Die Enzian Klassifikation und ihre klinische Bedeutungfinal.pdf · Die Enzian – Klassifikation...
21
Die Enzian – Klassifikation und ihre klinische Bedeutung Der Medizinischen Fakultät der Friedrich-Alexander-Universität Erlangen-Nürnberg zur Erlangung des Doktorgrades Dr.med. vorgelegt von Dietmar Haas Linz, Österreich
-
Upload
phungduong -
Category
Documents
-
view
213 -
download
0
Transcript of Die Enzian Klassifikation und ihre klinische Bedeutungfinal.pdf · Die Enzian – Klassifikation...

Die Enzian – Klassifikation und ihre klinische Bedeutung
Der Medizinischen Fakultät
der Friedrich-Alexander-Universität
Erlangen-Nürnberg
zur
Erlangung des Doktorgrades Dr.med.
vorgelegt von
Dietmar Haas
Linz, Österreich
Als Dissertation genehmigt von der
Medizinischen Fakultät der Friedrich-Alexander-Universität
Erlangen-Nürnberg
Vorsitzender des Promotionsorgans: Prof. Dr. Dr. h.c. J. Schüttler
Gutachter: Prof. Dr. P. Oppelt
Gutachter: Prof. Dr. M.W. Beckmann
Tag der mündlichen Prüfung: 10. Dezember 2013
Inhaltsverzeichnis
1. Zusammenfassung Seite 1
2. Einleitung Seite 2
3. Veröffentlichung: „ACTA Obstetricia et Gynecologica Scandinavica“:
Enzian classification: does it correlate with clinical symptoms and the
rASRM score? Acta Obstet Gynecol Scand. 2013 May;92(5):562-6.
3.1.1. Abstract Seite 4
3.1.2. Introduction Seite 5
3.1.3. Material and methods Seite 6
3.1.4. Results Seite 7
3.1.5. Discussion Seite 11
3.1.6. Conclusion Seite 12
4. Literaturverzeichnis Seite 13
5. Abkürzungsverzeichnis Seite 14
6. Lebenslauf Seite 15
Zusammenfassung
Hintergrund und Ziele: Evaluierung von Korrelationen der Enzian –
Klassifikation mit dem rASRM – Score und klinischen Symptomen bei tief
infiltrierender Endometriose.
Methode: 194 Patientinnen wurden aufgrund von tief infiltrierender
Endometriose operiert. Nach histologischer Sicherung wurden diese nach
rASRM und Enzian klassifiziert. Klinische Symptome wurden präoperativ
erhoben. Es wurden Korrelationen zwischen der Enzian – Klassifikation und
sowohl dem rASRM – Score als auch den klinischen Symptomen berechnet.
Zur statistischen Berechnung wurden Spearman’s rank correlation,
Spearman's partial rank-order correlation, exact chi-square tests, Fisher’s
exact tests, point biserial correlation und generalized Cochran-Mantel-
Haenszel tests verwendet.
Ergebnisse: Es zeigt sich eine deutliche Korrelation zwischen den
Schweregraden des rASRM – Scores und der Enzian – Klassifikation
(p<0.001). Weiters korrelieren die rASRM Schweregrade und klinische
Symptome mit den Lokalisationen in der Enzian – Klassifikation im Sinne tief
infiltrierender Endometriose markant. Schmerz und Dysmenorrhoe korrelieren
stark (p=0,002; p<0,001) mit dem Schweregrad der Enzian – Klassifikation.
Schlussfolgerungen: Tief infiltrierende Endometriose kann anhand der
Enzian – Klassifikation ergänzend zum rASRM – Score gut dargestellt werden.
Anhand des morphologisch grenzüberschreitenden Charakters der Erkrankung
zwischen Enzian und rASRM gibt es auch eine deutliche Korrelation zwischen
den beiden Klassifikationen. Lokalisationen in der Enzian – Klassifikation
korrelieren zum Teil mit klinischen Symptomen und ihre Schweregrade
korrelieren substantiell mit Schmerz und Dysmenorrhoe. Aufgrund dieser
klinischen Ergebnisse und zur detailierteren Beschreibung der Endometriose
ist es empfehlenswert die Enzian – Klassifikation ergänzend zum rASRM –
Score zu verwenden.
Einleitung
Endometriose ist eine der häufigsten gutartigen Erkrankungen von Frauen im
gebärfähigen Alter. Man schätzt, dass 5-15% der Frauen im gebärfähigen Alter
davon betroffen sind. Um diese häufige Erkrankung international vergleichen
zu können und um sich über Therapie und Therapieerfolge austauschen zu
können, bedarf es einer gemeinsamen Sprache im Sinne einer Klassifikation.
Die Anforderungen an eine derartige Klassifikation stellen die morphologische
Beschreibung der Erkrankung und eine Simplizität in der Anwendung dar.
Zudem sollte sie empirisch und wissenschaftlich basieren und allgemeine
Anerkennung und Anwendung aufweisen.
