Vorbereitung EBO¤sentationen...candidates (there is a pool of 500-600 MCQ-Questions, questions used...
68
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich Vorbereitung EBO Katarakt, Konjunktiva, Cornea Jörg Stürmer Augenklinik Kantonsspital Winterthur [email protected]
Transcript of Vorbereitung EBO¤sentationen...candidates (there is a pool of 500-600 MCQ-Questions, questions used...
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Vorbereitung EBOKatarakt, Konjunktiva, Cornea
Jörg Stürmer
Augenklinik Kantonsspital Winterthur

EBOD examination• Every year in may during the SFO, during 1 day• Morning: 3h MCQ’s
52 subjects, 5 questions pro subject = 260 responses
• After-noon: 1h oral partDiscussion among specialists in ophthalmology: between the candidate and thetwo examiners
G. Sunaric Mégev
https://www.ophthoquestions.com/
Online Fragensammlung:
Sehr gutes Review, sehr ausführlich
MCQ zum Review
Buch:
Beste Kombi würde ich sagen
Leseempfehlungen von Drazen Jurjevic
Wenn man Zeit hat
Inhaltlich super leider keine Bilder + Bilder
gering weniger Inhalt gegenüber Oxford
Viel Zeit mitbringen
6
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
MCQ Important:
Consist allways of a statement followed by 5 questions
Language is English
All questions have to be answered with «true» or «false»
Do only answer questions you are shure because every wrong answer will be counted negatively («Minuspunkte»)
None of these questions are available for training of candidates (there is a pool of 500-600 MCQ-Questions, questions used in the 2018 exams are banned for 5 years)
You have ample time, but please reserve at least 20 minutes at the end to fill in the card with your answers
7
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract
Cataract is the leading cause of preventable blindness worldwide
true false
More than 5 Million worldwide are blind due cataractstrue false
Tabac smoking is a major risc factor for cataract developmenttrue false
Cataract formation is less common in the 2. and 3. world
true false
Unilateral mature cataract in the absence of previous ocular trauma is very likely to bea due to Fuchs Uveitis Syndrome
true false
8
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract
Cataract is the leading cause of preventable blindness worldwide
true false
More than 5 Million worldwide are blind due cataractstrue false
Tabac smoking is a major risc factor for cataract developmenttrue false
Cataract formation is less common in the 2. and 3. world
true false
Unilateral mature cataract in the absence of previous ocular trauma is very likely to becaused by Fuchs Uveitis Syndrome
true false
9
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract surgery
Extracapsular cataract extraction has been introduced in 1748 by Jacques Daviel
true false
Implantation of IOL's has been introduced in the late 1970 by Sir Harold Ridley
true false
Intracapsular cataract extraction was the method of choice until the 1970iestrue false
Phacoemulsification was introduced in 1967 by Charles Kelman and adopted as thetechnique of choice soon thereafter
true false
The first foldable IOL's were introduced 1987true false
10
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract surgery
Extracapsular cataract extraction has been introduced in 1748 by Jacques Daviel
true false
Implantation of IOL's has been introduced in the late 1970 by Sir Harold Ridley
true false
Intracapsular cataract extraction was the method of choice until the 1970iestrue false
Phacoemulsification was introduced in 1967 by Charles Kelman and adopted as thetechnique of choice soon thereafter
true false
The first foldable IOL's were introduced 1987true false
11
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract surgery today
Phakoemulsification and PC-IOL-Implant is the standard procedure today
true false
The standard material used to produce IOL's is flexible hydrophobic PMMA
true false
For the comfort of the patient the best anaestetical technique is topical anaesthesiatrue false
Immediate sequential bilateral cataract surgery is dangerous because several cases ofbilateral endophthalmitis are reported
true false
Adapting the IOL-power of the second eye should allways be performed in the case ofrefractive surprise in the first eye
true false

12
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Cataract surgery today
Phakoemulsification and PC-IOL-Implant is the standard procedure today
true false
The standard material used to produce IOL's is flexible hydrophobic PMMA
true false
For the comfort of the patient the best anaestetical technique is topical anaesthesiatrue false
Immediate sequential bilateral cataract surgery is dangerous because several cases ofbilateral endophthalmitis are reported
true false
Adapting the IOL-power of the second eye should allways be performed in the case ofrefractive surprise in the first eye
true false
13
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Femtolaser-assisted cataract surgery (FLACS)
Femtolaser-assisted cataract surgery (FLACS) is the state of the art treatment
true false
The capsulorhexis created by the Laser is much more solid than a manualcapsulorhexis
true false
All patients profit from the better centration of the Laser-assisted capsulorhexistrue false
There is strong evidence that FLACS has less complications than manualPhakoemulsification
true false
There is some evidence that patients with Fuchs endothelial Dystrophy benefit fromFLACS
true false
14
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Femtolaser-assisted cataract surgery (FLACS)
Femtolaser-assisted cataract surgery (FLACS) is the state of the art treatment
true false
The capsulorhexis created by the Laser is much more solid than a manualcapsulorhexis
true false
All patients profit from the better centration of the Laser-assisted capsulorhexistrue false
There is strong evidence that FLACS has less complications than manualPhakoemulsification
true false
There is some evidence that patients with Fuchs endothelial Dystrophy benefit fromFLACS
true false
15
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Late-onset IOL luxations/subluxation
The incidence of IOL subluxation/luxation is approximately 1%
true false
Main risc factor is Pseudoexfolation syndrome
true false
Massive shrinking of the anterior capsule especially in the presence of a rather smallcapsulorhexis is often seen in these cases
true false
The implantation of a capsular tension ring during cataract surgery does prevent thisproblem
true false
The average time between cataract surgery and subluxation is 3.5 years
true false

