botox training
169
Basic & Advanced Applications Hands-On Workshop Presented by ELITE Aesthetic, Medical & Business Training Copyright 2008 ELITE 2011
-
Upload
ona-owner -
Category
Health & Medicine
-
view
21.362 -
download
2
Transcript of botox training

Basic & Advanced Applications
Hands-On Workshop
Presented by
ELITE Aesthetic, Medical & Business TrainingCopyright 2008 ELITE
2011
Founded in 2008
• Independent Company - not supported by pharmaceutical companies, no product bias.
• Independent Instructors performing procedures outside classroom setting.
ELITE Revolutionized the Industry:
• Overcoming major frustrations health care professional encounter.
• Most comprehensive, affordable, current, hands-on aesthetic training available.
• Dare 2 Compare.
• Various training options to accommodate needs of each health care professional.
• Offer a Business Implementation program.
• Offer not only non-invasive cosmetic procedures, but also Health & Wellness training.
Experience the Difference, Choose ELITE!
2011

Aesthetic Medicine
Botox Cosmetic & Dermal Filler (basic & advanced)
Cosmetic Lasers & Light based systems
Lipodissolve & Mesotherapy (basic & advanced)
Chemical peels & Microdermabrasion
Sclerotherapy
Medical Training
Sensible Weight Loss
Wellness Integration program
Fibromyalgia
Dermatology for Non-Dermatologists
Business Training
Marketing Your Practice Effectively
3-day Business Training & Business Implementation program
Experience the Difference, Choose ELITE!
2011
Experience the Difference, Choose ELITE!
2011
Participants will leave class feeling confident to incorporate the newly acquired knowledge/skills & procedures into their existing practice.
• Incorporate both ‘basic’ and ‘advanced’ applications.
• Extensive Hands-on workshop – LIVE models.
• Comfort level with these procedures will increase with experience.
Some providers may feel more comfortable beginning with friends
and family.

Experience the Difference, Choose ELITE!
2011
9:00 am Botox® Cosmetic Didactic Presentation
11:30 am Break
11:45am Dermal Filler Didactic Presentation
1:00pm Lunch Break
2:00pm Demonstration Videos
3:00pm Hands-on Workshop on LIVE models
7:00pm Q&A, Evaluation & Certification

Experience the Difference, Choose ELITE!
2011
In an ongoing effort of training improvement, we ask you to complete the EVALUATION form, and direct any questions or concerns directly to ELITE at:
•Phone: 1-877-847-9200
•E-mail: [email protected]
•All feedback will be used by ELITE to improve future training.
•ELITE will contact the instructor, if necessary and communicate with the provider.
ELITE provides RESOURCE CD
If additional practical training is needed, instructors are available for
private sessions.

Experience the Difference, Choose ELITE!
2011
2+ hours of LIVE Demonstrations
Regular Price $199
Seminar Participants ONLY $99
$100.00 Voucher for any other ELITE
TRAINING within 30 days

Experience the Difference, Choose ELITE!
2011
FAST CASH PROGRAM
$250.00 Instant CASH for EACH Paid Referral to one
of our Seminars or Private Training
$100.00 for each ONLINE Training Paid Referral
Unlimited
Flyers available

Experience the Difference, Choose ELITE!
2011
FAST CASH PROGRAM
$250.00 Instant CASH for EACH Paid Referral to one
of our Seminars or Private Training
$100.00 for each ONLINE Training Paid Referral
Unlimited
Flyers available

Experience the Difference, Choose ELITE!
2011
Become an ELITE Member Today And...
SAVE Huge on Training
SAVE Huge on Product
Stay UP-TO-DATE on the latest
JOIN our FREE WEBINARS!
And More...
Experience the Difference, Choose ELITE!
2011
Dr. Mike Van Thielen
Senior Instructor
Comprehensive Overview & Practical Applications
Presented by ELITE Aesthetic, Medical & Business Training
Copyright 2011 ELITE
Procedures in Cosmetic Dermatology Series, ISBN: 978-1-4160-4213-6
Reference: Botulinum Toxin – Carruthers & Carruthers – 2nd Edition
Introduction & History Statistics of Aesthetics Etiology of Aging Face Pharmacology & Physiology of Botulinum Toxin Functional & Practical Anatomy Storage, Handling & Dilution Indications, Contraindications & Complications Treatment of Upper Face Treatment of The Lower Face & Neck Adjunctive Treatments Client Education & Realistic Expectations Hands-on Workshop and/or (live) Demonstrations.
Love for Beauty
Ideal proportions &
Shapes
Normal
Relationship
Between Facial
Units
Harmony &
Balance
Looking Young For
Biological Age
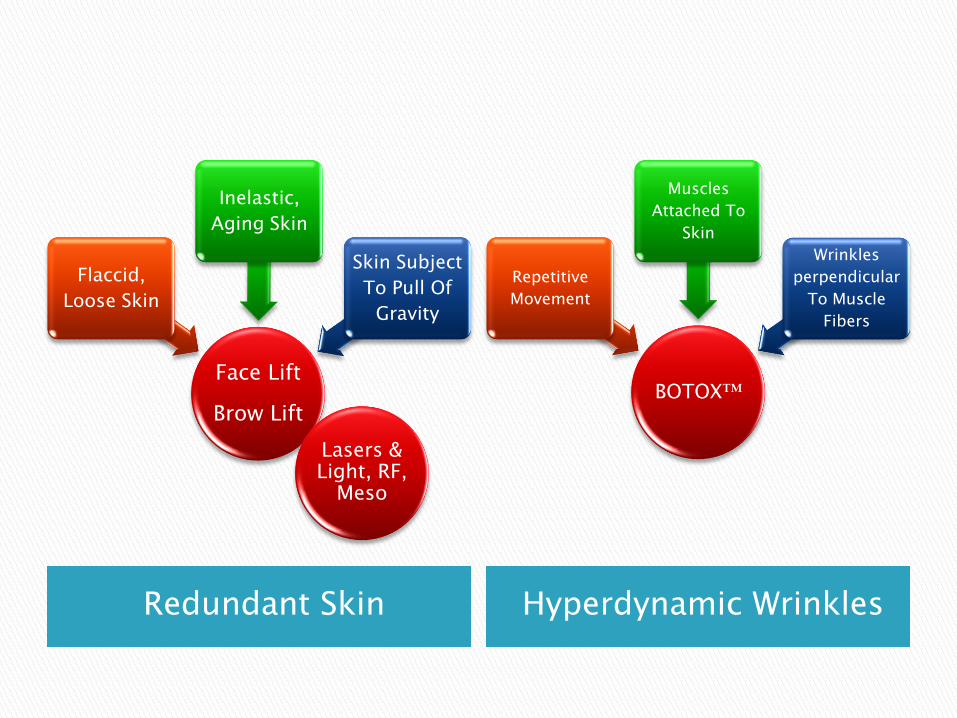
Redundant Skin Hyperdynamic Wrinkles
Face Lift
Brow Lift
Flaccid,
Loose Skin
Inelastic,
Aging Skin
Skin Subject
To Pull Of
Gravity
BOTOX™
Repetitive
Movement
Muscles
Attached To
Skin
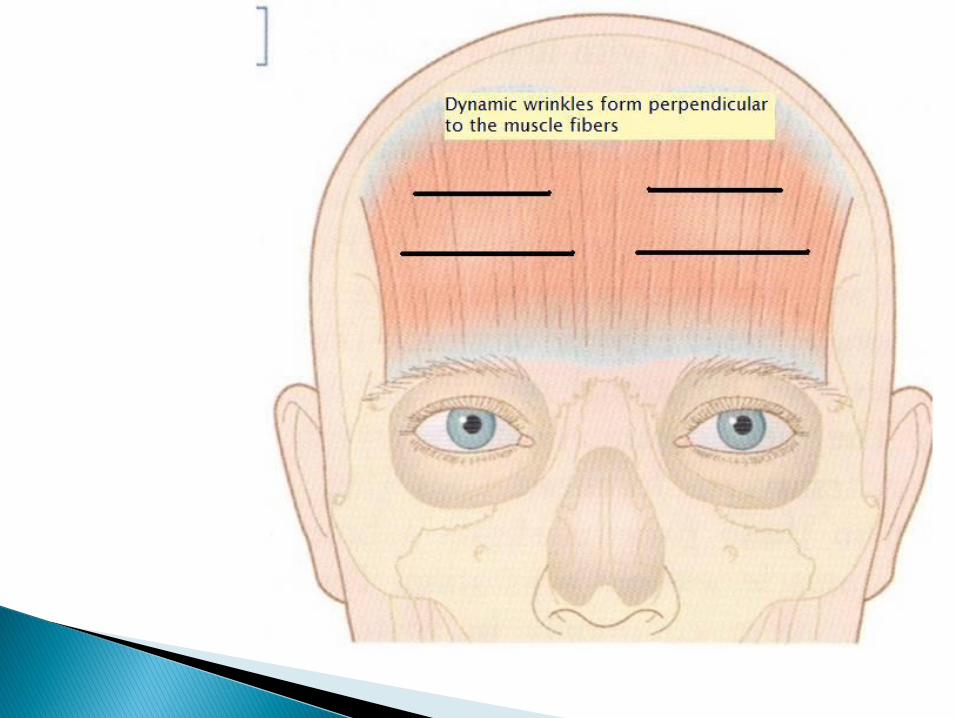
Wrinkles
perpendicular
To Muscle
Fibers
Lasers & Light, RF,
Meso
Strong contrast with current use of BTX.
Botulism:◦ Form of food poisoning („botulus‟ = sausage).
1895: Belgian picnic (34 people ill, 3 died after eating raw, salted ham).
Professor Emile Pierre Marie Van Ermengem identified the etiologic agent and named it „bacillus botulinus‟.
Renamed and reclassified as „Clostridium botulinum‟.
◦ Anaerobic, spore forming bacterium that under certain conditions can germinate and create a toxin.
Toxin:
Resists alcohol, mild acid and enzymes.
Not heat-resistant.
Some animals (dogs, chickens) unaffected by toxin.
Symptoms: blurred vision, nausea, dizziness, dry. mouth – may progress to flaccid paralysis and death.
Type A, B & E documented as causative strains for human cases of botulism.
1920:
isolation of toxins initiated by Dr. Herman Sommer.
1946:
Type A Toxin isolated by Edward Shantz (for US Army).
1949:
Burgen discovered mechanism of action.
1950‟s:
Dr. Vernon Brooks: 1st. medical use of botulium toxin.
1973:
Dr. Alan B. Scott: 1st study demonstrating therapeutic value of BTX was published.
Attempts to treat strabismus showed that BTX effectively weakens the eye muscles in primates.
1977:
Treatment for strabismus attempted in humans.
1979:
Dr. Schantz prepared 1st. Batch of 11-79, now called Botox.
The 150mg batch served as the source of all BTX-A used in humans in USA until 1997.
Limited FDA-approval to use of BTX-A for strabismus.
1985:
FDA-approval to include blepharospasm.
1987:
Carruthers & Carruthers performed joint dermatological-ophthalmologica research with Dr. Alan B. Scott.
Dr. Jean Carruthers observed significant improvement of dynamic rhytides in glabellar region while treating patients for blepharospasm.
1989:
Dr. Alan B. Scott‟s company Oculinum, Inc. acquired by Allergan, Inc.
Name of product changed to Botox.
FDA-approval to include hemifacial spasm.
1991-1992:
Drs. Jean & Alastair Carruthers reported and published initial findings of BTX-A for cosmetic usage, demonstrating the safe & effective treatment of dynamic rhytides in the glabella.
1993:
Blitzer and colleagues described use of BTX for rhytides of the forehead and elsewhere.
1997:
BTX-A source by Allergan Inc. (Irvine, CA) FDA-approved.
1999:
New England Journal of Medicine – Editorial „One Man‟s Poison – Clinical Applications of Botulinum Toxin‟ provides examples of historic uses:
Lower limb and upper limb spasticity in children.
Anal fissures.
2003:
FDA-approval for treatment of glabellar rhytides.
Subsequent publications and usage expanded the use of BTX to new area‟s of treatment:
Crow‟s feet, neck (platysma), oricular muscles.
Pain & spasms (migraine, torticollis).
Hyperhydrosis.
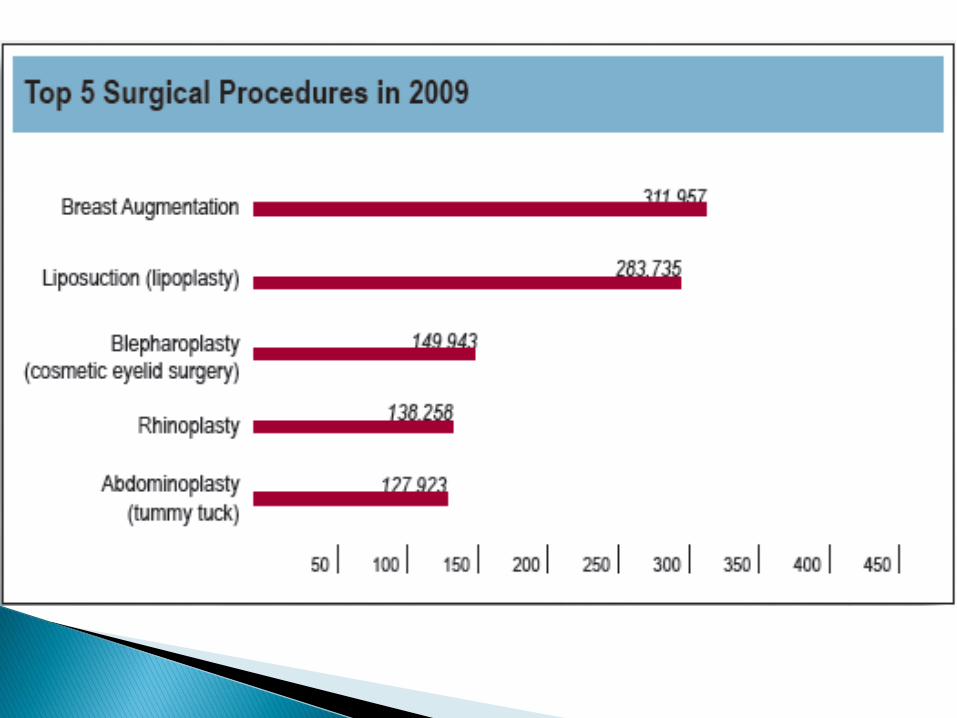
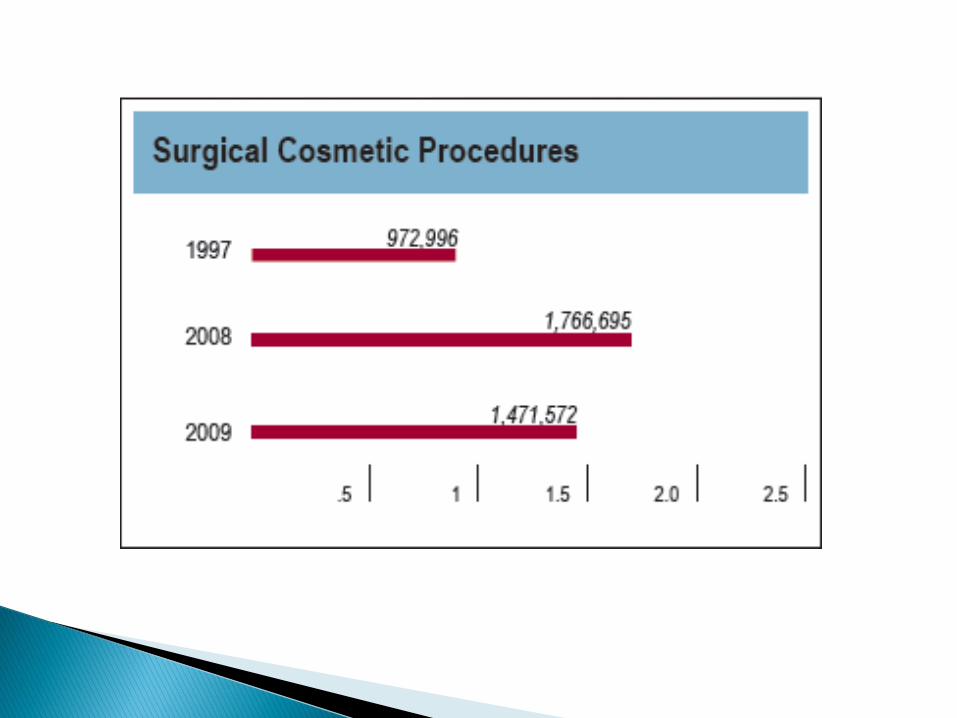
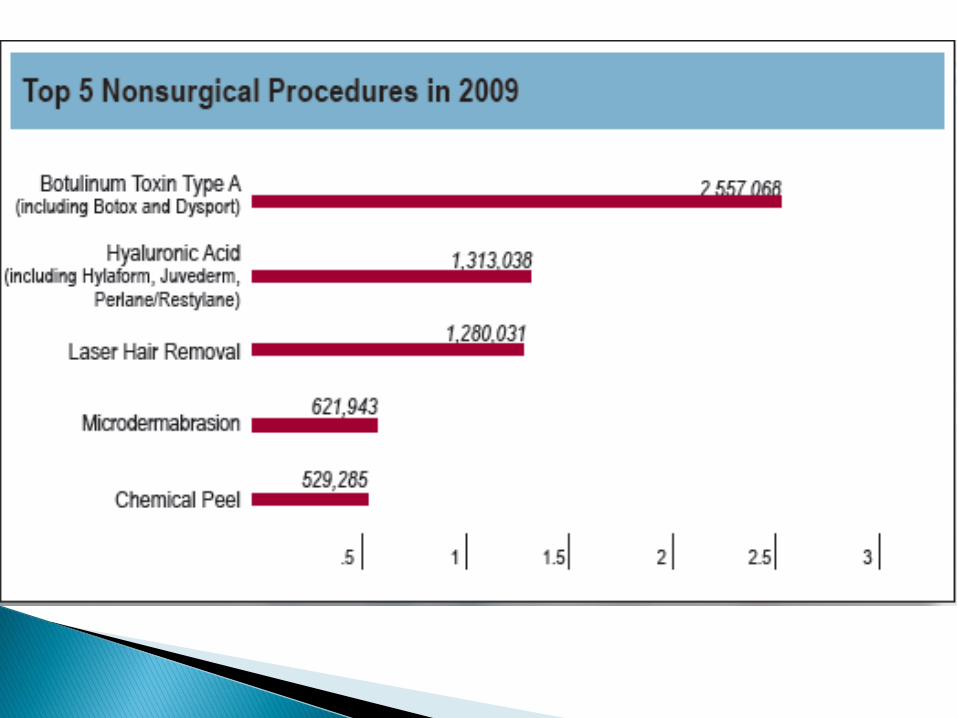
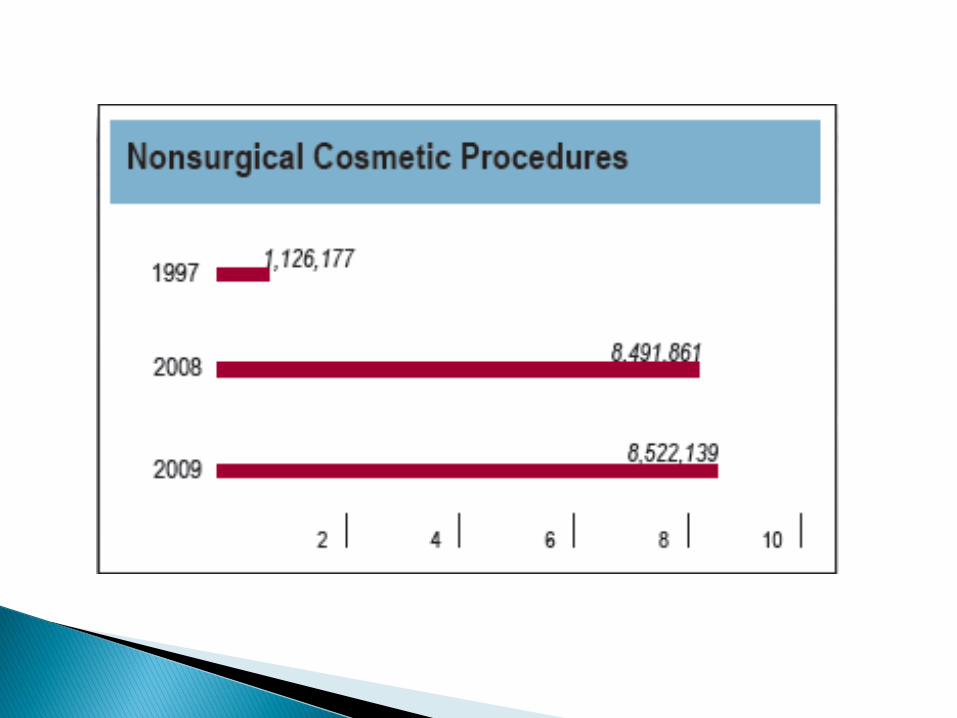
Statistical data courtesy of:
THE AMERICAN SOCIETY FOR AESTHETIC PLASTIC
SURGERY (ASAPS)
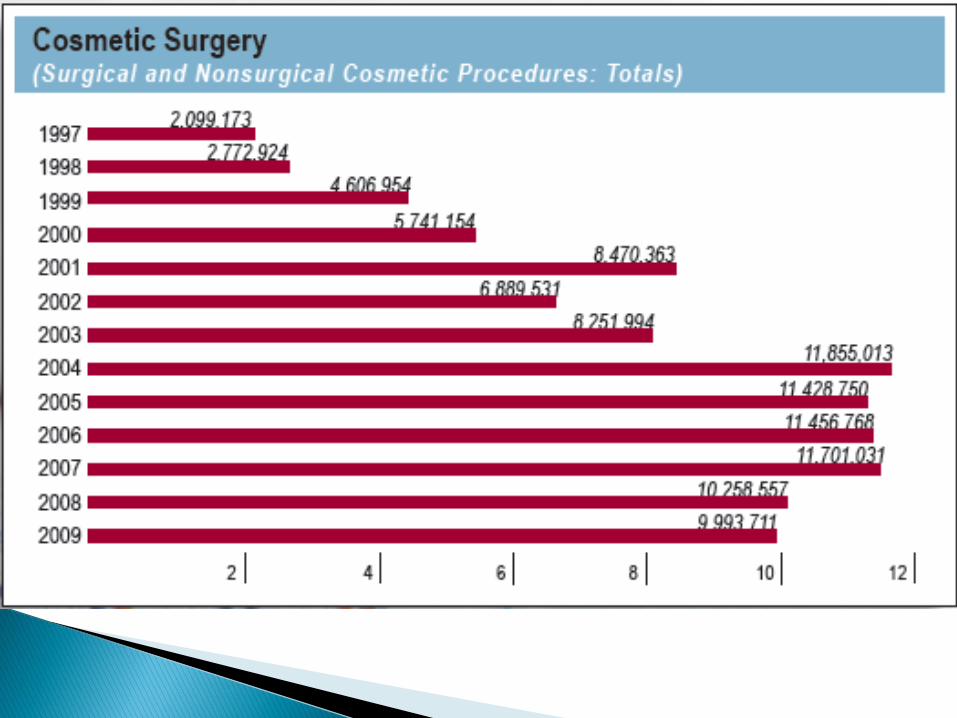
10 Million Cosmetic Procedures in 2009.
Increase of 147 percent since1997.
Repeat patients and those putting off surgery, are likely the reason for the growth in non-surgical cosmetic procedures.
Growth in demand will likely return as the recession eases and baby boomer's offspring begin to explore cosmetic procedures.
Cronic UV-damage to the skin.◦ Photo-aging due to cumulative sun exposure.
◦ Glogau Wrinkle Scale:
Type 1: 'Early Wrinkles'
Patient age: 20s to 30s
Early photo-aging
Mild pigment changes
Minimal wrinkles
No 'age spots'
Type 2: 'Wrinkles in Motion'
Patient age: 30s to 40s
Early to moderate photo-aging
Appearance of smile lines
Early brown 'age spots'
Skin pores more prominent
Early changes in skin texture
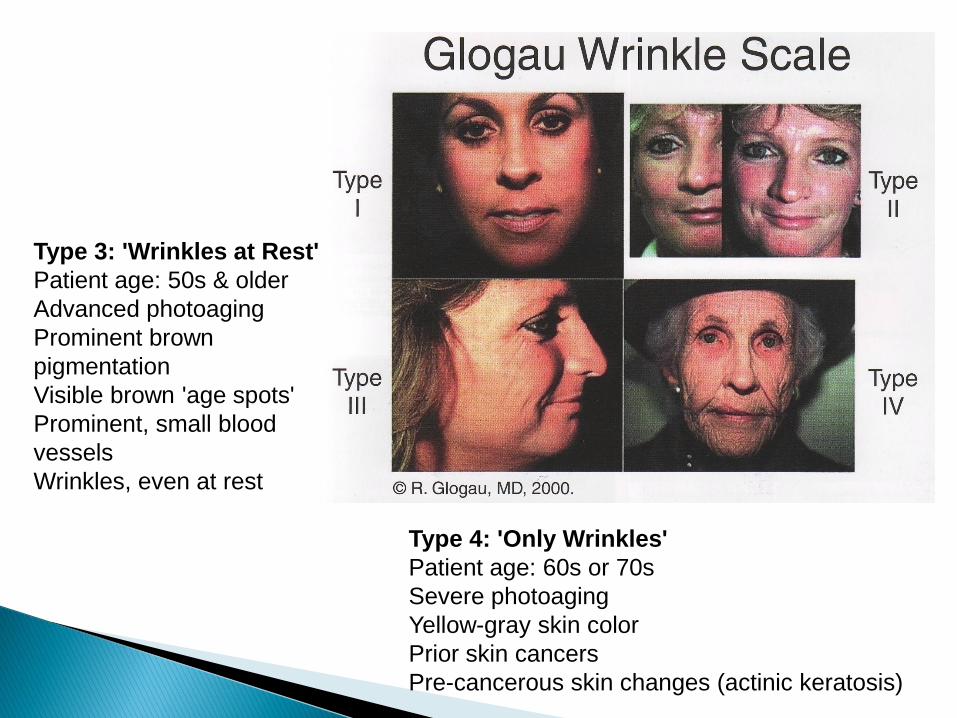
Type 3: 'Wrinkles at Rest'
Patient age: 50s & older
Advanced photoaging
Prominent brown
pigmentation
Visible brown 'age spots'
Prominent, small blood
vessels
Wrinkles, even at rest
Type 4: 'Only Wrinkles'
Patient age: 60s or 70s
Severe photoaging
Yellow-gray skin color
Prior skin cancers
Pre-cancerous skin changes (actinic keratosis)
Loss of subcutaneous fat.◦ Loss of volume and fullness/roundness.
◦ Flattened, sunken appearance.
◦ Facial contours and mouth.
Hyperdynamic wrinkles due to repetitive facial expression.◦ Smoking, frowning, squinting etc.
◦ Muscles that insert into skin.
Frontal, glabellar, periocular, nasolabial, perioral
◦ Initially only wrinkles with movement, later at rest.

