalysed on a sma
puted as the diffehe rate in the mopopulation.
we highlighted thas large as 1.2 (or
ould not be meassition. This is the nclusions for this dwn to be related t waiting time for
cally linked to the
from the Permaneficult to measure status. Indeed, p
cial reasons arethan 5% of the
ursement status financial disadvan
m an analysis of Such a represe
ed to ecological pk. Moreover, the dall scale, because
erence between tore advantaged
e indicators for wr 0.83 when the g
sured for all the incase for many of
dimension are largo social inequalitisome interventioninequalities shou
ent Sample (EPSthe impact of ineeople with a prefee people with e population. Onalso comprises p
ntage. The definiti
the small scale gentation is a wapoverty indices. data originating fre of the size of the
KCE Report
the overall rate igroup, divided b
which we observradient was rever
ndicators due to laf the quality indicagely incomplete. ies were not studns). A deeper focld be performed i
), only two statuteequalities at popuerential reimbursea very low inc
n the other handpeople with a phyion could be refin
eographical dispaay to highlight hThis was beyond
rom the HIS canne sample.
t 196
n the y the
ved a rse).
ack of ators.
ied in cus of in the
es are lation
ement come, d, the ysical
ned in
arities health d the
not be

KCE Report 196
8.2.2 Facts
This section is afor each indicawebsite).
8.2.2.1 IneqLife and HealthTo assess ineqof data on mortthe most receninequalities in lin health expeclevels are reposecondary highextreme groupsindicators, maklarge. Concentbecause they taTable 27 show2001. Large ineare observed ibetween a partinequalities is oyears in men. women, the sabetween each eThe gap betweand the Relative
6
and figures
a short summary ator in the Supple
qualities in indich Expectancies
qualities in life andtality, social positt and robust dataife expectancy109
ctancy.111 As merted in 5 categori
her, and higher eds are compared wking the differencetration inequality ake into account t
ws the life expectequalities in life en both sexes, deticular educationaobserved. The diff
The Relative Coame tendencies weducational level en the extreme ee Concentration I
of the detailed resement S1 of this
cators of Genera
d health expectanion and disability
a in Belgium conc, 110 and the year
entioned, in both es (no diploma, pducation). With thwith the pairwise es between the cindices are mor
the share of the soancy at 25 years
expectancy betweefined as the diffeal level to the higfference between oncentration Indewere observed aand the highest w
educational levels ndex in men was
Belgian
sults which are pr report (available
al Health Status
cies, complex proare needed.108 C
cern the year 200r 2004 for the ine
studies, the eduprimary, secondarhis way of groupinindices than for tcompared appearre appropriate mocial levels. s by educational een the educationerence in life expghest level. A grathe extreme leve
ex in men was 3s for men, but th
were smaller thanwas 5.9 years in3.7 %.
n Health System
resented e on the
ocessing Currently, 1 for the qualities
ucational ry lower, ng, more he other ring very
measures
level, in al levels
pectancy adient of els is 7.5 3.7%. In he gaps in men.
n women
Tain
D
HShSloPNT CCS
T2mindCeTwmthti
Performance
Table 27 – Life eabsolute differennequality indices
Diploma
Higher Secondary higher Secondary ower Primary No diploma Total
CII absolute CII relative Source: Deboosere
Table 28 shows th2001. Inequalities much larger thannequalities whendifference betweeConcentration Indexpectancy. In woThe gap betweenwomen. The Relameans that peoplhose with a highime in good health
expectancy at 25nce to highest es (CII) (Belgium 2
Men
Total Diff tolevel
55.0 52.5 -2.5
51.3 -3.7
49.3 -5.7 47.6 -7.5 51.4 -3.7 1.9 3.7
et al.112
he health expectabetween the edu
n for life expectan the educationan the extreme lev
dex in men is 15.omen, the same n the extreme eative Concentratile with low educa educational leveh.
5 years by sex aeducational leve2001)
W
o the highest T
55
5
555
ancy at 25 years bcational levels in ancy. Again, a gal level decreasevels is 18.6 years.3%, which is mutendencies were educational levelon Index in womational level not el, but also that t
nd educational el and concentr
Women
Total Diff to highest l
59.9 58.5 -1.4
58.0 -1.9
56.2 -3.7 54.0 -5.9 57.1 -2.8
0.8 1.4
by educational levhealth expectanc
gradient of increes is observed. s in men. The Reuch larger than foobserved as for s was 18.2 yea
men was 16.6%. only live shorter
they spend much
125
level, ration
the level
vel, in cy are asing
The elative or life men.
ars in This
r than h less

126
Table 28 – Helevel, absoluconcentration
Diploma
Higher
Secondary higher Secondary lower Primary
No diploma
Total
CII absolute
CII relative
Source : Van Oye
The self-perceImportant inequdifference of 2educational levAttributable Frathe whole poputhe rate of subjeInfant mortality Belgium, only p
ealth expectancyute difference
inequality indice
Men
Total Diflev
46.33 0.0
41.54 -4.
39.71 -6.
36.65 -9.
27.75 -18
40.5 5.9
6.2
15
en et al.113
eived health ualities are obser29% is observedvels (Table 29); action is 11%, meaulation would be 1ective health of this also known to
partial data exist a
y at 25 years bto highest e
es (Belgium 2004
ff to the highest vel
0
.8
.6
.7
8.6
9
2
5.3
rved in self-perced between the the relative risk aning that the glo11.2% if all educahe people of the ho be linked with sand confirm this f
Belgian
by sex and educeducational leve4)
Women
Total Diff highe
47.1
41.27 -5.8
42.01 -5.1
36.27 -10.8
28.92 -18.2
40.4 6.7
6.7
16.6
eived health. An alowest and the is 67%. The Pobal increase of th
ational levels expeighest educationasocio-economic sfact. For instance
n Health System
cational el and
to the est level
8
2
absolute highest
opulation e rate in erienced al level. tatus. In , a clear
ainth8Thleinre7Incsreha0Foabthsssba
Performance
association was fncomes and infanhis report. 8.2.2.2 InequaThe percentage ofhealth system forevel, with 27% of n the householdselative risk of 6.2
71%. nequalities of smcervix cancer. Lowsocio-economic seimbursement). T
highest educationand cervix cancer 0.76. For the indicators of the elderly), a against influenza better coverage inhey reside more osystematic. For thsurvey in childrenstatus (measured better coverage tassociation was no
found in Brussent mortality.114 Th
alities in the indif households repor financial reasondelay in the hous
s of the highest 2. The population
maller size are obswer coverage ratestatus (identifiedThe absolute diffeal levels were resscreening. The r
on vaccination (reverse phenom
in the elderly, mn the patients witoften in institutionhe vaccination ra in Wallonia (200with the educat
than children froot found in Flande
ls between the hese data are not
icators of accessorting to have delns was strongly seholds of the lowquintile (Table 2
n attributable frac
served for the sces are observed d by their entiterence of coveragspectively 14.3%
relative risks were
vaccination of chmenon was obseeasured with theth BIM. It could bns for elderly, wheate in children, in09), children with tional level of theom higher socio-ers.
KCE Report
number of houst presented in det
sibility ayed contacts witrelated to the in
west quintile versu29). This represection was as larg
creening of breasfor patients with tlement to increge between lowes
and 15.3% for be respectively 0.77
hildren and vaccinrved. The vaccin
e EPS data, showbe due to the facere vaccination is n the last vaccinlower socio-econ
e mother) had sl-economic level.
t 196
ehold tail in
th the come
us 4% nts a ge as
st and lower
eased st and breast 7 and
nation nation wed a ct that
more nation nomic lightly
This

KCE Report 196
8.2.2.3 IneqData by social care. Socio-econom• The follow
percentagerisk was 0.
No important in• Prescriptio• Physician e• % of peopl• Percentage
Provider ofReverse InequSome interveninterventions sicancer screenincoverage is higalso worse in thMissing data Unfortunately, fsocio-economicconsidered as l
v Cancer 5
relative suafter colonwithin onadmission(per 1000 admissionIncidence fracture (%(MDT) me
6
qualities in the instatus were only
mic inequalities cw-up of diabetic e of patients with 83, and the PAF wequality was obsen antibiotics accoencounter after hoe with at least a ce of people with f Care > 0.75)
ualities tions are not apigns a lack of apng outside the tarher in the advant
his group.
for a large numbc inequality couldargely incomplete
5-year relative survurvival rate after cern cancer; Deaths dune week after stans for asthma in adu
live births); Incidenns); Incidence of p
of pressure ulcers%); Patients with ceeting (%); Numbe
ndicators of quaavailable for som
ould be observepatients: the aba correct follow-
was 7.4%. erved for the follow
ording to guidelineospital discharge fcontact with a GP a high fidelity to
ppropriate. Hencepropriateness. Th
rget groups (< 50 aged social group
ber of interesting d not be measuree. The missing dat
vival rate after brervix cancer; Cancerue to suicide (/100 art of palliative cult patients (/100 00nce of hospital acqupost-operative sep
s in hospitals (%); Icancer discussed ar of contacts betwe
Belgian
ality of care me indicators of q
ed in: bsolute differenceup was 10%, the
wing indicators: es for eldery patientsin the year their GP (Index o
e, a high rate fohis is the case foor ≥ 70 years). S
ps, the appropriat
indicators of quaed. Conclusions ta concern 14 ind
east cancer; Cancer 5-year relative sur000 pop); Patients
care service (%); 00 pop); Caesareanuired MRSA infectionsis (/100 000 discn-hospital mortality
at the multidisciplineen the patient and
n Health System
quality of
e in the e relative
s (65+)
of Usual
or those or breast Since the eness is
ality, the must be icators.v
er 5-year rvival rate who died Hospital
n sections ns (/1000 charges); after hip
ary team d the GP
8DasdofophpTpoFgreth0imSosre
Performance
8.2.2.4 IndicaDaily smoking andand 2.11) betweesmoking, the absodaily smoking andobserved (-36.1 %or those 2 factopopulation health, health if all sociprevailing in the mThe rate of overwpresents more moof 14.7%. For the determinagenerally observeelative risk will nohe consumption 0.74, and PAF=1mportant, with a RStrong inequalitieof the people fromsupport, versus oepresents a RR o
during the 3 patients with
ators of the Healtd obesity presen
en the lowest andolute difference in d obesity, a high P% for smoking anrs, the inequalitieand that a large g
ial classes expemore educated groweight people (deoderate inequalitie
ants having a posed in the more ow be lower than of at least 200g 3.1%). For physi
RR of 0.56 and a Pes are observed im the lowest edonly 10.1% for tof 2.4, and a PAF
last months of life
pain always contro
th promotion domt a high relative
d highest educatiorates is as high a
Population Attributd -34.8% for obees have a large gain could be obta
erienced the leveoup. efined as the peoes, with a relative
sitive impact on heducated classe
1. We observe imof vegetables an
ical activity, the PAF 12.3%. n the level of socucational level rethe people of thof -34.8%.
e; Pain control durlled).
main risk (respectivelyonal groups. For as 8.9%. Moreovetable Fraction (PA
esity). This meansglobal impact o
ained in the popuel of smoking/ob
ople with a BMI risk of 1.45 and a
health, a higher raes, meaning tha
mportant inequalitiend 2 fruits daily inequalities are r
ial support, with 2eporting a poor she highest level.
ring hospitalisation
127
y 1.68 daily
er, for AF) is s that n the lation besity
≥ 25) a PAF
ate is at the es for (RR= rather
24.4% social
This
(% of

128
No or weak ineThe daily consimportant link wThe link betweclear. Data by socio-efilled teeth at (/100 000 pop).
Table 29 – Ineq
General HealthLife Expectancy aLife Expectancy aHealthy Life YearHealthy Life Year% of the populativery good iii
Accessibility oDelayed contactreasons (% of hoBreast cancer scCervix cancer scr
Appropriatene% of adult diabeof regular retinal
Health promot% of the populati% of the populati
equalities sumption of fruits
with the social stateen the consump
economic status age 12 (mean s
qualities express
h Status at 25 in men, 2001 at 25 in women, 200rs at 25 in men, 200rs at 25 in women, 2on (aged 15+) that
of care ts with health se
ouseholds) iv reening (% women reening (% women
ess etes patients receiviexams and blood te
tion on (aged 15+) that on (aged 15+) repo
s or vegetablestus. tion of alcohol a
were not availabscore at age 12
sed with absolut
i; ii 01 i; ii 01 i; ii 2001 i; ii assess their health
ervices because o
aged 50-69) v aged 25-64) v
ing appropriate carests v
reports to smoke daorting a poor social s
Belgian
once a day sho
nd social status
le for: Decayed/ 2) and Incidence
te difference, rela
Overvalue
51.3857.0940.4740.42
as good or 76.8%
of financial 14.0%
60.1%61.8%
re, in terms 54.0%
aily iii 20.5%support iii 15.5%
n Health System
owed no
was not
missing/ of HIV
ative difference,
all e (f)
Value inlowest sgroup (f
8 47.56 9 53.98 7 27.75 2 28.92 % 57.4%
% 27.0%
% 48.6% % 48.9%
% 48.0%
% 22.0% % 24.4%
Performance
and summary m
n social f)
Value in higher sogroup (f)
55.03 59.9 46.33 47.1 85.7%
4.0%
62.9% 64.2%
58.0%
13.1% 10.1%
measures
cial Absolute d
(lowest vs
-7.47 -5.92 -18.58 -18.18 -28.3%
23.0%
-14.3% -15.3%
-10.0%
8.9% 14.3%
difference
s highest)
Relat
(lowehighe
n.a.n.a.n.a.n.a.0.67
6.75
0.770.76
0.83
1.682.42
KCE Report
tive Risk
est vs est)
Summmeasuor PAF
3.73% 1.43% 15.30%16.56%11.6%
-71.4%
4.7% 3.9%
7.4%
-36.1%-34.8%
t 196
mary ure (CII F)
% %
%
% %

