Zubereitung und Applikation von Antibiotika – ein Beitrag ... · PDF file© Dr....
39
© Dr. Ulrike Porsche Zubereitung und Applikation von Antibiotika – ein Beitrag zu Therapieerfolg und Reduktion von Resistenzen Mag.pharm. Dr. Ulrike Porsche, aHPh Landesapotheke Salzburg Infektiologischer Arbeitskreis an den Salzburger Landeskliniken (SALK) Tag der Hygiene, Villach, 14. Oktober 2010
Transcript of Zubereitung und Applikation von Antibiotika – ein Beitrag ... · PDF file© Dr....

© Dr. Ulrike Porsche
Zubereitung und Applikation von Antibiotika – ein Beitrag zu Therapieerfolg und Reduktion von ResistenzenMag.pharm. Dr. Ulrike Porsche, aHPhLandesapotheke SalzburgInfektiologischer Arbeitskreis an den Salzburger Landeskliniken (SALK)
Tag der Hygiene, Villach, 14. Oktober 2010
© Dr. Ulrike PorscheIlse Fitzka

© Dr. Ulrike Porsche
Das Salzburger ModellInfektiologe + Apotheker + KH-Hygieniker + Mikrobiologe + Intensivmediziner
• Gründung 1996• Erstellung von Leitlinien/
Empfehlungen auf Abteilungs- und Hausebene
• Infektiologische Visiten• Publikation aller
Informationen auf einer Intranetseite des IAK
© Dr. Ulrike Porsche

LEO Dictionary 2010© Dr. Ulrike Porsche
Stewardship
Haushofmeisteramt, Verantwortung, Verwalteramt, Verwaltung
• Stewardship of available resources (sparsamerUmgang mit den Rohstoffen)
• Forrest stewardship council = FSC (Organisation zur Zertifizierung nachhaltiger Forstwirtschaft)
• Product stewardship (Produktverantwortung)
Dellit et al CID 2007© Dr. Ulrike Porsche
Active Antimicrobial Stewardship Strategies
• Prospective Audit with Intervention and Feedback
• Formulary Restriction and Preauthorization Requirements for Specific Agents
Dellit et al CID 2007© Dr. Ulrike Porsche
Supplemental Antimicrobial Stewardship Strategies
• Education• Guidelines and Clinical Pathways• Antimicrobial Cycling and Scheduled Antimicrobial Switch• Antimicrobial Order Forms• Combination Therapy; Prevention of Resistance versus
Redundant Antimicrobial Coverage• Streamlining or De-escalation of Therapy
• Dose Optimization• Parenteral to Oral Conversion
Bodi M. et al, clin. Microbiolog. Infect. 2001;7:32-33© Dr. Ulrike Porsche
Tarragona Strategy on Antibiotic Therapy
1. Look at your patient (recognizing the individual risk factors)2. Listen to your hospital (knowledge of the local epidemiology)
3. Hit hard and early (the therapy should be initiated immediately and be broad enough to reach the vast majority of likely pathogens; combination therapy of acylaminopenicillin or a 3rd generation cephalosporin or a carbapenem with a fluorchinolon as combination partner)
4. Get to the point (select antimicrobials with ideal pharmacokinetic and -dynamic properties to reach effective concentrations at the site of infection)
5. Focus, focus, focus (reevaluation of the initial therapy after 3 days, depending on the results from microbiology; proving the option to deescalate to a single narrow spectrum antimicrobial drug or even enteraladministration in selected cases to reduce selection pressure, and costs).
© Dr. Ulrike Porsche
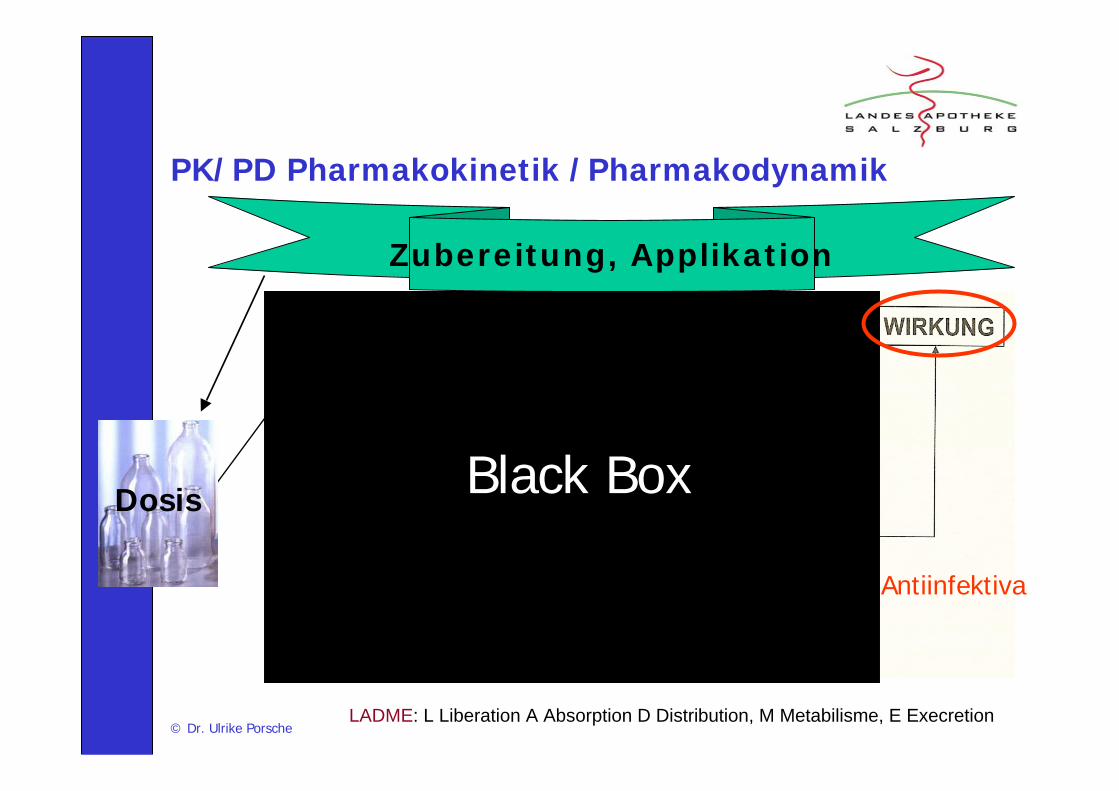
PK/PD Pharmakokinetik /Pharmakodynamik
LADME: L Liberation A Absorption D Distribution, M Metabilisme, E Execretion
Antiinfektiva
Zubereitung, Applikation
Black BoxDosis
© Dr. Ulrike Porsche
We know everything else about antimicrobials but
how much to give
Maxwell Finland (1902 – 1987)
© Dr. Ulrike Porsche
The Antimicrobial Therapy Puzzle: Could PK/ PD Relationship be helpfull in adressing the issue of appropriate Pneumonia Therapy in critically illpatients ? (Pea, CID 2006)
Antibiotic
Pathogen
+MIC
Infection site
Patient –pathophysio-
logy
YES !!!
