
2016-05 Pflegekongress - lymphome - gh 3108 · § B-cell receptor pathway inhibitors § SYK § BTK...
48
Wahlfach Mai 2016 LYMPHATISCHE NEOPLASIEN 1
Transcript of 2016-05 Pflegekongress - lymphome - gh 3108 · § B-cell receptor pathway inhibitors § SYK § BTK...
Wah
lfach
Mai
201
6
LYMPHATISCHE NEOPLASIEN
1

Wah
lfach
Mai
201
6
Lymphatische Systemerkrankungen
2

Wah
lfach
Mai
201
6
MALIGNE LYMPHOME –ALLGEMEINE EINFÜHRUNG
3

Wah
lfach
Mai
201
6
Definition
§ Maligne Lymphome umfassen eine Gruppe sehr heterogener Erkrankungen maligne entarteter lymphatischer Zellen § mit langsam verlaufenden bis rasch progredienten
Verlaufsformen sind unterschiedliche Entitäten eingeschlossen
§ Eine gebräuchliche Unterteilung in: „indolente und aggressive Lymphome“ kennzeichnet hierbei den biologischen Charakter der Erkrankungen

Wah
lfach
Mai
201
6
Historische Entwicklung§ 1832§ Erstbeschreibung: „on some morbid appearances of the
absorband glands“ durch T. Hodgkin 1832 à M. Hodgkin
§ ca. 1900§ Durch Beschreibung der Reed-Sternberg-Zelle
Unterteilung zwischen Hodgkin Lymphom und anderen Lymphomen (Non-Hodgkin)
§ Seit 1950 Klassifikationssysteme für NHL§ Kiel-Klassifikation (Klinik und Histologie), Working Group
(Morphologie), REAL (Fusionsklassifikation)§ WHO Klassifikation Version I-IV (2008)§ Seit WHO formal Bezeichnung für die NHL als „reifzellige
Maligne Lymphome“ der B- und T-Zell-Reihe§ Unterteilung dieser Gruppe nach Klinik in aggressive und
indolente Lymphome
Three things are for sure in life: „you gonna die, yougonna pay taxes andlymphoma classification will change“
Morpho-logie
-
Biologie
Wah
lfach
Mai
201
6
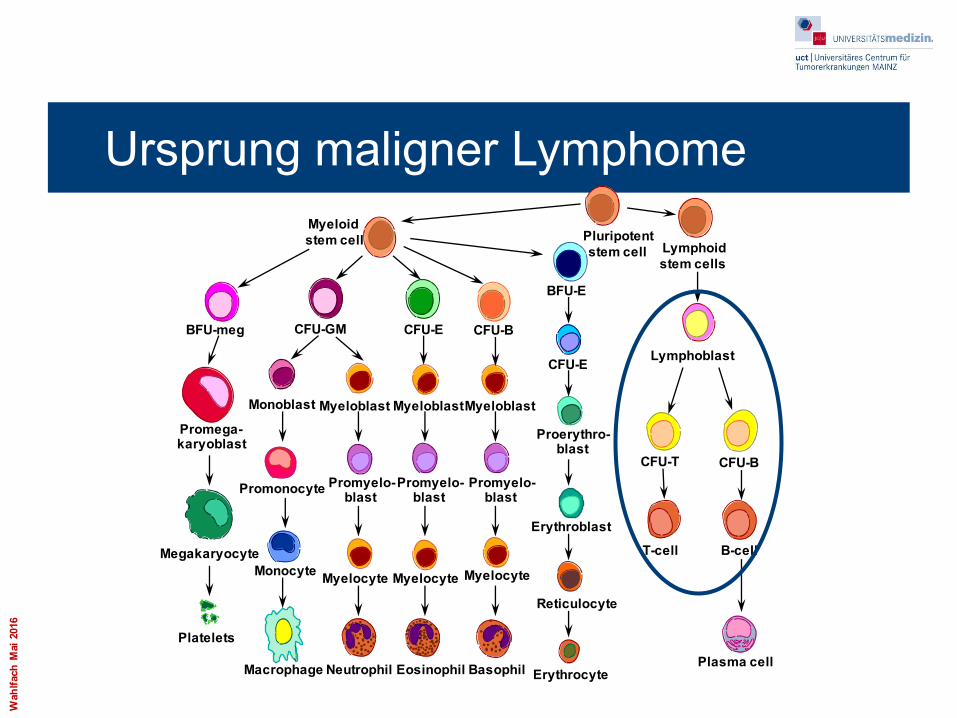
Ursprung maligner Lymphome
BFU-meg CFU-GM CFU-E CFU-B
BFU-E
CFU-E
CFU-T
Proerythro-blast
Erythroblast
Reticulocyte
ErythrocyteBasophilEosinophilNeutrophilMacrophage
Platelets
Megakaryocyte
Promega-karyoblast
Monocyte
Promonocyte
Myelocyte
Promyelo-blast
Promyelo-blast
Promyelo-blast
Myelocyte Myelocyte
Monoblast Myeloblast MyeloblastMyeloblast
CFU-B
T-cell B-cell
Plasma cell
Lymphoidstem cells
Pluripotentstem cell
Myeloidstem cell
Lymphoblast

