Kinderapheresen; extrakorporale Therapiekonzepte im ... · – 1 Priapismus – 3 prophylaktisch...
55
Kinderapheresen; extrakorporale Therapiekonzepte im Kindesalter Volker Witt St. Anna Kinderspital ÖGBT 2013 06.06.2013 1
Transcript of Kinderapheresen; extrakorporale Therapiekonzepte im ... · – 1 Priapismus – 3 prophylaktisch...
Kinderapheresen; extrakorporale
Therapiekonzepte im KindesalterTherapiekonzepte im Kindesalter
Volker Witt
St. Anna Kinderspital
ÖGBT 201306.06.2013 1
Therapiekonzepte
Was?
• Sammeln
• Reduzieren
• Ersetzen
Womit?
• Leukapherese
• Erythrozytapherese
• Plasmaaustausch• Ersetzen
• Austauschen
• Verbessern
• Behandeln
• Notfall
• Regelmäßig
• Plasmaaustausch
• Plasmaseparation plus Säule
• Manueller Austausch
• Aderlass
06.06.2013 ÖGBT 2013 2
Nicht zu vergessen:
• Venöser Zugang
• Eltern
HPC
06.06.2013 ÖGBT 2013 3
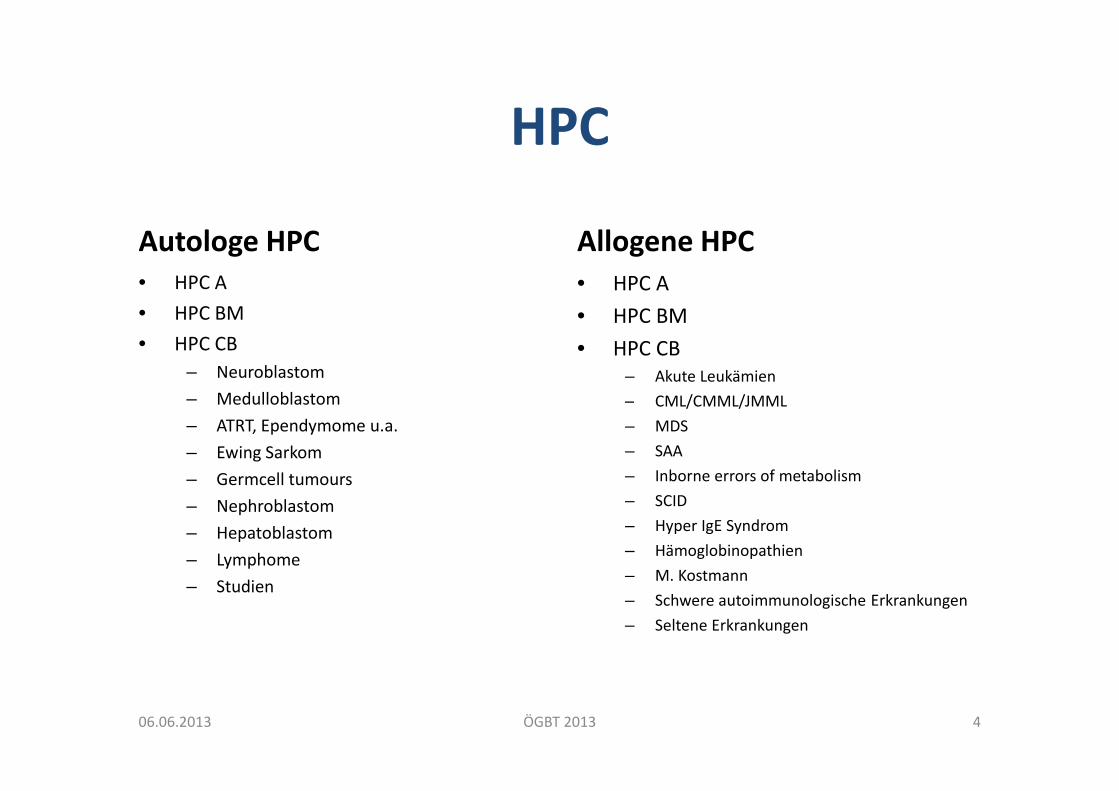
HPC
Autologe HPC
• HPC A
• HPC BM
• HPC CB
– Neuroblastom
– Medulloblastom
Allogene HPC
• HPC A
• HPC BM
• HPC CB– Akute Leukämien
– CML/CMML/JMML– Medulloblastom
– ATRT, Ependymome u.a.
– Ewing Sarkom
– Germcell tumours
– Nephroblastom
– Hepatoblastom
– Lymphome
– Studien
– CML/CMML/JMML
– MDS
– SAA
– Inborne errors of metabolism
– SCID
– Hyper IgE Syndrom
– Hämoglobinopathien
– M. Kostmann
– Schwere autoimmunologische Erkrankungen
– Seltene Erkrankungen
06.06.2013 ÖGBT 2013 4
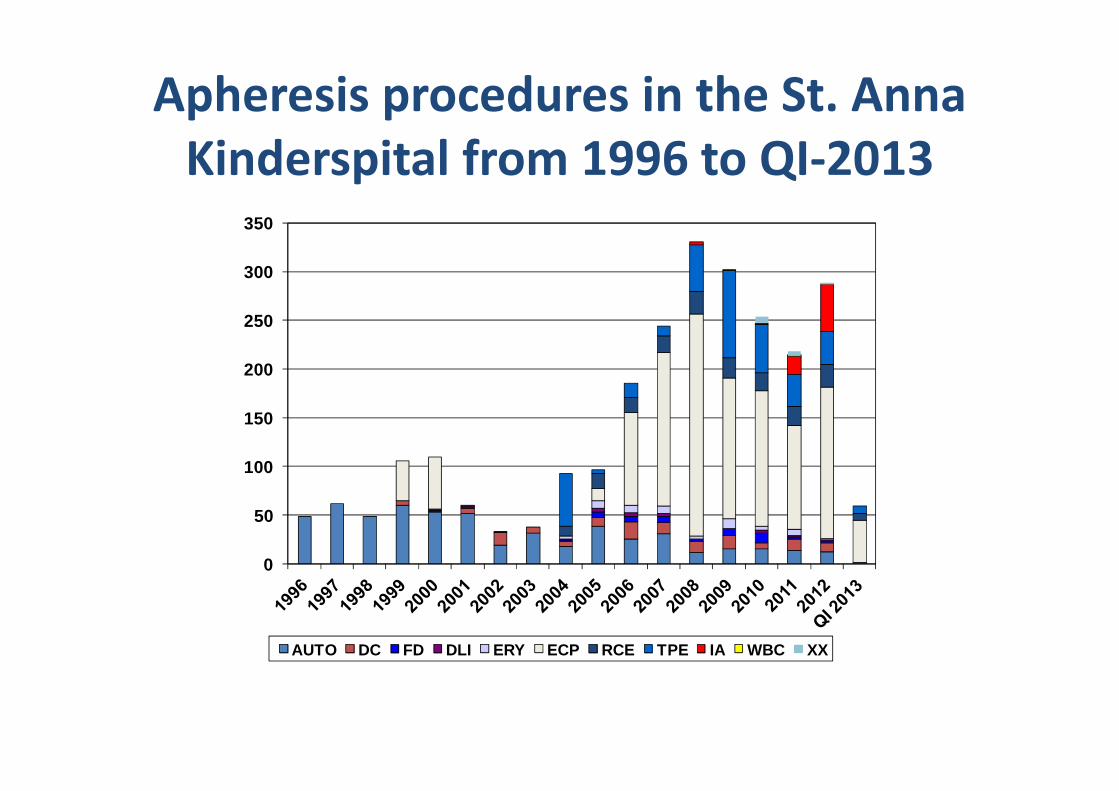
Apheresis procedures in the St. Anna
Kinderspital from 1996 to QI-2013
200
250
300
350
0
50
100
150
AUTO DC FD DLI ERY ECP RCE TPE IA WBC XX
Autologe HPC
06.06.2013 ÖGBT 2013 6
Allogene HPC
06.06.2013 ÖGBT 2013 7

Cell therapy
06.06.2013 ÖGBT 2013 8
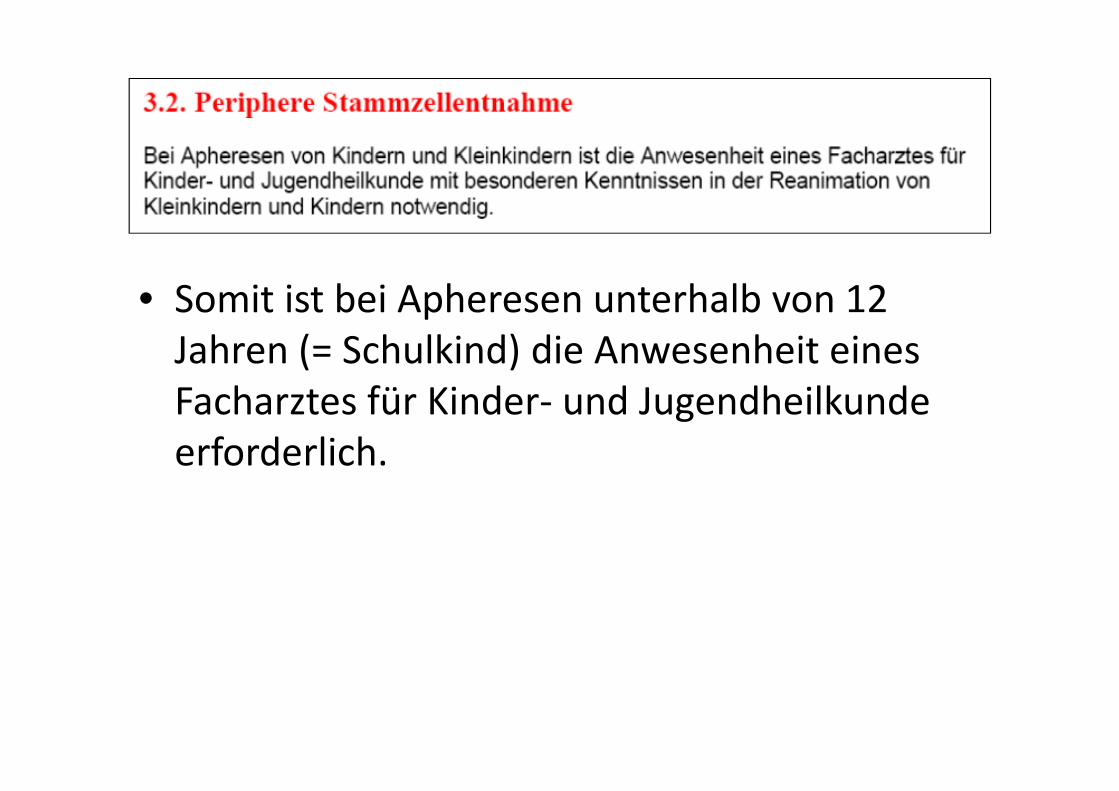
• Somit ist bei Apheresen unterhalb von 12 Jahren (= Schulkind) die Anwesenheit eines Facharztes für Kinder- und Jugendheilkunde Facharztes für Kinder- und Jugendheilkunde erforderlich.