DosageDosage interval Duration of ApplikationRoute of Applikation
© Dr. Ulrike Porsche
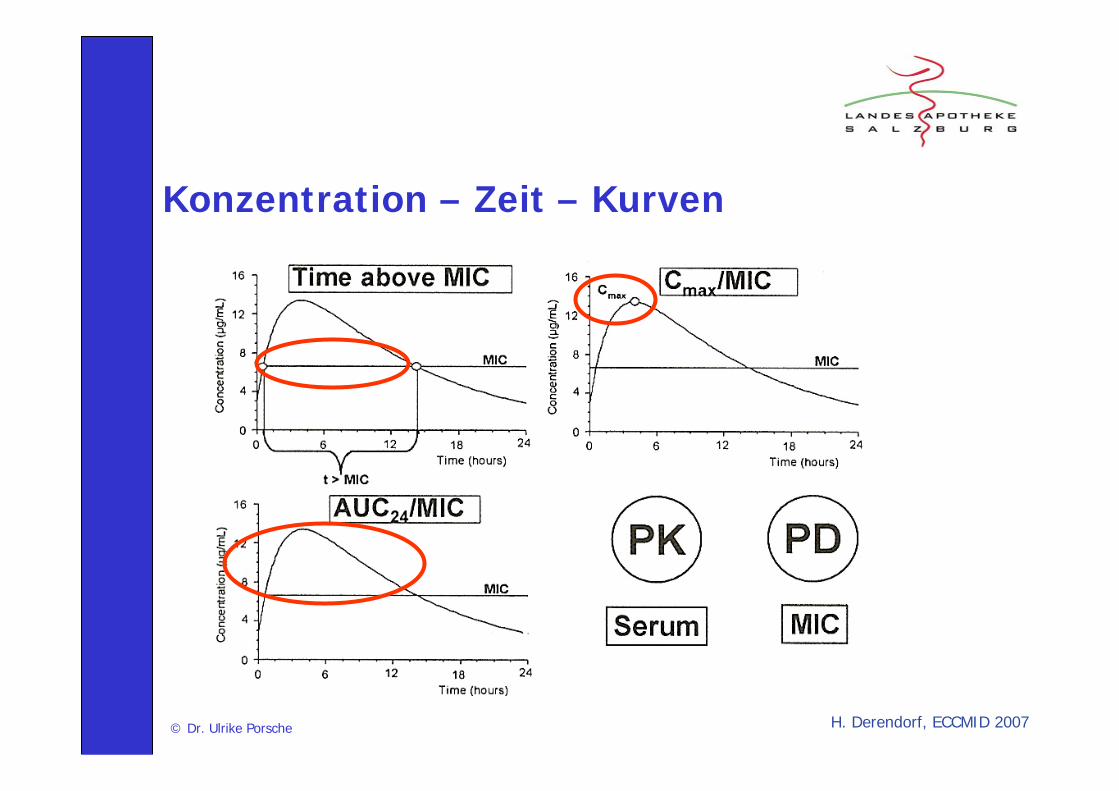
Konzentration – Zeit – Kurven
H. Derendorf, ECCMID 2007

Thalhammer, expert opinion 2009© Dr. Ulrike Porsche

© Dr. Ulrike Porsche
Betalaktame ... je länger desto besser ...
Voraussetzungen für die Möglichkeit einer verlängerten Infusionsdauer
• Ausreichende mikrobielle Stabilität der Infusionslösung• Ausreichende Kompatibilität der Infusionslösung mit
der Trägerlösung• Compliance des Patienten
© Dr. Ulrike Porsche
Prinzipien der Zubereitung und Applikation von Antiinfektiva
• Möglichst aseptische Zubereitung für eine optimale Stabilität
• Auflösung nach Bereitungsvorschrift zur Erzielung einer möglichst isotonen, gut verträglichen Infusionslösung
• Lange InfusionsdauerVancomycin, Fucidine u.a.: bessere Verträglichkeit
• Betalaktame: optimierte Wirkung
Optimierte Wirkung = weniger Resistenzen
© Dr. Ulrike Porsche
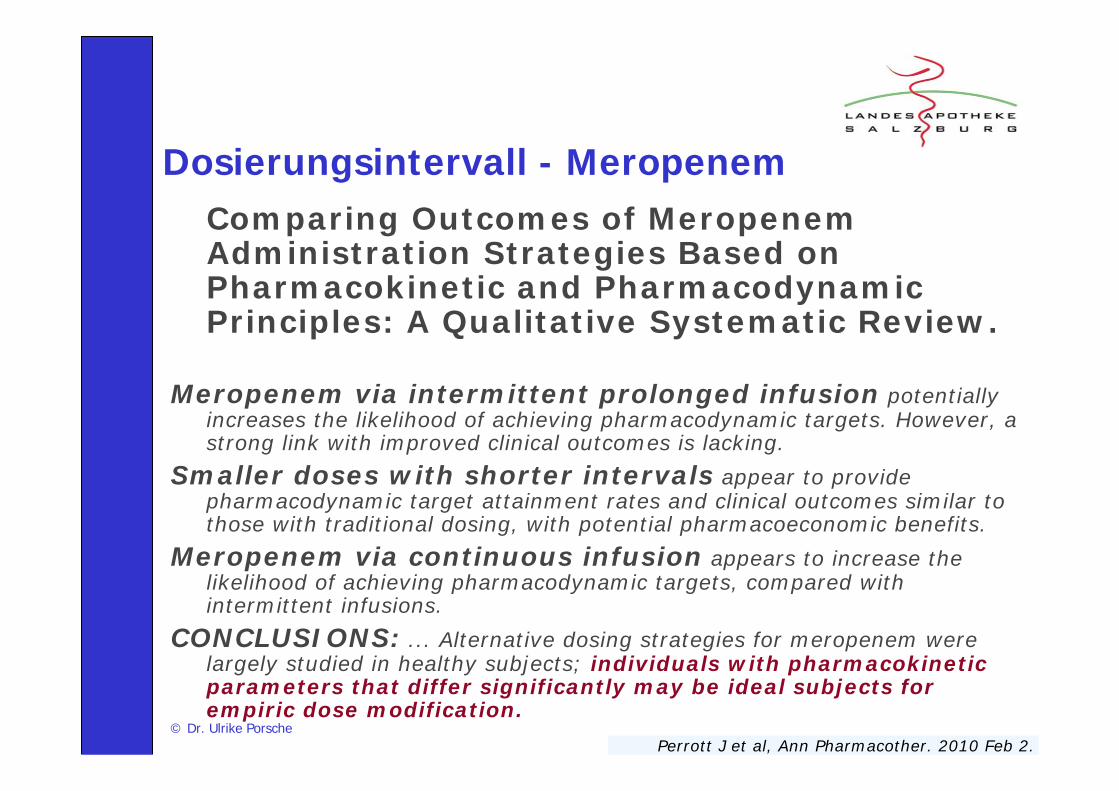
Dosierungsintervall - MeropenemComparing Outcomes of MeropenemAdministration Strategies Based on Pharmacokinetic and Pharmacodynamic Principles: A Qualitative Systematic Review.