Wah
lfach
Mai
201
6
Age specific incidences
7
Wah
lfach
Mai
201
6
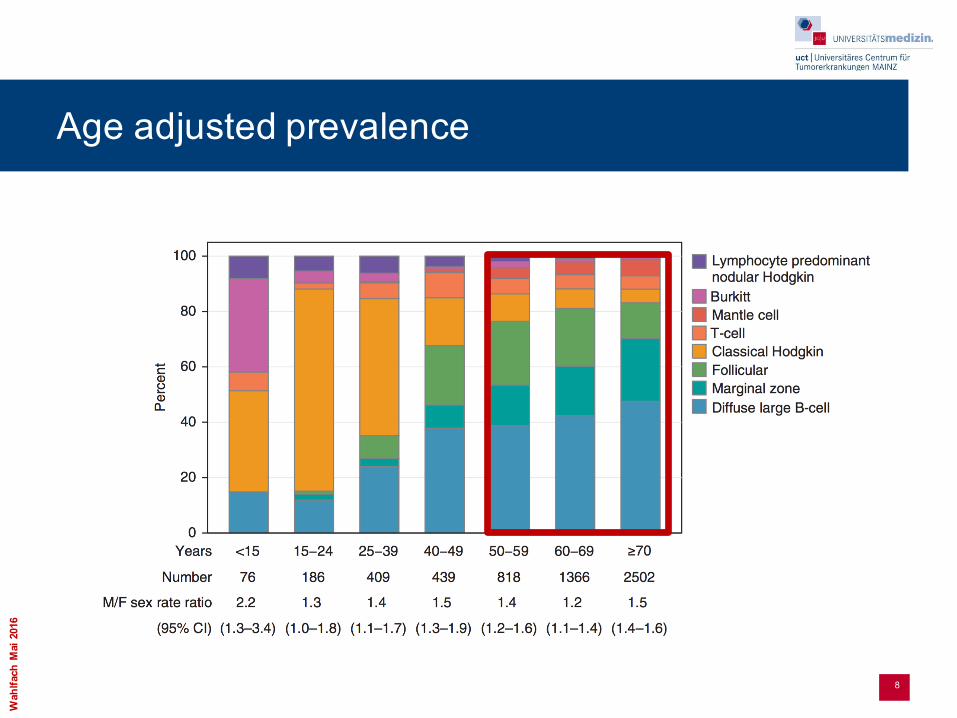
Age adjusted prevalence
8

