Tumor markers
62
Tumor Markers Guide: Dr. K.K.Kulkarni
-
Upload
appy-akshay-agarwal -
Category
Health & Medicine
-
view
14 -
download
3
Transcript of Tumor markers
Tumor Markers
Tumor Markers
Guide: Dr. K.K.Kulkarni
contents IntroductionDefinitionHistorical backgroundProperties of Ideal TMClassificationClinical applicationsSalient features of Individual TMMethods of detectionsTM & associated cancerRecent advances
IntroductionA major challenge in the management of patients with cancer is the lack of specific tools for The early detectionAccurate prediction of biological behavior Accurate assessment of prognosis.
Role of a Tumour marker Tumor markers can play a crucial role in detecting disease and assessing response to therapy
DefinitionAny cell product , viz, enzymes, serum proteins, metabolites, receptors, oncoproteins, oncofoetal proteins , can be used as a marker to diagnose the presence of a malignancy, as long as it is related to any event during tumour formation, proliferation, dedifferentiation, etc.A substance present in or produced by a tumorOR A substance produced by the host in response to the tumors presence
Historical background1846 Bence jones first identified BJ protein in urine of patients of MM1930-1990- Acid phosphatase served as marker for prostate cancer1960 radioimmunoassay 1963 AFP & 1965- CEA discovered as tumour marker for HCC & colon cancer respectively.1975- monoclonal Abs tech was developed which facilitates the discovery of new tumor markers including CA125, CA15.3, CA19.9
Historical background cont.1980 PSA Best cancer marker was discovered1970s & 1980s new concepts oncogenes and tumor suppressor genes came into picture.2001- Microarrays, Mass Spectrometry, Neural Networks, Multiparametric Analysis
Ideal tumour markerHighly sensitive Highly specific 100% accurate in differentiating between healthy individuals and tumor patients.Differentiate neoplastic and non-neoplastic disease show positive correlation with tumor volume and extent.Predict early recurrence and have prognostic value.Detectable at early stage of tumorIts levels should be preceding the neoplastic process. short half life to rapidly mirror treatment schedulesMeasured easily, reliably and cost-effectively using an assay with high analytic sensitivity and specificity.
ClassificationOncofetal antigens: AFP, CEATumor associated antigens : CA125, CA19-9, CA15-3, CA72-4, CA50 Hormones: -hCG, CalcitoninReceptors : ER, PR, EGFR Enzymes and Isoenzymes : PSA, PAP, NSE, PALP, Serum and tissue proteins : -2 microglobulin, monoclonal immunoglobulin/para proteins, GFAP, protein S-100, ferritin, fibrinogenOther biomolecules: polyaminesOncogenes: Ras, myc ,abl-bcrTumour supressor genes: BRCA1 , P53, Rb
Clinical Applications
Role in ScreeningTumor markers play a limited role for tumor screening, just because.relatively low sensitivitylack of specificity Not elevated in early stage Inappropriate for the detection of small in situ cancerExamples Used as screening tool:AFP in liver cancer in ChinaUrinary VMA and homovanillic acid for neuroblastoma in Japanese children PSA along with DRE for prostate cancer in >50 yr aged men
Role in DiagnosisMost tumor marker levels alone are often insufficient to diagnose cancer for the following reasons:TM levels can be elevated in people with benign conditions; TM levels are not elevated in every person with cancer, especially in the early stages of the disease; Many TM are not specific to a particular type of cancer;The level of a TM can be elevated by more than one type of cancer Tumor marker is not the key diagnostic tool, but can be a complementary sign to clinical finding & medical imagingAFP & HCC
Diagnosis contSeveral approaches have been suggested recently to improve the diagnostic yield of many tumor markers: The use of multiple markers. By improving both the specificity and sensitivity of a tumor markers, as in the case of serum PSA test, involves the measurement of the velocity & the density, complex PSA level , %fPSA
Role in staging/prognosisThe pre-therapeutic level of certain tumor marker can contributes a prognostic factor because of links with... Metabolic activityTumor sizeInvasion
Eg: -High PSA preoperatively associated with high gleason score, positive surgical margins, + lymph node status
- ER +ve breast tumors have good prognosis
- C-erb-2-gene(HER-2/neu) is prognostic for ovarian & breast cancer Allow doctors to refine therapeutic strategy by selecting groups with risk of failure response to treatment
