An#hormonelle Therapie 2017 - verständlich erläutert · BRCA Testung anbieten (falls klinische...
41
M.Thill PD Dr. M. Thill Klinik für Gynäkologie und Geburtshilfe Zertifiziertes Brustzentrum (DKG/DGS) Zertifiziertes Gynäkologisches Krebszentrum (DKG) Zertifiziertes Endometriosezentrum AGAPLESION Markus Krankenhaus Frankfurt am Main „Gemeinsam verstehen“ Pa0en0nnentag des interdisziplinären Brust und Genitalkrebszentrum am AGAPLESION Markus-Krankenhaus, 10.09.2017 An#hormonelle Therapie 2017 - verständlich erläutert -
Transcript of An#hormonelle Therapie 2017 - verständlich erläutert · BRCA Testung anbieten (falls klinische...

M.Thill
PD Dr. M. Thill Klinik für Gynäkologie und Geburtshilfe Zertifiziertes Brustzentrum (DKG/DGS)
Zertifiziertes Gynäkologisches Krebszentrum (DKG) Zertifiziertes Endometriosezentrum AGAPLESION Markus Krankenhaus
Frankfurt am Main
„Gemeinsamverstehen“Pa0en0nnentagdesinterdisziplinärenBrustundGenitalkrebszentrumamAGAPLESIONMarkus-Krankenhaus,10.09.2017
An#hormonelleTherapie2017-verständlicherläutert-
M.Thill
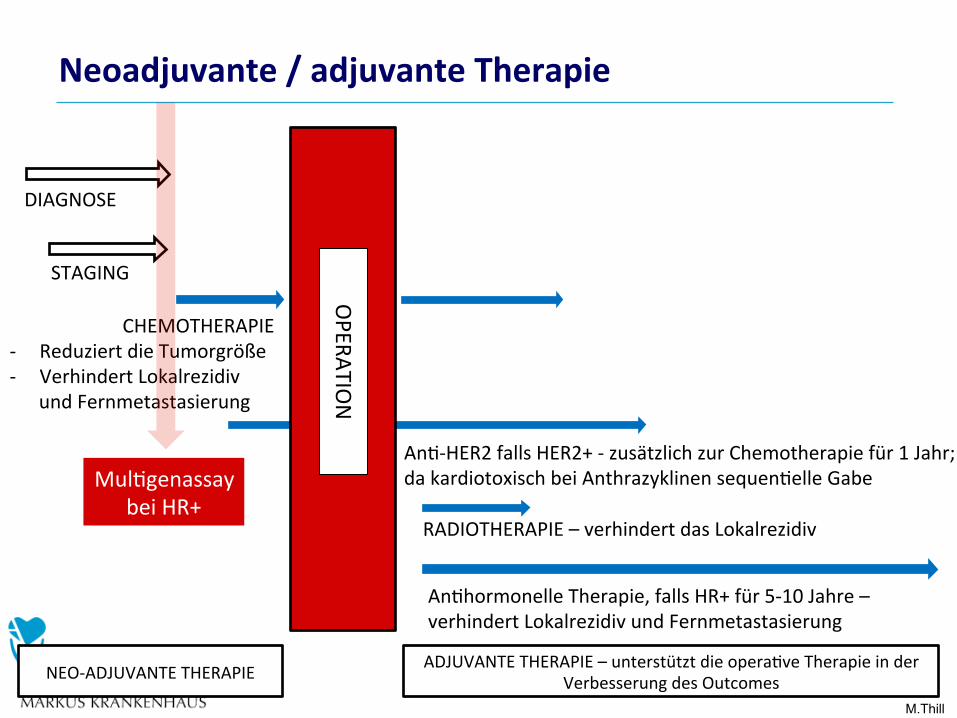
CHEMOTHERAPIE- ReduziertdieTumorgröße- VerhindertLokalrezidiv
undFernmetastasierung
ADJUVANTETHERAPIE–unterstütztdieopera0veTherapieinderVerbesserungdesOutcomes
DIAGNOSE
STAGING
NEO-ADJUVANTETHERAPIE
OPERATIO
N
RADIOTHERAPIE–verhindertdasLokalrezidiv
An0hormonelleTherapie,fallsHR+für5-10Jahre–verhindertLokalrezidivundFernmetastasierung
An0-HER2fallsHER2+-zusätzlichzurChemotherapiefür1Jahr;dakardiotoxischbeiAnthrazyklinensequen0elleGabeMul0genassay
beiHR+
Neoadjuvante/adjuvanteTherapie
M.Thill
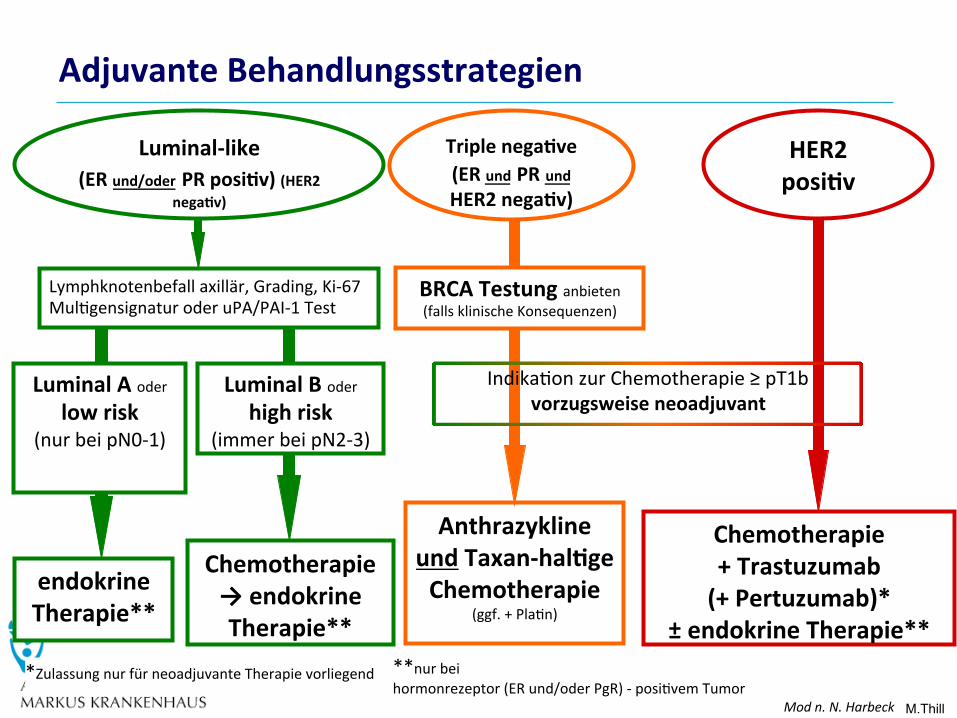
AdjuvanteBehandlungsstrategien
HER2posi#v
Chemotherapie+Trastuzumab(+Pertuzumab)*
±endokrineTherapie**
AnthrazyklineundTaxan-hal#geChemotherapie
(ggf.+Pla0n)
Triplenega#ve(ERundPRundHER2nega#v)
LuminalAoderlowrisk
(nurbeipN0-1)
LuminalBoderhighrisk
(immerbeipN2-3)
Lymphknotenbefallaxillär,Grading,Ki-67Mul0gensignaturoderuPA/PAI-1Test
endokrineTherapie**
Chemotherapie→endokrineTherapie**
Luminal-like(ERund/oderPRposi#v)(HER2
nega#v)
Indika0onzurChemotherapie≥pT1bvorzugsweiseneoadjuvant
BRCATestunganbieten(fallsklinischeKonsequenzen)
*ZulassungnurfürneoadjuvanteTherapievorliegend **nurbeihormonrezeptor(ERund/oderPgR)-posi0vemTumor
Modn.N.Harbeck
M.Thill
An#hormonelleTherapie
• Bes0mmteBruslumorzellenbenö0genzumWachsenweiblicheHormone,dieüberspezielle„Andockstellen“(sog.Rezeptoren)wirken.
• BlockiertmandieseRezeptorenoderdieHormonproduk0on,könnendieKrebszellennichtmehrwachsen.
• WelcheMedikamenteeingesetztwerden,hängtdavonab,obsichdiePa0en0nvorodernachdenWechseljahrenbefindet.
• Diean0hormonelleTherapiewirdsowohlimfrühenalsauchimfortgeschrilenenStadiumeingesetzt,entwederalssogenannteMonotherapieoderinKombina0onmitanderenTherapien(wiez.B.mitderChemotherapieoderderAn0körpertherapie)
M.Thill
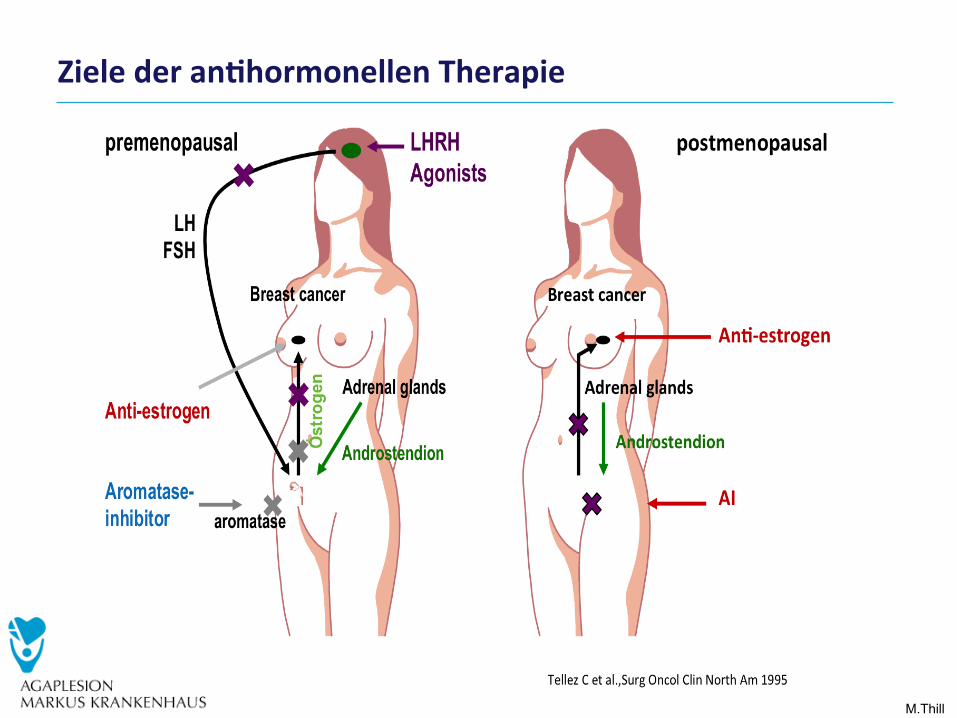
Zielederan#hormonellenTherapie
M.Thill
An#hormonelleTherapie=endokrineTherapie
Befund
Mein Befund:
Hormonrezeptorstatus (ER/PR)
Hormonrezeptorpositiver Brustkrebs?
Ja
Nein
Hormonrezeptorstatus (ER/PR)
Zellen stehen in ständigem Austausch mit ihrer Um-
gebung, denn sie sind Teil eines großen Ganzen,
eines Organismus. Wie in einer Gesellschaft z. B.
einzelnen Menschen unterschiedliche Aufgaben zu-
kommen, übernehmen in einem Organismus einzel-
nen Zelltypen ebenfalls unterschiedliche Aufgaben.
Damit Zellen mit anderen Zellen in Kontakt stehen
können, tragen sie Rezeptoren (Eiweißmoleküle),
an die z. B. Hormone oder Wachstumsfaktoren
„andocken” können.
Der Östrogenrezeptor (ER) oder der Progesteron-
rezeptor (PR) sind solche Eiweiße, an die diese
beiden weiblichen Geschlechtshormone (Östrogen
und Progesteron) binden können.
