Neue Erkenntnisse zur Wechselwirkung · Ultrasound of one shoulder per patient was performed by a...
64
Neue Erkenntnisse zur Wechselwirkung von Schmerz und Physiotherapie Prof. Dr. PD Hannu Luomajoki, PT OMT Leiter Masterausbildung msk Physiotherapie Zürcher Hochschule für Angewandte Wissenschaften H. Luomajoki PhysioAustria 2018
Transcript of Neue Erkenntnisse zur Wechselwirkung · Ultrasound of one shoulder per patient was performed by a...
Neue Erkenntnisse zur Wechselwirkung von Schmerz und Physiotherapie
Prof. Dr. PD Hannu Luomajoki, PT OMT
Leiter Masterausbildung msk Physiotherapie
Zürcher Hochschule für Angewandte WissenschaftenH. Luomajoki PhysioAustria 2018

Programm
1. Alte Theorien sind alt – Neues ist neu:
Die unglaublich gute Evidenz der Physiotherapie
2. Schmerzen: Mechanismen, wie klassifizieren, … und wie messen:
was ist wichtig?
3. Beispiele Physioforschung & eigene Studien… Rückenschmerzen,
Bewegung, Kontrolle
H. Luomajoki PhysioAustria 2018

Was ist Theorie (heute)?
Was ist Praxis (was soll sie sein)?
Was kann Praxis von Theorie lernen?
Was kann Theorie von Praxis lernen?
H. Luomajoki PhysioAustria 2018
Theorie…
• Früher…
H. Luomajoki PhysioAustria 2018
Dann…

Theorie heute.... Evidenzbasiert
• Evidenzbasierte (nach Studien belegte) Methoden (Untersuchungen und Behandlungen) und Vorgehensweisen bevorzugen und einsetzen in der Behandlung von individuelle Patienten
H. Luomajoki PhysioAustria 2018

René was wrong! Anatomie erklärt nicht Symptome...
Copyright 2014 by American Society of Neuroradiology.H. Luomajoki PhysioAustria 2018

RESULTS: Across all 10 study examinations, there were 49 distinct findings reported related to
the presence of a distinct pathology at a specific motion segment. Zero interpretive findings
were reported in all 10 study examinations and only one finding was reported in nine out of 10
study examinations. Of the interpretive findings, 32.7% appeared only once across all 10 of the
study examinations’ reports. A global Fleiss kappa statistic, computed across all reported
findings, was 0.20±0.06, indicating poor overall agreement on interpretive findings. The
average interpretive error count in the study examinations was 12.5±3.2 (both false-positives
and false-negatives). The average false-negative count per examination was 10.9±2.9 out of 25
and the average false-positive count was 1.6±0.9, which correspond to an average true-positive
rate (sensitivity) of 56.4%±11.7 and miss rate of 43.6%±11.7.
H. Luomajoki PhysioAustria 2018

AJR:197, October 2011
© American Roentgen Ray Society
MATERIALS AND METHODS. The study sample comprised 51 consecutively enrolled
subjects who had no symptoms in either shoulder. Ultrasound of one shoulder per
patient was performed by a musculoskeletal sonographer according to a defined protocol that
included imaging of the rotator cuff, tendon of the long head of the biceps brachii muscle,
subacromial-subdeltoid bursa, acromioclavicular joint, and posterior labrum. The shoulder
imaged was determined at random. The 51 scans were retrospectively analyzed by three
fellowship-trained musculoskeletal radiologists in consensus, and pathologic findings were
recorded. Subtle or questionable findings of mild tendinosis, bursal prominence, and mild
osteoarthritis were not recorded.
RESULTS. Twenty-five right and 26 left shoulders were imaged. The subject age range was
40–70 years. Ultrasound showed subacromial-subdeltoid bursal thickening in 78% (40/51) of
the subjects, acromioclavicular joint osteoarthritis in 65% (33/51), supraspinatus
tendinosis in 39% (20/51), subscapularis tendinosis in 25% (13/51), partial-thickness tear of
the bursal side of the supraspinatus tendon in 22% (11/51), and posterior glenoid labral
abnormality in 14% (7/51). All other findings had a prevalence of 10% or less.
CONCLUSION. Asymptomatic shoulder abnormalities were found in 96% of the subjects.
Ultrasound of the Shoulder:
Asymptomatic Findings in Men
Gandikota Girish, Lucas G. Lobo, Jon A. Jacobson, Yoav Morag,Bruce Miller, David A. Jamadar
H. Luomajoki PhysioAustria 2018

N=121
Biomechanik...?
H. Luomajoki PhysioAustria 2018
Das ist ja gut für die Physiotherapie, dass die alten Theorien nicht stimmen!

Grössere Kosten, Effekte gleich…
H. Luomajoki PhysioAustria 2018
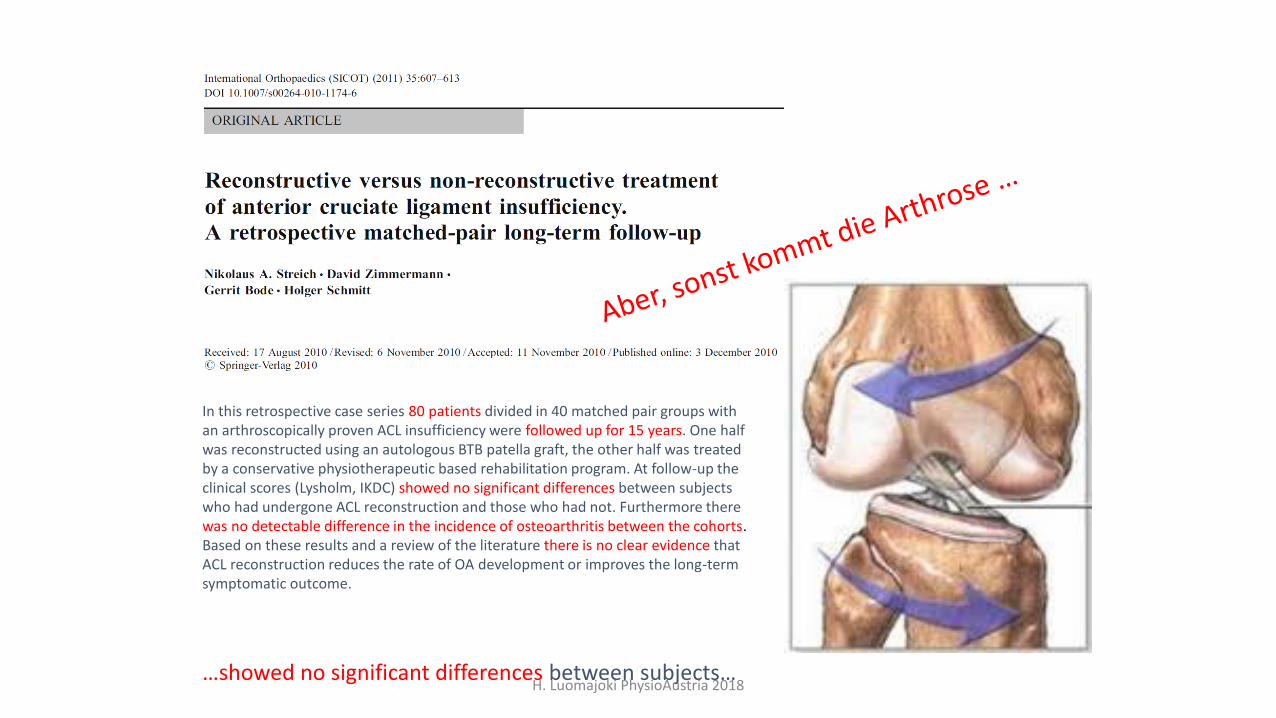
In this retrospective case series 80 patients divided in 40 matched pair groups with an arthroscopically proven ACL insufficiency were followed up for 15 years. One half was reconstructed using an autologous BTB patella graft, the other half was treated by a conservative physiotherapeutic based rehabilitation program. At follow-up the clinical scores (Lysholm, IKDC) showed no significant differences between subjects who had undergone ACL reconstruction and those who had not. Furthermore therewas no detectable difference in the incidence of osteoarthritis between the cohorts. Based on these results and a review of the literature there is no clear evidence that ACL reconstruction reduces the rate of OA development or improves the long-term symptomatic outcome.
…showed no significant differences between subjects… H. Luomajoki PhysioAustria 2018

