· 4/7/2020 · Board of Th e Egyptian Journal of Bronchology (EJB) Editor-in-Chief Tarek Safwat...
144
Board of e Egyptian Journal of Bronchology (EJB) Editor-in-Chief Tarek Safwat (Ain Shams) Deputy Editors Associate Editors Adel Kattab (Ain Shams Univ.) Adel Saeed (Ain Shams Univ.) Ashraf Hatem (Cairo Univ.) Essam Gouda (Alex. Univ.) Ashraf Madkour (Ain Shams Univ.) EJB BOARD Abd El Hakim Mahmoud (Cairo Univ.) Abd El Moneim Rabie (Alex. Univ.) Abd El Rehim Yousef (Zakazik Univ.) Adel Salah (Zakazik Univ.) Ahmed Abdel Rahman (Monoufeya Univ.) Ahmed Al Halfawy (Cairo Univ.) Ahmed El Gazzar (Benha Univ.) Ahmed El Noury (Ain Shams Univ.) Amgad Abdel Raouf (Tanta Univ.) Amr Badr El Din (Banha Univ.) Ehab Atta (Alex. Univ.) Emad Koraa (Ain Shams Univ.) Gamal El Khouly (Tanta Univ.) Gamal Rabie Agmy (Assiut Univ.) Hafez Abdel Hafeez (Azhar Univ.) Hatem El Mallawany (Alex. Univ.) Hesham Tarraf (Cairo Univ.) Hoda Abou Yousef (Cairo Univ.) Ibrahim Radwan (Azhar Univ.) Khaled Eid (Cairo Univ.) Khaled Wagih (Ain Shams Univ.) Magda Yehia Elseify (Ain Shams Univ.) Magdy Abou Rayan (Alex. Univ.) Magdy Zedan (Mansoura Univ.) Malak Shaheen (Ain Shams Univ.) Mamdouh Mahfouz (Cairo Univ.) Maysa Sharaf El Din (Cairo Univ.) Medhat Abdel Khalek (Cairo Univ.) Medhat Negm (Benha Univ.) Mohamed Abdel Sabour (Ain Shams Univ.) Mohamed Awad Ibrahim (Zagazig Univ.) Mohamed Dosouky Abou Shehata (Mansoura Univ.) Mohamed Khairy (Mansoura Univ.) Mohamed Metwally (Assiut Univ.) Nader Fasseeh (Alex. Univ.) Neveen Abd El Fattah (Ain Shams Univ.) Olfat El Shinawy (Assiut Univ.) Raef Hosni (Cairo Univ.) Ramadan Nafea (Zagazig Univ.) Salah Sorour (Alex. Univ.) Samiha Ashmawy (Ain Shams Univ.) Sayed Oraby (Ain Shams Univ.) Suzan Salama (Assiut Univ.) Tarek Mohsen (Cairo Univ.) Wafaa El Sheimy (Tanta Univ.) Walid El Sorougy (Cairo Univ.) Yasser Mostafa (Ain Shams Univ.) ADVISORY BOARD INTERNATIONAL FACULTY BOARD Mokhtar Madkour (Ain Shams Univ.) Mohamed Awad Tag El Din (Ain Shams Univ.) Ahmed Boseila (Germany) Alaa El Gendy (USA) Atul Mehta (USA) Heinrich D. Becker (Germany) Henri G. Colt (USA) James R. Jett (USA) Majdy M. Idrees (KSA) Petr Pohunek (Czech Republic) Richard W. Light (USA) Roland M. du Bois (UK) http://www.ejbronchology.eg.net/ Editorial Coordinator Amr Shoukri (Ain Shams Univ.)
Transcript of · 4/7/2020 · Board of Th e Egyptian Journal of Bronchology (EJB) Editor-in-Chief Tarek Safwat...
-
Board of Th e Egyptian Journal of Bronchology (EJB)
Editor-in-ChiefTarek Safwat (Ain Shams)
Deputy Editors
Associate Editors
Adel Kattab(Ain Shams Univ.)
Adel Saeed(Ain Shams Univ.)
Ashraf Hatem(Cairo Univ.)
Essam Gouda(Alex. Univ.)
Ashraf Madkour (Ain Shams Univ.)
EJB BOARDAbd El Hakim Mahmoud (Cairo Univ.)Abd El Moneim Rabie (Alex. Univ.)Abd El Rehim Yousef (Zakazik Univ.)Adel Salah (Zakazik Univ.)Ahmed Abdel Rahman (Monoufeya Univ.)Ahmed Al Halfawy (Cairo Univ.)Ahmed El Gazzar (Benha Univ.)Ahmed El Noury (Ain Shams Univ.)Amgad Abdel Raouf (Tanta Univ.)Amr Badr El Din (Banha Univ.)Ehab Atta (Alex. Univ.)Emad Koraa (Ain Shams Univ.)Gamal El Khouly (Tanta Univ.)Gamal Rabie Agmy (Assiut Univ.)Hafez Abdel Hafeez (Azhar Univ.)Hatem El Mallawany (Alex. Univ.)Hesham Tarraf (Cairo Univ.)Hoda Abou Yousef (Cairo Univ.)Ibrahim Radwan (Azhar Univ.)Khaled Eid (Cairo Univ.)Khaled Wagih (Ain Shams Univ.)Magda Yehia Elseify (Ain Shams Univ.)Magdy Abou Rayan (Alex. Univ.)Magdy Zedan (Mansoura Univ.)
Malak Shaheen (Ain Shams Univ.)Mamdouh Mahfouz (Cairo Univ.)Maysa Sharaf El Din (Cairo Univ.)Medhat Abdel Khalek (Cairo Univ.)Medhat Negm (Benha Univ.)Mohamed Abdel Sabour (Ain Shams Univ.)Mohamed Awad Ibrahim (Zagazig Univ.)Mohamed Dosouky Abou Shehata (Mansoura Univ.)Mohamed Khairy (Mansoura Univ.)Mohamed Metwally (Assiut Univ.)Nader Fasseeh (Alex. Univ.)Neveen Abd El Fattah (Ain Shams Univ.)Olfat El Shinawy (Assiut Univ.)Raef Hosni (Cairo Univ.)Ramadan Nafea (Zagazig Univ.)Salah Sorour (Alex. Univ.)Samiha Ashmawy (Ain Shams Univ.)Sayed Oraby (Ain Shams Univ.)Suzan Salama (Assiut Univ.)Tarek Mohsen (Cairo Univ.)Wafaa El Sheimy (Tanta Univ.)Walid El Sorougy (Cairo Univ.)Yasser Mostafa (Ain Shams Univ.)
ADVISORY BOARD INTERNATIONAL FACULTY BOARD
Mokhtar Madkour (Ain Shams Univ.)Mohamed Awad Tag El Din (Ain Shams Univ.)
Ahmed Boseila (Germany)Alaa El Gendy (USA)Atul Mehta (USA)Heinrich D. Becker (Germany)Henri G. Colt (USA)James R. Jett (USA)Majdy M. Idrees (KSA)Petr Pohunek (Czech Republic)Richard W. Light (USA)Roland M. du Bois (UK)
http://www.ejbronchology.eg.net/
Editorial CoordinatorAmr Shoukri (Ain Shams Univ.)
-
GUIDELINES FOR AUTHORS
Th e Egyptian Journal of Bronchology (EJB) welcomes submission of papers on clinical, experimental, cultural and historical topics from authors of diverse clinical and scientifi c interests and expertise, provided the paper has relevance to bronchology and related fi elds.
Papers are reviewed for publication assuming that its content have not been submitted simultaneously to another journal, have not been accepted for publication elsewhere and have not already been published.
Any attempt at dual publication will lead to automatic rejection and may prejudice acceptance of future submissions.Papers may be rejected after review in-house on account of lack of originality, a poorly conducted study or absence of a clinical message.
Th ree copies of the Manuscripts and all artwork should be submitted to the ESSB Secretariat with an electronic copy on an IBM-compatible disk in Microsoft Word format. A covering letter addressed to the EJB editor requesting submission and signed by all authors must accompany the Manuscript copies.
Th e EJB style follows the Uniform Requirements for Manuscripts Submitted to Biomedical Journals which can be downloaded free from the following site: www.icmje.org.
EthicsMaterial relating to human investigation and animal experiments must comply with and be approved by local ethics committees. Th e EJB reserves the right not to publish papers on the grounds that appropriate ethical or experimental standards have not been reached. Written consent must be obtained from the patients, legal guardian or executor for publication of any details or photographs that might identify an individual.
Manuscript PreparationManuscripts should not exceed 4000 words and should be typewritten on a good quality printer or typewriter, using a 12 pt font size, on A4 paper, with double spacing and at least 3cm margins. Th e pages of the manuscript should be numbered including the title page at the top right hand corner. Th e manuscript should NOT be written with a column formatting style. Each of the following sections should begin on a new page in the following order: title page; abstract; introduction; patients (materials) and methods, results, discussion, acknowledgment; references; tables; legends for illustrations.
Title PageTh e title page should contain: (1) Title of the Article, (2) Full name of each author, with highest academic degree(s), (3) Department(s) and institution(s) to which the work should be attributed, and (4) Name, address, phone, fax and e-mail address of author responsible for correspondence.
AbstractTh e abstract should be structured outlining the aim, methods, results and conclusions of the paper. Th e abstract should not exceed 200 words.
KeywordsTh ree words using terms from Index Medicus (MeSH catalogue) wherever possible should be chosen by the author.
TextThe outline of the text should be; (1) Introduction, (2) Patients (Materials) and Methods, (3) Results, (4) Discussion.
Tables and graphsPlease modify the table and graphs heading of the guidelines for authors as follows:
Each table should be typed on a separate sheet, must have an identifying number (please use Arabic numerals) and a short descriptive title. Do not use vertical lines in your tables. All tables should be linked with the text and should supplement, not duplicate, the text. For footnotes use the following symbols in the following sequence: *,†,‡,§,||,¶,**,††,‡‡. Graphs should be constructed in black and white with no gridlines. Th ree dimension graphs will not be accepted.
Illustrations (Figures)Figures should be submitted in the form of glossy prints. Each illustration should have a label pasted on the reverse side giving the name(s) of the author, its reference number in the text, and an arrow pointing at its upper border. If photographs of people are used, either the subjects must not be identifi able or their pictures must be accompanied by written permission to use the photograph. Legends for all illustrations should be typed on a separate sheet.
Abbreviations and symbolsTh e full term for which an abbreviation stands should precede its fi rst use in the text unless it is a standard unit of measurement. Avoid abbreviations in the title.
ReferencesTh e Egyptian Journal of Bronchology reference style follows the Uniform Requirements for Manuscripts Submitted to Biomedical Journals which is based largely on an ANSI standard style adapted by the National Library of Medicine (NLM) for its databases www. nlm.nih.gov/bsd/uniform_requirements.html Example for standard journal article:Halpern SD, Ubel PA, Caplan AL. Solid-organ transplantation in HIV-infected patients. N Engl J Med. 2002;347:284-7.For articles with more than six authors: List the fi rst six authors followed by et al.Rose ME, Huerbin MB, Melick J, Marion DW, Palmer AM, Schiding JK, et al. Regulation of interstitial excitatory amino acid concentrations after cortical contusion injury. Brain Res. 2002;935:40-6. Wherever possible should be chosen by the author.