Brustzellen besitzen diese Rezeptoren, denn der
Brust kommen im Lebenszyklus einer Frau unter-
schiedliche Aufgaben zu, die durch diese beiden
Hormone gesteuert werden.
hormonrezeptornegativen Brustkrebs erkrankt sind,
SUR¿WLHUHQ�6LH�QLFKW�YRQ�HLQHU�VROFKHQ�7KHUDSLH�
Kreuzen Sie hier an, ob Sie an einem hormon-
rezeptorpositiven Brustkrebs erkrankt sind und
wenn ja, tragen Sie ein, an welchem.
Erkrankt eine Frau an Brustkrebs, kann es sein,
dass diese Rezeptoren auf den Brustkrebszellen
entweder im Übermaß oder aber überhaupt nicht
mehr vorhanden sind. Man spricht von hormon-
rezeptorpositivem oder hormonrezeptornegativem
Brustkrebs. Die Bestimmung des Hormonrezeptor-
status kann auf zwei unterschiedliche Weisen
erfolgen. In einem Fall wird er in Prozenten, im
anderen Fall mit Zahlen von 1-12 ausgedrückt.
Halten Sie hierzu Rücksprache mit Ihrem Arzt, um
seine Einschätzung zu Ihrem persönlichen Rezep-
torstatus zu erhalten
Wenn Sie an einem hormonrezeptorpositiven
Brustkrebs erkrankt sind, können Sie von einer Anti-
+RUPRQWKHUDSLH�SUR¿WLHUHQ��:HQQ�6LH�DQ�HLQHP�
20 21
M.Thill
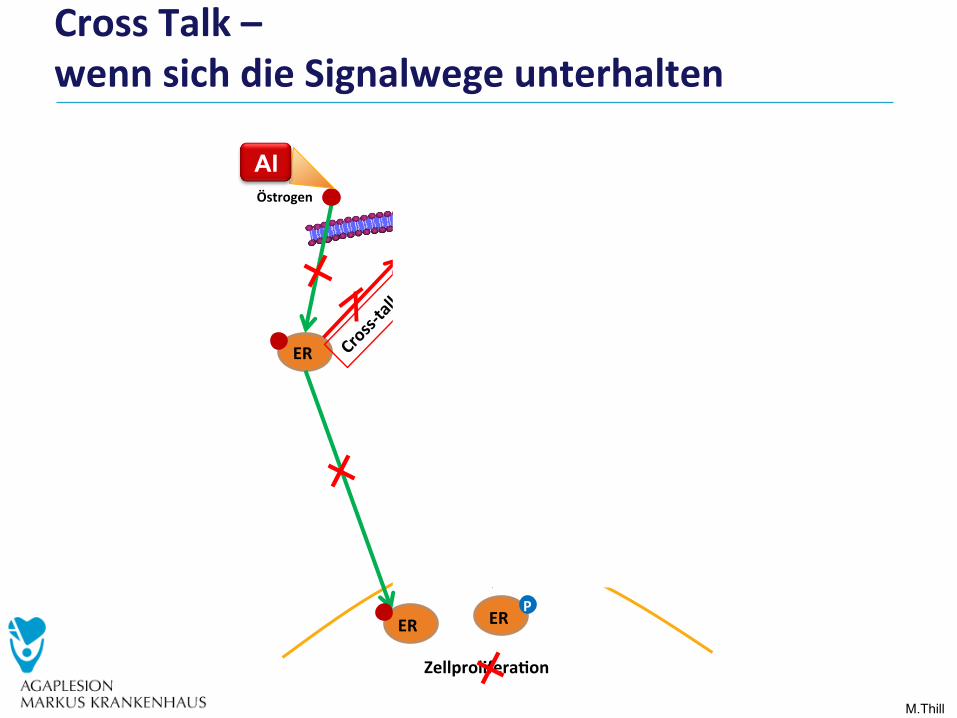
CrossTalk–wennsichdieSignalwegeunterhalten
mTOR
Akt
PI3K
Wachstumsfaktoren:IGF-1R,VEGFR,ÊGFR,HER-2
ER
ER
ER
Östrogen
P
P
P
Zellprolifera#on
AI
Everolimus
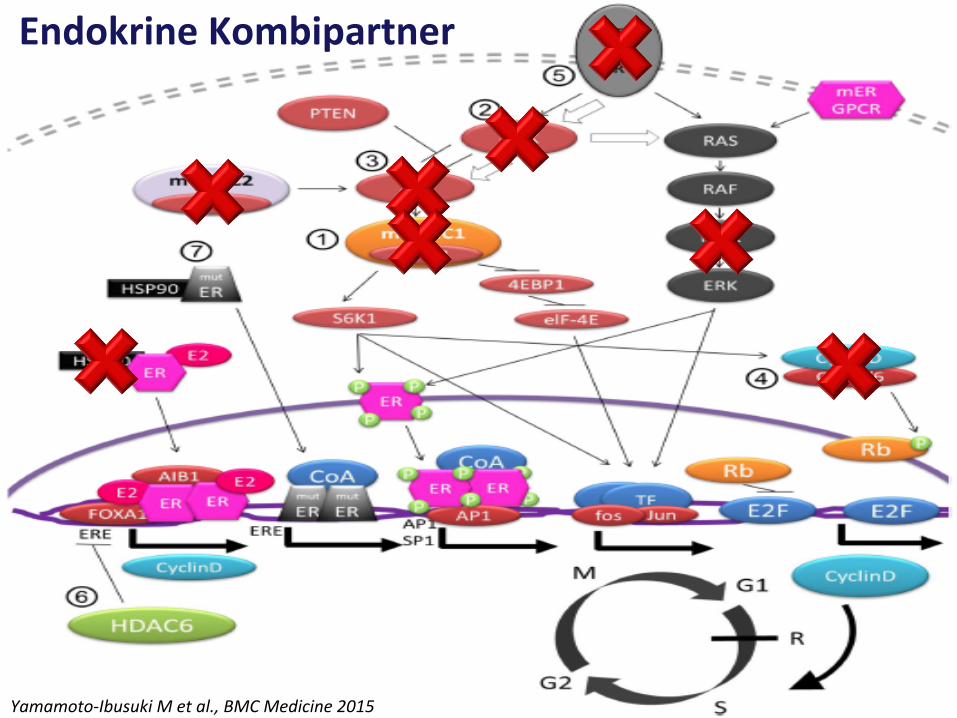
M.Thill Yamamoto-IbusukiMetal.,BMCMedicine2015
EndokrineKombipartner
M.Thill
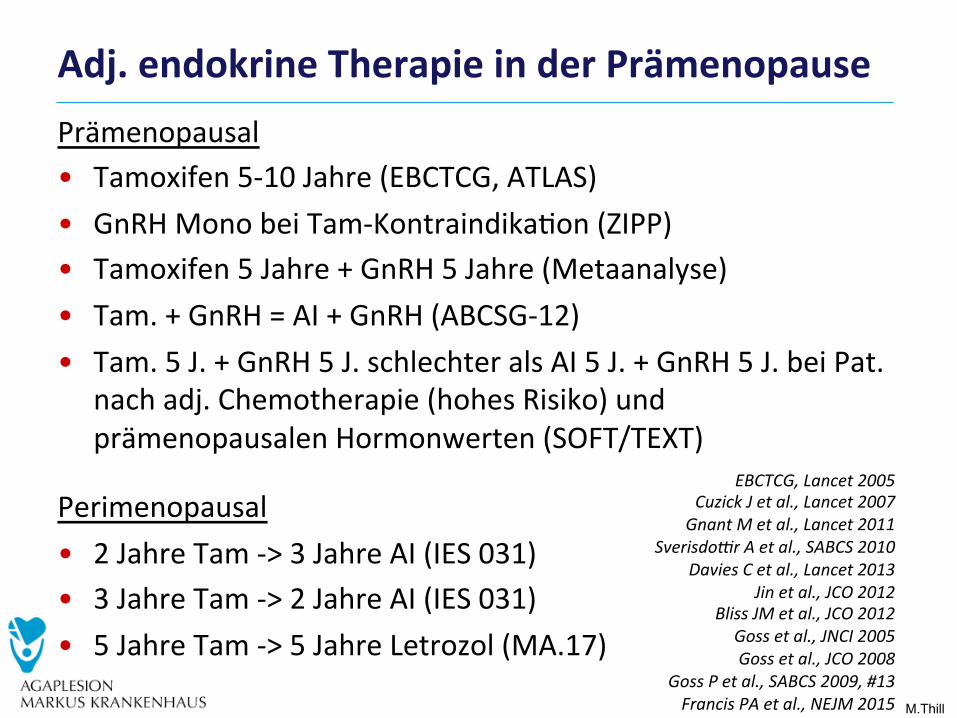
Prämenopausal• Tamoxifen5-10Jahre(EBCTCG,ATLAS)• GnRHMonobeiTam-Kontraindika0on(ZIPP)• Tamoxifen5Jahre+GnRH5Jahre(Metaanalyse)• Tam.+GnRH=AI+GnRH(ABCSG-12)• Tam.5J.+GnRH5J.schlechteralsAI5J.+GnRH5J.beiPat.
