





Plazenta und Vasa prävia Plazenta increta B-Bild und ... · [email protected] Plazenta und...
45
[email protected] Plazenta und Vasa prävia Plazenta increta B-Bild und Doppler Geräteeinstellung Alice Winkler Frauenklinik Luzern 24.11.2018
Transcript of Plazenta und Vasa prävia Plazenta increta B-Bild und ... · [email protected] Plazenta und...
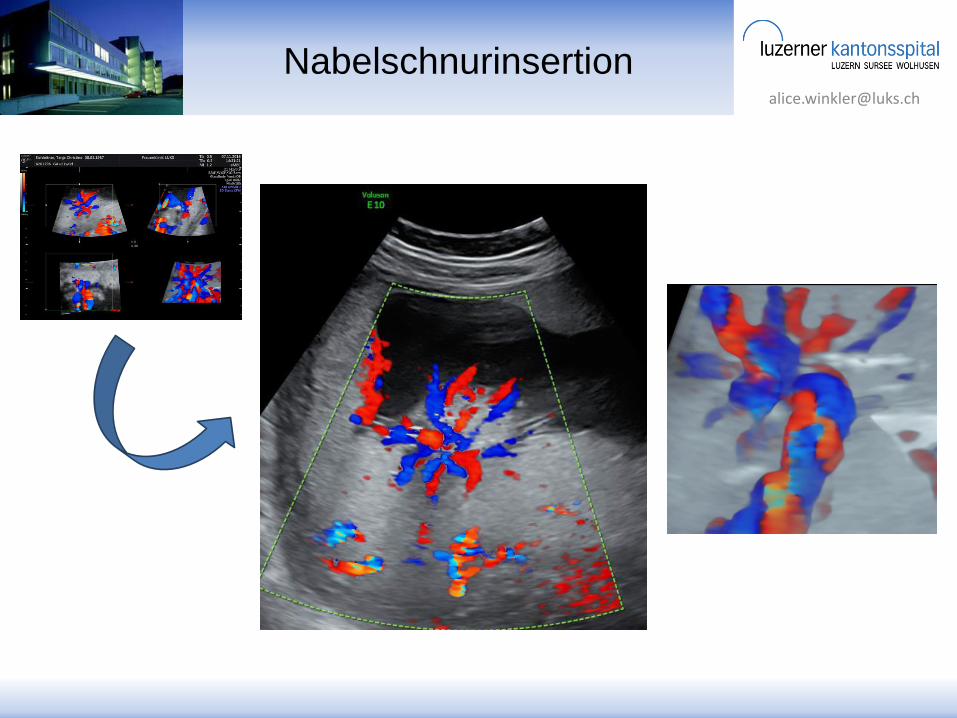
Plazenta und Vasa prävia
Plazenta increta
B-Bild und Doppler
Geräteeinstellung
Alice Winkler
Frauenklinik Luzern
24.11.2018