Wie geht man vor bei minderjährigen
Patienten / Spendern um?• Grundsätzlich nur etablierte Indikationen für eine
Stammzelltransplantation sind akzeptabel. • Nur Geschwistertransplantationen• Keine experimentellen Therapien bei Geschwistern als
Spender• Bei Spender älter als 14 Jahre muss dieser neben einem • Bei Spender älter als 14 Jahre muss dieser neben einem
Obsorgeberechtigten selber der geplanten Maßnahme zustimmen.
• Die Einwilligungserklärung muss in einer adäquatenSpracheverfasst sein.
• Vermeidung der Gabe von Medikamenten für den Spender, KM eher als PBSC
• Einschaltung des Pflegschaftgerichtes

Probleme bei minderjährigen
Spendern
• Gefährdung eines gesunden Mitgliedes der Familie (Verlustangst, Schuldgefühle)
• Psychischer Druck „ich bin gesund, ich muss gesund sein“sein“
• Insuffizienzgefühl, wenn eine Kontraindikation erhoben wird
• Schuldgefühle bei Misslingen der Transplantation bzw. Tod des Geschwisterkindes
1 adulto su 1000 è un bambino guarito da tumore
PBMNC / ECP
06.06.2013 ÖGBT 2013 14
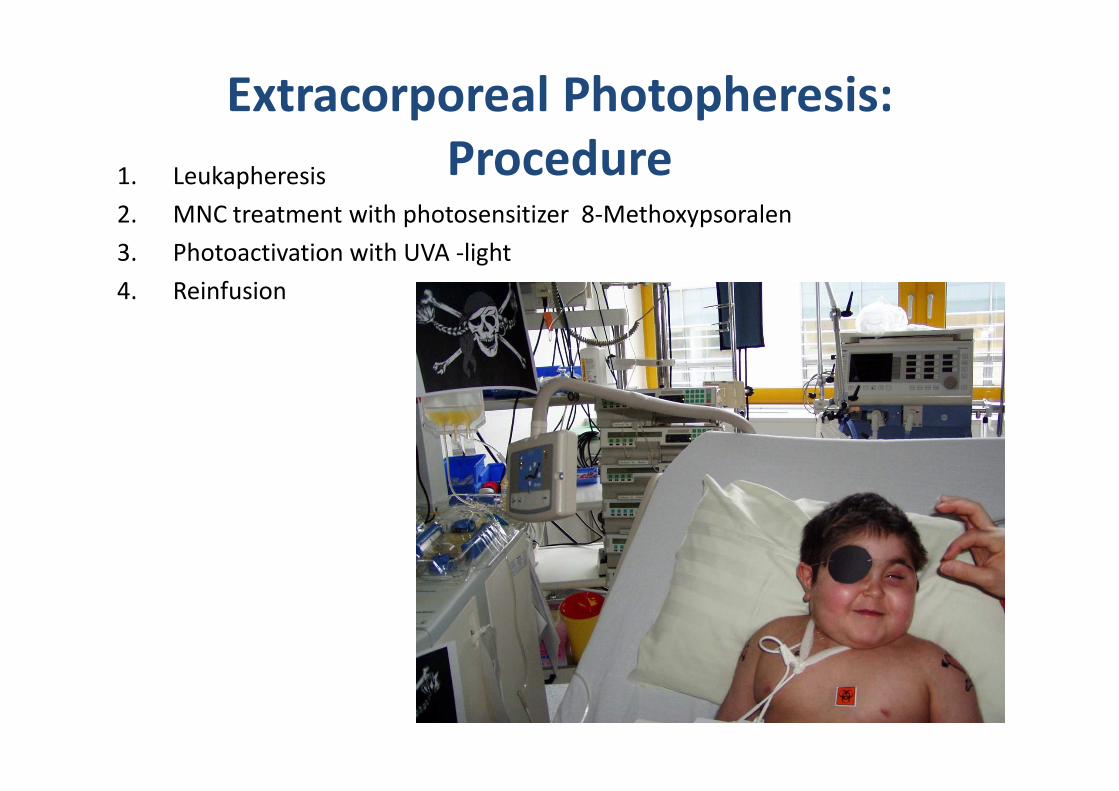
Extracorporeal Photopheresis:
Procedure1. Leukapheresis
2. MNC treatment with photosensitizer 8-Methoxypsoralen
3. Photoactivation with UVA -light
4. Reinfusion
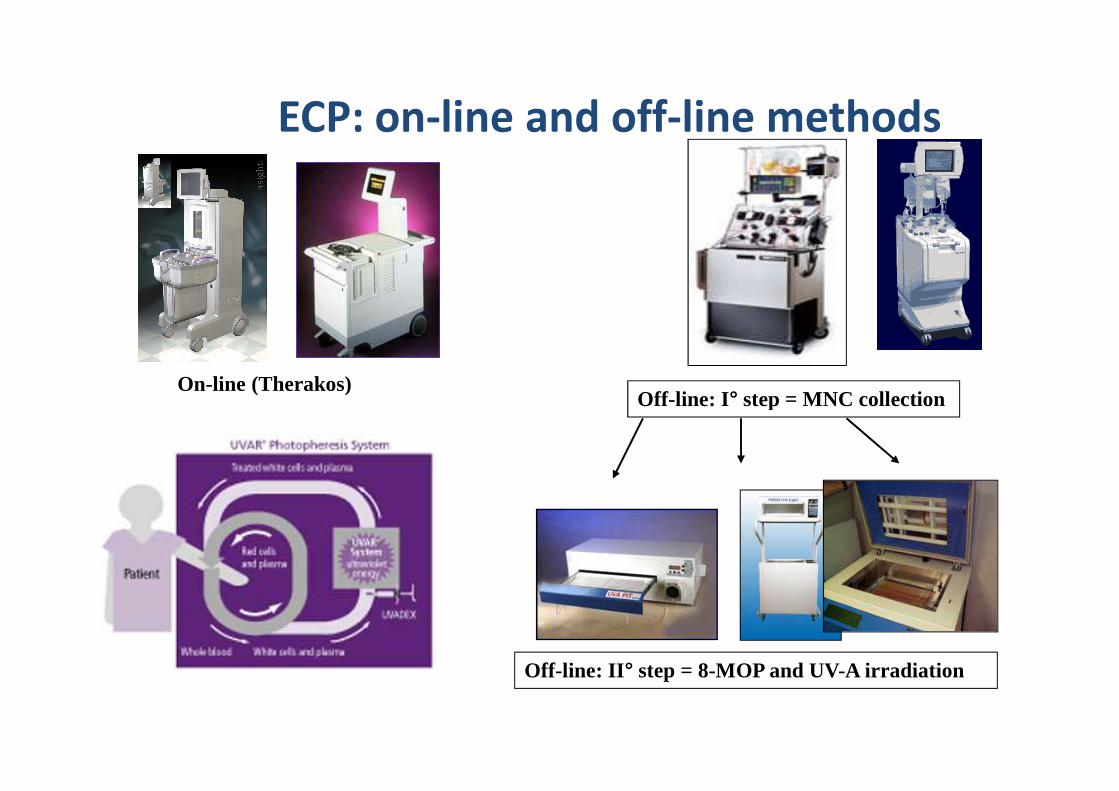
ECP: on-line and off-line methods
On-line (Therakos)Off-line: I° step = MNC collectionOff-line: I° step = MNC collection
Off-line: II° step = 8-MOP and UV-A irradiation
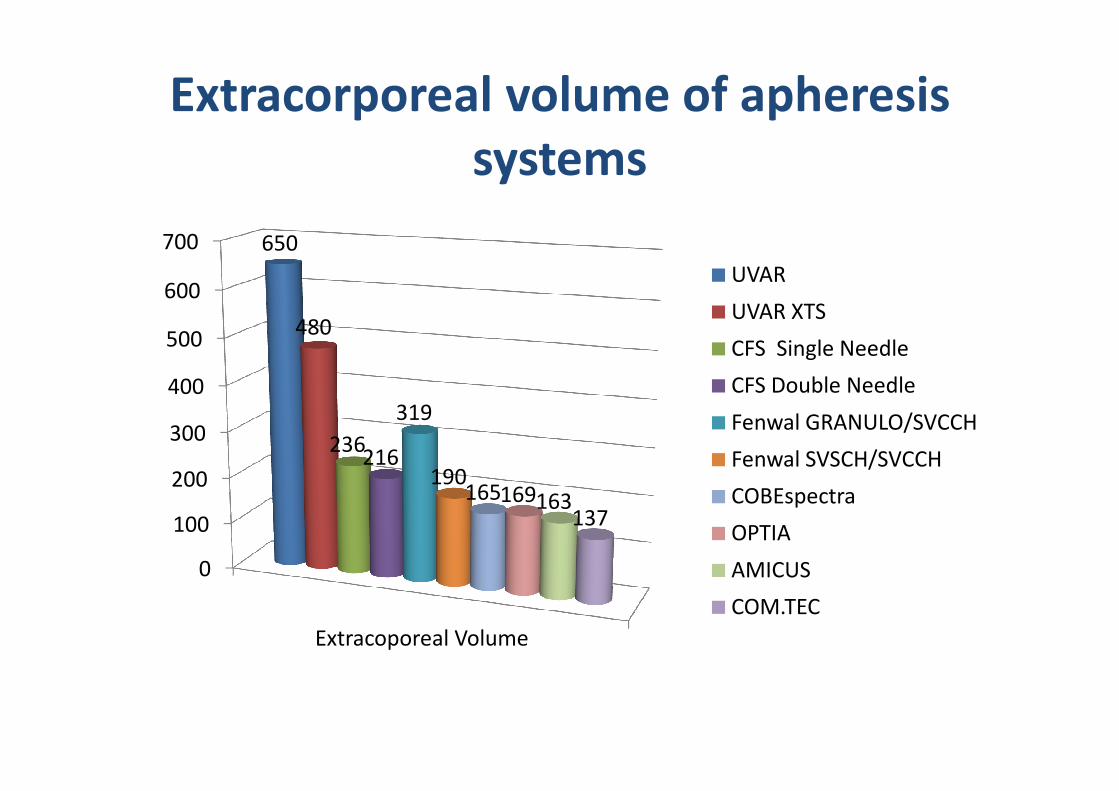
Extracorporeal volume of apheresis
systems
400
500
600
700 650
480
UVAR
UVAR XTS