16
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cataract Late-onset IOL luxations/subluxation
The incidence of IOL subluxation/luxation is approximately 1%
true false
Main risc factor is Pseudoexfolation syndrome
true false
Massive shrinking of the anterior capsule especially in the presence of a rather smallcapsulorhexis is often seen in these cases
true false
The implantation of a capsular tension ring during cataract surgery does prevent thisproblem
true false
The average time between cataract surgery and subluxation is 3.5 years
true false
17
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Which of the following conjunctival pathologies are caused byClamydia trachomatis
Ligneous conjunctivits true false
Adult inclusion conjunctivitis true false
Lymphogranuloma venereum true false
Trachoma true false
follicular conjunctivitis true false
18
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Which of the following conjunctival pathologies are caused byClamydia trachomatis
Ligneous conjunctivits true false
Adult inclusion conjunctivitis true false
Lymphogranuloma venereum true false
Trachoma true false
follicular conjunctivitis true false

19
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Conjunctival cicatrisation is associated with
ocular cicatricial pemphigoid true false
atopic kertoconjunctivitis true false
Stevens-Johnson syndrome true false
superior limbal keratoconjunctivits true false
Chemical burns true false
20
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Conjunctival cicatrisation is associated with
ocular cicatricial pemphigoid true false
atopic kertoconjunctivitis true false
Stevens-Johnson syndrome true false
superior limbal keratoconjunctivits true false
Chemical burns true false

21
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
22
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Pterygiummay cause astigmatism by flattening the involved meridian true false
may cause destruction of Bowman’s layer true false
A pigmented iron line (Ferry’s line) is found at the corneal edge of the lesiontrue false
simple excision leaving bare sclera is the best surgical optiontrue false
Mitomycine C application may reduce recurrence-rate true false
23
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Conjunctiva
Pterygiummay cause astigmatism by flattening the involved meridian true false
may cause destruction of Bowman’s layer true false
A pigmented iron line (Ferry’s line) is found at the corneal edge of the lesionStocker true false
simple excision leaving bare sclera is the best surgical optiontrue false
Mitomycine C application may reduce recurrence-rate true false

24
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich

25
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Bullous keratopathyis an inherited disease of the corneal epithelium true false
Is often painful true false
Is rarely associated with visual loss true false
May require DSEK or DMEK true false
Starts in the early childhood true false
26
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Bullous keratopathyis an inherited disease of the corneal epithelium true false
Is often painful true false
Is rarely associated with visual loss true false
May require DSEK or DMEK true false
Starts in the early childhood true false

27
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
28
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: KeratokonusThe disease is inherited as a x-linked recessive trait true false
Increasing irregular astigmatism is a common finding true false
The main progression of the disease usually occurs after the age of 40 true false
Corneal cross-linking is a treatment option for progressive keratokonus true false
When good visual acuity is no longer achieved with glasses,
rigid gas-permeable contact lenses may be an option true false

29
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: KeratokonusThe disease is inherited as a x-linked recessive trait true false
Increasing irregular astigmatism is a common finding true false
The main progression of the disease usually occurs after the age of 40 true false
Corneal cross-linking is a treatment option for progressive keratokonus true false
When good visual acuity is no longer achieved with glasses,
rigid gas-permeable contact lenses may be an option true false
30
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich

31
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Cornea verticillatais a whorl-like deposition of material in the corneal endothelium true false
is allways caused by amiodarone intake true false
may be seen in glycolipidosis (Fabry’s disease) true false
may be seen when Tamoxifen or Chloroquine is used true false
was first described in a patient with Fabry’s disease true false
32
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Cornea verticillatais a whorl-like deposition of material in the corneal endothelium true false
is allways caused by amiodarone intake true false
may be seen in glycolipidosis (Fabry’s disease) true false
may be seen when Tamoxifen or Chloroquine is used true false
was first described in a patient with Fabry’s disease true false
33
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich

