
Systemerkrankungen mit Nierenbeteiligung - niere …€¦ · Renal involvement in autoimmune...
28
Systemerkrankungen mit Nierenbeteiligung ÖGN Fuschl 2014 Irmgard Neumann
-
Upload
trinhduong -
Category
Documents
-
view
220 -
download
0
Transcript of Systemerkrankungen mit Nierenbeteiligung - niere …€¦ · Renal involvement in autoimmune...

Systemerkrankungen mit
Nierenbeteiligung
ÖGN Fuschl 2014
Irmgard Neumann
Renale Beteiligung bei rheumatoiden Erkrankungen Vaskulitis und Lupus Nephritis
- Rezente Arbeiten - Unbeantwortete Fragen
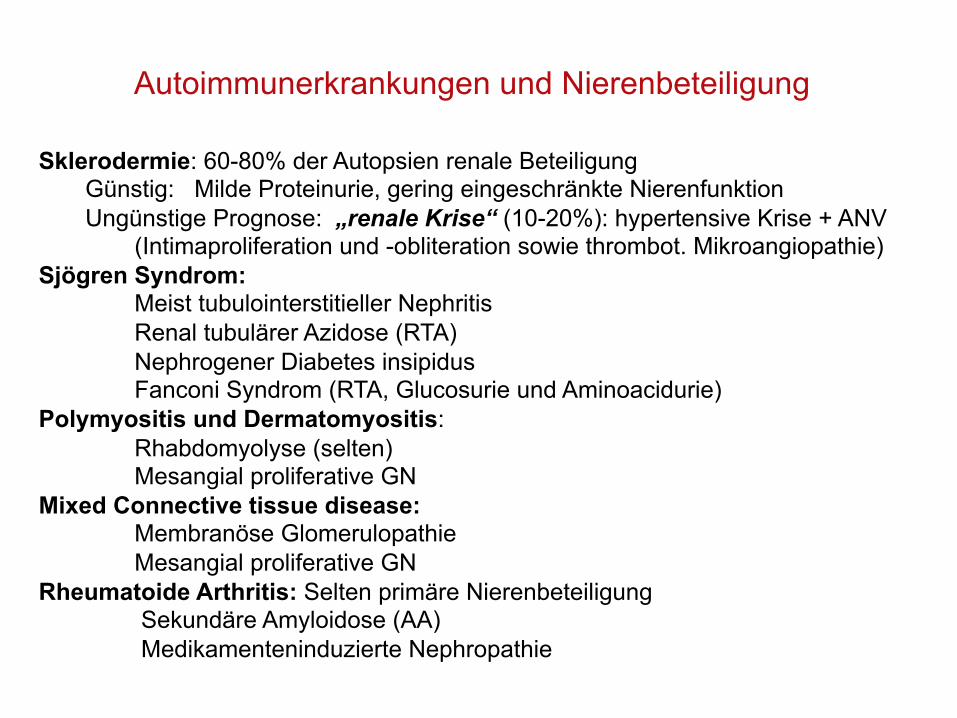
Sklerodermie: 60-80% der Autopsien renale Beteiligung Günstig: Milde Proteinurie, gering eingeschränkte Nierenfunktion Ungünstige Prognose: „renale Krise“ (10-20%): hypertensive Krise + ANV
(Intimaproliferation und -obliteration sowie thrombot. Mikroangiopathie) Sjögren Syndrom:
Meist tubulointerstitieller Nephritis Renal tubulärer Azidose (RTA) Nephrogener Diabetes insipidus Fanconi Syndrom (RTA, Glucosurie und Aminoacidurie)
Polymyositis und Dermatomyositis: Rhabdomyolyse (selten) Mesangial proliferative GN
Mixed Connective tissue disease: Membranöse Glomerulopathie Mesangial proliferative GN
Rheumatoide Arthritis: Selten primäre Nierenbeteiligung Sekundäre Amyloidose (AA) Medikamenteninduzierte Nephropathie
Autoimmunerkrankungen und Nierenbeteiligung
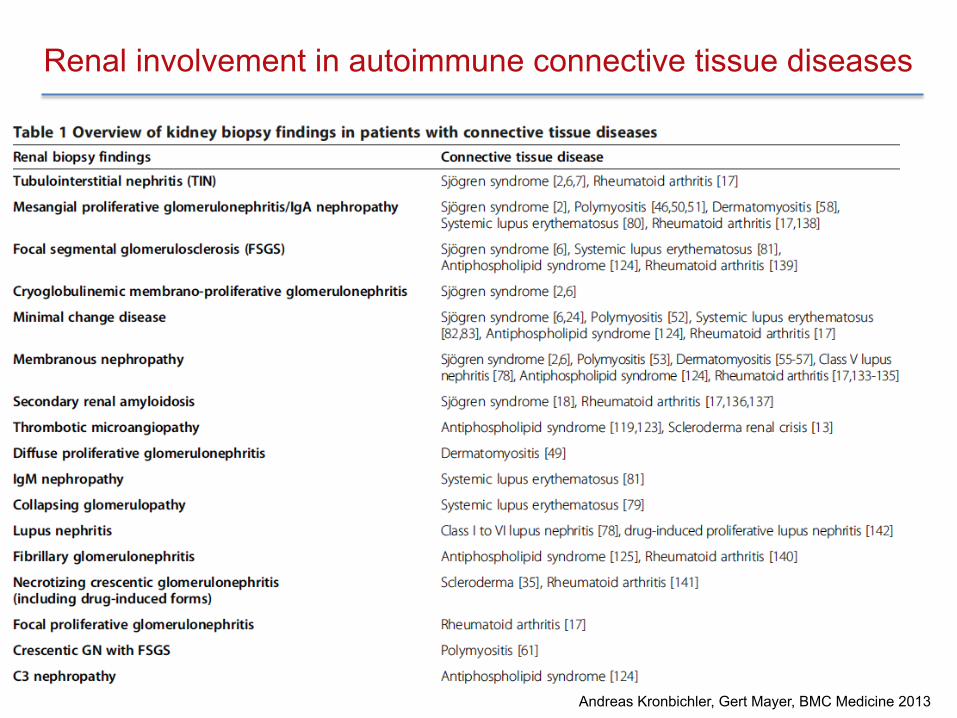
Renal involvement in autoimmune connective tissue diseases
Andreas Kronbichler, Gert Mayer, BMC Medicine 2013
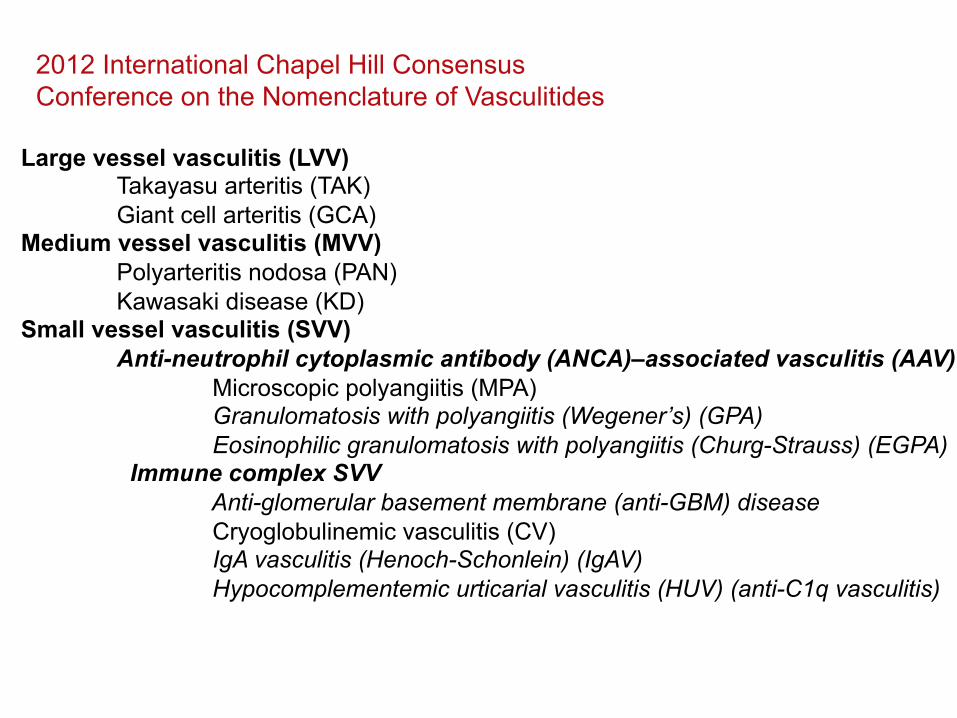
Large vessel vasculitis (LVV)
Takayasu arteritis (TAK) Giant cell arteritis (GCA)
Medium vessel vasculitis (MVV) Polyarteritis nodosa (PAN) Kawasaki disease (KD)