Beispiel Effektivität: Arthroskopie Knie
the bmj | BMJ 2015;350:h2747
• CH: ca. 20’000 Arthroskopien / Jahr • Effektgrösse (Effect size) in diesem Review
• 0.14 bei der Arthroskopie (Kosten zwischen CHF 3’000 – 5’000.-)• 0.5 - 0.64 bei Training und Übungen (Kosten ca. CHF 700.-)
H. Luomajoki PhysioAustria 2018

H. Luomajoki PhysioAustria 2018
Impact Factor 55,8:
300-400 000 readers weekly….
Also...die Evidenz sagt... Weiss das jemand...?
H. Luomajoki PhysioAustria 2018

Konservatives Management wird empfohlen als primäres Management bei Impingement und Rotator Cuff
Problemen
RCT’s: kein Unterschied zwischen OP ODER PhysiomanagementBrox et al 1993; BMJ; Haar et al .2005; Ann Rheum Dis ; Ketola et al 2008; J Bone Joint Surg Br
Systematisches Review über Impingement Management OP vs konservativ: keineUnterschiede in den Outcomes (Funktion, Behinderung, Schmerz)
Dorrestijn et al 2009 shoulder and elbow surgery
Rotator cuff Rupturen: Ein Syst. Review / Meta-analyse : ein sign. Unterschiedzugunsten der OP, Aber der Unterschied war nicht klinisch relevant.
Ryösa et al 2016 Disabil Rehabil
In der Schweiz werden jährlich 10 000 Operationen an der RotatorenManschette / Impingement durchgeführt!
15

Prädiktoren
H. Luomajoki PhysioAustria 2018
• Prospektive Kohortenstudie; n=1030; Follow-up nach 12 Monaten, Outcomes: SPADI und DASH
• Fünf psychologische Faktoren waren prädiktiv: niedriger Behinderungsgrad; pos. Erwartungshaltung; gute Selbstwirksamkeit; niedriger Ruheschmerz; Arbeitsfähigkeit
• Drei physische Faktoren: Gute Abduktionsbeweglichkeit; kleiner Unterschied zw. akt und pass. Bewegung, Verbesserung der Symptome durch Assistieren der Scapulabewegung

Spinalkanalstenose….
H. Luomajoki PhysioAustria 2018

What else?www.thelancet.com July, 2014
Efficacy of paracetamol for acute low-back pain: a double-blind, randomisedcontrolled trialChristopher M Williams, Christopher G Maher, Jane Latimer, Andrew J McLachlan, Mark J Hancock, Richard O Day, Chung-Wei Christine Lin
• n= ca. 1500 Patients
• Three groups: Paracetamol 4 g / day; like needed up tp 4 g / d, Placebo
• In all groups, after 17 days approximately, pain was gone
• No differences between groups….
H. Luomajoki PhysioAustria 2018

H. Luomajoki PhysioAustria 2018
ernüchternd

Ann Intern Med. doi:10.7326/M16-2367 Annals.org
This article was published at Annals.org on 14 February 2017.
Recommendation 1: …most patients with acute or subacute low back pain improve over time regardless of treatment, clinicians and patients shouldselect nonpharmacologic treatment ….with superficial heat (moderate-quality evidence), massage, acupuncture, or spinal manipulation (low-quality evidence).
Recommendation 2: …..chronic low back pain, clinicians and patients should initially select nonpharmacologictreatment with exercise, multidisciplinary rehabilitation, acupuncture, mindfulness-based stress reduction (moderate-quality evidence), tai chi, yoga, motor control exercise, progressive relaxation, electromyography biofeedback, low-level lasertherapy, operant therapy, cognitive behavioral therapy, or spinal manipulation (low-quality evidence). (Grade: strongrecommendation)
Recommendation 3: In patients with chronic low back pain who have had an inadequate response to nonpharmacologic therapy, clinicians and patients should consider pharmacologic treatment with nonsteroidal anti-inflammatory drugs as first-line therapy, or tramadol or duloxetine as second-line therapy. Clinicians should only consider opioids as an option in patients who have failed the aforementioned treatments and only if the potential benefits outweigh known risks and realistic benefits with patients. (Grade: weak recommendation, moderate-quality evidence)
…… Low cost treatments should be preferred…..!
Feb 2017
H. Luomajoki PhysioAustria 2018