Wah
lfach
Mai
201
6
Klinik§ Verlauf
§ Beginn meist beschwerdearm/-frei, heterogener Verlauf§ Unterschiedliche Wachstumskinetik
§ Symptome § Lymphknotenschwellung häufigster Primärbefund
§ Häufig am Hals, Nacken, aber auch in Axilla oder Leiste§ NHL können aber in fast allen Bereichen des Körpers primär
auftreten: Magen-Darm-Trakt, Lunge, extranodal: Gehirn, Haut, etc.§ Beschwerden/Komplikationen durch Beeinträchtigung großer Organe§ Blutbild-Veränderungen durch Knochenmarkinfiltration
§ Zytopenie: Anämie, Thrombopenie, Leukopenie / -zytose: Schwäche, Blutung, Infektionen
§ Allgemeinsymptome§ Fieber, Nachtschweiß, Gewichtsverlust (=B-Symptome), Juckreiz
§ Aber: „Bunte“ klinische Bilder: Schmerzen, Ikterus, Hämolyse, Einflussstauung…
MH NHL

Wah
lfach
Mai
201
6
Lymphome§ Hodgkin Lymphome: ca. 15% der Fälle
§ B-Zell-Lymphome: ca. 75% der Fälle§ aggressive Non-Hodgkin-Lymphome, vor allem
DLBCL§ indolenten Non-Hodkin-Lymphome, vor allem
follikuläre NHL
§ T-Zell-Lymphome: ca. 10% der Fälle

Wah
lfach
Mai
201
6
Diff. großzell. B-NHL35,0%Mantelzell-NHL
6,0%
Follikuläre NHL22,0%
MALT/Marginalzonen-NHL10,3%
sonstige13,9%
Periphere T-NHL5,0%
B-CLL/ Immunozytom7,9%
B-Zell-Lymphome - Verteilung

Wah
lfach
Mai
201
6
Ursprungszellen und Lymphomuntergruppe
CFU-T CFU-B
T-cell B-cell
Plasma cell
Lymphoidstem cells
Lymphoblast
Sehr hoch Sehr schnell Ja höchstaggressive
LymphomeAkute lymphatische Leukämie
Hoch Schnell Nein Hochaggressive nodale Lymphome Burkitt-Lymphom
Noch hoch Rasch Nein Aggressive Lymphome
Diffus großzelliges Lymphom
Mittel Mittel Nein Intermediär aggressive
Mantelzell-lymphom
Gering Langsam Nein Niedrigmaligne Lympome
Chronisch lymphatische Leukämie, Marginalzonen-lymphom, foll. Lymphom
selten selten nein Multiples Myelom
Teilungsrate Wachstum Selbsterhalt Tumorvariante Bezeichnung

Wah
lfach
Mai
201
6
Vereinfachte Einteilung maligner Lymphome
B-Zell (85-90%) T-Zell (10-15%)
Indolenter Verlauf FL, MZL, (CLL, MM) Kutane Lymphome
Aggressiver VerlaufDLCL
Burkitt-LymphomeAILD, peripheral T-cell lymphoma NOS
MCL
FL = Follikuläres Lymphom, DLCL = Diffus großzelliges Lymphom, MZL = Marginalzonenlymphom, MCL = Mantelzelllymphom; CLL = Chronische Lymphatische Leukämie, MM = Multiples Myelom, AILD = angioimmunoblastic lymphoma, NOS = not otherwise specified

Wah
lfach
Mai
201
6
Ann-Arbor-Klassifikation

Wah
lfach
Mai
201
6
2015 – Lymphoma prognosis
Smith et al, Br J Cancer, 2015
Paragranuloma
MCL
DLBCLBurkitt
cHDSystemic MZL FLMZL

Wah
lfach
Mai
201
6
AGGRESSIVE LYMPHOME -DLBCL
16

Wah
lfach
Mai
201
6
Klinik – aggressive Lymphome§ Aggressive Lymphome:
§ Schneller Fortschritt der Krankheit§ Lebenserwartung ohne Behandlung: ca. 1 Jahr
§ Zerstörung von Organen durch große Tumormasse (kann mehrere Kilogramm betragen)
Wah
lfach
Mai
201
6
Therapie – Grundsätze § Aggressive Lymphome („ Hoch- maligne“)
§ Homogene Wachstumsfraktion, Suszeptibilität gegenüber Systemtherapie.
§ primär kurative Therapieintention§ immer systemisch§ Heilung: 40 - 60 - 80 – 100%(?) in Abhängigkeit von
Prognoseparametern§ Ungünstig: double hit (bcl2, bcl6, myc)
§ Sehr aggressive Lymphome (Burkitt-NHL)§ Primär kurativ, 60- 70% Heilung§ ALL- ähnliche Mehrphasenprotokolle, i. th. Prophylaxe

