Osteo Chron Schmerz
8
8/10/2019 Osteo Chron Schmerz http://slidepdf.com/reader/full/osteo-chron-schmerz 1/8 JAOA • Supplement 4 • Vol 105 • No 9 • September 2005 • S29 Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic Pain C hronic pain is a common problem that has a relatively high incidence and a low recovery rate. 1 The incidence of relapse following initially successful treatment is also significant. Persistent or relapsing pain often results from mis- diagnosis or inadequate treatment. 2 In other instances, focusing on pain gen- erators alone overlooks important patient-centered treatment strategies that are capable of modulating pain per- ception and quality of life. Finally, non- compliance with otherwise successful treatment programs may result from inadequate education concerning the prognosis and management of chronic disorders such as arthritis. 3 Dissatisfied with ineffective, incom- plete, and sometimes impersonal approaches to chronic disorders, a growing number of patients actively pursue complementary or alternative care, including manual modes of therapy and mind-body practices. 4,5 Properly pre- scribed approaches may confer some clinically significant benefits. It is recog- nized that many other manual modes of therapy such as massage and chiropractic provide distinct solutions for patients with chronic pain that would otherwise be ignored by nontouch modalities. Osteopathic manipulative medicine (OMM) is a component of osteopathic medicine’s approach to total patient care. It emphasizes application of osteopathic philosophy and integrates recognized healing approaches known as osteopathic manipulative treatment (OMT). Although OMM is generally recognized as a mainstream discipline, the National Institutes of Health considers OMT to be one of several promising “complemen- tary” procedures among a variety of het- erogeneous manipulative and body- based practices. An OMM approach provides the balance that patients with persistent pain seek between state-of-the- art interventions and individualized patient-centered care. For such patients, OMM treatment offers two main recog- nized advantages: an expanded differ- ential of potentially treatable etiologies and an individualized, patient-centered pain prescription based on the applica- tion of osteopathic principles. Many osteopathic physicians emphasize patient education and offer a pragmatic philosophy similar to that adopted by multidisciplinary pain man- agement clinics. In addition, OMT offers patients an additional therapeutic option with a low risk-to-benefit ratio and a growing evidence base of efficacy. 6 General Considerations in Patients With Chronic Pain Chronic pain mechanisms encompass a complicated array of different processes (eg, genetics, neurophysiology, psy- chology, and biomechanics), each capable of contributing to clinical manifestations and symptoms. For OMM to be effec- tive, similar symptoms in different patients may require dissimilar treatment plans that focus on differing local, spinal, and supraspinal targets. For example, chronic pain initiated by peripheral trauma may result when supraspinal structures continue to respond as if the peripheral tissues were actively injured. In other chronic conditions like fibromyalgia, the process may reflect an autonomic dysregulatory phenomenon or a dysfunction of descending antinoci- Osteopathic manipulative medicine (OMM) incorporates diagnostic and ther- apeutic strategies that address body unity, homeostatic mechanisms, and struc- ture-function interrelationships. In regard to pain, osteopathic physicians take thorough histories guided by palpatory examination to determine the quality, duration, and origin of this condition, how it uniquely affects the individual, and whether segmental, reflex, or triggered pain phenomena coexist. Osteopathic manipulative medicine expands differential diagnoses by considering somatic dysfunction and treatment options by integrating specific aspects of comple- mentary care into state-of-the-art pain management practices. Prescriptions formulated through an OMM algorithm integrate each osteo- pathic tenet with biopsychosocial and patient education models and medica- tion, rehabilitation, and manual medicine techniques proportionate to individual needs. Address correspondence to Michael L. Kuchera, DO, FAAO, Professor and Director, OMM Research, Co-Director, Center for Chronic Disorders of Aging, Philadelphia College of Osteopathic Medicine, 4190 City Ave, Suite 320, Philadelphia, PA 19130- 1633. Dr Kuchera discloses that he has no conflicts of interest. E-mail: [email protected] Osteopathic Manipulative Medicine Considerations in Patients With Chronic Pain Michael L. Kuchera, DO This continuing medical education publication supported by an unrestricted educational grant from Purdue Pharma LP
-
Upload
butlerwilliamcarlos -
Category
Documents
-
view
221 -
download
0
Transcript of Osteo Chron Schmerz

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 1/8
JAOA • Supplement 4 • Vol 105 • No 9 • September 2005 • S29Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic Pain
Chronic pain is a common problemthat has a relatively high incidence
and a low recovery rate.1 The incidenceof relapse following initially successfultreatment is also significant. Persistent orrelapsing pain often results from mis-diagnosis or inadequate treatment.2 Inother instances, focusing on pain gen-
erators alone overlooks importantpatient-centered treatment strategiesthat are capable of modulating pain per-ception and quality of life. Finally, non-compliance with otherwise successful
treatment programs may result frominadequate education concerning theprognosis and management of chronicdisorders such as arthritis.3
Dissatisfied with ineffective, incom-plete, and sometimes impersonalapproaches to chronic disorders, agrowing number of patients actively
pursue complementary or alternativecare, including manual modes of therapyand mind-body practices.4,5 Properly pre-scribed approaches may confer someclinically significant benefits. It is recog-nized that many other manual modes of therapy such as massage and chiropracticprovide distinct solutions for patientswith chronic pain that would otherwise be ignored by nontouch modalities.
Osteopathic manipulative medicine(OMM) is a component of osteopathicmedicine’s approach to total patient care.It emphasizes application of osteopathicphilosophy and integrates recognizedhealing approaches known as osteopathicmanipulative treatment (OMT).