1979 wurde von der American Fertility Society (AFS) der AFS – Score (3)
vorgestellt, welcher sich nach Revision 1985 (rAFS – Score) als weltweit meist
angewandtes Klassifikationssystem etablierte. 1996 wurde dieser in den
rASRM – Score (American Society for Reproductive Medicine) umbenannt.
Der rASRM – Score stellt per se einen tatsächlichen Score dar. In ihm werden
Endometrioseläsionen am Peritoneum und an den Ovarien entsprechend ihrer
Größe mit Punkten bewertet. Analog werden Punkte für Adhäsionen an den
Ovarien und den Tuben vergeben. Weiterhin gibt es Punkte für eine partielle
oder komplette posterior cul-de-sac obliteration. Schließlich werden sämtliche
Punkte addiert und in vier Schweregrade eingeteilt (Grad I – IV).
Als Nachteil des ASRM – Scores erwies sich eine limitierte Reproduzierbarkeit
des Stagings bei Befall der Ovarien und des posterior cul-de-sac. Weiters
zeigte sich nur eine schwache Korrelation zwischen der Ausdehnung der
Endometriose und dem Schmerz und Sterilität. Ebenso wird der Befall von
retroperitonealen Strukturen im Sinne einer tief infiltrierenden Endometriose
nicht berücksichtigt.
Aufgrund der fehlenden Beschreibung retroperitonealer Strukturen im Sinne
einer tief infiltrierenden Endometriose wurde 2005 die Enzian – Klassifikation
entwickelt. Diese verstand sich nicht als Konkurrenz zum rASRM – Score,
sondern als Ergänzung zu diesem im Beschreiben tief infiltrierender
Endometriose.
Als Probleme der Enzian – Klassifikation zeigten sich eine schlechte
internationale Akzeptanz, Komplexizität in der Anwendung und teilweise nicht
gewünschte Überlappungen mit dem rASRM – Score. Aus diesen Gründen
wurde die Enzian – Klassifikation 2010 und 2011 revidiert um die
Klassifizierung zur vereinfachen und zu optimieren.
In den Ländern Deutschland, Österreich, Schweiz und Süd-Tirol (Italien) gibt
es derzeit 47 Endometriosekompetenzzentren der Stufe I, II und III. Die Stufen
I – III (höchste) richten sich nach den Kriterien der Stiftung Endometriose
Forschung (SEF), welche die Zertifizierungen auch durchführt. Im Rahmen
dieser Zertifizierungen und Rezertifizierungen werden alle Kompetenzzentren
der Stufe III (n=20) verpflichtet, sowohl nach rASRM als auch nach Enzian zu
klassifizieren.
Diese Arbeit untersucht folgende Punkte:
1. Korreliert die Höhe des rASRM - Schweregrades (rASRM - Stadium)
mit der Höhe des höchsten Enzian – Schweregrades in den
Kompartimenten A, B und C?
2. Korreliert die Höhe des rASRM - Schweregrades (rASRM - Stadium)
mit der Höhe des höchsten Enzian - Schweregrades, wenn bei
letzterem zusätzlich die Anzahl der Läsionen berücksichtigt wird?
3. Korreliert die Höhe des rASRM - Schweregrades (rASRM - Stadium)
mit den Lokalisationen in der Enzian – Klassifikation (befallene
Kompartimente)?
Bisher gibt es keine Untersuchungen, ob es Korrelationen zwischen der
Enzian – Klassifikation und klinischen Symptomen gibt.
4. Korrelieren klinische Endometriosesymptome mit den Lokalisationen in
der Enzian – Klassifikation (befallene Kompartimente)?
5. Korrelieren klinische Endometriosesymptome mit der Höhe des
höchsten Enzian – Schweregrades in den Kompartimenten A, B und
C?
6. Korrelieren klinische Endometriosesymptome mit der Höhe des
höchsten Enzian -Schweregrades, wenn bei diesem zusätzlich die
Anzahl der Läsionen berücksichtigt wird?

Abstract
Objective: To assess the extent to which the Enzian classification correlates
with the revised American Society for Reproductive Medicine (rASRM) score
and clinical symptoms in patients with deeply infiltrating endometriosis.
Design: Retrospective cohort study (Canadian Task Force classification II-2).
Setting: Endometriosis competence center specializing in minimally invasive
surgery.
Patients: Between January 1st, 2009 and December 31st, 2011, a total of 194
patients underwent surgery due to deeply infiltrating endometriosis. After
histological confirmation, they were classified using the rASRM and Enzian
systems. Clinical symptoms were recorded preoperatively.
Interventions: Operative laparoscopy to treat endometriosis.
Main outcome measures and results: A clear correlation was seen between
grades of severity in the rASRM score and the Enzian classification
(P < 0.001). In addition, the rASRM severity grade and clinical symptoms
correlated strikingly with the locations in the Enzian classification in relation to
deeply infiltrating endometriosis. Pain and dysmenorrhea correlated strongly
(P = 0.002, P < 0.001) with the severity grade in the Enzian classification.