Monitoring & recurrenceOne of the most useful applicationThe serum level of tumor markers reflects the success of surgery or the efficacy of chemotherapy. If the marker level in the blood goes down, that is almost always a sign that the treatment is effective If marker level after surgery remain elevated would indicate either incomplete removal of the tumor, recurrence, or the presence of metastases. The measurement of serum tumor markers during chemotherapy also gives an indication of the effectiveness of the antitumor drug used and a guide for the selection of the most effective drug for each individual case.Eg: PSA for prostate cancer, HCG for gestational trophoblastic tumours & germ cell tumours of ovaries & testicles CA 125 for epithelial ovarian cancer
Recommendations for ordering TM tests:
Never rely on the results of a single testWhen ordering serial testing be certain to order every test from the same laboratory using the same kitBe certain that the tumour marker selected for monitoring recurrence was elevated prior to the surgeryConsider half life of tumour marker when interpreting the resultConsider how the tumour marker is metabolized or removed from the circulation
Recommendations for ordering TM tests:
Consider ordering multiple markers to improve sensitivity and specificityOrder the non specific markers for cost saving and high sensitivity Be aware of the possibility of hook effect and lastly,Be aware of possibility of ectopic markers
Biochemical markersOncofetal antigenReference rangeCancersElevated in other benign cond.ApplicationSampleAFP < 10-20ng/ml HCC, Germ cell cancer of ovaries or testes Also elevated during pregnancy, benign liver disease Diagnosis. prognosis ,monitor treatment, and determine recurrenceBloodCEA < 5 ng/mlColorectal, lung, breast, gastric, pancreatic, liver,Elevated in hepatitis, COPD, colitis, pancreatitis, and in cigarette smokers Monitor treatment and determine recurrenceBlood
Carbohydrate antigenReference rangeCancersElevated in other benign cond.ApplicationSampleCA-125< 35U/mlOvarian endometriosis, Hepatitis,cirrhosis Early pregnancyHelp diagnose, Prognosismonitor treatment, and determine recurrenceBloodCA 15-3 < 30 U/mlBreast, adenocarcinoma of colon, lung ovary, pancreas cirrhosis, acute & chronic hepatitis, Benign breast ds,SLEsarcoidosis Monitor treatment & disease progression in metastatic breast ca. for follow up to detect recurrenceBlood
Carbohydrate antigenReference rangeCancersElevated in other benign cond.ApplicationSampleCA 27.29< 0-38U/mlBreast, adenocarcinoma of colon, lung, ovary, pancreas endometriosis, Hepatitis,cirrhosis Early pregnancyuseful for predicting early recurrence in treated breast pt.BloodCA 19-9 < 30 U/mlPancreatic, colorectal and bile ducts Pancreatitis and inflammatory bowel diseaseStage disease, monitor treatment, and determine recurrenceBlood
Carbohydrate antigenReference rangeCancersElevated in other benign cond.ApplicationSampleCA 72-4(TAG-72)< 4 U/mlGastric, lung, ovary,colorectal No evidence that it is better than CA-125 but may be useful when combined with it Monitoring treatment, Blood
HormonesReference rangeCancersElevated in other benign cond.ApplicationSample HCG< 0-38U/mlTrophoblastic &Testicular Elevated in pregnancy, testicular failure diagnose,Monitortreatment, andDeterminerecurrenceBloodUrineIn CSf To detect Mets inbrainCalcitonin < 10 ng/mlMedullary thyroid caBronchogenic ca Pernicious anemia,ThyroiditisHelp diagnose, monitor treatment, and determine recurrenceBlood
EnzymesReference rangeCancersOther remarksApplicationSamplePSA< 50 yr- 50 yr -< 4 ng/mlfPSA/PSA > 0.19 Prostate BPHProstatitisWith Age Screening and help diagnosis, monitor treatment, and determine recurrenceBloodNSE < 15ng/mlNeuroblastoma small cell lung cancer, carcinoid,pheochromocytoma & other NE tumourHemolytic anemia, Hepatic failure, ESRDNeurodegenrative dsStrokeBrain injuryMonitor treatment to determine prognosisBlood
PAP another test for prostate cancer which was used before PSA test was developed. It is rarely used now because PSA is much more sensitive
Protein Reference rangeCancersOther remarksApplicationSample2m*1000-2400 ng/mlMultiple myelomaCLLlymphomaElevated in CRF & dialysis pt without cancerDetermine prognosis, monitor treatment efficasy BloodTG < 25 ng/mlThyroidElevated in graves ds, Toxic nodular gotre,thyroiditisMonitor treatment , for follow up to detect recurrenceBlood
* CSF level useful to detect metastasis in CNS
Protein Reference rangeCancersOther remarksApplicationSampleMonoclonalIGMultiple myeloma and Waldenstroms macroglobulinemiaOverproduction of an immunoglobulin or antibody, usually detected by protein electrophoresisHelp diagnose, monitor treatment, and determine recurrenceBlood, urine
Methods of detectionImmuoassay by using monoclonal AbsRIAELISAIHC: ER,PR, Her-2 neuFISH: Her-2 neu RT-PCRHPLC
Common Cancers and Associated popular TM
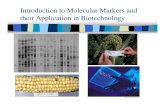
Bladder cancerAt present, no urinary tumour markers are recommended for bladder cancer screening. Bladder tumour antigen (BTA) and NMP22 can be used along with cystoscopy for diagnosis and follow-up although cystoscopy and urine cytology(gold standard) are still considered the current standard.