747 patients Entry setting was primary care, chiropractic, physiatry, and physical therapy. Relative to primary care, entry in physiatry increased risk for radiographs (OR = 3.46, P = 0.001), advanced imaging (OR = 3.38, P < 0.001), injections (OR = 4.91, P < 0.001), surgery (OR = 4.76, P = 0.012) and LBP-related costs (standardized Β = 0.67, P < 0.001). Entry in chiropractic was associated with decreased risk for advanced imaging (OR = 0.21, P = 0.001) or a surgeon visit (OR = 0.13, P = 0.005) and increased episode of care duration (standardized Β = 0.51, P < 0.001). Entry in physical therapy decreased risk of radiographs (OR = 0.39, P = 0.017) and no patient entering in physical therapy had surgery.
Conclusions Entry setting for LBP was associated with future health care utilization and costs. Consideration of where patients chose to enter care may be a strategy to improve outcomes and reduce costs.
Fazit für die Physiotherapie• Geringste Kosten• Bis 10 x weniger Injektionen und MRI• Niemand wurde innerhalb eines Jahres am Rücken operiert
Oct. 2015
H. Luomajoki PhysioAustria 2018
2. Wie sollten wir Schmerzpatienten klassifizieren / subgruppieren?
• Nach Schmerzmechanismus?
• Nach psychologische Status?
• Nach Generation?
• Nach Behinderungsgrad ? !
H. Luomajoki PhysioAustria 2018

Klassifizieren – nach Schmerzmechanismus!
• Periphere Probleme (klares Verhalten, klare Anamnese, on off…etc.)
• Zentrale Sensitivierung (unklares Verhalten, lange Anamnese, beliefs, Mystifikation, Ängste, Hoffnungslosigkeit…)
• Neurogen (hohes Leiden, klare Befunde, bracuhen häug^fig harte Drogen… )
H. Luomajoki PhysioAustria 2018

Quick repetition: Painmechanismen
3. Order Neuron
2. Order Neuron (WDR)
1. Order Neuron
Neuropathy
?
Primary Hyperalgesia
Secondary Hyperalgesia / Allodynia
Prognose
????
Lang
GutH. Luomajoki PhysioAustria 2018
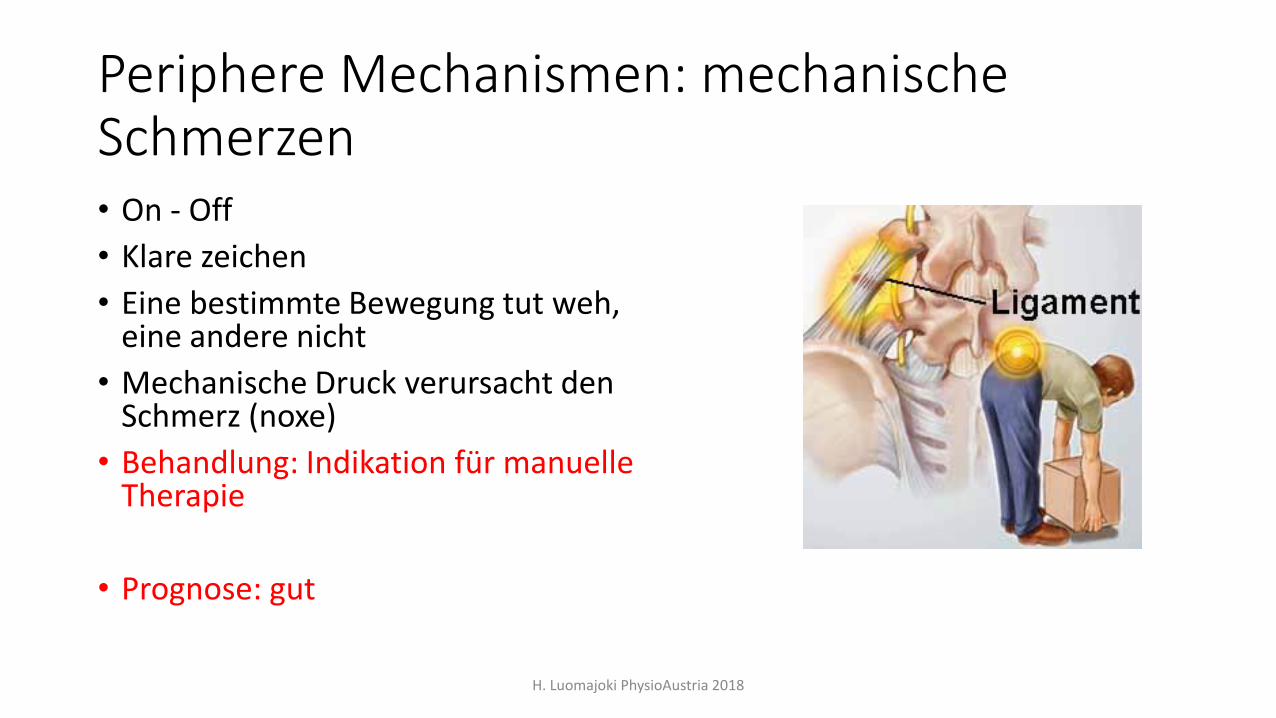
Periphere Mechanismen: mechanische Schmerzen• On - Off
• Klare zeichen
• Eine bestimmte Bewegung tut weh, eine andere nicht
• Mechanische Druck verursacht den Schmerz (noxe)
• Behandlung: Indikation für manuelle Therapie
• Prognose: gut
H. Luomajoki PhysioAustria 2018

Entzündliche Schmerzen: klinische Muster
• Steifigkeit, abhängig 24h
• Rötung, Schwellung, Druckgefühl, Wärme
• Ständige Schmerz (background ache)
• Reaktion auf NSAID:s klar
• Zeitfaktor
• Prognose: gut
H. Luomajoki PhysioAustria 2018
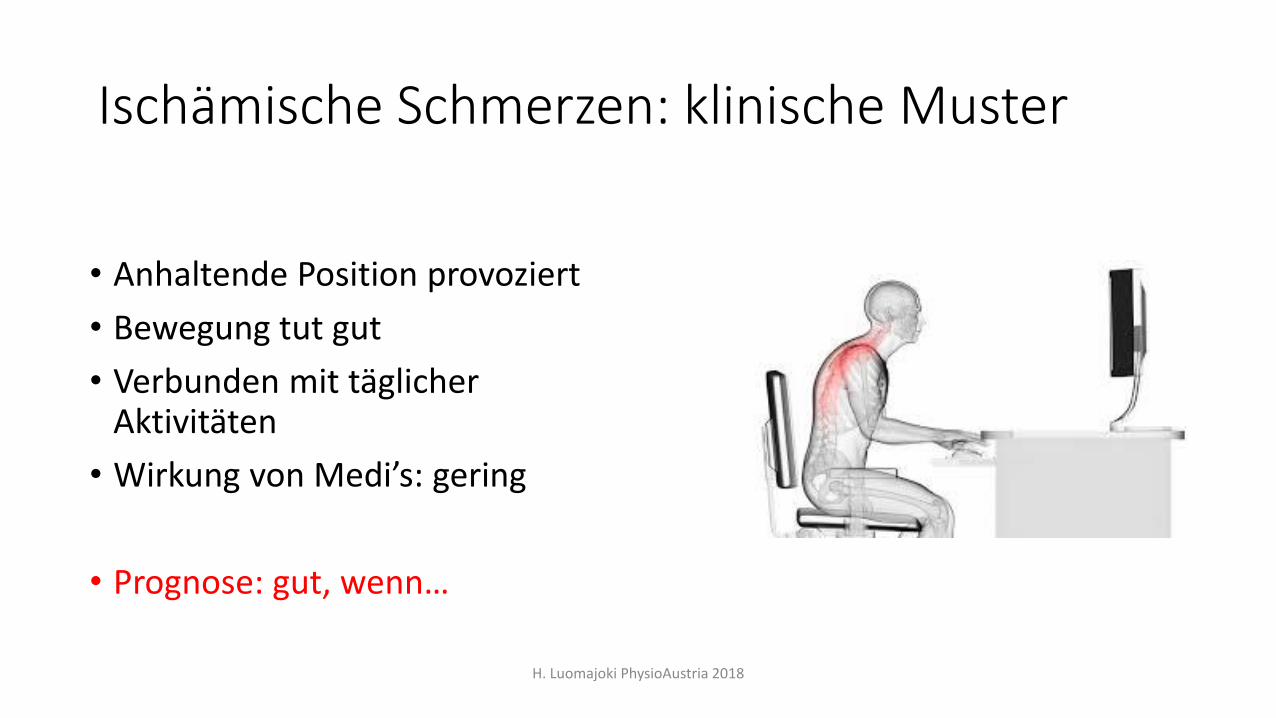
Ischämische Schmerzen: klinische Muster
• Anhaltende Position provoziert
• Bewegung tut gut
• Verbunden mit täglicher Aktivitäten
• Wirkung von Medi’s: gering
• Prognose: gut, wenn…
H. Luomajoki PhysioAustria 2018