Loss of elasticity due to gravitational changes.◦ Facial soft tissues lose resiliency and can no longer
resist stretching forces and movement; no rebound.
◦ Facial soft tissues start to sag as a result of gravity.
Remodeling of bony and cartilaginous structures.◦ Bone resorption results in decrease of facial
volume.
◦ Stretching of cartilage as a result of gravitational forces results in drooping of facial structures (nasal tip)
◦ Facial assymmetry may result.
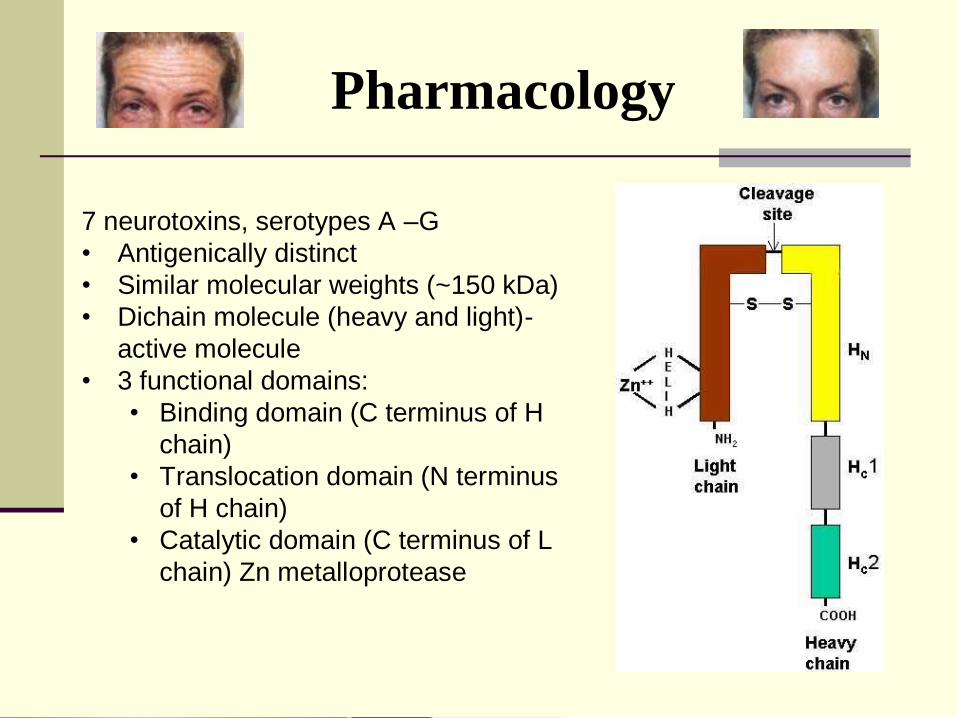
Pharmacology
7 neurotoxins, serotypes A –G
• Antigenically distinct
• Similar molecular weights (~150 kDa)
• Dichain molecule (heavy and light)-
active molecule
• 3 functional domains:
• Binding domain (C terminus of H
chain)
• Translocation domain (N terminus
of H chain)
• Catalytic domain (C terminus of L
chain) Zn metalloprotease
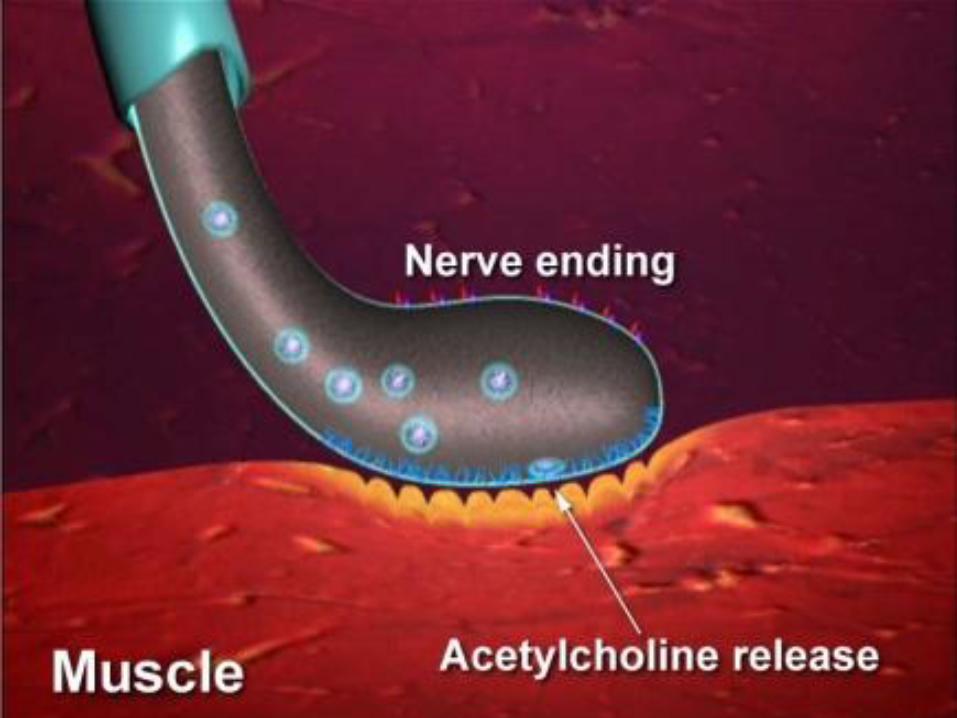
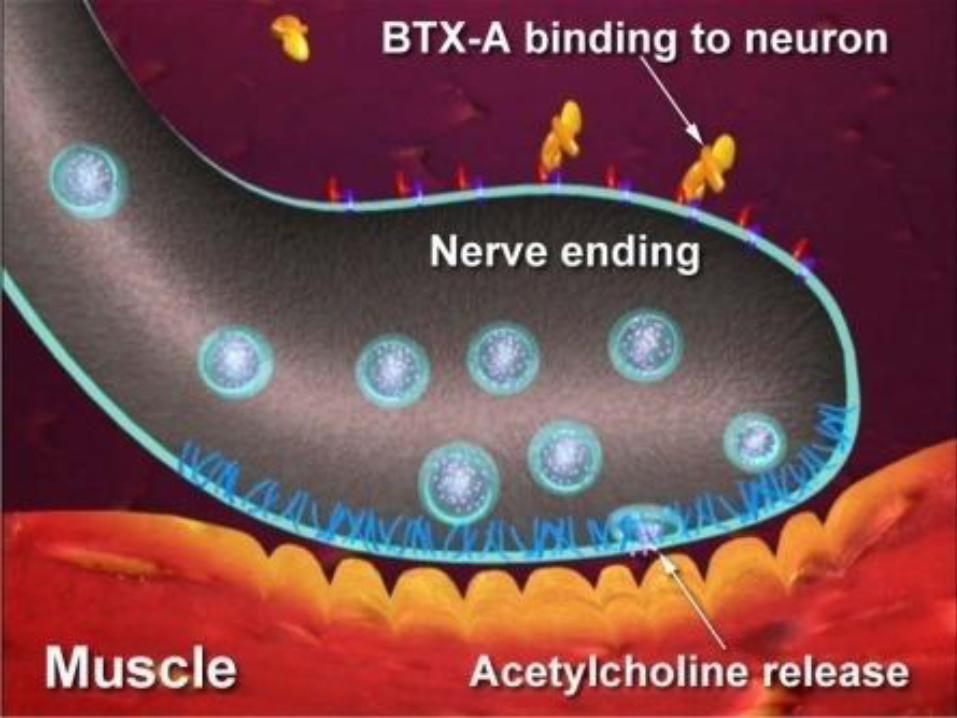
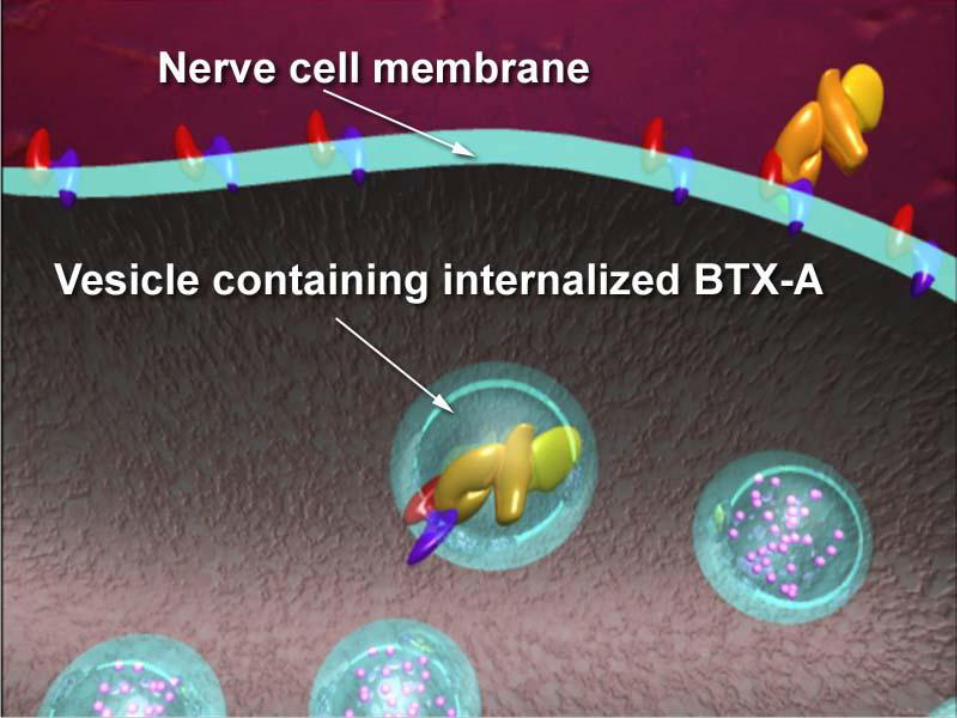
Pharmacology
Three step process
Irreversibly binds to presynaptic terminal of motor end
plate
Internalized into axon by endocytosis
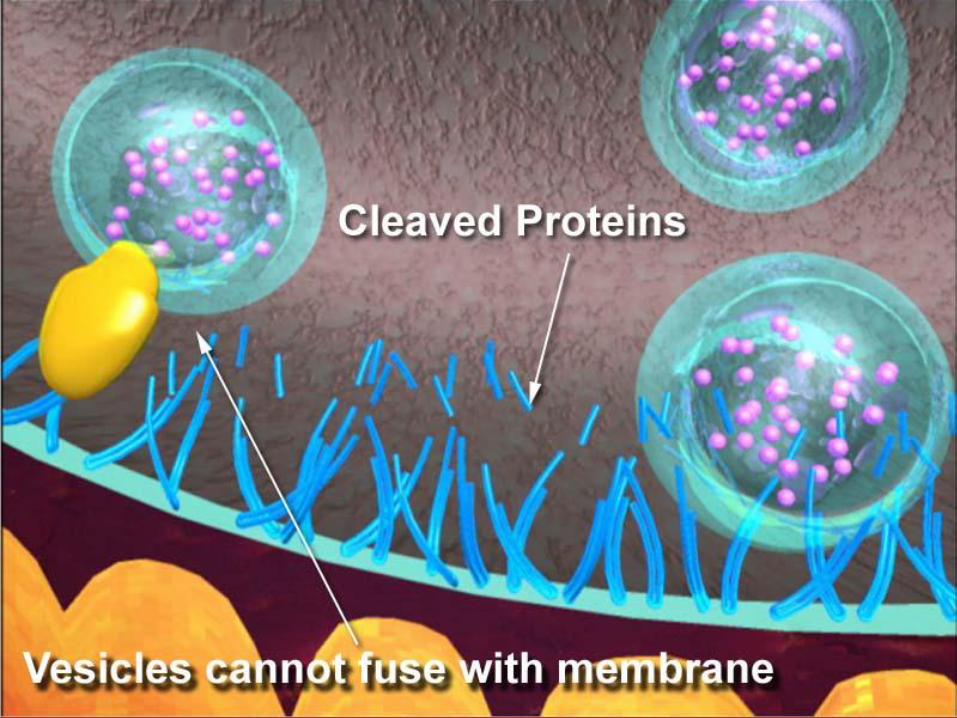
Cleavage of SNARE (receptor) proteins resulting in
inhibition of neurotransmitter release
SNARE proteins:
– N-ethylmaleimide sensitive factor attachment protein
receptor
– Each serotype binds to a specific residue of one of
the docking proteins
(Botox=SNAP-25, Myobloc=VAMP)
BOTOX® Myobloc
Solstice Neurosciences (San Fransisco, CA)
FDA-Approved Type-B 2500, 5000 & 10,000U Less potent (50-150 times
dose of BTX-A) More rapid onset (48 hours),
lasts 10-12 weeks Larger diffusion More stable, shipped in liquid
form, no reconstitution May be kept refrigerated at 2-
8°C for 21 months May be used when no
response to Type-A (antibodies to Type-A)
In the United States, prescription drugs and biologics arerequired to undergo rigorous laboratory, animal, andhuman clinical testing before they can be put on themarket. The Food and Drug Administration (FDA) reviewsthe results of these studies to: verify the identity,potency, purity, and stability of the "ingredients," anddemonstrate that the drug is safe and effective for itsintended use.
BOTOX® Cosmetic received FDA approval in 2003 for thetemporary treatment of moderate to severe frown linesbetween the brows in people 18 to 65 years of age.BOTOX® Cosmetic is available by prescription only.
Dysport (Reloxin)
FDA-approved 2009Other Type-A Toxins
Currently known as Dysport in UK (Ipsen, Inc., berkshire)
Type-A
Marketed by Medicis Esthetics (US)
300U and 500U vials
Excipient materials include lactose and albumin
Recommended reconstitution 500U with 1ml of saline
Estimated 2.5 – 3 times dosage compared with Botox
Puretox (Mentor)
Linurase (Prollenium)
Neuronox (Medy-Tox, South Korea)
CBTX A (China)
Clinical Trials:
◦ Topical Botulinum – Type A
GFX Technology-Radiofrequency ablation (www.acisurgery.com) and Radiage RF (available).
Lasers & Light-based systems.

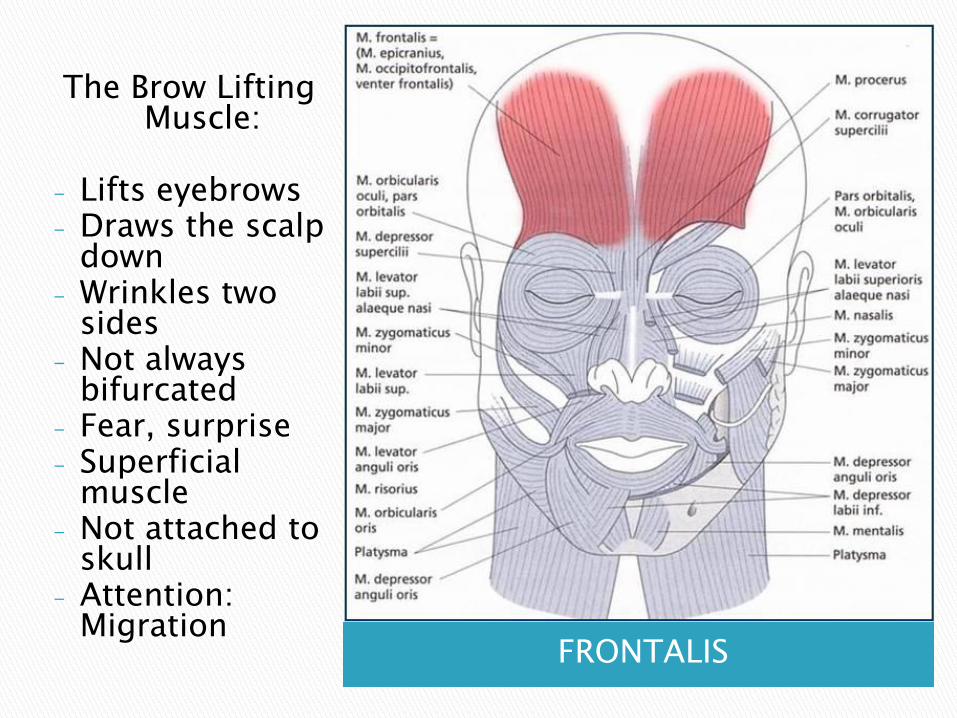
FRONTALIS
The Brow Lifting Muscle:
- Lifts eyebrows- Draws the scalp
down- Wrinkles two
sides- Not always
bifurcated- Fear, surprise- Superficial
muscle- Not attached to
skull- Attention:
Migration