34
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
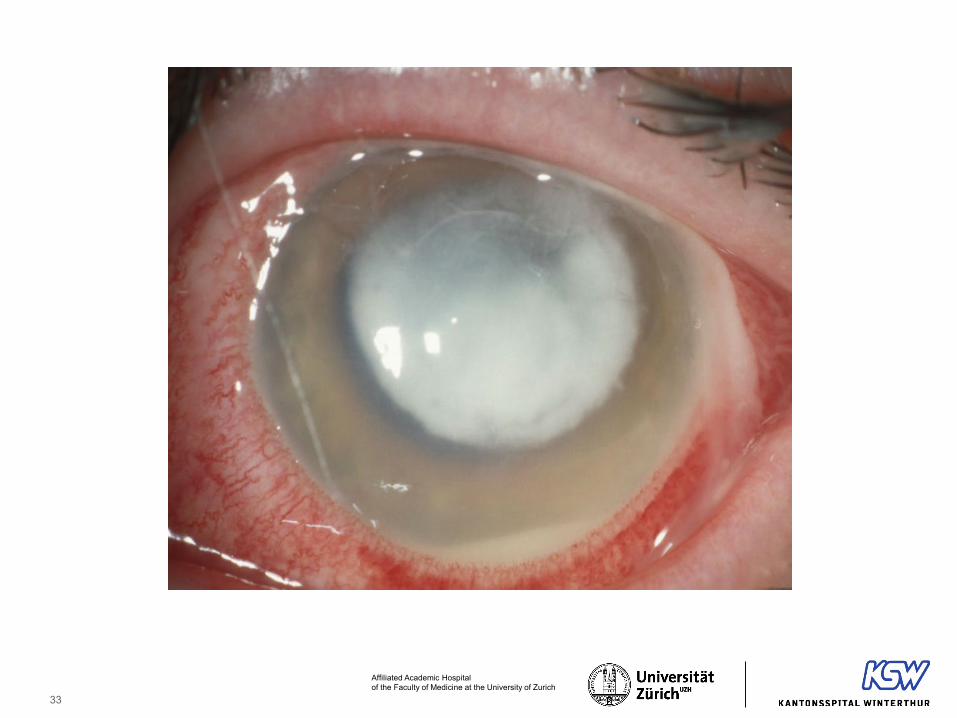
Questions Cornea
Which is/are true: Contact lens associated corneal ulcersOvernight wearing of soft contact lenses is a major risk factor true false
May be prevented by prohylactic use of antibiotics qid true false
Is never seen in patients wearing rigid gas-permeable contact lensestrue false
Infections with Pseudomonas have a worse prognosis true false
Incidence is lower in patients ordering their lenses via the Internet true false
35
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Contact lens associated corneal ulcersOvernight wearing of soft contact lenses is a major risk factor true false
May be prevented by prohylactic use of antibiotics qid true false
Is never seen in patients wearing rigid gas-permeable contact lensestrue false
Infections with Pseudomonas have a worse prognosis true false
Incidence is lower in patients ordering their lenses via the Internet true false
36
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich

37
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Herpetic KeratitisIs commonly caused by HSV-2 true false
Is the most common cause of corneal blindness worldwide true false
Treatment of epithelial form with antivirals is allways indicated true false
Rose bengal may be used to differentiate HSV from H. zoster lesion true false
Long-term low dose oral treatment with Acylovir reduces recurrence-rate
true false
38
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
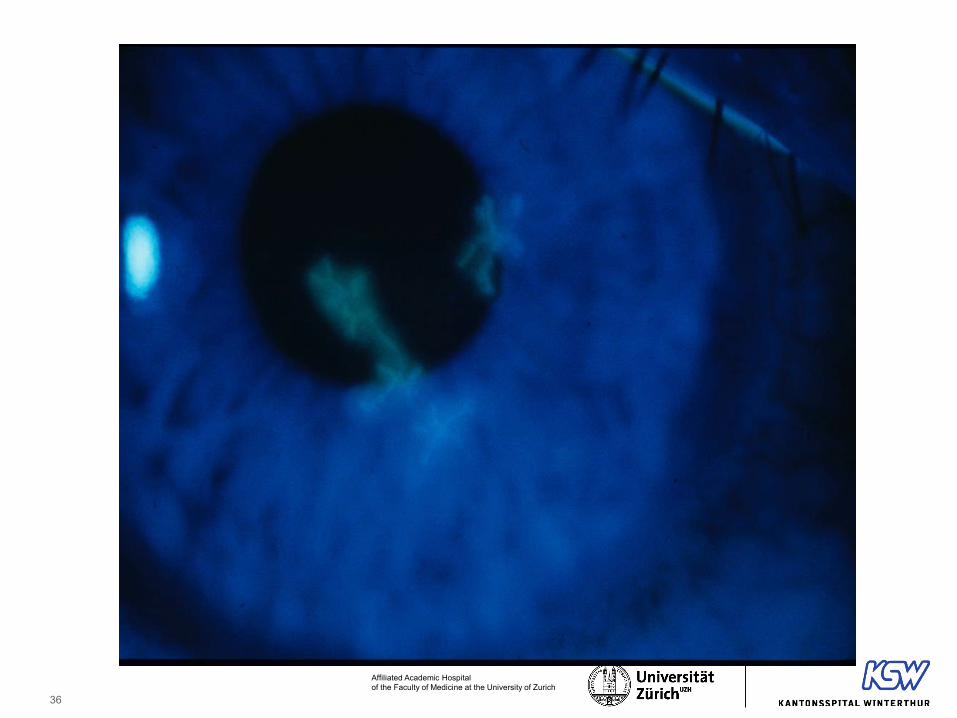
Questions Cornea
Which is/are true: Herpetic KeratitisIs commonly caused by HSV-2 true false
Is the most common cause of corneal blindness worldwide true false
Treatment of epithelial form with antivirals is allways indicated true false
Rose bengal may be used to differentiate HSV from H. zoster lesion true false
Long-term low dose oral treatment with Acylovir reduces recurrence-rate
true false
39
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Stromal corneal dystrophiesCorneal dystrophies are all inherited disorders true false
The most common form of stromal dystrophy is macular true false
Stromal deposits in granular dystrophy stain red with trichrome true false
A patient with granular dystrophy can remain asymptomatic for decades
true false
Symptomatic Map-Dot Fingerprint anterior Basement dystrophy may be treated byPhototherapeutic keratectomy with excimer laser true false