Periphere neurogene Schmerzen
Symptomgebiet
• Innervatiosnfeld eines Nervs oder Segment
• In einem bestimmten Nerv
Qualität
• Brennen, bohren, beängstigend, wie Zahnschmerzen…
• Kribbeln, Parästesien
• Prognose: OK…kann aber lange dauern …
H. Luomajoki PhysioAustria 2018

Zentrale Sensitisation
• Andauernde Symptome
• Summation & Latenz
• Unberechnebar
• „ Alles tut Weh “
• Ausdehnende Schmerzen
• Plötzliche Schmerzen
• „ Die Schmerzen machen was die wollen “
• „ Wunderheilungen?“
• Plazebo?
• Kognitive & Affektive Komponente
• etc...
H. Luomajoki PhysioAustria 2018
Prognose: … Hmm….. Kann auch gut sein… aber, sehr unterschiedlich… die Dauerder Anamnese erzhlt auch die Prognose
Subklassifizieren nach… Generation?
• Traditionalisten - bis ende 50 - Jahre
• Baby boomers 1960-1972
• Generation X 1970 – 1980
• Generation Y 1990
• Millenium babies ab 2000 …
H. Luomajoki PhysioAustria 2018

Nach psychologischen Status
• Adaptive copers
• Passive copers; dysfunctional
• Interpersonally distressed Verra et al 2006; the journal of pain; May 2006 Volume 7, Issue 5, Pages 327–336
• Negative mood
• Avoiders (fear)
• Provocators (endurers)
• Believers
• Etc….
H. Luomajoki PhysioAustria 2018

Nach selbst-empfundene Behinderungsgrad!
• Wie hoch ist die Behinderungsgrad?
• Fragebogen
• Roland Morris, Oswestry; Neck Disability Index; DASH; womacetc.
• Je höhere Punkte … um so schlechtere Prognose
• Je tiefere Punkte … um so bessere Prognose
• Muss gemessen werden… da sie schlecht mit phys. Befunde korreliert!
H. Luomajoki PhysioAustria 2018

H. Luomajoki PhysioAustria 2018
Minimale Behinderung
Geringe Behinderung (< 30%)
Mittlere Behinderung (30-50%)
Hohe Behinderung(> 50%)
Aktivitätslevel /Behinderungsgrad
Spitzensportler
Sportlich
Fitte Gesunde
Performance
Fitness
Zufriedenheit
Was wird gemessen?
Physische Befunde
Physische Befunde / Screening psych.soz.
Psych. soz. Items , Aktivität / Behinderungsgrad; Arbeitsfähigkeit
Behinderungsgrad,Arbeitsfähigkeit, Partizipation
Trainieren
Trainieren
Pass. / akt. Behandlung
Was für management?
Pass. Beh. + Indiv. Übungen
Aktive Übungen & Pat. Edukation
Pat. Edukation & generalle Aktivität
Interdisziplinär
Normale Gesundheit

Gute, auf Deutsch validierte Fragebogen… Beispiele• Rückenschmerzen (LBP): Roland Morris Disability Questionnaire
(RMQ), Oswestry, Patient Specific Functional Scale (PSFS), Keele Start Back Tool (Start)
• Nacken: Neck Disability Index (NDI)
• Schulter (SPADI)
• Obere Extremität: DASH
• Untere Extremität: WOMAC, KOOS
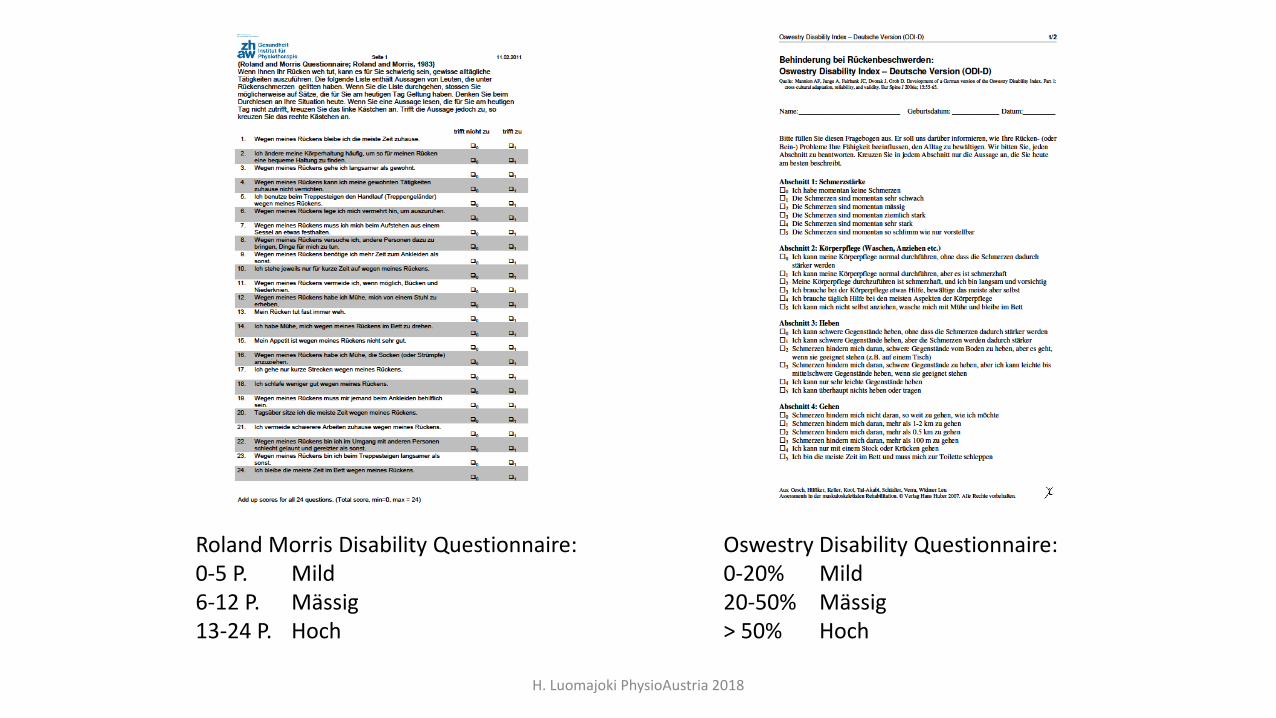
Roland Morris Disability Questionnaire:0-5 P. Mild6-12 P. Mässig13-24 P. Hoch
Oswestry Disability Questionnaire:0-20% Mild20-50% Mässig> 50% Hoch
H. Luomajoki PhysioAustria 2018