ANNUAL SUBSCRIPTION
Th e Egyptian Journal of Bronchology is will be published thrice a year, January, May and September to start with.
INFORMATION & CORRESPONDENCE
Any information requests or correspondence including paper submission, subscription order, change of address of subscriber and, advertising in the Journal, should be addressed to:ESSB Secretariat
Conference Organizing BureauDr. Shahenda El Hawary14, El Khalil St., Lebanon Sq., Mohandessin,Giza 12411, EgyptTel.: (202) 33023642 33027672 Fax: (202) 33027672E-mail: [email protected]
Information about the Journal is also available at the Egyptian Scientifi c Society of Bronchology website at:http://www.ejbronchology.eg.net/
-
Th e Egyptian Journal of BronchologyThe Offi cial Journal of the Egyptian Scientifi c Society of Bronchology
Vol. (12), No. (2), April-June, 2018
Review Article
137 Spontaneous pneumothorax: time to depart from the ‘chest tube underwater seal’?
Maged Hassan, Hany Shaarawy
Critical Care143 Noninvasive positive pressure ventilation in
acute hypercapnic respiratory failure Khaled Hussein
Airway diseases
Original articles149 Effectiveness of pulmonary rehabilitation on
pulmonary function parameters and dyspnea in patients with stable chronic obstructive pulmonary disease
Atef F. Al Karn, Wafaa A. Hassan, Abdel A. Abo El Fadl, Manal A. Mahmoud
154 Bronchial asthma: clinical phenotypes and endotypes and their relation with glucocorticoids circadian rhythm and parasympathetic activity
Magdy M. Zedan, Magdy Abd El Moneim El-Ziny, Abd Elazeez Atallah Shabaan, Youssef M. Mosaad, Wafaa Nabil Laimon
160 Correlation between serum periostin biomarker, spirometric airflow limitation, and airway dimensions by multidetector computed tomography in bronchial asthma
Eman R. Al-Adawy, Ashraf A. Gomaa, Ahmed M. Mohamed
173 Relationship between platelet count, platelet indices, and infl ammatory markers in stable and acute exacerbation of bronchiectasis patients
Burcu A. Yigitbas, Sibel Yurt, Berat Uslu, Celal Satici, Pelin Uysal, Ayse F. Kosar
180 Clinical phenotype as a predictor of outcome in mechanically ventilated chronic obstructive pulmonary disease patients
Alaa Eldin Metwally Mohamed Elgazzar
187 Assessment of the prevalence of depression in chronic obstructive pulmonary disease patients
Sherif A. Eissa, Tarek S. Essawy, Mohammad A. Almahdy, Shaymaa A. Mohammed, Mohammed M. El-Hamady
Bronchosocopy & Interventional Pulmonology
Original article193 Impact of a designed educational program on
elderly patients undergoing fl exible bronchoscopy Ali A. Hasan, Anwar M. Ali, Soad A. Sharkawy,
Hanan A. Abozeid, Martha M. Labieb
Critical Care
Original article200 Study of plasma copeptin level as a prognostic
marker in respiratory failure patients admitted in the ICU at Benha University Hospital
Mahmoud M. Al Salahy, Mohammad A. Elmahdy, Tahany M. Gouda, Khaled M. Belal, Shiemaa M. Elnahas
208 Validity of three scoring systems in assessing the severity and outcome in Al-Abbassia Chest Hospital Respiratory Intensive Care Unit patients
Taher Abd El-Hamid El-Naggar, Riham H. Raafat, Safaa A. Mohamed
218 Assessment of ventilator-induced diaphragmatic dysfunction in patients with chronic obstructive pulmonary disease using transthoracic ultrasonography
Shereen Farghaly, Ali A. Hasan, Hoda A. Makhlouf
Interstitial lung diseases
Original articles226 Prognostic factors and outcome of mechanically
ventilated interstitial lung disease patients Ashraf Zin El-Abdeen, Lamiaa H. Shaaban, Shereen
Farghaly, Yara Y. Omar
-
Miscellaneous
Original articles233 Pulmonary complications within the fi rst year
after bone marrow transplantation Amal Abd El-Azem Sadon, Rehab S. El-Hagrasy,
Mohamed A. Saraya
240 Neighbours affect each other; pulmonary affection after cardiac surgery
Reham M. Elkolaly, Mohab Sabry, Mohamed Abo-Elnasr, Amr Arafat
Pleural Disease
Original articles247 Prevalence, causes, and clinical implications of
pleural effusion in pulmonary ICU and correlation with patient outcomes
Mohamed Farrag, Ahmed El Masry, Amr M. Shoukri, Mona ElSayed
253 Study of pleurodesis using ethanolamine oleate through ultrasound-guided pigtail
Adel M. Saeed, Tamer M. Ali, Ashraf A. Gomaa, Mohamed N. Kamel
260 Role of transthoracic ultrasound in differentiation of the causes of pleural thickening
Khaled M. Kamel, Yasmine H. El-Hinnawy
Pulmonary Infections
Original articles266 Workplace pulmonary tuberculosis case detection
in Mansoura City and neighborhood villages Samah S. El Hadidy, Sohair F. El-Bestar, Emily A. Kamel,
Nesrein M. Shalabi
Case report
273 Unilateral lung hyperlucency in an adult: an unusual cause
Parul Kodan, Abanti Das, Surabhi Vyas, Animesh Ray, Surinder K. Sharma
Letter to Editor
Airway diseases276 Pulmonary function tests in patients with chronic
rhinosinusitis and the effect of surgery Mahmood D. Al-Mendalawi
-
Review article 137
Spontaneous pneumothorax: time to depart from the ‘chest tubeunderwater seal’?Maged Hassana,b, Hany Shaarawyb,
Initial management of spontaneous pneumothorax hastraditionally been inserting a chest tube and attaching it toan underwater seal and hospitalizing the patient. New optionshave emerged that allow management to be on an outpatientbasis without the need for hospitalization. These options areneedle aspiration (similar to aspiration of effusion) orattaching the chest tube to a one-way valve. So, ischaining a patient with spontaneous pneumothorax to theirhospital bed because of the heavy jar attached to the chesttube the most prudent way of management? This reviewattempts to answer this question.Egypt J Bronchol 2018 12:137–142© 2018 Egyptian Journal of Bronchology
© 2018 Egyptian Journal of Bronchology | Published by Wolters Kluwer - Medknow
Egyptian Journal of Bronchology 2018 12:137–142
Keywords: chest tube, Heimlich valve, needle aspiration, pneumothorax,practice guidelines
aCentre for Respiratory Medicine, Oxford University Hospitals, Oxford, UK,bDepartment of Chest Diseases, Faculty of Medicine, Alexandria University,
Alexandria, Egypt
Correspondence to Maged Hassan, MSc, Oxford Centre for Respiratory
Medicine, Churchill Hospital, Old Road, Headington OX3 7LE, Oxford, UK;
Tel: +44 796 035 7965; fax: +44(0) 1865 857109;
e-mail: [email protected]
Received 1 July 2017 Accepted 13 August 2017
This is an open access journal, and articles are distributed under the terms
of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0
License, which allows others to remix, tweak, and build upon the work
non-commercially, as long as appropriate credit is given and the new
creations are licensed under the identical terms.
IntroductionPneumothorax is the abnormal collection of airin the pleural space. The earliest report of thecondition dates back to an account made by anOttoman physician in the 15th century AD of a caseof traumatic pneumothorax [1]. Pneumothorax istermed ‘spontaneous’ when it is not precipitated byany type of injury. Pneumothorax can occur as acomplication of invasive medical procedures(iatrogenic) or a blunt or penetrating trauma to chestwall (traumatic) [2]. Spontaneous pneumothorax (SP)is divided into primary spontaneous pneumothorax(PSP) or secondary spontaneous pneumothorax(SSP), depending on the presence or lack ofstructural lung diseases and/or significant smokinghistory [3].
The initial management of SP is centered onevacuation of pleural air; the necessity and urgencyof which depends on the size of the pneumothorax, thepatient’s degree of symptoms, the presence of structurallung disease, and the general condition of the patient[4]. A small PSP in a stable patient without-dyspneacan usually be safely observed [3,5]. It is estimated thata pneumothorax will resolve at a rate of 1.5–2% of itsvolume per day as long as air leak has ceased [6]. SPhas the tendency to recur with a 1-year recurrencerate of 20–50% in PSP [7]. For this reason, recurrenceprevention is a crucial component in the managementof PSP and SSP at the first recurrence. Recurrenceprevention is occasionally indicated during thefirst incidence of pneumothorax if a recurringpneumothorax is feared to have serious consequencesto a patient’s well-being [3,4]. This review will focus onthe initial management of SP. Recurrence prevention isextensively covered elsewhere.
The traditional means of drainage of pleural air is byinserting a rubber/silicone drain in an intercostal spaceand connecting it to an underwater seal. This isgenerally a safe procedure, but it makes the hospitaladmission inevitable, imposing significant costs interms of hospital stay. In addition, connecting achest tube to the underwater seal obliges thepatient to be relatively immobile which is a riskfactor for venous thromboembolism [8]. This isespecially true for older patients who have otherrisk factors. Emergency department management ofpneumothorax in addition to outpatient follow-up hasbeen contemplated and tested by many as a means toaddress this problem.
The paradigm shiftThe concept of catheter aspiration for simplepneumothorax (CASP) was first suggested in 1962by Klassen et al. [9]. It emerged as a method ofhandling pneumothorax in a similar fashion to howchest physicians deal with pleural effusion. Thisnascent practice was criticized at the time owing tofear of imminent risk of lung laceration by theaspirating needle [10]. Since then, many case serieshave contested the claim that chest tube underwaterseal is the only safe means for pneumothorax drainageand refuted the perceived risk of iatrogenic lungtrauma [8,11,12]. These reports have examinedCASP in the setting of spontaneous and traumaticpneumothoraces.
DOI: 10.4103/ejb.ejb_58_17
mailto:[email protected]
-
138 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
Around the same period, Bernstein et al. [13] suggestedthe possibility of outpatient management ofpneumothorax by replacing the underwater seal witha one-way valve (called Heimlich valve) attached to thechest tube. This modification allowed patients to bedischarge within hours of putting in the chest tube andmaintained their mobility owing to the lack ofthe heavy jar used to create the underwater seal.This method of management has been termed‘ambulatory management’ of pneumothorax [4,14].
Figure 1
Specialized catheter for pleural aspiration (right) and an 18G cannulaattached to three-way stopcock.
Needle aspirationThe evidenceEarly studies suggested the safety of CASP, butevidence of its efficacy was more recently provedby successive randomized controlled trials (RCTs)[4]. The largest RCT on needle aspiration for PSPwas conducted by Ayed et al. [15] who randomized137 patients to either needle aspiration or chest tubedrainage. The immediate success rate was 62% forneedle aspiration compared with 68% success forchest tube drainage (difference not statisticallysignificant) [15]. Other RCTs reported successrates between 60 and 70% for simple aspiration[16,17]. To put matters in perspective, this meansthat avoiding admission is possible in seven of every10 patients presenting with a symptomatic PSP. A2007 Cochrane Review concluded that there was nosignificant difference in the success rates for needleaspiration versus chest tube drainage for patientspresenting with PSP [18]. The review also pointedout that needle aspiration was found to be associatedwith fewer hospitalizations. This compellingevidence led the British Thoracic Society (BTS)2010 guidelines to adopt needle aspiration asplausible management option for SP as long asenough expertise in the procedure is available (seebelow) [3].