Meropenem via intermittent prolonged infusion potentially increases the likelihood of achieving pharmacodynamic targets. However, a strong link with improved clinical outcomes is lacking.
Smaller doses with shorter intervals appear to provide pharmacodynamic target attainment rates and clinical outcomes similar to those with traditional dosing, with potential pharmacoeconomic benefits.
Meropenem via continuous infusion appears to increase the likelihood of achieving pharmacodynamic targets, compared with intermittent infusions.
CONCLUSIONS: ... Alternative dosing strategies for meropenem were largely studied in healthy subjects; individuals with pharmacokinetic parameters that differ significantly may be ideal subjects for empiric dose modification.
Perrott J et al, Ann Pharmacother. 2010 Feb 2.
Meropenem: LA. Trissel, Injectible Drugs 15th edition 2009, Doripenem: MEDIS 2010© Dr. Ulrike Porsche
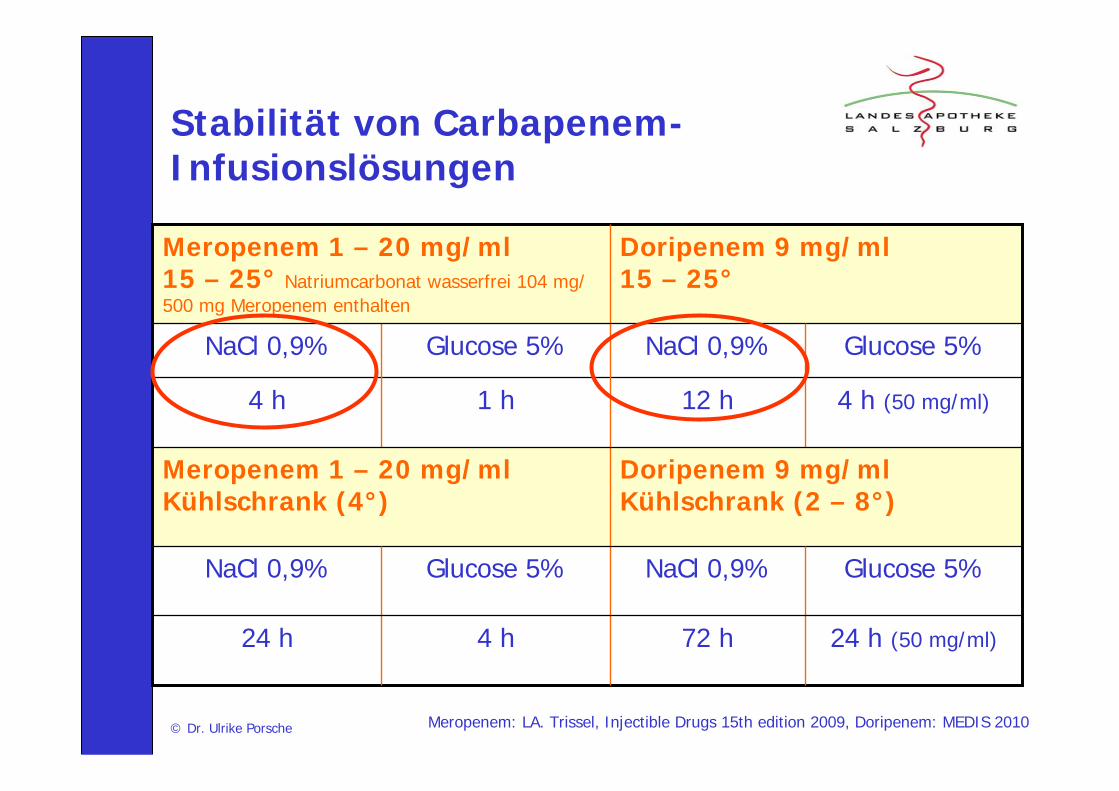
Stabilität von Carbapenem-Infusionslösungen
Glucose 5%NaCl 0,9%Glucose 5%NaCl 0,9%
24 h (50 mg/ml)72 h4 h24 h
Doripenem 9 mg/mlKühlschrank (2 – 8°)
Meropenem 1 – 20 mg/ml Kühlschrank (4°)
Doripenem 9 mg/ml15 – 25°