KCE Report 196
% of the adult po% of the adult obese (BMI ≥ 25)% of the populat2 fruits per day iii
% of the populatiper day iii i in years; ii 5 edurates are not adjuthe other indicatoSource: Health InPA: physical activ
6
pulation consideredpopulation conside
) iii ion reporting to eat
on reporting to prac
ucational levels; iii 4 usted for age; summors nterview Survey andvity
d as being obese (Bered as being ove
t at least 200g vege
ctice at least 30 min
educational levels; mary measures= CII
d EPS (WIV – ISP a
Belgian
BMI ≥ 30) iii 13.8%erweight or 46.9%
etables and 26.0%
nutes of PA 38.1%
iv 5 income levels; vI (Concentration Ind
and KCE calculation
n Health System
% 19.2% % 57.8%
% 21.7%
% 24.0%
v 2 reimbursement cdex of Inequalities) r
ns)
Performance
9.1% 40.0%
29.4%
42.8%
categories; relative for life and h
10.1% 17.8%
-7.7%
-18.8%
health expectancy,
2.111.45
0.74
0.56
PAF (Population At
-34.1%-14.7%
13.1%
12.3%
ttributable Fraction)
129
% %
for all

130
8.2.3 Key fiWith regard to• Life expec
social poshealth exphealth.
• Inequalitieinequalitieconditionsidentified
With regard to• Very large
financial r• Moderate
screening• On the con
disfavoure(with somegood poin
• Also the cless advan
With regard to• For most o
be measur• Moderate
people. With regard to• Very impo
obesity (w30%). As ohigher morepresents
indings o general health sctancy presents asition. This gradipectancy. Inequa
es in those globaes in factors influs, health determiand tackled.
o accessibility: e inequality is obreasons. inequality is obs. ntrary, for vaccined group is at leae partial data sho
nt for the action ocoverage of the gntaged groups.
o the quality of caof the indicatorsred. The conclusinequality was o
o health promotioortant inequalitieswith a Populationobesity and smoorbidity, tackling s a top priority.
status: a strong increasent is still much
alities are observ
al and “end of couencing them: soinants, health sy
bserved in the de
served in breast
nation, it seems ast as good as inowing even a beof preventive heaglobal medical re
are: , socio-economi
sions are incompobserved for the
on indicators: s are observed f Attributable Fraking are stronglythe inequality in
Belgian
ing gradient withmore important
ved in self-percei
ourse” indicatorsocial and living ystem. Those sho
elay of health car
and cervix cance
that the coveragn the favoured gretter coverage). Talth services. ecord is better in
c inequalities coplete. surveillance of d
for daily smokingaction of more thy associated wit
n those factors
n Health System
h the with
ived
s reflect
ould be
re for
er
ge in the roup
This is a
the
ould not
diabetic
g and han h a
•
•
88
EsatheshhbaaaptheTome
Performance
Inequalities afruits and vegphysical acti
Very importa
8.3 Equity of 8.3.1 How did
global leEquity is a controvsomething”. Howeapproaches. Indeehe unequals andequals. An exampso that everyonehorizontal equity ihave the same nebetween the richean attempt to approaches haveamong individualsprefer to equalize hought and showessentially normatTo establish equityof a healthcare symust reflect societequity of the health
are also observegetables, and in vity.
ant inequalities a
the health systd we evaluate theevel? versial dimensionever, there is aed, vertical equity horizontal equity
ple of vertical equi pays taxes bass the attempt to eeds. Equity impl
est and the pooresreconcile solida
been proposed. Some propose toutcomes119-121.
w how the definitiotive issues and they indicators in theystem requires antal choices. In thishcare system in a
ed for overweighta lesser extent f
are observed for
tem at a globae equity of the h
n. Generally, equita large heterogey is defined as they is defined as eity are tax systemsed on ability to provide the sameies therefore somst, between the harity and perso to define what to equalize resourThese theories o
on of fairness anderefore philosoph
e context of a repon approach as nes chapter, we havan indirect (or cont
KCE Report
t, eating enoughfor practising
the social suppo
l level ealth system at
ty refers to “equaeneity in the diffe unequal treatmeequal treatment o
ms which are orga pay. An exampe care to patientsme degree of solihealthy and the sional responsibilshould be equa
rces116-118, while offer interesting lin how to achieve iical issues. ort on the performeutral as possibleve evaluated the gtextual) way.
t 196
ort.
a
lity of ferent ent of of the nized
ple of s who darity ck. In lity115, alized others nes of it, are
mance e and global

KCE Report 196
Belgium backentitlement to itaken to promoavoid “catastropcategories of pSeveral BelgiaSupplement S2performance of
8.3.1.1 GloTwo contextual• the progres• the Gini coThe progressivbefore using thsharing” at thenon-reimbursabfinance the p(regressive) whsense) is incredefined as propcharacterize thfinancing of thprogressive thathe indirect taxeof the financingredistribution ebecause such aconsumption ofThese data arewith other counDoorslaer haveequity in financnot mention Be
6
kground: In Belgncreased reimbu
ote the financial aphic” health expepatients, such asan studies, and 2 of this report: “Tf health systems.”
obal or contextua indicators are dessivity of the finan
oefficient of inequaity of financing thhe system. By p
e point of care (i.ble drugs, premiupublic system. Ahen the average easing (decreasinportional when thehe relative progrehe Belgian healthan the social contes. Simple ratios ag for the period 2effect of the finanan evaluation impf care, all financine not totally availantries is not possie contributed in acing and deliveringlgium in their wor
gium, some spersement and the accessibility. The nditures and othe patients with chtheir results, are
The place of equ
al indicators escribed below: ncing of the healthality in income he healthcare sysprogressivity, we e. supplement, cms to private insuA financing is rate of “taxation”
ng) with the income average rate of
essivity of the mohcare system: thetributions which aare computed to d
2005-2011. We doncing and use olies the knowledgg sources and abable for Belgium ible due to lack oa substantive wayg of healthcare bk.122-128
Belgian
ecific measures sOmnio status hamaximum billing
er measures are thronic illness or ce discussed in dity in assessment
hcare system
stem translates thdo not mean th
co-payment, coinsurance …) but thedefined as pro” (considered in me. And the finaf taxation is constost important soue direct taxes are more progressdescribe the progo not evaluate th
of the healthcare ge of individual dabout the available and a robust com
of data. Wagstaff y to the evaluatiobut, unfortunately,
n Health System
such as ve been aims to
targeting children. detail in ts of the
he equity he “cost surance, e way to gressive a broad
ancing is tant. We urces of re more
sive than gressivity he global
system ata about
income. mparison and van
on of the they do
Wmaointobin8
Tfow
TthcinbtrTetatathNcaTstasp
Performance
We contextualize measured by theassociation betweobjective or subjenterpret and to coo characterize thebeen recently recondicators for the "8.3.2 Facts an
This section is a sor each indicatorwebsite).
The disparities of he indicators of contextual equity nequality) showsbecomes less proransfers) makes oThe public financiessentially for twoaxes) is increasinaxes and special hese two evolutioNevertheless, thecompare the Gini allowances). These two results substantial incomaxes and financesystem) using reprogressive.
also the equity ise Gini coefficien
een the income inective health.100, 1
ompute for Belgiue income inequaliommended by a WHealth 2020 targe
nd figures
hort summary of tr in the Supplem
health status andthe other dimeindicators (prog
s that the publicogressive and thour country one ofing of the healthc
o reasons: (1) the ng and (2) the pcontribution for s
ns make the finane Belgian society coefficient pre a
are not contradice redistribution u
e a specific colleesources (taxatio
ssue by means ofnt. Some authornequality and som129-131 The Gini cm and internationty in an internatioWHO workgroup ets".132
the detailed resultent S1 of this re
health consumptensions. The comressivity of the f
c financing of thhat our redistribuf the most egalitarcare system becopart of the regre
part of the progresocial security) isncing less progresy is one of the mand after taxation
tory because the using a large sysective sector (i.e. on and contribut
f the income ineqrs have showedme indications of coefficient is simpnal organizations onal perspective. which was workin
ts which are preseeport (available o
tion are presentedmputation of thefinancing and inhe healthcare syution system (taxrian in the world. omes less progressive receipts (inessive receipts (s decreasing. Glossive. most egalitarian n and transfers (s
society can organstem of transfersthe public health
ions) which are
131
quality d the f poor ple to use it It has ng on
ented n the
d with e two come ystem x and
essive direct direct
obally,
if we social
nize a s and hcare
little

132
Table 30 – Pro
Indicators of p
Ratio proportioRatio progressRatio regressivTotal Source: Vade me
Figure 38 – Gin
Source: DGSIE (Note: the Gini cothere is perfect in
ogressivity indica
progressivity
onal receipts/totsive receipts/totave receipts/total
ecum de la sécurité
ni coefficient bef
(Belgium) and OECDefficient is a coeffic
nequality, the coeffic
ators of the finan
tal receipts al receipts receipts
sociale, RIZIV – IN
fore and after tax
D Health Data 2012ient for inequality ofcient is 1 (one perso
Belgian
ncing of the publ
2005 (final accounts)
20ac
71.1% 7118.9% 1910.0% 10100.0% 10
NAMI, KCE calculatio
xation and transf
2 (international compf income in a populaon has all the reven
n Health System
ic healthcare sys
006 (final ccounts)
200acc
1.0% 72.09.0% 18.00.0% 10.000.0% 100on
fers (1998-2010)
parison) ation. When there is
nues). A lower coeffi
Performance
stem (2005-2011
07 (final counts)
2008(provacco
0% 70.6%0% 17.3%0% 12.1%0.0% 100.0
: Belgium and in
s perfect equality (eficient indicates a m
)
visional ounts)
200(proacc
% 69.4% 17.2% 13.40% 100
nternational comp
everybody has the sore equal distributio
09 ovisional counts)
201(bu
4% 64.2% 19.4% 15.0.0% 100
parison
same income, the coon of the incomes.
KCE Report
10 udget)
2011 (budg
.8% 61.4%
.4% 18.4%
.8% 20.2%0.0% 100.0%
oefficient is 0). Whe
t 196
get)
% % %
%
en

KCE Report 196
8.3.3 Key fiEquity in finan• Public fina
progressiv• The intern
because oIncome inequa• Income ine
redistribut• Thanks to
the most e• The high l
distributioon Belgian
6
indings ncing ancing of the Beve, certainly sinc
national comparisof the great diverality equality in Belgitive impact of taxthe system of ta
egalitarian countevel of income r
on of disposable n population hea
lgian healthcare ce 2005. son of the progrersity of systems.
um is relatively hxes and transferaxation and transtries. redistribution andincomes should
alth.
Belgian
system become
essivity is not re
high before the rs. sfers, Belgium is
d the more egalitd have a positive
n Health System
es less
elevant
s one of
tarian impact
9
Inimrebresae
AaTpthammpbhfu
FWinsaremh
Performance
9 TOWARHEALTHASSESSSHORTC
n this section, wmprove the evaluelate to the lack
better indicator oesult from the ma
section “Indicatorsavailable on the experts.
An indicator ofavoidable/amenaThe previous reppremature mortalithe age of 70 yearaction and was nomortality expressemeasurement of tproject establishebetween countriehealthcare systemuture set of perfor
Financial accessWhile the coveragn terms of the pservices is paid dand 14% of the peasons (with a str
mechanisms werhealthcare system
RDS A MORH SYSTEMSMENT: ADCOMINGS
we identified 10 liuation of the hea
of suitable indicr for more detaiany indicators for s under developmKCE website), a
f global health able mortality port included onety, expressed as rs. This indicator wot retained in this ed by group of cahe effectiveness d the list of cond
es are likely to ms.133 This indicatormance indicators
ibility: need for ae of the compulsoproportion of theirectly by patientspeople report to rong gradient withre introduced to
m. Examples are lu
RE COMPR PERFORMDDRESSIN mitations that sh
alth system perforators, the lack ofls. Some of the which we could
ment” in Supplemand from the disc
status with p
e indicator of heapotential years ofwas too general, report. Instead, th
auses could be mof health servicesditions for which
reflect variationor could replace ps.
a more comprehory health insurane population coves. Out-of pocket pdelay healthcare
h household incomo maintain a ump sums for the
REHENSIVMANCE NG CURRE
hould be addressrmance. Those isf data, the need following conclu
not find any datament S1 of this recussions with Be
potential for ac
alth status whichf life lost (PYLL) blimiting the poten
he avoidable/ameore informative fos. A recent EU fuvariations in mo
ns in performancpremature mortalit
ensive picture nce is quasi exhauered, part of covpayments remain e because of finame). Several protefinancially acces
e chronically ill an
133
E
ENT
ed to ssues for a
usions a (see eport, elgian
ction:
h was before tial of nable or the unded ortality ce of ty in a
ustive vered high,
ancial ection ssible
nd the

