Robotic-assisted Visceral Surgery: Where is it? „Die SGC muss das ...
25
SGC Journal SSC www.swiss-knife.org swiss knife 2008; 4 (novemberr) Robotic-assisted Visceral Surgery: Where is it? Monika E. Hagen, Oliver J. Wagner Stephan A. Vorburger, Daniel Candinas Philippe Morel Education Interview „Die SGC muss das Sprachrohr der Chirurgen sein, das in der Gesellschaft auf Resonanz stösst.“ Othmar Schöb Education Meta-Analyses: Advantages and Caveats Ueli Güller
Transcript of Robotic-assisted Visceral Surgery: Where is it? „Die SGC muss das ...
SGC Journal SSC
www.swiss-knife.org swiss knife 2008; 4 (novemberr)
Robotic-assisted Visceral Surgery: Where is it?Monika E. Hagen, Oliver J. WagnerStephan A. Vorburger, Daniel CandinasPhilippe Morel
Education
Interview„Die SGC muss das Sprachrohr der Chirurgen sein, das in der Gesellschaft auf Resonanz stösst.“Othmar Schöb
EducationMeta-Analyses: Advantages and CaveatsUeli Güller
Introducing the Endo Clip™ III 5mm Clip Applier.
BE BIG BE BLUNT BE COUNTED
Now, wishes come in threes.The next generation in clip applier technology has arrived – bringing with it new standards of consistency, reliability, versatility and performance. With its numerous advances in design and functionality, the new Endo Clip III 5mm clip applier enables surgeons to perform clip ligation the way it should be.
Only from Covidien.For more information on the Endo Clip III device, contact your local Covidien Surgical Device Representative, or visit us online at www.covidien.com/autosuture.
+41 (0)44 786 50 50 [tel]+41 (0)44 786 50 10 [fax]
CovidienSwitzerland Limited
Roosstrasse 538832 WollerauSwitzerland
www.covidien.comCOVIDIEN, COVIDIEN with logo, “positive results for life“ and ™ marked brands are trademarks of Covidien AG or its affiliate. © 2008 Covidien AG or its affiliate. All rigths reserved. S-LA-P-ECLIP3/GB - 05/2008
Introducing the Endo Clip™ III 5mm Clip Applier.
BE BIG BE BLUNT BE COUNTED
Now, wishes come in threes.The next generation in clip applier technology has arrived – bringing with it new standards of consistency, reliability, versatility and performance. With its numerous advances in design and functionality, the new Endo Clip III 5mm clip applier enables surgeons to perform clip ligation the way it should be.
Only from Covidien.For more information on the Endo Clip III device, contact your local Covidien Surgical Device Representative, or visit us online at www.covidien.com/autosuture.
COVIDIEN, COVIDIEN with logo, “positive results for life“ and ™ marked brands are trademarks of Covidien AG or its affiliate. © 2008 Covidien AG or its affiliate. All rigths reserved. S-LA-P-ECLIP3/GB - 05/2008
Introducing the Endo Clip™ III 5mm Clip Applier.
BE BIG BE BLUNT BE COUNTED
Now, wishes come in threes.The next generation in clip applier technology has arrived – bringing with it new standards of consistency, reliability, versatility and performance. With its numerous advances in design and functionality, the new Endo Clip III 5mm clip applier enables surgeons to perform clip ligation the way it should be.
Only from Covidien.For more information on the Endo Clip III device, contact your local Covidien Surgical Device Representative, or visit us online at www.covidien.com/autosuture.

�swiss knife 2008; 4
Editorial
ImpressumHerausgeber: Schweizerische Gesellschaft für Chirurgie SGC/SSC, Seltisbergerstrasse 16, CH-4419 Lupsingen, Switzerland, Tel. +41 (0)61 815 96 60, [email protected] in Zusammenarbeit mit Frehner Consulting AG Unternehmensberatung für PR, CH-9014 St. Gallen, Tel. +41 (0)71 272 60 80, [email protected] Produktion und Inseratemarketing: MetroComm AG, Zürcherstrasse 170, CH-9014 St.Gallen, Tel. +41 (0)71 272 80 50, [email protected] Projektverantwortung: Dr. Stephan Ziegler Geschäftsleitung: Natal Schnetzer Fotos: Peter Ruggle, Bodo Rüedi zVg Anzeigen-leitung: Walter Böni Gestaltung: Beatrice Lang swiss knife 2008; 4 (november) ISSN 1661-1381Nachdruck, auch auszugsweise, nur mit Genehmigung der MetroComm AG. Offizielles Publikationsorgan der Schweizerischen Gesellschaft für Chirurgie SGC-SSC. Erscheint viermal jährlich. Geht an alle Mitglieder der Schweizerischen Gesellschaft für Chirurgie SGC-SSC. Abonnementspreis für Nichtmitglieder CHF 36/Jahr.
EditorsPD Dr. Jürg Metzger (Luzern), Senior Editor [email protected]. med. Kuno Lehmann (Zürich), Junior [email protected] Ruhl (Basel), [email protected]
Editorial BoardDr. med. Jean-Jacques Brugger (Neuchâtel) [email protected] Dr. med. Ueli Güller, MHS (Basel/Toronto) [email protected]. med. Adriano Guerra (Bellinzona)[email protected] Dr. med. Michael Heinzelmann (Zürich) [email protected] Dr. med. Vital Schreiber (Aarau)[email protected]. Paul-Martin Sutter (Biel)[email protected]. med. Frédéric Ris (Genève)[email protected] Dr. med. Rachel Rosenthal (SGC-Vorstand)[email protected]. med. Stephan Vorburger (Bern) [email protected]
04 | Information Unterstützungsprojekt der Armee 2. Weiterbildungstag des Forums Junger Chirurgen SGC Der Vorstand der SGC und ihre Gremien 2008-2010
06 | Interview I Othmar Schöb „Die SGC als Sprachrohr, das in der Gesellschaft auf Resonanz stösst“
09 | Interview II Thorsten Carstensen, Urs Studer Businessplan statt Dienstplan
12 | Education I Monika E. Hagen, Oliver J. Wagner, Stephan A. Vorburger, Daniel Candinas, Philippe Morel Robotic-assisted Visceral Surgery: Where is it?
16 | Education II Ueli Güller Meta-Analyses: Advantages and Caveats
18 | Research Surgical Research in Switzerland
Liebe Leserin, lieber Leser
Zu Beginn der zweiten Hälfte des Jahres 2008 hatte ich die grosse Ehre, von Markus Zuber das Amt des „Senior Editors“ dieser Zeitschrift übernehmen zu dürfen. Er hat diese verantwortungsvolle Tätigkeit einerseits durch sei-ne sprichwörtliche, akribische Sorgfalt in Detailfragen und andererseits durch seinen flexiblen und ideenreichen Um-gang mit konzeptionellen Neuerungen äusserst souverän gemeistert.Die erste dieser Eigenschaften ist mir bereits anfangs der neunziger Jahre, während meiner chirurgischen Ausbil-dung an der Universität Basel, vom damaligen Oberarzt Zuber aufs Eindrücklichste eingetrichtert worden. Denn sein legendärer, gelber „Stabilo Boss“-Stift, liess absolut keine Gelegenheit aus, jedes herumliegende Stück Papier mit einem dezidierten Kommentar seines Besitzers zu ver-zieren.In den konzeptionellen Bereich und die übrigen Geheimnisse der „Editorial - Arbeit“ bin ich seit anfangs 2008 von meinem Vorgänger mit viel Geduld und Sachverstand eingeführt worden.Dafür, lieber Markus, danke ich Dir ganz herzlich!Nach der erfolgreichen Startphase dieses Blattes, stehen für einen neu an-tretenden „Senior Editor“ primär keine konzeptionellen Änderungen auf der Tagesordnung. Dies schliesst aber nicht aus, dass die aktuelle Qualität des seit fünf Jahren bestehenden Sprachrohrs der Schweizerischen Chirurgen-gesellschaft auch von den Ideen und Anregungen seiner Leserschaft sowie einer jungen Redaktorenschar aus den verschiedenen Sprachregionen sowie aus den Institutionen innerhalb und ausserhalb der Universität abhängt. Besonders freue ich mich auf die Zusammenarbeit mit dem neuen SGC-Prä-sidenten, Professor Othmar Schöb, der sich in dieser Ausgabe freundlicher-weise für ein Interview zur Verfügung gestellt hat.
Ihr Jürg MetzgerSenior Editor swiss knife
swiss knife – das erfolgreiche Sprachrohr der SGC-Mitglieder
swiss knife, le porte-voix écouté des membres de la SSC
Chère lectrice, cher lecteur,
Au début du deuxième semestre 2008, j’ai eu le grand honneur de remplacer Markus Zuber au poste de «rédac-teur en chef» de ce magazine. Il a souverainement maîtrisé cette tâche lourde de responsabilités, d’une part en met-tant un soin proverbial et méticuleux à traiter les questions de détail et d’autre part en étudiant avec flexibilité et ima-gination les concepts nouveaux. J’avais déjà été extrêmement impressionné par la pre-mière de ces qualités au début des années nonante, pen-dant ma formation de chirurgien à l’université de Bâle, où Markus Zuber était à l’époque médecin-chef. En effet, son légendaire marqueur jaune «Stabilo Boss» ne manquait absolument aucune occasion d’orner le moindre morceau de papier abandonné d’un commentaire pertinent de son propriétaire. Depuis le début de 2008, mon prédécesseur m’a initié,
avec beaucoup de patience et de compétence, aux aspects conceptuels et aux autres secrets du «travail d‘éditorialiste». Pour cela, mon cher Markus, je te remercie de tout mon cœur!Après les débuts réussis de ce magazine, le nouveau «rédacteur en chef» ne voit a priori aucune raison d’inscrire à l’ordre du jour des modifications d’or-dre conceptuel. Mais il faut reconnaître que la qualité dont fait preuve depuis cinq ans le porte-voix de la Société suisse de chirurgie doit aussi beaucoup aux idées et aux suggestions de ses lecteurs, à une foule de jeunes rédac-teurs des différentes régions linguistiques et à des institutions intérieures et extérieures à l’université. Je suis particulièrement heureux de la collaboration avec le nouveau prési-dent de la SSC, le professeur Othmar Schöb, qui s’est aimablement proposé pour une interview que vous pourrez lire dans ce numéro.
Jürg MetzgerRédacteur en chef de swiss knife

4
Information I
swiss knife 2008; 4
(Text gilt sinngemäss auch für Ärztinnen)
Durch die zunehmende Spezialisierung der medizinischen Versorgung ge-hen breite umfassende Allgemeinkenntnisse und Erfahrungen bei den jungen Ärzten verloren. Dies gilt besonders im Bereiche der Kriegs- und Katastro-phenmedizin.
Die Armee bildet keine Ärzte aus. Sie ist jedoch für die Weiter- und Fort-bildung der Militärärzte in den Belangen des Armeesanitätsdienstes zustän-dig. Die besonderen Anforderungen für den militärärztlichen Einsatz werden im Rahmen der Kaderschulen bei der Ausbildung zum Militärarzt (San Of) vermittelt. In Fachdienstkursen (FDK) erfolgt die gezielte Fortbildung einer-seits im Rahmen der Armee, andererseits im Rahmen der Schweizerischen Akademie für Militär- und Katastrophenmedizin (SAMK) entsprechend den Bedürfnissen der Armee.
Für die stationäre medizinische Versorgung der Angehörigen der Armee ba-siert die Armee heute auf den zivilen Spitalorganisationen. Zur Sicherstellung und Erhaltung einer kriegschirurgischen Kompetenz an Schweizerischen Spitälern mit Auftrag zur Traumaversorgung und für allfällige Auslandeinsät-ze im Rahmen der Armee oder des Schweizerischen Katastrophenhilfskorps unterstützt die Armee deshalb die unfall- und katastrophenmedizinische Weiter- und Fortbildung ausgebildeter Chirurgen durch die Finanzierung von Rotationsstellen an universitären Unfallkliniken in der Schweiz. Vorerst sollen jährlich bis maximal 4 Rotationsstellen von 6 Monaten finanziert werden.
Der weiterzubildende Chirurge hat eine feste Anstellung als Oberarzt/Leiten-der Arzt an einem schweizerischen Akutspital mit einem Auftrag zur Trauma-versorgung seiner Region und möglichst eine abgeschlossene Weiterbildung in Chirurgie mit Schwerpunkt Allgemeinchirurgie/Traumatologie oder ortho-pädische Chirurgie und Traumatologie des Bewegungsapparates. Er wird für die Rotationsstelle von seiner Stammklinik freigestellt und kehrt anschlies-send wieder an seine angestammte Stelle zurück.
Die Anstellungsbedingungen für die Rotationsstelle werden zwischen SAMK und Traumazentrum vertraglich geregelt. Der wissenschaftliche Beirat der SAMK beteiligt sich an der Definition des Ausbildungsplanes und begleitet die Ausbildung der Rotationschirurgen nach Bedarf. Die Rotationszeit am Traumazentrum soll (soweit noch notwendig) Anrechnung an eine allfällige Weiterbildung haben.
Das Anforderungsprofil für die Rotationschirurgen wird wie folgt festgelegt:• Facharzt für Chirurgie mit Schwerpunkt Allgemeinchirurgie und Unfallchir-
urgie oder Orthopädische Chirurgie und Traumatologie des Bewegungs-apparates. Ausnahmsweise können auch Kandidaten berücksichtigt werden, die kurz vor Abschluss der entsprechenden Facharztausbildung stehen und am Stammspital bereits in entsprechender Funktion tätig sind.
• Ev. EBSQ-Trauma Certification. (Europ. Board of Surgery Qualification)• Schweizer Bürger; Angehöriger der Armee
Rotationsstellen für die unfall- und katastrophenchirurgische Weiter- und Fortbildung
eines ausgebildeten Chirurgen an einem Traumazentrum:Ein Unterstützungsprojekt der Armee
Schweizerische Akademie für Militär- und Katastrophenmedizin SAMK Arbeitsgruppe Fachzentrum Traumatologie
Adrian Leutenegger, [email protected]
Wenn möglich soll der Rotationschirurg eine militärärztliche Ausbildung und Funktion haben. Angehörige der Armee ohne Offiziersgrad sollen nach Ab-schluss der speziellen Ausbildung befördert und als Fach-Offiziere einge-setzt werden.
Die Finanzierung erfolgt über das Budget der SAMK.
Interessenten für eine solche Rotationsstelle erhalten weitere Auskünf-te beim Dekanat der Schweizerischen Akademie für Militär- und Katas-trophenmedizin SAMK, Sanitätsinspektorat, Worblentalstrasse 36, 3063 Ittigen oder direkt beim Dekan SAMK Prof. Dr. med. A. Leutenegger, Kro-nengasse 9, 7000 Chur ([email protected])
Vorankündigung
2. Weiterbildungstag des Forums Junger Chirurgen SGCThema: „How I do it“praxisbezogene Fortbildung für junge ChirurgenSamstag 18. April 2009 Beginn 9:00 UhrLuzern, Hörsaal des Kantonsspitals LuzernInformationen und Anmeldung via Email: [email protected]
03 07 2008 / J Biaggi
Vorstand 2008 – 2010 Vertretungen in Kommissionen
Kommission Vertreter der SGC E-Mail
Ärztekammer Prof. Othmar Schöb
Dr. Jean Biaggi
FMCH Plenarversammlung Prof. Othmar Schöb
Dr. Jean Biaggi
FMCH Vorstand Dr. Philippe Rheiner [email protected]
KWFB Dr. Brigitte Muff
Prof. Philippe Morel
UEMS Dr. Jean Biaggi
Dr. Brigitte Muff
BJS Prof. Philippe Morel
Prof. Ralph Schmid