Although OMM is generally recognizedas a mainstream discipline, the NationalInstitutes of Health considers OMT to beone of several promising “complemen-tary” procedures among a variety of het-erogeneous manipulative and body- based practices. An OMM approachprovides the balance that patients withpersistent pain seek between state-of-the-art interventions and individualizedpatient-centered care. For such patients,OMM treatment offers two main recog-
nized advantages: an expanded differ-ential of potentially treatable etiologiesand an individualized, patient-centeredpain prescription based on the applica-tion of osteopathic principles.
Many osteopathic physiciansemphasize patient education and offera pragmatic philosophy similar to thatadopted by multidisciplinary pain man-agement clinics. In addition, OMT offerspatients an additional therapeutic optionwith a low risk-to-benefit ratio and a
growing evidence base of efficacy.6
General Considerationsin Patients With Chronic PainChronic pain mechanisms encompass acomplicated array of different processes(eg, genetics, neurophysiology, psy-chology, and biomechanics), each capableof contributing to clinical manifestationsand symptoms. For OMM to be effec-tive, similar symptoms in differentpatients may require dissimilar treatment
plans that focus on differing local, spinal,and supraspinal targets. For example,chronic pain initiated by peripheraltrauma may result when supraspinalstructures continue to respond as if theperipheral tissues were actively injured.In other chronic conditions likefibromyalgia, the process may reflect anautonomic dysregulatory phenomenonor a dysfunction of descending antinoci-
Osteopathic manipulative medicine (OMM) incorporates diagnostic and ther-apeutic strategies that address body unity, homeostatic mechanisms, and struc-ture-function interrelationships. In regard to pain, osteopathic physicians takethorough histories guided by palpatory examination to determine the quality,duration, and origin of this condition, how it uniquely affects the individual,and whether segmental, reflex, or triggered pain phenomena coexist. Osteopathicmanipulative medicine expands differential diagnoses by considering somaticdysfunction and treatment options by integrating specific aspects of comple-mentary care into state-of-the-art pain management practices.
Prescriptions formulated through an OMM algorithm integrate each osteo-pathic tenet with biopsychosocial and patient education models and medica-
tion, rehabilitation, and manual medicine techniques proportionate to individualneeds.
Address correspondence to Michael L. Kuchera,DO, FAAO, Professor and Director, OMM Research,Co-Director, Center for Chronic Disorders of Aging,Philadelphia College of Osteopathic Medicine,4190 City Ave, Suite 320, Philadelphia, PA 19130-1633.
Dr Kuchera discloses that he has no conflicts ofinterest.
E-mail: [email protected]
Osteopathic ManipulativeMedicine Considerations inPatients With Chronic Pain
Michael L. Kuchera, DO
This continuing medical education publication supported byan unrestricted educational grant from Purdue Pharma LP

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 2/8
ception pathways. Other conditions suchas myofascial trigger points (MTrPs)demonstrate specific peripheral dys-function at a spinal level perpetuated bynonspecific biomechanical factors, eg,untreated postural strain, or through vis-cerosomatic reflexes.
In many cases, chronic pain path-ways involving allodynia (generalizedlowered thresholds to pain) develop aschanging gene expression allows silentreceptors to become active in the spinalcord, or when facilitatory modulationresults in what is called “spinal cordlearning.”7,8 In each case, the patient maysimply present with persistent pain.
Therefore, rational OMT of patientswith persistent pain cannot have a sin-gular focus, nor can it be treated as a
static phenomenon. In formulating mul-timodal treatment plans, OMMapproaches embrace body unity princi-ples and integrate palpation and OMTtechniques into each patient’s prescrip-tion. Choices concerning OMT tech-niques and goals depend on each indi-vidual’s unique pain presentation, thesuspected pathways involved in that pre-sentation, and the regions diagnosed ascontaining somatic dysfunction.
A total review of diagnostic regi-
mens and therapeutic options for per-sistent pain is beyond the scope of thisarticle. Therefore, this article provides aconcise overview of the OMM paradigmand introduces a general algorithm forpain management. Discussion of persis-tent pain management is limited to gen-eralities that concern the integration of osteopathic principles and practice (OPP)in the use of OMT. Where pertinent, spe-cific common chronic pain presentationsare described as examples supporting
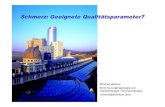
the algorithm ( Figure1).
AlgorithmWhen patients present with chronic pain,especially pain that persists despite seem-ingly appropriate care, an algorithm( Figure 1) can suggest an approach forapplying OPP and OMT. It is structuredto identify and address frequently over-looked underlying etiologies includedin an osteopathic differential diagnosisas well as the persistent tangible andholistic impact of pain on the body unit.Evaluation of the patient’s capability to
mount a homeostatic response and theunderlying pathophysiologic status asinterpreted by components of palpatedsomatic dysfunction guide the physi-cian’s timing for implementing OMMtreatment strategies.
Treatment protocols formulated
from this algorithm incorporate the inter-dependence of all tenets of osteopathicmedicine and result in an individuallydesigned prescription to address eachpatient with persistent pain.
Structure-Function Considerations:Somatic Causes of Persistent PainCertain somatic findings have been con-sistently documented in various persis-tent pain conditions. Depending on thecondition, the somatic dysfunction may
be causative, reflexive, reactive, or per-petuating, or a combination. Thus, dif-ferential diagnoses and treatment con-siderations depend on both the specificregion and underlying pathophysiologyinvolved. The algorithm ( Figure 1) con-tains generalities taking these factors andstructure-function interrelationships intoconsideration.
An osteopathic palpatory examina-tion often provides clues to the under-lying mechanism of injury.2 Such palpa-
tory insights lead to further questions,examinations, and tests designed to iden-tify structural factors associated with spe-cific pain generators or those that mayinterfere with certain self-healing mech-anisms. The findings lead the physicianto explore functional demand issues asso-ciated with potential mechanisms of repeated injury or of cumulative micro-trauma resulting from postural, habitual,or occupational ergonomic stresses.