CFS Single Needle
CFS Double Needle
0
100
200
300
400
Extracoporeal Volume
236216
319
190165169163
137
CFS Double Needle
Fenwal GRANULO/SVCCH
Fenwal SVSCH/SVCCH
COBEspectra
OPTIA
AMICUS
COM.TEC
ECP program from 2005 until 2011
• Patients non responsive to SIT– aGVHD
– cGVHD
• System
CP 2012
• System– > 40 kg UVAR XTS
• (1x Apherese, 2x Reinfusion)
– < 40 kg AMICUS, Fenwal CS plus COMBI light plus and later on MACOGENIC
– in special cases „MINI“ ECP
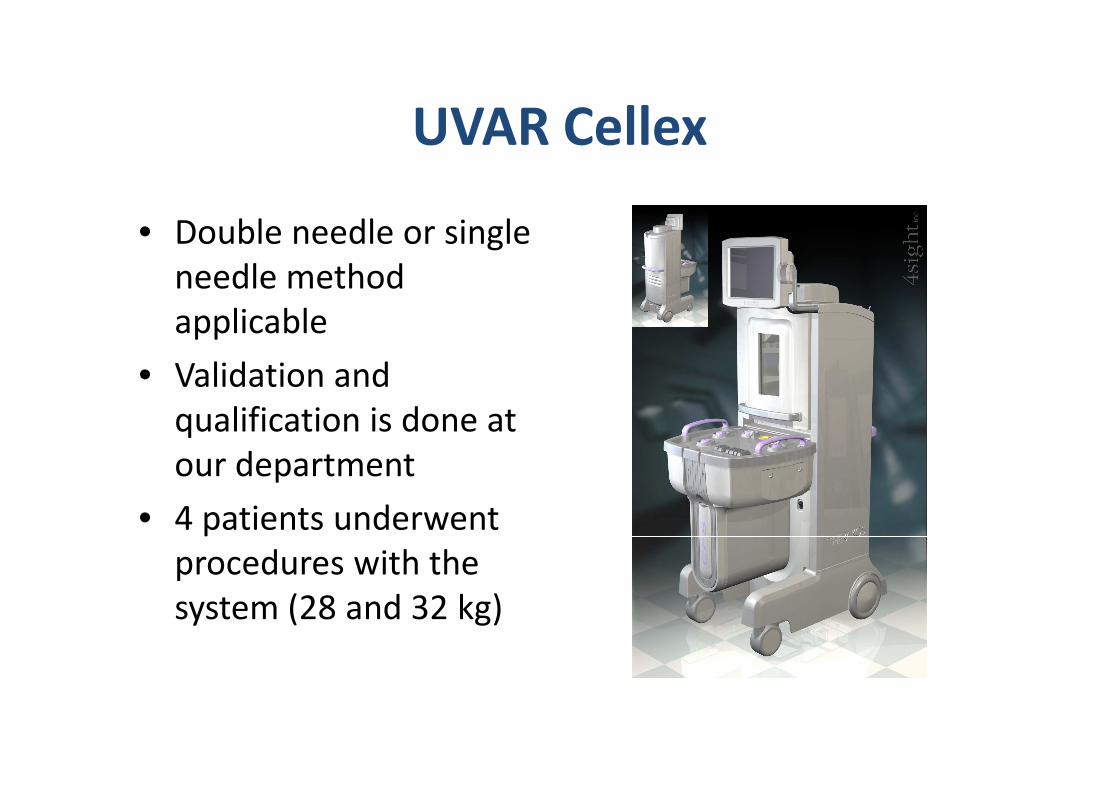
UVAR Cellex
• Double needle or singleneedle methodapplicable
• Validation andValidation andqualification is done atour department
• 4 patients underwentprocedures with thesystem (28 and 32 kg)
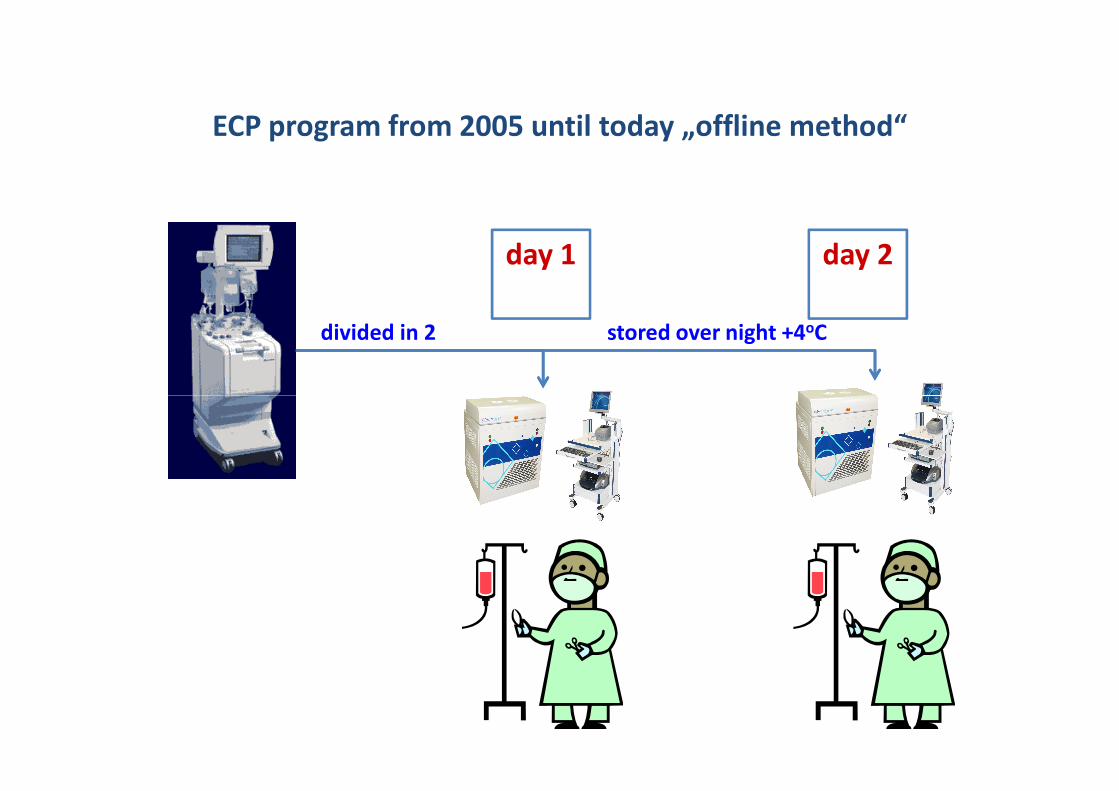
ECP program from 2005 until today „offline method“
day 1 day 2
divided in 2 stored over night +4oC
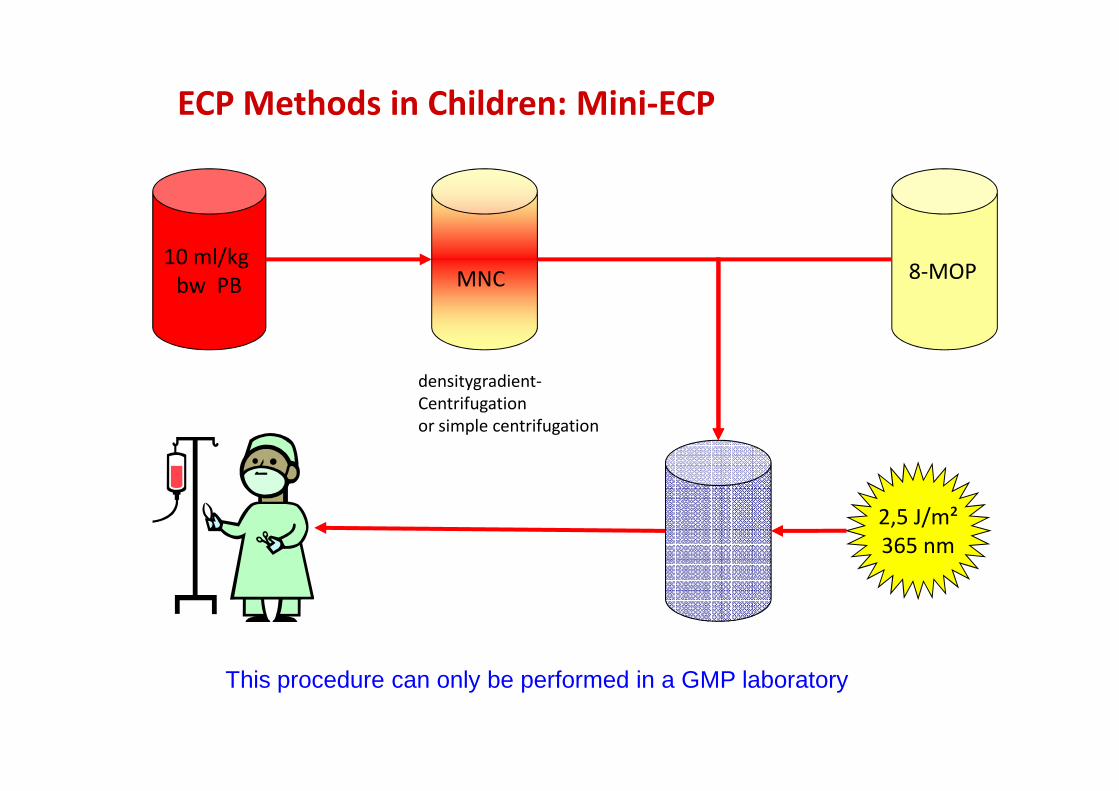
10 ml/kg bw PB
densitygradient-Centrifugation
8-MOPMNC
ECP Methods in Children: Mini-ECP
Centrifugationor simple centrifugation
2,5 J/m²365 nm
This procedure can only be performed in a GMP laboratory
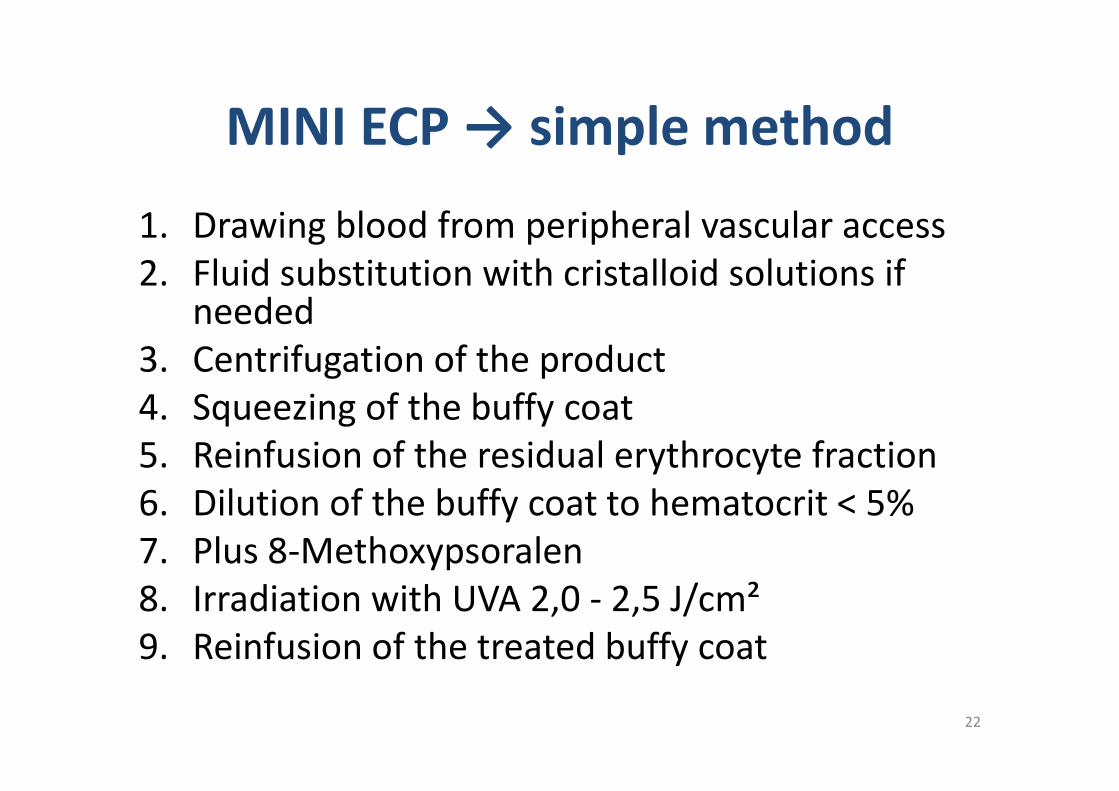
MINI ECP → simple method
1. Drawing blood from peripheral vascular access2. Fluid substitution with cristalloid solutions if
needed3. Centrifugation of the product4. Squeezing of the buffy coat4. Squeezing of the buffy coat5. Reinfusion of the residual erythrocyte fraction6. Dilution of the buffy coat to hematocrit < 5%7. Plus 8-Methoxypsoralen8. Irradiation with UVA 2,0 - 2,5 J/cm²9. Reinfusion of the treated buffy coat
22

Time needed
3. + 4. + 6. +7. 8.
