Oxaliplatin Neuropathie - Prophylaxe und Therapie 1/2_Supportive... · Universitätsklinikum Essen...
29
Westdeutsches Tumorzentrum WTZ UK Essen WTZ Westdeutsches Tumorzentrum WTZ UK Essen WTZ Dr. med. Tanja Trarbach Innere Klinik (Tumorforschung) Universitätsklinikum Essen Direktor: Prof. Martin Schuler Oxaliplatin Neuropathie - Prophylaxe und Therapie
Transcript of Oxaliplatin Neuropathie - Prophylaxe und Therapie 1/2_Supportive... · Universitätsklinikum Essen...

Westdeutsches Tumorzentrum WTZ UK EssenWTZ Westdeutsches Tumorzentrum WTZ UK Essen
WTZ
Dr. med. Tanja Trarbach
Innere Klinik (Tumorforschung)
Universitätsklinikum Essen
Direktor: Prof. Martin Schuler
Oxaliplatin Neuropathie -
Prophylaxe und Therapie

Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Möglicher Pathomechanismus Na+
Einflusshemmung –Chelatbildung von
Oxalat mit Ca2+
ATP ATP
EXTRA
Membran
INTRA
Ca2+
Oxalat
Dach-Pt
Na+
Oxaliplatin
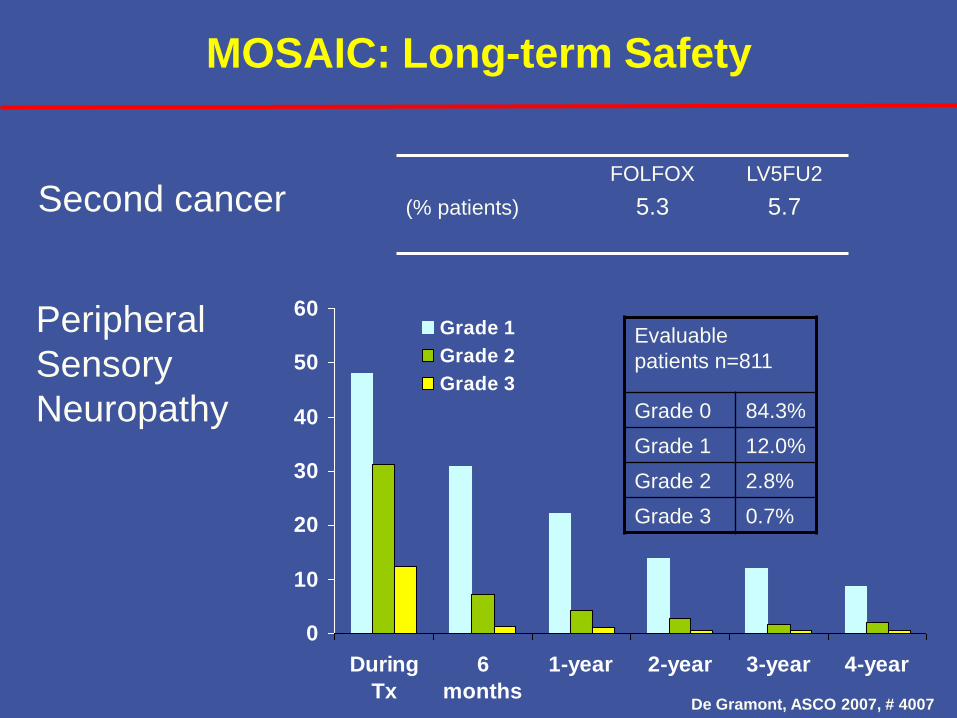
MOSAIC: Long-term Safety
(% patients)
FOLFOX
5.3
LV5FU2
5.7
0
10
20
30
40
50
60
During
Tx
6
months
1-year 2-year 3-year 4-year
Grade 1
Grade 2
Grade 3
Second cancer
Peripheral
Sensory
Neuropathy
Evaluable
patients n=811
Grade 0 84.3%
Grade 1 12.0%
Grade 2 2.8%
Grade 3 0.7%
De Gramont, ASCO 2007, # 4007
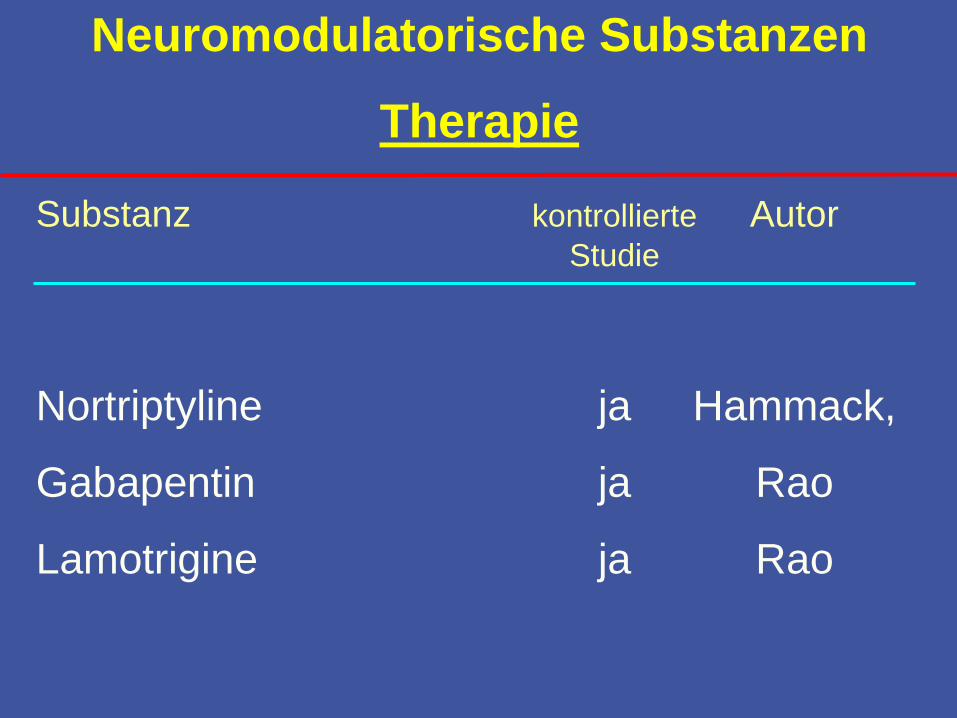
Substanz kontrollierte AutorStudie
Nortriptyline ja Hammack,
Gabapentin ja Rao
Lamotrigine ja Rao
Neuromodulatorische Substanzen
Therapie
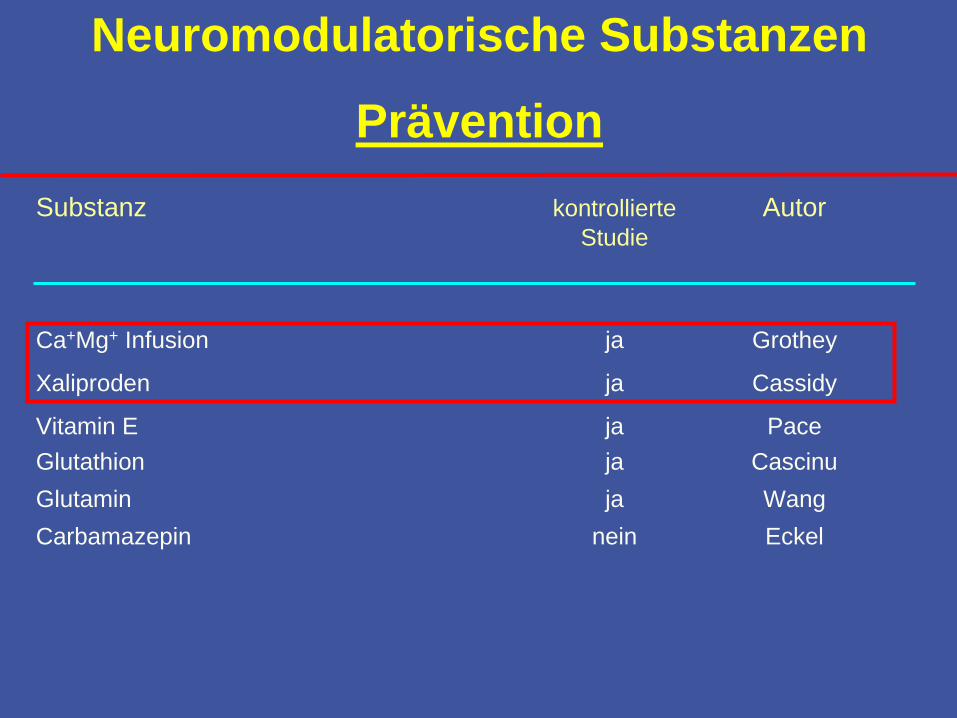
Substanz kontrollierte AutorStudie
Ca+Mg+ Infusion ja Grothey
Xaliproden ja Cassidy
Vitamin E ja Pace
Glutathion ja Cascinu
Glutamin ja Wang
Carbamazepin nein Eckel
Neuromodulatorische Substanzen
Prävention

Substanz kontrollierte AutorStudie
Ca+Mg+ Infusion ja Grothey
Xaliproden ja Cassidy
Vitamin E ja Pace
Glutathion ja Cascinu
Glutamin ja Wang
Carbamazepin nein Eckel
Neuromodulatorische Substanzen
Prävention
STOP and GO ?