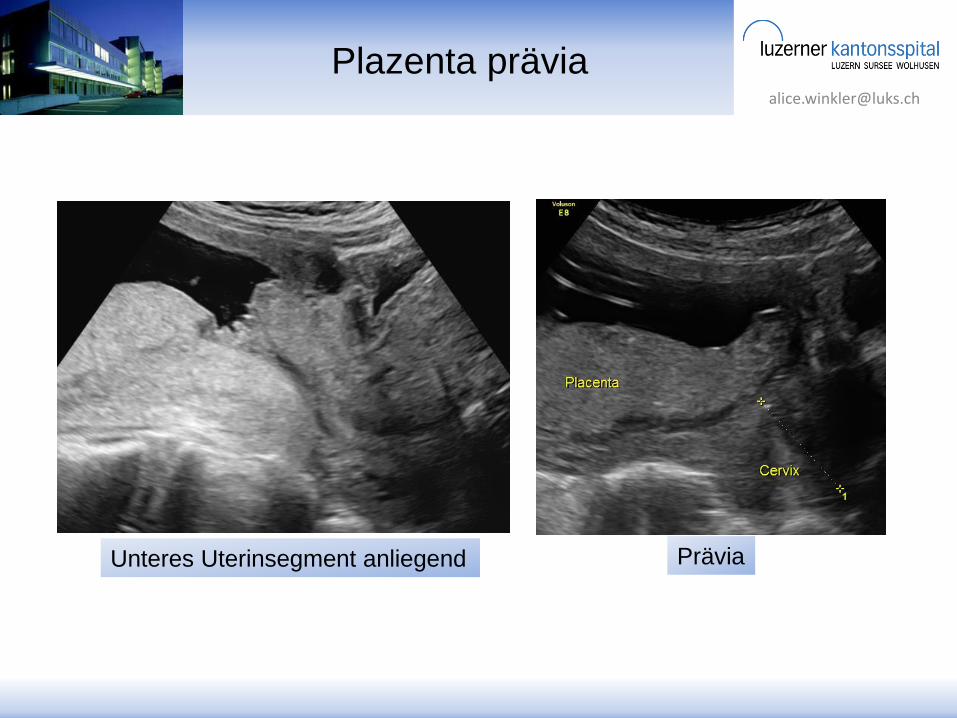
Plazentiefsitz
Sectio wenn ≤ 2 cm Abstand
1-2 cm: vaginale Geburt 77%
0-1 cm: vaginale Geburt 27%
Bronsteen R et al, UOG, 2009

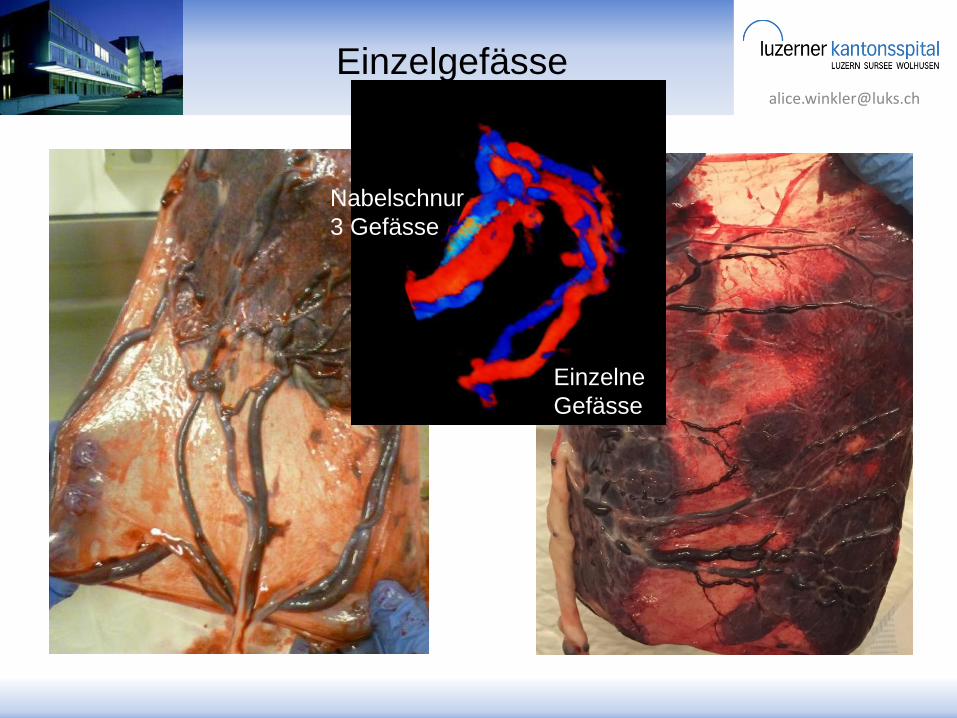
Abnorm invasive Plazenta
Diagnose klinisch - sonographisch - histologisch
Fokale Accreta → Flächige Perkreta
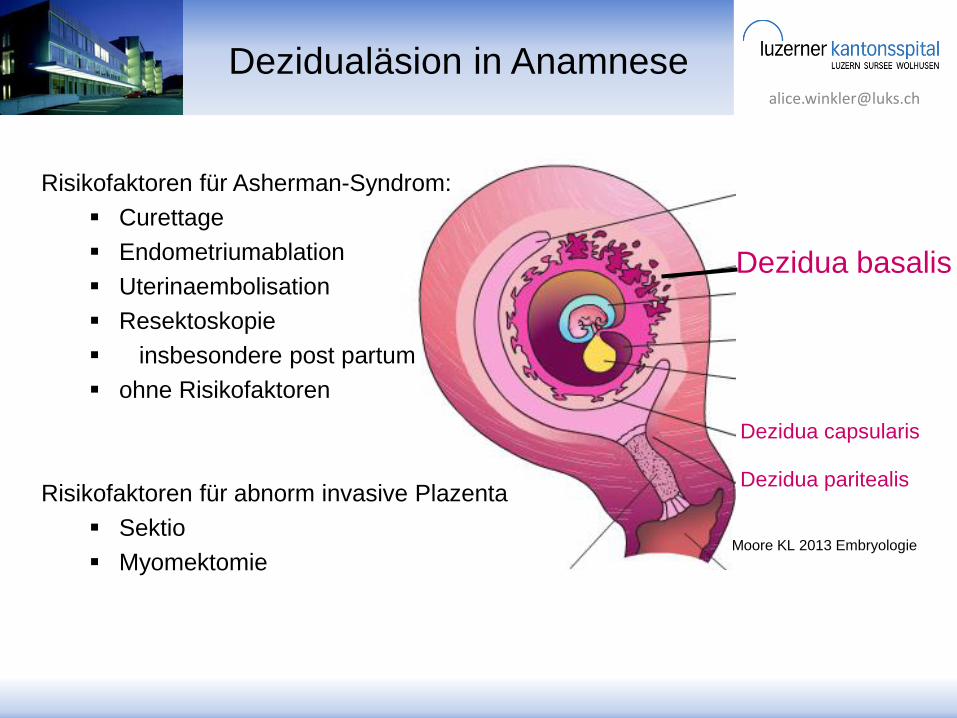
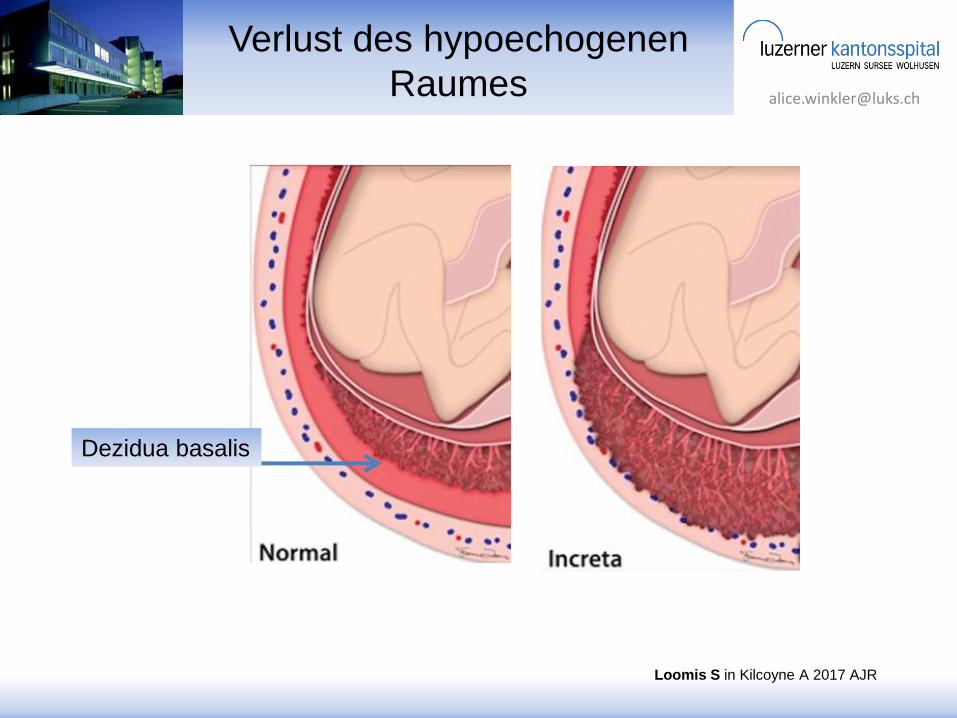
Dezidua basalis
Dezidualäsion in Anamnese
Dezidua paritealis
Dezidua capsularis
Moore KL 2013 Embryologie