40
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Questions Cornea
Which is/are true: Stromal corneal dystrophiesCorneal dystrophies are all inherited disorders true false
The most common form of stromal dystrophy is macular
granular true false
Stromal deposits in granular dystrophy stain red with trichrome true false
A patient with granular dystrophy can remain asymptomatic for decades
true false
Symptomatic macular stromal dystrophy may be treated by Phototherapeutic keratectomywith excimer laser true false
41
Affiliated Academic Hospital of the Faculty of Medicine at the University of Zurich
Oral exam
2 experts are examining the candidate in
1 expert will be from Switzerland, the other from abroad
4 different topics
Language English is mandatory (because all other EBO Candidates would be examined also in English)
The Swiss expert may help in case of problems by changing to German or French (but the 2nd Expert may not be able to understand German or French)
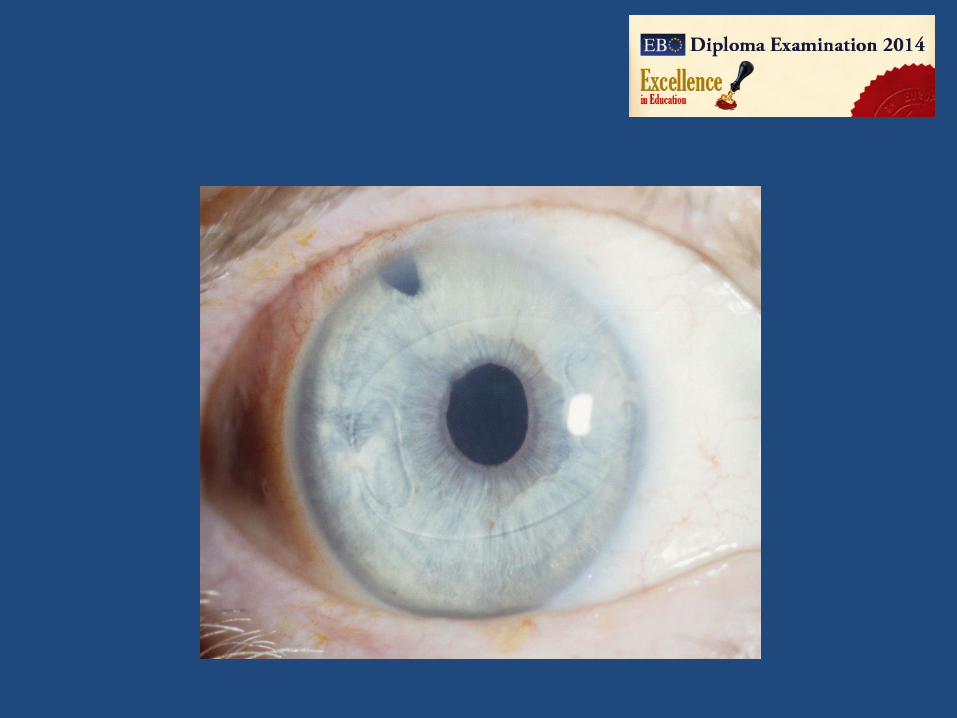
Case 3: 61 year old man (Gl 3)
• 21.03.2011 Presented with inflamed red eye RE and pain– Treated previously for 10 days by GP with Maxitrol
• Visual acuity: RE 0.4, LE 1.0 (mild myopia)• IOP: RE 50 mmHg, LE 14 mmHg• AC: RE deep, Cells ++, Flare ++