OPTIMOX 1
Tournigand et al., JCO 2006
6x FOLFOX7- 12x sLV5FU2 - 6x FOLFOX7
FOLFOX4
623 Pat
R
Kum. Oxali 780 1560
(%) FOLFOX4 FOLFOX7
RR 58.5 58.3
PFS 9.0 9.2
OS 20.0 21.6
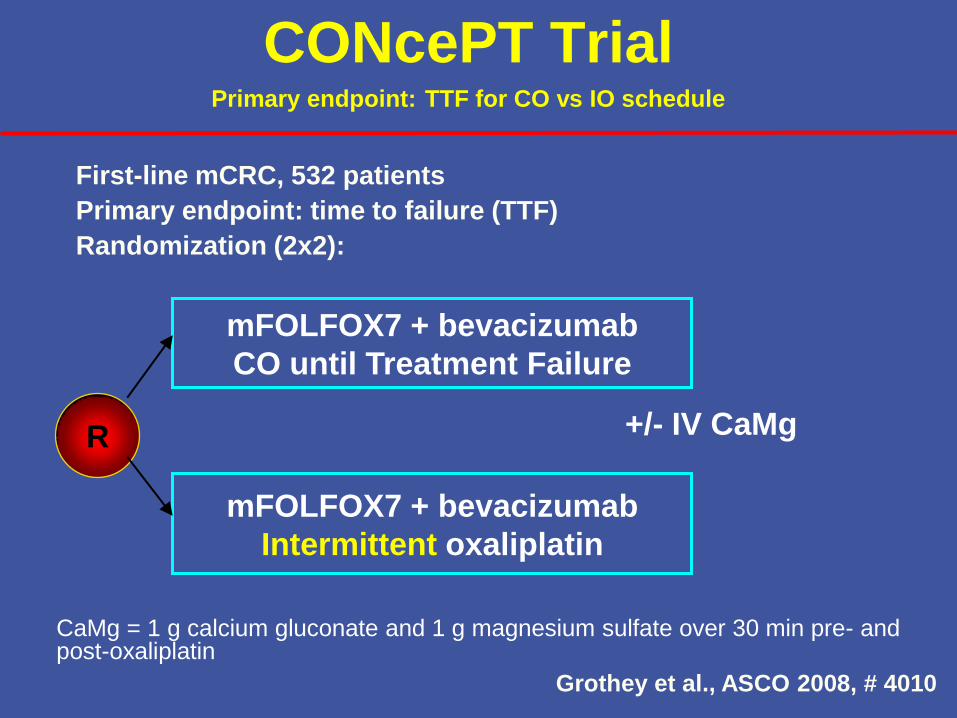
CaMg = 1 g calcium gluconate and 1 g magnesium sulfate over 30 min pre- and post-oxaliplatin
CONcePT TrialPrimary endpoint: TTF for CO vs IO schedule
First-line mCRC, 532 patients
Primary endpoint: time to failure (TTF)
Randomization (2x2):
mFOLFOX7 + bevacizumab
CO until Treatment Failure
mFOLFOX7 + bevacizumab
Intermittent oxaliplatin
+/- IV CaMgR
Grothey et al., ASCO 2008, # 4010

CaMg = 1 g calcium gluconate and 1 g magnesium sulfate over 30 min pre- and post-oxaliplatin
CONcePT TrialPrimary endpoint: TTF for CO vs IO schedule
No randomization to placebo after protocol amendment
First-line mCRC, 532 patients
Primary endpoint: time to failure (TTF)
Randomization (2x2):
mFOLFOX7 + bevacizumab
CO until Treatment Failure
mFOLFOX7 + bevacizumab
Intermittent oxaliplatin
+/- IV CaMgR
270 pts
Grothey et al., ASCO 2008, # 4010
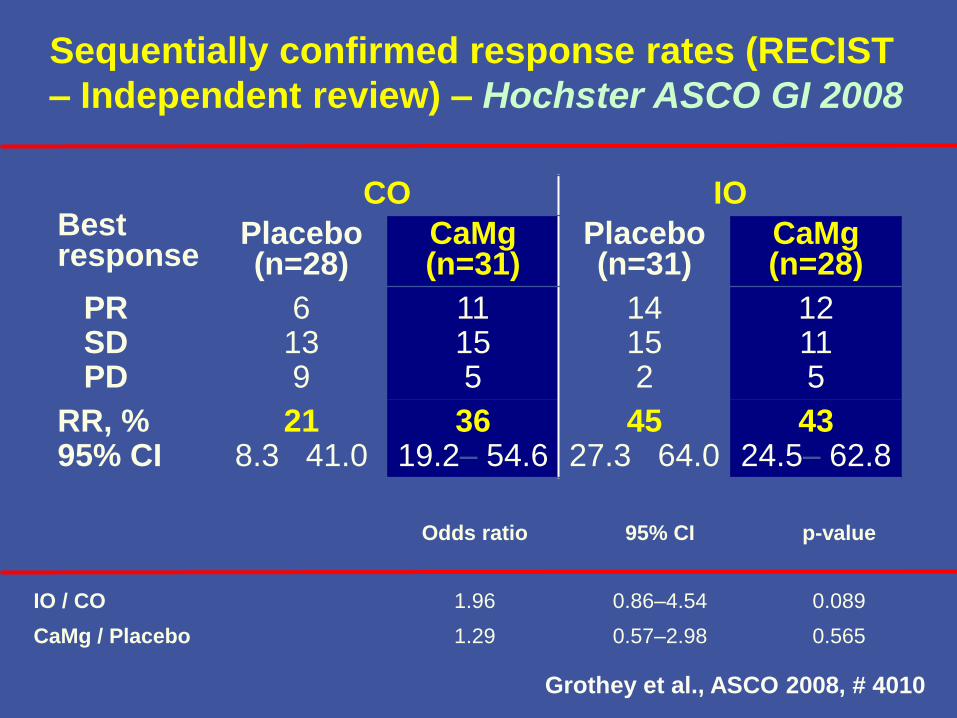
Sequentially confirmed response rates (RECIST
– Independent review) – Hochster ASCO GI 2008
Best response
CO IO
Placebo (n=28)
CaMg(n=31)
Placebo (n=31)
CaMg(n=28)
PRSDPD
6139
11155
14152
12115
RR, %95% CI
218.3– 41.0
3619.2– 54.6
4527.3– 64.0
4324.5– 62.8
Odds ratio 95% CI p-value
IO / CO 1.96 0.86–4.54 0.089