134
maximum billinmechanisms, inservices. A pretransparency ininsurances (thewhat is specific
Workforce couon the need siAn effective heglobal policy takData on the supCurrent head cimprovement othe medical wmedical doctorsector or not). Hinto account. Swhich evaluatephysicians. Fopractising nurseHowever, the interpret, as ndefined. Internainterpretable wvaries across coData on the neeWorkforce planinformation thatIndeed, severamet, at least asthat there is gecontinuously riageing populaexpectations, re
ng system (MABndividual private
erequisite to guiden ambulatory supe percentage of pally covered by th
unts: better datade still lacking
ealthcare workforcking into account pply side counts of practisf the information orkforce was estrs (regardless of However, the rea
Since 2009, this ces the number or the first timees by sector of acdensity of prac
no optimal densiational compariso
without taking intoountries. ed side nning also requiret is currently scarcl informal sources
s far as the nurse eneral lack of nurssing and changiations, technoloequire a larger an
).134 In addition insurances reimb
e policy within thipplements as we
people with privatehese private insura
a on the supply
ce planning shoulsupply and patien
sing physicians ucompared with ttimated by the t
f whether they wal activity level of count is conducteof full-time equi, preliminary co
ctivity are now avactising healthcarety to meet popuns are of little hel
o account the org
es information once. s point out that thworkforce is conc
ses in the Belgianing demand for ogical advancesd more skilled nu
Belgian
to these publiclyburse several hes domain is an imell as in private e hospital insuranances).135, 136
side available, b
ld be considered nt needs.
ndoubtedly reprehe former situatiototal number of worked in the hephysicians was ned by the RIZIV –valents (FTE) ounts of the num
ailable. e workers is difulation needs halp here since theyganisation of care
n the need/dema
he needs are insucerned. It is wideln hospitals. Moreo
health services, s and higher rsing workforce.13
n Health System
y-funded ealthcare mproved hospital
nce, and
but data
within a
esent an on when licensed
ealthcare ot taken – INAMI, of active mber of
fficult to as been y are not e, which
nd side,
ufficiently y known over, the
due to patient
37
MrelailfotojoNre
McInthcsminownInc“A12
34
5
Performance
Macro-level data eflect the situationarge-scale Europlustrated that in Bor more patients co be dissatisfiedob.79,138 No indicators of teflection should c
Mental healthcachanges in the sen the field of menhe recent major ccentury, a strong dsector has led to model, the “balndustrialized couoffered wheneverwhen ambulatory needs. n Belgium, the mcare model focusArt. 107 project”) . Prevention an
2. Intensive, comchronic physic
3. Rehabilitation4. Intensive res
problems that5. Specific resid
or home-repla
on the needs shn at the micro leve
pean nursing worBelgian hospitals compared to othe
d with their job a
he needs have bcontinue on this to
re: current indector
ntal health, the curchanges in the sede-institutionalizat
the developmenanced care” mntries.139 It implie
r possible, while care cannot pro
most recent reform on the developmoriented to 5 func
nd promotion of mmmunity based, trcal conditions; teams focusing o
sidential teams ft require inpatient ential facilities in
acing environment
hould be complemel. An example of
rkforce study basnurses have, on
er EU countries.79
and have the in
been defined yet opic.
dicators do not
rrently available inector. Indeed, sinction movement in
nt of new modelsmodel is gaininges that communihospital services
ovide a good an
m efforts to attain ment of “care nectional modules:
mental health; reatment teams fo
on social integratiofor acute and ctreatment; which care can bt.140
KCE Report
mented with dataf micro data is a rsed on survey da
average, to take9 More nurses repntention to leave
in this report, bu
t reflect the re
ndicators do not rce the end of the the mental health
s of organization.g influence in ty services shous should be avanswer to the pat
a balanced integetworks” (the so-c
or acute as well a
on; chronic mental h
be provided in a
t 196
a that ecent ata. It e care ported
their
ut the
ecent
reflect e 20th hcare One most ld be
ailable tient’s
grated called
as for
health
home

KCE Report 196
Some indicatorpercentage of expenditures spmental health limitations in the(e.g. suicide ratepisode (e.g. reAt internationainitiatives, a recsuicide rates another data weorganizations shealthcare. Howoften limited. Fyears prescribedrug (%)” in thno operationalpublished studanticholinergiccomparison ofhampered.
Continuity andnew pathwaysThe fact that nchronic renal faevaluated, showmakers.142 We edition of this reSome other rele• The experi
care. SomGermany, surveys to is currently
6
rs can be propospatients with
pent on communicare). They co
e current data. Instes) or indicators
e-admission ratesal level, despitcent survey of twnd the number of ere scarce.141 Euch as the OECDwever, the operatFor instance, desed antidepressante OECD shortlist development odies disagree a
side effects.63,
f mental health
d coordination ofs in ambulatory cnew pathways inailure patients wews the importanc
plan to include eport. evant indicators hence of the patien
me countries suCanada, U.S. oanswer that ques
y still not measure
sed to monitor thcase managemeity care comparedould not yet bestead, we had to focusing on the p
; involuntary commte several perf
wenty-five EU coupsychiatric beds w
Efforts are undeD62 to propose indional developmenspite the inclusiots using an anticht for mental healtof this indicator. about what is
64 As a concare system pe
f care: new data care, but still mann ambulatory carre recently startee of the coordinathe results of th
have been identifient with regard to tch as the Netr Australia20, 143
stion. This indicatoed in Belgium.
Belgian
hese evolutions (ent; the percend to total expendi measured becarely on general inpsychiatric hospitmittals). formance measntries noted that were readily availertaken by intericators specific fo
nt and data availan of “Persons agholinergic anti-depthcare indicators,
What’s more, an antidepressa
nsequence, intererformance is s
soon available wny gaps remainre for type 2 diad and are currenttion of care for th
hose projects in t
ed, for instance: the coordination oherlands, Francehave performed
or, although being
n Health System
(e.g. the ntage of tures on ause of
ndicators talization
urement data on
lable but rnational
or mental bility are ged 65+ pressant there is the few
ant with rnational seriously
with the
abetic or tly being he policy the next
of his/her e, U.K., specific
g central,
•
P
Pdainm••
InssacuowObPhTc
Performance
The availabilitby all care ppatient electrindicators unpractices withpatients for wis accessible as the “Réseand pilot pro(http://www.viand currently e-Health platfo
Patient centeredn
Patient centeredndata, because it answer to the partnvolvement. To methodological ap Self-report me External obse
behaviour codn Belgium, the Hself-reported by tsatisfaction with thabove, but which concepts and onunderstanding on on satisfaction wilwith ambulatory hOECD questionnabe included in the Patient centerednhealthcare systemThree of them arcommitment of t
ty of the whole heroviders is a cenronic medical reder development
h access to the howhich information o
at any setting. Soeau Santé Walloojects are beingtalink.be/), but wiwithout much da
orm should have
ness: many initia
ess is intrinsicallis related to the ticular needs of th
effectively mepproaches used:14
easures of doctorservation of consuding system.
Health Interview Sthe population. Ithe health systemis subject to ma
n the measures patient experiencll be replaced by healthcare servicaire.15 Patient expfollowing update ess is neverthele
m: several initiatire described belothe healthcare
ealth information ontral question, linecord, and to tht reflect this issu
ospital data of theion medication pre
ome initiatives areon” (https://www.rg run, such as thout many conne
ata to evaluate thean important role
atives but few da
y difficult to meahealth system’s
he patient or to eeasure this, th44 s’ patient-centeredltation process: r
Survey (HIS) is at provides a mea
m, an indicator thany critiques, bothof satisfaction.77
ces, in the next waa question on th
ces (GP or specperience with amof this report.
ess a matter of coves have been ow. These 3 initsystem to the
of a patient at anyked to the one o
he access to it. ue: the % of geir patient, and theescribed at any s
e already in place,reseausantewallon
Vitalink in Flanections between tem. In this matteto play.
ata
asure with quantiability to succes
encourage the pathere are two
dness;145 rating scales or v
major source ofasure of the patat has been discuh on the validity o7, 78 To improveave of the HIS thehe patient’s expercialists), based obulatory care will
oncern for the Belaunched in Beliatives emphasizpatient centered
135
y time of the
Two eneral e % of etting such n.be/) nders them,
er, the
tative ssfully tient’s main
verbal
f data tient’s ussed of the e our e item rience n the l thus
elgian gium. e the dness

136
approach. Morequality. First, since 20complaints in pmotive of compthe follow-up oversus 9 026 icarefully: morealso to more availability, compatients’ culturdevelop a simresolution procoperational. Second, since financial suppomediation coornegative impacmediators havemode of organavailability durinhours in case oHealth ensuresassessment enbooklet editing.needs and rescomply to all laare taken carestarted recentlconferences). Iwith interculturaThis project willThird, some pithe patients' inquality manage
e detailed analys
03, an ombudsmpublic hospitals. Tplaints each year of the complaints.in 2006. Howeve registered comp
effective ombumprehensivenessre of complaints.ilar indicator for
cess in general p
1999, general anort to create a pordinator. Linguistct on access ane done more than nization is hospitang office hours onof an emergencys the follow-up ancompasses patie.. However, an asponses quality isnguage translatio of in some hospy (2012) to allon this pilot projecal support and all be evaluated eaclot projects are rvolvement in dec
ement systems. In
sis should be per
man service existThis service recobut does not as
In 2010, 16 907er, these numberplaints can refer udsman servicess of the recordin There is also aassessing the e
practice146-148. In
d psychiatric Belgost of interculturaltic and cultural nd quality of car80 000 interventi
al dependent: onenly or also very exy. The coordinatioand the assessmeents encounters,ssessment of reas lacking. Moreovons (no less than pitals). In this co
ow mediation suct, a network is slso local medical ch year. recently launchedcision concerning n 2013, several p
Belgian
rformed to evalua
ts for managing ords the number sess the justifica
7 records were rers should be intto declining serv
s in terms of vg… or a changean international existence of a coBelgium, this is
gian hospitals canl mediator or intebarriers have in
re. In 2009, inteons in 17 language or several medxceptionally duringon cell of the FPSent of the reques
care providers l patients’ (or phyver, it remains di170 different nati
ontext, a pilot propport by interneset up between hhome or health
in Flanders to stheir disease in
public hospitals w
n Health System
ate their
patients’ and the tion and
egistered erpreted
vices but visibility, e in the trend to omplaint not yet
n ask for ercultural ndeed a ercultural ges. The diator(s); g out-of-S Public sts. The training,
ysicians’) fficult to onalities
oject has t (video
hospitals centres.
stimulate hospital
will allow
thM
LBLnlotoSdinepndinAdTccUs(cdth
w
Performance
he participation oMeasurement of q
Long-term care: BelRAI assessmeLong-term care ineeding assistancong-term care relaopic have been diSome indicators disabled elderly pan residential careelderly physically pressure ulcers annot been measurdomain. Howeverndicators. At the internationdeveloping a projeThe proposed framcare services wilcountries (AustralUnited States). Tsafety as key qincluding respons
coordination and development of pohe shortcomings.
w The Residen
assess the cextended witBelgium a nimplemented care, for longto the Belgiaperformance
of patients’ represuality indicators is
no data currentent n this report ref
ce (mainly in residated to mental heiscussed above. have been chosatients, as the pree or receiving ho
restrained, the nd the problem ofred, which highli, the BelRAIw wil
al level, a workiect specifically fomework for monitol be based on tia, Canada, Engl
This framework pquality dimensionsiveness, empow
integration. Tholicies to achieve The release of th
nt Assessment Inscare needs of the th instruments for
national pilot projec in all care setting
g-term care facilitiesan situation. Data a
report.
sentatives in thes soon expected i
tly, waiting for fi
fers to long-termdential care or recealth problems. In
sen to assess thevalence of malnu
ome care (BMI <1prevalence of fa
f polymedication. Tights the currentll soon provide d
ng group from thor long-term care4
oring and improvithe national framland, Finland, theprioritised care efns, followed by werment and com
e final phase quality in long-ter
he report is planne
strument (RAI)44 is elderly in institutiodifferent care sett
ct (the BelRAI) is gs. The assessmens and acute care haare expected before
KCE Report
ir board of govern this domain.
irst results using
m care for the eceiving home caredicators from the
he long-term carutrition in elderly 19), the percentaalls, the incidencThose indicators t lack of data inata on some sel
he OECD is cur45, focusing on qung quality in long
mework of six Oe Netherlands anffectiveness and patient centered
mmunication) and in the report isrm care and to aded for the end of 2
originally developons, and has later tings and subgrouongoing, but is no
nt instruments for ave already been ade the edition of the
t 196
rnors.
g the
elderly e) and
latter
re for being ge of ce of could
n this ected
rrently uality. g-term ECD-d the user
dness care
s the dress
2012.
ped to been
ps. In ot yet home
dapted e next