More recently, RCTs have expanded the scope ofexperimenting CASP in patients presenting withtraumatic pneumothorax [17] or SSP [19]. Thelleet al. [19] randomized 127 patients presenting withSP (including 48 patients with SSP) to either needleaspiration or chest drainage and proved for the firsttime that needle aspiration was safe for patient withSSP, who, additionally, had better immediate successrates for this procedure when compared with chestdrainage (69 vs. 32%) [19]. They also foundsignificantly shorter durations of hospitalization forthe needle aspiration group; a finding corroboratedby the previous series and RCTs. There was nosignificant difference in recurrence at 1-year usingeither modality [20]. Another benefit cited in most
of these studies (and a point not difficult to understand)is that needle aspiration was associated withsignificantly less discomfort/pain [4]. Needleaspiration is also associated with less anxiety, andlimited scar formation unlike chest tubes [21].Available evidence has also shown that, withincreased use of aspiration, PSP can be treated morefrequently as an emergency department-based diseaseinstead of an in-hospital disease, with positive effectson the costs of medical care [21].
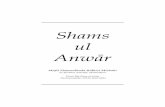
The techniqueAfter confirmation of the presence of pneumothorax, adiagnosis was usually made with the aid of an erectchest radiography; the decision to drain is usually takendepending on how dyspneic the patient is. Theprocedure side is marked and then the skin at thefront of the chest is properly cleansed. The optimalsite for aspiration is the second intercostal space at themidclavicular line. Local anesthesia usually suffices aslong as the skin and the parietal pleura are generouslyanesthetized. Final confirmation of the presence ofpneumothorax is achieved when the needle injectingthe local anesthetic is able to aspirate air. In manyinstitutes, a specific kit is available for pleural aspirationand is composed of a catheter over needle attached to asyringe with a stopcock (Fig. 1). An 18 G intravenouscannula attached to a three-way stopcock is more thansufficient for the job if the special kit is not available(Fig. 1). Regardless of the instrument used, thetechnique is the same. After proper anesthesia, the
-
Outpatient management of pneumothorax Hassan and Shaarawy 139
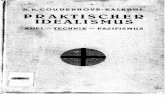
catheter is introduced with needle inside it. Once air isaspirated, the catheter/cannula is advanced over theneedle till its end and then the needle is withdrawn toavoid injury to the underlying lung. Manual aspirationfollows by the means of a syringe draining to a bag.Meticulous calculation of the volume of aspirated air isnecessary. The process is continued until no air isaspirated or the patient feels chest pain. A chestradiography should be done very shortly afterward.If the residual pneumothorax in the new radiographyis small and patients experience improvementin dyspnea, they can be discharged. If air iscontinuously aspirated beyond 2.5 l (a sign ofongoing air leak), the procedure should beconsidered unsuccessful and a chest tube should beinserted. Also if the follow-up radiography does notshow resolution of pneumothorax, chest tube insertionrather than a second trial of aspiration is warranted.Figure 2 shows a case of PSP successfully managed byneedle aspiration at the Chest Diseases Department inAlexandria University. Overall, 1100ml of air wasaspirated in this case, and immediate postprocedure
Figure 2
(a) Chest radiography at presentation showing left pneumothorax andshowing only a small apical cap of pneumothorax. (c) Chest radiograph
radiography shows near total resolution of thepneumothorax (Fig. 2b).
Ambulatory managementThe evidenceThe attachment of a one-way valve to a chest tube inthe emergency department as well as the subsequentdischarge from hospital has been proved as a feasibleand safe option for patients with different types ofpneumothorax since the 1970s [14]. In a pilot study in2006, Marquette et al. [22] inserted an 8-F pigtailcatheter attached to a Heimlich valve in 41 patientspresenting with the first episode of PSP. Patients whodid not show good re-expansion after 2 h had theirtubes attached to suction. If expansion occurred (withor without suction), patients were discharged and had afollow-up appointment every other day. Patients whocontinued to have air leak at 4 days were referred forthoracoscopy [22]. The 1-week success rate wasreported in 85% of study patients [22]. The samegroup later repeated the study on 60 patients withPSP and reported a very similar 1-week success rate
collapsed lung (arrows). (b) Immediate postaspiration radiographyy done 4 weeks after procedure confirms nonrecurrence.
-
140 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
of 83% [23]. Further studies using different variationsof the Heimlich valve that recruited patients with PSPas well as SSP and iatrogenic pneumothorax reportedsuccess rates of 73–78% [24,25]. Ho et al. [26]randomized 48 patients with PSP to either needleaspiration or chest drain with one-way valveand found very similar success rates. A systematicreview of studies on ambulatory management ofpneumothorax using a Heimlich valve type found apooled success rate of outpatient management ofpatients with different types of pneumothorax to bebetween 75 and 80% [14]. None of the studies reviewedreported any fatality or serious complication like lung/visceral pleural laceration [14]. The main criticism forthe reported studies in the review was the lack of RCTsthat directly compare this modality to the standardtechnique of chest tube with underwater seal [14]. Toaddress this research need, there are currently twolarge multicentre UK RCTs comparing ambulatorymanagement of pneumothorax to traditional chesttube in patients with PSP (ISRCTN 79151659) andSSP (ISRCTN 79956557).
Figure 4
The techniqueAll studies reporting the use of ambulatorymanagement use either small-bore chest drains(8–12 F) inserted with Seldinger technique (Fig. 3)or specialized CASP kits (Fig. 1). Larger chest drains(>16 F) are rarely needed, as there is evidence of theequivalent efficacy with smaller sized drains, with theadvantage of the latter of causing less pain and smallerscars [27]. The insertion site is usually either the secondintercostal space at the midclavicular line or at thetriangle of safety (midaxillary line above the sixth rib).The earlier site is preferred by some because thecatheter and the attached device would not interfere
Figure 3
Special kit for 12-F chest drain for insertion by Seldinger’s technique.
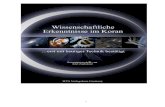
with arm movements during walking or if the patientwants to sleep on that side. After confirmation ofsuccessful insertion, the catheter/drain is attached toa one-way valve of the many types commerciallyavailable (Fig. 4). The different types of valves comewith fitting tubes to allow attachment to eitherconventional chest tubes or smaller catheters. Apostprocedure radiography is done to confirm re-expansion of the lung. Most centers do not prefer toremove the catheter at this stage but rather to dischargethe patient and follow them up in 24–48 h and theneither daily or every other day until a week has elapsed.The tube is removed at any point during the follow-upif a chest radiography is showing near-completeexpansion and no air is coming from the valve.Persistent air leak or failure of re-expansion shouldprompt surgical referral.
Guidelines and everyday practiceThe most widely cited management guidelines forpneumothorax are the American College of ChestPhysicians statement issued in 2001 [5] and theBTS guidelines published in 2010 [3]. The uptakeof these relatively new ‘outpatient’ managementstrategies varies between the two societies mainlybecause of the availability of good quality evidencewhen each document was prepared.
Although the American College of Chest Physiciansstatement does not support needle aspiration for
(a) Pneumostat atrium valve; (b) classical Heimlich valve.
-
Outpatient management of pneumothorax Hassan and Shaarawy 141
managing SP, the BTS guidelines advocate it for anypatient with symptomatic large PSP (>2 cm) and forpatients with small symptomatic SSP (1–2 cm indepth) [3]. The BTS puts emphasis on theimportance of performing the technique bypractitioners who are familiar with it and haveexperience with dealing with pleural diseases.Patients who are too unwell or present with tensionor bilateral pneumothoraces should proceed directly tochest tube and hospital admission.
Despite the fact that this scheme is considered thestandard of care in many parts of the world, deviationfrom this practice is widely reported [28]. In Egypt, thechest tube underwater seal is still the standard of carefor all patients with SP who need drainage [29].
Given the compelling evidence of the safety ofoutpatient management of stable patient with SP(both PSP and SSP), the question arises as to whythese techniques do not replace the insertion of theordinary chest drains and the underwater seal as theinitial management in patients with SP? It is curious tonote that some respiratory centers have established anambulatory service for pneumothorax, where needleaspiration is first tried (as per BTS guidelines) and ifunsuccessful, a chest tube is inserted and attachedto a one-way valve thus eliminating the need ofhospitalization in a significant portion of theirpatients [30]. It is worth mentioning that a smallbut significant subset of patients with SP will needhospitalization and a standard chest tube because ofindications cited above. In addition, patients who aretoo frail or who cannot return to hospital in due courseif problems arise should be hospitalized and have thetraditional chest drain. However, for the remainingmajority, is it safe to say that it is time to depart fromthe chest tube underwater seal as the title of the reviewsuggests? Widespread application of these techniquescan save several hundreds of days of hospitalizationsacross the country and redirect resources to othercrucial respiratory conditions. The current statussuggests that this is unlikely to happen in the nearfuture, as it is not easy to change the conviction ofclinicians about procedures that are regarded as goldstandard. It is hoped from this brief review to plantsome seeds of curiosity in the minds of respiratoryphysicians to explore more about these options andhopefully apply them in the future.
ConclusionIt seems appropriate to conclude that, in themanagement of SP, ‘less is more’. Needle aspiration
is successful in many patients, which made it arecommended practice. Ambulatory managementwith one-way valves is emerging as a viable option,and results of ongoing RCTs will potentially affect thesynthesis of future guidelines. Even in the situationwhere a chest tube with underwater seal is required,very small drains (8–12 F) are as effective as the largerones.
AcknowledgementsMaged Hassan is a recipient of European RespiratorySociety long-term research fellowship − ERS LTRF7333.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References1 Kaya SO, Karatepe M, Tok T, Onem G, Dursunoglu N, Goksin I. Were
pneumothorax and its management known in 15th-century anatolia? TexHeart Inst J 2009; 36:152–153.
2 Bintcliffe OJ, Hallifax RJ, Edey A, Feller-Kopman D, Lee YCG, MarquetteCH, et al. Spontaneous pneumothorax: time to rethink management?Lancet Respir Med 2015; 3:578–588.
3 MacDuff A, Arnold A, Harvey J, on behalf of the BTS Pleural DiseaseGuideline Group. Management of spontaneous pneumothorax: BritishThoracic Society pleural disease guideline 2010. Thorax 2010; 65:ii18–ii31.
4 Tschopp J-M, Bintcliffe O, Astoul P, Canalis E, Driesen P, Janssen J, et al.ERS task force statement: diagnosis and treatment of primaryspontaneous pneumothorax. Eur Respir J 2015; 46:321–335.
5 Baumann MH, Strange C, Heffner JE, Light R, Kirby TJ, Klein J, et al.Management of spontaneous pneumothorax: an American Collegeof Chest Physicians Delphi consensus statement. Chest 2001;119:590–602.
