Molekular-diagnostische Algorithmen beim … GI Oncology...Molekular-diagnostische Algorithmen beim...
21
Molekular-diagnostische Algorithmen beim Sporadischen und Hereditären Kolorektalen Karzinom: Was ist wann zu tun ? Reinhard Büttner Institut für Pathologie Universität Köln CIO Köln Bonn [email protected] GI-Oncology Wiesbaden 5-7-2014
Transcript of Molekular-diagnostische Algorithmen beim … GI Oncology...Molekular-diagnostische Algorithmen beim...
Molekular-diagnostische Algorithmen beim
Sporadischen und Hereditären Kolorektalen Karzinom:
Was ist wann zu tun ?
Reinhard Büttner
Institut für Pathologie Universität Köln
CIO Köln Bonn
GI-Oncology Wiesbaden 5-7-2014
1. Anstellungsverhältnis oder Führungsposition
Direktor des Instituts für Pathologie, Universität zu Köln
Gründer, Miteigentümer und Scientific CEO Targos Molecular Pathology GmbH, Kassel, Köln & San Francisco
2. Beratungstätigkeit
SAB AstraZeneca, BeyerHealthcare, BMS, Boehringer-Ingelheim, Merck-Serono, MSD, Novartis, Pfizer, Roche
3. Aktienbesitz
none
4. Honorare
Für SABs (s.o.)
5. Finanzierung wissenschaftlicher Untersuchungen
DFG, Deutsche Krebshilfe, BMBF, Pfizer (ROS, ALK Diagnostik)
6. Gutachtertätigkeit
DFG, Krebshilfe, Wilhelm-Sander-Stiftung, Marlene Porsche Stiftung, Rüdiger Stiftung, Vladimir Totovic Stiftung
7. Andere finanzielle Beziehungen
keine
Offenlegung potentieller Interessenkonflikte
I. Sporadische Kolonkarzinome number of polyps
predictive biomarkers
II. Familiäre Kolonkarzinome
1. HNPCC - Lynch Syndrom I, II 2.5 %
- Muir-Torre-Syndrom 0.5 %
2. FAP - Klassische Formen 1 %
- Atypische Form, MAP 1 %
3. Nichtadenomatöse Polyposis 0.1 %
- Peutz-Jeghers
- Juvenile Polyposis
- Cowden Syndrom
III. Kolonkarzinome bei CED time, activity
HNPCC
Diagnostische Algorithmen
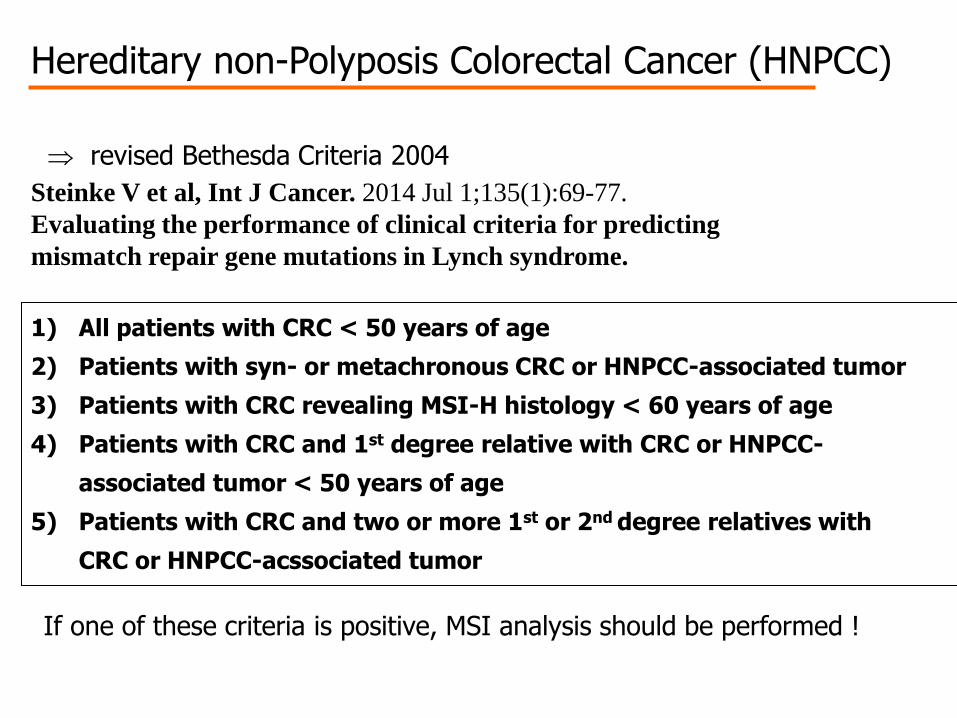
Hereditary non-Polyposis Colorectal Cancer (HNPCC)
revised Bethesda Criteria 2004
Steinke V et al, Int J Cancer. 2014 Jul 1;135(1):69-77.
Evaluating the performance of clinical criteria for predicting
mismatch repair gene mutations in Lynch syndrome.