One way to determine whether a
given structure or somatic dysfunction isa primary cause of significant discomfortis to determine if it is a “pain generator”tissue. Comparing quality, anatomic loca-tion, and unique referral distribution withknown sclerotomal, myotomal, and neu-rologic pain maps increases the chance of locating a pain generator. Often, suchdiagnoses are confirmed by an effectivetherapeutic response, even temporarily,to local anesthetic injection or manual cor-rection of dysfunction.
Sclerotomal tissues (skeletal, arthro-dial, and ligamentous generators) typi-
cally mediate pain described as being“deep, dull, and toothache-like.” Sclero-tomal pain patterns are frequently over-looked because they may project somedistance from their pain generators andare infrequently taught to osteopathicphysicians. The “Glossary of Osteopathic
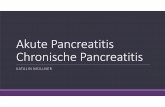
Terminology” contains sclerotomal mapsrelating spinal segmental levels to scle-rotomal appendicular pain.9 Figure2 illus-trates segmentally related sclerotomalexamples of ligamentous pain patternscommonly seen in low back pain (LBP).Patients with ligamentous pain genera-tors often cannot find a comfortable posi-tion and are continuously shifting posi-tion, a presentation some refer to as“theatre cocktail party syndrome.”10
Myotomal (muscle) pain is also
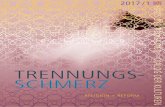
poorly localized, and the patient maydescribe symptoms located at a signifi-cant distance from the actual lesion site.Patients typically describe myotomalpain as “achy,” “stiff,” or “crampy,” andthe pain often “grabs” them. Muscle dys-function may include latent and activeMTrPs11 that when overused refer pain inrecognizable patterns12,13 ( Figure3). Anti-gravity muscles harboring MTrPs arefrequently hypertonic, whereas posturalantagonist muscles demonstrate weak-
ness to strength testing.10 Both are likelyto contain taut bands demonstrating alocal twitch response within the affectedmuscle during perpendicularly appliedsnapping palpatory examination. Thisphenomenon has been linked to the pres-ence of segmentally related spinalreflexes (segmental facilitation).14,15
Peripheral myotomal pain genera-tors can originate in a single muscle.Alternatively, multiple peripheral inputsmay establish more complex patterns of
muscle dysfunction. Peripheral input canalso produce a central imprint that per-sists as a central source of pain-modi-fying peripheral referral patterns(somatosomatic reflex). Commonmyotomal patterns also include thosesharing the same radicular innervation(as occurs in discogenic disease) or thosemuscles contributing to the same gen-eral function (as in the myotatic unit pat-tern occurring in an overuse syndrome).
In structure-function considerations,osteopathic diagnostic palpation seeksto identify “any impaired or altered
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic PainS30 • JAOA • Supplement 4 • Vol 105 • No 9 • September 2005

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 3/8
skeletal, arthrodial, and/or myofascialfunction” (viz “somatic dysfunction”9)adding to the nociceptive load and torecognize any related neural, vascular,and/or lymphatic elements that mightcomplicate underlying pathophysiologicconditions. The palpatory characteristicssought include sensitivity to measuredpalpation, tissue texture change, asym-metry, and restricted motion (STAR char-acteristics). Tissue texture changes oftenprovide the most important informationconcerning the underlying pathophysi-
ologic status of the periphery and thepatient’s homeostatic response status.
Osteopathic manipulative treatmentmay be delivered to reduce or removethe identified somatic dysfunction or toattempt to modulate central and periph-eral mechanisms involved in pain gen-eration after weighing risk-to-benefitratios associated with the resultant ten-tative diagnosis. Currently, palpatedperipheral tissue texture characteristicshave the greatest influence on the physi-cian’s choice of an activating force for
the OMT. Sophistication should improve,however, as studies reveal how differingmanual forces affect mechanoreceptorsand mechanonociceptors in the tenseg-rity-integrin model, spinal cord gatingmechanisms, and synaptic plasticity.16
Exemplars: Low Back Pain andHeadaches—The two best-documentedexemplars for the application of struc-ture-function approaches in diagnosisand treatment of patients with persistentpain symptoms are LBP and cervicogenicheadache. These two high-incidence con-
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic Pain JAOA • Supplement 4 • Vol 105 • No 9 • September 2005 • S31
Consider Body Unity Issues Consider Homeostatic Issues
History of Persistent PainDespite Traditional Workup and Treatment
Consider Structure-Function Issues
Consider specific somaticdysfunctions affecting eachtenet of osteopathic medicineabove and models in Figure 4
Body Unity Treatment forIndividual
OMT (somatoemotional?) Percussion hammer OMT Antidepressant treatment Patient education and counseling
Homeostatic Mechanism Treatmentfor Individual
OMT: ANS model OMT: Respiratory-circulatory model OMT: Postural model Medication to support homeostasis
Structure-Function Treatment forIndividual
Patient education re habits,ergonomics
OMT addressing specific somaticdysfunction
Exercise/rest (specific); anti-inflammatory treatment
Orthotics (if needed)
Post-Osteopathic ManipulativeTreatment (OMT) recurrent pattern?
Consider viscerosomatic-somatovisceral reflexes
Post-OMT recurrence
Consider perpetuating factors
Rational osteopathic manipulative medicine(OMM) care considers each of these three issues
History ofpotentialemotional-spiritual issuelinked toregion?
Evidence ofdepression orexcessivefatigue?
Postural
decompensation(primary orperpetuatingfactor)
History of
poorergonomicsor habits
Specific
neuromusculo-skeletaldysfunctionfindings
Biomechanical issue?Specific painsyndromes
Functional demand?Dysfunction of central biochemistry
Dysfunction of local biochemistry
Dysfunction of primary and/orsecondary respiration
Increased autonomic nervoussystem (ANS) response
Figure 1. Algorithm for integration of osteopathic principles and practice and osteopathic manipulative medicine in diagnosis and treatment of persistent pain.