KCE Report 196
Efficiency desObviously, efficfew indicators efficiency meascould certainly
End-of-life car
The few indicatpatients dying palliative care patients eligibleavailability. Moron accessibilitylocal studies (eon restricted nuover time, and aim is to be repof care, end-of-international org
Health promotalready availabHealth literacy in health managto understand aindividuals the as a priority of atools have beenhealth literacy build and validaof health literaBelgium did not
6
erves more attenciency in healthca
selected in thissures which explbe an interesting
re: many local stu
tors measured in from cancer, orat home. This d
e for palliative creover, so far no
y nor on quality ofespecially from Flumber of patientshence cannot be
produced every fe-life care is little oganisations.
tion: data on heble in other Eurois a relatively newgement. It can beand manage factoopportunity to maaction for the 200n used in the worhas developed a
ate 12 indicators. acy. A first survet participate.97
ntion in future rere cannot be suffs work. Internatiicitly identify inpuarea of research.
udies in Belgium
this report are bar on the populatidoes not cover are, which highlidata at national lef end-of-life care landers) are well
s, do not allow stue included in a peew years. Compaor not at all repres
alth literacy are opean countries w concept considee defined as the iors interacting withake healthier cho
08-2013 Europeanrld to measure it. a comprehensiveThose intend to
ey occurred in Eu
Belgian
eport iciently assessed onal literature puts and outputs.8
m, but few nation
ased on the popuion of patients rthe whole populights a real gap evel have been pin Belgium. Resuavailable, but ar
udying evolution oerformance repor
ared to the other dsented in databas
lacking, while t
ered as a crucial rndividual skills neh one’s health. Th
oices. It has beenn Union strategy. DThe European pr questionnaire ameasure various urope in 2010-20
n Health System
with the proposes 8, 16 This
al data
ulation of receiving lation of in data
ublished ults from re based of trends rt whose domains ses from
they are
resource ecessary his gives defined Different roject on iming to aspects
011, but
1TpsrepqItminessBsfoseeRmadpmo
Performance
10 GENERAThis report preseperformance of thstudy. By means eport intends to
performance, poinquestions for furtht represents a submore comprehensndicators. Moreoevolution. Also, imsince the last editsurvival. Belgium is not thesigning of the 200ormally committedsystem performanexperience with example for this rReport. One of measurement (alsavailability of up todynamic publishinproblem. Yet, this makers commit thof the performance
AL CONCLents the resultse Belgian health of seventy-four
o provide an ovnting to some direer follow-up or resbstantial improvemsive and by updaover, it allows important previoustion, like the caus
e first country hav08 Tallinn Charter d themselves to tnce. Several neihealth system preport. This is cethe weaknesses
so identified in foro date data. Regung of results onis only one of the
hemselves to a sye of the Belgian h
LUSION of a first globsystem, building indicators with n
verall overview oections for policy asearch. ment over the pre
ating the former sn some cases s gaps in basic se-specific mortal
ving exercised thon health system
the monitoring anighbouring countperformance meaertainly true for ths hampering surmer Dutch perfoular updating of a
n a website coue options that can ystematic measurealth care system
bal evaluation oon a former feas
numerical valuesof the health syactions and gener
evious report, by set with more relthe measuremedata have been ity rates or the ca
his challenge. Witms, the Member Snd evaluation of htries, having yeaasurement servehe Dutch Performccessful performrmance reports)
administrative datald partially solvebe considered if p
rement and monitm.
137
f the sibility s, this ystem rating
being evant nt of filled
ancer
th the States health ars of ed as mance mance is the a and e this policy toring

138
APPEAPPENDTIER OF Health Status
• Life expec• Health exp• Self-perce• Infant mor
Dimension
Accessibility
ENDICESIX 1. LIST THE HEAL
ctancy pectancy eived health rtality rate
DomGen
•
•
•
•
•
S OF INDICA
LTH SYSTE
main of care neric
Number of practphysicians (per population) Number of practnurses (per population) Coverage hinsurance statuthe population Amount of payments and opocket payments% of people delay con
Belgian
ATORS MEEM, DOMA
Preventiv
tising 1000
tising 1000
health s of
co-ut-of-
s who
ntacts
• Covecance
• Covecervicscree
• Covevaccicover
• Coveinfluevaccielder
n Health System
EASURED AIN OF CAR
Healthcare
ve Care Cu
erage breast er screening
erage cal cancer ening erage nation rage children
erage enza nation for ly
Performance
IN THE 20RE AND DI
e
urative Care
12 REPORIMENSION
Long-t(elderlyhealth)• Nu
resfacpoye
• % ovrepinfo
RT, CLASS
term care y/mental ) umber of beds in sidential care cilities per pulation 65 ars and older
of population er 50 years old porting to be an formal carer
KCE Report
IFIED BY
End-of-Life Ca
• % of pawho died wone week start palliative service
t 196
are
atients within
after of
care

KCE Report 196
Quality - Effec
Quality - Appropriatene
6
tiveness
ess
because of finareasons
Belgian
ancial
• %aged old wmamwithinyears
• % aged old wmamwithinyears
n Health System
•
•
•
•
of women 40-49 years
who had a mogram n the last two s of women 70-79 years
who had a mogram n the last two s
•
•
•
•
Performance
5-year survival ratebreast cancestage 5-year survival ratecervix cancestage 5-year survival ratecolon cancestage Hospital admfor asthma Prescription antibiotics acto guidelines % of adult dreceiving appcare, in terregular retinal and blood testsGeographic vain caesarean s(per 1000 live bAverage daily qof me(antidepressanantipsychotics,hypnotics anxiolytics) prescribed
relative e after er, by
relative e after er, by
relative e after er, by
missions
• Su• Ra
copehope
• Paby mewoem
of ccording
iabetics propriate rms of
exams s ariability sections births) quantity dication
nts, ,
and
uicide rate ate of involuntary mmittals as a rcentage of all spitalizations r year
articipation rates people with
ental illness of orking age in mployment
• % of capatients receiving chemotherin the lasdays of life
139
ancer
rapy st 14 e

140
Quality - Safet
Quality - ContiCare
Quality - Patiecenteredness
Equity
y •
inuity of •
•
nt •
•
•
Medical radiexposure of population
Coverage of gmedical record Usual providercare index
Satisfaction health care servic
Indicators of progressivity of phealthcare financGini coefficient band after taxation
Belgian
iation the
global
r of
with ces
the public cing efore n and
n Health System
•
•
•
•
•
•
•
•
Performance
Incidence of acquired infections Incidence of operative sepsIncidence of pulcers in hospitIn-hospital mafter hip fractu% of persons65 years or prescribed antidepressantan antichoantidepressant% of cancer discussed amultidisciplinarmeeting % of phencounter hospital dischaelderly patients
Assessment olevel hospitalization
hospital MRSA
f post-sis pressure tals
mortality re s aged
older
ts using olinergic t drug
patients at the ry team
hysician after
arge for s (65+)
• % fropareapsypaocda(scbip
of pain during
of discharges om psychiatric in-tient care admitted to ychiatric in-tient care that curred within 30 ys
chizophrenia, polar disorder)
KCE Report
• Number contacts between patient andGP in the months of
• Patients in their place residence
t 196
of
the d the last 3 life
dying usual
of

KCE Report 196
Efficiency
Sustainability
Health Promot
Type of indica
Health outcom
Intermediate healthy lifesenvironments
Health promot
6
•
•
• • •
•
tion
tor
mes
health outstyles and
tion outcomes
transfers % prescription ofcost drugs
Medical gradubecoming GP Mean age of GPNursing graduate% of GPs usinelectronic medicaHealth expendi(total, distributioof gross domproduct, per capi
Indicat
• % • Av• Inc
tcomes: healthy
• % • % • % • % • % • % • % • % • To
Belgian
f low-
uates
es g an al file tures n, %
mestic ta)
tor
of overweight or verage number of cidence of HIV of daily smokers of problematic alcof daily consumpof daily physical aoffer of physical ahealth promotionof schools with hof persons with p
obacco Control Sc
n Health System
••
•
obese adults decayed, missing
cohol drinkers (3
ption of fruits and vactivity activity at primary policies in the muealth promotion d
poor social supporcale
Performance
% surgical dayAverage lengstay for delivery Acute care be(number per ca
g, filled teeth in ch
indicators) vegetables
y and secondary leunicipalities
dimension in their rt
y-case gth of normal
ed days apita)
hildren at age 12
evel in schools
school project
141

142
APPENDThis section list
Indicator in 20
Accessibility
A1: Number ofNo data availa
A4: Coverage
A5: AdditionalNo data availa
Quality
QA1: Prescripacute otitis meNo data availa
QA3A: Utilisat(laparoscopic
IX 2. LIST ts the modification
010 report
f physicians andble for the numb
of preventive ch
illness-related cble in 2010
ption according tedia, uncomplicable in 2010
tion of minimal acholecystectom
OF CHANGns that were done
d nurses ber of nurses in 2
hild health care
costs for chronic
to guidelines (Uated hypertensio
and non-invasiveies, PCIs)
Belgian
GES TO INe to indicators sinc
2010
cally ill people
rinary tract infecon)
e surgical techni
n Health System
NDICATORce the 2010 report
Status in
Some da
RemovedRationaleaim was tcriteria) onational accessibi
RemovedRationalepeople wstudy of feasible w
ction, Modified
iques RemovedRationaleoperativeefficiencypatients minimal-i(sustainainterventi
Performance
RS COMPAt. Indicators for w
n 2012 Report
ta available in 20
d in 2012 e: this indicator wto focus on infant
or infants from milevel were availaility.
d in 2012 e: The calculatiowould require a go
each identified cwithin the time-fra
in 2012
d in 2012 e: the use of mine complications, ley. However, thesand careful patienvasive techniqu
ability). In 2012, laons.
RED TO THhich no data were
12
was defined as ants from underprivilgrants. The previ
able, which makes
n of additional iood definition of chronic disease. me of the present
imal-invasive techength of stay andse techniques arent selection is es is also considaparoscopic chol
HE 2010 Re available in 2010
n indicator of accleged families (deious report showes it less interesti
llness-related cochronic diseasesThis is a projectt project.
hniques is a mead costs. It is there not considerenecessary. The
dered to be an inecystectomies an
KCE Report
EPORT 0 are in red.
cessibility, as its iefined according ted that only resulng as an indicato
osts for chronicals and a cost-of-illt in itself, and is
ans for reducing prefore an indicatod appropriate fouse of these nedication of innovand PCIs are stan
t 196
nitial o six lts at or of
ly ill ness s not
post-or of
or all ewer ation dard

KCE Report 196
QA4: Percentguidelines oprocesses
QA6: Hysterec
QC1: Number
QC2: Average
QE03: ColorecNo data availa
QE06: Acute influenza
QE07.3: Salt co
6
tage of institutiutlining proced
ctomy by social c
of people who a
length of stay (L
ctal cancer screeble in 2010
care hospital
onsumption
ons that use sdures for hig
class
re not registered
LOS) in acute car
ening
ization rates f
Belgian
special protocogh-risk or com
d with a GP
re hospitals
for pneumonia
n Health System
ls or mplex
RemovedRationaleindicatorsBelgian hdata will b
RemovedRationalesocial clapublicatio
Modified Rationale DMG, thwith a Gpercentag
Modified ChangedRationaleof care. efficient tspecific dused by t
Some da
and Modified Rationalethe mostvaccinatioredundanwhich is a
RemovedRationalestudy pub
Performance
d in 2012 e: this indicator, os, could only be ehospitals, and wasbe available in the
d in 2012 e: the results for 2ass, and hystereons on which this
in 2012 e: as the concept is indicator was r
GMD – DMG”. It ge indicates bette
in 2012 to more specific
e: this indicator waHowever, expertthe healthcare sydiagnosis was chothe OECD.
ta available in 20
in 2012 e: this indicator ist effective preveon, which is alrent. It was modifiealso an indicator u
d in 2012 e for exclusion: tblished in 2008, w
originally from thestimated via the ds furthermore base near future.
2010 showed no ctomies rates haindicator was orig
of “registered withredefined more sp
was also changer coverage).
LOS for normal das previously sees were convince
ystem is. Instead osen: LOS for nor
12, but data still to
s a measure of eention measure eady an indicatoed into “Acute cused by the OECD
he results for thiwhich will not be re
e Dutch healthcardiffusion and use osed on non-valida
differences in hyave been declininginally based.
h a GP” in Belgiumpecifically as “perged into a posit
elivery n as an indicator d that it was moof all hospitalizat
rmal delivery, whic
oo premature to p
effectiveness of pagainst influenzaor for influenza, are hospitalizatioD.
is indicator were epeated.
re performance sof clinical pathwa
ated results. No b
sterectomies rateng steadily since
m refers to the GMcentage of populative indicator (hi
of the good contiore indicative of tions in acute carch is also an indic
perform evaluation
preventive care. Sa and pneumoni
makes the indicon rates for asth
based on a Be
143
et of ys in
better
es by e the
MD –ation gher
nuity how
re, a cator
n
Since ia is cator ma”,
lgian

