State of the art der Bluttransfusion bei akuter Blutung ... · Schaf zu Mensch 1667 Denis J. Philos...
50
State of the art der Bluttransfusion bei akuter Blutung / perioperativ. Martin Brüesch / Donat R. Spahn
Transcript of State of the art der Bluttransfusion bei akuter Blutung ... · Schaf zu Mensch 1667 Denis J. Philos...

State of the art der Bluttransfusion
bei akuter Blutung / perioperativ.
Martin Brüesch / Donat R. Spahn

Conflict-of-Interest

"Die Transfusion ist einer der
sichersten chirurgischen Eingriffe.
Die Sterberate liegt bei einem von
drei Patienten. Damit ist sie noch
niedriger als nach der Behandlung
von Eingeweidebrüchen und
entspricht etwa der Sterberate von
Amputationen. "
1. Transfusion von
Schaf zu Mensch
1667
Denis J. Philos Trans R Soc Lond (1667) 3: 489

Gravitator
Blundell J. Med Chir Trans (1819) 10: 296
Blundell J. Lancet (1829) 1: 431


Hygiene Institut der Universität Wien (um 1900)

Karl Landsteiner
(1868-1943)
Nobel Preis 1930
Why bother about allogeneic blood transfusions ?
Intermittent blood shortages
Adverse effects / risks
High costs
Questionable efficacy
Hemodilution tolerance
Public concern
Spahn D.R. et al. Anesthesiology (2000) 93: 242
Eaton L. BMJ (2004) 329: 308
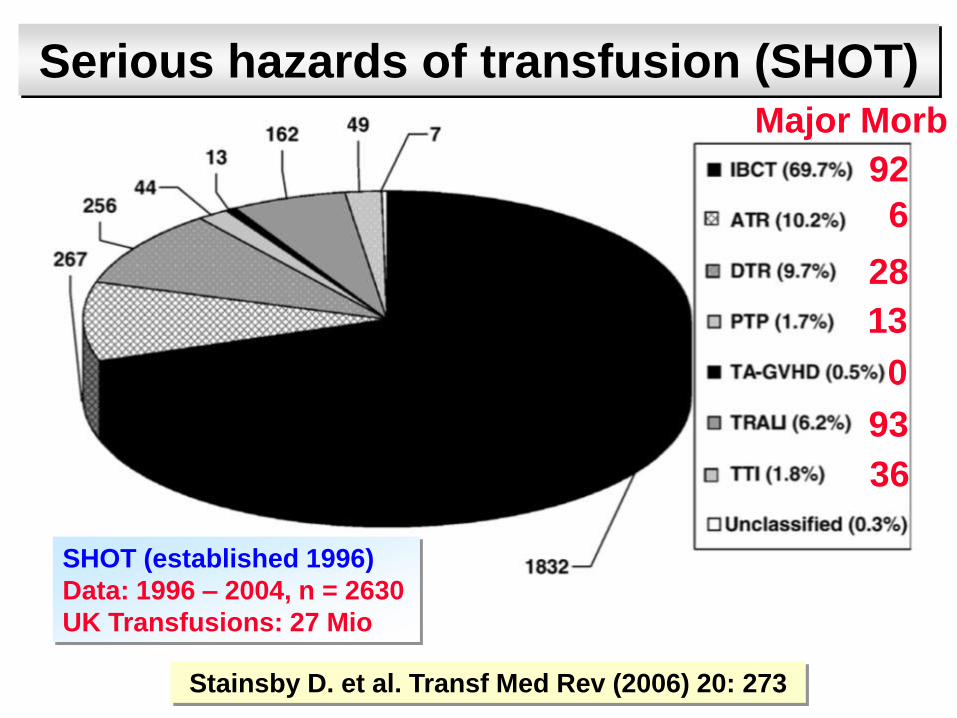
Stainsby D. et al. Transf Med Rev (2006) 20: 273
Serious hazards of transfusion (SHOT)
SHOT (established 1996)
Data: 1996 – 2004, n = 2630
UK Transfusions: 27 Mio
92
6
28
13
0
93
36
Major Morb

Adverse effectsAcute reactionsMistransfusions 1:14’000-26’000Transmission of infectious diseases HIV, Hepatitis B, C, HTLV I, II Hepatitis E, G, TT virus, HHV8, unknown virus Parasitic and bacterial diseases Prion diseases (February and August 2004) 4 cases
Immunosuppression Increased cancer recurrence Increased postoperative infections
Transfusion related acute lung injury TRALITransfusion related circulatory overload TACO
Spahn D.R. et al. Anesthesiology (2000) 93: 242
Llewelyn, C. A., et al., Lancet (2004) 363: 417 (+ editorial Aguzzi 411)
Peden A.H. et al. Lancet (2004) 364: 527 (+ editorial Wilson 477)
Rana R. et al. Transfusion (2006) 46: 1478

TRALI
Lindgren L. et al. Acta Anaesthesiol Scand (1996) 40: 641
Silliman C.C. et al. Blood (2005) 105: 2266
Crit Care Med (2006) 5 Suppl.