Risikofaktoren für Asherman-Syndrom:
Curettage
Endometriumablation
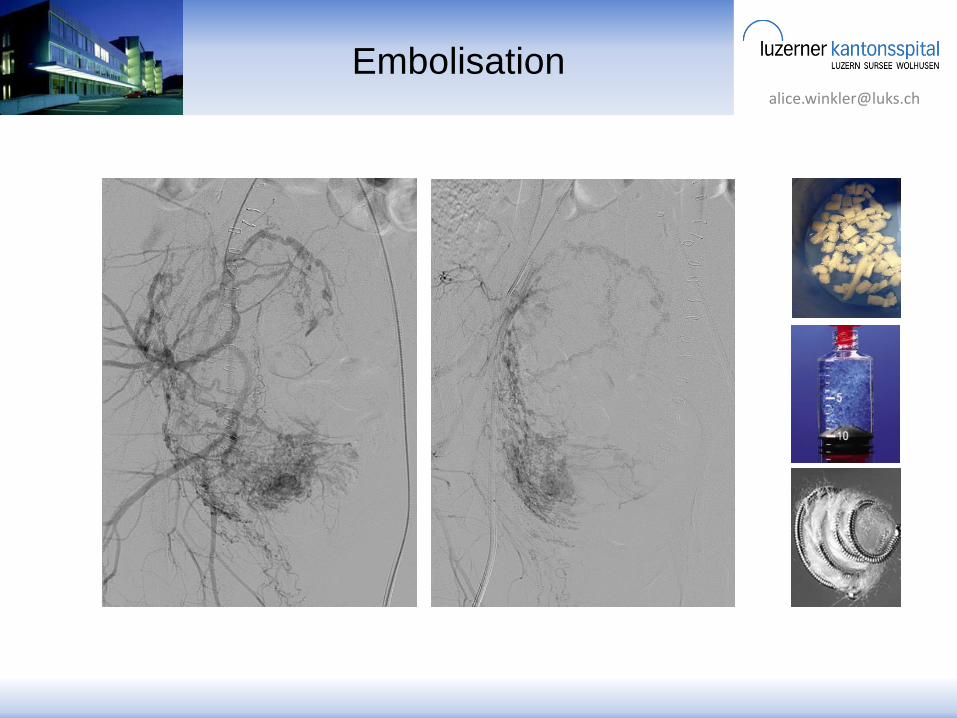
Uterinaembolisation
Resektoskopie
insbesondere post partum
ohne Risikofaktoren
Risikofaktoren für abnorm invasive Plazenta
Sektio
Myomektomie

Standardisierte Kriterien
Farbdoppler
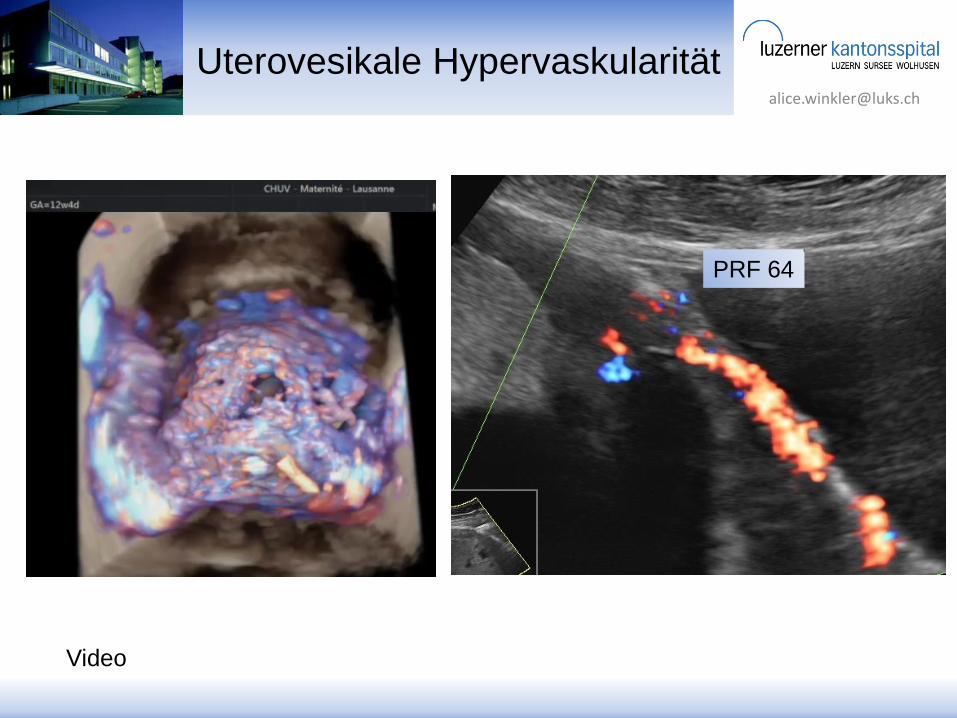
uterovesikale
Hypervaskularität
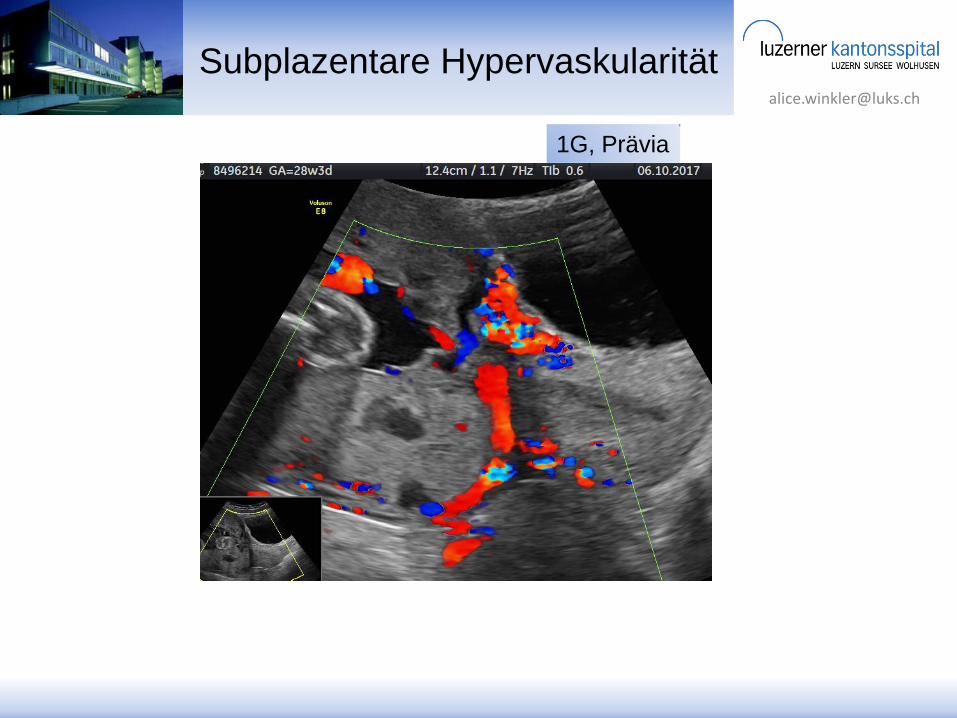
Subplazentare
Hypervaskularität
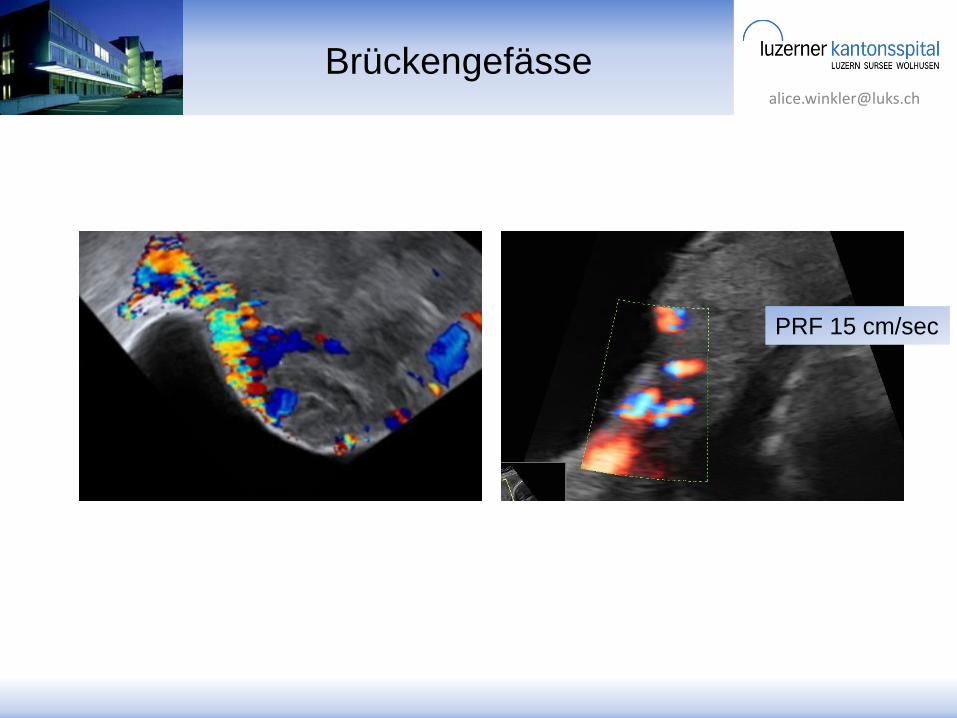
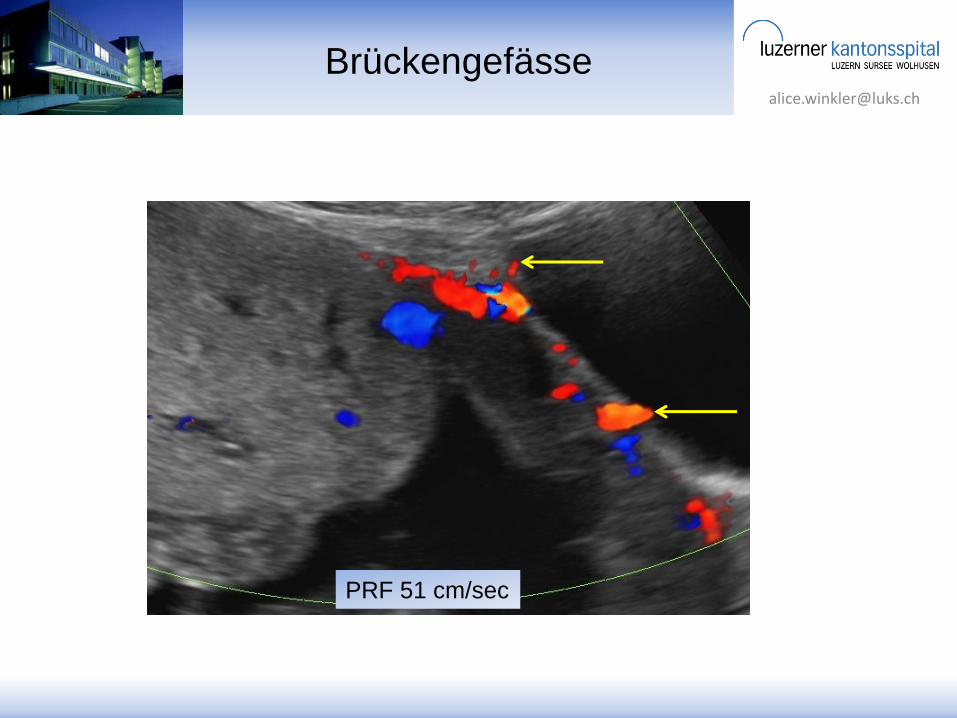
