
Phenotypic and Genotypic Analysis of Multidrug-Resistant...
7
Research Article Phenotypic and Genotypic Analysis of Multidrug-Resistant Mycobacterium tuberculosis Isolates from Sudanese Patients Solima M. A. Sabeel, 1,2 Mohamed Ahmed Salih, 3 Manasik Ali, 4 Salah-Eldin EL-Zaki, 5 Nadir Abuzeid, 6 Zeinab Abubaker Mohammed Elgadi, 7 Hisham N. Altayb, 8 Asrar M. A. Elegail, 9 Nuha Y. Ibrahim, 9 and Bahaeldin K. Elamin 1,10 1 Department of Microbiology, Faculty of Medical Laboratory Sciences, University of Khartoum, Khartoum, Sudan 2 Microbiology Department, Faculty of Medical Laboratory Sciences, Ibn Sina University, Khartoum, Sudan 3 Department of Bioinformatics, Africa City of Technology, Khartoum, Sudan 4 Sudan Academy of Sciences, Khartoum, Sudan 5 Department of Epidemiology, Tropical Medicine Research Institute, National Center for Research, Khartoum, Sudan 6 Department of Microbiology, Faculty of Medical Laboratory Sciences, Omdurman Islamic University, Khartoum, Sudan 7 Veterinary Research Institute, Khartoum, Sudan 8 Microbiology Department, College of Medical Laboratory Sciences, Sudan University of Science and Technology, Khartoum, Sudan 9 National Reference Laboratory-Tuberculosis (NRL-TB), National Public Health Laboratory, Khartoum, Sudan 10 Department of Microbiology and Parasitology, College of Medicine, University of Bisha, Bisha, Saudi Arabia Correspondence should be addressed to Solima M. A. Sabeel; [email protected] Received 22 July 2016; Revised 7 November 2016; Accepted 22 December 2016; Published 18 January 2017 Academic Editor: Vincent Jarlier Copyright © 2017 Solima M. A. Sabeel et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Currently, mutations in rpoB, KatG, and rrs genes and inhA promoter were considered to be involved in conferring resistance to rifampicin, isoniazid, and streptomycin in Mycobacterium tuberculosis (MTB). Objective. e aims of this study were to detect the prevalence of first-line tuberculosis (TB) drug resistance among a group of previously treated and newly detected TB patients, to determine the association between prevalence of multidrug resistance (MDR) and demographic information (age and sex), to explain genes correlated with MDR Mycobacterium tuberculosis, and to characterize MTB via 16S ribosomal RNA (16S rRNA) analysis. Methods. A hundred MTB isolates from Sudanese pulmonary TB patients were included in the study. e proportional method of drug susceptibility test was carried out on L¨ owenstein-Jensen media. Multiplex PCR of rpoB and KatG genes and inhA promoter was conducted; then rrs genes were amplified by conventional PCR and were sequenced. e sequences of the PCR product were compared with known rrs gene sequences in the GenBank database by multiple sequence alignment tools. Result. e prevalence of MDR was 14.7% among old cases and 5.3% among newly diagnosed cases. Conclusion. Mutations in rrs could be considered as a diagnostic marker. 1. Introduction Monitoring of tuberculosis (TB) caused by drug-resistant Mycobacterium tuberculosis (MTB) has become one of the major problems throughout the world [1]. However, the detection of drug-resistant phenotypes of MTB takes at least 3–6 weeks by direct and indirect methods, respectively. us, treatment was prescribed empirically. Patients who fail to respond to drugs remain infectious [2]. ey may be a source of transmission of infections [3]. Sudan is surrounded by high burden countries [4] and it harbors a high TB incidence among the East Mediterranean countries. e prevalence of TB infection in Sudan is prob- ably variable in different regions [5]. e country has been severely affected by war, famine, and flood in recent decades and has a large population of internally displaced persons, Hindawi Tuberculosis Research and Treatment Volume 2017, Article ID 8340746, 6 pages https://doi.org/10.1155/2017/8340746
Transcript of Phenotypic and Genotypic Analysis of Multidrug-Resistant...

Research ArticlePhenotypic and Genotypic Analysis of Multidrug-ResistantMycobacterium tuberculosis Isolates from Sudanese Patients
Solima M A Sabeel12 Mohamed Ahmed Salih3 Manasik Ali4 Salah-Eldin EL-Zaki5
Nadir Abuzeid6 Zeinab Abubaker Mohammed Elgadi7 Hisham N Altayb8
Asrar M A Elegail9 Nuha Y Ibrahim9 and Bahaeldin K Elamin110
1 Department of Microbiology Faculty of Medical Laboratory Sciences University of Khartoum Khartoum Sudan2 Microbiology Department Faculty of Medical Laboratory Sciences Ibn Sina University Khartoum Sudan3 Department of Bioinformatics Africa City of Technology Khartoum Sudan4 Sudan Academy of Sciences Khartoum Sudan5 Department of Epidemiology Tropical Medicine Research Institute National Center for Research Khartoum Sudan6 Department of Microbiology Faculty of Medical Laboratory Sciences Omdurman Islamic University Khartoum Sudan7 Veterinary Research Institute Khartoum Sudan8 Microbiology Department College of Medical Laboratory Sciences Sudan University of Science and Technology Khartoum Sudan9 National Reference Laboratory-Tuberculosis (NRL-TB) National Public Health Laboratory Khartoum Sudan10Department of Microbiology and Parasitology College of Medicine University of Bisha Bisha Saudi Arabia
Correspondence should be addressed to Solima M A Sabeel solima89gmailcom
Received 22 July 2016 Revised 7 November 2016 Accepted 22 December 2016 Published 18 January 2017
Academic Editor Vincent Jarlier
Copyright copy 2017 Solima M A Sabeel et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Background Currently mutations in rpoB KatG and rrs genes and inhA promoter were considered to be involved in conferringresistance to rifampicin isoniazid and streptomycin inMycobacterium tuberculosis (MTB) ObjectiveThe aims of this study wereto detect the prevalence of first-line tuberculosis (TB) drug resistance among a group of previously treated and newly detectedTB patients to determine the association between prevalence of multidrug resistance (MDR) and demographic information (ageand sex) to explain genes correlated with MDR Mycobacterium tuberculosis and to characterize MTB via 16S ribosomal RNA(16S rRNA) analysis Methods A hundred MTB isolates from Sudanese pulmonary TB patients were included in the study Theproportional method of drug susceptibility test was carried out on Lowenstein-Jensen media Multiplex PCR of rpoB and KatGgenes and inhA promoter was conducted then rrs genes were amplified by conventional PCR and were sequenced The sequencesof the PCR product were compared with known rrs gene sequences in the GenBank database bymultiple sequence alignment toolsResult The prevalence of MDR was 147 among old cases and 53 among newly diagnosed cases Conclusion Mutations in rrscould be considered as a diagnostic marker
1 Introduction
Monitoring of tuberculosis (TB) caused by drug-resistantMycobacterium tuberculosis (MTB) has become one of themajor problems throughout the world [1] However thedetection of drug-resistant phenotypes of MTB takes at least3ndash6 weeks by direct and indirect methods respectivelyThustreatment was prescribed empirically Patients who fail to
respond to drugs remain infectious [2]Theymay be a sourceof transmission of infections [3]
Sudan is surrounded by high burden countries [4] and itharbors a high TB incidence among the East Mediterraneancountries The prevalence of TB infection in Sudan is prob-ably variable in different regions [5] The country has beenseverely affected by war famine and flood in recent decadesand has a large population of internally displaced persons
HindawiTuberculosis Research and TreatmentVolume 2017 Article ID 8340746 6 pageshttpsdoiorg10115520178340746
2 Tuberculosis Research and Treatment
which is considered risk factor of spreading TB Cases amongmen exceeded those found in women by a ratio of 2 1 [6]
Multidrug-resistant TB (MDR-TB) is defined as MTBthat is resistant to first-line anti-TB drugs such as rifampicin(RIF) and isoniazid (INH) [7] RIF is a broad spectrumantimicrobial agent which remains the most effective drugagainst M tuberculosis Resistance of rifampicin occurs viamutation in rpoB gene that encodes the 120573-subunit of RNApolymerase [8] INH has the most powerful bactericidalactivity against TB and has good tolerance and low price [7]It is a prodrug requiring activation through oxidation by amycobacterial catalase-peroxidase enzyme encoded by katGgene [9] Activated isoniazid interferes with the biosynthesisof essential mycolic acids through inhibition of nicotinamideadenine dinucleotide hydrogen (NADH) dependent enoyl-acyl carrier protein reductase which is encoded by inhApromoter Alterations in katG gene and inhA promoterwere strongly associated with isoniazid resistance [10 11]Streptomycin (SM) was the foremost antibiotic successfullyused against TB Resistance to SM emerged as a result ofmonotherapy administration [12] SM is an aminocyclitol gly-coside that acts against actively growing bacilli by inhibitingthe initiation of translation in protein synthesis at the level ofthe 30S subunit of the ribosome specifically at the ribosomalprotein S12 and the 16S rRNA coded by rpsL and rrs genesrespectively [13 14] Consequently mutations in rpsL and rrsare the major mechanisms of resistance [10] The aims of thecurrent studywere to detect the prevalence ofmonoresistanceand multidrug-resistantMycobacterium tuberculosis (MDR)to determine the association between prevalence of MDRand demographic information (age and sex) to explain themolecular characterization of M tuberculosis through 16SrRNA and to illustrate the frequency of rrsmutations amongstreptomycin-resistantM tuberculosis isolates
2 Materials and Methods
This study was approved by the Ethics Committee of theAfrica City of Technology and the University of KhartoumSudan
