Improving Medical Decision Making and Health Promotion ...
23
Improving Medical Decision Making and Health Promotion through Culture-Sensitive Health Communication: An Agenda for Science and Practice Cornelia Betsch, PD Dr phil Dipl-Psych, Robert Bo ¨hm, Dr Dipl-Psych, Collins O. Airhihenbuwa, PhD, MPH, Robb Butler, MA, Gretchen B. Chapman, PhD, Niels Haase, Dipl-Psych, MA, Benedikt Herrmann, Dr, Tasuku Igarashi, PhD, Shinobu Kitayama, PhD, Lars Korn, MSc, U ¨ lla-Karin Nurm, Dr, Bernd Rohrmann, MSc, Dr phil, Dr phil habil, Alexander J. Rothman, PhD, Sharon Shavitt, PhD, John A. Updegraff, PhD, Ayse K. Uskul, Dr This review introduces the concept of culture-sensitive health communication. The basic premise is that congru- ency between the recipient’s cultural characteristics and the respective message will increase the communication’s effectiveness. Culture-sensitive health communication is therefore defined as the deliberate and evidence-informed adaptation of health communication to the recipients’ cul- tural background in order to increase knowledge and improve preparation for medical decision making and to enhance the persuasiveness of messages in health promo- tion. To achieve effective health communication in vary- ing cultural contexts, an empirically and theoretically based understanding of culture will be indispensable. We therefore define culture, discuss which evolutionary and structural factors contribute to the development of cultural diversity, and examine how differences are con- ceptualized as scientific constructs in current models of cultural differences. In addition, we will explicate the im- plications of cultural differences for psychological theoriz- ing, because common constructs of health behavior theories and decision making, such as attitudes or risk perception, are subject to cultural variation. In terms of communication, we will review both communication strat- egies and channels that are used to disseminate health messages, and we will discuss the implications of cultural differences for their effectiveness. Finally, we propose an agenda both for science and for practice to advance and apply the evidence base for culture-sensitive health com- munication. This calls for more interdisciplinary research between science and practice but also between scientific disciplines and between basic and applied research. Key words: disease and infection control; health communica- tion; targeting and tailoring; treatment choice; basic and applied research. (Med Decis Making 2016;36:811–833) H ealth communication can have different goals. While approaches in medical decision making strive to support informed and unbiased shared decision processes (e.g., between different cancer treatments), health promotion practices strive to change people’s behavior toward a desired end state (e.g., taking up a healthy lifestyle). This article will focus on both medical decision making and health promotion and the interplay between the displayed information or message and the cultural background of the recipient. We argue that the way in which a message takes cultural differences into account will affect understanding and the effectiveness of health communication. From an extensive literature review, we derive conclusions directed to scientists working in the fields of medical decision making and health promotion as well as to field workers in health organizations, hospitals, or agencies who are charged with developing decision aids and craft- ing and disseminating health messages. Medical decision making is often understood as a patient-centered approach in which evidence- based information facilitates shared decision making Ó The Author(s) 2015 Reprints and permission: http://www.sagepub.com/journalsPermissions.nav DOI: 10.1177/0272989X15600434 MEDICAL DECISION MAKING/OCTOBER 2016 811 REVIEW Konstanzer Online-Publikations-System (KOPS) URL: http://nbn-resolving.de/urn:nbn:de:bsz:352-2-1pwfffv3iyuxh3 Erschienen in: Medical Decision Making ; 36 (2016), 7. - S. 811-833 https://dx.doi.org/10.1177/0272989X15600434
Transcript of Improving Medical Decision Making and Health Promotion ...

Improving Medical Decision Making andHealth Promotion through Culture-Sensitive
Health Communication An Agendafor Science and Practice
Cornelia Betsch PD Dr phil Dipl-Psych Robert Bohm Dr Dipl-PsychCollins O Airhihenbuwa PhD MPH Robb Butler MA Gretchen B Chapman PhD
Niels Haase Dipl-Psych MA Benedikt Herrmann Dr Tasuku Igarashi PhDShinobu Kitayama PhD Lars Korn MSc Ulla-Karin Nurm Dr
Bernd Rohrmann MSc Dr phil Dr phil habil Alexander J Rothman PhDSharon Shavitt PhD John A Updegraff PhD Ayse K Uskul Dr
This review introduces the concept of culture-sensitivehealth communication The basic premise is that congru-ency between the recipientrsquos cultural characteristics andthe respective message will increase the communicationrsquoseffectiveness Culture-sensitive health communication istherefore defined as the deliberate and evidence-informedadaptation of health communication to the recipientsrsquo cul-tural background in order to increase knowledge andimprove preparation for medical decision making and toenhance the persuasiveness of messages in health promo-tion To achieve effective health communication in vary-ing cultural contexts an empirically and theoreticallybased understanding of culture will be indispensableWe therefore define culture discuss which evolutionaryand structural factors contribute to the development ofcultural diversity and examine how differences are con-ceptualized as scientific constructs in current models of
cultural differences In addition we will explicate the im-plications of cultural differences for psychological theoriz-ing because common constructs of health behaviortheories and decision making such as attitudes or riskperception are subject to cultural variation In terms ofcommunication we will review both communication strat-egies and channels that are used to disseminate healthmessages and we will discuss the implications of culturaldifferences for their effectiveness Finally we propose anagenda both for science and for practice to advance andapply the evidence base for culture-sensitive health com-munication This calls for more interdisciplinary researchbetween science and practice but also between scientificdisciplines and between basic and applied research Keywords disease and infection control health communica-tion targeting and tailoring treatment choice basic andapplied research (Med Decis Making 201636811ndash833)
Health communication can have different goalsWhile approaches in medical decision making
strive to support informed and unbiased shareddecision processes (eg between different cancertreatments) health promotion practices strive tochange peoplersquos behavior toward a desired end state(eg taking up a healthy lifestyle) This article willfocus on both medical decision making and healthpromotion and the interplay between the displayed
information or message and the cultural backgroundof the recipient We argue that the way in whicha message takes cultural differences into accountwill affect understanding and the effectiveness ofhealth communication From an extensive literaturereview we derive conclusions directed to scientistsworking in the fields of medical decision makingand health promotion as well as to field workers inhealth organizations hospitals or agencies whoare charged with developing decision aids and craft-ing and disseminating health messages
Medical decision making is often understood asa patient-centered approach in which evidence-based information facilitates shared decision making
The Author(s) 2015Reprints and permissionhttpwwwsagepubcomjournalsPermissionsnavDOI 1011770272989X15600434
MEDICAL DECISION MAKINGOCTOBER 2016 811
REVIEW
Konstanzer Online-Publikations-System (KOPS) URL httpnbn-resolvingdeurnnbndebsz352-2-1pwfffv3iyuxh3
Erschienen in Medical Decision Making 36 (2016) 7 - S 811-833 httpsdxdoiorg1011770272989X15600434
and helps to evaluate the option in the light of the val-ues held by the patient1ndash16 This type of decision mak-ing is also called preference-sensitive choice Thismeans that in such type of medical decisions thereis no best choice but the values of the options arestrongly determined by the personal values and pref-erences of the decision maker (eg the decision for oragainst the use of postmenopausal hormone therapy)Since the shared decision-making paradigm is centralto treatment decision making17 decision aids in theform of computerized systems have been designed asone tool among others1819 to support a balanced pre-sentation of options20 and to communicate risks andbenefits in an unbiased way21 They serve the purposeof presenting evidence-based treatment options insitu International Patient Decision Aids Standards22
strive for improving patient decision aids to fosterpatientsrsquo understanding of the alternativesrsquo costs ben-efits and lifestyle implications4 and how the alterna-tives relate to personal values
In contrast to the medical decision-makingapproach health promotion strategies strive to per-suade or nudge the recipient to take up healthy or tostop unhealthy behaviors (eg wash their handsexercise eat healthy quit smoking) This goal ofhealth promotion is usually ethically justified whenthere is agreement that the behaviors have exclusivelyor mostly positive consequences Decades of healthpromotion research have suggested ways to presentinformation in a way such that the desired behaviorbecomes more likely2324 Techniques such as framingor nudging are deliberately used to make health pro-motion more effective2526 Individual and cultural dif-ferences are known to moderate some effects such aseffects of framing messages in terms of gain or loss27
For health promotion the evaluation criteria are usu-ally changes in attitudes intentions or behaviors2829
One may raise doubt however as to whether unbi-ased decision processes exist at all because decisionaids have to choose one way or another to present riskinformation or information about treatment optionsMinimal pieces of information such as the framing ofthe decision task in terms of gains or losses28 can influ-ence the decisions remarkably29 and are known to bemoderated by individual and cultural differences Like-wise characteristics of the receiver can systematicallyinfluence the way in which information is processedIn the area of medical decision making individual dif-ferences such as numeracy seem to play a role30 Themedical decision-making literature however showsa considerable gap regarding the role of cultural differ-ences28 which may affect the effectiveness of healthpromotion programs as well Hence a fit between indi-vidual differences and characteristics of the decisionsupport will enhance the decision aidrsquos effectiveness28
Receivers of the very same messages can varyremarkably in their cultural background This maybe the case due to human mobility in the form of inter-nal and external migration and growing shifts in pop-ulation and language dynamics even if messagerecipients live in the same continent country orstate This proves particularly challenging for bothinternational health agencies such as the World HealthOrganization (WHO) or European Centre for DiseasePrevention and Control (ECDC) who strive to serveand support national health entities with their commu-nications and advocacy and the national Centers forDisease Control and Prevention (CDCs) or public healthinstitutes responsible for supporting their health carepersonnel by offering information messages and mate-rials Even if interventions decision aids or messagesare designed based on theories of shared decision mak-ing preventive health behavior or behavior change
Received 31 August 2014 from the Center for Empirical Research inEconomics and Behavioral Sciences (CEREB) University of ErfurtErfurt Germany (CB LK) School of Business and Economics RWTHAachen University Aachen Germany (RB) Department of Biobehavio-ral Health Penn State University University Park PA USA (COA) WorldHealth Organization Regional Office for Europe Copenhagen Den-mark (RB) Institute for Health Healthcare Policy and Aging ResearchRutgers University New Brunswick NJ USA (GBC) Department ofPsychology University of Erfurt Erfurt Germany (NH) Institute forHealth and Consumer Protection Joint Research Centre of the Euro-pean Commission Ispra Italy (BH) Graduate School of Educationand Human Development Nagoya University Nagoya Japan (TI)Department of Psychology University of Michigan Ann Arbor MIUSA (SK) European Centre for Disease Prevention and Control Stock-holm Sweden (U-KN) Roman Research Road Melbourne Australia(BR) University of Minnesota Minneapolis MN USA (AJR) Departmentof Business Administration University of Illinois Champaign IL USA(SS) Kent State University Kent OH USA (JAU) and School of Psy-chology University of Kent Canterbury UK (AKU) This work was sup-ported by the financial support of the World Health Organization (WHO)Regional Office for Europe European Centre for Disease Preventionand Control (ECDC) German Research Foundation (DFG BE 39706-1) University of Erfurt and RWTH Aachen University The fundingagreement ensured the authorsrsquo independence in designing the meet-ing and the resulting publication The following authors are employed bythe sponsors Robb Butler (WHOEurope) Ulla-Karin Nurm (ECDC)Cornelia Betsch (University of Erfurt) Robert Bohm (RWTH Aachen Uni-versity) All authors report no conflicts of interest Opinions expressed bythe authors are their own and not necessarily those of their institutionsRevision accepted for publication 17 July 2015
Address correspondence to Cornelia Betsch Center for EmpiricalResearch in Economics and Behavioral Sciences (CEREB) Universityof Erfurt Nordhaeuserstrasse 63 Erfurt 99089 Germany telephone+49 361-737 1631 fax +49 361-737 2209 e-mail corneliabetschuni-erfurtde
BETSCH AND OTHERS
812 MEDICAL DECISION MAKINGOCTOBER 2016
these theories usually do not account for cultural differ-ences as will be outlined below Further designinghealth messages in a culture-sensitive way is a chal-lenge31 Thus the effectiveness of materials producedby international and national agenciesmdashin terms ofenhancing understanding and leading to behavioralchangemdashis not well understood both from a theoreticaland practical point of view
This contribution discusses how the interplaybetween the health message and the recipientsrsquo cul-tural characteristics will influence the understandingand effectiveness of health communication Thebasic premise is that congruency between the recipi-entrsquos cultural characteristics and the respective mes-sage as stated in the cultural congruency hypothesis27
will increase message effectiveness leading to deeperprocessing and better understanding in the case ofdecision support or to changes in behavior in thecase of health promotion Culture-sensitive healthcommunication will help to reduce disparities inhealth outcomes by making messages equally under-standable meaningful and effective2232 To achieveeffective health communication in varying culturalcontexts an empirically and theoretically basedknowledge of culture is indispensable In the firstpart of the article we will therefore provide in-depthdefinitions of culture and discuss the etiology of cul-tural differences We will then outline different psy-chological models of culture As theories of(preventive) health behavior and medical decisionmaking do not explicitly incorporate culture asa determinant or moderator we will discuss how cen-tral theoretical constructs such as perceptions ofhealth attitudes or risk vary as a function of cultureWe will also summarize how culture affects the effec-tiveness of communication channels and how it mod-erates well-established effects such as framing Basedon this focused overview of the literature we will pro-vide suggestions for improving culture-sensitivehealth communication in practice (Table 1) We willfinally propose an agenda for health communicatorsfor how to improve structural requirements forculture-sensitive health communication Because ofthe current state of the research literatures the pro-posals identified in this article are evidence-informedrather than evidence-based Thus we will also suggestan agenda for scientists to further improve the evidencebase for culture-sensitive health communication
DEFINING CULTURE-SENSITIVE HEALTHCOMMUNICATION
The idea that medical interventions and treat-ments should be evidence based is well accepted33
In the area of health promotion there is growinginterest in the acknowledged idea that lsquolsquoinforminginfluencing and motivating individual institu-tional and public audiences about important healthissuesrsquorsquo is an art and science itself3435 Further thereis growing understanding that audience insight andapplication of the social sciences and medicalhumanities to diagnose define design and test com-munication interventions is crucial for optimal effec-tiveness and impact36 (for an example of increasingaudience insight see the Guide to Tailoring Immuni-zation Programs (TIP)37 or publications on healthcommunication produced by ECDC38) Psychologicalresearch demonstrates that messages will be pro-cessed more thoroughly28 and be more persuasiveand effective if their content is tailored to the recipi-entsrsquo cognitive affective and motivational character-istics39 (for a broad overview on person 3 situationmodels see ref 40) These characteristics of the recip-ient depend largely on his or her cultural backgroundThis suggests that effective message design woulddepend on understanding these characteristics asthey relate to the cultural infrastructure of messagedelivery41 Further congruency between the messagedesign and the receiverrsquos cultural characteristic willenhance message persuasiveness (cultural congru-ency hypothesis27) Thus when health messages aredesigned to encourage people to exercise eat lessfloss get vaccinated or wash their hands the mes-sagersquos congruence with the recipientrsquos cultural back-ground and the context in which it is delivered affectsthe effectiveness of the message in eliciting individ-ual health behaviors Beyond this targeting (generalcultural adaptation) and tailoring (adaptation to indi-vidual differences within a culture) are not only rele-vant methods in the area of health promotion2842 butalso useful to make the contents of a decision aidmore relevant and understandable to members of dif-ferent cultures For example Hispanic Americansmay perceive the consequences of treatments notonly as relevant for the self but also for related otherssuch as family28 When the information offered iscongruent with cultural values the content is likelyto lead to lsquolsquodeeper thinking which should in turnimprove important accuracy regarding possible bene-fits and harms choices that are more consistent withinformed values and increased participation in deci-sion makingrsquorsquo28(p3) Thus the design of decision aidsshould also take cultural differences into account Wetherefore define culture-sensitive health communica-tion as the deliberate and evidence-informed adapta-tion of health communication to the recipientsrsquocultural background in order to increase knowledgeand improve preparation for medical decision
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 813
making and to enhance the persuasiveness of mes-sages in health promotion
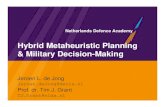
Figure 1 illustrates the idealized process and theinterdisciplinary nature of health communicationFurther it shows where culture-sensitive health com-munication should be included in the process ofdesigning decision aids or health promotion mes-sages Findings from medical science (eg abouttreatments or preventive measures) form the basis ofevidence-based information (facts) that is to be com-municated Behavioral social and communicationscience informs the process of message and informa-tion design (eg questions concerning decision pro-cesses determinants of health) To increase theeffectiveness of messages314344 health communica-tors then adapt these inputs to the receiversrsquo individ-ual psychological characteristics in this case theircultural background This can be done for exampleby targeting cultural subgroups in a campaign withperipheral or linguistic adaptations28 or by tailoringcontents displayed in a decision aid to culturalaspects that are assessed at the beginning of a decisionaid (for examples and items to assess cultural aspectssee Kreuter and others45 Alden and others28)
CULTURE AND CULTURAL DIFFERENCES
Having explicated the definition and need forculture-sensitive health communication we willnow take a closer look at culture as a scientific con-struct which evolutionary and structural factors con-tribute to the development of cultural diversity andhow cultural differences are conceptualized as scien-tific constructs in current models
Defining Culture
Culture is a collective sense of consciousness withboth quantifiable and unquantifiable componentsthat can audibly or silently reveal themselves throughhistory and language46 Culture is never static andis commonly reinforced through structures eventhough those structures are not always palpable andvisible as are physical structures47 Cultural normsmay be acquired in large part through reinforcementlearning While interacting with other members of thesociety individuals are likely to infer what normsexpectations and rules might exist in specific socialsituations Once such social rules are inferred theindividuals will organize their behaviors accord-ingly If the behaviors are accepted or approved bythe others because they are in fact congruent with
the relevant social norms held by others the inferredrules will be reinforced and thus will gradually beinternalized as perceived social norms Recentresearch showed that individuals differ in the degreeto which cultural norms are successfully inferred andacquiredmdashcarriers of certain alleles showed morepronounced cultural differences4849 Thus noteveryone in a cultural group may internalize thenorms of their cultures to the same degree whichleads to individual differences within a culture Cul-tural norms beliefs and practices are influenced bya variety of ecological factors such as traditions inherding versus farming which could explain someof the systematic cultural variability across differentregions of the world today Compared to herdingfarming requires greater degrees of social coordina-tion and interdependence with others (v indepen-dence of each individual)50 Moreover as comparedwith wheat farming rice farming requires far greaterextents of social coordination51 It is plausible thenthat one important reason why Asians tend to bemore interdependent and collectivistic today relativeto Western Europeans is that in Asia (but not in therest of the world) rice has been the primary crop ofthe region over the past several thousand years Cul-ture can also be influenced by numerous relativelymore short-term factors such as settlement historiesSome of the factors that encourage independence ofthe self from others (as opposed to social relationsand interdependence with others) include high resi-dential mobility52 low population density or theabsence of social infrastructures53ndash56 Moreoverrecent cultural neuroscience work has shown thatthis cultural influence is truly lsquolsquodeeprsquorsquo in the sensethat it is inscribed into brain mechanisms5758
Psychological Models of Cultural Differences
A number of organizing dimensions and frame-works have been proposed to account for theobserved cultural differences and provide a theoreti-cal stage for testing predictions One majordimension of cultural difference is the distinctionbetween independence and interdependence of theself vis-a-vis others in the same community59 Ina broad sense contemporary Western cultures tendto be more independent whereas contemporaryAsian cultures tend to be more interdependentCultural systems organized by independence orinterdependence influence every aspect of humanpsychology including cognition emotion and moti-vation5759 Other dimensions include tight versusloose cultures6061 masculine versus feminine
BETSCH AND OTHERS
814 MEDICAL DECISION MAKINGOCTOBER 2016
cultures62 survival versus self-expression63 and cul-tures of honor versus dignity versus face64 Some ofthe proposed frameworks emphasize the systemicinteractions between or mutual constitution ofsocialecological environments and human mindbehavior (eg the socioecological model65ndash67 thecultural ecosystem model68 and sociocultural mod-els69ndash71) Although the field is increasingly witness-ing the examination of different constructs andframeworks to date the one dimension that has cap-tured most attention is the one noted above namelyindividualism and collectivism5960627273 at thelevel of cultural norms or independence and inter-dependence at the level of individual differences
Individualism refers to a cultural syndrome that isorganized by the model of the self as independent Inindividualistic cultures internal attributes are seenas self-defining and both personal autonomy andself-expression are considered as major culturaltasks5960617374 Moreover individuals tend to focuson rights (above duties) with greater priority placedon their personal goals over social welfare or socialgoals They view themselves as agentic using theirpersonal goals and desires to regulate their decisionsand actions In terms of their self-regulatory tenden-cies they are more motivated toward promotion(that is pursuing opportunities) rather than towardprevention (that is not making mistakes) focusingon the positive outcomes they hope to approach
rather than the negative outcomes they hope toavoid75 By contrast collectivism implies a culturalsyndrome that is organized by the model of the selfas interdependent Collectivistic cultures are charac-terized by context dependency malleability andheavy reliance on social relations and membershipsin groups for onersquos self-definition5960 In such cul-tures the focus is on social mutual obligations thefulfillment of in-group expectations and mainte-nance of group harmony59606273 In terms of self-regulatory tendencies in collectivistic cultures peo-ple are more motivated to not make mistakes than topursue opportunities focusing on the negative out-comes they hope to avoid rather than the positive out-comes they hope to achieve75ndash77 The notions ofindependence and interdependence (or individual-ism and collectivism) have been useful to under-stand and predict cross-cultural differences ina variety of psychological processes includinghealth promotion78 There are several scales avail-able that are designed to assess these differences(individualism and collectivism on the level of cul-tural norms62 and independent v interdependentself-construals on the level of individual differen-ces79 and for a short list of items to include as a mea-surement in health promotion tools see ref 80)8182
There remains some debate on the validity of thesemeasures as applied to indices of culturalsyndromes83
Figure 1 The idealized process of culture-sensitive health communication as an evidence-informed way of communicating evidence-
based medical information adapted to the cultural background of the messagersquos receiver
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 815
Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

