Corrective plastic surgery of the cleft nose
12
50 O. Neuner Wassmund, M.: Lehrbuch der praktischen Chirurgie des Mundes und der Kiefer. Bd. II, Barth/Meusser, Leipzig 1939 Wassmund, M.: Der Verschlufl des Kieferspaltes und Nasenbodens bei vollst~ndiger Spaltbildung - Zeit- punkt und Methoden. Fortschr. Kiefer- u. Gesichts- chir. 1 (1955) 27-36 Weitzel, E.: Nachuntersuchungen der yon 1. Januar 1953 bis zum 31. Dezember 1957 an der Westdeut- schen Kieferklinik operierten Lippen-Kiefer-Gau- menspalten. Inaug.Diss., Dfisseldorf 1960 Wulff, J.: Erfahrungen bei der Sprecherziehung von Gaumenspaltenpatienten. Fortschr. Kiefer- u. Ge- siehtschir. 1 (1955) 112-119 Prof. Wolfgang Koberg, M.D., D.M.D. lngolf Koblin, M.D., D.M.D., Clinic of Maxillofacial Surgery Westdeutsche Kieferklinik, 4 Diisseldorf, Moorenstrafle 5 J, max.-fac. Surg. 1 (1973) 50 61 © Georg Thieme Verlag, Stuttgart Corrective Plastic Surgery of the Cleft Nose* Otto Neuner Department of Maxillofacial Surgery (Head: Prof. O. Neuner, M.D., D.M.D.) University of Berne, Switzerland Summary I5 years' experience allows the author to state that secondary corrective plastic operations on the osseous framework, the septum and the triangular cartilage are always a must by cleft nose patients. The procedures for unilaterally or bilaterally involved nose differ, lateral deviation and asymmetry being the main de- formities in the first case, and underdeveloped septum and columella and a widened nasal tip in the second. The author describes techniques which are either en- tirely his own, or through him modified. Diagrams and clinical cases illustrate and fully explain such techniques. Key-Words: Cleft-nose correction. back because of the retral position of the alar groove. The columella is distorted. The major part of the septum is deflected to the healthy side and the anterior part to the cleft side; this leads to a deviation of the cartilaginous nose, and often also of the bony framework. Introduction Corrective nasal plastic operations are performed on cleft-patients both for functional and aesthetic reasons. With almost all degrees of cleft lip, from the notched lip to the severest form of complete bilateral cleft, we are confronted with a more or less pronounced nasal malformation. In case of a unilateral cleft lip, the lateral nose deviation and the external naris asymmetry are the main deformities. The cleft-side ala is flattened because of its far too dorsal, lateral, and deep attachment (Fig. 1). On the cleft-side the nasal tip is flat, and the nasal cavity shifted ': Paper read at the First Congress of the European Association for Maxillo-Facial Surgery, Ljubljana, Yugoslavia, 28.9.-1.10. 1972. Fig. 1 Typical nasal malformation in case of a uni- lateral cleft. In case of a bilateral cleft, the columella is gen- erally too short, so that the nasal tip snubs down towards the base of the upper lip. The alae extend much too laterally and are flattened on the groove resulting in a very wide nasal tip and very ob- lique nares (Fig. 2). An underdeveloped tip and a cartilaginous and sometimes osseous hump due to growth disturbances are present. A saddle is rarely seen. The osseous nose is almost always rather wide. As regards the appropriate time, corrective plasty of the nostrils can, as a rule, be undertaken
Transcript of Corrective plastic surgery of the cleft nose

50 O. Neuner
Wassmund, M.: Lehrbuch der praktischen Chirurgie des Mundes und der Kiefer. Bd. II, Barth/Meusser, Leipzig 1939
Wassmund, M.: Der Verschlufl des Kieferspaltes und Nasenbodens bei vollst~ndiger Spaltbildung - Zeit- punkt und Methoden. Fortschr. Kiefer- u. Gesichts- chir. 1 (1955) 27-36
Weitzel, E.: Nachuntersuchungen der yon 1. Januar 1953 bis zum 31. Dezember 1957 an der Westdeut- schen Kieferklinik operierten Lippen-Kiefer-Gau- menspalten. Inaug.Diss., Dfisseldorf 1960
Wulff, J.: Erfahrungen bei der Sprecherziehung von Gaumenspaltenpatienten. Fortschr. Kiefer- u. Ge- siehtschir. 1 (1955) 112-119
Prof. Wolfgang Koberg, M.D., D.M.D. lngolf Koblin, M.D., D.M.D., Clinic of Maxillofacial Surgery Westdeutsche Kieferklinik, 4 Diisseldorf, Moorenstrafle 5
J, max.-fac. Surg. 1 (1973) 50 61 © Georg Thieme Verlag, Stuttgart
Corrective Plastic Surgery of the Cleft Nose*
Otto Neuner
Department of Maxillofacial Surgery (Head: Prof. O. Neuner, M.D., D.M.D.) University of Berne, Switzerland
Summary I5 years' experience allows the author to state that secondary corrective plastic operations on the osseous framework, the septum and the triangular cartilage are always a must by cleft nose patients. The procedures for unilaterally or bilaterally involved nose differ, lateral deviation and asymmetry being the main de- formities in the first case, and underdeveloped septum and columella and a widened nasal tip in the second. The author describes techniques which are either en- tirely his own, or through him modified. Diagrams and clinical cases illustrate and fully explain such techniques.
Key-Words: Cleft-nose correction.
back because of the re t ra l posi t ion of the a lar groove. The columella is distorted. The m a j o r pa r t of the septum is def lected to the hea l thy side and the anter ior pa r t to the cleft side; this leads to a deviat ion of the car t i laginous nose, and often also of the bony f ramework.
Introduction
Corrective nasa l plast ic operat ions are per formed on clef t -pat ients both for funct ional and aesthetic reasons. W i t h almost al l degrees of cleft lip, from the notched lip to the severest form of complete b i la te ra l cleft, we are confronted with a more or less pronounced nasal malformat ion. In case of a un i la te ra l cleft lip, the la te ra l nose deviat ion and the external naris asymmet ry are the main deformities. The cleft-s ide ala is f la t tened because of its far too dorsal, lateral, and deep at tachment (Fig. 1). On the cleft-side the nasal t ip is flat, and the nasal cavi ty shifted
': Paper read at the First Congress of the European Association for Maxillo-Facial Surgery, Ljubljana, Yugoslavia, 28.9.-1.10. 1972.
Fig. 1 Typical nasal mal format ion in case of a uni- lateral cleft.