CaMg / Placebo 1.29 0.57–2.98 0.565
Grothey et al., ASCO 2008, # 4010
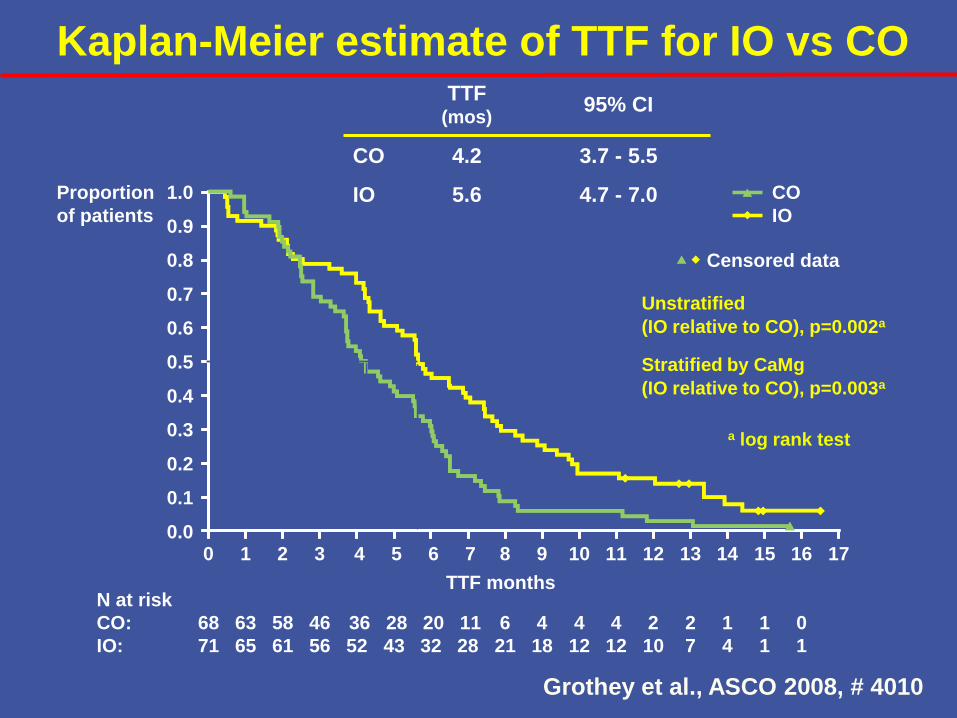
Kaplan-Meier estimate of TTF for IO vs CO
a log rank test
Unstratified
(IO relative to CO), p=0.002a
Stratified by CaMg
(IO relative to CO), p=0.003a
Proportion
of patients
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 2 4 6 8 10 12 14 16 17
TTF months
CO
IO
Censored data
N at risk
CO:
IO:
1 3 5 7 9 11 13 15
68
71
58
61
36
52
20
32
6
21
4
12
2
10
1
4
0
1
63
65
46
56
28
43
11
28
4
18
4
12
2
7
1
1
TTF (mos)
95% CI
CO 4.2 3.7 - 5.5
IO 5.6 4.7 - 7.0
Grothey et al., ASCO 2008, # 4010
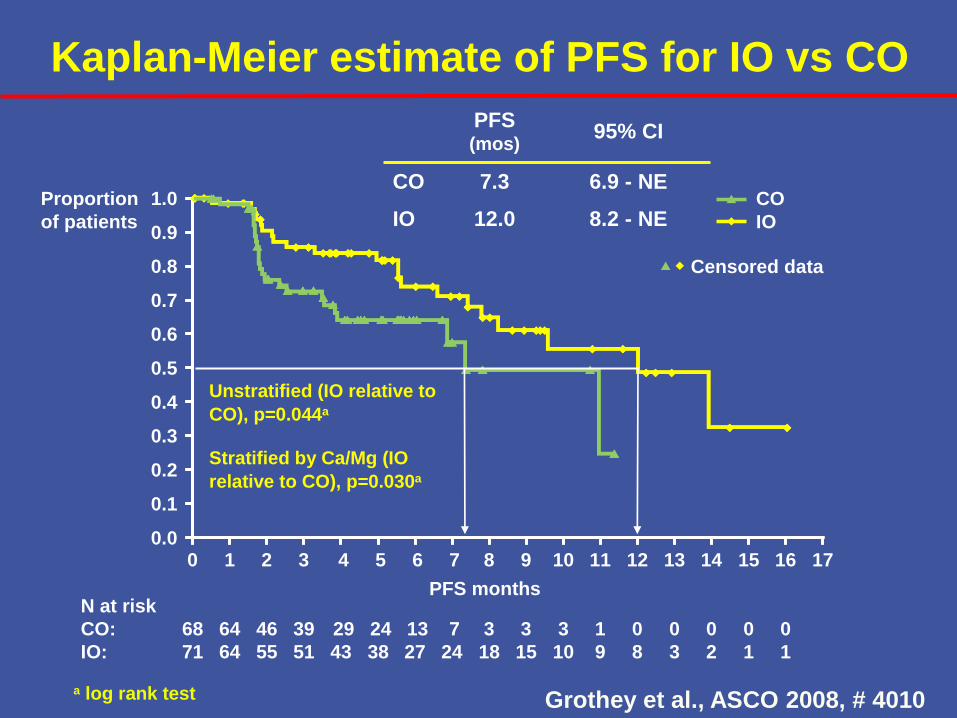
Kaplan-Meier estimate of PFS for IO vs CO
a log rank test
Unstratified (IO relative to
CO), p=0.044a
Stratified by Ca/Mg (IO
relative to CO), p=0.030a
Proportion
of patients
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 2 4 6 8 10 12 14 16 17
PFS months
CO
IO
Censored data
N at risk
CO:
IO:
1 3 5 7 9 11 13 15
68
71
46
55
29
43
13
27
3
18
3
10
0
8
0
2
0
1
64
64
39
51
24
38
7
24
3
15
1
9
0
3
0
1
PFS (mos)
95% CI
CO 7.3 6.9 - NE
IO 12.0 8.2 - NE
Grothey et al., ASCO 2008, # 4010
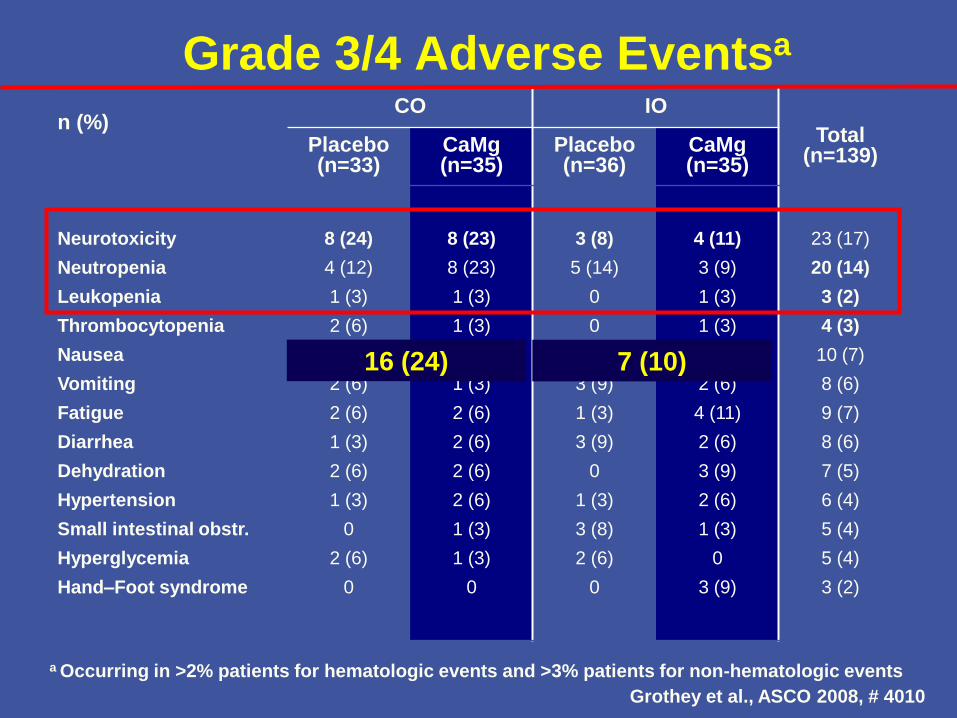
Grade 3/4 Adverse Eventsa
n (%)CO IO
Total(n=139)
Placebo(n=33)
CaMg(n=35)
Placebo(n=36)
CaMg(n=35)
Neurotoxicity
Neutropenia
Leukopenia
Thrombocytopenia
Nausea
Vomiting
Fatigue
Diarrhea
Dehydration
Hypertension
Small intestinal obstr.