Sensitivity %Specificity%Method of detectionBTA55-70%70-75%EIANMP-2280-85%75-80%ELISACytology30-40%> 90%
Sensitivity is higher but specificity is lower than cytology
29
NegativePositive
Control
Test
identify urinary NMP22 levels > 10 U/ml
29
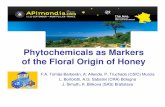
Breast cancer At present, no tumour marker has been found to be useful for screening or for diagnosis of early stage breast cancer. At the time of diagnosis, breast cancer tissue should be tested for ER & PR, as well as HER2 antigen. These markers provide information on how aggressive the cancer can be and how likely it will respond to certain treatments.Methods IHC, FISH, CISH, RT-PCR
Her 2 receptor overexpression detection
Breast cancer cont. CA15-3 and CA27.29:used to monitor therapy in Pt with advanced breast cancer .No role in screening & detection of early breast cancer. CA 27.29 has better sensitivity and specificity than CA 15-3One study - 27.29 was highly specific and sensitive in detecting preclinical metastasis, and this may lead to prompt imaging of probable sites of metastasis, possibly decreasing morbidity because of earlier treatment.FDA approved CA 27.29 for detection of recurrent breast cancer in Pts with stage II & or stage III disease.Method: ELISA using monoclonal Abs RIA
Colorectal cancerAt present, neither CEA nor CA19-9 is useful as a screening test for colorectal cancer. An elevated CEA level before surgery may indicate worse prognosis. If all the cancer has been removed, CEA should return to normal levels in about 4 to 6 weeks after treatment.CEA measurement every 3 to 6 months should be considered to help early diagnosis of recurrence. CEA is also used to monitor patients being treated for advanced or recurrent disease. If CEA is not elevated in patients with advanced or recurrent disease, CA19-9 may be used to follow the disease.
Liver cancerPeriodic screening by serum AFP measurement and ultrasound for chronic hepatitis carriers are useful to detect liver cancer at early stage. AFP can also be used to follow up patients after treatment
Lung cancerAt present, no TM have been proven to be useful as screening tests .Tumour markers that can be raised in lung cancer include CEA in non-small cell lung cancer and NSE in small cell lung cancer. Because lung cancer is usually visible on CXR or other imaging studies, TM play a less important role in follow-up.
Prostate cancerPSA is commonly used to detect prostate cancer at early stage. Levels above 4ng/ml suggest cancer whereas levels above 10 ng/ml strongly suggest cancer.PSA is very useful in follow-up. After curative surgery, PSA level should be zero or very close to zero. Those treated with radiotherapy should also have a significant drop in PSA after treatment. A subsequent rise in PSA after treatment could indicate relapse. PSA can also be used to assess response to treatment for advanced disease. In rare cases, prostate cancers that do not have raised PSA levels and do not respond well to hormonal therapy may turn out to have neuroendocrine features. Patients with these cancers may have higher levels of Chromogranin A.
Ovarian cancerCA125 is very effective to assess response of epithelial ovarian cancer to treatment or to detect recurrence. CA125 can be used to screen for ovarian cancer in women with strong family history of ovarian cancers. Such women usually receive regular ultrasounds together with CA125 measurements. Patients with ovarian germ cell tumours often have raised levels of HCG and / or AFP, which are useful in diagnosis and follow-up.
Melanoma skinAt present, no tumour marker is of value in early detection of melanoma. Tumour markers TA-90 and S-100 can be used to test tissue samples to help diagnose melanoma. Serum level of S-100 is elevated when disease is widespread. Thus it can be used to look for progression of melanoma. Blood levels of TA-90 have been used to assess the chance of metastasis of melanoma.