Conclusions: Deeply infiltrating endometriosis is well characterized using the
Enzian classification as a supplement to the rASRM score. There is also a
clear correlation between the rASRM and Enzian classifications, due to the
way in which the disease crosses morphological boundaries. The locations in
the Enzian classification correlate partially with clinical symptoms, and the
classification’s severity grades correlate substantially with pain and
dysmenorrhea. In view of these clinical results, use of the Enzian classification
can be recommended as a supplement to the rASRM score for detailed
description of endometriosis.
Introduction
Endometriosis is one of the most frequent benign diseases in women of child-
bearing age. It is estimated that 5–15% of women of childbearing age are
affected by it (9). A common terminology in the form of a classification system
is needed in order to be able to compare this frequent disease internationally
and exchange information about treatment and therapeutic success. A
classification of this type needs to provide a morphological description of the
disease and must be easy to use. In addition, it should have an empirical and
scientific basis and should be generally recognized and widely used (1).
The American Fertility Society (AFS) published the AFS score in 1979 (10);
following revision in 1985 (becoming the rAFS score) (11), it became
established as the most widely used classification system throughout the
world. In 1996, it was renamed as the revised American Society for
Reproductive Medicine (rASRM) score (2). The advantages and disadvantages
of the rASRM score have been discussed in the literature (6).
Due to the lack of description of retroperitoneal structures in cases of deeply
infiltrating endometriosis, the Enzian classification was developed in 2005 (12).
This was not intended to compete with the rASRM score, but to supplement it
for the description of deeply infiltrating endometriosis. Problems that emerged
with the Enzian classification were its poor level of international acceptance,
complexity of use, and unintended partial overlapping with the rASRM score
(4). For these reasons, the Enzian classification was revised in 2010 and 2011
in order to simplify and optimize it (6). In a subsequent study, it was shown that
the revised Enzian classification had resolved this problem (5).
The rASRM score and the supplementary Enzian classification for describing
deeply infiltrating endometriosis thus reflect different manifestations of
endometriosis. The present study therefore investigated whether the level of
the rASRM severity grade (the rASRM stage) correlates with the level of the
highest Enzian severity grade in compartments A, B, and C and whether the
level of the rASRM severity grade (the rASRM stage) correlates with the level
of the highest Enzian severity grade, if the latter also takes the number of
lesions into account. It also investigated whether the level of the rASRM
severity grade (the rASRM stage) correlates with the locations in the Enzian
classification (the involved compartments).
To date, there have not been any studies investigating whether there is any
correlation between the Enzian classification and clinical symptoms. The study
therefore investigated whether the clinical symptoms of endometriosis
correlate with the locations in the Enzian classification (involved
compartments) and wether the clinical symptoms of endometriosis correlate
with the level of the Enzian severity grades.
Material and methods
Approval from the local institutional ethics committee was obtained on June
14th, 2012 (ref. no. K-20-12). Between January 1st, 2009 and December 31st,
2011, a total of 194 patients were treated for deeply infiltrating endometriosis
at the General Hospital in Linz, Austria. Endometriosis was confirmed
histologically after laparoscopic surgery. All of the operations were carried out
by the same team of five surgeons, in which each surgeon had previously
carried out at least 200 laparoscopies. In addition, the patients were classified
using the rASRM and Enzian systems. For each case, there were two
observers to assign the scores.
The following clinical symptoms were noted preoperatively as prospectively
observed clinical complaints: infertility, general abdominal pain, premenstrual
lower abdominal pain, chronic lower abdominal pain, dysmenorrhea,
dyspareunia, hypermenorrhea, menometrorrhagia, bowel symptoms, and
bladder symptoms. Seven of the 194 patients could only be classified using the
Enzian score, as they only had uterine adenomyosis, which is not taken into
account in the rASRM score. Deeply infiltrating involvement in compartments
A, B, or C was not found in 14 of the 194 patients. For statistical analysis, there
were therefore three cohorts with different numbers of patients in each (n =
180, n = 187, and n = 194).
It should be noted that in the Enzian classification, a single lesion is
classified only once — i.e., it is assigned either to compartment A, B, or C.
When endometriosis is located on the margin between two intersecting
compartments, the lesion is assigned to the larger compartment affected by
endometriosis and not to both compartments. Multiple designations are only
made when several lesions are found in different locations — i.e., when
several compartments are affected. When several lesions are observed inside
a single compartment, only the larger lesion is taken into account for
classification purposes.
Statistical analysis
Spearman’s rank correlation coefficient (rs) was calculated for the rASRM and
Enzian severity grades. Spearman’s partial rank–order correlation coefficient
(rsp) was used for additional lesion adjustment. Correlations between affected
compartments and rASRM severity were calculated using exact chi-squared
tests; correlations between affected compartments and clinical endometriosis
symptoms were assessed using Fisher’s exact tests. Point biserial correlation
coefficients (rpb) were used to assess correlations between Enzian severity
grades and clinical endometriosis symptoms; generalized Cochran–Mantel–
Haenszel tests were used for additional lesion adjustment. All of the tests were
two-tailed, with a confidence level of 95% (P < 0.05). No adjustment for type I
error was made; the P values given are therefore only descriptive. The
statistics programs R and Bias version 10.0 were used for the calculations.