Hyperglycemia
Hand–Foot syndrome
8 (24)
4 (12)
1 (3)
2 (6)
2 (6)
2 (6)
2 (6)
1 (3)
2 (6)
1 (3)
0
2 (6)
0
8 (23)
8 (23)
1 (3)
1 (3)
2 (6)
1 (3)
2 (6)
2 (6)
2 (6)
2 (6)
1 (3)
1 (3)
0
3 (8)
5 (14)
0
0
2 (6)
3 (9)
1 (3)
3 (9)
0
1 (3)
3 (8)
2 (6)
0
4 (11)
3 (9)
1 (3)
1 (3)
4 (11)
2 (6)
4 (11)
2 (6)
3 (9)
2 (6)
1 (3)
0
3 (9)
23 (17)
20 (14)
3 (2)
4 (3)
10 (7)
8 (6)
9 (7)
8 (6)
7 (5)
6 (4)
5 (4)
5 (4)
3 (2)
a Occurring in >2% patients for hematologic events and >3% patients for non-hematologic events
16 (24) 7 (10)
Grothey et al., ASCO 2008, # 4010
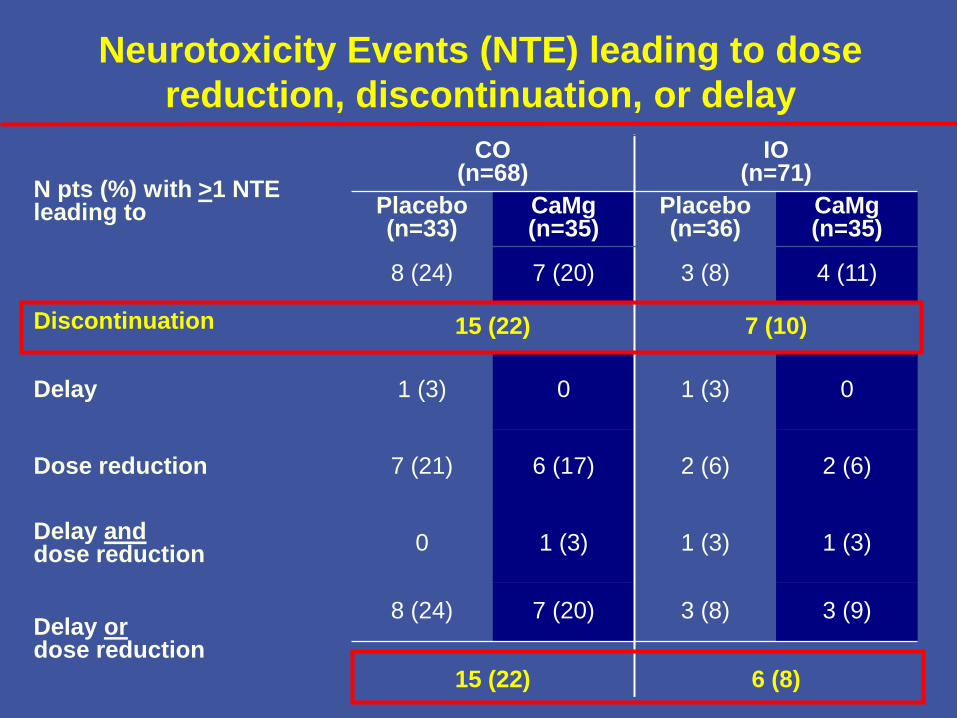
Neurotoxicity Events (NTE) leading to dose
reduction, discontinuation, or delay
N pts (%) with >1 NTE leading to
CO (n=68)
IO(n=71)
Placebo(n=33)
CaMg(n=35)
Placebo(n=36)
CaMg(n=35)
Discontinuation
8 (24) 7 (20) 3 (8) 4 (11)
15 (22) 7 (10)
Delay 1 (3) 0 1 (3) 0
Dose reduction 7 (21) 6 (17) 2 (6) 2 (6)
Delay anddose reduction
0 1 (3) 1 (3) 1 (3)
Delay ordose reduction
8 (24) 7 (20) 3 (8) 3 (9)
15 (22) 6 (8)
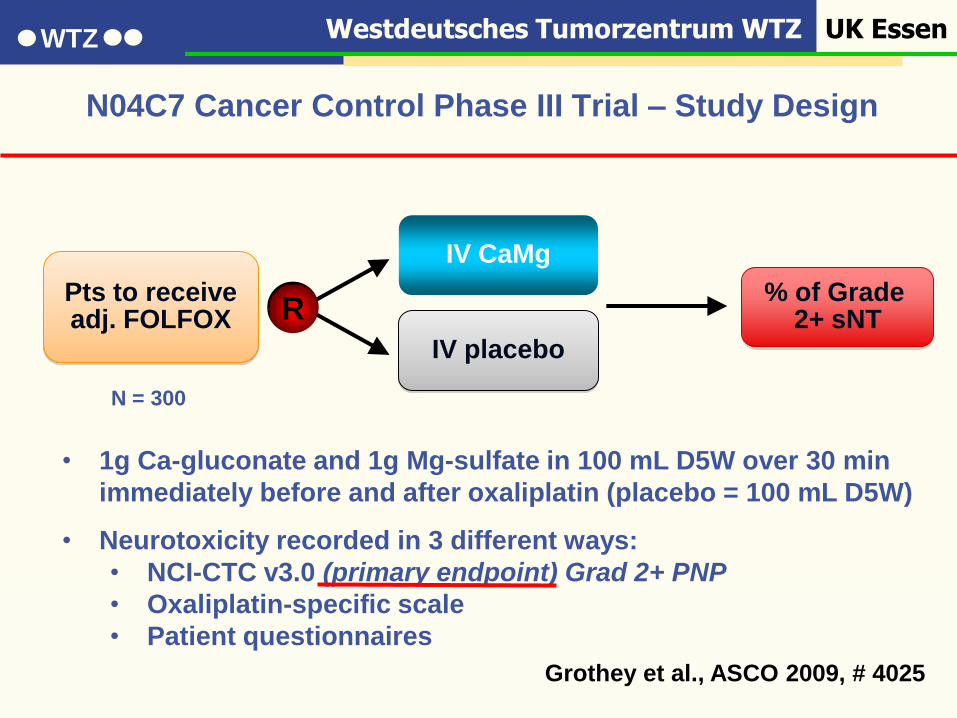
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
N04C7 Cancer Control Phase III Trial – Study Design
• 1g Ca-gluconate and 1g Mg-sulfate in 100 mL D5W over 30 min
immediately before and after oxaliplatin (placebo = 100 mL D5W)
• Neurotoxicity recorded in 3 different ways:
• NCI-CTC v3.0 (primary endpoint) Grad 2+ PNP
• Oxaliplatin-specific scale
• Patient questionnaires
Pts to receiveadj. FOLFOX
IV CaMg
% of Grade 2+ sNTR
IV placebo
Grothey et al., ASCO 2009, # 4025