and helps to evaluate the option in the light of the val-ues held by the patient1ndash16 This type of decision mak-ing is also called preference-sensitive choice Thismeans that in such type of medical decisions thereis no best choice but the values of the options arestrongly determined by the personal values and pref-erences of the decision maker (eg the decision for oragainst the use of postmenopausal hormone therapy)Since the shared decision-making paradigm is centralto treatment decision making17 decision aids in theform of computerized systems have been designed asone tool among others1819 to support a balanced pre-sentation of options20 and to communicate risks andbenefits in an unbiased way21 They serve the purposeof presenting evidence-based treatment options insitu International Patient Decision Aids Standards22
strive for improving patient decision aids to fosterpatientsrsquo understanding of the alternativesrsquo costs ben-efits and lifestyle implications4 and how the alterna-tives relate to personal values
In contrast to the medical decision-makingapproach health promotion strategies strive to per-suade or nudge the recipient to take up healthy or tostop unhealthy behaviors (eg wash their handsexercise eat healthy quit smoking) This goal ofhealth promotion is usually ethically justified whenthere is agreement that the behaviors have exclusivelyor mostly positive consequences Decades of healthpromotion research have suggested ways to presentinformation in a way such that the desired behaviorbecomes more likely2324 Techniques such as framingor nudging are deliberately used to make health pro-motion more effective2526 Individual and cultural dif-ferences are known to moderate some effects such aseffects of framing messages in terms of gain or loss27
For health promotion the evaluation criteria are usu-ally changes in attitudes intentions or behaviors2829
One may raise doubt however as to whether unbi-ased decision processes exist at all because decisionaids have to choose one way or another to present riskinformation or information about treatment optionsMinimal pieces of information such as the framing ofthe decision task in terms of gains or losses28 can influ-ence the decisions remarkably29 and are known to bemoderated by individual and cultural differences Like-wise characteristics of the receiver can systematicallyinfluence the way in which information is processedIn the area of medical decision making individual dif-ferences such as numeracy seem to play a role30 Themedical decision-making literature however showsa considerable gap regarding the role of cultural differ-ences28 which may affect the effectiveness of healthpromotion programs as well Hence a fit between indi-vidual differences and characteristics of the decisionsupport will enhance the decision aidrsquos effectiveness28
Receivers of the very same messages can varyremarkably in their cultural background This maybe the case due to human mobility in the form of inter-nal and external migration and growing shifts in pop-ulation and language dynamics even if messagerecipients live in the same continent country orstate This proves particularly challenging for bothinternational health agencies such as the World HealthOrganization (WHO) or European Centre for DiseasePrevention and Control (ECDC) who strive to serveand support national health entities with their commu-nications and advocacy and the national Centers forDisease Control and Prevention (CDCs) or public healthinstitutes responsible for supporting their health carepersonnel by offering information messages and mate-rials Even if interventions decision aids or messagesare designed based on theories of shared decision mak-ing preventive health behavior or behavior change
Received 31 August 2014 from the Center for Empirical Research inEconomics and Behavioral Sciences (CEREB) University of ErfurtErfurt Germany (CB LK) School of Business and Economics RWTHAachen University Aachen Germany (RB) Department of Biobehavio-ral Health Penn State University University Park PA USA (COA) WorldHealth Organization Regional Office for Europe Copenhagen Den-mark (RB) Institute for Health Healthcare Policy and Aging ResearchRutgers University New Brunswick NJ USA (GBC) Department ofPsychology University of Erfurt Erfurt Germany (NH) Institute forHealth and Consumer Protection Joint Research Centre of the Euro-pean Commission Ispra Italy (BH) Graduate School of Educationand Human Development Nagoya University Nagoya Japan (TI)Department of Psychology University of Michigan Ann Arbor MIUSA (SK) European Centre for Disease Prevention and Control Stock-holm Sweden (U-KN) Roman Research Road Melbourne Australia(BR) University of Minnesota Minneapolis MN USA (AJR) Departmentof Business Administration University of Illinois Champaign IL USA(SS) Kent State University Kent OH USA (JAU) and School of Psy-chology University of Kent Canterbury UK (AKU) This work was sup-ported by the financial support of the World Health Organization (WHO)Regional Office for Europe European Centre for Disease Preventionand Control (ECDC) German Research Foundation (DFG BE 39706-1) University of Erfurt and RWTH Aachen University The fundingagreement ensured the authorsrsquo independence in designing the meet-ing and the resulting publication The following authors are employed bythe sponsors Robb Butler (WHOEurope) Ulla-Karin Nurm (ECDC)Cornelia Betsch (University of Erfurt) Robert Bohm (RWTH Aachen Uni-versity) All authors report no conflicts of interest Opinions expressed bythe authors are their own and not necessarily those of their institutionsRevision accepted for publication 17 July 2015
Address correspondence to Cornelia Betsch Center for EmpiricalResearch in Economics and Behavioral Sciences (CEREB) Universityof Erfurt Nordhaeuserstrasse 63 Erfurt 99089 Germany telephone+49 361-737 1631 fax +49 361-737 2209 e-mail corneliabetschuni-erfurtde
BETSCH AND OTHERS
812 MEDICAL DECISION MAKINGOCTOBER 2016
these theories usually do not account for cultural differ-ences as will be outlined below Further designinghealth messages in a culture-sensitive way is a chal-lenge31 Thus the effectiveness of materials producedby international and national agenciesmdashin terms ofenhancing understanding and leading to behavioralchangemdashis not well understood both from a theoreticaland practical point of view
This contribution discusses how the interplaybetween the health message and the recipientsrsquo cul-tural characteristics will influence the understandingand effectiveness of health communication Thebasic premise is that congruency between the recipi-entrsquos cultural characteristics and the respective mes-sage as stated in the cultural congruency hypothesis27
will increase message effectiveness leading to deeperprocessing and better understanding in the case ofdecision support or to changes in behavior in thecase of health promotion Culture-sensitive healthcommunication will help to reduce disparities inhealth outcomes by making messages equally under-standable meaningful and effective2232 To achieveeffective health communication in varying culturalcontexts an empirically and theoretically basedknowledge of culture is indispensable In the firstpart of the article we will therefore provide in-depthdefinitions of culture and discuss the etiology of cul-tural differences We will then outline different psy-chological models of culture As theories of(preventive) health behavior and medical decisionmaking do not explicitly incorporate culture asa determinant or moderator we will discuss how cen-tral theoretical constructs such as perceptions ofhealth attitudes or risk vary as a function of cultureWe will also summarize how culture affects the effec-tiveness of communication channels and how it mod-erates well-established effects such as framing Basedon this focused overview of the literature we will pro-vide suggestions for improving culture-sensitivehealth communication in practice (Table 1) We willfinally propose an agenda for health communicatorsfor how to improve structural requirements forculture-sensitive health communication Because ofthe current state of the research literatures the pro-posals identified in this article are evidence-informedrather than evidence-based Thus we will also suggestan agenda for scientists to further improve the evidencebase for culture-sensitive health communication
DEFINING CULTURE-SENSITIVE HEALTHCOMMUNICATION
The idea that medical interventions and treat-ments should be evidence based is well accepted33
In the area of health promotion there is growinginterest in the acknowledged idea that lsquolsquoinforminginfluencing and motivating individual institu-tional and public audiences about important healthissuesrsquorsquo is an art and science itself3435 Further thereis growing understanding that audience insight andapplication of the social sciences and medicalhumanities to diagnose define design and test com-munication interventions is crucial for optimal effec-tiveness and impact36 (for an example of increasingaudience insight see the Guide to Tailoring Immuni-zation Programs (TIP)37 or publications on healthcommunication produced by ECDC38) Psychologicalresearch demonstrates that messages will be pro-cessed more thoroughly28 and be more persuasiveand effective if their content is tailored to the recipi-entsrsquo cognitive affective and motivational character-istics39 (for a broad overview on person 3 situationmodels see ref 40) These characteristics of the recip-ient depend largely on his or her cultural backgroundThis suggests that effective message design woulddepend on understanding these characteristics asthey relate to the cultural infrastructure of messagedelivery41 Further congruency between the messagedesign and the receiverrsquos cultural characteristic willenhance message persuasiveness (cultural congru-ency hypothesis27) Thus when health messages aredesigned to encourage people to exercise eat lessfloss get vaccinated or wash their hands the mes-sagersquos congruence with the recipientrsquos cultural back-ground and the context in which it is delivered affectsthe effectiveness of the message in eliciting individ-ual health behaviors Beyond this targeting (generalcultural adaptation) and tailoring (adaptation to indi-vidual differences within a culture) are not only rele-vant methods in the area of health promotion2842 butalso useful to make the contents of a decision aidmore relevant and understandable to members of dif-ferent cultures For example Hispanic Americansmay perceive the consequences of treatments notonly as relevant for the self but also for related otherssuch as family28 When the information offered iscongruent with cultural values the content is likelyto lead to lsquolsquodeeper thinking which should in turnimprove important accuracy regarding possible bene-fits and harms choices that are more consistent withinformed values and increased participation in deci-sion makingrsquorsquo28(p3) Thus the design of decision aidsshould also take cultural differences into account Wetherefore define culture-sensitive health communica-tion as the deliberate and evidence-informed adapta-tion of health communication to the recipientsrsquocultural background in order to increase knowledgeand improve preparation for medical decision
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 813
making and to enhance the persuasiveness of mes-sages in health promotion
Figure 1 illustrates the idealized process and theinterdisciplinary nature of health communicationFurther it shows where culture-sensitive health com-munication should be included in the process ofdesigning decision aids or health promotion mes-sages Findings from medical science (eg abouttreatments or preventive measures) form the basis ofevidence-based information (facts) that is to be com-municated Behavioral social and communicationscience informs the process of message and informa-tion design (eg questions concerning decision pro-cesses determinants of health) To increase theeffectiveness of messages314344 health communica-tors then adapt these inputs to the receiversrsquo individ-ual psychological characteristics in this case theircultural background This can be done for exampleby targeting cultural subgroups in a campaign withperipheral or linguistic adaptations28 or by tailoringcontents displayed in a decision aid to culturalaspects that are assessed at the beginning of a decisionaid (for examples and items to assess cultural aspectssee Kreuter and others45 Alden and others28)
CULTURE AND CULTURAL DIFFERENCES
Having explicated the definition and need forculture-sensitive health communication we willnow take a closer look at culture as a scientific con-struct which evolutionary and structural factors con-tribute to the development of cultural diversity andhow cultural differences are conceptualized as scien-tific constructs in current models
Defining Culture
Culture is a collective sense of consciousness withboth quantifiable and unquantifiable componentsthat can audibly or silently reveal themselves throughhistory and language46 Culture is never static andis commonly reinforced through structures eventhough those structures are not always palpable andvisible as are physical structures47 Cultural normsmay be acquired in large part through reinforcementlearning While interacting with other members of thesociety individuals are likely to infer what normsexpectations and rules might exist in specific socialsituations Once such social rules are inferred theindividuals will organize their behaviors accord-ingly If the behaviors are accepted or approved bythe others because they are in fact congruent with
the relevant social norms held by others the inferredrules will be reinforced and thus will gradually beinternalized as perceived social norms Recentresearch showed that individuals differ in the degreeto which cultural norms are successfully inferred andacquiredmdashcarriers of certain alleles showed morepronounced cultural differences4849 Thus noteveryone in a cultural group may internalize thenorms of their cultures to the same degree whichleads to individual differences within a culture Cul-tural norms beliefs and practices are influenced bya variety of ecological factors such as traditions inherding versus farming which could explain someof the systematic cultural variability across differentregions of the world today Compared to herdingfarming requires greater degrees of social coordina-tion and interdependence with others (v indepen-dence of each individual)50 Moreover as comparedwith wheat farming rice farming requires far greaterextents of social coordination51 It is plausible thenthat one important reason why Asians tend to bemore interdependent and collectivistic today relativeto Western Europeans is that in Asia (but not in therest of the world) rice has been the primary crop ofthe region over the past several thousand years Cul-ture can also be influenced by numerous relativelymore short-term factors such as settlement historiesSome of the factors that encourage independence ofthe self from others (as opposed to social relationsand interdependence with others) include high resi-dential mobility52 low population density or theabsence of social infrastructures53ndash56 Moreoverrecent cultural neuroscience work has shown thatthis cultural influence is truly lsquolsquodeeprsquorsquo in the sensethat it is inscribed into brain mechanisms5758
Psychological Models of Cultural Differences
A number of organizing dimensions and frame-works have been proposed to account for theobserved cultural differences and provide a theoreti-cal stage for testing predictions One majordimension of cultural difference is the distinctionbetween independence and interdependence of theself vis-a-vis others in the same community59 Ina broad sense contemporary Western cultures tendto be more independent whereas contemporaryAsian cultures tend to be more interdependentCultural systems organized by independence orinterdependence influence every aspect of humanpsychology including cognition emotion and moti-vation5759 Other dimensions include tight versusloose cultures6061 masculine versus feminine
BETSCH AND OTHERS
814 MEDICAL DECISION MAKINGOCTOBER 2016
cultures62 survival versus self-expression63 and cul-tures of honor versus dignity versus face64 Some ofthe proposed frameworks emphasize the systemicinteractions between or mutual constitution ofsocialecological environments and human mindbehavior (eg the socioecological model65ndash67 thecultural ecosystem model68 and sociocultural mod-els69ndash71) Although the field is increasingly witness-ing the examination of different constructs andframeworks to date the one dimension that has cap-tured most attention is the one noted above namelyindividualism and collectivism5960627273 at thelevel of cultural norms or independence and inter-dependence at the level of individual differences
Individualism refers to a cultural syndrome that isorganized by the model of the self as independent Inindividualistic cultures internal attributes are seenas self-defining and both personal autonomy andself-expression are considered as major culturaltasks5960617374 Moreover individuals tend to focuson rights (above duties) with greater priority placedon their personal goals over social welfare or socialgoals They view themselves as agentic using theirpersonal goals and desires to regulate their decisionsand actions In terms of their self-regulatory tenden-cies they are more motivated toward promotion(that is pursuing opportunities) rather than towardprevention (that is not making mistakes) focusingon the positive outcomes they hope to approach
rather than the negative outcomes they hope toavoid75 By contrast collectivism implies a culturalsyndrome that is organized by the model of the selfas interdependent Collectivistic cultures are charac-terized by context dependency malleability andheavy reliance on social relations and membershipsin groups for onersquos self-definition5960 In such cul-tures the focus is on social mutual obligations thefulfillment of in-group expectations and mainte-nance of group harmony59606273 In terms of self-regulatory tendencies in collectivistic cultures peo-ple are more motivated to not make mistakes than topursue opportunities focusing on the negative out-comes they hope to avoid rather than the positive out-comes they hope to achieve75ndash77 The notions ofindependence and interdependence (or individual-ism and collectivism) have been useful to under-stand and predict cross-cultural differences ina variety of psychological processes includinghealth promotion78 There are several scales avail-able that are designed to assess these differences(individualism and collectivism on the level of cul-tural norms62 and independent v interdependentself-construals on the level of individual differen-ces79 and for a short list of items to include as a mea-surement in health promotion tools see ref 80)8182
There remains some debate on the validity of thesemeasures as applied to indices of culturalsyndromes83
Figure 1 The idealized process of culture-sensitive health communication as an evidence-informed way of communicating evidence-
based medical information adapted to the cultural background of the messagersquos receiver
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 815
Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