21 Mycobacterium tuberculosis Growth Properties A hun-dred sputum samples were collected from pulmonary TBpatients as a cross-sectional descriptive study conducted atthe National Reference Laboratory-Tuberculosis (NRL-TB)Khartoum Sudan Samples were processed under biosafetycabinet level II via adding twice the volume of 4 NaOHto sputum in 50mL centrifuge tube for decontaminationand homogenization Samples were neutralized by bufferfollowed by centrifugation at 3000 RCF (Relative CentrifugeForce) for 20min Inoculation was adjusted by pipetting 3ndash5 drops of deposit in three Lowenstein-Jensen media (twocontaining glycerol and one containing pyruvate) which areegg based media Then cultured media were incubated at37∘C in slant position Subsequently weekly observation wasmade to check the growth of bacteria [15ndash17]
22 Drugs Susceptibility Test Drugs susceptibility test wasdone through the conventional proportional method on
Lowenstein-Jensen (LJ) media containing drugs according toCDC standard procedures [16 18] The grown colonies werepicked up from the media and emulsified in a thick wall glasstube containing DW+ glass beads by shaking the tubes wellfurthermore turbiditywas adjustedwithMcFarland standard(number 05)The diluted suspension 10minus4 was cultured on LJdrug-free media as a control and drug containing 02 120583gmLisoniazid (INH) 400 120583gmL rifampicin (RIF) 40120583gmLstreptomycin (SM) and 20 120583gmL ethambutol (EMB) Thecultured media were incubated at 37∘C and were observedafter 4 weeks If there are no colonies or if the ratio betweenthe number of colonies in the media containing drug andthe number of colonies in drug-free media is less than 1it will be considered sensitive while if the ratio between thenumber of colonies in media including drug and the numberof colonies in drug-free media is more than 1 it will beinterpreted as resistant to all four drugs Species identificationof Mycobacterium was carried out via testing the ability togrow on p-nitrobenzoic acid (PNB) All isolates were testedtwice in media to confirm the accuracy of the results [19 20]
23 Guanidine ChlorideDNAExtractionMethod All scrapedcolonies were washed with phosphate buffer saline (PBS)followed by the addition of 2mL lysis buffer 5 120583L proteinaseK 1mL guanidine chloride and 300 120583L ammonium acetateSuspensions were incubated overnight at 37∘C on the nextday 2mL of chilled chloroform was added After centrifuga-tion the clear upper layer was collected in a new tube andcold absolute ethanol was added to enhance precipitationof DNA The pellet was washed with 70 ethanol and thendecanted by 70 ethanol and allowed to dry The pelletwas then resuspended with nuclease-free water and qualifiedusing NanoDrop ND-1000 spectrophotometer (NanoDropTechnologies USA) The DNA samples were stored at minus20∘Cuntil used for conventional PCR [21 22]
24 GenoLyse Extraction Method DNA extraction was per-formed as recommended by the manufacturer (Hain Life-science) Firstly collected bacterial colonies were heated for20 minutes at 100∘C in a water bath and then suspended in100 120583L of kit lysis buffer followed by incubation at 95∘C for5min finally 100 120583L of neutralization buffer was added Themixture was spun at full speed in a tabletop centrifuge withan aerosol tight rotor and then stored at minus20∘C and then usedfor multiplex PCR in Line Probe Assay [23]
25 Conventional PCR Fifteen genomic DNA were used astemplates for PCR amplification of complete rrs gene (16SrRNA) The two primers used were forward primer namely27F (51015840-AGAGTTTGATCCTGGCTCAG-31015840) and reverseprimer namely 1495R (51015840-CTACGGCTACCTTGTTACGA-31015840) The 25 120583L reaction mixture contained 1 120583L DNA 1xreaction buffer (10x) with 3mM MgCl
2 25 U i-Taq DNA
polymerase (5U120583L) 25mM dNTPs 1 120583L of 10 pmol of eachprimer and 1x of gel loading buffer followed by completingthe volume to 25120583L by DW PCR amplifying procedure wasas follows 5min at 94∘C 30 cycles of 1min at 94∘C 1minat 58∘C 2min at 72∘C and then 10min at 72∘C which
Tuberculosis Research and Treatment 3
was performed on a Bio-Rad (DNA engineDyad Peltier)automatic thermal cycler Duplicate PCR of every samplewere carried out for more confirmation The products ofamplificationwere checked through running on 06 agarosegel electrophoresis [24 25]
26 Multiplex PCR Hybridization and detection were per-formed using the hybridization kits Seventy-five isolatedDNA were used by taking 5 120583L of each DNA and mixingit with 10 120583L Amplification Mix A and 35 120583L AmplificationMix B containing biotinylated primers The PCR amplifyingprocedure was as follows 15min at 95∘C 10 cycles of 30seconds at 95∘C 20 cycles of 40 seconds at 50∘C and 8minat 70∘C which was performed on a Hain Lifescience thermalcycler The amplification product was visualized throughreverse hybridization probes complementary to amplifiednucleic acids on membrane strips [26]
27 Sequencing of 16S rRNA Isolates were packaged accord-ing to the International Air Transport Association guidelinesand shipped with authorized permission to Macrogen Com-pany (Seoul SouthKorea) Purification and standard forwardsequencing of 16S rRNA were done by ABI Genetic Analyser(Applied Biosystems)
28 Statistical and Bioinformatic Analysis The result wasanalysed statistically using IBM SPSS Statistics version 21(Statistical Package for the Social Sciences) which is asoftware package for statistical analysis the chi-square testwas used to check the statistical significance [27] Thechromatogram sequences were visualized through FinchTV program version 140 [28] The nucleotides sequencesof the rrs gene were searched for sequences similarityusing nucleotide BLAST [29] Highly similar sequenceshave accession numbers HM007576 KF796661 JX303293and GU142936 and sequences of the reference M tuber-culosis H37Rv strain [X555881] were retrieved from NCBI(httpswwwncbinlmnihgov) and subjected to multi-ple sequence alignment using BioEdit software version725 [30] Newick format was withdrawn from ClustalW(httpwwwebiacukToolsmsaclustalw2) [31] to create aphylogenetic tree in Phylogenyfr software [32]
29 Nucleotide Sequence Accession Numbers The nucleotidesequences of the rrs genes containing novel mutations weredeposited in the GenBank database (National Center forBiotechnology Information httpswwwncbinlmnihgov)under the following accession numbers KU372152KU372153 KU372154 KU372155 KU372156 and KU372157
3 Results
Among 100 sputum samples twenty of them revealed nogrowth two were contaminated one was lysed and twohad grown in PNB indicating Mycobacterium other thantuberculosis (MOTT) The growth rate on LJ media is asfollows 39 (2975) showed +3 (200ndash500 colonies) 33(2575) showed +2 (100ndash200 colonies) 267 (2075) showed+1 (10ndash99 colonies) and 13 (175) showed 4 colonies
Table 1 Percentage of MDR in different age groups
Age group MDR Account (number)le30 60 931ndash40 133 241ndash50 133 251ndash60 133 2gt60 0 0
Most of the MDR growth appeared as +1 and probably hadgrown at 2ndash4 weeks (119875 value 0426) showing a statisticallyinsignificant association between growth rate and MDRTheprevalence of MDR was 20 (1575) and 147 (1115) amongpreviously treated and old cases and 53 (415) amongnewly diagnosed cases (119875 value 0003) which means drugresistance was associated with previous treatment 733 ofMDR cases were males while 267 were females (119875 value0536) Sixty percent (915) of MDR cases were found inthe age group le 30 years (119875 value 0652) (Table 1) Amongseventy-fiveMycobacterium tuberculosis isolates 56 (4275)were streptomycin-resistant 29 (2275) were rifampicin-resistant 20 (1575) were ethambutol-resistant and 28(2175) were isoniazid-resistant 20 (1575) were resistant toRIF and INH 16 (1275) were resistant to all four drugsThe run progression of the final separation of PCR productswas visualized under UV transilluminator documentationmachine Most of them fluoresced sharply but two of themfluoresced faintly and were excluded The most commonmutation detected by LPA in the rpoB gene was S531L (801215) followed by H526D in KatG gene the most commonmutation was S315T (67 1015) and in InhA promoter it wasC15T (333 721)
Sixty-two percent (813 isolates) of streptomycin-resistantisolates revealed mutations in rrs gene which were identifiedin seven groups four isolates (31) have G rarr A transitionat nucleoside position 892 three isolates (23) have Crarr Atransversion at nucleoside position 222 two isolates (15)have ArarrG transition at nucleoside position 904 one isolate(8) has Grarr T transversion at nucleoside position 855 oneisolate (8) has ArarrG transition at nucleoside position 906one isolate (8) has Trarr A transversion at nucleoside posi-tion 1238 and two isolates have Grarr AGrarr C at nucleosideposition 1400 which are more explained in Table 2
31 Phylogenetic Tree A phylogenetic tree represents therelationships among a set of Mycobacterium tuberculosisThe tree is classified into two branches All isolates have acommon ancestor except for isolate-9 which was outgroupIsolate-2 and isolate-4 were sister groups as shown in Figure 1
4 Discussions
The study found novel transversion mutation of C rarr Aat position 222 To our knowledge the present study isthe first study that demonstrated 16S rRNA analysis amongmultidrug-resistantM tuberculosis isolates from Sudan andthus the prevalence ofMDRwas 20 (1575) and 147 (1115)among old cases and 53 (415) among newly diagnosed
4 Tuberculosis Research and Treatment
Table 2 Explaining the position and frequency of polymorphism with resistance pattern of isolates
Mutation position Polymorphism Frequency () Resistance patternRIF INH STM EMB
222 Crarr A 23R R R SS S R SR S R S
885 Grarr T 8 S S R S
892 Grarr A 31
S R R SS S R SR R R SR R R R
904 Ararr G 15 S R R SR R R R
906 Ararr G 8 S R R STrarr A 8 R S R S
1400 Grarr A 8 R R R RGrarr C 8 S S R S
R resistance S sensitive RIF rifampicin INH isoniazid STM streptomycin EMB ethambutol