Information I
swiss knife 2008; 4
(Le texte a été écrit au masculin, mais il s’applique également aux doctoresses)
En raison de la spécialisation croissante des soins médicaux, les jeunes mé-decins disposent de moins en moins de connaissances générales et d’expé-riences globales. Et ce, tout particulièrement dans le domaine de la médecine de guerre et de catastrophe.
L’armée ne forme pas de médecins. Elle est toutefois responsable de la for-mation continue et du perfectionnement de l’instruction des médecins mili-taires pour le service sanitaire de l’armée. Les exigences particulières pour l’engagement médico-militaire sont transmises au niveau des écoles de ca-dres et de l’instruction pour devenir médecin militaire (of san). Dans les cours de spécialistes (CS), la formation continue visée a lieu d’une part dans le ca-dre de l’armée, d’autre part dans le cadre de l’Académie suisse de médecine militaire et de catastrophe (ASMC) en fonction des besoins de l’armée. Les soins médicaux donnés de manière stationnaire aux militaires reposent sur les organisations hospitalières civiles.
Pour assurer et maintenir un certain niveau de compétences en chirurgie de guerre dans les hôpitaux suisses chargés des soins en traumatologie et pour d’éventuels engagements à l’étranger dans le cadre de l’armée ou du CSA, les chirurgiens traumatologues nécessitent d’avoir la possibilité de suivre un perfectionnement ciblé grâce au financement de postes de rotation au sein d’un centre de formation primaire dans le cadre de l‘Académie suisse de médecine militaire et de catastrophe Afin de pouvoir assurer la formation continue d’un nombre suffisant de chirurgiens traumatologues de langue al-lemande et française pour les différentes cliniques de traumatologie de toute la Suisse, quatre postes de rotation au maximum par année, d’une durée de six mois chacun, seront financés pour le moment.
Il est tout d’abord prévu que les hôpitaux universitaires deviennent des centres de formation primaire. Le chirurgien à perfectionner est engagé de manière fixe en tant que médecin-chef/médecin responsable dans un hôpital suisse pour cas aigus et il est en charge des soins en traumatologie de sa région. Sa clinique de base le libère pour qu’il puisse occuper son poste de rotation et, une fois les six mois écoulés, il retourne à son poste habituel. Le centre de formation en traumatologie obtient dans le cadre des accords contractuels avec l’ASMC un poste médecin chef payé pour l’embauche d’un chirurgien
Création d’un poste de rotation pour le perfectionnement en chirurgie traumatologique et de catastrophe d’un chirurgien diplômé
dans un centre de traumatologie:Un projet de support de l’armée
Académie suisse de médecine militaire et de catastrophe ASMC Groupe de travail du Centre de formation en trau-matologie
Adrian Leutenegger, [email protected]
diplômé avec spécialisation en traumatologie/chirurgie générale ou en chirur-gie orthopédique et traumatologie du système moteur pour une période de perfectionnement limitée dans le temps (poste de rotation).
Le comité consultatif scientifique de l’ASMC prend part à la définition du plan de formation et accompagne, selon les besoins, la formation des chirurgiens en rotation. La période de rotation au centre de traumatologie doit (dans la mesure où cela est encore nécessaire) être imputée à un éventuel perfection-nement. Les certificats seront établis par le centre de traumatologie.
Le profil requis pour les chirurgiens en rotation doit correspondre aux points suivants:• Médecin spécialisé en chirurgie avec spécialisation en chirurgie générale
et chirurgie traumatologique ou en chirurgie orthopédique et traumatologie du système moteur. De manière exceptionnelle, les candidatures de mé-decins étant sur le point de terminer leur formation spécialisée et occupant déjà leur fonction spécialisée dans leur hôpital de base, peuvent aussi être prises en compte.
• Eventuellement certificat en traumatologie EBSQ (Europ. Board of Surgery Qualification)
• Citoyen suisse. Militaire.
Le chirurgien en rotation doit de préférence posséder une formation et une fonction médico-militaires. Les militaires sans grade d’officier doivent être promus après avoir terminé leur formation spécialisée et être engagés en tant qu’of spéc.
Le budget de l’ASMC permet le financement du projet.
Les personnes intéressées pat un tel poste peuvent obtenir des informa-tions détaillées de l’Académie suisse de médecine militaire et de catas-trophe ASMC, Inspectorat des affaires sanitaires, Worblentalstrasse 36, 3063 Ittigen ou directement via le Doyen ASMC le Prof. Dr. med. A. Leu-tenegger, Kronengasse 9, 7000 Chur ([email protected]).
Information II
swiss knife 2008; 4 �
03.07.2008 / J. Biaggi
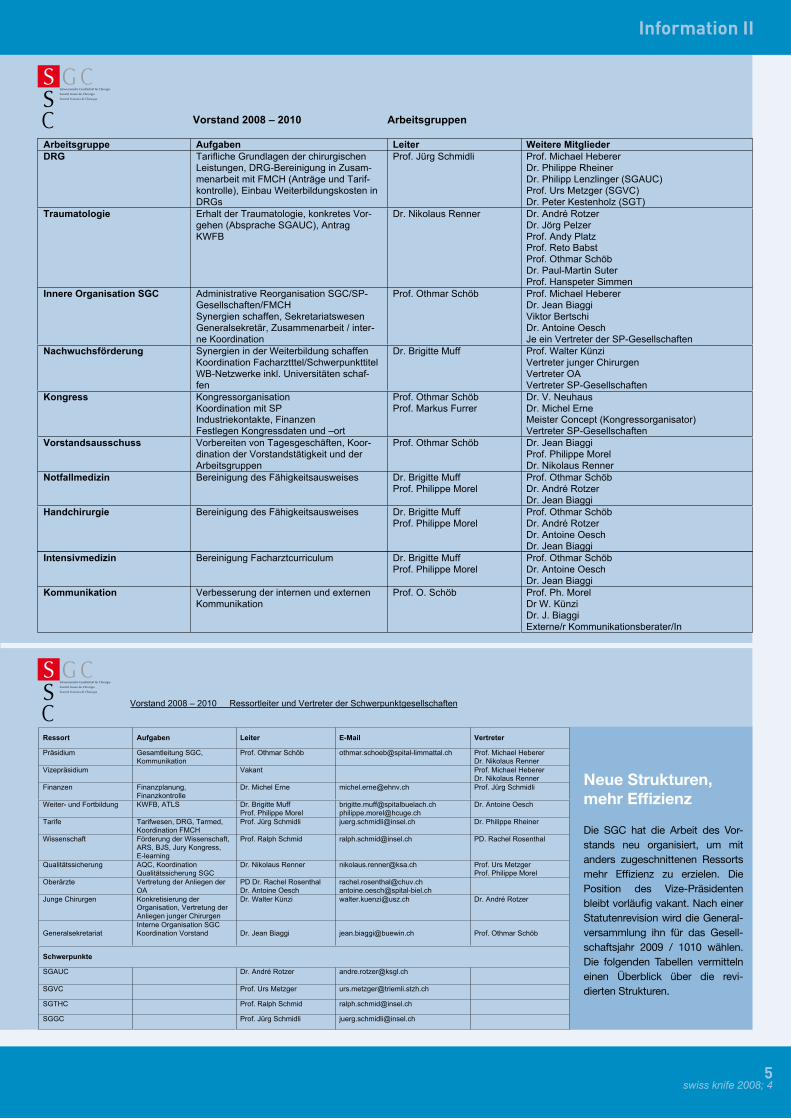
Vorstand 2008 – 2010 Arbeitsgruppen
Arbeitsgruppe Aufgaben Leiter Weitere Mitglieder
DRG Tarifliche Grundlagen der chirurgischenLeistungen, DRG-Bereinigung in Zusam-menarbeit mit FMCH (Anträge und Tarif-kontrolle), Einbau Weiterbildungskosten inDRGs
Prof. Jürg Schmidli Prof. Michael HebererDr. Philippe RheinerDr. Philipp Lenzlinger (SGAUC)Prof. Urs Metzger (SGVC)Dr. Peter Kestenholz (SGT)
Traumatologie Erhalt der Traumatologie, konkretes Vor-gehen (Absprache SGAUC), AntragKWFB
Dr. Nikolaus Renner Dr. André RotzerDr. Jörg PelzerProf. Andy PlatzProf. Reto BabstProf. Othmar SchöbDr. Paul-Martin SuterProf. Hanspeter Simmen
Innere Organisation SGC Administrative Reorganisation SGC/SP-Gesellschaften/FMCHSynergien schaffen, SekretariatswesenGeneralsekretär, Zusammenarbeit / inter-ne Koordination
Prof. Othmar Schöb Prof. Michael HebererDr. Jean BiaggiViktor BertschiDr. Antoine OeschJe ein Vertreter der SP-Gesellschaften
Nachwuchsförderung Synergien in der Weiterbildung schaffenKoordination Facharztttel/SchwerpunkttitelWB-Netzwerke inkl. Universitäten schaf-fen
Dr. Brigitte Muff Prof. Walter KünziVertreter junger ChirurgenVertreter OAVertreter SP-Gesellschaften
Kongress KongressorganisationKoordination mit SPIndustriekontakte, FinanzenFestlegen Kongressdaten und –ort
Prof. Othmar SchöbProf. Markus Furrer
Dr. V. NeuhausDr. Michel ErneMeister Concept (Kongressorganisator)Vertreter SP-Gesellschaften
Vorstandsausschuss Vorbereiten von Tagesgeschäften, Koor-dination der Vorstandstätigkeit und derArbeitsgruppen
Prof. Othmar Schöb Dr. Jean BiaggiProf. Philippe MorelDr. Nikolaus Renner
Notfallmedizin Bereinigung des Fähigkeitsausweises Dr. Brigitte MuffProf. Philippe Morel
Prof. Othmar SchöbDr. André RotzerDr. Jean Biaggi
Handchirurgie Bereinigung des Fähigkeitsausweises Dr. Brigitte MuffProf. Philippe Morel
Prof. Othmar SchöbDr. André RotzerDr. Antoine OeschDr. Jean Biaggi
03.07.2008 / J. Biaggi
Intensivmedizin Bereinigung Facharztcurriculum Dr. Brigitte MuffProf. Philippe Morel
Prof. Othmar SchöbDr. Antoine OeschDr. Jean Biaggi
Kommunikation Verbesserung der internen und externenKommunikation
Prof. O. Schöb Prof. Ph. MorelDr W. KünziDr. J. BiaggiExterne/r Kommunikationsberater/In
03.07.2008 / J. Biaggi / 06.11.2008
Vorstand 2008 – 2010 Ressortleiter und Vertreter der Schwerpunktgesellschaften
Ressort Aufgaben Leiter E-Mail Vertreter
Präsidium Gesamtleitung SGC,Kommunikation
Prof. Othmar Schöb [email protected] Prof. Michael HebererDr. Nikolaus Renner
Vizepräsidium Vakant Prof. Michael HebererDr. Nikolaus Renner
Finanzen Finanzplanung,Finanzkontrolle
Dr. Michel Erne [email protected] Prof. Jürg Schmidli
Weiter- und Fortbildung KWFB, ATLS Dr. Brigitte MuffProf. Philippe Morel
[email protected]@hcuge.ch
Dr. Antoine Oesch
Tarife Tarifwesen, DRG, Tarmed,Koordination FMCH
Prof. Jürg Schmidli [email protected] Dr. Philippe Rheiner
Wissenschaft Förderung der Wissenschaft,ARS, BJS, Jury Kongress,E-learning
Prof. Ralph Schmid [email protected] PD. Rachel Rosenthal
Qualitätssicherung AQC, KoordinationQualitätssicherung SGC
Dr. Nikolaus Renner [email protected] Prof. Urs MetzgerProf. Philippe Morel
Oberärzte Vertretung der Anliegen derOA
PD Dr. Rachel RosenthalDr. Antoine Oesch
[email protected]@spital-biel.ch
Junge Chirurgen Konkretisierung derOrganisation, Vertretung derAnliegen junger Chirurgen
Dr. Walter Künzi [email protected] Dr. André Rotzer
GeneralsekretariatInterne Organisation SGCKoordination Vorstand Dr. Jean Biaggi [email protected] Prof. Othmar Schöb
Schwerpunkte
SGAUC Dr. André Rotzer [email protected]
SGVC Prof. Urs Metzger [email protected]
SGTHC Prof. Ralph Schmid [email protected]
SGGC Prof. Jürg Schmidli [email protected]
Neue Strukturen, mehr Effizienz
Die SGC hat die Arbeit des Vor-stands neu organisiert, um mit anders zugeschnittenen Ressorts mehr Effizienz zu erzielen. Die Position des Vize-Präsidenten bleibt vorläufig vakant. Nach einer Statutenrevision wird die General-versammlung ihn für das Gesell-schaftsjahr 2009 / 1010 wählen. Die folgenden Tabellen vermitteln einen Überblick über die revi-dierten Strukturen.