Prognostische Fragebogen
• TSK (Tampa Scale of Kinesiofobia)
• FABQ (Fear Avoidance Beliefs Questionnaire)
• DEPS (Depression Scale)
• PCS (Pain Catastrophizing Score)
• CPAQ (Chronic Pain AcceptanceQuestionnaire)
• ….
H. Luomajoki PhysioAustria 2018

Forschung aus Praxis aus…
• Beispiele eigener Forschung …
• Rückenschmerzen und Bewegungskontrolldysfunktion
H. Luomajoki PhysioAustria 2018

Klassifikation derRückenschmerzen (O‘Sullivan 2005)
spezifische
Rückenschmerzen
(10%)
unspezifische
Rückenschmerzen
(90%)
nicht mechanisch
(30%)
mechanisch
(70%)
„Zentraler maladaptiverSchmerz“
• Yellow Flags• Psychosoz.
Faktoren
Klare medizinische Befunde:• Frakturen• Tumoren• Anomalien• Nervenwurzel-
affektionen• Spinalkanal-
stenose
bewegungs-abhängig (35%)
• richtungs-spezifisch
• Hypomobilität
haltungs-abhängig (35%)
• richtungs-spezifisch
H. Luomajoki PhysioAustria 2018

Patientenbeispiele
H. Luomajoki PhysioAustria 2018

(Luomajoki et al 2007
H. Luomajoki PhysioAustria 2018

Odds Ratio by Cut off 2/6 Tests Positive = 8.0
Cross sectional studyN= 210100 Healthy controls110 Patients with LBP
H. Luomajoki PhysioAustria 2018

Tactile acuity and lumbopelvic motorcontrol in patients with back pain andhealthy controls
Luomajoki, H., & Moseley, G. L. (2011). Tactile acuity and lumbopelvic motor control in patientswith back pain and healthy controls. Br J Sports Med, 45(5), 437-440
Two Point Discrimination (TPD) Low Back Pain (LBP) andMovement Control Tests (MCT)
Case controls study; N=90 (LBP =44 / healthy =46)
H. Luomajoki PhysioAustria 2018
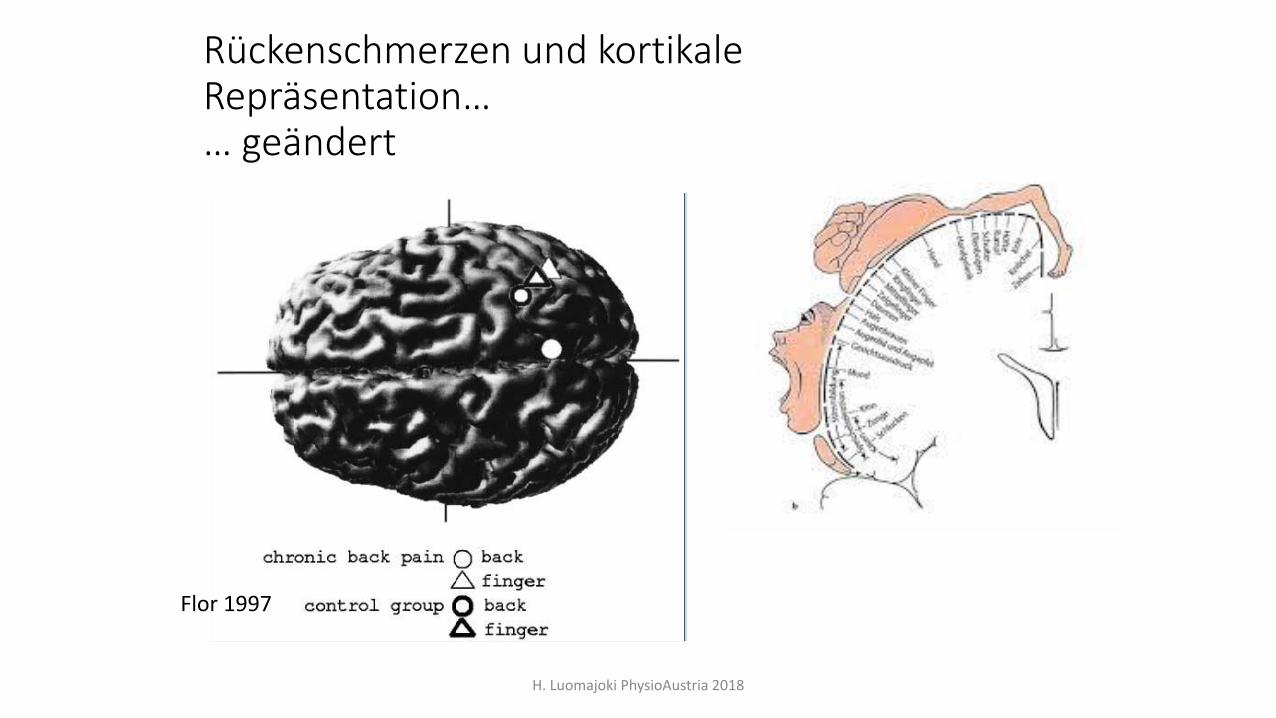
Flor 1997
Rückenschmerzen und kortikale Repräsentation…… geändert
H. Luomajoki PhysioAustria 2018