23
2.1. 5. 9.
180 min
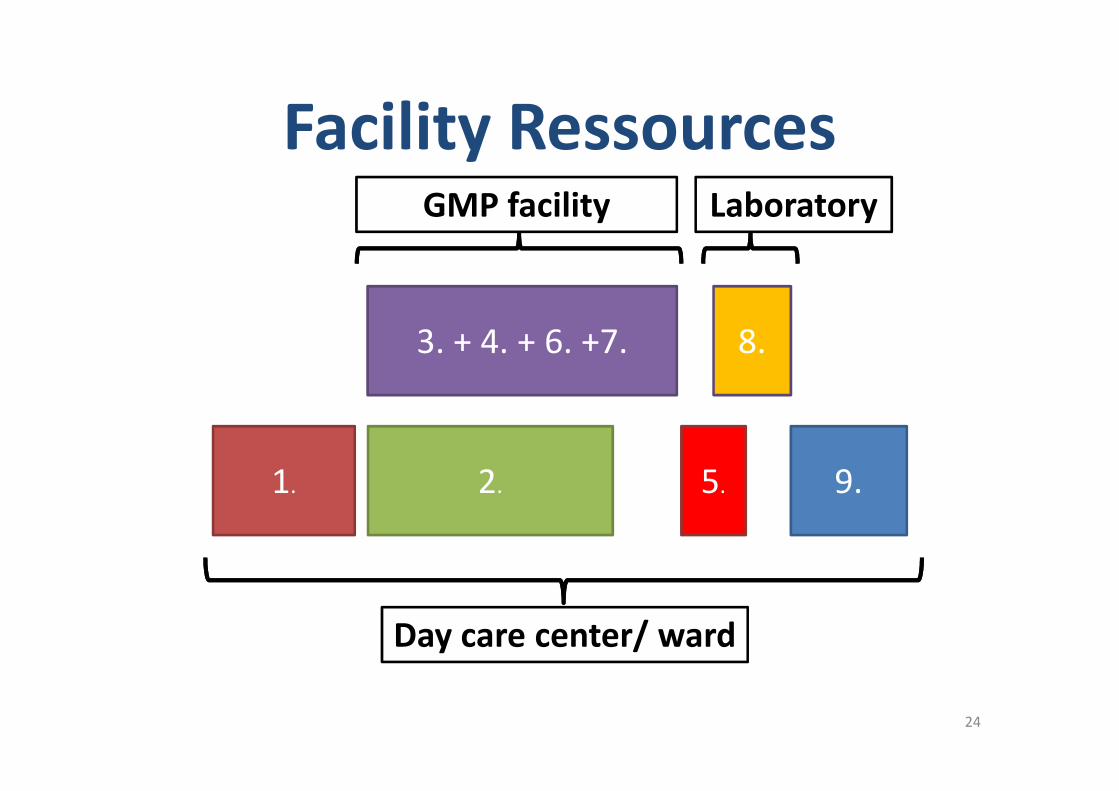
Facility Ressources
3. + 4. + 6. +7. 8.
GMP facility Laboratory
24
2.1. 5. 9.
Day care center/ ward

MINI ECP in practise
25
Blood drawing by arterial punction
26
200 ml peripheral blood
27

Reinfusion by peripheral venous access
28
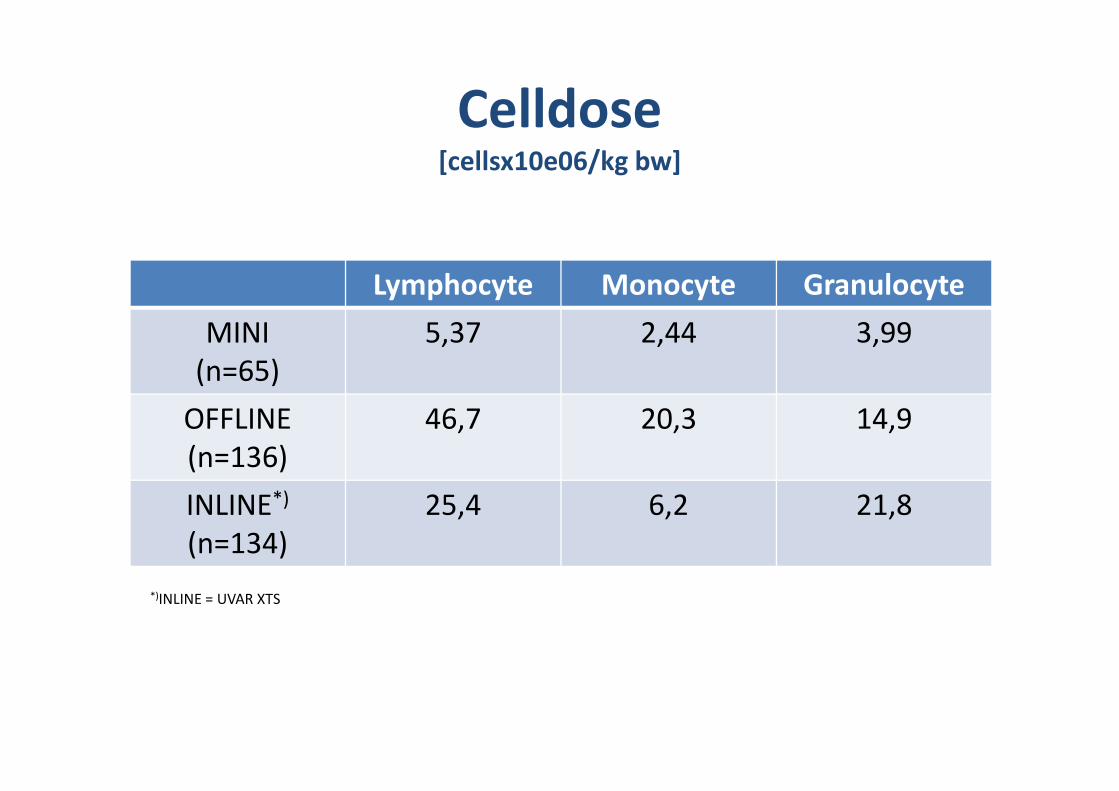
Celldose[cellsx10e06/kg bw]
Lymphocyte Monocyte Granulocyte
MINI (n=65)
5,37 2,44 3,99
OFFLINE (n=136)
46,7 20,3 14,9
INLINE*)
(n=134)25,4 6,2 21,8
*)INLINE = UVAR XTS

Adverse Events
offline inline
Analysable ECPs 270 438
ECPs with adverse events 20/270; 7,41% 34/438; 7,76%
Patients with adverse events 7/25; 28% 7/19; 36,84%
Side effects and adverse eventsoffline inline
adverse events Pat. adverse events Pat.adverse events Pat. adverse events Pat.
circulatory problems 1/20 1/7 31/34 6/7
nausea, vomiting 6/20 4/7 4/34 2/7
hypocalcemia, cramps 2/20 2/7 0 0
abdominal pain 11/20 4/7 0 0
itching, wheals 2/20 1/7 0 0
cuffing 1/20 1/7 0 0
metallic taste 0 0 1/34 1/7
gastric bleeding 0 0 1/34 1/7
Venous access
• An experienced team in pediatric apheresisshould decide on the vascular access to beused
• The decision about the apheresis system used• The decision about the apheresis system usedis crucial for the venous or vascular accessused.