144
QE08: Breast f
QE09: Annual
QE10: DecayedNo data availa
QE11: CardiovNo data availa
QE12: Colon CNo data availa
QE13.1: PremaNo data availa
QE14: Breast CNo data availa
QE15: CervicaNo data availa
QE16b: In-hos(CAP)
feeding at 6 mon
check-up at the
d, missing, filledble in 2010
vascular screeninble in 2010
Cancer 5-year suble in 2010.
ature mortality. ble in 2010
Cancer 5-year suble in 2010
al Cancer 5-year sble in 2010
spital mortality a
nths of age
dentist for child
d teeth at age 12
ng in individuals
rvival rate
urvival rate
survival rate
after community-
Belgian
ren
s aged 45-75
-acquired pneum
n Health System
RemovedRationaleproposedexclusivein Belgiumand ONEONE: 24
RemovedAfter a thpossible t
Some da
This indicRationalespecific nnew GMD
Data avaSource: B
RemovedPrematurcorrelatedhas no Avoidable
Data avaSource: B
Data avaSource: B
monia RemovedRationaleafter hip
Performance
d in 2012 e: a new set of indd, and experts dide breast feeding ism. Moreover, the
E were not compaweeks).
d in 2012 horough examinatto isolate prevent
ta available in 20
cator was removee: this indicator wanomenclature codD – DMG+, which
ilable in 2012 Belgian Cancer Re
d in 2012 re mortality, expd with indicators potential for actie mortality would
ilable in 2012 Belgian Cancer Re
ilable in 2012 Belgian Cancer Re
d in 2012 e: this indicator wfracture”, both be
dicators to assessd not retain this ins hardly compatibl
previous report sarable, due to diffe
tion of the nomenive care at the de
12
d. as not measurabl
des. Since 2011 cwill be monitored
egistry
pressed as Potealready in the seion, as it does be a better indica
egistry
egistry
was linked to the eing indicators in
s performance of ndicator, mainly ble with the length showed that data erent time frames
nclature codes, it ntist for children.
e in the 2010 repcardiovascular pred.
ential Years of t (infant mortalitynot highlight the
ator.
indicator “QE16ancluded in feedba
KCE Report
health promotion because six month
of the maternity lefrom Kind and G
s used (KG: 3 mon
appears that it is
ort because of lacevention is part o
Life Lost (PYLL, life expectancy)e potential proble
a: In-hospital morack on quality of
t 196
was hs of eave
Gezin nths,
s not
ck of f the
L) is and ems.
rtality care

KCE Report 196
QS1: Incidence
QS2: Incidence
QS4: Incidence
QS5: Incidencindividuals at No data availa
Sustainability
S1.1: Amount
S2: Qualificatio
S4: Yearly amo
6
e of serious adve
e of healthcare r
e of post-operati
ce of pressure urisk ble in 2010
reimbursed by th
on levels of heal
ount of the Spec
erse effects of b
related infections
ive surgical site
lcers in long-ter
he maximum bill
lthcare providers
cial Solidarity Fun
Belgian
lood transfusion
s
infections
rm care facilities
ling system
s
nd (SSF)
n Health System
sent by thteam decindicator the 2010
n RemovedExtremely
RemovedChangedRationaleincidenceredefinedinfection”
ChangedRationaletype of osepsis”, national cindicators
s and Data not Source: B
Removed
Modified
RemovedRationaleand decisincluded
Performance
he FPS Public Hecided that the latthan mortality aftereport).
d in 2012 y rare events, so
d in 2012 to prevalence of
e: this indicator is e of all healthcad more specifical”, which is measur
to post-operativee: this indicator haperations coveredwhich can be mcoverage and a ws.
yet available in 20BelRAI
d in 2012
in 2012.
d in 2012 e: the SSF acts assions to reimbursein the previous s
ealth to Belgian hotter indicator, moer CAP, to assess
difficult to interpre
HAI, currently no not measurable (
are related infectly as “the inciderable.
e sepsis as low coverage, d. It has been cha
measured by admwider range of inte
012 (but soon).
s a safety net, bese treatment are bset as a sustaina
ospitals. During thortality after hip fs safety of care (a
et evolution over t
data. no surveillance sytions). This indic
ence of hospital-a
in terms of numbanged into “incideministrative data, erventions. It is a
sides the compulsbased on a case pability indicator, s
he review processracture, was a band not efficacy, a
time.
ystem can monitocator has thus bacquired bloodstr
ber of hospitals anence of post-opera
and hence inclulso included in O
sory health insuraper case basis. It showing the syste
145
s, the better as in
or the been ream
nd of ative udes ECD
ance, was
em’s

146
S6.1: Number
of acute care beds (per 1000 pop
Belgian
pulation)
n Health System
capacity tthe SSF (EMA), aThis is thsystem.
RemovedRationaledays, numoccupanc
Performance
to be responsive are usually thos
and are reimbursehus not a very re
d in 2012 e: this is a secondmber per capita”.cy rate and length
to emerging needse waiting for aped by compulsoryelevant indicator
dary indicator link. The latter was p
h of stay.
ds. However, treapproval by Europy health insurancof the sustainab
ked to the indicatopreferred because
KCE Report
tments reimbursepean Medical Agece after this approility of the health
or “S6 acute caree it also account
t 196
ed by ency oval.
hcare
bed s for

KCE Report 196
APPENDMEASURThis appendix evaluate the pewill be availableto present thoseFor each indicaare indicated. Health Promotio• % of peop
DMG+) (preventiveThe globalGP. The additional cplay a majstate of p(vaccinatioGMD – DMcoverage promotion.Source of d
Continuity of ca• Percentag
chronic caencounterchronic caPathways fof these papatients wphysicians registrationregistered participatio
6
IX 3. LIST RABLE IN A
lists the indicaterformance of the e in a near futuree results in the ne
ator, a short ration
on ple (aged 45-75) (specific consue care) medical record iGMD – DMG+,
component of preor role in health pplay of risk fac
on and screening)MG+ is a tool to
of the GMD –
data: RIZIV – INAare ge of patients reare (diabetes/renr for patients reare (diabetes/renfor chronic care aathways is to impwith chronic di
and other hn in a pathway
in the pathwayson in this public inv
OF INDICAA NEAR FUtors that were sBelgian health sy
e (i.e. in a 3-yearsext issue of this renale is provided, a
with a global multation on h
is a medical file cintroduced in A
evention and healtpromotion. It is thctors, organize ), and counsel forhelp the GP in
DMG+ is thus
AMI
egistered in an anal failure) and gistered in an a
nal failure) are set up in Belgprove follow-up aisease, general
healthcare profesis voluntary, the
s of care is a ivestment. Accord
Belgian
ATORS UTURE selected as pertystem, and for whs time frame). Theeport. and (future) source
edical mecord+ealth promotio
centrally managedApril 2011, contath promotion. Thehe right person to
preventive intervr healthy behaviothis task. Monitoan indicator of
ambulatory pathfrequency of ph
ambulatory path
gium since 2009. nd collaboration b
practitioner, sssionals. Becau
e percentage of ndicator of the
ding to the RIZIV –
n Health System
tinent to hich data e idea is
e of data
(GMD –on and
d by the ains an
e GP can make a
ventions urs. The
oring the f health
way for hysician way for
The aim between
specialist use the
patients patients’ – INAMI,
•
Performance
there were 20renal failure currently unknwhich aims tobe presented Source of data
% of visits mental healthAlthough unfohealth, mentaindicator of pcommunity trmental healthutilization ratehigh.150 Highlyto enter treatneed for emeeffective liaisoresources redservices/clienvisits are nocommunity. overcrowding likelihood of mIn the US, it hroom visits arthe importanchealth in emenumber of visspecialist in eshould be a accessible forSource of datRCM – MKG)not be measu
0 176 registered on 31 October 2
nown. This item wo evaluate the pain May 2013. a: ACHIL project to the Emergenh and/or substanoreseen and unaval health related poor coordinationreatment system h related problees of emergencyy accessible outpment before reacergency room vison between emeduces the use ots. High rates of
ot only a concerIt is also a c
results in decrmedical error.150
has been illustratere on the rise for mce of the availabrgency rooms to mits for psychiatric
every emergency minimum protoco
r immediate care fta: RHM – MZG s. Due to delays inred in this report.
pathways for dia011.142 But the will be estimated thways for chroni
ncy Rooms in gnce-related problvoidable emergen
emergency roomn of care and se
to support servems is regarded y departments of atient care is con
ching the crisis stsits.149 In additiorgency rooms an
of emergency roomental health rel
rn for members concern that emeased quality of
ed that mental heamore than one de
bility of expertise manage these criproblems, availabroom may not b
ol by which menfor every citizen.15
since 2008 (informn accessing the da
abetes and 15 42exact denominat by the ACHIL pic care. Evaluatio
general hospitallems cies do arise in mm use is used aervice failures.149
vices for peopleas ineffective
general hospitalnsidered to help ptage and minimiz
on, it is assumednd mental health oms for mental hlated emergency of the mental h
mergency departf care and incre
alth related emergecade.151 This stre
in the field of mses. Depending obility of a mental h
be practical. Still, tal health expert52 mation not availabata, this indicator
147
28 for tor is roject
on will
s for
mental as an 9 The with when s are eople
ze the d that crisis
health room
health tment eased
gency esses
mental on the health there ise is
ble in could

148
Patient-centere• Patient ex
Patient-cencommunicaaddressed A good com(listening, questionnathe quality the Healthinstrument Source of d
Long-term CareThe majority of
x The Resid
assess theinstrumeninstitutionacare, acustructuredplanning different itthe elderly
In Belgiumimplemencare and are adapte
The interstandardizpreferenceinstitutionaconsistentassessmethe functiouse of caspecific tr
edness periences with antered care is ation so that patieand patients und
mmunication is noexplaining, court
aire on patient exof the consultatio
h Interview Survdedicated to the
data: next Health e indicators will be
dent Assessment Ie care needs of the
nts for different caal mental healthcaute hospital care d and standardized and quality monitotems, resulting in a y. m a pilot project (thted in all care setfor long-term care ed to the Belgian sitrRAI for long-terzed instrument to ees of the residents al setting) and aimt assessment sys
ent instrument givesonal capacity, the mare of the individuriggers for care p
ambulatory servisupported by
ents’ needs and wderstand and partot easy as it requitesy…) In 2011 txperiences with soon.15 The WIV –vey (2013) the patient experiencInterview Survey,
based on the Bel
nstrument (RAI)44
e elderly in institutionare settings and sare, ambulatory mand persons withassessment aims t
oring. Different caremultidisciplinary ap
he BelRAI) is ongoittings. The assessmfacilities, for acute tuation. rm care facilitiesevaluate the needsin a long-term care
ms to stimulate thstem and a paties a description of thmental and physica
ual resident, wherelanning. Next to t
Belgian
ces good provide
wants are understticipate in their owres several compthe OECD has eome questions reISP decided to inmodule of the
ces with ambulator, WIV – ISP
lRAI project x
was originally devens, but is later extenubgroups (post-acu
mental healthcare, h mental disabilitieto realize a high-que providers can aspproach of the care
ing and is not yet nment instruments fcare and for pallia
s (interRAI-LTCF)s, the competencese setting (care homehe continuity of caent-focused approahe most important aal health, the needseby most items funhe assessment ins
n Health System
r-patient tood and wn care. etencies edited a elated to nclude in OECD ry care.
eloped to nded with ute care, palliative es). The ality care
ssess the needs of
nationally for home ative care
153 is a s and the e or other are via a ach. The aspects of s and the nction as strument,
•
•
Performance
Evolution ovinstitution)Source: BelRA
Prevalence oOlder personcomplicationsand swallowincognitive funindicator will belongs to thproject.45 Source of data
analysis protinterRAI-LTFDutch and FrThe InterRAassessment patients but ahospitalisatiopreferences oclient. The (standardisedSome items risks for funcCAPs. Theseand for indivdomains anmultidisciplinathe priority ofsituation and
ver time in utiliz
AI of malnutrition byns are particulars such as changesng problems, chanction and deter
be available in he set of indicato
a: BelRAI
tocols are developeC has been adapte
rench (BelRAI-LTCFAI for home care
system to guide also for patients wit
on). The evaluatioof the client indicate
interRAI-HC cod scoring scheme) of the instrument fctional deterioratione CAPs contain gevidualized care an
nd each triggeredary consultation to f each CAP. The intranslated into Dutc
zation of BelRA
y elderly (BMI <1rly vulnerable tos in appetite and
ange in nutritionalriorating vision.15
the BelRAI datrs in the OECD
ed as guidance for
ed to the Belgian situF). e (interRAI-HC)154
the home care plth post-acute care n of the needs, e the functioning anonsists of the
and the CAPs (clifunction as triggersn and link the inteneral guidelines fo
nd services. The 3d CAP needs todetermine the neceterRAI-HC has beech and French (BelR
KCE Report
AI (home care an
9) o malnutrition du
energy level, chel requirements, lo55 The data fortabase. This indlong-term care q
r the care planninguation and translate
4 is a person-cenanning for chronicneeds (for examplethe strengths an
nd the quality of life assessment instrunical analysis proto for specific probleerRAI-HC to a serr the further asses
30 CAPs cover difo be discussed dessary care service
en adapted to the BRAI-HC).
t 196
nd in
ue to ewing oss of r this icator
quality
g. The ed into
ntered c care e after d the of the ument ocols). ems or ries of sment fferent during
es and elgian