1) All patients with CRC < 50 years of age
2) Patients with syn- or metachronous CRC or HNPCC-associated tumor
3) Patients with CRC revealing MSI-H histology < 60 years of age
4) Patients with CRC and 1st degree relative with CRC or HNPCC-
associated tumor < 50 years of age
5) Patients with CRC and two or more 1st or 2nd degree relatives with
CRC or HNPCC-acssociated tumor
If one of these criteria is positive, MSI analysis should be performed !
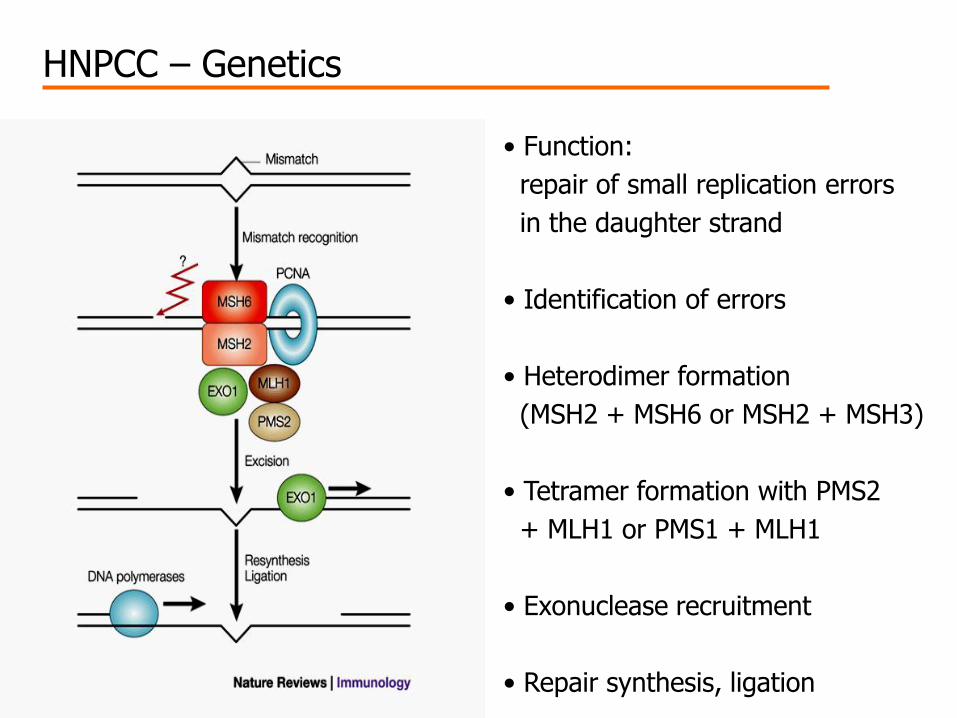
HNPCC – Genetics
• Function:
repair of small replication errors
in the daughter strand
• Identification of errors
• Heterodimer formation
(MSH2 + MSH6 or MSH2 + MSH3)
• Tetramer formation with PMS2
+ MLH1 or PMS1 + MLH1
• Exonuclease recruitment
• Repair synthesis, ligation
42 J, CRC
"Leber-CA" 40 J. Gebärmutter-