N = 300
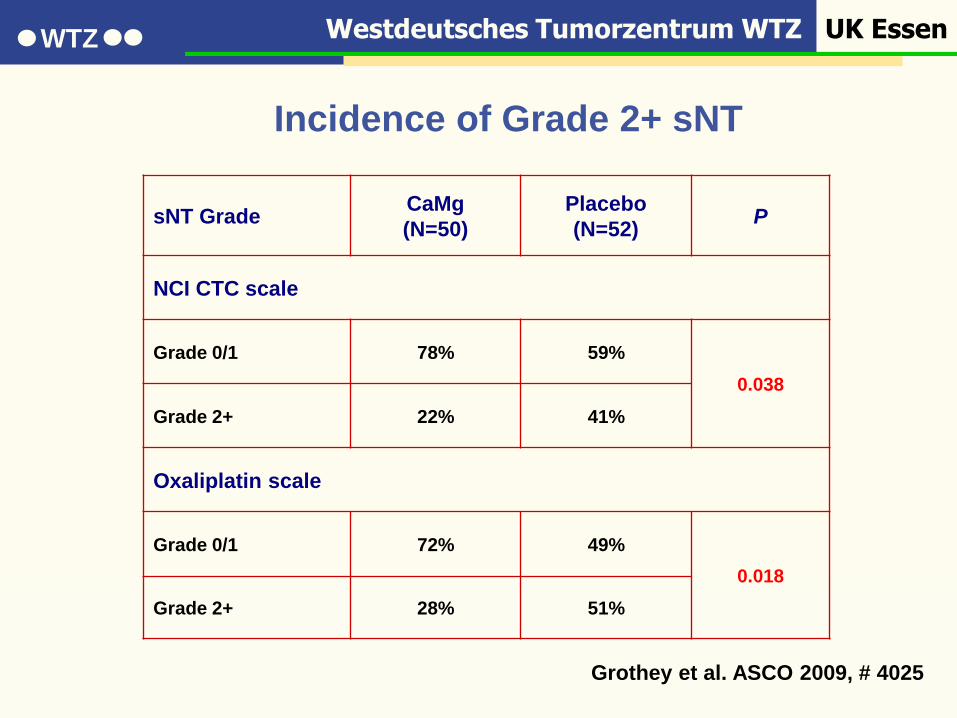
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Incidence of Grade 2+ sNT
sNT GradeCaMg
(N=50)
Placebo
(N=52)P
NCI CTC scale
Grade 0/1 78% 59%
0.038
Grade 2+ 22% 41%
Oxaliplatin scale
Grade 0/1 72% 49%
0.018
Grade 2+ 28% 51%
Grothey et al. ASCO 2009, # 4025
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
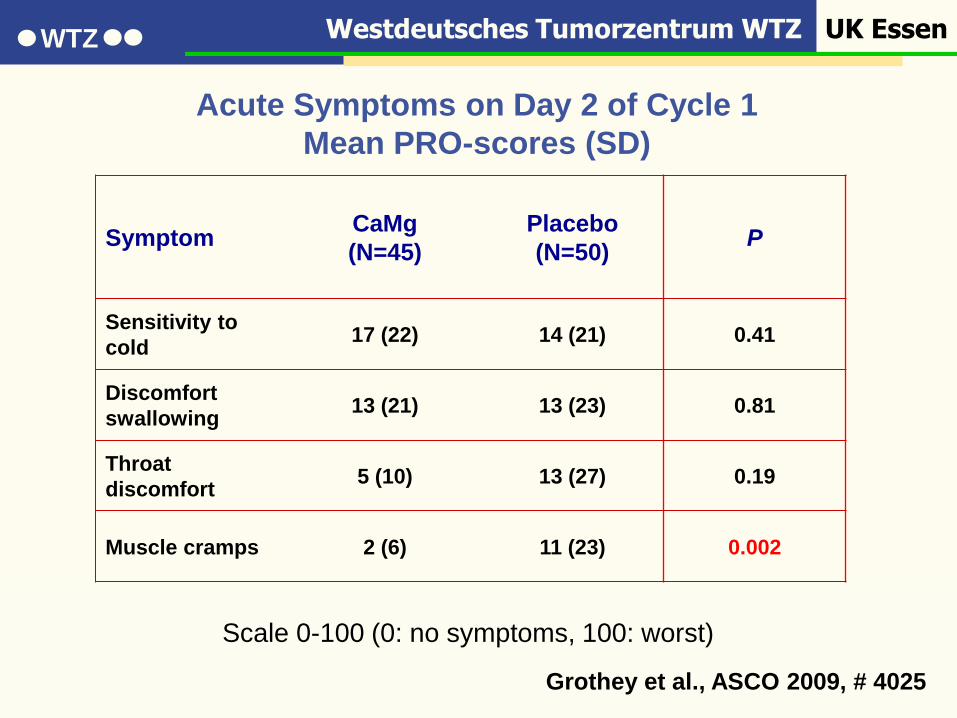
Acute Symptoms on Day 2 of Cycle 1
Mean PRO-scores (SD)
SymptomCaMg
(N=45)
Placebo
(N=50)P
Sensitivity to
cold17 (22) 14 (21) 0.41
Discomfort
swallowing13 (21) 13 (23) 0.81
Throat
discomfort5 (10) 13 (27) 0.19
Muscle cramps 2 (6) 11 (23) 0.002
Scale 0-100 (0: no symptoms, 100: worst)
Grothey et al., ASCO 2009, # 4025
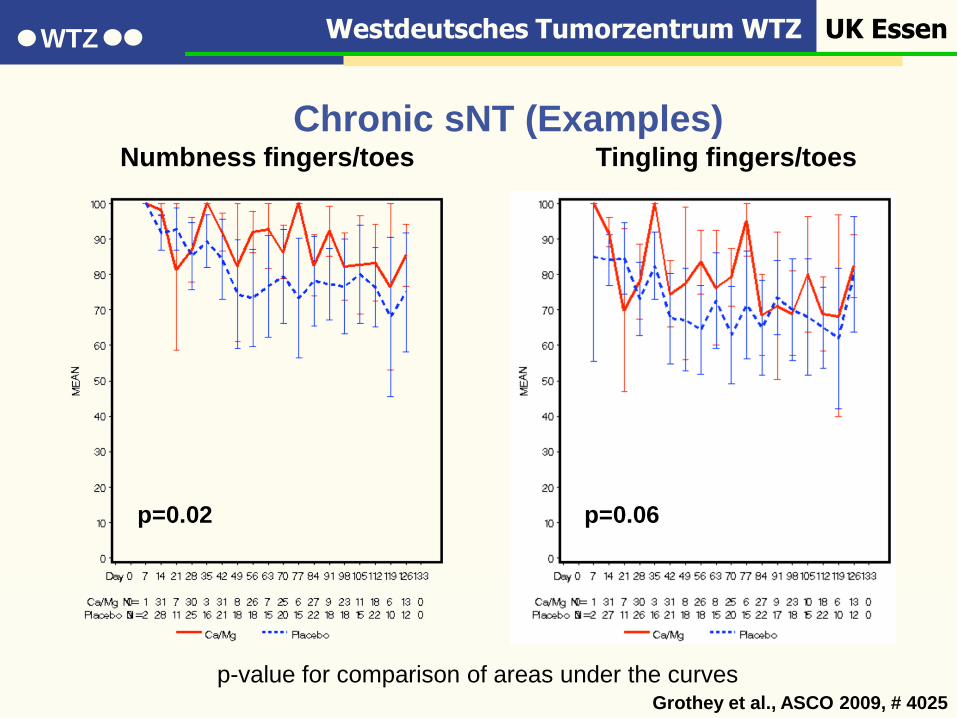
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Chronic sNT (Examples)Numbness fingers/toes Tingling fingers/toes
p=0.02 p=0.06
p-value for comparison of areas under the curvesGrothey et al., ASCO 2009, # 4025

Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Chronic sNT (Examples)Numbness fingers/toes Tingling fingers/toes
p=0.02 p=0.06
p-value for comparison of areas under the curvesGrothey et al., ASCO 2009, # 4025
Keine
Effektivitätsdaten
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
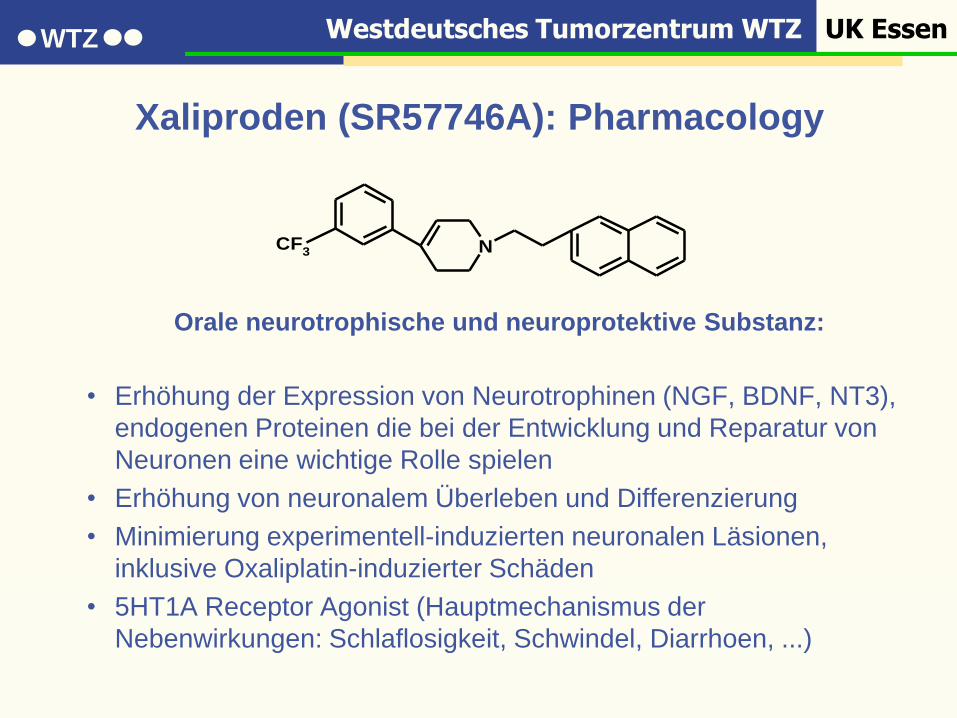
Xaliproden (SR57746A): Pharmacology
Orale neurotrophische und neuroprotektive Substanz:
• Erhöhung der Expression von Neurotrophinen (NGF, BDNF, NT3),