nachadj.Chemotherapie(hohesRisiko)undprämenopausalenHormonwerten(SOFT/TEXT)
Perimenopausal• 2JahreTam->3JahreAI(IES031)• 3JahreTam->2JahreAI(IES031)• 5JahreTam->5JahreLetrozol(MA.17)
Adj.endokrineTherapieinderPrämenopause
EBCTCG,Lancet2005CuzickJetal.,Lancet2007
GnantMetal.,Lancet2011SverisdoHrAetal.,SABCS2010
DaviesCetal.,Lancet2013Jinetal.,JCO2012
BlissJMetal.,JCO2012Gossetal.,JNCI2005Gossetal.,JCO2008
GossPetal.,SABCS2009,#13FrancisPAetal.,NEJM2015
M.Thill
PaganiOetal.,oralpresentaTonASCO2014PaganiOetal.,NEJM2015FrancisPAetal.,NEJM2015
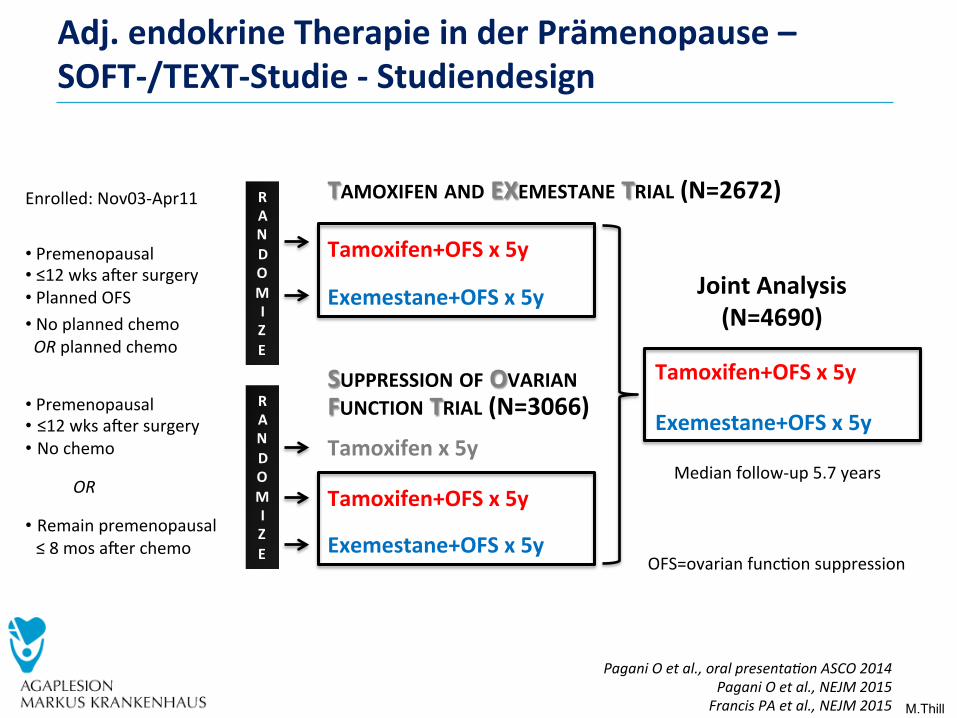
Adj.endokrineTherapieinderPrämenopause–SOFT-/TEXT-Studie-Studiendesign
RANDOMIZE
Tamoxifen+OFSx5y
Exemestane+OFSx5y
RANDOMIZE
Tamoxifenx5yTamoxifen+OFSx5y
Exemestane+OFSx5y
Tamoxifen+OFSx5yExemestane+OFSx5y
JointAnalysis(N=4690)
• Premenopausal• ≤12wksatersurgery• Nochemo
OR
• Remainpremenopausal≤8mosaterchemo
• Premenopausal• ≤12wksatersurgery• PlannedOFS• NoplannedchemoORplannedchemo
SUPPRESSIONOFOVARIANFUNCTIONTRIAL(N=3066)
TAMOXIFENANDEXEMESTANETRIAL(N=2672)
OFS=ovarianfunc0onsuppression
Enrolled:Nov03-Apr11
Medianfollow-up5.7years
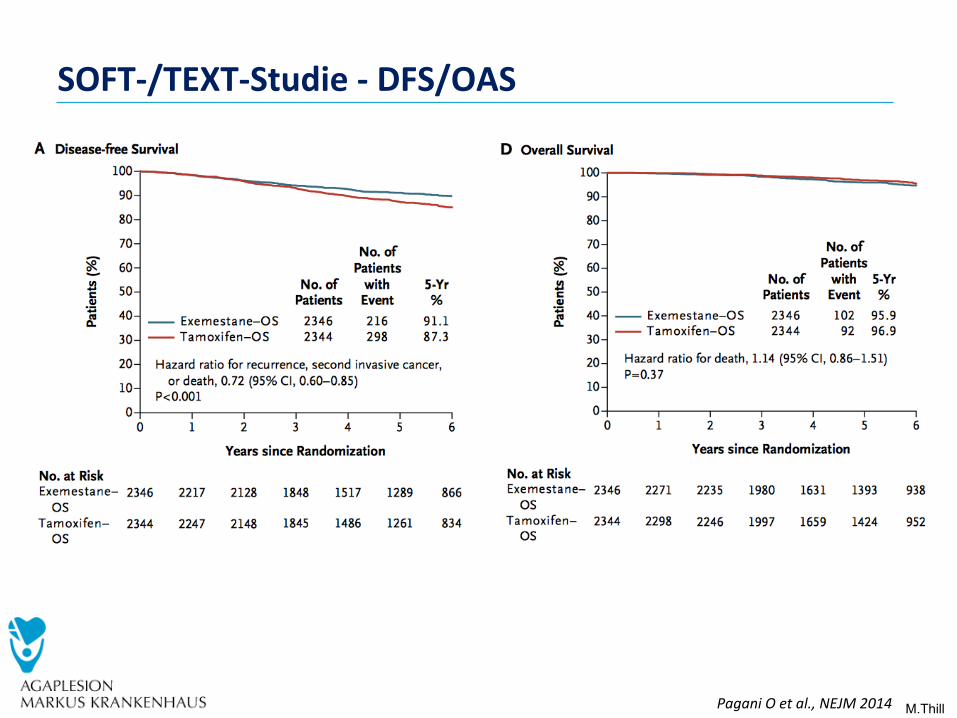
M.Thill PaganiOetal.,NEJM2014
SOFT-/TEXT-Studie-DFS/OAS
M.Thill
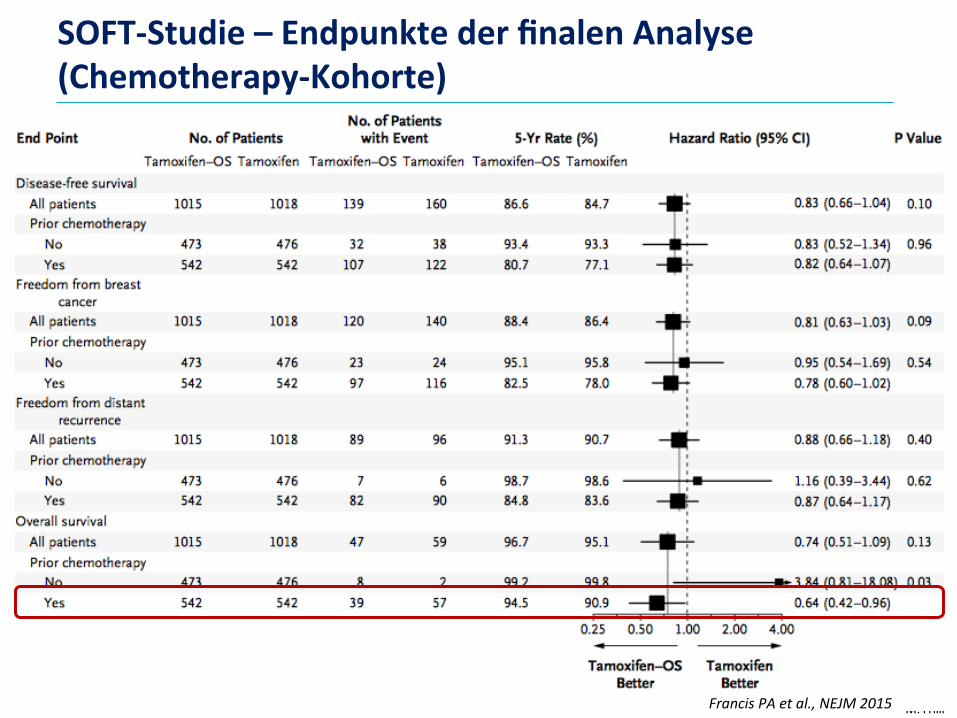
SOFT-Studie–EndpunktederfinalenAnalyse(Chemotherapy-Kohorte)
FrancisPAetal.,NEJM2015
M.Thill
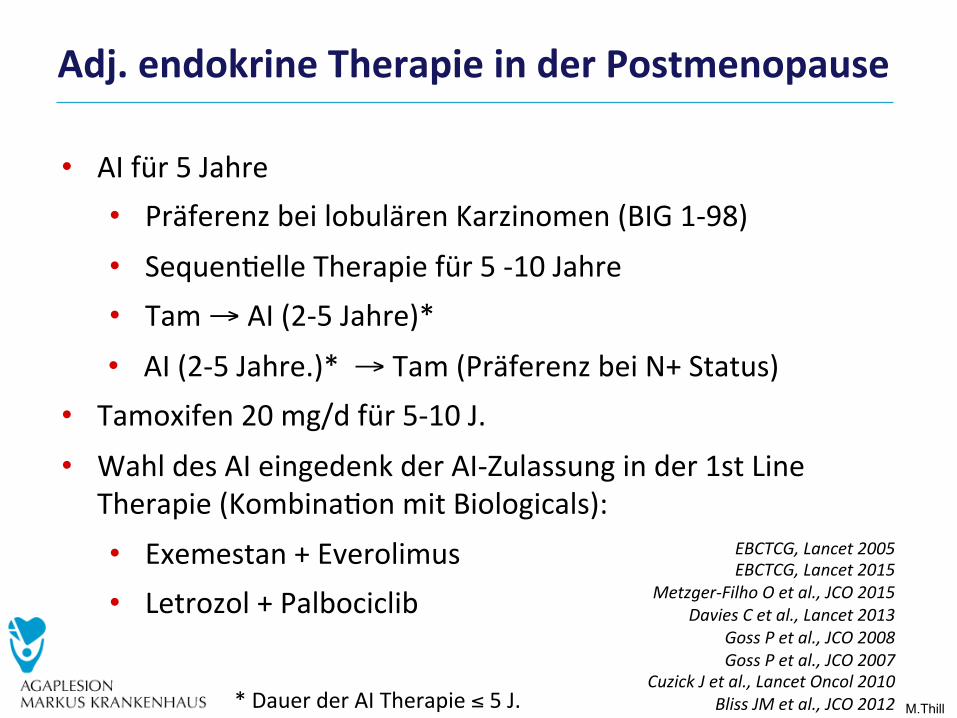
Adj.endokrineTherapieinderPostmenopause
EBCTCG,Lancet2005EBCTCG,Lancet2015
Metzger-FilhoOetal.,JCO2015DaviesCetal.,Lancet2013
GossPetal.,JCO2008GossPetal.,JCO2007
CuzickJetal.,LancetOncol2010BlissJMetal.,JCO2012
• AIfür5Jahre • PräferenzbeilobulärenKarzinomen(BIG1-98)
• Sequen0elleTherapiefür5-10Jahre • Tam→AI(2-5Jahre)*
• AI(2-5Jahre.)*→Tam(PräferenzbeiN+Status) • Tamoxifen20mg/dfür5-10J.
• WahldesAIeingedenkderAI-Zulassunginder1stLineTherapie(Kombina0onmitBiologicals):• Exemestan+Everolimus• Letrozol+Palbociclib
*DauerderAITherapie≤5J.