Meropenem 1 – 20 mg/ml 15 – 25° Natriumcarbonat wasserfrei 104 mg/ 500 mg Meropenem enthalten
Glucose 5%NaCl 0,9%
4 h (50 mg/ml)12 h1 h4 h
Glucose 5%NaCl 0,9%
EMEA 2009© Dr. Ulrike Porsche
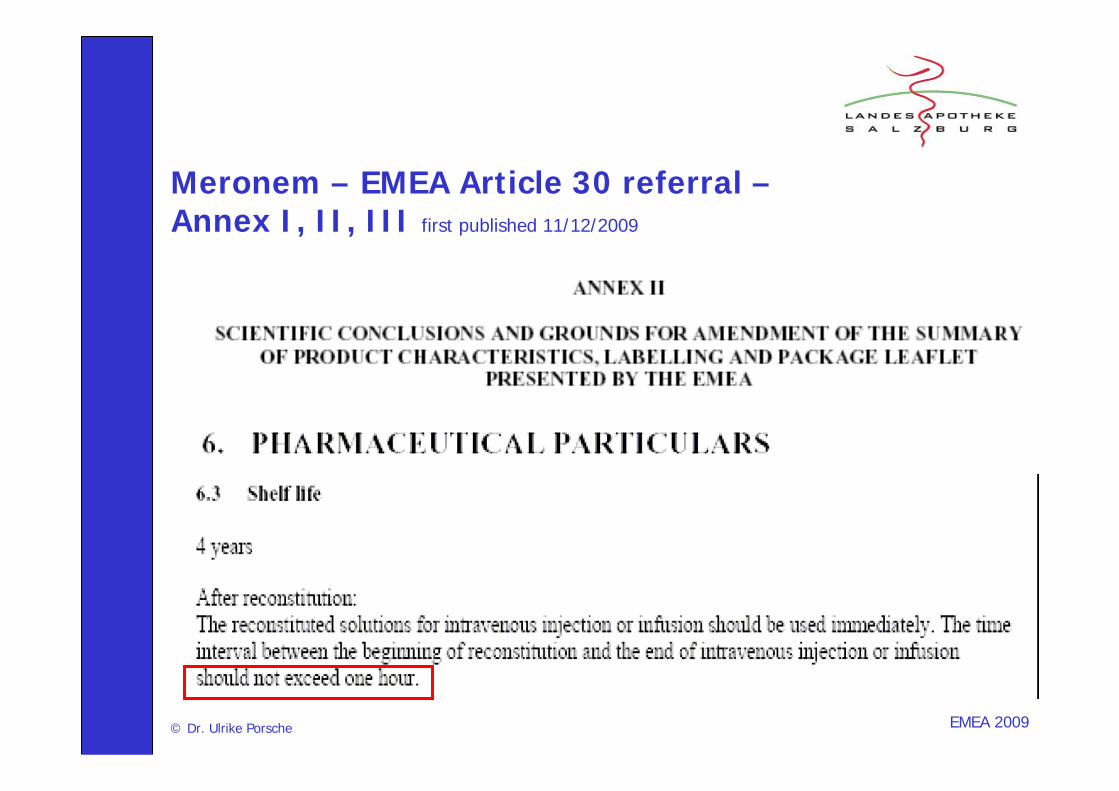
Meronem – EMEA Article 30 referral –Annex I, II, III first published 11/12/2009
K. Berthoin et al., JAC Februar 2010© Dr. Ulrike Porsche
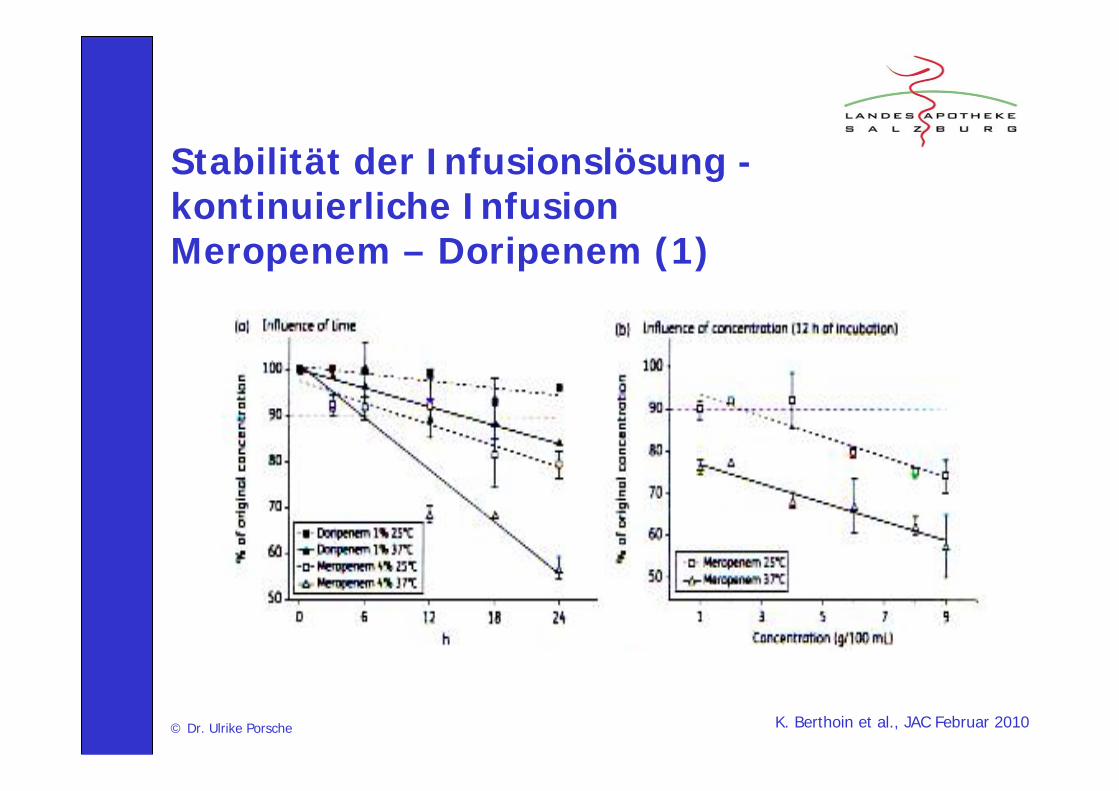
Stabilität der Infusionslösung -kontinuierliche Infusion Meropenem – Doripenem (1)
K. Berthoin et al., JAC Februar 2010© Dr. Ulrike Porsche
Stabilität der Infusionslösung -kontinuierliche Infusion Meropenem – Doripenem (2)
• niedriger konzentrierte Infusionslösungen sind stabiler als höher konzentrierte (Meropenem, für Doripenem keine Daten, weil Limitationen der Löslichkeit)
• Die Stabilität einer Lösung sinkt mit zunehmender Zeit und Temperatur (Meropenem, Doripenem)
• Bei 37° ist Doripenem stabiler als Meropenem
Auszug aus den Empfehlungen für die SALK 2010, basierend auf Fachinfos© Dr. Ulrike Porsche
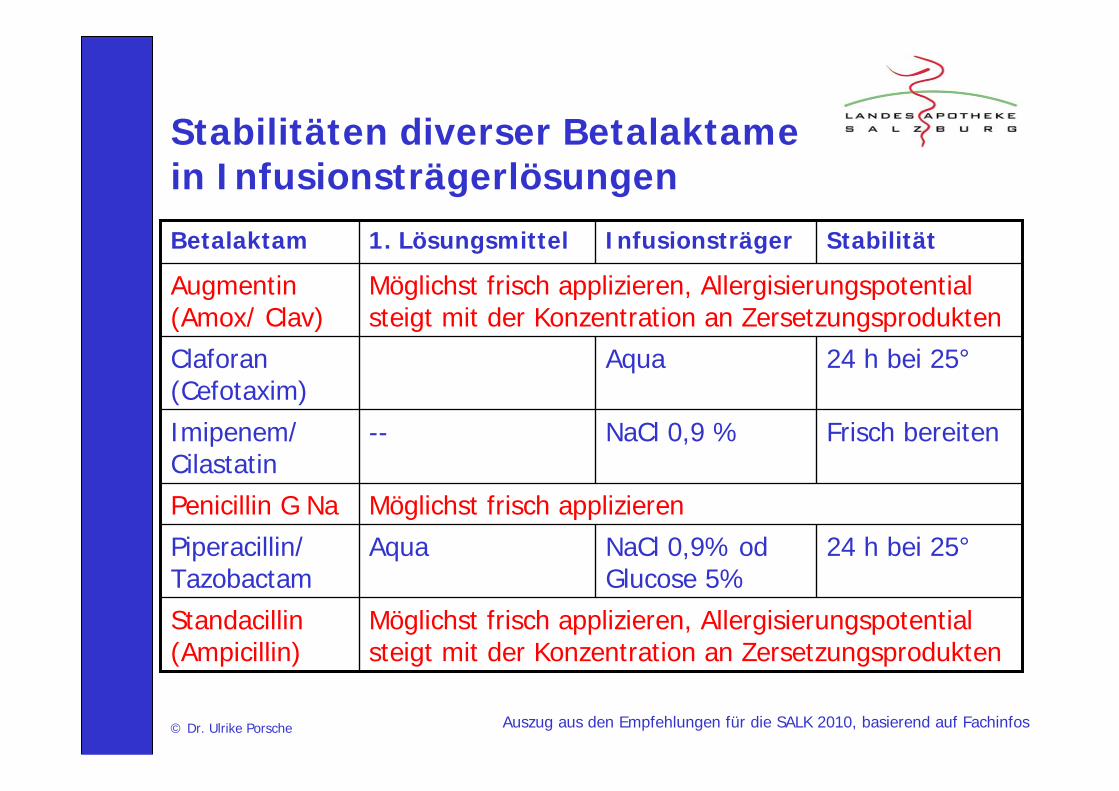
Stabilitäten diverser Betalaktame in Infusionsträgerlösungen
Möglichst frisch applizieren, Allergisierungspotential steigt mit der Konzentration an Zersetzungsprodukten
Standacillin(Ampicillin)