Transfusion Related Acute Lung Injury
« TRALI is the leading cause of transfusion associated mortality »
Incidence 1:5’000 – with 25 mio transfusion per year in the US – 5000 cases
With a mortality of 6% - 300 deaths annually
FDA conference on TRALI in 2004
National Heart Lung and Blood Institute convened a working group to identify areas of research need
First step: Creating a common clinical definition
Toy P. et al. Crit Care Med (2005) 33: 721
Silliman C.C. et al. Blood (2005) 105: 2266
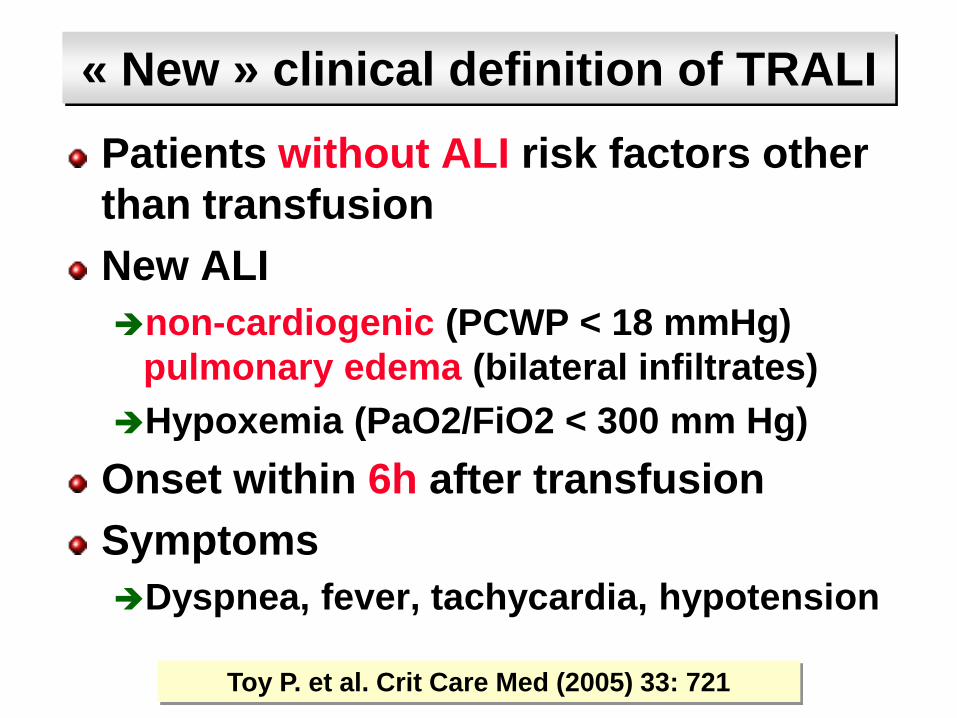
« New » clinical definition of TRALI
Patients without ALI risk factors other
than transfusion
New ALI
non-cardiogenic (PCWP < 18 mmHg)
pulmonary edema (bilateral infiltrates)
Hypoxemia (PaO2/FiO2 < 300 mm Hg)
Onset within 6h after transfusion
Symptoms
Dyspnea, fever, tachycardia, hypotension
Toy P. et al. Crit Care Med (2005) 33: 721
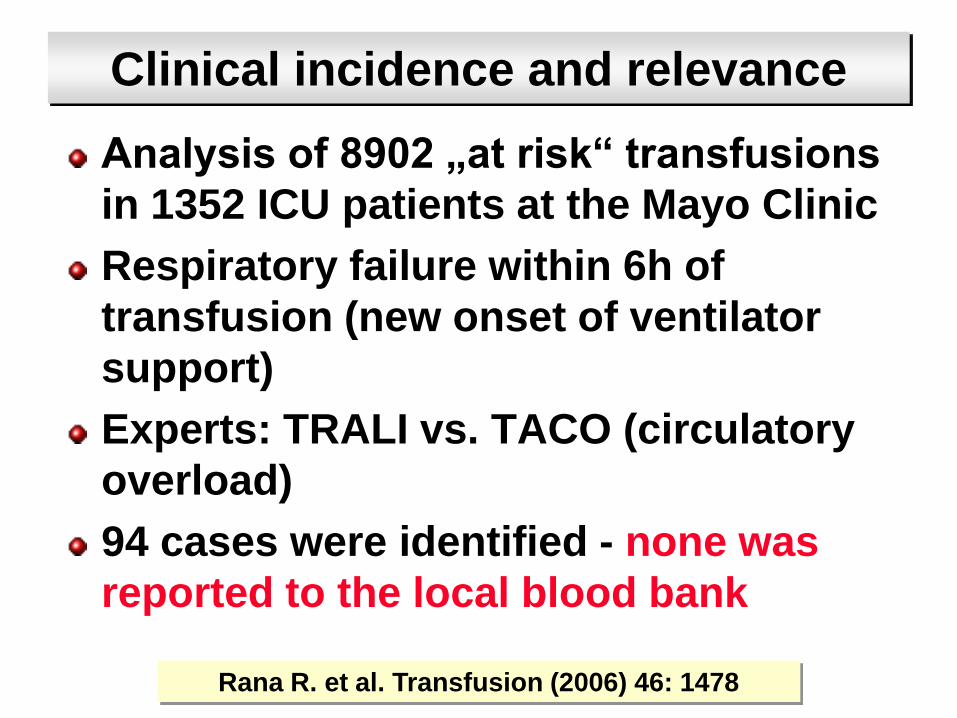
Clinical incidence and relevance
Analysis of 8902 „at risk“ transfusions
in 1352 ICU patients at the Mayo Clinic
Respiratory failure within 6h of
transfusion (new onset of ventilator
support)
Experts: TRALI vs. TACO (circulatory
overload)
94 cases were identified - none was
reported to the local blood bank
Rana R. et al. Transfusion (2006) 46: 1478

Clinical incidence and relevance
Transfusion of:
5044 RBC
2745 FFP
885 Platelet
228 Cryoprecipitate
Incidence of suspected TRALI 1: 1271
Incidence of possible TRALI 1: 534
Incidence of TACO: 1: 356
Mortality: TRALI: 67%, TACO: 20%, Control: 11%
Rana R. et al. Transfusion (2006) 46: 1478