krebs 33 J.
40 & 53 J. CRC
71 J. Duodenal-Ca
59 J. Talgdrüsenadenome 41 & 54 J. CRC
32 J. CRC
36 J. CRC
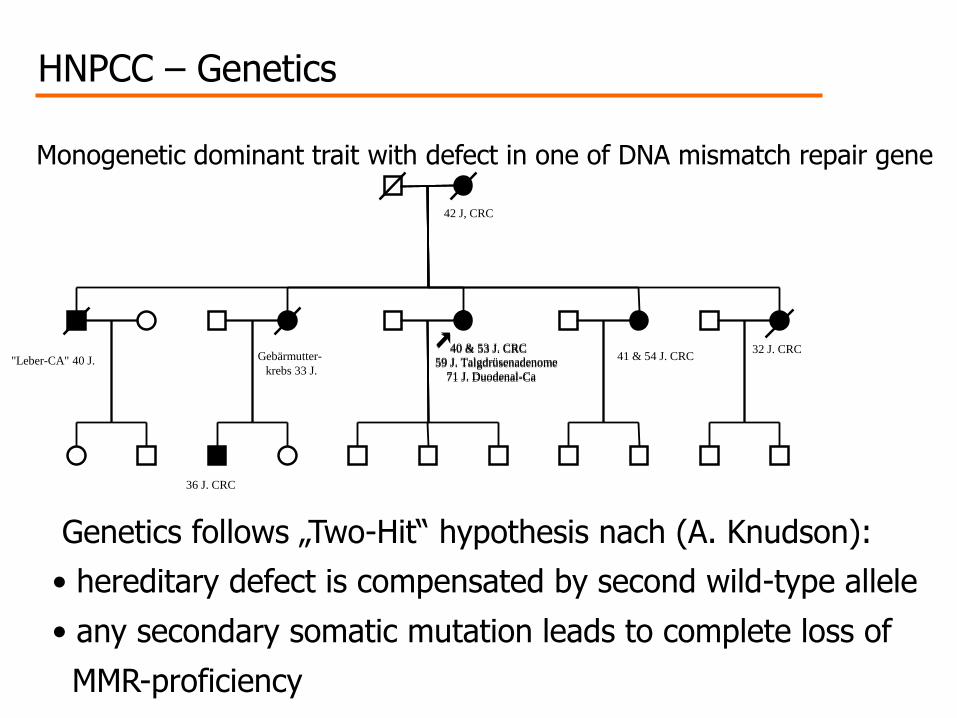
HNPCC – Genetics
Genetics follows „Two-Hit“ hypothesis nach (A. Knudson):
• hereditary defect is compensated by second wild-type allele
• any secondary somatic mutation leads to complete loss of
MMR-proficiency
Monogenetic dominant trait with defect in one of DNA mismatch repair gene
40 & 53 J. CRC
71 J. Duodenal-Ca
59 J. Talgdrüsenadenome
AT AT AT
AT AT AT
1
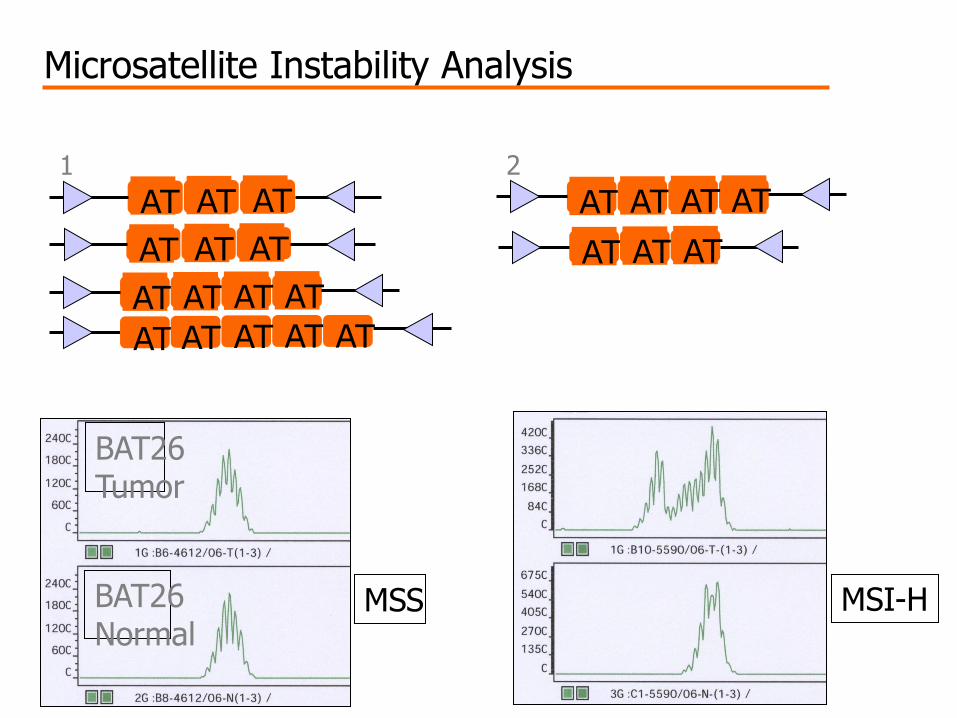
Microsatellite Instability Analysis
Agarosegelelektrophorese
1 2
AT AT AT AT
AT AT AT AT AT
AT AT AT
AT AT AT AT 2
BAT26 Tumor
BAT26 Normal
MSS MSI-H
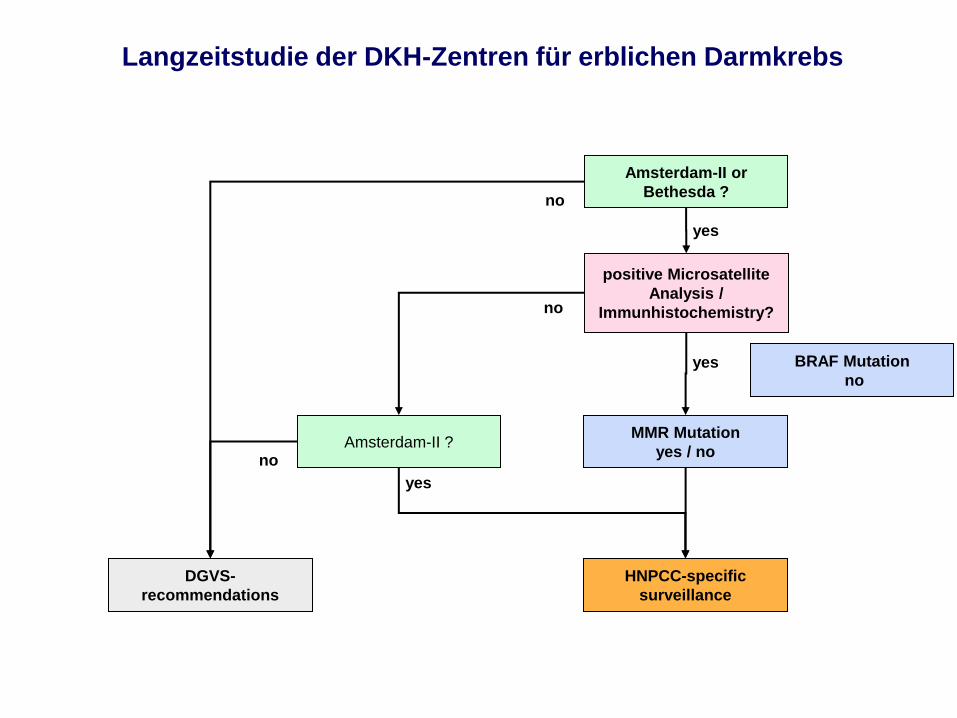
positive Microsatellite
Analysis /
Immunhistochemistry?