PROCERUS
The Flaring NostrilsMuscle:
Small pyramidal slip of muscle (flame shaped)
Helps to pull that part of the skin between the eyebrows downwards, which assists in flaring the nostrils.
Anger Produces
transverse wrinkles or „bunny lines‟
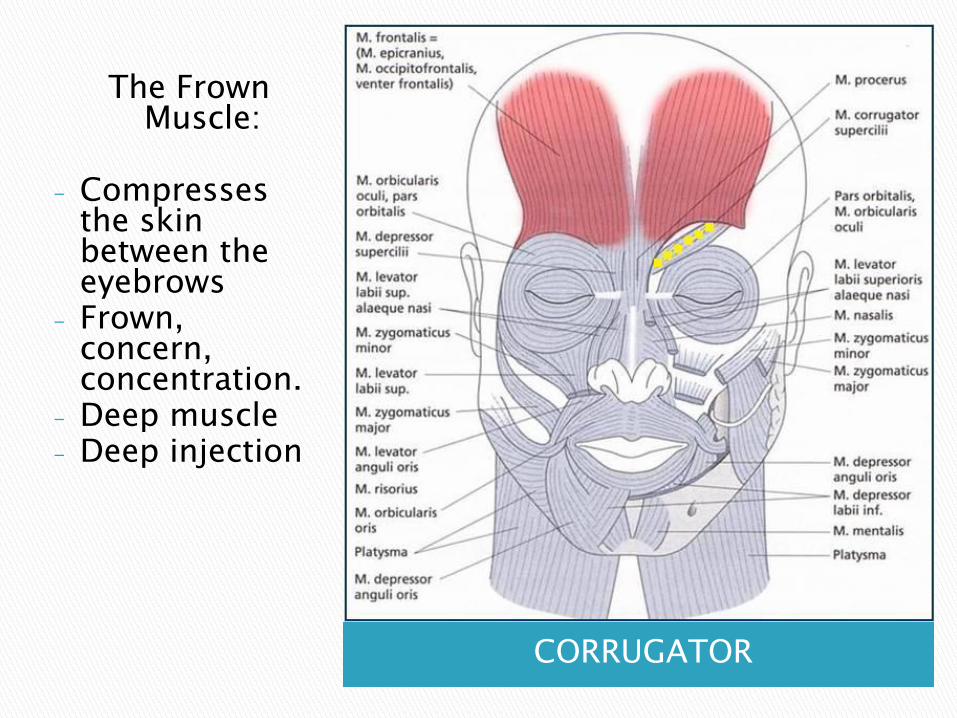
CORRUGATOR
The Frown Muscle:
- Compresses the skin between the eyebrows
- Frown, concern, concentration.
- Deep muscle- Deep injection
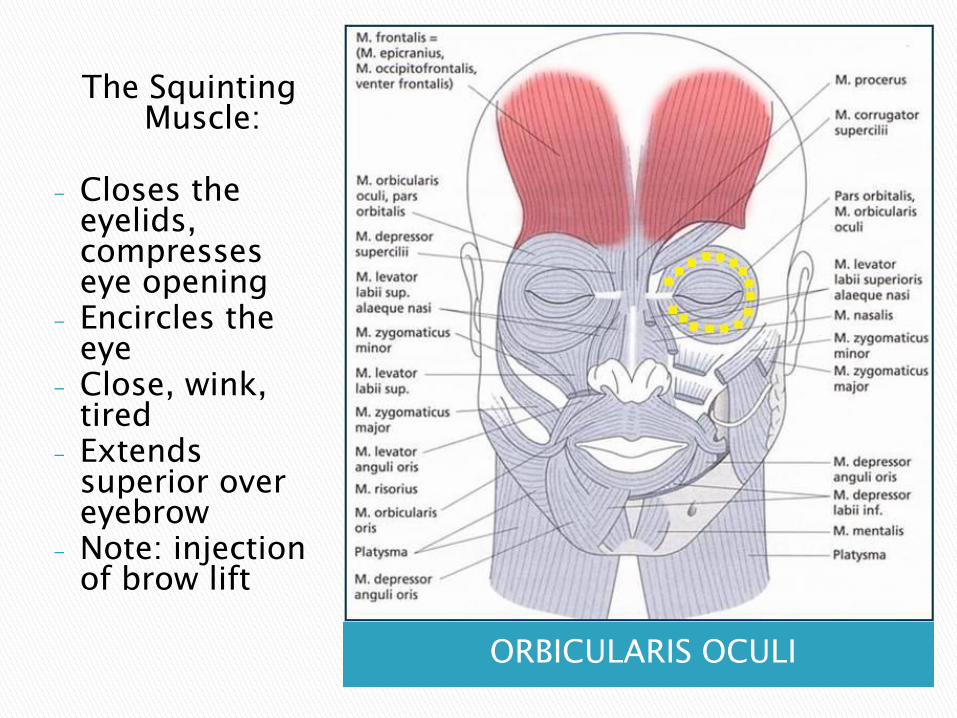
ORBICULARIS OCULI
The Squinting Muscle:
- Closes the eyelids, compresses eye opening
- Encircles the eye
- Close, wink, tired
- Extends superior over eyebrow
- Note: injection of brow lift
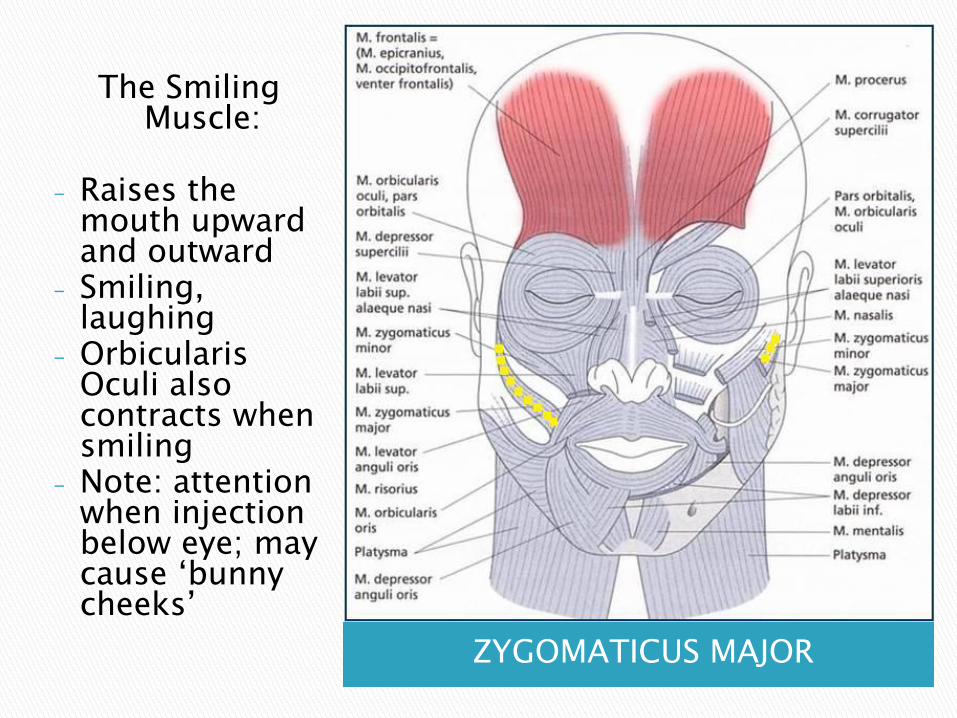
ZYGOMATICUS MAJOR
The Smiling Muscle:
- Raises the mouth upward and outward
- Smiling, laughing
- OrbicularisOculi also contracts when smiling
- Note: attention when injection below eye; may cause „bunny cheeks‟
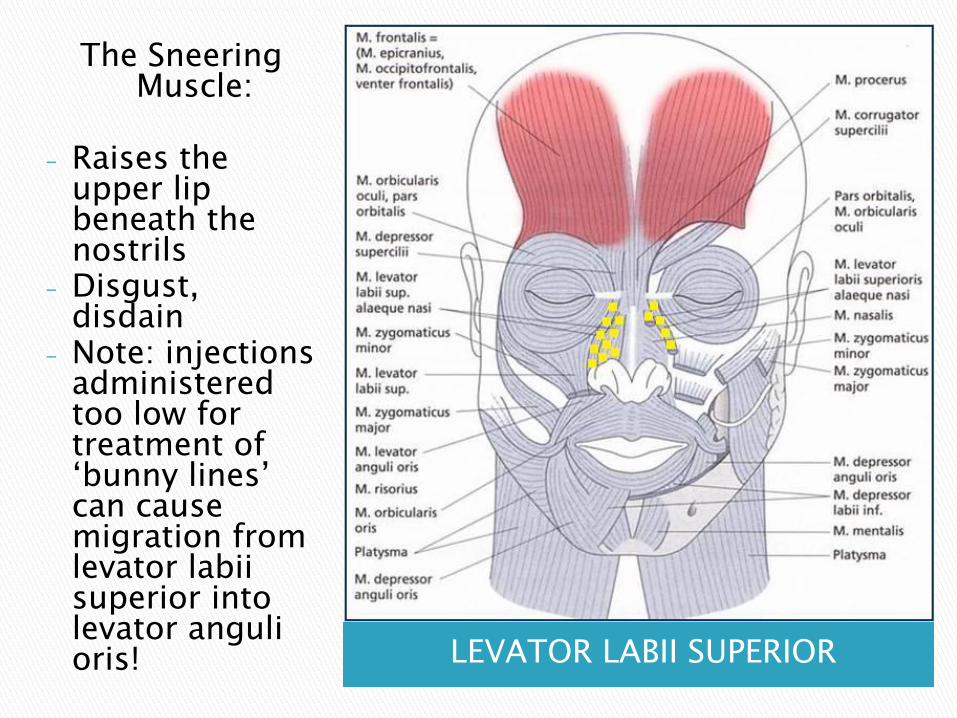
LEVATOR LABII SUPERIOR
The Sneering Muscle:
- Raises the upper lip beneath the nostrils
- Disgust, disdain
- Note: injections administered too low for treatment of „bunny lines‟ can cause migration from levator labiisuperior into levator angulioris!
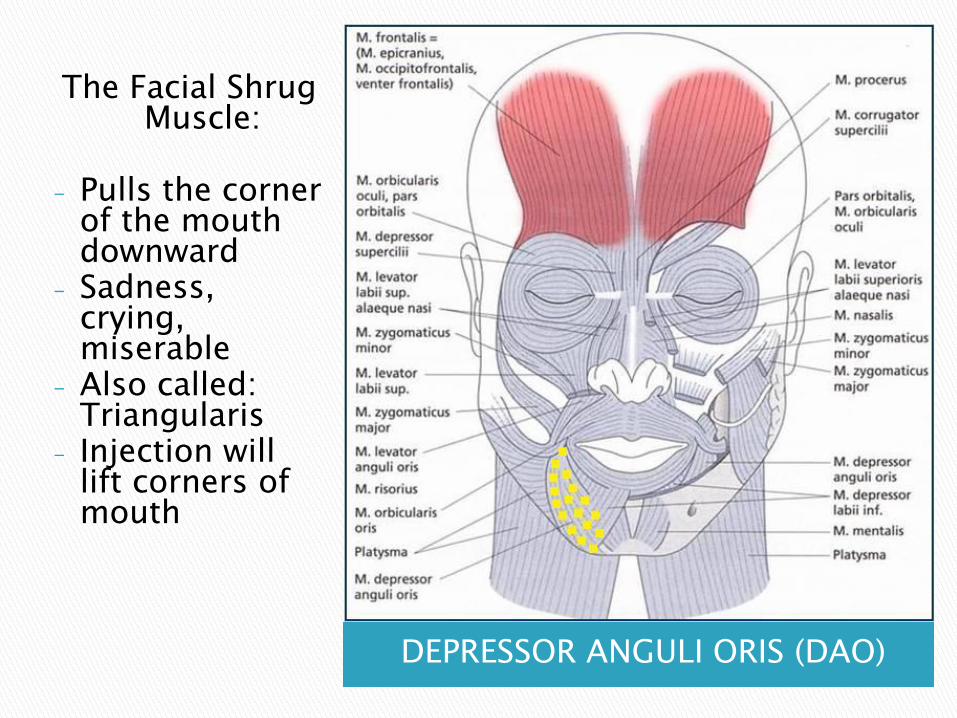
DEPRESSOR ANGULI ORIS (DAO)
The Facial Shrug Muscle:
- Pulls the corner of the mouth downward
- Sadness, crying, miserable
- Also called: Triangularis
- Injection will lift corners of mouth
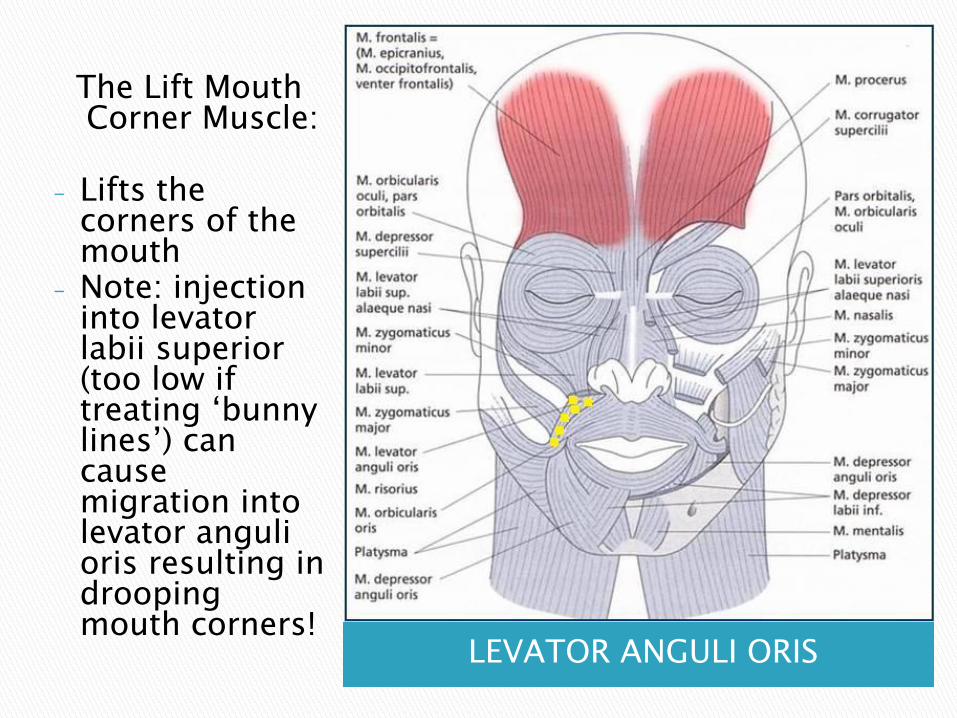
LEVATOR ANGULI ORIS
The Lift Mouth Corner Muscle:
- Lifts the corners of the mouth
- Note: injection into levatorlabii superior (too low if treating „bunny lines‟) can cause migration into levator angulioris resulting in drooping mouth corners!
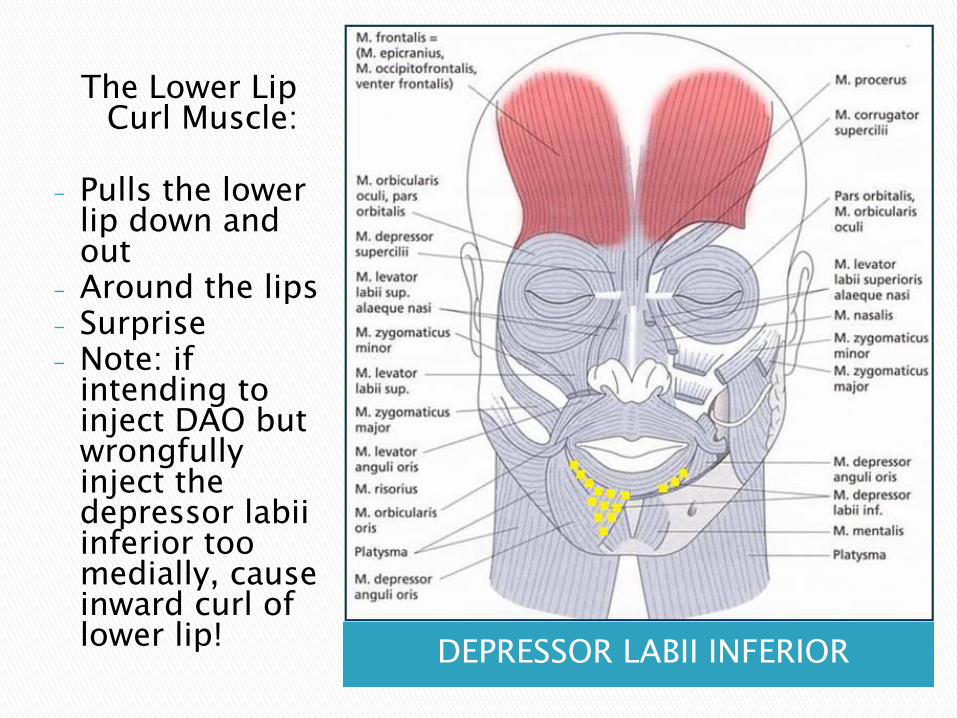
DEPRESSOR LABII INFERIOR
The Lower Lip Curl Muscle:
- Pulls the lower lip down and out
- Around the lips- Surprise- Note: if
intending to inject DAO but wrongfully inject the depressor labiiinferior too medially, cause inward curl of lower lip!
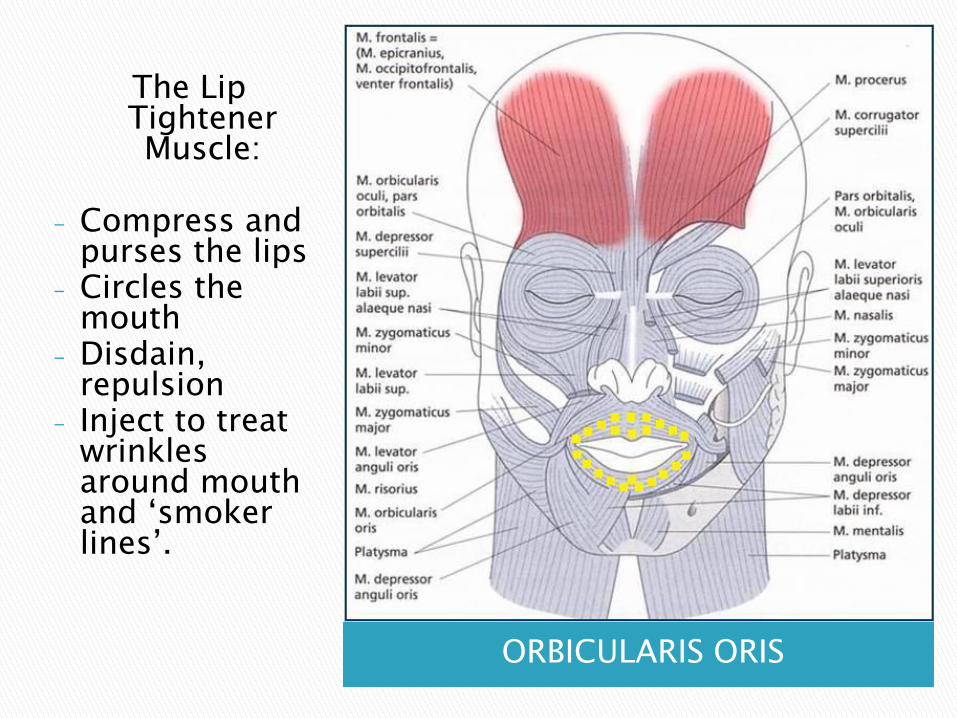
ORBICULARIS ORIS
The Lip TightenerMuscle:
- Compress and purses the lips
- Circles the mouth
- Disdain, repulsion
- Inject to treat wrinkles around mouth and „smoker lines‟.
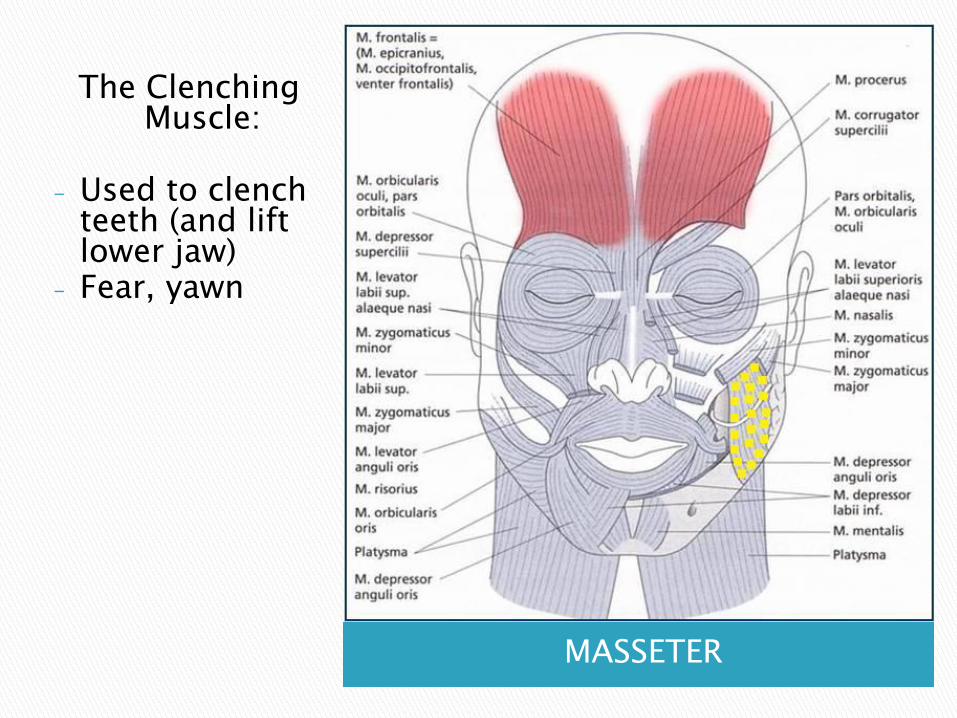
MASSETER
The Clenching Muscle:
- Used to clench teeth (and lift lower jaw)
- Fear, yawn
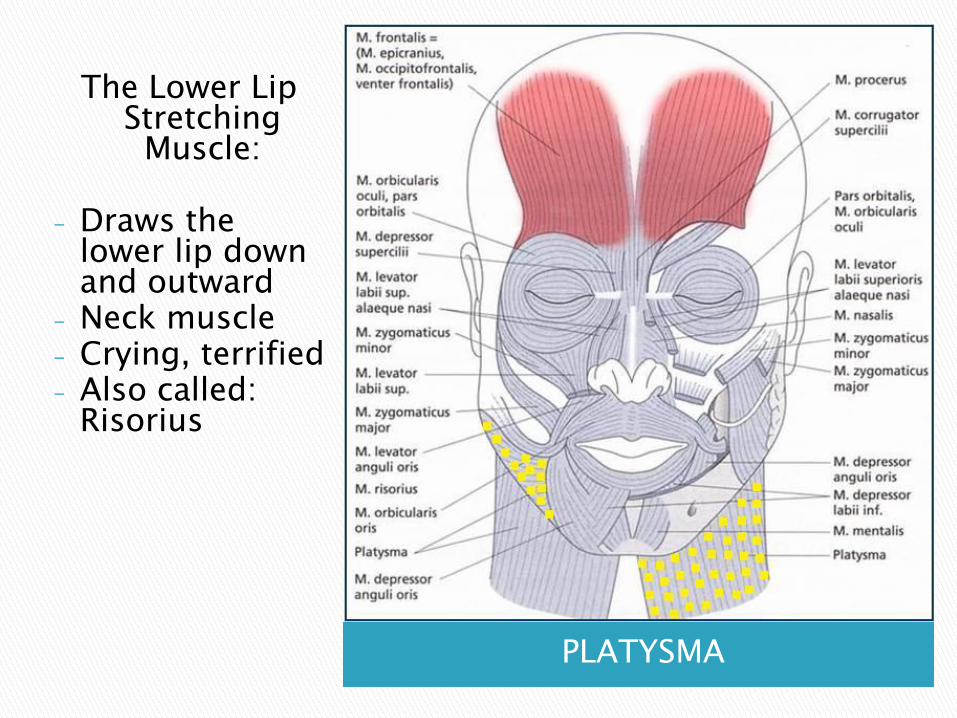
PLATYSMA
The Lower Lip Stretching Muscle:
- Draws the lower lip down and outward
- Neck muscle- Crying, terrified- Also called:
Risorius
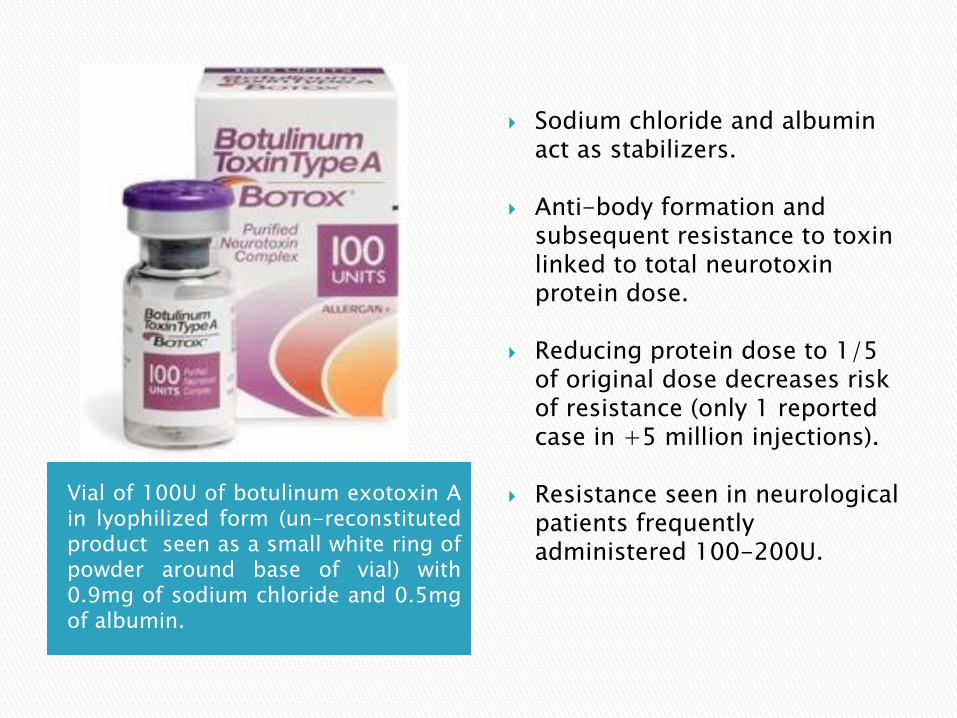
Vial of 100U of botulinum exotoxin Ain lyophilized form (un-reconstitutedproduct seen as a small white ring ofpowder around base of vial) with0.9mg of sodium chloride and 0.5mgof albumin.
Sodium chloride and albumin act as stabilizers.
Anti-body formation and subsequent resistance to toxin linked to total neurotoxin protein dose.
Reducing protein dose to 1/5 of original dose decreases risk of resistance (only 1 reported case in +5 million injections).
Resistance seen in neurological patients frequently administered 100-200U.
BOTOX® is shipped frozen, and must be kept at refrigerator or freezer temperatures; traditionally a frozen temperature of -5°C is recommended prior to use (no evidence). Lower temperatures reduce potency.
Manufacturer recommends using BOTOX® within 4 hours of reconstitution :◦ Mandated by FDA for any product reconstituted with preservative-free saline
◦ For sterility issues, not a loss in efficacy!
Potency controversy:◦ Originally thought to degrade sharply:
Gartland & Hoffman noted significant loss of toxicity within 12 hours of reconstitution.
Lowe noted a 50% reduction in potency after 1 week.
◦ Other studies show effects up to 30 days:
Garcia & Fulton reported continued potency 4 weeks after reconstitution.
Hexsel found no statistical difference in efficacy or duration of action between bottles of Botox reconstituted at the time of injection, 2 weeks, 4 weeks, and even 6 weeks prior to injection (recent controlled study with 88 patients).
Storage:◦ Keep refrigerated after use (4 hours – 30 days)
Strong vacuum in vial.
Use 1.0 or 2.5 cc sterile saline per 100 u vial (4U/0.1ml).
Greater dilution results in greater diffusion.
Use (preservative free) saline (NaCl 0.9%).
Introduce saline VERY slowly into BOTOX® vial.
Do not shake vial! Make every effort to avoid foaming (foaming will denature protein).
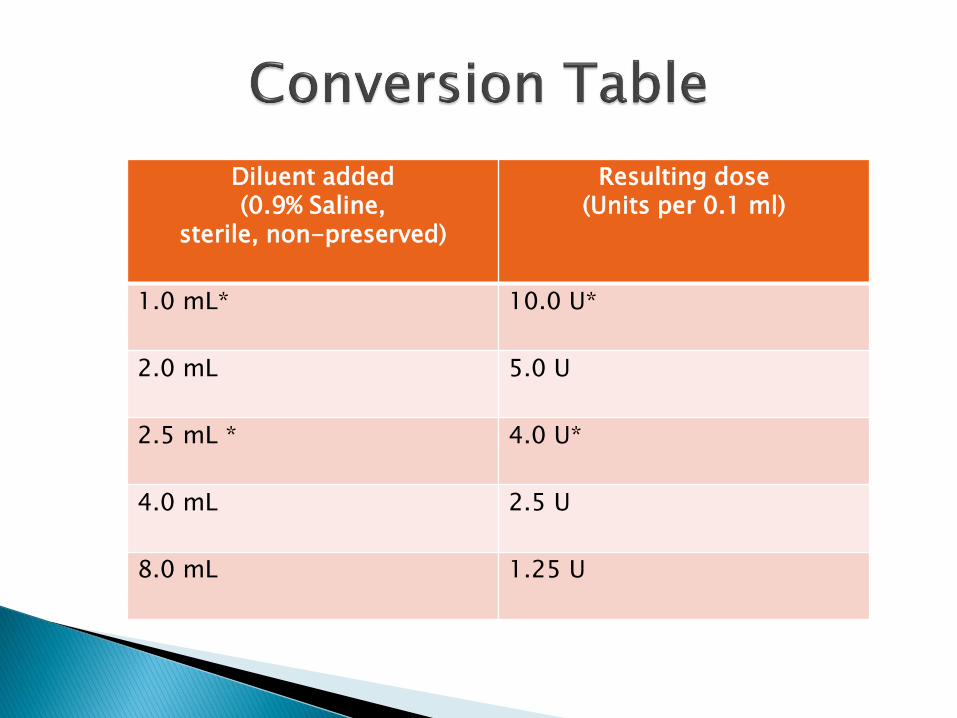
Diluent added(0.9% Saline,
sterile, non-preserved)
Resulting dose(Units per 0.1 ml)
1.0 mL* 10.0 U*
2.0 mL 5.0 U
2.5 mL * 4.0 U*
4.0 mL 2.5 U
8.0 mL 1.25 U
Consensus Recommendations
The manufacturing process is slightly different, which leads to some potential, subtle differences in clinical practice.
Some people feel that Dysport® may provide a slightly faster onset of action (24 hours versus 72 hours for Botox®).
It is important to know that the unit size of Dysport® is smaller than the unit size of Botox®.
According to the FDA, it takes a minimum of two times more units of Dysport® to get the same effect as Botox®. So, if the patient has opted for Botox® and received 20 units, the same patient will need 40 units of Dysport® for an equivalent treatment. (Cost for Botox® @ $9.99 per unit vs. Dysport® @ $3.99 per unit). However among physicians, it has been debated, yet somewhat accepted, that 1 unit of Botox is “similar” to 2.5 or 3 units of Dysport.
Dysport® has been shown to “drift” or diffuse more than Botox®, increasing the chances of an accidental droopy eyelid or unintentional relaxation of a neighboring muscle due to diffusion of the product.
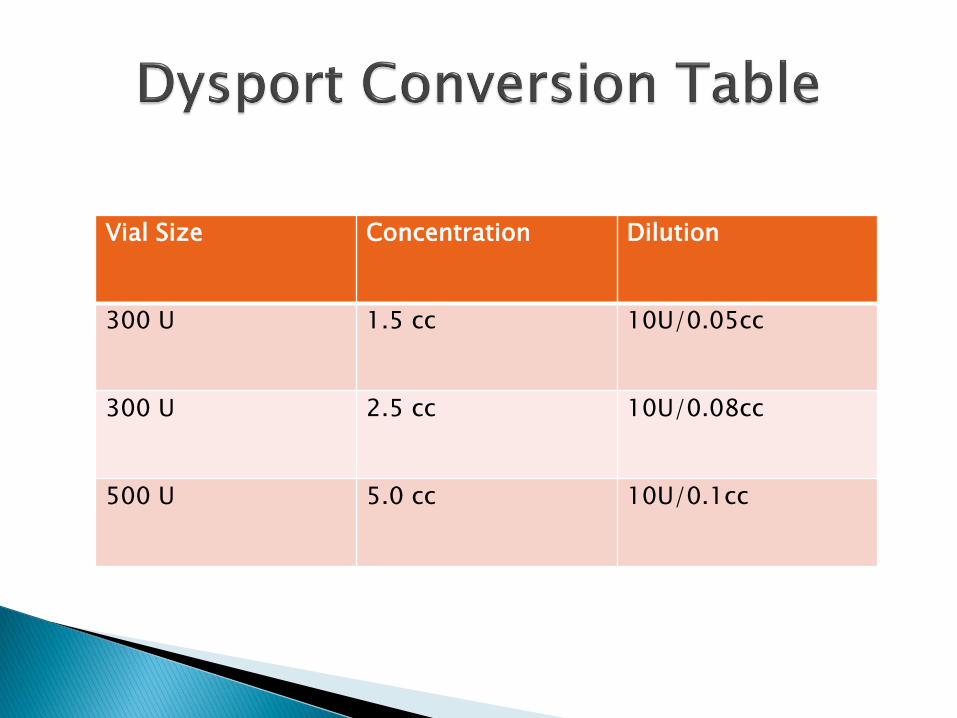
Vial Size Concentration Dilution
300 U 1.5 cc 10U/0.05cc
300 U 2.5 cc 10U/0.08cc
500 U 5.0 cc 10U/0.1cc
Digital camera.
Soft eyeliner pencil (only if marking).
Botox-vial & preserved saline (0.9% NaCL).
Bottle opener (remove rubber stopper of vial).
30 gauge ½ inch needle (for drawing larger gauge).
For skin preparation & sterility: alcohol (wipes), gloves, cotton balls, 4x4 sterile gauze.
Ice (pack) pre/post tx.
Syringes:
◦ 1ml syringes.
Needles:
◦ 30 gauge ½ inch needles to administer.
◦ 21-25 gauge (1/2 – 1 inch) for mixing and drawing up solution.