Results
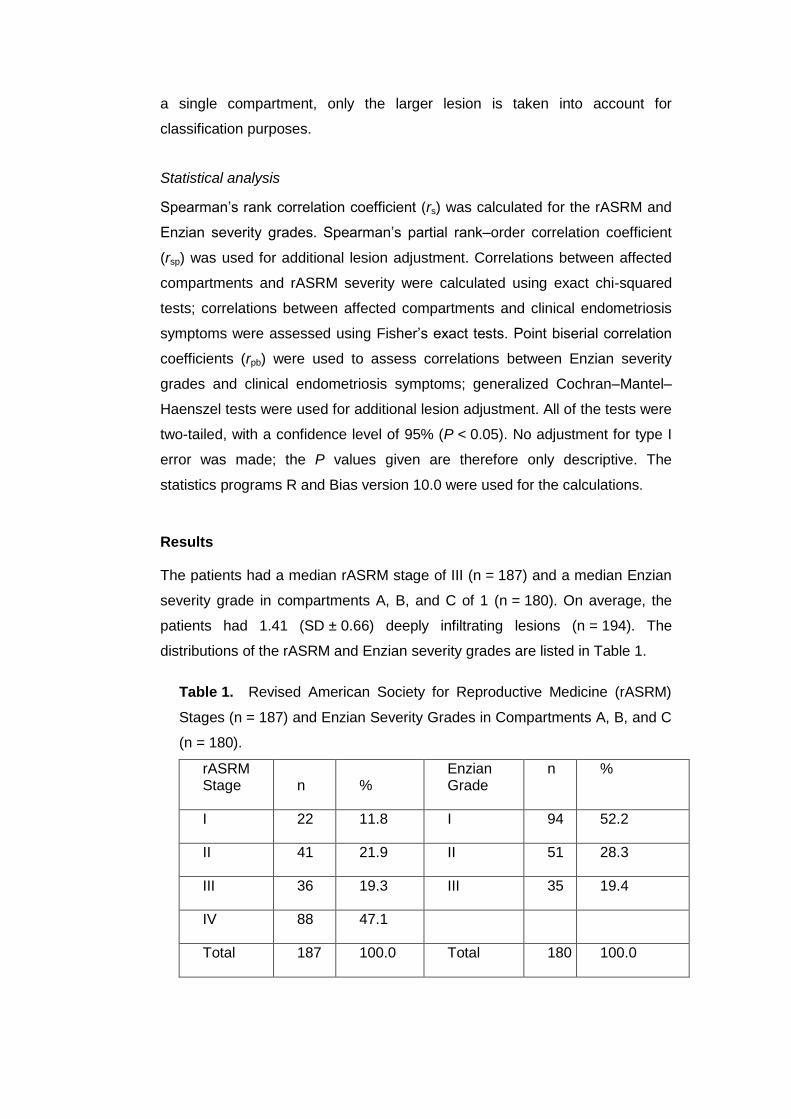
The patients had a median rASRM stage of III (n = 187) and a median Enzian
severity grade in compartments A, B, and C of 1 (n = 180). On average, the
patients had 1.41 (SD ± 0.66) deeply infiltrating lesions (n = 194). The
distributions of the rASRM and Enzian severity grades are listed in Table 1.
Table 1. Revised American Society for Reproductive Medicine (rASRM)
Stages (n = 187) and Enzian Severity Grades in Compartments A, B, and C
(n = 180).