24 h bei 25°AquaClaforan(Cefotaxim)
StabilitätInfusionsträger1. LösungsmittelBetalaktam
24 h bei 25°NaCl 0,9% od Glucose 5%
AquaPiperacillin/ Tazobactam
Möglichst frisch applizierenPenicillin G Na
Frisch bereitenNaCl 0,9 %--Imipenem/ Cilastatin
Möglichst frisch applizieren, Allergisierungspotential steigt mit der Konzentration an Zersetzungsprodukten
Augmentin(Amox/ Clav)
© Dr. Ulrike Porsche
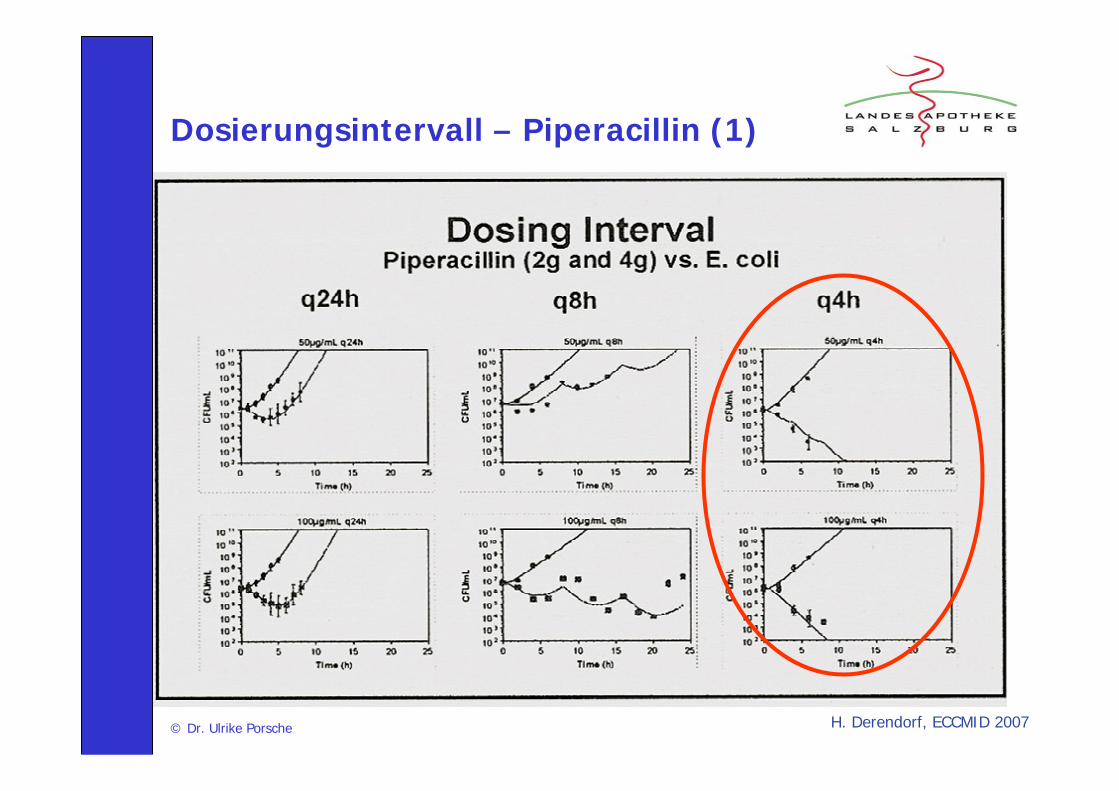
Dosierungsintervall – Piperacillin (1)
H. Derendorf, ECCMID 2007
© Dr. Ulrike Porsche
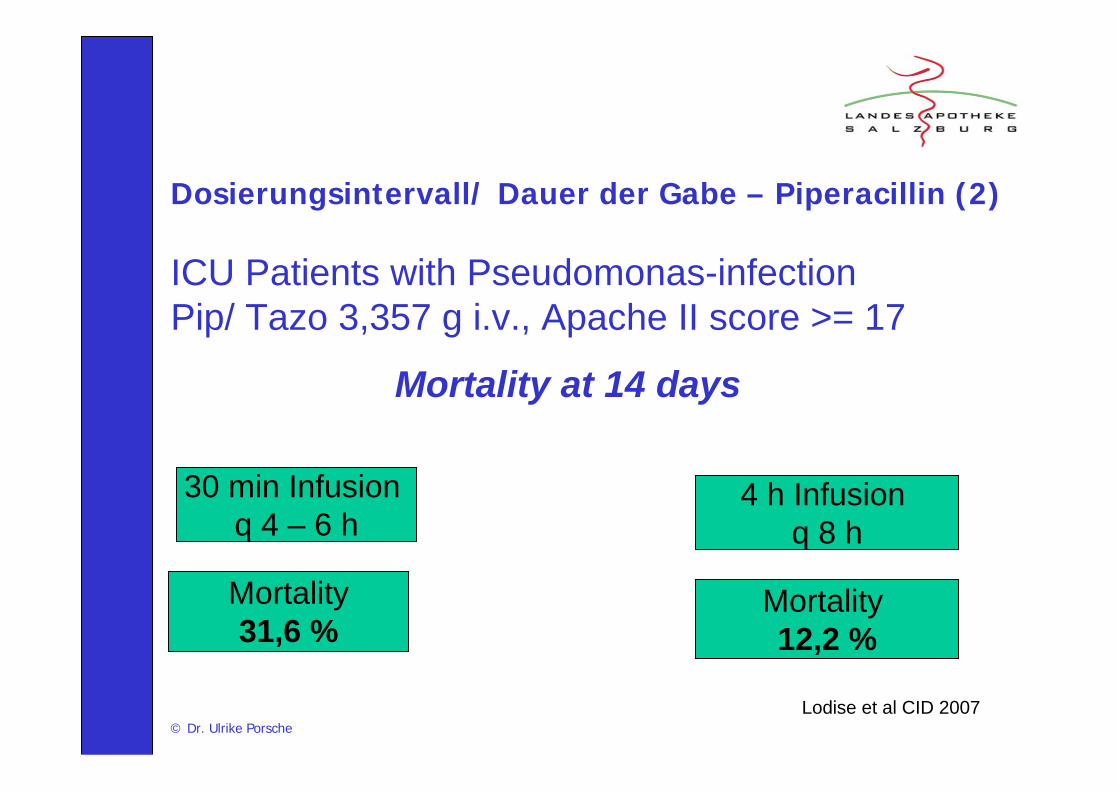
Dosierungsintervall/ Dauer der Gabe – Piperacillin (2)
ICU Patients with Pseudomonas-infectionPip/ Tazo 3,357 g i.v., Apache II score >= 17
Mortality at 14 days
30 min Infusion q 4 – 6 h
Mortality31,6 %
4 h Infusion q 8 h
Mortality 12,2 %
Lodise et al CID 2007
© Dr. Ulrike Porsche
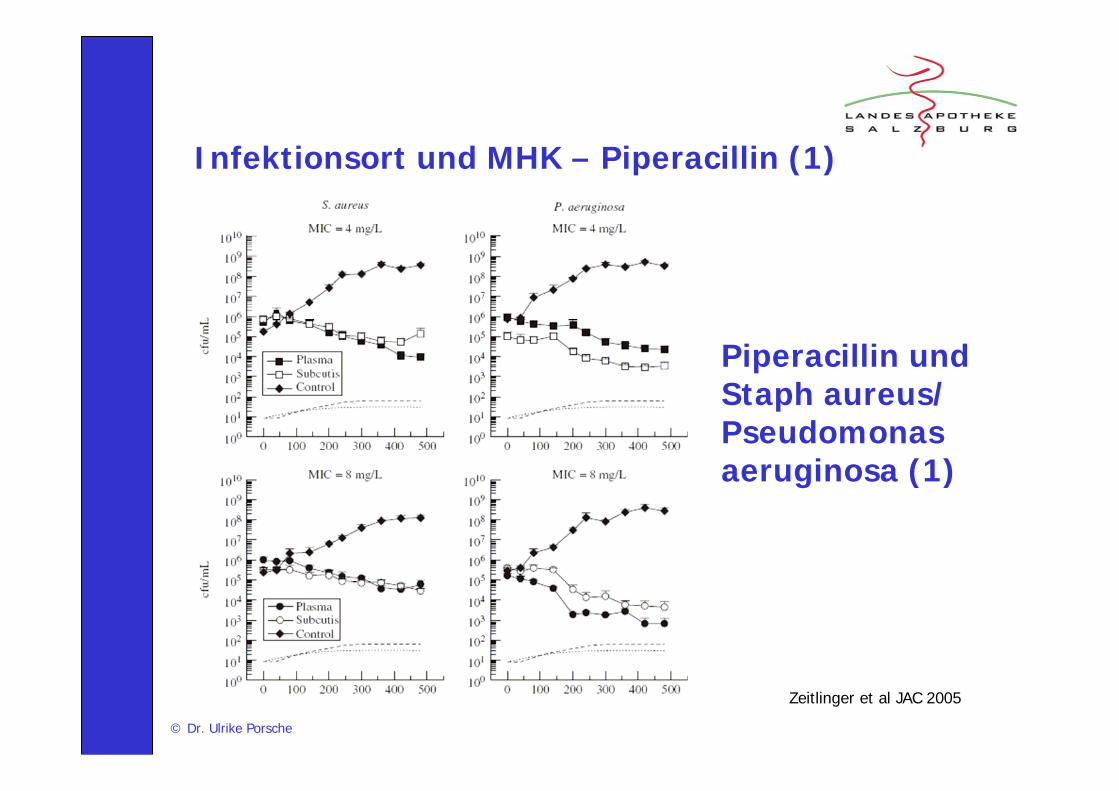
Piperacillin und Staph aureus/ Pseudomonas aeruginosa (1)
Zeitlinger et al JAC 2005
Infektionsort und MHK – Piperacillin (1)
© Dr. Ulrike Porsche
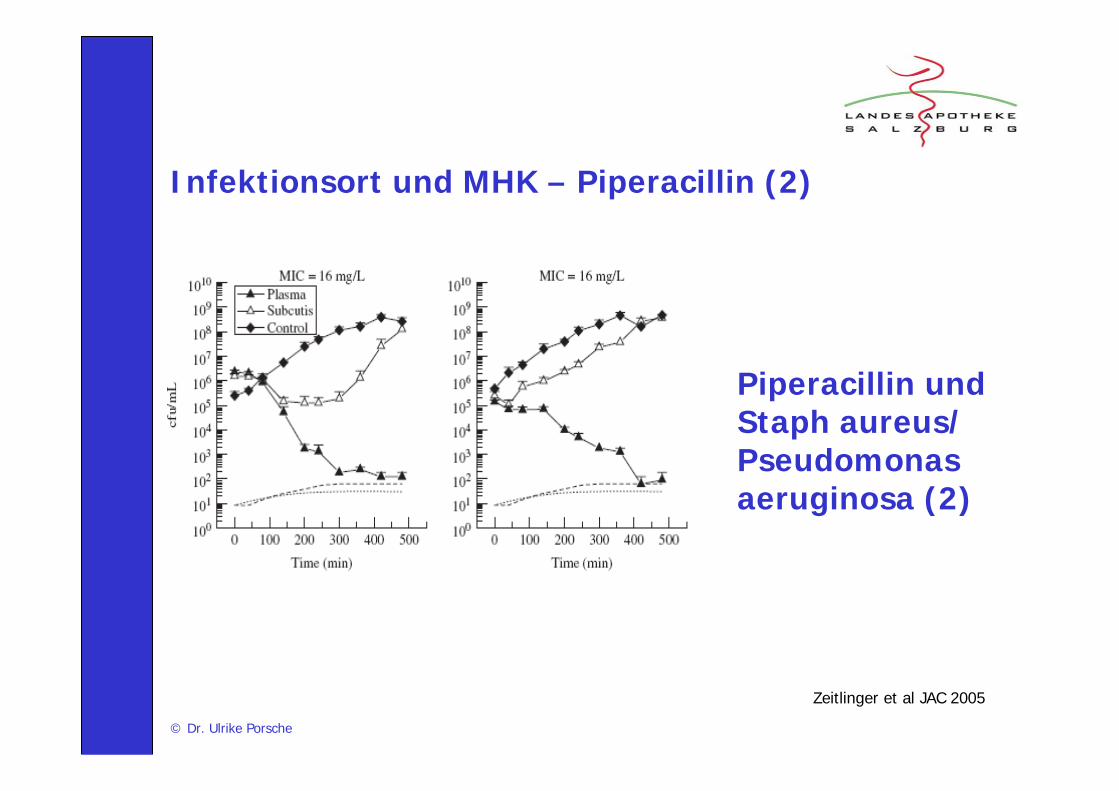
Piperacillin und Staph aureus/ Pseudomonas aeruginosa (2)
Zeitlinger et al JAC 2005
Infektionsort und MHK – Piperacillin (2)