KCE Report 196
• Percentagthe last 7 dRestraint-frHowever, ilong-term cOECD longSource of d
• PercentagFall incideelderly. Peincidents. T12 monthsan accidencause of thand in persthe fall cauBelRAI-LTCdeterminescare qualitrelated fracsafety.45 Source of d
• Incidence individualsThe occurrserious nega much prwith good qit will be pindicator is
6
ge of residents wdays ree care should n reality, physicacare.156 This indicg-term care qualitydata: BelRAI
ge of residents wents are a commersons who fell onThe most recent H
s preceding the innt resulting in a mhe accidents weresons of 65 years aused a fracture. WCF and the Bels the risk on fututy project the indctures is proposed
data: BelRAI of pressure ulc
s at risk (home crence of a pressgative impact on rolonged hospitalquality nursing capossible to evaluas also included in
who were physi
be the aim of hl restraints are co
cator belongs to thy project.45
who had a fall durmon cause of mnce, have an incHealth Survey Int
nterview 7% of thmedical consultatioe falls (54%) and and older. In moreWithin the domainlRAI-HC, a subdure fall incidents.dicator on the incd as example of a
cers: a. in long-tcare) sure ulcer in a hothe individual’s h stay. Pressure re.58, 59 Currently ate this indicator n the set of OEC
Belgian
ically restrained
igh quality nursinommonly used in he set of indicato
ring the last 30 dorbidity and mor
creased risk on futerview reports the Belgian populaon.157 The most cwere common in e than 40% of then of state of healtdomain on fall i In the OECD locidence of falls aa quality outcome
term care faciliti
ospitalised patienealth57 and often ulcers can be prno data are availausing BelRAI da
CD indicators in q
n Health System
d during
ng care. geriatric rs in the
days rtality in uture fall at in the tion had common children
e elderly, th of the ncidents ong-term and fall- on user
es b. in
nt has a leads to
revented able, but ata. This quality of
•
E•
Performance
long-term careSource of data
Prevalence oThe WIV – ISbe avai(http://www.nsSource: WIV –
Efficiency Chronic care
patients withThere are diffThe patients peritoneal diatransplant, eittransplantatiowhenever posSubstitution oless expensivcentres and pmany other comechanisms modified the fof introducingis categoriseddialysis is notis also considSource of datthe EPS, but draw any condatabase.
e.45 a: BelRAI
of MRSAs in nursP is currently finailable at sih.be/nursing_ho– ISP
e: patients with h dialysis ferent treatment o
can be dialysealysis. In both casther from a decean is considered
ssible. of the more expeve alternatives sucperitoneal dialysisountries. This is tfor dialysis. Sinc
financing system incentives for sud in the performat indicated for all pered an indicator ta: IMA. Preliminathe sample of p
nclusion. Analyses
sing homes alizing a study, of
the enomes/inleiding_fr.a
home dialysis a
options for patiened, either with hses patients can
ased or a living dod to be the mo
ensive haemodialych as low-care has has been slowhought to be partce 1995 the Bela couple of times
ubstitution. For thiance dimension epatients with end-of appropriatenes
ary analyses for tatients under dias will have to be
f which the resultd of asp).
s a percentage
nts whose kidneyhaemodialysis or
also receive a konor. Ultimately, kost preferable o
ysis in hospital baemodialysis in sawer in Belgium thtly due to the finalgian governments, with the explicits reason, the ind
efficiency. Since -stage renal diseass. his report were ru
alysis was too smdone on the tota
149
ts will 2012
of all
s fail. with
kidney kidney ption,
by the atellite an in
ancing t has t goal icator home ase, it
un on mall to al IMA

150
REFEERENCES
Belgiann Health System
1
2
3
4
5
6
7
8
9
1
1
Performance
. Vlayen J, Kohn L, etthe BelgiaKnowledg
2. WHO RegassessmeCopenhagEurope; 20
3. WHO RegSystems fOrganisathttp://www8.pdf
4. Arah OA, frameworkInt. J. Qua
5. OECD. Hefor Econom
6. Vlayen J, RamaekerBelgian He41
7. Coppens Eactieplan s
8. AHRQ IdeEfficiency Available f
9. Smith PC,an agendaEurope anPolicies; 2
0. WHO. Woperforman
1. OECD. He
Vanthomme K, Ct al. A first step to
an healthcare syste Centre (KCE); 2
gional Office for Eent, a tool for healtgen: World Health012.
gional Office for Efor Health and Weion; 2008. Availab
w.euro.who.int/__d
Westert GP, Hursk for the OECD Heal. Health Care. 20ealth at a Glance mic Co-operation Van De Water G,rs D, et al. Indicatealth Care Knowle
ES, G. Van Audensuïcidepreventie (
entifying, CategoriMeasures. AHRQfrom: http://www.a, Papanicolas I. Ha for policy, informnd European Obse2012. Policy Summorld Health Reportnce. Geneva: Worealth at a Glance
amberlin C, Piérawards measuringtem. Brussels: Be2010. KCE Reporurope. Health systh governance in
h Organization, Re
urope. The Tallin ealth. Copenhagenble from: data/assets/pdf_fi
st J, Klazinga NS.ealth Care Quality006;18(SUPPL. 12011, OECD Indicand Developmen Camberlin C, Pateurs de qualité cledge Centre (KCE
nhove, C. De eva(2006-2010). Leuvzing, and Evaluat
Q; 2008. AHRQ Pahrq.gov/qual/efficealth System Per
mation and researervatory on Healthmary 4 t 2000. Health sysrld Health Organiz2010 Europe. OE
KCE Report
art J, Walckiers D, the performance lgian Health Carerts 128 stems performancthe 21st century.
egional office for
Charter: Health n: World Health
le/0008/88613/E9
A conceptual y Indicators Proje):5-13. cators. Organisat
nt; 2011. ulus D, Leys M, iniques. BrusselsE); 2006. KCE rep
luatie van het Vlaven: Lucas; 2011ting Health Care ublication No. 08-ciency/efficiency.prformance comparch. Brussels: WHh Systems and
stems: improving zation; 2002. ECD Publishing; 2
t 196
, of
e
ce
9143
ct.
ion
: ports
aams .
-0030 pdf rison: O
010.

KCE Report 196
12. OECD.operatio
13. Europe[2012. Ahttp://ec
14. BjörnbePowerh
15. OECD.patient operatio
16. JacobsCare. C
17. Stahl TPoliciesHealth
18. WHO reimplemCopenh
19. WHO repolicy fWorld Hhttp://wHealth2
20. Westercare peNationa
21. CIHI. Hrationa
22. NationaPerformHealth
23. WHO. OOrganiz
6
Health at a Glancon and Developm
ean Commission HAvailable from: c.europa.eu/healterg A. Euro Healthhouse; 2012. Health Care Quaexperiences. Paron and Developm
s R., Smith PC, StCambridge: CambT, Wismar M, Olillas, Prospects and Systems and Polegional Office for
mentation of the Tahagen: World Heaegional Office for for health - HealthHealth Organisatio
www.euro.who.int/_2020_110419_engrt G, van den Bergerformance reportal Institute for Pub
Health indicatiors 2le. Ottowa: Canadal Health Performamance Framework Ottawa Charter fozation; 1986. Ava
ce Europe. Organment; 2012. HEIDI data tool: he
th/indicators/indicah Consumer Index
ality Indicators. OEris: Organisation fo
ment; 2011. reet A. Measuring
bridge University Pa E, Lahtinen E, LPotentials. Europeicies; 2006. Europe. Interm re
allinn Charter (stillalth Organisation; Europe. Develop 2020 (working paon; 2011 Available__data/assets/pdfg.pdf g M, Koolman X, Vt 2008. Bilthoven. blic Health and the2010: definitions, dian Institute for Hance Commitee (k Report. Brisbane
or Health Promotioilable from:
Belgian
nisation for Econo
ealth status indica
ators/index_en.htx 2012. Health Co
ECD pilot questionor Economic Co-
g Efficiency in HeaPress; 2006. Leppo K. Health inean Observatory
eport on the l in draft version). 2012. ing the new Europaper). Copenhague from: f_file/0010/13429
Verkleij H. Dutch hThe Netherlands
e Environment; 20data sources and
Health InformationNHPC). National e: 2001. Queensla
on. World Health
n Health System
omic Co-
ators
m onsumer
ns on
alth
n All on
pean ue:
9/07E_
health : 008.
n; 2010. Health and
2
2
2
2
22
3
3
3
3
3
Performance
http://wwwa_Charter
24. OECD, Eulongterm coperation
25. Van de VoAppraisal,Health Ca
26. Meeus P.,bilan de saInsurance
27. DGSIE. Ev- Belgiqueet Informa
28. European 29. Eurostat. E
http://epp._database
30. FPS HealtAanbod GGezondheGegevensService Pu
31. Communacolorectal http://wwwang=fr
32. Candeur Mdépistage
33. Hoeck S., bevolkingshttp://www
34. IMA-AIM. 2002-2003
w.euro.who.int/__dr.pdf urostat, WHO. Cocare expenditure. and Developmen
oorde C, Léonard Health Services
are Knowledge Ce, Van Aubel X. Peanté. Brussels: Na (NIHDI); 2012. volution de l'espé
e et régions (1997ation Economique
Commission - DGEurostat databaseeurostat.ec.europ
e th Food Chain Sa
Gezondheidsberoeeidszorgberoepenskoppeling Verpleublic Health 2012auté française Proen Communauté
w.cancerintestin.be
M., Carbonnelle S. Santé en CommVan Roosbroek S
sonderzoek naar dw.dikkedarmkankeProgramme de D3 et 2004-2005. 2
data/assets/pdf_fi
nceptual framewoOrganisation for t; 2088. C. Search for EviResearch (HSR).
entre (KCE); 2007erformance de la mational Institute fo
rance de vie à la -2010). Direction ; 2012. G Health and Cone. EUROSTAT; 20pa.eu/portal/page/
afety and Environmepen - Dienst Stran. Voorlopige resuegkunde 2004-20.
ogramme de dépisfrançaise [Availae/spip.php?rubriq
S., Vandenbrouckemunauté françaiseS., Van Hal G. Pilodikkedarmkanker
er.be Dépistage du Canc2007 2007, Septem
le/0004/129532/O
ork and definition Economic Co-
idence and Critica Brussels: Belgian. KCE Process no
médecine généralor Health and Disa
naissance, en anGénérale Statistiq
nsumers. 2012. 012. Available fro/portal/statistics/se
ment - Cel Planninategische Coördinltaten PlanKAD
009, Federal publi
stage du cancer ble from:
que35&mode=pub
e A. Cancer colore. Mars 2011;6. ootproject . 2011. Available
cer du Sein. Périomber.
151
Ottaw
of
al n otes le, ability
nées que
om: earch
ng atie
c
blic&l
ectal:
from:
odes

152
35. HulstaeM. DépPapillomKnowle
36. Arbyn Met al. APap smcervix (2009;48
37. Sabbe BelgiumSurveil
38. SuperioSaison Supérie
39. WHO. PEpidemFifty-Sixhttp://a
40. IMA-AI2008 etima.be/pport%
41. Van dede SanProjectCentre
42. Gielen expendbetweePolicy.
43. Gielen onder d
ert F, Ramaekers pistage du cancer mavirus humain (edge Centre (KCEM, Simoens C, Vanalysis of 13 millio
mears, colposcopie(Belgium, 1996–28(5):438-43. M, Hue D, Hutse
m from January tol. 2011;16(16). or Health Council.hivernale 2007 –
eur de la santé n°Prevention and C
mics. World Healthxth World Health pps.who.int/gb/arcM. Vaccination cot 2008-2009. 201/library/documents20hivers%202007
en Bosch K, Willemde S, et al. Residions 2011-2025. B(KCE); 2011. KCB, Remacle A, Me
diture during the laen age categories 2010;97:53-61. B, Remacle A, Me
de loep: de cijfers
D, Puddu M, Vincdu col de l’utérusHPV). Brussels: B
E); 2006. KCE Repan Oyen H, Foidaron individual patiees, biopsies and s000). Preventive
V, Goubau P. Meo mid-April 2011: a
. Vaccination cont– 2008. In: Publica
8354.; 2007. ontrol of Influenza
h Organization; 20Assembly (WHA5chive/pdf_files/WHontre la grippe au 1. Available from:s/health_monitori7-2008%202008-2mé P, Geerts J, Bential care for oldBrussels: Belgian E Reports 169 ertens R. Patternsast 6 months of lifein cancer and no
ertens R. De CM . Christian Sickne
Belgian
ck I, Huybrechts Ms et recherche du Belgian Health Caports 38 rt J-M, Goffin F, Sent records pertaisurgery on the uteMedicine.
easles resurgencea preliminary repo
tre la grippe saisoation du Conseil
a Pandemics and 003. Resolution of56.19) Available frHA56/ea56r19.pdcours des hivers http://www.nic-ng/Grippe%20FR2009%20AIM.pdfreda J, Peeters S
der persons in BelHealth Care Kno
s of health care use in Belgium: diffen-cancer patients
neemt het levensess Fund; 2008.
n Health System
M, Arbyn
are
Simon P, ning to
erine
e in ort. Euro
onnière.
Annual f the rom: df 2007-
R%20Raf S, Van gium: wledge
se and erences . Health
seinde
4
4
4
4
4
4
5
5
5
5
Performance
44. InterRAI ASystems [http://www
45. OECD. LoOrganisat
46. Van Hoof Goolaerts Wetensch2012.
47. Reynders AudenhovrechercherégionalesLucas; 20
48. MambourgDépistageHealth Ca
49. Mambourgentre 70 eCentre (KC
50. FPS HealtmultidimenSafety and
51. Jacques JRamaekeren Belgiqu(KCE); 20
52. Gordts B, 2007 Belginfections.
53. Jans B, Deziekenhuizhttp://wwwhttp://www
An overview of the2012 [cited 30th o
w.interrai.org/sectiong-term care quaion for Economic E, Remue E, LenJ. Evaluatie van appelijk Instituut V
AV, B. Scheedreve, C. L'effet des fe d'aide sur le coms entre la Wallonie11. g F, Robays J, Ca
e du cancer du seiare Knowledge Ceg F, Robays J, Geet 74 ans. BrusselsCE); 2012. KCE Rth Food Chain Sansionnel. Federal d Environment; 20J, Gillain D, Fechers D, et al. Etude ue. Brussels: Belg06. KCE Reports Vrijens F, Hulstae
gian national preva. The Journal of henis O. Surveillanzen: tweede semew.nsih.be/surv_mrw.nsih.be/surv_mr
e interRAI. Family of Mai]. Available on/view/?fnode=1
ality project: propoCo-operation and
naerts L, De Wandhet Kankerplan 20Volksgezondheid,
r, G. Declercq, A.facteurs sociocog
mportement suicide, La Flandre et L
amberlin C, Vlayein entre 40 et 49 a
entre (KCE); 2010erkens S. Dépistas: Belgian Health
Reports 176B afety and Environm
Public Service H008. er F, Van de Sanddes disparités de
gian Health Care K42
ert F, Devriese S,alence survey for ospital infection. 2
nce van MRSA in ester 2010. 2010.rsa/download_fr.arsa/download_nl.a
KCE Report
of Assessment from:
10 osed framework. d Development; 20deler E, Mores B, 008-2010. Brusse, Kankercentrum;
Molenberghs, G.nitifs et de la aire différences es Pays-Bas. Leu
n J, Gailly J. ans. Brussels: Be. KCE Reports 12ge du cancer du sCare Knowledge
ment. Feedback ealth, Food Chain
de S, Vrijens F, la chirurgie électi
Knowledge Centre
Van de Sande Shospital-acquired2010;75(3):163-7de Belgische acuAvailable from:
asp and asp
t 196
012.
el:
., Van
uven:
lgian 29 sein
n
ive e
. The d . te