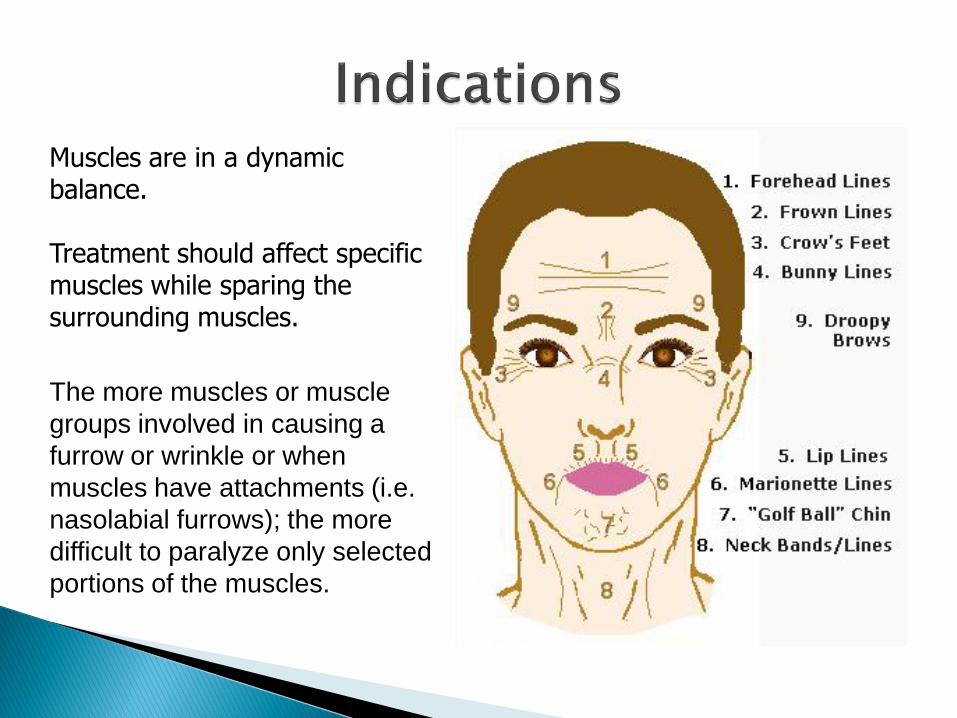
Muscles are in a dynamic balance.
Treatment should affect specific muscles while sparing the surrounding muscles.
The more muscles or muscle
groups involved in causing a
furrow or wrinkle or when
muscles have attachments (i.e.
nasolabial furrows); the more
difficult to paralyze only selected
portions of the muscles.
Have an infection where BOTOX® Cosmetic will be injected (eyelids).
Are allergic to any of the ingredients in BOTOX®
Cosmetic (eg. Albumin/egg allergy).
Serious preexisting disease : DM1 or DM2 (not controlled), CHF, uncompensated CAD, RA/SLE etc.
Blood donors (can‟t donate after BOTOX® for a period of time determined by the blood bank).
Underage clients (need parental consent).
Any diseases that affect your nerves and cause a generalized impairment of muscle strength (i.e. myasthenia gravis, Eaton-Lambert syndrome). These diseases may increase your chance of side effects with BOTOX® Cosmetic treatment.
Pregnant or planning to become pregnant soon.
Breastfeeding.
Antibiotics used to treat infections, such as gentamicin, tobramycin, clindamycin, and lincomycin.
Treatment with A.S.A. or other non-steroidal anti-inflammatory drugs 1 week prior to Tx (patient more likely to bruise or bleed).
Medicines used to treat heart rhythm problems, such as quinidine; and anti-coagulants (coumadine).
Medicines used to treat different conditions, such as myasthenia gravis or Alzheimer‟s disease.
Any over-the-counter medicines or herbal products.
This is not a complete list of medicines that can interact with BOTOX® Cosmetic. Review the Professional Package Insert for complete information.
Glabellar frown lines
Horizontal forehead lines
Crow‟s feet
Note: age-related loss of dermal elasticity versus hyperactivity of facial muscles
Assessment:◦ Identify hyperkinetic lines by asking patient to
make facial expressions (maximal smiling and frowning).
◦ The novice can use a soft eyeliner pencil to mark hyperkinetic lines.
Treatment:◦ Reconstitute vial of BTX if indicated.
◦ Desired dose of BTX is drawn into the syringe.
◦ Follow standard procedures to ensure sterility and skin preparation.
◦ No anesthesia necessary; ice post-tx.
If alcohol is used, make sure injection site is completely dry prior to injection (alcohol can interfere with toxin).
Injection is site-specific (in mass of facial muscle, not necessary the hyperkinetic line) and IM (some exceptions apply to reduce bruising).
Multiple injections may be necessary (less diffusion in corrugator and orbicularis oculi than in frontalis).
Injection techniques:◦ Have client make facial expression (frown, squint,
smile etc.) and inject during facial expression; or
◦ Have client make facial expression, let client relax and inject; or
◦ Have client make facial expression, mark the muscle mass (eyeliner or paper reinforcement stickers), let client relax and inject; or
◦ Palpate muscle mass and inject.
◦ Inject into muscle mass (belly), if not sure go deep to the periosteum and slightly retract needle (pain).
Frontalis: superfical injections (frontalis not attached to skull).
Crow‟s feet: superficial injections (avoid bruising).
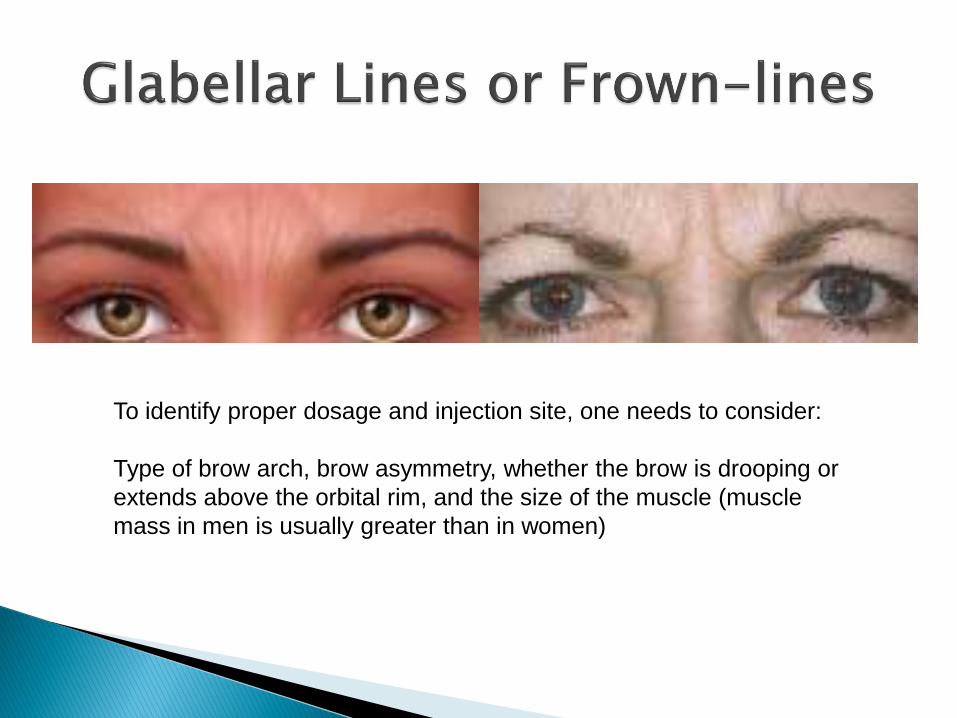
To identify proper dosage and injection site, one needs to consider:
Type of brow arch, brow asymmetry, whether the brow is drooping or
extends above the orbital rim, and the size of the muscle (muscle
mass in men is usually greater than in women)
Common doses to treat glabellar frown lines is 40-60 units for males and 20-40 units for females.
If more units are indicated, one can reduce the total volume by reducing the amount of saline used to reconstitute the BTX.
Patient seated position.