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 4/8
ditions are multifactorial, yet typicallyneuromusculoskeletal in origin, and theyeach have great propensity for disability.The evidence base is strongest in thesetwo regions for interexaminer reliabilityof STAR objective findings in palpatorydiagnosis,17 as well as for the measur-
able benefit from manual treatment inreducing pain and disability.18-21 Fur-thermore, studies specifically identify aspecific role for OMT in LBP manage-ment.6
The role for manual modes of therapy such as OMT has been docu-mented for acute, subacute, and chronicLBP18-21; in patients with LBP; specifi-cally, spinal manipulation has effects sim-ilar to efficacious prescription NSAIDsand better effects than either physical
therapy or home back exercises (or both).21 Positive long-term functional out-comes have also been demonstrated.22
Based on the literature, Mein23 postulatesthat populations with subacute (sec-ondary) and chronic (tertiary) LBP would benefit most from manipulative carerather than using more costly functionalrestoration, behavioral modification, andchronic pain management programs.
Using a structure-function approach,Greenman24 examined 183 patients who
had persistent LBP for an average of 31 months. With osteopathic palpation,he identified three or more of six
common diagnoses in 50% of this cohort(Table). Treatment with OMT to elimi-nate the identified somatic dysfunctionresulted in nearly 75% of the dysfunc-tional group returning to work or to theiractivities of daily living. This author hasalso noted that undiagnosed somatic dys-
function, particularly “nonphysiologicdysfunctions” (such as pelvic shears),may result in years of persistent pain,either locally, or at distant sites linkedthrough compensatory mechanisms orthe development of MTrPs.25(pp463-512)
Dysfunction of one sacroiliac joint dueto nonphysiologic pelvic shears greatlyincreases functional demand on the othersacroiliac joint and its stabilizing liga-ment.
Removal of myofascial somatic dys-
function, including MTrPs, has also beenshown to be extremely effective inreducing or eliminating persistent LBP.Patients with trigger points displayed onthe common composite MTrP chartsshown in Figure 3 responded well to awide range of treatment modalities,including various OMT techniques suchas counterstrain, post–isometric relax-ation muscle energy, and myofascialrelease variants.11,12 Manual correction of myofascial or articular somatic dysfunc-
tion also proves to be an effective adjunctregardless of whether pain also radiatesinto the lower extremity.12(pp168-185),26
With recurrence of the same patternof pain and somatic dysfunction afterotherwise effective OMT, the clinicianshould consider dysfunctional homeo-static mechanisms and a range of per-petuating factors (including posturaldecompensation), as well as site-specific
primary viscerosomatic reflexes( Figure 1).Similarly, headache and neck pain
have been extensively studied withrespect to various somatic dysfunctionsand manual approaches.21,27,28 Forexample, placebo-controlled, diagnosticinvestigations have documented theimportance of cervical pain from dys-function of the zygapophyseal joints inpatients with chronic neck pain andheadache after whiplash injury.29
Functional Demand and SomaticPerpetuating Factors—Functionaldemand plays a precipitating or perpet-uating role (or both) in various persis-tent pain disorders and recurrent somaticdysfunction. Increased functionaldemand on somatic structures underliesrepetitive strain injuries ranging fromcarpal tunnel syndrome in keyboardoperators and poultry-processing knifehandlers30 to those with L5–S1 isthmicspondylolisthesis who must stand for
prolonged periods.10,14 Prolonged func-tional strain can lead to peripheral struc-tural pathologic change coupled with
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic PainS32 • JAOA • Supplement 4 • Vol 105 • No 9 • September 2005
A B C
Figure 2. Sclerotomal pain referral regions from ligaments: (A) iliolumbar ligament, (B) sacrospinous and sacrotuberous ligaments,(C) posterior sacroiliac ligament.

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 5/8
central structural-functional modulationsresulting from persistent pain patterns.Postural strain is among the most fre-quent of functional demand conditionsthat create persistent pain from muscu-loskeletal sources.
Inattention to ergonomics at workor play increases functional demand thatcan perpetuate chronic or recurrent pain.Thus, osteopathic physicians shouldreview patients’ occupational and per-sonal biomechanical stressors as part of
the history. By providing patient educa-tion, they can address persistent painthat derives from prolonged periods of activities such as holding a phone between the ear and shoulder, using akeyboard with improper seating relativeto desk height, or falling asleep slumpedforward in a recliner.
Effective pain management strate-gies aimed at treatment of peripheralpain generators will fail outright or sec-ondary to recurrence of the original
problem in the presence of excessivefunctional demand or other perpetuatingfactors. Unfortunately, prior failure mayeliminate such strategies from theirrightful place in the total treatmentapproach early on or cause the patientor the physician to dismiss them later inthe program when the complicating pos-tural stress or adjacent dysfunctions have been addressed.
Timing, tissue response, and multi-factorial conditions within the body unitaffect OMM treatment strategiesprompted by applying the structure-func-
tion principle. These conditions can bothaffect and be affected by other portions of the proposed algorithm ( Figure 1). Phys-ical examination of patients with persis-tent pain must go beyond identification of peripheral pain generators (especiallyfrom among the most commonly over-looked somatic sources) and screeningfor other perpetuating causes of pain: A
properly constructed OMM approachcannot focus on one principle alone.
Body Unity Considerations:Tangible Impact of Persistent PainWhile acute pain provides essential infor-mation for survival, persistent pain oftenresults in anxiety, depression, and areduction in the quality of life. Such body
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic Pain JAOA • Supplement 4 • Vol 105 • No 9 • September 2005 • S33
A B C D
Figure 3. Myotomal pain referral regionsfrom muscle trigger points: (A) quadratuslumborum, (B) piriformis, (C) iliopsoas, (D)rotatores and multifidi muscles.