endogenen Proteinen die bei der Entwicklung und Reparatur von
Neuronen eine wichtige Rolle spielen
• Erhöhung von neuronalem Überleben und Differenzierung
• Minimierung experimentell-induzierten neuronalen Läsionen,
inklusive Oxaliplatin-induzierter Schäden
• 5HT1A Receptor Agonist (Hauptmechanismus der
Nebenwirkungen: Schlaflosigkeit, Schwindel, Diarrhoen, ...)
NCF3
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
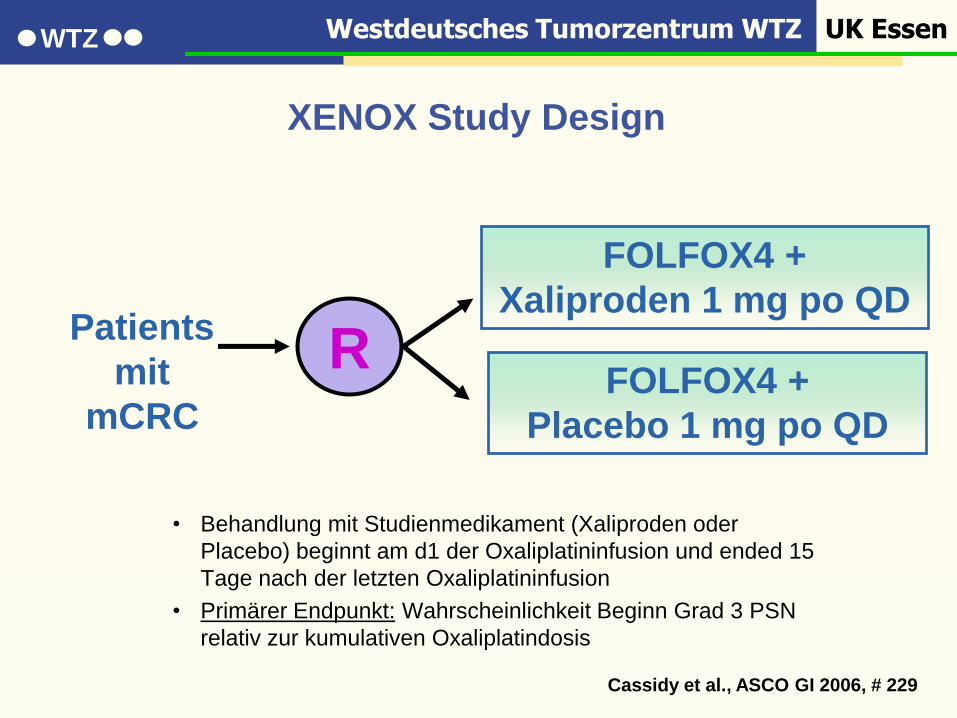
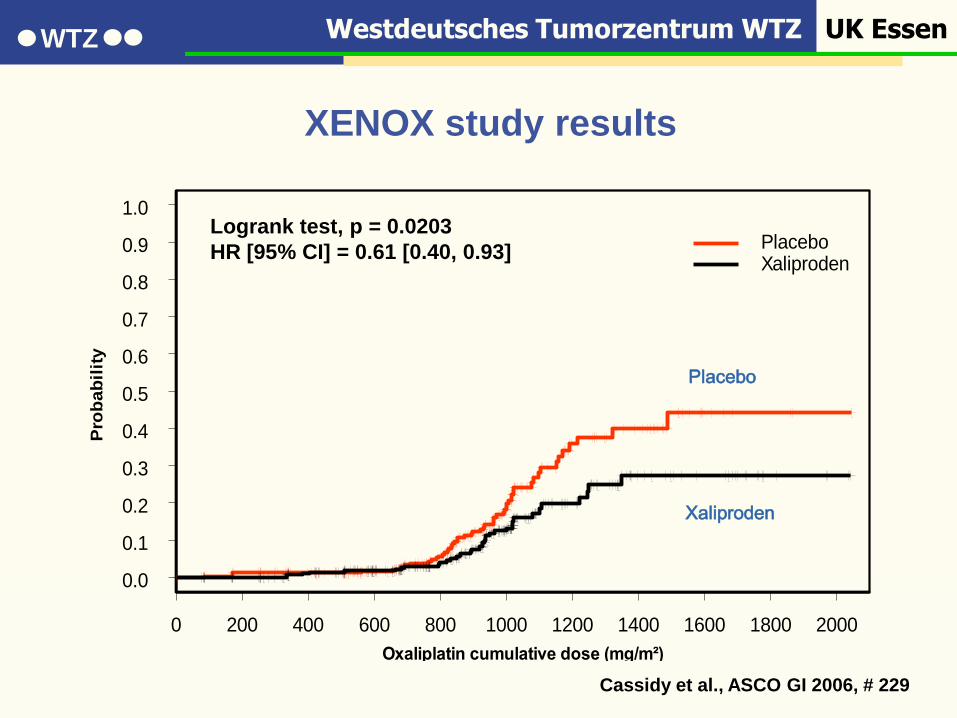
XENOX Study Design
• Behandlung mit Studienmedikament (Xaliproden oder
Placebo) beginnt am d1 der Oxaliplatininfusion und ended 15
Tage nach der letzten Oxaliplatininfusion
• Primärer Endpunkt: Wahrscheinlichkeit Beginn Grad 3 PSN
relativ zur kumulativen Oxaliplatindosis
R
FOLFOX4 +
Xaliproden 1 mg po QD
FOLFOX4 +
Placebo 1 mg po QD
Patients
mit
mCRC
Cassidy et al., ASCO GI 2006, # 229
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
0 200 400 600 800 1000 1200 1400 1600 1800 2000
Oxaliplatin cumulative dose (mg/m²)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
ba
bil
ity
PlaceboXaliproden
Patients at risk:
Placebo 324 303 275 240 199 104 34 23 6 3 1
Xaliproden 325 308 281 248 200 119 50 23 16 5 2
Logrank test, p = 0.0203
HR [95% CI] = 0.61 [0.40, 0.93]
Placebo
Xaliproden
XENOX study results
Cassidy et al., ASCO GI 2006, # 229
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
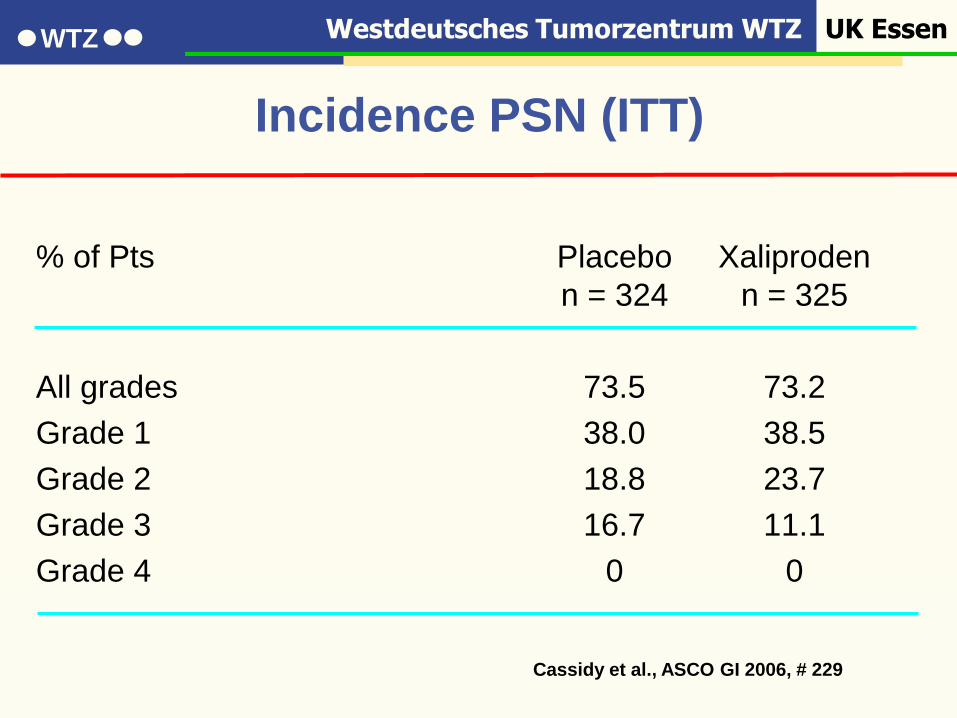
% of Pts Placebo Xaliproden
n = 324 n = 325
All grades 73.5 73.2