Regardless the brow position, the injections are always above or outside of the supra-orbital ridge.
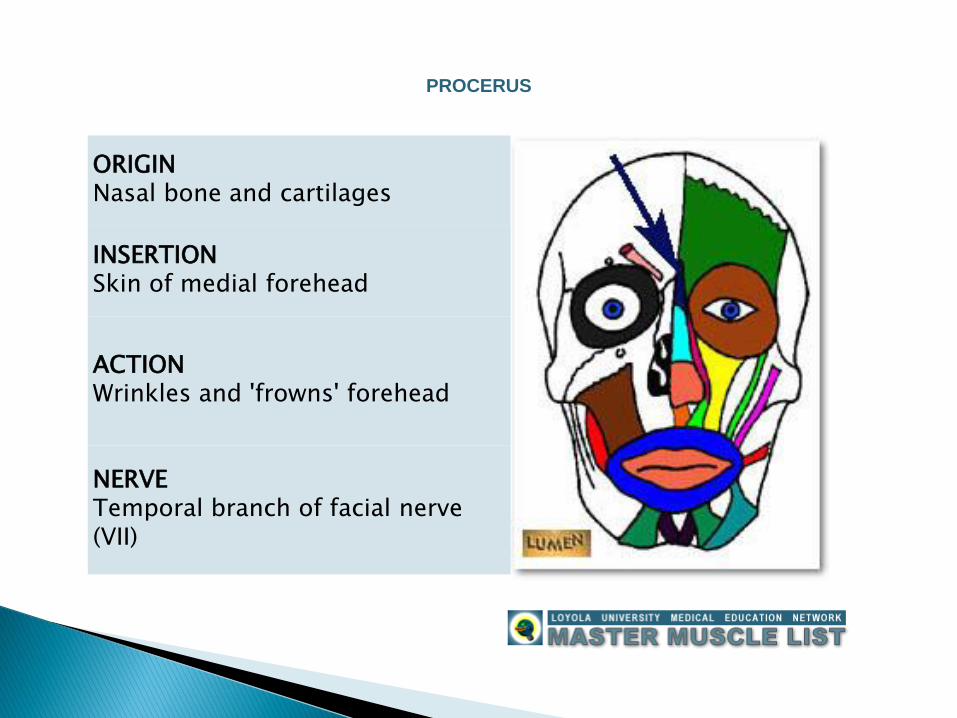
ORIGINNasal bone and cartilages
INSERTIONSkin of medial forehead
ACTIONWrinkles and 'frowns' forehead
NERVETemporal branch of facial nerve (VII)
PROCERUS
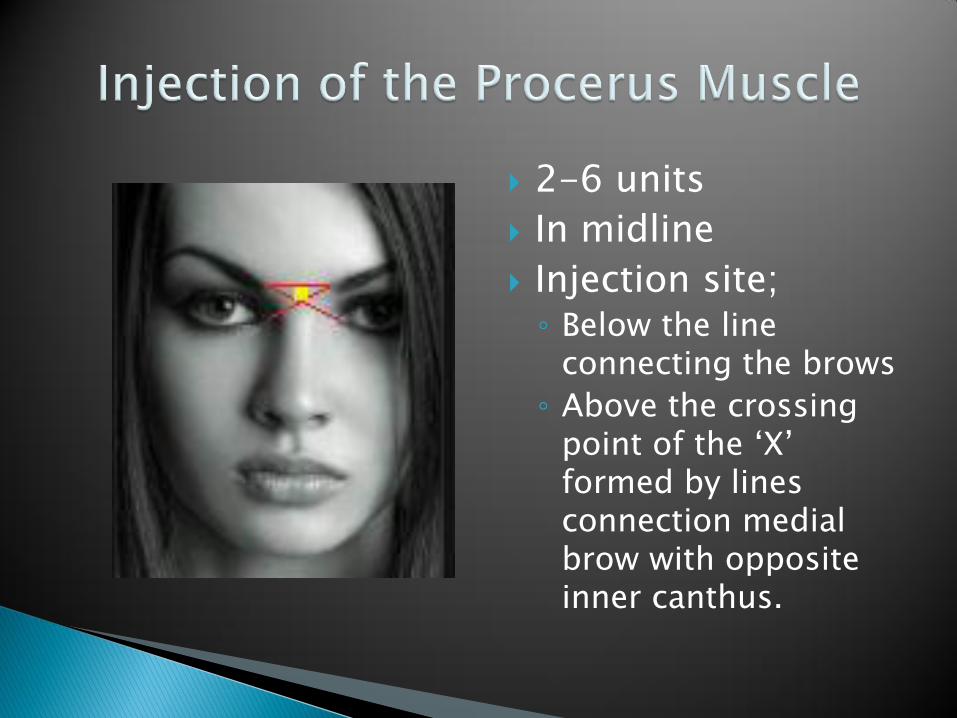
2-6 units
In midline
Injection site;◦ Below the line
connecting the brows
◦ Above the crossing point of the „X‟ formed by lines connection medial brow with opposite inner canthus.
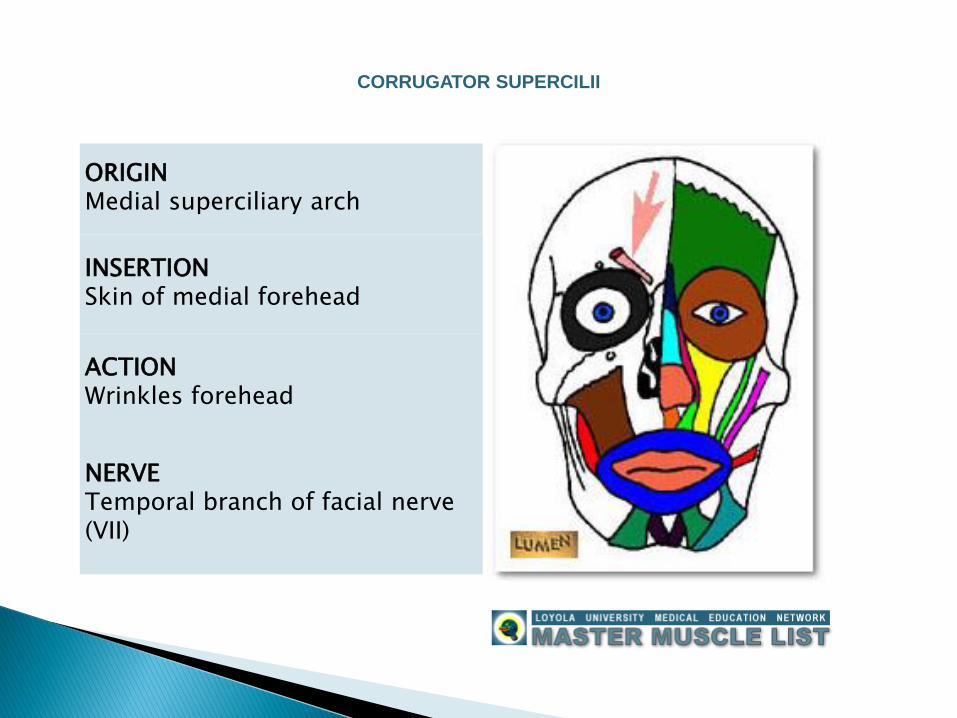
ORIGINMedial superciliary arch
INSERTIONSkin of medial forehead
ACTIONWrinkles forehead
NERVETemporal branch of facial nerve (VII)
CORRUGATOR SUPERCILII
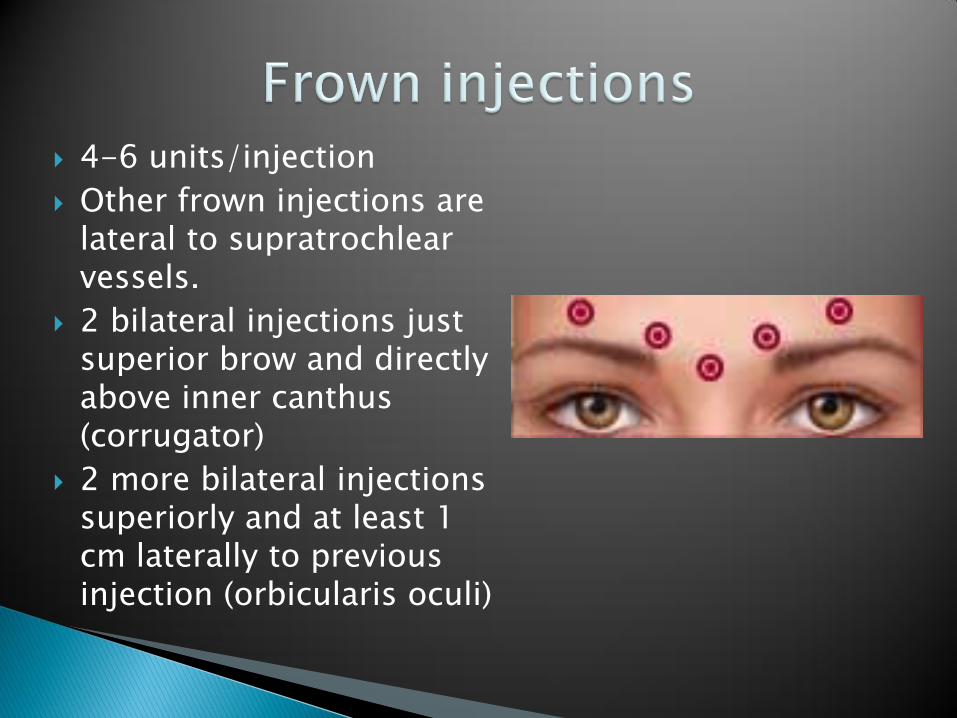
4-6 units/injection
Other frown injections are lateral to supratrochlear vessels.
2 bilateral injections just superior brow and directly above inner canthus (corrugator)
2 more bilateral injections superiorly and at least 1 cm laterally to previous injection (orbicularis oculi)
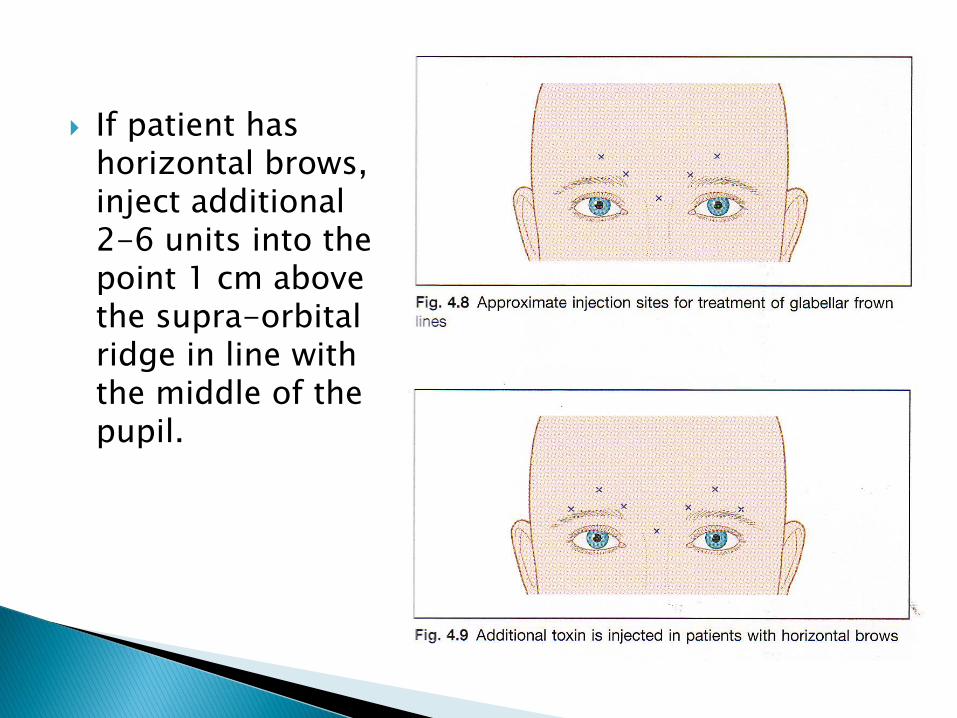
If patient has horizontal brows, inject additional 2-6 units into the point 1 cm above the supra-orbital ridge in line with the middle of the pupil.
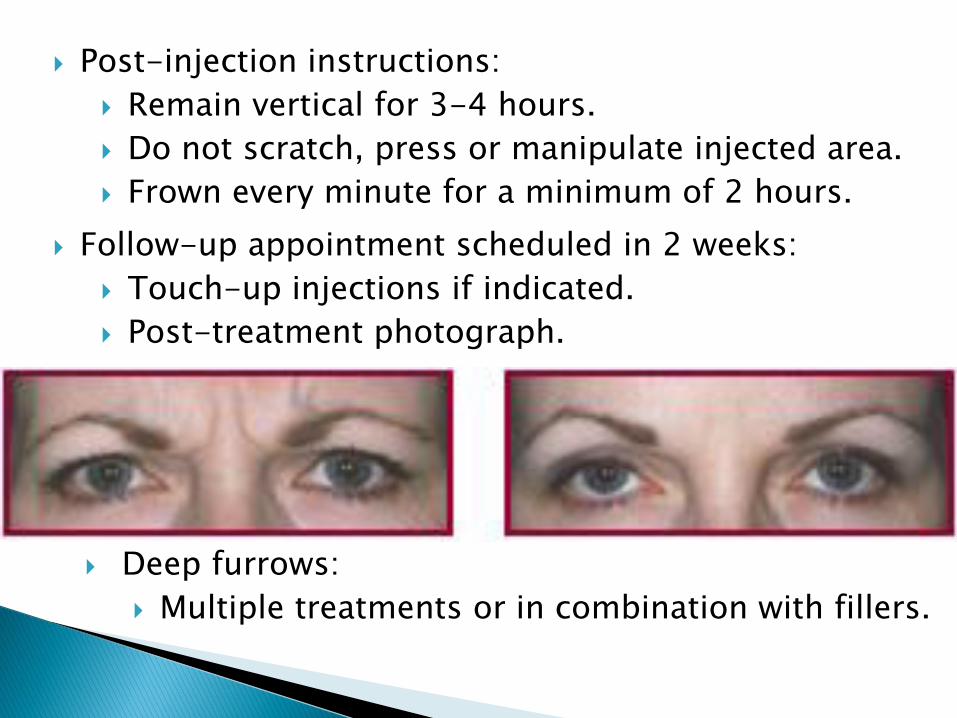
Post-injection instructions:
Remain vertical for 3-4 hours.
Do not scratch, press or manipulate injected area.
Frown every minute for a minimum of 2 hours.
Follow-up appointment scheduled in 2 weeks:
Touch-up injections if indicated.
Post-treatment photograph.
Deep furrows:
Multiple treatments or in combination with fillers.
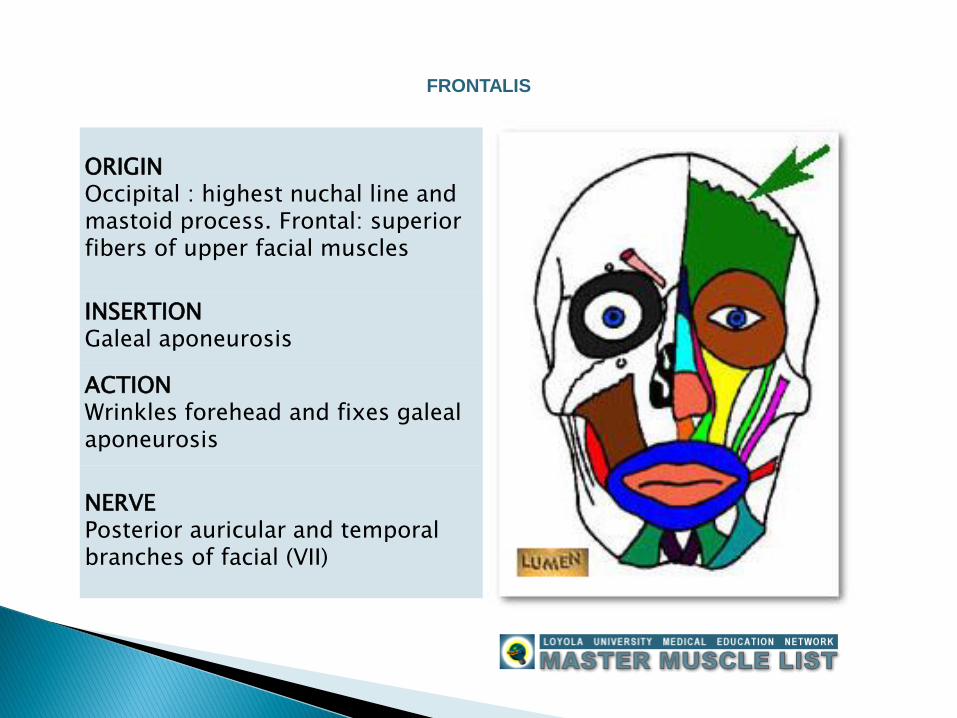
ORIGINOccipital : highest nuchal line and mastoid process. Frontal: superior fibers of upper facial muscles
INSERTIONGaleal aponeurosis
ACTIONWrinkles forehead and fixes galeal aponeurosis
NERVEPosterior auricular and temporal branches of facial (VII)
FRONTALIS
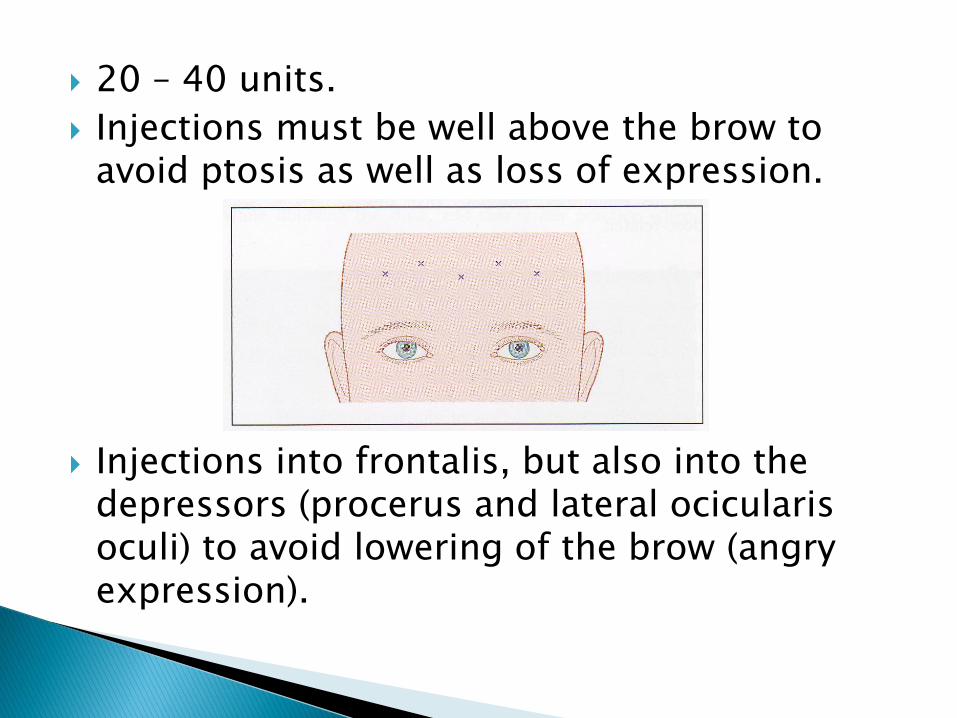
20 – 40 units.
Injections must be well above the brow to avoid ptosis as well as loss of expression.
Injections into frontalis, but also into the depressors (procerus and lateral ocicularis oculi) to avoid lowering of the brow (angry expression).
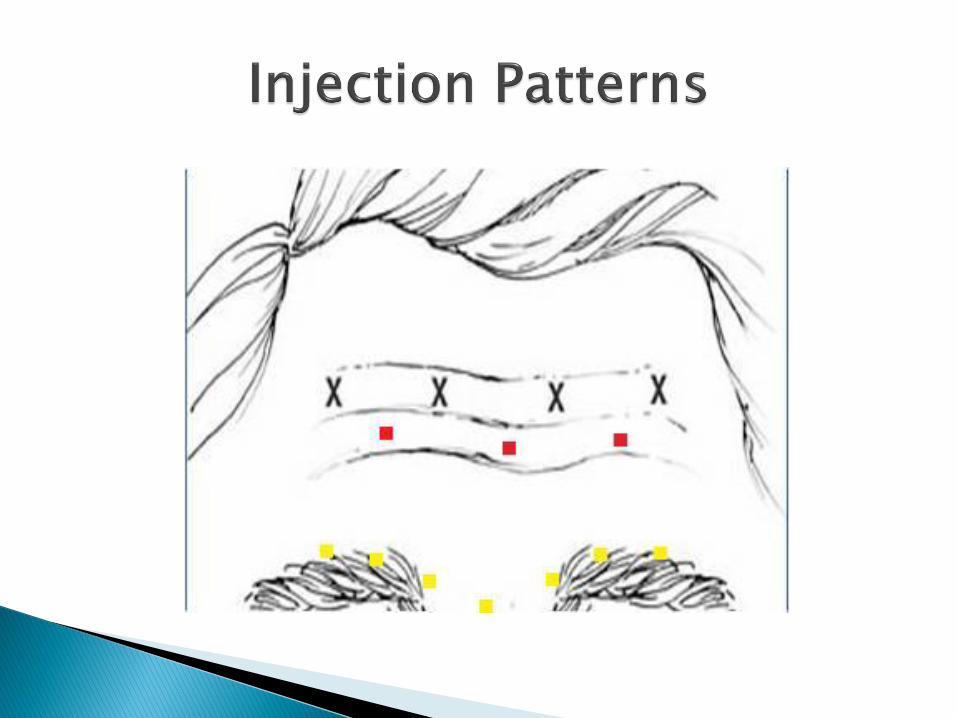
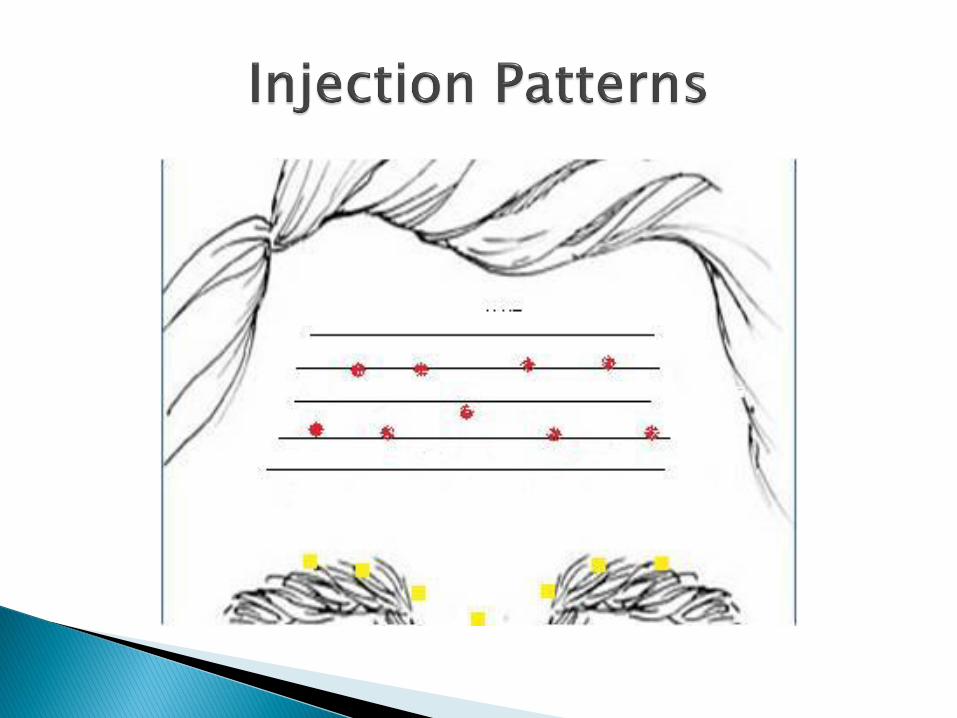
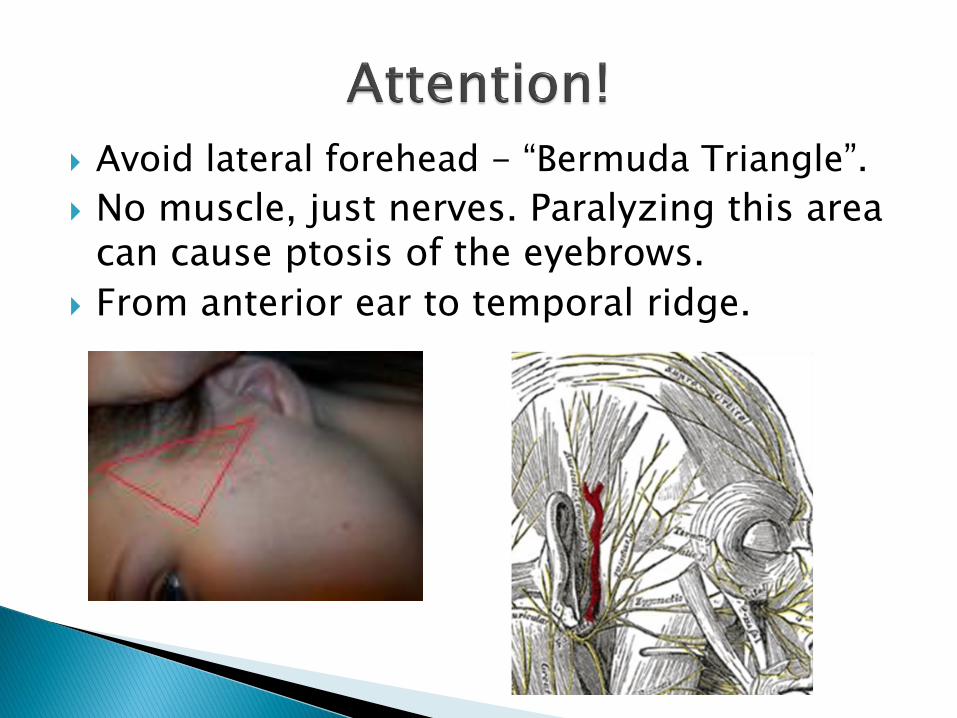
Avoid lateral forehead - “Bermuda Triangle”.
No muscle, just nerves. Paralyzing this area can cause ptosis of the eyebrows.
From anterior ear to temporal ridge.
“Spa Brow” (raising lateral brow)
Commonly seen as a result of treating the glabella and/or forehead lines:◦ Injections are only administered to the frontal plane
of the forehead, therefore paralyzing the frontal part of the frontalis muscle.
◦ The lateral part is not injected (“bermuda triangle”) and the increase in tone results in a lateral brow lift.
Eyebrow position and shape:◦ Can be influenced by the dosage injected in the
frontalis muscle. Moving the treatment area more medially or laterally can effect eyebrow shape.
◦ Treatment of eyebrow asymmetry is possible.
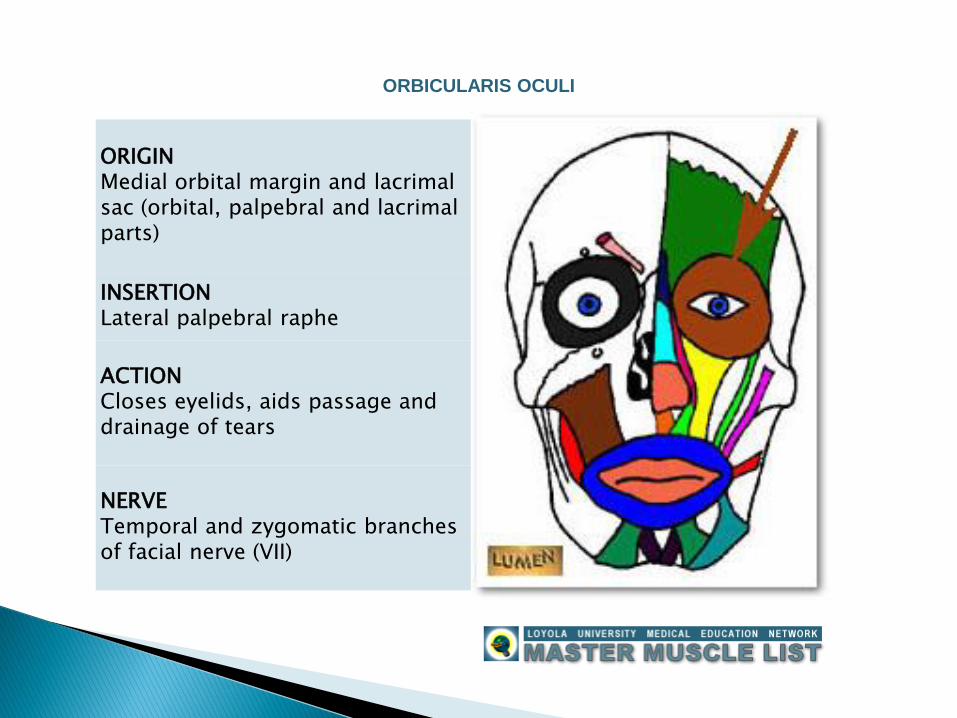
ORIGINMedial orbital margin and lacrimalsac (orbital, palpebral and lacrimalparts)
INSERTIONLateral palpebral raphe
ACTIONCloses eyelids, aids passage and drainage of tears
NERVETemporal and zygomatic branches of facial nerve (VII)
ORBICULARIS OCULI
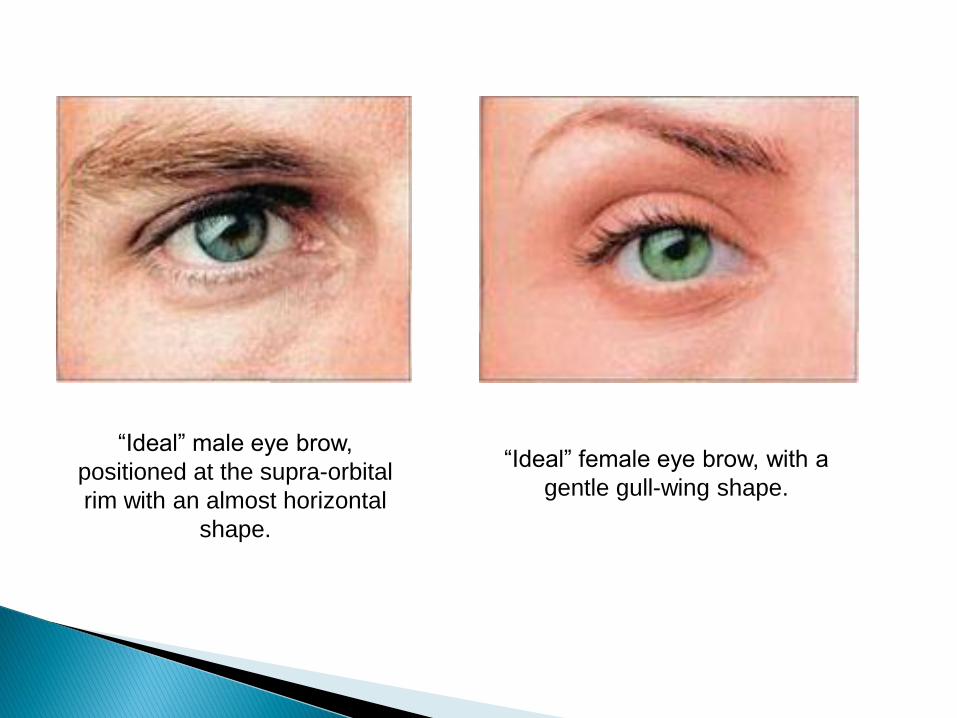
“Ideal” male eye brow,
positioned at the supra-orbital
rim with an almost horizontal
shape.
“Ideal” female eye brow, with a
gentle gull-wing shape.
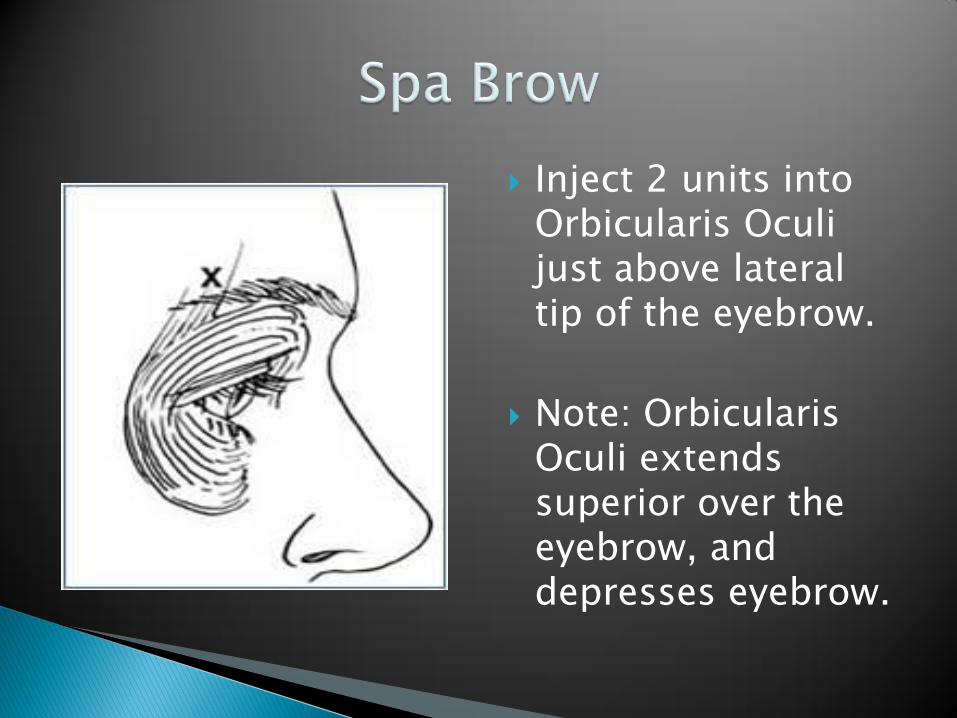
Inject 2 units into Orbicularis Oculi just above lateral tip of the eyebrow.
Note: Orbicularis Oculi extends superior over the eyebrow, and depresses eyebrow.