KCE Report 196
54. OECD Co-opefrom: http://w39_1_1
55. AHRQ.Healthcfrom: http://w
56. FPS HePatient HôpitauEnviron
57. GoreckDealey patients83.
58. McInneSupporDataba
59. Reddy system
60. Project Belgischttp://w
61. Hermanmental Paris: O
62. OECD.mental Co-ope
63. van Eijkof highlrandomBMJ. 2
6
HCQI Patient Saferation and Develo
www.oecd.org/doc1_1_1,00.html Patient Safety In
care Research an
www.qualityindicatealth Food Chain Safety Indicators
ux Belges.. FPS Hnment, ; 2011 Aprki C, Brown JM, N
C, et al. Impact os: a systematic re
es E, Jammali-Blart surfaces for prease Syst Rev. 201M, Gill SS, Rochoatic review. JAMAPUMap. Studie v
che ziekenhuizen www.decubitus.be/nn RC, Mattke S. health care at the
OECD; 2004. OEC Health Care Quahealth subgroup
eration and Develok ME, Avorn J, Poly anticholinergic a
mised trial of group001;322(7287):65
fety Indicators [Oropment;2009 [cite
ument/34/0,3343,
dicators Resourcnd Quality; 2011. 2
tors.ahrq.gov/ModSafety and Enviro
s: la Sécurité des Health Food Chainril 2011. elson EA, Briggs
of pressure ulcerseview. J Am Geria
asi A, Bell-Syer SEssure ulcer preve1(4):CD001735.
on PA. PreventingA. 2006;296(8):97van de decubitusp2008. 2008. Avail/downloads/PUMASelecting indicato
e health systems lCD Health Techniality Indicators: bameeting. Paris: Oopment; 2011. orsius AJ, de Boeantidepressants fop versus individua54-7.
Belgian
rganisation of Ecoed 21 Feb]. Availa
,en_2649_33929_
es. Agency for 2012, 21 Feb Ava
dules/psi_resourceonment. FeedbacPatients dans les n Safety and
M, Schoonhoven on quality of life itr Soc. 2009;57(7
E, Dumville JC, Cuention. Cochrane
g pressure ulcers:74-84. prevalentie in de lable from: AP_NL.pdf ors for the quality level in OECD coucal Papers 17 (17
ackground paper tOrganisation for Ec
r A. Reducing preor elderly people:
al academic detail
n Health System
onomic able
_370905
ilable
es.aspx ck des
L, in older
7):1175-
ullum N.
a
of untries. 7) to the conomic
escribing ing.
6
6
6
6
6
6
7
7
7
7
Performance
64. Mintzer J, people. J
65. van Eijk Met al. Use related preanticholine
66. Vander StSoenen Khomes in Centre (KC
67. Berendsenvan der Veexperiencecare: ConsCouns. 20
68. Haggerty JMcKendry2003;327(
69. Reid R, HaConcepts Final repo2002.
70. Salisbury continuity Pract. 200
71. van Serveand qualityconditions
72. van Walrabetween creview. J E
73. CommissiDignity. Secare homeLocal Gov
Burns A. AntichoR Soc Med. 2000
ME, Bahri P, Dekkeof prevalence andescribing of antideergic effects. J Clitichele RH, Van de
K, Smet M, et al. MBelgium. BrusselsCE); 2006. KCE Rn AJ, Groenier KHeen WJ, Dekker Jes across the intesumer Quality Ind
009;77(1):123-7. JL, Reid RJ, Free
y R. Continuity of c(7425):1219-21. aggerty J, McKenand measures of
ort. Canadian Hea
C, Sampson F, Rof care in primary
09;59(561):e134-4ellen G, Fongwa My care outcomes f
s: A literature revieaven C, Oake N, Jcontinuity of care aEval Clin Pract. 20on on Dignity in Cecuring dignity in es. A report for covernment, Associa
olinergic side-effec0;93(9):457-62. er G, Herings RMd incidence measepressants with ain Epidemiol. 200e Voorde C, Elsev
Medication use in rs: Belgian Health Reports 47C H, de Jong GM, MJ, et al. Assessmeerface between prdex Continuum of
eman GK, Starfieldcare: a multidiscip
ndry R. Defusing tcontinuity of heallth Services Rese
Ridd M, Montgomey health care be a41. M, Mockus D'Erricfor people experieew. Nurs Health SJennings A, Forsteand outcomes: a s010;16(5):947-56
Care for Older Peocare for older peo
onsultation. NHS Cation and Age UK;
cts of drugs in eld
M, Porsius A, Avorsures to describe and without 0;53(6):645-51. viers M, Verrue Crest and nursing Care Knowledge
Meyboom-de Jongent of patient's rimary and secondcare. Patient Edu
d BH, Adair CE, plinary review. BM
he confusion: lthcare. March 20
earch Foundation.
ery AA. How shouassessed? Br J Ge
o E. Continuity of encing chronic Sci. 2006;8(3):185er AJ. The associasystematic and cr. ople. Delivering ople in hospitals aConfederation, the; 2012.
153
erly
n J, age-
C,
B,
dary uc
MJ.
02. .
ld en
f care
5-95. ation ritical
and e

154
74. Cabanaoutcom
75. Patkar Cancerthe rolejournal
76. AbarshMeeusspractitioJourna
77. Davis Ssub-acu504.
78. Redmacare. R
79. Aiken LMcKee care: crcountrie
80. GomesDavesoadvancGermaOncolo
81. Houttekfuture tdata: a 2011;1
82. OECD.countrieDevelo
83. Nutbeaand sol
a MD, Jee SH. Domes? Journal of Fa
V, Acosta D, Davr multidisciplinary e of clinical decisioof breast cancer.i E, Echteld MA, Vsen K, et al. Use ooner visits at the el of pain and symp
S, Byers S, Walshute health care se
an RW, Lynn MR. Res Theory Nurs PLH, Sermeus W, V M, et al. Patient sross sectional sures in Europe and
s B, Higginson IJ, on BA, et al. Prefeces cancer: a popuny, Italy, the Neth
ogy. 2012. kier D, Cohen J, Srends in place of shift from hospita1:228-38. Health Data 2010es. In: Organisatiopment; 2010.
am D. Evaluating Hlutions. Health Pro
oes continuity of camily Practice. 20vidson T, Jones A,team meetings: eon support techno 2011;2011:83160Van den Block L, of palliative care send-of-life in the Nptom managemen
h F. Measuring peetting. Aust Health
Assessment of paPract. 2005;19(3):Van den Heede Ksafety, satisfactiorveys of nurses anthe United StatesCalanzani N, Coh
erences for place ulation survey in E
herlands, Portugal
Surkyn J, Deliens death in Belgium
als to care homes
0. Statistics and inon for Economic C
Health Promotion omotion Internatio
Belgian
care improve patie04;53(12):974-80, Fox J, Keshtgar
evidence, challengology. Internationa05. Donker G, Bossuservices and geneNetherlands and Bnt. 2011;41(2):436rson-centred care
h Rev. 2008;32(3)
atient expectation275-85. , Sloane DM, Busn, and quality of hnd patients in 12 s. BMJ. 2012;344:hen J, Deliens L, of death if faced wEngland, Flanders and Spain. Anna
L. Study of recenusing death certif. BMC Public Hea
ndicators for OECCo-operation and
- progress, probleonal. 1998;13(1):2
n Health System
ent 0.
M. ges, and al
uyt N, eral Belgium. 6-48. e in a ):496-
ns for
sse R, hospital
:e1717.
with s, als of
nt and ficate alth.
CD
ems 27-44.
8
8
8
8
8
8
9
9
9
9
Performance
84. Cellule Intsystème ddentaire dfrom: http://www
85. VanobbergBelgian ch
86. Sasse A, Vet de l'infeBrussels:
87. Ewing JA.1984;252(
88. VIGEZ DeGezondhehttp://vig.koryGUID=
89. WHO. WHRecommeHealth Org
90. Ministère ffédérées bPlan natio
91. Pate RR, et al. Physthe CenteCollege of
92. Bouchard Exercise, Knowledg
93. Buytaert BVerslag va(tabak, vogemeenteZiekteprev
teruniversitaire d'Ed'enregistrement ee la population be
w.inami.fgov.be/infgen J, Martens L,hildren: a review. Verbrugge R, Van
ection à VIH en BeIPH, surveillance Detecting alcoho(14):1905-7. e actieve voedingseidspromotie;2012kanker.be/content=025d941e-6a63-4HO Global Strategendations for Physganization; 2004.fédéral de la Santbelges ayant la Sa
onal nutrition santéPratt M, Blair SN,sical activity and prs for Disease Cof Sports MedicineC, Shephard R, SFitness, and Heae. In: IL C, editor.
B, Moens O, Tamban de indicatorenmeding, beweging)
en. Vlaams Instituuventie; 2010. Avai
Epidémiologie. Raet de surveillance elge 2008- 2010 »
formation/fr/studie Declerk D. CarieInt J Paediatr Denn Beekchoven D. elgique; situation aof communicale d
olism. The CAGE
sdriehoek [Vlaams2. Available from: t/category/categor4540-a522-b3c20gy on Diet, Physicasical Activity for H té Publique et Minanté publique dané pour la Belgique Haskell WL, Mac
public health. A reontrol and Prevent. JAMA. 1995;273Stephens T, Suttolth. A Consensus Human Kinetics buyzer J, Woutersmeting 2009 van h in Vlaamse bedriut voor Gezondheilable from:
KCE Report
apport final du prode la santé bucco
». 2012. Available
es/study53/index.es prevalence in nt. 2001;11(3):164Epidémiologie duau 31 décembre 2diseases; 2011. questionnaire. JA
s Instituut voor
rycontent.aspx?C08832529 al Activity and He
Health. Geneva: W
nistères des entiténs leurs attributione, 2005 -2010. 200cera CA, Boucharecommendation frtion and the Amer3(5):402-7. on J, McPherson B
of Current Books; 1990. p. 3s E, Vauhauwaerthet gezondheidsbijven, scholen en
eidspromotie en
t 196
ojet « o-
htm
4-70. u Sida 2010.
AMA.
ateg
ealth. World
és ns. 04. rd C, om rican
B.
3-28. t E. beleid