Brückengefässe
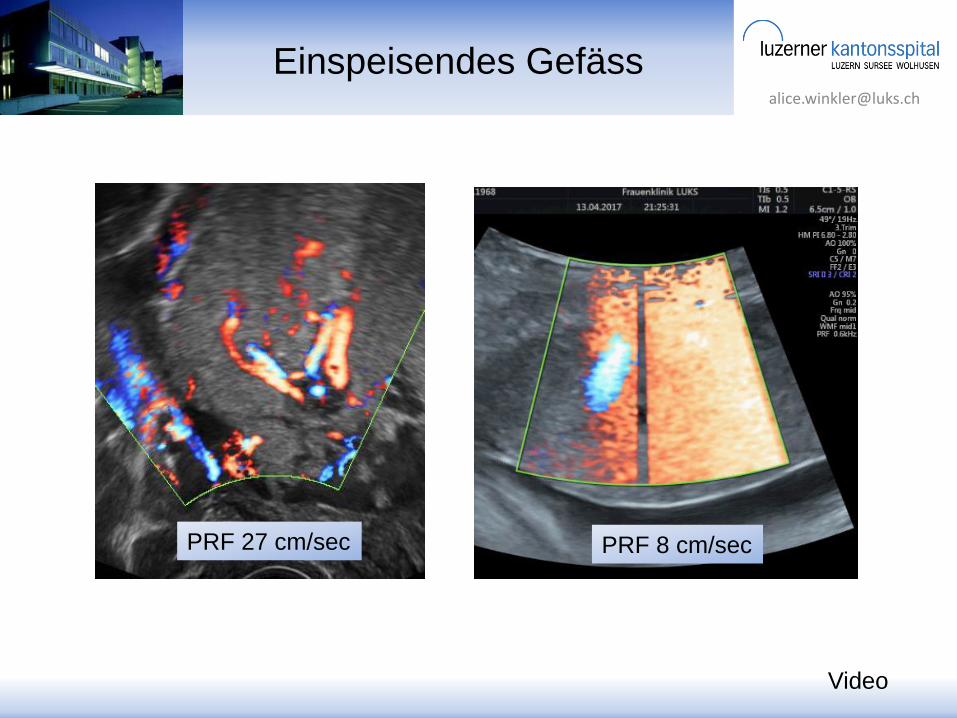
Einspeisendes Gefäss
B-Bild
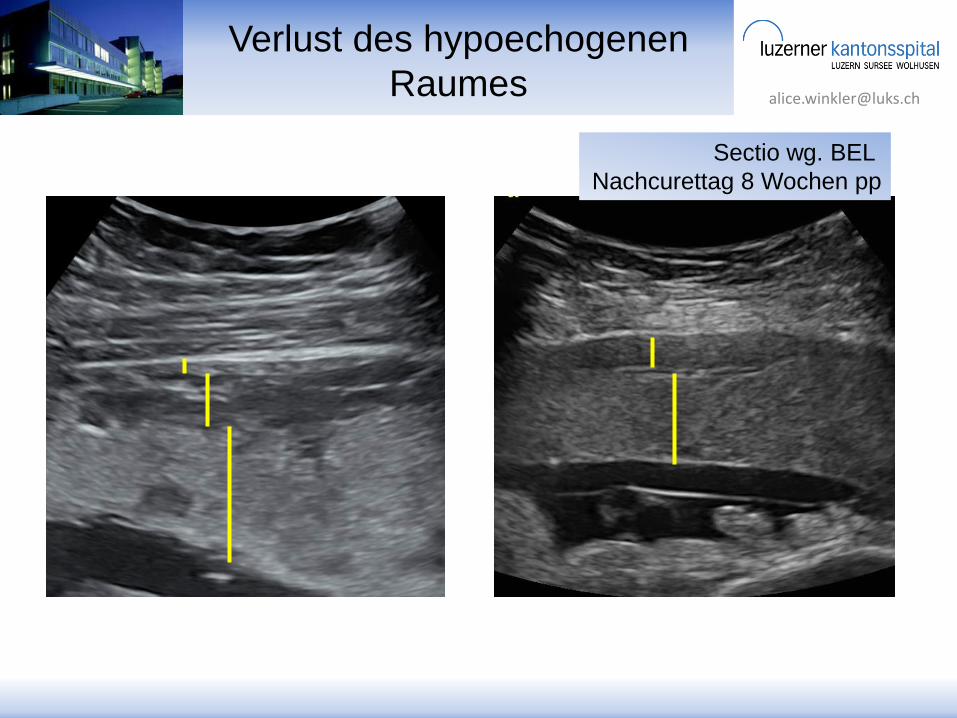
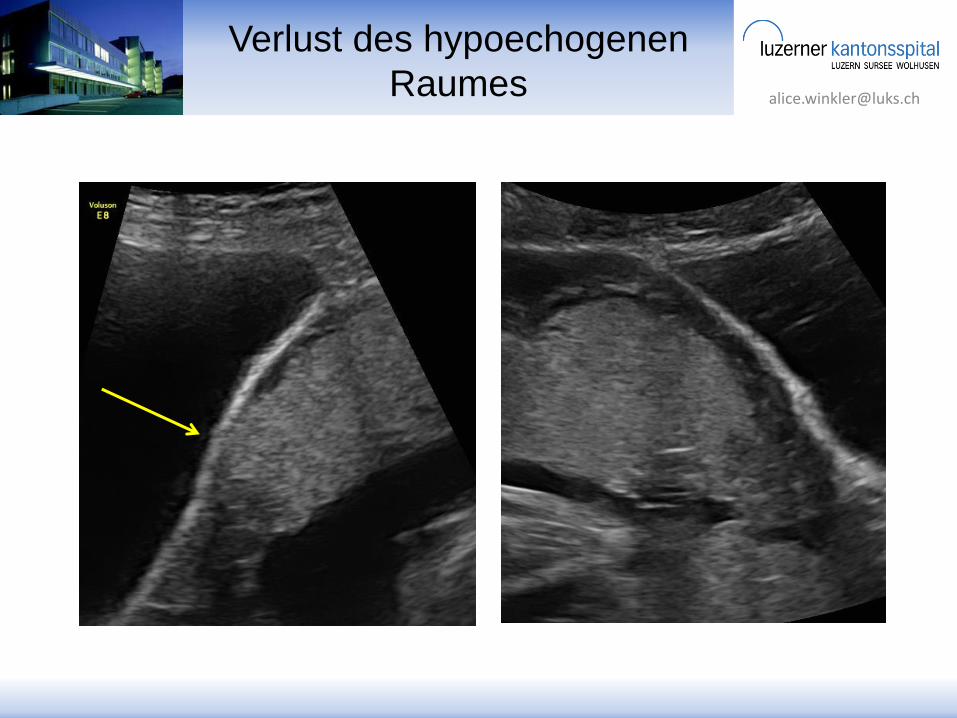
Verlust d. hypoechogenen Raumes
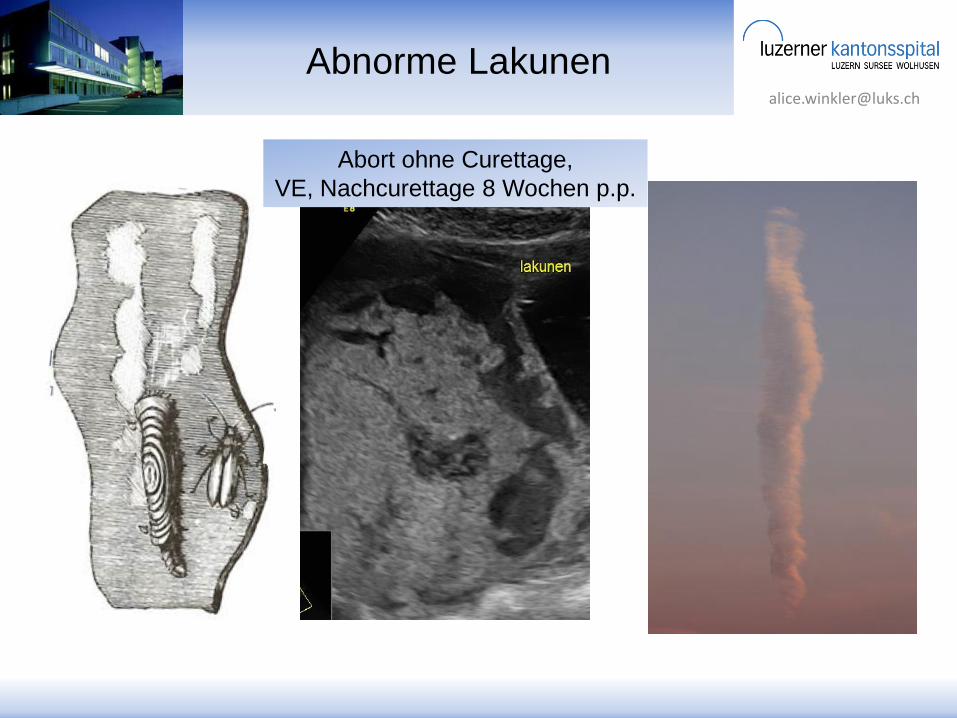
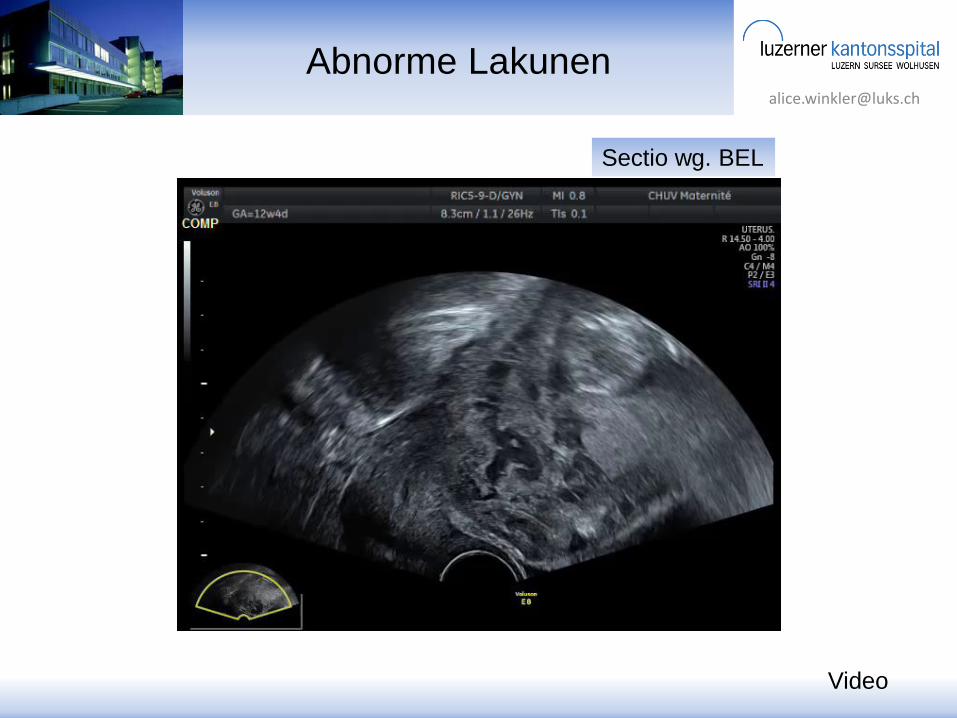
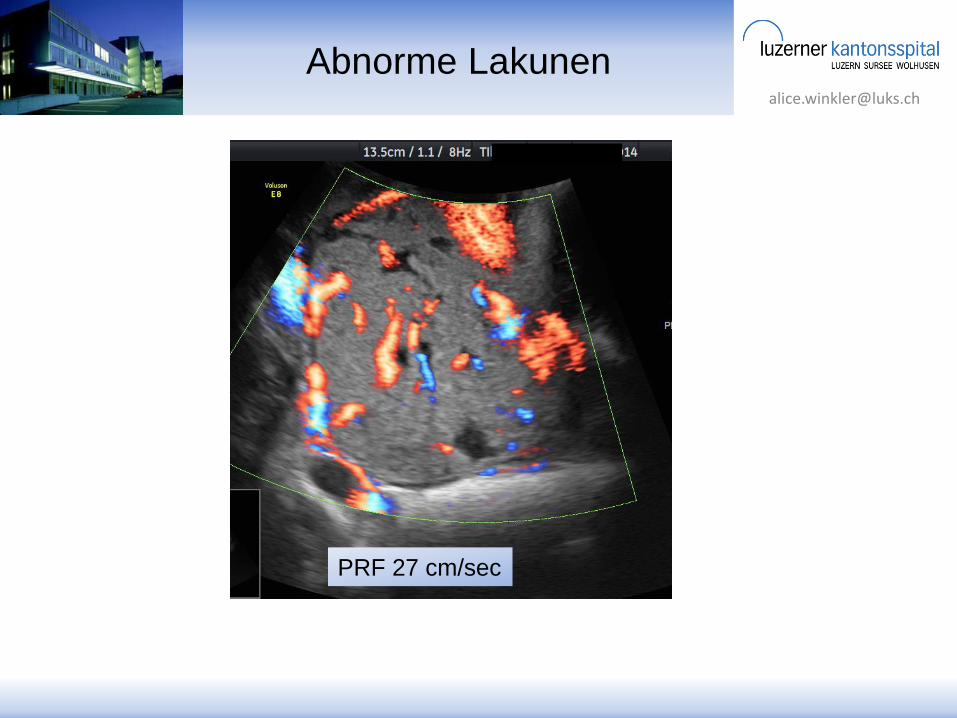
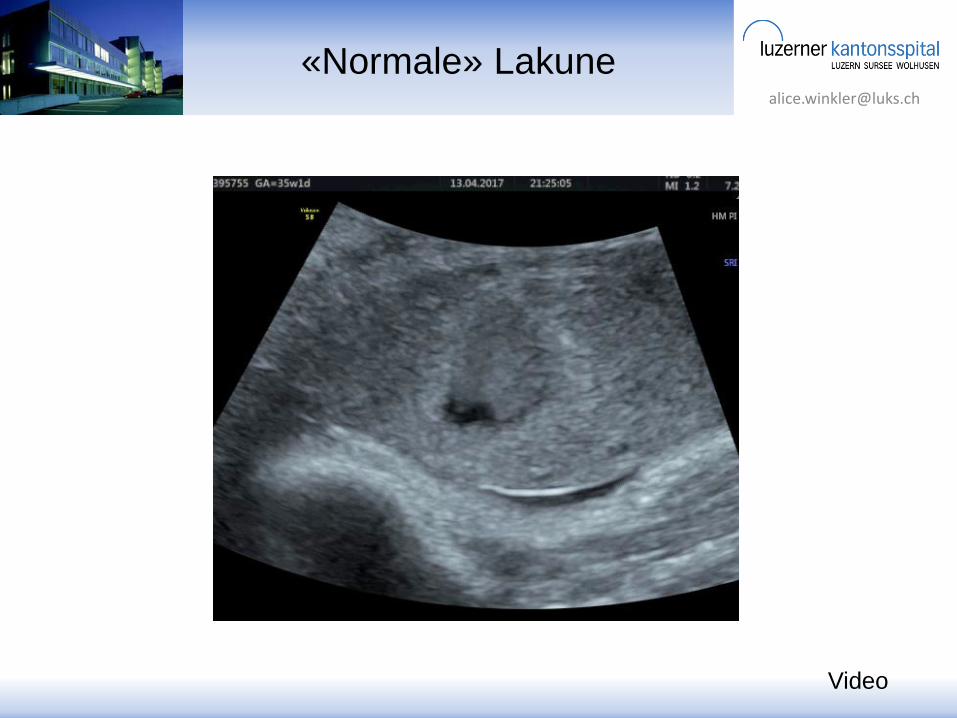
Abnorme Lakunen
Unterbrechung der Blasenwand
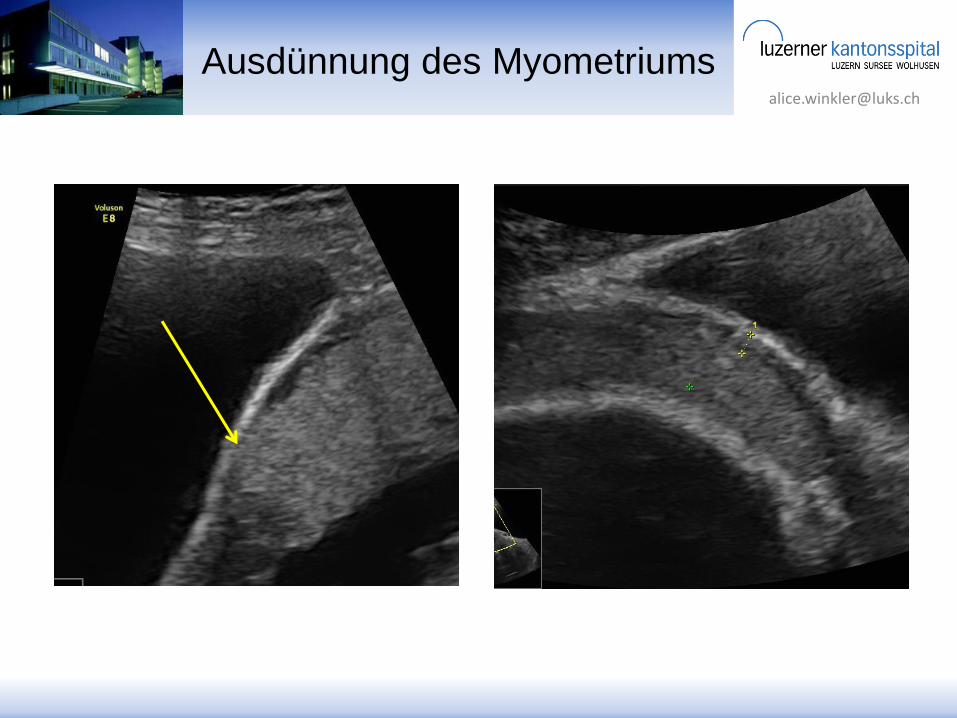
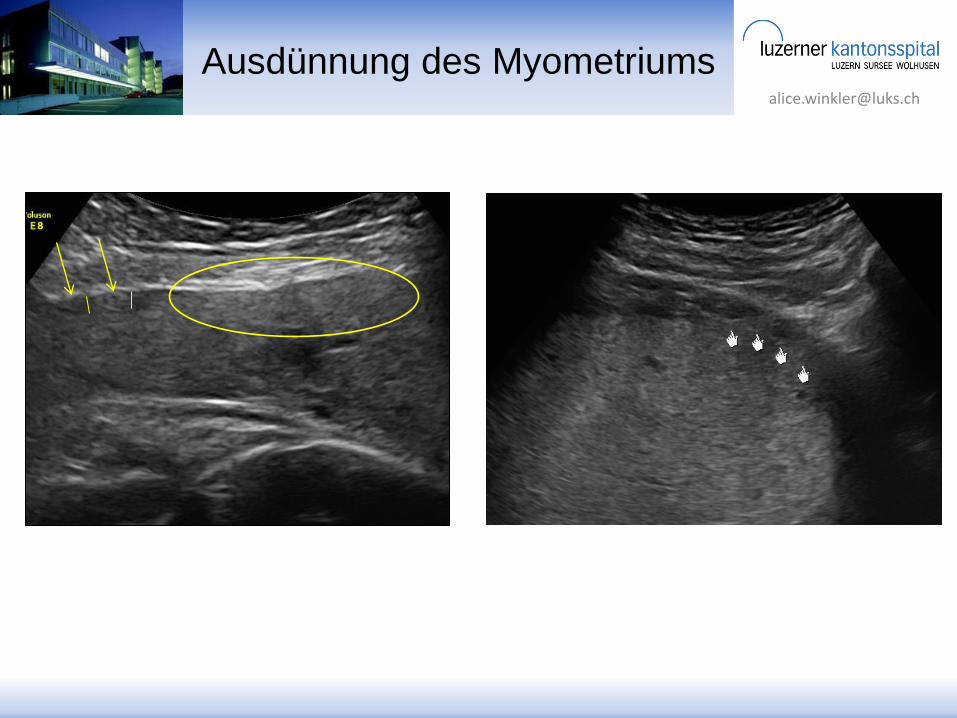
Ausdünnung d. Myometriums