Courtesy of Allure Medica
Courtesy of Mark Berkowitz
Crow‟s feet
2-3 injections into the lateral Orbicularis Oculi muscle, lateral to the lateral orbital rim.
Equal doses of 2-6 units/injection site (or a total of 6-18 units/eye) are administered.
Few and superficial injections recommended to prevent bruising.
Have the client smile maximally and identify the center of the crow‟s feet; this is your 1st injection site (approximately 1-2cm lateral to the lateral orbital rim).
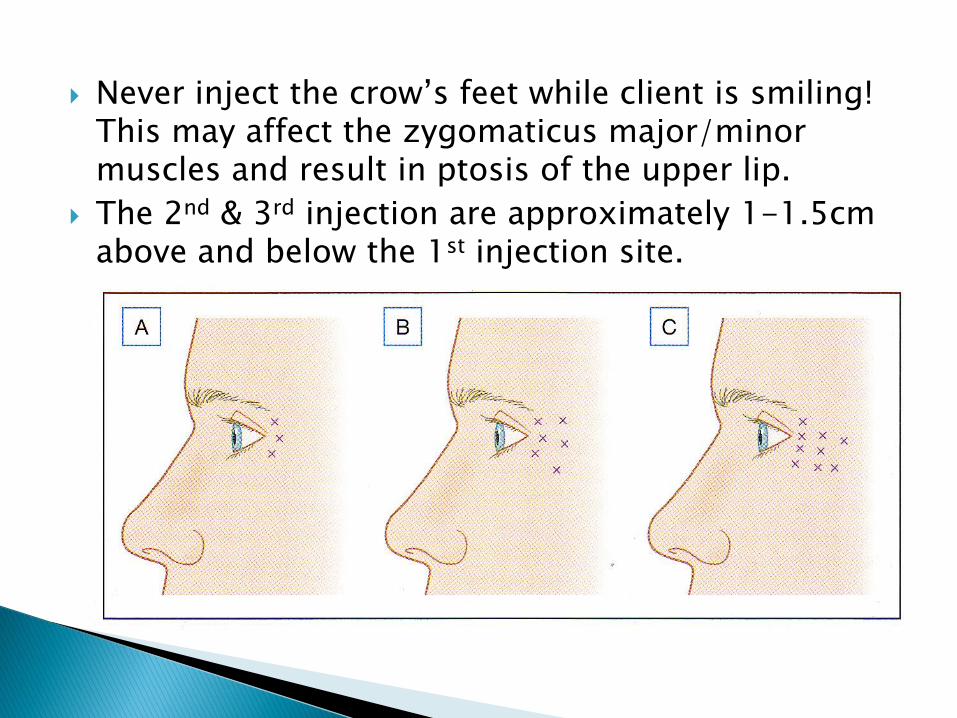
Never inject the crow‟s feet while client is smiling! This may affect the zygomaticus major/minor muscles and result in ptosis of the upper lip.
The 2nd & 3rd injection are approximately 1-1.5cm above and below the 1st injection site.