6 Kelly A-M, Loy J, Tsang AYL, Graham CA. Estimating the rate of re-expansion of spontaneous pneumothorax by a formula derived fromcomputed tomography volumetry studies. Emerg Med J 2006; 23:780–782.
7 Hallifax RJ, Yousuf A, Jones HE, Corcoran JP, Psallidas I, Rahman NM.Effectiveness of chemical pleurodesis in spontaneous pneumothoraxrecurrence prevention: a systematic review. Thorax 2016; Online First:01 November 2016. doi: 10.1136/thoraxjnl-2015-207967.
8 Hamilton AA, Archer GJ. Treatment of pneumothorax by simple aspiration.Thorax 1983; 38:934–936.
9 Klassen KP, Meckstroth CV. Treatment of spontaneous pneumothorax:prompt expansion with controlled thoracotomy tube suction. JAMA 1962;182:1–5.
10 Ruckley CV, McCormack RJ. The management of spontaneouspneumothorax. Thorax 1966; 21:139–144.
11 Obeid FN, Shapiro MJ, Richardson HH, Horst HM, Bivins BA. Catheteraspiration for simple pneumothorax (CASP) in the outpatient managementof simple traumatic pneumothorax. J Trauma 1985; 25:882–886.
12 Vallee P, Sullivan M, Richardson H, Bivins B, Tomlanovich M. Sequentialtreatment of a simple pneumothorax. Ann Emerg Med. 1988; 17:936–942.
13 Bernstein A, Waqaruddin M, Shah M. Management of spontaneouspneumothorax using a Heimlich flutter valve. Thorax 1973; 28:386–389.
14 Brims FJH, Maskell NA. Ambulatory treatment in the management ofpneumothorax: a systematic review of the literature. Thorax 2013;68:664–669.
-
142 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
15 AyedAK, ChandrasekaranC, SukumarM. Aspiration versus tube drainagein primary spontaneous pneumothorax: a randomised study. Eur Respir J.2006; 27:477–482.
16 Noppen M, Alexander P, Driesen P, Slabbynck H, Verstraeten A. Manualaspiration versus chest tube drainage in first episodes of primaryspontaneous pneumothorax: a multicenter, prospective, randomizedpilot study. Am J Respir Crit Care Med 2002; 165:1240–1244.
17 Parlak M, Uil SM, van den Berg JWK. A prospective, randomised trial ofpneumothorax therapy: manual aspiration versus conventional chest tubedrainage. Respir Med 2012; 106:1600–1605.
18 Wakai A, O’Sullivan RG, McCabe G. Simple aspiration versus intercostaltube drainage for primary spontaneous pneumothorax in adults.CochraneDatabase Syst Rev 2007; 24:CD004479.
19 Thelle A, Gjerdevik M, SueChu M, Hagen OM, Bakke P. Randomisedcomparison of needle aspiration and chest tube drainage in spontaneouspneumothorax. Eur Respir J 2017; 49:1601296.
20 Devanand A, Koh MS, Ong TH, Low SY, Phua GC, Tan KL, et al. Simpleaspiration versus chest-tube insertion in the management of primaryspontaneous pneumothorax: a systematic review. Respir Med 2004;98:579–590.
21 Janssen J, Cardillo G. Primary spontaneous pneumothorax: towardsoutpatient treatment and abandoning chest tube drainage. Respiration2011; 82:201–203.
22 Marquette C-H., Marx A, Leroy S, Vaniet F, Ramon P, Caussade S, et al.Simplified stepwise management of primary spontaneous pneumothorax:a pilot study. Eur Respir J. 2006; 27:470–476.
23 Massongo M, Leroy S, Scherpereel A, Vaniet F, Dhalluin X, ChahineB, et al. Outpatient management of primary spontaneous pneumo-thorax: a prospective study. Eur Respir J 2014; 43:582–590.
24 Voisin F, Sohier L, Rochas Y, Kerjouan M, Ricordel C, Belleguic C, et al.Ambulatory management of large spontaneous pneumothorax? Withpigtail catheters. Ann Emerg Med 2014; 64:222–228.
25 Woo WG, Joo S, Lee GD, Haam SJ, Lee S. Outpatient treatment forpneumothorax using a portable small-bore chest tube: a clinical report.Korean J Thorac Cardiovasc Surg 2016; 49:185–189.
26 HoKK,OngMEH, KohMS,WongE, Raghuram J. A randomized controlledtrial comparing minichest tube and needle aspiration in outpatientmanagement of primary spontaneous pneumothorax. Am J Emerg Med2011; 29:1152–1157.
27 Baumann MH, Patel PB, Roney CW, Petrini MF. Comparison of function ofcommercially available pleural drainage units and catheters. Chest 2003;123:1878–1886.
28 Kelly A-M, Clooney M, Spontaneous Pneumothorax Australia StudyGroup. Deviation from published guidelines in the management ofprimary spontaneous pneumothorax in Australia. Intern Med J 2008;38:64–67.
29 Korraa E, Madkour A, Shoukri A, Ahmed S. Outcome of patients withspontaneous pneumothorax admitted in Abbasia Chest Hospital. Egypt JBronchol 2016; 10:355.
30 Thomas K, Naeem M, Reddy R. P173 ambulatory management ofspontaneous pneumothorax. Thorax 2014; 69:A150–A151.
-
Review article 143
Noninvasive positive pressure ventilation in acute hypercapnicrespiratory failureKhaled Hussein
NPPV is well established in the management of acute onchronic hypercapnic respiratory failure secondary to acuteexacerbation of COPD (AECOPD), obesity hypoventilationsyndrome, and restrictive thoracic disorders. Because of itsdesign, success depends largely on patient cooperation andacceptance. The most commonly used interfaces in acutehypercapnic respiratory failure are oronasal masks. Duringnoninvasive ventilation patients respiratory system ismaintained throughout the whole respiratory cycle at aconstant pressure higher than the atmospheric pressure,usually termed the positive end-expiratory pressure(PEEP). Pressure support ventilation (PSV), is the mostfamous mode of partial ventilatory support that duringspontaneous inspiratory efforts imposes a set level ofpositive pressure in a patient with intact respiratory drive.Bilevel positive airway pressure (BiPAP) include PSV duringinspiration and EPAP during expiration. The highest pressure
© 2018 Egyptian Journal of Bronchology | Published by Wolters Kluwer - Medknow
reached during inspiration is called inspiratory positive airwaypressure (IPAP) which equal PSV+EPAP.Egypt J Bronchol 2018 12:143–148© 2018 Egyptian Journal of Bronchology
Egyptian Journal of Bronchology 2018 12:143–148
Keywords: chronic obstructive pulmonary disease, noninvasive positivepressure ventilation, obesity hypoventilation syndrome
Department of Pulmonology and Critical Care, Assiut University, Assiut,
Egypt
Correspondence to Khaled Hussein, MD, Department of Pulmonology and
Critical care, Assiut University, Assiut, 71111, Egypt;
Tel: +20 106 121 2172;
e-mail: [email protected]
Received 23 July 2017 Accepted 29 July 2017
Acute hypercapnic respiratory failure ofchronic obstructive pulmonary diseaseNoninvasive positive pressure ventilation (NPPV) is awell-established technique used in the management ofacute hypercapnic respiratory failure secondary to acuteexacerbation of chronic obstructive pulmonary disease(AECOPD) [1], as shown in Fig. 1.
Physiological rationale of noninvasive positivepressure ventilation in acute exacerbation ofchronic obstructive pulmonary diseaseAsshown inFig. 2, theupwardyellowarrowmentions theeffect of continuous positive airway pressure or PEEP tocounterbalance intrinsic positive end-expiratory pressure(PEEP) (decrease work of breathing with better trigger)[1]. The downward yellow arrow mentions the effect ofpressure support to unload respiratory muscles andimproving ventilation (decrease PaCO2).
Indications of noninvasive positive pressureventilationNPPV should be started when pH is below 7.35 afterstandard medical treatment including oxygen therapy(Fig. 3) [2]. pH plays an important role for selection oflocation of admission and for decision of intubation asin the following:
(1)
This is an open access journal, and articles are distributed under the terms
pH higher than 7.35: prophylactic use of NPPVand no benefit versus conventional therapy.
of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0
License, which allows others to remix, tweak, and build upon the work
(2)
non-commercially, as long as appropriate credit is given and the new
creations are licensed under the identical terms.
pH from 7.25 to 7.35: mandatory use of NPPV inemergency department or respiratory ward but notICU with excellent prognosis.
(3)
pH below 7.25: mandatory use of NPPV andmandatory admission to ICUwith good prognosis.(4)
pH below 7.20: expect the need for intubation andchance for successful NPPV is decreased.(5)
pH below 7.10: NPPV is contraindicated andintubation is mandatory.Modes of noninvasive positive pressureventilation in acute exacerbation of chronicobstructive pulmonary diseaseThere are main and accessory modes of NPPV:
(1)
Themain mode acts during inspiration to augmentspontaneous breathing such as pressure support(PSV), proportional assist, or volume assuredpressure support (VAPS).(2)
Accessory mode uses either expiratory positiveairway pressure (EPAP) or pressure controlventilation (timed mode or T).Pressure support ventilationThis mode is a part of S or S/T modes, where S is thespontaneous mode and is called bilevel positive airwaypressure and includes PSV during inspiration and EPAPduring expiration (Fig. 4). The highest pressure reachedduring inspiration is called inspiratory positive airwaypressure (IPAP), which equal PSV+EPAP [3].
DOI: 10.4103/ejb.ejb_65_17
mailto:[email protected]
-
Figure 1
Acute exacerbation of COPD with respiratory failure is the commonest indication for NPPV.
144 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
On the contrary, S/T (Fig. 5) is S mode plus Tmode. T mode is delivered only if patient failed toinitiate trigger within a time governed by backuprate.
Benefits of expiratory positive airway pressure
(1)
Counterbalance auto PEEP.
(2)
Maintain patency of upper airways at the end ofexpiration.
(3)
Helps CO2 wash from exhalation port anddecrease its rebreathing.
How to set S/T mode
(1)
EPAP: 5–7 cmH2O.
(2)
Set pressure support at least 8 cmH2O andincreased in increments of 2 cmH2O every30min targeting tidal volume of 8ml/kg andSPO2 above 90%.
(3)
IPAP is preferred not exceeding 20 cmH2O toprevent gastric insufflation.Proportional assist ventilationThe second common mode used in acute exacerbationof COPD (Fig. 6).
(1)
It is proportional to patient effort by deliveringvolume assist and flow assist according to elastanceand resistance [4]. Thus, pressure, volume, and floware variable from breath to breath as shown in belowfigure.
(2)
It is indicated if there is good triggering, otherwiseS/T is indicated.Volume assured pressure support
(1)
A recent dual mode with target tidal volume(average VAPS) or target alveolar ventilation(intelligent VAPS).(2)
It is thought to augment alveolar ventilation withenhanced CO2 wash and improved acidosis.Monitoring during noninvasive positivepressure ventilation
(1)
Continuous:(a) SpO2.(b) ECG.(c) Respiratory rate.
Intermittent:
(2)
(a) Arterial blood gases.(b) Leaks.(c) Patient–ventilator synchrony.