M.Thill
5 Jahre
5 Jahre
2 Jahre
2 Jahre
5 Jahre
5 Jahre
3 Jahre
3 Jahre
2-3 Jahre
2-3 Jahre 2-3 Jahre
3 Jahre
3 Jahre 2 Jahre
3 Jahre
5 Jahre
2 Jahre
5Jahre
5 Jahre 5 Jahre
5 Jahre 5 Jahre
5Jahre
5 Jahre Bis 5 Jahre
5 Jahre
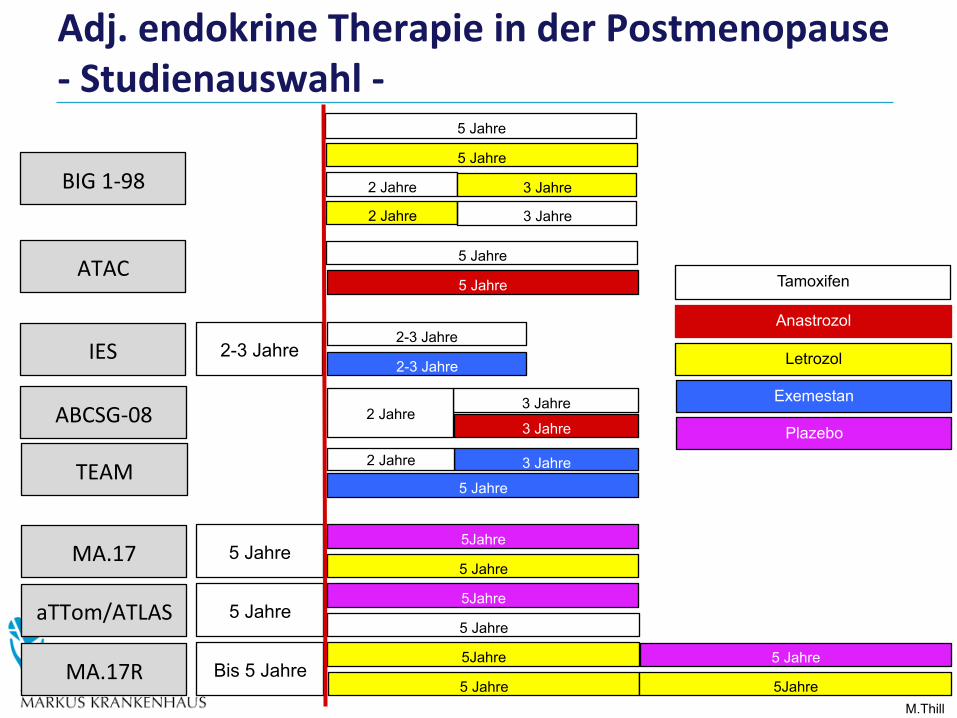
Tamoxifen
Anastrozol
Letrozol
Exemestan
Plazebo
BIG1-98
ATAC
IES
ABCSG-08
TEAM
MA.17R
aTTom/ATLAS
MA.17
5Jahre
5Jahre
Adj.endokrineTherapieinderPostmenopause-Studienauswahl-

M.Thill
0 5 10 15 200
15
30
45
%, CI
Dis
tan
t re
curr
ence
years
14% T1N0 (score=1)
22% T1N1-3 or T2N0
29% T2N1-3
41% T1N4-9
47% T2N4-9 (score=6)
PanHetal.EBCTCG,ASCO2016,#505
Rezidivrisikonach5-jährigerendokrinerTherapieadjus#ertanTumorgrößeundNodalstatus
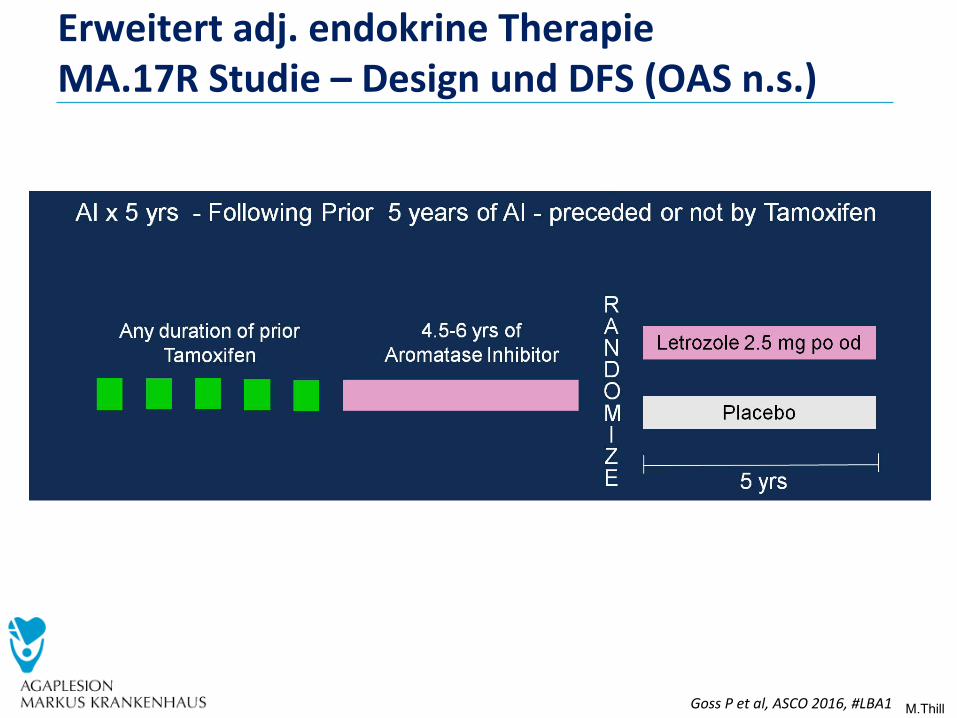
M.Thill GossPetal,ASCO2016,#LBA1
Erweitertadj.endokrineTherapieMA.17RStudie–DesignundDFS(OASn.s.)
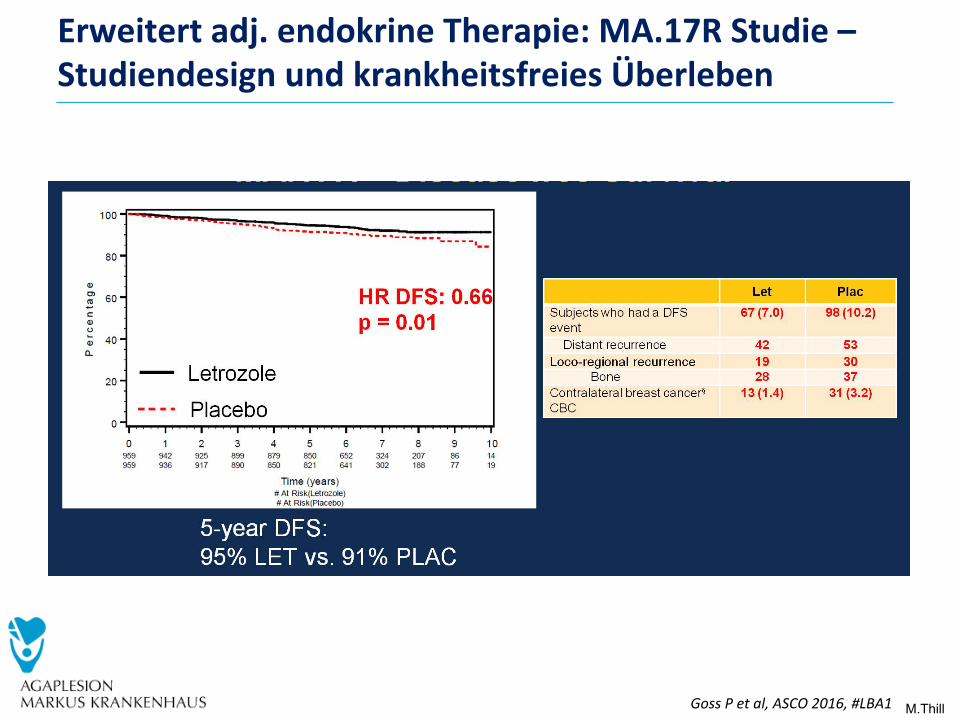
M.Thill GossPetal,ASCO2016,#LBA1
Erweitertadj.endokrineTherapie:MA.17RStudie–StudiendesignundkrankheitsfreiesÜberleben
M.Thill
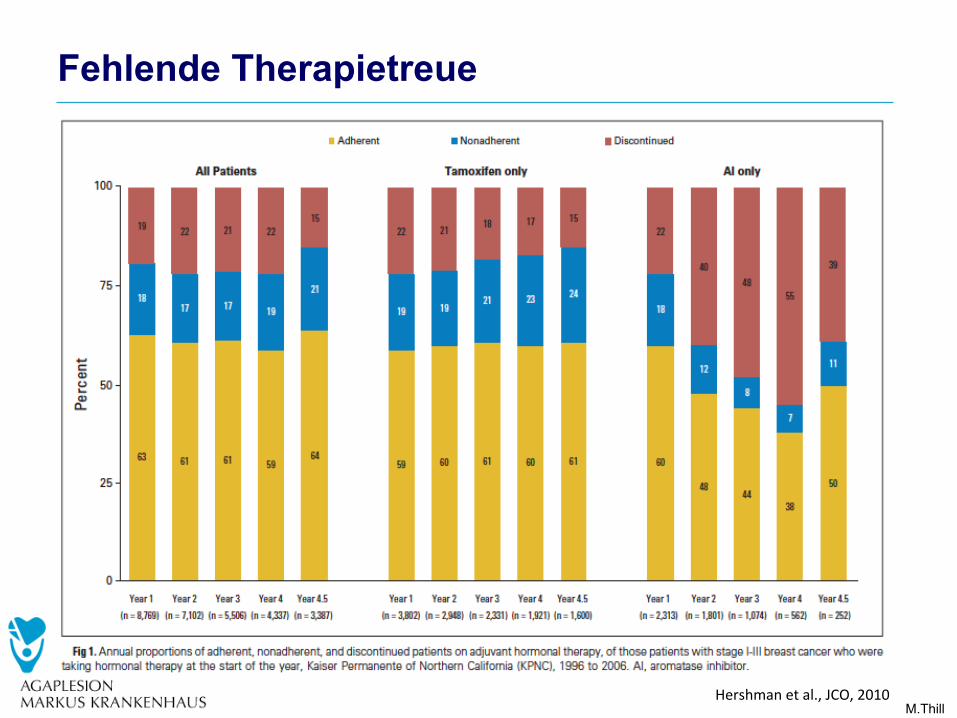
Fehlende Therapietreue
Hershmanetal.,JCO,2010
M.Thill
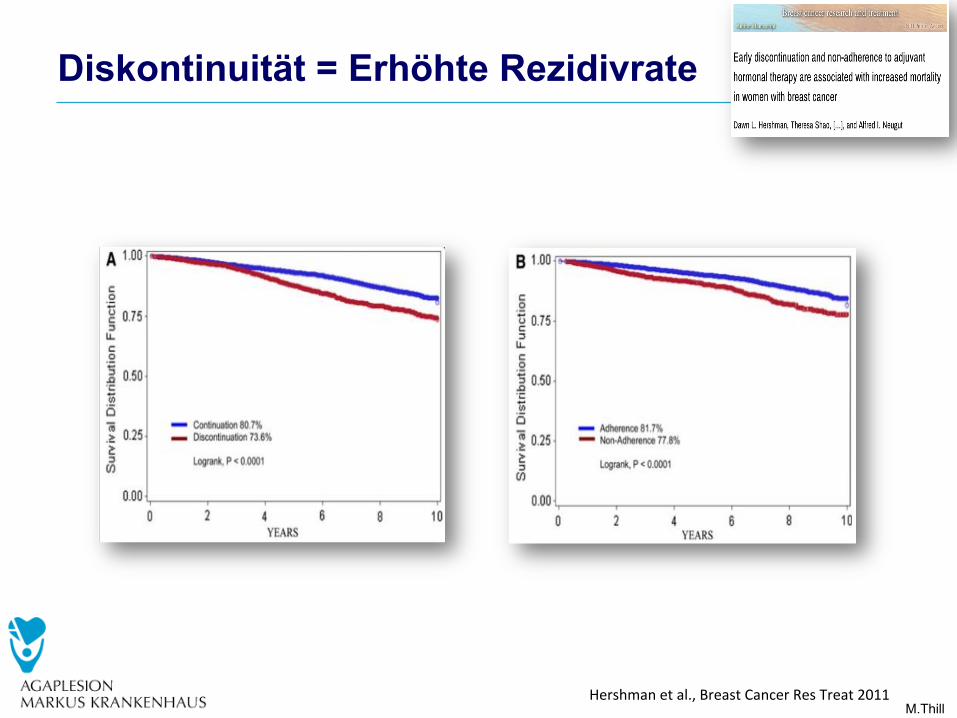
Diskontinuität = Erhöhte Rezidivrate
Hershmanetal.,BreastCancerResTreat2011
M.Thill
GynäkologischeProbleme

M.Thill
VaginaleAtrophie–Östradiol0,03mg
BuchholzSetal.,Climacteric2015
M.Thill
lower (maximum 43.70 pg/ml) and occurred later (at6–8 h) after 4 weeks (visit C2, day 28) and at this visit half
of the subjects did not have at all any quantifiable con-
centrations of E3 (Table 1). The Cmax (Table 2) was sig-nificantly lower at visit C2 compared to visit E
(p \ 0.0001).
E3 levels (Table 3; Fig. 3) were below the LLOQ forall, except two subjects. One had a E3 serum concentration
of 22.3 pg/ml at C1, and one had E3 levels of 49.2 pg/ml
and 14.5 pg/ml at C1 and C2, respectively. The troughconcentrations for E2 and E1 were always below LLOQ.
There were no statistically significant changes of LH
and SHBG serum concentrations during treatment. Atvisit C2, FSH showed a scant, but significant decrease of
serum concentration compared to E (p = 0.025), but no
significant differences were observed at visits C1, C3, andC4.