6
Interview I
swiss knife 2008; 4
„Die SGC muss das Sprachrohr der Chirurgen sein, das in der Gesellschaft auf Resonanz stösst“
Othmar Schöb, der neue Präsident der SGC, nimmt Stellung zu aktuellen Auseinandersetzungen, formuliert Sor-gen und Problemfelder und möchte die Rolle der SGC als politische Interessenvertretung stärken. Die Fragen stell-ten Jürg Metzger und Felix Ruhl.
Was sind die dringlichsten standespolitischen Herausforderungen und wie sollte die SGC darauf reagieren?Herausfordernd für die SGC ist zum einen die zukünftige Vertretung und Einbettung der Traumatologie innerhalb der Chirurgie und die Klärung des Verhältnisses zur Schweizerischen Gesellschaft für Orthopädie in dieser Angelegenheit. Weiter muss das Verhältnis zwischen der SGC und ihren Schwerpunktgesellschaften zwecks Verhinderung von Doppelspurigkeiten und der Schaffung effizienterer Strukturen genau definiert werden.
Die grösste externe Herausforderung ist die bevorstehende Einführung von DRG-Fallpauschalen. Wir verstehen es als unseren Auftrag, zunächst eine adäquate Abgeltung und Abbildung der ärztlichen Leistungen durchzusetzen und zusätzlich die Frage der Vergütung der Aus- und Weiterbildungskosten zu klären.
In welchem Entwicklungsstadium befindet sich die SGC im Moment?Die SGC ist eine bedeutende Fachgesellschaft. Wir laufen aktuell Gefahr, dass das, was die SGC ausmacht, aufgrund der immer weiter gehenden Spezialisierungen irgendwann nicht mehr existiert. Es ist einerseits wichtig, dass Entwicklung und Emanzipation von Subspezialitäten gefördert und zugelassen werden. Anderseits ist es aber auch notwendig, den Rahmen, in welchem diese stattfinden, zu definieren und als Muttergesellschaft Leit-planken zu bilden, die für alle Spezialisten innerhalb der Chirurgie Gültigkeit haben und somit strukturell so aufgestellt zu sein, dass sich alle “heimisch“ fühlen.
Aus diesem Grund müssen wir diejenigen Elemente, mit denen wir alle Mit-glieder erreichen, besonders pflegen, für aktiven Erfahrungsaustausch sor-gen und uns um diejenigen Fragen kümmern, die für alle bedeutsam sind. Es sind dies die Nachwuchsförderung und Weiterbildung, die Tarifpolitik, die Qualitätssicherung und das stetige Bemühen um eine einheitliche standes-politische Vertretung.
Welche Ziele haben Sie sich persönlich für Ihre Amtszeit gesetzt?Mir ist es ein besonderes Anliegen, die Existenz der Traumatologie in der SGC langfristig zu sichern. Ausserdem wünsche ich Strukturen für die Wei-terbildung, welche die Kandidaten frühzeitig wissen lassen, welche Schritte sie wann unternehmen müssen um ihre Ziele rasch zu erreichen.
Generell möchte ich einen Beitrag dazu leisten, dass die SGC in der Bevölke-rung stärker wahrgenommen wird. Gelingt uns dies, entsteht die Möglichkeit, unsere Interessen und Sorgen in der Öffentlichkeit und gegenüber den Medi-en plausibel darzulegen. Die SGC muss das Sprachrohr der Chirurgen sein, das in der Gesellschaft auf Resonanz stösst.
Wie ist es um den chirurgischen Nachwuchs bestellt?Chirurg zu sein, gilt im Moment als nicht allzu attraktiv. Zum Teil ist dies ein hausgemachtes Problem, weil Unsicherheiten im Curriculum bestehen. Un-abhängig davon ist die Tätigkeit der Chirurgen aber mit einem hohem Ar-beitsethos und einem enormen und lebenslangen Engagement verbunden. Sind wir ehrlich, das scheint heute nicht mehr so gefragt zu sein. Um diesem Trend entgegenzuwirken, müssen wir alles unternehmen, die fachliche und finanzielle Attraktivität unseres Berufs zu erhöhen und den Nachwuchs ge-zielt zu fördern, wie dies mein Vorgänger mit dem Aufbau des Forums Junge Chirurgen bereits begonnen hat.
Ich kann nicht verbergen, dass sich die verändernden politischen und ökono-mischen Rahmenbedingungen negativ auf unsere Arbeit auswirken könnten. Operationen müssen schneller und rentabler erfolgen, so dass weniger Gele-genheit zum Teaching bleibt. Eine fundierte chirurgische Ausbildung erfordert aber viel Zeit und praktisches Handeln. Der Nachwuchs muss deshalb ehr-lich darüber informiert werden, dass die angestrebte Verbesserung der Wei-terbildungsstruktur allein nicht genügt. Das Erreichen des High-End-Stadi-ums in der Chirurgie erfordert zusätzliche Bereitschaft und auch Fähigkeiten. Dies muss der heutige Nachwuchs zu Kenntnis nehmen und die Politik und die Gesellschaft sollten dies auch erfahren, damit sie es fördern (und nicht dauernd behindern) und letztlich auch honorieren können.
Was halten Sie von der steigenden Anzahl von festangestellten Spital-ärzten auf unseren Abteilungen?Der Gedanke, auf den Abteilungen stets einen ärztlichen Ansprechpartner zu haben, ist gut, denn die Chirurgen sind nun einmal notgedrungen häufig un-abkömmlich. In der Praxis haben wir mit dieser Einrichtung gute wie negative Erfahrungen gemacht. Kandidaten, die sich um die Stelle von Spitalärzten bewerben, stehen häufig vor dem Sprung in eine eigene Praxis oder beab-sichtigen einen Wechsel in ihrer Karriere, so dass die Fluktuation gross ist.
Othmar Schöb Jürg Metzger Felix Ruhl

Interview I
swiss knife 2008; 4 �
Ich glaube, wir müssten, um eine gute Idee zu retten, das Berufsfeld mit gezielten Investitionen aufwerten. Ein Spitalarzt muss klare Kompetenzen besitzen und angemessen bezahlt werden, damit es für ihn interessant ist, sich langfristig zu binden.
Welche Auswirkungen werden die Swiss DRG auf unsere tägliche Arbeit haben?Die Auswirkungen sind schwer vorherzusagen, denn das System der Swiss DRG ist noch nicht abschliessend definiert. Es ist noch nicht klar, ob es even-tuell kantonal unterschiedliche DRGs geben wird, ob die Fallpauschalen für alle Spitäler, also auch die Universitätsspitäler, gelten sollen und vor allem, inwiefern die ärztlichen Leistungen erkennbar sein werden.
Die SGC macht ihren Einfluss geltend, um zu gewährleisten, dass der ärzt-lichen Weiterbildung mit einem relevanten Prozentsatz Rechnung getragen wird – und zwar nicht nur an den Universitäten. Wir fordern ausserdem, dass schwere Risiken geregelt sein müssen. Der grösste Fehler bei der aktuellen Konzeption besteht darin, dass Fallpauschalen nur für die stationär erbrach-ten Leistungen gelten sollen (fehlender Anreiz für den längst fälligen Schritt, mehr chirurgische Leistungen ambulant anzubieten). Glücklicherweise sind wir in den Konstituierungsprozess der Swiss DRG involviert. Gelingt es uns,
die Swiss DRG zu korrigieren, habe ich mit Fallpauschalen kein Problem. Ich finde die Idee, dass hinter einer Leistung eine Pauschalisierung steht, nicht grundsätzlich falsch und halte es für gut möglich, dass positive ökonomische Effekte resultieren. Fallpauschalen dürfen aber nicht auf Kosten schwer kran-ker Menschen gehen.
Wie wird sich der „Machtkampf“ zwischen Traumatologen und Orthopä-den entwickeln? Stirbt der Allgemeinchirurg aus - wird er gemäss deut-schem Modell durch einen „allgemeinen“ Viszeralchirurgen ersetzt?In der Deutschschweiz ist die Traumatologie ein wichtiger Bestandteil der Chirurgie. Aus diesem Grund muss die reale Arbeit eines Chirurgen im Ti-tel sichtbar sein, denn unsere allgemein und traumatologisch tätigen Chir-urgen sind in der Notfallversorgung des Traumapatienten – das dürfen wir in aller Bescheidenheit sagen – mindestens so fundiert ausgebildet wie die Orthopäden. Wir versuchen diese Unschärfe in der Titelstruktur (Name des Schwerpunktes Allgemein- und Unfallchirurgie) aktuell auszumerzen, indem der Begriff “Traumatologie des Bewegungsapparates“ dort zu erkennen sein wird. Weiter glaube ich, ist es dringend und wichtig für unseren Nachwuchs einen Schulterschluss mit den Orthopäden anzustreben, um mittelfristig zu einer gemeinsamen (auch landesweiten) Lösung zu kommen. Am nächsten Chirurgenkongress wird dieses Anliegen übrigens ein Hauptthema sein.