© Dr. Ulrike Porsche
Piperacillin – Plasmaspiegel versusGewebenspiegel bei Patienten im septischen Schock
In 6 patients with septic shock, interstitial piperacillinconcentrations in skeletal muscle and subcutaneousadipose tissue were five- to ten-fold lower thancorresponding free plasma concentrations (p <.03).Mean piperacillin concentrations in subcutaneous adiposetissue never exceeded 11 microg/mL, which is belowthe minimal inhibitory concentration for a range of relevant pathogens in patients with septic shock.
Joukhadar et al., Crit Care Med. 2001
© Dr. Ulrike Porsche
Piperacillin in Patienten mit Sepsis
• Kürzere Halbwertszeit gegenüber gesunden Probanden• Gewebespiegel sind bis zu 5x niedriger als Spiegel im Plasma• Bolus-Dosierung (4 g Piperacillin über 20 min alle 6 h)
produziert niedrigere T> MIC als kontinuierliche Infusion (12 g/ 24 h)
• Bolus-Dosierung produzierte zu niedrige Talspiegel im Gewebe
• Eine um 25% niedrigere Dosierung erreichte ein höheres pharmakodynamisches Target im Gewebe
• Für MIC > 4 ist eine kontinuierliche Infusion von Vorteil
Jason et al., Crit. Care. Med. 2009, Vol 37, No 3
© Dr. Ulrike Porsche
Therapie mit Vancomycin (1)
Vancomycin on the way out?