Eine einfache Möglichkeit die Körperwahrnehmung zu messen:
ZweipunktdiskriminationstestTwo Point Discrimination test (TPD)
H. Luomajoki PhysioAustria 2018

Resultate
H. Luomajoki PhysioAustria 2018
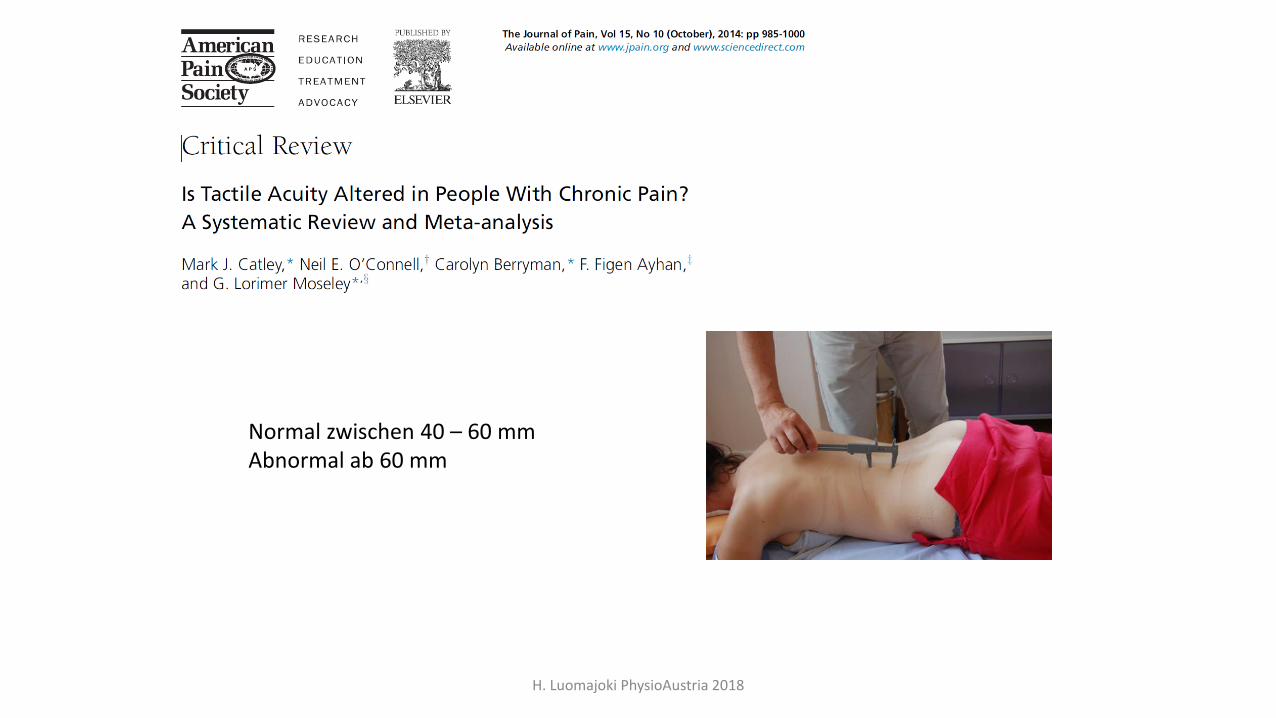
Normal zwischen 40 – 60 mmAbnormal ab 60 mm
H. Luomajoki PhysioAustria 2018
Kann Bewegungskontrolle geändert / verbessert werden?
H. Luomajoki PhysioAustria 2018

Case Series StudyN=40 PatOhne Kontrollgruppe
H. Luomajoki PhysioAustria 2018

RCT’s
H. Luomajoki PhysioAustria 2018
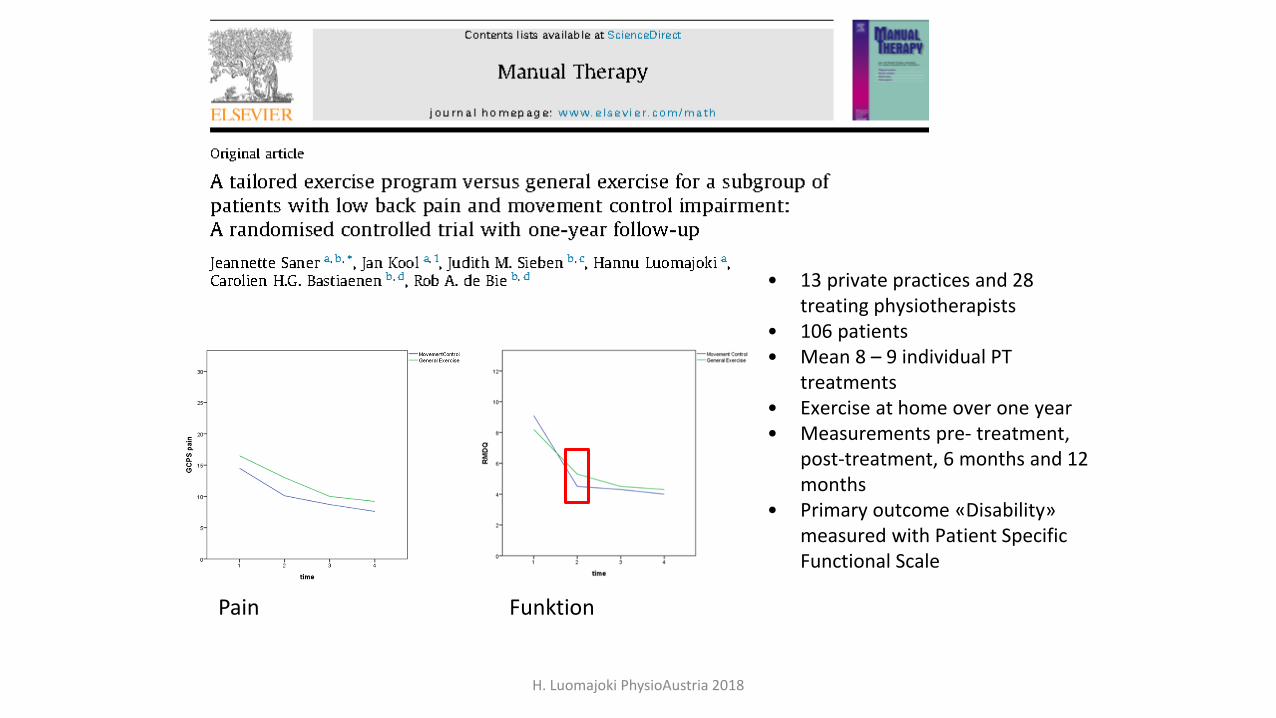
Pain Funktion
• 13 private practices and 28 treating physiotherapists
• 106 patients• Mean 8 – 9 individual PT
treatments• Exercise at home over one year• Measurements pre- treatment,
post-treatment, 6 months and 12 months
• Primary outcome «Disability» measured with Patient SpecificFunctional Scale
H. Luomajoki PhysioAustria 2018