TRALI in a Medical ICU (n=841)
Khan H. et al. Chest (2007) 131: 1308
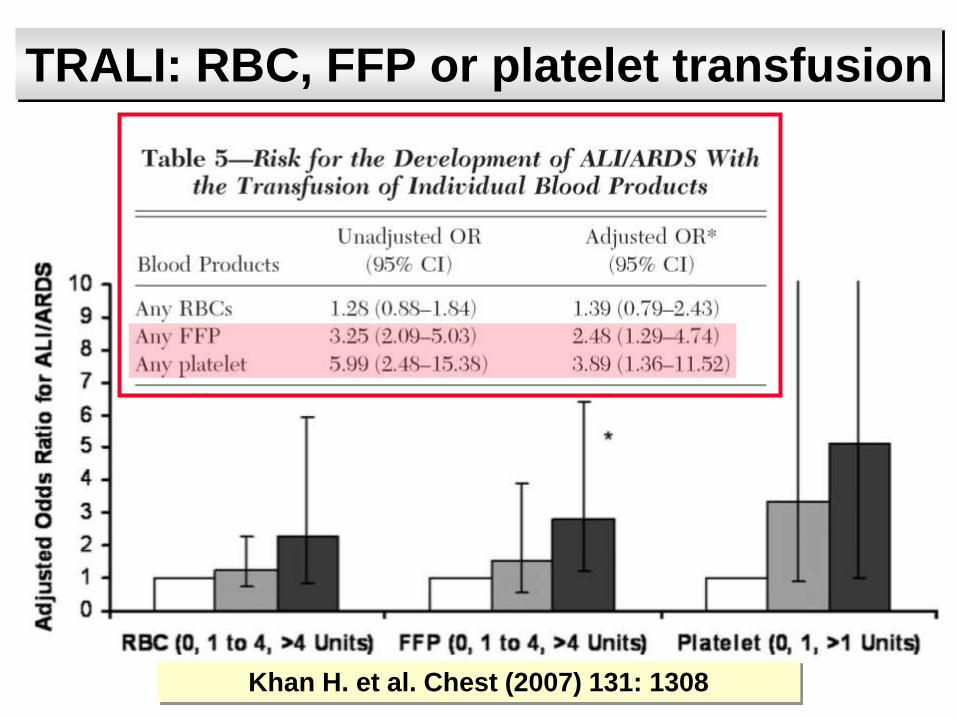
TRALI: RBC, FFP or platelet transfusion
Khan H. et al. Chest (2007) 131: 1308
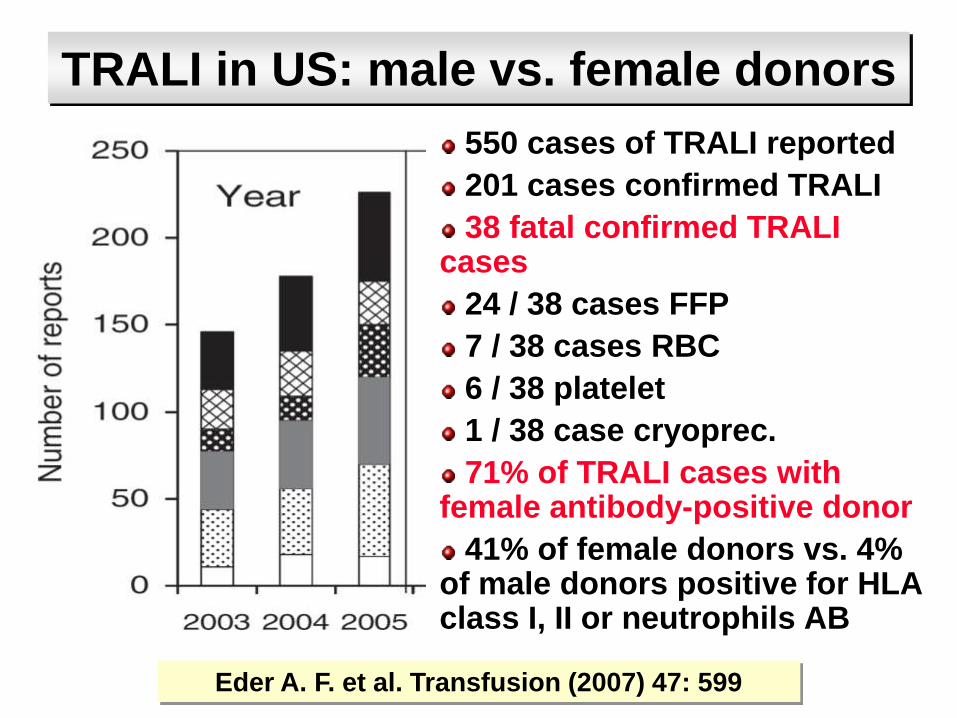
TRALI in US: male vs. female donors
550 cases of TRALI reported
201 cases confirmed TRALI
38 fatal confirmed TRALI cases
24 / 38 cases FFP
7 / 38 cases RBC
6 / 38 platelet
1 / 38 case cryoprec.
71% of TRALI cases with female antibody-positive donor
41% of female donors vs. 4% of male donors positive for HLA class I, II or neutrophils AB
Eder A. F. et al. Transfusion (2007) 47: 599
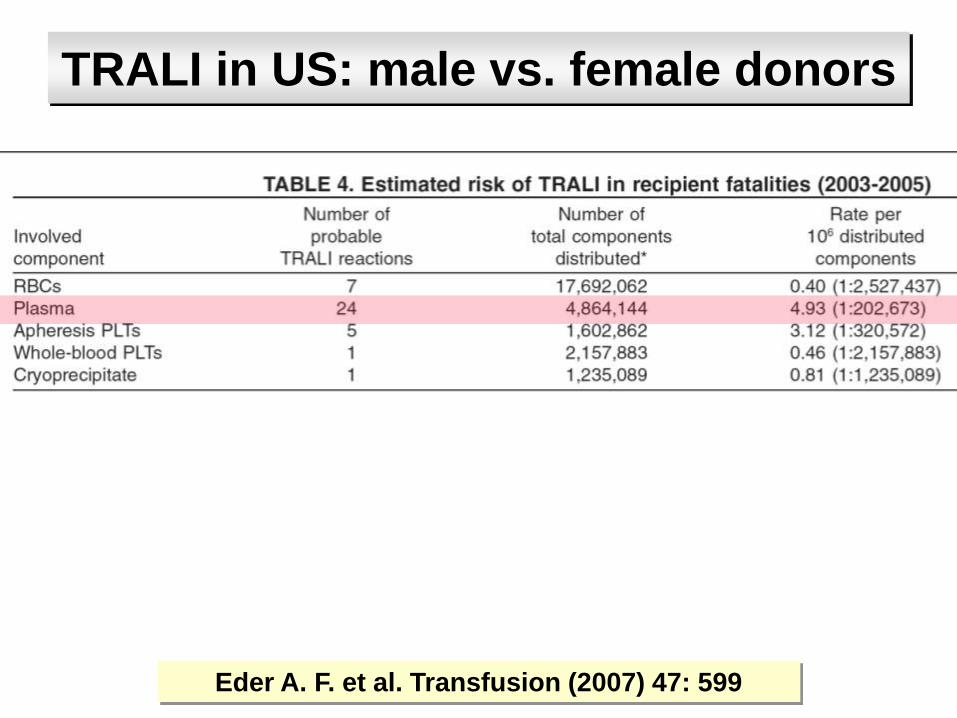
TRALI in US: male vs. female donors
Eder A. F. et al. Transfusion (2007) 47: 599

TRALI in US: male vs. female donors
Eder A. F. et al. Transfusion (2007) 47: 599
TRALI fatalities: 1:200‘000
Underreporting
Stroncek D. F. and Klein H. G. Transfusion (2007) 47: 559
Triulzi D. J. et al. Transfusion (2007) 47: 563