Wah
lfach
Mai
201
6
Klinische Prognosesysteme: IPI
Risikofaktoren Parameter BeschreibungAlter > 60Stadium III-IVExtranodaler Befall > 1 RegionWHO-Performance > 1LDH erhöht
International Prognostic Index (IPI) Risikogruppen Anzahl der Risikofaktorenlow 0-1low intermediate 2high intermediate 3high 4
Age adjusted index <60 J Risikogruppen Anzahl der Risikofaktorenlow 0low intermediate 1high intermediate 2high 3
International Prognostic Risk Index
grau hinterlegt die RF, die auch im Age adjusted Index verw endet w erden
A predictive model for aggressive non-Hodgkin’s lymphoma. The InternationalNHL Prognostic Factors Project. N. Engl. J. Med. 329, 987–994 (1993).
Wah
lfach
Mai
201
6
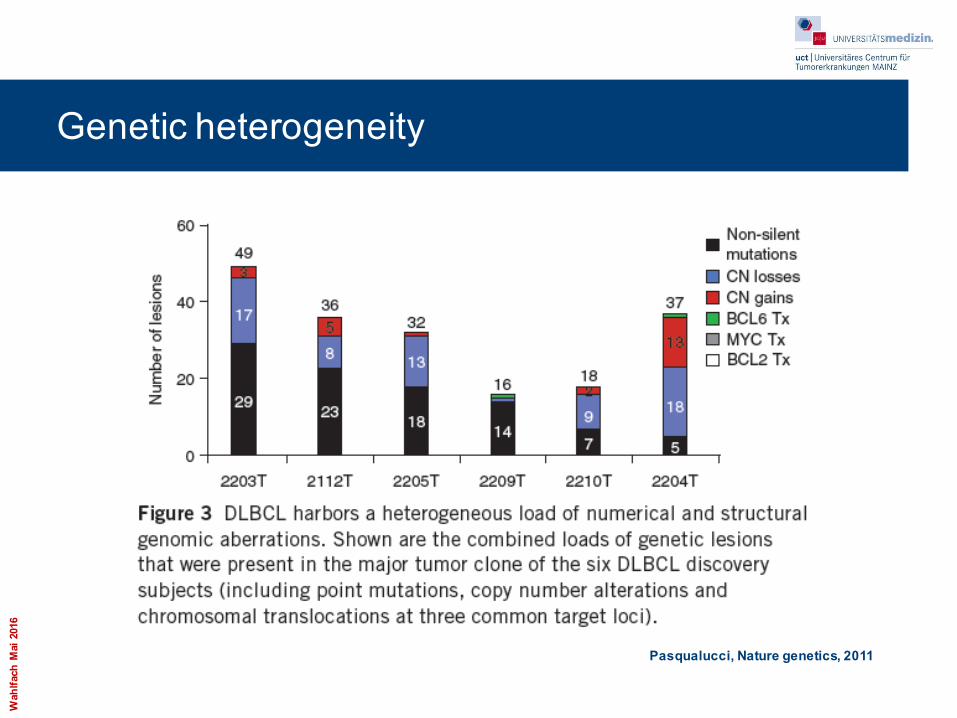
Genetic heterogeneity
Pasqualucci, Nature genetics, 2011

Wah
lfach
Mai
201
6
GEP predicts survival in DLBCL
21Lenz et Staudt, NEJM, 2010

Wah
lfach
Mai
201
6
THERAPIE
22

Wah
lfach
Mai
201
6
Hit it hard and early

Wah
lfach
Mai
201
6
GELA LNH 98-5
24Coiffier et al, NEJM , 2002

Wah
lfach
Mai
201
6
Lack of response and early relapse define poorest riskpopulation
25