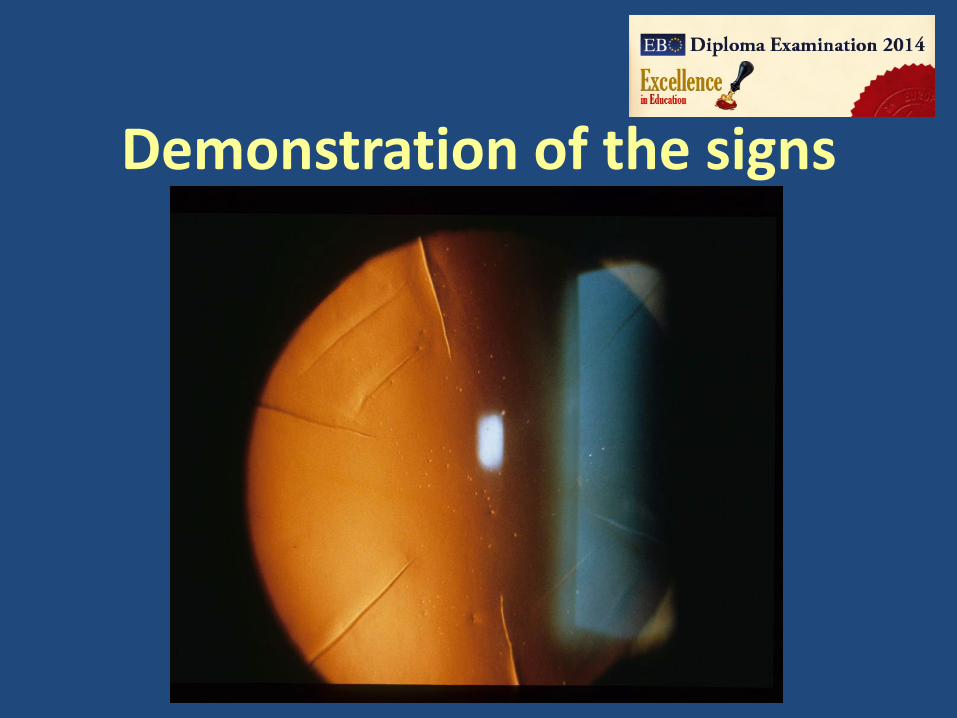
Demonstration of the signs
Case 3: questions
1. What is your diagnosis ?2. What is the differential diagnosis ?3. How would you confirm the diagnosis ?4. What is your treatment of choice ?
Case 3: Continued• Treatment:
– systemic Valacyclovir 2x 1000 mg p.o.– Diamox 3 x 125 mg p.o.– Topical: Dexafree0.1% hourly, Atropin 1% 3x1, Betablocker/CAI combo
2x1
• AC-Tap for HSV PCR +• 1 Week later: VA 0.6, IOP 10 mmHg, inflammation much less

Case 5: 37 year old woman (R 1)
• Was high myopic and astigmatic in her youth• Had some surgery for this condition in South America when she
was 23 years old• Complains about straylight and some-times blurred vision• Unaided visual acuity has decreased• VA sc RE: 0.5 LE: 0.8• Refraction: RE: -0.75=-1.75/20°, LE: -0.5 =-1.0/45°
Demonstration of the signs