2016
• Same setting as Saner et al 2015• 70 Pat. (drop-out rate: 12.9 %). • Between group difference (PSFS) -1.9 Points (-3.9 to -0.5) 95% (CI).
H. Luomajoki PhysioAustria 2018
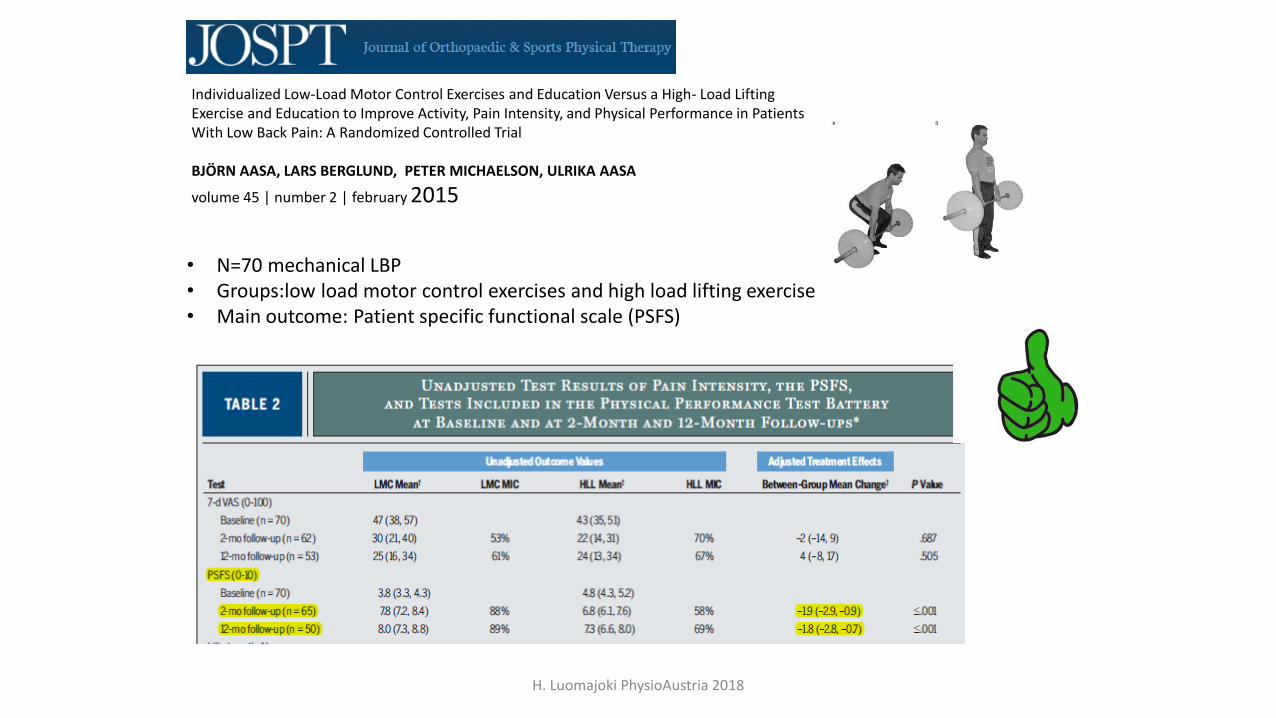
• N=70 mechanical LBP• Groups:low load motor control exercises and high load lifting exercise• Main outcome: Patient specific functional scale (PSFS)
Individualized Low-Load Motor Control Exercises and Education Versus a High- Load Lifting Exercise and Education to Improve Activity, Pain Intensity, and Physical Performance in PatientsWith Low Back Pain: A Randomized Controlled Trial
BJÖRN AASA, LARS BERGLUND, PETER MICHAELSON, ULRIKA AASA
volume 45 | number 2 | february 2015
H. Luomajoki PhysioAustria 2018
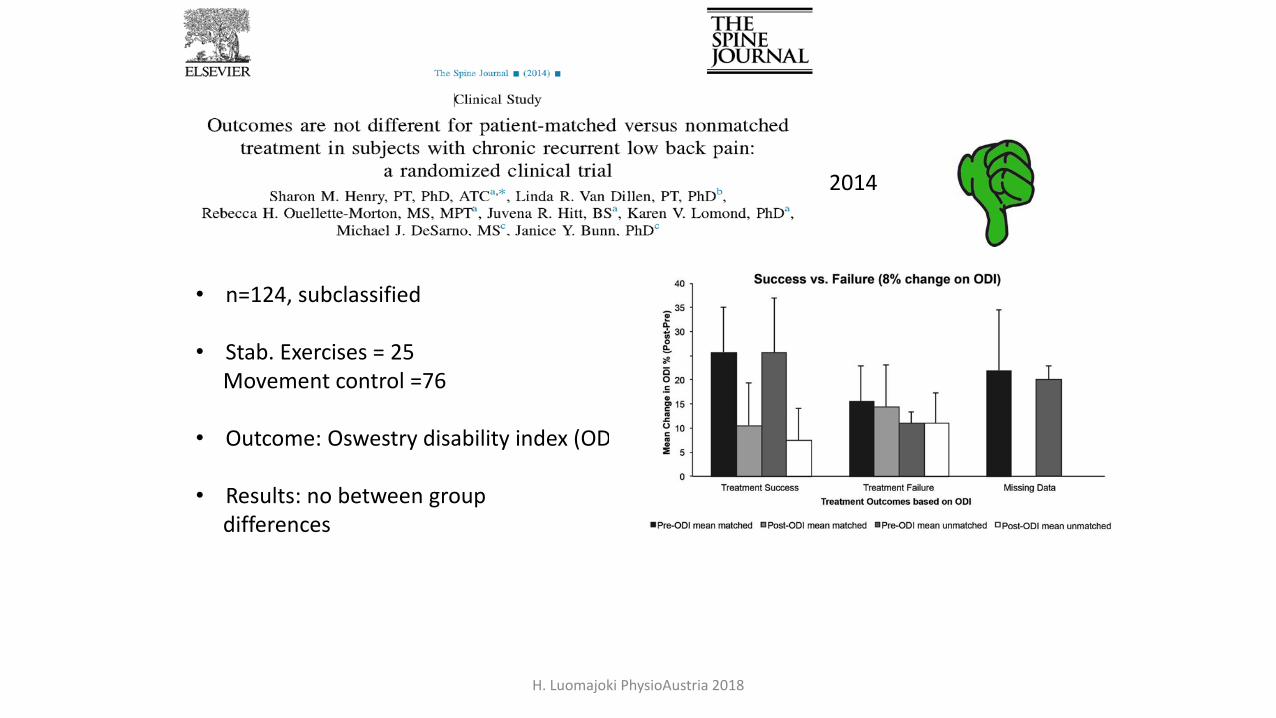
• n=124, subclassified
• Stab. Exercises = 25Movement control =76
• Outcome: Oswestry disability index (ODI)
• Results: no between groupdifferences
2014
H. Luomajoki PhysioAustria 2018
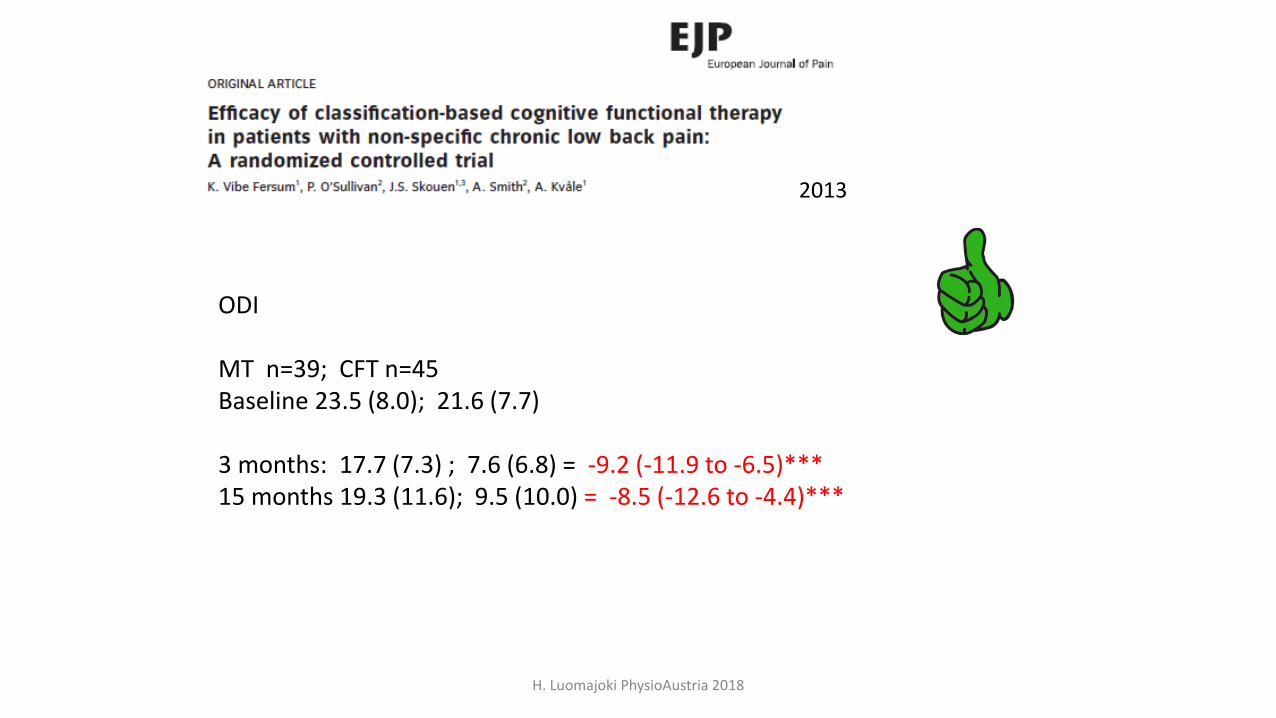
ODI
MT n=39; CFT n=45Baseline 23.5 (8.0); 21.6 (7.7)
3 months: 17.7 (7.3) ; 7.6 (6.8) = -9.2 (-11.9 to -6.5)***15 months 19.3 (11.6); 9.5 (10.0) = -8.5 (-12.6 to -4.4)***
2013
H. Luomajoki PhysioAustria 2018