Table“Dirty Half-Dozen” Dysfunctions in Persistent Low Back Pain (PLBP)
Somatic Dysfunction (SD) SD in PLBP, %in PLBP (n183)* Key Palpatory Findings†‡
Nonphysiologic pelvic 76 Palpatory “step off” betweenSD (pubic shears) pubic rami at the pubicsymphysis; tenderness
Nonphysiologic pelvic 15 (1) Iliac crest-ASIS-PSIS-ischialSD (sacroiliac shears) tuberosity all elevated on one side;
or (2) dramatically inferior andslightly posterior inferolateral sacralangle on the side of the deepsacral sulcus
Sacral nutation failure 49 Sphinx test; Spring test(including nonneutral and (particularly painful with type II L5 SDbackward sacral torsion SD) rotating in opposite direction from S1)
Pelvic tilt/”Short-leg 63 Post-OMT standing combined withsyndrome”/unlevel sacral base seated flexion tests; standing unlevel
iliac crests and greater trochanters;possible functional scoliosis
Muscle imbalance 90 Asymmetric muscle balance; psoatic(including psoas syndrome) or scoliotic posturing; sharp
tenderness over iliacus or psoas muscles
Type II lumbar SD 85 Typically a single lumbar segmentdemonstrating F R
xS
xor E R
xS
x
* From Greenman PE. Syndromes of the lumbar spine, pelvis, and sacrum. Phys Med Rehabil Clin North Am.1996;7:773–785.
† Note: In PLBP, patients had between three and six of these diagnoses; osteopathic manipulativetreatment corrected 75%.
‡ ASIS indicates anterior superior iliac spine; PSIS, posterior superior iliac spine; OMT, osteopathicmanipulative treatment; F RxSx, E RxSx, where E indicates extension; R, rotation; S, side bending, and x,left or right.

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 6/8
unity (or mind-body-spirit) effects of per-sistent pain are frequently uncoveredwith careful, yet traditional, history andphysical examination skills supple-mented by palpation. Such findings pro-vide diagnostic clues as well as targets of opportunity to reduce precipitating, per-
petuating, and magnifying factors asso-ciated with persistent pain.Discovery of a body unity dysfunc-
tion often shifts the traditional focus fromsimply identifying and removing anunderlying organic disease (pain gener-ator) to consideration of adding strate-gies designed to empower patients withchronic pain to reduce disability throughmodification of environmental and cog-nitive processes. Well-established behav-ioral interventions, including patient edu-
cation, are commonly used in body unityapproaches to chronic disabling pain con-ditions. Body-Mind Unity and PersistentPain—Chronic persistent pain is notsimply acute pain that has lasted a longtime. Positron emission tomography of patients with chronic neuropathic painshows a shift of acute pain activity in thesensory cortex to regions such as the ante-rior cingulate gyrus associated with affec-tive-motivational processing.31 For this
reason, patients with chronic pain oftenattempt to describe their “suffering” andits impact rather than simply providinga location and quality description of their“pain.”
An osteopathic palpatory examina-tion will also aid physicians in eliciting acomplete chronic pain history by gainingthe patient’s trust.2 An integrated historyis essential in determining the impact of pain on physical, mental, emotional, andspiritual functions unique to the indi-
vidual. Understanding physical limita-tions, the most obvious manifestationsof persistent pain, is part of a standardosteopathic medical education. Non-physical limitations in the mental andemotional realms, however, are less oftenarticulated by patients and requiregreater recognition by physicians.
Osteopathic medicine’s considera-tion of mind-body connections in per-sistent pain largely parallels biopsycho-social models embraced by multi-disciplinary pain clinics. In such models,chronic pain is a frequent, well-estab-
lished cause of depression32 with impacton both central and autonomic nervoussystems. Furthermore, it is empiricallyrecognized that physical pain may betemporally linked to anger, fear, orloss.33,34 An example of this link is apatient’s pain traumatically introduced
during an accident in which there wastime to hopelessly anticipate the othercar’s approach. Both fascial dysfunctionand emotions associated with the injuryserve to anchor such pain in thesepatients. Such persons may require addi-tional counseling for the subsequentlyexpressed nonphysical factors.
Conversely, hands-on managementof somatic dysfunction offers a uniqueand often effective access to these body-mind connections. Effects of OMT are
occasionally dramatic, as in the catharsiseffect of certain somatoemotionalreleases. Treatment of somatic dysfunc-tion often offers an opportunity to opendiscussion and seek coping strategies toreduce patients’ mental, spiritual, andemotional pain.
Persistent Pain,Somatic Dysfunction, andHomeostatic ResponsesVarious homeostatic coping and regu-
lating mechanisms influence physiologicprocesses responsible for maintainingpain.35-37 Homeostasis may be alteredthrough focused psychosympathetic, bio-chemical, or neuroendocrine mechanismsaffecting specific structures or targetreceptors, or both. Conversely, an inte-grated series of homeostatic mechanismsmay provide for panstructural biome-chanical changes such as shifting weight- bearing responsibilit ies away frompainful sites. The process creates easily
recognizable patterns associated withcertain pain syndromes.
Because OMT has long been notedto have an independent positive effecton certain autonomic, respiratory, circu-latory, postural, and neuroendocrinemechanisms, it is rational to consider thatinfluencing these mechanisms may pos-itively impact pain modulation, as well( Figure 4). Autonomic System Homeostasis:Pain and Osteopathic ManipulativeMedicine—The importance of sympa-thetic nervous system involvement in
certain forms of neuropathic pain led totaxonomy distinguishing sympatheti-cally maintained pain (SMP) from sym-pathetically independent pain (SIP)38,39:SMP, defined as “pain attributable tosympathetic efferent function in periph-eral tissues,”39 is, by definition, abolished
when the sympathetic supply to thepainful region is modulated. In contrast,SIP is not dependent on sympatheticefferent function and thus not affected by techniques affecting this system.