Small vessel vasculitis (SVV) Anti-neutrophil cytoplasmic antibody (ANCA)–associated vasculitis (AAV) Microscopic polyangiitis (MPA) Granulomatosis with polyangiitis (Wegener’s) (GPA) Eosinophilic granulomatosis with polyangiitis (Churg-Strauss) (EGPA) Immune complex SVV Anti-glomerular basement membrane (anti-GBM) disease Cryoglobulinemic vasculitis (CV) IgA vasculitis (Henoch-Schonlein) (IgAV) Hypocomplementemic urticarial vasculitis (HUV) (anti-C1q vasculitis)
2012 International Chapel Hill Consensus Conference on the Nomenclature of Vasculitides
Variable vessel vasculitis (VVV) Behcet’s disease (BD) Cogan’s syndrome (CS)
Single-organ vasculitis (SOV) Cutaneous leukocytoclastic angiitis Cutaneous arteritis Primary central nervous system vasculitis Isolated aortitis
Vasculitis associated with systemic disease Lupus vasculitis Rheumatoid vasculitis Sarcoid vasculitis
Vasculitis associated with probable etiology Hepatitis C virus–associated cryoglobulinemic vasculitis Hepatitis B virus–associated vasculitis Syphilis-associated aortitis Drug-associated immune complex vasculitis Drug-associated ANCA-associated vasculitis Cancer-associated vasculitis
2012 International Chapel Hill Consensus Conference on the Nomenclature of Vasculitides
Renale Beteiligung bei rheumatoiden Erkrankungen Vaskulitis und Lupus Nephritis
- Rezente Studien - Unbeantwortete Fragen
AAV- Unanswered Questions
• Rituximab-Induktion: Was dann? Erhaltungstherapie ? Welche? - RIT- Induktion (RAVE) - - RIT- Erhaltung - Timing ? Dosierung? à 4 Studien
• Soll eine Erhaltungstherapie abgesetzt werden? • Ist Rituximab effektiv bei - ANCA negativen Patienten?
- Limited disease/Granulomen? • Rituximab über Jahre – was ist das Risiko?