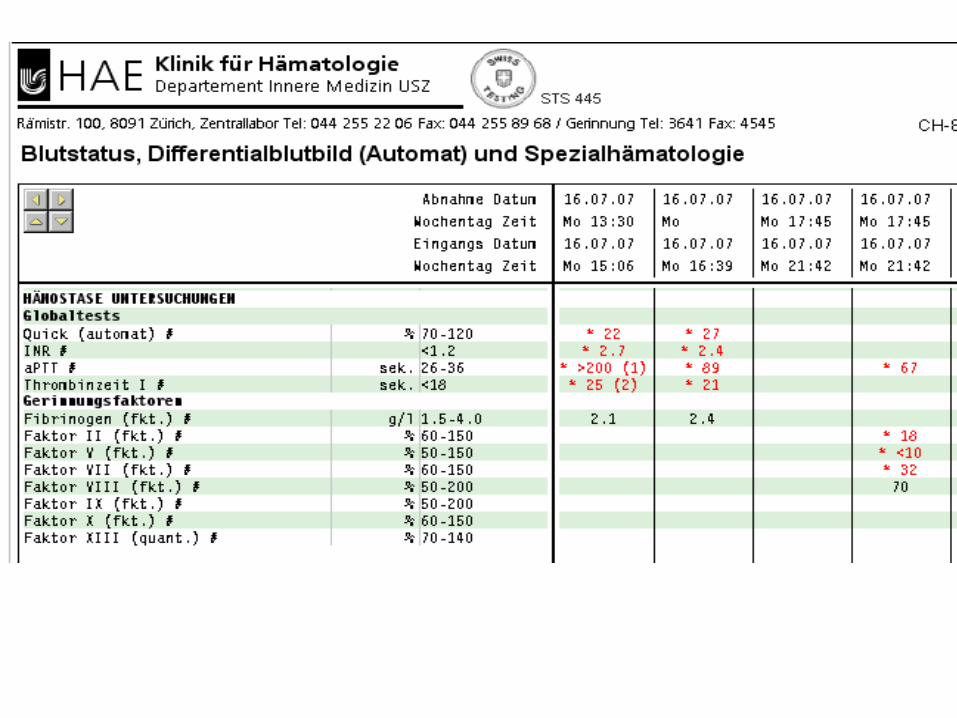
Fresh Frozen Plasma
Indikationen:
Massive Blutung (Blutverlust > 120%), wenn
korrekte Gerinnungstherapie
Faktor V und Faktor XI Mangel
Thrombotisch-thrombozytopenische
Purpura
Leberparenchymerkrankungen mit
Koagulopathie
DIC