• Toxic agent• Slow bactericidal activity• Protein binding 60% • Old antiinfective (1958)
Lode H, ECCMID 2008
Rybak et al., Am J Health-Syst Pharm, Voll 66, Jan 1, 2009© Dr. Ulrike Porsche
Rybak et al., Am J Health-Syst Pharm, Voll 66, Jan 1, 2009© Dr. Ulrike Porsche
Vancomycin – Management auf der ICU• Dosierung 2 – 3x 15 – 20 mg/kg/die mit loading dose von
25 – 30 mg/kg für Patienten mit normaler Nierenfunktion und für Keime mit MHK < = 1
• Talspiegel (Abnahme vor der 5. Dosis) sollten 15 – 20 mcg/ml betragen um bei MHK-Werten <= 1 mcg/ml eine AUC von 400 und damit einen therapeutische Erfolg zu erzielen
• Talspiegel sind immer über 10 mcg/ml zu halten um der Bildung von Resistenzen vorzubeugen
• Fazit: Bei kritisch Kranken ist die Bestimmung des MHK-Wertes als Therapie-Entscheidungshilfe sinnvoll
© Dr. Ulrike Porsche
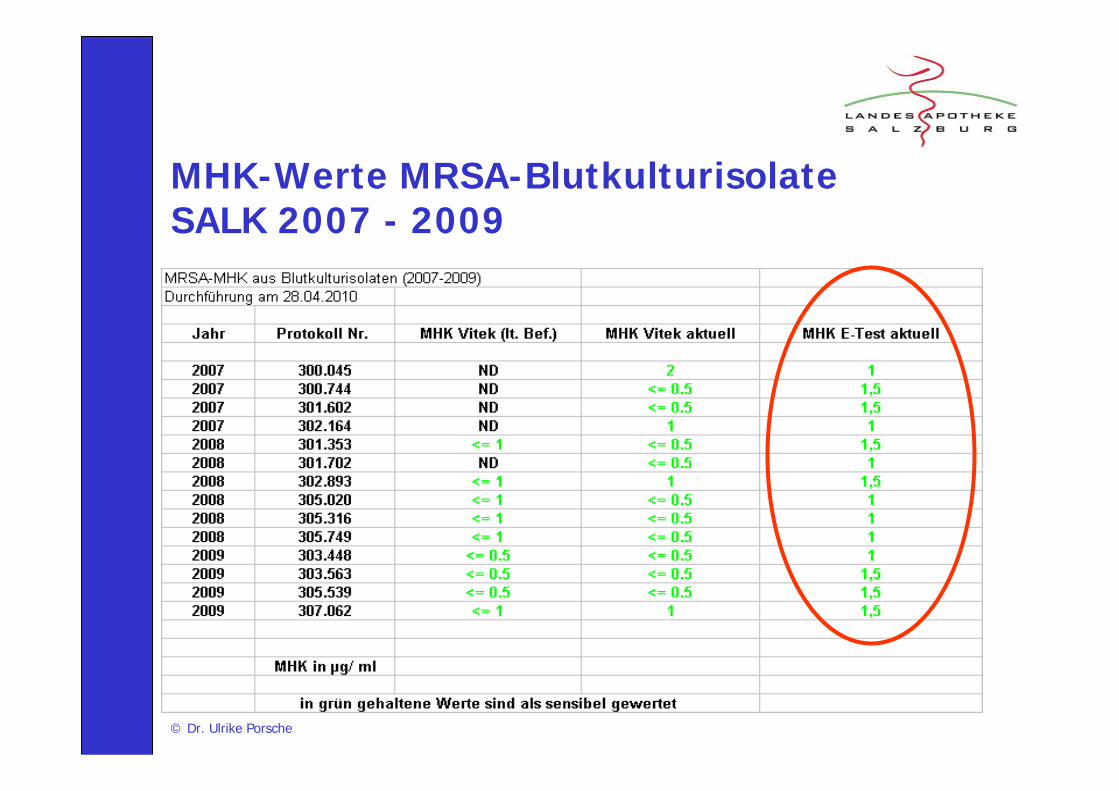
MHK-Werte MRSA-Blutkulturisolate SALK 2007 - 2009
© Dr. Ulrike Porsche
Vancomycin „Axellia“ Austria Codex 2010
Empfindliche Mikroorganismen (MIC ± 4µg/ml): Staphylokokken, Streptokokken, Enterokokken, Pneumokokken. Staphylococcus aureus-Stämme mit mittlerer Empfindlichkeit gegenüber Vancomycin (VISA) wurden berichtet. Methicillinresistente Staphylococcus aureus(MRSA)-Stämme mit verminderter Vancomycin-Empfindlichkeit wurden beschrieben.
Mikroorganismen mittlerer Empfindlichkeit (4 µg/ml < MIC < 8 µg/ml): Actinomyces, Clostridium und Corynebacterium(Diphteriodes) Spezies.
Nicht empfindliche Mikroorganismen (MIC > 8 µg/ml): Gramnegative Stäbchen. Leuconostoc, Lactobacillus, Pediococcus und Erysipelothrix. Es wurde eine Kreuzresistenz mit Teicoplanin berichtet.
© Dr. Ulrike Porsche
Therapie mit Vancomycin (2)
Grenzwerte für den Talspiegel von Vancomycin
1. 5 – 8 mcg/ml2. 5 – 10 mcg/ml3. 8 – 12 mcg/ml4. 5 – 15 mcg/ml5. 15 – 20 mcg/ml
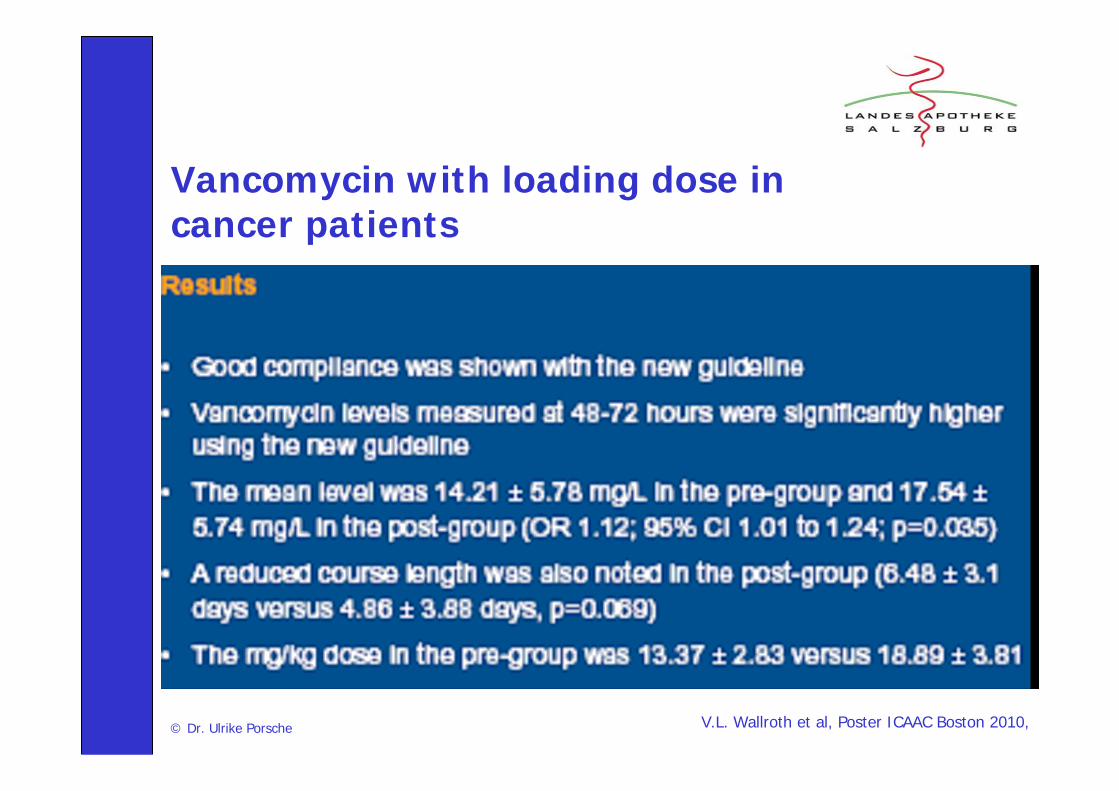
V.L. Wallroth et al, Poster ICAAC Boston 2010, © Dr. Ulrike Porsche
Vancomycin with loading dose in cancer patients
© Dr. Ulrike Porsche
Applikation von Vancomycin i.v.