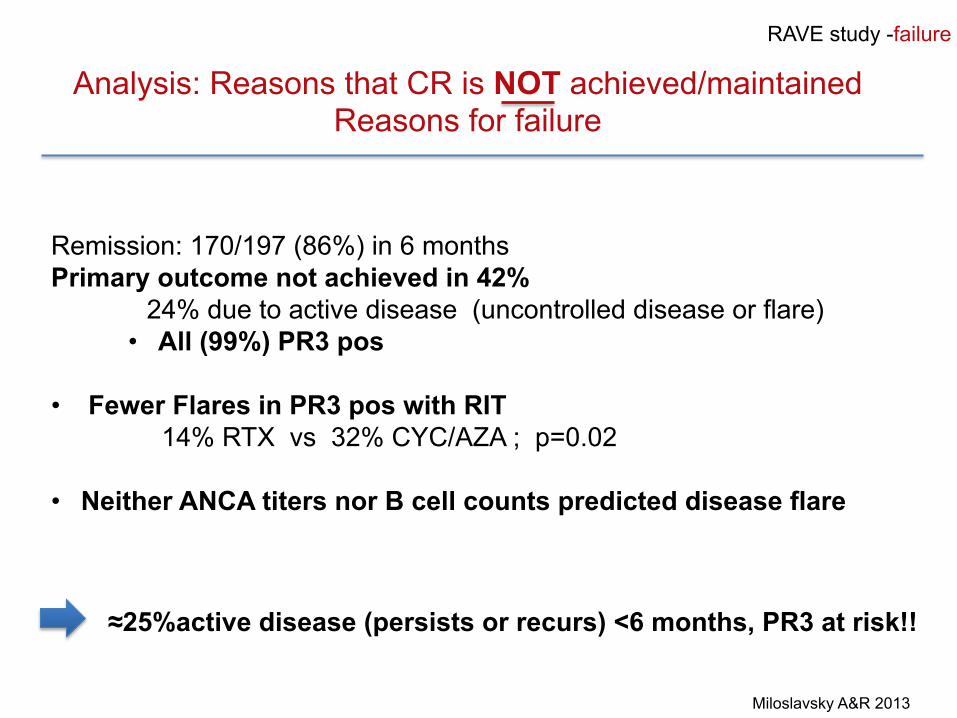
RAVE study -failure
Analysis: Reasons that CR is NOT achieved/maintained Reasons for failure
Remission: 170/197 (86%) in 6 months Primary outcome not achieved in 42%
24% due to active disease (uncontrolled disease or flare) • All (99%) PR3 pos
• Fewer Flares in PR3 pos with RIT
14% RTX vs 32% CYC/AZA ; p=0.02 • Neither ANCA titers nor B cell counts predicted disease flare
Miloslavsky A&R 2013
≈25%active disease (persists or recurs) <6 months, PR3 at risk!!
Specks NEJM 2013
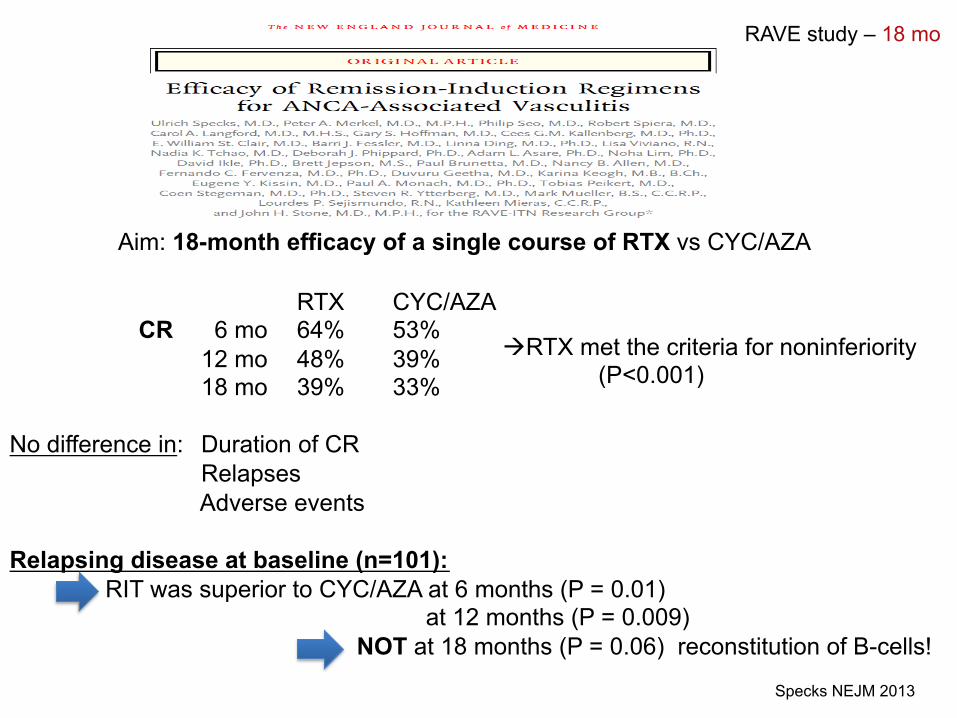
Aim: 18-month efficacy of a single course of RTX vs CYC/AZA
RTX CYC/AZA CR 6 mo 64% 53% 12 mo 48% 39% 18 mo 39% 33%
No difference in: Duration of CR Relapses Adverse events
Relapsing disease at baseline (n=101):
RIT was superior to CYC/AZA at 6 months (P = 0.01) at 12 months (P = 0.009) NOT at 18 months (P = 0.06) reconstitution of B-cells!