Case 5: questions
1. What type of surgery had this patient ?2. How could you improve the present situation ?3. Would you recommend clear lens extraction ?4. What is the main problem if later on cataract
surgery is required ?
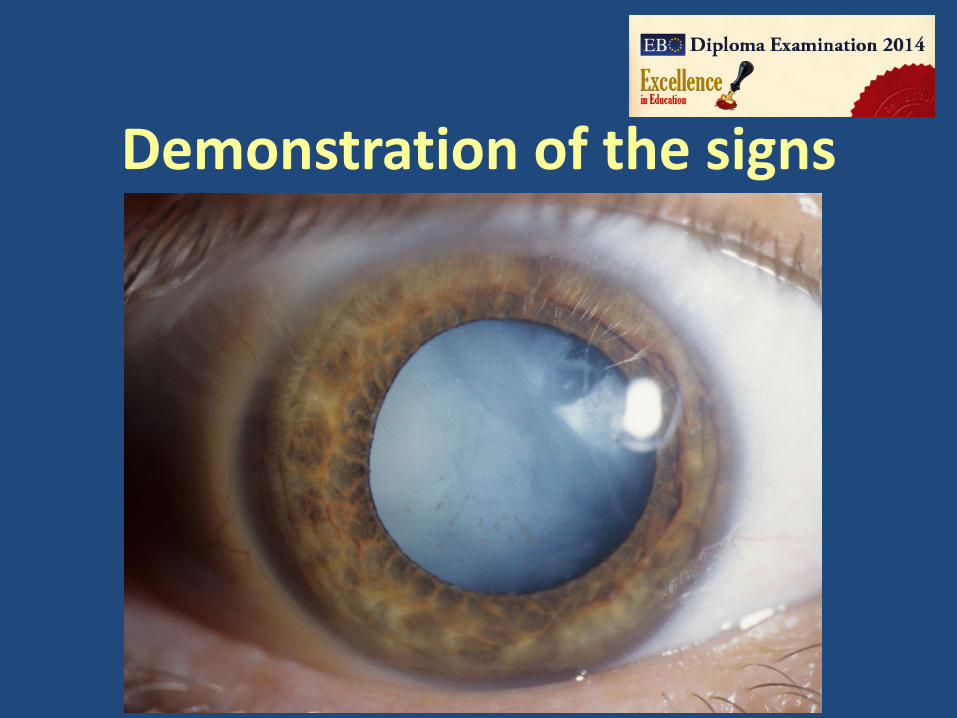
Case 6: 57 year old woman (R 2)
• Was high myopic in her youth• Had surgery for this condition 6 years ago• Complains about sudden onset of decreased vision in her left
eyes 5 days ago• VA sc RE: 0.8 LE: 0.3• Refraction: RE: -0.5=-0.75/40°, LE: 0.75=-3.0/30°
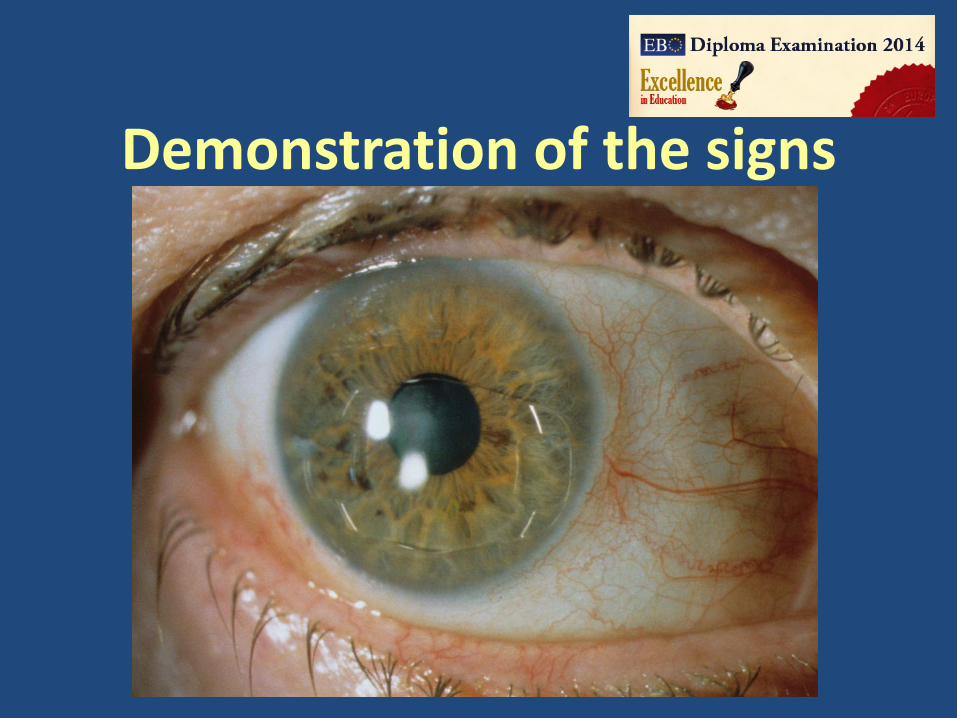
Demonstration of the signs

Demonstration of the signs
Case 6: questions
1. What type of surgery had this patient ?2. What is the cause of the worsening in LE ?3. What is your treatment ?4. Is this an emergency which has to be cured the
same day and if yes why ?