Wah
lfach
Mai
201
6
Relapse Treatment: PARMA study: High dose therapy vs salvage chemotherapy in relapsed DLBCL
P = .0010
20
40
60
80
100
EFS
(%)
0 15 30 45 60 9075Mos After Randomization
P = .0380
20
40
60
80
100
OS
(%)
0 15 30 45 60 9075Mos After Randomization
TransplantationConventional treatment
Philip T et al. N Engl J Med 1995;333:1540-1545
Wah
lfach
Mai
201
6
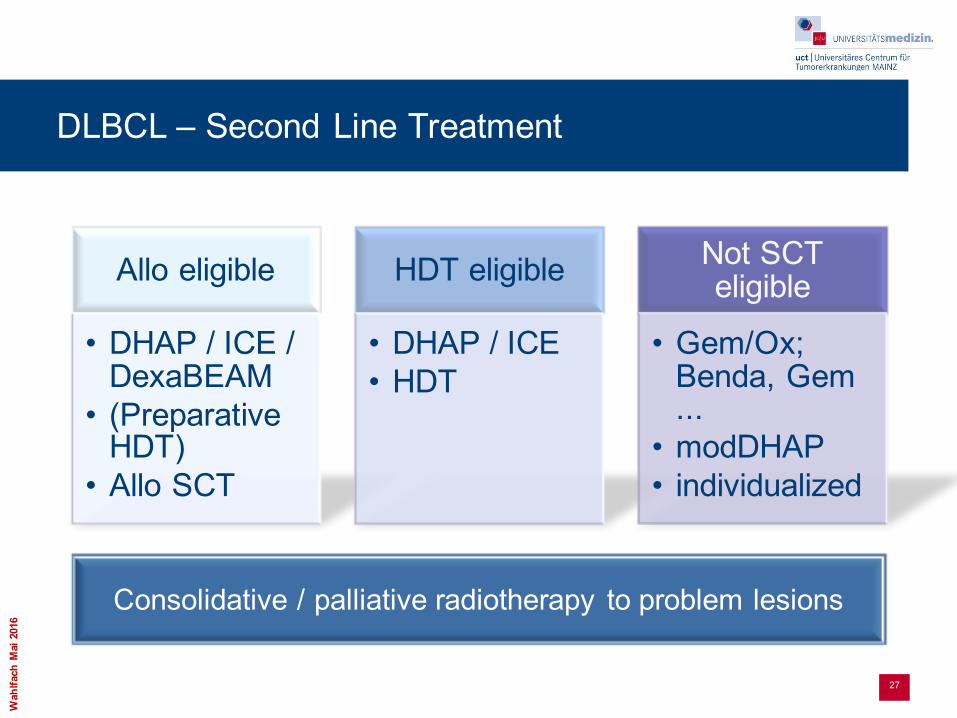
DLBCL – Second Line Treatment
27
Allo eligible
• DHAP / ICE / DexaBEAM
• (PreparativeHDT)
• Allo SCT
HDT eligible
• DHAP / ICE• HDT
Not SCT eligible
• Gem/Ox; Benda, Gem...
• modDHAP• individualized
Consolidative / palliative radiotherapy to problem lesions

Wah
lfach
Mai
201
6
INDOLENTE LYMPHOME
28

Wah
lfach
Mai
201
6
„indolente“ versus „aggressive“ Lymphomen§ DiemalignenLymphomeumfasseneineGruppesehrheterogener Erkrankungen
maligneentarteterlymphatischerZellen
§ KlinischerVerlauf§ IndolenteLymphomesinddurcheinen langsamen,oftasymptomatischen
Verlaufcharakterisiert§ AggressiveLymphomesinddemgegenüber inderRegelraschprogredient
§ TherapeutischeKonsequenz§ DurchdieniedrigeWachstumsfraktion geltenindolente Lymphomeals
inkurable Erkrankung undwerdenbeiklinischenBeschwerdentherapiert§ DiegleichförmigeWachstumsfraktion beiaggressiven Lymphomen erlaubt
einenkurativen TherapieansatzdurchdirektenEinsatzeinerSystemtherapie