SMP/SIP taxonomy dissociates thepresence of pain from gross signs of sym-pathetic dysregulation (eg, altered tem-perature, excessive sweating, trophicchanges), so that such obvious evidenceof abnormal sympathetic activity neednot accompany SMP. Thus, while SMP
syndromes such as causalgia and reflexsympathetic dystrophy are often relieved by sympathetic ganglion blocks,40 per-sistent pain with lesser SMP may beaddressed with OMT techniquesdesigned to treat somatic dysfunctionand modulate hypersympatheticactivity.41
Modulation of hypersympathictoniahas been linked to pain reduction,enhanced healing rates, and improve-ment in a variety of visceral and somatic
functions. It is considered to be a hall-mark effect of the OMM approach andwarrants consideration in chronic painconditions. Respiratory-Circulatory HomeostasisRole in Pain—Controlled breathing andpain relief have long been linked. Theancient Chinese prescribed controlled breathing for reducing arthritic pain; layand professional persons have used it toreduce pain of labor and delivery. Even beyond the body-mind effect of focused
respiration as used in meditation andlowering blood pressure, heart rate, andpain perception, the respiratory-circula-tory model popularized by Zink42 is char-acterized by reduction of edema andassociated peripheral biochemicalmolecules linked to nociception.
The treatment goals associated withthe Zink respiratory-circulatory modelare traditionally administered in the fol-lowing sequence. Opening fascial pathways: Somaticdysfunction associated with fascialrestriction to fluid flow is corrected with
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic PainS34 • JAOA • Supplement 4 • Vol 105 • No 9 • September 2005

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 7/8
OMT at the body’s four regional transi-tion zones; Maximizing primary-secondary res-
piration: Effective, deep synchronizedrespiration is sought using a variety of
OMT techniques, including doming of the thoracoabdominopelvic dia-phragms; Augmenting lymphaticovenousdrainage: Homeostatic OMT is applied(often using one or more rhythmic lym-phaticovenous pumps) to effect pressurechanges between the thorax and adja-cent regions. Recent literature suggeststhat such rhythmic motion may also havean effect on release of the homeostaticmolecule, endothelial nitric oxide syn-
thetase27,43; Enhancing cellular level health: Localtissue techniques (such as effleurage) areused to mobilize local edema.
The act of deep breathing createsobvious motion in 136 joints and is pal-pable into all body tissues. It is a contin-uous motion with active and passivecomponents. Through tensegrity rela-tionships, the patient or physician canfocus deep breathing to remove motionrestrictions or engage neuromuscularreflexes to achieve tightening or relax-ation of selected tissues.44
Postural Homeostasis in Pain andDysfunction—Chronic or recurrent painsyndromes have been linked to condi-tions predisposing to postural stress (eg,lower extremity asymmetry, unlevel
sacral base, scoliotic changes, altered lor-dotic-kyphotic curves, unlevel cranial base, postural muscle imbalance). Travelland Simons12 note that postural decom-pensation is the most common precipi-tating and perpetuating cause of MTrPs.These MTrPs are themselves implicatedin many chronic pain syndromes rangingfrom LBP and headaches to carpal tunnelsyndrome, temporomandibular joint dys-function, and pain perceived as angina.13
Pain associated with postural stress
and strain can be sclerotomal (posturalligaments) or myotomal (postural mus-cles). It can also have a significant rolein radiculopathies associated withosteoarthritic and discogenic conditions.45
Irvin46 demonstrated that chronic com-plaints throughout the body could beattributed to an unlevel sacral base andthat reestablishing postural homeostasisremoved most of these symptoms.
The OMM approach to postural careis described thoroughly in Foundations for Osteopathic Medicine and consists of patient education, OMT, exercise, and
sometimes an appropriateorthotic regimen.14(pp603-632)
The Zink respiratory-circula-tory approach42 describedearlier is also applicable in
preparing the tissues for pos-tural homeostasis because of the body unit’s tendency tocompensate for posturalimbalance at the regionaltransition zones.
CommentPersistent nonmalignant pain is not asingle entity. It has many different causesand manifestations, each with varied char-acteristics and names. Osteopathic manip-
ulative medicine employs a history andphysical examination designed to revealany previously unidentified pain gener-ator or underlying cause for persistence of pain. In addition, OMM screens for signsof depression or other significant non-physical links contributing to pain. Basedon the OMM examination, physicians candevelop an individualized osteopathicprescription to address these findings withthe goal of decreasing pain and empow-ering patients to reduce its impact on their
quality of life.In addition to appropriate strategies
to manage the symptom of pain, theOMM algorithm incorporates osteopathicprinciples to identify and address avariety of host factors directed towardthe underlying cause and the tangibleimpact of persistent pain on the patient.These principles provide a frameworkfor patient education to foster compli-ance built on understanding complexinterrelationships.
Each osteopathic prescription seeksto discover and incorporate the factors
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic Pain JAOA • Supplement 4 • Vol 105 • No 9 • September 2005 • S35
Figure 4. Sample osteopathic manipulative treatment (OMT)
protocols for enhancing home-ostatic responses. CV-4 indicatescompression of the fourth ven-tricle; BMT, balanced menbra-nous tension; SBS, sphenobasilar
synchondrosis; IX–X, glossopha-
ryngeal and vagus cranial nerves; OA-AA-C2, occipitoat-lantal, atlantoaxial, and second cervical vertebral units; SI joint,
sacroiliac joint.