KCE Report 196
http://w49de67
94. Godin ICommu
95. Nutbea1986;1
96. Nutbea2008;67
97. Consor98. Joosse
BrusseAvailabhttp://wL.pdf
99. Bravemepidem
100. BravemConcepNutritio
101. Black Dworking
102. Feinstehealth:1993;v7
103. WHO Cgap in adeterm
104. EU ExeProgramEurope
105. Sondik healthyHealth.
6
www.vigez.be/uplo7cf9835b9a1.pdf I, Piette D. Etude unauté française dam D. Health prom(1):113-27.
am D. The evolvin7(12):2072-8. rtium HLS-EU. Thens L, Raw M. Thels: Association of
ble from: www.ensp.org/sites
man P, Gruskin S. miology and commman PA. Monitorinptual Framework. on. 2003;31(3):181D. Inequalities in hg group- Departmein J. S. The relatiA review of the lit71:p. 279-94.
Commission on Soa generation: heainants of health G
ecutive Agency fomme of Commun
ean Commission; 2EJ, Huang DT, K
y people 2010 goa 2010;31:271-81
oads/documentenb
écoles liées aux ede Belgique, rapp
motion glossary. H
g concept of heal
e European Healte Tobacco Controthe European Ca
s/default/files/TCS
Defining equity inmunity health. 2003ng Equity in Health
Journal of Health1-92. health. London: Reent of Health andonship between sterature. The Milk
ocial Determinantalth equity throughGeneva: World Her Health and Consity Action in the F2007.
Klein RJ, Satcher Dals and objectives4 p folliwng 81.
Belgian
bank/f9c7c649098
enquêtes HBSC port à paraître. 20Health Promot.
th literacy. Soc Sc
th Literacy Surveyol Scale 2010 in Eancer Leagues; 20
S_2010_in_Europ
n health. Journal o3;57(4):254-8. h and Healthcare:h Population and
eport of a researc Social Security; 1socioeconomic stakbank Quarterly.
s on Health. Closh action on the socealth Organisationsumer. Second ield of Health 200
D. Progress towar. Annu Rev Public
n Health System
88b8b4
10.
ci Med.
y. urope. 010.
pe_FINA
of
A
ch 1980. atus and
ing the cial ; 2008.
08-2013.
rd the c
1
1
1
1
1
1
1
1
1
Performance
06. Mackenbaeconomic illustrated medicine.
07. Harper S, J. Implicit Inequalitie
08. CharafeddVan OyenAlternativecensus. Bsurveillanc
09. DeboosereExpectanccensus an
10. Van OyenDemarest trend in hePublic Hea
11. Van Oyenevolutie vaPress A, eGent: Fed
12. Debooseresociales eCharafediBelgique.
13. Van OyenDemarest santé. In: inégalités Press; 201
14. Haeltermaindicateurs
ach JP, Kunst AE.inequalities in hewith two example1997;44(6):757-7King NB, MeersmValue Judgments
es. Milbank 2010;8dine R, Gadeyne S H Social inequal
e methods of estimrussels: Directionce, Institut Scientie P GS, Van Oyecy by educational nd population regis H CR, DebooserS. Contribution o
ealth inequality at alth. 2011;21:781 H CR, Debooseran sociale ongelijkeditor. Sociale ongeraal Wetenschae P, Gadeyne S, V
en espérance de vnne R., editor. LeBrussels: Academ H, CharafeddineS. L'évolution deVan Oyen H. DP,sociales de santé10. an E, De Spiegelas de santé périna
. Measuring the malth: an overview
es from Europe. S71. man C, Reichman s in the Measurem88(4-29). S, Deboosere P, Bities in healthy lifemation in the abse Opérationnelle Sifique de Santé Pun H. The 1991-20level in Belgium bster data. Eur J Pre P, Cox B, Loranof mortality and dis
the turn of centur-7.
re P, Cox B, Lorankheid in gezonde gelijkheden in gezpsbeleid; 2011. pVan Oyen H. L'év
vie. In: Van Oyen s inégalités socia
mia Press; 2010. R, Deboosere P,s inégalités en es Lorant V., Chara
é en Belgique. Bru
aere M, Masuy-Strtale en Région de
magnitude of socioof available meas
Social science &
ME, Breen N, Lyment of Health
Berger N, Demaree expectancy. ence of the nation
Santé publique et ublique; 2011. 004 evolution in Libased on linked
Popul. 2009;25:175nt V, Nusselder Wsability to the secury in Belgium. Eur
nt V, Demarest S.levensverwachtin
zondheid in België. 27-43.
volution des inégaH. DP, Lorant V., les de santé en
Cox B, Lorant V,spérance de vie enafedinne R., editorussels: Academia
roobant E. Les e Bruxelles capita
155
o-sures
nch
est S,
nal
ife
5-96. W, ular r J
De ng. In: ë.
alités
, n r. Les
le

156
1998-2Bruxelle
115. Léonarparadigéconom
116. DworkiPhiloso
117. Dworki2002;1
118. DworkiAffairs.
119. RoemeEconom
120. Roeme(April/M
121. RoemeUnivers
122. van DomedicaAssocia
123. van DoSome i1992(1
124. van DoCitoni Gfinance1999;18
125. Wagstaon (andof FinaWashin
126. WagstaSome i1992;1
004. Brussels: Obes-Capitale; 2007rd C. La responsagme pour refondemique/Ethics and n R. What is Equa
ophy and Public An R. Sovereign Vi13(October):106-4n R. Equality, Luc2003;31(2):190-8
er J. Egalitarianismmics and Philosoper J. Equality and May)). er JE. Equality of Osity Press; 1998. oorslaer E, Masseal care by income ation Journal. 200
oorslaer E, Wagstanternational comp1):389-411.
oorslaer E, WagstaG, Di Biase R, et ae in twelve OECD 8(3):291-313. aff A. Measuring Ed Alternatives to) tncing Index. In: Pngton: World Bankaff A, Van Doorslanternational comp1(4):361-7.
bservatoire de la s7. bilisation capacitar l'Etat-providenceEconomics. 2012ality? Part 2: Equa
Affairs. 1981;10(4)irtue Revisited. Et43.
ck and Hierarchy. 8. m, responsibility, aphy. 1987;3:215-4responsibility. Bos
Opportunity. Cam
ria C, Koolman X.in developed cou
06;174(2):177-83.aff A. Equity in theparisons. Journal
aff A, van der Bural. The redistributcountries. Journa
Equity in Health Cthe World Health
Policy Research Wk; 2001. aer E. Equity in theparisons. Journal
Belgian
santé et du Socia
ante: un nouveau e? Éthique et ;9(2):45-65. ality of Resources:283-345. thics.
Philosophy and P
and information. 44. ston Review. 1995
bridge: Harvard
. Inequalities in acntries. Canadian
e delivery of healtof Health Econom
rg H, Christiansenive effect of health
al of Health Econo
Care Financing. refOrganization's Fa
Working Paper.
e finance of healtof Health Econom
n Health System
l de
s.
Public
5;XX(2
ccess to Medical
th care: mics.
T, h care omics.
flections airness
h care: mics.
1
1
1
1
1
1
1
1
1
1
Performance
27. Wagstaff ADelivery. IEconomic
28. Wagstaff AChristianssome furthEconomic
29. Daniels NCambridge
30. Jackson Téconomie
31. Van OyenGender galimitationsmacro-lev
32. WHO. Devmeeting oOrganizat
33. Plug I, HoEuropean health sysUnion, towSystems);
34. SchokkaeDe Graevehealth carBrussels: KCE repo
35. De GraeveVoorde C.of supplem(KCE); 20
36. Van de Voinsurance
A, Van Doorslaer n: Culyer AJ, News: North-Holland; A, van Doorslaer sen T, Citoni G, ether international cs. 1999;18(3):263. Just Health. Meee University Press
T. Prospérité sansdurable. Bruxelle H CB, Nusselderaps in life expectas at age 50 in the Eel structural factoveloping indicatorf the expert groupion; 2012. ffmann R, MackeUnion: Towards b
stems. In: AMIEHSwards better Indica 2011. rt E, Guillaume J,e D, et al. [Effectsre consumption anBelgian Health Carts 80 e D, Lecluyse A, S. [Personal contribments]. Brussels: 06. KCE reports 5oorde C, Kohn L, Vfor persons with a
E. Equity in Healtwhouse JP, editor2000. p. 1804-62E, van der Burg Ht al. Equity in the fcomparisons. Jour3-90. eting Health Needs; 2008.
s croissance. La tres; 2010. r W, Jagger C, Caancy and expectedEuropean Union: rs. Eur J Ageing. rs for the health 20p (18-19 June). Ut
nbach J. Avoidabbetter indicators foS (Amenable Mortators for the Effec
Lecluyse A, Avals of the Maximum nd financial accesare Knowledge C
Schokkaert E, Vabution for health cBelgian Health Ca50 Vinck I. [Entitlemea chronic illness o
KCE Report
th Care Finance ars. Handbook of h2. H, Calonge S, finance of health crnal of Health
ds Fairly. Cambrid
ransition vers une
ambois E, Robine d years with activiAssociations with2010;7:229-39. 020 targets. First trecht: World Hea
le mortality in the for the effectivenetality in the Europctiveness of Healt
losse H, Cornelis Billing system on
ss to health care]. entre (KCE); 2008
n Ourti T, Van de care in Belgium. Imare Knowledge C
ent to a hospital or handicap]. Brus
t 196
and ealth
care:
dge:
JM. ity
h
lth
ss of pean h
K, n
8.
mpact entre
ssels:

KCE Report 196
Belgian166
137. SimoenOECD
138. Van deLesaffrehospita
139. WHO. Pthe cha
140. Eyssenvan geeen perswetensKnowle
141. Garcia-measurOECD Papers
142. NIHDI. et d'évaand Dis
143. Schoenconditioin eight
144. Mead Nand rev2000;5
145. Davies Sakowsto suppquality 76.
146. Europescientif2008.
6
n Health Care Kno
ns S, Villeneuve, MCountries Paris: O
en Heede K, Florqe E, et al. Effectiv
als: A mixed methoPolicies and practallenges. Copenhan M, Leys M, Desoestelijke gezondhsisterende mentalschappelijke basisedge Centre (KCE-Armesto S, Medering and comparincountries. Paris: O
s Evaluer les trajet
aluer les donnéessability Insurance;n C, Osborn R, Hoon: experiences ot countries, 2008. N, Bower P. Patieview of the empiric1(7):1087-110. E, Shaller D, Edg
ski J, et al. Evaluaport improvementsimprovement coll
ean Practice Assefically developed q
owledge Centre (K
M., Hurst, J. TackOECD; 2005. uin M, Bruyneel L
ve strategies for nod study. Int J Nutices for mental heagen: World Healtomer A, Arnaud Seidszorg voor mee aandoening. W
s? Brussel: BelgiaE); 2010. KCE Repeiros H, Wei L. Infng quality of mentOECD; 2008. OE
ts de soins: accords. Bruxelles: Natio; 2012. Communiqow SK, Doty MM, of patients with com
Health Aff (Millwont-centredness: acal literature. Soc
gman-Levitan S, Sating the use of a s in patient-centreaborative. Health
ssment - EPA. Eaquality manageme
Belgian
KCE); 2011. KCE
kling Nurse Shorta
L, Aiken L, Diya L,urse retention in ars Stud. 2011. ealth in Europe: mth Organization; 2
S, Léonard C. Orgaensen met een ernat is de n Health Care ports 144 formation Availibiltal health care acrCD Health Techn
d sur la façon de nal Institute for Hqué de presse Peugh J. In chronmplex health careood). 2009;28(1):wa conceptual frame Sci Med.
Safran DG, Oftedamodified CAHPS
ed care: lessons frExpect. 2008;11(
asy to use and ent for general pra
n Health System
reports
ages in
, acute
meeting 2008. anisatie nstige
ity for ross ical
récolter ealth
nic e needs, w1-16. ework
ahl G, survey rom a (2):160-
actice.
1
1
1
1
1
1
1
1
1
1
Performance
47. The RoyaPractices,from: http://wwwStandards
48. The Royafor ExcellePractice 2http://www
49. Merrick ELChanging indicators.
50. Owens PLAbuse-ReAHRQ, HE2010. Stat
51. Larkin G, departmenPsychiatric
52. McEwan KIndicators Health Ca
53. Morris J, BGebruikshWashingto
54. Morris J, Fal. GebruiWashingto
55. WHO Nutr[cited 30th
56. Mohler R, preventinggeriatric ca2011(2):C
l Australian Colleg 4th Edition - 2010
w.racgp.org.au/CosforGeneralPracticl New Zealand Coence – RNZCGP S2011-2014 [2011 [w.rnzcgp.org.nz/quL, Hodgkin D, Hormental health gat
. J Behav Health SL, Mutter R, Stockelated Emergency EALTHCARE COStistical Briefs Claassen C, Emont visits for mentac Services. 2005;KL, Goldner E. Acfor Mental Health
anada; 2001. Berg K, Fries B, Hhandboek voor deon, D.C.: InterRAIFries B, Bernabei kshandboek voor on, D.C.: InterRAIrition for older perh of Mai]. Richter T, Kopke
g and reducing theare. Cochrane Da
CD007546.
ge of GPs Standa0, [2011 [cited No
ontent/NavigationMces/Standards4thollege of General Standard for New[cited November]. uality-standards rgan CM, Garnicktekeeping: effectsServ Res. 2007;3
ks C. Mental HealtDepartment Visit
ST AND UTILIZA
ond J, al. e. Trendal health conditions56(6):671-7.
ccountability and Ph Services and Su
Hawes C, Phillips C InterRAI-LTCF (B; 2006. R, Steel K, Ikegade interRAI-HC (; 2006.
rsons [World Heal
e S, Meyer G. Intee use of physical atabase of System
ards for General ovember]. Availab
Menu/PracticeSupEdition.pdf Practitioners Aim
w Zealand GeneraAvailable from:
k DW, McLaughlins on performance 5(1):3-19. th and Substancets among Adults.
ATION PROJECT;
s in US emergencs, 1992 to 2001.
Performance upports. Ottawa (O
CM, Mor V, et al. BelRAI-LTCF).
mi N, Carpenter IBelRAI-HC).
lth Organization;2
rventions for restraints in long-
matic Reviews.
157
le
pport/
ing l
n TJ.
cy
ON):
, et
2012
-term

158
157. Van deTafforeDirectioBruxelle
er Heyden J, Gisleeau J. Enquête deon Opérationnellees, Institut Scient
e L, Demarest S, D santé, 2008. Rap Santé publique eifique de Santé P
Belgian
Drieskens S, Hesspport I - Etat de saet surveillance, 20ublique; 2010.
n Health System
se E, anté.
010;
Performance KCE Reportt 196