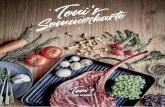
In case of a b i l a te ra l cleft, the columella is gen- e ra l ly too short, so that the nasal tip snubs down towards the base of the upper lip. The alae extend much too la te ra l ly and are f la t tened on the groove resul t ing in a very wide nasal tip and very ob- l ique nares (Fig. 2). A n underdeveloped tip and a car t i laginous and sometimes osseous hump due to growth dis turbances are present. A saddle is ra re ly seen. The osseous nose is almost a lways ra ther wide. As regards the appropr ia te time, corrective p las ty of the nostr i ls can, as a rule, be under taken
Corrective Plastic Surgery of the Cleft Nose 51
at any age, whereas the cartilaginous and osseous framework should better not be touched before the age of 15 or 16. Corrective plastic surgery of the cleft-nose, fol- lows not only the conventional principles of rhinoplasty, but also procedures specifically con- ceived for that purpose.
sliding-plasty between the inner and outer skin layers.
d) Corrections of the form, position and attach- ment of the cleft ala to match the healthy side which are generally accomplished at the same time as the lip correction (Trauner 1958, Neuner 1965, 1967).
Fig. 2 Typical nasal mal format ion in case of a bi la- teral cleft.
Corrective Operations of the Unilaterally Involved Nose
Osseous Frameworh
a) Straightening of the deviated nose: oblique, medial and asymmetrical lateral osteotomies (Neuner 1966).
b) Hump removal (if necessary), followed by oblique and lateral osteotomies (Neuner 1971b).
Nasal Septum and Triangular Cartilage
Straightening of the Septum and narrowing of the triangular cartilage.
Tip and Nostril
a) Reshaping and repositioning of the deviated alar cartilage.
b) Size reduction of both alar cartilages for nose narrowing and tip symmetrization.
c) Reshaping of the involved nostril to match the healthy side through appropriate skin, and, if" necessary, cartilage excisions and
Corrective Operations of the Bilaterally Involved Nose
Osseous Framework
a) Narrowing and straightening of saddle and flat noses; curved extended osteotomy (Neuner 1966).
b) Narrowing of the broad nose: oblique, median and lateral osteotomies and median bone re- section (Neuner 1970).
c) Removal, if necessary, of the osseous and cartilaginous hump with subsequent oblique and lateral osteotomles.
Nasal Septum and Triangular Cartilages
a) Lengthening or lowering, if necessary, of the anterior septal edge by parallel forward dis- placement of a free or pediculate cartilaginous septal band (Neuner 1970).
b) Implantation of the hump into the columella (Neuner 1970, 1971@
c) Insertion of a straight or angular free cartilage graft (Schmid 1957, Trauner 1958).