Acute hypercapnic respiratory failure ofobesity hypoventilation syndromeIn the Western world, the prevalence of obesepatients in ICUs is increasing. Additionally, morbid
-
Figure 2
Flow chart for physiological rationale of application of NPPV in acute hypercapnic respiratory failure of COPD.
Figure 3
Flow chart for the application of NPPV in acute exacerbation ofCOPD, according to the severity of respiratory acidosis.
Figure 4
Pressure, flow, and volume tracers during pressure support.
NPPV in acute hypercapnic RF Hussein 145
obesity has dramatic consequences on pulmonaryfunction. Therefore, respiratory physicians andintensivistsare more likely to manage a largernumber of acute hypercapnic respiratory failure(AHRF) episodes in patients with a BMI of atleast 30 [5]. Cor pulmonale is a major causeof ICU admission, which requires mechanical
ventilation with higher mortality in obese comparedwith nonobese patients. It is, therefore, surprising thatexperience of AHRF in obese patients has rarely beenreported in the literature and, consequently, evidence-based guidelines remain to be established. There arecumulating reports that suggest that NPPV plays akey role in the treatment of obese patients withAHRF [6].
-
Figure 6
Pressure, flow, and volume tracers during proportional assist ventilation.
Figure 5
Different parameters for setting S/T mode.
146 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
Physiological rationale of noninvasive positivepressure ventilation in obesity hypoventilationsyndromeTo control upper airways obstruction and overcome therespiratory muscle load, a high EPAP and highinspiratory driving pressure are required.
Specifically, the EPAP should set to optimiserespiratory mechanics by modifying lung volume
and the operating position on pressure volumecurve as well as overcoming upper airwaysobstruction (reduce work of breathing) [7].
IPAP should be titrated to ensure satisfactory chestwall excursion with supplemental oxygen achievingtarget saturation from 90 to 92% [7].
Modes of noninvasive positive pressure ventilation inobesity hypoventilation syndromeThe optimal ventilatory mode is pressure support,using turbine-driven ventilators or ICU ventilators.A backup frequency rate is required in most cases,owing to the likelihood of sleep central apneas [8].
If a single circuit is used, it should be equipped with anexpiratory valve or an intentional calibrated leak [7]. Inthis previous case, a slight expiratory positive pressure isrequired to limit CO2 rebreathing. Clinical series showthat obesity hypoventilation syndrome (OHS) patientswith AHRF require high levels of inspiratory positivepressures (often 22 cmH2O) owing to low thoraciccompliance in this disease [8].
Another ventilatory mode in these patients is flow-preset mode that allows a better control of deliveredvolumes. AHRF in obese patients is one of the lastmedical situations where pressure support may be lesseffective than flow-preset modes [9]. After discharge,most OHS patients are managed with nocturnal bilevelNPPV without additional oxygen.
Noninvasive positive pressure ventilation settings inobesity hypoventilation syndrome
(1)
EPAP set at 8–10 cmH2O aiming SpO2≥90%.
(2)
IPAP set at 18–24 cH2O aiming pH ≥7.35 andtidal volume 8–10ml/kg of ideal body weight [10].
(3)
Inspiratory time limit 1.4 s.Acute hypercapnic respiratory failure ofrestrictive thoracic disordersPatients with severe kyphoscoliosis and acuterespiratory failure exhibit marked decrease ofpulmonary compliance but, contrary to in COPD,increase in airway resistance, and intrinsic PEEPseem to play only a secondary role [11]. Becausecough is not impaired like in neuromuscular diseases(NMD), secretion management is not so critical in thiscontext, and management of ARF may be easier [11].
In neuromuscular disorders (NMD) (Fig. 7), thenormality of the respiratory function requires the
-
Figure 7
Pathophysiology of muscle weakness in neuromuscular disease.
NPPV in acute hypercapnic RF Hussein 147
integrity of three main respiratory muscles: (i)inspiratory muscles, responsible for ventilation; (ii)expiratory muscles, involved in the ability to cough;and (iii) bulbar muscles, which protect against therisk of aspiration [12]. Acute NMD (such asGuillain–Barre’s syndrome) together with the ICUacquired NMD are the most frequent NMDassociated with ARF [13].
Concerning the mode of NPPV, it is preferable to usevolume-cycled ventilators in assist control, with hightidal volumes, for sufficient lung expansion andto allow air-stacking for coughing. This can beperformed during the day using a mouthpiece and atnight with a nasal or oral interface [12].
When patients with amyotrophic lateral sclerosis underhome mechanical ventilation need to be hospitalizedbecause of ARF, there are some technical as well asethical aspects that need to be considered. It needs to beconfirmed if all noninvasive respiratory aids wereoptimized at home, if the patient has refusedtracheostomy, if bulbar impairment is severe, and ifthe risk of aspiration is high. Lung function status,previous to the decompensation, can be helpful in thedecision making [14].
Another issue is when nonbulbar patients with NMDare intubated because of failure of noninvasiveventilation or because of a more-conventionalapproach. In this context, it is a common attitude togradually reduce the support of the ventilator until thepatient is weaned [15]. Unfortunately patients withNMDwith a pre-existing respiratory dysfunction oftenfail to wean off invasive ventilation and are almostinvariably tracheostomized [14].
Noninvasive positive pressure ventilation in patientswith an acute pneumothoraxFor patients with NMD, or any other condition inwhich the risk of acute pneumothorax is high whorequire NPPV [16], the following strategies can beused:
(1)
Insert chest drain.
(2)
Use pressure preset, pressure limited ventilator toreduce peak airway pressure.
(3)
Use the lowest IPAP and EPAP settings that arecomparable to arterial blood gas tensions andsymptoms.
(4)
Temporarily withdraw NPPV.Contraindications of noninvasive positivepressure ventilationThe boundaries for the use of NPPV continue toexpand. NPPV is not appropriate in well-documented end-stage disease or when several co-morbidities are present.
There are no absolute contraindications, althougha number of them have been suggested. In part,these ‘contraindications’ have been determinedby the fact that they were exclusion criteria forthe controlled trials [1]. It is therefore morecorrect to state that NPPV is not proven inthese circumstances rather than that it iscontraindicated.
Whether NPPV is contraindicated or not mustdepend on individual circumstances. For instance,if invasive ventilation is not considered appropriatebut NPPV would be acceptable, there is nothing tobe lost by a trial of NPPV and there are nocontraindications [2].
The possible contraindications for NPPV can besummarized as follow:
(1)
Facial trauma/burns.
(2)
Recent facial, upper airway, or upper gastro-intestinal tract surgery.
(3)
Fixed obstruction of the upper airway.
(4)
Inability to protect airway.
(5)
Cardiorespiratory arrest.
(6)
Uncontrolled life-threatening arrhythmia.
(7)
Hemodynamic instability.
(8)
Severe co-morbidity.
(9)
Coma.(10)
Vomiting and hematemesis.
(11)
Bowel obstruction.
(12)
Undrained pneumothorax
-
148 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
NPPV may be used, despite the presence ofthese contraindications (except for facial trauma/burn, and fixed obstruction of the upper airway),provided contingency plans for tracheal intubationhave been made, or if it is to be the ‘ceiling’ oftreatment in patients who are not candidates forintubation.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References1 Elliott MW. Non invasive ventilation for acute exacerbations of chronic
obstructive pulmonary disease: do not think twice, its alright. Am J RespirCrit Care Med 2012; 185:121–123.
2 Ambrosino N, Vaghegginni G. Non invasive ventilation in acute caresettings: where are we? Eur Respir I 2008; 31:874–886.
3 Austin MA. Effect of high flow oxygen on mortality of chronic obstructivepulmonary disease patients in pre hospital setting: randomized controlledtrial. BMJ 2010; 341:5426.
4 Colombo D. Physiologic response to varying levels of pressure supportand neurally adjusted ventilatory assist in patients with acute respiratoryfailure. Intensive Care Med 2008; 34:2010–2018.
5 El-Solh A, Sikka P, Bozkanat E, Jaafar W, Davies J. Morbid obesity in themedical ICU. Chest 2001; 120:1989–1997.
6 Jubber AS. Respiratory complications of obesity. Int J Clin Pract 2004;58:573–580.
7 Cuvelier A, Muir JF. Acute and chronic respiratory failure in patients withobesity hypoventilation syndrome: a new challenge for noninvasiveventilation. Chest 2005; 128:483–485.
8 Cuvelier A, Muir JF. Obesity-hypoventilation syndrome and noninvasivemechanical ventilation: new insights in the Pickwick papers? Chest 2007;131:7–8.
9 Pastores SM. Morbidly obese patients with acute respiratory failure: don’treach for the endotracheal tube yet!. Crit Care Med 2007; 35:956–957.
10 Mokhlesi B, Kryger MH, Grunstein RR. Assessment and management ofpatients with obesity hypoventilation syndrome. Proc Am Thorac Soc2008; 5:218–225.
11 Conti G, Rocco M, Antonelli M. Respiratory system mechanics in the earlyphase of acute respiratory failure due to severe kyphoscoliosis. IntensiveCare Med 1997; 23:539–544.
12 Benditt JO. The neuromuscular respiratory system physiology,pathophysiology, and a respiratory care approach to patients. RespirCare 2006; 51:829–837.
13 Hughes RA, Wijdicks EF, Benson E, Cornblath DR, Hahn AF, MeythalerJM. Supportive care for patients with Guillain-Barre’s syndrome. ArchNeurol 2005; 62:1194–1198.
14 Farrero E, Prats E, Povedano M, Martinez-Matos JA, Manresa F,Escarrabill J. Survival in amyotrophic lateral sclerosis with homemechanical ventilation: the impact of systematic respiratory assessmentand bulbar involvement. Chest 2005; 127:2132–2138.
15 Servera E, Sancho J, Zafra MJ, Catala A, Vergara P, Marin J. Alternativesto endotracheal intubation for patients with neuromuscular diseases. Am JPhys Med Rehabil 2005; 84:851–857.
16 Seneviratne J, Mandrekar J, Wijdicks EF, Rabinstein AA. Noninvasiveventilation in myasthenic crisis. Arch Neurol 2008; 65:54–58.
-
Original article 149
Effectiveness of pulmonary rehabilitation on pulmonary functionparameters and dyspnea in patients with stable chronicobstructive pulmonary diseaseAtef F. Al Karn, Wafaa A. Hassan, Abdel A. Abo El Fadl, Manal A. Mahmoud
Background Chronic obstructive pulmonary disease(COPD) is a common preventable and treatable diseasecharacterized by persistent airflow limitation that is usuallyprogressive. The characteristic symptoms of COPD arechronic and progressive dyspnea, cough, and sputumproduction. Breathing exercises aim to reduce hyperinflation,improve respiratory muscle performance, and reducedyspnea.
Aim The aim of the study was to assess the effectiveness ofbreathing exercises among patients with stable COPD inimprovement of pulmonary function parameters, 6-min walkdistance, and dyspnea score.
Patients and methods Randomized controlled design wasused in this study. Patients recruited for this study wereenrolled from the outpatient clinic of Department of ChestDiseases and Tuberculosis. Overall, 15 patients with stableCOPD were enrolled in pulmonary rehabilitation group andunderwent breathing exercises for 12 weeks. Moreover, 15patients were enrolled in the control group. Statisticalpackage for the social sciences (SPSS version 20) softwarewas used for statistical analysis.
