
Seite 1 von 25 182/001: In -flight Cardiopulmonary ... · Seite 2 von 25 182/001: In -flight...
25
Seite 1 von 25 182/001: In-flight Cardiopulmonary Resuscitation Reference 12 Study design Participants Drop out rate Intervention Control Primary endpoint Main result Comment Brown A, Rittenberger J, Ammon C, Harrington S, Guyette F. In- flight automated external defibrillator use and consultation patterns. Prehosp Emerg Care. 2010;14(2):235- 239. Retrospective analysis of data Data from a total of 169 AED applications with 40 cardiac arrests. N/A N/A N/A Use of AED during flight Use of AEDs resulted in 50% survival among those with VF/VT in flight and 15% overall survival for cardiac arrest. Limitations: serious Inconsistency: Non-serious Indirectness: Non-serious Imprecision: Non-serious Evidence: low Conclusion: Use of AEDs resulted in 50% survival among those with VF/VT in flight and 15% overall survival for cardiac arrest.
Transcript of Seite 1 von 25 182/001: In -flight Cardiopulmonary ... · Seite 2 von 25 182/001: In -flight...

Seite 1 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 12
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Brown A, Rittenberger J, Ammon C, Harrington S, Guyette F. In-flight automated external defibrillator use and consultation patterns. Prehosp Emerg Care. 2010;14(2):235-239.
Retrospective analysis of data
Data from a total of 169 AED applications with 40 cardiac arrests.
N/A
N/A
N/A
Use of AED during flight
Use of AEDs resulted in 50% survival among those with VF/VT in flight and 15% overall survival for cardiac arrest.
Limitations: serious Inconsistency: Non-serious Indirectness: Non-serious Imprecision: Non-serious Evidence: low
Conclusion: Use of AEDs resulted in 50% survival among those with VF/VT in flight and 15% overall survival for cardiac arrest.

Seite 2 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 25
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Mahony P, Griffiths R, Larsen P, Powell D. Retention of knowledge and skills in first aid and resuscitation by airline cabin crew. Resuscitation. 2008;76(3):413-418
Prospective observational study
35 cabin crew
N/A
use the bag-mask correctly, perform CPR, and place AED
N/A
Correct use of the bag-mask, perform CPR, and place AED
The results of this study indicate that cabin crew may not have sufficiently high levels of skill to manage a cardiac arrest adequately
Limitations: Serious Inconsistency: none Indirectness: none Imprecision: none Evidence: moderate
Conclusion: While theoretical first aid knowledge was high, the participants held low levels of self-confidence in their CPR and AED skills. The results of this study indicate that cabin crew may not have sufficiently high levels of skill to manage a cardiac arrest adequately.
Seite 3 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 26
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
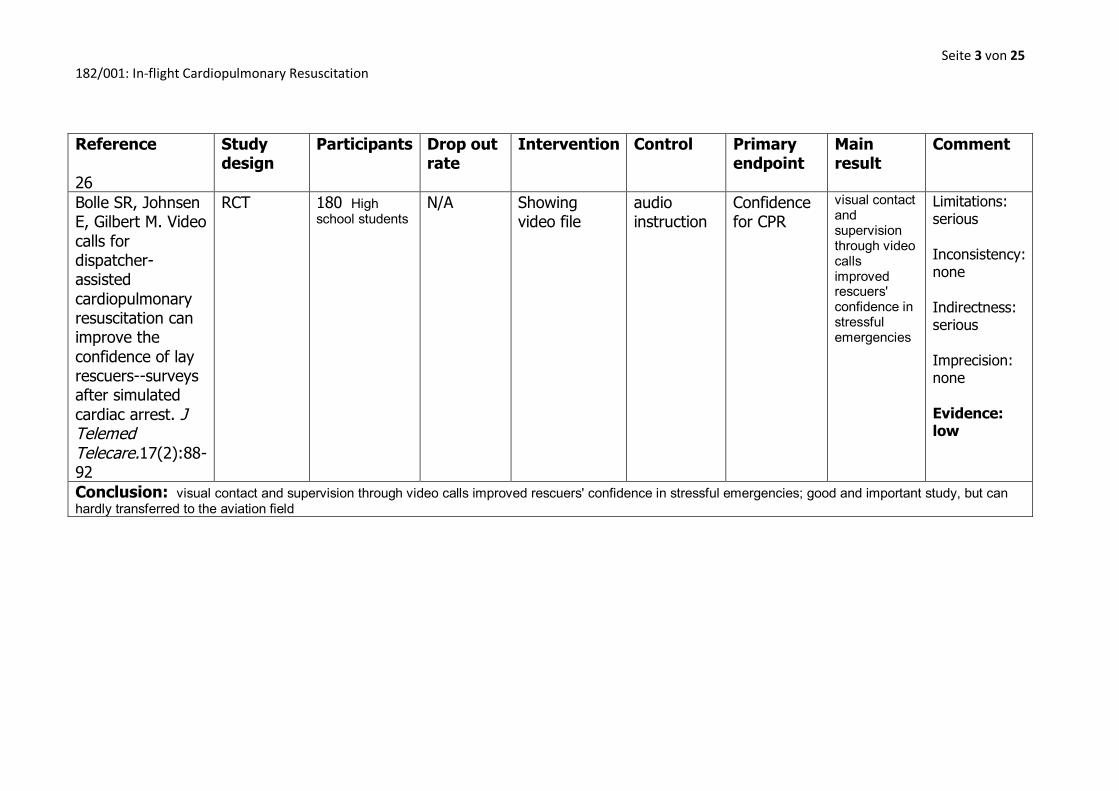
Bolle SR, Johnsen E, Gilbert M. Video calls for dispatcher-assisted cardiopulmonary resuscitation can improve the confidence of lay rescuers--surveys after simulated cardiac arrest. J Telemed Telecare.17(2):88-92
RCT
180 High school students
N/A
Showing video file
audio instruction
Confidence for CPR
visual contact and supervision through video calls improved rescuers' confidence in stressful emergencies
Limitations: serious Inconsistency: none Indirectness: serious Imprecision: none Evidence: low
Conclusion: visual contact and supervision through video calls improved rescuers' confidence in stressful emergencies; good and important study, but can hardly transferred to the aviation field
Seite 4 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 28
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
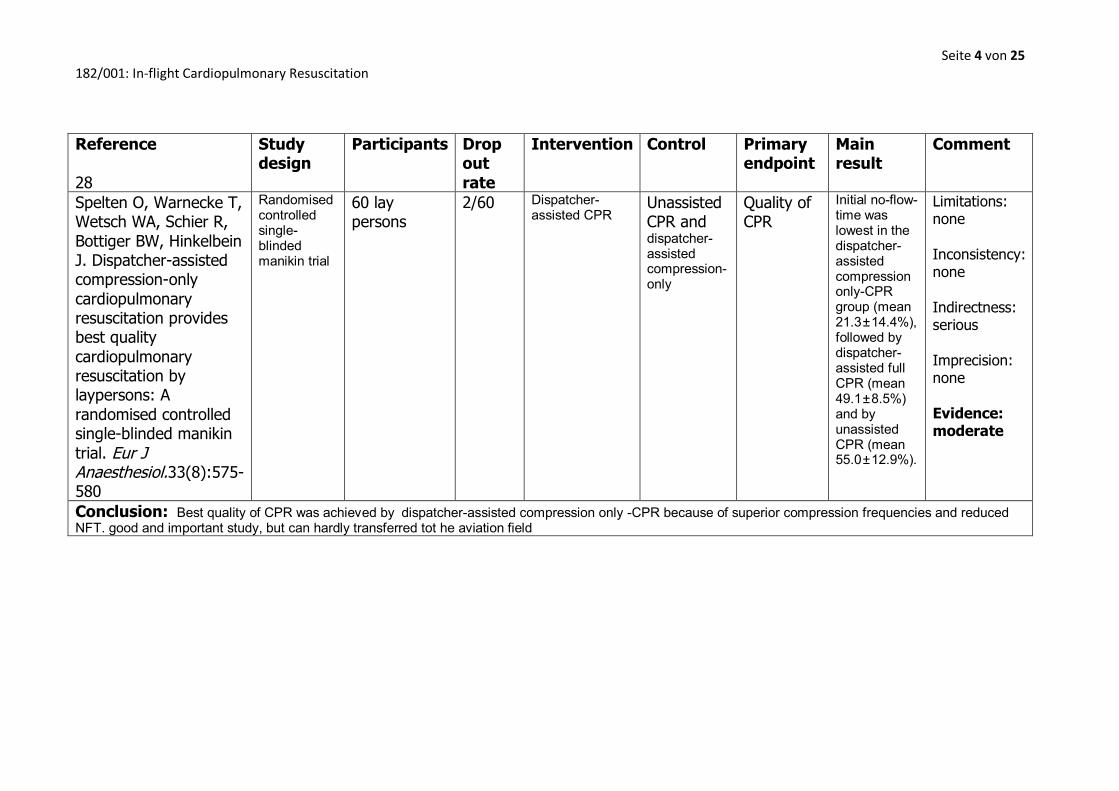
Spelten O, Warnecke T, Wetsch WA, Schier R, Bottiger BW, Hinkelbein J. Dispatcher-assisted compression-only cardiopulmonary resuscitation provides best quality cardiopulmonary resuscitation by laypersons: A randomised controlled single-blinded manikin trial. Eur J Anaesthesiol.33(8):575-580
Randomised controlled single-blinded manikin trial
60 lay persons
2/60 Dispatcher-assisted CPR Unassisted
CPR and dispatcher-assisted compression-only
Quality of CPR
Initial no-flow-time was lowest in the dispatcher-assisted compression only-CPR group (mean 21.3 ± 14.4%), followed by dispatcher-assisted full CPR (mean 49.1 ± 8.5%) and by unassisted CPR (mean 55.0 ± 12.9%).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: Best quality of CPR was achieved by dispatcher-assisted compression only -CPR because of superior compression frequencies and reduced NFT. good and important study, but can hardly transferred tot he aviation field