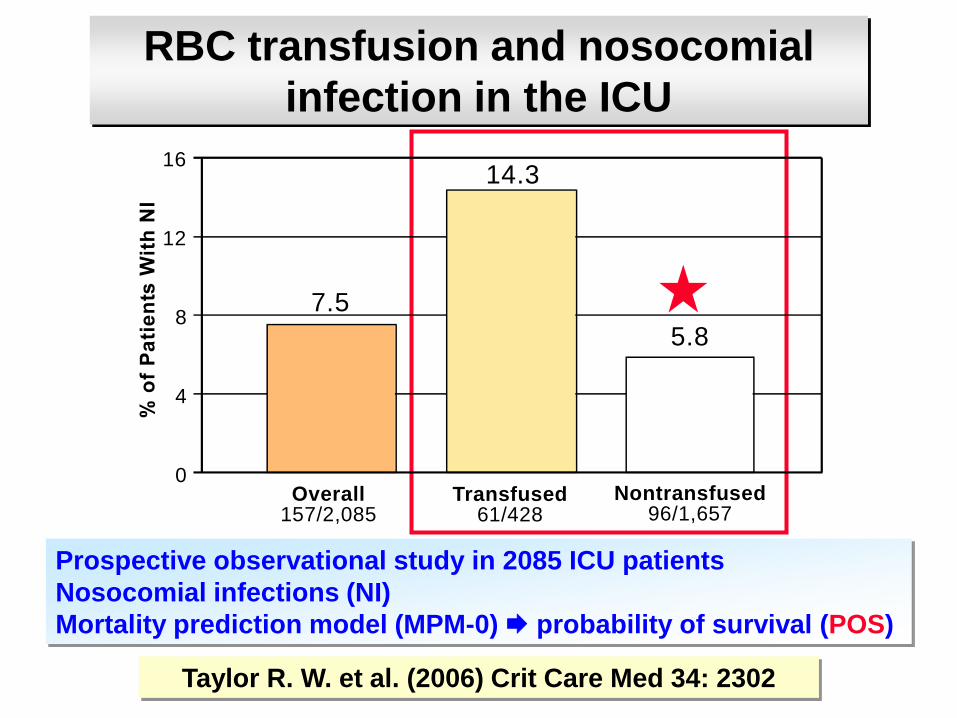
RBC transfusion and nosocomial
infection in the ICU
Taylor R. W. et al. (2006) Crit Care Med 34: 2302
Prospective observational study in 2085 ICU patients
Nosocomial infections (NI)
Mortality prediction model (MPM-0) probability of survival (POS)
16
12
8
4
0
7.5
14.3
5.8
Overall157/2,085
Transfused61/428
Nontransfused96/1,657
Efficacy of RBC transfusion
Mortality
Morbidity
Function of the organism
Organ function
Indications for RBC transfusions
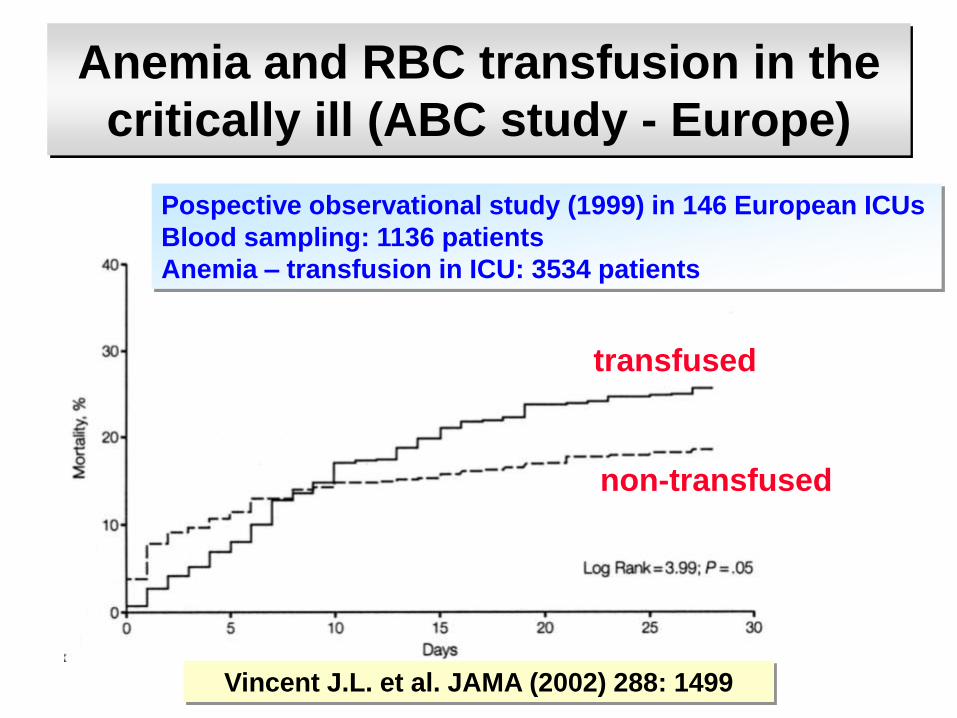
Anemia and RBC transfusion in the
critically ill (ABC study - Europe)
Vincent J.L. et al. JAMA (2002) 288: 1499
Pospective observational study (1999) in 146 European ICUs
Blood sampling: 1136 patients
Anemia – transfusion in ICU: 3534 patients
transfused
non-transfused
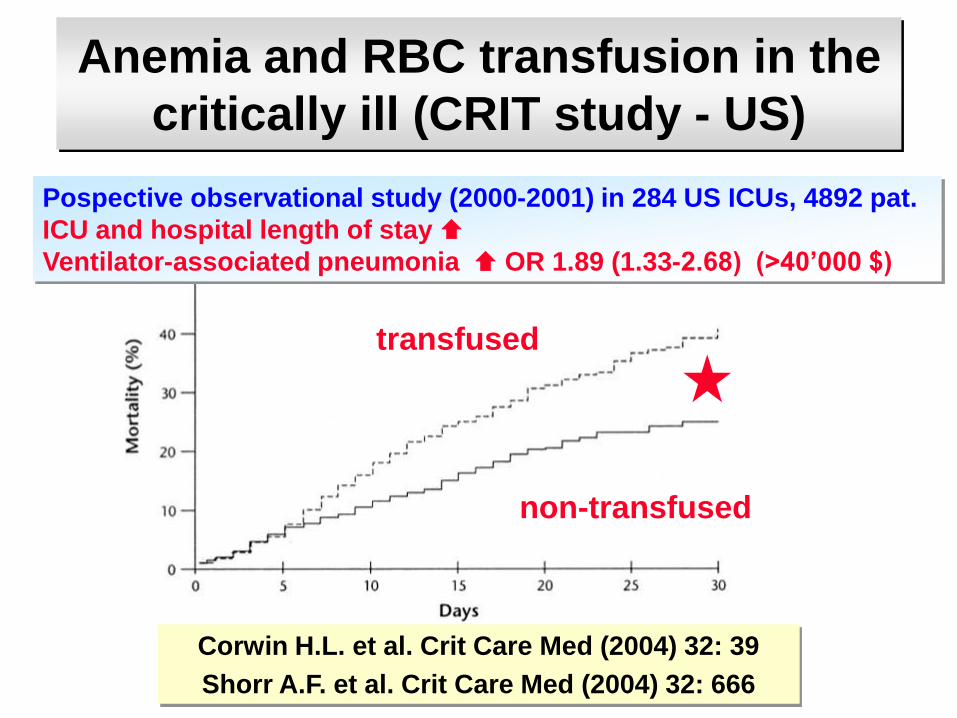
Anemia and RBC transfusion in the
critically ill (CRIT study - US)
Pospective observational study (2000-2001) in 284 US ICUs, 4892 pat.
ICU and hospital length of stay
Ventilator-associated pneumonia OR 1.89 (1.33-2.68) (>40’000 $)
transfused
non-transfused
Corwin H.L. et al. Crit Care Med (2004) 32: 39
Shorr A.F. et al. Crit Care Med (2004) 32: 666
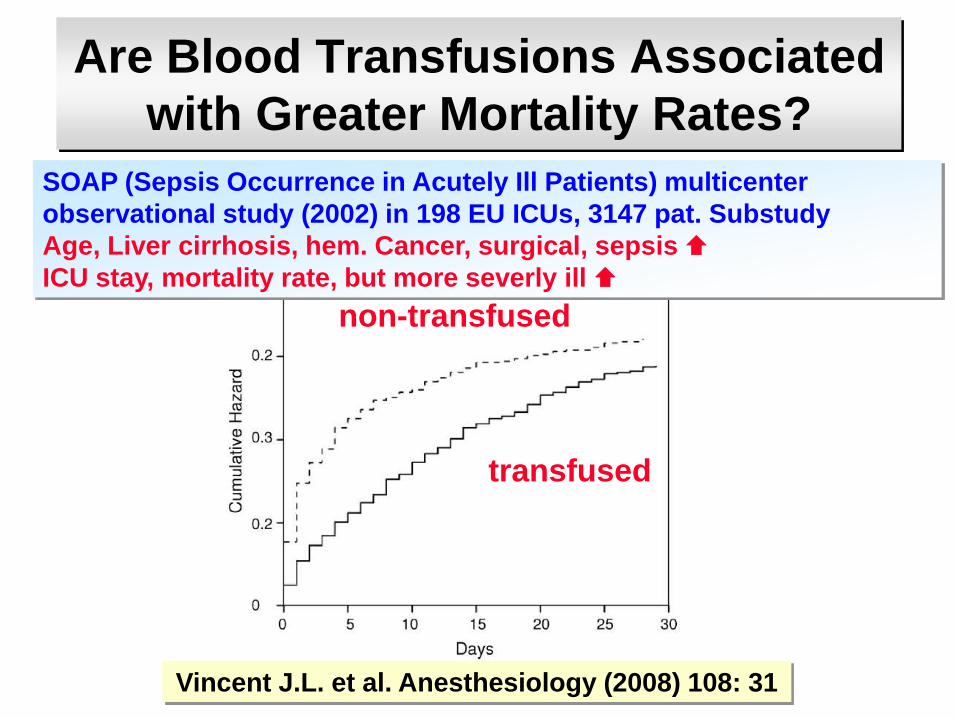
Are Blood Transfusions Associated
with Greater Mortality Rates?
SOAP (Sepsis Occurrence in Acutely Ill Patients) multicenter
observational study (2002) in 198 EU ICUs, 3147 pat. Substudy
Age, Liver cirrhosis, hem. Cancer, surgical, sepsis
ICU stay, mortality rate, but more severly ill
transfused
non-transfused
Vincent J.L. et al. Anesthesiology (2008) 108: 31