d) Reduction and narrowing of the triangular cartilages.
Tip and External Naris
a) Lengthening the membranous nasal passage. b) Raising and narrowing the tip by reshaping
and advancing medially the lateral alar limbs. Size reduction of both alar cartilages. The form, position and attachment of the alae are highly improved through steps a, b, and c. However the last touch corrections are firs1 undertaken when reoperating the lip.
c) d)
Osseous Framework
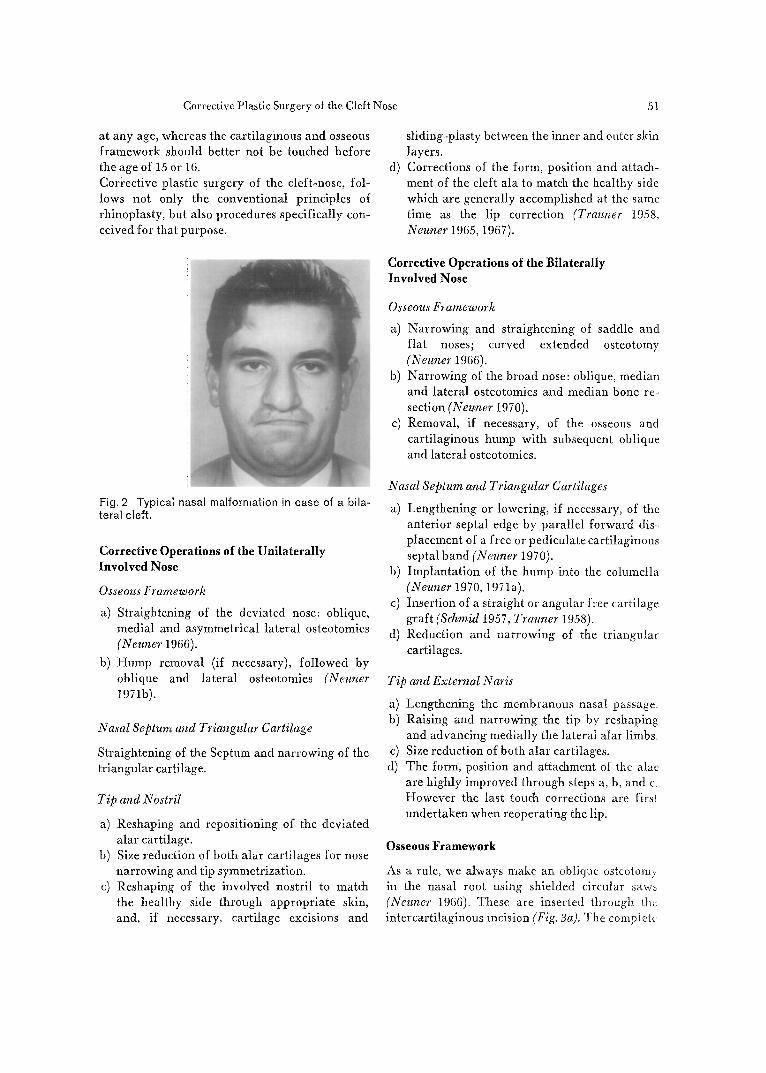
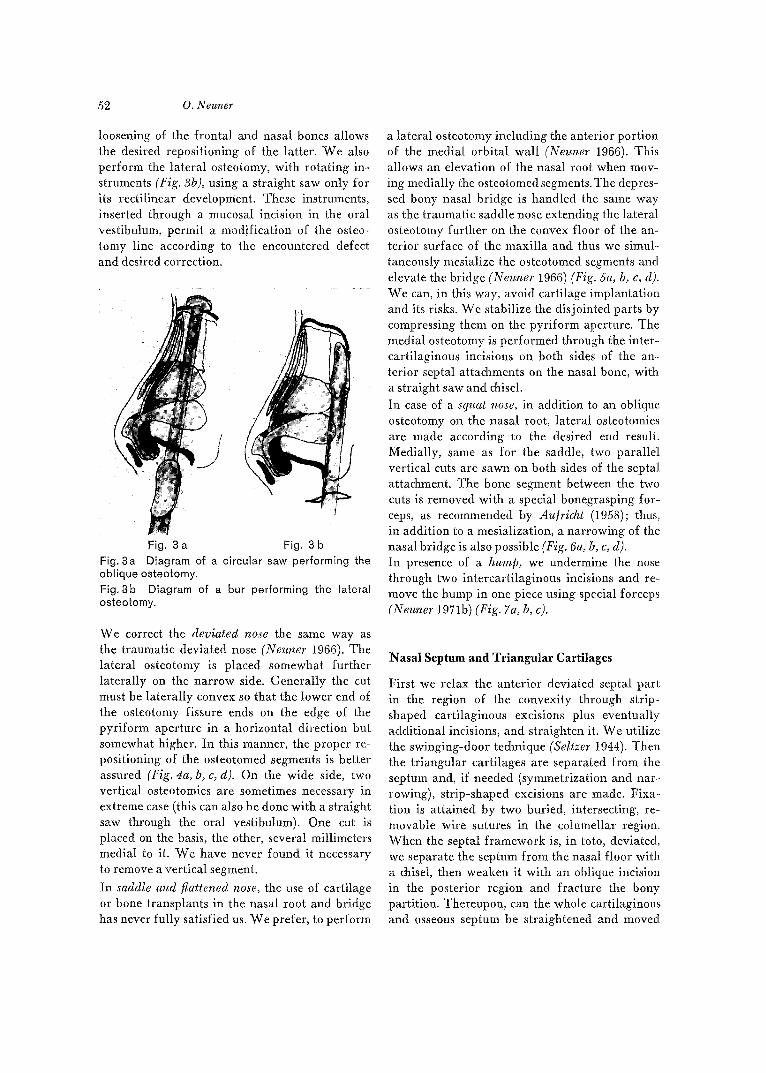
As a rule, we always make an oblique osteotomv in the nasal root using shielded circular saws (Neuner 1966). These are inserted through the intercartilaginous incision (Fig. 8a). The complete
52 O. Neuner
loosening of the frontal and nasal bones allows the desired repositioning of the latter. We also perform the lateral osteotomy, with rotating in- struments (Fig. 3b), using a straight saw only for its rectilinear development. These instruments, inserted through a nmcosal incision in the oral vestibulura, permit a modification of the osteo- tomy line according to the encountered defect and desired correction.
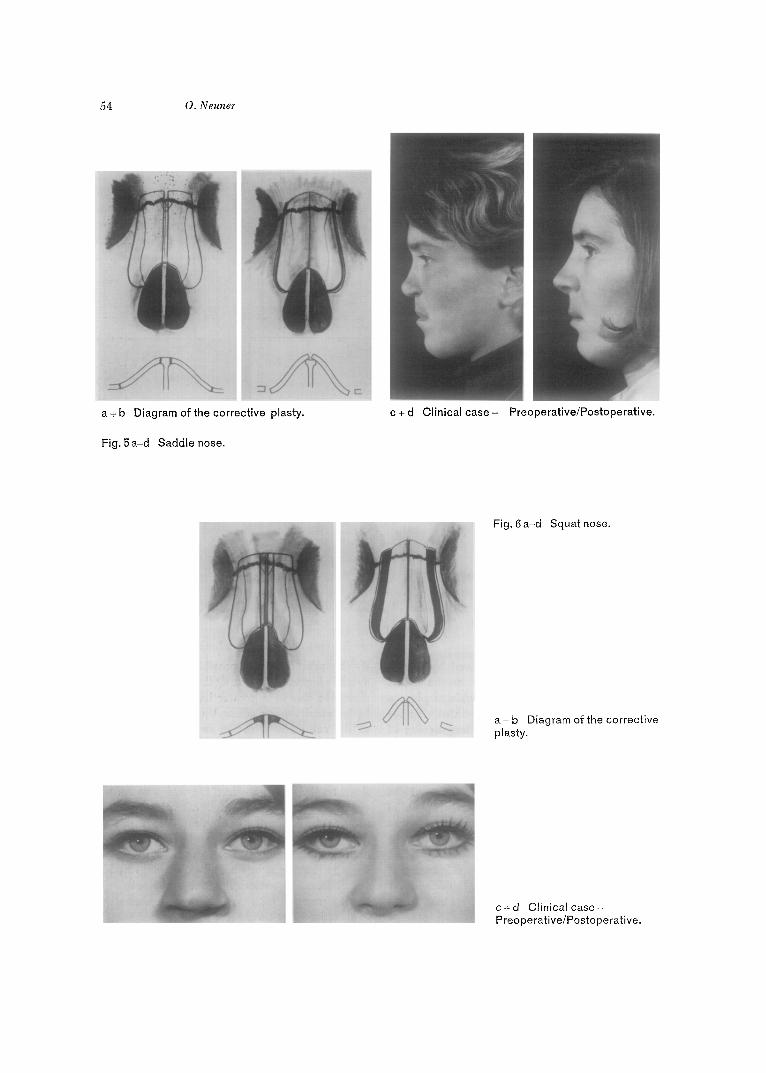
a lateral osteotomy including the anterior portion of the medial orbital wall (Neuner 1966). This allows an elevation of the nasal root when mov- ing medially the osteotomed segments. The depres- sed bony nasal bridge is handled the same way as the traumatic saddle nose extending the lateral osteotomy further on the convex floor of the an- terior surface of the maxilla and thus we simul- taneously mesialize the osteotomed segments and elevate the bridge (Neuner 1966) (Fig. 5a, b, c, d). We can, in this way, avoid cartilage implantation and its risks. We stabilize the disjointed parts by compressing them on the pyriform aperture. The medial osteotomy is performed through the inter- cartilaginous incisions on both sides of the an- terior septal attachments on the nasal bone, with a straight saw and chisel. In case of a squat nose, in addition to an oblique osteotomy on the nasal root, lateral osteotomies are made according to the desired end result. Medially, same as for the saddle, two parallel vertical cuts are sawn on both sides of the septal attachment. The bone segment between the two cuts is removed with a special bonegrasping for- ceps, as recommended by Aufricht (1958); thus, in addition to a mesialization, a narrowing of the nasal bridge is also possible (Fig. 6a, b, c, d). In presence of a hump, we undermine the nose through two intercartilaginous incisions and re- move the hump in one piece using special forceps (Neuner 1971b) (Fig. 7a, b, c).