• „to use what the patient has“ politics[Fischmeister et.al. BMT 2000]
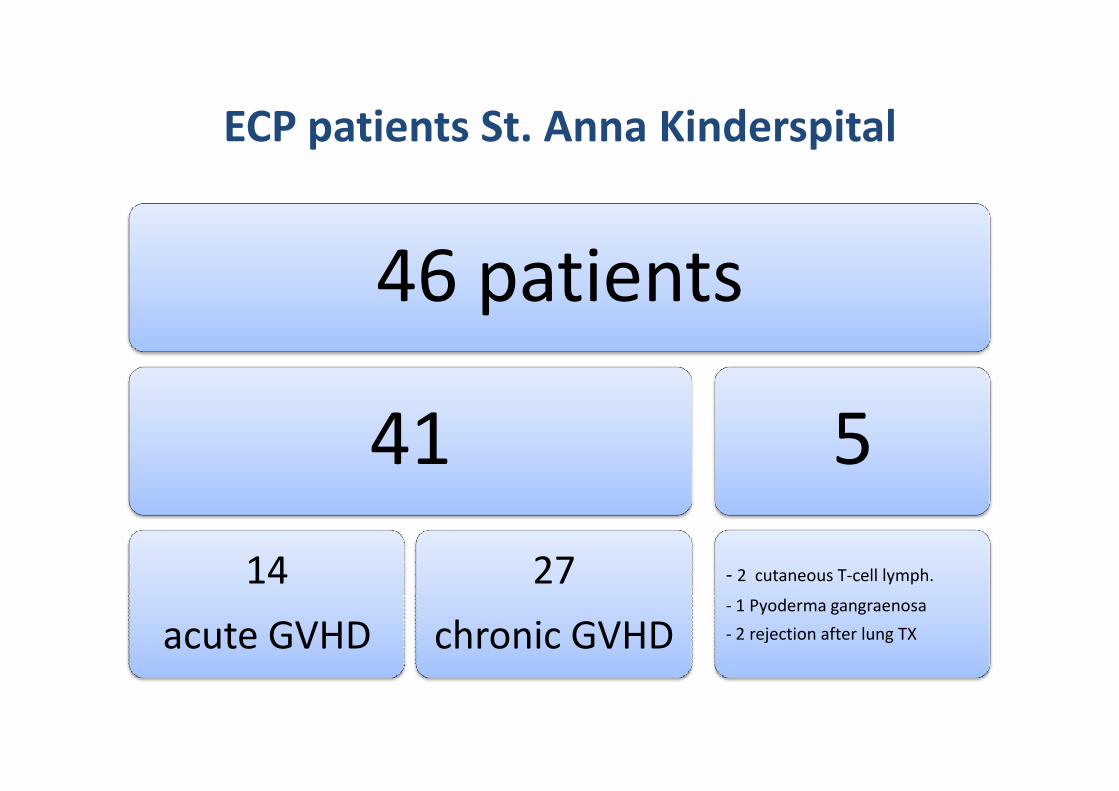
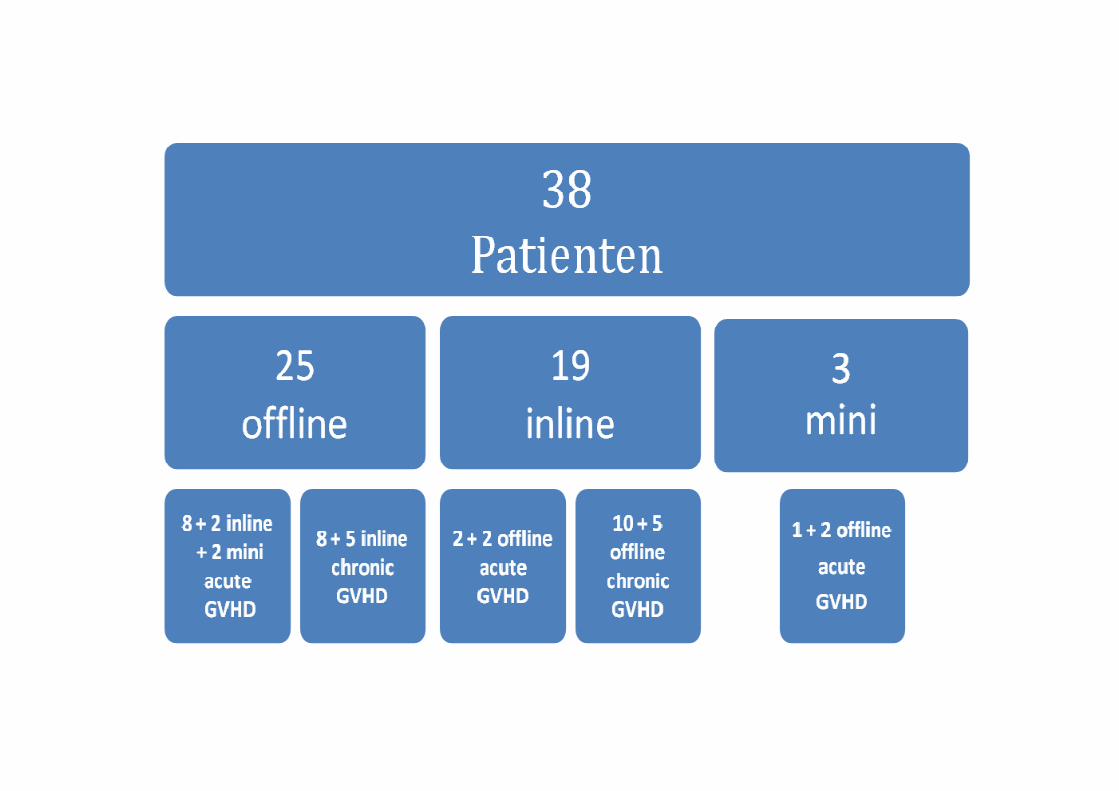
ECP patients St. Anna Kinderspital
46 patients
41 541
14
acute GVHD
27
chronic GVHD
5
- 2 cutaneous T-cell lymph.
- 1 Pyoderma gangraenosa
- 2 rejection after lung TX
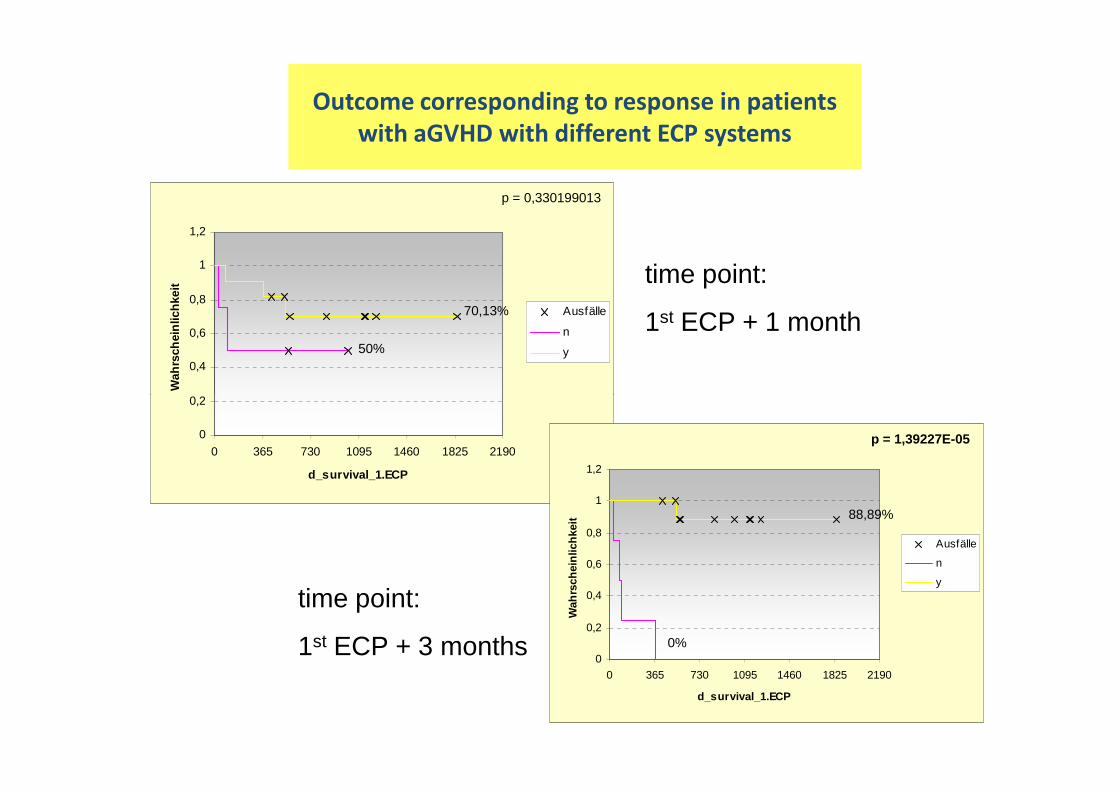
Outcome corresponding to response in patients
with aGVHD with different ECP systems
0,2
0,4
0,6
0,8
1
1,2
Wah
rsch
einl
ichk
eit
Ausfälle
n
y
time point:
1st ECP + 1 month
p = 0,330199013
70,13%
50%
0
0,2
0 365 730 1095 1460 1825 2190
d_survival_1.ECP
0
0,2
0,4
0,6
0,8
1
1,2
0 365 730 1095 1460 1825 2190
d_survival_1.ECP
Wah
rsch
einl
ichk
eit
Ausfälle
n
y
time point:
1st ECP + 3 months
p = 1,39227E-05
88,89%
0%
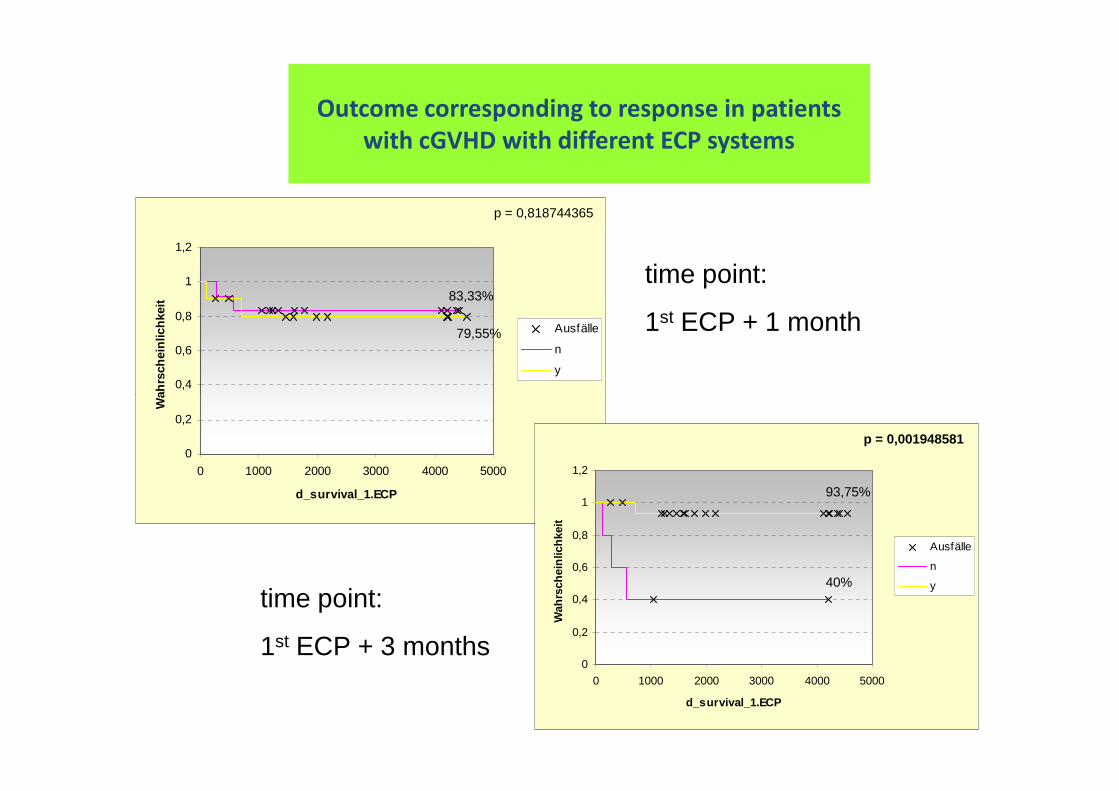
Outcome corresponding to response in patients
with cGVHD with different ECP systems
0,4
0,6
0,8
1
1,2
Wah
rsch
einl
ichk
eit
Ausfälle
n
y
p = 0,818744365
79,55%
83,33%time point:
1st ECP + 1 month
0
0,2
0 1000 2000 3000 4000 5000
d_survival_1.ECP
Wah
rsch
einl
ichk
eit
0
0,2
0,4
0,6
0,8
1
1,2
0 1000 2000 3000 4000 5000
d_survival_1.ECP
Wah
rsch
einl
ichk
eit