Results In the breathing exercise group, there was asignificant increase in the mean forced expiratory volume in
© 2018 Egyptian Journal of Bronchology | Published by Wolters Kluwer - Medknow
first second (P= 0.001), forced vital capacity (P= 0.001), andinspiratory capacity (P=0.015). There was a significantdecrease in themean functional residual capacity (P= 0.005),residual volume (P=0.001), and total lung capacity(P=0.001). There was no significant difference between thevalues of the previous parameters in the control group.
Conclusion In stable COPD, breathing exercises improvedpulmonary function parameters, 6-min walk distance, anddyspnea score.Egypt J Bronchol 2018 12:149–153© 2018 Egyptian Journal of Bronchology
Egyptian Journal of Bronchology 2018 12:149–153
Keywords: chronic obstructive pulmonary disease, dyspnea, pulmonaryrehabilitation
Department of Chest Diseases and Tuberculosis, Assiut University Hospital,
Assiut, Egypt
Correspondence to Manal Ahmed El Khawaga, Department of Chest
diseases and tuberculosis, Faculty of Medicine, Assiut university
Tel: + 20 882 413 711; fax: 088/2350177;
e-mail: [email protected]
Received 26 May 2016 Accepted 28 February 2017
IntroductionChronic obstructive pulmonary disease (COPD) is acommon preventable and treatable disease characterizedby airflow limitation that is usually progressive [1].Airflow limitation is usually associated with airtrapping and hyperinflation. Lung hyperinflation resultsin disruption of neuroventilatory coupling, increasedwork of breathing, and the perception of dyspnea.Breathing exercises are designed to retain the breathingpattern, reduce breathlessness, increase exercise capacity,alter respiratory muscle recruitment, improve respiratorymuscle performance, reduce dyspnea, and improvewell-being for patients with COPD [2].
The aim of the study was to evaluate the effect ofbreathing exercises on hyperinflation in patients withstable COPD. Exertional dyspnea, pulmonary functiontests parameters, and 6-min walk distance were themain outcome measures.
This is an open access journal, and articles are distributed under the terms
of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0
License, which allows others to remix, tweak, and build upon the work
non-commercially, as long as appropriate credit is given and the new
creations are licensed under the identical terms.
Patients and methodsThis prospective cross-sectional randomized controlledstudy was carried out in Chest Outpatient Clinic.The total duration the study was 12 weeks from
January 2014 to March 2015. All patients providedwritten consent, and the study was approved by therespective ethics committees and institutional reviewboards.
The inclusion criteria were diagnosis as stableCOPD ‘moderate, severe, and very severe’ accordingto Global Initiative for Obstructive Lung Diseaseguidelines 2015 [1] [post bronchodilator forcedexpiratory volume in first second (FEV1)/forced vitalcapacity (FVC) 120% predicted by plethysmography].
The main exclusion criteria were bronchial asthma,heart diseases, musculoskeletal disorders, peripheralvascular diseases, respiratory failure, decompensatedcorpulmonale, acute pulmonary embolism, uncontrolledcardiac arrhythmia, and any disabling conditions thatwould interfere with the tests.
DOI: 10.4103/ejb.ejb_43_16
mailto:[email protected]
-
150 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
Following an initial screening visit at the outpatientclinic to assess eligibility, patients who fulfilled theinclusion criteria were asked to return after 2 weeksfor the baseline visit. Patients were kept on theircurrent treatment (such as inhaled corticosteroids andlong-acting B2 agonist). Patients were randomized atthe baseline visit through the closed envelop method toallocate each of them either into breathing exercisesgroup, which underwent exercises to mobilize one sideof the chest, mobilize the upper chest, stretch thepectoralis muscles, and mobilize the upper chest andshoulders and pursed lip breathing, or into the controlgroup. Patients in the control group were kept onlyon their current treatment. Clinic visits were scheduledafter 4, 8, and 12 weeks following randomization.Assessment of dyspnea by modified Medical ResearchCouncil (mMRC),6-minwalkdistance, andperformingpulmonary function testing including spirometry andbody plethysmography (D97723;Zan 300,Oberthulba,Germany) were done at baseline and at all clinic visits.Measurements were performed according to AmericanThoracic Society criteria.[3].
Statistical analysisAll results were tabulated and statistically analyzedusing the statistical package for the social sciences(SPSS version 20; SPSS Inc., Chicago, Illinois,USA) software. Data were expressed as mean±SDor frequencies. The t-test was used for comparisonof continuous variables between the two groups.Wilcoxon’s sign rank test was used for comparing theresults in the same group before and after the therapy.
Table 2 Pulmonary function test parameters at the baselinevisit (n=30)
Variables Controlgroup (N=15)
Breathingexercises group
P value
ResultsA total of 30 patients were selected for this study, with15 patients in each group.
(mean±SD) (N=15) (mean±SD)
FEV1%predicted
35.07±13.20 40.93±19.83 0.305
FVC% predicted 51.53±7.25 57.00±21.91 0.092
FEV /FVC% 65.73±12.12 70.73±12.20 0.399
Patient demographicsAge, weight, height, BMI, smoking status, and packper year index were determined in all patients (Table 1).
Table 1 Demographic characteristics of the study patients atthe baseline visit (n=30)
Variables Control (N= 15)(mean±SD)
Breathingexercise (N=15)
(mean±SD)
P value
Age (years) 64.47±6.99 64.87±8.56 0.976
Height (cm) 162.87±7.21 166.47±6.13 0.170
Weight (kg) 65.53±14.29 65.20±6.95 0.935
BMI (kg/m2) 24.62±4.65 23.49±1.73 0.524
Smoking status [n (%)]
Current smoker 1 (6.7) 2 (13.3) 0.697
Ex-smoker 14 (93.3) 13 (86.7)
Pack per year 22.40±7.94 22.80±4.71 0.943
There was no statistical significant differenceregarding the baseline pulmonary function testsparameters at baseline visit among the study groups(Table 2).
In the control group, therewas anonsignificant differencebetween the baseline values and the values obtained after12 weeks regarding spirometric parameters such asFEV1 (P=0.107), FVC (P=0.089), and inspiratorycapacity (IC) (P=0.239); plethysmographic parameterssuch as functional residual capacity (FRC) (P=0.148),residual volume (RV) (P=0.116), and TLC (P=0.840);dyspnea score (P=0.115); and 6-min walking distance(P=0.327) (Table 3).
In the breathing exercise group, there was a significantimprovement in FEV1 (P=0.001), FVC (P=0.001),IC (P=0.015), FRC (P=0.005), RV (P=0.001),TLC (P=0.001), RV/TLC (P=0.010), dyspnea score(P=0.005), and 6-min walking distance (P=0.001)whereas there was a nonsignificant difference regardingbaseline and 12-week values for FEV1/FVC (P=0.637)(Table 4).
DiscussionThe present study was designed to evaluate pulmonaryfunctions, dyspnea score, and 6-min walking distancefollowing12weeks courseof breathing exercises that aimtodecreasehyperinflation inpatientswith stableCOPD.
Regarding the characteristics of the study participants,the present study showed that the mean age of study
1
predicted
IC% predicted 42.27±10.20 47.87±16.78 0.093
FRC% predicted 158.20±39.23 156.13±37.99 0.097
RV % predicted 141.27±11.75 136.00±4.46 0.154
TLC% predicted 143.67±30.81 141.27±10.38 0.168
RV/TLC %predicted
160.93±29.09 152.07±29.02 0.112
Dyspnea score(mMRC)
3.27±0.46 3.43±0.46 0.028
6-min walkingdistance (m)
50.87±9.46 51.73±7.06 0.660
FEV1, forced expiratory volume in 1 s; FRC, functional residualcapacity; FVC, forced vital capacity; IC, inspiratory capacity;mMRC, modified Medical Research Council; RV, residual volume;TLC, total lung capacity.
-
Table 3 Pulmonary function test parameters before and after 12 weeks in the control group (n=15)
Variables Baseline After 12 weeks P value
FEV1% predicted 35.07±13.20 35.13±9.55 0.107
FVC% predicted 51.53±7.25 53.27±9.08 0.089
FEV1/FVC% predicted 65.73±12.12 64.47±10.70 0.181
IC% predicted 42.27±10.20 42.73±9.48 0.239
FRC% predicted 158.20±39.23 157.07±39.11 0.148
RV% predicted 141.27±11.75 142.93±11.41 0.116
TLC% predicted 143.67±30.81 147.53±28.96 0.840
RV/TLC% predicted 160.93±29.09 158.20±25.43 0.092
Dyspnea score (mMRC) 3.27±0.46 3.18±0.41 0.115
6-min walking distance (m) 50.87±9.46 49.87±9.43 0.327
FEV1, forced expiratory volume in 1 s; FRC, functional residual capacity; FVC, forced vital capacity; IC, inspiratory capacity; mMRC,modified Medical Research Council; RV, residual volume; TLC, total lung capacity.
Table 4 Pulmonary function test parameters before and after 12 weeks in the pulmonary rehabilitation group
Variables Baseline After 12 weeks P value
FEV1% predicted 40.93±19.83 47.00±19.98 0.001*
FVC% predicted 57.00±21.91 63.60±22.45 0.001*
FEV1/FVC% predicted 70.73±12.20 68.87±11.58 0.637
IC% predicted 47.87±16.78 59.13±16.42 0.015*
FRC% predicted 156.13±37.99 140.60±37.77 0.005*
RV% predicted 136.00±4.46 124.60±4.24 0.001*
TLC% predicted 141.27±10.38 130.87±10.08 0.001*
RV/TLC% predicted 152.07±29.02 142.53±33.95 0.010*
Dyspnea score (mMRC) 3.43±0.46 3.10±0.00 0.005*
6min walking distance(m) 51.73±7.06 63.80±10.06 0.001*
FEV1, forced expiratory volume in 1 s; FRC, functional residual capacity; FVC, forced vital capacity; IC, inspiratory capacity; mMRC,modified Medical Research Council; RV, residual volume; TLC, total lung capacity.
Pulmonary rehab. for COPD patients Al Karn et al. 151
groups was 64 years. These patients are appropriatecandidates for the study and were not to be excludedbased on age alone.
Some pulmonary rehabilitation studies have excludedpatients older than 70 years, and rationale for ageexclusion was not given in these studies; however, allthree also excluded patients with other disablingconditions, including arthritis, ischemic heart disease,and heart failure [4]. Thus, elderly patients mayhave been considered inappropriate for pulmonaryrehabilitation because it was believed that they were‘too old’, that they would not tolerate aggressivetreatment, or that the physiologic effects of aging andcomorbid illness would limit their ability to improveexercise capacity [5].
Regarding outcome measures after rehabilitation,the present study showed that there was animprovement in baseline dyspnea score grade inbreathing exercise training group compared withthe control group.
The findings by Wedzicha et al. [6] were fullyconsistent with this; they showed that the effect ofexercise training in patients with COPDmight depend
on the initial level of dyspnea. Patients with moderatedyspnea (MRC grade 2/3), who were regularly mobileoutside the home, showed quite large improvements inexercise capacity after physical training. In contrast,patients with severe disability (MRC grade 4), whowere largely housebound owing to dyspnea, showed noimprovement in exercise performance followingindividualized physical training [6].