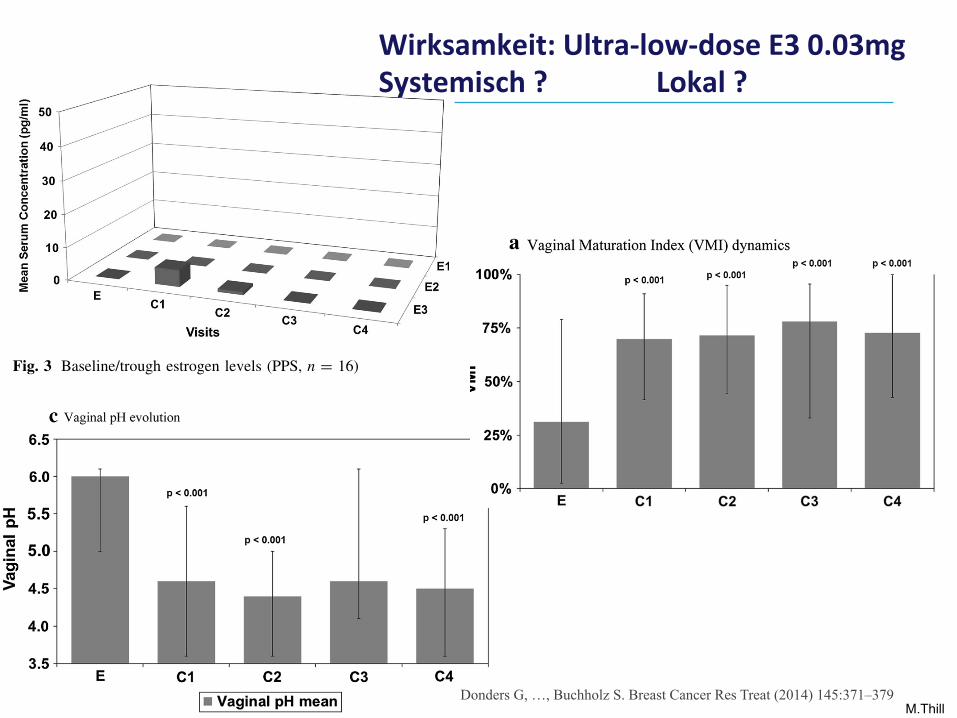
VMI improved rapidly already after 2 weeks of treat-ment from 31 % at entry to 70 % at visit C1 (p \ 0.0001)
and to 72 % at the end of initial therapy, and was main-
tained until the end of maintenance therapy at 73 %(Fig. 4, panel a).
Maximum E3 levels inversely correlated with VMI
values at visit E and visit C2 (R2 = 0.62, Fig. 5), demon-strating that the maturing epithelium rapidly precludes
further E3 absorption after the initial therapy.
Another important efficacy variable was LBG. At thestudy entry, the majority of subjects had grossly abnormal
vaginal flora (LBG III, 81 %), the remainder being LBG
IIb (moderately disturbed). After the 28 days of therapy,almost complete normalisation of the vaginal flora was
observed (Fig. 4, panel b): it had become only slightly
disturbed (LBGIIa, 63 %) or normal (LBGI, 25 %). Furthersignificant improvements were observed during the main-
tenance therapy: at C4, the majority of women had a stable
and normal vaginal flora (LBGI, 69 %; p = 0.039).Vaginal pH showed statistically significant decrease
(Fig. 4, panel c) from entry (mean 6.0) to visits C1, C2, and
C4 (mean 4.4–4.6; p \ 0.001), and remained unchanged
thereafter during maintenance therapy.Clinical symptoms of vaginal atrophy like dryness,
soreness, and dyspareunia all improved during treatment.
Dryness and soreness improved dramatically from entry tocontrol visits (p \ 0.001), while statistical evaluation of
the improvement in dyspareunia was hampered by low
numbers. At entry, sexual intercourse was reported only by19 % of women, whereas 31 % reported intercourse at visit
C4 (p [ 0.05). The experience of vaginal dischargeincreased significantly from entry to C2 (p \ 0.01), and
then decreased to the end of treatment. Vaginal paleness
Fig. 3 Baseline/trough estrogen levels (PPS, n = 16)
Fig. 4 Vaginal characteristics during the entry and follow-up phasesof the study
376 Breast Cancer Res Treat (2014) 145:371–379
123
lower (maximum 43.70 pg/ml) and occurred later (at6–8 h) after 4 weeks (visit C2, day 28) and at this visit half
of the subjects did not have at all any quantifiable con-
centrations of E3 (Table 1). The Cmax (Table 2) was sig-nificantly lower at visit C2 compared to visit E
(p \ 0.0001).
E3 levels (Table 3; Fig. 3) were below the LLOQ forall, except two subjects. One had a E3 serum concentration
of 22.3 pg/ml at C1, and one had E3 levels of 49.2 pg/ml
and 14.5 pg/ml at C1 and C2, respectively. The troughconcentrations for E2 and E1 were always below LLOQ.
There were no statistically significant changes of LH
and SHBG serum concentrations during treatment. Atvisit C2, FSH showed a scant, but significant decrease of
serum concentration compared to E (p = 0.025), but no
significant differences were observed at visits C1, C3, andC4.
VMI improved rapidly already after 2 weeks of treat-ment from 31 % at entry to 70 % at visit C1 (p \ 0.0001)
and to 72 % at the end of initial therapy, and was main-
tained until the end of maintenance therapy at 73 %(Fig. 4, panel a).
Maximum E3 levels inversely correlated with VMI
values at visit E and visit C2 (R2 = 0.62, Fig. 5), demon-strating that the maturing epithelium rapidly precludes
further E3 absorption after the initial therapy.
Another important efficacy variable was LBG. At thestudy entry, the majority of subjects had grossly abnormal
vaginal flora (LBG III, 81 %), the remainder being LBG
IIb (moderately disturbed). After the 28 days of therapy,almost complete normalisation of the vaginal flora was
observed (Fig. 4, panel b): it had become only slightly
disturbed (LBGIIa, 63 %) or normal (LBGI, 25 %). Furthersignificant improvements were observed during the main-
tenance therapy: at C4, the majority of women had a stable
and normal vaginal flora (LBGI, 69 %; p = 0.039).Vaginal pH showed statistically significant decrease
(Fig. 4, panel c) from entry (mean 6.0) to visits C1, C2, and
C4 (mean 4.4–4.6; p \ 0.001), and remained unchanged
thereafter during maintenance therapy.Clinical symptoms of vaginal atrophy like dryness,
soreness, and dyspareunia all improved during treatment.
Dryness and soreness improved dramatically from entry tocontrol visits (p \ 0.001), while statistical evaluation of
the improvement in dyspareunia was hampered by low
numbers. At entry, sexual intercourse was reported only by19 % of women, whereas 31 % reported intercourse at visit
C4 (p [ 0.05). The experience of vaginal dischargeincreased significantly from entry to C2 (p \ 0.01), and
then decreased to the end of treatment. Vaginal paleness
Fig. 3 Baseline/trough estrogen levels (PPS, n = 16)
Fig. 4 Vaginal characteristics during the entry and follow-up phasesof the study
376 Breast Cancer Res Treat (2014) 145:371–379
123
lower (maximum 43.70 pg/ml) and occurred later (at6–8 h) after 4 weeks (visit C2, day 28) and at this visit half
of the subjects did not have at all any quantifiable con-
centrations of E3 (Table 1). The Cmax (Table 2) was sig-nificantly lower at visit C2 compared to visit E
(p \ 0.0001).
E3 levels (Table 3; Fig. 3) were below the LLOQ forall, except two subjects. One had a E3 serum concentration
of 22.3 pg/ml at C1, and one had E3 levels of 49.2 pg/ml
and 14.5 pg/ml at C1 and C2, respectively. The troughconcentrations for E2 and E1 were always below LLOQ.
There were no statistically significant changes of LH
and SHBG serum concentrations during treatment. Atvisit C2, FSH showed a scant, but significant decrease of
serum concentration compared to E (p = 0.025), but no
significant differences were observed at visits C1, C3, andC4.
VMI improved rapidly already after 2 weeks of treat-ment from 31 % at entry to 70 % at visit C1 (p \ 0.0001)
and to 72 % at the end of initial therapy, and was main-
tained until the end of maintenance therapy at 73 %(Fig. 4, panel a).
Maximum E3 levels inversely correlated with VMI
values at visit E and visit C2 (R2 = 0.62, Fig. 5), demon-strating that the maturing epithelium rapidly precludes
further E3 absorption after the initial therapy.
Another important efficacy variable was LBG. At thestudy entry, the majority of subjects had grossly abnormal
vaginal flora (LBG III, 81 %), the remainder being LBG
IIb (moderately disturbed). After the 28 days of therapy,almost complete normalisation of the vaginal flora was
observed (Fig. 4, panel b): it had become only slightly
disturbed (LBGIIa, 63 %) or normal (LBGI, 25 %). Furthersignificant improvements were observed during the main-
tenance therapy: at C4, the majority of women had a stable
and normal vaginal flora (LBGI, 69 %; p = 0.039).Vaginal pH showed statistically significant decrease
(Fig. 4, panel c) from entry (mean 6.0) to visits C1, C2, and
C4 (mean 4.4–4.6; p \ 0.001), and remained unchanged
thereafter during maintenance therapy.Clinical symptoms of vaginal atrophy like dryness,
soreness, and dyspareunia all improved during treatment.
Dryness and soreness improved dramatically from entry tocontrol visits (p \ 0.001), while statistical evaluation of
the improvement in dyspareunia was hampered by low
numbers. At entry, sexual intercourse was reported only by19 % of women, whereas 31 % reported intercourse at visit
C4 (p [ 0.05). The experience of vaginal dischargeincreased significantly from entry to C2 (p \ 0.01), and
then decreased to the end of treatment. Vaginal paleness
Fig. 3 Baseline/trough estrogen levels (PPS, n = 16)
Fig. 4 Vaginal characteristics during the entry and follow-up phasesof the study
376 Breast Cancer Res Treat (2014) 145:371–379
123
Wirksamkeit:Ultra-low-doseE30.03mgSystemisch?Lokal?
Donders G, …, Buchholz S. Breast Cancer Res Treat (2014) 145:371–379
M.Thill
EndokrineTherapiebeendigungwegenLebensqualitätsverlustbeivaginalerAtrophie15-20%-keingesteigertesKrebsrisiko
The Use of Vaginal Estrogen in Women With a History of Estrogen-Dependent Breast CancerABSTRACT: Cancer treatment should address female-specific survivorship issues, including the hypoes-trogenic-related adverse effects of cancer therapies or of natural menopause in survivors. Systemic and vaginal estrogen are widely used for symptomatic relief of vasomotor symptoms, sexual dysfunction, and lower urinary tract infections in the general population. However, given that some types of cancer are hormone sensitive, there are safety concerns about the use of local hormone therapy in women who currently have breast cancer or have a history of breast cancer. Nonhormonal approaches are the first-line choices for managing urogenital symptoms or atrophy-related urinary symptoms experienced by women during or after treatment for breast cancer. Among women with a history of estrogen-dependent breast cancer who are experiencing urogenital symptoms, vaginal estrogen should be reserved for those patients who are unresponsive to nonhormonal remedies. The decision to use vaginal estrogen may be made in coordination with a woman’s oncologist. Additionally, it should be preceded by an informed decision-making and consent process in which the woman has the information and resources to consider the benefits and potential risks of low-dose vaginal estrogen. Data do not show an increased risk of can-cer recurrence among women currently undergoing treatment for breast cancer or those with a personal history of breast cancer who use vaginal estrogen to relieve urogenital symptoms.
Recommendations and ConclusionsThe American College of Obstetricians and Gynecologists makes the following recommendations and conclusions:
• Nonhormonal approaches are the first-line choices for managing urogenital symptoms or atrophy-related urinary symptoms experienced by women during or after treatment for breast cancer.
• Among women with a history of estrogen-dependent breast cancer who are experiencing urogenital symp-toms, vaginal estrogen should be reserved for those patients who are unresponsive to nonhormonal remedies.
• The decision to use vaginal estrogen may be made in coordination with a woman’s oncologist. Additionally, it should be preceded by an informed decision-making and consent process in which the woman has the information and resources to con-
sider the benefits and potential risks of low-dose vaginal estrogen.
• Data do not show an increased risk of cancer recur-rence among women currently undergoing treat-ment for breast cancer or those with a personal history of breast cancer who use vaginal estrogen to relieve urogenital symptoms.