Seite 5 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 39
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Page R, Joglar J, Kowal R, Zagrodzky J, Nelson L, Ramaswamy K, Barbera S, Hamdan M, McKenas D. Use of automated external defibrillators by a U.S. airline. N Engl J Med. 2000;343(1210-1216)
Retrospective analysis
Data of 200 patients
N/A
N/A
N/A
Use of an AED
The rate of survival to discharge from the hospital after shock with the automated external defibrillator was 40 percent
Limitations: serious Inconsistency: none Indirectness: none Imprecision: none Evidence: low
Conclusion: The use of the automated external defibrillator aboard commercial aircraft is effective, with an excellent rate of survival to discharge from the hospital after conversion of ventricular fibrillation.
Seite 6 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 42
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
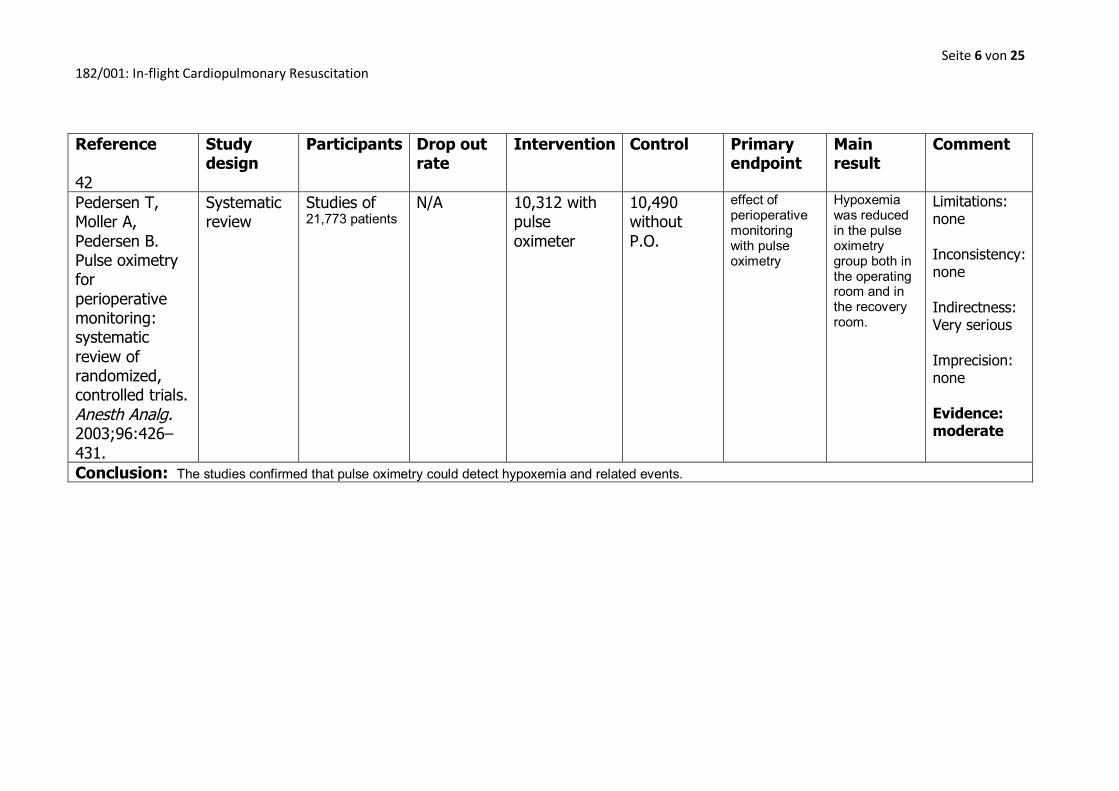
Pedersen T, Moller A, Pedersen B. Pulse oximetry for perioperative monitoring: systematic review of randomized, controlled trials. Anesth Analg. 2003;96:426–431.
Systematic review
Studies of 21,773 patients
N/A
10,312 with pulse oximeter
10,490 without P.O.
effect of perioperative monitoring with pulse oximetry
Hypoxemia was reduced in the pulse oximetry group both in the operating room and in the recovery room.
Limitations: none Inconsistency: none Indirectness: Very serious Imprecision: none Evidence: moderate
Conclusion: The studies confirmed that pulse oximetry could detect hypoxemia and related events.