these theories usually do not account for cultural differ-ences as will be outlined below Further designinghealth messages in a culture-sensitive way is a chal-lenge31 Thus the effectiveness of materials producedby international and national agenciesmdashin terms ofenhancing understanding and leading to behavioralchangemdashis not well understood both from a theoreticaland practical point of view
This contribution discusses how the interplaybetween the health message and the recipientsrsquo cul-tural characteristics will influence the understandingand effectiveness of health communication Thebasic premise is that congruency between the recipi-entrsquos cultural characteristics and the respective mes-sage as stated in the cultural congruency hypothesis27
will increase message effectiveness leading to deeperprocessing and better understanding in the case ofdecision support or to changes in behavior in thecase of health promotion Culture-sensitive healthcommunication will help to reduce disparities inhealth outcomes by making messages equally under-standable meaningful and effective2232 To achieveeffective health communication in varying culturalcontexts an empirically and theoretically basedknowledge of culture is indispensable In the firstpart of the article we will therefore provide in-depthdefinitions of culture and discuss the etiology of cul-tural differences We will then outline different psy-chological models of culture As theories of(preventive) health behavior and medical decisionmaking do not explicitly incorporate culture asa determinant or moderator we will discuss how cen-tral theoretical constructs such as perceptions ofhealth attitudes or risk vary as a function of cultureWe will also summarize how culture affects the effec-tiveness of communication channels and how it mod-erates well-established effects such as framing Basedon this focused overview of the literature we will pro-vide suggestions for improving culture-sensitivehealth communication in practice (Table 1) We willfinally propose an agenda for health communicatorsfor how to improve structural requirements forculture-sensitive health communication Because ofthe current state of the research literatures the pro-posals identified in this article are evidence-informedrather than evidence-based Thus we will also suggestan agenda for scientists to further improve the evidencebase for culture-sensitive health communication
DEFINING CULTURE-SENSITIVE HEALTHCOMMUNICATION
The idea that medical interventions and treat-ments should be evidence based is well accepted33
In the area of health promotion there is growinginterest in the acknowledged idea that lsquolsquoinforminginfluencing and motivating individual institu-tional and public audiences about important healthissuesrsquorsquo is an art and science itself3435 Further thereis growing understanding that audience insight andapplication of the social sciences and medicalhumanities to diagnose define design and test com-munication interventions is crucial for optimal effec-tiveness and impact36 (for an example of increasingaudience insight see the Guide to Tailoring Immuni-zation Programs (TIP)37 or publications on healthcommunication produced by ECDC38) Psychologicalresearch demonstrates that messages will be pro-cessed more thoroughly28 and be more persuasiveand effective if their content is tailored to the recipi-entsrsquo cognitive affective and motivational character-istics39 (for a broad overview on person 3 situationmodels see ref 40) These characteristics of the recip-ient depend largely on his or her cultural backgroundThis suggests that effective message design woulddepend on understanding these characteristics asthey relate to the cultural infrastructure of messagedelivery41 Further congruency between the messagedesign and the receiverrsquos cultural characteristic willenhance message persuasiveness (cultural congru-ency hypothesis27) Thus when health messages aredesigned to encourage people to exercise eat lessfloss get vaccinated or wash their hands the mes-sagersquos congruence with the recipientrsquos cultural back-ground and the context in which it is delivered affectsthe effectiveness of the message in eliciting individ-ual health behaviors Beyond this targeting (generalcultural adaptation) and tailoring (adaptation to indi-vidual differences within a culture) are not only rele-vant methods in the area of health promotion2842 butalso useful to make the contents of a decision aidmore relevant and understandable to members of dif-ferent cultures For example Hispanic Americansmay perceive the consequences of treatments notonly as relevant for the self but also for related otherssuch as family28 When the information offered iscongruent with cultural values the content is likelyto lead to lsquolsquodeeper thinking which should in turnimprove important accuracy regarding possible bene-fits and harms choices that are more consistent withinformed values and increased participation in deci-sion makingrsquorsquo28(p3) Thus the design of decision aidsshould also take cultural differences into account Wetherefore define culture-sensitive health communica-tion as the deliberate and evidence-informed adapta-tion of health communication to the recipientsrsquocultural background in order to increase knowledgeand improve preparation for medical decision
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 813
making and to enhance the persuasiveness of mes-sages in health promotion
Figure 1 illustrates the idealized process and theinterdisciplinary nature of health communicationFurther it shows where culture-sensitive health com-munication should be included in the process ofdesigning decision aids or health promotion mes-sages Findings from medical science (eg abouttreatments or preventive measures) form the basis ofevidence-based information (facts) that is to be com-municated Behavioral social and communicationscience informs the process of message and informa-tion design (eg questions concerning decision pro-cesses determinants of health) To increase theeffectiveness of messages314344 health communica-tors then adapt these inputs to the receiversrsquo individ-ual psychological characteristics in this case theircultural background This can be done for exampleby targeting cultural subgroups in a campaign withperipheral or linguistic adaptations28 or by tailoringcontents displayed in a decision aid to culturalaspects that are assessed at the beginning of a decisionaid (for examples and items to assess cultural aspectssee Kreuter and others45 Alden and others28)
CULTURE AND CULTURAL DIFFERENCES
Having explicated the definition and need forculture-sensitive health communication we willnow take a closer look at culture as a scientific con-struct which evolutionary and structural factors con-tribute to the development of cultural diversity andhow cultural differences are conceptualized as scien-tific constructs in current models
Defining Culture
Culture is a collective sense of consciousness withboth quantifiable and unquantifiable componentsthat can audibly or silently reveal themselves throughhistory and language46 Culture is never static andis commonly reinforced through structures eventhough those structures are not always palpable andvisible as are physical structures47 Cultural normsmay be acquired in large part through reinforcementlearning While interacting with other members of thesociety individuals are likely to infer what normsexpectations and rules might exist in specific socialsituations Once such social rules are inferred theindividuals will organize their behaviors accord-ingly If the behaviors are accepted or approved bythe others because they are in fact congruent with
the relevant social norms held by others the inferredrules will be reinforced and thus will gradually beinternalized as perceived social norms Recentresearch showed that individuals differ in the degreeto which cultural norms are successfully inferred andacquiredmdashcarriers of certain alleles showed morepronounced cultural differences4849 Thus noteveryone in a cultural group may internalize thenorms of their cultures to the same degree whichleads to individual differences within a culture Cul-tural norms beliefs and practices are influenced bya variety of ecological factors such as traditions inherding versus farming which could explain someof the systematic cultural variability across differentregions of the world today Compared to herdingfarming requires greater degrees of social coordina-tion and interdependence with others (v indepen-dence of each individual)50 Moreover as comparedwith wheat farming rice farming requires far greaterextents of social coordination51 It is plausible thenthat one important reason why Asians tend to bemore interdependent and collectivistic today relativeto Western Europeans is that in Asia (but not in therest of the world) rice has been the primary crop ofthe region over the past several thousand years Cul-ture can also be influenced by numerous relativelymore short-term factors such as settlement historiesSome of the factors that encourage independence ofthe self from others (as opposed to social relationsand interdependence with others) include high resi-dential mobility52 low population density or theabsence of social infrastructures53ndash56 Moreoverrecent cultural neuroscience work has shown thatthis cultural influence is truly lsquolsquodeeprsquorsquo in the sensethat it is inscribed into brain mechanisms5758
Psychological Models of Cultural Differences
A number of organizing dimensions and frame-works have been proposed to account for theobserved cultural differences and provide a theoreti-cal stage for testing predictions One majordimension of cultural difference is the distinctionbetween independence and interdependence of theself vis-a-vis others in the same community59 Ina broad sense contemporary Western cultures tendto be more independent whereas contemporaryAsian cultures tend to be more interdependentCultural systems organized by independence orinterdependence influence every aspect of humanpsychology including cognition emotion and moti-vation5759 Other dimensions include tight versusloose cultures6061 masculine versus feminine
BETSCH AND OTHERS
814 MEDICAL DECISION MAKINGOCTOBER 2016
cultures62 survival versus self-expression63 and cul-tures of honor versus dignity versus face64 Some ofthe proposed frameworks emphasize the systemicinteractions between or mutual constitution ofsocialecological environments and human mindbehavior (eg the socioecological model65ndash67 thecultural ecosystem model68 and sociocultural mod-els69ndash71) Although the field is increasingly witness-ing the examination of different constructs andframeworks to date the one dimension that has cap-tured most attention is the one noted above namelyindividualism and collectivism5960627273 at thelevel of cultural norms or independence and inter-dependence at the level of individual differences
Individualism refers to a cultural syndrome that isorganized by the model of the self as independent Inindividualistic cultures internal attributes are seenas self-defining and both personal autonomy andself-expression are considered as major culturaltasks5960617374 Moreover individuals tend to focuson rights (above duties) with greater priority placedon their personal goals over social welfare or socialgoals They view themselves as agentic using theirpersonal goals and desires to regulate their decisionsand actions In terms of their self-regulatory tenden-cies they are more motivated toward promotion(that is pursuing opportunities) rather than towardprevention (that is not making mistakes) focusingon the positive outcomes they hope to approach
rather than the negative outcomes they hope toavoid75 By contrast collectivism implies a culturalsyndrome that is organized by the model of the selfas interdependent Collectivistic cultures are charac-terized by context dependency malleability andheavy reliance on social relations and membershipsin groups for onersquos self-definition5960 In such cul-tures the focus is on social mutual obligations thefulfillment of in-group expectations and mainte-nance of group harmony59606273 In terms of self-regulatory tendencies in collectivistic cultures peo-ple are more motivated to not make mistakes than topursue opportunities focusing on the negative out-comes they hope to avoid rather than the positive out-comes they hope to achieve75ndash77 The notions ofindependence and interdependence (or individual-ism and collectivism) have been useful to under-stand and predict cross-cultural differences ina variety of psychological processes includinghealth promotion78 There are several scales avail-able that are designed to assess these differences(individualism and collectivism on the level of cul-tural norms62 and independent v interdependentself-construals on the level of individual differen-ces79 and for a short list of items to include as a mea-surement in health promotion tools see ref 80)8182
There remains some debate on the validity of thesemeasures as applied to indices of culturalsyndromes83
Figure 1 The idealized process of culture-sensitive health communication as an evidence-informed way of communicating evidence-
based medical information adapted to the cultural background of the messagersquos receiver
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 815
Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