Fig. 3 a Fig. 3 b Fig. 3a Diagram of a circular saw performing the oblique osteotomy. Fig. 3b Diagram of a bur performing the lateral osteotomy.
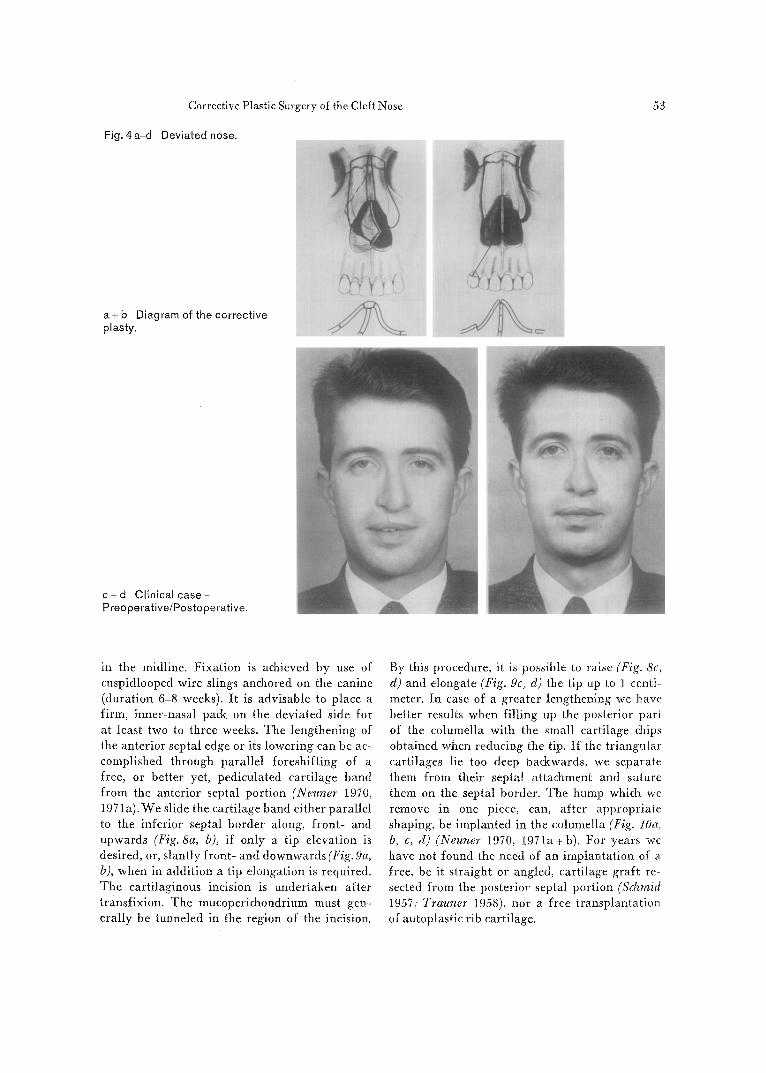
We correct the deviated nose the same way as the traumatic deviated nose (Neuner 1966). The lateral osteotomy is placed somewhat further laterally on the narrow side. Generally the cut must be laterally convex so that the lower end of the osteotomy fissure ends on the edge of the pyriform aperture in a horizontal direction but somewhat higher. In this manner, the proper re- positioning of the osteotomed segments is better assured (Fig. 4a, b, c, d). On the wide side, two vertical osteotomies are sometimes necessary in extreme case (this can also be done with a straight saw through the oral vestibulum). One cut is placed on the basis, the other, several millimeters medial to it. We have never found it necessary to remove a vertical segment.
In saddle and flattened nose, the use of cartilage or bone transplants in the nasal root and bridge has never fully satisfied us. We prefer, to perform
Nasal Septum and Triangular Cartilages
First we relax the anterior deviated septal part in the region of the convexity through strip- shaped cartilaginous excisions plus eventually additional incisions, and straighten it. We utilize the swinging-door technique (Seltzer 1944). Then the triangular cartilages are separated from the septum and, if needed (symmetrization and nar- rowing), strip-shaped excisions are made. Fixa- tion is attained by two buried, intersecting, re- movable wire sutures in. the columellar region. When the septal framework is, in toto, deviated, we separate the septum from the nasal floor with a chisel, then weaken it with an oblique incision in the posterior region and fracture the bony partition. Thereupon, can the whole cartilaginous and osseous septum be straightened and moved
Corrective Plastic Surgery of the Cleft Nose
Fig. 4a-d Deviated nose.
53
a+ b Diagram of the corrective plasty.
c + d Clinical c a s e - Preoperative/Postoperative.