The present study also reported improvement indyspnea score within the respiratory training groupthan the control group.
Harver et al. [7] were fully consistent with this; theyfound that targeted inspiratory muscle trainingresults in significant increases in respiratorymuscle function and significant reductions indyspnea. This supports the concept that anincrease in the strength of inspiratory muscles canameliorate dyspnea [7].
Another study by Lisboa et al. [8] found that thetrained patients were able to make greater effortsand perform harder tasks than they were beforeinspiratory muscle training and were able to carryout activities faster without dyspnea.
-
152 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
Exercise tolerance was measured using the 6-minwalking distance. Timed walking tests such as the 6-min walking test have gained popularity for use in clinicalpractice and research setting to assess changes infunctional capacity following pulmonary rehabilitationintervention [9,10].
The present study showed that 6-min walking distanceincreased to 63m after 12 weeks of respiratory trainingprogram.This improvementwas statistically significant.
Redelmeier et al. [11] suggested that the minimalclinically meaningful increase in the 6-min walkingdistance is ∼54m.
The improvement in exercise capacity after aerobictraining program may be because of the following:(a) improving ventilatory muscle function and (b)desensitization to dyspnea.
This finding correlated with a meta-analysis doneby Bendtrup et al. [12], where in a controlled 12-week study of outpatient pulmonary rehabilitation,the 6-min walking distance increased by 80m at6 weeks (half-way in the program), 113m at theend of the program, and 96m 12 weeks after theprogram ended. Another study demonstrated that6-min walking distance increased by 71.75m after6 weeks of outpatient pulmonary rehabilitation[12,13].
However, De-Torres et al. [14] demonstratedthat the mean improvement in 6-min walkingdistance was 65m after 6–8 weeks of pulmonaryrehabilitation. Another study by Seals et al. [15]noted an increase of 78.41m in 6-min walkingdistance after 6 months of outpatient and home-based program.
Significant spirometric and plethysmographicimprovements were observed in patient who weresubjected to 12 weeks course of breathing exercisetraining, where significant increases in FEV1(P=0.001), FVC (P=0.001), and IC (P=0.015) wereobserved in addition to significant reduction inRV (P=0.001), TLC (P=0.001), FRC (P=0.005),and RV/TLC (P=0.010) in comparison with controlgroup. These results were in concordance with theresults of Liu et al. [16].
Results of Tout et al. [17] were in agreement with theresults of this study; spirometric and plethysmographicoutcomes were similar across all the breathingexercises examined (diaphragmatic breathing, pursed
lip breathing, exercise to mobilize one side of the chest,exercise to mobilize the upper chest and stretch thepectoralis muscles, exercise to mobilize the upper chestand shoulders, and to increase expiration during deepbreathing).
In contrast, in other studies, no significantmodification of pulmonary functions was markedafter a training program. Pulmonary rehabilitationcauses modification in peripheral myopathy but notventilatory limitation. The airflow limitation in mostcases is both progressive and associated with anabnormal inflammatory response of the lungs tonoxious particles or gases [18,19].
Other studies have shown some improvement inFVC, which may have been because of the improvedrespiratory muscle function and a reduction in smallairways disease; the improvement in FEV1 in thosecases was small and not statistically significant [14].Stav et al. [20] demonstrated that outpatient prolongedpulmonary rehabilitation program (3 years) did notimprove FEV1, but has an important beneficialeffect on the rate of FEV1 decline. In addition, itincreased endurance time and work, so pulmonaryrehabilitation should be considered as a diseasemodifier.
Estève et al. [21] found that breathing pattern training,enhanced with visual feedback, increased the FEV1and FVC in patients with COPD.
However, another study by Singh et al. [22] reportedno improvement following pulmonary rehabilitationhaving breathing exercises as a component.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References1 Global Initiative for Chronic Obstructive Lung Disease. Global strategy
for diagnosis, management, and prevention of chronic obstructivepulmonary disease. (Updated 2015). http://www.goldcopd.org.
2 Holland AE, Hill CJ, Jones AY, McDonald CF. Breathing exercises forchronic obstructive pulmonary disease. Cochrane Database Syst Rev2012;17:CD008250.
3 Redllch CA, Tarlo SM, Hankinson JL, Townsend MC, Eschenbacher WL,von Essan SG, et al. Official American Thoracic Society TechnicalStandards: spirometry in the occupational setting. Am J Respir CritCare Med 2011; 189:984–994.
4 Tydeman DE, Chandler AR, Graveling BM, Culot A, Harrison BD. Aninvestigation into the effects of exercise tolerance training on patients withchronic airways obstruction. Physiotherapy 1984; 70:261–264.
http://www.goldcopd.org
-
Pulmonary rehab. for COPD patients Al Karn et al. 153
5 Ward JA, Akers G, Ward DG, Pinnuck M, Williams S, Trott J, et al.Feasibility and effectiveness of a pulmonary rehabilitation program in acommunity hospital setting. Br J Gen Pract 2002; 52:539–542.
6 Wedzicha JA, Bestall JC, Garrod R, Garnham R, Paul EA, Jones PW.Randomized controlled trial of pulmonary rehabilitation in severe chronicobstructive pulmonary disease patients, stratified with the MRC dyspnoeaScale. Eur Respir J 1998; 12:363–369.
7 Harver A, Mahler DA, Daubenspeck JA. Targeted inspiratory muscletraining improves respiratory muscle function and reduces dyspnea inpatients with chronic obstructive pulmonary disease.Ann InternMed 1989;111:117–124.
8 Lisboa C, Villafranca C, Leiva A, Cruz E, Pertuzé J, Borzone G. Inspiratorymuscle training in chronic airflow limitation: effect on exerciseperformance. Eur Respir J 1997; 10:537–542.
9 Kervio G, Ville NS, Leclercq C, Daubert JC, Carré F. Intensity and dailyreliability of the six-minute walk test in moderate chronic heart failurepatients. Arch Phys Med Rehabil 2004; 85:1513–1518.
10 Kesten S, Casaburi R, Kukafka D, Cooper C. Improvement in self-reported exercise participation with the combination of tiotropium andrehabilitative exercise training in COPD patients. Int J COPD 2008;3:127–136.
11 Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting smalldifferences in functional status: the six minute walk test in chronic lungdisease patients. Am J Respir Crit Care Med 1997; 155:1278–1282.
12 Bendstrup KE, Ingemann J, Holm S, Bengtsson B. Out-patientrehabilitation improves activities of daily living, quality of life andexercise tolerance in chronic obstructive pulmonary disease. Eur RespirJ 1997; 10:2801–2806.
13 Yerg JE, Seals DR, Hagberg JM, Holloszy JO. Effect of enduranceexercise training on the ventilatory function in older individuals. J ApplPhysiol 1985; 58:791–794.
14 De-Torres JP, Pinto-Plata V, Ingenito E, Bagley P, Gray A, Berger R, CelliB. Power of outcomemeasurements to detect clinically significant changesin pulmonary rehabilitation of patients with COPD. Chest 2002; 121:1092–1098.
15 Seals DR, Chakraborty K, Das KM, Ganguly S, Ballav A. A low costpulmonary rehabilitation program for COPD patients: is it any good?IJPMR 2006; 17:26–32.
16 Liu YQ, Ling XY, Li YZ, Quing HS, XuRM. Conspicuous effect on treatmentof mild to moderate COPD by combining deep-breathing exercise withoxygen inhalation. Int J Clin Exp Med 2015; 8:9918–9924.
17 Tout R, Tayara L, Halimi M. The effects of respiratory muscle training onimprovement of the internal and external thoraco pulmonary respiratorymechanism in COPD patients. Ann Phys Rehabil Med 2013; 56:193–211.
18 Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF, Wasserman K.Reductions in exercise lactic acidosis and ventilation as a result of exercisetraining in patients with obstructive lung disease. AmRev Respir Dis 1991;143:9–18.
19 Mercken EM, Hageman GJ, Schols AM, Akkermans MA, Bast A, WoutersEF. Rehabilitation decreases exercise-induced oxidative stress in chronicobstructive pulmonary disease. Am J Respir Crit Care Med 2005; 172:994–1001.
20 Stav D, Raz M, Shpirer I. Three years of pulmonary rehabilitation: inhibitthe decline in airflow obstruction, improves exercise endurance time, andbody-mass index, in chronic obstructive pulmonary disease. BMC PulmMed 2009; 9:26.
21 Estève F, Blanc-Gras N, Gallego J, Benchetrit G. The effects of breathingpattern training on ventilatory function in patient with COPD. BiofeedbackSelf Regul 1996; 21:311.
22 Singh V, Khandelwal DC, Khandelwal R, Abusaria S. Pulmonaryrehabilitation in patients with chronic obstructive pulmonary disease.Indian J Chest Dis Allied Sci 2003; 45:13–17.
-
154 Original article
Bronchial asthma: clinical phenotypes and endotypes and theirrelation with glucocorticoids circadian rhythm andparasympathetic activityMagdy M. Zedana, Magdy Abd El Moneim El-Zinyb, Abd Elazeez AtallahShabaanb, Youssef M. Mosaadc, Wafaa Nabil Laimond
Introduction Asthma is a heterogeneous disease andpresents in different clinical patterns ‘phenotypes’ as a resultof diverse pathobiological background ‘endotypes’.
Objectives Theaimof this studywas tostudyserum interleukin-13 (IL-13) levels and the frequency of (IL-13) +1923C/T genepolymorphism in Egyptian children with asthma and to studyglucocorticoids circadian rhythm in nocturnal asthma.
Patients and methods The frequency of (IL-13) +1923C/Tgene polymorphism genotypes was determined in 114asthmatic Egyptian children and compared with a matchedgroup of 152 healthy controls using PCR. Serum IL-13 andcortisol a.m. and p.m. concentrations in serumwere assessedusing enzyme linked immunosorbent assay.
Results Serum IL-13 was found to be significantly higher inasthmatic patients when compared with the control group(P
-
Figure 1
Genotyping of IL-13 C1923T rs1295686 by agarose gel electropho-resis. Lane 1, 2: PCR amplified product at 302 base pair (bp). Lane 0:GeneRuler 50 bp DNA Ladder. Lanes: 4, 5, 7-9, 12, 14 and 16-19 and12-15=CT genotype (three bands at 294, 230, and 64 bp). Lanes: 6=CC genotype (two band at 230 and 64 bp), Lane 10, 11, 13 and 15=TTgenotype (single band at 294 bp).
Bronchial asthma: phenotypes and endotypes Laimon 155
or asthma, and having a normal forced expiratoryvolume in 1 s (FEV1). The characteristics of thestudied groups have been presented in Table 1. Thestudy protocol was approved by the Ethical Committeeof Mansoura Faculty of Medicine, Egypt, on 11 July2013 with code numberMD/16. Informed consent wasobtained from the parents of all patients.
Serum level of IL-13 was assessed using commercialenzyme linked immunosorbent assay (ELISA) kits fromR&D Systems Inc. (Minneapolis, Minnesota, USA).
Serum cortisol was measured at 9 a.m. and 9 p.m. forpatients and controls. It was measured with ELISAusing the Calbiotech Inc. (CBI) cortisol ELISA kit(Calbiotech Inc., Spring Valley, CA, USA).