Plazentare Vorwölbung
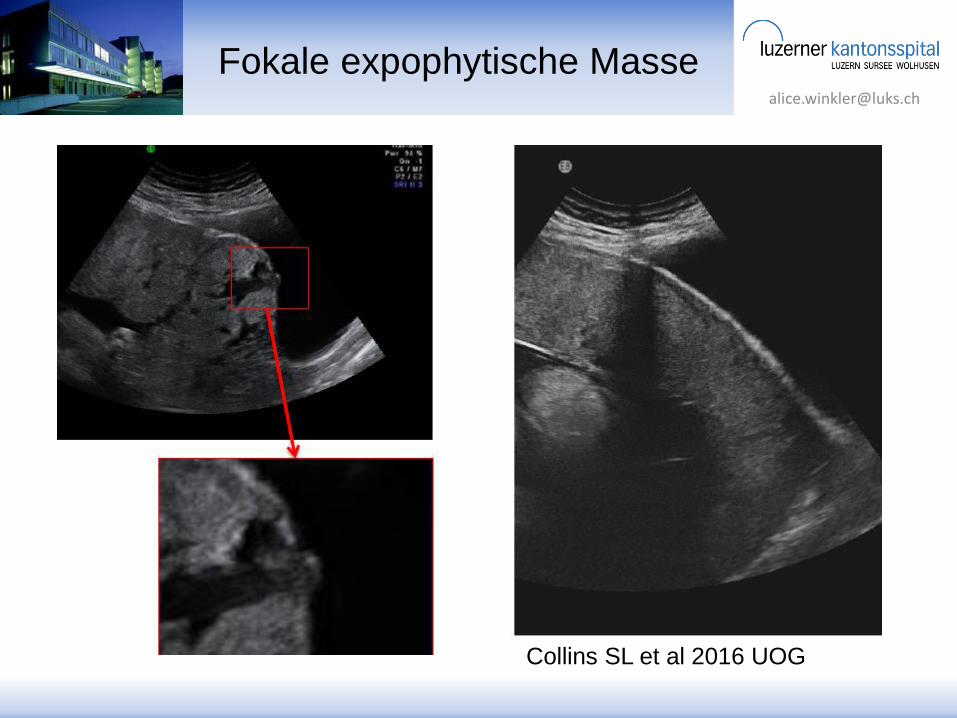
Fokale exophytische Masse
European Working Group on AIP 2015
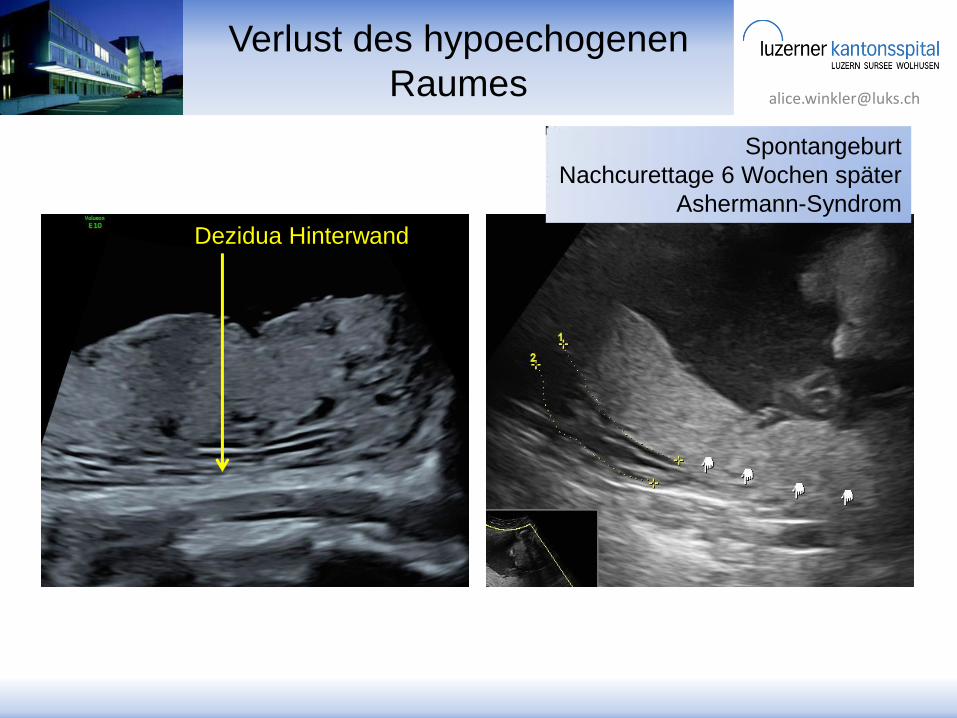
Verlust des hypoechogenen
Raumes
Dezidua Hinterwand
Spontangeburt
Nachcurettage 6 Wochen später
Ashermann-Syndrom

Standardisierte Kriterien
Farbdoppler
uterovesikale
Hypervaskularität
Subplazentare
Hypervaskularität
Brückengefässe
Einspeisendes Gefäss
B-Bild
Verlust d. hypoechogenen Raumes
Abnorme Lakunen
Unterbrechung der Blasenwand
Ausdünnung d. Myometriums