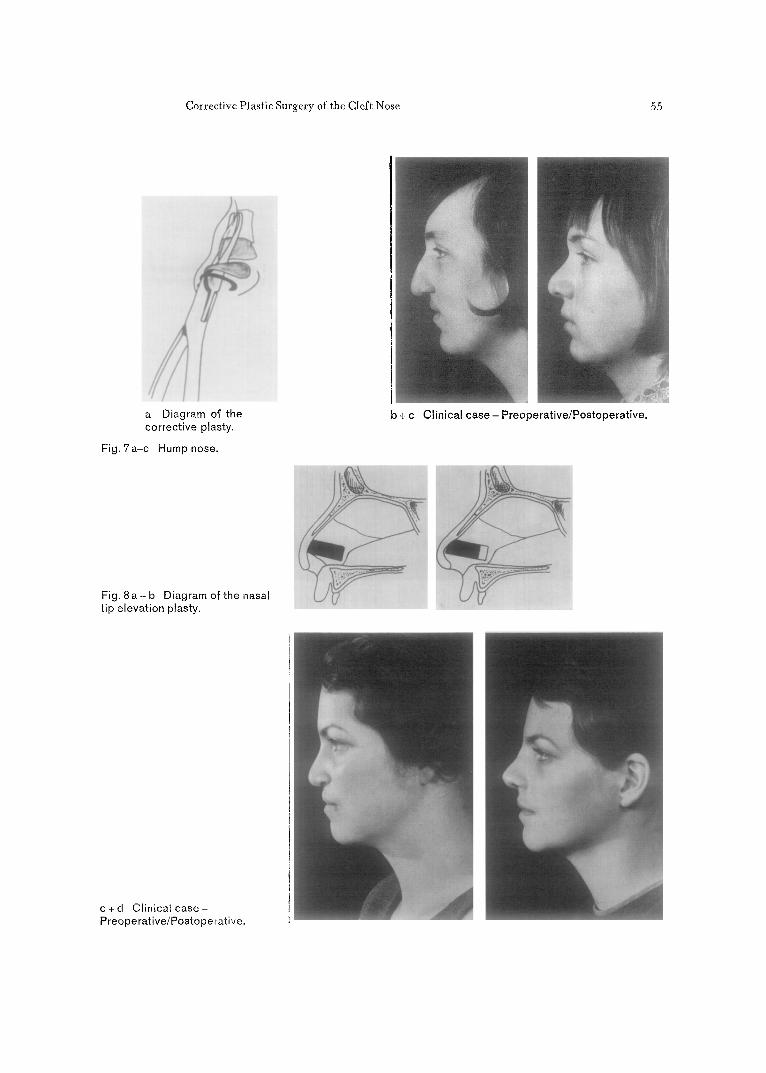
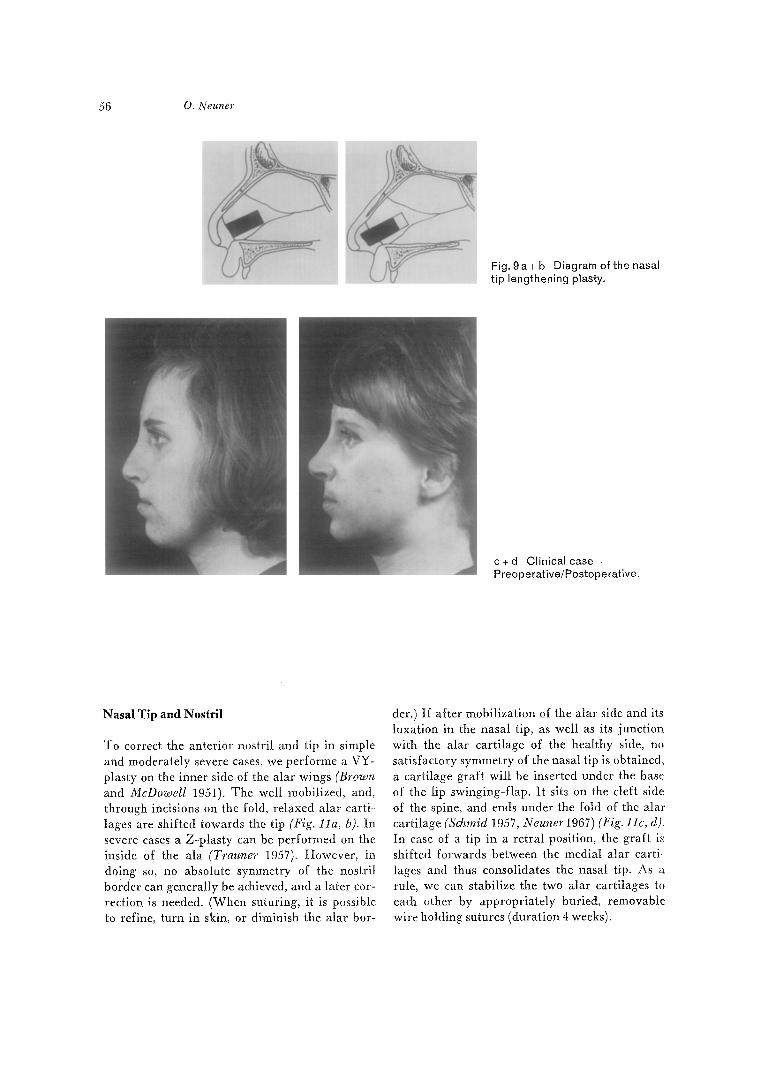
in the midline. Fixation is achieved by use of cuspidlooped wire slings anchored on the canine (duration 6-8 weeks). It is advisable to place a firm, inner-nasal pack on the deviated side for at least two to three weeks. The lengthening of the anterior septal edge or its lowering can be ac- complished through parallel foreshifting of a free, or better yet, pediculated cartilage band from the anterior septal portion (Neuner 1970, 197 la). We slide the cartilage band either parallel to the inferior septal border along, front- and upwards (Fig. 8a, b), if only a tip elevation is desired, or, slantly front- and downwards (Fig. 9a, b), when in addition a tip elongation is required. The cartilaginous incision is undertaken after transfixion. The mucoperichondrium must gen- erally be tunneled in the region of the incision.
By this procedure, it is possible to raise (Fig. 8c, d) and elongate (Fig. 9c, d) the tip up to 1 centi- meter. In case of a greater lengthening we have better results when filling up the posterior part of the columella with the small cartilage chips obtained when reducing the tip. I f the triangular cartilages lie too deep backwards, we separate them from their septal attachment and suture them on the septal border. The hump which we remove in one piece, can, after appropriate shaping, be implanted in the columella (Fig. lOa, b, c, d) (Neuner 1970, 1971a+b). For years we have not found the need of an implantation of a free, be it straight or angled, cartilage graft re- sected from the posterior septal portion (Schraid 1957, Trauner 1958), nor a free transplantation of autoplastic rib cartilage.
54 O. Neuner
C3 C
a + b Diagram of the corrective plasty.
Fig. 5 a-d Saddle nose.
c + d Clinical c a s e - Preoperative/Postoperative.
Fig, 6 a-d Squat nose.
a+ b Diagram of the corrective plasty.
c + d Clinical case- Preoperative/Postoperative.
Corrective Plastic Surgery of the Cleft Nose 55
a Diagram of the corrective plasty.
Fig. 7a-c Hump nose.
b + c Clinical case- Preoperative/Postoperative.
Fig. 8 a + b Diagram of the nasal tip elevation plasty.
c + d Clinical case- Preope rative/Postoperative.
56 O. Neuner
Fig. 9a+b Diagram of the nasal tip lengthening plasty.
c + d Clinical c a s e - Preoperative/Postoperative.
Nasal Tip and Nostri l
To correct the anterior nostril and tip in simple and moderately severe cases, we performe a VY- plasty on the inner side of the alar wings (Brown and McDowell 1951). The well mobilized, and, through incisions on the fold, relaxed Mar carti- lages are shifted towards the tip (Fig. l la, b). In severe cases a Z-plasty can be performed on the inside of the ala (Trauner 1957). However, in doing so, no absolute symmetry of the nostril border can generally be achieved, and a later cor- rection is needed. (When suturing, it is possible to refine, turn in skin, or diminish the alar bor-
der.) If after mobilization of the alar side and its luxation in the nasal tip, as well as its junction with the alar cartilage of the healthy side, no satisfactory symmetry of the nasal tip is obtained, a cartilage graft will be inserted under the base of the lip swinging-flap. It sits on the cleft side of the spine, and ends under the fold of the alar cartilage (Schmid 1957, Neuner 1967) (Fig. 11c, d). In case of a tip in a retral position, the graft is shifted forwards between the medial alar carti~ lages and thus consolidates the nasal tip. As a rule, we can stabilize the two alar cartilages to each other by appropriately buried, removable wire holding sutures (duration 4 weeks).