RAVE study – 18 mo
àRTX met the criteria for noninferiority (P<0.001)
Specks NEJM 2013
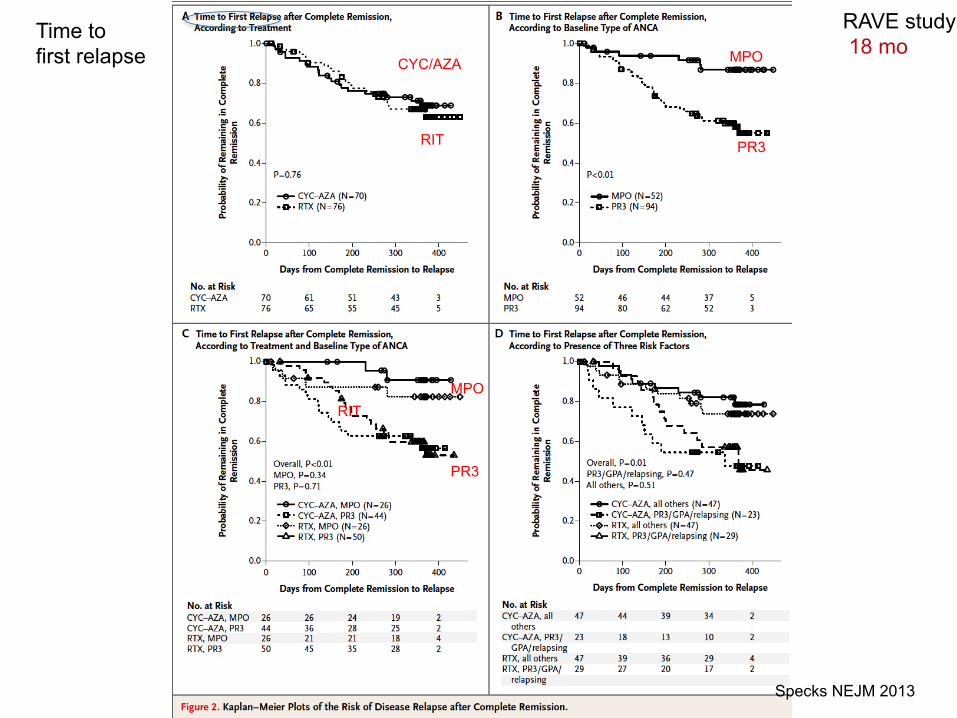
CYC/AZA
RIT
MPO
PR3
MPO
PR3
RIT
RAVE study 18 mo
Time to first relapse
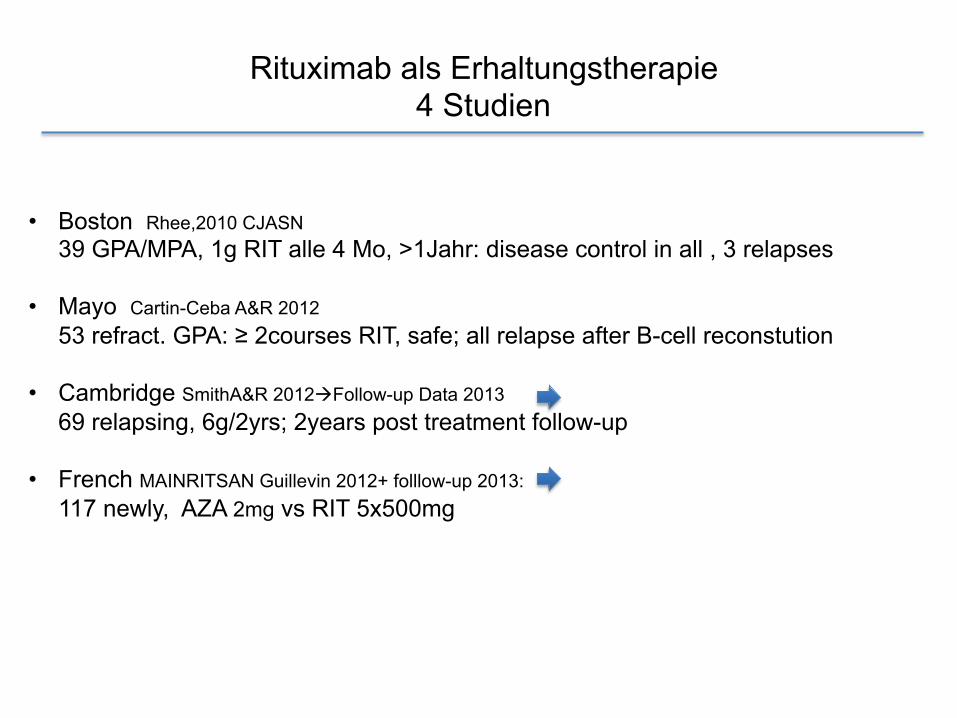
• Boston Rhee,2010 CJASN 39 GPA/MPA, 1g RIT alle 4 Mo, >1Jahr: disease control in all , 3 relapses
• Mayo Cartin-Ceba A&R 2012
53 refract. GPA: ≥ 2courses RIT, safe; all relapse after B-cell reconstution • Cambridge SmithA&R 2012àFollow-up Data 2013
69 relapsing, 6g/2yrs; 2years post treatment follow-up
• French MAINRITSAN Guillevin 2012+ folllow-up 2013: 117 newly, AZA 2mg vs RIT 5x500mg
Rituximab als Erhaltungstherapie 4 Studien
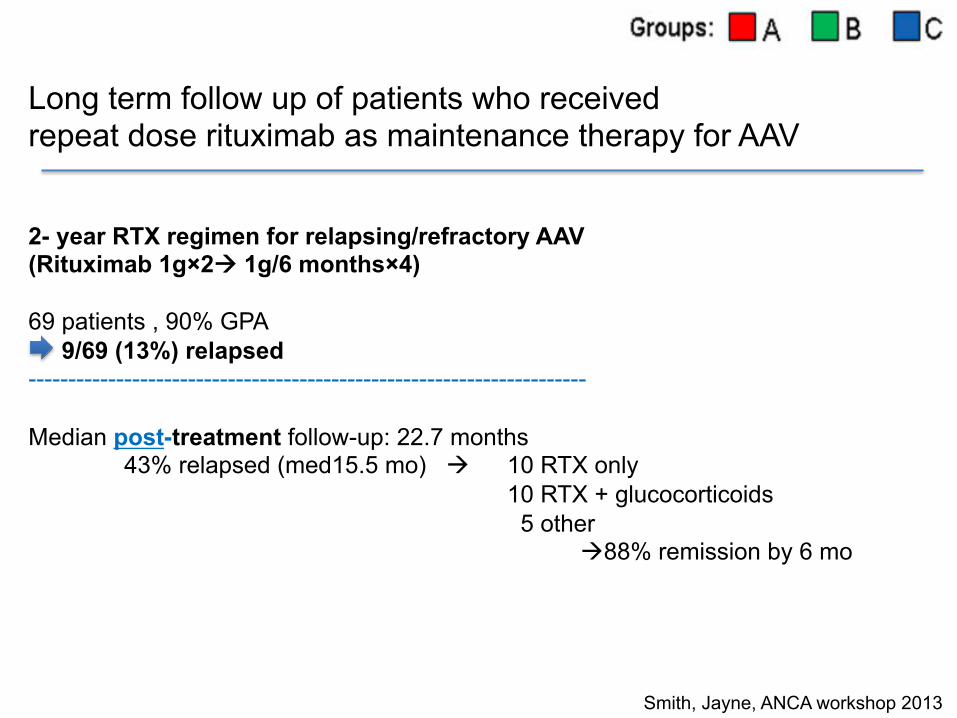
Long term follow up of patients who received repeat dose rituximab as maintenance therapy for AAV
2- year RTX regimen for relapsing/refractory AAV (Rituximab 1g×2à 1g/6 months×4) 69 patients , 90% GPA 9/69 (13%) relapsed ---------------------------------------------------------------------- Median post-treatment follow-up: 22.7 months
43% relapsed (med15.5 mo) à 10 RTX only 10 RTX + glucocorticoids 5 other à88% remission by 6 mo
Smith, Jayne, ANCA workshop 2013
• ANCAs post RIT: 54/69 became ANCA neg
12/54 (22%) became ANCA pos à 75% relapsed (1.6 mo after ANCA return) 15/69 remained ANCA pos à20% relapsed 48% ANCA pos at relapse B-cells: B-cell counts available in 81%