Nuttall G. A. Anesthesiology (2008) 108: 3
„Therefore, the limitations discussed
above suggest that the results
reported by Vincent et al. must be
interpreted with caution.“

RBC transfusion: benefit or harm ?
Transfused patients were
Older
Lower admission hemoglobin
Higher admission lactate
More frequently in shock at admission
SOFA score
APACHE II score
ISS score
Spahn D.R. et al. Critical Care (2004) 8: 89
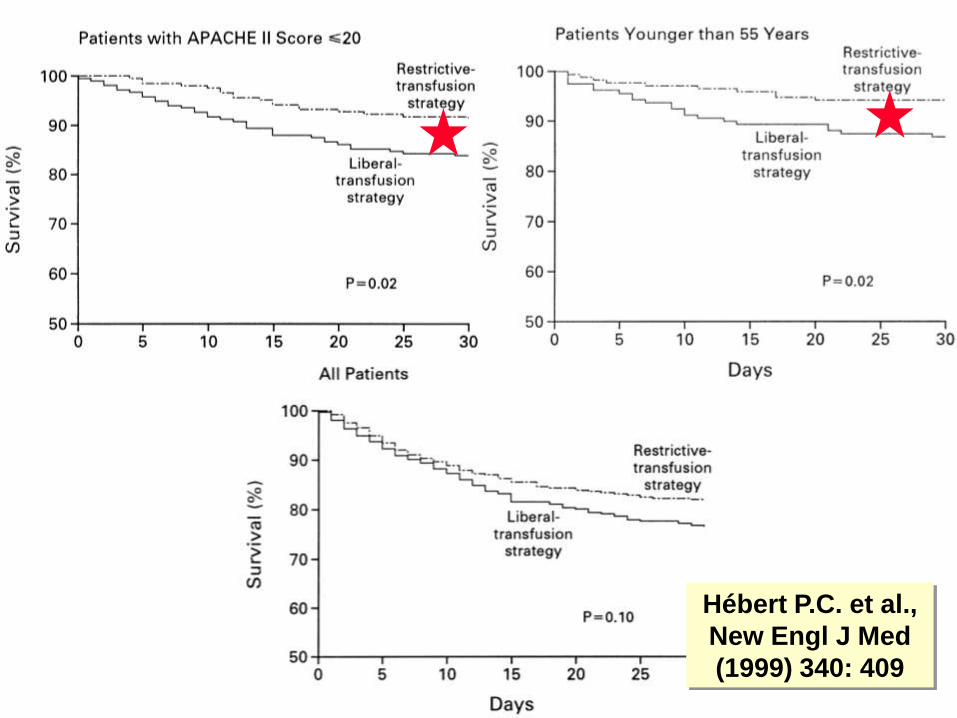
Hébert P.C. et al.,
New Engl J Med
(1999) 340: 409
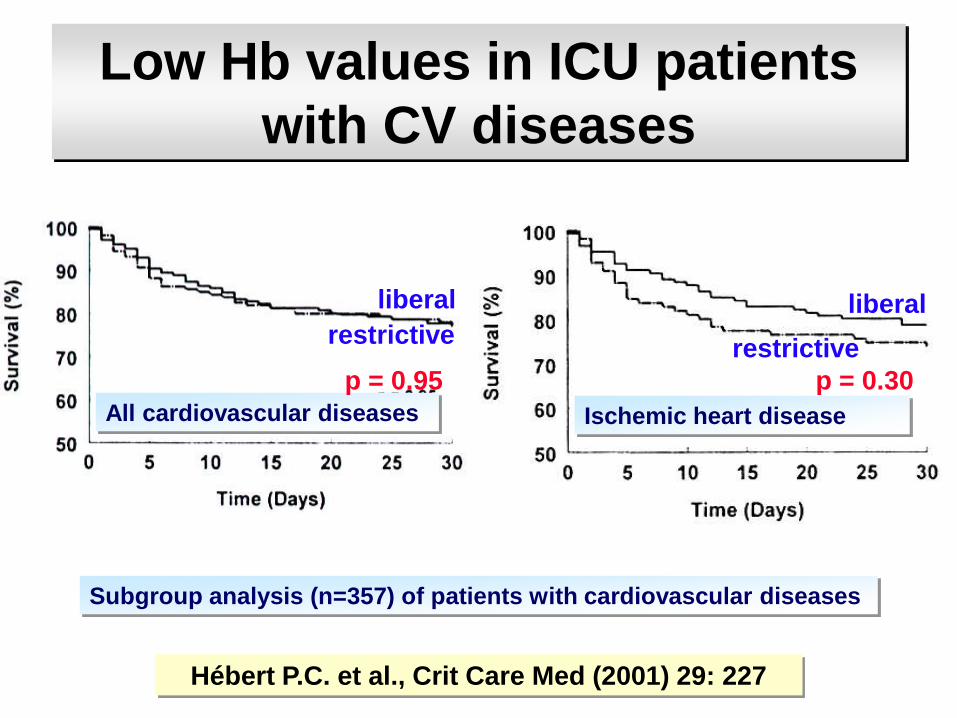
Low Hb values in ICU patients
with CV diseases
Subgroup analysis (n=357) of patients with cardiovascular diseases
Hébert P.C. et al., Crit Care Med (2001) 29: 227
All cardiovascular diseases Ischemic heart disease
p = 0.95 p = 0.30
liberal
restrictiverestrictive
liberal

Lacroix J. et al. New Engl J Med (2007) 356: 1609
RBC transfusions in children
637 stable critically ill children (3 days – 14
years) with Hb < 9.5 g/dL
Transfusion trigger: < 7.0 g/dL vs. < 9.5 g/dL
Lowest Hb: 8.7±0.4 vs. 10.8 ± 0.5 g/dL, p< 0.001
Restrictive Group:
44% fewer RBC transfusions
No RBC transfusions: 54% vs. 2%
New or progressive MOF: 38 vs. 39 cases
Mortality: 14 vs. 14 cases
RBC: prestorage leukocyte-reduced
Lacroix J. et al. New Engl J Med (2007) 356: 1609