making and to enhance the persuasiveness of mes-sages in health promotion
Figure 1 illustrates the idealized process and theinterdisciplinary nature of health communicationFurther it shows where culture-sensitive health com-munication should be included in the process ofdesigning decision aids or health promotion mes-sages Findings from medical science (eg abouttreatments or preventive measures) form the basis ofevidence-based information (facts) that is to be com-municated Behavioral social and communicationscience informs the process of message and informa-tion design (eg questions concerning decision pro-cesses determinants of health) To increase theeffectiveness of messages314344 health communica-tors then adapt these inputs to the receiversrsquo individ-ual psychological characteristics in this case theircultural background This can be done for exampleby targeting cultural subgroups in a campaign withperipheral or linguistic adaptations28 or by tailoringcontents displayed in a decision aid to culturalaspects that are assessed at the beginning of a decisionaid (for examples and items to assess cultural aspectssee Kreuter and others45 Alden and others28)
CULTURE AND CULTURAL DIFFERENCES
Having explicated the definition and need forculture-sensitive health communication we willnow take a closer look at culture as a scientific con-struct which evolutionary and structural factors con-tribute to the development of cultural diversity andhow cultural differences are conceptualized as scien-tific constructs in current models
Defining Culture
Culture is a collective sense of consciousness withboth quantifiable and unquantifiable componentsthat can audibly or silently reveal themselves throughhistory and language46 Culture is never static andis commonly reinforced through structures eventhough those structures are not always palpable andvisible as are physical structures47 Cultural normsmay be acquired in large part through reinforcementlearning While interacting with other members of thesociety individuals are likely to infer what normsexpectations and rules might exist in specific socialsituations Once such social rules are inferred theindividuals will organize their behaviors accord-ingly If the behaviors are accepted or approved bythe others because they are in fact congruent with
the relevant social norms held by others the inferredrules will be reinforced and thus will gradually beinternalized as perceived social norms Recentresearch showed that individuals differ in the degreeto which cultural norms are successfully inferred andacquiredmdashcarriers of certain alleles showed morepronounced cultural differences4849 Thus noteveryone in a cultural group may internalize thenorms of their cultures to the same degree whichleads to individual differences within a culture Cul-tural norms beliefs and practices are influenced bya variety of ecological factors such as traditions inherding versus farming which could explain someof the systematic cultural variability across differentregions of the world today Compared to herdingfarming requires greater degrees of social coordina-tion and interdependence with others (v indepen-dence of each individual)50 Moreover as comparedwith wheat farming rice farming requires far greaterextents of social coordination51 It is plausible thenthat one important reason why Asians tend to bemore interdependent and collectivistic today relativeto Western Europeans is that in Asia (but not in therest of the world) rice has been the primary crop ofthe region over the past several thousand years Cul-ture can also be influenced by numerous relativelymore short-term factors such as settlement historiesSome of the factors that encourage independence ofthe self from others (as opposed to social relationsand interdependence with others) include high resi-dential mobility52 low population density or theabsence of social infrastructures53ndash56 Moreoverrecent cultural neuroscience work has shown thatthis cultural influence is truly lsquolsquodeeprsquorsquo in the sensethat it is inscribed into brain mechanisms5758
Psychological Models of Cultural Differences
A number of organizing dimensions and frame-works have been proposed to account for theobserved cultural differences and provide a theoreti-cal stage for testing predictions One majordimension of cultural difference is the distinctionbetween independence and interdependence of theself vis-a-vis others in the same community59 Ina broad sense contemporary Western cultures tendto be more independent whereas contemporaryAsian cultures tend to be more interdependentCultural systems organized by independence orinterdependence influence every aspect of humanpsychology including cognition emotion and moti-vation5759 Other dimensions include tight versusloose cultures6061 masculine versus feminine
BETSCH AND OTHERS
814 MEDICAL DECISION MAKINGOCTOBER 2016
cultures62 survival versus self-expression63 and cul-tures of honor versus dignity versus face64 Some ofthe proposed frameworks emphasize the systemicinteractions between or mutual constitution ofsocialecological environments and human mindbehavior (eg the socioecological model65ndash67 thecultural ecosystem model68 and sociocultural mod-els69ndash71) Although the field is increasingly witness-ing the examination of different constructs andframeworks to date the one dimension that has cap-tured most attention is the one noted above namelyindividualism and collectivism5960627273 at thelevel of cultural norms or independence and inter-dependence at the level of individual differences
Individualism refers to a cultural syndrome that isorganized by the model of the self as independent Inindividualistic cultures internal attributes are seenas self-defining and both personal autonomy andself-expression are considered as major culturaltasks5960617374 Moreover individuals tend to focuson rights (above duties) with greater priority placedon their personal goals over social welfare or socialgoals They view themselves as agentic using theirpersonal goals and desires to regulate their decisionsand actions In terms of their self-regulatory tenden-cies they are more motivated toward promotion(that is pursuing opportunities) rather than towardprevention (that is not making mistakes) focusingon the positive outcomes they hope to approach
rather than the negative outcomes they hope toavoid75 By contrast collectivism implies a culturalsyndrome that is organized by the model of the selfas interdependent Collectivistic cultures are charac-terized by context dependency malleability andheavy reliance on social relations and membershipsin groups for onersquos self-definition5960 In such cul-tures the focus is on social mutual obligations thefulfillment of in-group expectations and mainte-nance of group harmony59606273 In terms of self-regulatory tendencies in collectivistic cultures peo-ple are more motivated to not make mistakes than topursue opportunities focusing on the negative out-comes they hope to avoid rather than the positive out-comes they hope to achieve75ndash77 The notions ofindependence and interdependence (or individual-ism and collectivism) have been useful to under-stand and predict cross-cultural differences ina variety of psychological processes includinghealth promotion78 There are several scales avail-able that are designed to assess these differences(individualism and collectivism on the level of cul-tural norms62 and independent v interdependentself-construals on the level of individual differen-ces79 and for a short list of items to include as a mea-surement in health promotion tools see ref 80)8182
There remains some debate on the validity of thesemeasures as applied to indices of culturalsyndromes83
Figure 1 The idealized process of culture-sensitive health communication as an evidence-informed way of communicating evidence-
based medical information adapted to the cultural background of the messagersquos receiver
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 815
Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

cultures62 survival versus self-expression63 and cul-tures of honor versus dignity versus face64 Some ofthe proposed frameworks emphasize the systemicinteractions between or mutual constitution ofsocialecological environments and human mindbehavior (eg the socioecological model65ndash67 thecultural ecosystem model68 and sociocultural mod-els69ndash71) Although the field is increasingly witness-ing the examination of different constructs andframeworks to date the one dimension that has cap-tured most attention is the one noted above namelyindividualism and collectivism5960627273 at thelevel of cultural norms or independence and inter-dependence at the level of individual differences
Individualism refers to a cultural syndrome that isorganized by the model of the self as independent Inindividualistic cultures internal attributes are seenas self-defining and both personal autonomy andself-expression are considered as major culturaltasks5960617374 Moreover individuals tend to focuson rights (above duties) with greater priority placedon their personal goals over social welfare or socialgoals They view themselves as agentic using theirpersonal goals and desires to regulate their decisionsand actions In terms of their self-regulatory tenden-cies they are more motivated toward promotion(that is pursuing opportunities) rather than towardprevention (that is not making mistakes) focusingon the positive outcomes they hope to approach
rather than the negative outcomes they hope toavoid75 By contrast collectivism implies a culturalsyndrome that is organized by the model of the selfas interdependent Collectivistic cultures are charac-terized by context dependency malleability andheavy reliance on social relations and membershipsin groups for onersquos self-definition5960 In such cul-tures the focus is on social mutual obligations thefulfillment of in-group expectations and mainte-nance of group harmony59606273 In terms of self-regulatory tendencies in collectivistic cultures peo-ple are more motivated to not make mistakes than topursue opportunities focusing on the negative out-comes they hope to avoid rather than the positive out-comes they hope to achieve75ndash77 The notions ofindependence and interdependence (or individual-ism and collectivism) have been useful to under-stand and predict cross-cultural differences ina variety of psychological processes includinghealth promotion78 There are several scales avail-able that are designed to assess these differences(individualism and collectivism on the level of cul-tural norms62 and independent v interdependentself-construals on the level of individual differen-ces79 and for a short list of items to include as a mea-surement in health promotion tools see ref 80)8182
There remains some debate on the validity of thesemeasures as applied to indices of culturalsyndromes83
Figure 1 The idealized process of culture-sensitive health communication as an evidence-informed way of communicating evidence-
based medical information adapted to the cultural background of the messagersquos receiver
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 815
Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

Tightness versus looseness is another way toconceptualize cross-cultural differences in psycho-logical processes This dimension was initially intro-duced by anthropologist Pelto84 and has receivedattention more recently6185 According to this per-spective tight cultures are those that have manyenforced rules and in which individualsrsquo tolerancefor deviance is low and loose cultures are thosethat have few strongly endorsed rules and in whichindividualsrsquo tolerance for deviance is high It hasrecently been shown that there are cross-country61
and within-country85 differences on this dimensionand it can be used to account for cultural (or state-level) variation in personality traits several societalinstitutions and practices and level of constraint ineveryday situations In this recent research tightnessversus looseness has been measured to assess indi-vidualsrsquo perceptions of the tightness versus loosenessof the social norms in the society that they are partof81 rather than individualsrsquo subjective orientationsas tight or loose people To our knowledge howeverthere is no research to date that has employed thisdimension to investigate (or predict) cross-culturallyvariable psychological outcomes related to healthcommunication
In sum culture seems to be a product of historicaldevelopments in herding and farming of social learn-ing and the internalization of norms This accountsfor measurable differences in individualism andcollectivism or equivalently independence andinterdependence which is the most researched con-ceptualization of cultural differences The followingsection focuses on psychological constructs of theo-ries of (preventive) health behavior where literaturesuggests systematic cultural differences
CULTURE AS CONTEXT OF HEALTH BEHAVIORTHEORIES
Theories of preventive health behavior assumethat the attitude toward a preventive behavior pre-dicts uptake of this behavior (eg theory of plannedbehavior8687 theory of reasoned action8889) andthat higher perceived risk will increase preventivebehavior (eg health belief model9091 protectionmotivation theory 9293 overview9495) Interventionsdirected at health promotion often aim at influencingsuch constructs in order to increase healthy orpreventive behavior however the predictive validityof the constructs or the structure of the constructs itselfmay vary according to cultural background96ndash98 Inter-ventions that aim at supporting unbiased decision
making require that the decision makers have a thor-ough understanding of the displayed information(eg of risk information or information relevant toform an attitude toward an intervention or treat-ment)99 A mismatch between the culturally bredmind-set and the information format however mayimpede thorough understanding28 One of the reasonsfor this may be that the aforementioned theorieswhich inform the interventions are not designed toaddress cultural differences regarding the structureof attitudes or the propensity to risky behavior Fur-ther the motivational basis for maintaining healthmay also vary among cultures From a public healthpoint of view maintaining health relies on the contri-bution and cooperation of a large number of individu-alsmdashideally the whole society This is especiallyrelevant for controlling communicable diseases100
To reach societal goals cooperation among individu-als is necessary Cooperation in structurally similardecision situations (eg public goods games) hasbeen shown to vary across cultures101102 The nextparagraphs will therefore discuss findings suggestingthat if interventions aim to influence such basic con-cepts communicators need to consider the recipientsrsquocultural background Table 1 summarizes the dis-cussed aspects and conclusions for culture-sensitivehealth communication
Culture and the Concept of Health and Illness
Culture is an essential building block for con-structing personal understanding of health and ill-ness whether it is in relation to perceptions peoplemay have about their health or in describing theirhealth-seeking practices Understanding the struc-tural influences of dominant cultures is particularlyimportant in any examination of health disparitiesand health decision making The cultural differencesin the views of the self and relationships discussedabove have implications for how health and illnessare experienced and acted upon Individualism onone hand is likely to make individuals focus on thephysical body and wellness thus having a healthybody can be characterized as a goal within an individ-ualistic frame In literature focusing explicitly onAmerican individualism the health-individualismlinkage becomes evident103104 in the American cul-tural focus on wellness avoidance of illness andimprovement of health which is linked to the Amer-ican cultural focus on self-actualization and personalresponsibility Similarly Americansrsquo desire to main-tain their health matches their desire to be autono-mous individuals105106 Collectivism on the other
BETSCH AND OTHERS
816 MEDICAL DECISION MAKINGOCTOBER 2016
Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

Table 1 Summary of Cultural Differences and Implications for Culture-Sensitive Health CommunicationSupporting Medical Decision Making and Optimizing Health Promotion
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Perception of healthand illness
Individualism Focus on physical bodywellness avoidance of illness serves goals ofself-actualization personal responsibilityand autonomyCollectivism Illness as a to-be-avoidedbreakdown in onersquos abilities to carry outobligations concerned with the socialconsequences of health problems health isa resource that facilitates fitting into the socialorder
Medical decision making Personal values mayvary according to cultural backgroundDecision support should provide necessaryinformation (eg about social implicationsof treatments) for the value clarificationprocess
Health promotion Communication strategiesshould address different goals of health orpreventive measures self-actualizationpersonal responsibility and autonomy inindividualistic cultures and socialfunctioning and social consequences incollectivist settings
Attitudes Individualistic cultures Person-centric modelof attitudes Assumed agency of theindividual stable personal preferences guideindependent choice
Collectivistic cultures Normative-contextualmodel of attitudes Attitudes contingent tocontext and integrate the views of others andnorms
Medical decision making Decision supportshould provide necessary information (egabout social implications of treatments) forthe value clarification process
Health promotion While communicationstrategies in individualistic settings shouldfocus on changing personal preferences (egquitting smoking is good for your skin)strategies in collectivistic settings shouldfocus on explicating installing oremphasizing normative factors (eg quittingsmoking reduces secondhand smoke andbenefits the persons around you)
Risk propensity Dread risk and unknown risk are the maindrivers of risk perceptions across culturesMembers of collectivist cultures may rely onsocial resources when taking (financial) risksbut at the same time try to avoid beinga burden to others when it comes to health
Medical decision making Risk communicationfocusing on dread risk (low probability highconsequences) is likely to affect membersfrom different cultures similarly For valueclarification it seems necessary to includeinformation about treatment effects for theself and others depending on culturalcontext
Health promotion Communication strategiesdirected to members from collectivistcultures should stress the avoidance ofpotential losses (loss framing)
Cooperation Punishment is more effective in promotingcooperation in high-trust cultures than inlow-trust cultures
Health promotion Communication strategiesthat rely on punitive incentives of health-related cooperation (eg vaccination) shouldbe used only in high-trust societies
Concepts of power Vertical individualist cultural orientationachieving status and recognition from othersthrough competition power is used foradvancing onersquos personal agenda
Horizontal collectivist cultural orientationsociable and benevolent relations with otherspower is used for benefiting others
Patient-doctor relationship Physiciansrsquocommunication strategies that emphasizeempathy and compassion should be used inhorizontal collectivistic cultures comparedwith vertical individualistic ones
(continued)
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 817
hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

hand is likely to posit illness as a to-be-avoidedbreakdown in onersquos abilities to carry out obliga-tions107108 Having a healthy body can be character-ized as a resource that facilitates fitting into thesocial order within a collectivistic frame Thus forcollectivists the desire to avoid the negative socialobligation consequences of ill health is likely to
matter Although cultural differences and similaritiesin how health is perceived have been understudiedavailable evidence linking self-construal to severalhealth- and illness-related outcomes provides impor-tant insights For example individuals rating them-selves as relational and collective report being moreconcerned with the social consequences of health
Table 1 (continued)
Cultural DifferencesRegarding Description
Implication for Culture-SensitiveHealth Communication
Framing Individualism Approach-oriented moresensitive and responsive to positive outcomesemphasized in gain-framed messages
Collectivism Prevention or avoidanceoriented more sensitive and responsive tonegative outcomes emphasized in loss-framed messages
Medical decision making To enhanceinformation processing and understandingframing of the information should be tailoredto the individual cultural background and bethus congruent with the patientrsquos mind-seteg loss-framed messages for collectivistindividuals and gain-framed messages forindividualistic individuals
Health promotion Communication strategiesto promote a particular health behaviorshould use loss-framed messages forindividuals from collectivistic culturalbackgrounds whereas gain-framed messagesare likely to be more effective for individualsfrom individualistic cultures
Social norms Individualism Individual attitudes rather thannorms predict behavior
Collectivism Social norms predict behaviorTight societies Violations of norms seen asa disruption of social harmony low tolerancefor devianceLose societies High tolerance for deviancefrom social norms
Health promotion Communication strategiesaddressing norms in health messages shouldbe used in collectivistic and tight culturesrather than in individualistic and loosecultures
Strategies relying on punishment should beused in tight rather than loose cultures
Strategies that aim at changing the personalattitude toward a behavior should be used inindividualistic rather than collectivisticcultures
Trust in the media and(health) organizations
individualism Societal components asatomistic autonomous agents and inorganic
Collectivism Social entities are perceived asrelational dynamic and human-like
Medical decision making and healthpromotion Communication strategies todeliver health-related messages byprofessional organizations in individualisticcultures should be more human-like than incollectivistic cultures
Social networks Individualism Companionship and emotionalsupport within large networks
Collectivism Practical assistance and advicewithin small networks
Medical decision making Communicate notonly to the patient but also to the family orsocial network when the patient hasa collectivistic cultural background
Health promotion Communication strategiesin collectivistic cultures should aim atfinding an entering point in small networks(family or intimate peers) and spread fromthere while in individualistic culturesmessages from a larger network may also beaccepted
BETSCH AND OTHERS
818 MEDICAL DECISION MAKINGOCTOBER 2016
problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