Iso_11Iso_10Iso5_1rstIsolate 2Isolate 4Iso_6Isolate 3H37RvUSA_CtrlPoland_CtrlIran_CtrlGermany_CtrlIso_9
Iso_11Iso_10
Iso5_1rst
Isolate 2
Isolate 4
Iso_6Iso_7
Isolate 3
H37Rv
USA_CtrlPoland_Ctrl
Iran_Ctrl
Germany_Ctrl
Iso_9
CGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGG
GGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGG
GCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGAGGTGTGGGGAGGTGTGGGGAGGTGTGGG
ATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCC
TGTTGGTGGGGTGACGGCCTACCAAGGCGACGACGGGTAGCCGGCCTGAGAGG
(a)
(c)(d)
(b)
Figure 1 (a) Gel electrophoresis of PCR product Lanes 1 and 5 DNA marker 1000+ Lanes 2 3 and 4 amplified DNA products 1500 bp(b) Chromatogram sequence of 16S rRNA visualized via Finch TV software (c) Alignment determining novel mutation at position 222transversion of C to A in isolates 9 10 and 11 via BioEdit software (d) Phylogenetic tree using Phylogenyfr software
cases which was lower than Francersquos study with a prevalenceof 23323 (71) in newly diagnosed patients and 33105(314) in re-treated patients [33] this difference could bedue to the geographical variation In the present study733 of MDR cases were males while 267 were femaleswhich agreed with Raizada et alrsquos study where MDR-TB waspredominant inmales (72 230320) [34] contrary toMelzer
et alrsquos study where 567 in males and 433 in females [35]may be due to the large numbers of males when comparedwith females included in this study Most MDR cases werefound in the age group le 30 years (60) correspondingwith Melzer et alrsquos study [35] The genotype MTBDRplustest identifiedmost frequent mutations involved in resistanceto RIF and INH as follows in rpoB gene S531L was 54
Tuberculosis Research and Treatment 5
(1222) this is similar to the findings of Barnard et al [36]The final result of mutation frequency in rrs gene is 62which is approximately similar to Ashorsquos study conductedin Pakistan that detected 3550 (70) strains [37] Alsoadditional studies in China Japan and Latvia have reportedthe highest frequencies 857 778 and 85 respectively[38ndash40] whereas in North India no mutation had beendetected in streptomycin-resistant isolates [41] Regardingmutation in the 912 region 23 of the isolates have beenrevealed A rarr G transition at position 904 corresponds tostudies in Germany [42] On the other hand a study inBarcelona did not detect mutation in the rrs912 region [43]The mutation at loop 530 of the rrs coding region had notbeen identified which agreed with New Yorkrsquos study [44] andconflicted with Polandrsquos study [45] Novel mutation could beused as a diagnostic marker that represents a tool for rapidmonitoring of streptomycin resistance and could be of valueto the clinician
Small sample size was one of the drawbacks that limitedour study therefore a large sample size in further studiescould be useful for the determination of other biomarkersthat assist the diagnosis of streptomycin-resistant MTB
5 Conclusion
Analysis of 16S rRNA sequences is considered the goldenstandard method for the identification and assessment ofphylogenetic relationships among bacterial isolates
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to Africa City of TechnologyNational Public Health Laboratory Molecular TuberculosisLaboratory and all members of the National ReferenceLaboratory of Tuberculosis (NRL-TB) Sudan Khartoum
References
[1] World Health Organization Global Tuberculosis Report 2015chapter 4 WHOHTMTB201522 Geneva Switzerland 20thedition 2015
[2] D A Mitchison and A J Nunn ldquoInfluence of initial drugresistance on the response to short-course chemotherapy of pul-monary tuberculosisrdquo American Review of Respiratory Diseasevol 133 no 3 pp 423ndash430 1986
[3] A L Kritski M J Ozorio Marques M F Rabahi et al ldquoTrans-mission of tuberculosis to close contacts of patients withmultidrug-resistant tuberculosisrdquo American Journal of Respira-tory and Critical CareMedicine vol 153 no 1 pp 331ndash335 1996
[4] WHO Global Tuberculosis Control 2014 WHO GenevaSwitzerland 2014 httpwwwwhointtbpublicationsglobalreport
[5] World Health OrganizationIUATLD ldquoGlobal project on anti-tuberculosis drug resistance surveillancerdquo Report 3 WorldHealth OrganizationIUATLD Geneva Switzerland 2003
[6] A S Rhines ldquoThe role of sex differences in the prevalence andtransmission of tuberculosisrdquo Tuberculosis vol 93 no 1 pp104ndash107 2013
[7] J A Caminero Ed Guidelines for Clinical and Opera-tional Management of Drug-Resistant Tuberculosis Interna-tional Union Against Tuberculosis and Lung Disease ParisFrance 2013
[8] A Somoskovi L M Parsons and M Salfinger ldquoThe molecularbasis of resistance to isoniazid rifampin and pyrazinamide inMycobacterium tuberculosisrdquo Respiratory Research vol 2 no 3pp 164ndash168 2001
[9] Y Zhang B Heym B Allen D Young and S Cole ldquoThecatalasemdashperoxidase gene and isoniazid resistance ofMycobac-terium tuberculosisrdquoNature vol 358 no 6387 pp 591ndash593 1992
[10] S H Gillespie ldquoEvolution of drug resistance inMycobacteriumtuberculosis clinical and molecular perspectiverdquo AntimicrobialAgents and Chemotherapy vol 46 no 2 pp 267ndash274 2002
[11] B Heym Y Zhang S Poulet D Young and S T Cole ldquoChar-acterization of the katG gene encoding a catalase-peroxidaserequired for the isoniazid susceptibility of Mycobacteriumtuberculosisrdquo Journal of Bacteriology vol 175 no 13 pp 4255ndash4259 1993
[12] J Crofton and D A Mitchison ldquoStreptomycin resistance inpulmonary tuberculosisrdquo British Medical Journal vol 2 pp1009ndash1015 1948
[13] D Moazed and H F Noller ldquoInteraction of antibiotics withfunctional sites in 16S ribosomalRNArdquoNature vol 327 no 6121pp 389ndash394 1987
[14] M Finken P Kirschner A Meier A Wrede and E C BottgerldquoMolecular basis of streptomycin resistance in Mycobacteriumtuberculosis alterations of the ribosomal protein S12 geneand point mutations within a functional 16S ribosomal RNApseudoknotrdquo Molecular Microbiology vol 9 no 6 pp 1239ndash1246 1993
[15] WHO Laboratory Services in Tuberculosis Control Part II andIII Microscopy and Culture WHO 1998
[16] P T Kent and G P Kubica Public Health MycobacteriologyGuides For Level III Laboratory US Department of Health andHuman Services Public Health Service CDC 1985
[17] S-J Kim G-H Bai and H-D Hwang ldquoEfficiency of the directand concentrationmethods in demonstrating tubercle bacilli inthe sputum specimensrdquo Tuberculosis and Respiratory Diseasesvol 36 no 4 pp 354ndash361 1989
[18] V Vincent and M C Gutierrez ldquoMycobacterium laboratorycharacteristics of slowly growing mycobacteriardquo in Manualof Clinical Microbiology pp 573ndash588 American Society forMicrobiology Washington DC USA 2007
[19] C Collins J Grange andM YatesOrganization and Practice inTuberculosis Bacteriology Butterworth London UK 1985
[20] G CanettiW Fox A Khomenko et al ldquoAdvances in techniquesof testing mycobacterial drug sensitivity and the use of sensi-tivity tests in tuberculosis control programmesrdquo Bulletin of theWorld Health Organization vol 41 no 1 pp 21ndash43 1969
[21] DNA Extraction Guanidine Method Modified from Black wellLab Cambridge UK
[22] S A Miller D D Dykes and H F Polesky ldquoA simple saltingout procedure for extracting DNA from human nucleated cellsrdquoNucleic Acids Research vol 16 no 3 p 1215 1988
[23] Hain Life Science Hardwiesenstraszlige Nehren Germanyhttpwwwhain-lifesciencede
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Tuberculosis Research and Treatment
which is considered risk factor of spreading TB Cases amongmen exceeded those found in women by a ratio of 2 1 [6]
Multidrug-resistant TB (MDR-TB) is defined as MTBthat is resistant to first-line anti-TB drugs such as rifampicin(RIF) and isoniazid (INH) [7] RIF is a broad spectrumantimicrobial agent which remains the most effective drugagainst M tuberculosis Resistance of rifampicin occurs viamutation in rpoB gene that encodes the 120573-subunit of RNApolymerase [8] INH has the most powerful bactericidalactivity against TB and has good tolerance and low price [7]It is a prodrug requiring activation through oxidation by amycobacterial catalase-peroxidase enzyme encoded by katGgene [9] Activated isoniazid interferes with the biosynthesisof essential mycolic acids through inhibition of nicotinamideadenine dinucleotide hydrogen (NADH) dependent enoyl-acyl carrier protein reductase which is encoded by inhApromoter Alterations in katG gene and inhA promoterwere strongly associated with isoniazid resistance [10 11]Streptomycin (SM) was the foremost antibiotic successfullyused against TB Resistance to SM emerged as a result ofmonotherapy administration [12] SM is an aminocyclitol gly-coside that acts against actively growing bacilli by inhibitingthe initiation of translation in protein synthesis at the level ofthe 30S subunit of the ribosome specifically at the ribosomalprotein S12 and the 16S rRNA coded by rpsL and rrs genesrespectively [13 14] Consequently mutations in rpsL and rrsare the major mechanisms of resistance [10] The aims of thecurrent studywere to detect the prevalence ofmonoresistanceand multidrug-resistantMycobacterium tuberculosis (MDR)to determine the association between prevalence of MDRand demographic information (age and sex) to explain themolecular characterization of M tuberculosis through 16SrRNA and to illustrate the frequency of rrsmutations amongstreptomycin-resistantM tuberculosis isolates
2 Materials and Methods
This study was approved by the Ethics Committee of theAfrica City of Technology and the University of KhartoumSudan