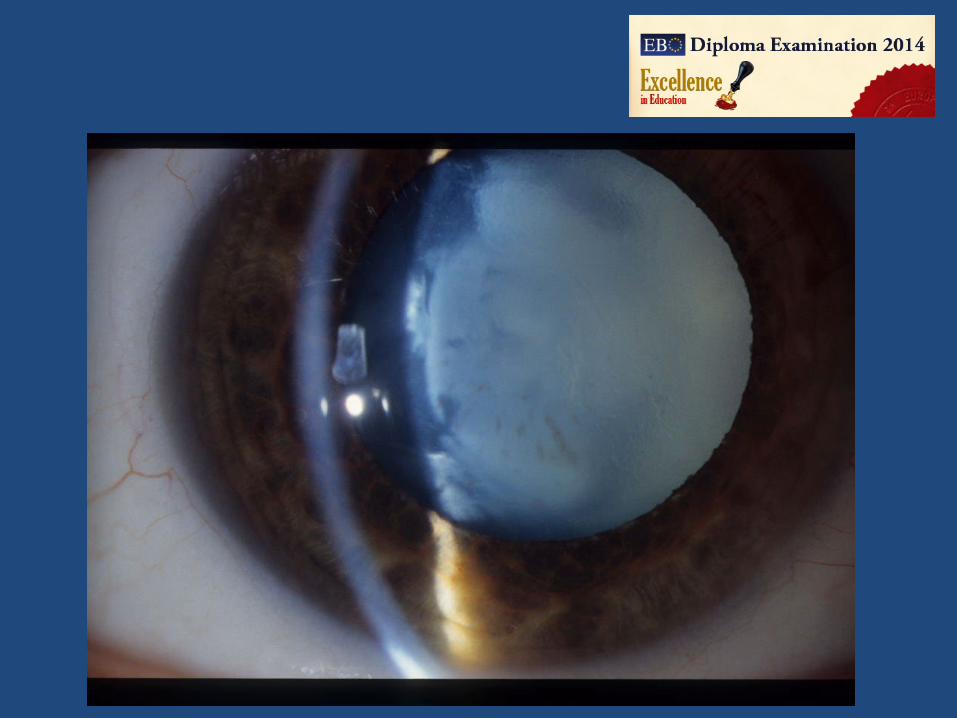
Case 8: 37 year old woman (C 1)
• Presents with loss of vision in her right eye, uncertain about how long and how fast
• VA sc RE Light Perception, LE 1.0• IOP: RE 22 mmHg, LE 12 mmHg• No previous ocular trauma
Demonstration of the signs
Case 8: questions
1. What is your diagnosis ?2. What is the most likely cause ? 3. Which additional investigations should be done ?4. What are the important points to discuss with the
patient to get informed consent for cataract surgery ?
Case 9: 9 year old girl (C 2)
• Presents with reduced vision RE• VA sc RE 0.4, LE 0.9• Refraction +- emmetropic• Normal posterior segment

Demonstration of the signs
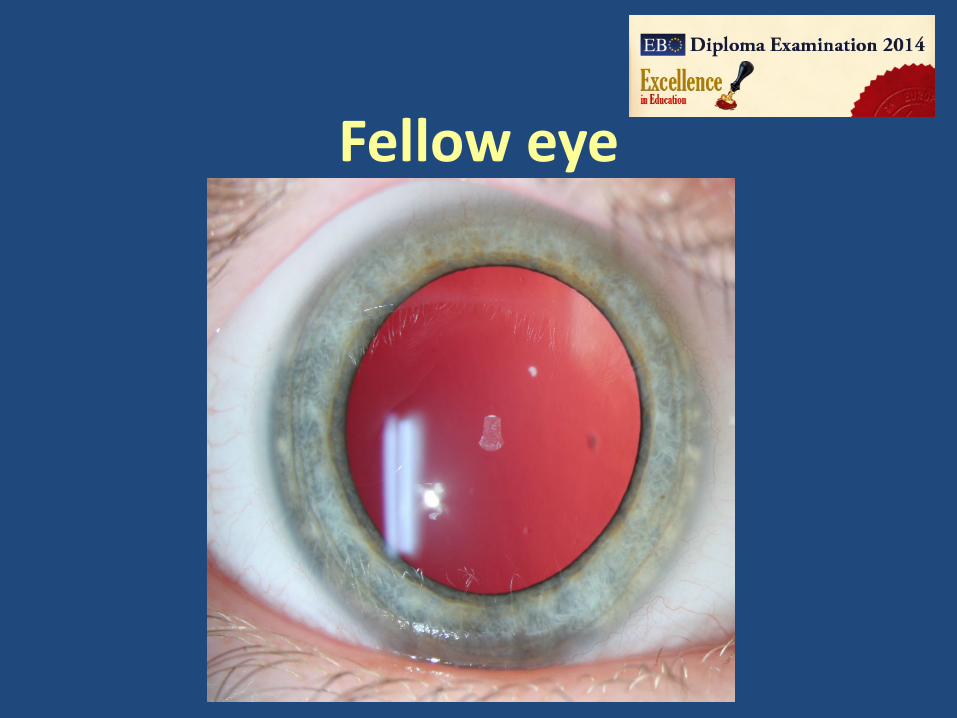
Fellow eye
Case 9: questions
1. What is your diagnosis ?2. Which additional investigations should be done ?3. What is your treatment approach ?4. What are the pros and cons of cataract surgery in
this case ?