Seite 7 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 44
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Havel C, Schreiber W, Riedmuller W, Haugk M, Richling N, Trimmel H, Malzer R, Sterz F, Herkner H. Quality of closed chest compression in ambulance vehicles, flying helicopters and at the scene. Resuscitation. 2007;73:264—270
randomised cross-over trial
11 European Resuscitation Council (ERC) approved health care professionals
N/A
Interventions during resuscitation: (a) in a moving ambulance, (b) in a flying helicopter, were compared to those staying at the (c) scene (control).
N/A
Direct comparison of the quality of resuscitation at the scene, during a helicopter flight and in a moving ambulance
Compared to resuscitation at the scene, efficiency of chest compressions during a helicopter flight was 86% and 95% in the moving ambulance 95%.
Limitations: none Inconsistency: none Indirectness: none Imprecision: none
Evidence: high
Conclusion: Resuscitation during transport is feasible and relatively efficient. There is some difference between the environments, but there is no relevant difference between helicopters and ambulances regarding the effectiveness of CPR.
Seite 8 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 45
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
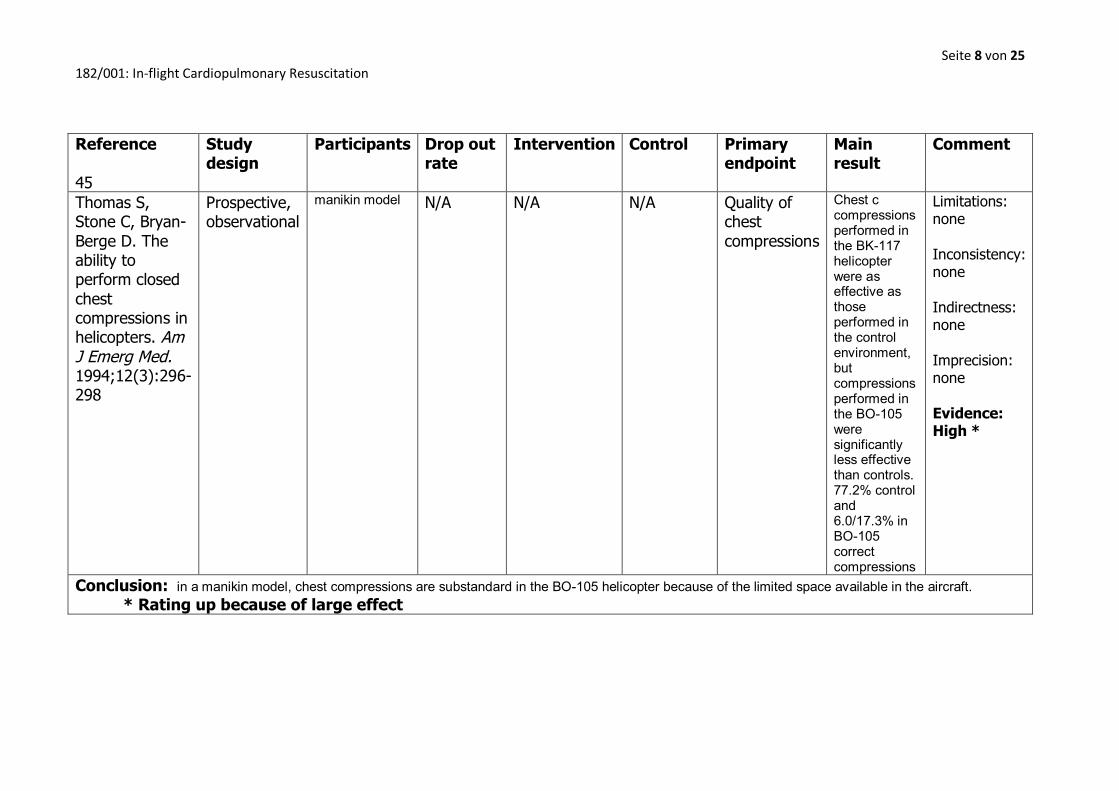
Thomas S, Stone C, Bryan-Berge D. The ability to perform closed chest compressions in helicopters. Am J Emerg Med. 1994;12(3):296-298
Prospective, observational
manikin model
N/A N/A N/A Quality of chest compressions
Chest c compressions performed in the BK-117 helicopter were as effective as those performed in the control environment, but compressions performed in the BO-105 were significantly less effective than controls. 77.2% control and 6.0/17.3% in BO-105 correct compressions
Limitations: none Inconsistency: none Indirectness: none Imprecision: none Evidence: High *
Conclusion: in a manikin model, chest compressions are substandard in the BO-105 helicopter because of the limited space available in the aircraft. * Rating up because of large effect

Seite 9 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 46
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Handley A, Handley J. Performing chest compressions in a confined space. Resuscitation. 2004;61:55-61
Prospective observational study
Nineteen airline employees
N/A
one-person over-the-head
two-person straddle
Quality of CPR
There were no statistically significant differences between the one-person methods of chest compression (St-1 and OTH) for the average compression rate, the number of chest compressions achieved in a minute, or the average hands-off time per cycle
Limitations: none Inconsistency: none Indirectness: none Imprecision: none Evidence: low
Conclusion: in this study, hand placement during chest compression was poor, and additional training may be necessary before it can be considered a safe technique.