Amsterdam-II or
Bethesda ?
yes
MMR Mutation
yes / no Amsterdam-II ?
no
DGVS-
recommendations
HNPCC-specific
surveillance
no
no
yes
Langzeitstudie der DKH-Zentren für erblichen Darmkrebs
yes BRAF Mutation
no
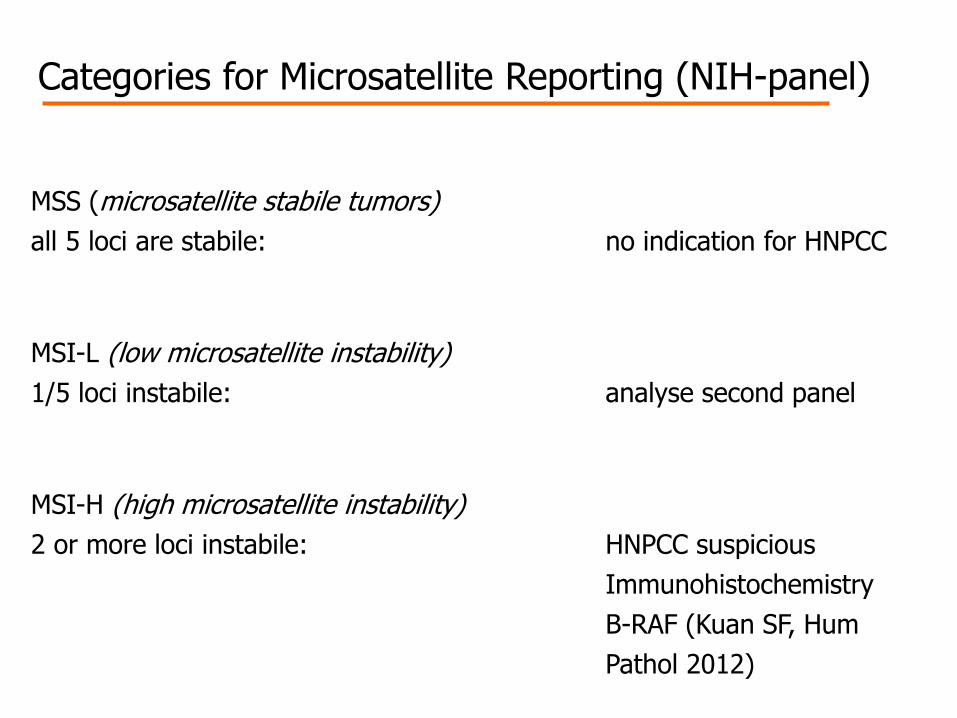
Categories for Microsatellite Reporting (NIH-panel)
MSS (microsatellite stabile tumors)
all 5 loci are stabile: no indication for HNPCC
MSI-L (low microsatellite instability)
1/5 loci instabile: analyse second panel
MSI-H (high microsatellite instability)
2 or more loci instabile: HNPCC suspicious
Immunohistochemistry
B-RAF (Kuan SF, Hum
Pathol 2012)
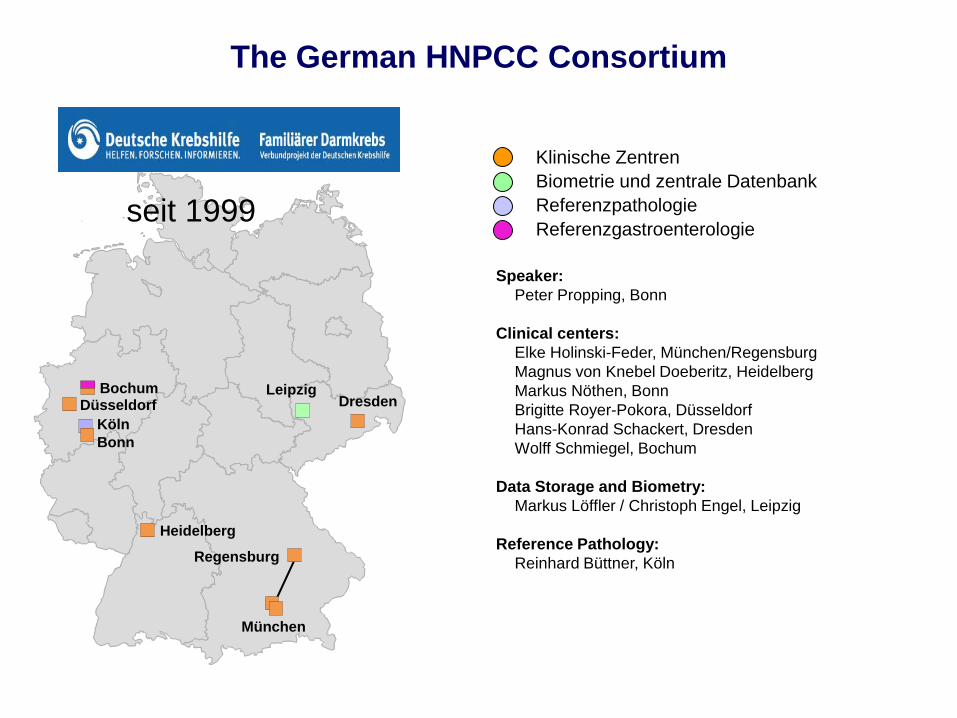
München
Heidelberg
Düsseldorf
Bonn
Dresden Bochum
Regensburg
Leipzig
seit 1999
Klinische Zentren
Biometrie und zentrale Datenbank