Ausfälle
n
y
p = 0,001948581
93,75%
40%
time point:
1st ECP + 3 months
TPE
06.06.2013 ÖGBT 2013 36

TPE TPE atat St. Anna Kinderspital St. Anna Kinderspital fromfrom 2008 2008 toto 20122012
• Indications– TTP– Myasthenia gravis– Opsoklonus Myoklonus Syndrom– Sepsis– SIRS– SIRS– ITP– MTX-Intoxication– Hyper IgE– Dysproteinemia– AIHA– Autoimmune disease– Rhabdomyolysis
TPE TPE atat St. Anna Kinderspital St. Anna Kinderspital fromfrom 2008 2008 toto 20122012
• In 30 patients 282TPE – Median age 13.8 y (0.94 – 22.7)
– Median bw 40 kg (9.9 – 80)
• In median 6 TPE per patient (1 – 40)In median 6 TPE per patient (1 – 40)
• In median 1940 ml plasma exchange (372 – 5270)
• In median 48.2 ml/kg plasma exchange (13 – 99)
• In median 10 Octaplas™ (2 – 19)
• In total 2244 units Octaplas™ (70% (2244/3178) of all transfused Octaplas™)

Cell separators
Cobe spectra™
OPTIA™ AMICUS™ Life18™
Cobe spectra™
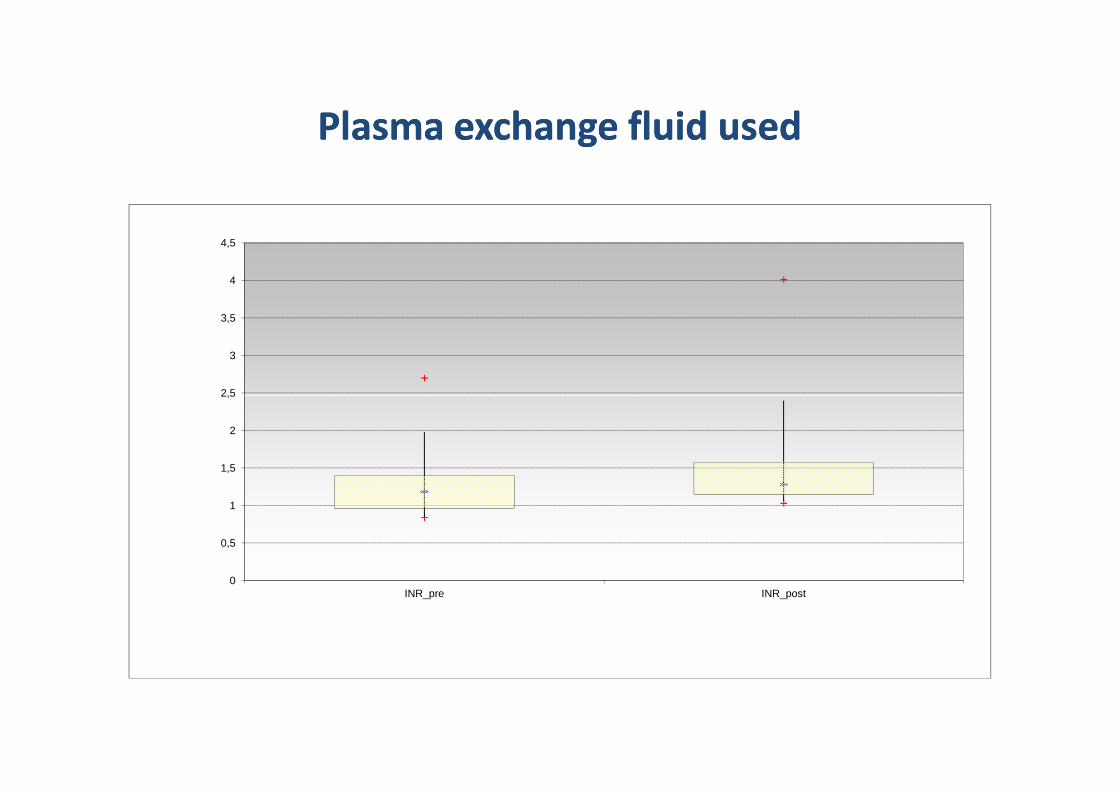
Plasma Plasma exchangeexchange fluid fluid usedused
2,5
3
3,5
4
4,5
0
0,5
1
1,5
2
2,5
INR_pre INR_post
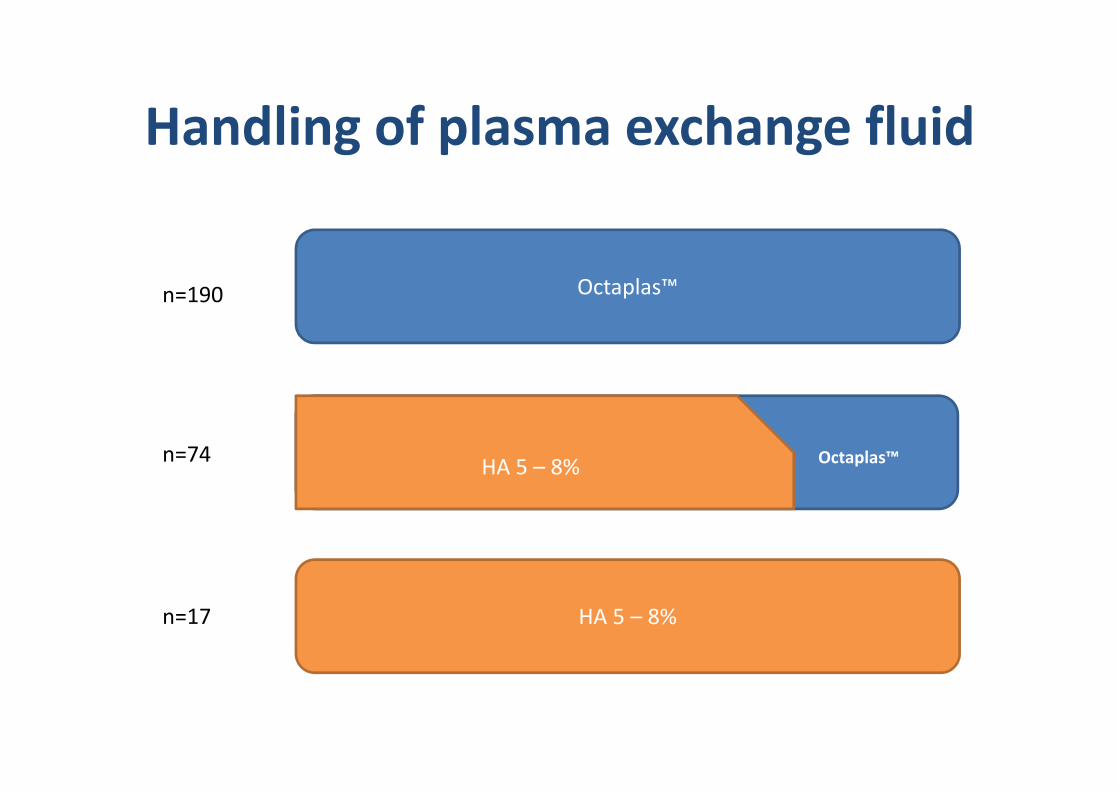
Handling of plasma exchange fluid
Octaplas™n=190
HA 5 – 8%
HA 5 – 8% Octaplas™
n=17
n=74