Background Oncologic care providers are increasingly recognizing that cancer treatment should address female-specific survivorship issues, including the hypoestrogenic-related adverse effects of cancer therapies or of natural meno-pause in survivors. Obstetrician–gynecologists and other health care providers frequently face the challenge of understanding and addressing these issues among an increasing cohort of women cancer survivors who experi-ence urogenital symptoms, either from cancer therapy or
COMMITTEE OPINIONNumber 659 • March 2016
Committee on Gynecologic PracticeThis Committee Opinion was developed by the American College of Obstetricians and Gynecologists’ Committee on Gynecologic Practice. Member contributors included Ruth Farrell, MD. This document reflects emerging clinical and scientific advances as of the date issued and is subject to change. The information should not be construed as dictating an exclusive course of treatment or procedure to be followed.
The American College of Obstetricians and GynecologistsWOMEN’S HEALTH CARE PHYSICIANS
The Use of Vaginal Estrogen in Women With a History of Estrogen-Dependent Breast CancerABSTRACT: Cancer treatment should address female-specific survivorship issues, including the hypoes-trogenic-related adverse effects of cancer therapies or of natural menopause in survivors. Systemic and vaginal estrogen are widely used for symptomatic relief of vasomotor symptoms, sexual dysfunction, and lower urinary tract infections in the general population. However, given that some types of cancer are hormone sensitive, there are safety concerns about the use of local hormone therapy in women who currently have breast cancer or have a history of breast cancer. Nonhormonal approaches are the first-line choices for managing urogenital symptoms or atrophy-related urinary symptoms experienced by women during or after treatment for breast cancer. Among women with a history of estrogen-dependent breast cancer who are experiencing urogenital symptoms, vaginal estrogen should be reserved for those patients who are unresponsive to nonhormonal remedies. The decision to use vaginal estrogen may be made in coordination with a woman’s oncologist. Additionally, it should be preceded by an informed decision-making and consent process in which the woman has the information and resources to consider the benefits and potential risks of low-dose vaginal estrogen. Data do not show an increased risk of can-cer recurrence among women currently undergoing treatment for breast cancer or those with a personal history of breast cancer who use vaginal estrogen to relieve urogenital symptoms.
Recommendations and ConclusionsThe American College of Obstetricians and Gynecologists makes the following recommendations and conclusions:
• Nonhormonal approaches are the first-line choices for managing urogenital symptoms or atrophy-related urinary symptoms experienced by women during or after treatment for breast cancer.
• Among women with a history of estrogen-dependent breast cancer who are experiencing urogenital symp-toms, vaginal estrogen should be reserved for those patients who are unresponsive to nonhormonal remedies.
• The decision to use vaginal estrogen may be made in coordination with a woman’s oncologist. Additionally, it should be preceded by an informed decision-making and consent process in which the woman has the information and resources to con-
sider the benefits and potential risks of low-dose vaginal estrogen.
• Data do not show an increased risk of cancer recur-rence among women currently undergoing treat-ment for breast cancer or those with a personal history of breast cancer who use vaginal estrogen to relieve urogenital symptoms.
Background Oncologic care providers are increasingly recognizing that cancer treatment should address female-specific survivorship issues, including the hypoestrogenic-related adverse effects of cancer therapies or of natural meno-pause in survivors. Obstetrician–gynecologists and other health care providers frequently face the challenge of understanding and addressing these issues among an increasing cohort of women cancer survivors who experi-ence urogenital symptoms, either from cancer therapy or
COMMITTEE OPINIONNumber 659 • March 2016
Committee on Gynecologic PracticeThis Committee Opinion was developed by the American College of Obstetricians and Gynecologists’ Committee on Gynecologic Practice. Member contributors included Ruth Farrell, MD. This document reflects emerging clinical and scientific advances as of the date issued and is subject to change. The information should not be construed as dictating an exclusive course of treatment or procedure to be followed.
The American College of Obstetricians and GynecologistsWOMEN’S HEALTH CARE PHYSICIANS
M.Thill
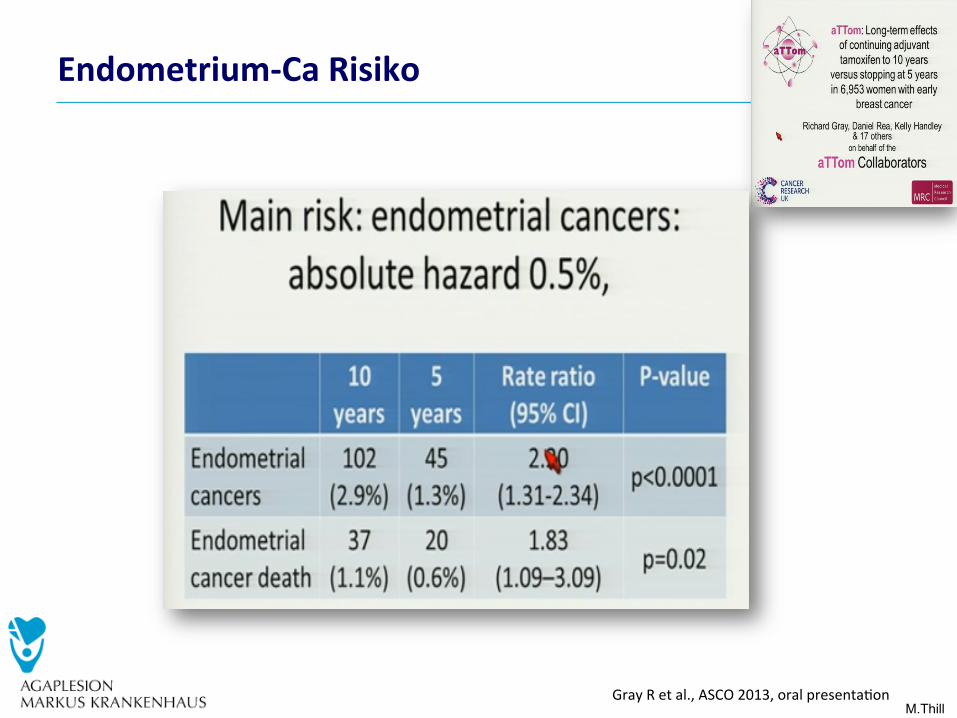
Endometrium-CaRisiko
GrayRetal.,ASCO2013,oralpresenta0on
M.Thill
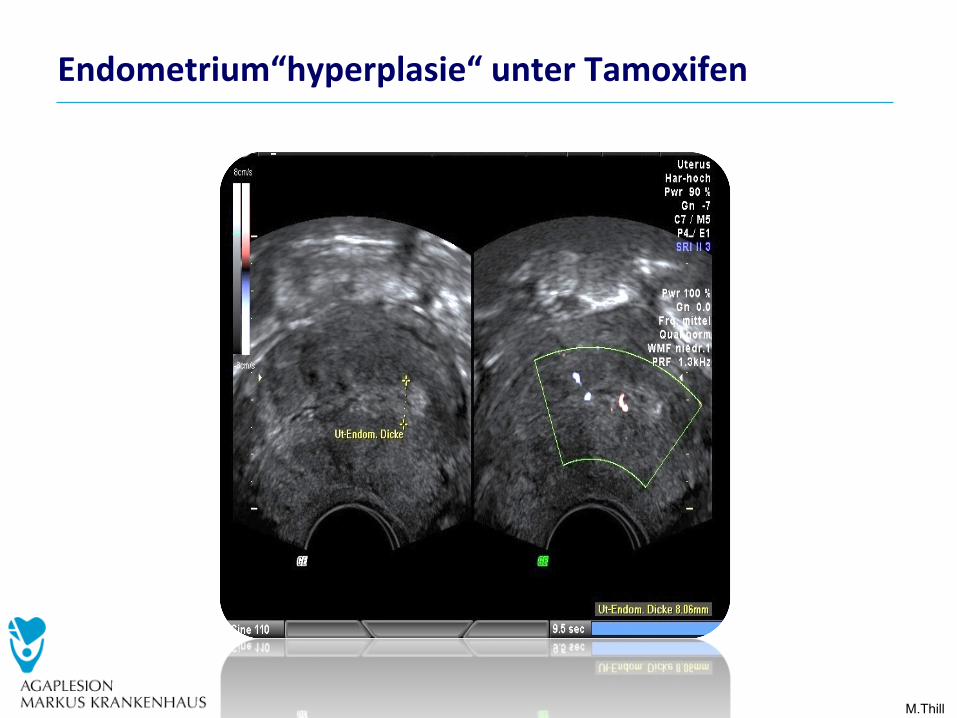
Endometrium“hyperplasie“unterTamoxifen
M.Thill
EndometriumveränderungenunterTamoxifen
• Endometriumhyperplasie?• Meistens
– Gutar0ge(benigne)Polypen– Wassereinlagerung(Ödem)desEndometriums/Myometriums
• Wasistzutun?– FallskeinevaginaleBlutungautril:ABWARTEN– oder:diagnos0scheGebärmulerspiegelung(Hysteroskopie)undAusschabung(frak0onierteAbrasio)
– Keinewiederholtenfrak0oniertenAbrasiones
M.Thill
Hitzewallungen
M.Thill
Akupunkturvs.VenlaflaxinzurBehandlungvasomotorischerSymptomebeiHR+Brustkrebs:EinerandomisiertekontrollierteStudie• N=50• 12WochenAkupunktur(N=25)vs.12WochenVenlafaxin(N=25)• NachdurchgeführterInterven0onsignifikanteVerbesserungder
HitzewallungenunddepressivenVers0mmungeninbeidenGruppen
• ABER:Nach3MonatenLangzeitverbesserungnurinderAkupunktur-Gruppe
• 18vs.0AEs(Venlafaxinvs.Akupunktur)
Walkeretal.,JCO2010
M.Thill
Women With Early-
• N=38• Fragebogen(BriefPainInventory-Shortform(BPI-SF),WOMAC
(Osteoarthri0s-Index),M-SACRAGchronicrheumatoidaffec0onsofthehands
• 12xAkupunkturvs.12xShamAkupunkturen(oberflächlicheNadeleinführung)innerhalbvon6Wochen
• Baseline,3und6Wochen• SignifikanteVerbesserungderGelenkbeschwerdenund
GelenksteifigkeitinderAkupunktur-Gruppe
Walkeretal.,JCO2010
© AGO e. V. in der DGGG e.V. sowie in der DKG e.V. Guidelines Breast Version 2016.1D
www.ago-online.de
Oxford AGO LoE / GR
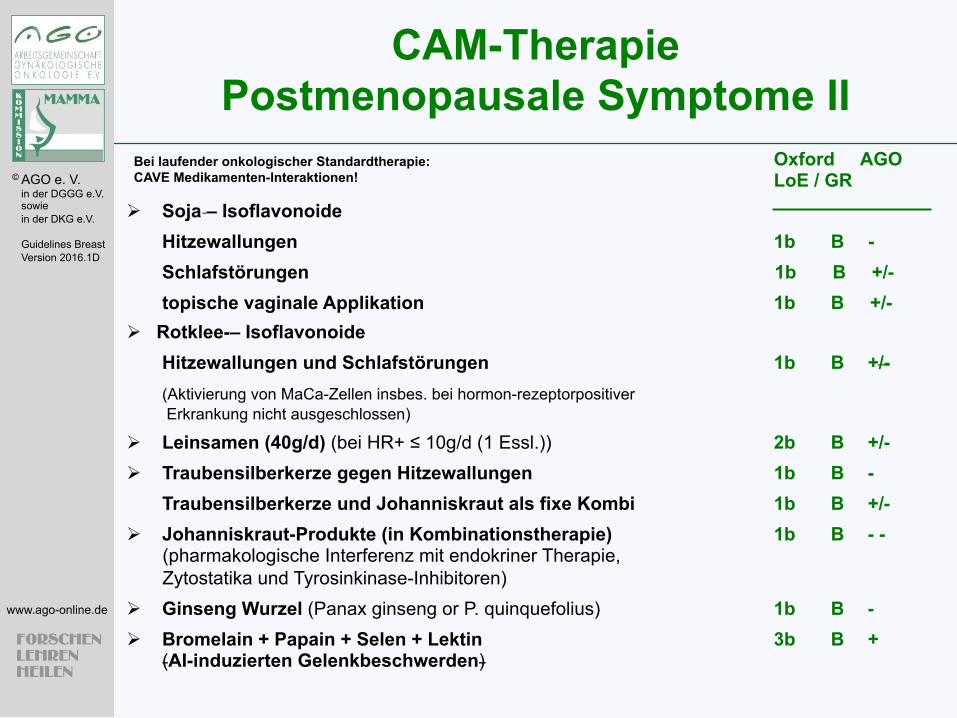
Ø Soja – Isoflavonoide Hitzewallungen 1b B - Schlafstörungen 1b B +/- topische vaginale Applikation 1b B +/-
Ø Rotklee-– Isoflavonoide Hitzewallungen und Schlafstörungen 1b B +/- (Aktivierung von MaCa-Zellen insbes. bei hormon-rezeptorpositiver Erkrankung nicht ausgeschlossen)
Ø Leinsamen (40g/d) (bei HR+ ≤ 10g/d (1 Essl.)) 2b B +/- Ø Traubensilberkerze gegen Hitzewallungen 1b B -
Traubensilberkerze und Johanniskraut als fixe Kombi 1b B +/- Ø Johanniskraut-Produkte (in Kombinationstherapie) 1b B - -
(pharmakologische Interferenz mit endokriner Therapie, Zytostatika und Tyrosinkinase-Inhibitoren)
Ø Ginseng Wurzel (Panax ginseng or P. quinquefolius) 1b B - Ø Bromelain + Papain + Selen + Lektin 3b B +
(AI-induzierten Gelenkbeschwerden)
Bei laufender onkologischer Standardtherapie: CAVE Medikamenten-Interaktionen!