Perioperative blood conservation
Correction of preoperative anemia
Incidence, type of anemia – treatment options
Minimizing RBC loss during
Optimal surgical technique
Cell salvage
ANH – compensatory mechanisms
Tolerance of minimal Hb levels
Prevention of coagulopathy
Anesthesiological techiques (FiO2, MAP, CVP)
Pharmacologic agents (Fg, antifibrinolytics, rFVIIa)
Optimizing blood transfusion practice
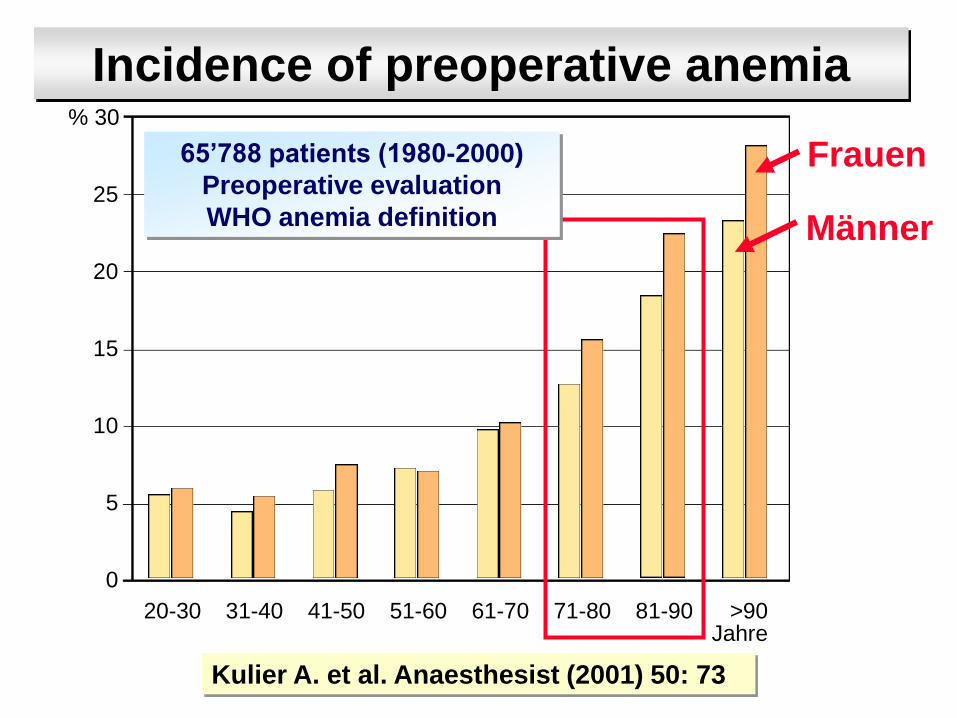
% 30
25
20
15
10
5
0
20-30 31-40 41-50 51-60 61-70 71-80 81-90 >90 Jahre
Incidence of preoperative anemia
Kulier A. et al. Anaesthesist (2001) 50: 73
Frauen
Männer
65’788 patients (1980-2000)
Preoperative evaluation
WHO anemia definition
Preoperative EPO
Preoperative iron deficiency anemia
Treatment with iv iron
Pilot study in orthopedic surgery
20 patients with iron deficiency anemia
Hb < 12 g/dl in women
Hb < 13 g/dl in men
3 x 300 mg iron iv (10 days)
Theusinger O. M. et al. Anesthesiology (2007) 107: 923
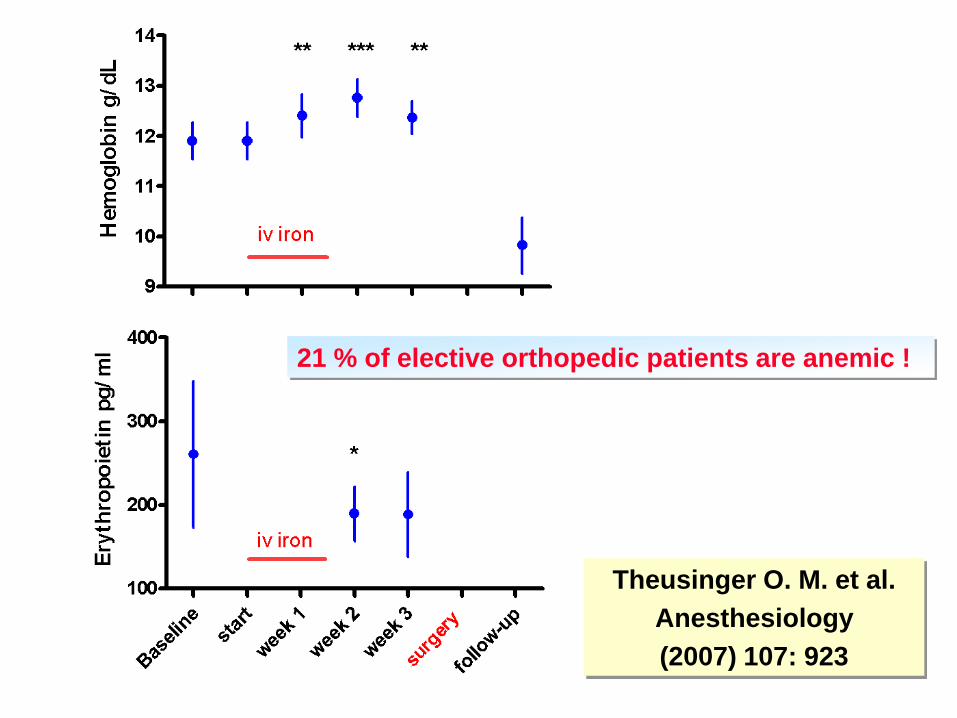
21 % of elective orthopedic patients are anemic !
Theusinger O. M. et al.
Anesthesiology
(2007) 107: 923
4804 patients for CABG surgery
72 institutions, 17 countries
28% of male and 36% of female
patients were anemic (WHO)
Prespecified adverse outcomes
Kulier A. et al. Circulation (2007) 116: 471