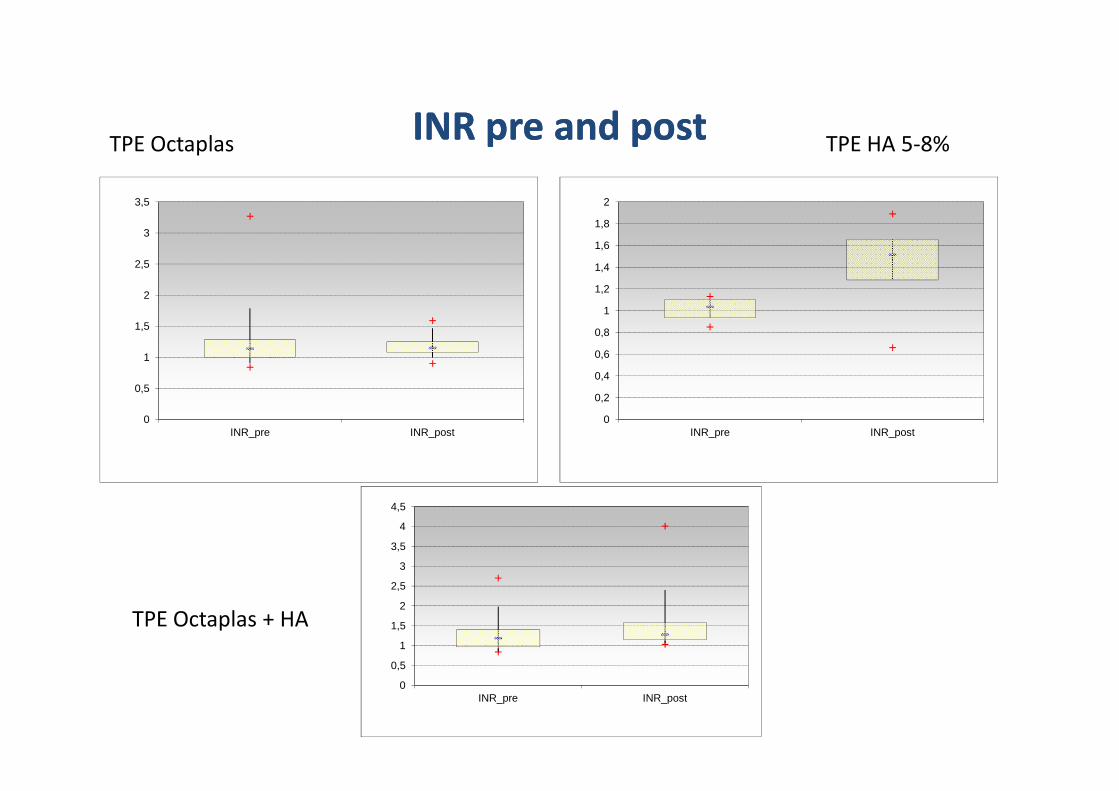
INR INR prepre andand postpost
0,5
1
1,5
2
2,5
3
3,5
TPE Octaplas TPE HA 5-8%
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
2
0INR_pre INR_post
0
0,2
INR_pre INR_post
TPE Octaplas + HA
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
INR_pre INR_post


Tandem Model St. Anna Kinderspital
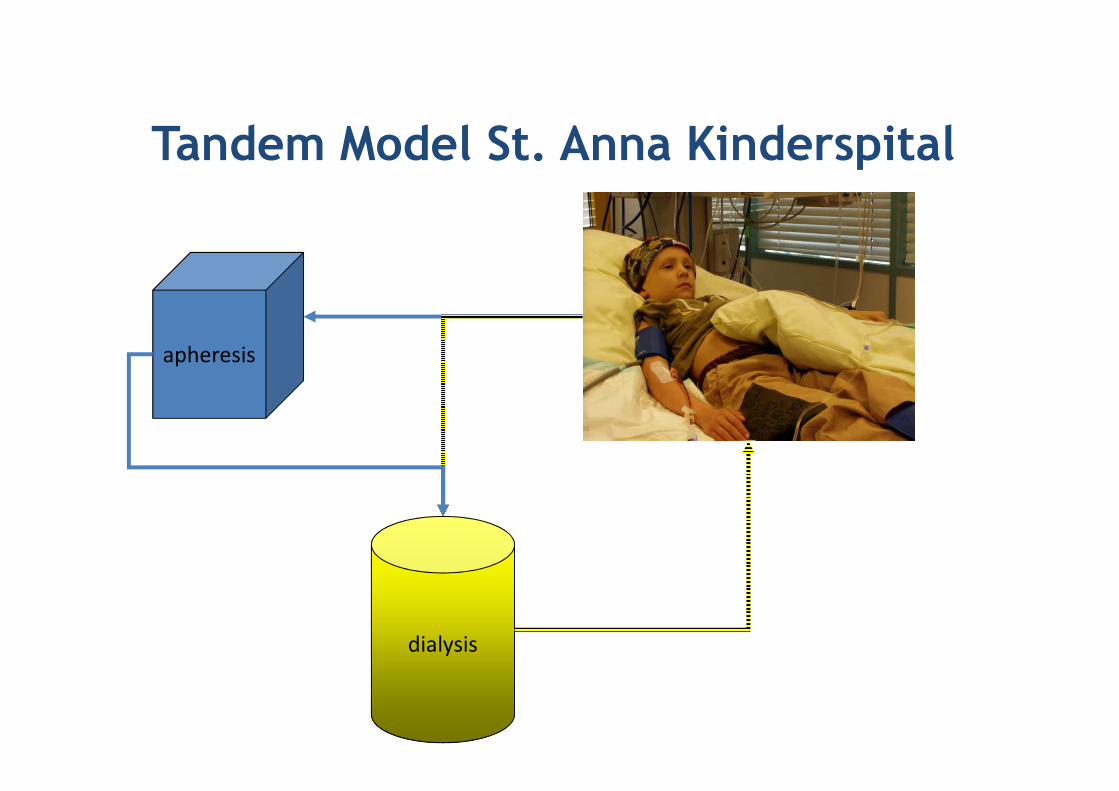
Tandem Model St. Anna Kinderspital
apheresis
dialysis
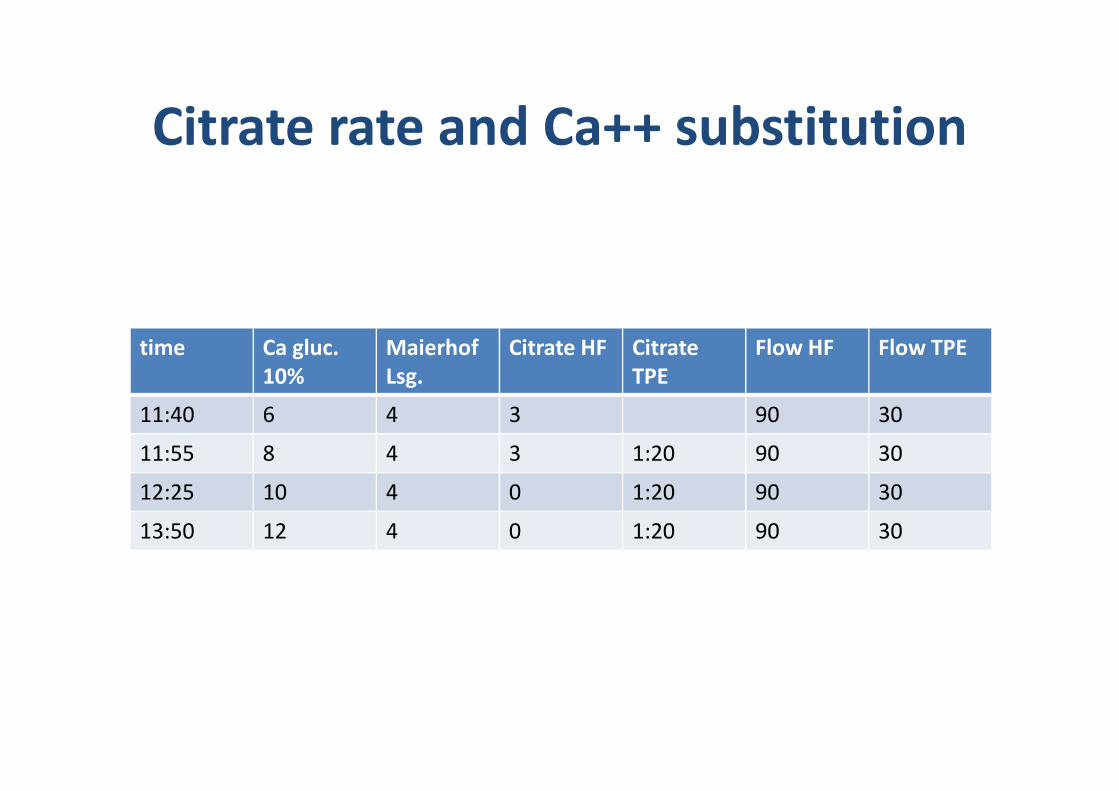
Citrate rate and Ca++ substitution
time Ca gluc.
10%
Maierhof
Lsg.
Citrate HF Citrate
TPE
Flow HF Flow TPE
11:40 6 4 3 90 30
11:55 8 4 3 1:20 90 30
12:25 10 4 0 1:20 90 30
13:50 12 4 0 1:20 90 30
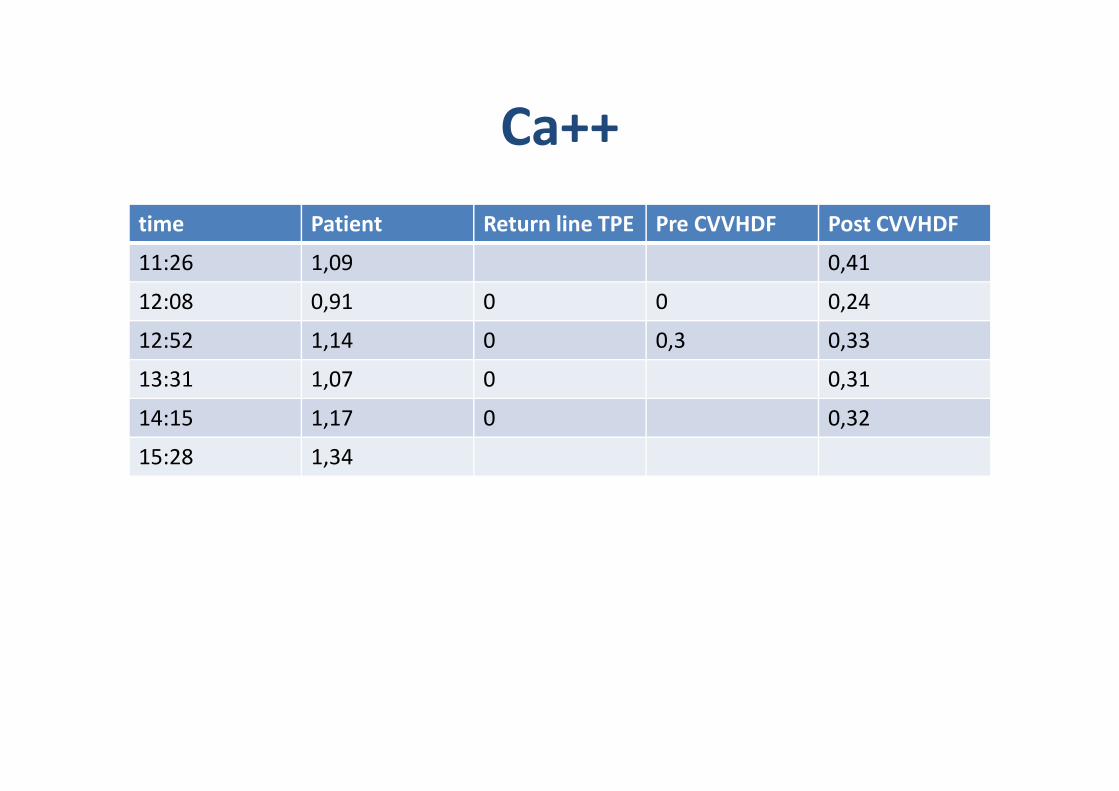
Ca++
time Patient Return line TPE Pre CVVHDF Post CVVHDF
11:26 1,09 0,41
12:08 0,91 0 0 0,24
12:52 1,14 0 0,3 0,33
13:31 1,07 0 0,31
14:15 1,17 0 0,32
15:28 1,34
• Since 2004 82 procedures in 18 patients• Age from 9 months to 19 years• Diagnosis
– 1 TTP
Tandem Model St. Anna Kinderspital
– 1 TTP – 10 Sepsis with MOF after SCT
– 2 FHL – 1 Histiocytosis (eventually familiar)
• Outcome all but 2 patient died (2 patients) due to second septic hit (12 patients) or underlying disease (2 patient)
