Kardiopulmonaler Fluch oder Segen? - Dialyseshunt · Kardiopulmonaler Fluch oder Segen? ... •...
18
1 Kardiopulmonaler Fluch oder Segen? Die arteriovenöse Verbindung als Gefäßzugang zur Hämodialyse
-
Upload
hoangkhanh -
Category
Documents
-
view
213 -
download
0
Transcript of Kardiopulmonaler Fluch oder Segen? - Dialyseshunt · Kardiopulmonaler Fluch oder Segen? ... •...
1
Kardiopulmonaler Fluch oder Segen?
Die arteriovenöse Verbindung als Gefäßzugang zur Hämodialyse


• Haupttodesursache der Hämodialysepatienten ist ein kardiovaskuläres Ereignis: 50% Collins et al.: Am J med Sci; 3256: 163-167)
• Herzinsuff. bei 30-60% aller Patienten mit GFR < 60 ml/min.
• Bei 29% aller hospitalisierten u. nicht hospitalisierten Patienten mit CHF lag das Kreatinin > 1.5 mg/dl, die GFR < 53 ml/min.(Smith et al.: J Am Coll Cardiol 2006; 47: 1987-1996)
• 30% aller Patienten, die wegen Herzinsuff. stationär behandelt werden, sind chronisch niereninsuffizient (Kreatinin > 2 mg/dl)(Acute Decompensated Heart Failure National Registry database) (Am Heart J 2005; 149:209-216)
• Inzidenz chron. Herzinsuff. liegt bei neuen Dialysepatienten bei ca. 33%, 71/1000 Patientenjahre(Stack et al.:Am J Kid Dis 2001; 38: 992-1000)
• Inzidenz akutes Koronarsyndrom legt bei 29/1000 bei ESRD laut US Renal Data System and Morbidity Study WAVE 2 (Trespalacios et al.: Am J Kidney Dis 2003; 41: 1267-1277)
4

Copyright © 2014 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc. 2
Is left ventricular hypertrophy a modifiable risk factor in end-stage renal disease. Charytan, David Current Opinion in Nephrology & Hypertension. 23(6):578-585, November 2014. DOI: 10.1097/MNH.0000000000000067
FIGURE 1 . Contributors to adverse remodeling of the left ventricle in end-stage renal disease. Factors contributing to capillary dropout and left ventricular hypertrophy in end-stage renal disease. FGF-23, fibroblast growth factor 23; HTN, hypertension; LVH, left ventricular hypertrophy; mTOR, mammalian target of rapamycin.

6
Hämodynamische Veränderungen nach Shuntanlage
Abfall des systemischen Widerstandes
Anstieg Schlagvolumens, HMV, CI, EF
Anstieg des LVEDD und LVEDV,
RV, RVEDD
Anstieg pulmonalart. Druck
vermindert TAPSE(tricuspid annular plane excursions)
Anstieg linksatrialer Durchmesser; LVEDD
Zunahme des Durchmessers der zuführenden Arterie
Erhöhte SEVR(subendocardial viability ratio)
Anstieg myokardialer Sauerstoffverbrauch
Kein linearer Anstieg des HMV im Verhältnis zum Shuntfluß
Exzentrische Herzhypertrophie

7
Echocardiography Criteria of heart disease∗
LV = left ventricle; LVH = left ventricular hypertrophy; RV = right ventricle; TAPSE = tricuspid annular plane systolic excursion.
∗At least 1 (of 8) listed criteria must be abnormal to fulfill the definition of echocardiographic evidence of heart disease.
Chawla et al.: J of the American College of Cardiologie Vol. 63, 13,
April 2014, Pages 1246–1252
• LVH (LV mass index >110 g/m2 for women and >130 g/m2 for men or >47
g/m2.7 for women and >50 g/m2.7 for men). Latter measure is LV mass
calculated by the area-length method and indexed to height
• Increased LV volume index >86 ml/m2 diastolic or >37 ml/m2 systolic.
• Left atrial enlargement (left atrial volume index ≥34 ml/m2).
• Diastolic dysfunction (ASE grade ≥2).
• Moderate to severe mitral or aortic valvular disease (stenosis or
regurgitation).
• RV systolic dysfunction by accepted criteria (e.g., TAPSE <17 mm).
• LV ejection fraction ≤45%
• Regional wall motion abnormality of LV (>10% of the myocardium).