21 Mycobacterium tuberculosis Growth Properties A hun-dred sputum samples were collected from pulmonary TBpatients as a cross-sectional descriptive study conducted atthe National Reference Laboratory-Tuberculosis (NRL-TB)Khartoum Sudan Samples were processed under biosafetycabinet level II via adding twice the volume of 4 NaOHto sputum in 50mL centrifuge tube for decontaminationand homogenization Samples were neutralized by bufferfollowed by centrifugation at 3000 RCF (Relative CentrifugeForce) for 20min Inoculation was adjusted by pipetting 3ndash5 drops of deposit in three Lowenstein-Jensen media (twocontaining glycerol and one containing pyruvate) which areegg based media Then cultured media were incubated at37∘C in slant position Subsequently weekly observation wasmade to check the growth of bacteria [15ndash17]
22 Drugs Susceptibility Test Drugs susceptibility test wasdone through the conventional proportional method on
Lowenstein-Jensen (LJ) media containing drugs according toCDC standard procedures [16 18] The grown colonies werepicked up from the media and emulsified in a thick wall glasstube containing DW+ glass beads by shaking the tubes wellfurthermore turbiditywas adjustedwithMcFarland standard(number 05)The diluted suspension 10minus4 was cultured on LJdrug-free media as a control and drug containing 02 120583gmLisoniazid (INH) 400 120583gmL rifampicin (RIF) 40120583gmLstreptomycin (SM) and 20 120583gmL ethambutol (EMB) Thecultured media were incubated at 37∘C and were observedafter 4 weeks If there are no colonies or if the ratio betweenthe number of colonies in the media containing drug andthe number of colonies in drug-free media is less than 1it will be considered sensitive while if the ratio between thenumber of colonies in media including drug and the numberof colonies in drug-free media is more than 1 it will beinterpreted as resistant to all four drugs Species identificationof Mycobacterium was carried out via testing the ability togrow on p-nitrobenzoic acid (PNB) All isolates were testedtwice in media to confirm the accuracy of the results [19 20]
23 Guanidine ChlorideDNAExtractionMethod All scrapedcolonies were washed with phosphate buffer saline (PBS)followed by the addition of 2mL lysis buffer 5 120583L proteinaseK 1mL guanidine chloride and 300 120583L ammonium acetateSuspensions were incubated overnight at 37∘C on the nextday 2mL of chilled chloroform was added After centrifuga-tion the clear upper layer was collected in a new tube andcold absolute ethanol was added to enhance precipitationof DNA The pellet was washed with 70 ethanol and thendecanted by 70 ethanol and allowed to dry The pelletwas then resuspended with nuclease-free water and qualifiedusing NanoDrop ND-1000 spectrophotometer (NanoDropTechnologies USA) The DNA samples were stored at minus20∘Cuntil used for conventional PCR [21 22]
24 GenoLyse Extraction Method DNA extraction was per-formed as recommended by the manufacturer (Hain Life-science) Firstly collected bacterial colonies were heated for20 minutes at 100∘C in a water bath and then suspended in100 120583L of kit lysis buffer followed by incubation at 95∘C for5min finally 100 120583L of neutralization buffer was added Themixture was spun at full speed in a tabletop centrifuge withan aerosol tight rotor and then stored at minus20∘C and then usedfor multiplex PCR in Line Probe Assay [23]
25 Conventional PCR Fifteen genomic DNA were used astemplates for PCR amplification of complete rrs gene (16SrRNA) The two primers used were forward primer namely27F (51015840-AGAGTTTGATCCTGGCTCAG-31015840) and reverseprimer namely 1495R (51015840-CTACGGCTACCTTGTTACGA-31015840) The 25 120583L reaction mixture contained 1 120583L DNA 1xreaction buffer (10x) with 3mM MgCl
2 25 U i-Taq DNA
polymerase (5U120583L) 25mM dNTPs 1 120583L of 10 pmol of eachprimer and 1x of gel loading buffer followed by completingthe volume to 25120583L by DW PCR amplifying procedure wasas follows 5min at 94∘C 30 cycles of 1min at 94∘C 1minat 58∘C 2min at 72∘C and then 10min at 72∘C which
Tuberculosis Research and Treatment 3
was performed on a Bio-Rad (DNA engineDyad Peltier)automatic thermal cycler Duplicate PCR of every samplewere carried out for more confirmation The products ofamplificationwere checked through running on 06 agarosegel electrophoresis [24 25]
26 Multiplex PCR Hybridization and detection were per-formed using the hybridization kits Seventy-five isolatedDNA were used by taking 5 120583L of each DNA and mixingit with 10 120583L Amplification Mix A and 35 120583L AmplificationMix B containing biotinylated primers The PCR amplifyingprocedure was as follows 15min at 95∘C 10 cycles of 30seconds at 95∘C 20 cycles of 40 seconds at 50∘C and 8minat 70∘C which was performed on a Hain Lifescience thermalcycler The amplification product was visualized throughreverse hybridization probes complementary to amplifiednucleic acids on membrane strips [26]
27 Sequencing of 16S rRNA Isolates were packaged accord-ing to the International Air Transport Association guidelinesand shipped with authorized permission to Macrogen Com-pany (Seoul SouthKorea) Purification and standard forwardsequencing of 16S rRNA were done by ABI Genetic Analyser(Applied Biosystems)
28 Statistical and Bioinformatic Analysis The result wasanalysed statistically using IBM SPSS Statistics version 21(Statistical Package for the Social Sciences) which is asoftware package for statistical analysis the chi-square testwas used to check the statistical significance [27] Thechromatogram sequences were visualized through FinchTV program version 140 [28] The nucleotides sequencesof the rrs gene were searched for sequences similarityusing nucleotide BLAST [29] Highly similar sequenceshave accession numbers HM007576 KF796661 JX303293and GU142936 and sequences of the reference M tuber-culosis H37Rv strain [X555881] were retrieved from NCBI(httpswwwncbinlmnihgov) and subjected to multi-ple sequence alignment using BioEdit software version725 [30] Newick format was withdrawn from ClustalW(httpwwwebiacukToolsmsaclustalw2) [31] to create aphylogenetic tree in Phylogenyfr software [32]
29 Nucleotide Sequence Accession Numbers The nucleotidesequences of the rrs genes containing novel mutations weredeposited in the GenBank database (National Center forBiotechnology Information httpswwwncbinlmnihgov)under the following accession numbers KU372152KU372153 KU372154 KU372155 KU372156 and KU372157
3 Results
Among 100 sputum samples twenty of them revealed nogrowth two were contaminated one was lysed and twohad grown in PNB indicating Mycobacterium other thantuberculosis (MOTT) The growth rate on LJ media is asfollows 39 (2975) showed +3 (200ndash500 colonies) 33(2575) showed +2 (100ndash200 colonies) 267 (2075) showed+1 (10ndash99 colonies) and 13 (175) showed 4 colonies
Table 1 Percentage of MDR in different age groups
Age group MDR Account (number)le30 60 931ndash40 133 241ndash50 133 251ndash60 133 2gt60 0 0
Most of the MDR growth appeared as +1 and probably hadgrown at 2ndash4 weeks (119875 value 0426) showing a statisticallyinsignificant association between growth rate and MDRTheprevalence of MDR was 20 (1575) and 147 (1115) amongpreviously treated and old cases and 53 (415) amongnewly diagnosed cases (119875 value 0003) which means drugresistance was associated with previous treatment 733 ofMDR cases were males while 267 were females (119875 value0536) Sixty percent (915) of MDR cases were found inthe age group le 30 years (119875 value 0652) (Table 1) Amongseventy-fiveMycobacterium tuberculosis isolates 56 (4275)were streptomycin-resistant 29 (2275) were rifampicin-resistant 20 (1575) were ethambutol-resistant and 28(2175) were isoniazid-resistant 20 (1575) were resistant toRIF and INH 16 (1275) were resistant to all four drugsThe run progression of the final separation of PCR productswas visualized under UV transilluminator documentationmachine Most of them fluoresced sharply but two of themfluoresced faintly and were excluded The most commonmutation detected by LPA in the rpoB gene was S531L (801215) followed by H526D in KatG gene the most commonmutation was S315T (67 1015) and in InhA promoter it wasC15T (333 721)
Sixty-two percent (813 isolates) of streptomycin-resistantisolates revealed mutations in rrs gene which were identifiedin seven groups four isolates (31) have G rarr A transitionat nucleoside position 892 three isolates (23) have Crarr Atransversion at nucleoside position 222 two isolates (15)have ArarrG transition at nucleoside position 904 one isolate(8) has Grarr T transversion at nucleoside position 855 oneisolate (8) has ArarrG transition at nucleoside position 906one isolate (8) has Trarr A transversion at nucleoside posi-tion 1238 and two isolates have Grarr AGrarr C at nucleosideposition 1400 which are more explained in Table 2
31 Phylogenetic Tree A phylogenetic tree represents therelationships among a set of Mycobacterium tuberculosisThe tree is classified into two branches All isolates have acommon ancestor except for isolate-9 which was outgroupIsolate-2 and isolate-4 were sister groups as shown in Figure 1
4 Discussions
The study found novel transversion mutation of C rarr Aat position 222 To our knowledge the present study isthe first study that demonstrated 16S rRNA analysis amongmultidrug-resistantM tuberculosis isolates from Sudan andthus the prevalence ofMDRwas 20 (1575) and 147 (1115)among old cases and 53 (415) among newly diagnosed
4 Tuberculosis Research and Treatment
Table 2 Explaining the position and frequency of polymorphism with resistance pattern of isolates
Mutation position Polymorphism Frequency () Resistance patternRIF INH STM EMB
222 Crarr A 23R R R SS S R SR S R S
885 Grarr T 8 S S R S
892 Grarr A 31
S R R SS S R SR R R SR R R R
904 Ararr G 15 S R R SR R R R
906 Ararr G 8 S R R STrarr A 8 R S R S
1400 Grarr A 8 R R R RGrarr C 8 S S R S
R resistance S sensitive RIF rifampicin INH isoniazid STM streptomycin EMB ethambutol
Iso_11Iso_10Iso5_1rstIsolate 2Isolate 4Iso_6Isolate 3H37RvUSA_CtrlPoland_CtrlIran_CtrlGermany_CtrlIso_9