Tumour markers commonly elevated in patients with testicular cancer are HCG and AFP. Seminoma: About 10% of men with seminoma will have raised HCG. None will have elevated AFP. Non-seminoma: More than half of men with early stage disease have raised HCG or AFP or both. The markers will be elevated in most men with advanced disease. HCG is almost always raised and AFP is never elevated in choriocarcinoma. In contrast, AFP but not HCG is raised in yolk sac tumour or endodermal sinus tumour.
Testicular cancer
DiseaseMarkerScreeningDetection and diagnosisStaging and prognosisFollow upSarcoma:Synovial sarcomat(X;18)XXEwing's sarcomat(11;22)XAlveolar rhabdomyosarcomat(2;13)XGranolytic sarcomat((9;11)X
DiseaseMarkerScreeningDetection and diagnosisStaging and prognosisFollow upMyxoid liposarcomat(12;16)XRound cell liposarcomat(12;16)XCongenital fibrosarcomat(2;15)XClear cell sarcomat(12;22)X
DiseaseMarkerScreeningDetection and diagnosisStaging and prognosisFollow upDermatofibrosarcoma protuberanst(17;22)XMelanomaTyrosinaseXAdrenal carcinomaSteroidsXCatecholaminesX
DiseaseMarkerScreeningDetection and diagnosisStaging and prognosisFollow upLymphomat(8;14)XXXt(11;14)XXXt(2;5)XXXt(3;14)XXXsCD25XsCD44XLeukaemiaNumerous cytogenetic alterationsXX
Recent advances
Mechanisms for Induction of Carcinogenesis by Mitogenic Pathway Elements Growth factors: a. Overproduction by cell into surroundings b. Interaction of growth factors with high affinity receptorsGrowth factor a. Overexpression leading to high concentration of dimers receptor b. Loss of extracellular domain resulting in permanent dimerization of GFR and continuous signaling c. Amino acid substitutions in transmembrane domain leading to permanent dimerizationCytosolic proteins a. Overexpression of normal G-proteins and protein kinases b. Amino acid substitutions that permanently change conformation to activated form c. Mutations that remove regulatory domains of kinases
Nuclear oncoproteins a. Overexpression of transcription and replication proteins b. Mutations in antioncogene proteins that inactivate them c. Mutations that remove regulatory domains
Growth FactorsSince various growth factors are believed to play a role in influencing cellular proliferation during tumorigenesis and since growth factors are actively secreted into the extracellular environment, they are potentially attractive targets for detection in blood during cancer development.TGF & PDGFbFGFEGF & HGF
TGF & serum assays for TGF-:useful for diagnosis and follow up in HCCUseful for diagnosis of invasive bladder cancer bcz of high sensitivity and specificity TGF : useful in screening the patients for the presence of malignant tumours unlike TGF not tumour specific Effective predictor of the occurrence of malignancies at an early stage. Eg. Elevated in people with asbestosis showing progression to lung ca
PDGFSignificantly elevated in over 15% of patients with carcinomas, sarcomas, and lymphomas but not at all in normal individuals. Excellent correlation between the serum level and the stage of the breast cancer. Higher levels predict shorter survival.
bFGFMarkedly elevated in > 50% pateints of RCC Also elevated in the sera of over 50% of patients with CNS tumors, 90% of patients with lung cancers and >60% of patients with lymphomas Recently, elevated serum levels of bFGF have been found to be a good prognostic factor in patients with non-small-cell carcinomas of the lung.
Growth factor receptorTransmembrane growth factor receptors : EGFr & Her2/neu Encoded by the erbB family of oncogenes.Attractive targets for detection in blood during cancer development. Extracellular domains of these receptors enter circulation and can be detected using immunoassays.