Plazentare Vorwölbung
Fokale exophytische Masse
European Working Group on AIP 2015
Kombination der Ultraschall- und Dopplerzeichen
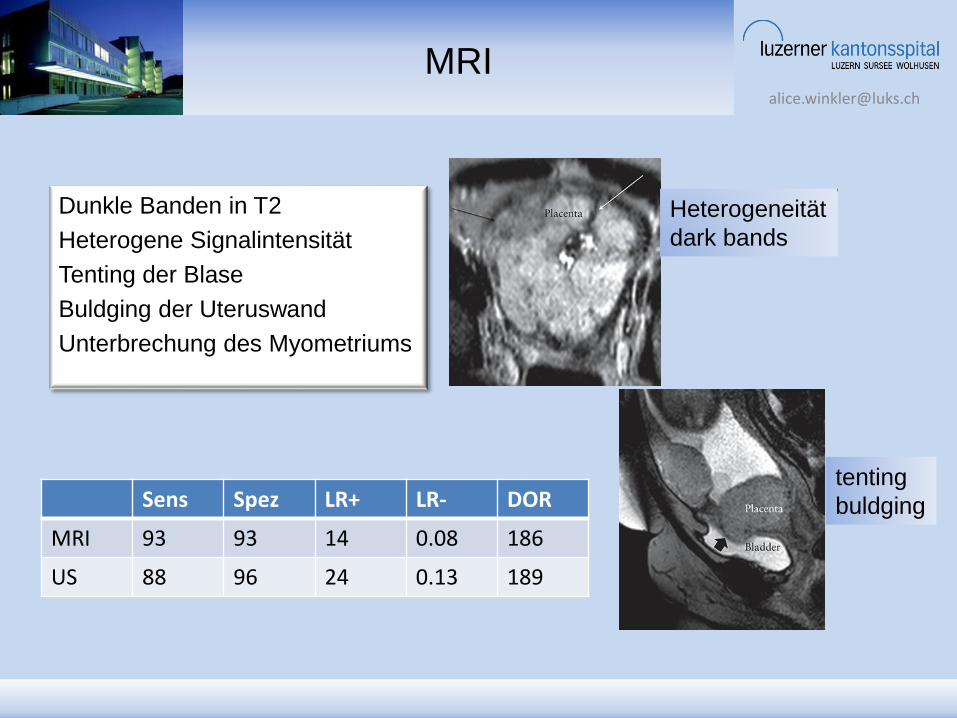
MRI
Dunkle Banden in T2
Heterogene Signalintensität
Tenting der Blase
Buldging der Uteruswand
Unterbrechung des Myometriums
Heterogeneität
dark bands
tenting
buldging Sens Spez LR+ LR- DOR
MRI 93 93 14 0.08 186
US 88 96 24 0.13 189
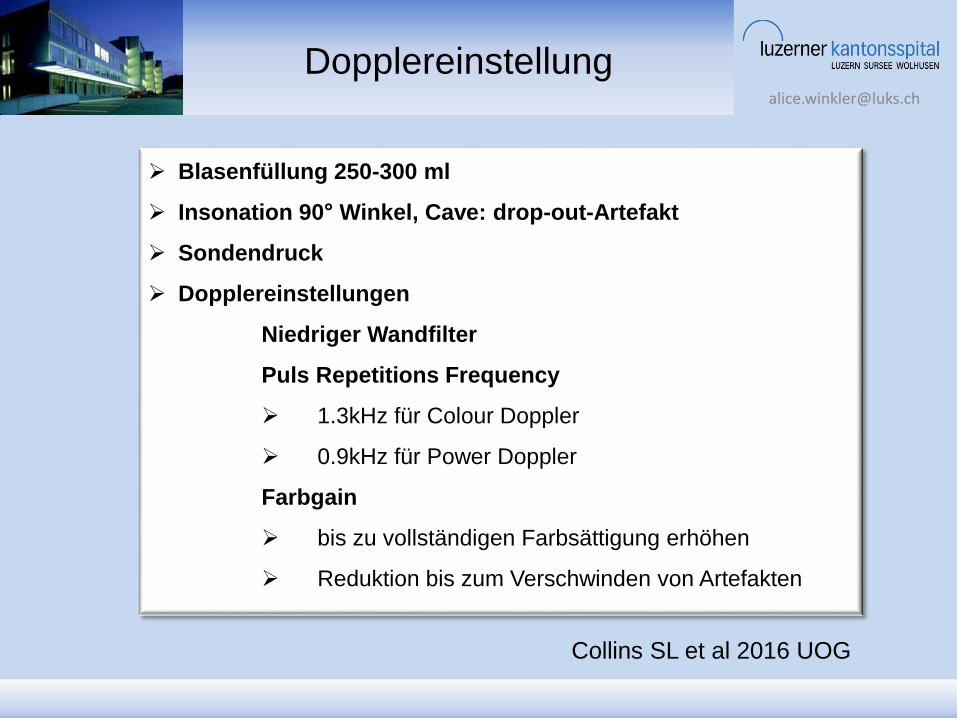
Dopplereinstellung
Blasenfüllung 250-300 ml