8
Mostovaya IM, Bots ML, van den Dorpel MA, Goldschmeding R, den Hoedt CH, et al. (2014) Left Ventricular Mass in Dialysis
Patients, Determinants and Relation with Outcome. Results from the COnvective TRansport STudy (CONTRAST). PLoS ONE 9(2):
e84587. doi:10.1371/journal.pone.0084587

9
Classification is determined by a dyspnea
assessment before and after renal
replacement therapy (RRT)/ultrafiltration
(UF). When patients have the same class
assessment before and after RRT/UF, they
are scored by their post-treatment assess-
ment. The classification scheme assumes
that the class assignment represents the
patient's achievement of optimized UF and is
representative of the patient's usual level of
dyspnea before and after RRT/UF. *If
dyspnea symptoms improve to class I levels,
the patient would be classified as class 2R.
‡If dyspnea symptoms improve to class II
levels, the patient would be classified as class
3R.
ADQI = Acute Dialysis Quality Initiative;
ESRD = end-stage renal disease;
NYHA = New York Heart Association.
Chawla et al.: J of the American College of
Cardiologie Vol. 63, 13, April 2014, Pages
1246–1252
ADQI Heart Failure in ESRD Classification System

10
Chawla et al.: J of the American College of
Cardiologie Vol. 63, 13, April 2014, Pages
1246–1252
Changes in Right Heart Pressures Over 8 Days in Patients Undergoing Hemo-dialysis Eight-day continuous hemo-dynamic trend from a patient who underwent thrice-weekly hemodialysis (HD). A marked reduction in right ventricular systolic pressure (RVSP) and right ventricular diastolic pressure (RVDP), as well as estimated pulmonary artery diastolic (ePAD) pressure, was seen during each dialysis session, followed by progressive pressure increments until the next dialysis session. The most marked increase in cardiac pressures was seen the day after a weekend (i.e., an extra day without dialysis). The solid line shows the median value, and the shaded areas are the range (6th and 94th percentiles). HD procedures are indi-cated at the top of the graph. bpm = beats/min. (Permission pending.)

11
Symptome der kardialen Dekompensation
Dyspnoe (Ruhe o. geringe Belastung)
periphere u. zentrale Ödeme
erhöhtes Herzminutenvolumen (> 8 l/min) o. CI > 3.9 l/min
Neu aufgetretene Tachykardie
warme Peripherie
systol. Geräusch Mitral- u.o Trikuspidalklappe.
High Output Cardiac Failure
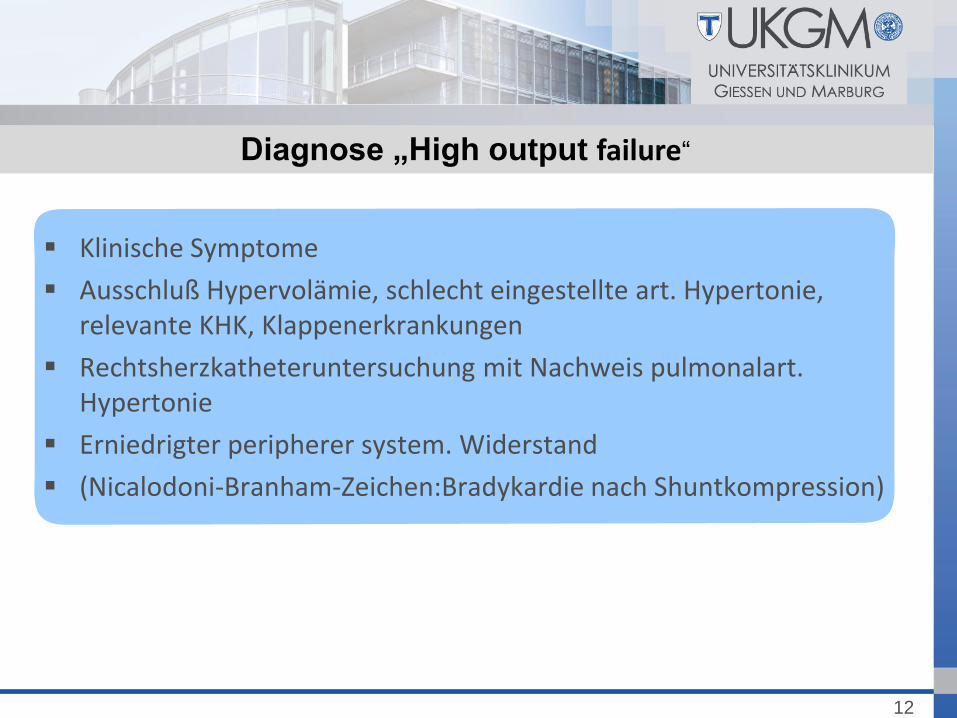
Klinische Symptome
Ausschluß Hypervolämie, schlecht eingestellte art. Hypertonie, relevante KHK, Klappenerkrankungen
Rechtsherzkatheteruntersuchung mit Nachweis pulmonalart. Hypertonie
Erniedrigter peripherer system. Widerstand
(Nicalodoni-Branham-Zeichen:Bradykardie nach Shuntkompression)
12
Diagnose „High output failure“