rASRM Stage n %
Enzian Grade
n %
I 22 11.8 I 94 52.2
II 41 21.9 II 51 28.3
III 36 19.3 III 35 19.4
IV 88 47.1
Total 187 100.0 Total 180 100.0
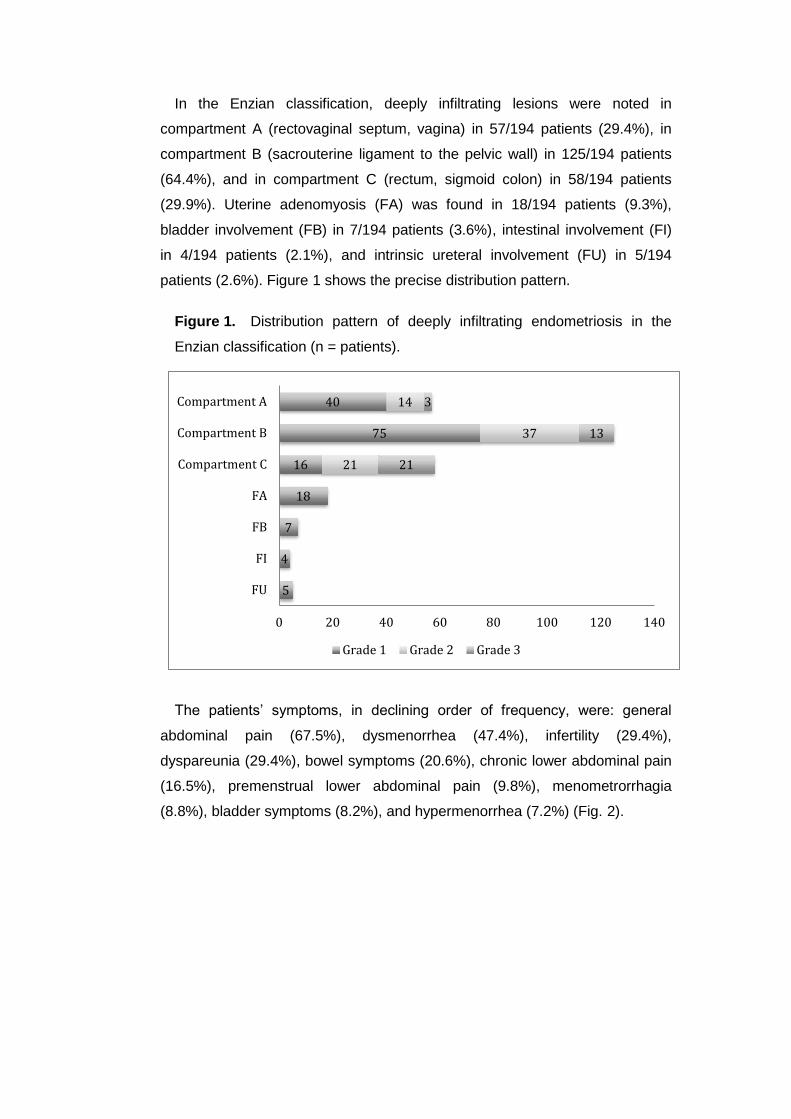
In the Enzian classification, deeply infiltrating lesions were noted in
compartment A (rectovaginal septum, vagina) in 57/194 patients (29.4%), in
compartment B (sacrouterine ligament to the pelvic wall) in 125/194 patients
(64.4%), and in compartment C (rectum, sigmoid colon) in 58/194 patients
(29.9%). Uterine adenomyosis (FA) was found in 18/194 patients (9.3%),
bladder involvement (FB) in 7/194 patients (3.6%), intestinal involvement (FI)
in 4/194 patients (2.1%), and intrinsic ureteral involvement (FU) in 5/194
patients (2.6%). Figure 1 shows the precise distribution pattern.
Figure 1. Distribution pattern of deeply infiltrating endometriosis in the
Enzian classification (n = patients).
The patients’ symptoms, in declining order of frequency, were: general
abdominal pain (67.5%), dysmenorrhea (47.4%), infertility (29.4%),
dyspareunia (29.4%), bowel symptoms (20.6%), chronic lower abdominal pain
(16.5%), premenstrual lower abdominal pain (9.8%), menometrorrhagia
(8.8%), bladder symptoms (8.2%), and hypermenorrhea (7.2%) (Fig. 2).
5
4
7
18
16
75
40
21
37
14
21
13
3
0 20 40 60 80 100 120 140
FU
FI
FB
FA
Compartment C
Compartment B
Compartment A
Grade 1 Grade 2 Grade 3
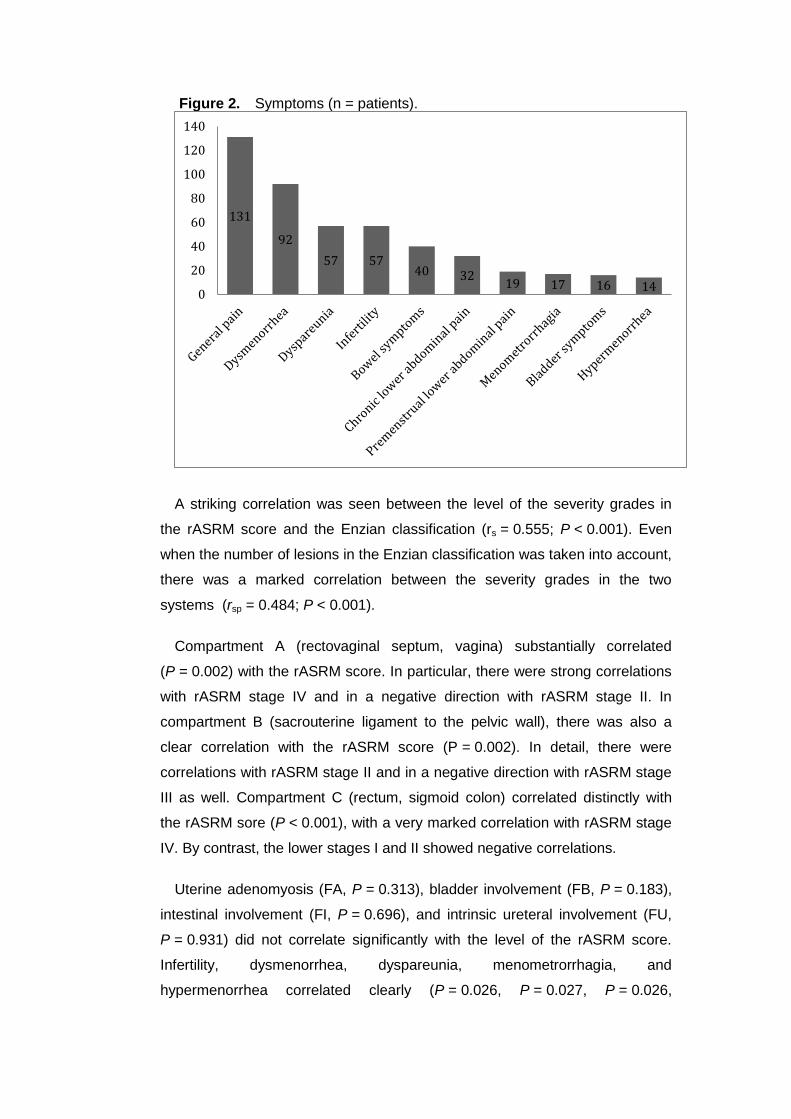
Figure 2. Symptoms (n = patients).