Iso_11Iso_10
Iso5_1rst
Isolate 2
Isolate 4
Iso_6Iso_7
Isolate 3
H37Rv
USA_CtrlPoland_Ctrl
Iran_Ctrl
Germany_Ctrl
Iso_9
CGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGG
GGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGG
GCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGAGGTGTGGGGAGGTGTGGGGAGGTGTGGG
ATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCC
TGTTGGTGGGGTGACGGCCTACCAAGGCGACGACGGGTAGCCGGCCTGAGAGG
(a)
(c)(d)
(b)
Figure 1 (a) Gel electrophoresis of PCR product Lanes 1 and 5 DNA marker 1000+ Lanes 2 3 and 4 amplified DNA products 1500 bp(b) Chromatogram sequence of 16S rRNA visualized via Finch TV software (c) Alignment determining novel mutation at position 222transversion of C to A in isolates 9 10 and 11 via BioEdit software (d) Phylogenetic tree using Phylogenyfr software
cases which was lower than Francersquos study with a prevalenceof 23323 (71) in newly diagnosed patients and 33105(314) in re-treated patients [33] this difference could bedue to the geographical variation In the present study733 of MDR cases were males while 267 were femaleswhich agreed with Raizada et alrsquos study where MDR-TB waspredominant inmales (72 230320) [34] contrary toMelzer
et alrsquos study where 567 in males and 433 in females [35]may be due to the large numbers of males when comparedwith females included in this study Most MDR cases werefound in the age group le 30 years (60) correspondingwith Melzer et alrsquos study [35] The genotype MTBDRplustest identifiedmost frequent mutations involved in resistanceto RIF and INH as follows in rpoB gene S531L was 54
Tuberculosis Research and Treatment 5
(1222) this is similar to the findings of Barnard et al [36]The final result of mutation frequency in rrs gene is 62which is approximately similar to Ashorsquos study conductedin Pakistan that detected 3550 (70) strains [37] Alsoadditional studies in China Japan and Latvia have reportedthe highest frequencies 857 778 and 85 respectively[38ndash40] whereas in North India no mutation had beendetected in streptomycin-resistant isolates [41] Regardingmutation in the 912 region 23 of the isolates have beenrevealed A rarr G transition at position 904 corresponds tostudies in Germany [42] On the other hand a study inBarcelona did not detect mutation in the rrs912 region [43]The mutation at loop 530 of the rrs coding region had notbeen identified which agreed with New Yorkrsquos study [44] andconflicted with Polandrsquos study [45] Novel mutation could beused as a diagnostic marker that represents a tool for rapidmonitoring of streptomycin resistance and could be of valueto the clinician
Small sample size was one of the drawbacks that limitedour study therefore a large sample size in further studiescould be useful for the determination of other biomarkersthat assist the diagnosis of streptomycin-resistant MTB
5 Conclusion
Analysis of 16S rRNA sequences is considered the goldenstandard method for the identification and assessment ofphylogenetic relationships among bacterial isolates
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to Africa City of TechnologyNational Public Health Laboratory Molecular TuberculosisLaboratory and all members of the National ReferenceLaboratory of Tuberculosis (NRL-TB) Sudan Khartoum
References
[1] World Health Organization Global Tuberculosis Report 2015chapter 4 WHOHTMTB201522 Geneva Switzerland 20thedition 2015
[2] D A Mitchison and A J Nunn ldquoInfluence of initial drugresistance on the response to short-course chemotherapy of pul-monary tuberculosisrdquo American Review of Respiratory Diseasevol 133 no 3 pp 423ndash430 1986
[3] A L Kritski M J Ozorio Marques M F Rabahi et al ldquoTrans-mission of tuberculosis to close contacts of patients withmultidrug-resistant tuberculosisrdquo American Journal of Respira-tory and Critical CareMedicine vol 153 no 1 pp 331ndash335 1996
[4] WHO Global Tuberculosis Control 2014 WHO GenevaSwitzerland 2014 httpwwwwhointtbpublicationsglobalreport
[5] World Health OrganizationIUATLD ldquoGlobal project on anti-tuberculosis drug resistance surveillancerdquo Report 3 WorldHealth OrganizationIUATLD Geneva Switzerland 2003
[6] A S Rhines ldquoThe role of sex differences in the prevalence andtransmission of tuberculosisrdquo Tuberculosis vol 93 no 1 pp104ndash107 2013
[7] J A Caminero Ed Guidelines for Clinical and Opera-tional Management of Drug-Resistant Tuberculosis Interna-tional Union Against Tuberculosis and Lung Disease ParisFrance 2013
[8] A Somoskovi L M Parsons and M Salfinger ldquoThe molecularbasis of resistance to isoniazid rifampin and pyrazinamide inMycobacterium tuberculosisrdquo Respiratory Research vol 2 no 3pp 164ndash168 2001
[9] Y Zhang B Heym B Allen D Young and S Cole ldquoThecatalasemdashperoxidase gene and isoniazid resistance ofMycobac-terium tuberculosisrdquoNature vol 358 no 6387 pp 591ndash593 1992
[10] S H Gillespie ldquoEvolution of drug resistance inMycobacteriumtuberculosis clinical and molecular perspectiverdquo AntimicrobialAgents and Chemotherapy vol 46 no 2 pp 267ndash274 2002
[11] B Heym Y Zhang S Poulet D Young and S T Cole ldquoChar-acterization of the katG gene encoding a catalase-peroxidaserequired for the isoniazid susceptibility of Mycobacteriumtuberculosisrdquo Journal of Bacteriology vol 175 no 13 pp 4255ndash4259 1993
[12] J Crofton and D A Mitchison ldquoStreptomycin resistance inpulmonary tuberculosisrdquo British Medical Journal vol 2 pp1009ndash1015 1948
[13] D Moazed and H F Noller ldquoInteraction of antibiotics withfunctional sites in 16S ribosomalRNArdquoNature vol 327 no 6121pp 389ndash394 1987
[14] M Finken P Kirschner A Meier A Wrede and E C BottgerldquoMolecular basis of streptomycin resistance in Mycobacteriumtuberculosis alterations of the ribosomal protein S12 geneand point mutations within a functional 16S ribosomal RNApseudoknotrdquo Molecular Microbiology vol 9 no 6 pp 1239ndash1246 1993
[15] WHO Laboratory Services in Tuberculosis Control Part II andIII Microscopy and Culture WHO 1998
[16] P T Kent and G P Kubica Public Health MycobacteriologyGuides For Level III Laboratory US Department of Health andHuman Services Public Health Service CDC 1985
[17] S-J Kim G-H Bai and H-D Hwang ldquoEfficiency of the directand concentrationmethods in demonstrating tubercle bacilli inthe sputum specimensrdquo Tuberculosis and Respiratory Diseasesvol 36 no 4 pp 354ndash361 1989
[18] V Vincent and M C Gutierrez ldquoMycobacterium laboratorycharacteristics of slowly growing mycobacteriardquo in Manualof Clinical Microbiology pp 573ndash588 American Society forMicrobiology Washington DC USA 2007
[19] C Collins J Grange andM YatesOrganization and Practice inTuberculosis Bacteriology Butterworth London UK 1985
[20] G CanettiW Fox A Khomenko et al ldquoAdvances in techniquesof testing mycobacterial drug sensitivity and the use of sensi-tivity tests in tuberculosis control programmesrdquo Bulletin of theWorld Health Organization vol 41 no 1 pp 21ndash43 1969
[21] DNA Extraction Guanidine Method Modified from Black wellLab Cambridge UK
[22] S A Miller D D Dykes and H F Polesky ldquoA simple saltingout procedure for extracting DNA from human nucleated cellsrdquoNucleic Acids Research vol 16 no 3 p 1215 1988
[23] Hain Life Science Hardwiesenstraszlige Nehren Germanyhttpwwwhain-lifesciencede
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Tuberculosis Research and Treatment 3
was performed on a Bio-Rad (DNA engineDyad Peltier)automatic thermal cycler Duplicate PCR of every samplewere carried out for more confirmation The products ofamplificationwere checked through running on 06 agarosegel electrophoresis [24 25]
26 Multiplex PCR Hybridization and detection were per-formed using the hybridization kits Seventy-five isolatedDNA were used by taking 5 120583L of each DNA and mixingit with 10 120583L Amplification Mix A and 35 120583L AmplificationMix B containing biotinylated primers The PCR amplifyingprocedure was as follows 15min at 95∘C 10 cycles of 30seconds at 95∘C 20 cycles of 40 seconds at 50∘C and 8minat 70∘C which was performed on a Hain Lifescience thermalcycler The amplification product was visualized throughreverse hybridization probes complementary to amplifiednucleic acids on membrane strips [26]
27 Sequencing of 16S rRNA Isolates were packaged accord-ing to the International Air Transport Association guidelinesand shipped with authorized permission to Macrogen Com-pany (Seoul SouthKorea) Purification and standard forwardsequencing of 16S rRNA were done by ABI Genetic Analyser(Applied Biosystems)
28 Statistical and Bioinformatic Analysis The result wasanalysed statistically using IBM SPSS Statistics version 21(Statistical Package for the Social Sciences) which is asoftware package for statistical analysis the chi-square testwas used to check the statistical significance [27] Thechromatogram sequences were visualized through FinchTV program version 140 [28] The nucleotides sequencesof the rrs gene were searched for sequences similarityusing nucleotide BLAST [29] Highly similar sequenceshave accession numbers HM007576 KF796661 JX303293and GU142936 and sequences of the reference M tuber-culosis H37Rv strain [X555881] were retrieved from NCBI(httpswwwncbinlmnihgov) and subjected to multi-ple sequence alignment using BioEdit software version725 [30] Newick format was withdrawn from ClustalW(httpwwwebiacukToolsmsaclustalw2) [31] to create aphylogenetic tree in Phylogenyfr software [32]
29 Nucleotide Sequence Accession Numbers The nucleotidesequences of the rrs genes containing novel mutations weredeposited in the GenBank database (National Center forBiotechnology Information httpswwwncbinlmnihgov)under the following accession numbers KU372152KU372153 KU372154 KU372155 KU372156 and KU372157
3 Results