Expansion of Biopsychosocial ModelTouch-Stress ReductionBasilar Decompression–CV 4
Sympathetic Model
Respiratory–Circulatory(Venous Lymphatic) Model
Collateral ganglion inhibitionParaspinal inhibition
Thoracolumbar/costal OMTRib raising
Soft tissue OMT
III: Inion BMT; SBSVII: Sphenopalatine
ganglion OMTIX–X: OA-AA-C2,
occipitomastoid
Pelvic Splanchnics: SI joint
Parasympathetic Model
Open fascial pathways attransition zones
Redome thoracoabdominaldiaphragms
Lymphaticovenous pumpsMobilize peripheral edema

8/10/2019 Osteo Chron Schmerz
http://slidepdf.com/reader/full/osteo-chron-schmerz 8/8
needed to address the individual’s uniqueresponse to his or her pain. The emphasisin treating patients with persistent non-malignant pain should be on improvingfunction, decreasing peripheral nocicep-tion and central facilitation, and empow-ering the patient to move forward in
resuming their activities of daily living.Applying osteopathic principles aspart of an effective treatment strategy forpatients with chronic pain results in anindividualized care plan combining non-drug treatment strategies with pharma-cotherapy. Patient education included inthe comprehensive plan helps to improvequality of life and break the vicious cycleseen in the pathophysiology of persis-tent pain.
References1. Elliott AM, Smith BH, Hannaford PC, Smith WC,Chambers WA. The course of chronic pain in thecommunity: results of a 4-year follow-up study.Pain. 2002;Sept;99(1-2):299– 307.
2. Stanton DF, Dutes J-C. Chronic pain and thechronic pain syndrome: the usefulness of manipu-lation and behavioral interventions. Phys Med Rehabil Clin North Am. 1996;7:863–875.3. Turk DC, Rudy TE. Neglected topics in the treat-ment of chronic pain patients—relapse, noncom-pliance, and adherence enhancement. Pain.1991;44:5–28.4. Eisenberg DM, Davis RB, Ettner SL, et al. Trendsin alternative medicine use in the United States,1990–1997: results of a follow-up national survey.
JAMA. 1998;280:1569–1575.5. Oken BS. Complementary and alternativemedicine: overview and definitions. In: Oken BS, ed.Complementary Therapies in Neurology: An Evi-dence-Based Approach. New York, NY: TheParthenon Publishing Group; 2004:1–7.
6. Licciardone JC, Brimhall A, King L. Osteopathicmanipulative treatment for low back pain: a sys-tematic review and meta-analysis of randomizedcontrolled trials. Data reviewed at the OsteopathicResearch Council meeting OCCTIC VI: “Hot Topicsin Osteopathic Manipulative Research.” April 7–8,2005; Fort Worth, Texas.
7. Patterson MM, Steinmetz JE. Long-lasting alter-ations of spinal reflexes: a basis for somatic dys-function. Manual Med . 1986;2:38–42.
8. Mantyh PW, DeMaste E, Malhotra A, Ghilardi JR,Rogers SD, Mantyh CR, et al. Receptor endocytosisand dendrite reshaping in spinal neurons aftersomatosensory stimulation. Science.1995;268:1629–1632.9. Educational Council on Osteopathic Principles.Glossary of osteopathic terminology. In: Ward RC,ed. Foundations for Osteopathic Medicine. 2nded. Baltimore, Md: Lippincott, Williams & Wilkins;2003:1229–1253.10. Kuchera ML. Gravitational stress, musculoliga-mentous strain and postural alignment. In: DormanT, ed. Spine: State of the Art Reviews. Philadel-phia, Pa: Hanley & Belfus; 1995:463–490.11. Kuchera ML, McPartland J. Myofascial trigger
points as somatic dysfunction. In: Ward RC, ed.Foundations for Osteopathic Medicine. 2nd ed.Baltimore, Md: Lippincott, Williams & Wilkins;2003:1034–1050.
12. Travell JG,Simons DG. Myofascial Pain and Dys-function. The Trigger Point Manual . Vol 2. Balti-more, Md: Williams & Wilkins; 1992.
13. Simons DG, Travell JG, Simons LS. Upper Half of the Body. 2nd ed. Baltimore, Md: Lippincott,Williams & Wilkins; 1999. Simons DG, Travell JG,Simons LS, eds. Travell and Simons’ Myofascial Painand Dysfunction: The Trigger Point Manual . Vol 1.
14. Kuchera ML. Postural considerations in coronal,horizontal, and sagittal planes. In: Ward RC, ed.Foundations for Osteopathic Medicine, 2nd ed.Baltimore, Md: Lippincott, Williams & Wilkins;2003:603–632.
15. Mense S, Simons DG. Muscle Pain: Under- standing the Nature, Diagnosis, and Treatment .Philadelphia, Pa: Lippincott, Willliams & Wilkins;2001.
16. Ingber DE, Heidemann SR, Lamoureux P,Buxbaum RE. Opposing views on tensegrity as astructural framework for understanding cellmechanics. J Appl Physiol . 2000;89:1663–1678.
17. Seffinger M, Adams A, Najm W, Dickerson V,Mishra SI, Reinsch S, Murphy L. Spinal palpatorydiagnostic procedures utilized by practitioners ofspinal manipulation: annotated bibliography of
content validity and reliability studies. Journal of theCanadian Chiropractic Association. 2003;47(2):93–109.
18. van Tulder MW; Koes BW; Bouter LM. Con-servative treatment of acute and chronic nonspe-cific low back pain: a systematic review of ran-domized controlled trials of the most commoninterventions. Spine. 1997;22:2128–2156.
19. Giles LGF, Muller R. Chronic spinal pain: A ran-domized clinical trial comparing medication,acupuncture, and spinal manipulation. Spine.2003;28:1490–1502.