A striking correlation was seen between the level of the severity grades in
the rASRM score and the Enzian classification (rs = 0.555; P < 0.001). Even
when the number of lesions in the Enzian classification was taken into account,
there was a marked correlation between the severity grades in the two
systems (rsp = 0.484; P < 0.001).
Compartment A (rectovaginal septum, vagina) substantially correlated
(P = 0.002) with the rASRM score. In particular, there were strong correlations
with rASRM stage IV and in a negative direction with rASRM stage II. In
compartment B (sacrouterine ligament to the pelvic wall), there was also a
clear correlation with the rASRM score (P = 0.002). In detail, there were
correlations with rASRM stage II and in a negative direction with rASRM stage
III as well. Compartment C (rectum, sigmoid colon) correlated distinctly with
the rASRM sore (P < 0.001), with a very marked correlation with rASRM stage
IV. By contrast, the lower stages I and II showed negative correlations.
Uterine adenomyosis (FA, P = 0.313), bladder involvement (FB, P = 0.183),
intestinal involvement (FI, P = 0.696), and intrinsic ureteral involvement (FU,
P = 0.931) did not correlate significantly with the level of the rASRM score.
Infertility, dysmenorrhea, dyspareunia, menometrorrhagia, and
hypermenorrhea correlated clearly (P = 0.026, P = 0.027, P = 0.026,
131
92
57 57 40 32
19 17 16 14 0
20
40
60
80
100
120
140

P = 0.002, and P = 0.005, respectively) with uterine adenomyosis (FA).
General abdominal pain correlated distinctly with lesions in compartment A
(rectovaginal septum, vagina; P = 0.012) and with uterine adenomyosis (FA;
P = 0.002). Bowel symptoms correlated distinctly with compartment C (rectum,
sigmoid colon; P = 0.011). Premenstrual lower abdominal pain, chronic lower
abdominal pain, and bladder symptoms did not show a clear correlation with
any locations in the Enzian classification.
The maximum severity grade in compartments A, B, and C in the Enzian
classification correlated clearly with the symptoms of general abdominal pain,
dysmenorrhea, and bowel symptoms (Table 2). There was a distinct
correlation here between the level of the highest Enzian severity grade and the
symptoms of general abdominal pain (P = 0.012), dysmenorrhea (P < 0.001),
and bowel symptoms (P = 0.021).
Table 2. Correlation of the highest Enzian severity grade with clinical
symptoms.
Maximum Enzian severity grade
Premenstrual lower abdominal pain rPb –0.014
P 0.853
Infertility rPb 0.101
P 0.177
General abdominal pain rPb 0.233
P 0.002
Dysmenorrhea rPb 0.297
P <0.001
Hypermenorrhea rPb –0.090
P 0.231
Dyspareunia rPb 0.053
P 0.478
Menometrorrhagia rPb –0.018
P 0.811
Bowel symptoms rPb 0.231
P 0.002
Chronic lower abdominal pain rPb –0.112
P 0.135
Bladder symptoms rPb 0.021
P 0.781
Discussion
The results show a distinct correlation between the rASRM score and the
Enzian classification. The rASRM score and the Enzian classification describe
different manifestations of endometriosis, with the Enzian system providing a
supplementary classification of deeply infiltrating lesions. It is important that a
single lesion should not be duplicated in the two systems (4). Clearly, the ideal
was to determine the depth of infiltration by histological examination and
should at least reach 5 milimeters (7). Despite this, the results show that
endometriosis is not limited by the morphologically established boundaries in
the two classification systems. Instead, it appears generally as either high-
grade or low-grade, irrespective of such boundaries.