75% had B-cell return after a median of 11 months 68% had detectable B cells at relapse 11/17 (65%) B cells 6 months preceding relapse
• Conclusion
• 43% relapse after 22.5 months • Relapses were rapidly controlled by further RTX • Relapse predictor: ANCA negativity à positivity • But: ANCAs negative in ≈50% of relapses
Smith, Jayne, ANCA workshop 2013
!
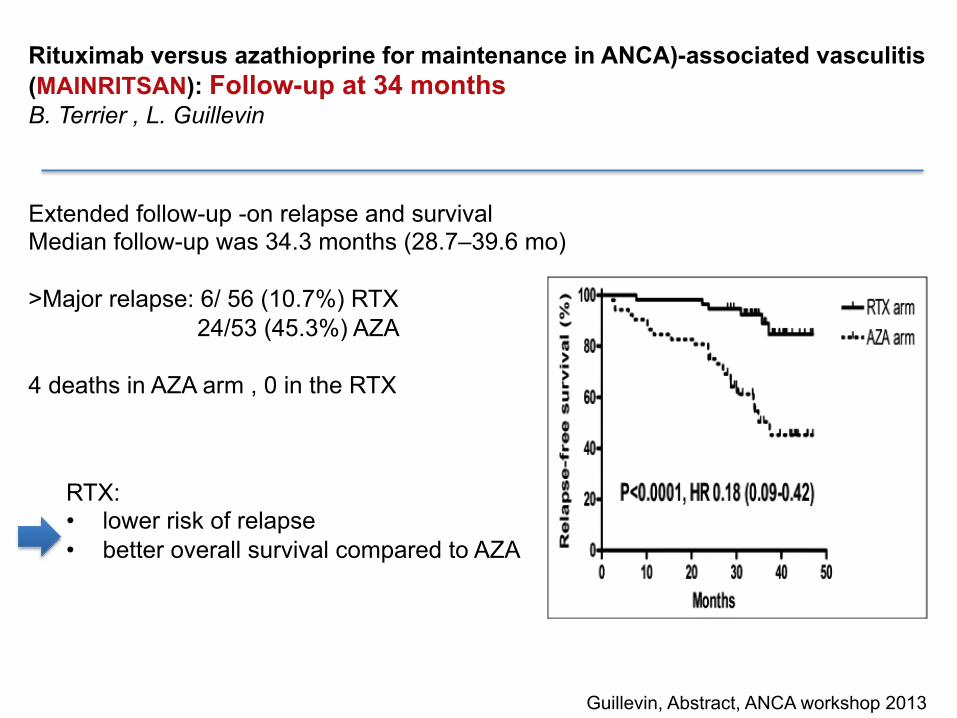
Rituximab versus azathioprine for maintenance in ANCA)-associated vasculitis (MAINRITSAN): Follow-up at 34 months B. Terrier , L. Guillevin
Extended follow-up -on relapse and survival Median follow-up was 34.3 months (28.7–39.6 mo) >Major relapse: 6/ 56 (10.7%) RTX
24/53 (45.3%) AZA 4 deaths in AZA arm , 0 in the RTX
Guillevin, Abstract, ANCA workshop 2013
RTX: • lower risk of relapse • better overall survival compared to AZA
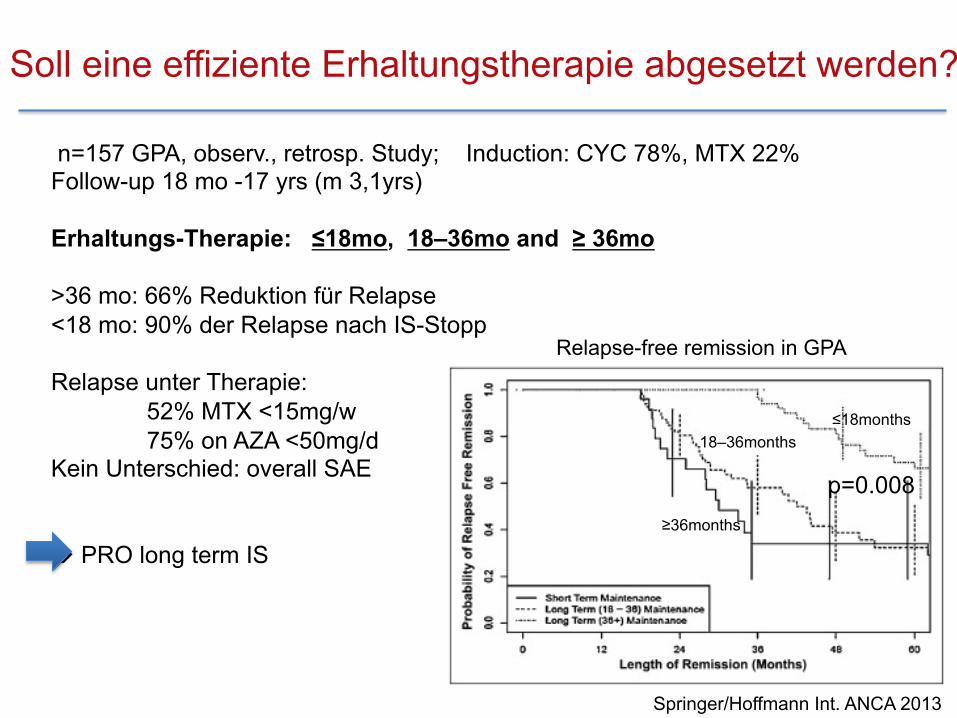
n=157 GPA, observ., retrosp. Study; Induction: CYC 78%, MTX 22% Follow-up 18 mo -17 yrs (m 3,1yrs) Erhaltungs-Therapie: ≤18mo, 18–36mo and ≥ 36mo >36 mo: 66% Reduktion für Relapse <18 mo: 90% der Relapse nach IS-Stopp Relapse unter Therapie:
52% MTX <15mg/w 75% on AZA <50mg/d
Kein Unterschied: overall SAE à PRO long term IS
Springer/Hoffmann Int. ANCA 2013 !
Relapse-free remission in GPA
p=0.008
≤18months 18–36months
≥36months
Soll eine effiziente Erhaltungstherapie abgesetzt werden?
RAVE: Steroids ex at 6 months: Relapse rate high !! Remission at 18 months:
80% of MPO pos only 50% with all 3 risk factors: PR3 pos, GPA, relapsing at baseline