20. Assendelft WJJ, Morton SC, Yu EI, Suttorp MJ,Shekelle PG. Spinal manipulative therapy for lowback pain: a meta-analysis of effectiveness rela-
tive to other therapies. Ann Intern Med .2003;138:871–881.
21. Bronfort G, Haas M, Evans R, Bouter LM. Effi-cacy of spinal manipulation and mobilization forlow back pain and neck pain: a systematic reviewand best evidence synthesis. Spine J . 2004;4:335–356.
22. Ongley MJ, Klein RG, Dorman TA, Eek BC,Hubert LJ. A new approach to the treatment ofchronic low back pain. Lancet . 1987;2:143–146.
23. Mein EA. Low back pain and manual medicine:a look at the literature. In: Stanton DF, Wein EA,eds. Phys Med Rehabil Clin North Am. 1996;7:715-727.
24. Greenman PE. Syndromes of the lumbar spine,
pelvis, and sacrum. Phys Med Rehabil Clin North Am. 1996;7:773–785.
25. Kuchera WA, Kuchera ML. Osteopathic Princi- ples in Practice. 2nd ed re-revised. Columbus, Ohio:Greyden Press; 1994.
26. Blomberg S. A Pragmatic Approach to Low-Back Pain Including Manual Therapy and Steroid Injections: A Multicentre Study in Primary HealthCare [dissertation]. Uppsala, Sweden: Faculty ofMedicine, Acta Universitatis Upsaliensis; 1993.
27. Kuchera ML. Osteopathic considerations inneurology. In: Oken BS, ed. Complementary Ther-apies in Neurology: An Evidence-Based Approach.New York, NY: Parthenon Publishing Group;2000;51–93.
28. Kuchera ML. Osteopathic principles and prac-tice/osteopathic manipulative treatment consider-ations for cephalgia. J Am Osteopath Assoc .1998;98(suppl):S14–S19.
29. Lord SM, Barnsley L, Wallis BJ, Bogduk N.Chronic cervical zygapophyseal joint pain afterwhiplash: a placebo controlled prevalence study.Spine. 1996;21:1737–1744.
30. Fagarasanu M, Kumar S. Work-related carpaltunnel syndrome: current concepts. Journal of Mus-culoskeletal Research. 2003;7(2):87–96.
31.Hsieh JC, Belfrage M, Stone-Elander S, HanssonP, Ingvar M. Central representation of chronicongoing neuropathic pain studied by positronemission tomography. Pain. 1995;63:225–236.
32. Magni G, Marchetti M, Moreschi C, Merskey H,Luchini SR. Chronic musculoskeletal pain anddepressive symptoms in the National Health andNutrition Examination. I. Epidemiologic follow-upstudy. Pain. 1993;53:163–168.
33. Sullivan M, Thorn B, Haythornthwaite J, KeefeF, Martin M, Bradley L, et al. Theoretical perspec-tives on the relation between catastrophizing andpain. Clin J Pain. 2001;17(1):52–64.
34. Hamilton NA, Karoly P, Kitzman H. Self-regu-lation and chronic pain: the role of emotion. Cog-nitive Therapy Research. 2004;28(5):559–576.
35. Sterling P, Eyer J. Allostasis: a new paradigm to
explain arousal pathology. In: Fisher S, Reason J, eds.Handbook of Life Stress, Cognition and Health.New York, NY: John Wiley & Sons; 1988:629–649.
36. Seeman, TE, Singer BH, Rowe JW, Horwitz RI,McEwen BS. Price of adaptation—allostatic loadand its health consequences: McArthur studies ofsuccessful aging. J Cl in Endocrinol Metab.1997;157:2259–2268.
37. McEwen BS. Protective and damaging effectsof stress mediators. N Engl J Med . 1998;338:178–179.
38. Roberts WJ. A hypothesis on the physiologicalbasis for causalgia and related pain. Pain.1986;24:297–311.
39. Campbell JN, Raja SN, Selig DK, Belzberg AJ,
Meyer RA. Diagnosis and management of sympa-thetically maintained pain. In: Fields HL, LiebeskindJC, eds. Progress in Pain Research and Manage-ment . Vol 1. Seattle, Wash: IASP Press;1994:85–100.
40. Bonica JJ, Causalgia and other reflex sympa-thetic dystrophies. In: Bonica JJ, Liebeskind JC,Albe-Fessard D, eds. Advances in Pain Researchand Therapy . Vol 3. New York, NY: Raven Press;1979:141–166.
41. Van Buskirk RL. Nociceptive reflexes and thesomatic dysfunction: a model. J Am Osteopath
Assoc . 1990;90:792–794, 797–809.
42. Zink JG, Lawson WB. An osteopathic structuralexamination and functional interpretation of thesoma. Osteopathic Annals. 1979;7:12–19.
43. Salamon E, Zhu W, Stefano G. Nitric oxide as apossible mechanism for understanding the thera-peutic effects of osteopathic manipulativemedicine. Int J Mol Med . 2004;14:443–449.
44. Lewit K. Manipulative Therapy in Rehabilita-tion of the Motor System. London, England: But-terworths; 1985:35–38.
45. Kuchera ML. Treatment of gravitational strainpathophysiology. In: Vleeming A. Mooney V, Sni- jders C, Stoeckert R, eds. Movement, Stability and Low Back Pain: The Essential Role of the Pelvis.New York, NY: Churchill Livingstone; 1997:477–499.
46. Irvin RE. Suboptimal posture: the origin of themajority of idiopathic pain of the musculoskeletalsystem. In: Vleeming A. Mooney V, Snijders C,
Stoeckert R, eds. Movement, Stability and Low Back Pain: The Essential Role of the Pelvis. NewYork, NY: Churchill Livingstone; 1997:133–155.
Kuchera • Osteopathic Manipulative Medicine Considerations in Chronic PainS36 • JAOA • Supplement 4 • Vol 105 • No 9 • September 2005