Referenzpathologie
Speaker:
Peter Propping, Bonn
Clinical centers:
Elke Holinski-Feder, München/Regensburg
Magnus von Knebel Doeberitz, Heidelberg
Markus Nöthen, Bonn
Brigitte Royer-Pokora, Düsseldorf
Hans-Konrad Schackert, Dresden
Wolff Schmiegel, Bochum
Data Storage and Biometry:
Markus Löffler / Christoph Engel, Leipzig
Reference Pathology:
Reinhard Büttner, Köln
The German HNPCC Consortium
Köln
Referenzgastroenterologie
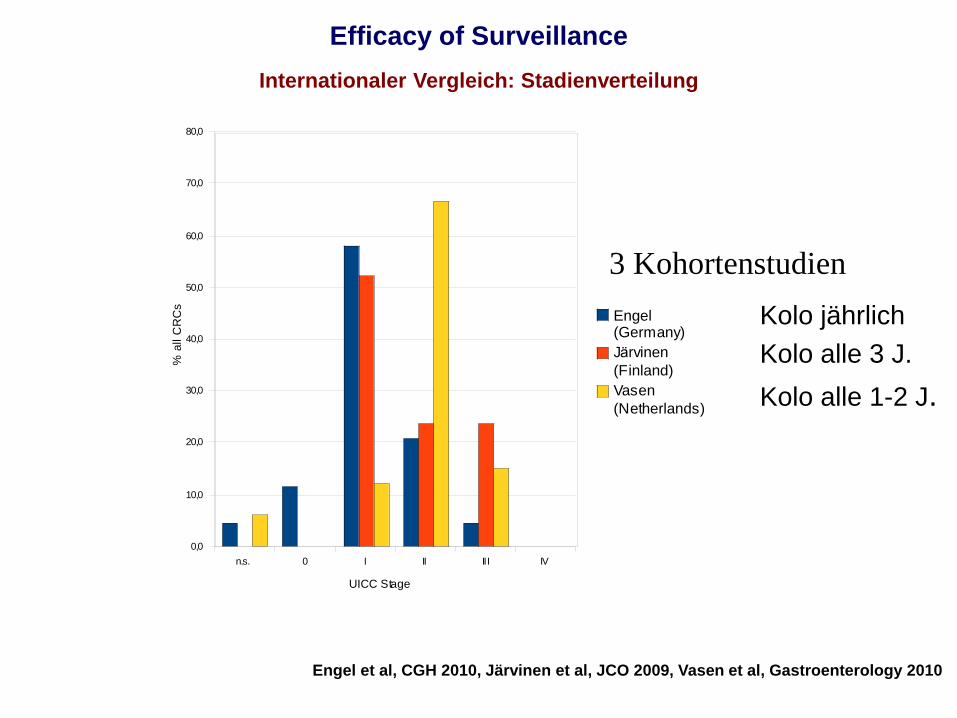
n.s. 0 I II III IV
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
Engel (Germany)
Järvinen
(Finland)
Vasen
(Netherlands)
UICC Stage
% a
ll C
RC
s
Engel et al, CGH 2010, Järvinen et al, JCO 2009, Vasen et al, Gastroenterology 2010
Kolo jährlich
Kolo alle 3 J.
Kolo alle 1-2 J.