CAM-Therapie Postmenopausale Symptome II
© AGO e. V. in der DGGG e.V. sowie in der DKG e.V. Guidelines Breast Version 2016.1D
www.ago-online.de
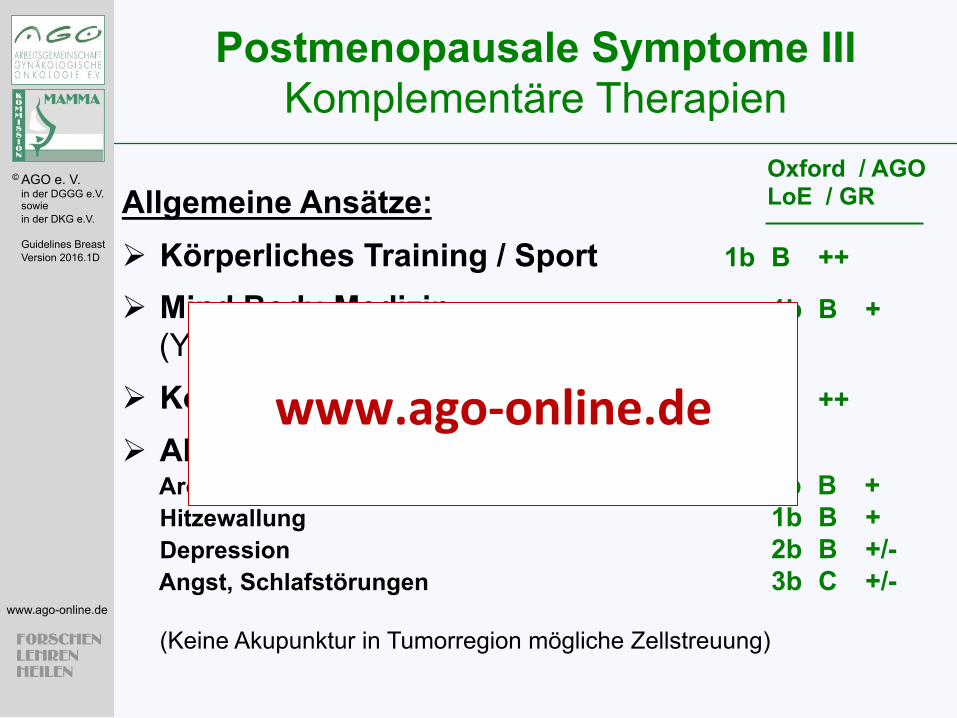
Allgemeine Ansätze: Ø Körperliches Training / Sport 1b B ++ Ø Mind Body-Medizin 1b B +
(Yoga, Hypnose, Schulung, Beratung) Ø Kognitive Verhaltenstherapie 1b B ++
Ø Akupunktur Aromatase-Inhibitor induzierte Arthralgie 2b B + Hitzewallung 1b B + Depression 2b B +/- Angst, Schlafstörungen 3b C +/- (Keine Akupunktur in Tumorregion mögliche Zellstreuung)
Oxford / AGO LoE / GR
Postmenopausale Symptome III Komplementäre Therapien
www.ago-online.de
M.Thill
MuskuloskelevaleProbleme
M.Thill
Arthralgien(Gelenkbeschwerden)-Fakten
• AIassoziierteArthralgie- InklinischenStudien5-35%- AußerhalbklinischerStudien>40%- In2/3mitmoderatembisschweremSchweregrad
• VerbesserungwährendderTherapie• UnterbrechungderTherapiein25-40%• AIassoziierteArthralgieisteinhäufigerGrundfüreinen
Therapiestopp
M.Thill
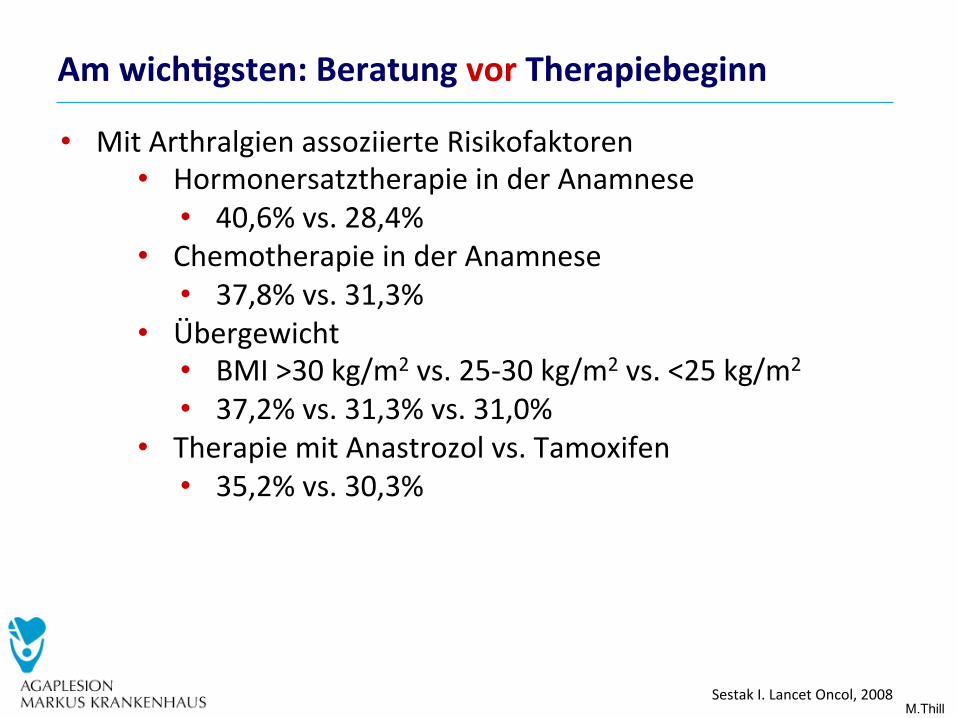
Amwich#gsten:BeratungvorTherapiebeginn
• MitArthralgienassoziierteRisikofaktoren• HormonersatztherapieinderAnamnese
• 40,6%vs.28,4%• ChemotherapieinderAnamnese
• 37,8%vs.31,3%• Übergewicht
• BMI>30kg/m2vs.25-30kg/m2vs.<25kg/m2
• 37,2%vs.31,3%vs.31,0%• TherapiemitAnastrozolvs.Tamoxifen
• 35,2%vs.30,3%
SestakI.LancetOncol,2008
M.Thill
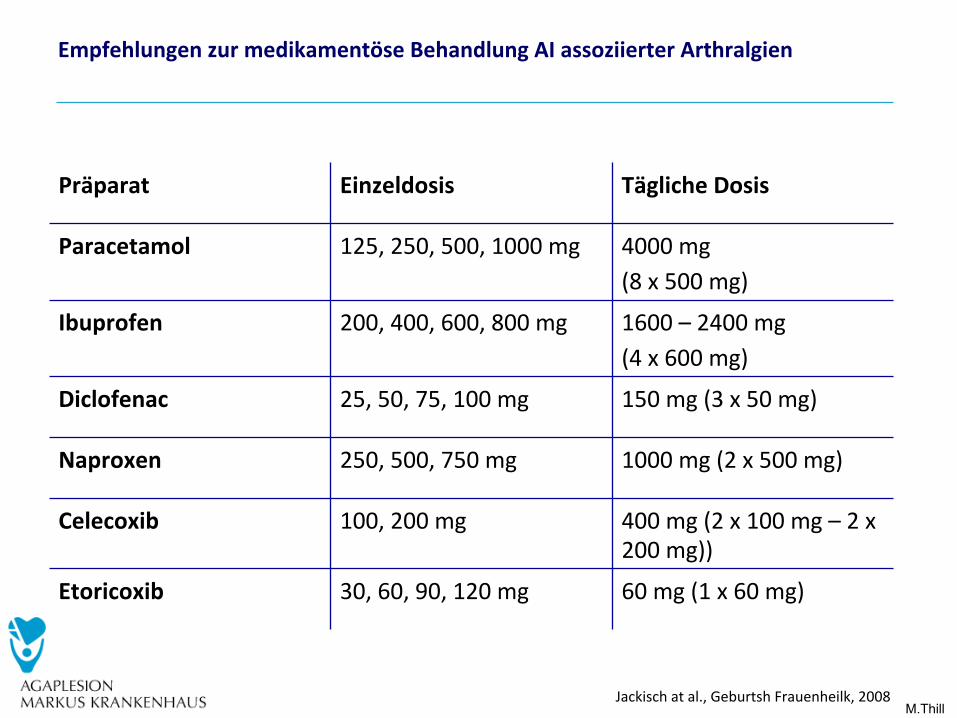