Grade 1 38.0 38.5
Grade 2 18.8 23.7
Grade 3 16.7 11.1
Grade 4 0 0
Incidence PSN (ITT)
Cassidy et al., ASCO GI 2006, # 229
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
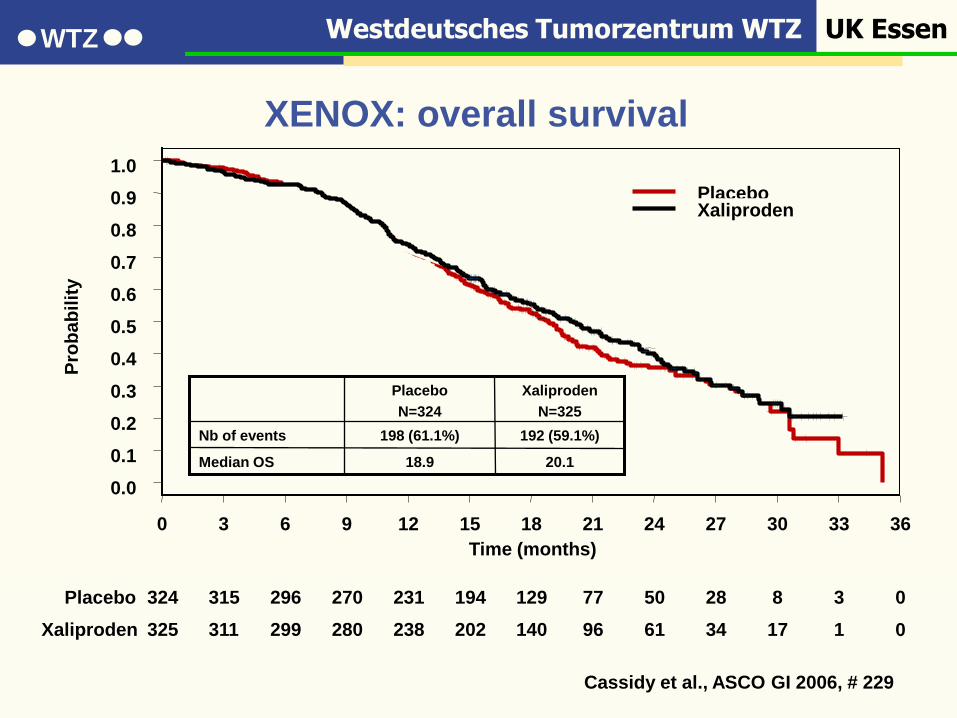
Placebo 324 315 296 270 231 194 129 77 50 28 8 3 0
Xaliproden 325 311 299 280 238 202 140 96 61 34 17 1 0
0 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
ba
bil
ity
PlaceboXaliproden
20.1
192 (59.1%)
Xaliproden
N=325
18.9Median OS
198 (61.1%)Nb of events
Placebo
N=324
XENOX: overall survival
Cassidy et al., ASCO GI 2006, # 229
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
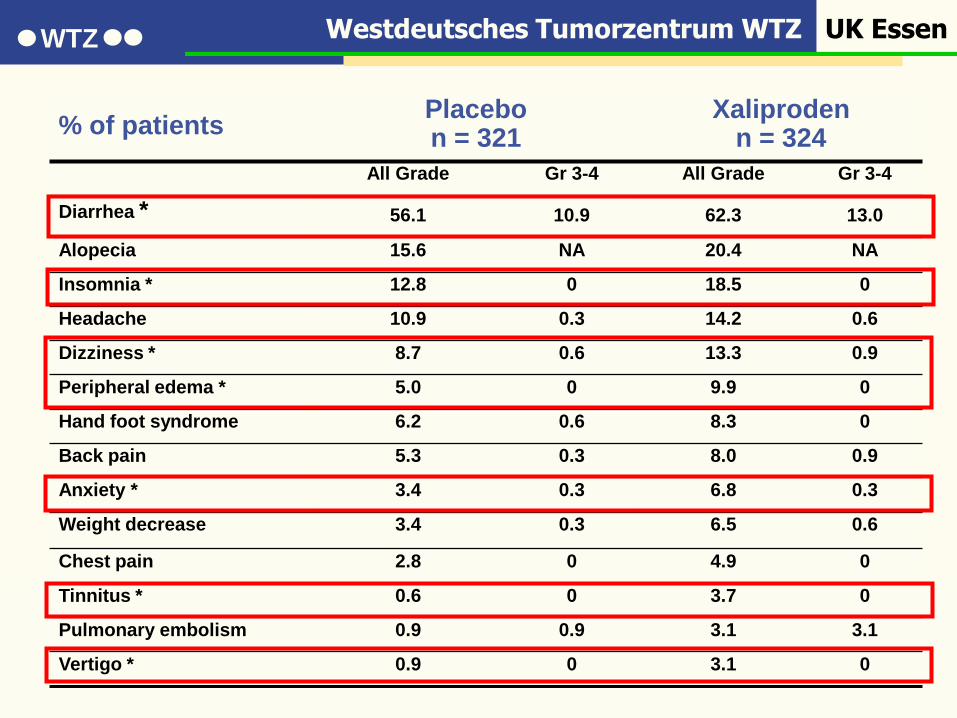
XENOX: all-Grade adverse events 2% higher incidence in Xaliproden vs Placebo
% of patientsPlacebon = 321
Xaliproden n = 324
All Grade Gr 3-4 All Grade Gr 3-4
Diarrhea * 56.1 10.9 62.3 13.0
Alopecia 15.6 NA 20.4 NA
Insomnia * 12.8 0 18.5 0
Headache 10.9 0.3 14.2 0.6
Dizziness * 8.7 0.6 13.3 0.9
Peripheral edema * 5.0 0 9.9 0
Hand foot syndrome 6.2 0.6 8.3 0
Back pain 5.3 0.3 8.0 0.9
Anxiety * 3.4 0.3 6.8 0.3
Weight decrease 3.4 0.3 6.5 0.6
Chest pain 2.8 0 4.9 0
Tinnitus * 0.6 0 3.7 0
Pulmonary embolism 0.9 0.9 3.1 3.1
Vertigo * 0.9 0 3.1 0
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
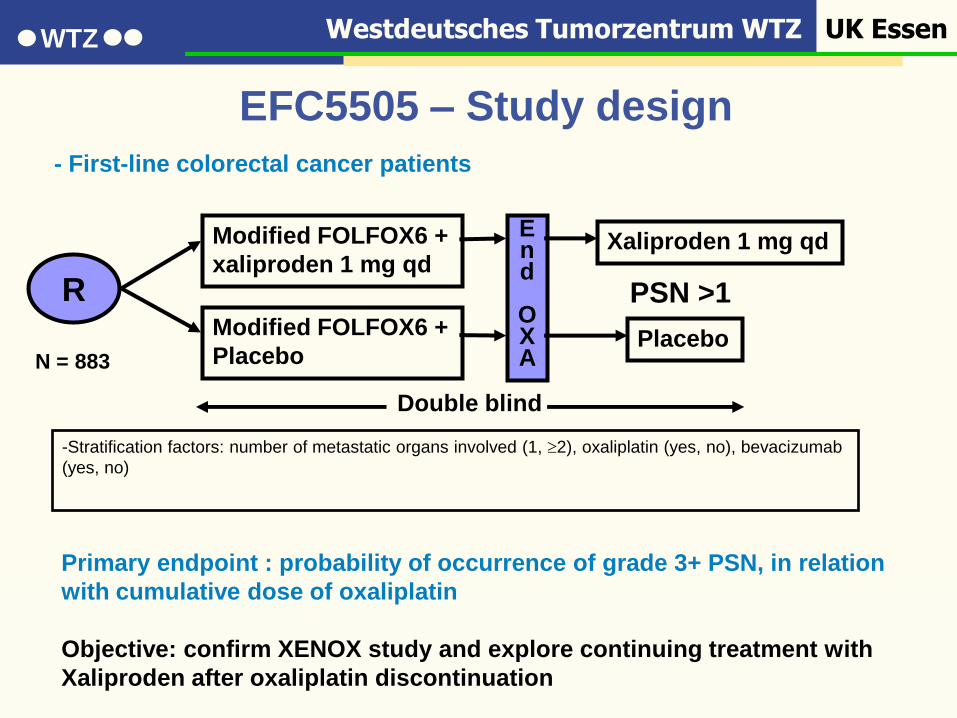
EFC5505 – Study design
Modified FOLFOX6 +
xaliproden 1 mg qd
Modified FOLFOX6 +
Placebo
End
OXA
Xaliproden 1 mg qd
Placebo
R PSN >1
Double blind
-Stratification factors: number of metastatic organs involved (1, 2), oxaliplatin (yes, no), bevacizumab
