
Rolle der Internistischen Thorakoskopie im Management des ... · Rolle der Internistischen...
40
Rolle der Internistischen Thorakoskopie im Management des Pneumothorax Wolfgang Frank Lungenklinik Amsee Waren/Müritz DGP Thorakoskopiekurs St. Elisabeth & St. Barbara Kankenhaus, Halle 25. – 27. April 2012 Frühling am Tiefwarensee
Transcript of Rolle der Internistischen Thorakoskopie im Management des ... · Rolle der Internistischen...

Rolle der Internistischen Thorakoskopie im Management des Pneumothorax
Wolfgang FrankLungenklinik Amsee
Waren/Müritz
DGP ThorakoskopiekursSt. Elisabeth & St. Barbara Kankenhaus, Halle
25. – 27. April 2012
Frühling am Tiefwarensee

Historische Anmerkungen• 1860 – 1920: Tb Zeit -> Bettruhe• 1920 – 1960: „Gummischlauch“ Ära * ->
Thoraxdrainagen Lindskog GE. Spontaneous pneumothorax. Arch Surg 1957;75:69
• 1970 – 1990: Chirurgische Ära• 1990 – 2010: Differentialindikationen in der
Behandlung des PTX« The use of large-bore intercostal tubes as an initial method of drainage of PSP should now be considered as unacceptedmedical practice »Miller AC 2008

Therapieziele beim Spontanpneumothorax (SPTX)
•Beseitigung•Prävention
Mit wieviel Auwand und Patientenbelastung ?
Mit wieviel Aufwand und Patientenbelastung ?
+ -

Therapeutische Optionen beim Spontanpneumothorax
konservativinternistisch chirurgisch
(VATS, Mini-thorakotomie, formale Thorakotomie)
Beobachtungambulant/klinisch+ Analgetika+ low flow O2
- Absaugung (Aspiration)- englumige Drainage( 8-16 F)
- weitlumige Drainage (> 20 F)- Thorakoskopie+ Pleurodese (Tetrazyklin, „talcage“) + Kauterisation
- Resektion von Blasen und Bullae,
- Kauterisation- Strang- u. –Adhäsionslösung
- Pleurodese- Pleurektomie
interventionell

The PTX-debate still goes on in 2008.....
„A multiplicity of therapeutic options are available for treatment of PSP…. This and the paucity of …prospective randomized clinical trialsprobably explains why the present … opinion based expert guidelines are only poorly followed…“Noppen M et al Pneumothorax Respiration2008:76:121.

Rezidivraten* beim konservativ behandelten PTX
RezidivrateEreignis
Primärer PTXSpanne Mittel
Sekundärer PTXSpanne Mittel
nach Erst-ereignis
13-54 30% 39-52 47%
nach 1. Rezidiv 62% 69%
nach 2. Rezidiv 83% > 90%
* zu 70% innerhalb 2 Jahren, zu 25% bilateralB.T.S.R.C. 1993, V.A.C.S. Light 1990, Gobel 1963, Lippert 1991, Sadikot 1997
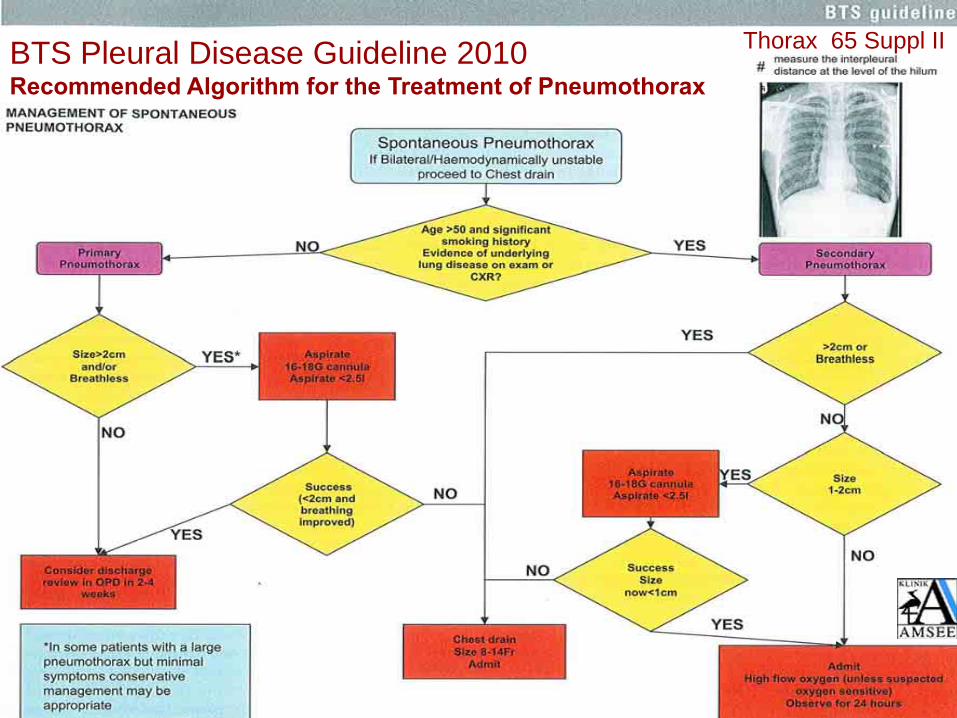
BTS Pleural Disease Guideline 2010 Recommended Algorithm for the Treatment of Pneumothorax
Thorax 65 Suppl II