problems such as being a burden to and unable to ful-fill responsibilities toward loved ones107 Similarlycollectivistic individuals report experiencing emo-tions that are more socially engaging when thinkingabout imagined and real physical health problems109
for example shame and embarrassment both ofwhich help the individual continue engaging in andassimilating in relationships58110 This could haveconsequences for decision aids for example by usingtailoring to selectively implement information aboutsocial consequences of treatments in decision aidsor by implementing this in the process of clarifyingvalues2845 Thus culture may determine the motiva-tion behind preventive health behavior or medicaldecisions Pointing to the pursued goals may bea potential strategy to adapt communication to cul-tural differences
Culture and the Structure of Attitudes
Attitude toward a behavior or toward treatments isan important predictor in health theories (eg theoryof reasoned action8889 theory of planned behav-ior8687) The currently dominant view of attitudesemphasizes the centrality of personal preferencestheir stability and their internal consistency Thisperson-centric model of attitudes equates personalpreferences with attitudes reflecting primarily West-ern sociocultural assumptions about the agency of theindividual and the importance of stable personalpreferences for guiding independent choice111 Inthis model adjustment to norms often involves aneffortful struggle between the authentic self andexogenous forces However the accumulating cross-cultural literature suggests the need for a complemen-tary perspective a normative-contextual model ofattitudes to acknowledge that in many non-Westerncultural settings attitudes are generally context con-tingent and willingly integrate the views of othersand the norms of the situation111 According to thismodel attitudes need not be personal or necessarilystable and internally consistent and are functionalonly to the extent that they help one to adjust auto-matically to shifting normative and contextualexpectations
The implications of such a model for understand-ing health attitudes and their role in health promo-tion are significant For example it suggests that topromote healthy behaviors in more collectivistic con-texts communication strategies should focus on nor-mative factors rather than personal preferences Themodel highlights the importance of managing thesocial identities that are brought to mind by health
communications112 selectively emphasizing thosereference groups whose normative behaviors are con-gruent with the health message Thus health commu-nication that aims to change attitudes will profit fromconsidering cultural differences in the psychologicalstructure of attitudes and their implications Prefer-ences expressed and decisions made in differentsituations may vary in cultures where attitudestability or cross-situational consistency is neitherexpected nor valued Especially in more hierarchicalcollectivistic cultures this may very much changethe process of shared decision making Unlike inWestern cultures in which it is assumed that thepatient and doctor participate equally attitudesexpressed by the patient in non-Western culturesmay reflect the doctorrsquos views and the norms of thesituation more and make the process less indepen-dent (see also the paragraph below on culture andpower in doctor-patient communications that elabo-rates more on this topic)
Culture and the Propensity for Risky Behavior
Preventive health behavior is strongly related torisk perception If individuals perceive risk theyaim to protect themselves (eg protection motivationtheory9293 health belief model9091) Risk perceptionprocesses have been examined in psychological andsociological research The observations experiencesand subjective evaluations of risky activities wereinvestigated for people who are or may be exposedto hazards The core results of such cross-culturalresearch are socio-psychological models of the cogni-tive structure of judgments about the magnitudeand acceptability of risks with which individualshave to deal113ndash116 Research has explored disparitiesbetween different societal groups looked at the rele-vance of personal links and compared risk judg-ments across countries in which risk issues ingeneral as well as particular risk sources (eg naturalhazards industrial facilities medical dangers) havedifferent salience115117118 Discrepancies betweensocietal groups regarding perceived risk magnitudeand acceptance of risks were stronger than thosebetween countries (eg Australia Brazil GermanyJapan) Other findings show that the two main factorsthat have been identified as main predictors of riskperceptionmdashdread risk and unknown risk116mdashcanbe replicated across a wide range of countries119
Although the cognitive architecture119 appears simi-lar across cultures attitudes toward risky behaviorseem to differ between cultures With regard to finan-cial risks members of collectivistic cultures are less
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 819
risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

risk averse120ndash122 This seems to be in contrast to dif-ferences in regulatory focus123 individuals witha more interdependent self-construal should bemore prevention- or avoidance-oriented in their moti-vations they generally seek to avoid mistakes andfocus on negative outcomes they hope to avoid76
However the findings regarding the risk attitude areexplained by the cushion hypothesis that is theidea that in strong social networks other membersof the network can cushion potential losses Thisshows that by influencing social contact structuresculture can also affect the propensity to riskybehaviors
Culture and Cooperation
To prevent communicable diseases on a societallevel strategies are applied for infection controlthat go beyond the single contribution of one individ-ual One such strategy is herd immunity124 whichmeans that disease transmission in a society isreduced if vaccine uptake is high
This creates a classical situation of a multilateralsocial dilemma in which the decision of one individ-ual determines also the benefit to other people Inother words whereas vaccination causes costs tothe individual (eg due to time money side effects)it protects the vaccinating individual and also pro-vides to everybody around an additional indirect pro-tection Because of this indirect protection byforothers the decision on whether or not to participatein a vaccination program becomes a strategic socialinteraction125126 In such situations the individualbenefit of a preventive measure (such as vaccina-tion100125127) may be smaller than the social benefitTherefore health-related behavior can be partly seenas a prosocial action
Although it is well known that incentives (egrewards and punishments128) and other-regardingpreferences129 are main predictors of cooperationand prosocial behaviors cultural evolution is likelyto have had important effects on the development ofhuman cooperation too130131 Indeed there is atleast some empirical evidence that cooperation isslightly higher in collectivistic cultures than in indi-vidualistic cultures101 However recent research hasshown that these effects are more complicated andmoderated by other factors For instance it has beenshown that cultural variation in cooperation is partic-ularly large in the presence of the possibility to pun-ish39102132 One possible explanation is thattrustmdashthe belief about other peoplersquos benevolencemdashisrequired in order to make punishment work
effectively133 Generalized trust may vary not only onthe individual level but also on the aggregated societallevel134 Therefore punishment more strongly pro-motes cooperation in high-trust (eg China Denmark)than in low-trust (eg Turkey South Africa) culturalgroups and societies which gives potential insightsin how to design and incentivize messages focusingon health-related cooperation If this difference inenforcement of cooperation translates also to vaccina-tion behavior it might be that public appeals toimpose peer pressure on others to go for vaccinationsmight be effective in some but not all cultures Futureresearch will clarify this question One might expectthat institutional punitive incentives to foster health-related cooperation (eg monetary fines in case ofnonvaccination) may be more effective in high-trustthan in low-trust countries
In sum this section posits that even establishedtheoretical concepts that relate to health perceptionand behavior such as attitudes risky behavior orcooperation are subject to cultural variation Thisreduces the generalizability of results across culturesdramatically and in a quite disregarded way The con-cluding agenda for science at the end of this articlewill take up this point and discuss the missingemphasis on culture in health theories
COMMUNICATION STRATEGIES
In this section we will give an overview of differ-ent communication strategies widely used in healthcommunication practice and discuss the implica-tions of cultural differences for the strategiesrsquo effec-tiveness Framing is one of the most researchedcommunication strategies It is used both in persua-sive approaches to health promotion and in decisionaids In addition we will discuss the possibility ofstressing norms and social values to promote healthbehavior
Framing
One basic way in which health communicationscan be distinguished is by how the consequences ofa behavior are framed30135 Health messages thatuse a gain frame emphasize the positive consequen-ces associated with adherence to a behavior such aslsquolsquoIf you stop smoking you will lower your chancesof getting lung cancerrsquorsquo Health messages that usea loss frame emphasize the negative consequencesassociated with nonadherence such as lsquolsquoIf you con-tinue to smoke you will increase your chances of
BETSCH AND OTHERS
820 MEDICAL DECISION MAKINGOCTOBER 2016
getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

getting lung cancerrsquorsquo In the context of health promo-tion framing is welcome as a technique to promotebehavioral change In the context of shared decisionmaking framing represents a challenge as it is lsquolsquodiffi-cult () to avoid influencing decisions in one direc-tion or another () given a) the large number ofbiases that are induced by how information is framedand b) the fact that information must be framed oneway or anotherrsquorsquo20(p7)
Nearly 2 decades of health promotion researchshow that there are differences in the contexts inwhich gain- and loss-framed messages are most effec-tive in producing behavior change One context has todo with the type of behavior being promoted gain-framed messages work somewhat better than loss-framed messages for promoting behaviors that pre-vent the onset of a health condition136 Howeverthe context that appears to most strongly determinethe most effective manner of framing a message hasto do with individual differences related to the mes-sage recipient137 particularly the motivational orien-tation of the message recipient By motivationalorientation we refer to the tendency for a person tobe predominantly motivated by either approachingpositive outcomes (approach motivation) or thetendency to be motivated by avoiding negative out-comes (avoidance motivation138139) This approach-avoidance distinction shares some commonalitywith the promotion-prevention distinction made byregulatory focus theory123 For people who are dispo-sitionally more approach motivated or promotion ori-ented gain-framed messages are more effective Incontrast for people who are dispositionally moreavoidance oriented or prevention focused loss-framedmessages are typically more effective This has beenfound across a wide variety of health behaviorsincluding oral health140 human papillomavirus vacci-nation141142 diet143144 and smoking prevention145
As outlined above people from more individualis-tic cultures may be more promotion or approach ori-ented and therefore more sensitive and responsive tothe positive outcomes emphasized in gain-framedmessages On the other hand people from more col-lectivistic cultures may be more prevention or avoid-ance oriented and therefore more sensitive andresponsive to the negative outcomes emphasized inloss-framed messages Several recent studiesmdashallconducted in the domain of oral healthmdashsupportthese hypotheses In Iran a moderately collectivisticcountry a loss-framed (v gain-framed) message led tosignificantly greater levels of flossing at 2-wk and 6-mo follow-ups as well as better overall periodontalhealth at a 6-mo follow-up146 Among East Asians
living in the United Kingdom loss-framed messageswere viewed as more persuasive than gain-framedmessages whereas the reverse was true among whitesliving in the United Kingdom27 Furthermore thesegroup differences were mediated by individual dif-ferences in motivational orientation Lastly a recentstudy of nearly 900 adults residing in the UnitedStates (the most individualistic country) founda strong relationship between exposure to US cultureand peoplersquos responses to framed messages147
Among adults who had the greatest exposure to USculturemdashin terms of parental heritage and proportionof life spent in the United Statesmdashthere was if any-thing a greater advantage for gain-framed messagesHowever among adults with less exposure to USculturemdashhaving parents born in another countryandor less proportion of their life spent in the UnitedStatesmdashthere was a significant advantage of loss-framed messages
Taken together these recent studies suggest thatmessage framing is one important aspect of culture-sensitive health communication If the goal of a mes-sage is to promote a particular health behavior then itmay be that loss-framed messages will be more effec-tive for individuals from collectivistic cultural back-grounds Of course more research is needed to testthese cultural hypotheses with a wider range of popu-lations and health behaviors In reference to shareddecision making there is still no solution of how toframe information Displaying both gain- and loss-framed information can be a solution future researchshould investigate however if cultural backgroundsmakes either of the 2 frames more salient
Addressing Norms and Social Values
Health behaviors are affected not only by individ-ualsrsquo own attitudes and risk perceptions but also byperceived attitudes and behaviors of others If certainvalues beliefs attitudes and behaviors are generallyapproved in a certain social environment theystrongly guide individualsrsquo behaviors Such subjec-tive norms89 or social norms119 may influence indi-viduals either as a response to the perception ofprevalent behaviors (descriptive norms) or as a pres-sure to conform (injunctive norms)148 Clearly com-municating social norms may be relevant in healthpromotion to persuade people to adopt healthybehaviors by communicating both lsquolsquodosrsquorsquo (eg lsquolsquoVac-cinatersquorsquo) and lsquolsquodonrsquotsrsquorsquo (eg lsquolsquoDonrsquot smokersquorsquo)
Although social norms exist across cultures andsocieties the importance and even the content ofsocial norms may differ largely For example
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 821
smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

smoking is socially more accepted in Europe than inthe United States149 Addressing the impact of onersquossmoking behavior on others may therefore be a moresuccessful persuasion strategy to stop smoking inthe United States than in Europe Besides their con-tent social norms are generally more important forindividual behavioral intentions in collectivistic cul-tures compared with individualistic cultures wherepersonal preferences receive more weight and areless likely to incorporate normative content111150151
In addition cultures differ in how norm violationsare sanctioned that is the presence of injunctivenorms tight societies have clear and pervasive socialnorms and violations from these rules are seen asa disruption of social harmony61152 Therefore giventhat a certain health behavior is shared as a socialnorm addressing this norm in health promotion mes-sages is likely to have more impact on individualbehaviors in collectivistic and tight cultures than inindividualistic and loose cultures111 Decision aidsas mentioned earlier should reflect cultural differen-ces in social norms and values in targeting andtailoring the programs to the user28 It is argued thattailored information leads to increased engagementand processing fluency which in turn lead to moregist knowledge and higher preparation for decisionmaking one of the outcome measures that are usedto evaluate decision aids28
The literature discussed so far concentrated on thereceiver of health messages and on the potentialeffects of culture on attitudes risk perception andbehavior as well as the effectiveness of communica-tion techniques The following section will turnto the channels that are used to disseminate theinformation
CULTURE AND CHANNELS OF HEALTHCOMMUNICATION
For the process of shared decision making thepatient usually needs information materials such asdecision aids or pamphlets and a personal face-to-face interaction with a doctor In this direct com-munication between practitioners and patientsconcepts of power that are related to cultural differen-ces may affect the impact of the information Healthpromotion messages often use channels other thanface-to-face communication They often originatefrom national or international health organizationssuch as the CDC ECDC or WHO Health care person-nel disseminate the information or it finds its waydirectly to the decision maker either through a broad
range of media such as television newspapers theInternet or through virtual or real social networks153
Culture shapes how people act and interact in dyadssocial networks or how they trust their nationalmedia The following paragraph therefore discussescultural differences that may affect the effectivenessof channels used to disseminate health informationfrom direct face-to-face communication to mediaand social networks
Culture and Power in Doctor-PatientCommunications
Doctors are in a position of considerable powerA review about doctor-patient communicationconcludes that due to this power lsquolsquoHippocrates sug-gested that doctors may influence patientsrsquo health Effective doctor-patient communication can bea source of motivation incentive reassurance andsupportrsquorsquo154(p42) Likewise in the literature poweris seen as instrumental for achieving culturally nur-tured goals155 However those goals are likely to dif-fer as a function of cultural values national cultureand ethnic group As a result recent research showsthat the meanings and goals associated with powerare culturally patterned156157 A vertical individual-istic cultural orientation characterized by concernsabout achieving status and recognition from othersthrough competition is linked to seeing power assomething to be used for advancing onersquos personalagenda and promoting onersquos powerful status158 a per-sonalized power concept In contrast a horizontalcollectivistic cultural orientation characterized byan emphasis on sociable and benevolent relationswith others is linked to seeing power as somethingto be used for benefiting others a socialized powerconcept
Differences in power can endanger the process ofshared decision making159 One implication of thesedistinct power concepts is that cultural groups thatdiffer in these cultural orientations differ in the waythey tend to evaluate power holders such as doctorsBecause physicians are often in positions of powerover patients evaluations of onersquos medical care arelinked to distinct normative expectations about phy-sician behavior For instance there is evidence thatwhen power is salient (versus not salient) a physi-cianrsquos level of compassion may be more importantin predicting the satisfaction of patients from hori-zontal collectivist cultures (eg Hispanics) versuspatients from vertical individualist cultures (egAnglo whites) because horizontal collectivist cul-tures tend to emphasize empathy and support in
BETSCH AND OTHERS
822 MEDICAL DECISION MAKINGOCTOBER 2016
power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

power relationships to a greater degree160 Peoplefrom more horizontal collectivistic compared withvertical individualistic cultural backgrounds mayalso differ in the sources they turn to for supplement-ing the advice they receive from physicians Forinstance friends and family may be more importantsources of advice for people from horizontal collec-tivistic cultural backgrounds As a result physiciansmay be advised to communicate not only with theirpatients but also with their family members In addi-tion health communication efforts in horizontalcollectivistic cultural contexts would be advised toplace greater emphasis on stimulating word-of-mouth communication among trusted sources ofsocial support Knowing about cultural differencesthat affect doctor-patient relationships and patientsatisfaction can thus improve health communicationefforts
Culture and Trust in (Health) Organizationsand Media
Trust in health organizations governments andthe media facilitates effective health communica-tion161 The concept of trust includes several aspectsof beliefs and feelings such as credibility securityand reliability162 and is established through interac-tions in diverse social networks (eg family friendsand acquaintances) An analysis of trust and itsmeaning for health care systems states that lsquolsquohealthsystems are inherently relational and so many of themost critical challenges for health systems are rela-tionship and behavior problemsrsquorsquo163 Trust as inany personal relationship has been identified asa central factor also because national health organi-zations are part of a political system that decides oncertain public health measures Trust is thereforeclosely related to the legitimacy of state actionswithin a health system thus health organizationscan be seen as the executive arm of political struc-tures163 Traditionally there is much cultural varia-tion of trust in governments We will not go intosociological and political details here but refer onlyto psychological differences that are relevant for dif-ferences in trust
People with independent self-construals concep-tualize societal components as atomistic and autono-mous agents whereas those with interdependentself-construals conceive social entities as relationaland dynamic164165 In a similar vein collectivisticindividuals are more likely to perceive social groupsas cohesive united and intrastructured166 as well asto show greater anthropomorphism toward
nonhuman agents167 than do more individualisticpeople Thus the persuasiveness of a message deliv-ered by health organizations might differ according toculture To those who are suspicious about trustwor-thiness of these institutions health-related messagesmight be more reachable if they are delivered byhuman-like entities rather than inorganic ones Com-pared with members of individualistic culturesmembers of collectivistic cultures would interpreta message from health organizations as if they receiveit from other people This may increase the effective-ness of such messages
Culture and Social Networks
Health organizations increasingly use onlinesocial networks such as Facebook or Twitter todirectly disseminate health messages In summer2015 WHO for example had more than 25 millionfollowers on Twitter and CDC shares its Facebookmessages with more than 480000 followers Onlinenetworks are likely to reach even more peopleindirectly because followers often share informationwithin their social networks Social networkembeddedness tends to motivate people to pass alonghealth-related information (for an overview see ref168) Such an indirect information exchange may beeven more effective than direct information becauseof the trust and obligations in private social net-works169 There is evidence of cultural differencesin what is emphasized within a social network offriends Adams and Plaut164 compared the conceptof friendship shared in an individualistic country(United States) with that of a collectivistic country(Ghana) based on the assumption that independentand interdependent self-construals establish aninternalized system for constructing social realityIn terms of friendship members of the individualis-tic culture tended to highlight companionship andemotional support within large networks whereascollectivists tended to accentuate practical assis-tance and advice within small networks Thuseffective ways to deliver health messages in socialnetworks could vary based on culture People inindividualistic cultures might accept messagesfrom those who are well intentioned to help Con-versely people in collectivistic cultures mightapprove messages from their family or intimatepeers who feel obligated to help This may apply toreal and virtual social networks however moreresearch is needed to clarify whether the culturaldifferences in patterns of communication are alsofound in large-scale online social networks
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 823
including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