8
Interview I
swiss knife 2008; 4
Sind Sie für eine Zentralisierung von „high risk“-Eingriffen (Leber, Pank-reas, Oesophagus) und wenn ja, auf welcher Stufe: nur noch in den Uni-versitäten respektive Kantonsspitälern oder rein nach Fallzahlen?Unbestritten ist, dass für komplexe Operationen ein erfahrener Spezialist von Vorteil ist. Ob ein sehr erfahrener Spezialist, der sich nur noch mit einem be-grenzten Gebiet (ein Organ, resp. eine Organregion) beschäftigt, wesentlich besser ist als ein sehr aktiver breit tätiger Operateur, weiss ich effektiv nicht und es ist für schweizerische Verhältnisse auch nicht beweisbar. Ein hoher Caseload muss nicht zwingend an ein Organ respektive an eine Organregion gebunden sein, sondern der Caseload an komplexen Eingriffen insgesamt ist möglicherweise ähnlich zu gewichten.
Ich möchte meinen Standpunkt dahingehend zusammenfassen: Lasst uns die Chirurgie nicht überregulieren. Ich empfehle besonders, dass niemand aus der Chirurgenfamilie etwas in die Medien transportiert, das für uns hier in der Schweiz keine eindeutige Gültigkeit hat. Dies ist die wirkliche Gefahr. Dies führt zur Zerreisprobe und lässt uns uneinheitlich erscheinen.
Mit welchen Problemen wird die Schweizer Chirurgie in absehbarer Zu-kunft konfrontiert sein?Ich sehe eine Gefahr für den Nachwuchs. Es droht ein echter Mangel. Zusätz-lich scheint sich abzuzeichnen, dass Chefärzte mit einem breiten Spektrum, mit der heutigen Bereitschaft aktive Weiterbildner zu sein, mit Führungsquali-täten und umfassenden weiteren match-entscheidenden Fähigkeiten schwer zu finden sein werden. Kommen diese beiden Punkte zusammen, bekom-men wir in der Schweiz ein Versorgungsproblem. Der Beruf Chirurg muss vor allen die Attraktivität bedrohenden Einflüssen gezielt geschützt werden – das ist eine politische Forderung.
Wie bringen Sie Familie, die Tätigkeit als Chefarzt und die neue zeitauf-wendige Funktion als SGC-Präsident unter einen Hut?Das funktioniert natürlich nur mit sehr viel Arbeit und einem sehr gut organi-siertem Umfeld. In meiner Klinik sind alle Aufgaben gut verteilt. In der Familie leiste ich meinen Beitrag, weiss aber und bin dafür dankbar, dass meine Frau in der Hauptrolle Grossartiges leistet.
Was erwarten Sie vom „swiss knife“?Swiss knife ist ein attraktives Organ mit interessanten Beiträgen. Es ist vor allem eines, das gelesen wird, was ja nicht all den Papieren passiert, mit de-nen wir überschwemmt werden. Ich finde, die Redaktion antizipiert interes-sante Probleme und Fragestellungen sehr gut. Ich wünsche mir, dass dies so bleibt und dass swiss knife auch noch einer anderen Leserschaft (am liebsten einer politischen) zugeführt wird und es sich so zu einem standespolitischen Sprachrohr entwickeln und Resonanz in den Medien erzeugen könnte.
PersönlichOthmar Schöb ist Facharzt für Chirurgie, speziell Viszeral- und Thorax-chirurgie und Titularprofessor der Universität Zürich. Seine Habilitation zum Thema minimal-invasive Chirurgie reichte er 1995 ein.In seiner Zeit am Universitätsspital Zürich war er aktives Mitglied des Transplantationsteams. Früh entwickelte er standespolitisches Interesse, und früh – im Alter von 36 Jahren – trat er die Stelle als Chefarzt am Spital Limmattal an. Othmar Schöb ist verheiratet, hat vier Kinder und lebt in Urdorf.
Stationen der Weiterbildung:* Assistenzarzt in Wetzikon, Baden und am Universitätsspital Zürich (1988-1994)* 1994/95 Clinical and Research-Fellow an der University of New Mexico unter Karl A. Zucker* Oberarzt Viszeralchirurgie am Universitätsspital Zürich (1995-1998)* Chefarzt am Spital Limmattal (seit 1999)* Titularprofessur an der medizinischen Fakultät Zürich (seit 2004)* Ärztlicher Direktor (seit 2005) des Gesundheitszentrums Zürich West* Mitglied im Editorial Board von Surgical Laparoscopy and Endoscopy und der Zeitschrift Minimal invasive Chirurgie
Standespolitische Gremien• 1999-2006 Leiter der AQC (Arbeitsgemeinschaft für Qualitätssicherung in der Chirurgie)• seit 1999 Vorstandsmitglied und Vizepräsident (2004-2008) der Chefärztegesellschaft des Kantons Zürich• 2002 bis heute Vorstand der SGC• 2004 bis 2008 Vorstandsmitglied der fmCh
Interview II
swiss knife 2008; 4 9
Businessplan statt Dienstplan
Welche Veränderungen eine Niederlassung für den Chirurgen mit sich bringen
Viele Mitglieder der SGC sind in einer Praxis niedergelassen und nicht mehr an einem öffentlichen Spital angestellt. Der Entscheid zur selbst-ständigen Tätigkeit stellt im chirurgischen Berufsleben einen markanten Schritt dar. In den letzten Jahren haben sich die Rahmenbedingungen stark geändert. Zulassungsstopp, Schwerpunkttitel, Interdisziplinarität, neues Tarifwesen und Anstellungen an Privatspitälern sind nur einige Beispiele dafür. Um einen Einblick in die Erfahrungen mit einer Nieder-lassung im heutigen Umfeld zu erlangen, haben wir zwei Chirurgen be-fragt, welche in den letzten zwanzig Monaten ihre Praxis eröffnet haben. Die Fragen stellte Vital Schreiber*.
* Redaktionsmitglied swiss knife; Oberarzt Chirurgie Kantonsspital Aarau
Was hat Sie zum Ergreifen der selbstständigen ärztlichen Tätigkeit be-wogen?Thorsten Carstensen: Die Selbstständigkeit als solche reizte mich als Her-ausforderung. Beruflich und privat war der Zeitpunkt günstig.
Urs Studer: Ich kann nicht einen einzelnen Grund nennen. Es war eine Viel-zahl von Gründen ausschlaggebend, eine Art Bilanz oder ein Abwägen, aus dem heraus ich dann meine Entscheidung getroffen habe.
Welche Kriterien führten zu Ihrer Standortwahl?T.C: Es war purer Zufall, der Praxisinhaber hat auf ein Inserat reagiert, somit hat sich die Möglichkeit einer Praxisübernahme erst ergeben.
U.S: Aus familiären Gründen wollte ich mich in meiner bisherigen Wohn-region niederlassen. Persönlich war mir ein ländliches (Patienten-)Umfeld wichtig. Die Region bietet zudem die Möglichkeit zur Belegarzttätigkeit. Eine Bedarfsabklärung / Standortanalyse zeigte, dass die Neueröffnung einer chirurgischen Praxis hier möglich ist.
Wie und wie schnell kamen Sie zur kantonalen Berufsausübungsbewil-ligung? T.C: Ich konnte eine bereits etablierte chirurgische Praxis von meinem Vor-gänger übernehmen. Die Berufsausübungsbewilligung wurde innerhalb einer Woche ausgestellt.
U.S: Diese habe ich beantragt und nach rund drei Monaten zugesprochen er-halten, da die Region als unterversorgt beurteilt wurde. Durch das Verfahren entstand keine Verzögerung.
Wie hat sich die Finanzierungshilfe gestaltet? Wie lange dauerte es bis zur Wiedererlangung eines ähnlichen Lohnes wie bei der letzten Anstel-lung?
T.C: Ein Budgetplan muss erstellt werden, professionelle und vertrauenswür-dige Unterstützung ist unabdingbar.
U.S: Die Finanzierung konnte durch Bankkredite gesichert werden, auf der Basis eines professionell erstellten Businessplans. Im ersten Praxisjahr konn-te ich die Höhe des letzten Lohnes noch nicht erreichen, im zweiten klappt es möglicherweise. Der Jahresabschluss liegt aber noch nicht vor.
Konnten Sie mit den von Ihnen gewünschten Privatkliniken problemlos Verträge aushandeln? Half eine Subspezialisierung Ihrerseits bei der Vertragsfindung?T.C: Verträge wurden keine ausgehandelt, ich habe mich um die Zulassung als Belegarzt bemüht. Auf die Akkreditierungsanträge ist mit unterschied-lichem Interesse reagiert worden. Die Zulassung ist primär temporär, meist ein Jahr. Teilweise nimmt das Auswahlverfahren viel Zeit in Anspruch. Die Subspezialisierungen als Viszeralchirurg und Koloproktologe sind für die Ak-kreditierung auch an öffentlichen Spitälern nützlich. Die Vertragskonditionen sind primär vorgegeben, bzw. verhandelbar, wenn ein absolutes Nischenpro-dukt angeboten werden kann.
U.S: Ich konnte mich als Belegarzt in einem relativ kurzen und einfachen Verfahren an zwei Privatkliniken akkreditieren lassen. Der Schwerpunkttitel spielte dabei kaum eine Rolle.
Würden Sie bei einem Einstieg in ein Privatspitalnetz eine Belegarzttä-tigkeit oder eine Anstellung empfehlen?T.C: Ich rate ohne Zweifel zu einer Belegarzttätigkeit.
U.S: Bei einer Belegarzttätigkeit bleibt man unabhängig, man trägt auf der anderen Seite aber das gesamte unternehmerische Risiko. Ich glaube, dass diese Unabhängigkeit bei der unsicheren Entwicklung in unserem Gesund-heitswesen noch ein relativ sicherer Wert ist.
Erachten Sie den Anschluss an eine 24h-Notfallstation als notwendig?T.C: Aus meiner beruflichen Situation heraus: Ja.
U.S: Für meine operierten Patienten betreibe ich selber den 24h-Notfall-dienst. Eine Notfallstation kann nützlich sein, beim Auftreten von Komplikati-onen oder für die Anwerbung der Patienten. Unabdingbar ist sie aber sicher nicht.
Wie wurden Sie von den Kollegen (facheigen und fachfremd) lokal und in den Kliniken aufgenommen?T.C: Ich durfte sehr gemischte Erfahrungen gewinnen.
Name, Vorname: Carstensen ThorstenStaatsexamensjahr: 1995Facharzt FMH seit: 2002Zeitpunkt der Praxiseröffnung: Mai 2008Kanton der Niederlassung: St.Gallen
Name, Vorname: Studer UrsStaatsexamensjahr: 1989Facharzt FMH seit: 2000Zeitpunkt der Praxiseröffnung: Feb. 2007Kanton der Niederlassung: Aargau
ERBEJET® 2 – DIE NEUE DIMENSION DER WASSERSTRAHL-CHIRURGIE.
ERBEJET 2 ist leicht und handlich, modular und ausbaufähig. Und schafft Platz im OP. Entweder als Einzelgerät auf Decken versorgungseinheit oder integriert und kombiniert mit ERBE VIO-HF-Chirurgiesystem.
ERBEJET 2
integriert im
VIO-System;
mit eigener
Bedien-
oberfl äche.
Perfektion, die dem Menschen dient
Die Anwendungsvorteile ...
Präzises und sicheres Dissezieren und Präparieren von Gewebe
Maximale Schonung von Blutgefäßen und Nerven
Besseres Blutungsmanagement
Gute Sicht auf das OP-Feld
Für offene und laparoskopische Chirurgie
... z.B. in folgenden Disziplinen:
Chirurgie z.B. Leberresektion, TME
Urologie z.B. nerverhaltende Prostatektomie
Neurochirurgie, Tumorresektion
Gastroenterologie
Fordern Sie weitere Info an:
ERBE SWISS AG Fröschenweidstrasse 10 · CH-8404 WinterthurTelefon 052/2333727 · Fax 052/2333301 [email protected] · www.erbe-swiss.ch
Separierte Blutgefäße
im Leberparenchym.
Wer informiert, überzeugt.
goinggoingpublicDen Gang an die Börse können wir keinem Unternehmen
abnehmen. Den Schritt in die Öffentlichkeit hingegen
schon. Wir entwickeln für Sie massgeschneiderte
Magazine für Ihre Kundinnen und Kunden oder für ein
breites Publikum. Und wir bieten Ihnen ein äusserst inter-
essantes Finanzierungsmodell an. Damit Ihr Going-public
gelingt. Denn Ihre Leistungen verdienen es, erfolgreich
kommuniziert zu werden. Kontaktieren Sie uns, es lohnt
sich: Telefon +41 (0)71 272 60 80 oder
Internet www.frehner-consulting.com.
Frehner Consulting AGUnternehmensberatung für Public Relations
St. Gallen • Genf • Bern
Interview II
11swiss knife 2008; 4
U.S: So heterogen unser Kollegium ist, so unterschiedlich waren auch die Reaktionen: Ich habe viele neue Kontakte geknüpft und sehr gute Unter-stützung in fachlichen, organisatorischen und persönlichen Angelegenheiten erhalten. Andererseits ist man gelegentlich auch mit dem Futterneid von Kol-legen konfrontiert.
Wie wurden Sie durch die Fachgesellschaft und / oder die kantonale Ärztegesellschaft beim Praxis-Start unterstützt?T.C: Ich bin weder über Angebote der Fachgesellschaft noch der kantonalen Ärztegesellschaft orientiert. Es gibt diverse Praxis - Start - Seminare, eine frühe Teilnahme ist zur groben Orientierung sinnvoll. Im Rahmen des An-trages auf eine Mitgliedschaft ist mir ein Angebot eines Treuhänders zuge-stellt worden.
U.S: Einerseits basiert die Vergabe der Zulassungsbewilligung auf der Beur-teilung der Versorgungslage durch die kantonale Fachgruppe und durch die Bezirksärztegesellschaft und andererseits sind die regelmässigen Anlässe der Bezirksärztegesellschaft eine gute Plattform, um sich persönlich vorzu-stellen, sich bekannt zu machen und Kontakte zu pflegen.
Wie haben Sie den Kontakt zu den Zuweisern hergestellt? Konnten Sie dadurch die Anzahl Zuweisungen erhöhen?T.C: Meine Kontakte entstanden durch persönliche Vorstellung, Informati-onsschreiben (Flyer), Zeitungsinserate, Internetauftritt (Homepage) und Fort-bildungen.
U.S: Wie erwähnt über die Bezirksärztegesellschaft und dann durch persön-liche Kontaktnahme. Die Kontaktpflege ist der eigentliche Schlüssel zu den Zuweisungen.
Beteiligen Sie sich am allgemein-medizinischen Notfallarztdienst? Falls ja: Warum und wie häufig?T.C: Eine aktive Teilnahme am lokalen Notfalldienst wird gewünscht, um u.a. die Kollegen zu entlasten. In unserer Region steht ausserdem ein Genera-tionswechsel bevor, d.h. einige Kollegen werden altersbedingt (ab 60) vom Notfalldienst befreit. Für mich ist es ausserdem zum Praxisstart sehr geeig-net, Patienten und ihre behandelnden Hausärzte kennen zu lernen. Zurzeit leiste ich 1-3x monatlich Notfallarztdienst.
U.S: Ja, generell ist dies obligatorisch und mit der Zulassungsbewilligung verknüpft. Es sind 1-2 Dienste pro Monat zu leisten. Es ist möglich, sich vom Notfalldienst frei zu kaufen, was ich bisher aus finanziellen und aus Gründen der Solidarität nicht gemacht habe.
Konnten Sie, falls Sie eine Praxis übernommen haben, von dem Patien-tenstamm profitieren?T.C: Ja, durchaus.
U.S: (Anmerkung der Redaktion: Urs Studer hat eine neue Praxis gegrün-det.)
Hat sich Ihre fachliche Subspezialisierung (welche?) positiv auf die bis-herigen Zuweisungen ausgewirkt?T.C: Die koloproktologische Subspezialisierung war von Nutzen, die viszeral-chirurgische kann ich noch nicht definitiv beurteilen.
U.S: Nein, bisher nicht.
Welche Zusatzausbildungen zum Facharzt für Chirurgie FMH betrach-ten Sie als empfehlenswert?T.C: Eine Schwerpunktausbildung ist sicher empfehlenswert für eine spätere Praxistätigkeit. Orientierend und hilfreich sind auch die diversen angebote-nen Praxisseminare.
U.S: Vielleicht den Fähigkeitsausweis in Marketing, Gesundheitspolitik und Tarifwesen.
Hatte die Aufnahme der Praxis-Tätigkeit einen Einfluss auf Ihre operative Tätigkeit? Wie beurteilen Sie eine allfällig stattgefundene Änderung?T.C: Ja, in der Frequenz operiere ich bisher deutlich weniger, auch die grös-seren (viszeralchirurgischen) Eingriffe fehlen noch.
U.S: Auf jeden Fall. Das Spektrum der Operationen verlagert sich auf die Chirurgie des Häufigen. Die Gesamtzahl der Eingriffe nimmt zu, mit einer Verschiebung zu den kleineren Eingriffen. Die ganz kleinen Eingriffe werden wieder wichtiger.
Haben Sie einen eigenen Operationssaal (welcher Kategorie) in Ihrer Praxis? Wenn ja: Können Sie diesen zeitlich und finanziell auslasten?T.C: Ich verfüge über einen Operationssaal der Kategorie II; voll ausgelastet ist dieser noch nicht.
U.S: Ja. Ich habe in meiner Praxis einen OP I realisiert. Ich bin der Auffas-sung, dass die ambulante Chirurgie in der Arztpraxis weiter zunehmen wird und habe die Erfahrung gemacht, dass die Patienten dies sehr schätzen. Im Moment bin ich dabei, meine eigene ambulante operative Tätigkeit auszu-bauen. Mittelfristig kann ich mir vorstellen, den OP auch anderen Kollegen zur Verfügung zu stellen.
Inwiefern hat sich Ihre Arbeitszeit gegenüber Ihrer letzen Anstellung geändert? T.C: Charakteristisch ist eine hohe Präsenzzeit (auf Abruf), um eine gute Er-reichbarkeit für Hausärzte und Patienten gewährleisten zu können. Flexiblere Arbeitszeiten sind möglich. Die Anzahl der (Wochenend-)Dienste ist deutlich gesunken.
U.S: Insofern, dass ich keine Arbeitszeiterhebung mehr durchführe. Die Ar-beitszeit richtet sich nach dem Patientenanfall, dabei gibt es in der Aufbau-phase grosse Schwankungen.
Nennen Sie bitte für jüngere Kollegen die drei wichtigsten Bedingungen, welche erfüllt sein sollten, damit ein Kollege heute eine privatärztliche Tätigkeit aufnehmen kann und Ihre drei wichtigsten Empfehlungen für diesen Schritt:T. C: – fundierte allgemeinchirurgische Ausbildung mit ausreichend Berufs- erfahrung und möglicher Subspezialität – Aufbau eines Netzwerkes, idealerweise vor der Niederlassung – Der finanzielle Rahmen muss stimmen.
U. S.: Ich habe noch nicht die Erfahrung, jüngeren Kollegen Ratschläge zu erteilen. Vielleicht aber dies: Prüfe den Standort für deine Praxiseröffnung gut. Investiere mit Mass und bleibe sparsam, unsere Tarife sind es auch. Behandle deine Patienten gut und sorgfältig.

12swiss knife 2008; 4
Education I
Robotic-assisted Visceral Surgery: Where is it?
The robot overcomes the technical limitations of laparoscopy by restoring the feel of open surgery in a minimal invasive environment.
Monika E. Hagen, [email protected] J. Wagner, [email protected] A. Vorburger, [email protected] Candinas, [email protected] Morel, [email protected]
Within the past decades, modern surgery has anticipated the concepts of evidence-based medicine. Also, within this development, initial post-operative course and pain has been adopted as important factors of the surgical outcome. Minimal invasive surgery demonstrated its su-periority concerning the early postoperative course when compared to traditional open surgery1-3. Still, minimal invasive surgery has not been overwhelmingly adopted and remains the less used method especially for advanced surgery in the US and Europe in all surgical fields4-6! But why has the majority of surgeons not yet incorporated this patient-wise advantageous method of laparoscopy when evidence-based medicine support their use?
Laparoscopy is difficult to learn and to perform7! Novices to the field of mi-nimal invasive surgery face a significant learning curve. Many advanced procedures contain a level of difficulty even beyond the possibilities of tra-ditional laparoscopic surgery mainly because of the technical limitations of laparoscopy: Two-dimensional imaging leads to impaired depth perception and disorientation. Laparoscopic rigid instrumentation offers a limited range of motion and fewer degrees of freedom when compared to the surgeon’s hand. Fixed trocars act as a fulcrum and lead to motion reversal and motion scaling of the tip of the laparoscopic instrument. Due to the length of lapa-roscopic instruments, the surgeon’s resting tremor is enhanced. Frequently, the surgeon is forced to perform in an uncomfortable and inefficient position and instruments, monitors and surgeon are misaligned.
But how can we overcome these technical limitations to provide secure mini-mal invasive surgery to benefit the patient’s outcome? The solution has been developed over the past decades: Robotic surgery7,8!
History of robotic surgeryDevelopment of Robotic surgery started in the late 70ies and early 80ies and was mainly driven by two US institutions: The army and the NASA. The original motivator was to perform tele-surgery on patients in remote places such as a battle-field or the outer space. Both projects were more or less equally successful and lead to the development of two different robotic systems: the da Vinci® Surgical System (US army in cooperation with the Stanford Research Institute) and the Zeus robot (NASA). Both projects were commercialized, the da Vinci® Surgical System by Intuitive and the Zeus ro-bot by Computer Motion, and received the FDA approval for laparoscopic abdominal surgery in the years 2000 and 2001, respectively. Even before
FDA approval, a first robotic cholecystectomy was performed on a patient in Belgium with “Mona”, the preliminary version of the da Vinci® Surgical Sys-tem9. Another landmark in robotic surgery was the operation Lindbergh in 2001: The first trans-atlantic cholecystectomy took place with the surgeon operating in New York and the patient being treated in Strasbourg, France10. This surgical event never received the deserved attention mainly because of the tragic events of 9/11 that happened only a few days after.
In the year 2003, Intuitive bought the company Computer Motion and set an end to the Zeus robot: All intellectual property was incorporated and products of Computer Motion were no longer available on the market. Since then all robotic surgeons face the unfavourable situation of Intuitive`s indefeasible monopole with all its strategic effects such as outrageous pricing. But exactly because of this monopole, the da Vinci® Surgical System was blessed with growing figures in sales and further developments. Until now, more than 650 surgical systems are in clinical use worldwide and new features are develo-ped on a regular base. The latest technical innovation is the integration of a high definition visualization system which is already commercially available.
The Robotic system (daVinci®)The da Vinci® Surgical System was specifically designed to address the technical limitations of conventional laparoscopic surgery: The robot delivers a high-quality, magnified, surgeon-controlled 3-dimensional, stable image, contains of instruments that allow intuitive control with tremor reduction, motion scaling and wristed movements7,8. The robot contains 4 major ele-ments: The surgeon’s console, the surgical patient-side cart, EndoWrist® instruments and the laparoscopic tower. The surgeon’s console is the work
Picture 1: The da Vinci® Surgical Console
Monika E. Hagen Oliver J. Wagner Stephan A. Vorburger