Kulier A. et al. Circulation (2007) 116: 471
Adverse outcome and preop. Hb
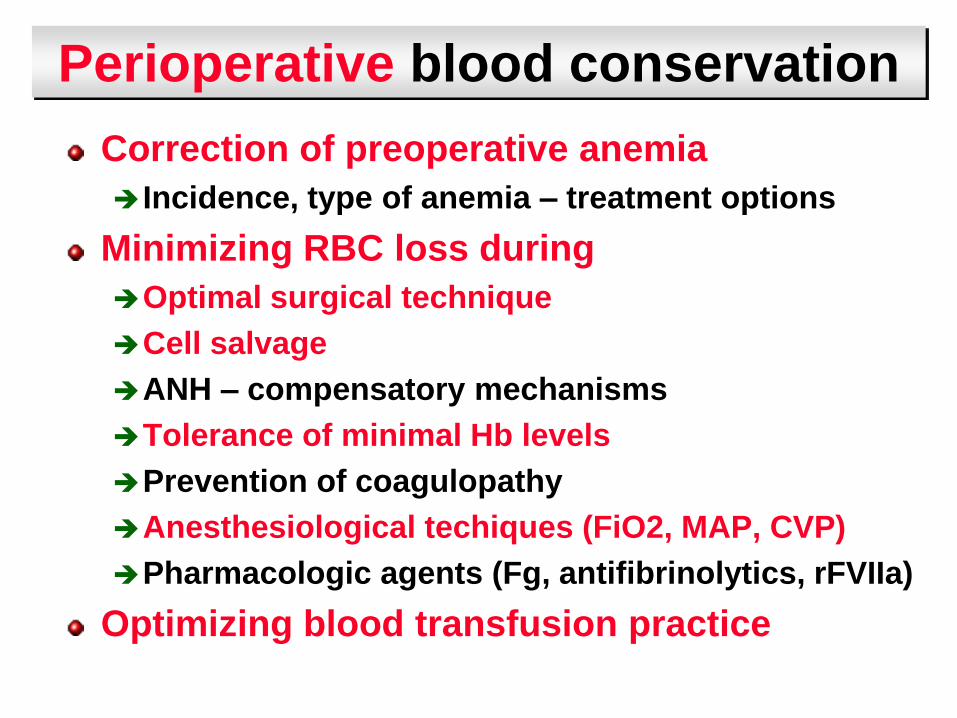
Perioperative blood conservation
Correction of preoperative anemia
Incidence, type of anemia – treatment options
Minimizing RBC loss during
Optimal surgical technique
Cell salvage
ANH – compensatory mechanisms
Tolerance of minimal Hb levels
Prevention of coagulopathy
Anesthesiological techiques (FiO2, MAP, CVP)
Pharmacologic agents (Fg, antifibrinolytics, rFVIIa)
Optimizing blood transfusion practice

Physiologic transfusion triggers
Physiologic signs of insufficient
oxygenation of an organ / organism
Hemoglobin based transfusion trigger
Hemoglobin < (arbitrary) threshold
Spahn D.R. and Madjdpour C. Anesthesiology (2006) 104: 905
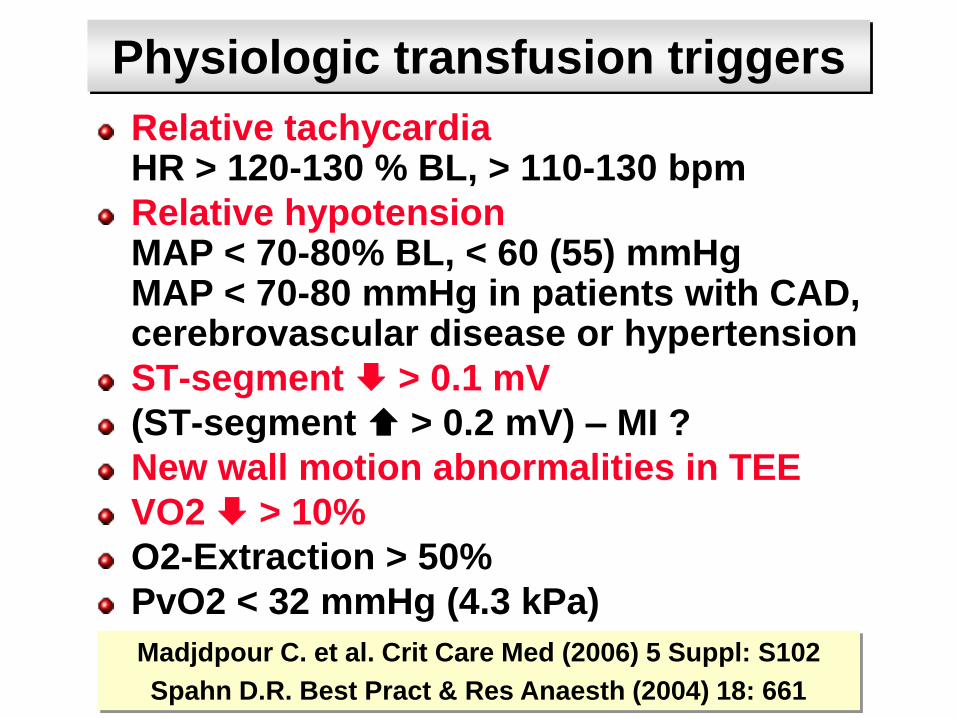
Physiologic transfusion triggers
Relative tachycardiaHR > 120-130 % BL, > 110-130 bpm
Relative hypotensionMAP < 70-80% BL, < 60 (55) mmHgMAP < 70-80 mmHg in patients with CAD, cerebrovascular disease or hypertension
ST-segment > 0.1 mV
(ST-segment > 0.2 mV) – MI ?
New wall motion abnormalities in TEE
VO2 > 10%
O2-Extraction > 50%
PvO2 < 32 mmHg (4.3 kPa)
Madjdpour C. et al. Crit Care Med (2006) 5 Suppl: S102
Spahn D.R. Best Pract & Res Anaesth (2004) 18: 661

Hb TT – Evidence and Reality
Evidence Reality in hospital
publ./teaching
OR / ICU Ward
All patients 6 g/dL 6-7 g/dL 7-8 g/dL
> 80 years 7-8 g/dL 8-9 g/dL
Severe CAD 8 g/dL 8-9 g/dL
Signs of CHF 8 g/dL 8-9 g/dL
Cerebro-VD 8 g/dL 8-9 g/dL
> 1 catechol 8 g/dL na
SaO2 < 90% 8-9 g/dL 9 g/dL
Madjdpour C. et al. Crit Care Med (2006) 5 Suppl: S102
Spahn D.R. Best Pract & Res Anaesth (2004) 18: 661