A clear correlation was observed between the rASRM severity grade and the
location of the lesion in the Enzian classification. The marked correlation
between compartment A (rectovaginal septum, vagina) and rASRM grade IV is
easily understandable clinically. Partial or total obliteration of the cul-de-sac is
often observed in this type of involvement, which is given a very high grade in
the rASRM system. The correlation between compartment B (sacrouterine
ligament to the pelvic wall) and rASRM score II and in a negative direction with
rASRM score III is also interesting. This type of involvement often reflects
solitary low-grade peritoneal lesions that nevertheless infiltrate deeply into the
sacrouterine ligament and cause the typical rectovaginally palpable nodes
there. The correlation between compartment C (rectum, sigmoid colon) and
rASRM grade IV is also frequently observed intraoperatively. When there is
bowel involvement, adhesions, peritoneal lesions, and partial or total
obliteration of the cul-de-sac are often found. Consistently with such findings,
bowel endometriosis is rarely seen with low rASRM stages.
In addition to the strong correlation between uterine adenomyosis and
various symptoms, there was also a clear correlation between pain and
involvement of compartment A (rectovaginal septum, vagina). Many of the
symptoms reported in uterine adenomyosis are already familiar from the
literature (3, 8). It is surprising, however, that compartment A only correlates
with pain, but not in any notable way with dyspareunia. In addition to uterine
adenomyosis, endometriotic involvement of the rectovaginal septum, vagina
(compartment A), and involvement of the sacrouterine ligament (compartment
B) are often found clinically as a reason for dyspareunia. However, this is not

reflected in the results. The correlation between bowel symptoms and bowel
involvement (compartment C) is hardly surprising, but no such correlation is
seen between bladder symptoms and involvement of the bladder (FB).
A clinically interesting and important finding is the substantial correlation that
appeared between the Enzian severity grade and symptoms of general pain,
dysmenorrhea, and bowel symptoms. These correlations with clinical
symptoms represent a major advantage of the Enzian classification.
Conclusions
Endometriosis becomes manifest with various types of involvement. Deeply
infiltrating endometriosis can be well described using the Enzian classification
as a supplement to the rASRM score. As it is in the nature of the disease to
cross morphological boundaries, there is also a clear correlation between the
two classifications. A major advantage of the Enzian classification lies in its
clinical value. The locations used in the Enzian classification correlate partly
with clinical symptoms, and its severity grades correlate substantially with pain.
In view of these results and the detailed description of endometriosis the
classification provides, use of the Enzian classification as a supplement to the
rASRM score can be recommended.
Literaturverzeichnis
1. Adamson GD. Endometriosis classification: an update. Curr Opin
Obstet Gynecol. 2011;23:213–20.1. Schweppe KW. [Endometriosis —
a disease that has no lobby]. Zentralbl Gynakol. 2003;125:233.
German.
2. American Society for Reproductive Medicine. Revised American
Society for Reproductive Medicine classification of endometriosis:
1996. Fertil Steril. 1997;67:817–21.
3. Garcia L, Isaacson K. Adenomyosis: review of the literature. J Minim
Invasive Gynecol. 2011;18:428–37.
4. Haas D, Chvatal R, Habelsberger A, Wurm P, Schimetta W, Oppelt P.
Comparison of revised American Fertility Society and ENZIAN staging:
a critical evaluation of classifications of endometriosis on the basis of
our patient population. Fertil Steril. 2011;95:1574–8.
5. Haas D, Wurm P, Shamiyeh A, Shebl O, Chvatal R, Oppelt P. Efficacy
of the revised Enzian classification: a retrospective analysis. Does the
revised Enzian classification solve the problem of duplicate
classification in rASRM and Enzian? Arch Gynecol Obstet. 2012; DOI:
10.1007/s00404-012-2647-1
6. Haas D, Shebl O, Shamiyeh A, Oppelt P. The rASRM score and the
Enzian classification for endometriosis: their strengths and
weaknesses. Acta Obstet Gynecol Scand. 2012;91:
DOI:10.1111/aogs.12026.
7. Koninckx PR, Martin DC. Deep endometriosis: a consequence of
infiltration or retraction or possibly adenomyosis externa? Fertil Steril.
1992 Nov;58(5):924-8.
8. Matalliotakis IM, Katsikis IK, Panidis DK. Adenomyosis: what is the
impact on fertility? Curr Opin Obstet Gynecol. 2005;17:261–4.
9. Schweppe KW. [Endometriosis — a disease that has no lobby].
Zentralbl Gynakol. 2003;125:233. German.
10. The American Fertility Society . Classification of endometriosis. Fertil
Steril. 1979;32:633–634
11. The American Fertility Society . Revised American Fertility Society
classification of endometriosis: 1985. Fertil Steril. 1985;43:351–352
12. Tuttlies F, Keckstein J, Ulrich U, Possover M, Schweppe KW, Wustlich
M, Buchweitz O, Greb R, Kandolf O, Mangold R, Masetti W, Neis K,
Rauter G, Reeka N, Richter O, Schindler AE, Sillem M, Terruhn V,
Tinneberg HR. [ENZIAN-score, a classification of deep infiltrating
endometriosis]. Zentralbl Gynakol. 2005;127:275–81. German.