à Future-Trials: PEXIVAS: reduced OGC (0.5 mg/kg/d) versus standard (1mg/kg/d) CLEAR : Rolle von Complement 5a inhibitor , einige Pat ohne OGC
Discontinuation of Steroids in AAV ?
Therapie sparen bei: • Alten Patienten • Niereninsuffizienz • Zunehmender Co-Morbidität • Niederem Relapse-Risiko
Vorsicht bei erhöhtem Relapse-Risiko: • GPA oder PR3-ANCA (vs. MPA) • St.p Relapse • ANCA positiv in Remission • Steigende ANCA-Titer • HNO, Lungenbeteiligung • Weniger CYC zur Induktion (CYCOPS, MYCYC??)
Discontinuation of Therapy in AAV ?
Rituximab- Safety
- Keine Knochenmarkssuppression - Keine mutagene Effekte
- Solide Tumore - Teratogen - Sterilität
Rituximab- Safety
Infusions-Reaktionen: mild bis 20% (inkl Bronchospasmus), schwer 1%
• PML: generell sehr selten, bei AAV bisher nicht beschrieben; kumulative Immunsuppression? bei RA 1:23 000
• HCV +ive: erhöhtes Risiko für hepatalen Schub +/- (?) • HBV : Reaktivierung beschrieben
à pre-emptiv antivirale Therapie bei pos virus load • Pneumocystis jiruvecii Pneumonie - Prophylaxe empfohlen +/-
(Inzidenz nur ca 1,2%) • Immunglobuline ê 33-71%, meist bei wiederholter Dosierung
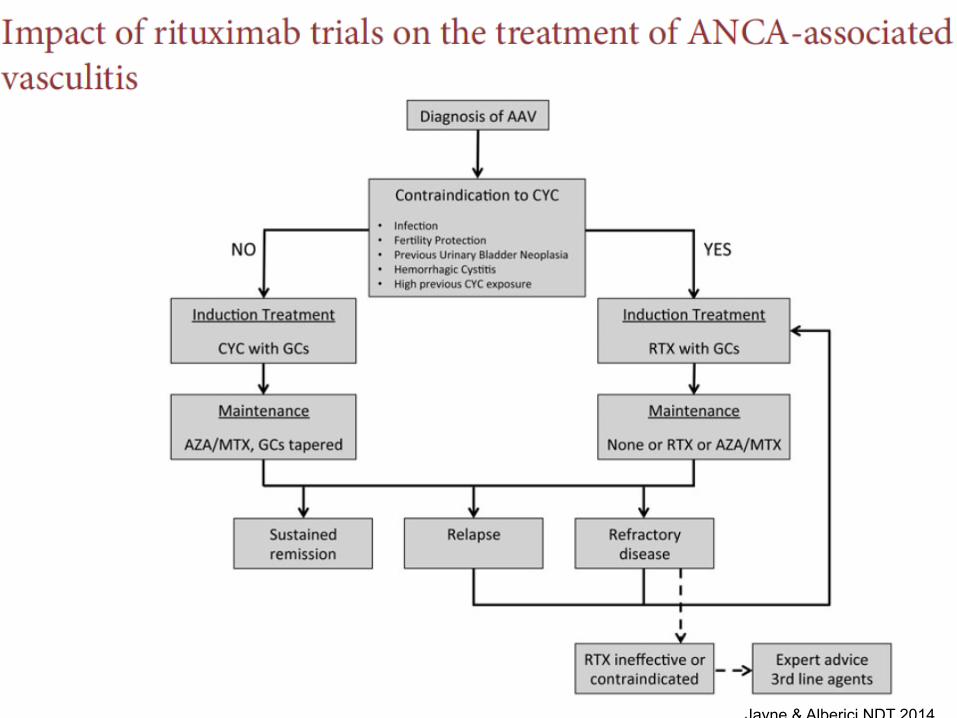
Jayne & Alberici NDT 2014
• Renale Beteiligung bei rheumatoiden Erkrankungen • Vaskulitis • Lupus Nephritis - schwere LN: CYC vs MMF – still discussed
- Maintenance Therapy – for how long? - Rituximab- good in real life, bad in controlled studies?