Attention: Due to the baggy, loose skin under the eyes, BTX may migrate
into unwanted area’s and cause drooping op the mouth (by affecting the
levator labii superior and consequently the levator anguli oris).
Under the eyes
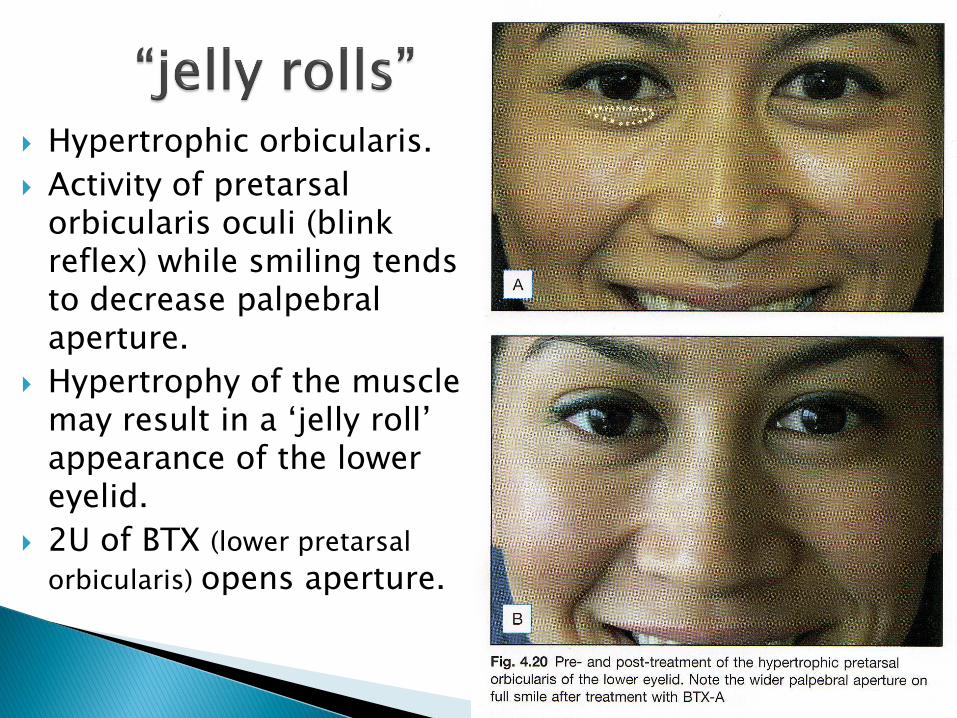
Hypertrophic orbicularis.
Activity of pretarsal orbicularis oculi (blink reflex) while smiling tends to decrease palpebral aperture.
Hypertrophy of the muscle may result in a „jelly roll‟ appearance of the lower eyelid.
2U of BTX (lower pretarsal
orbicularis) opens aperture.
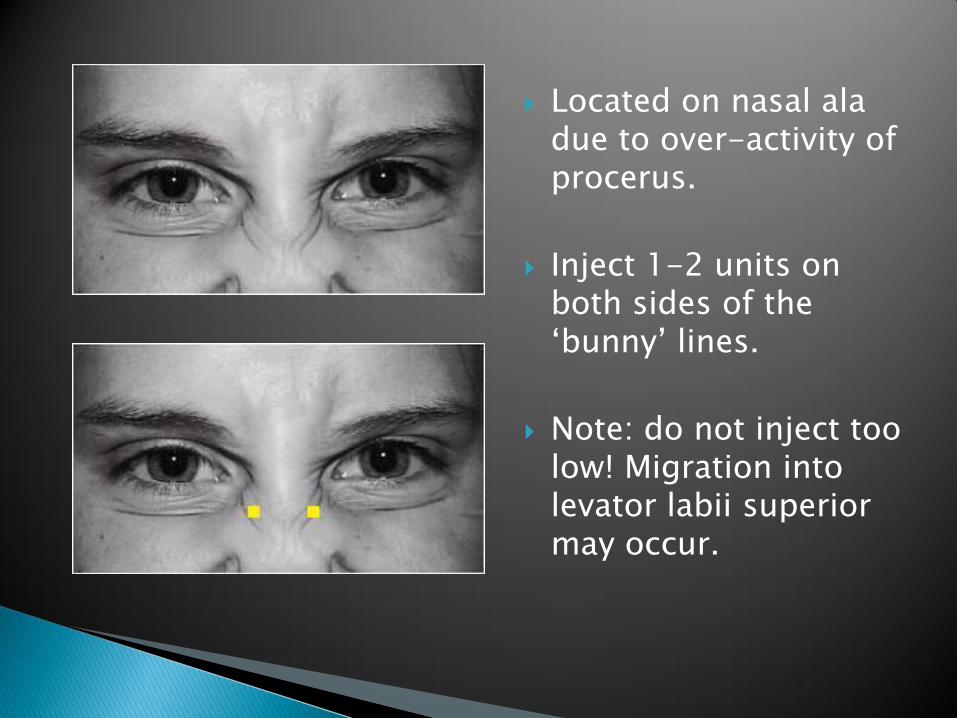
Located on nasal ala due to over-activity of procerus.
Inject 1-2 units on both sides of the „bunny‟ lines.
Note: do not inject too low! Migration into levator labii superior may occur.
Spasm of lower eyelids
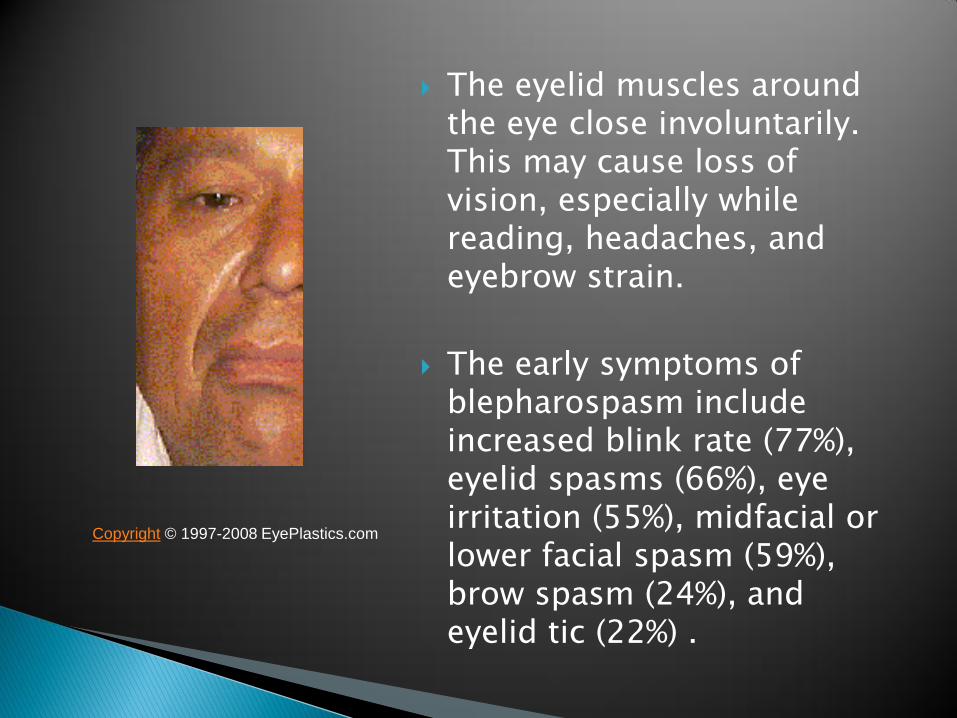
The eyelid muscles around the eye close involuntarily. This may cause loss of vision, especially while reading, headaches, and eyebrow strain.
The early symptoms of blepharospasm include increased blink rate (77%), eyelid spasms (66%), eye irritation (55%), midfacial or lower facial spasm (59%), brow spasm (24%), and eyelid tic (22%) .
Copyright © 1997-2008 EyePlastics.com
Medical Therapy:
◦ Anticholinergics have been the most common and effective drugs with GABA-ergic drugs as the second most effective group.
Anderson procedure (1970's): Dr. Rick Anderson described a procedure called "full myectomy" in which the surgeon meticulously excises virtually all of the orbicularis muscle as well as the corrugator superciliaris and procerus muscles.
BTX-A approved in 1989 by the FDA and replaced a full myectomy procedure as the treatment of choice.
BTX-A:
◦ Long-term follow-up studies have shown it to be a very safe and effective treatment, with up to 90 percent of patients obtaining almost complete relief of their blepharopspam.
◦ Side effects include ptosis, blurred vision, and double vision (diplopia). Lagophthalmos, ectropion, sagging of the mouth, brow droop, epiphora.
◦ The sites of the injection will vary slightly from patient to patient and according to physician preference.
◦ The injection is usually given on the eyelid, the brow, and the muscles under the lower lid.
Upper Face
BTX-A safety well established:◦ Extremely safe
◦ NO long-term side-effects or health hazards
Adverse reactions are mild & temporary:◦ Local bruising, erythema and swelling, mild
headache, flu-like symptoms
Poor injection technique
Poor patient selection
Neglect of post-treatment instructions
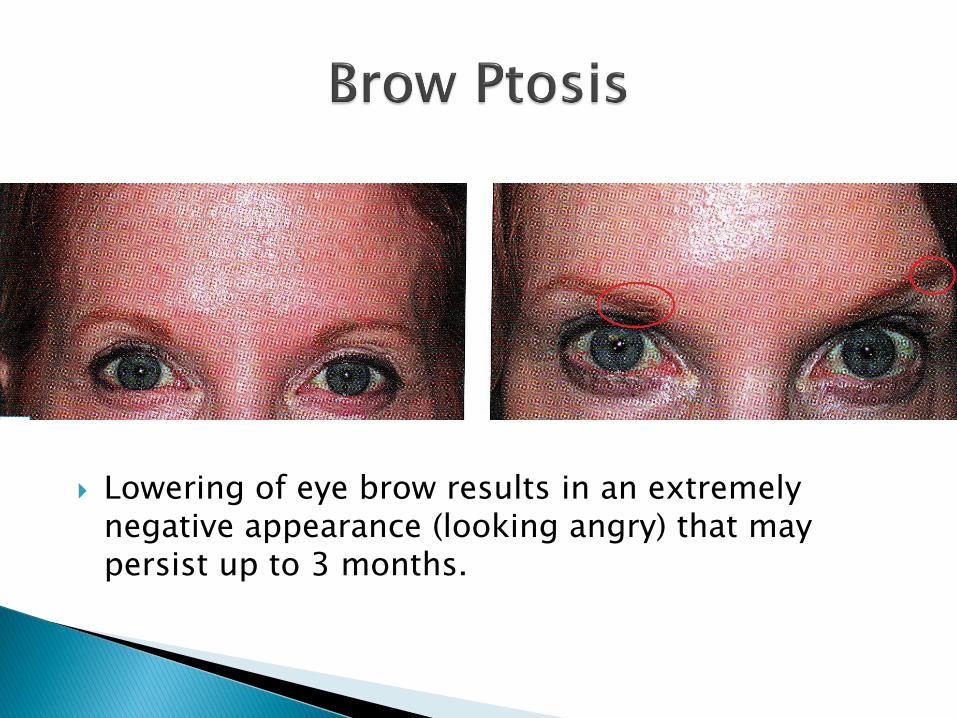
Lowering of eye brow results in an extremely negative appearance (looking angry) that may persist up to 3 months.
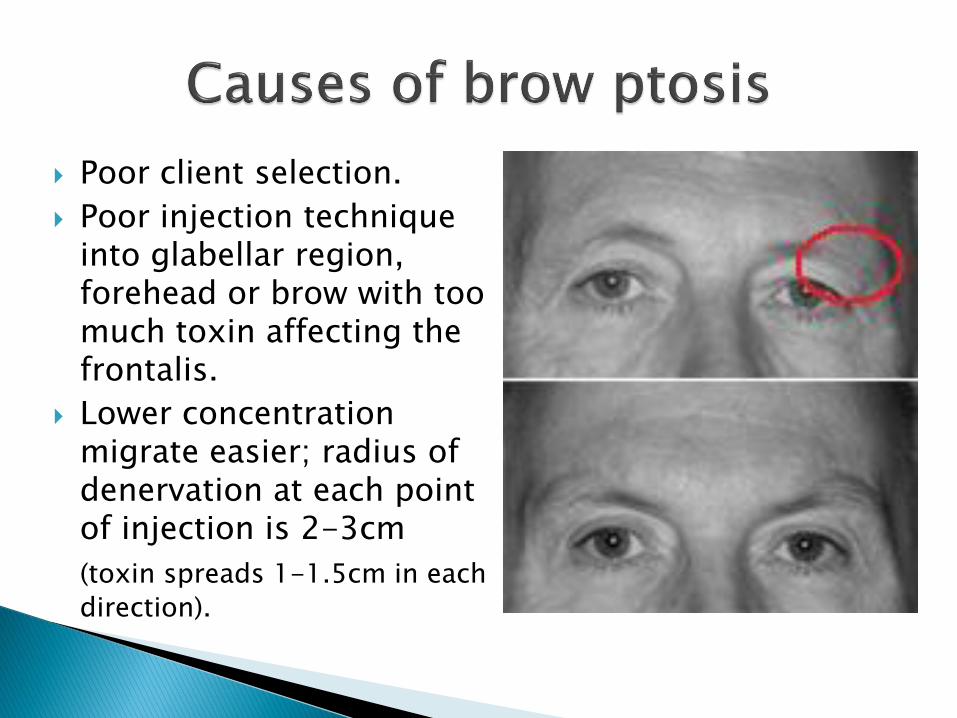
Poor client selection.
Poor injection technique into glabellar region, forehead or brow with too much toxin affecting the frontalis.
Lower concentration migrate easier; radius of denervation at each point of injection is 2-3cm
(toxin spreads 1-1.5cm in each
direction).
Plenty experience/practice.
Importance of post-treatment instructions.
Use higher concentrations (dilute with 1.0ml saline).
Appropriate client selection: avoid injecting frontalis in clients with significant brow ptosis!
Pre-injection of brow depressors if indicated (clients with low-set brows/mild ptosis and older clients).
Inject frontalis above lowest fold when client elevates frontalis or 3 cm above brow.
Inject glabella and forehead in multiple sessions.
Post-treatment instructions + Lean head back.
No effective treatment!
Evident 48 hours – 14 days post-injection.
May last 2 – 12 weeks.
Causes:◦ Poor technique: toxin diffuses through orbital
septum and effects elevators of eyelid; usually with treatment of glabellar complex.
Prevention:◦ Accurate technique: injections no closer than 1 cm
above the central bony orbital rim; no injections at or under the mid-brow!
◦ Post-treatment instructions.
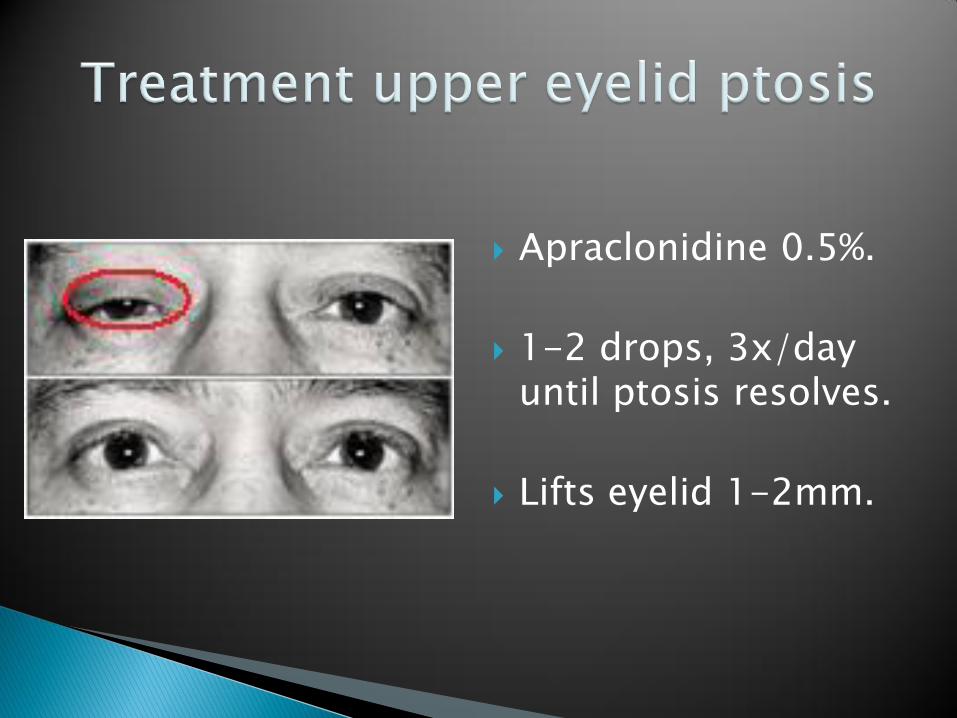
Apraclonidine 0.5%.
1-2 drops, 3x/day until ptosis resolves.
Lifts eyelid 1-2mm.
Apraclonidine (Iopidine 0.5%):
◦ Alpha-adenergic agonist ophthalmic eye drops.
◦ Stimulate Müller‟s muscle. Compensates for weakness of levator palpebrae superioris.
This is a short muscle controlled by the sympathetic nerves of the body. It generally is contracted while you are awake so that it lifts the eyelid. When tired or asleep, it is relaxed letting the eyelid sag and droop. The eyelids can now close with minimal orbicularis tone.
◦ Disguises eyelid ptosis.
◦ Allergic contact conjunctivitis may occur with long-term use.
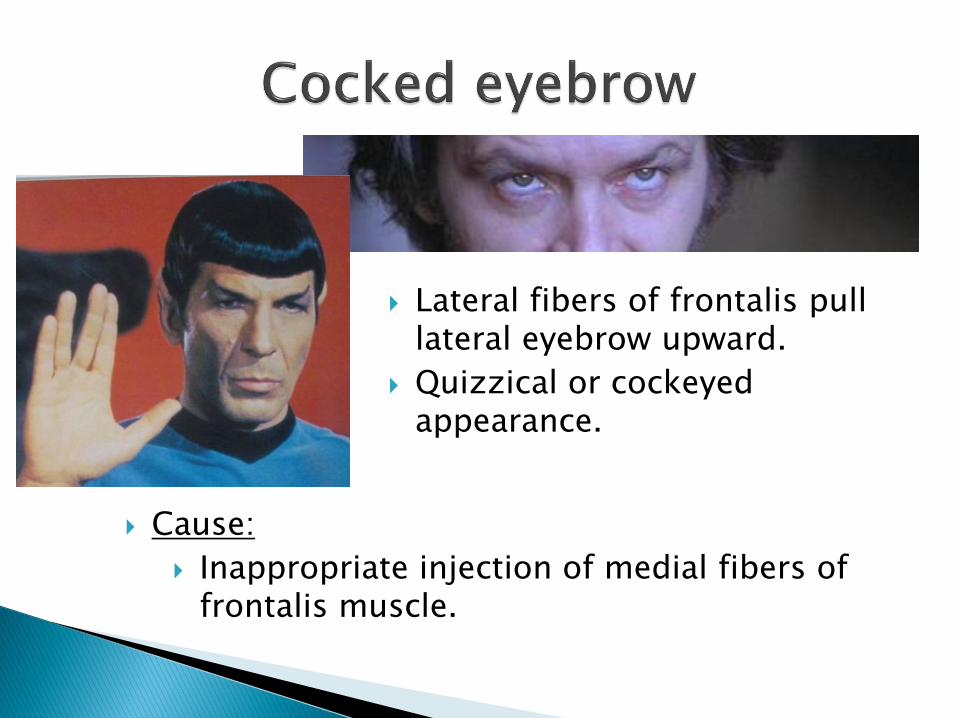
Lateral fibers of frontalis pull lateral eyebrow upward.
Quizzical or cockeyed appearance.
Cause:
Inappropriate injection of medial fibers of frontalis muscle.
Prevention:◦ Keep glabellar treatments more medial with future
treatments so the increased tone in frontalis causes a smooth arch to the brow.
Treatment:◦ 2-3 units of BTX into the fibers of lateral forehead.
◦ Caution: overcompensation may result in an irreversible and unsightly hooded brow that partially covers the eye!
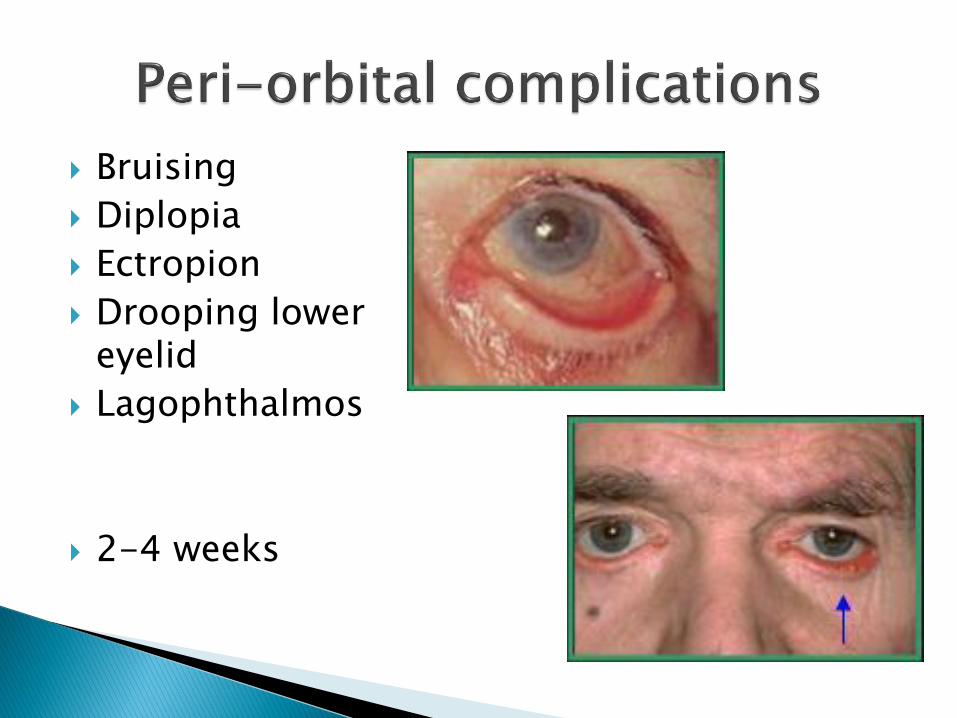
Bruising
Diplopia
Ectropion
Drooping lower eyelid
Lagophthalmos
2-4 weeks
Inject superficially (blebs); not IM.
Inject 1cm outside bony orbit, or 1.5 cm lateral to lateral canthus.
Do not inject close to inferior margin of zygoma.
Use ice pre-and post-treatment.
Use pressure post treatment.
Use arnica or traumeel post-treatment.