Wah
lfach
Mai
201
6
Differentialbetrachtung indolenter Lymphome
30
Follikuläres Lymphom
• LK-Befall• Zytopenien• B-Symptome• Infektionen
Marginalzonen-lymphome
• Versch. Formen • Häufig in
Drüsengewebe, Milzbefall
• Assoziation mit bakteriellen und viralen Infektionen
• Verlauf und Therapie ähnlich FL
M. Waldenström
• Lymphoplasmo-zyischesLymphom mit IgM
• Knochenmark-befall, selten LK-Vergrößerungen
• Komplikationen durch IgM-Vermehrung (Neuropathie, rheolog. Ver-änderungen)
• Eigene Behandlungs-standards
Haarzell-leukämie
• Typische Trias: Splenomegalie, Zytopenie, Infektionen
• Therapie mit Nukleosid-analoga
Wah
lfach
Mai
201
6
FOLLIKULÄRES LYMPHOM ALS MODELLERKRANKUNG
31

Wah
lfach
Mai
201
6
§ Verlauf§ Heterogener, oft asymptomatischer Verlauf bei
Großteil der Patienten, von daher§ Diagnose von ca. > 90% aller Patienten im
fortgeschrittenem Stadium§ Klinik
§ Lymphknotenvergrößerung bei >80%§ Gelegentlich fluktuierend§ Häufig axilläre, cervikale, inguinale,
hiläre und abdominelle LK undabdomineller Bulk (Tu > 7,5cm)
§ B-Symptome bei ca. 20-30%§ Splenomagalie bei ca. 40%§ KM-Infiltration bei ca. 60-70%
Das häufigste Indolente NHL
§ Inzidenz§ 25% aller B-NHL in westlichen Ländern, 4-
6/10000/a§ Variabilität in verschieden Ethnien: Kaukasier
>> Asiaten, Schwarzafrikaner § Keine validierten Risikofaktoren, seltene
familiäre Fälle§ Erkrankungsgipfel > 60 Jahre§ Subtypen (WHO 2008)
§ Indolent§ Grade 1,2 – 75%§ Grade 3A – 20%
§ Aggressiv§ Grade 3B – 5%

Wah
lfach
Mai
201
6
Abschätzung der Lebenserwartung und Risikostratifizierung„FL international prognostic index (FLIPI)“
§ Parameter§ ≥ 5 befalle LK-Stationen§ Erhöhte LDH§ Alter ≤ 60 versus > 60 years§ Ann Arbor Stadium 3/4§ Hämoglobin <12 g/dL
§ Risikogruppen§ Niedriges Risiko: 0-1§ Mittleres Risiko: 2§ Hohes Risiko: 3+
33Solal-Celigny, P. et al. Blood 2004;104:1258-1265

Wah
lfach
Mai
201
6
Early Progression of Disease (POD)
§ Definitions:§ Early POD: within 2 years of
diagnosis§ OS of early POD: from time of
progression§ OS for no early POD: from 2
years after diagnosis§ Limitations:
§ Early POD is a post-treatment variable for risk stratification
§ Patients dying within 2 years without documented POD are not evaluable
§ Conclusion:§ Clinical need for a pre-treatment
risk algorithm
surv
ival
pro
babi
lity
overall survival (OS) [months]
no early POD
early POD19% of patients
Jurinovic V et al. Abstract No. 333