FEV1 was measured with a spirometer (Spirobank IIbasic, MIR Medical International Research, Roma,Italy); the highest of the three successive measurementswas taken. For patients and controls, PFTs wereperformed at 9 a.m. and at 9 p.m. as well. Referencevalues were adjusted according to the recommendation ofAmericanThoracic Society standards of acceptability andreproducibility [9]. The predicted values for eachparticipant was calculated according to the data enteredto the device before the maneuver, including age, sex,weight, and height.
GenomicDNAwas extracted fromwhole venousEDTAblood using the GeneJET whole blood genomic DNApurification mini-kits (lot 00138029; Thermo Scientific,Lithuania, UK) and stored at −20°C until use. Thegenotypes of (IL-13) +1923C/T single nucleotidepolymorphisms (SNPs) were analyzed using the PCR-restriction fragment length polymorphism according tothe method of Li et al. [10]. The sequences of the senseand antisense primers were 5′-AAT GAG ACA GTCCCT GGA AAG-3′ and 5′-CCG CCT ACC CAAGAC ATT T-3′, respectively (prepared by Eurofins
Table 1 Clinical characteristics of the study sample
Asthmatic pati
Number of participants 114
Mean age 10±2.3
Sex ratio (girls/boys) 0.67 (46/68
Total frequency of female patients (%) 40.4
Total frequency of male patients (%) 59.6
Total serum IgE (IU/ml) 184.2±85
Serum IL-13 (pg/ml) 74.6 ±31.82
Peripheral blood eosinophilic (%) 3 (0.4–18)
FEV1 (% predicted) 75.5±15.62
FEV1, forced expiratory volume in 1 s; IgE, immunoglobulin E; IL-13, intrange. The Mann–Whitney test for comparison of FEV1, serum IgE, eos*Statistical significance was defined as P≤0.05.
Genomics, Ebersberg bei München, Germany). Therestriction enzyme used was BsaAI (Fig. 1).
The activity of the parasympathetic system wasevaluated by performing ECG for all patients andcontrols twice, once at 9 a.m. and the other at 9p.m., to assess heart rate variability.
Mean heart rateMean heart rate value is measured on the entire (ECG)recording. Mean heart rate is measured in beats perminute (bpm).
Mean NNMeanNN is ameanheart beat interval valuemeasured onentire ECG recording (NN means normal-to-normalbeats). It is called the mean RR interval when it isderived from ECG recording (N-N interval=R-Rinterval).MeanNNismeasured inmilliseconds (ms) [11].
Statistical analysisThe Hardy–Weinberg equilibrium was estimated.Data were analyzed using Statistical Package for
ents Healthy controls P value
152
10±2.8 0.9
) 0.78 (67/85) 0.5
56
44
41.5±2
-
156 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
Social Sciences underWindows (version 22) (Armonk,NY: IBM Corp.). Numerical data, which showeda nonparametric distribution according to theKolmogorov–Smirnov test, were expressed as medianand range, whereas parametric data were expressed asmedian and SD. Categorical data were expressed asnumbers and %. Differences in genotype and allelefrequencies were evaluated using the χ2-test. Oddsratio and 95% confidence interval values werecalculated using Epi info 7 program (Developed byCDC, Atlanta, Georgia, US). A P value less than 0.05was considered significant.
ResultsSerum IL-13 was found to be significantly higher inasthmatic patients when compared with the controlgroup (P
-
Table 4 Pulmonary function tests, heart rate variability, and serum cortisol levels in patients with nocturnal asthma incomparison with asthmatic patients without nocturnal symptoms
Patients with nocturnal asthma (n=71) Patients without Nocturnal asthma (n=43) P value
FEV1 (a.m.) (% predicted) 75.4±14 75.8±18.11 0.9
FEV1 (p.m.) (% predicted) 68.8±14.63 75±18 0.1
FVC (a.m.) (% predicted) 71.1±14.21 69.7±16.42 0.6
FVC (p.m.) (% predicted) 66.2±13.73 69.1±16.43 0.06
FEV1/FVC ratio (a.m.) 75.3 (50.4–105.4) 75.6 (45.5–111.4) 0.9
FEV1/FVC ratio (p.m.) 70 (47–104) 74.3 (44.3–108) 0.14
Mean heart rate (a.m.) 99.6±11.92 100.6±12.83 0.7
Mean heart rate (a.m.) 95.8±13.41 92.2±13.64 0.17
Mean R-R interval (a.m.) 561±38.71 562±45.73 0.9
Mean R-R interval (p.m.) 575.5±56 573±45.45 0.8
Serum cortisol (a.m.) 62.8±17.73 59.1±19.41 0.24
Serum cortisol (p.m.) 28.7±13.74 55.4±19.22
-
158 Egyptian Journal of Bronchology, Vol. 12 No. 2, April-June 2018
However, (IL-13) +1923C/T locus was reported as asusceptibility factor for asthma in Mauritian Indianchildren [33]. A meta-analysis, which retrieved26 articles including 17 642 asthma patients and 42402 controls, found out that this (IL-13) +1923C/Tpolymorphism is a risk factor for asthma development[7]. Such diverse findings may be due tovariable genetic makeup in different ethnic groupsand also due to variable sample sizes. Furthercase–control studies with more ethnicities are stillneeded.
Nocturnal asthma is defined as worsening of asthmasymptoms and airway responsiveness at night timeresulting in poor quality of life [34]. Our primaryhypothesis was to identify key predictors for theoccurrence of nocturnal symptoms over time. Asignificantly lower serum cortisol pm was found inasthmatic patients with nocturnal symptoms whencompared with those without nocturnal symptoms.However, there were no significant differencesbetween the two groups as regards PFTs andparasympathetic activity (which were assessed bymeans heart rate variability).
According to the circadian rhythm of cortisol, itreaches its trough level during the early biologicalnight, close to habitual bedtime [35]. Asthma is aninflammatory airway disease and this inflammationleads to AHR and if untreated it will lead to airwayremodeling. Glucocorticoids being a potent anti-inflammatory agent, their circadian rhythm affectthe diurnal variation of asthma symptoms [36]. Thiscan explain why serum cortisol (at night) was lower inthe studied nocturnal asthma cohort. Moreover, in aprevious study, mometasone furoate dry powderinhaler (200 μg) was administered once/day at nighttime and it was found to significantly improve PFTs inpatients previously using short-acting β2 agonists alonefor asthma control [37]. Understanding the biologicalclock of cortisol release in cases of nocturnal asthma canjustify the timing of administration of steroid therapyor what is called ‘chronotherapy’ for better symptomcontrol.
ConclusionWe can easily recognize the complex nature of asthmasyndrome, which led to a paradox in asthmamanagement; we have effective treatments that arenot biologically informative, and we haveinformative treatments that are less effective.Relating the observable phenotype to the underlyingendotype, including physiological, biological, and
genetic indicators, can provide better identificationof asthma phenotypes, better preventative strategies,and more wise application of precision medicineapproaches.
Genetic determinants are an attractive approach to detectsusceptibility for asthma. However, further studies ondifferent ethnic groups should be conducted to upgradethe level of evidence. Studying glucocorticoids circadianrhythm in nocturnal asthma is a promising approach forchronotherapy in such cases.
Financial support and sponsorshipThis research work was funded by Academy ofScientific Research and Technology (ASRT) in Egypt.
Conflicts of interestThere are no conflicts of interest.
References1 GINA. The Global Strategy for Asthma Management and Prevention.
Available at: http://www.ginasthma.org/; 2016. [Accessed 24 August2016].
2 Landgraf-Rauf K, Anselm B, Schaub B. The puzzle of immune phenotypesof childhood asthma. Mol Cell Pediatr 2016; 3:27.
3 Zedan MM, El-Chennawi FA, Fouda AE. Interleukin-12 and peripheralblood invariant natural killer T cells as an axis in childhood asthmapathogenesis. Iran J Allergy Asthma Immunol 2010; 9:43–48.
4 Wenzel SE. Asthma phenotypes: the evolution from clinical to molecularapproaches. Nat Med 2012; 18:716–725.
5 Lötvall J, Akdis CA, Bacharier LB, Bjermer L, Casale TB, Custovic A, et al.Asthma endotypes: a new approach to classification of disease entitieswithin the asthma syndrome. J Allergy Clin Immunol 2011; 127:355–360.
6 Custovic A, Ainsworth J, Arshad H, Bishop C, Buchan I, Cullinan P, et al.The Study Team for Early Life Asthma Research (STELAR) consortium‘Asthma e-lab’: team science bringing data, methods and investigatorstogether. Thorax 2015; 70:799–801.
7 Xu Y, Li J, Ding Z, Li J, Li B, Yu Z, Tan W. Association between IL-13+1923C/T polymorphism and asthma risk: a meta-analysis based on 26case–control studies. Biosci Rep 2017; 37:BSR20160505.
8 Litinski M, Scheer FA, Shea SA. Influence of the circadian system ondisease severity. Sleep Med Clin 2009; 4:143–163.
9 Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A,et al. ATS/ERS Task Force Standardisation of spirometry. Eur Respir J2005; 26:319–338.
10 Li H, Xiaoyan D, Quanhua L, Jie L, Yixiao B. Single-nucleotidepolymorphisms in genes predisposing to asthma in children of ChineseHan nationality. J Investig Allergol Clin Immunol 2009; 19:391–395.
11 Lutfi MF. Review article: heart rate variability. Sud JMS 2011; 6:43–50.
12 Chung HL. Asthma in childhood: a complex, heterogeneous disease.Korean J Pediatr 2011; 54:1–5.
13 Xie M, Wenzel SE. A global perspective in asthma: from phenotype toendotype. Chin Med J (Engl). 2013; 126:166–174.
14 Zedan MM, Laimon WN, Osman AM, Zedan MM. Clinical asthmaphenotyping: a trial for bridging gaps in asthma management. World JClin Pediatr 2015; 4:13–18.
15 Zedan M, Settin A, Farag M, Ezz-Elregal M, Osman E. Prevalence ofbronchial asthma among Egyptian school children. Egypt J Bronchol 2009;3:124–130.
16 Pukelsheim K, Stoeger T, Kutschke D, Ganguly K, Wjst M. Cytokineprofiles in asthma families depend on age and phenotype. PLoS one2010. 5:e14299.
17 Corren J. Role of interleukin-13 in asthma.Curr Allergy Asthma Rep 2013;13:415–420.
http://www.ginasthma.org/
-
Bronchial asthma: phenotypes and endotypes Laimon 159
18 Lee YC, Lee KH, Lee HB, Rhee YK. Serum levels of interleukins (IL)-4, IL-5, IL-13, and interferon-gamma in acute asthma. J Asthma 2001;38:665–671.
19 Joseph J, Benedict S, Safa W, Joseph M. Serum interleukin-5 levels areelevated in mild and moderate persistent asthma irrespective of regularinhaled glucocorticoid therapy. BMC Pulm Med 2004; 4:2.
20 Siddiqui S, Cruse G, Mckenna S, Monteiro M, Mistry M, Wardlaw A, et al.IL-13 expression by blood T cells and not eosinophils is increased inasthma compared to non-asthmatic eosinophilic bronchitis. BMC PulmMed 2009; 9:34.
21 B