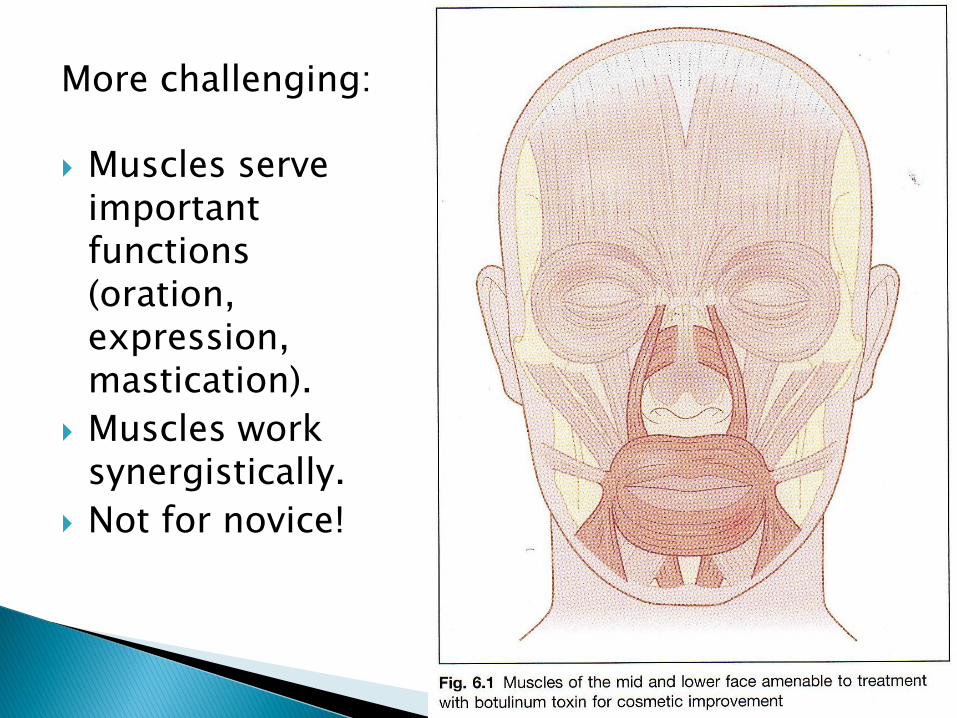
More challenging:
Muscles serve important functions (oration, expression, mastication).
Muscles work synergistically.
Not for novice!
And „smoker lines‟
Hypertrophic orbicularis oris; intensified by age, sun expore and smoking (using straw).
BTX is good treatment for mild wrinkles; for moderate wrinkles use bTX in combination with fillers, chemical peels and/or laser resurfacing.
BTX by itself can cause lip eversion resulting in more upper lip fullness.
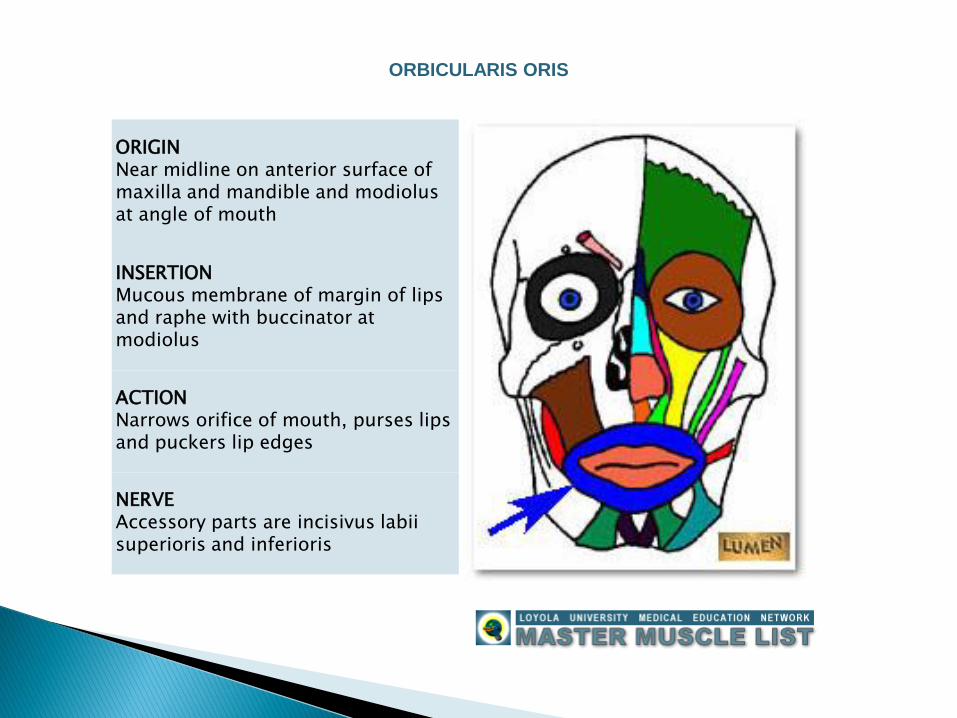
ORIGINNear midline on anterior surface of maxilla and mandible and modiolus at angle of mouth
INSERTIONMucous membrane of margin of lips and raphe with buccinator at modiolus
ACTIONNarrows orifice of mouth, purses lips and puckers lip edges
NERVEAccessory parts are incisivus labiisuperioris and inferioris
ORBICULARIS ORIS
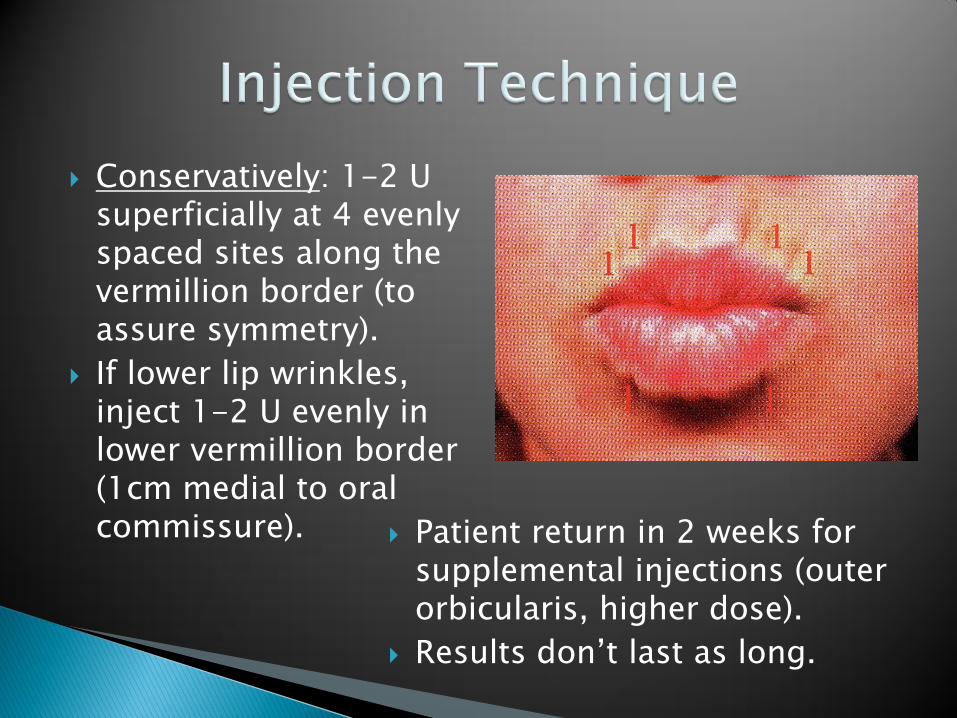
Conservatively: 1-2 U superficially at 4 evenly spaced sites along the vermillion border (to assure symmetry).
If lower lip wrinkles, inject 1-2 U evenly in lower vermillion border (1cm medial to oral commissure). Patient return in 2 weeks for
supplemental injections (outer orbicularis, higher dose).
Results don‟t last as long.
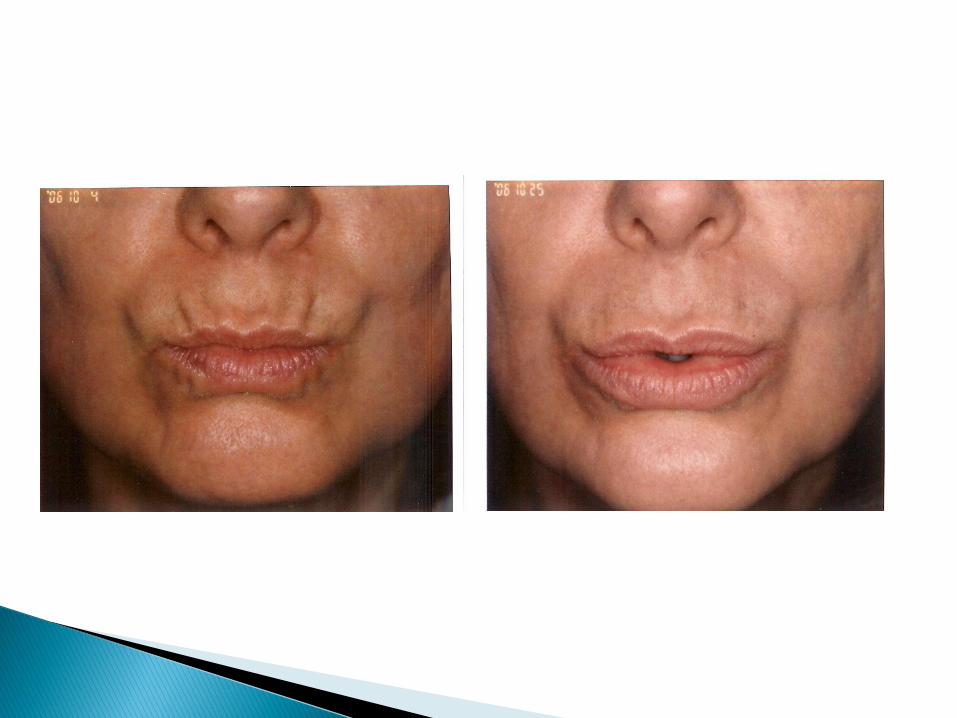
Difficulty with swishing and spitting, puckering, sipping from a straw, whistling, kissing, and pronouncing letters „p‟ and „b‟.
Sphincter dysfunction = dose-specific!
Treat conservatively, assess response and inject more only if indicated!
Asymmetry: plan carefully and inject evenly.
Treatment of the „gummy smile‟
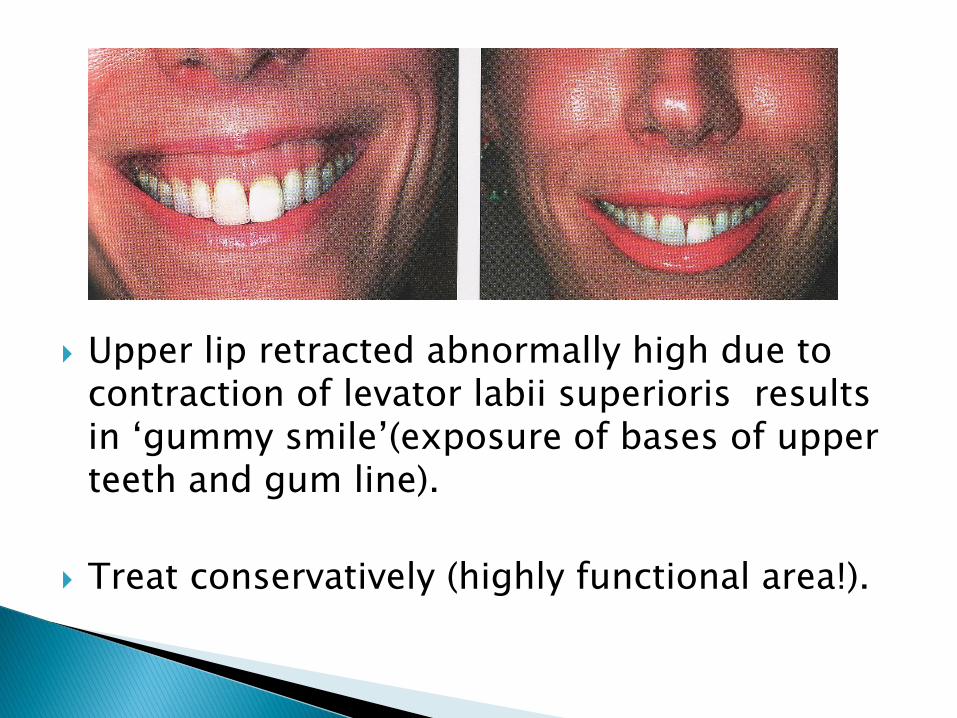
Upper lip retracted abnormally high due to contraction of levator labii superioris results in „gummy smile‟(exposure of bases of upper teeth and gum line).
Treat conservatively (highly functional area!).
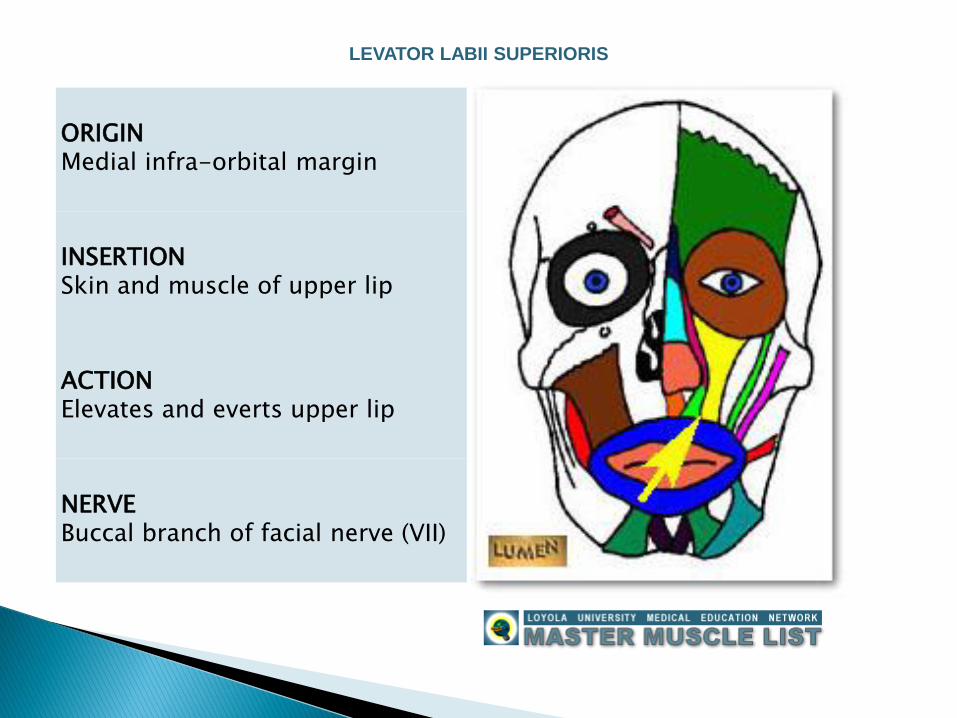
ORIGINMedial infra-orbital margin
INSERTIONSkin and muscle of upper lip
ACTIONElevates and everts upper lip
NERVEBuccal branch of facial nerve (VII)
LEVATOR LABII SUPERIORIS
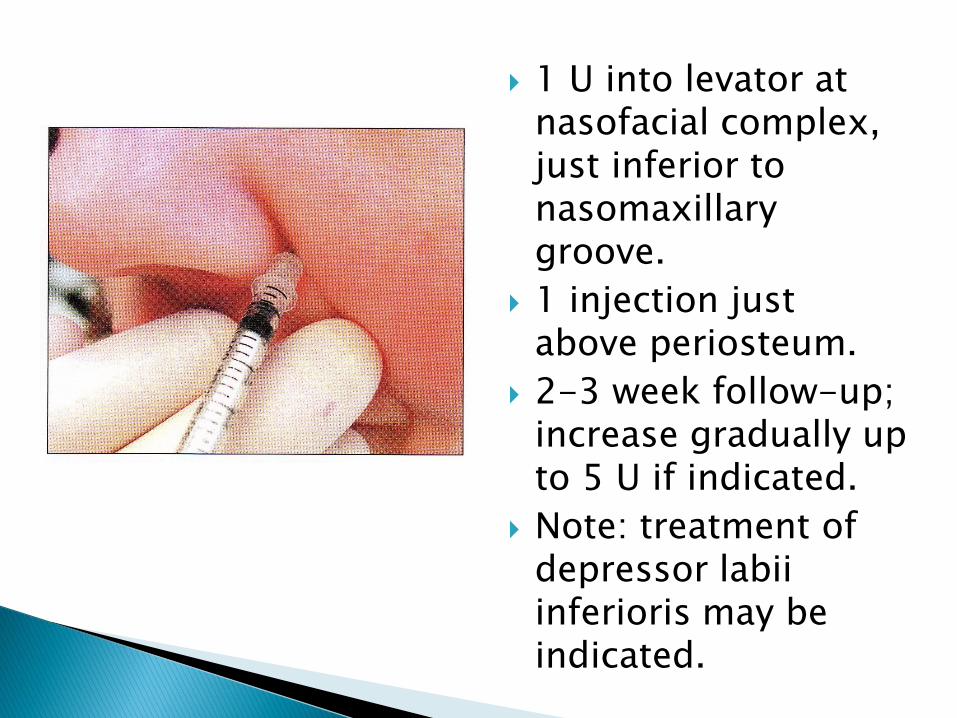
1 U into levator at nasofacial complex, just inferior to nasomaxillarygroove.
1 injection just above periosteum.
2-3 week follow-up; increase gradually up to 5 U if indicated.
Note: treatment of depressor labiiinferioris may be indicated.
Caution:
◦ Client who already exhibits drooped mouth corners!
◦ Asymmetry.
◦ Too high dose may cause:
Upper lip ptosis (takes longer to dissolve: 6 weeks).
Excessive lengthening.
Lower lip protrusion.
BTX indicated for mild to moderate nasolabial fold accentuation.
Controversy:◦ Treatment of levator labii superioris.
Refer to lip lengthening for technique!
Note: this treatment will also lengthen lips!
◦ Treatment of zygomaticus major/minor (caution: disfigured smile).
Other treatment options: dermal fillers, implants, mid-face lift.
“marionette lines”
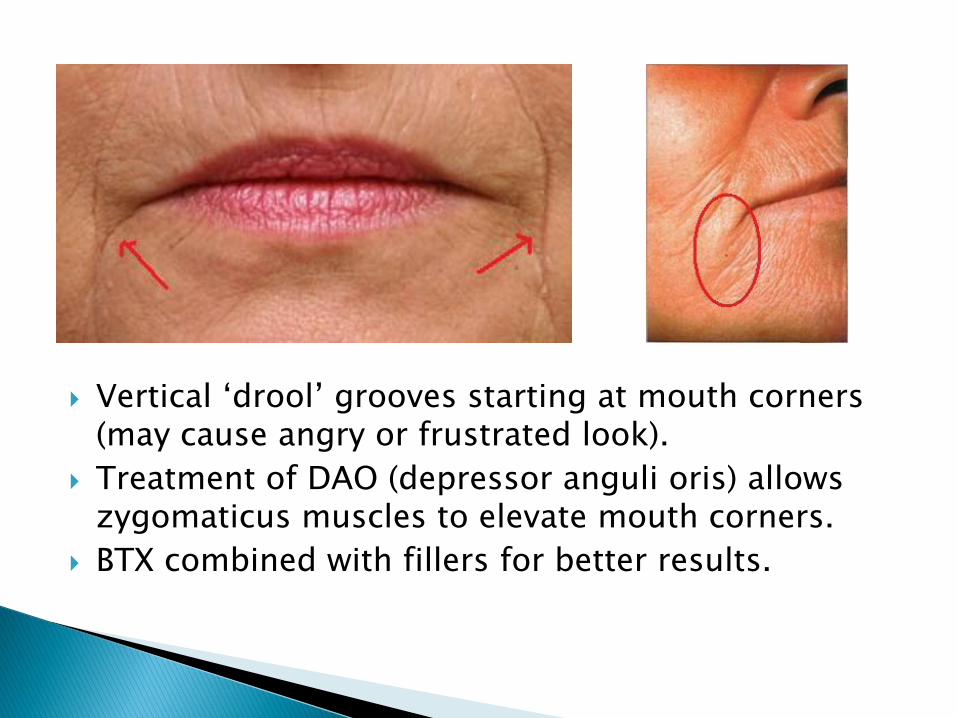
Vertical „drool‟ grooves starting at mouth corners (may cause angry or frustrated look).
Treatment of DAO (depressor anguli oris) allows zygomaticus muscles to elevate mouth corners.
BTX combined with fillers for better results.
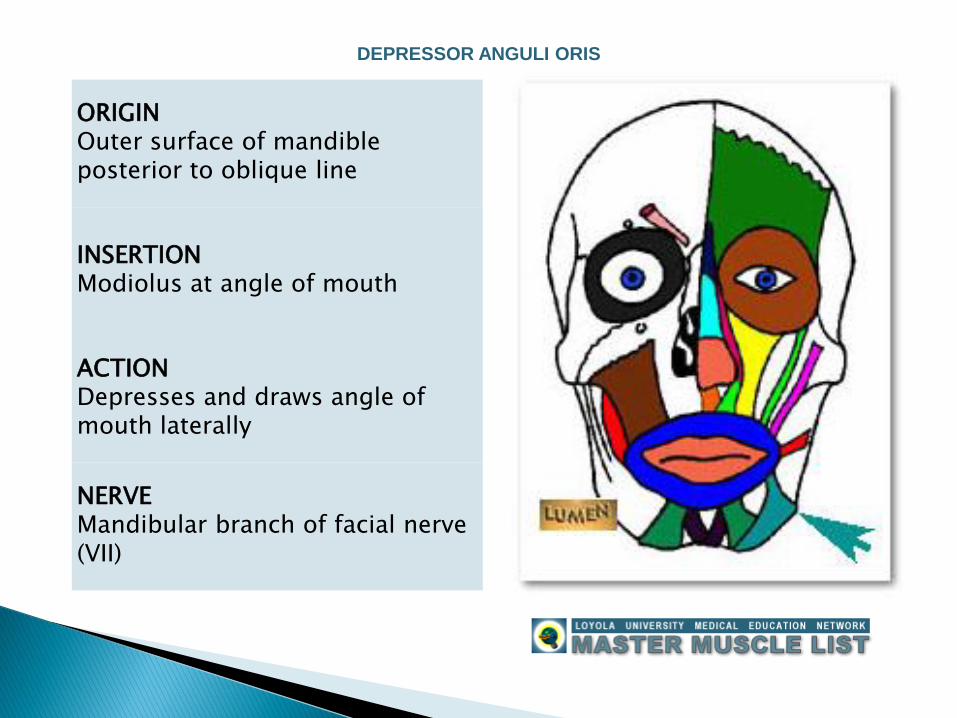
ORIGINOuter surface of mandible posterior to oblique line
INSERTIONModiolus at angle of mouth
ACTIONDepresses and draws angle of mouth laterally
NERVEMandibular branch of facial nerve (VII)
DEPRESSOR ANGULI ORIS
Into mid & lower 1/3 of muscle (intertwined with fibers of platysma).
1-2 U bilaterally:◦ lateral to oral commissure (diffusion into depressor
labii inferior may cause lower lip protrusion).
◦ Medial to buccinator (diffusion into buccinator may predispose client to biting and cause trauma to buccal mucosa).
Optimal results in combination with fillers; BTX will only slightly lift the mouth corners.
“peach pit” chin or “apple dumpling” deformity
ORIGINIncisive fossa on anterior aspect of mandible
INSERTIONSkin of chin
ACTIONElevates and wrinkles skin of chin and protrudes lower lip
NERVEMandibular branch of facial nerve (VII)
MENTALIS
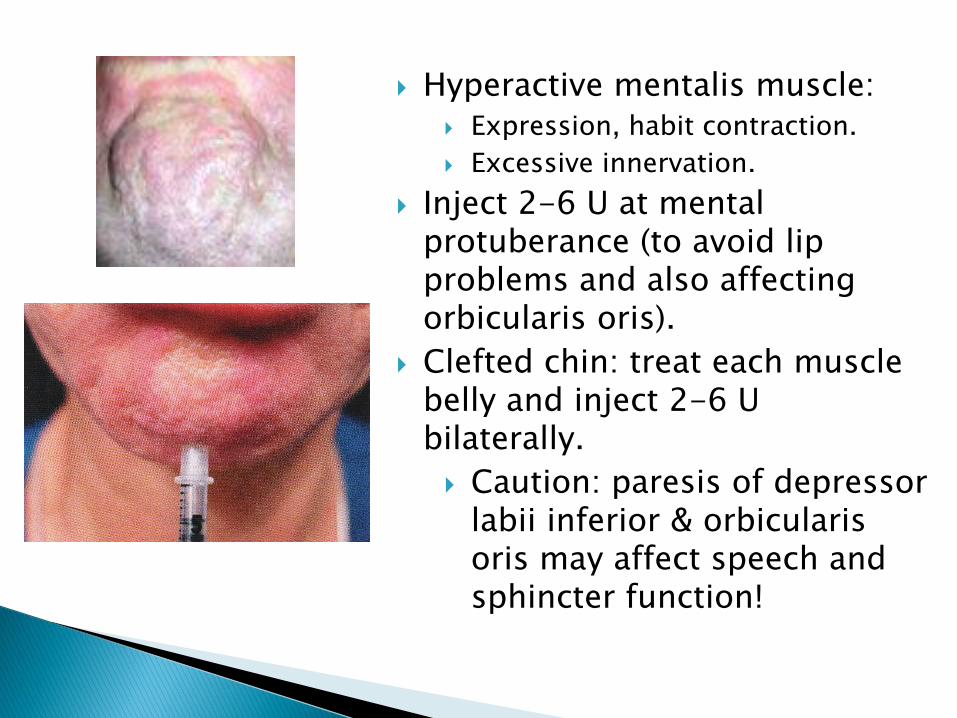
Hyperactive mentalis muscle: Expression, habit contraction.
Excessive innervation.
Inject 2-6 U at mental protuberance (to avoid lip problems and also affecting orbicularis oris).
Clefted chin: treat each muscle belly and inject 2-6 U bilaterally.
Caution: paresis of depressor labii inferior & orbicularisoris may affect speech and sphincter function!
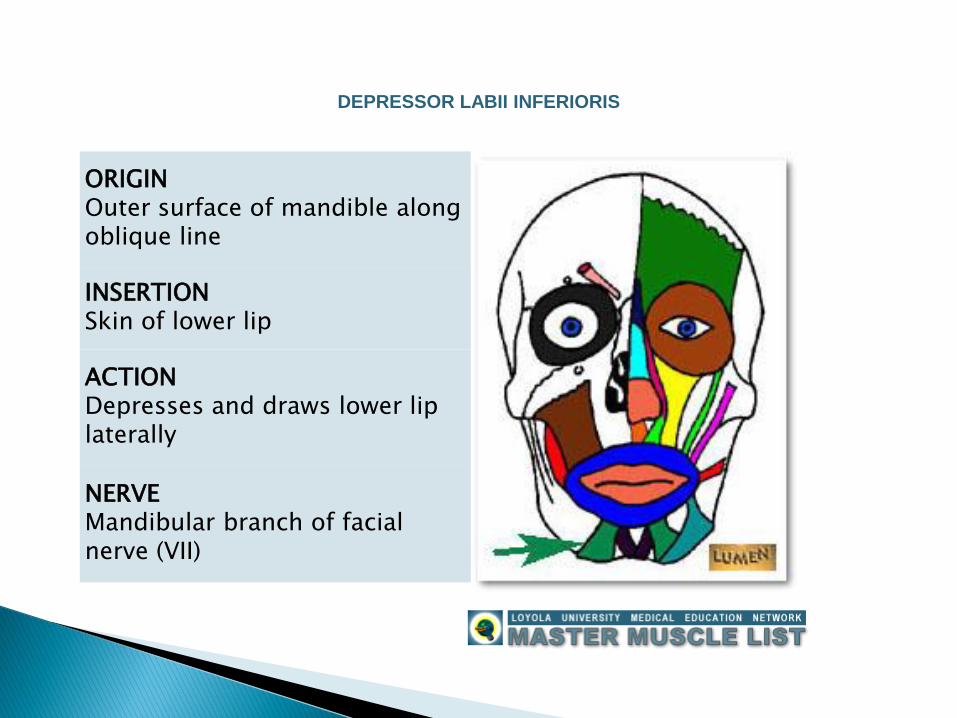
ORIGINOuter surface of mandible along oblique line
INSERTIONSkin of lower lip
ACTIONDepresses and draws lower lip laterally
NERVEMandibular branch of facial nerve (VII)
DEPRESSOR LABII INFERIORIS
Asymmetrical smile:
Lower lip position varies from one side to the other due to imbalance of depressor labii inferior:◦ Hyperactivity: lower lip depression on affected side.
◦ Hypoactivity: lower lip elevation on affected side.
1-3 U into overactive depressor labii inferior.◦ Use minimum dose to correct asymmetry.
◦ Too much may cause excessive weakening and therefore elevate the lower lip (overcorrection).
Caution: close proximity to DAO, orbicularis oris and mentalis!
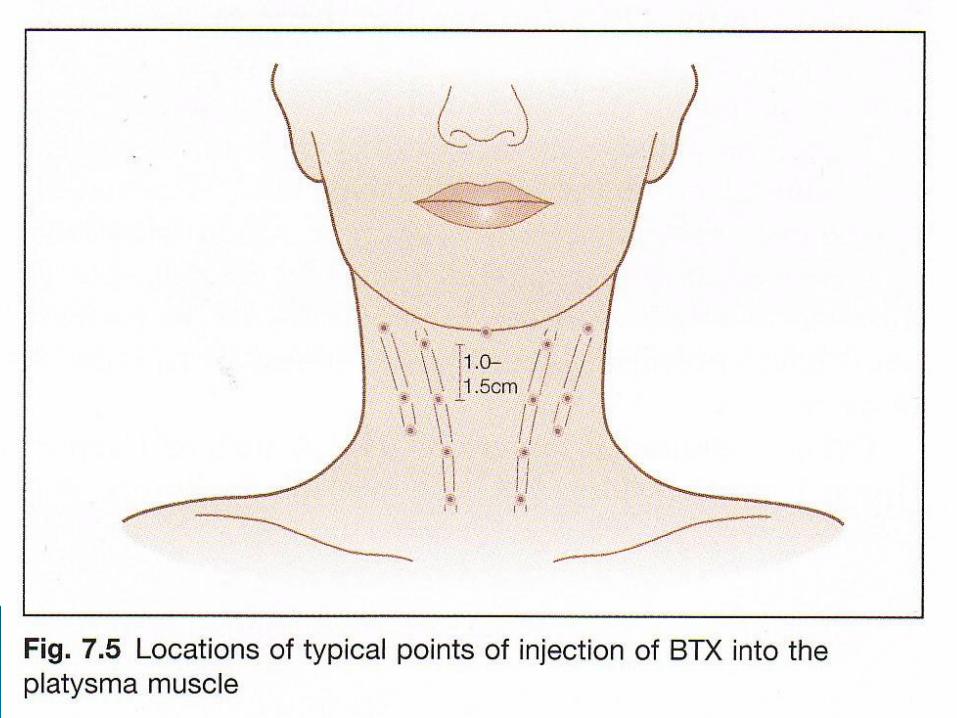
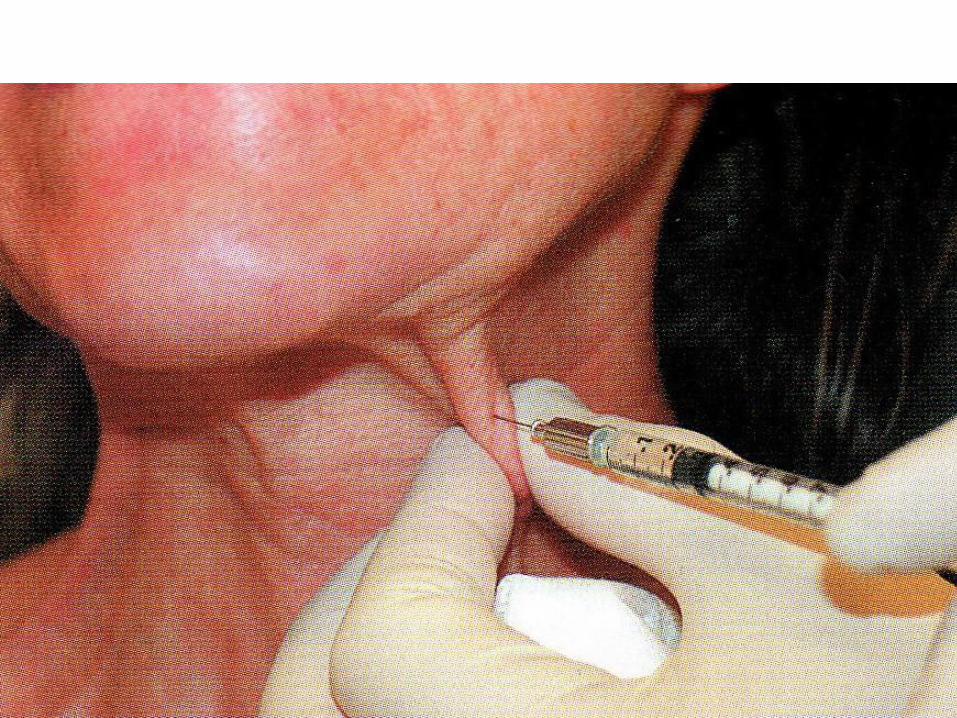
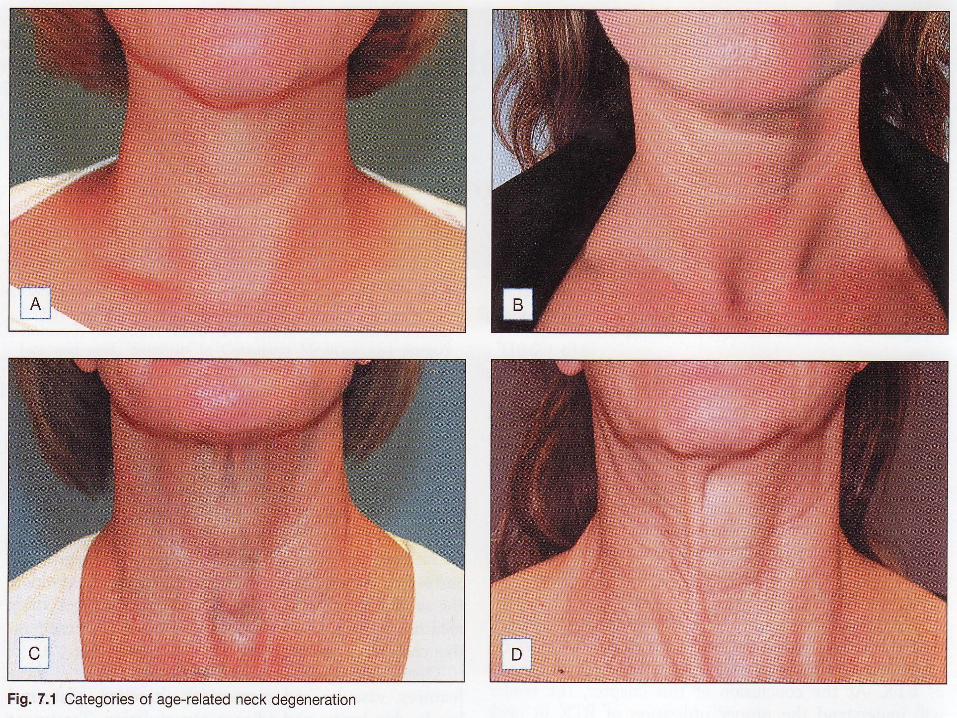
Platysmal bands & horizontal „necklace‟ lines
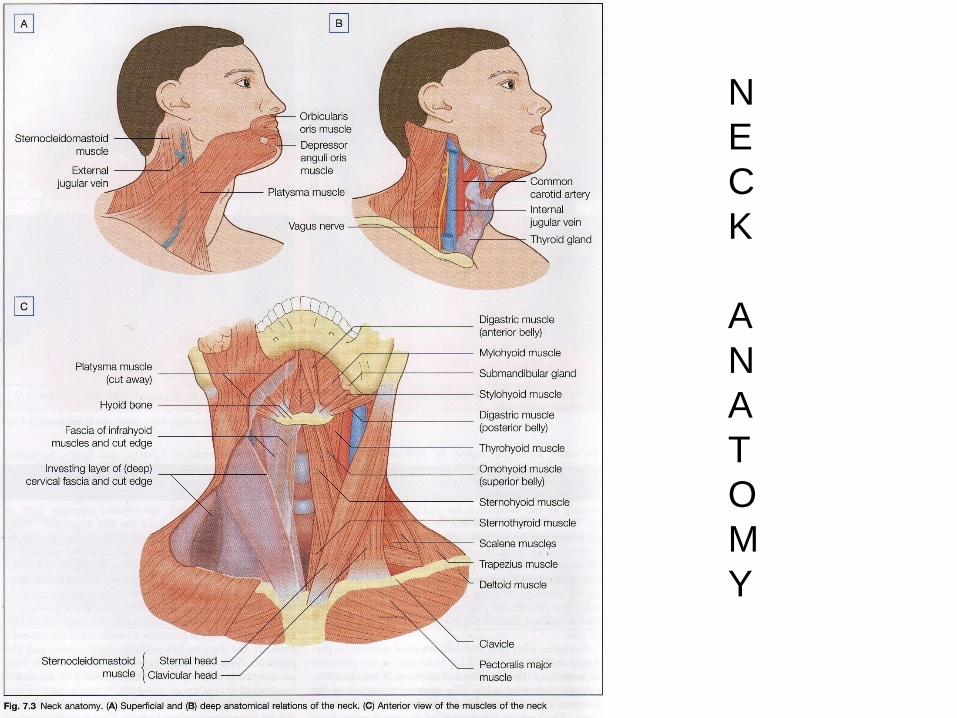
N
E
C
K
A
N
A
T
O
M
Y
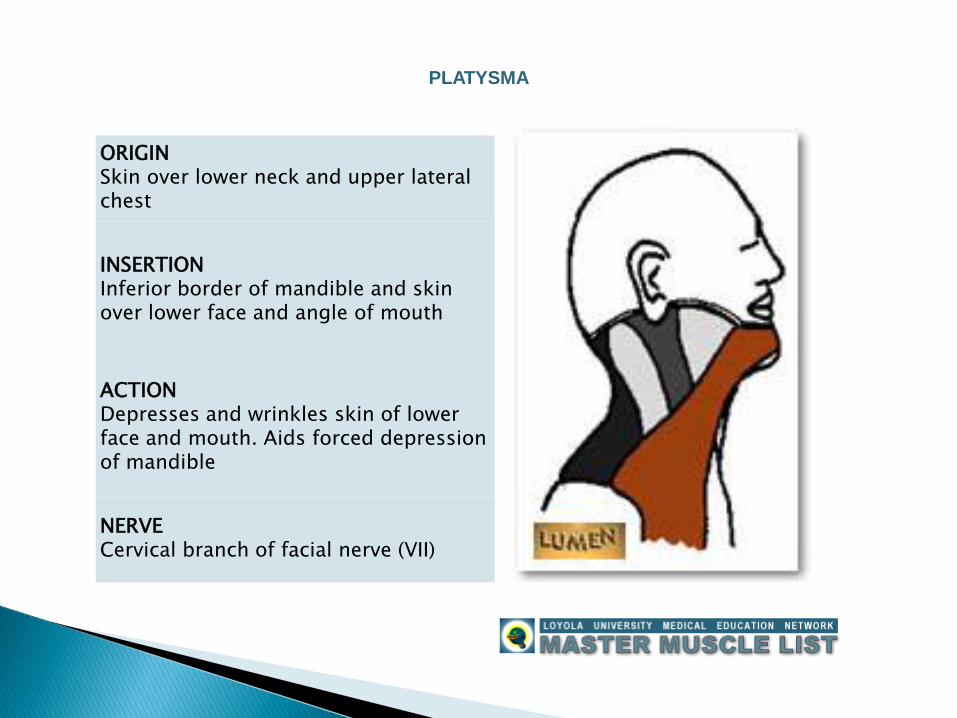
ORIGINSkin over lower neck and upper lateral chest
INSERTIONInferior border of mandible and skin over lower face and angle of mouth
ACTIONDepresses and wrinkles skin of lower face and mouth. Aids forced depression of mandible
NERVECervical branch of facial nerve (VII)
PLATYSMA