Wah
lfach
Mai
201
6
Warum „Watch and Wait“?
35Ardeshna et al, Lancet, 2003
Wah
lfach
Mai
201
6
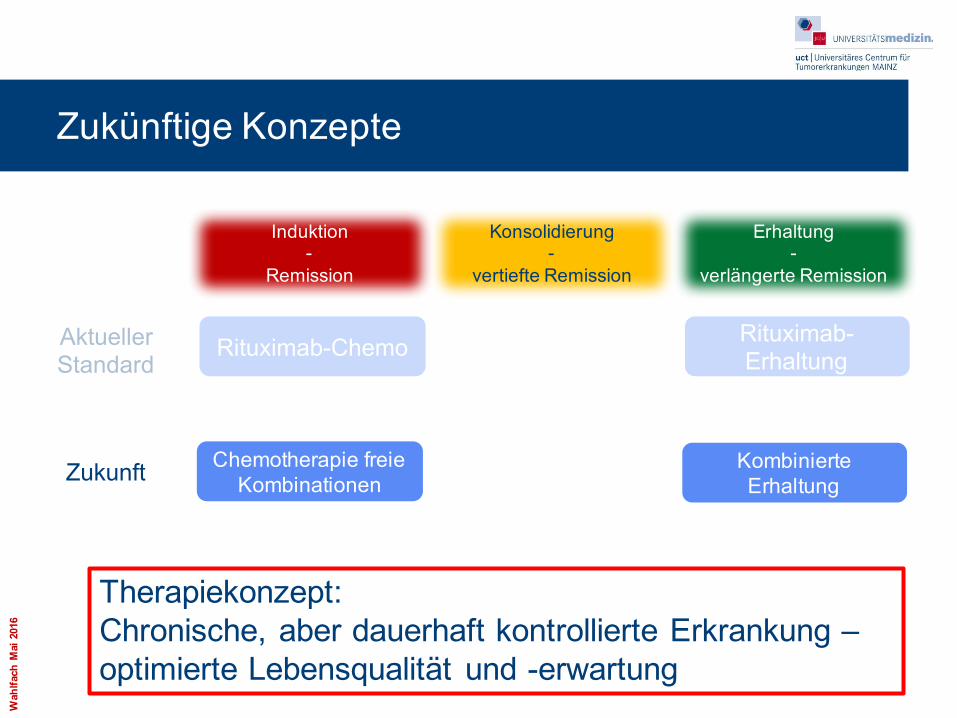
Zukünftige Konzepte
Induktion-
Remission
Konsolidierung-
vertiefte Remission
Erhaltung-
verlängerte Remission
AktuellerStandard
Zukunft
Rituximab-Chemo Rituximab-Erhaltung
Chemotherapie freie Kombinationen
Kombinierte Erhaltung
Therapiekonzept: Chronische, aber dauerhaft kontrollierte Erkrankung –optimierte Lebensqualität und -erwartung
Wah
lfach
Mai
201
6
Zusammenfassung indolente Lymphome§ Langsam verlaufende, initial oft asymptomatische Erkrankungen§ Klinik: LK-Schwellungen, Anämie, Schwäche, Infekte
§ Nur in limitierten Stadien mit konventioneller Therapie (Radiatio) heilbar§ Therapieeinleitung aufgrund klinischer Beschwerden§ In fortgeschrittenen Stadien sehr viele Therapieoptionen – individuelle
Entscheidung§ Antikörpertherapie fester Bestandteil der Systemtherapie§ Rezidivtherapie wiederholt möglich, Auswahl abhängig vom bisherigen
Erkrankungs- und Therapieverlauf§ Refraktäre Erkrankung und Transformation therapeutische
Herausforderung§ Neue zielgerichtete Therapien schon zugelassen, weitere in Entwicklung
§ Überleben heute im Median ca. 15 + Jahre, Verbesserung mit weiteren Therapieoptionen möglich

Wah
lfach
Mai
201
6
Weiterentwicklung der Therapie verbessert die Prognose der Patienten nachhaltig
OS
(%)
1995-20101987–19961976–19861960–1975
years
100
80
60
40
20
0
0 5 10 15 20 25 30

Wah
lfach
Mai
201
6
Novel agents in lymphoma

Wah
lfach
Mai
201
6
New drugs for lymphoma§ Monoclonal antibodies
§ Cold antibodies§ CD20’s§ Elotzumab, Daratumomab
§ Toxin bound antibodies § Radioimmunotherapy§ Immune engagers§ Checkpoint regulators§ CAR’s
§ Cytostatic drugs§ Pixantrone
§ HDAC-inhibitors
§ Vaccines
§ B-cell receptor pathway inhibitors§ SYK§ BTK§ PI3K§ AKT§ PKCߧ mTOR§ Others: MALT1, JAK-STAT
§ Other TKI’s § ALK§ Alisertib
§ Inducers of Apoptosis§ ABT199
§ Immunmodulators§ Lenalidomide, Pomalidomide
§ Proteasome Inhibitors§ Bortezomib