Efficacy of Surveillance
Internationaler Vergleich: Stadienverteilung
3 Kohortenstudien
Sporadische CRCs
Biomarker Diagnostik im
Netzwerk Genomische Medizin
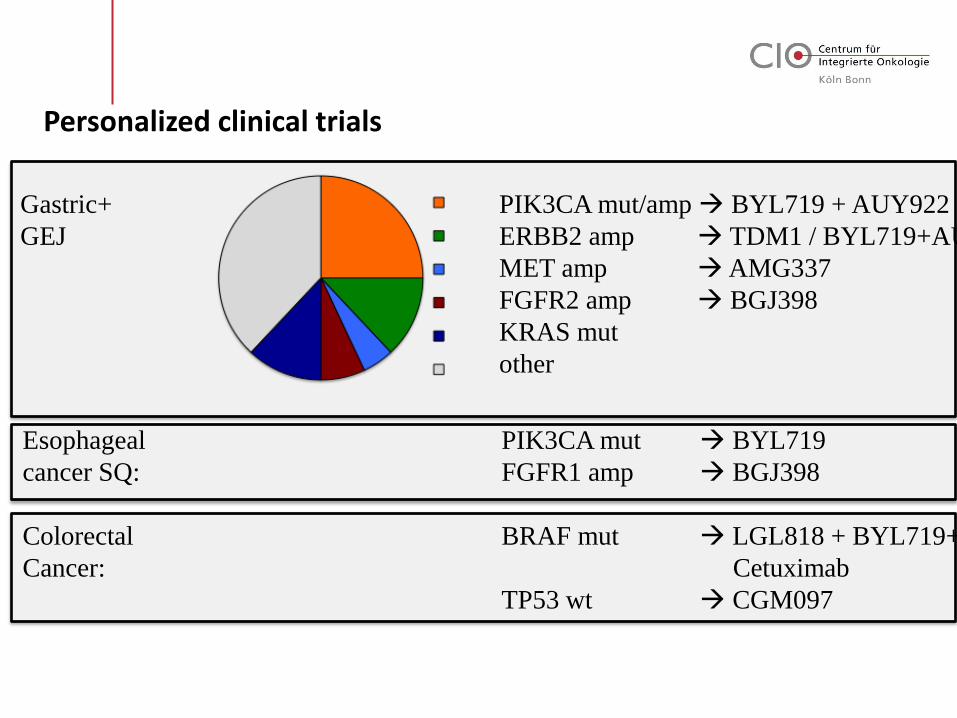
Personalized clinical trials
Esophageal PIK3CA mut BYL719
cancer SQ: FGFR1 amp BGJ398
Colorectal BRAF mut LGL818 + BYL719+
Cancer: Cetuximab
TP53 wt CGM097
Gastric+ PIK3CA mut/amp BYL719 + AUY922
GEJ ERBB2 amp TDM1 / BYL719+AUY922
MET amp AMG337
FGFR2 amp BGJ398
KRAS mut
other
Previous work
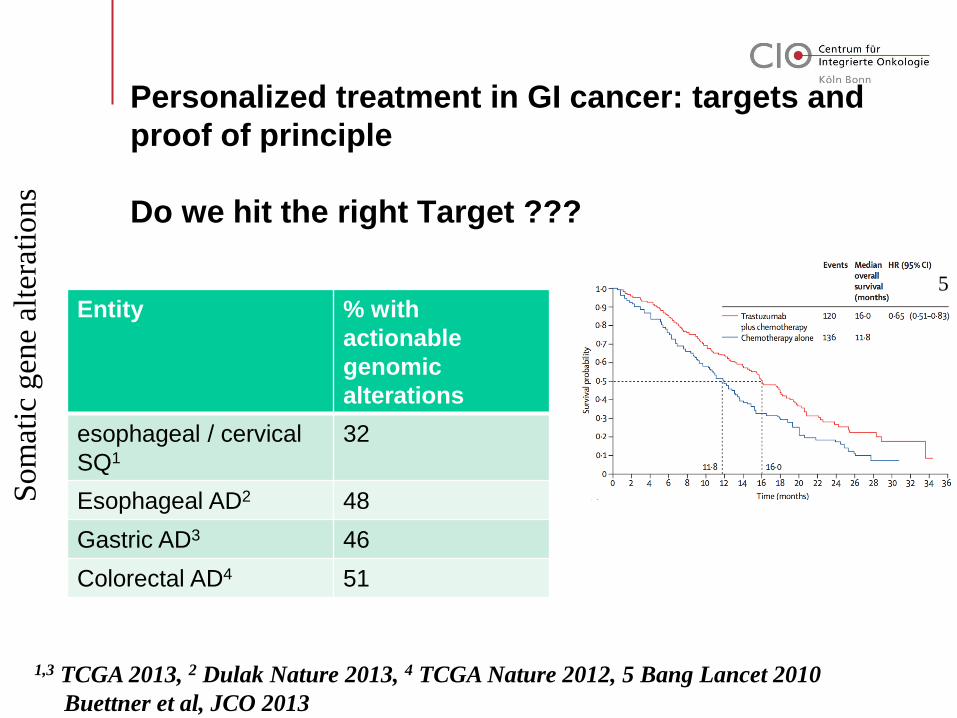
Personalized treatment in GI cancer: targets and
proof of principle
Do we hit the right Target ???