1�swiss knife 2008; 4
Education I
space of the surgeon (picture 1). It contains the binocular viewers of the In-site® Vision System (picture 2), joy-stick-like instrument controllers (picture 2) and foot-paddles for steering the camera and coagulation devices. On top of this, the console allows the surgeon to control the setup and it is embedding both, the computers hard- and software. Due to two three-chip cameras and two optical channels creating two images as well as sophisticated image processing equipment, the Insite® Vision System offers a spectacular high-resolution true-to-life 3-D image (picture 2 and 3). Two light sources optimize the light intensity and the surgeon himself can control focus and position of the camera. Otherwise, the surgeon is sitting comfortable in an ergono-mically optimal and comfortable position, controlling the instruments with his fingers in the master controls (joy-sticks) below the display while having elbows resting on a padded bar and the forehead against a pad above the vision system. Approximation of thumb and index (or middle finger) operates the jawed instruments in a completely intuitive fashion. The transmission of surgical commands from the surgical console to the surgical cart is accom-plished by multiple wires.
The surgeon’s cart provides either three or four mechanical arms (picture 4). The endoscope arm holds the camera and further instrument arms execute the surgeon’s commands. The arms carry a series of multiple positioning joints which provide the excellent range of motion during surgery. A full range of different surgical EndoWrist® instruments are available including energetic instrumentation such as the Harmonic Ace or the Gyrus forceps (picture 5 and 6). Those instruments can be changed very rapidly by the patient-side assistance without influencing the position of the robotic arms. All instru-ments except the Harmonic Ace (Ultrasound technically cannot flow around corners) offer six degrees of freedom at the tip plus the seventh degree by the action of the instruments itself. All instruments are semi-disposable and can be sterilized between 10 and 20 times.
What makes da Vinci special?The laparoscopic tower incorporates all features of a standard endoscopic stack such as assistant’s monitor, insufflators, high-intensity illuminators and a camera unit. For better conversation between the surgeon and his team, the laparoscopic tower is furthermore equipped with both speakers and a microphone. All in all, through the specific “da Vinci®”-characteristics of 3-D vision, motion scaling, tremor filtration, ambidexterity, hand-eye-alignment and improved ergonomics, the robot overcomes the technical limitations of laparoscopy by restoring the “feel” of open surgery in a minimal invasive environment.
Therefore, robotic surgery is the most beneficial in procedures that are very difficult or even not suitable to perform with the instruments of conventio-nal laparoscopy. In the field of Urology, robotics already induced a dramatic change: Traditionally by open surgery performed radical prostatectomy is now more and more accomplished with the robot. Many studies suggest that robotic prostatectomy may offer enhanced cancer control and lower incidence of impotence and urinary incontinence when compared to both open and conventional laparoscopic prostatectomy. These improved clinical outcomes in combination with strategic marketing activities have established robotic prostatectomy as a frequently desired approach by patients and dro-ve to growing markets for robotic urologists. Especially in the US, traditional urologists without robotic experience are facing more and more a dramatic loss of patients.
Role of robotic-assisted surgery in visceral surgeryUnlike in Urology, an advantage of robotic-assisted surgery in the GI-tract over laparoscopic or “open” surgery has yet to be shown. Despite an in-creasing amount of literature about robotics in visceral surgery only few studies offer valuable data. Case-reports account for most of the literature. They indicate, that, robotic-assisted surgery is basically feasible for nearly all intra-abdominal procedures11-13. In view of the enhanced dexterity and the improved vision of the device compared to laparoscopy, this is not surpri-sing. The adaptation of the robotic system for interventions that have only been possible with the open technique, are sometimes stunning and even daring. Hemihepatectomies, pancreatic resection including Whipple-Opera-tions, gastrectomies for malignancy and oesophagus-resections have been reported11,14-16.
Picture 2: The da Vinci® Insite Vision System and Joy-sticks
Picture 3: The da Vinci® 30 and 0 degree endoscopes with 2 cameras
Picture 4: The da Vinci® Surgical Cart
Daniel Candinas Philippe Morel

Education I
swiss knife 2008; 4 14
Most of the robotic visceral surgery literature deals with robotic cholecystec-tomy. Prospective randomized trials report longer OR-times, due to instal-lation of the robot and increased costs compared to the laparoscopic ap-proach9,16,17. The same has been found for robotic fundoplication (Nissen) and robotic splenectomy11,18,19. Clinically, both procedures result in compa-rable outcomes. Newer reports found improved OR-times in fundoplication and rectal resections. All of the findings, however, are limited to the outcomes studied; it is, for example, not yet evidenced if robotic surgery could improve postoperative pain, postoperative recovery or wound infection.
Our experience in Geneva and BernOur initial experience in Geneva and Bern is similar to the described litera-ture. The extended OR-times are mainly due to a rather complex setting-up and docking of the robot, both can be significantly reduced with increasing routine, not only of the surgeons in charge but more importantly of the OR-team. In rather easy interventions with short OR-time, the loss of time due to the above mentioned factors cannot be overcome by a facilitated, hence, faster preparation. Evaluation of our first 50 procedures revealed a median robotic docking time of merely ten minutes, an insignificant amount of time for more complex procedures, like i.e. gastric bypass surgery.
Why then, should robotic surgery be performed for procedures that are lapa-roscopically easy to do (other than the, admittedly, thrill of handling a novel, 2Mio CHF gadget that looks cool)? (After all, we are surgeons...) – Despite being tagged “intuitive” by name, robotic surgery has to be learned and standardized, simple and frequent procedures are excellent training ground for the whole robotic team. The emphasis here is on “team”, meaning that “Lagerungspfleger, technische Op-Assistenten, Anästhesisten, Assistenten und Operateur”, all have to adapt to this new approach. Cholecystectomy and fundoplications are a great help in getting started with robotic surgery. However, our mutual experience in Geneva and Bern is that whereas chole-cystectomies are, indeed, well standardized and frequent, “easy” might not completely reflect reality. A cholecystectomy, in our opinion, is one of a few procedures, that are actually harder to do with the robot than laparoscopical-ly. This is due to the fact that many steps of the preparation are easier and faster done with true tactile feed-back (this is especially true in the presence of inflammation).
What are we training for?If simple laparoscopic interventions only serve as training, one question still remains: “what are we training for”? Where would robotic surgery be reasonable to do? We have little doubt that the more complex and difficult to access an intervention is, the better will robotic surgery perform against other means of surgery. Limitations are the extent of the OR field due to the
limited range of motion of the robot (with the new DaVinci S system, this range has greatly improved) and the higher magnification (10x vs. 4x with standard laparoscope). Hence, the oesophagus, upper gastric region, pelvis and retroperitoneum are operation sites where the robotic system can excel. Our experience with robotic assisted transhiatal oesophagectomy on cada-vers showed that preparation under direct vision and collection of lympha-tic nodes up to the height of the jugulum could be performed. Accordingly, first reports on robotic assisted transhiatal oesophagectomy are enthusias-tic about this possibility. In rectal cancer, 2-4 years experience with several hundred participants showed the ease of the preparation of the lower rectum compared to laparoscopy20,21. – Nowadays, the robotic system is increasingly utilized in an area, where laparoscopic surgery has previously shown con-siderable advantages over open surgery: bariatric surgery. Despite being a procedure that involves almost the whole abdominal cavity (which is not very hard to access) robotic surgery adds to laparoscopic gastric bypass the pos-sibility to sew intracorporally. First studies about robotic gastric bypass from 2005 reported fewer complications related to the anastomoses (leakage and stricture) and a reduction in OR time22,23. Further data followed, confirming the initial experience of the Stanford group23-25. Since we have introduced the da Vinci Surgical System into the Geneva bariatric programme in summer 2006, we are closing in on the 45th patient and we have observed no compli-cations regarding the anastomoses. We learned that the quality of robotically sewn anastomoses regarding the rate of leakage and stricture is superior to stapled anastomoses in conventionally laparoscopic gastric bypass.
From the currently available data, that show similar clinical outcome after laparoscopic or robotic interventions, one could deduce, that the relatively novel approach of robotic surgery has a) a very steep learning curve (is easier to perform) compared to laparoscopy and/or b) will have a clinically better outcome in time, compared to laparoscopic procedure, which developed over the last 18 years to the levels of today. In other words could we com-pare laparoscopic results from the first hours to the results achieved with the robot today, the advantage of the latter would be obvious. The assumption that robotic surgery will ultimately become favourable over laparoscopy in more complex procedures, is, however, only correct, if the current robots will be continuously improved.
Lessons learnedWith all the praise from the last paragraph, why is not everybody doing ro-botic surgery? After all, nor Geneva nor Bern have been at the forefront of robotic surgery. Why were robots bought, used, put in the storage room and then forgotten (we are talking about visceral surgery here. Urologist and gy-naecologist have quickly learned to integrate the additional opportunities of robotic surgery in their daily business). – The two main reasons often were miscommunication and lack of focus. Even if a surgical director realized the potential of robotic surgery, the patience and dedication to reach the exper-tise of positioning the robot and performing operations where it could make a difference was minimal and enthusiasm was quickly replaced by scepti-cism. More often robots in visceral surgery were doomed due to the lack of communication: OR team members and colleagues alike did not realize that, in order to acquire the skills above mentioned, the robot had to be introdu-ced in standardized, simple and frequent operations. This initial phase led to the perception, that robotic surgery is a costly, time-consuming gadget that yields at best the same results as the fast and simple laparoscopy. Subse-quently, the robot-assisted operations were limited to times when the OR was not used. The resulting low frequency of these operations did not allow the OR personal to familiarize with the equipment, hence, robotic set-up per-sistently used very much time, amplifying the negative perception.
We experienced, that once it has been clearly communicated to all OR per-sonal, that there will be a longish initial phase, during which time and money has to be invested to reach the next level and that, ultimately, robotic sur-gery will be useful for more complex interventions, critical voices diminis-
Picture 5: The 5 mm da Vinci® Instruments

Education I
1�swiss knife 2008; 4
hed significantly. Interestingly, the OR personal are now adept to install the necessary equipment in short time and they are keen to be part of robotic interventions.
Future of robotic surgeryStill, missing data is generally a great problem of robotics in digestive surge-ry. We have promising preliminary results from feasibility studies, but we lack of further scientific evidence as available in urology for radical prostatecto-my. Main reason for this is that only few digestive centres operate with the system. Furthermore, many digestive procedures are not as standardized as a radical prostatectomy which makes multicenter randomization an extreme-ly difficult undertaking, if not even impossible. Another concern is the large number of patients needed for a properly powered prospective, randomized trial comparing robotic versus laparoscopic procedures. All in all, satisfying outcomes are nearly impossible to create at this point.
But, if data is not perfectly convincing and the da Vinci® Surgical System so massively expensive, why should we bother working with the robot? Where is our benefit? Let’s change the point of view: The robot is not just the overp-riced, time-consuming toy that brings no actual benefit to the clinic; the robot is our future by resembling an information system with arms. Mid and long term, we will be able to integrate all surgical functions into our information system “robot”26,27. We will be able to superimpose scans and x-rays onto the
References
1. Bittner R. The standard of laparoscopic cholecystectomy. Langenbecks Arch Surg
2004; 389: 157-63
2. Memon MA. Review. Laparoscopic appendicectomy: current status. Ann R Coll
Surg Engl 1997; 79: 393-402
3. Slim K. [Laparoscopic colorectal surgery in the era of evidence- based medicine].
Gastroenterol Clin Biol 2001; 25: 1096-1104
4. Heemskerk J, Zandbergen R, Maessen JG, Greve JW, Bouvy ND. Advantages of
advanced laparoscopic systems. Surg Endosc 2006; 20: 730-733
5. Rassweiler J., Frede T., Guillonneau B. Advanced Laparoscopy. European Urology
2002; 42: I-XII
6. Schlaerth AC, Abu-Rustum NR. Role of minimally invasive surgery in gynecologic
cancers. Oncologist 2006; 11: 895-901
7. Gutt CN et al. Robot-assisted abdominal surgery. Br J Surg 2004; 91: 1390-1397
8. Broeders I.A.M.J., Ruurda J. Robotics revolutionizing surgery: the Intuitive Surgical
„Da Vinci“ system. Industrial Robot 2001; 28: 387-392
9. Himpens J, Leman G, Cadiere GB. Telesurgical laparoscopic cholecystectomy.
Surg Endosc 1998; 12: 1091
10. Marescaux J et al. Transatlantic robot-assisted telesurgery. Nature 2001; 413:
379-380
11. Giulianotti PC et al. Robotics in general surgery: personal experience in a large
community hospital. Arch Surg 2003; 138: 777-784
12. Hanly EJ, Talamini MA. Robotic abdominal surgery. Am J Surg 2004; 188:
19S-26S
13. Jacob BP, Gagner M. Robotics and general surgery. Surg Clin North Am 2003; 83:
1405-1419
14. Heemskerk J et al. First results after introduction of the four-armed da Vinci Surgical
System in fully robotic laparoscopic cholecystectomy. Dig Surg 2005; 22: 426-431
15. Ruurda JP, Visser PL, Broeders IA. Analysis of procedure time in robot-assisted
surgery: comparative study in laparoscopic cholecystectomy. Comput Aided Surg
2003; 8: 24-29
16. Vidovszky TJ, Smith W, Ghosh J, Ali MR. Robotic cholecystectomy: learning curve,
advantages, and limitations. J Surg Res 2006; 136: 172-178
17. Kim VB et al. Early experience with telemanipulative robot-assisted laparoscopic
cholecystectomy using da Vinci. Surg Laparosc Endosc Percutan Tech 2002; 12:
33-40
18. Hanisch E, Markus B, Gutt C, Schmandra TC, Encke A. [Robot-assisted laparosco-
pic cholecystectomy and fundoplication--initial experiences with the Da Vinci sys-
tem]. Chirurg 2001; 72: 286-288
19. Horgan S, Vanuno D. Robots in laparoscopic surgery. J Laparoendosc Adv Surg
Tech A 2001; 11: 415-419
20. Pigazzi A, Ellenhorn JD, Ballantyne GH, Paz IB. Robotic-assisted laparoscopic low
anterior resection with total mesorectal excision for rectal cancer. Surg Endosc
2006; 20: 1521-1525
21. Veldkamp R et al. Laparoscopic resection of colon Cancer: consensus of the
European Association of Endoscopic Surgery (EAES). Surg Endosc 2004; 18:
1163-1185
22. Mohr CJ, Nadzam GS, Curet MJ. Totally robotic Roux-en-Y gastric bypass. Arch
Surg 2005; 140: 779-786
23. Mohr CJ, Nadzam GS, Alami RS, Sanchez BR, Curet MJ. Totally robotic laparos-
copic Roux-en-Y Gastric bypass: results from 75 patients. Obes Surg 2006; 16:
690-696
24. Ali MR, Bhaskerrao B, Wolfe BM. Robot-assisted laparoscopic Roux-en-Y gastric
bypass. Surg Endosc 2005; 19: 468-472
25. Yu SC et al. Robotic assistance provides excellent outcomes during the learning
curve for laparoscopic Roux-en-Y gastric bypass: results from 100 robotic-assisted
gastric bypasses. Am J Surg 2006; 192: 746-749
26. Satava RM. The operating room of the future: observations and commentary. Semin
Laparosc Surg 2003; 10: 99-105
27. Satava RM. Future trends in the design and application of surgical robots. Semin
Laparosc Surg 2004; 11: 129-135
28. Satava RM. Surgical education and surgical simulation. World J Surg 2001; 25:
1484-1489
29. Marescaux J et al. Virtual university applied to telesurgery: from teleeducation to
telemanipulation. Stud Health Technol Inform 2000; 70: 195-201
30. Marescaux J, Rubino F. Telesurgery, telementoring, virtual surgery, and telerobotics.
Curr Urol Rep 2003; 4: 109-113
31. Ruckauer KD, Nord M, Marescaux J, Farthmann EH. [Telesurgery: standards--con-
sultations--continuing education]. Langenbecks Arch Chir Suppl Kongressbd 1997;
114: 644-646
32. Sebajang H et al. The role of telementoring and telerobotic assistance in the provi-
sion of laparoscopic colorectal surgery in rural areas. Surg Endosc 2006; 20: 1389-
1393
robotic vision system and we will use such technology for intra-operative na-vigation. Furthermore, exact planning of procedures and preparing of crucial steps will be possible. On top of this, surgical training will be conducted very easily and in an extremely effective fashion with the help of the robot28. Ano-ther underestimated issue in robotics is the possibility of tele-surgery10,29-32. Highly specialized procedures can be transmitted to remote areas and by doing so, quality of surgical care can be increased dramatically.
In summary, we are at the doorstep to a new era in surgery. The whole surgi-cal landscape will change dramatically. The next big step towards the surgi-cal future will be the breakdown of the currently very strong patents in lapa-roscopic robotics that are held by one company causing the massive costs of robotic surgery. Imagine that surgical robots sooner or later will be affordable for everybody. We will easy be able to create enough scientific data and the progress will go ahead! We can either invest in this revolutionary technology or watch the others taking over the lead! So, let’s go for the future!
Picture 6: Examples of 8 mm da Vinci® Instruments