Seite 10 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 47
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Perkins G, Stephenson B, Smith C, Gao F. A comparison between over-the-head and standard cardiopulmonary resuscitation. Resuscitation. 2004;61(2):155-161
RCT
Twenty volunteers
N/A
OTH CPR
Standard CPR
Quality of CPR
Chest compression depth and ventilation volume declined over time (0-3 min P < 0.001). There was no difference in compression rate, depth, duty cycle or ventilation rate, inflation rate and ventilation volume between techniques
Limitations: none Inconsistency: none Indirectness: none Imprecision: none Evidence: high
Conclusion: OTH CPR appears equally effective as standard CPR with some marginal advantages in correct hand placement.

Seite 11 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 48
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
McIntosh S, Swanson E, McKeone A, Barton E. Location of airway management in air medical transport. Prehosp Emerg Care. 2008;12(4):438-442
Retrospective analysis
Patient records of nine hundred thirty-eight patients
N/A
N/A
N/A
Success rate of airway management
Airway management was performed with a high success rate in a variety of locations and patient characteristics by our air medical crew.
Limitations: serious Inconsistency: none Indirectness: none Imprecision: none Evidence: low
Conclusion: Caution should be used, however, when considering intubating in-flight because of slightly lower success rates.
Seite 12 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 50
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
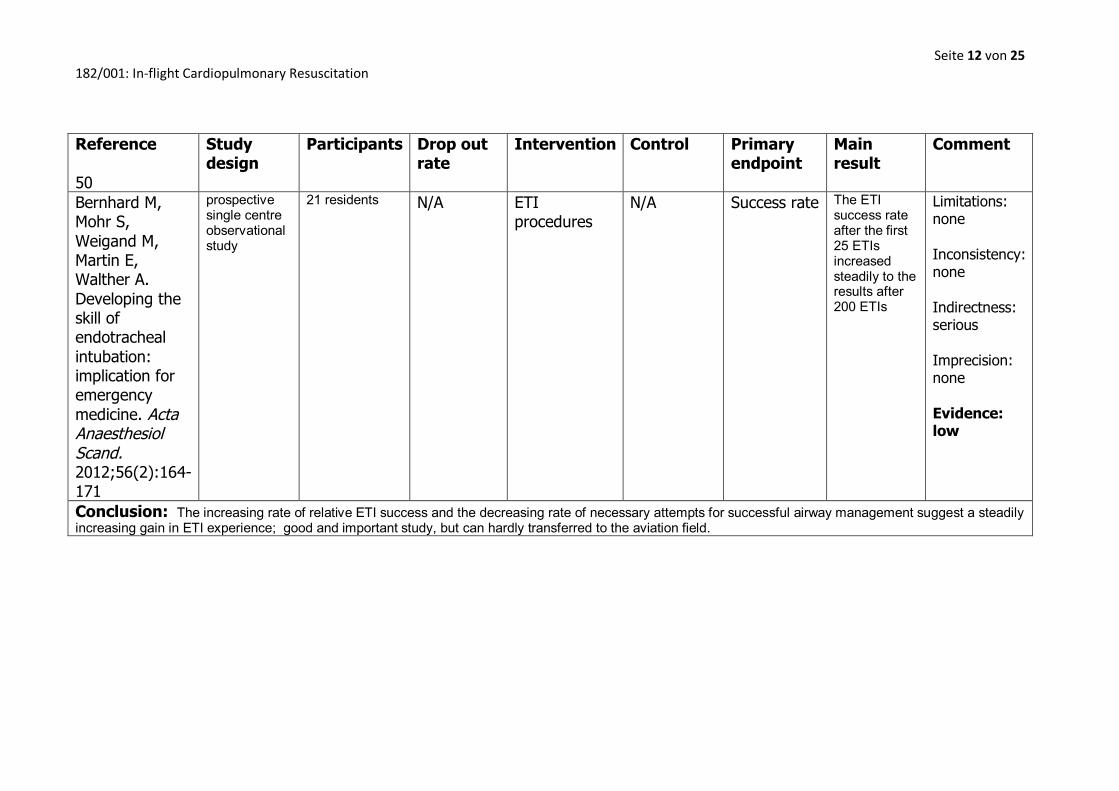
Bernhard M, Mohr S, Weigand M, Martin E, Walther A. Developing the skill of endotracheal intubation: implication for emergency medicine. Acta Anaesthesiol Scand. 2012;56(2):164-171
prospective single centre observational study
21 residents
N/A
ETI procedures
N/A
Success rate
The ETI success rate after the first 25 ETIs increased steadily to the results after 200 ETIs
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: low
Conclusion: The increasing rate of relative ETI success and the decreasing rate of necessary attempts for successful airway management suggest a steadily increasing gain in ETI experience; good and important study, but can hardly transferred to the aviation field.

Seite 13 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 51
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Mohr S, Weigand M, Hofer S, Martin E, Gries A, Walther A, Bernhard M. Developing the skill of laryngeal mask insertion. Anaesthesist. 2013;62:447-452
This prospective single center observational study
10 anesthesiology resident physicians
N/A
Success rate
N/A
Success rate
The LMI success rate after the first 5 LMIs increased steadily up to the results after 40 LMIs per resident
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: low
Conclusion: The increasing LMI success rate and the decreasing rate of LMI attempts for successful airway management correlated to a learning curve and development of LMI dexterity over time; good and important study, but can hardly transferred to the aviation field.