RCA
06.06.2013 ÖGBT 2013 50
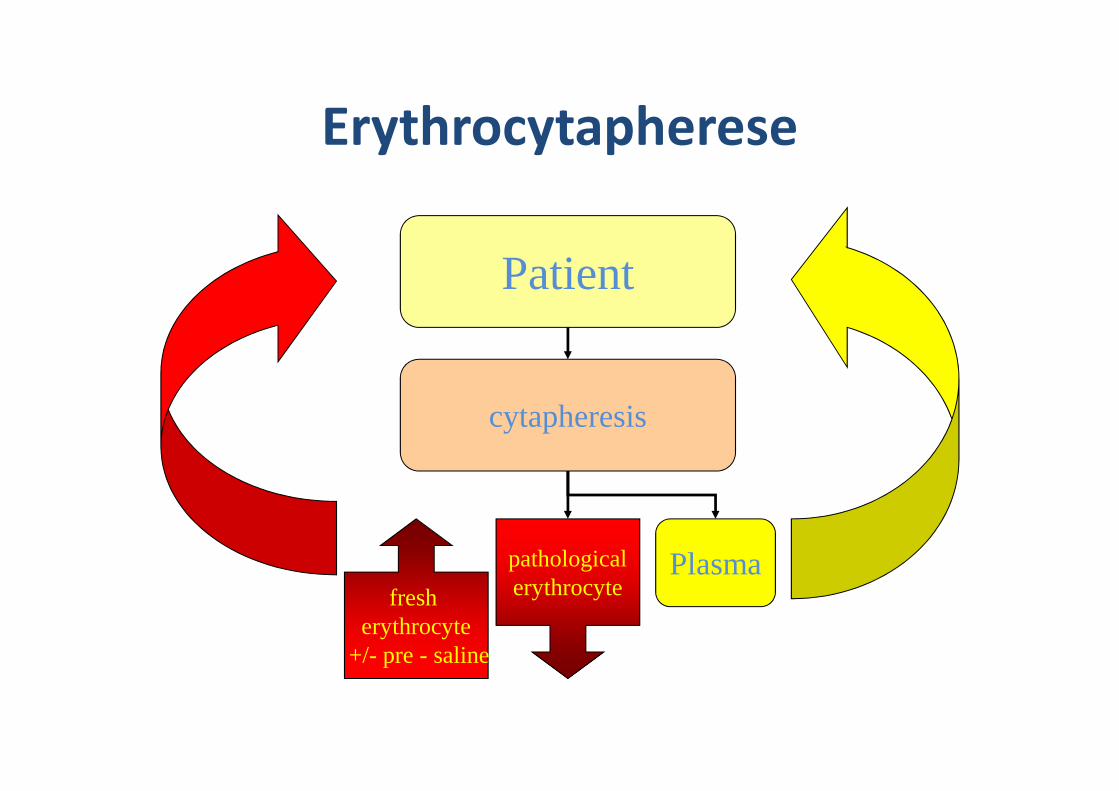
Erythrocytapherese
Patient
cytapheresis
Plasmapathologicalerythrocytefresh
erythrocyte+/- pre - saline
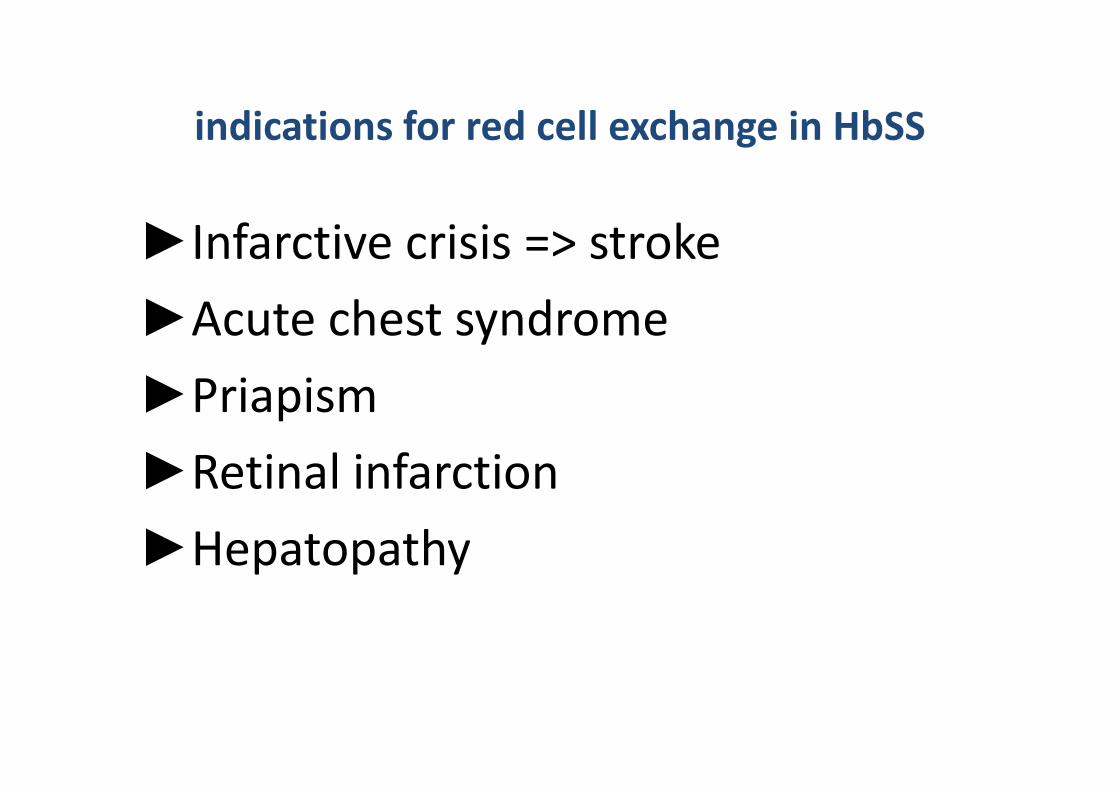
►Infarctive crisis => stroke
►Acute chest syndrome
►Priapism
indications for red cell exchange in HbSS
►Priapism
►Retinal infarction
►Hepatopathy
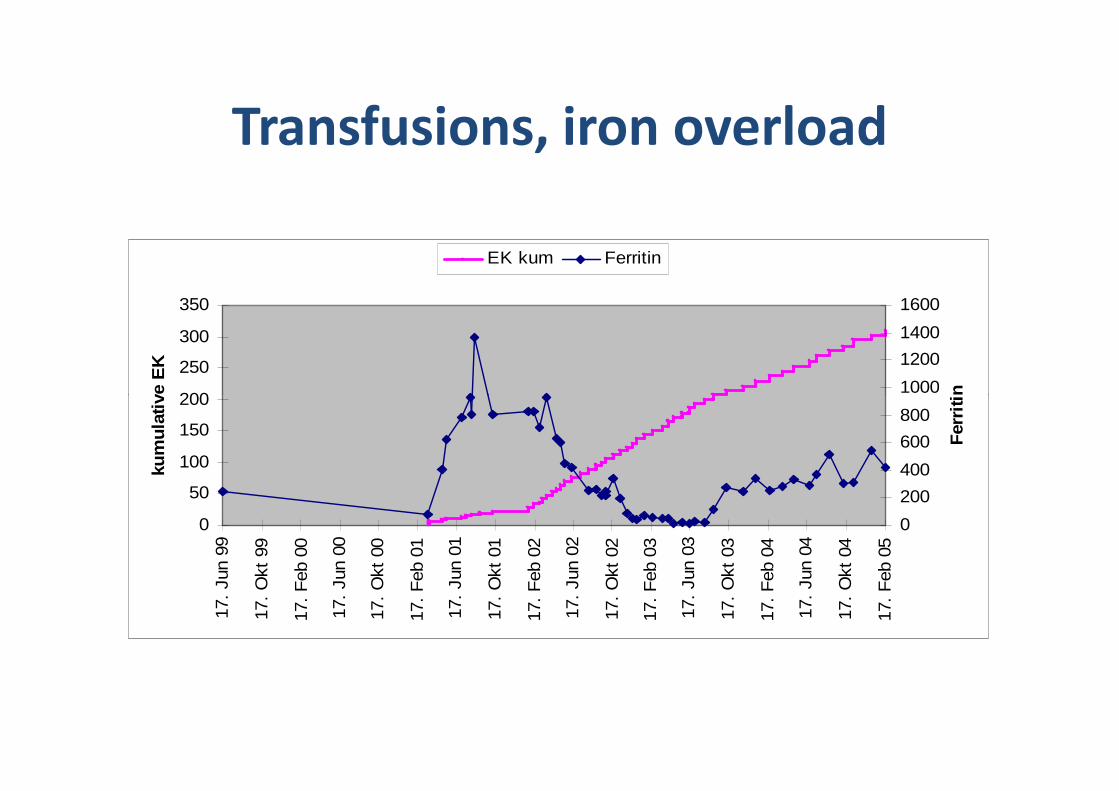
Transfusions, iron overload
200
250
300
350
kum
ulat
ive
EK
1000
1200
1400
1600
Fer
ritin
EK kum Ferritin
0
50
100
150
200
17.
Jun
99
17.
Okt
99
17.
Feb
00
17.
Jun
00
17.
Okt
00
17.
Feb
01
17.
Jun
01
17.
Okt
01
17.
Feb
02
17.
Jun
02
17.
Okt
02
17.
Feb
03
17.
Jun
03
17.
Okt
03
17.
Feb
04
17.
Jun
04
17.
Okt
04
17.
Feb
05
kum
ulat
ive
EK
0
200
400
600
800
1000
Fer
ritin
Patienten mit regelmäßigen RCA
am St. Anna Kinderspital
• 5 HBSS
– 1 Priapismus
– 3 prophylaktisch gegen stroke bei pathologischer intracerebraler Gefäßsituation (Stenosen, intracerebraler Gefäßsituation (Stenosen, Flußanomalien) trotz Litalir™
– 1 prophylaktisch bei rekurrierenden Milzsequestrationen
• 1 Pyrovatkinasedefizienz
06.06.2013 ÖGBT 2013 54

Plasmodium falciparum