Disability by 3 months follow up
Luomajoki kipukurssi AURON 2018

Luomajoki kipukurssi AURON 2018

By the way… wir haben auch Test Batterien für den
Nacken, Kopf und untere Extremitäten …
H. Luomajoki PhysioAustria 2018

H. Luomajoki PhysioAustria 2018

H. Luomajoki PhysioAustria 2018

Zukunftsrichtung…:Das Gehirn und Rückenschmerzen
• Kognitive Ebene: Angst, Katastrophisierung, Hypervigilanz = Explain Pain
• Sensorische Ebene: Körperwahrnehmung, Spüren wo der Rücken ist etc.
• Motorische Ebene: Bewegungskontrolle, Koordination, Propriozeption etc
H. Luomajoki PhysioAustria 2018

Results
Twenty-eight patients (46% male, mean age 41.5 years (SD 10.6)) were randomized to MMT (n = 14) or
UPT (n = 14). Patients’ adherence to treatment was >80% in both groups. Pain reduction (NRS; [95%CI])
was 2.14 [1.0 to 3.5] in the MMT and 0.69 [-2.0 to 2.5.] in the UPT. The between-group difference was 1.45
[0.0 to 4.0] (p = 0.03), representing a moderate effect size of 0.66 [-0.1 to 1.5]. Reduction in disability on the
RMDQ was 6.71 [4.2 to 9.3] in MMT and 4.69 [1.9 to 7.4] in UPT, with a non-significant between-group difference of 2.02 [-1.5 to 5.6] (p = 0.25). The
H. Luomajoki PhysioAustria 2018

Take home message
• Physiotherapie hat erstaunlich gute Evidenz
• Es lohnt sich Patienten subklassifizieren
• Im Alltag soll die von Patienten selbst wahrgenommene Behinderung ermittelt werden
• Forschung aus der Praxis: Subgruppenspezifische Probleme brauchen auch spezifische Übungen
H. Luomajoki PhysioAustria 2018

Vielen Dank!
• Kauft das neue Buch!
H. Luomajoki PhysioAustria 2018
![Fahrdynamik - Fahrsicherheit - Fahrerplatz · analysis of the musculoskeletal system [8] Auch wenn eine zufriedenstellende Be der tatsächlichen urteilungauf Fahrerbelastung Grundlage](https://static.fdokument.com/doc/165x107/609527d3eedca951db2cec16/fahrdynamik-fahrsicherheit-fahrerplatz-analysis-of-the-musculoskeletal-system.jpg)