Among 100 sputum samples twenty of them revealed nogrowth two were contaminated one was lysed and twohad grown in PNB indicating Mycobacterium other thantuberculosis (MOTT) The growth rate on LJ media is asfollows 39 (2975) showed +3 (200ndash500 colonies) 33(2575) showed +2 (100ndash200 colonies) 267 (2075) showed+1 (10ndash99 colonies) and 13 (175) showed 4 colonies
Table 1 Percentage of MDR in different age groups
Age group MDR Account (number)le30 60 931ndash40 133 241ndash50 133 251ndash60 133 2gt60 0 0
Most of the MDR growth appeared as +1 and probably hadgrown at 2ndash4 weeks (119875 value 0426) showing a statisticallyinsignificant association between growth rate and MDRTheprevalence of MDR was 20 (1575) and 147 (1115) amongpreviously treated and old cases and 53 (415) amongnewly diagnosed cases (119875 value 0003) which means drugresistance was associated with previous treatment 733 ofMDR cases were males while 267 were females (119875 value0536) Sixty percent (915) of MDR cases were found inthe age group le 30 years (119875 value 0652) (Table 1) Amongseventy-fiveMycobacterium tuberculosis isolates 56 (4275)were streptomycin-resistant 29 (2275) were rifampicin-resistant 20 (1575) were ethambutol-resistant and 28(2175) were isoniazid-resistant 20 (1575) were resistant toRIF and INH 16 (1275) were resistant to all four drugsThe run progression of the final separation of PCR productswas visualized under UV transilluminator documentationmachine Most of them fluoresced sharply but two of themfluoresced faintly and were excluded The most commonmutation detected by LPA in the rpoB gene was S531L (801215) followed by H526D in KatG gene the most commonmutation was S315T (67 1015) and in InhA promoter it wasC15T (333 721)
Sixty-two percent (813 isolates) of streptomycin-resistantisolates revealed mutations in rrs gene which were identifiedin seven groups four isolates (31) have G rarr A transitionat nucleoside position 892 three isolates (23) have Crarr Atransversion at nucleoside position 222 two isolates (15)have ArarrG transition at nucleoside position 904 one isolate(8) has Grarr T transversion at nucleoside position 855 oneisolate (8) has ArarrG transition at nucleoside position 906one isolate (8) has Trarr A transversion at nucleoside posi-tion 1238 and two isolates have Grarr AGrarr C at nucleosideposition 1400 which are more explained in Table 2
31 Phylogenetic Tree A phylogenetic tree represents therelationships among a set of Mycobacterium tuberculosisThe tree is classified into two branches All isolates have acommon ancestor except for isolate-9 which was outgroupIsolate-2 and isolate-4 were sister groups as shown in Figure 1
4 Discussions
The study found novel transversion mutation of C rarr Aat position 222 To our knowledge the present study isthe first study that demonstrated 16S rRNA analysis amongmultidrug-resistantM tuberculosis isolates from Sudan andthus the prevalence ofMDRwas 20 (1575) and 147 (1115)among old cases and 53 (415) among newly diagnosed
4 Tuberculosis Research and Treatment
Table 2 Explaining the position and frequency of polymorphism with resistance pattern of isolates
Mutation position Polymorphism Frequency () Resistance patternRIF INH STM EMB
222 Crarr A 23R R R SS S R SR S R S
885 Grarr T 8 S S R S
892 Grarr A 31
S R R SS S R SR R R SR R R R
904 Ararr G 15 S R R SR R R R
906 Ararr G 8 S R R STrarr A 8 R S R S
1400 Grarr A 8 R R R RGrarr C 8 S S R S
R resistance S sensitive RIF rifampicin INH isoniazid STM streptomycin EMB ethambutol
Iso_11Iso_10Iso5_1rstIsolate 2Isolate 4Iso_6Isolate 3H37RvUSA_CtrlPoland_CtrlIran_CtrlGermany_CtrlIso_9
Iso_11Iso_10
Iso5_1rst
Isolate 2
Isolate 4
Iso_6Iso_7
Isolate 3
H37Rv
USA_CtrlPoland_Ctrl
Iran_Ctrl
Germany_Ctrl
Iso_9
CGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGG
GGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGG
GCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGAGGTGTGGGGAGGTGTGGGGAGGTGTGGG
ATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCC
TGTTGGTGGGGTGACGGCCTACCAAGGCGACGACGGGTAGCCGGCCTGAGAGG
(a)
(c)(d)
(b)
Figure 1 (a) Gel electrophoresis of PCR product Lanes 1 and 5 DNA marker 1000+ Lanes 2 3 and 4 amplified DNA products 1500 bp(b) Chromatogram sequence of 16S rRNA visualized via Finch TV software (c) Alignment determining novel mutation at position 222transversion of C to A in isolates 9 10 and 11 via BioEdit software (d) Phylogenetic tree using Phylogenyfr software
cases which was lower than Francersquos study with a prevalenceof 23323 (71) in newly diagnosed patients and 33105(314) in re-treated patients [33] this difference could bedue to the geographical variation In the present study733 of MDR cases were males while 267 were femaleswhich agreed with Raizada et alrsquos study where MDR-TB waspredominant inmales (72 230320) [34] contrary toMelzer
et alrsquos study where 567 in males and 433 in females [35]may be due to the large numbers of males when comparedwith females included in this study Most MDR cases werefound in the age group le 30 years (60) correspondingwith Melzer et alrsquos study [35] The genotype MTBDRplustest identifiedmost frequent mutations involved in resistanceto RIF and INH as follows in rpoB gene S531L was 54
Tuberculosis Research and Treatment 5
(1222) this is similar to the findings of Barnard et al [36]The final result of mutation frequency in rrs gene is 62which is approximately similar to Ashorsquos study conductedin Pakistan that detected 3550 (70) strains [37] Alsoadditional studies in China Japan and Latvia have reportedthe highest frequencies 857 778 and 85 respectively[38ndash40] whereas in North India no mutation had beendetected in streptomycin-resistant isolates [41] Regardingmutation in the 912 region 23 of the isolates have beenrevealed A rarr G transition at position 904 corresponds tostudies in Germany [42] On the other hand a study inBarcelona did not detect mutation in the rrs912 region [43]The mutation at loop 530 of the rrs coding region had notbeen identified which agreed with New Yorkrsquos study [44] andconflicted with Polandrsquos study [45] Novel mutation could beused as a diagnostic marker that represents a tool for rapidmonitoring of streptomycin resistance and could be of valueto the clinician
Small sample size was one of the drawbacks that limitedour study therefore a large sample size in further studiescould be useful for the determination of other biomarkersthat assist the diagnosis of streptomycin-resistant MTB
5 Conclusion
Analysis of 16S rRNA sequences is considered the goldenstandard method for the identification and assessment ofphylogenetic relationships among bacterial isolates
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to Africa City of TechnologyNational Public Health Laboratory Molecular TuberculosisLaboratory and all members of the National ReferenceLaboratory of Tuberculosis (NRL-TB) Sudan Khartoum
References
[1] World Health Organization Global Tuberculosis Report 2015chapter 4 WHOHTMTB201522 Geneva Switzerland 20thedition 2015
[2] D A Mitchison and A J Nunn ldquoInfluence of initial drugresistance on the response to short-course chemotherapy of pul-monary tuberculosisrdquo American Review of Respiratory Diseasevol 133 no 3 pp 423ndash430 1986
[3] A L Kritski M J Ozorio Marques M F Rabahi et al ldquoTrans-mission of tuberculosis to close contacts of patients withmultidrug-resistant tuberculosisrdquo American Journal of Respira-tory and Critical CareMedicine vol 153 no 1 pp 331ndash335 1996
[4] WHO Global Tuberculosis Control 2014 WHO GenevaSwitzerland 2014 httpwwwwhointtbpublicationsglobalreport
[5] World Health OrganizationIUATLD ldquoGlobal project on anti-tuberculosis drug resistance surveillancerdquo Report 3 WorldHealth OrganizationIUATLD Geneva Switzerland 2003
[6] A S Rhines ldquoThe role of sex differences in the prevalence andtransmission of tuberculosisrdquo Tuberculosis vol 93 no 1 pp104ndash107 2013
[7] J A Caminero Ed Guidelines for Clinical and Opera-tional Management of Drug-Resistant Tuberculosis Interna-tional Union Against Tuberculosis and Lung Disease ParisFrance 2013
[8] A Somoskovi L M Parsons and M Salfinger ldquoThe molecularbasis of resistance to isoniazid rifampin and pyrazinamide inMycobacterium tuberculosisrdquo Respiratory Research vol 2 no 3pp 164ndash168 2001
[9] Y Zhang B Heym B Allen D Young and S Cole ldquoThecatalasemdashperoxidase gene and isoniazid resistance ofMycobac-terium tuberculosisrdquoNature vol 358 no 6387 pp 591ndash593 1992
[10] S H Gillespie ldquoEvolution of drug resistance inMycobacteriumtuberculosis clinical and molecular perspectiverdquo AntimicrobialAgents and Chemotherapy vol 46 no 2 pp 267ndash274 2002
[11] B Heym Y Zhang S Poulet D Young and S T Cole ldquoChar-acterization of the katG gene encoding a catalase-peroxidaserequired for the isoniazid susceptibility of Mycobacteriumtuberculosisrdquo Journal of Bacteriology vol 175 no 13 pp 4255ndash4259 1993
[12] J Crofton and D A Mitchison ldquoStreptomycin resistance inpulmonary tuberculosisrdquo British Medical Journal vol 2 pp1009ndash1015 1948
[13] D Moazed and H F Noller ldquoInteraction of antibiotics withfunctional sites in 16S ribosomalRNArdquoNature vol 327 no 6121pp 389ndash394 1987
[14] M Finken P Kirschner A Meier A Wrede and E C BottgerldquoMolecular basis of streptomycin resistance in Mycobacteriumtuberculosis alterations of the ribosomal protein S12 geneand point mutations within a functional 16S ribosomal RNApseudoknotrdquo Molecular Microbiology vol 9 no 6 pp 1239ndash1246 1993
[15] WHO Laboratory Services in Tuberculosis Control Part II andIII Microscopy and Culture WHO 1998
[16] P T Kent and G P Kubica Public Health MycobacteriologyGuides For Level III Laboratory US Department of Health andHuman Services Public Health Service CDC 1985