Seite 14 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 52
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Berden H, Bierens J, Willems F, Hendrick J, Pijls N, Knape J. Resuscitation skills of lay public after recent training. Ann Intern Med. 1994;23(5):1003-1008
Cross-sectional assessment of practical CPR skills
151 laypeople who were trained twice in the preceding 20 to 24 months
N/A
CPR
N/A
six primary recorded variables that describe the quality of CPR techniques in a training situation
Thirty-three percent of the participants were able to perform adequate CPR. The compression:relaxation ratio, the breathing volume, and the breathing interval were points of concern
Limitations: severe Inconsistency: none Indirectness: none Imprecision: none Evidence: low
Conclusion: Practical skills in basic CPR after a 12-month training interval, though better in this study than in many previous studies, are insufficient in the majority of laypeople.

Seite 15 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 53
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Abella B, Sandbro N, Vassilatos P, et a. Chest compression rates during cardiopulmonary resuscitation are suboptimal — a prospective study during in-hospital cardiac arrest. Circulation. 2005;111(428-434)
prospective observational study
various
N/A
N/A
N/A
CPR quality
In 36.9% of the total number of segments, compression rates were <80 compressions per minute (cpm), and 21.7% had rates <70 cpm.
Limitations: None Inconsistency: none Indirectness: Very serious Imprecision: none Evidence: Very low
Conclusion: In-hospital chest compression rates were below published resuscitation recommendations, and suboptimal compression rates in our study correlated with poor return of spontaneous circulation. good and important study, but can hardly transferred to the aviation field.
Seite 16 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 55
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
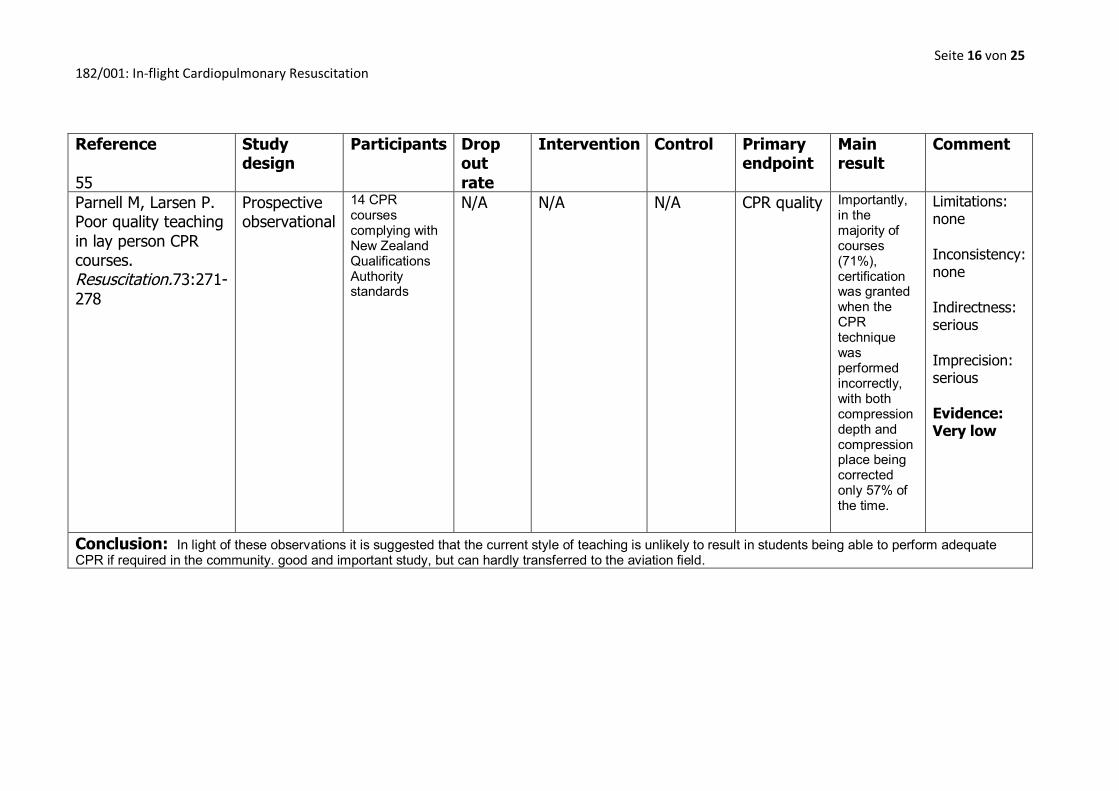
Parnell M, Larsen P. Poor quality teaching in lay person CPR courses. Resuscitation.73:271-278
Prospective observational
14 CPR courses complying with New Zealand Qualifications Authority standards
N/A
N/A
N/A
CPR quality
Importantly, in the majority of courses (71%), certification was granted when the CPR technique was performed incorrectly, with both compression depth and compression place being corrected only 57% of the time.
Limitations: none Inconsistency: none Indirectness: serious Imprecision: serious Evidence: Very low
Conclusion: In light of these observations it is suggested that the current style of teaching is unlikely to result in students being able to perform adequate CPR if required in the community. good and important study, but can hardly transferred to the aviation field.