Corrective Plastic Surgery of the Cleft Nose 57
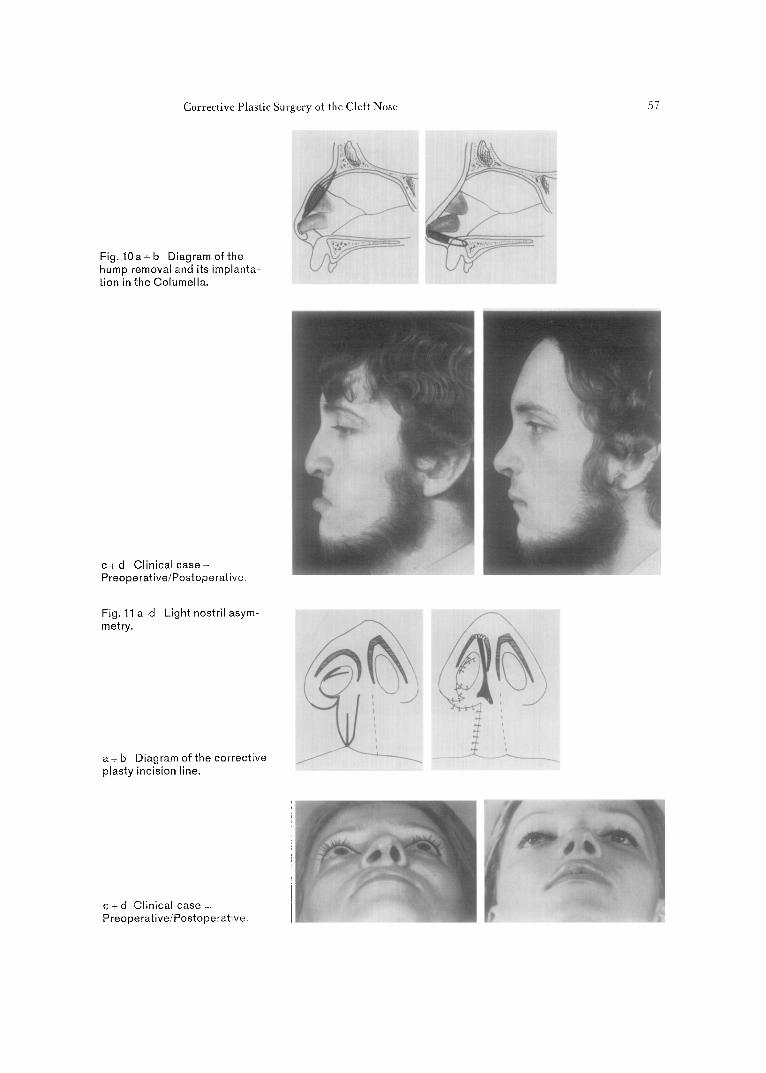
Fig. l O a + b Diagramof the hump removal and its implanta- tion in the Columella.
c 4 d Clinical case - Preoperative/Postoperative,
Fig. 11 a-d Light nostril asym- metry.
a + b Diagram of the corrective plasty incision line.
7
c + d Clinical case .- Preoperative/Postoperative.
58 O. Neuner
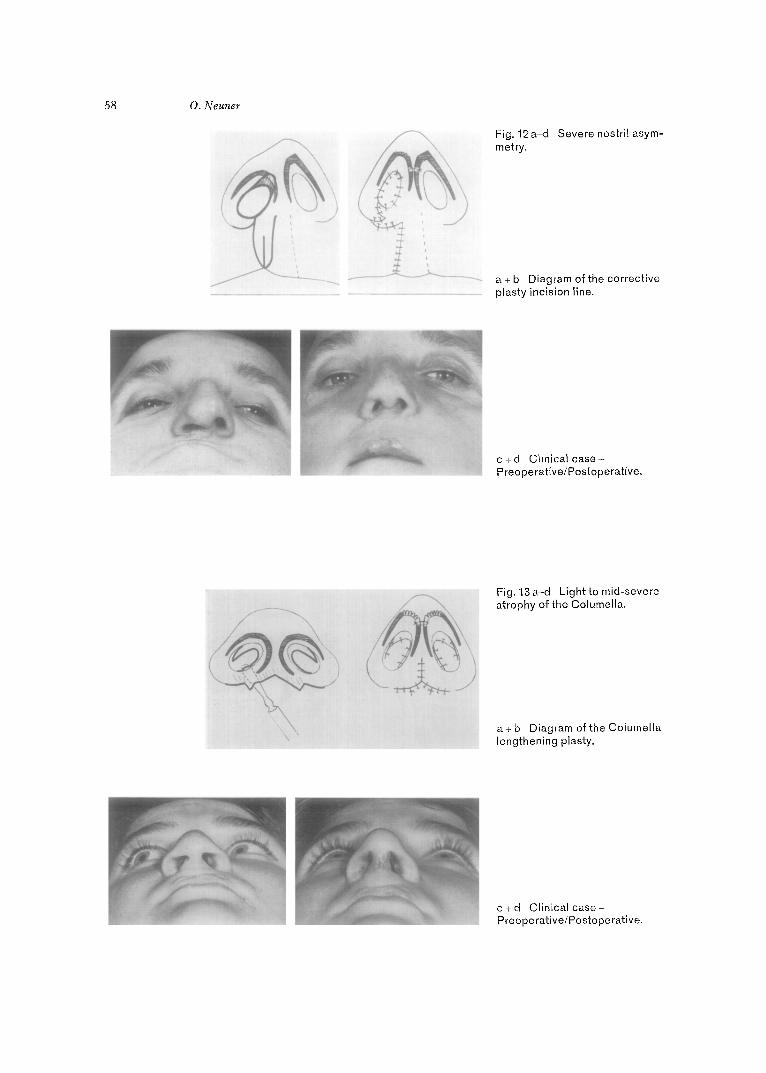
Fig. 12a-d Severe nostril asym- metry.
a+ b Diagram of the corrective plasty incision line.
c +d Clinical case- Preoperative/Postoperative.
\
Fig. 13a-d Lightto mid-severe atrophy of the Columella.
a+ b Diagram of the Columella lengthening plasty.
c + d Clinical case-- Preoperative/Postoperative.