[17] S-J Kim G-H Bai and H-D Hwang ldquoEfficiency of the directand concentrationmethods in demonstrating tubercle bacilli inthe sputum specimensrdquo Tuberculosis and Respiratory Diseasesvol 36 no 4 pp 354ndash361 1989
[18] V Vincent and M C Gutierrez ldquoMycobacterium laboratorycharacteristics of slowly growing mycobacteriardquo in Manualof Clinical Microbiology pp 573ndash588 American Society forMicrobiology Washington DC USA 2007
[19] C Collins J Grange andM YatesOrganization and Practice inTuberculosis Bacteriology Butterworth London UK 1985
[20] G CanettiW Fox A Khomenko et al ldquoAdvances in techniquesof testing mycobacterial drug sensitivity and the use of sensi-tivity tests in tuberculosis control programmesrdquo Bulletin of theWorld Health Organization vol 41 no 1 pp 21ndash43 1969
[21] DNA Extraction Guanidine Method Modified from Black wellLab Cambridge UK
[22] S A Miller D D Dykes and H F Polesky ldquoA simple saltingout procedure for extracting DNA from human nucleated cellsrdquoNucleic Acids Research vol 16 no 3 p 1215 1988
[23] Hain Life Science Hardwiesenstraszlige Nehren Germanyhttpwwwhain-lifesciencede
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
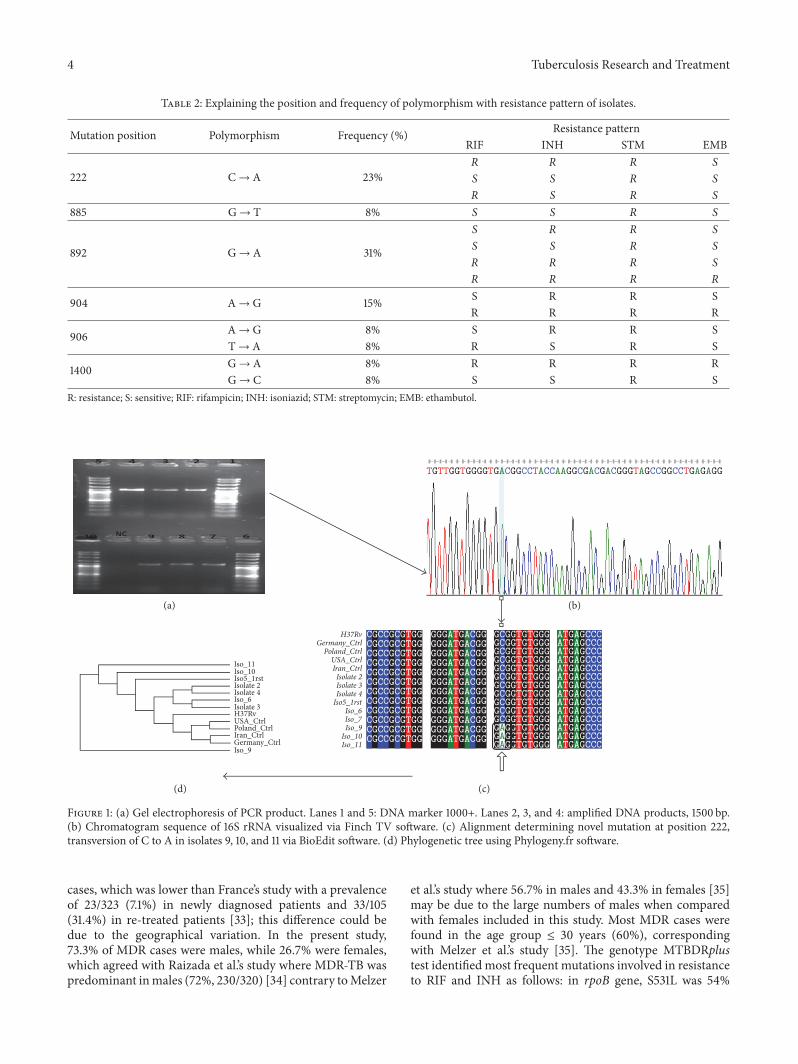
4 Tuberculosis Research and Treatment
Table 2 Explaining the position and frequency of polymorphism with resistance pattern of isolates
Mutation position Polymorphism Frequency () Resistance patternRIF INH STM EMB
222 Crarr A 23R R R SS S R SR S R S
885 Grarr T 8 S S R S
892 Grarr A 31
S R R SS S R SR R R SR R R R
904 Ararr G 15 S R R SR R R R
906 Ararr G 8 S R R STrarr A 8 R S R S
1400 Grarr A 8 R R R RGrarr C 8 S S R S
R resistance S sensitive RIF rifampicin INH isoniazid STM streptomycin EMB ethambutol
Iso_11Iso_10Iso5_1rstIsolate 2Isolate 4Iso_6Isolate 3H37RvUSA_CtrlPoland_CtrlIran_CtrlGermany_CtrlIso_9
Iso_11Iso_10
Iso5_1rst
Isolate 2
Isolate 4
Iso_6Iso_7
Isolate 3
H37Rv
USA_CtrlPoland_Ctrl
Iran_Ctrl
Germany_Ctrl
Iso_9
CGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGGCGCCGCGTGG
GGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGGGGGATGACGG
GCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGCGGTGTGGGGAGGTGTGGGGAGGTGTGGGGAGGTGTGGG
ATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCCATGAGCCC
TGTTGGTGGGGTGACGGCCTACCAAGGCGACGACGGGTAGCCGGCCTGAGAGG
(a)
(c)(d)
(b)
Figure 1 (a) Gel electrophoresis of PCR product Lanes 1 and 5 DNA marker 1000+ Lanes 2 3 and 4 amplified DNA products 1500 bp(b) Chromatogram sequence of 16S rRNA visualized via Finch TV software (c) Alignment determining novel mutation at position 222transversion of C to A in isolates 9 10 and 11 via BioEdit software (d) Phylogenetic tree using Phylogenyfr software
cases which was lower than Francersquos study with a prevalenceof 23323 (71) in newly diagnosed patients and 33105(314) in re-treated patients [33] this difference could bedue to the geographical variation In the present study733 of MDR cases were males while 267 were femaleswhich agreed with Raizada et alrsquos study where MDR-TB waspredominant inmales (72 230320) [34] contrary toMelzer
et alrsquos study where 567 in males and 433 in females [35]may be due to the large numbers of males when comparedwith females included in this study Most MDR cases werefound in the age group le 30 years (60) correspondingwith Melzer et alrsquos study [35] The genotype MTBDRplustest identifiedmost frequent mutations involved in resistanceto RIF and INH as follows in rpoB gene S531L was 54
Tuberculosis Research and Treatment 5
(1222) this is similar to the findings of Barnard et al [36]The final result of mutation frequency in rrs gene is 62which is approximately similar to Ashorsquos study conductedin Pakistan that detected 3550 (70) strains [37] Alsoadditional studies in China Japan and Latvia have reportedthe highest frequencies 857 778 and 85 respectively[38ndash40] whereas in North India no mutation had beendetected in streptomycin-resistant isolates [41] Regardingmutation in the 912 region 23 of the isolates have beenrevealed A rarr G transition at position 904 corresponds tostudies in Germany [42] On the other hand a study inBarcelona did not detect mutation in the rrs912 region [43]The mutation at loop 530 of the rrs coding region had notbeen identified which agreed with New Yorkrsquos study [44] andconflicted with Polandrsquos study [45] Novel mutation could beused as a diagnostic marker that represents a tool for rapidmonitoring of streptomycin resistance and could be of valueto the clinician
Small sample size was one of the drawbacks that limitedour study therefore a large sample size in further studiescould be useful for the determination of other biomarkersthat assist the diagnosis of streptomycin-resistant MTB
5 Conclusion
Analysis of 16S rRNA sequences is considered the goldenstandard method for the identification and assessment ofphylogenetic relationships among bacterial isolates
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to Africa City of TechnologyNational Public Health Laboratory Molecular TuberculosisLaboratory and all members of the National ReferenceLaboratory of Tuberculosis (NRL-TB) Sudan Khartoum
References
[1] World Health Organization Global Tuberculosis Report 2015chapter 4 WHOHTMTB201522 Geneva Switzerland 20thedition 2015
[2] D A Mitchison and A J Nunn ldquoInfluence of initial drugresistance on the response to short-course chemotherapy of pul-monary tuberculosisrdquo American Review of Respiratory Diseasevol 133 no 3 pp 423ndash430 1986
[3] A L Kritski M J Ozorio Marques M F Rabahi et al ldquoTrans-mission of tuberculosis to close contacts of patients withmultidrug-resistant tuberculosisrdquo American Journal of Respira-tory and Critical CareMedicine vol 153 no 1 pp 331ndash335 1996
[4] WHO Global Tuberculosis Control 2014 WHO GenevaSwitzerland 2014 httpwwwwhointtbpublicationsglobalreport
[5] World Health OrganizationIUATLD ldquoGlobal project on anti-tuberculosis drug resistance surveillancerdquo Report 3 WorldHealth OrganizationIUATLD Geneva Switzerland 2003
[6] A S Rhines ldquoThe role of sex differences in the prevalence andtransmission of tuberculosisrdquo Tuberculosis vol 93 no 1 pp104ndash107 2013
[7] J A Caminero Ed Guidelines for Clinical and Opera-tional Management of Drug-Resistant Tuberculosis Interna-tional Union Against Tuberculosis and Lung Disease ParisFrance 2013
[8] A Somoskovi L M Parsons and M Salfinger ldquoThe molecularbasis of resistance to isoniazid rifampin and pyrazinamide inMycobacterium tuberculosisrdquo Respiratory Research vol 2 no 3pp 164ndash168 2001
[9] Y Zhang B Heym B Allen D Young and S Cole ldquoThecatalasemdashperoxidase gene and isoniazid resistance ofMycobac-terium tuberculosisrdquoNature vol 358 no 6387 pp 591ndash593 1992
[10] S H Gillespie ldquoEvolution of drug resistance inMycobacteriumtuberculosis clinical and molecular perspectiverdquo AntimicrobialAgents and Chemotherapy vol 46 no 2 pp 267ndash274 2002
[11] B Heym Y Zhang S Poulet D Young and S T Cole ldquoChar-acterization of the katG gene encoding a catalase-peroxidaserequired for the isoniazid susceptibility of Mycobacteriumtuberculosisrdquo Journal of Bacteriology vol 175 no 13 pp 4255ndash4259 1993
[12] J Crofton and D A Mitchison ldquoStreptomycin resistance inpulmonary tuberculosisrdquo British Medical Journal vol 2 pp1009ndash1015 1948
[13] D Moazed and H F Noller ldquoInteraction of antibiotics withfunctional sites in 16S ribosomalRNArdquoNature vol 327 no 6121pp 389ndash394 1987
[14] M Finken P Kirschner A Meier A Wrede and E C BottgerldquoMolecular basis of streptomycin resistance in Mycobacteriumtuberculosis alterations of the ribosomal protein S12 geneand point mutations within a functional 16S ribosomal RNApseudoknotrdquo Molecular Microbiology vol 9 no 6 pp 1239ndash1246 1993
[15] WHO Laboratory Services in Tuberculosis Control Part II andIII Microscopy and Culture WHO 1998
[16] P T Kent and G P Kubica Public Health MycobacteriologyGuides For Level III Laboratory US Department of Health andHuman Services Public Health Service CDC 1985
[17] S-J Kim G-H Bai and H-D Hwang ldquoEfficiency of the directand concentrationmethods in demonstrating tubercle bacilli inthe sputum specimensrdquo Tuberculosis and Respiratory Diseasesvol 36 no 4 pp 354ndash361 1989
[18] V Vincent and M C Gutierrez ldquoMycobacterium laboratorycharacteristics of slowly growing mycobacteriardquo in Manualof Clinical Microbiology pp 573ndash588 American Society forMicrobiology Washington DC USA 2007
[19] C Collins J Grange andM YatesOrganization and Practice inTuberculosis Bacteriology Butterworth London UK 1985
[20] G CanettiW Fox A Khomenko et al ldquoAdvances in techniquesof testing mycobacterial drug sensitivity and the use of sensi-tivity tests in tuberculosis control programmesrdquo Bulletin of theWorld Health Organization vol 41 no 1 pp 21ndash43 1969
[21] DNA Extraction Guanidine Method Modified from Black wellLab Cambridge UK
[22] S A Miller D D Dykes and H F Polesky ldquoA simple saltingout procedure for extracting DNA from human nucleated cellsrdquoNucleic Acids Research vol 16 no 3 p 1215 1988
[23] Hain Life Science Hardwiesenstraszlige Nehren Germanyhttpwwwhain-lifesciencede
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Tuberculosis Research and Treatment 5
(1222) this is similar to the findings of Barnard et al [36]The final result of mutation frequency in rrs gene is 62which is approximately similar to Ashorsquos study conductedin Pakistan that detected 3550 (70) strains [37] Alsoadditional studies in China Japan and Latvia have reportedthe highest frequencies 857 778 and 85 respectively[38ndash40] whereas in North India no mutation had beendetected in streptomycin-resistant isolates [41] Regardingmutation in the 912 region 23 of the isolates have beenrevealed A rarr G transition at position 904 corresponds tostudies in Germany [42] On the other hand a study inBarcelona did not detect mutation in the rrs912 region [43]The mutation at loop 530 of the rrs coding region had notbeen identified which agreed with New Yorkrsquos study [44] andconflicted with Polandrsquos study [45] Novel mutation could beused as a diagnostic marker that represents a tool for rapidmonitoring of streptomycin resistance and could be of valueto the clinician