Entity % with
actionable
genomic
alterations
esophageal / cervical
SQ1
32
Esophageal AD2 48
Gastric AD3 46
Colorectal AD4 51
Som
atic
gen
e al
tera
tions
1,3 TCGA 2013, 2 Dulak Nature 2013, 4 TCGA Nature 2012, 5 Bang Lancet 2010
Buettner et al, JCO 2013
5
Introduction
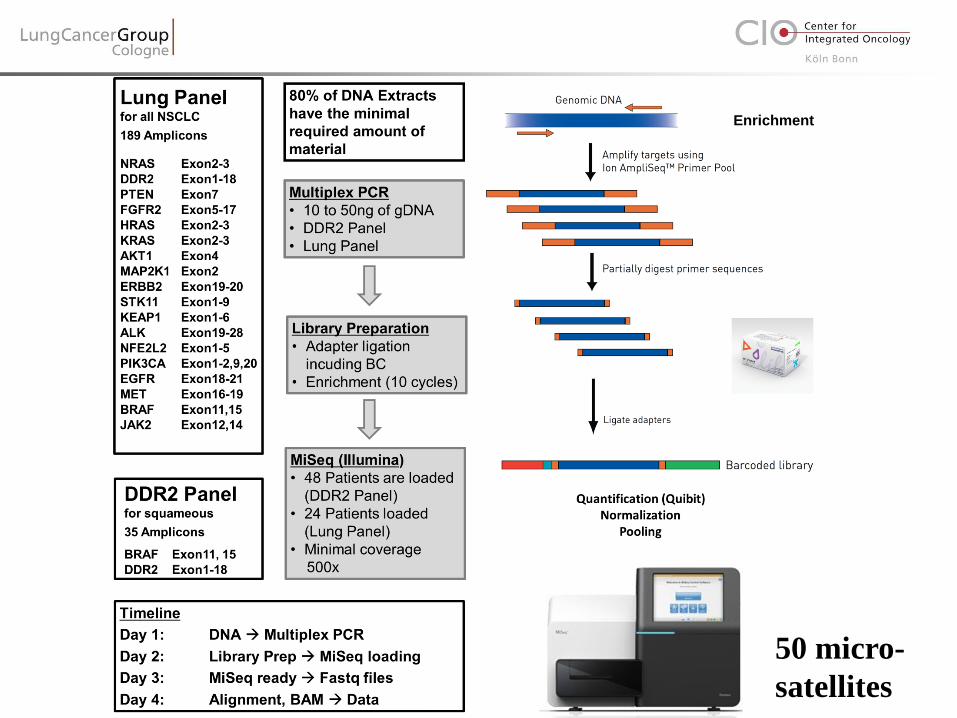
Enrichment
50 micro-
satellites
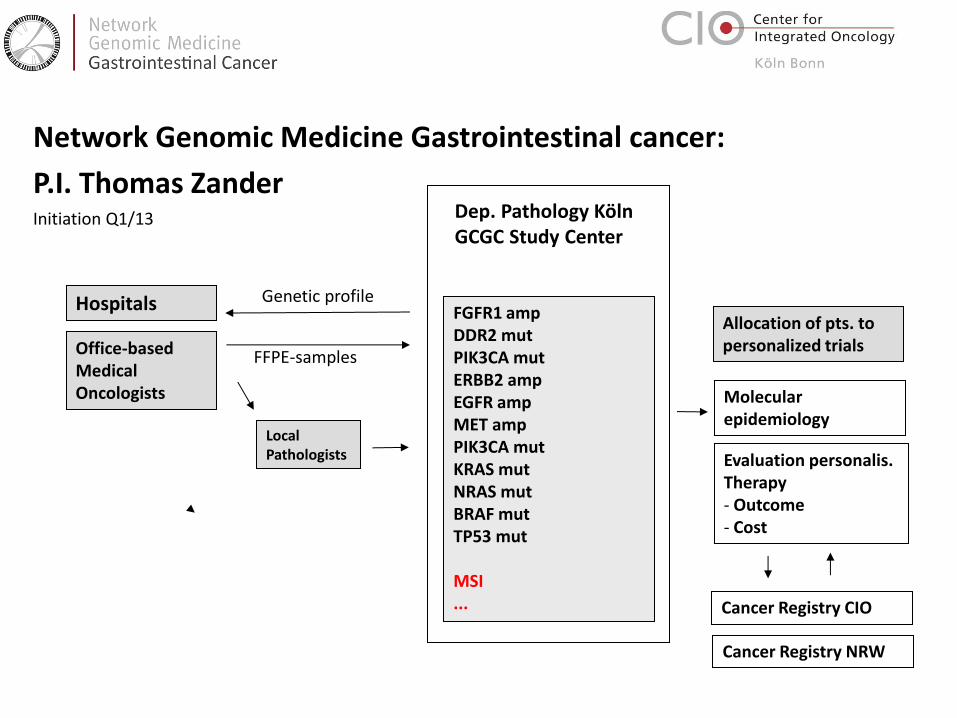
Hospitals
Office-based Medical Oncologists
FGFR1 amp DDR2 mut PIK3CA mut ERBB2 amp EGFR amp MET amp PIK3CA mut KRAS mut NRAS mut BRAF mut TP53 mut MSI ...