Wah
lfach
Mai
201
6
B-cell-receptor pathway inhibitors
Wiestner, A. J Clin Oncol. 2013;31(1):128-130.c

Wah
lfach
Mai
201
6
Idelalisib – Mode of action

Wah
lfach
Mai
201
6
Lenalidomide – mode of action
Wah
lfach
Mai
201
6
Cancer Immunotherapy
§ bispecific antibodies
§ CAR-T
§ checkpoint modifier
Wah
lfach
Mai
201
6
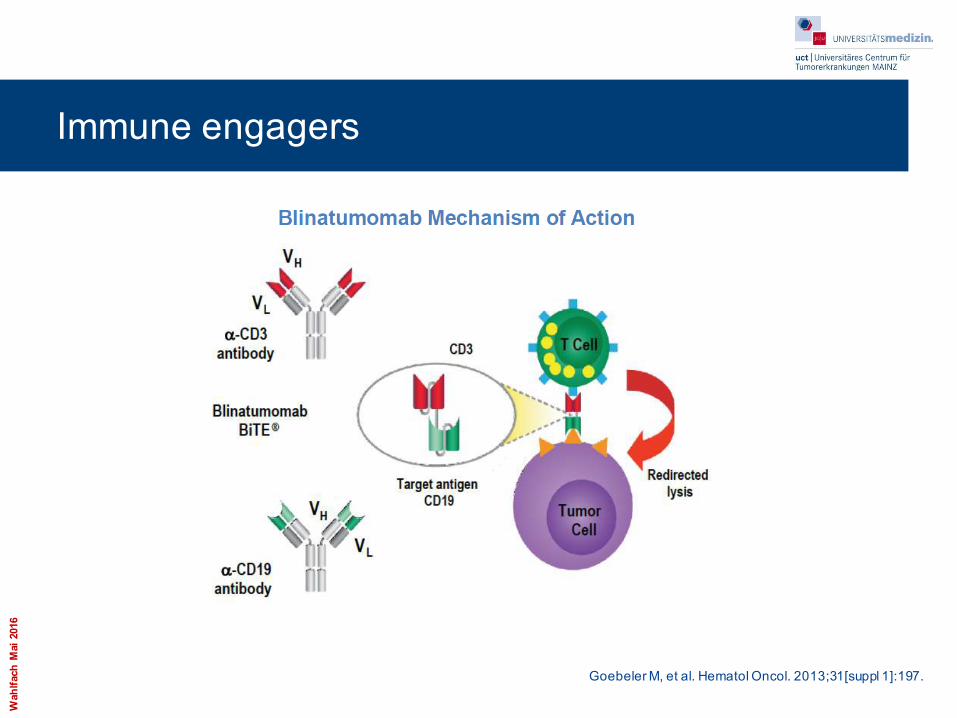
Immune engagers
Goebeler M, et al. Hematol Oncol. 2013;31[suppl 1]:197.

Wah
lfach
Mai
201
6
CAR-T
Maus et al, Blood, 2014

Wah
lfach
Mai
201
6
T cell targets for immunoregulatory antibody therapy
Mellmann I et al. Nature 2011;480(22):480-9

Wah
lfach
Mai
201
6
BCL-2-inhibitors












![Gurū Nānak Gurmukhi & Transliteration für deutsche ... srw guxw ky gwh ] suixAY syK pIr pwiqswh ] suixAY ADy pwvih rwhu ] suixAY hwQ hovY Asgwhu ] nwnk Bgqw sdw ivgwsu ] suixAY](https://static.fdokument.com/doc/165x107/5af994667f8b9a19548cd241/guru-nanak-gurmukhi-transliteration-fr-deutsche-srw-guxw-ky-gwh-suixay-syk.jpg)