13
Pulmonale Hypertonie bei ESRD
mPAP > 25 mm Hg in Ruhe, erhöhter PVR
Normale linksventrikuläre Drücke
Prävalenz PH bei ESRD mit AVF 27-58%
Schwere pulmonale Hypertonie bei ca. 7-29%
Höheres HMV
Meistens asymptomatisch
NO- Metabolit-Spiegel bei ESRD-Patienten mit PH niedriger als bei nicht PH ESRD
Patienten
Bd. Gruppen haben erhöhte Endothelin 1 u. ADMA-Spiegel
Blutfluß signifikant höher bei den PH Patienten
Zeit des Vorhandenseins einer AV-Verbindung
und PH-Entwicklung korrelieren
Nach NTX Normalisierung bzw. Besserung der PH
Mortalität der PH-Patienten ist dreifach gegenüber den nicht-PH-Patienten erhöht
Sise M; Kidney international 2013 84, 682-692

WHO group Examples Epidemiological overlap with
kidney disease
1. PAH IPAH, heritable IPAH, connective tissue
disease, portal hypertension, HIV
infection, and drug and toxin–induced
PAH
Recurrent episodes of AKI in IPAH
patients. Overlap syndromes: HIV,
scleroderma, nephrogenic sclerosing
dermatopathy, and end-stage liver
disease
2. Pulmonary hypertension owing to left
heart disease
Systolic dysfunction, diastolic
dysfunction, or valvular heart disease
High prevalence of systolic and diastolic
heart failure in CKD and ESRD patients
3. Pulmonary hypertension owing to
disorders of the lung/respiratory system
COPD, interstitial lung disease, sleep
apnea, and obesity hypoventilation
High prevalence of sleep apnea and
COPD in CKD and ESRD patients
4. Chronic thromboembolic pulmonary
hypertension
Proximal or distal thomboembolic
occlusion of the proximal or distal
pulmonary vasculature
Increased incidence of VTE in ESRD
patients Pulmonary embolism following
AV-access thrombectomy
5. Pulmonary hypertension with unclear
or multifactorial mechanisms
Myeloproliferative disorders,
sarcoidosis, glycogen-storage disease,
chronic kidney disease, and
miscellaneous disorders
Unexplained PH in CKD/ESRD
14
WHO Diagnostic Groups of pulmonary hypertension
Abbreviations: AKI, acute kidney injury; AV, arteriovenous; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; ESRD, end-stage
renal disease; IPAH, idiopathic pulmonary arterial hypertension; PH, pulmonary hypertension; VTE, venous thromboemoblic disease; WHO, World Health
Organization.
Sise M; Kidney international 2013 84, 682-692

Assoziation zwischen Gefäßzugang und Morbiditäts/Mortalitätsrisiko
Mortalität (risk ratio=1.53, 95% CI=1.41-1.67) schwere Infektionen (2.12, 1.79-2.52)
kardiovaskuläre Ereignisse (1.38, 1.24-1.54)
Vorhofkatheter versus Graft:
AV-Fistel versus Graft:
Mortalität (risk ratio 1.38, 1.25-1.52) schwere Infektionen (1.49, 1.15-1.93)
kardiovaskuläre Ereignisse (1.26, 1.11-1.43)
Mortalität (1.18, 1.09-1.27) schwere Infektionen (1.36, 1.17-1.58) kein erhöhtes Risiko für kardiovaskuläre Ereignisse (1.07, 0.95-1.21)
Ravani et al.: JASN 2013 Feb;24(3):465-73
Vorhofkatheter versus AV-Fisteln:

16
Friesen T., Clin Exp Nephrol (2015)
19:514–520
Cardiac dimensions by trans-thoracic echocardiography (TTE, A) and cardiac magnetic resonance imaging (CMR, B) at baseline and after 1 year of nocturnal home hemodialysis (NHD). IVS inter-ventricular septum, PWT posterior wall thickness, LVMI left ventricular mass index, RVMI right ventricular mass index, LAVI left atrial volume index, RAVI right atrial volume index

17
Baseline 2 Weeks 3 Months Overall
significance
CF-PWV
(m/s) 12.6 ± 3.5 11 ± 3 11 ± 2.8 0.02
AIx% 22 ± 9 19 ± 9 20 ± 10 0.04
CO (L/min) 6.5 ± 1.5 7.6 ± 2 7.3 ± 1.3 0.01
TPR
(mmHg·s/mL) 1.0 ± 0.2 0.8 ± 0.2 0.8 ± 0.15 0.01
SV (mL) 113 ± 33 124 ± 41 126 ± 37 0.18
HR (b.p.m.) 60 ± 11 64 ± 10 62 ± 10 0.05
Central SBP
(mmHg) 133 ± 26 121 ± 19 120 ± 21 0.01
Central DBP
(mmHg) 73 ± 13 67 ± 11 64 ± 11 0.001
EF% 45 ± 13 52 ± 12 53 ± 11 0.001
Effect of AVF creation on arterial stiffness, systemic
haemodynamics, BPs and EF in 21 patients with successful AVF
formation who completed all three study sessions using repeated
measures one-way ANOVA designa
Korsheed S., Nephrol. Dial. Transplant. (2011) 26 (10): 3296-3302
Dres. med. Brescia, Cimino, Appel; Bronx Veterans Administration Hospital; New York 1965