Small sample size was one of the drawbacks that limitedour study therefore a large sample size in further studiescould be useful for the determination of other biomarkersthat assist the diagnosis of streptomycin-resistant MTB
5 Conclusion
Analysis of 16S rRNA sequences is considered the goldenstandard method for the identification and assessment ofphylogenetic relationships among bacterial isolates
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors are grateful to Africa City of TechnologyNational Public Health Laboratory Molecular TuberculosisLaboratory and all members of the National ReferenceLaboratory of Tuberculosis (NRL-TB) Sudan Khartoum
References
[1] World Health Organization Global Tuberculosis Report 2015chapter 4 WHOHTMTB201522 Geneva Switzerland 20thedition 2015
[2] D A Mitchison and A J Nunn ldquoInfluence of initial drugresistance on the response to short-course chemotherapy of pul-monary tuberculosisrdquo American Review of Respiratory Diseasevol 133 no 3 pp 423ndash430 1986
[3] A L Kritski M J Ozorio Marques M F Rabahi et al ldquoTrans-mission of tuberculosis to close contacts of patients withmultidrug-resistant tuberculosisrdquo American Journal of Respira-tory and Critical CareMedicine vol 153 no 1 pp 331ndash335 1996
[4] WHO Global Tuberculosis Control 2014 WHO GenevaSwitzerland 2014 httpwwwwhointtbpublicationsglobalreport
[5] World Health OrganizationIUATLD ldquoGlobal project on anti-tuberculosis drug resistance surveillancerdquo Report 3 WorldHealth OrganizationIUATLD Geneva Switzerland 2003
[6] A S Rhines ldquoThe role of sex differences in the prevalence andtransmission of tuberculosisrdquo Tuberculosis vol 93 no 1 pp104ndash107 2013
[7] J A Caminero Ed Guidelines for Clinical and Opera-tional Management of Drug-Resistant Tuberculosis Interna-tional Union Against Tuberculosis and Lung Disease ParisFrance 2013
[8] A Somoskovi L M Parsons and M Salfinger ldquoThe molecularbasis of resistance to isoniazid rifampin and pyrazinamide inMycobacterium tuberculosisrdquo Respiratory Research vol 2 no 3pp 164ndash168 2001
[9] Y Zhang B Heym B Allen D Young and S Cole ldquoThecatalasemdashperoxidase gene and isoniazid resistance ofMycobac-terium tuberculosisrdquoNature vol 358 no 6387 pp 591ndash593 1992
[10] S H Gillespie ldquoEvolution of drug resistance inMycobacteriumtuberculosis clinical and molecular perspectiverdquo AntimicrobialAgents and Chemotherapy vol 46 no 2 pp 267ndash274 2002
[11] B Heym Y Zhang S Poulet D Young and S T Cole ldquoChar-acterization of the katG gene encoding a catalase-peroxidaserequired for the isoniazid susceptibility of Mycobacteriumtuberculosisrdquo Journal of Bacteriology vol 175 no 13 pp 4255ndash4259 1993
[12] J Crofton and D A Mitchison ldquoStreptomycin resistance inpulmonary tuberculosisrdquo British Medical Journal vol 2 pp1009ndash1015 1948
[13] D Moazed and H F Noller ldquoInteraction of antibiotics withfunctional sites in 16S ribosomalRNArdquoNature vol 327 no 6121pp 389ndash394 1987
[14] M Finken P Kirschner A Meier A Wrede and E C BottgerldquoMolecular basis of streptomycin resistance in Mycobacteriumtuberculosis alterations of the ribosomal protein S12 geneand point mutations within a functional 16S ribosomal RNApseudoknotrdquo Molecular Microbiology vol 9 no 6 pp 1239ndash1246 1993
[15] WHO Laboratory Services in Tuberculosis Control Part II andIII Microscopy and Culture WHO 1998
[16] P T Kent and G P Kubica Public Health MycobacteriologyGuides For Level III Laboratory US Department of Health andHuman Services Public Health Service CDC 1985
[17] S-J Kim G-H Bai and H-D Hwang ldquoEfficiency of the directand concentrationmethods in demonstrating tubercle bacilli inthe sputum specimensrdquo Tuberculosis and Respiratory Diseasesvol 36 no 4 pp 354ndash361 1989
[18] V Vincent and M C Gutierrez ldquoMycobacterium laboratorycharacteristics of slowly growing mycobacteriardquo in Manualof Clinical Microbiology pp 573ndash588 American Society forMicrobiology Washington DC USA 2007
[19] C Collins J Grange andM YatesOrganization and Practice inTuberculosis Bacteriology Butterworth London UK 1985
[20] G CanettiW Fox A Khomenko et al ldquoAdvances in techniquesof testing mycobacterial drug sensitivity and the use of sensi-tivity tests in tuberculosis control programmesrdquo Bulletin of theWorld Health Organization vol 41 no 1 pp 21ndash43 1969
[21] DNA Extraction Guanidine Method Modified from Black wellLab Cambridge UK
[22] S A Miller D D Dykes and H F Polesky ldquoA simple saltingout procedure for extracting DNA from human nucleated cellsrdquoNucleic Acids Research vol 16 no 3 p 1215 1988
[23] Hain Life Science Hardwiesenstraszlige Nehren Germanyhttpwwwhain-lifesciencede
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
6 Tuberculosis Research and Treatment
[24] W Liu Q Bao Jirimutu et al ldquoIsolation and identification oflactic acid bacteria from Tarag in Eastern Inner Mongolia ofChina by 16S rRNA sequences and DGGE analysisrdquo Microbi-ological Research vol 167 no 2 pp 110ndash115 2012
[25] iNtRONBIOTECHNOLOGYMaxime PCRPreMix Kit (i-Taq)for 20120583l rxn Cat NO 25025 httpwwwintronbiocom
[26] ldquoGenotype MTBDRplus version 10 [product insert]rdquoNehren Germany Hain Lifescience GmbH Hain lifesciencewebsite httpwwwhainlifesciencecompdf304xx pblpdf
[27] IBM SPSS Statistics for Windows Version 210 Armonk NYIBM Corp Released 2012 httpwwwibmcomanalyticsusentechnologyspss
[28] httpwwwgeospizacomProductsfinchtvshtml[29] httpsblastncbinlmnihgovBlastcgi[30] T A Hall ldquoBioEdit a user-friendly biological sequence align-
ment editor and analysis program for Windows 9598NTrdquoNucleic Acids Symposium Series vol 41 pp 95ndash98 1999
[31] H McWilliam W Li M Uludag et al ldquoAnalysis Tool WebServices from the EMBL-EBIrdquoNucleic acids research vol 41 ppW597ndashW600 2013
[32] A Dereeper V Guignon G Blanc et al ldquoPhylogenyfr robustphylogenetic analysis for the non-specialistrdquo Nucleic AcidsResearch vol 36 pp W465ndashW469 2008
[33] J Lyu M-N Kim J W Song et al ldquoGenoType MTBDRplusassay detection of drug-resistant tuberculosis in routine prac-tice inKoreardquoTheInternational Journal of Tuberculosis and LungDisease vol 17 no 1 pp 120ndash124 2013
[34] N Raizada K S Sachdeva D S Chauhan et al ldquoA Multi-site validation in India of the line probe assay for the rapiddiagnosis of multi-drug resistant tuberculosis directly fromsputum specimensrdquo PLoS ONE vol 9 no 2 Article ID e886262014
[35] MMelzer N Gupta I Petersen S Cook and BHall ldquoPrevioustreatment in predicting drug-resistant tuberculosis in an areabordering East London UKrdquo International Journal of InfectiousDiseases vol 14 no 8 pp e717ndashe722 2010
[36] M Barnard H Albert G Coetzee R OrsquoBrien and M EBosman ldquoRapid molecular screening for multidrug-resistanttuberculosis in a high-volume public health laboratory in SouthAfricardquo American Journal of Respiratory and Critical CareMedicine vol 177 no 7 pp 787ndash792 2008
[37] A Ali R Hasan K Jabeen N Jabeen E Qadeer and ZHasan ldquoCharacterization of mutations conferring extensivedrug resistance to Mycobacterium tuberculosis isolates in Pak-istanrdquo Antimicrobial Agents and Chemotherapy vol 55 no 12pp 5654ndash5659 2011
[38] X-Q Wu Y Lu J-X Zhang et al ldquoDetection of streptomycinresistance in Mycobacterium tuberculosis clinical isolates usingfourmolecular methods in ChinardquoActa Genetica Sinica vol 33no 7 pp 655ndash663 2006
[39] C Katsukawa A Tamaru Y Miyata C Abe M Makinoand Y Suzuki ldquoCharacterization of the rpsL and rrs genesof streptomycin-resistant clinical isolates of Mycobacteriumtuberculosis in Japanrdquo Journal of Applied Microbiology vol 83no 5 pp 634ndash640 1997
[40] T Tracevska I Jansone A Nodieva O Margab G Skenderscand V Baumanisa ldquoCharacterization of rpsl rrs and embBmutation associated Streptomycin and Euthambutol resistancein Mycobacterium Tuberculosisrdquo Microbiological Research vol155 pp 830ndash834 2007
[41] N Siddiqi M Shamim S Hussain et al ldquoMolecular character-ization of multidrug-resistant isolates ofMycobacterium Tuber-culosis from patients in North Indiardquo Antimicrobial Agents andChemotherapy vol 46 no 2 pp 443ndash450 2002
[42] A Meier P Kirschner F-C Bange U Vogel and E C BottgerldquoGenetic alterations in streptomycin-resistant Mycobacteriumtuberculosis mapping of mutations conferring resistancerdquoAntimicrobial Agents and Chemotherapy vol 38 no 2 pp 228ndash233 1994
[43] G Tudo E Rey S Borrell et al ldquoCharacterization of mutationsin streptomycin-resistant Mycobacterium tuberculosis clinicalisolates in the area of Barcelonardquo Journal of AntimicrobialChemotherapy vol 65 no 11 Article ID dkq322 pp 2341ndash23462010
[44] R C Cooksey G P Morlock A Mcqueen S E Glickmanand J T Crawford ldquoCharacterization of streptomycin resistancemechanisms among Mycobacterium tuberculosis isolates frompatients in New York Cityrdquo Antimicrobial Agents and Chemo-therapy vol 40 no 5 pp 1186ndash1188 1996
[45] T Jagielski H Ignatowska Z Bakuła et al ldquoScreening for strep-tomycin resistance-conferring mutations in Mycobacteriumtuberculosis clinical isolates from Polandrdquo PLoS ONE vol 9 no6 Article ID e100078 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom






![Resistant Hypertension โรคความ’นโลต,ง./อ1อการ3 ... · 2017. 7. 19. · Resistant Hypertension ระ’บความ’นโลต.ZงไXสามารถควบ\มไ]](https://static.fdokument.com/doc/165x107/5fe4ea108d199a1b3b0e0871/resistant-hypertension-aaaaaaaaaaaaaa1aaaa3.jpg)