Insonation 90° Winkel, Cave: drop-out-Artefakt
Sondendruck
Dopplereinstellungen
Niedriger Wandfilter
Puls Repetitions Frequency
1.3kHz für Colour Doppler
0.9kHz für Power Doppler
Farbgain
bis zu vollständigen Farbsättigung erhöhen
Reduktion bis zum Verschwinden von Artefakten
Collins SL et al 2016 UOG

Standardisierte Anamnese
Risikofaktoren
St.n. Sektio(-nes)
St.n. (Saug-)Curettage
St.n. abnorm invasiver Plazenta
St.n. Myomektomie
St.n. Endometriumablation
IVF
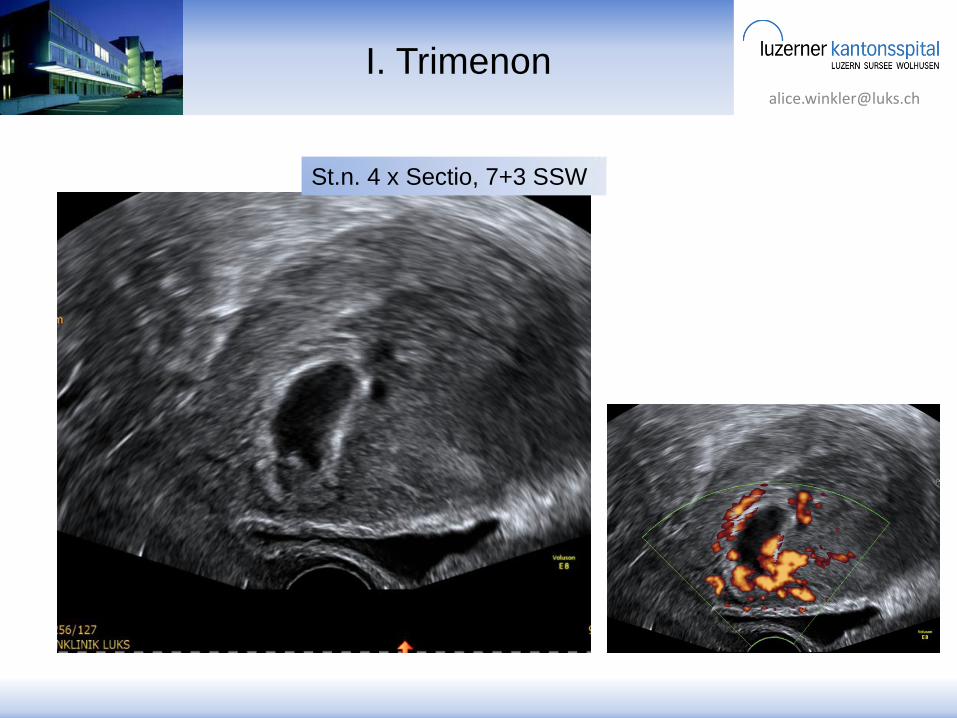
Narbenschwangerschaft I. Trim.