including a mixture of people from diverse culturalbackgrounds
AN AGENDA FOR SCIENCE
In this section we will propose an agenda for sci-entists to further develop the evidence base for cul-ture-sensitive health communication both regardinghealth promotion and the area of medical decisionmaking We will first discuss the implications of theprevious paragraphs for theorizing and research prac-tices Further a range of open research questions andmethodological considerations will be summarizedFinally we will discuss the relationship betweenbasic and applied research and argue for a greaterintegration of the two
Theorizing and Research Practices in Psychologyand the Ignorance of Cultural Differences
Faced with the challenge of addressing a publichealth issue practitioners are advised to rely on evi-dence-based strategies and to use these strategies ina manner that is sensitive to the cultural back-ground(s) of the targeted population We believethese to be sound recommendations but the abilityof practitioners to follow them and to employevidence-based culturally sensitive communicationstrategies depends on the utility of the current empir-ical evidence and theoretical models Althoughinvestigators have demonstrated that communicationstrategies such as framing can vary in their effective-ness when used across different cultural groups27
the majority of these findings have yet to be integratedinto a model that would afford clear precise predic-tions regarding when and for whom different inter-vention approaches should be used In the absenceof a model that integrates theories of culture with the-ories of health behavior and behavior change practi-tioners are able to observe that communicationstrategies can work differently across cultural groupsbut will find it difficult to predict a priori when thesestrategies will and will not differ in their effective-ness across cultural groups Thus to obtain thedesired advances in practice it is essential that inves-tigators initiate a scientific agenda that will enablethe synthesis and testing of theories of culture andtheories of health communication
As stated earlier theories of health behavior andbehavior change do not explicitly incorporate cul-tural differences even though the theoretical con-structs used to predict behavior or the predicted
behavior (or outcome) itself may differ in structurebetween cultures At the moment it seems as if thereis a divide between cultural psychology and psychol-ogy It is important to recognize however that psy-chological research always includes culturemdashwhileit may not take a comparative view the theories andresults may be generalizable to only a certain culturalbackground This may apply to disciplines other thanpsychology as well such as communication or publichealth Seeing a greater impact of cultural researchand more awareness of the influence of culture onmainstream theorizing will make theories more prac-tical for global public health efforts Future researchshould focus on how engaging with cultural variabil-ity in theoretical constructs can shape and expandthe theoretical questions posed and the interpretationof answers obtained Scientific attention should bedirected to the questions of which theories and con-structs are interculturally applicable or informedand how this can be determined170 This followsfrom the idea that lsquolsquoboth theorists as well as interven-tionists need to treat a theory as a dynamic entitywhose form and value rests upon it being rigorouslyapplied tested and refined in both the laboratoryand the fieldrsquorsquomdashin a cross-cultural setting171(p1)
One example for an important step is the expansionof the attitude concept with a cross-cultural perspec-tive111 The normative-contextual model of attitudesexplicitly addresses non-Western contexts andthereby explicates the potential limitations of gener-alizing the Western perspectivesmdashthe person-centricmodel of attitudes that guided decades of attituderesearch
Research practices also contribute to the neglect ofcultural differences Cross-cultural research is expen-sive and makes international cooperation necessaryOften convenience samples are used and culturaldifferences are assessed in terms of differencesbetween countries However culture should beunderstood as individual differences in motivationaland cognitive characteristics rather than be deter-mined by state borders Thus when researchers arefocusing on cultural differences they should expli-cate the psychological background of their conceptof culture and the implications for theoretical con-cepts and theorizing Research examining psycholog-ical consequences linked to independence andinterdependence originates primarily from compara-tive studies conducted in the West (primarily NorthAmerica) and the East (primarily East Asia) becauseas noted above Western cultures are hypothesized tobe relatively more independent or less interdepen-dent compared with Asian cultures Thus as with
BETSCH AND OTHERS
824 MEDICAL DECISION MAKINGOCTOBER 2016
most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

most research in psychology cross-cultural researchis carried out in so-called WEIRD countries (whereWEIRD stands for Western Educated IndustrializedRich Democratic) Even cross-cultural research canbe restricted to WEIRD countries for example if weconsider a comparison between university studentsin the United States and Singapore There is a consid-erable lack of research in this area conducted in Rus-sia Africa South America or even (Eastern) EuropeRecently however there is an increasing effort toexamine understudied cultural contexts such as theMiddle East50 and Europe53 This research helps usrefine the dimension of independence and interde-pendence (or individualism and collectivism) byintroducing different forms in which these conceptscan occur and account for psychological pro-cesses172173 Ideally the samples should be extendedto less educated participants by recruiting partici-pants from nonuniversity and understudied settingsThis seems especially important in a health contextin which effective messages are necessary to dissem-inate information also to hard-to-reach groups whichare usually not university students
Research Questions
The common thread in this article stresses the exis-tence of differences among cultures However moreresearch is needed to determine the conditions underwhich cultural differences are and are not relevant tomedical decision making and the successful imple-mentation of an intervention strategy One suchexample in health promotion is nudging This tech-nique for encouraging health behavior has gainedrecent popularity29174 Nudging refers to alteringthe design of the choice environment so as to facili-tate selection of the healthy option while maintain-ing the freedom to select any option In a well-known example175 in some European countries theorgan donation default is donation such that one ispresumed to be a donor unless one opts out whereasin other European countries the default is nondona-tion such that one is presumed to be a nondonorunless one opts in Donation rates are much higherin the former countries than the latter even thoughresidents of both types of countries have both optionsavailable In addition to defaults other nudges thathave been shown to influence health behaviorsinclude framing effects prompts to form implemen-tation intentions the order in which options are pre-sented social norms and financial incentivesVirtually all research on nudging has been conductedin Western and WEIRD contexts and it is currently
unknown whether some nudges fit certain culturalcontexts better than others As the summarizedresearch above suggests at least some nudgesmdashframing emphasis of social normsmdashshould be adap-ted to the cultural background
Next as stressed before there is a great need tounderstand cultural differences based not on nationaldifferences but on individual differences2845 Oneimportant question is which instrument of measure-ment can make these differences easily accessibleand measurablemdashalso for practitioners Alden andcolleagues28 suggest applying a short measure of indi-vidual differences45176 before the actual decision aidstarts This purpose makes it evident that the meas-ures need to be short easy to use and valid If we can-not come up with a short and easy measure it will benecessary to search for proxies that can be used toestimate cultural characteristics and facilitate thedecision if culture-sensitive communication strate-gies are required
Beyond the individualismcollectivism dimen-sion we will need a better understanding of howother basic dimensions of culture such as tightnesslooseness61 or cultural values62 relate and interactwith basic features of messaging (format channelsframing etc) Further the implications of culturaldifferences for culture-sensitive health communica-tion that were summarized in Table 1 all describeimportant research questions these assumptions stillneed to be tested in applied settings
Methodological Considerations
The effect of health communication can beassessed with a variety of research methodologiesincluding focus groups questionnaire studies andlaboratory experiments One of the most powerfuland convincing techniques however are random-ized field experiments in which participants receivethe targeted health communication intervention orthe control condition in a real-world setting withoutever being aware that a research study is being con-ducted Such a design allows researchers to assessthe interventionrsquos impact on understanding of theissue as well as actual behavior within the partici-pantsrsquo real cultural setting This may prevent demandeffects reactance or other influences of participantsknowing that they are part of a research study Suchfield studies are labor intensive to launch and oftenrequire critical partnerships with local healthorganizations but they are especially important forculture-sensitive research in which cultural differ-ences may be most apparent when individuals are
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 825
behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

behaving in their everyday environments rather thanin a research laboratory or responding to questions ona survey
Cultural factors also have fundamental implica-tions for interpretation of research results Particu-larly for measures of sensitive topics such as healthself-reports distinct patterns of socially desirableresponding are likely to complicate the interpretationof substantive cultural differences Indeed researchshows that cultural differences map onto 2 distinctforms of socially desirable responding self-deceptiveenhancement refers to the tendency to provideinflated assessments of onersquos skills and quali-ties177178 and is more likely to be observed amongWesterners179 or in situations in which an indepen-dent self-construal is salient180 Impression manage-ment refers to the tendency to downplay onersquostransgressions in order to appear normatively appro-priate177178 and is more likely to be observed amongEast Asians179 or in situations in which an interde-pendent self-construal is salient180 These resultssuggest that Westerners may be more likely to giveinflated self-reports of their health knowledge andskills (eg in decision aid settings) whereas Eastern-ers may be more likely to downplay their unhealthybehaviors and transgressions (eg in health promo-tion settings) Such patterns will appear as substan-tive differences between cultural groups althoughthey may actually reflect distinct response styles
Relationship between Basic and Applied Research
Traditionally researchers engaged in basicresearch focus on increasing understanding of scien-tific questions and phenomena whereas researchersengaged in applied research focus on how estab-lished research findings can be used to benefit indi-viduals or society One implication of this construalis that it frames basic and applied research activityas lsquolsquoseparate ventures pursued by different peo-plersquorsquo181 Moreover it may serve to undermine thegrowing need for greater engagement between theoryand practice182 As illustrated by the issues raisedearlier in this article advances in the use of culturallysensitive health communication will depend on moreengaged interaction between researchers and practi-tioners To this end initiatives are needed that willbetter integrate basic and applied research activityand in particular that will support investigatorswho are actively engaged in pursuing advances inunderstanding and use what Stokes182 has character-ized as Pasteurrsquos quadrant (for further discussion ofthese issues see refs 182 183)
AN AGENDA FOR HEALTH COMMUNICATIONPRACTICE
Also from an applied point of view we would liketo stress the importance of a strong partnershipbetween research and practice In the following wewill discuss the value of taking up a more generalapproach to evidence-informed health communica-tion and rethink traditional structures and traditionsin health communication Further we argue thathealth communication expertise should be strength-ened in organizations both regarding training of pro-fessionals as well as regarding the knowledge aboutcultural backgrounds of target groups Health com-munications training should also be strengthenedand scaled up as part of standard medical educationand possible stand-alone in-service training mod-ules As a positive example of successful health com-munication we will summarize the actions taken upto curtail polio in Israel a highly culturally diversecountry
Partnership between Science and Practice
It is the responsibility of national health authori-ties supported by international health organizationsto facilitate networking between public health profes-sionals and researchers to exchange experience andmake evidence-based information easily accessiblefor those who work in the field Studies on health com-munication have brought valuable insights to thetopic but it has been also recognized that there is animportant need to better understand the factors thatdetermine the effectiveness of communication inreal-life situations in different countries As aforemen-tioned more resources are needed to systematicallytest and compare culture-sensitive interventions inthe field Health authorities should recognize theimportance of supporting such studies and providinga stable partnership with researchers
By drawing on research from behavioral econom-ics the medical humanities psychology and neuro-science to understand how humans behave andmake decisions in everyday life and by better under-standing how people respond to different contextsand incentives communicators will be better equip-ped to tackle not only communicable diseases butequally noncommunicable diseases and potentiallyimprove community-based care messaging andpatient activation Developing the tools to gain betterconsumer insight including cultural context andspecificity also has considerable potential impacton responding to outbreaks and in health emergency
BETSCH AND OTHERS
826 MEDICAL DECISION MAKINGOCTOBER 2016
settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

settings where a rapid and accurate understanding ofthe populations affected by the outbreak or emer-gency is essential to appropriate planning andresponse strategy184
Training of Health Communicators
The complexity of culturemdashas well as of design-ing decision aids or changing behavior throughcommunicationmdashshows that health communicatorsneed academic training Only few social scientists orpsychologists work in communication sections ofnational or international health authorities or agen-cies This is the case despite the fact that the transferalof research to practice the implementation of communi-cation interventions and initiatives that are sensitive tocultural specificities are dependent on an investmentin human resource capacity building and skills alignedwith communication research design and evaluationBehavioral insights among health authorities are essen-tial to ensure that communication knowledge is bothshared and integrated across communicable and non-communicable disease prevention programs alike Nota-ble progress has been made in forwarding this agendaThe WHO European Regional Office for Europe forexample has been successful in encouraging nationalhealth authorities to invest in behavioral insights pro-grams and the diagnosis of factors determining health-seeking behavior One example is the application ofTIP37 a guide developed to diagnose demand- and sup-ply-side barriers and motivators of behavior The find-ings can assist authorities in designing low-cost subtleinterventions that influence the behavior of the publicand result in bottom-line health impact The TIP toolhas been used in 3 countries to date and capacity withinthose health authorities was enhanced as a result of itsapplication185
Knowledge about Cultural Differences in Practice
Health communicators need a strategy to assessand address cultural differences As an example wewill sketch a model that may be a useful tool forexploring cultural differences especially if the best-case scenario is not possible in which the communi-cator is from within the cultural context or commu-nity and is engaged in designing the responsemessaging and materials The PEN-3 model offersa cultural lens for addressing health issues and prob-lems186 It provides the analyst with 3 levels of anal-ysis namely 1) cultural identity 2) relationship andexpectations and 3) cultural empowerment Eachlevel can be further described with 3 aspects (cultural
identity person extended family neighbors rela-tionships and expectations perceptions enablersnurturers cultural empowerment positive existen-tial negative) The analysis can be completed in 2phases In the assessment phase the analysts conductinterviews to generate qualitative data which arethen categorized into 9 cells In the interventionphase the community groups the data into the PEN-3 categories The community and analyst then sharepoints of agreement and differences In the end theanalyst and community discuss and prioritize whatwould be the most impactful domain for a culture-sensitive communication or intervention based onthe 3 cultural identity domains As a consequencePEN-3 helps researchers to reexamine assumptionsabout health-related behaviors and thus to reexaminecultural biases This may be the starting point fora culture-sensitive approach of health communica-tion It can assist in cultural targeting and to craft spe-cifically tailored messages responding to individualdifferences that were identified within subgroupsand the cultural context This model has been suc-cessfully applied in the context of HIVAIDS inAfrica
Another very positive example of successfulculture-sensitive health communication we wouldlike to outline is the communication campaign inIsrael in 2013185 Wild polio virus was found in sew-age samples which made supplementary immuniza-tion activities necessary The challenges weremanifold the population was largely immune dueto high vaccination coverage However especiallychildren born after 2005 had to be revaccinatedwith a vaccine that reduced transmission This wasthe case because in 2005 Israel changed their vacci-nation policies to use a vaccine that reduced therisk of vaccine-induced polio but offered no reduc-tion in disease transmission once infected Theymade a prosocial appeal lsquolsquoJust two drops and the fam-ily is protected from the risk of poliorsquorsquo From a psycho-logical point of view we can interpret that there wasa good match between Israelrsquos tendency to low indi-vidualism (eg as compared with the UnitedStates187) This match may have led to a high effec-tiveness of the campaign in this country Moreovera sophisticated system of communication surveil-lance consisted of all types of mediamdashnot onlyprinted pamphlets but also electronic and socialmedia Surveillance means that communication wasalso reactive thus large parts of the iterative commu-nication process was listening and responding to theconcerns and needs of the people Different strategiestook cultural differences into account (eg by
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 827
including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