(yes, no)
- First-line colorectal cancer patients
Primary endpoint : probability of occurrence of grade 3+ PSN, in relation
with cumulative dose of oxaliplatin
Objective: confirm XENOX study and explore continuing treatment with
Xaliproden after oxaliplatin discontinuation
N = 883
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
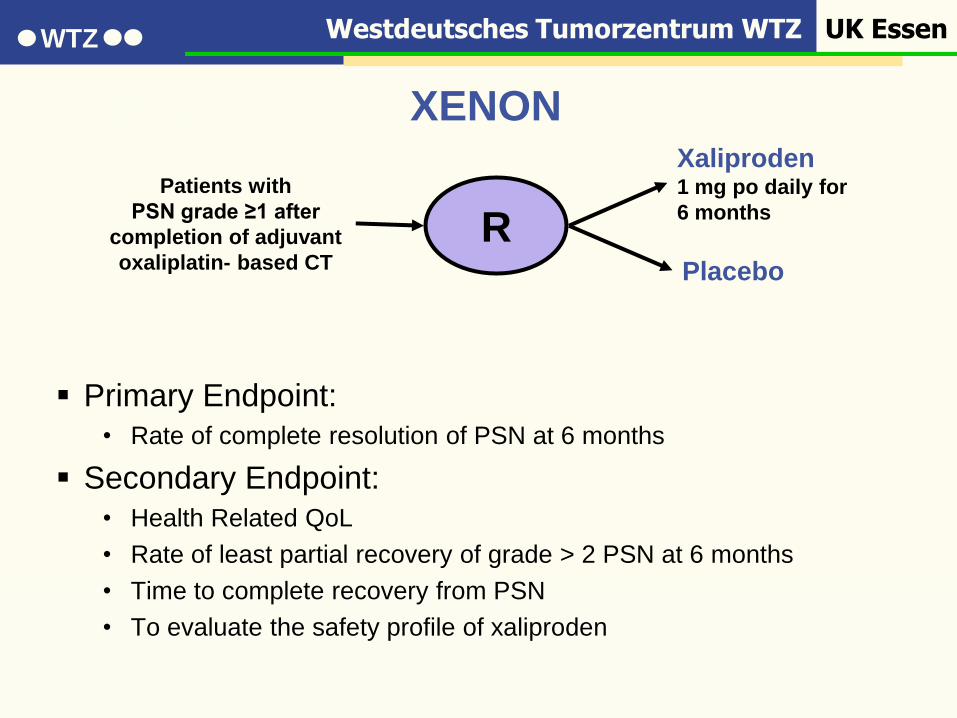
XENON: “Curative study”
Primary Endpoint:
• Rate of complete resolution of PSN at 6 months
Secondary Endpoint:
• Health Related QoL
• Rate of least partial recovery of grade > 2 PSN at 6 months
• Time to complete recovery from PSN
• To evaluate the safety profile of xaliproden
R
Xaliproden1 mg po daily for
6 months
Placebo
Patients with
PSN grade ≥1 after
completion of adjuvant
oxaliplatin- based CT
XENON
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Medikamentöse Therapie der PSN enttäuschend
STOP and GO Strategien in den Alltag integrieren
In der adjuvanten Situation Hinweise auf protektive
Ca/Mg Infusionen, aber Effektivitätsdaten fehlen
Zusammenfassung
Westdeutsches Tumorzentrum WTZ UK EssenWTZ
Vielen Dank für Ihre
Aufmerksamkeit !





![Multizentrische Phase II-Studie mit Docetaxel, Oxaliplatin ... · soziation mit der Helicobacter pylori induzierten Typ-B-Gastritis vermutet [5]. Ein direk-ter Zusammenhang konnte](https://static.fdokument.com/doc/165x107/5e2fef6a3a8a88238517d277/multizentrische-phase-ii-studie-mit-docetaxel-oxaliplatin-soziation-mit-der.jpg)