Prävia
European Working Group on AIP 2015
Standardisierte Anamnese
und Interpretation
Risikofaktoren
St.n. Sektio(-nes)
St.n. (Saug-)Curettage
St.n. abnorm invasiver Plazenta
St.n. Myomektomie
St.n. Endometriumablation
IVF
Narbenschwangerschaft I. Trim.
Prävia
European Working Group on AIP 2015
Interpretation
fokal oder diffus
Beteiligung
Parametrien
Niedriges,
intermediäres,
hohes Risiko
Inzidenz
1950 1 : 25000
1980 1 : 2500
2005-2010 1 : 550
Comstock et al 2005 UOG
Collins SL et al 2016 UOG
St.n. 1x Sectio Risikoanstieg bis 3%
St.n. 4x Sectio Risikoanstieg bis 70%
Plazenta Prävia: in 9% d.F. Accreta
Keine Prävia: in 0,004% d.F. Accreta
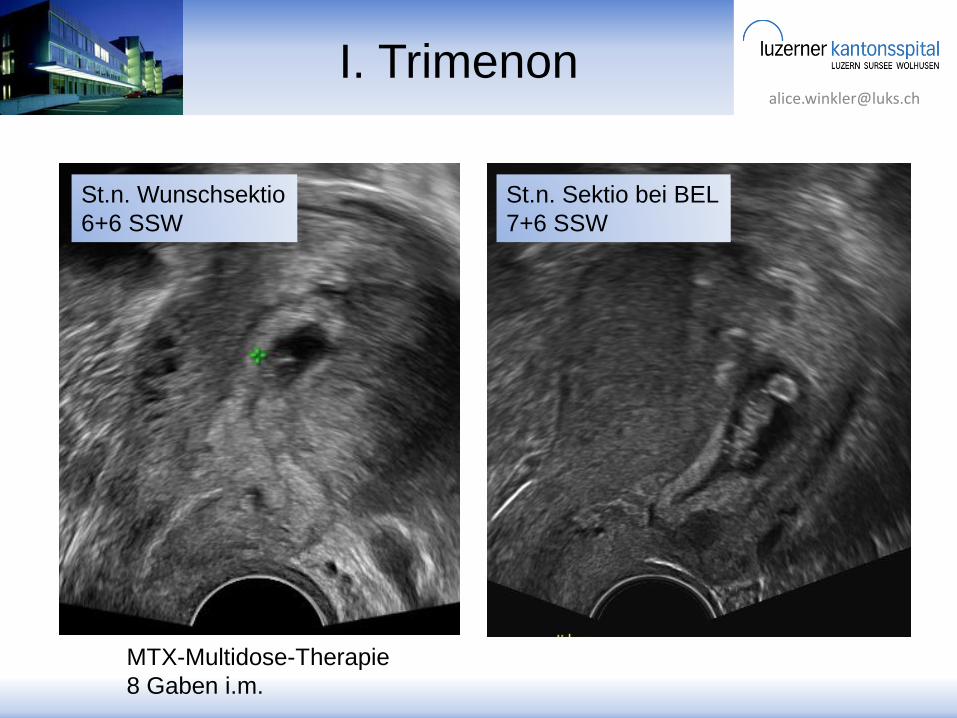
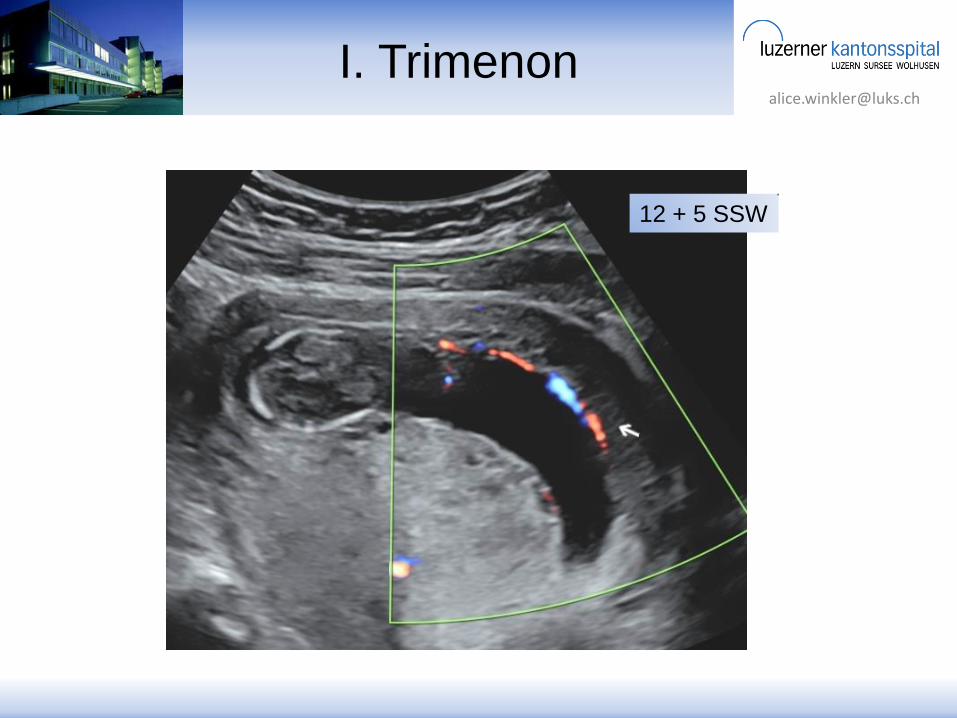
I. Trimenon
MTX-Multidose-Therapie
8 Gaben i.m.
St.n. Wunschsektio
6+6 SSW
St.n. Sektio bei BEL
7+6 SSW


