• Während oder kurz nach einer schnellen Infusion können anaphylaktische Reaktionen auftreten. Die Reaktionen klingen im Allgemeinen binnen 20 Minuten bis 2 Stunden nach Beendigung der Infusion ab MEDIS 2010
• Infusionsdauer mindestens 60 min MEDIS 2010
• Bei Vancomycin-Einzeldosen von mehr als 1,0 g (1,5 g oder 2 g) sind die Infusionszeiten auf 1,5 – 2 h zu verlängernRybak et al AJHP 2009
• Eine kontinuierliche Infusion hat keinen entscheidenden therapeutischen Vorteil gegenüber einer intermittierenden Gabe Rybak et al AJHP 2009
• Perioperative Prophylaxe mit Vancomycin: Beginn der Infusion 1h vor Hautschnitt !

S. Sivagnanam et al., Crit Care. 2003; 7(2): 119–120. © Dr. Ulrike Porsche
Red man syndrome
• 4 – 10 min after begin of infusion or soon after end of infusion• It is often associated with rapid (<1 hour) infusion of the first dose of
vancomycin.• It typically consists of pruritus, an erythematous rash that involves the
face, neck, and upper torso. Less frequently, hypotension and angioedema can occur. Patients commonly complain of diffuse burningand itching and of generalized discomfort. They can rapidly become dizzy and agitated, and can develop headache, chills, fever, and paresthesia around the mouth. In severe cases, patients complain of chest pain and dyspnea. In many patients, the syndrome is a mild, evanescent pruritus at the end of the infusion that goes unreported.
• Antibiotics such as ciprofloxacin, amphotericinB, rifampcin and teicoplanin can potentially cause red man syndrome.
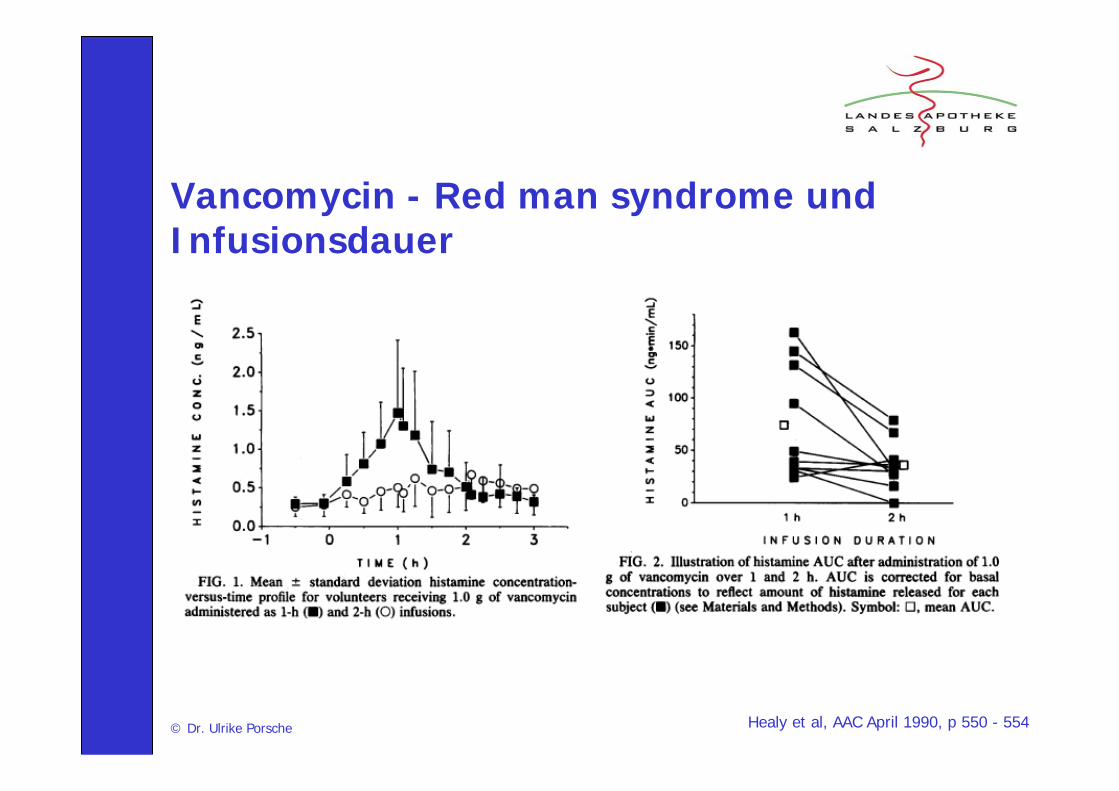
Healy et al, AAC April 1990, p 550 - 554© Dr. Ulrike Porsche
Vancomycin - Red man syndrome und Infusionsdauer
© Dr. Ulrike Porsche
i.v.-Schwerkraftapplikation und Restvolumen von Antiinfektiva
Dosisrelevanter Verlust bei• Kurzinfusion von kleinen Volumina (50 ml)• Therapie mit Niedrigdosierungenca. 20 ml Restvolumen kann im
Schlauchsystem verbleiben !!
© Dr. Ulrike Porsche
Take Home Massage
Eine adäquate Zubereitung und Applikation (Infusionsdauer !) von Antibiotika kann bei Patienten mit septischem Zustandsbild:
• den Therapieerfolg optimieren • die Therapiedauer verkürzen und Kosten sparen • die Verträglichkeit verbessern• Und somit das Auftreten von Resistenzen minimieren