EmpfehlungenzurmedikamentöseBehandlungAIassoziierterArthralgien
Jackischatal.,GeburtshFrauenheilk,2008
Präparat Einzeldosis TäglicheDosis
Paracetamol 125,250,500,1000mg 4000mg(8x500mg)
Ibuprofen 200,400,600,800mg 1600–2400mg(4x600mg)
Diclofenac 25,50,75,100mg 150mg(3x50mg)
Naproxen 250,500,750mg 1000mg(2x500mg)
Celecoxib 100,200mg 400mg(2x100mg–2x200mg))
Etoricoxib 30,60,90,120mg 60mg(1x60mg)
M.Thill IrwinMetal.,SABCS2013
M.Thill
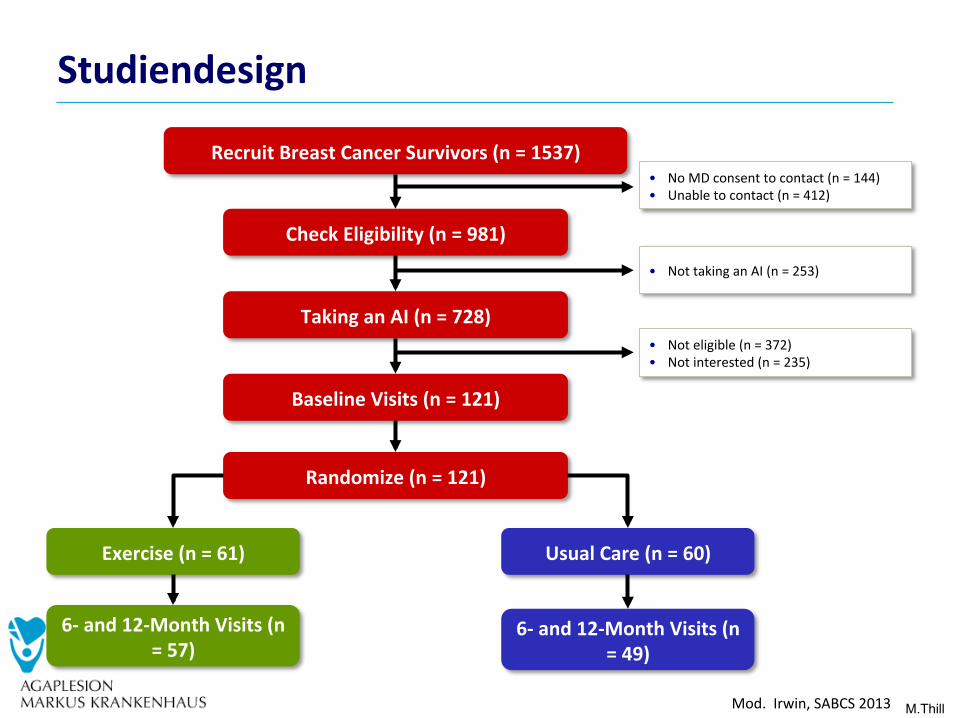
Studiendesign
Mod.Irwin,SABCS2013
RecruitBreastCancerSurvivors(n=1537)
CheckEligibility(n=981)
TakinganAI(n=728)
BaselineVisits(n=121)
Randomize(n=121)
Exercise(n=61) UsualCare(n=60)
6-and12-MonthVisits(n=57)
6-and12-MonthVisits(n=49)
• NoMDconsenttocontact(n=144)• Unabletocontact(n=412)
• NottakinganAI(n=253)
• Noteligible(n=372)• Notinterested(n=235)
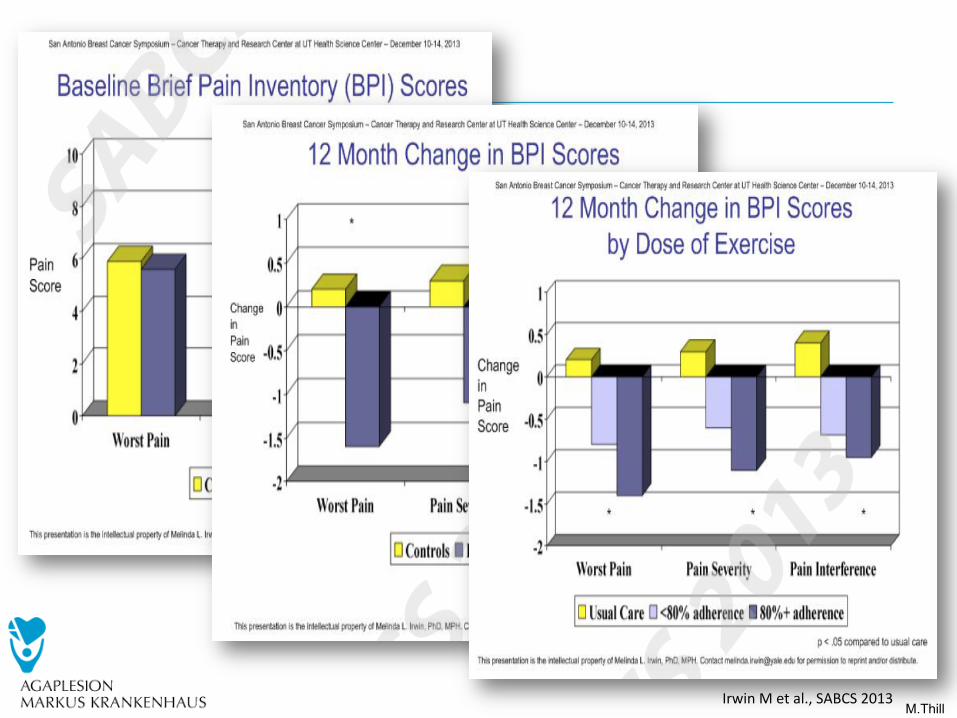
M.Thill IrwinMetal.,SABCS2013
M.Thill
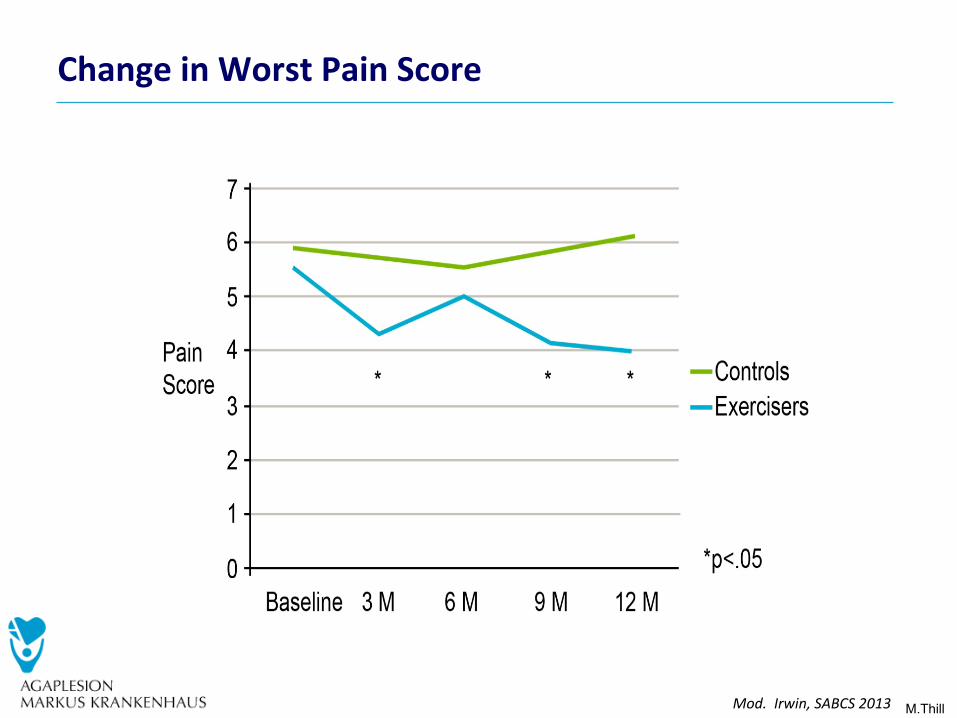
ChangeinWorstPainScore
Mod.Irwin,SABCS2013
M.Thill
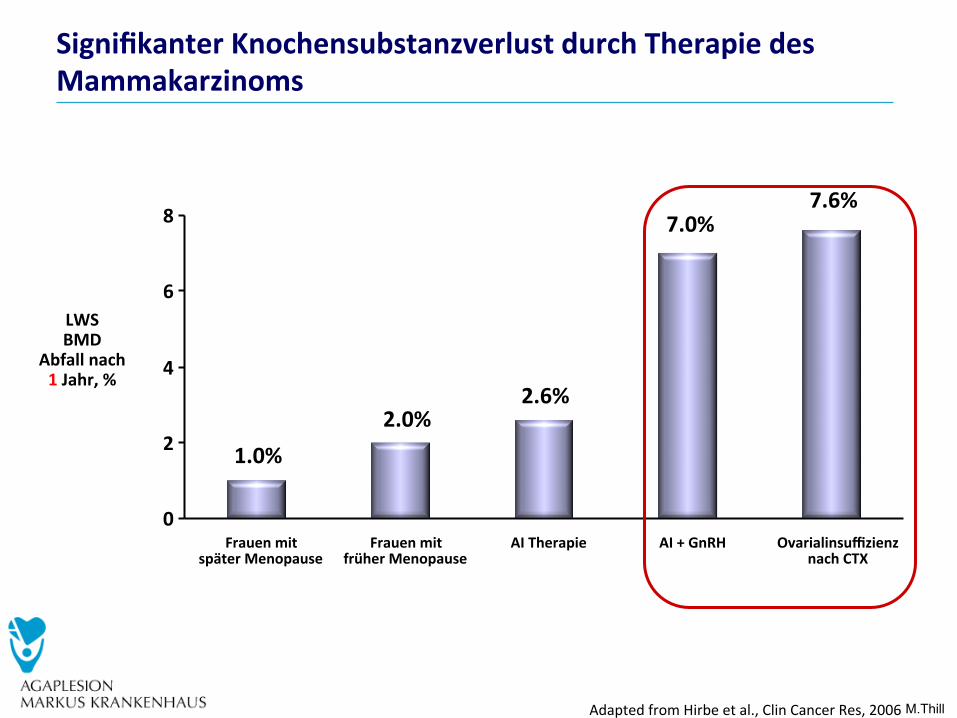
SignifikanterKnochensubstanzverlustdurchTherapiedesMammakarzinoms
AdaptedfromHirbeetal.,ClinCancerRes,2006
1.0%2.0%
7.0%7.6%
2.6%
0
2
4
6
8
FrauenmitspäterMenopause
FrauenmitfrüherMenopause
AITherapie AI+GnRH OvarialinsuffizienznachCTX
LWSBMD
Abfallnach1Jahr,%
M.Thill
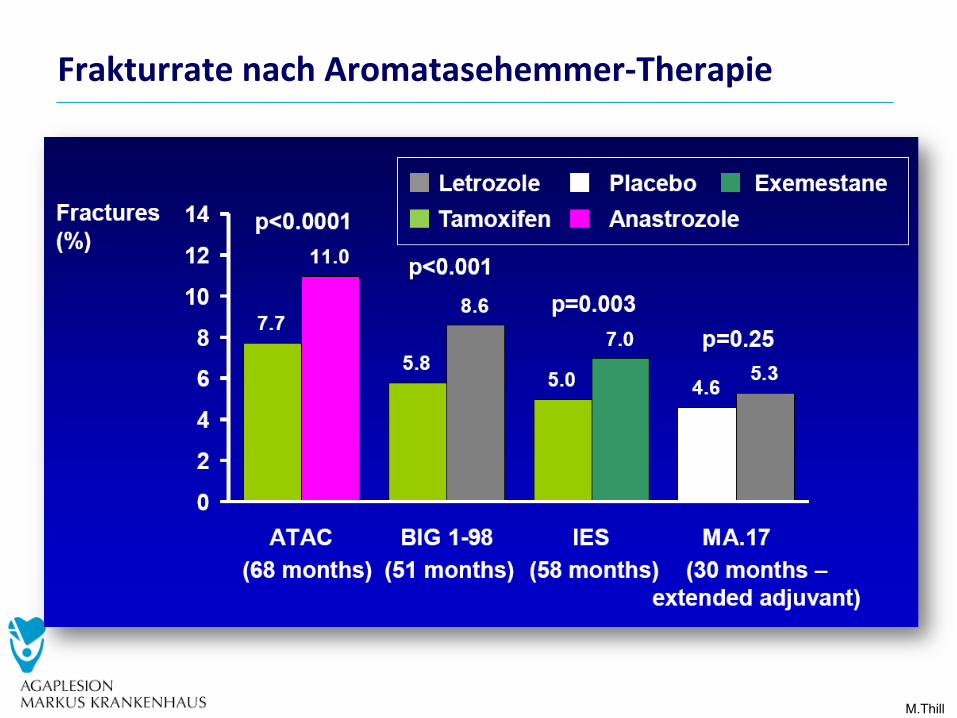
FrakturratenachAromatasehemmer-Therapie