Case 12: 76 year old lady (C 5)
• Presents as emergency because of pain and reduced vision RE• Had uncomplicated cataract surgery elsewhere 2 days ago• All findings where normal on the 1st post-op day• VA sc RE 0.1, LE 0.6• IOP 18 mmHg BE

Demonstration of the signs
Case 12: questions1. What is your diagnosis ?2. What is your treatment plan?3. What additional investigations should be
performed ?
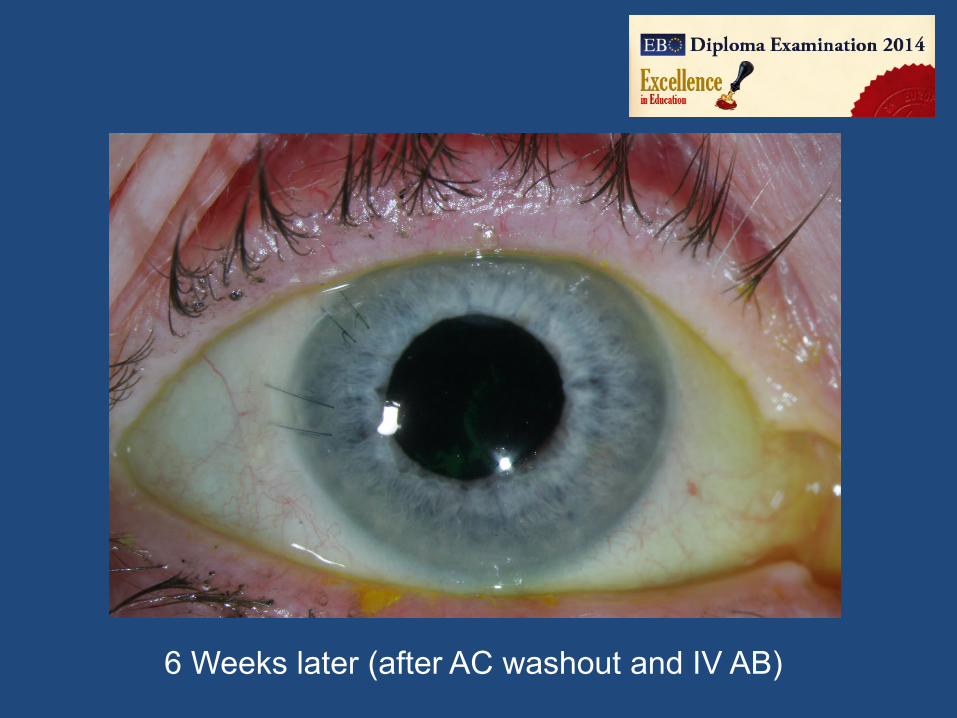
6 Weeks later (after AC washout and IV AB)
Case 13: 86 year old lady (C 6)
• Presents as emergency because of reduced vision LE• Had uncomplicated cataract surgery 7 years ago LE• VA sc RE 1.0, LE 0.2• IOP RE 18 mmHg, LE 24 mmHg
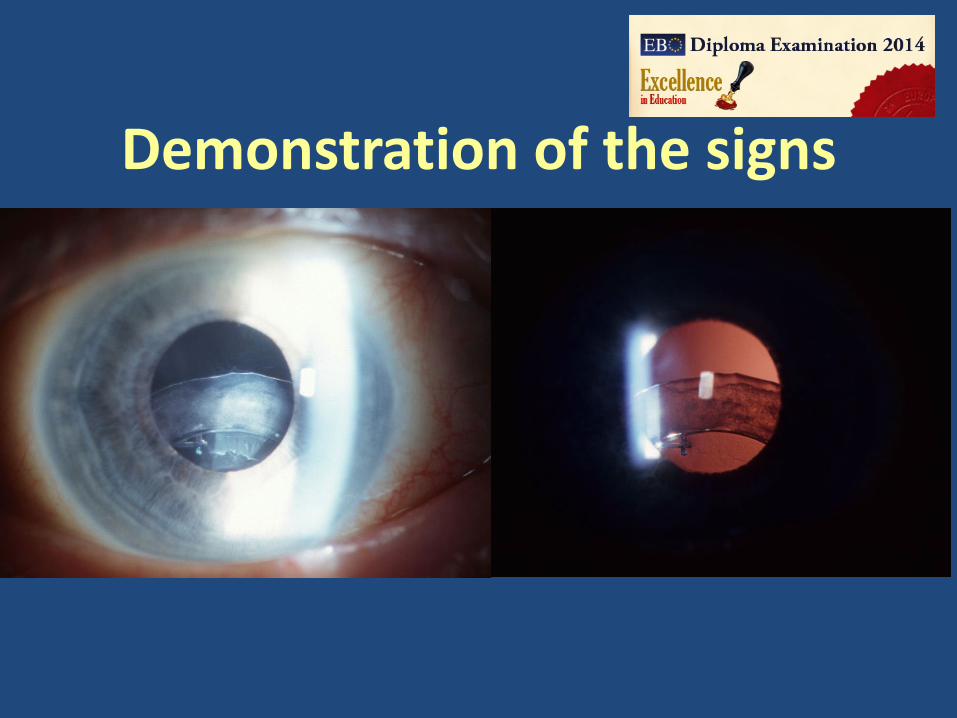
Demonstration of the signs
Case 13: questions
1. What is your diagnosis ?2. Is this a rare complication?3. What are the different options for treatment ?