Corrective Plastic Surgery of the Cleft Nose 59
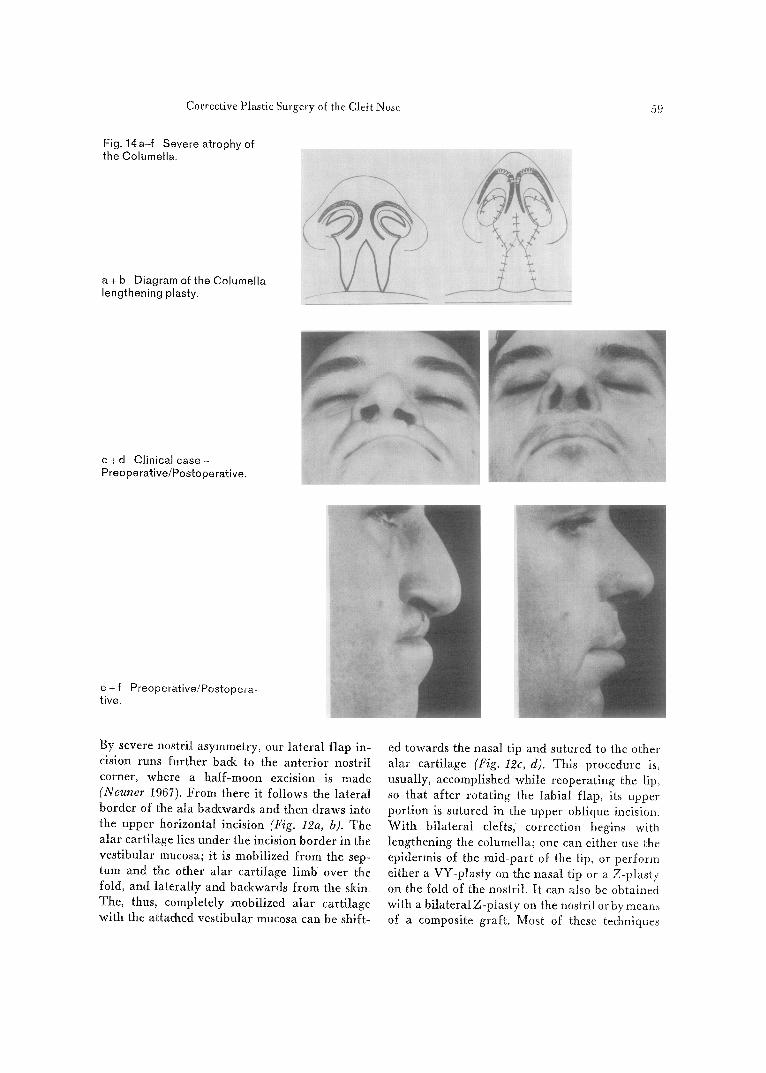
Fig. 14a- f Severe atrophy of the Columel la.
a + b Diagram of the Columel la lengthening plasty.
c + d Cl inical case .~ Preoperat ive/Postoperat ive.
e + f Preoperat ive/Postopera- tive.
By severe nostril asymmetry, our lateral flap in- cision runs further back to the anterior nostril corner, where a half-moon excision is made (Negner 1967). From there it follows the lateral border of the ala backwards and then draws into the upper horizontal incision (Fig. 12a, b). The alar cartilage lies under the incision border in the vestibular mucosa; it is mobilized from the sep- tum and the other alar cartilage limb over the fold, and laterally and backwards from the skin. The, thus, completely mobilized alar cartilage with the attached vestibular mucosa can be shift-
ed towards the nasal tip and sutured to the other alar cartilage (Fig. 12c, d). This procedure is, usually, accomplished while reoperating ~he lip, so that after rotating the labial flap, its upper portion is sutured in the upper oblique incision. With bilateral clefts, correction begins with lengthening the columella; one can either use the epidermis of the mid-part of the lip, or perform either a VY-ptasty on the nasal tip or a Z-plashy on the fold of the nostril. It can also be obtained with a bilateralZ-plasty on the nostril orby means of a composite graft. Most of these techniques
60 O. N eu~wr
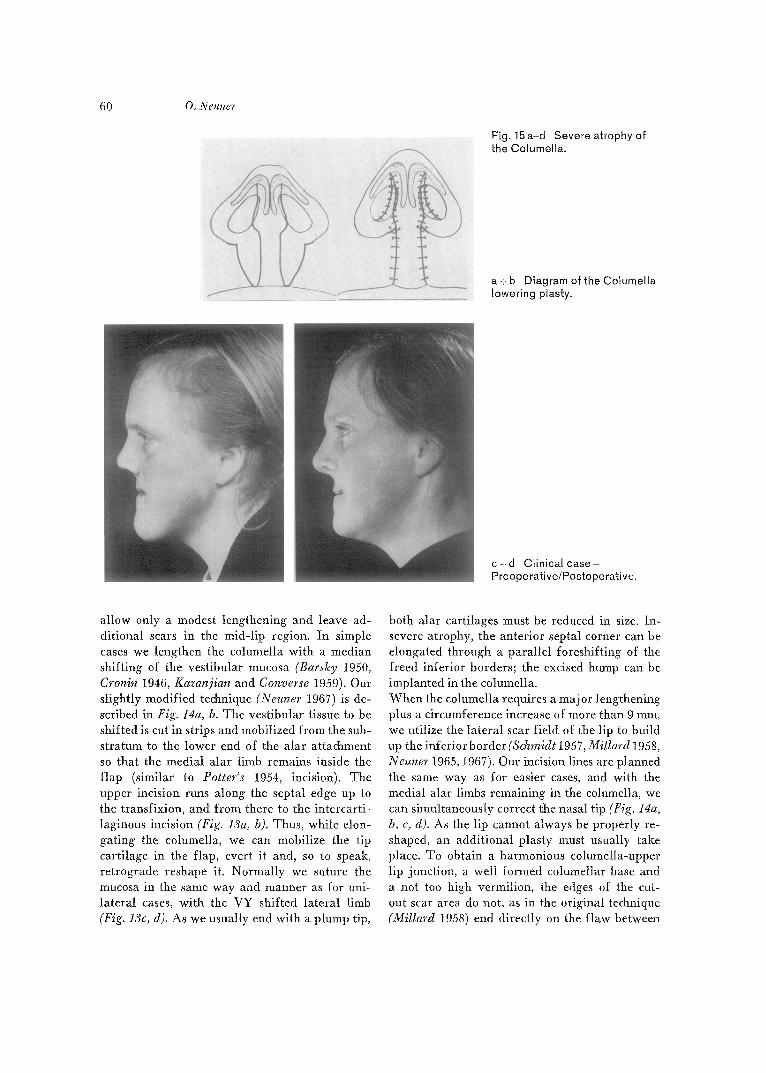
Fig. 15a-d Severe atrophy of the Columella.