16
Education II
swiss knife 2008; 4
Meta-Analyses: Advantages and Caveats
Interpretation of the surgical literature: a brief overview of the advantages and potential limitations of meta-analyses
Ueli Güller, [email protected]
Meta-analyses are used with increasing frequency in surgical research. A recent review demonstrates that over the past decade, appearances of meta-analyses in the medical literature have increased by a factor of 41. Therefore, in the current flourishing culture of evidenced-based medicine, the practicing surgeon and surgical resident must possess a basic understanding of the advantages and caveats of meta-analyses. Unfortunately, surgeons and surgical residents often lack this essential knowledge. The objective of the present educational review is to provi-de a brief overview of the advantages as well as potential drawbacks and caveats of meta-analyses.
The vast majority of meta-analyses combine different randomized controlled trials and, to a much lesser extent, cohort studies. In the interest of brevity, I will focus this short educational review on meta-analyses of randomized clinical trials only. Meta-analyses use statistical techniques to weigh each individual study and provide an overall result. By definition, a meta-analy-sis combines at least two (but usually more) randomized clinical trials. The use of such statistical techniques is not new. Reports of combining results of different investigations have been documented back to the start of the last century. In 1904, the statistician Karl Pearson reviewed seven studies assessing infection and mortality in typhoid-vaccinated British Army units2. Although this first meta-analysis may be questioned based on current stati-stical techniques, it nonetheless established a method for the future pooling of trial results. Since that first appearance in the medical literature, meta-analyses have come a long way. The effort of performing high-quality, metho-dologically sound, and critically appraised meta-analyses culminated in the creation of the Cochrane Group. Set up 15 years ago and named after Archie Cochrane, a British researcher who greatly contributed to the development of modern epidemiology, the Cochrane group is an international collabo-ration of over 10,000 investigators who appraise and compile high quality meta-analyses. With collaborators all over the world, the Cochrane group publishes meta-analyses on numerous topics, over 1,600 to date. One must emphasize from the outset that a meta-analysis does not simply calculate a mean measurement of all the available data from different randomized trials. The overall result of a meta-analysis is constructed by individually weighting each included trial based on its sample size. Larger randomized clinical trials carry more weight and will impact the overall result to a greater extent than will smaller studies.
Steps in Performing a Meta-Analysis3
It is of cardinal importance that the reader appreciates the process of perfor-ming a meta-analysis. The different steps include: 1. Formulating a research question.2. Stating the a priori hypothesis (a hypothesis generated prior to collecting
the data). 3. Writing a protocol, in which research question as well as inclusion and
exclusion criteria for the trials to be pooled in the meta-analysis are clear-ly outlined.
4. Performing a thorough literature search using several different search engines (e.g., Pubmed, Embase, Cochrane, etc.). 5. Performing a quality assessment and extraction of studies (usually performed by two independent investigators).6. Extracting the data from the randomized controlled trials.7. Performing a statistical analysis (including sensitivity analysis).8. Stating conclusions and providing recommendations.
In deconstructing the steps of performing a meta-analysis, one must high-light certain aspects. First, as for any study, the value of a meta-analysis can be assessed using the mnemonic ‘FINER’. That is, it must be Feasible, Interesting, Novel, Ethical, and Relevant4. If a meta-analysis is feasible and ethical but not relevant and novel, it will be worthless. Second, the search for randomized clinical trials is undertaken only after a protocol has been written a priori and inclusion and exclusion criteria have been clearly defined. Ideally, two independent investigators should search for studies that meet the inclusion criteria. Furthermore, the search should be as comprehensive as possible, that is, not limited to Medline but rather spread among other scientific databases such as Embase and Cochrane. Similarly, limits on lan-guage and date should be avoided. Moreover, as explained in greater detail below, performing a systematic search for unpublished studies is imperative. Finally, two independent investigators must assess the quality and suitability of retrieved studies. Agreement should be based on inclusion and exclusion criteria outlined in the protocol.
Interpretation of Forest PlotsIn a meta-analysis, data of the different randomized clinical trials are typically presented as forest plots (Figure 1)5. The correct interpretation of these forest plots is crucial for the surgical reader and therefore worth a short paragraph. Forest plots use boxes and whiskers (horizontal lines representing the 95% confidence interval) to represent individual trials. The astute reader will re-alize that the size of the boxes varies among different studies. In fact, box size correlates directly with the sample size (number of patients enrolled) of a given randomized controlled trial. If the trial includes a large sample size, the box size will be large, and vice versa. For instance, in Figure 1, the Z et al. trial has a larger sample size (larger box) compared to the studies by X et al. and Y et al. The whiskers represent the 95% confidence intervals. These confidence in-tervals represent the range of values, for which you can be 95% confident that the true value is included6. Confidence intervals provide the reader with an appreciation of the reliability of the results. The wider the confidence in-terval, the higher the uncertainty that the reported results are accurate6. The width of the 95% confidence interval is indirectly proportional to the sample size of the randomized clinical trial: if the trial includes a large number of pa-tients (e.g., Z et al., Figure 1), the width of the 95% confidence interval will be narrow, and vice versa. Finally, the whiskers show the astute reader whether or not the individual study is statistically significant6. If the 95% confidence interval crosses the vertical line of no effect (0 for a difference between two groups and 1 for a ratio of two groups), then that trial result individually is not statistically significant (e.g., X et al. trial in Figure 1). Conversely, if the 95% confidence interval does not cross the vertical line of no effect, the result is statistically significant (e.g., studies by Y et al. and Z et al. in Figure 1). The overall result (summary effect) is represented by the diamond shape. In Figure 1 it does not cross the line of no effect, representing a statistically significant overall result (p<0.05).

1�
Education II
swiss knife 2008; 4
Advantages of Meta-AnalysesThe primary advantage of meta-analyses is an increase in power over that of individual randomized controlled trials. Power is defined as the proba-bility of detecting a statistically significant result if the patient samples are truly different6, 7. Single randomized clinical trials are often underpowered. In other words, they frequently enroll too few patients to prove that a clinically relevant difference is statistically significant(6, 7). The result is a negative study (p-value is non-significant). Meta-analyses may overcome this limitation by combining different randomized clinical trials. This increases the overall sam-ple size and thus increasing the power. Another important advantage is that, in the case of various randomized clinical trials concluding differently, a meta-analysis may provide a unifying conclusion.
Limitations of Meta-AnalysesWhen conducted optimally with high-quality data, meta-analyses are now considered the highest level of evidence (level 1a evidence). Nonetheless, the surgical reader should heed several caveats in regards to meta-analyses.Garbage in – Garbage out Phenomenon: Conceivably, a researcher may per-form an optimal, methodologically sound meta-analysis on suboptimal data. It is crucial to realize that combining different randomized clinical trials using fancy statistical techniques will not improve the quality of trials included in a meta-analysis. If the randomized clinical trials are poorly designed and poorly conducted, the meta-analysis summarizing these trials will also be of poor quality. Remember: garbage in – garbage out8!Publication Bias: The scientific literature extensively documents a well-known phenomenon whereby positive trials (studies that produce a statis-tically significant result) are much more likely to be published than so-called “negative trials” (studies producing no statistically significant association)9,10. This publication bias may lead to overestimating the effect of a particular meta-analytic intervention. To ensure that a meta-analysis produces approp-riate results, one must systematically search for negative trials for inclusion. A variety of methods are used to detect potential publication biases. Funnel plots are one way of graphically representing them10,11. Furthermore, since 2004, medical randomized controlled trials must be registered prior to ac-crual (at www.clinicaltrials.gov). Several highly ranked medical and surgical journals will no longer publish manuscripts of unregistered randomized clini-cal trials. Thus, in the spirit of preventing the skewing of meta-analysic data, the effort to prevent negative trial data from “disappearing” is undoubtedly a worthy one.Heterogeneity – Comparing Apples and Oranges: Since peri-operative care and surgical techniques are not necessarily uniform or easily standardizab-le12, meta-analyses are more difficult to perform on surgical interventions than on drug trials. Dealing with heterogeneity may be difficult. Not only is there a risk of heterogeneity within the randomized controlled trial, but this heterogeneity may be amplified when comparing between trials. There-fore, if the heterogeneity among the various randomized trials included in a meta-analysis is high, the investigator risks comparing apples and oranges. Although it may occur by chance alone, heterogeneity is most commonly associated with diversity in technical ability among trial surgeons12. Optimally constructed multi-center surgical randomized controlled trials now contain some validation of standardized technical ability. For instance, standardiza-tion can be achieved by peer-review of surgical procedures. A good example is the COST trial comparing open and laparoscopic colectomies for cancer13. Before the laparoscopic surgeons were allowed to enroll patients into the tri-al, their surgical techniques were submitted to peer review, thereby ensuring a baseline standard. The peer review process diminishes the risk of subopti-mal technical skills being a potential confounder for poor outcomes, and also enhances homogeneity of surgical skills among similar trials.‘Sensitivity Analysis’ is one method of evaluating heterogeneity among dif-ferent trials, whereby certain potentially diverse groups within the meta-ana-lysis are compared. What is important is not whether the subgroups remain statistically significant with respect to the overall research question, but whether any statistically significant differences exist between them. Also, if
homogeneity exists, then omitting a certain trial from the analysis should not change the overall result. Conversely, if heterogeneity is present, then omit-ting a key trial may well change the pooled estimate. It follows that the more similar the included randomized controlled trials, the less the heterogeneity. If much heterogeneity exists among different randomized clinical trials, per-forming a meta-analysis may not make sense, and the reporting of different studies in a systematic review (without using statistical methods to combine the results of different investigations) may be more appropriate.
SummaryBasic knowledge of the advantages and limitations of meta-analyses is es-sential to the surgical resident and practicing surgeon. Although meta-ana-lyses are considered the highest level of evidence and an essential part of medical research, the clinician must heed its potential limitations. Combining independent randomized clinical trials using statistical techniques will incre-ase the power, though this does not necessarily translate into higher quality research if the individual studies are of poor quality.
References:
1. Mahid SS, Hornung CA, Minor KS, et al.. Systematic reviews and meta-analysis for
the surgeon scientist. Br J Surg 2006; 93: 1315-1324.
2. Engels EA, Falagas ME, Lau J, et al.. Typhoid fever vaccines: a meta-analysis of
studies on efficacy and toxicity. Bmj 1998; 316: 110-116.
3. Sauerland S, Seiler CM. Role of systematic reviews and meta-analysis in evidence-
based medicine. World J Surg 2005; 29: 582-587.
4. Hulley SB, Cummings SR, Browner WS, et al.. Designing clinical research: an epi-
demiologic approach, 2ed. Philadelphia: Lippincott Williams & Wilkins, 2001.
5. Lewis S, Clarke M. Forest plots: trying to see the wood and the trees. Bmj 2001;
322: 1479-1480.
6. Guller U, DeLong ER. Interpreting statistics in medical literature: a vade mecum for
surgeons. J Am Coll Surg 2004; 198: 441-458.
7. Guller U, Oertli D. Sample size matters: a guide for surgeons. World J Surg 2005;
29: 601-605.
8. Guller U. Caveats in the interpretation of the surgical literature. Br J Surg 2008; 95:
541-546.
9. Dickersin K. The existence of publication bias and risk factors for its occurrence.
Jama 1990; 263: 1385-1389.
10. Mahid SS, Quadan M, Hornung CA, et al.. Assessment of publication bias for the
surgeon scientist. Br J Surg 2008; 95: 943-949.
11. Egger M, Davey Smith G, Schneider M, et al.. Bias in meta-analysis detected by a
simple, graphical test. Bmj 1997; 315: 629-634.
12. Guller U. Surgical outcomes research based on administrative data: inferior or comple-
mentary to prospective randomized clinical trials? World J Surg 2006; 30: 255-266.
13. A comparison of laparoscopically assisted and open colectomy for colon cancer. N
Engl J Med 2004; 350: 2050-2059.
Figure 1: A simplified, hypothetical example of a forest plot demonstrating three randomized controlled trials and an overall (pooled) effect, which is statistically significant (it does not cross the line of no effect).