Seite 17 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 56
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Kaye W, Wynne G, Marteau T, et a. An advanced resuscitation course for pre-registration house officers. J R Coll Phys Lond. 1990;24(1):51-54
two consecutive groups
Fifty-nine newly qualified doctors
N/A
N/A
N/A
Quality of CPR
The knowledge and skills of both groups immediately after training were significantly improved and at 5 months skills were subject to modest decay only
Limitations: None Inconsistency: none Indirectness: Very serious Imprecision: none Evidence: Very low
Conclusion: Experience of managing cardiac arrests was not a substitute for formal practical training. This study can hardly transferred to the aviation field.
Seite 18 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 58
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
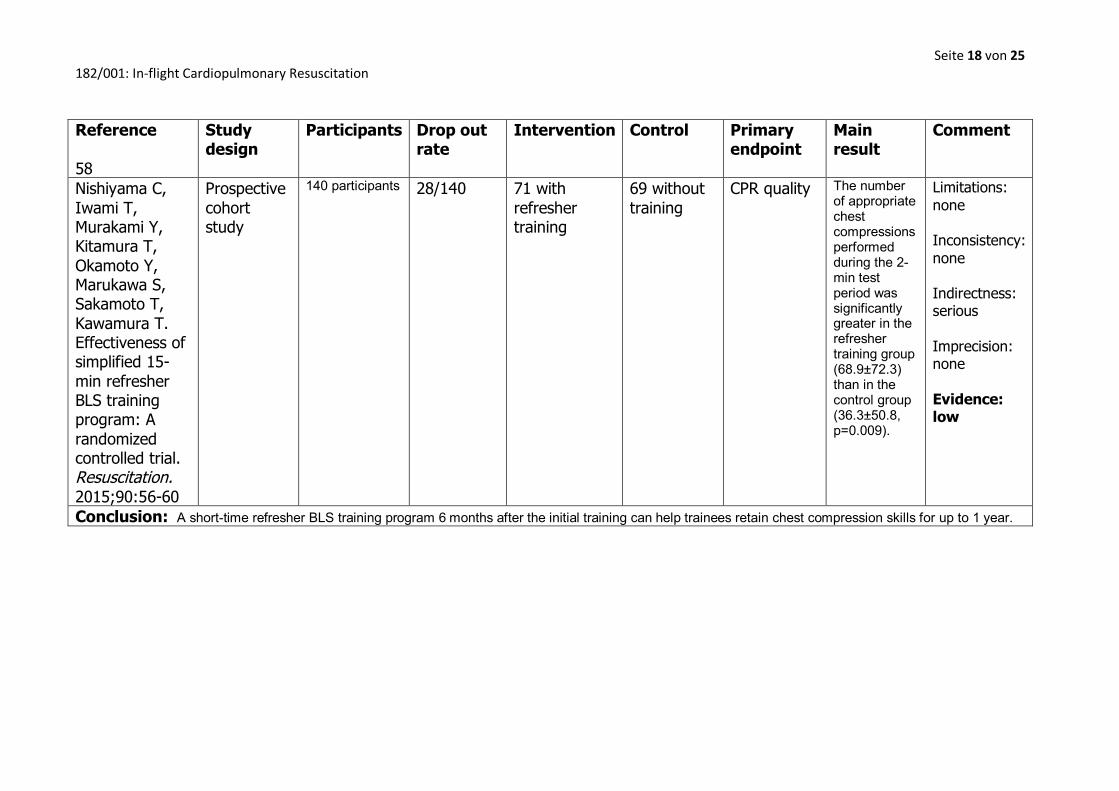
Nishiyama C, Iwami T, Murakami Y, Kitamura T, Okamoto Y, Marukawa S, Sakamoto T, Kawamura T. Effectiveness of simplified 15-min refresher BLS training program: A randomized controlled trial. Resuscitation. 2015;90:56-60
Prospective cohort study
140 participants
28/140
71 with refresher training
69 without training
CPR quality
The number of appropriate chest compressions performed during the 2-min test period was significantly greater in the refresher training group (68.9±72.3) than in the control group (36.3±50.8, p=0.009).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: low
Conclusion: A short-time refresher BLS training program 6 months after the initial training can help trainees retain chest compression skills for up to 1 year.
Seite 19 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 59
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
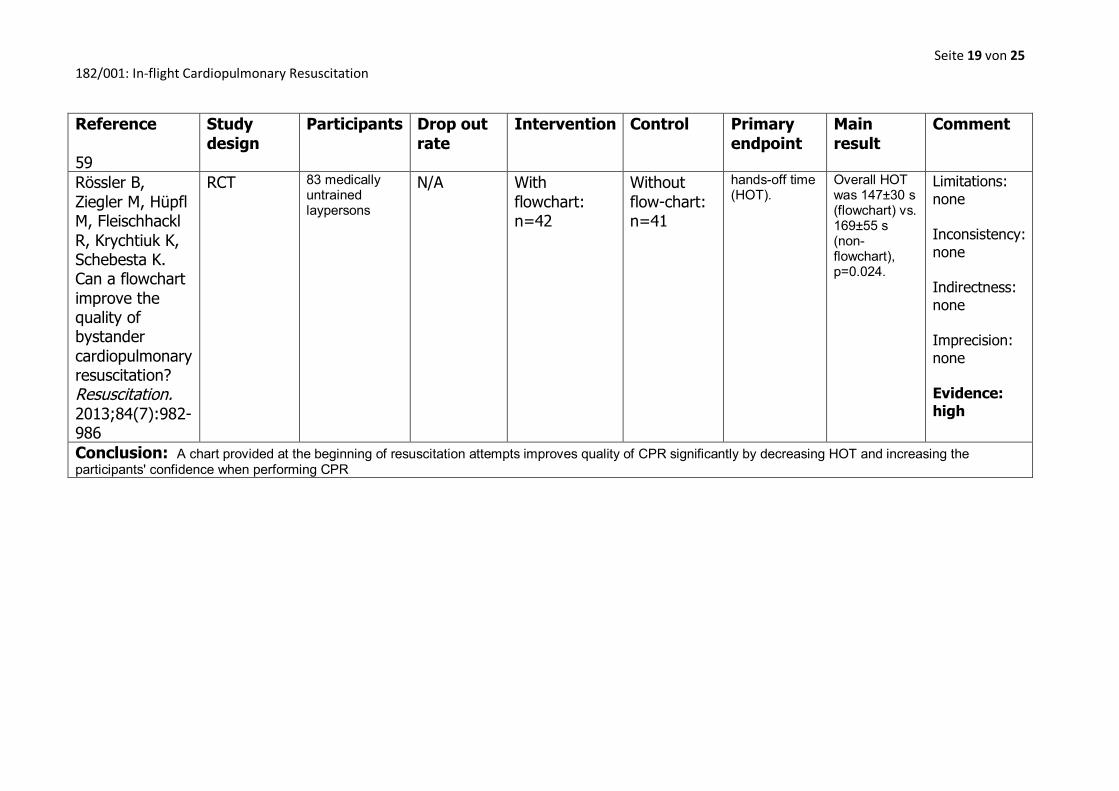
Rössler B, Ziegler M, Hüpfl M, Fleischhackl R, Krychtiuk K, Schebesta K. Can a flowchart improve the quality of bystander cardiopulmonary resuscitation? Resuscitation. 2013;84(7):982-986
RCT
83 medically untrained laypersons
N/A
With flowchart: n=42
Without flow-chart: n=41
hands-off time (HOT).
Overall HOT was 147±30 s (flowchart) vs. 169±55 s (non-flowchart), p=0.024.
Limitations: none Inconsistency: none Indirectness: none Imprecision: none Evidence: high
Conclusion: A chart provided at the beginning of resuscitation attempts improves quality of CPR significantly by decreasing HOT and increasing the participants' confidence when performing CPR