including religious leaders) The example of Israelshows that it is very important that health communi-cators know their audience very well and withregard to crisis communication they ideally knowtheir audience before any crisis emerges Thusa step toward culture-sensitive health communica-tion can be to move from telling to listening to learn-ing about cultural differences and contexts
CONCLUSIONS
In sum it is clear that culture-sensitive healthcommunication is important for both improvingunderstanding in the medical decision-making pro-cesses as well as promoting health behavior acrossa large and growing cultural diversity within coun-tries and continents There is considerable knowl-edge about certain cultural concepts such asindividualism and collectivism Yet many other cul-tural differences exist and there is still no techniquefor practitioners to easily identify cultural character-istics that could facilitate adopting culture-sensitivecommunication strategies Moreover the relativeeffectiveness of alternative cultural communicationtechniques remains unclear Considerable theoreticaland empirical exchange with practitioners shouldadvance culture-sensitive health communicationWith this contribution we aim to inspire a lsquolsquopoly-loguersquorsquo that is a conversation with complete multi-lateral influence188189 We would like to promotethe need for more interdisciplinary research bothbetween scientific disciplines and between scienceand practice As a guiding example and motivationfor higher-level engagement between practitionersand social scientists we believe the image of Pas-teurrsquos quadrant should be displayed on the walls inmore officesmdashof basic and applied scientists as wellas health agencies and communicators as partners
ACKNOWLEDGMENTS
This contribution is based on intense discussions amongthis articlersquos authors The discussions took place during thescientific small-group meeting of experts on lsquolsquoCulture-Sensi-tive Health Communicationrsquorsquo Cornelia Betsch and RobertBohm convened the meeting in Erfurt Germany in May2014 The organizers gratefully acknowledge the meetingrsquosgenerous support by the WHO Regional Office for EuropeECDC German Research Foundation (DFG BE39706-1)University of Erfurt and RWTH Aachen University
REFERENCES
1 Charles C Gafni A Whelan T Decision-making in the
physicianndashpatient encounter revisiting the shared treatment
decision-making model Soc Sci Med 199949(5)651ndash61
2 Hoerger M Epstein RM Winters PC et al Values and options in
cancer care (VOICE) study design and rationale for a patient-
centered communication and decision-making intervention for
physicians patients with advanced cancer and their caregivers
BMC Cancer 201313(1)188
3 Whitney SN A new model of medical decisions exploring the
limits of shared decision making Med Decis Making 200323(4)
275ndash80
4 Braddock CH The emerging importance and relevance of
shared decision making to clinical practice Med Decis Making
201030(5)5ndash7
5 Pauker SG Medical decision making how patients choose Med
Decis Making 201030(5)8ndash10
6 Halvorsen PA What information do patients need to make
a medical decision Med Decis Making 201030(5)11ndash3
7 Mathieu E The Internet and medical decision making can it
replace the role of health care providers Med Decis Making
201030(5)14ndash6
8 Fowler FJ The origins of the DECISIONS survey Med Decis
Making 201030(5)17ndash9
9 Zikmund-Fisher BJ Couper MP Singer E et al The DECISIONS
study a nationwide survey of United States adults regarding 9
common medical decisions Med Decis Making 201030(5)
20ndash34
10 Fagerlin A Sepucha KR Couper MP Levin CA Singer E
Zikmund-Fisher BJ Patientsrsquo knowledge about 9 common health
conditions the DECISIONS survey Med Decis Making 2010
30(5)35ndash52
11 Hoffman RM Lewis CL Pignone MP et al Decision-making
processes for breast colorectal and prostate cancer screening
the DECISIONS survey Med Decis Making 201030(5)53ndash64
12 Ratanawongsa N Zikmund-Fisher BJ Couper MP Van Hoe-
wyk J Powe NR Race ethnicity and shared decision making for
hyperlipidemia and hypertension treatment the DECISIONS sur-
vey Med Decis Making 201030(5)65ndash76
13 Sepucha KR Fagerlin A Couper MP Levin CA Singer E
Zikmund-Fisher BJ How does feeling informed relate to being
informed The DECISIONS survey Med Decis Making 2010
30(5)77ndash84
14 Zikmund-Fisher BJ Couper MP Singer E et al Deficits and
variations in patientsrsquo experience with making 9 common medical
decisions the DECISIONS survey Med Decis Making 201030(5)
85ndash95
15 Dillard AJ Couper MP Zikmund-Fisher BJ Perceived risk of
cancer and patient reports of participation in decisions about
screening the DECISIONS study Med Decis Making 201030(5)
96ndash105
16 Couper MP Singer E Levin CA Fowler FJ Fagerlin A
Zikmund-Fisher BJ Use of the Internet and ratings of information
sources for medical decisions results from the DECISIONS survey
Med Decis Making 201030(5)106ndash14
BETSCH AND OTHERS
828 MEDICAL DECISION MAKINGOCTOBER 2016
17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

17 Barry MJ Edgman-Levitan S Shared decision makingmdashthe
pinnacle of patient-centered care N Engl J Med 2012366(9)
780ndash1
18 Stacey D Legare F Col NF et al Decision aids for people fac-
ing health treatment or screening decisions Cochrane Database
Syst Rev 20141CD001431
19 Chapman GB Sonnenberg FA Decision Making in Health
Care Theory Psychology and Applications Cambridge Cam-
bridge University Press 2003
20 Abhyankar P Volk RJ Blumenthal-Barby J et al Balancing the
presentation of information and options in patient decision aids
an updated review BMC medical informatics and decision mak-
ing 201313(2)6
21 Trevena LJ Zikmund-Fisher BJ Edwards A et al Presenting
quantitative information about decision outcomes a risk commu-
nication primer for patient decision aid developers BMC Med
Inform Decis Making 201313(2)7
22 International Decision Aid Standards (IPDAS) Collaboration
Resources [Internet] 2015 [modified 2013 Nov 29] Available
from URL httpipdasohricaresourceshtml
23 Prochaska JO DiClemente CC Stages and processes of self-
change of smoking toward an integrative model of change J Con-
sult Clin Psychol 198351(3)390ndash5
24 Andreasen AR Marketing Social Change Changing Behavior
to Promote Health Social Development and the Environment
San Francisco Jossey-Bass 1995
25 Updegraff JA Rothman AJ Health message framing modera-
tors mediators and mysteries Social and Personality Psychology
Compass 20137(9)668ndash79
26 Li M Chapman GB Nudge to health harnessing decision
research to promote health behavior Social Psychology Compass
20137(3)187ndash98
27 Uskul AK Sherman DK Fitzgibbon J The cultural congruency
effect culture regulatory focus and the effectiveness of gain- vs
loss-framed health messages J Exp Soc Psychol 200945535ndash41
28 Alden DL Friend J Schapira M Stiggelbout A Cultural target-
ing and tailoring of shared decision making technology a theoreti-
cal framework for improving the effectiveness of patient decision
aids in culturally diverse groups Soc Sci Med 20141051ndash8
29 Trevena L Zikmund-Fisher B Edwards A et al Presenting
probabilities In Volk R Llewellyn-Thomas H eds Update of
the International Patient Decision Aids Standards (IPDAS) Collab-
orationrsquos Background Document Chapter C [Internet] 2012
Available from URL httpipdasohricaresourceshtml
30 Reyna VF Nelson WL Han PK Dieckmann NF How numer-
acy influences risk comprehension and medical decision making
Psychol Bull 2009135(6)943
31 Kreuter MW McClure SM The role of culture in health com-
munication Annu Rev Public Health 200425439ndash55
32 Kreps GL Communication and racial inequities in health care
Am Behav Sci 200649(6)760ndash74
33 Eddy DM Evidence-based medicine a unified approach
Health Aff 200524(1)9ndash17
34 Healthy People 2010 2nd ed Washington DC US Department
of Health and Human Services 2000
35 Bernhardt JM Communication at the core of effective public
health Am J Public Health 200494(12)2051ndash3
36 Wurz A Nurm UK Ekdahl K Enhancing the role of health
communication in the prevention of infectious diseases J Health
Commun 201318(12)1566ndash71
37 World Health Organization Guide to Tailoring Immunization
Programs (TIP) Available from URL httpwwweurowhoint
enhealth-topicscommunicable-diseasespoliomyelitispublicati
ons2013guide-to-tailoring-immunization-programmes
38 European Centre Disease Prevention and Control Publica-
tions Available from URL httpwwwecdceuropaeuenhealth
topicshealth_communicationPagespublicationsaspx
39 Gachter S Herrmann B Reciprocity culture and human coop-
eration previous insights and a new cross-cultural experiment
Phil Trans R Soc B Biol Sci 2009364(1518)791ndash806
40 Rothman AJ Baldwin AS A person X intervention strategy
approach to understanding health behavior In Deaux K Snyder
M eds Handbook of Personality and Social Psychology New
York Oxford University Press 2012 P 729ndash52
41 Airhihenbuwa CO Makoni S Iwelunmor J Munodawafa D
Sociocultural infrastructure communicating identity and health
in Africa J Health Commun 201419(1)1ndash5
42 Kreuter MW Wray RJ Tailored and targeted health communi-
cation strategies for enhancing information relevance Am J Health
Behav 200327(3)227ndash32
43 Committee on Communication for Behavior Change in the 21st
Century Improving the Health of Diverse Populations Speaking of
Health Assessing Health Communication Strategies for Diverse
Populations Washington DC National Academy Press 2002
44 Institute of Medicine The Future of the Publicrsquos Health in the
21st Century Washington DC National Academies Press 2003
45 Kreuter MW Lezin NL Social capital theory implications for
community-based health promotion In DiClemente RJ Crosby
RA Kegler M eds Emerging Theories in Health Promotion Prac-
tice and Research San Francisco Jossey-Bass 2002 p 228ndash54
46 Airhihenbuwa CO Liburd L Eliminating health disparities in
the African American population the interface of culture gender
and power Health Educ Behav 200633(4)488ndash501
47 Airhihenbuwa CO Ford CA Iwelunmor J Why culture mat-
ters in health interventions lessons from HIVAIDS stigma and
NCDs Health Educ Behav 201441(1)78ndash84
48 Sasaki JY Kim HS Mojaverian T Kelley LD Park I Janusonis
S Religion priming differentially increases prosocial behavior
among variants of dopamine D4 receptor (DRD4) gene Soc Cogn
Affect Neurosci 20138209ndash15
49 Kitayama S King A Tompson S Huff S Yoon C Liberzon I
The dopamine receptor gene (DRD4) moderates cultural difference
in independent versus interdependent social orientation Psychol
Sci 201425(6)1169ndash77
50 Uskul AK Kitayama S Nisbett RE Ecocultural basis of cogni-
tion farmers and fishermen are more holistic than herders Proc
Natl Acad Sci USA 2008105(25)8552ndash6
51 Talhelm T Zhang X Oishi S et al Discovery of large-scale psy-
chological differences within China explained by rice vs wheat
agriculture Science 2014344(6184)603ndash8
52 Oishi S Talhelm T Residential mobility what psychological
research reveals Curr Direct Psychol Sci 201221(6)425ndash30
53 Kitayama S Conway LG III Pietromonaco PR Park H Ethos of
independence across regions in the united States Am Psychol
201065(6)559ndash74
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 829
54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

54 Kitayama S Park H Sevincer AT Karasawa M Uskul AK A
cultural task analysis of implicit independence comparing North
America Western Europe and East Asia J Pers Soc Psychol
200997(2)236ndash55
55 Kitayama S Snibbe AC Markus HR Suzuki T Is there any
lsquolsquofreersquorsquo choice Self and dissonance in two cultures Psychol Sci
200415(8)527ndash33
56 Na J Kitayama S Will people work hard on a task they choose
Social-eyes priming in different cultural contexts J Exp Soc Psy-
chol 201248(1)284ndash90
57 Kitayama S Uskul AK Culture mind and the brain current
evidence and future directions Annu Rev Psychol 201162(1)
419ndash49
58 Park J Kitayama S Interdependent selves show face-induced
facilitation of error processing cultural neuroscience of self-threat
Soc Cogn Affect Neurosci 20149(2)201ndash8
59 Markus HR Kitayama S Culture and the self Implications for
cognition emotion and motivation Psychol Rev 199198(2)224
60 Triandis HC Individualism amp Collectivism Boulder (CO)
Westview Press 1995
61 Gelfand MJ Raver JL Nishii L et al Differences between tight
and loose cultures a 33 nation study Science 20113321100ndash4
62 Hofstede G Culturersquos Consequences International Differences
in Work-Related Values Beverly Hills (CA) Sage 1980
63 Inglehart R Modernization and Postmodernization Cultural
Economic and Political Change in 43 Societies Princeton (NJ)
Princeton University Press 1997
64 Leung AKY Cohen D Within-and between-culture variation
individual differences and the cultural logics of honor face and
dignity cultures J Pers Soc Psychol 2011100(3)507
65 Oishi S The psychology of residential mobility implications
for the self social relationships and well-being Perspect Psychol
Sci 201055ndash21
66 Oishi S Socio-ecological psychology Annu Rev Psychol
201465581ndash609
67 Oishi S Graham J Social ecology lost and found in psycholog-
ical science Perspect Psychol Sci 20105(4)356ndash77
68 Medin D Ojalehto B Marin A Bang M Culture and epistemol-
ogies putting culture back into the ecosystem In Gelfand M Chiu
CY Hong YY eds Advances in Culture and Psychology Series
New York Oxford University Press 2013 p 177ndash217
69 Adams G The cultural grounding of personal relationship
enemyship in North American and West African worlds J Pers
Soc Psychol 200588948ndash68
70 Maynard AE Greenfield PM Implicit cognitive development
in cultural tools and children lessons from Mayan Mexico Cogni-
tive Development 200318489ndash510
71 Plaut VC Markus HR Lachman ME Place matters consensual
features and regional variation in American well-being and self J
Pers Soc Psychol 200283160ndash84
72 Hofstede G Culturersquos Consequences Comparing Values
Behaviors Institutions and Organizations across Nations 2nd ed
Thousand Oaks (CA) Sage 2001
73 Oyserman D Coon HM Kemmelmeier M Rethinking individ-
ualism and collectivism evaluation of theoretical assumptions
and meta-analyses Psychol Bull 2002128(1)3ndash72
74 Kim HS Sherman DK lsquolsquoExpress yourselfrsquorsquo culture and the effect
of self-expression on choice J Pers Soc Psychol 200792(1)1ndash11
75 Elliot AJ Chirkov VI Kim Y Sheldon KM A cross cultural
analysis of avoidance (relative to approach) personal goals Psy-
chol Sci 200112505ndash10
76 Lee AY Aaker JL Gardner WK The pleasures and pains of dis-
tinct self-construals the role of interdependence in regulatory
focus J Pers Soc Psychol 2000781122ndash34
77 Lockwood P Jordan CH Kunda Z Motivation by positive and
negative role models regulatory focus determines who will best
inspire us J Pers Soc Psychol 200283854ndash64
78 Sherman DK Uskul AK Updegraff JA The role of the self in
responses to health communications a cultural perspective Self
and Identity 201110(3)284ndash94
79 Triandis HC Singelis TM Training to recognize individual
differences in collectivism and individualism within culture
International Journal of Intercultural Relations 199822(1)35ndash47
80 Kreuter MW Lukwago SN Bucholtz RDDC Clark EM
Sanders-Thompson V Achieving cultural appropriateness in
health promotion programs targeted and tailored approaches
Health Educ Behav 200330133ndash46
81 Singelis TM The measurement of independent and interde-
pendent self construals Pers Soc Psychol Bull 199420(5)580ndash91
82 Singelis TM Triandis HC Bhawuk DPS Gelfand MJ Horizon-
tal and vertical dimensions of individualism and collectivism
a theoretical and measurement refinement Cross-Cultural
Research 199529240ndash75
83 Kitayama S Culture and basic psychological processesmdashto-
ward a system view of culture comment on Oyserman et al Psy-
chol Bull 2002128(1)89ndash96
84 Pelto PJ The differences between lsquolsquotightrsquorsquo and lsquolsquoloosersquorsquo socie-
ties Society 19685(5)37ndash40
85 Harrington J Gelfand M Tightnessndashlooseness across the 50
united states Proc Natl Acad Sci 2014 Available from URL
httpwwwpnasorgcontent111227990fullpdf+html
86 Ajzen I Attitudes Personality and Behavior Chicago Dorsey
Press 1988
87 Ajzen I The theory of planned behavior Organizational
Behavior and Human Decision Processes 199150179ndash211
88 Fishbein M Ajzen I Belief Attitude Intention and Behavior
An Introduction to Theory and Research Reading (MA) Addison-
Wesley 1975
89 Ajzen I Fishbein M Understanding Attitudes and Predicting
Social Behavior Englewood Cliffs (NJ) Prentice-Hall 1980
90 Hochbaum GM Public Participation in Medical Screening
Programs A Socio-Psychological Study Public Health Service
Publication No 572 Washington DC United States Government
Printing Office 1958
91 Rosenstock IM Why people use health services Milbank
Memorial Fund Quarterly19664494ndash127
92 Rogers RW A protection motivation theory of fear appeals and
attitude change J Psychol 19759193ndash114
93 Rogers RW Cognitive and physiological process in fear
appeals and attitude change a revised theory of protection motiva-
tion In Cacioppo JT Petty RE eds Social Psychophysiology A
Source Book New York Guilford Press 1983 p 153ndash76
BETSCH AND OTHERS
830 MEDICAL DECISION MAKINGOCTOBER 2016
94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