18swiss knife 2008; 4
Research
N Engl J Med. 2008; 359: 766-768 IF (2007) 52.589 Cancer Res. 2008; 68: 5152-5158 IF (2007) 7.672 Ann Surg. 2008; 248: 259-265 IF (2007) 7.446
New England Journal of Medi-cine
Glucagon-like peptide 1-receptor scans to localize occult insulinomas
Wild D, Mäcke H, Christ E, Gloor B, Reubi JC
University Hospital Basel, University Hospital Berne, University of Berne
The precise localization of some insulinomas (islet-cell adenomas that secrete insulin) with the use of conventi-onal imaging techniques, such as computed tomography (CT), magnetic resonance imaging (MRI), endosonogra-phy, and indium-111 (111In)–labeled pentetreotide scin-tigraphy (OctreoScan), is a challenging clinical problem. In vitro studies have demonstrated that receptors for glu-cagon-like peptide 1 (GLP-1) are highly overexpressed in almost all insulinomas. Therefore, GLP-1-like radioligands retaining high binding affinity to GLP-1 receptors have been developed. One such radioligand, [Lys40(Ahx-DTPA-111In)NH2]exendin-4, successfully targeted insulinomas in the Rip1-Tag2 mouse. We evaluated the diagnostic value of GLP-1–receptor scintigraphy in two patients with insulinomas that either were not localized (Patient 1) or were unsatisfactorily localized (Patient 2) with the use of conventional imaging methods. The radioligand was la-beled with 111In and was administered intravenously (90 MBq) during a 5-minute period. Whole-body planar ima-ging and single-photon-emission CT (SPECT) imaging of the abdomen were performed at various times. The results provided proof of concept that a GLP-1–receptor scan can identify barely detectable insulinomas that express GLP-1 receptor. Histologic analysis of surgically removed tissues that corresponded to the tumor „hot spots“ identified in both patients confirmed that the lesions were insulinomas containing GLP-1 receptors in high density. In Patient 1, a 64-year-old man with neuroglycopenia and endogenous hyperinsulinism, the tumor could not be localized with any of the conventional preoperative imaging methods (including CT, endoscopic ultrasonography, octreoscan scintigraphy, and selective arterial calcium stimulation and hepatic venous sampling), whereas GLP-1–receptor scin-tigraphy precisely identified the lesion, which was confir-med on removal as an ectopic insulinoma. In Patient 2, a 31-year-old woman with endogenous hyperinsulinism, the tumor location on the GLP-1–receptor scan was found to overlap with that of a suspicious lesion seen on endosono-graphy. All other imaging methods had been unsuccess-ful. In both patients, the GLP-1–receptor scan enabled the surgeon to localize and resect the tumor. Not only were the SPECT images decisive, but the large accumulation of radioactivity in these small tumors also permitted in situ localization with a probe during surgery.
Cancer Research
Serotonin regulates macrophage-mediated angiogenesis in a mouse model of colon cancer allografts
Nocito A, Dahm F, Jochum W, Jang JH, Georgiev P, Bader M, Graf R, Clavien PA
Swiss HPB Center, Department of Visceral and Trans-plant Surgery, University Hospital of Zurich
Serotonin, a neurotransmitter with numerous functions in the central nervous system (CNS), is emerging as an im-portant signaling molecule in biological processes outside of the CNS. Recent advances have implicated serotonin as a regulator of inflammation, proliferation, regeneration, and repair. The role of serotonin in tumor biology in vivo has not been elucidated. Using a genetic model of sero-tonin deficiency (Tph1(-/-)) in mice, we show serotonin to be crucial for the growth of s.c. colon cancer allografts in vivo. Serotonin does not enhance tumor cell proliferation but acts as a regulator of angiogenesis by reducing the expression of matrix metalloproteinase 12 (MMP-12) in tumor-infiltrating macrophages, entailing lower levels of angiostatin-an endogenous inhibitor of angiogenesis. Ac-cordingly, serotonin deficiency causes slower growth of s.c. tumors by reducing vascularity, thus increasing hyp-oxia and spontaneous necrosis. The biological relevance of these effects is underscored by the reconstitution of serotonin synthesis in Tph1(-/-) mice, which restores al-lograft phenotype in all aspects. In conclusion, we show how serotonin regulates angiogenesis in s.c. colon cancer allografts by influencing MMP-12 expression in tumor-in-filtrating macrophages, thereby affecting the production of circulating angiostatin.
Annals of Surgery
A multivariate analysis of potential risk factors for intra- and postope-rative complications in 1316 elective laparoscopic colorectal procedures
Kirchhoff P, Dincler S, Buchmann P
Department of Surgery, City Hospital Waid, Zurich
Background: To identify predictive risk factors for intra- and postoperative complications in patients undergoing lapa-roscopic colorectal surgery. In emergency situations or in elective open and laparoscopic colorectal surgery, there are many risk factors that should be recognized by the surgeon to reduce complications and initiate adequate treatment. Most available data, thus far, refer to open colorectal sur-gery and literature that focuses mainly on a laparoscopic approach is still rare.
Methods: Univariate and multivariate analyses of a pro-spectively gathered database (1993-2006) were performed on a consecutive series of patients (1316) undergoing lapa-roscopic colorectal surgery who were operated at a single institution (first referral center). Patients were assessed for demographic data, operative indications, type of resection, and intra- and postoperative complications. Altogether, we analyzed 20 potential risk factors to identify significant influ-ence on the intra- and postoperative outcome.
Results: Significant risk factors that led to intraoperative complications consisted of age > or = 75 years and ma-lignant neoplasia. Increased postoperative rate of surgical complications was significantly influenced by male gender, age > or = 75 years, American Society of Anesthesiology class > or = III, malignant neoplasia, and the experience of the surgeon. The analysis of specific medical postoperative complications revealed even more significant predictive risk factors. In addition, our analysis showed that specific risk factors predict specific complications such as postoperative bleeding, anastomotic leakage, and surgical site infections. The type of surgical procedure performed also influenced patient outcome.
Conclusions: This large single center study provides the first evidence of the significance of predictive risk factors for intra- and postoperative complications in laparoscopic colorectal surgery.
Surgical Research in Switzerland

Research II
19
Swiss Medical Weekly
Lehmann K1, Guller U2, Bugnon S1, Zuber M1
1Department of Surgery, Kantonsspital Olten2Department of Surgery, University Hospital Basel
Background: The objective of the present investigation is twofold: first, to assess how interdisciplinary tumour boards in Switzerland are designed, established, and ra-ted in clinical practice; and second, to evaluate the per-ception regarding the determination of cancer centres as required by the Swiss National Cancer Program.
Methods: An anonymous questionnaire was sent to the heads of surgical departments in Switzerland (n=110). Among the contacted clinics were 11 large referral cen-tres (type A clinics), 48 surgical departments of cantonal hospitals (type B clinics), and 51 regional surgical depart-ments (type C clinics).
Results: For most type A and B clinics, tumour boards are held on a weekly basis (A: 100 per cent, B: 88 per cent, C: 26 per cent; P<0.001). On average, 66 per cent of respondents (A: 90 per cent, B: 71 per cent, C: 52 per cent; P=0.059) consider tumour boards as a standard of care for every cancer patient. Determination of cancer centres was favoured by 49 per cent of all respondents (A: 80 per cent, B: 56 per cent, C: 32 per cent; P=0.012).
Conclusions: The present survey in Switzerland clearly shows significant differences in the use of tumour boards and in their perception as a standard of care between type A, B, and C clinics. There are large discrepancies in the perceived need to determine cancer centres in Swit-zerland as required by the Swiss National Cancer Pro-gram. Continued education regarding the importance of tumour boards is necessary, as their implementation is associated with more optimal cancer patients` care.
Swiss Medical Weekly
Lessons learned from one thousand consecutive colonic resections in a teaching hospital
Buchs NC, Gervaz P, Bucher P, Huber O, Mentha G, Morel P
Department of Surgery, University Hospital Geneva
Background: The aim of this study was to assess the risk factors associated with mortality and morbidity following colorectal surgery.
Methods: All data regarding patients who underwent colonic resection in our institution between November 2002 and February 2006 were prospectively entered into a computerised database.
Results: Over a 40-month period 1,016 colonic resections were performed (43 ileocecal; 225 right; 11 transverse; 98 left; 287 sigmoid; 52 subtotal; 108 low anterior; 29 ab-dominoperineal resections; 103 Hartmann; 46 reversal of Hartmann; and 14 proctocolectomy). The most common indications for surgery were: adenocarcinoma (44%); di-verticulosis (19%); complicated diverticulitis (12%); ade-noma (4%); and inflammatory bowel disease (4%). There were 719 (71%) elective and 297 (29%) emergency pro-cedures. Overall mortality and morbidity rates were 5.4% and 20.7% respectively. The anastomotic leak rate was 3.8% (31 leaks out of 809 anastomoses). In univariate analysis, patients who underwent elective surgery had lower mortality (0.7% vs. 17%, p <0.001) and morbidity rates (17% vs. 30%, p <0.001), as well as a shorter hospi-tal stay (12.4 days vs. 19.9 days, p <0.001). In multivariate analysis ASA score ≤3 and emergency surgery were both associated with increased mortality (p <0.001) and mor-bidity (p <0.001) following colonic resection.
Conclusions: Elective colectomies are standard proce-dures carrying below 1% mortality; by contrast, emer-gency colonic resections remain surgical challenges in compromised and/or elderly patients and are associated with high complication rates.
Journal of laparoendoscopic & advanced surgical techniques. Part A
Assessment of construct validity of a virtual reality laparoscopy simulator
Rosenthal R, Gantert WA, Hamel C, Hahn-loser D, Metzger J, Kocher T, Vogelbach P, Scheidegger D, Oertli D, Clavien PA
Departments of Anesthesiology and Surgery, University Hospital
Background: The aim of this study was to assess whether virtual reality (VR) can discriminate between the skills of no-vices and intermediate-level laparoscopic surgical trainees (construct validity), and whether the simulator assessment correlates with an expert‘s evaluation of performance.
Methods: Three hundred and seven (307) participants of the 19th-22nd Davos International Gastrointestinal Surgery Workshops performed the clip-and-cut task on the Xitact LS 500 VR simulator (Xitact S.A., Morges, Switzerland). Ac-cording to their previous experience in laparoscopic surgery, participants were assigned to the basic course (BC) or the intermediate course (IC). Objective performance parameters recorded by the simulator were compared to the standar-dized assessment by the course instructors during laparos-copic pelvitrainer and conventional surgery exercises.
Results: IC participants performed significantly better on the VR simulator than BC participants for the task comple-tion time as well as the economy of movement of the right instrument, not the left instrument. Participants with maxi-mum scores in the pelvitrainer cholecystectomy task perfor-med the VR trial significantly faster, compared to those who scored less. In the conventional surgery task, a significant difference between those who scored the maximum and those who scored less was found not only for task com-pletion time, but also for economy of movement of the right instrument.
Conclusions: VR simulation provides a valid assessment of psychomotor skills and some basic aspects of spatial skills in laparoscopic surgery. Furthermore, VR allows discrimina-tion between trainees with different levels of experience in laparoscopic surgery establishing construct validity for the Xitact LS 500 clip-and-cut task. Virtual reality may become the gold standard to assess and monitor surgical skills in laparoscopic surgery.
Swiss Med Wkly 2008; 138: 123-127 IF (2006) 1.346 Swiss Med Wkly 2007; 137: 259-264 IF (2006) 1.346 J Lap Adv Surg Tech A 2007; 17: 407-413 IF (2006) 0.718
Research
19
Cellular and Molecular Life Sciences
Role of serotonin in the hepato-gas-troIntestinal tract: an old molecule for new perspectives
Lesurtel M, Soll C, Graf R, Clavien PA
Swiss HPB Center, Department of Visceral and Trans-plant Surgery, University Hospital of Zurich
Beside its role as a neurotransmitter in the central ner-vous system, serotonin appears to be a central physio-logic mediator of many gastrointestinal (GI) functions and a mediator of the brain-gut connection. By acting directly and via modulation of the enteric nervous system, sero-tonin has numerous effects on the GI tract. The main gut disturbances in which serotonin is involved are acute chemotherapy-induced nausea and vomiting, carcinoid syndrome and irritable bowel syndrome. Serotonin also has mitogenic properties. Platelet-derived serotonin is involved in liver regeneration after partial hepatectomy. In diseased liver, serotonin may play a crucial role in the progression of hepatic fibrosis and the pathogenesis of steatohepatitis. Better understanding of the role of the serotonin receptor subtypes and serotonin mechanisms of action in the liver and gut may open new therapeutic strategies in hepato-gastrointestinal diseases.
International Journal of Cancer
Cancer testis antigen expression in gastrointestinal stromal tumors: new markers for early recurrence
Perez D, Herrmann T, Jungbluth AA, Samartzis P, Spagnoli G, Demartines N, Clavien PA, Marino S, Seifert B, Jaeger D
Department of Visceral and Transplant Surgery, Uni-versity Hospital Zurich
Cancer testis antigens (CTAs) are expressed in a variety of malignant tumors but not in any normal adult tissues except germ cells and occasionally placenta. Because of this tumor-associated pattern of expression, CTAs are regarded as potential vaccine targets. The expression of CTAs in gastrointestinal stromal tumors (GIST) has not been analyzed systematically previously. The present study was performed to analyze the expression of CTA in GIST and to determine if CTA expression correlates with prognosis. Thirty-five GIST patients were retrospectively analyzed for their expression of CTAs by immunohisto-chemistry using the following monoclonal antibodies (mAb/antigen): MA454/MAGE-A1, M3H67/MAGE-A3, 57B/MAGE-A4, CT7-33/MAGE-C1 and E978/NY-ESO-1. Fourteen tumors (40%) expressed 1 or more of the 5 CTAs tested. Fourteen percent (n = 5/35) were positive for MAGE-A1, MAGE-A3 or MAGE-A4, respectively. Twenty-six percent (n = 9/35) stained positive for MAGE-C1 and 20% (n = 7/35) for NY-ESO-1. A highly significant cor-relation between CTA expression and tumor recurrence risk was observed (71% vs. 29%; p = 0.027). In our study population, the high-risk GIST expressed CTAs more fre-quently than low-risk GIST (p = 0.012). High-risk GISTs which stained positive for at least 1 CTA, recurred in 100% (n = 25) of the cases. This is the first study ana-lyzing CTA expression in GIST and its prognostic value for recurrence. The CTA staining could add information to the individual patient prognosis and represent an interes-ting target for future treatment strategies.
British Journal of Surgery
Characterization of time-related changes after experimental bile duct ligation
Georgiev P, Jochum W, Heinrich S, Jang JH, Nocito A, Dahm F, Clavien PA
Swiss HPB Center, Department of Visceral and Trans-plant Surgery, University Hospital of Zurich
Background: Although bile duct ligation (BDL) in mice is used to study cholestasis, a detailed description of this ani-mal model is lacking. The aim of this study was to define specific phases of acute and chronic injury and repair in the different cellular compartments of the liver.
Methods: C57BL/6 mice underwent BDL or sham laparo-tomy, and serum and liver tissue were analysed between 8 h and 6 weeks later.
Results: Biliary infarcts and alanine aminotransferase le-vels revealed acute hepatocellular injury peaking at days 2-3, paralleled by enhanced transcription of pro-proliferative mediators and followed by a distinct peak of hepatocellu-lar proliferation at day 5. Cholangiocellular proliferation oc-curred in large bile ducts on days 2-3 and in small bile ducts on day 5. Neutrophil infiltration occurred within 8 h, with neutrophils remaining the predominant immune cell type until day 3. Acute injury was followed by continuous tissue repair, lymphocyte and Kupffer cell infiltration, and accumu-lation of collagen during the second week. Thereafter, the number of alpha-smooth muscle actin-positive cells and the expression of transforming growth factor beta1, tissue inhi-bitor of metalloproteinases 1 and procollagen (I) decreased, and liver fibrosis stabilized.
Conclusions: BDL elicits dynamic changes in mouse liver. The chronological dissection and quantification of these events identified specific phases of acute and chronic cho-lestatic liver injury.
Cell Mol Life Sci. 2008; 65: 940-952 IF (2007) 5.239 Int J Cancer. 2008; 123: 1551-1555 IF (2007) 4.555 Br J Surg. 2008; 95: 646-656 IF (2007) 4.304