Seite 20 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 64
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Kilgannon J, Jones A, Parrillo J, Dellinger R, Milcarek B, Hunter K, Shapiro N, Trzeciak S. Relationship Between Supranormal Oxygen Tension and Outcome After Resuscitation From Cardiac Arrest. Circulation. 2011;123:2717-2722
multicenter retrospective cohort study
IMPACT database, 4459 patients
N/A
4459 patients
N/A
in-hospital mortality
Over ascending ranges of oxygen tension, we found significant linear trends of increasing in-hospital mortality and decreasing survival as functionally independent.
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: In this large sample of postresuscitation patients, we found a dose-dependent association between supranormal oxygen tension and risk of in-hospital death. good and important study, but can hardly transferred to the aviation field.

Seite 21 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 65
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Kilgannon J, Jones A, Shapiro N, Angelos M, Milcarek B, Hunter K, Parrillo J, Trzeciak S. Association Between Arterial Hyperoxia Following Resuscitation From Cardiac Arrest and In-Hospital Mortality. J Am Med Assoc. 2010;303(21):2165-2171
Multicenter retrospective cohort study
6326 patients in IMPACT critical care database
N/A
6326 patients
N/A
In-hospital mortality
The hyperoxia group had significantly higher in-hospital mortality (732/1156 [63%; 95% confidence interval {CI}, 60%-66%]) compared with the normoxia group (532/1171 [45%; 95% CI, 43%-48%]; proportion difference, 18% [95% CI, 14%-22%]) and the hypoxia group (2297/3999 [57%; 95% CI, 56%-59%]; proportion difference, 6% [95% CI, 3%-9%]).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: Among patients admitted to the ICU following resuscitation from cardiac arrest, arterial hyperoxia was independently associated with increased in-hospital mortality compared with either hypoxia or normoxia. good and important study, but can hardly transferred to the aviation field.

Seite 22 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 68
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Hinkelbein J, Glaser E, Doerrstein J, Genzwuerker H. Oxygen delivery comparison of two constant-flow masks during flight to 6863 m. Aviat Space Environ Med. 2006;77(5):540-544
RCT
parachutists (n=31)
8/31
HiOx mask (TST) n=17
Basic mask (BAS) n=14
oxygen saturation (SpO2)
Above 3965 m (13,000 ft) the TST required significantly less oxygen flow than the BAS to maintain the target SpO2. At 6863 m (22,500 ft), mean oxygen flow was 5.5 +/- 3.5 L x min(-1) for the BAS vs. 3.4 +/- 2.3 L x min(-1) for the TST (p = 0.029).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: The TST required significantly less oxygen flow compared with the BAS at high altitudes and may, therefore, reduce total oxygen use, resulting in reduced costs and longer oxygen availability during a flight
Seite 23 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 70
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
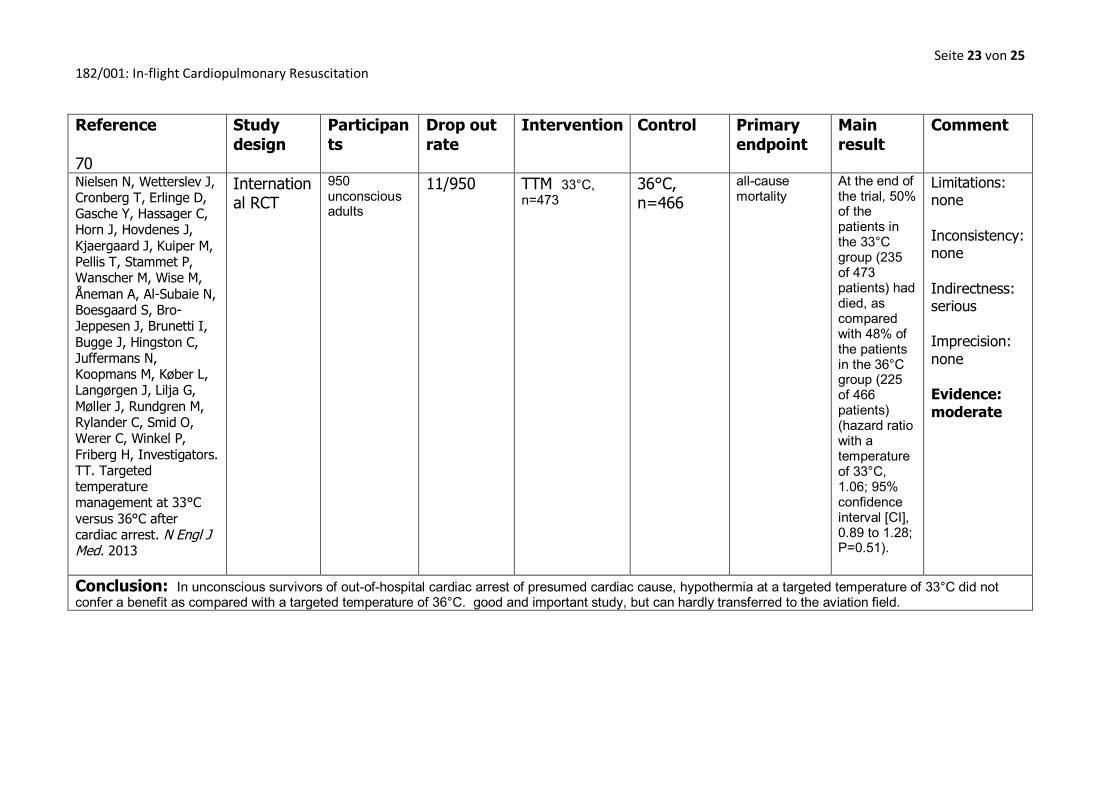
Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise M, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge J, Hingston C, Juffermans N, Koopmans M, Køber L, Langørgen J, Lilja G, Møller J, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H, Investigators. TT. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013
International RCT
950 unconscious adults
11/950
TTM 33°C, n=473
36°C, n=466
all-cause mortality
At the end of the trial, 50% of the patients in the 33°C group (235 of 473 patients) had died, as compared with 48% of the patients in the 36°C group (225 of 466 patients) (hazard ratio with a temperature of 33°C, 1.06; 95% confidence interval [CI], 0.89 to 1.28; P=0.51).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: In unconscious survivors of out-of-hospital cardiac arrest of presumed cardiac cause, hypothermia at a targeted temperature of 33°C did not confer a benefit as compared with a targeted temperature of 36°C. good and important study, but can hardly transferred to the aviation field.