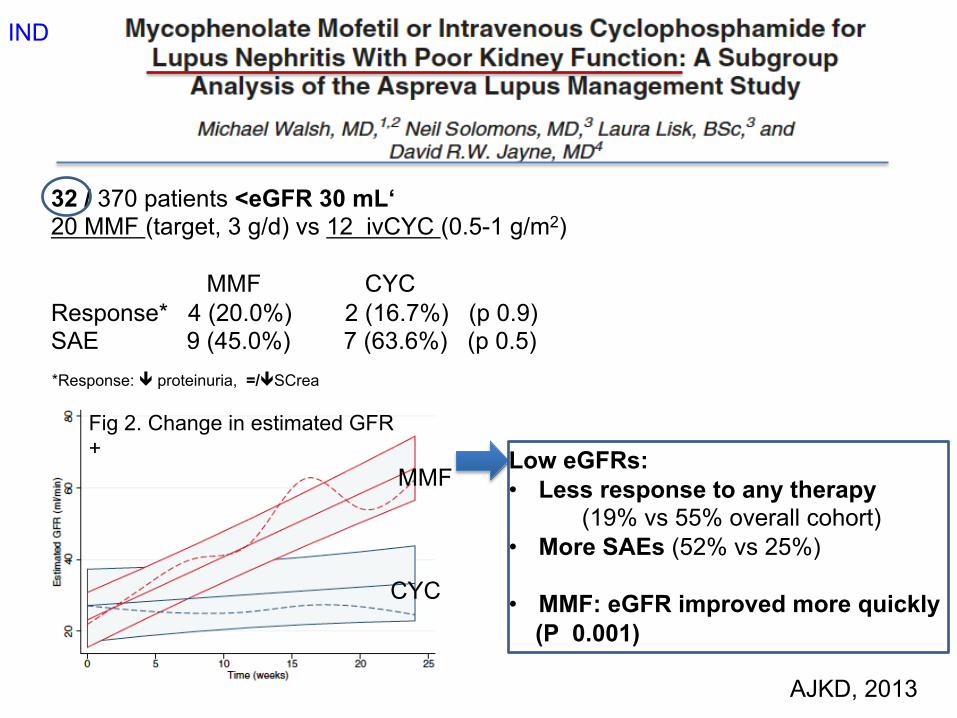
32 / 370 patients <eGFR 30 mL‘ 20 MMF (target, 3 g/d) vs 12 ivCYC (0.5-1 g/m2)
MMF CYC Response* 4 (20.0%) 2 (16.7%) (p 0.9) SAE 9 (45.0%) 7 (63.6%) (p 0.5)
AJKD, 2013
Low eGFRs: • Less response to any therapy (19% vs 55% overall cohort) • More SAEs (52% vs 25%)
• MMF: eGFR improved more quickly (P 0.001)
Fig 2. Change in estimated GFR +
CYC
MMF
IND
*Response: ê proteinuria, =/êSCrea
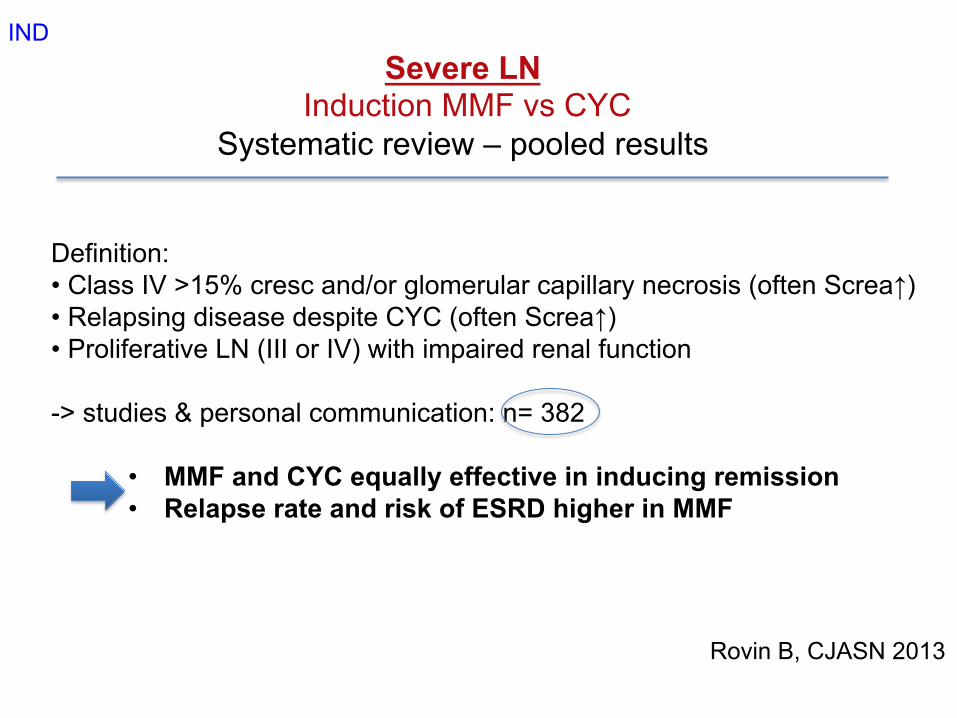
Severe LN Induction MMF vs CYC
Systematic review – pooled results
Definition: • Class IV >15% cresc and/or glomerular capillary necrosis (often Screa↑) • Relapsing disease despite CYC (often Screa↑) • Proliferative LN (III or IV) with impaired renal function
-> studies & personal communication: n= 382
• MMF and CYC equally effective in inducing remission • Relapse rate and risk of ESRD higher in MMF
Rovin B, CJASN 2013
IND
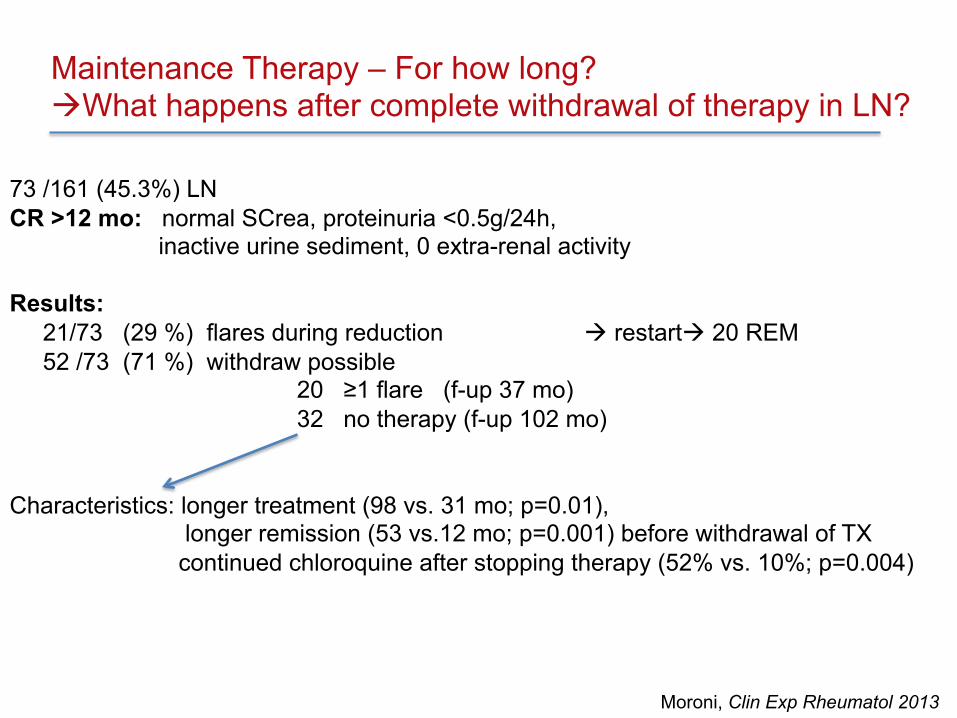
Maintenance Therapy – For how long? àWhat happens after complete withdrawal of therapy in LN?
73 /161 (45.3%) LN CR >12 mo: normal SCrea, proteinuria <0.5g/24h,
inactive urine sediment, 0 extra-renal activity Results: 21/73 (29 %) flares during reduction à restartà 20 REM 52 /73 (71 %) withdraw possible
20 ≥1 flare (f-up 37 mo) 32 no therapy (f-up 102 mo)
Characteristics: longer treatment (98 vs. 31 mo; p=0.01),