Local Pathologists
Dep. Pathology Köln GCGC Study Center
Molecular epidemiology
Allocation of pts. to personalized trials
Evaluation personalis. Therapy - Outcome - Cost
Cancer Registry CIO
Network Genomic Medicine Gastrointestinal cancer:
P.I. Thomas Zander Initiation Q1/13
FFPE-samples
Cancer Registry NRW
Genetic profile
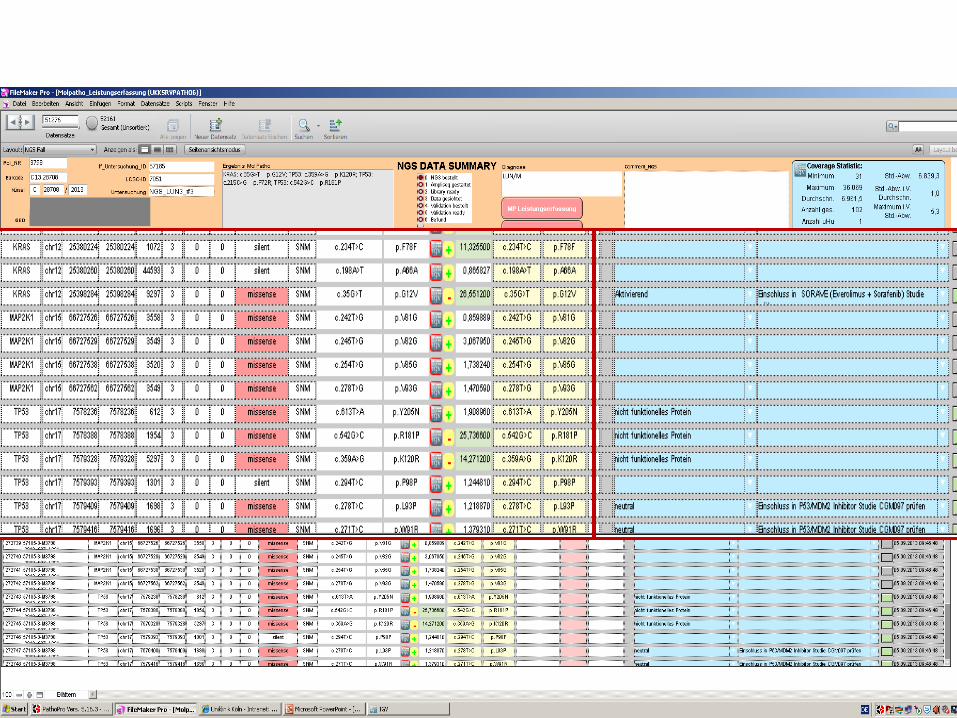
NGS – Datenauswertung: Filemaker
The value of genomic sequencing
> higher sensitivity
> correct histotyping
> pretherapeutic diagnostics of
Lynch Syndrome patients
> staging of multiple tumors
> comprehensive biomarker testing
> co-occurrance of genotypes and
therapy response
Combined Histology and Molecular
Diagnostics

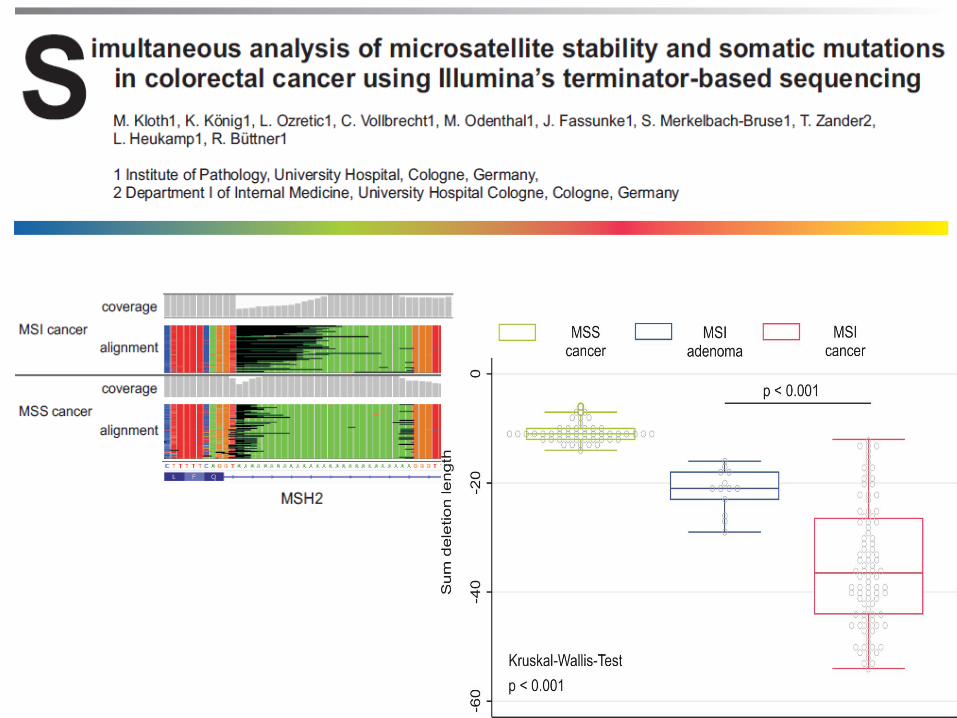
DDR2 mutations occur in a higher
frequency in Adeno compared to SCC
revealed by NGS
Lukas Heukamp Institute of Pathology, Cologne
Margarethe Odenthal
Claudia Vollbrecht
Sabine Merkelbach-Bruse
Jana Fassunke
Michaela Ihle
Helen Künstlinger
Carina Heydt
Theresa Buhl
Ursula Rommerscheidt-Fuss
Alexandra Florin
Frank Ueckeroth
Michael Kloth
Michal R Schweiger
Peter Nürnberg Cologne Center for Genomics (Cologne)
Janine Altmüller
Kerstin Becker
Christian Becker
Roman Thomas Institute of Genomics (Cologne)
Martin Peifer
Thomas Henkel Targos (Kaseel)
Katrin Stamm
Thomas Zander, Jürgen Wolf
Center for Integrated Oncology Cologne/ Bonn
GI- Cancer Group Cologne