Seite 24 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 71
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
Bro-Jeppesen J, Hassager C, Wanscher M, et al. Post-hypothermia fever is associated with increased mortality after out-of-hospital cardiac arrest. Resuscitation. 2013;84(1734-1740)
consecutive cohort of comatose survivors
270 patients resuscitated after OHCA
N/A
Cooling, no PHF, n=134
No cooling, PHF, n=136
30-days mortality
PHF (≥38.5°C) was associated with a 36% 30-days mortality rate compared to 22% in patients without PHF, plog-rank=0.02, corresponding to an adjusted hazard rate (HR) of 1.8 (95% CI: 1.1-2.7), p=0.02).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: Post-hypothermia fever ≥38.5°C is associated with increased 30-days mortality, even after controlling for potential confounding factors. Avoidance of PHF as a therapeutic target should be evaluated in prospective randomized trials. good and important study, but can hardly transferred to the aviation field.
Seite 25 von 25 182/001: In-flight Cardiopulmonary Resuscitation
Reference 72
Study design
Participants
Drop out rate
Intervention
Control
Primary endpoint
Main result
Comment
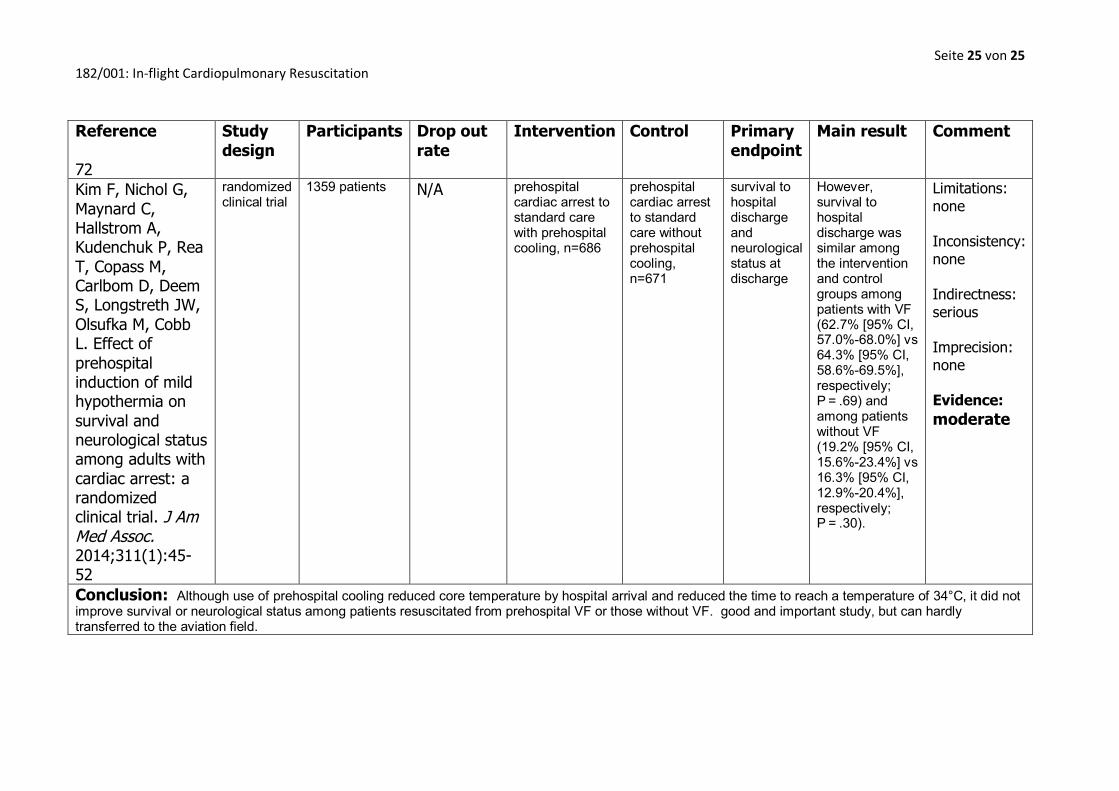
Kim F, Nichol G, Maynard C, Hallstrom A, Kudenchuk P, Rea T, Copass M, Carlbom D, Deem S, Longstreth JW, Olsufka M, Cobb L. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. J Am Med Assoc. 2014;311(1):45-52
randomized clinical trial
1359 patients
N/A
prehospital cardiac arrest to standard care with prehospital cooling, n=686
prehospital cardiac arrest to standard care without prehospital cooling, n=671
survival to hospital discharge and neurological status at discharge
However, survival to hospital discharge was similar among the intervention and control groups among patients with VF (62.7% [95% CI, 57.0%-68.0%] vs 64.3% [95% CI, 58.6%-69.5%], respectively; P = .69) and among patients without VF (19.2% [95% CI, 15.6%-23.4%] vs 16.3% [95% CI, 12.9%-20.4%], respectively; P = .30).
Limitations: none Inconsistency: none Indirectness: serious Imprecision: none Evidence: moderate
Conclusion: Although use of prehospital cooling reduced core temperature by hospital arrival and reduced the time to reach a temperature of 34°C, it did not improve survival or neurological status among patients resuscitated from prehospital VF or those without VF. good and important study, but can hardly transferred to the aviation field.















![Flight! Magazin - Flight! März 2012 [CLASSICS]](https://static.fdokument.com/doc/165x107/568ca7871a28ab186d95bb74/flight-magazin-flight-maerz-2012-classics.jpg)