a+ b Diagram of the Columella lowering plasty.
c 4- d Clinical case- Preoperative/Postoperative.
allow only a modest lengthening and leave ad- ditional scars in the mid-lip region. In simple cases we lengthen the columella with a median shifting of the vestibular mucosa (Barshy 1950, Cronin 1946, Kazanjian and Converse 1959). Our slightly modified technique (Neuner 1967) is de- scribed in Fig. 14a, b. The vestibular tissue to be shifted is cut in strips and mobilized from the sub- stratum to the lower end of the alar attachment so that the medial alar limb remains inside the flap (similar to Potter's 1954, incision). The upper incision runs along the septal edge up to the transfixion, and from there to the intercarti- laginous incision (Fig. 13a, D). Thus, while elon- gating the columella, we can mobilize the tip cartilage in the flap, evert it and, so to speak, retrograde reshape it. Normally we suture the mucosa in the same way and manner as for uni- lateral cases, with the VY shifted lateral limb (Fig. 13c, d). As we usually end with a plump tip,
both alar cartilages must be reduced in size. In- severe atrophy, the anterior septal corner can be elongated through a parallel foreshifting of the freed inferior borders; the excised hump can be implanted in the columella. When the columella requires a major lengthening plus a circumference increase of more than 9 ram, we utilize the lateral scar field of the lip to build up the inferior border (Schmidt 1957, Millard 1958, Neuner 1965, 1967). Our incision lines are planned the same way as for easier cases, and with the medial alar limbs remaining in the columella, we can simultaneously correct the nasal tip (Fig. 14a, b, c, d). As the lip cannot always be properly re- shaped, an additional plasty must usually take place. To obtain a harmonious columella-upper lip junction, a well formed columellar base and a not too high vermilion, the edges of the cut- out scar area do not, as in the original technique (Millard 1958) end directly on the flaw between

Corrective Plastic Surgery of the Cleft Nose 61
columella and lip, but are slowly d rawn into the ver t ical scar (Fig. 14f, g). The columellar base can thus be symmetr ica l ly reshaped, and the upper lip can be sl ightly elevated and the vermil ion somewhat prot ruded. Through these procedures the alae acquire a l ready a more media l position, however they must genera l ly undergo another correction during the lip reoperation. Only in the presence of a very large scar field wil l the mid- pa r t of the lip be used to elongate the columella. In case of a severe a t rophy of the septum, the
nose can be too short in the ver t ical dimension. W e lower the columella by recl ining 180 ° up- wards two flaps from the la te ra l lip scar fields and suturing them in incisions made on the~ columella border . These pedicula ted flaps have an attachment on the nasa l threshold (Neuner 1967, 1969 a+b) (Fig. 15 a-d) . A cart i lage chip can be implanted to stiffen the new columelta. This is, however, seldom needed, the accumulat ion of scar tissue, brought by the two flaps, on the scptal border giving a sat isfactory stiffness.
References
Aufricht, G.: Surgery of the radix and the bony nose - Preliminary report of a new type of nasal clamp. Plast. reconstr. Surg. 22 (1958) 315
Barshy, A. J.: Principles and practice of plastic surgery. Williams & Wilkins, Baltimore 1950
Brown, ]. B., F. McDowelh Plastic surgery of the Nose. Kimpton, London 1951
Cronin, T. D.: Lenthening the columella by use of skin from nasal floor and alae. Plast. reconstr. Surg. I (1946) 145
Kazanjian, V., J. M. Converse: The surgical treatment of facial injuries. Williams & Wilkins, Baltimore 1959
Millard, D. R. jr.: Columella lengthening by a forked flap. Plast. reconstr. Surg. 22 (1958) 454
Neuner, 0.: Sekund~ire KorrekturmSglichkeiten bei Lippen-Kiefer-Gaumenspalt-Patienten. Osterr. Z. Stomat. 62 (1965) 268
Neuner, 0.: Plastische Versorgung yon Zertriimme- rungen, Defektbildungen und WachstumsstSrungen im Bereich der Gesichtsknochen. Hdb. Plast. Chir, Bd. II. de Gruyter, Berlin 1966
Neuner, 0.: The functional and cosmetic treatment of cleft lip and palate. Excerpta med .(Amst.) Int. Congr. Set. No. 141 (1967) 118
Neuner, 0.: Secondary correction of cleft lip and palate (with particular reference to the construction of the philtrum). Excerpta reed. (Amst.) Int. Congr. Ser. No. 174 (1969) 390
Neuner, 0.: Special problems in full rehabilitation of the nasal base and upper lip in single and double clefts. Cleft Palate J. 6 (1969) 384
Neuner, 0.," Operationen bei Spalttr/igern im Erwach- senenalter. Hdb. Plast. Chir., Bd. II. de Gruytcr, Berlin 1970
Neuner, 0.: Secondary Repair of cleft Lip and Palate Deformities. Image reed. Photo rep. Roche 40 (1971) 2
Neuner, 0.: A simple procedure for correction of the Hump Nose. Brit. J. plast. Surg. (1971)
Potter, ].: Some nasal tip deformities due to alar carti- lage abnormalities. Plast. reconstr. Surg. 13 (1954) 358
Schmid, E.: Wiederherstellungsprobleme im Philtrum- bereich der Lippe, unter besonderer Berii&sichtigung der Unterentwi&lung des Nasensteges. Dtsch. Zahn-, Mund- u. Kieferheilk. 26 (1957) 397
Seltzer, A. P.: The nasal septum: Plastic repair of the deviated septum associated with a deflected tip. Arch Otolaryng 40 (1944) 483
Trauner, R., F. Wirth: Nasenkorrckturen bei einseitigcn Lippen-Kiefer-Gaumenspalten. Z. Laryng. Rhlnol. (Stuttg.) 36 (1957) 621
Trauner, R., F. Wirth: Nasenkorrekturen bei doppel- seitigen Lippen-Kiefer-Gaumenspalten. Z. Laryng. Rhinol. (Stuttg.) 37 (1958) 655
Pro[. Otgo Neuner, M.D., D.M.D., Department of Maxillofacial and Plastic Smgery, Freibm'gerstra[~e 7 3008 Berne~Switzerland