EGFrElevations (> 636 fmol/mL) of circulating levels of ECD of EGFr ,found in patients either have an asbestos-associated malignancy or subsequently develop such malignancy. EGFr appears to be an excellent marker for asbestos-induced tumors
Her 2/neuElevated in the sera of patients with a number of different epithelial cell cancers, including breast, lung, colorectal, and ovarian cancers About 25% of patients with breast cancer over express HER2, which is associated with aggressive disease, poor clinical outcomes and shortened overall survivalSamples of tumour tissue (not blood sample) are used to test for HER2 statusClinical relevance:Correlates with poor prognosisCorrelates with lower response to endocrine therapyHer2 positive tumors often have lost expression of ER/PRPredicts response to anthracyclines through linkage to TOPO2 gene, with which it is often co-amplifiedPredicts response to targeted therapy (Trastuzumab/Herceptin)
P185 ECD of Her2/neu receptorOverexpression is accompanied by cleavage of the ECD of the receptor with its accumulation in the extracellular environment. Thus, detection of increased amounts of it in blood is a potential biomarker of cancer development.In breast cancer : serum level correlate with tumor load and stage. More sensitive ELISA assay for it, helpful in detecting carcinoma in situ .In pulmonary cancer : Markedly elevated in Pt with pnemoconioses prior to onset of frank malignancy thus it is a highly sensitive marker for pulmonary cancer
P185 ECD of Her2/neu cont.Elevated in almost 100% of East Asian poeple who have known risk factors for developing HCC. Thus good sensitive marker like TGF.Direct correlation between serum levels of p185 ECD and tumor size for premalignant adenomas of the colon . Since colonic neoplasia usually progresses through well-defined steps from adenoma to carcinoma with the malignant potential of adenomas increasing with size, serum erbB-2 ECD levels may be useful in monitoring these progression.
G protein cytosolic protein gene encoded G proteinNormally transmit growth signals from cell membrane to cytosolic kinase Overexpression AA substitution leading to mutated formUncontrolled cell division & carcinogenesis
Process is well documented for ras encoded p21 proteinMutant p21 protein abnormal activation of alternate unregulated signal transduction pathways Gain access to extracellular environment by unexplained mechanisms detected by immunoblotting with monoclonal antibodies.
Elevated serum p21 is a biomarker of early malignant disease in patients with a known predisposition. Known to be increased in patients with pneumoconiosis with later progression to cancer. Mutated p21 found in serum of patients of angiosarcoma with a known exposure to vinyl chloride. there is direct correlation between duration of exposure & occurrence of mutant p21.K-ras, mutation detected by molecular technology in stool and lavage fluid, pancreatic and duodenal juices, and sputum and lavage fluids for colorectal, pancreas and lung cancers, respectively.
Nuclear oncoproteinsImportant nuclear oncoproteins : p53 tumour supressor gene protein p62/64 protein encoded by c-myc oncogene nuclear matrix proteinsp53 Antioncogene repress mitotic process & activate proapoptotic protein which promote apoptosis in transformed cells.
mutation in p53Loss of normal growth inhibitory functionP53 proteins with increased half lives accumulate in cellsleak into extracellular environment
Increased mutant p53 found in HCC & cirrhosis which is risk factor of HCC. Thus elevated mutant p53 level in cirrhosis patient is an early indicator of carcinogenesis.In breast cancer, p53 mutation is associated with more aggressive disease and worse overall survival. Mutant p53 also found in shed cells in the urine of bladder cancer patients so these noninvasive test can be used for screening with other markers. Elevated levels of p53 antibodies are found in patients with ovarian and colon malignancies, lung ca, breast ca including intraductal ca.Anti-p53 antibodies found in patients with oral premalignant lesions - marker for early detection of oral ca.
C-myc encoded protein : P62 overexpressed in burkitts lymphoma.C-myc protein elevated in the serum of patients of breast ca & colon ca & marked diminution with treatment. so useful in following the course of these tumour.P62 overexpression seen in breast ca using IHC, staining intensity greater with increased stage of tumour. Anti c-myc protein antibodies:Found in sera of pateints with colorectal cancer, myeloid leukemia & burkitts lymphoma.
Nuclear matrix protein:NMP22 protein 10-20 times higher in malignant transitional epithelial cells than normal cells. this the basis for the detection of this protein into urine of bladder ca patients by ELISA.Sensitivity in detection of malignant invasive cancer is 90% & for ca in situ 75% specificity is 90%.Even higher sensitivity than cytology in Grade I, II,& III TCCClinical trial data showed that the NMP22 test, when performed 6-40 days post-surgery, correctly predicted the presence of recurrent disease.US FDA approved this method for screening & follow up of bladder ca patient who have been treated for this disease.
summaryTumour markers may be used to help diagnose cancer, predict and monitor response to treatment and determine whether cancer has recurred after treatment. In general, tumour markers alone cannot be used to diagnose cancer, they must be combined with other tests. Studies are being done to determine if tumour markers can be used in early detection and diagnosis of cancer.
Thank you