Abkürzungsverzeichnis
AFS American Fertility Society
rAFS revised American Fertility Society
rASRM revised American Society for Reproductive Medicine

LEBENSLAUF
Name Dr. med. univ. Dietmar Haas
Anschrift Schubertstraße 40
A – 4020 Linz
Mobil: +43/650-5107473
E-mail [email protected]
Geburtsdatum 27. November 1973, Steyr
Familienstand verheiratet, zwei Kinder
Staatsbürgerschaft Österreich
Schulausbildung
1980 – 1984 Volksschule Mauthausen
1984 – 1992 Bischöfliches Gymnasium am Kollegium Petrinum in
Linz/Urfahr
Juni 1992 Matura
Studium
1992 – 1994 Studium WiTech (Wirtschaftsingenieurwesen Technische
Chemie) an der Johannes Kepler Universität Linz
1995 – 2005 Medizinstudium an der Karl Franzens Universität Graz
und Promotion
Famulatur
September 2003 Famulatur an der Inneren und Onkologischen Abteilung
der medizinischen Universitätsklinik Graz; Graz,
Österreich
März 2005 Famulatur an der Chirurgischen Abteilung des
Krankenhauses der Barmherzigen Brüder Graz; Graz,
Österreich
Juni 2005 Famulatur an der Internen Abteilung des Krankenhauses
der Barmherzigen Brüder Graz; Graz, Österreich
Juli 2005 Famulatur an der Allgemeinen Inneren und
Gastroenterologischen Abteilung der medizinischen
Universitätsklinik Graz; Österreich
August 2005 Famulatur an der Intensivstation (CCU) der
medizinischen Universitätsklinik Graz; Graz, Österreich
Berufspraxis
1999 – 2003 Selbständige Tätigkeit als Handelswarenpräsentator für
Medizinprodukte. Leitung von Mitarbeitern für Beratung
und Verkauf von Medizinprodukten.
September 2005 Ärztliche Tätigkeit und Weiterbildung in der
Tauchmedizin im Medical Center Kuramathi, Malediven
Leitung: Abteilung für Anästhesie der Universitätsklinik
Halle, Deutschland.
Jänner – März Turnusarzt im Krankenhause der Kreuzschwestern
2006 Sierning; Sierning, Östereich.
April 2006 - Turnusarzt im Allgemeinen Krankenhaus der Stadt Linz,
Jänner 2009 Linz, Österreich.
Seit Oktober 2008 Ausbildung zum Facharzt für Gynäkologie und
Geburtshilfe,
Abteilung für Gynäkologie und Geburtshilfe,
Allgemeines Krankenhaus der Stadt Linz, Österreich
Vorstand: Prim. Priv.-Doz. Dr. med. Peter Oppelt, MBA
Zusatzqualifikationen
Mai 2000 Teilnahme am 2 tägigen Management-Skills Seminar mit
Andreas Ackermann; Wien, Österreich.
2001 Pragmatische Diagnostik, Motivation und Therapie bei
Suchtkranken an der Psychiatrischen Abteilung der
medizinischen Universitätsklinik Graz; Graz, Österreich.
2004 – 2005 Vertiefte Ausbildung in der Notfallmedizin an der
medizinischen Universitätsklinik Graz, Graz, Österreich.
September 2005 Spezialausbildung für Tauchmedizin im Medical Center
Kuramathi, Malediven,
Leitung: Abteilung für Anästhesie der Universitätsklinik
Halle, Deutschland.
November 2006 Zertifikat Abdomen Sonographie Grundkurs
entsprechend der ÖGUM, LKH Hohenems; Hohenems,
Österreich.
Oktober 2007 bis Ärztekammer für Oberösterreich
Juni 2008 PSY 1 Diplom der ÖÄK: Psychosoziale Medizin
September 2008 Notarztdiplom der ÖÄK und ERC-ALS-Provider Diplom
2008 Absolvierung des Train the Trainer-Seminar zur
Schulung von Diabetes-Patienten, Ärztekammer für
Oberösterreich, Linz, Österreich.
November 2008 Bestandene Prüfung zum Arzt für Allgemeinmedizin und
Approbation für Allgemeinmedizin, Linz, Österreich
Dezember 2010 Ausbildung zum Qualitätsbeauftragten für
Gesundheitswesen
Allgemeines Krankenhaus der Stadt Linz, Österreich.
Dezember 2011 Zertifikat Grund-, Aufbau- und Abschlusskurs
Ultraschalldiagnostik nach den Richtlinien der KBV und
DEGUM, Charite Berlin, Berlin, Deutschland.
März 2012 Zertifikat Grundkurs Gynäkologische Endoskopie MIC I;
Allgemeines Krankenhaus der Stadt Linz, Österreich
Juli 2012 Zertifikat GCP – Kurs; Allgemeines Krankenhaus der
Stadt Linz, Österreich

Mitgliedschaften
OEGGG – Österreichische Gesellschaft für Gynäkologie und Geburtshilfe
DGGG - Deutsche Gesellschaft für Gynäkologie und Geburtshilfe
SEF – Stiftung Endometrioseforschung
EEL – Europäische Endometrioseliga