94 Brewer NT Chapman GB Gibbons FX Gerrard M McCaul KD
Weinstein ND Meta- analysis of the relationship between risk per-
ception and health behavior the example of vaccination Health
Psychol 200726(2)136ndash45
95 Rothman AJ Salovey P The reciprocal relation between prin-
ciples and practice social psychology and health behavior In Kru-
glanski A Higgins ET eds Social Psychology Handbook of Basic
Principles 2nd ed New York Guilford Press 2007 p 826ndash49
96 Stewart SL Rakowski W Pasick RJ Behavioral constructs and
mammography in five ethnic groups Health Educ Behav 2009
36(5)36ndash54
97 Pasick RJ Barker JC Otero-Sabogal R Burke NJ Joseph G
Guerra C Intention subjective norms and cancer screening in
the context of relational culture Health Educ Behav 200936(5)
91ndash110
98 Fishbein M Yzer MC Using theory to design effective health
behavior interventions Communication Theory 200313(2)
164ndash83 Available from URL httpswwwk4healthorgsites
default filesUsing20theory20to 20design20health20
interventionspdf
99 International Decision Aid Standards (IPDAS) Collaboration
Homepage [Internet] 2015 [modified 2013 Oct 3] Available
from URL httpipdasohricaindexhtml
100 Betsch C Bohm R Korn L Inviting free-riders or appealing to
pro-social behavior Game theoretical reflections on communicat-
ing herd immunity in vaccine advocacy Health Psychol 2013
32(9)978ndash85
101 Wong RYM Hong Y Dynamic influences of culture on coop-
eration in the prisonerrsquos dilemma Psychol Sci 200516429ndash34
102 Gachter S Herrmann B Thoni C Culture and cooperation
Phil Trans R Soc B Biol Sci 2010365(1553)2651ndash61
103 Rose N Identity genealogy history In Hall S duGay P eds
Questions of Cultural Identity London Sage 1996 p 128ndash50
104 Lock M The politics of health identity and culture In Con-
trada R Ashmore R eds Self Social Identity and Physical Health
New York Oxford 1999 p 43ndash70
105 Crawford R A cultural account of health self-control
release and the social body In McKinlay J ed Issues in the Polit-
ical Economy of Health Care London Tavistock 1984 p 60ndash103
106 Baumeister RF The self and society changes problems and
opportunities In Ashmore RD Jussim L eds Self and Identity
Fundamental Issues Rutgers Series on Self and Social Identity
Vol 1 New York Oxford 1997 p 191ndash217
107 Uskul AK Hynie M Self-construal and concerns elicited by
imagined and real health problems J Appl Soc Psychol 200737
2156ndash89
108 Uskul AK Oyserman D When message-frame fits salient
cultural-frame messages feel more persuasive Psychol Health
201025321ndash37
109 Uskul AK Hynie M The role of self-aspects in emotions
elicited by threats to physical health Psychol Health 201429
199ndash217
110 Markus HR Kitayama S The cultural construction of self and
emotion implications for social behavior In Kitayama S Markus
HR eds Emotion and Culture Empirical Studies of Mutual Influ-
ence Washington DC American Psychological Association 1994
p 89ndash130
111 Riemer H Shavitt S Koo M Markus HR Preferences donrsquot
have to be personal expanding attitude theorizing with a cross-
cultural perspective Psychol Rev 2014121(4)619ndash48
112 Oyserman D Fryberg SA Yoder N Identity-based motivation
and health J Pers Soc Psychol 2007931011ndash27
113 Dake K Myths of nature culture and the social construction
of risk J Soc Issues 19924821ndash37
114 Fischhoff B Bostrom A Quadrel MJ Risk perception and
communication In Detels R McEwen J Omenn G eds Oxford
Textbook of Public Health London Oxford University Press
1997 p 987ndash1002
115 Rohrmann B Perception of risk research results relevance
In Gough J ed Sharing the Future Risk Communication in Prac-
tice Christchurch (UK) CAE University of Canterbury 2003 p
21ndash44
116 Slovic P The Perception of Risk London Earthscan 2000
117 Rohrmann B Risk perception of different societal groups
Australian findings and cross-national comparisons Aust J Psy-
chol 199446150ndash63
118 Rohrmann B Cross-cultural studies on the perception and
evaluation of hazards In Renn O Rohrmann B eds Cross-Cul-
tural Risk Perception A Survey of Empirical Studies Dordrecht
(the Netherlands) Kluwer Academic Publishers 2000 p 103ndash44
119 Rosa EA Matsuda N Kleinhesselink RR eds The cognitive
architecture of risk Pancultural unity or cultural shaping In
Renn O Rohrmann B eds Cross-Cultural Risk Perception Dor-
drecht (the Netherlands) Springer 2000 p 185ndash210
120 Bontempo RN Bottom WP Weber EU Cross-cultural differ-
ences in risk perception a model-based approach Risk Anal
199717(4)479ndash88
121 Weber EU Hsee CK Models and mosaics investigating
cross-cultural differences in risk perception and risk preference
Psychon Bull Rev 19996(4)611ndash7
122 Wang M Fischbeck PS Evaluating lotteries risks and risk-
mitigation programs J Risk Res 200811(6)775ndash95
123 Higgins ET Promotion and prevention regulatory focus as
a motivational principle Adv Exp Soc Psychol 1998301ndash46
124 Fine P Eames K Heymann DL lsquolsquoHerd immunityrsquorsquo a rough
guide Clin Infect Dis 201152911ndash6
125 Bauch CT Earn DJ Vaccination and the theory of games Proc
Natl Acad Sci USA 2004101(36)13391ndash4
126 Chapman GB Li M Vietri J et al Using game theory to exam-
ine incentives in influenza vaccination behavior Psychol Sci
2012231008ndash15
127 Betsch C Bohm R Korn L Strategic Vaccination Experi-
mental Evidence from an Interactive Vaccination Game Submitted
2014
128 Fehr E Gachter S Cooperation and punishment in public
goods experiments Am Econ Rev 200090(4)980ndash94
129 Fehr E Schmidt KM The economics of fairness reciprocity
and altruismmdashexperimental evidence and new theories In Kolm
S-C Ythier JM eds Handbook of the Economics of Giving Altru-
ism and Reciprocity Amsterdam Elsevier 2006 p 615ndash91
130 Boyd R Richerson PJ Henrich J Rapid cultural adaptation
can facilitate the evolution of large-scale cooperation Behav Ecol
Sociobiol 201165(3)431ndash44
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 831
131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

131 Henrich J Henrich N Why Humans Cooperate A cultural
and Evolutionary Explanation Oxford Oxford University Press
2007
132 Henrich J McElreath R Barr A et al Costly punishment
across human societies Science 2006312(5781)1767ndash70
133 Balliet D Van Lange PA Trust punishment and cooperation
across 18 societies a meta-analysis Perspect Psychol Sci 2013
8(4)363ndash79
134 Inglehart R Basanez M Moreno AM Human Values and
Beliefs A Cross-Cultural Sourcebook Political Religious Sexual
and Economic Norms in 43 Societies Findings from the 1990-1993
World Value Survey Ann Arbor University of Michigan Press
1998
135 Rothman AJ Salovey P Shaping perceptions to motivate
healthy behavior the role of message framing Psychol Bull
1997213ndash19
136 Gallagher KM Updegraff JA Health message framing effects
on attitudes intentions and behavior a meta-analytic review
Ann Behav Med 201243101ndash16
137 Covey J The role of dispositional factors in moderating mes-
sage framing effects Health Psychol 201433(1)52
138 Carver CS White TL Behavioral inhibition behavioral acti-
vation and affective responses to impending reward and punish-
ment J Pers Soc Psychol 199467319ndash33
139 Elliot AJ Thrash TM Approach-avoidance motivation in per-
sonality J Pers Soc Psychol 200282804ndash18
140 Sherman DK Updegraff JA Mann T Improving oral health
behavior a social psychological approach J Am Dent Assoc
2008139(10)1382ndash7
141 Gerend MA Shepherd JE Using message framing to promote
acceptance of the human papillomavirus vaccine Health Psychol
200726745ndash52
142 Nan X Communicating to young adults about HPV vaccina-
tion consideration of message framing motivation and gender
Health Commun 20122710ndash8
143 Gerend MA Shepherd M Message framing it does a body
good effects of message framing and motivational orientation on
young womenrsquos calcium consumption J Health Psychol 2012
181296ndash306
144 Latimer AE Williams-Piehota P Katulak NA et al Promoting
fruit and vegetable intake through messages tailored to individual
differences in regulatory focus Ann Behav Med 200835363ndash9
145 Zhao G Pechmann C The impact of regulatory focus on ado-
lescentsrsquo response to antismoking advertising campaigns J Market
Res 200744671ndash87
146 Pakpour AH Yekaninejad MS Sniehotta FF Updegraff JA
Dombrowski SU The effectiveness of gain- versus loss-framed
health messages in improving oral health in Iranian secondary
schools a cluster-randomized controlled trial Ann Behav Med
201447(3)376ndash87
147 Sherman DK Brick C Binning KR Mintzer RE McCully SN
Updegraff JA Culture and Health Communication The Role of
Cultural Exposure in Health Message Framing Unpublished man-
uscript 2014
148 Cialdini RB Reno RR Kallgren CA A focus theory of norma-
tive conduct recycling the concept of norms to reduce littering in
public places J Pers Soc Psychol 1990581015ndash26
149 Cutler DM Glaeser EL Why do Europeans smoke more than
Americans In Wise D ed Developments in the Economics of
Aging Chicago University of Chicago Press 2009 p 255ndash82
150 Davidson AR Jaccard JJ Triandis HC Morales ML
Diaz-Guerrero R Cross-cultural model testing toward a solution
of thee etic-emic dilemma Int J Psychol 1976111ndash13
151 Han SP Shavitt S Persuasion and culture advertising
appeals in individualistic and collectivistic societies J Exp Soc
Psychol 199430(4)326ndash50
152 Gelfand MJ Nishii LH Raver JL On the nature and impor-
tance of cultural tightnessndash looseness J Appl Psychol 200691
1225ndash44
153 Kummervold PE Chronaki CE Lausen B et al eHealth trends
in Europe 2005ndash2007 a population-based survey J Med Internet
Res 200810(4)e42
154 Ha JF Longnecker N Doctor-patient communication
a review Ochsner J 201010(1)38ndash43
155 Russell B Power A New Social Analysis London Routledge
Classics 1938
156 Torelli CJ Shavitt S Culture and concepts of power J Pers
Soc Psychol 201099(4)703ndash23
157 Torelli C Shavitt S The impact of power on information pro-
cessing depends on cultural orientation J Exp Soc Psychol 2011
47(5)959ndash67
158 Shavitt S Torelli CJ Wong J Identity-based motivation con-
straints and opportunities in consumer research J Consum Psy-
chol 200919(3)261ndash6
159 Joseph-Williams N Edwards A Elwyn G Power imbalance
prevents shared decision making BMJ 2014348g3178
160 Torelli C Shavitt S Cho Y Johnson T Holbrook A Weiner S
Justice or compassion Cultural differences in power norms affect
consumer satisfaction with power-holders Int Market Rev In
press
161 Tokuda Y Fujii S Jimba M Inoguchi T The relationship
between trust in mass media and the healthcare system and indi-
vidual health evidence from the AsiaBarometer Survey BMC
Med 20097(1)4
162 Yamagishi T Trust The Evolutionary Game of Mind and
Society New York Springer 2011
163 Gilson L Trust and the development of health care as a social
institution Soc Sci Med 200356(7)1453ndash68
164 Adams G Plaut VC The cultural grounding of personal rela-
tionship friendship in North American and West African worlds
Personal Relationships 200310333ndash48
165 Nisbett R The Geography of Thought How Asians and West-
erners Think Differentlyand Why New York Free Press 2003
166 Haslam N Holland E Karasawa M Essentialism and entita-
tivity across cultures In Yuki M Brewer MB eds Culture and
Group Processes New York Oxford University Press 2013 p
17ndash37
167 Epley NWaytz A Cacioppo JT On seeing human a three-factor
theory of anthropomorphism Psychol Rev 2007114864ndash86
168 Betsch C Brewer NT Brocard P et al Opportunities and
challenges of Web 20 for vaccination decisions Vaccine 2012
303727ndash33
169 Igarashi T Kashima Y Kashima ES et al Culture trust and
social networks Asian J Soc Psychol 20081188ndash101
BETSCH AND OTHERS
832 MEDICAL DECISION MAKINGOCTOBER 2016
170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833

170 Rothman AJ Capitalizing on opportunities to nurture and
refine health behavior theories Health Educ Behav 200926
150ndash5
171 Rothman AJ Is there nothing more practical than a good the-
ory Why innovations and advances in health behavior change will
arise if interventions are more theory-friendly Int J Behav Nutr
Phys Activity 2004111
172 Boiger M Gungor D Karasawa M Mesquita B Defending
honour keeping face interpersonal affordances of anger and
shame in Turkey and Japan Cogn Emot 201428(7)1255ndash69
173 Gungor D Mesquita B Boiger M Dincxer D Karasawa M Fit-
ting in or sticking together the prevalence and adaptivity of confor-
mity relatedness and autonomy in Japan and Turkey [published
online 28 August 2014] Journal of Cross-Cultural Psychology
174 Thaler RH Sunstein CR Nudge Improving Decisions about
Health Wealth and Happiness New Haven (CT) Yale University
Press 2008
175 Johnson EJ Goldstein D Do defaults save lives Science
20033021338ndash39
176 Cross SE Hardin EE Gercek-Swing B The what how why
and where of self-construal Pers Soc Psychol Rev 201115
142ndash79
177 Paulhus DL Measurement and control of response bias In
Robinson JP Shaver PR Wrightsman LS eds Measures of Person-
ality and Social Psychological Attitudes San Diego (CA) Aca-
demic Press 1991 p 17ndash59
178 Sackeim HA Gur RC Self-deception other-deception and
self-reported psychopathology J Consult Clin Psychol 197947
213ndash5
179 Lalwani AK Shavitt S Johnson T What is the relation
between cultural orientation and socially desirable responding J
Pers Soc Psychol 200690165ndash78
180 Lalwani AK Shavitt S The lsquolsquomersquorsquo I claim to be cultural self-
construal elicits self-presentational goal pursuit J Pers Soc Psy-
chol 200997(1)88ndash102
181 Stokes DE Pasteurrsquos Quadrant Basic Science and Technolog-
ical Innovation Washington DC Brookings Institution Press 1997
182 Rothman AJ Klein WMP Cameron LD Advancing innova-
tions in socialpersonality psychology and health opportunities
and challenges Health Psychol 201332602ndash8
183 Klein WMP Shepperd JA Suls J Rothman AJ Croyle RT
Realizing the promise of social psychology in improving public
health [published online 30 June 2014] Pers Soc Psychol Rev
184 Kaliner E Moran-Gilad J Grotto I et al Silent reintroduction
of wild-type poliovirus to Israel 2013mdashrisk communication chal-
lenges in an argumentative atmosphere Euro Surveill 201419(7)
20703
185 Word Health Organization Tailoring immunization pro-
grammes to reach underserved groupsmdashthe TIP approach Avail-
able from URL httpwwweurowhointenhealth-topicsdise
ase-preventionvaccines-and-immunizationactivitiestailoring-
immunization-programmes-to-reach-underserved-groups-the-tip-
approach
186 Airhihenbuwa CO Healing Our Differences The Crisis of
Global Health and the Politics of Identity New York Rowman
and Littlefield 2007
187 The Hofstede Centre Israel Available from URL httpgeer-
t-hofstedecomisraelhtml
188 Wimmer FM Interkulturelle Philosophie eine Einfuhrung
[Intercultural Philosophy An Introduction] Wien Austria
WUV 2004
189 Chen HI The concept of the lsquolsquopolyloguersquorsquo and the question of
lsquolsquointerculturalrsquorsquo identity Intercultural Communication Studies
201019(3)54ndash64
CULTURE-SENSITIVE HEALTH COMMUNICATION
REVIEW 833