longer remission (53 vs.12 mo; p=0.001) before withdrawal of TX continued chloroquine after stopping therapy (52% vs. 10%; p=0.004)
Moroni, Clin Exp Rheumatol 2013
Conclusion: Complete withdrawal of therapy:
- in selected patients (ca ⅓) - stable remission after long-term treatment - reduction of treatment must be done in a very gradual manner!
- chloroquine may help to maintain remission
Moroni, Clin Exp Rheumatol 2013
What happens after complete withdrawal of therapy in LN?
Poor prognostic factors: • Most important: - persistent proteinuria and - failure to normalise renal function at 6 months • African, Hispanic ethnicity • young age, male • BX: crescents • Delayed response to immunosuppressive therapy • persistently elevated APL-AB • persistently low levels of C3 • frequent relapses (up to 35%) • Lack of compliance • Suboptimal global care
Maintenance Therapy - For how long ??
Gunnarson, Lupus 2013
1) Observational studies: n=90 (BX), follow-up at least 6-12 mo
CR in 36/90 (40%) PR in 33/90 (37%), Non responders 21/90 (23%)
à 77% overall response (CR or PR) after rituximab
Rituximab in LN- where do we stand?
2) Two registries • The French Autoimmunity and Rituximab (AIR) registry 42 LN, follow-up data in 31: 74% CR or PR at 6 months • UK-BIOGEAS: registry, 9 European centres, 164 LN refractory or relapses->126 for follow-up 67% renal response at both 6 and 12 months


