20swiss knife 2008; 4
Research
British Journal of Surgery
Prospective randomized study of monopolar scissors, bipolar vessel sealer and ultrasonic shears in lapa-roscopic colorectal surgery
Hubner M, Demartines N, Muller S, Dindo D, Clavien PA, Hahnloser D
Department of Visceral and Transplantation Surgery, University Hospital of Zurich
Background: Many instruments are used for laparosco-pic dissection, including monopolar electrosurgery scis-sors (MES), electrothermal bipolar vessel sealers (BVS) and ultrasonically coagulating shears (UCS). These three devices were compared with regard to dissection time, blood loss, safety and costs.
Methods: Sixty-one consecutive patients undergoing laparoscopic left-sided colectomy were randomized to MES, BVS or UCS. The primary endpoint was dissection time.
Results: Patient and operation characteristics did not differ between the groups. Median dissection time was significantly shorter with BVS (105 min) and UCS (90 min) than with MES (137 min) (P < 0.001). With BVS and UCS, significantly fewer additional clips were required (MES 9 versus BVS 0 versus UCS 3; P < 0.001) and there was a trend towards lower blood loss (125 versus 50 versus 50 ml respectively; P = 0.223) and a reduced volume of suction fluid (425 versus 80 versus 110 ml; P = 0.058). Overall satisfaction was similar for the three instruments. Dissection with BVS and UCS was significantly cheaper than with MES, assuming a centre volume of 200 cases per year (P = 0.009).
Conclusions: BVS and UCS shorten dissection time in laparoscopic left-sided colectomy and are cost-effective compared with MES.
Br J Surg. 2008; 95: 1098-1104 IF (2007) 4.304
Cancer Gene Therapy
Dual induction of PKR with E2F-1 and IFN-alpha to enhance gene therapy against hepatocellular carcinoma
Roh V, Laemmle A, Von Holzen U, Stro-ka D, Dufour JF, Hunt KK, Candinas D, Vorburger SA
Department of Visceral and Transplantation Surgery, Inselspital, Bern University Hospital
Overexpression of the transcription factor E2F-1 induces apoptosis in tumor cells. This apoptotic effect is partly mediated through the induction of the double-stranded RNA-activated protein kinase (PKR). Here, we investi-gate if agents that upregulate PKR could enhance the apoptotic effect of E2F-1 overexpression in liver tumors. In human hepatocellular carcinoma (HCC) cells (Hep3B, HepG2, Huh7), adenovirus-mediated overexpression of E2F-1 (AdCMV-E2F) transcriptionally increased PKR mRNA. The subsequent increase of total and phospho-rylated PKR protein was followed by induction of apop-tosis. When AdCMV-E2F was combined with the PKR modifier interferon alpha (IFNalpha), PKR was additionally upregulated and both PKR activation and apoptosis were increased. Subcutaneous xenograft tumors were selec-tively targeted using an adenoviral vector expressing E2F-1 under the control of the human telomerase reverse transcriptase (hTERT) promoter (AdhTERT-E2F). Weekly systemic administration of AdhTERT-E2F inhibited tumor growth. The tumor suppressive effect of AdhTERT-E2F therapy was further enhanced in combination with IFNal-pha.Our results demonstrate that PKR activating agents enhance the anti-tumor effect of E2F-1 overexpression in HCC in-vitro and in-vivo. Hence, modulation of PKR is a potential strategy to increase the efficacy of PKR-depen-dent anti-tumor therapies.
Cancer Gene Ther. 2008; 15: 636-644 IF (2007) 3.89
British Journal of Surgery
Long-term follow-up of proximal ver-sus distal laparoscopic gastric by-pass for morbid obesity
Müller MK, Räder S, Wildi S, Hauser R, Clavien PA, Weber M
Br J Surg. 2008; 95: 1375-1379 IF (2007) 4.304
Department of Visceral and Transplant Surgery, Uni-versity Hospital Zurich
Background: Laparoscopic gastric bypass is the ‚gold standard‘ for treatment of morbidly obese patients in many centres. There is debate regarding the optimal length for small bowel limbs. This study aimed to deter-mine whether the proximal or distal approach is better.
Methods: Twenty-five patients undergoing primary distal gastric bypass in 2000-2002 were randomly matched for age, sex and preoperative body mass index (BMI) with 25 patients having a primary proximal bypass. All distal operations were performed laparoscopically; one proxi-mal procedure was converted to open surgery.
Results: Mean operating time was 170 min for proximal and 242 min for distal bypasses (P = 0.004); median hos-pital stay was similar in the two groups. There were no deaths and the overall complication rate was similar, as was weight loss at 4 years: BMI decreased from 45.9 to 31.7 kg/m(2) for the proximal and from 45.8 to 33.1 kg/m(2) for the distal approach. Co-morbidities decreased after surgery in both groups; the prevalence of diabetes, arterial hypertension and dyslipidaemia at all time points was similar in the two groups.
Conclusions: Proximal and distal laparoscopic gastric bypass operations are feasible and safe, with no dif-ferences in weight loss or reduction of co-morbidity in unselected morbidly obese patients.

Research
21
Liver Transplantation
Ischemic preconditioning and inter-mittent clamping confer protection against ischemic injury in the cirrho-tic mouse liver
Jang JH, Kang KJ, Kang Y, Lee IS, Graf R, Clavien PA
Department of Surgery, School of Medicine, Institute for Medical Genetics, Keimyung University, Daegu, Korea
Surgery on cirrhotic livers is fraught with complications, and many surgeons refrain from operating on patients with cirrhosis. Surgical procedures include temporal oc-clusion of blood flow resulting in ischemia. The mecha-nisms of protective strategies to prevent ischemic injury in patients with cirrhosis are not fully understood. The aim of this study was to evaluate how the cirrhotic liver tole-rates an ischemic insult, whether mechanisms other than those observed in the normal liver are active, and whether intermittent clamping and preconditioning, which are known as safe surgical strategies in normal and steatotic livers, confer protection to the cirrhotic liver. We applied partial hepatic inflow occlusion to cirrhotic mice fed car-bon tetrachloride according to different vascular occlusi-on protocols: intermittent clamping with 15 or 30 minute cycles of ischemia or ischemic preconditioning prior to 60 or 75 minutes of ischemia. Continuous ischemia (60 or 75 minutes) served as controls. The results showed that the cirrhotic liver was significantly more susceptible to 60 minutes of ischemia than the normal liver. Apopto-sis was higher in the normal liver, whereas necrosis was a predominant feature in the cirrhotic liver. Both proto-cols of intermittent vascular occlusion and ischemic pre-conditioning dramatically prevented injury compared to continuous occlusion for 60 minutes. This protection was associated with reduced necrosis and apoptosis, and particularly reduced activation of the apoptotic pathway through mitochondria. In conclusion, this study extends the protective effects of ischemic preconditioning and in-termittent clamping to the cirrhotic liver, highlighting a di-minished apoptotic pathway with dramatic improvement in the development of necrosis.
Surgical Endoscopy
Bucher P, Wutrich P, Pugin F, Gonzales M, Gervaz P, Morel P
Visceral Surgery, Department of Surgery, Geneva Uni-versity Hospital
Background: A number of surgical techniques for colo-rectal anastomosis have been described for laparoscopic left-sided colectomies. Due to the complexity of these procedures, open preparation of the proximal bowel for circular stapler anastomosis through a Pfannenstiel inci-sion has become the gold standard. We report a new la-paroscopic technique for totally intracorporeal colorectal circular anastomosis (TLCCA) using a circular stapler.
Methods: Preliminary experience using TLCCA in three patients scheduled for laparoscopic left colectomies (two) and sigmoidectomy (one).
Results: Side-to-end colorectal anastomosis through TLCCA was feasible in all patients scheduled for preli-minary experience. Median time from anvil insertion into abdominal cavity to anastomosis was 14 (11-17) minutes. No postoperative complications were recorded.
Conclusions: Side-to-end anastomosis can be easily and safely performed using conventional circular stapler through TLCCA. TLCCA is performed using four laparos-copic ports without additional skin incision (except tro-cars incision) and allows the retrieval of surgical pieces through a specimen bag.
Nutrition Reviews
Role of nutrition in liver transplan-tation for end-stage chronic liver di-sease
Stickel F, Inderbitzin D, Candinas D
Institute of Clinical Pharmacology, Inselspital, University of Berne
Patients with end-stage liver disease often reveal significant protein-energy malnutrition, which may deteriorate after listing for transplantation. Since malnutrition affects post-transplant survival, precise assessment must be an integral part of pre- and post-surgical management. While there is wide agreement that aggressive treatment of nutritional de-ficiencies is required, strong scientific evidence supporting nutritional therapy is sparse. In practice, oral nutritional sup-plements are preferred over parenteral nutrition, but enteral tube feeding may be necessary to maintain adequate calorie intake. Protein restriction should be avoided and administra-tion of branched-chain amino acids may help yield a suffici-ent protein supply. Specific problems such as micronutrient deficiency, fluid balance, cholestasis, encephalopathy, and comorbid conditions need attention in order to optimize pa-tient outcome.
Liver Transpl. 2008; 14: 980-988 IF (2007) 3.751 Surg Endosc. 2007 (Epub ahead of print) IF (2007) 2.242 Nutr Rev. 2008; 66: 47-54 IF (2007) 2.860
Totally intracorporeal laparoscopic colorectal anastomosis using circu-lar stapler

22swiss knife 2008; 4
Research
Obesity Surgery
Quality of Life After Bariatric Surgery-A Comparative Study of Laparosco-pic Banding vs. Bypass
Müller MK, Wenger C, Schiesser M, Clavien PA, Weber M
Division of Visceral and Transplantation Surgery, Uni-versity Hospital Zürich
Background: Laparoscopic gastric banding and Roux-en-Y gastric bypass are widely used for the treatment of morbid obesity. The impact of these two procedures on health-related quality of life has not been analyzed in comparative studies.
Methods: A matched-pair analysis of a prospectively collected database was performed. Fifty-two consecutive patients with laparoscopic gastric bypass were randomly matched to fifty-two patients with laparoscopic gastric banding according to age, BMI, and gender. Quality of life was assessed using two standardized questionnaires (SF 36 and Moorehead-Ardelt II).
Results: Mean preoperative BMI was 45.7 kg/m(2) for the bypass patients and 45.3 kg/m(2) for the banding patients. Mean BMI after 3 years follow-up of was 30.4 kg/m(2) and 33.1 kg/m(2) (p = 0.036). In the SF 36 ques-tionnaire, gastric bypass patients yielded a mean total score of 613 versus 607 points in the gastric banding group (p = 0.543), which is comparable to the normal population in Europe. In the Moorhead-Ardelt II questi-onnaire, the gastric bypass patients scored a mean to-tal of 1.35 points and the gastric banding patients 1.28 points (p = 0.747). Of the patients, 97% with a gastric bypass and 83% with a gastric banding were satisfied with the result of the operation (p = 0.145).
Conclusions: The patients after laparoscopic gastric by-pass and laparoscopic gastric banding have a high level of satisfaction 3 years after the operation and have similar quality of life scores compared to the normal population. Quality of life indexes were not different between the two procedures and were independent of weight loss in suc-cessfully operated patients.
Obes Surg. 2008; (Epub ahead of print) IF (2007) 2.852
The American Journal of Surgery
Laparoscopic mesh-augmented hi-atoplasty as a treatment of gastroe-sophageal reflux disease and hiatal hernias-preliminary clinical and func-tional results of a prospective case series
Müller-Stich BP, Linke GR, Borovicka J, Marra F, Warschkow R, Lange J, Mehrabi A, Köninger J, Gutt CN, Zerz A
Department of General, Abdominal and Transplant Surgery, University of Heidelberg; Cantonal Hospital of St.Gallen
Background: Because fundoplication-related side effects are frequent, we evaluated laparoscopic mesh-augemen-ted hiatoplasty (LMAH) as a potential treatment option for gastroesophageal reflux disease and/or symptomatic hi-atal herania. LMAH aims to prevent reflux solely by mesh-reinforced narrowing of the hiatus and lengthening of the intra-abdominal esophagus.
Methods: Twenty-two consecutive patients with LMAH were evaluated prospectively using a modified Gas-trointestinal Symptom Rating Scale questionnaire, pH measurement, manometry, and endoscopy. Follow-up was scheduled at 3 and 12 months after surgery.
Results: Total reflux decreased from 16.3% before sur-gery to 3.5% 3 months after surgery (P = .001). The reflux score decreased from 3.8 before surgery to 2.1 1 year after surgery (P = .001). The respective values of the indi-gestion score were 3.4 and 2.0 (P < .001). After surgery, all patients were able to belch. Vomiting was impossible only for 2 patients, and 90% of patients assessed their results as good to excellent.
Conclusions: LMAH seems to be feasible, safe, and has no significant side effects.
Am J Surg. 2008; 195: 749-756 IF (2008) 2.337
Diseases of the Colon and Rectum
Clinical and Morphologic Correla-tion after Stapled Transanal Rectal Resection for Obstructed Defecation Syndrome
Dindo D, Weishaupt D, Lehmann K, Hetzer FH, Clavien PA, Hahnloser D
Dis Colon Rect. 2008; (Epub ahead of print) IF (2007) 2.621
Department of Surgery, Division of Visceral and Trans-plantation Surgery, University Hospital Zurich
Background: The clinical and morphologic outcome of patients with obstructed defecation syndrome after stapled transanal rectal resection was prospectively eva-luated.
Methods: Twenty-four consecutive patients (22 women; median age, 61 (range, 36-74) years) who suffered from obstructed defecation syndrome and with rectal redun-dancy on magnetic resonance defecography were en-rolled in the study. Constipation was assessed by using the Cleveland Constipation Score. Morphologic changes were determined by using closed-configuration magnetic resonance defecography before and after stapled transa-nal rectal resection.
Results: After a median follow-up of 18 (range, 6-36) months, Cleveland Constipation Score significantly de-creased from 11 (range, 1-23) preoperatively to 5 (range, 1-15) postoperatively (P = 0.02). In 15 of 20 patients, pre-existing intussusception was no longer visible in the ma-gnetic resonance defecography. Anterior rectoceles were significantly reduced in depth, from 30 mm to 23 mm (P = 0.01), whereas the number of detectable rectoceles did not significantly change. Complications occurred in 6 of the 24 patients; however, only two were severe (1 blee-ding and 1 persisting pain requiring reintervention).
Conclusions: Clinical improvement of obstructed defe-cation syndrome after stapled transanal rectal resection correlates well with morphologic correction of the rec-tal redundancy, whereas correction of intussusception seems to be of particular importance in patients with obstructed defecation syndrome.

Das Magazin
der Zentralbahn
Winter 2007/2008, Ausgabe Nr. 2
WelcomeWelcomeWelcomeWelcome
LEADER
Juni/Juli 2008 ıı 1
hintergrund
DAS UNTERNEHMERMAGAZIN
Das kleine GrosseErfolgsgeschichte Appenzellerland:Karg im Umgang mit Luxus, aberreich im Erfinden von Produkten. seite 57
Top-Leader 2008:Konrad Hummler «Strukturverteidiger gibtes genug» seite 8
Werner Signer,Direktor Konzert und Theater St.Gallen«Sie können Skandale nicht programmieren» seite 40
Ausgabe für die Ostschweiz und das Fürstentum Liechtensteinwww.leaderonline.ch Preis Fr. 8.50
Juni/
06 2
008

Stryker Osteonics SA Swiss Sales & Distribution, CP 916, CH-1212 Grand-Lancy 1 / GETel. +4122 884 0120, Fax. +4122 794 7304 www.stryker.chThis advertisement is intended solely for the use of healthcare professionals. The information presented in this advertisement is intended to demonstrate the breadth of Stryker product offerings. Always refer to the package insert, product label and/or user instructions before using any Stryker product. Products may not be available in all markets. Product availability is subject to the regulatory or medical practices that govern individual markets. Please contact your Stryker representative if you have questions about the availability of Stryker products in your area. Products referenced with ™ designation are trademarks of Stryker. Products referenced with ® designation are registered trademarks of Stryker.
Ihr Kompetenzpartner
Precision saw
Variax system
Endoscopy tower