Rolle der Thorakoskopie beim PTX - Pro?
Außer DiskussionSeropneumothoraxHämatopneumothoraxPyopneumothoraxMinimalpneumothorax (< 15%)
Im FokusInterventionspflichtiger Spontan(Spannungs)pneumothorax
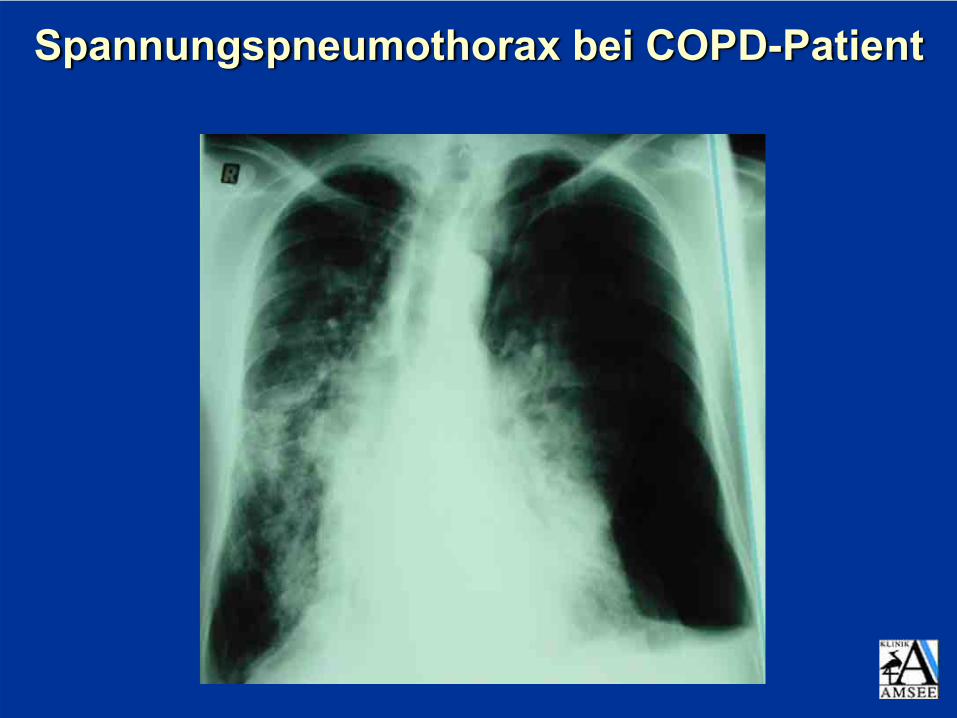
Spannungspneumothorax bei COPD-Patient

Erfolgsquoten der konservativen bzw. internistischen Therapie beim SPTX
Management PrimärerSPTX
Sekundärer SPTX
Beobachtung, O2Aspirationdünnlumige Katheter(< Ch 14)
Thoraxdrainagen(> Ch 20)
k. A. 59-83% (66%)84-94% (89%)
93-97% (95%)
k. A.31-67%(45%)80%*
92%*
Definition des Erfolgs: PTX-Liquidation innerhalb 7 (max. 10) Tagen und mindestens 30 Tage anhaltend
Noppen 2002, Baumann 2000, Conces 1998, Miller 1996, Light 1993, Matthys 1988, Videm 1987, Withers 1964 *inklusive multipler Drainagen

Aspiration (A) vs tube drainage (TD) inPSP 1st episode
• n= 137 randomised A vs TD• Results- recurrence rate 3 months: 15 / 8- recurrence rate 1 yr: 16 (22%) / 17 (24%)- recurrence rate 2 yrs: 20 (31%) /18 (24%)- complications: 1 (2%) / 5 (7%)- analgesia: 22 (34%) / 40 (56%)*- less hospital stay and inability to work in A*(* p < .05) Ayed AK Eur Respir J 2006;27:477
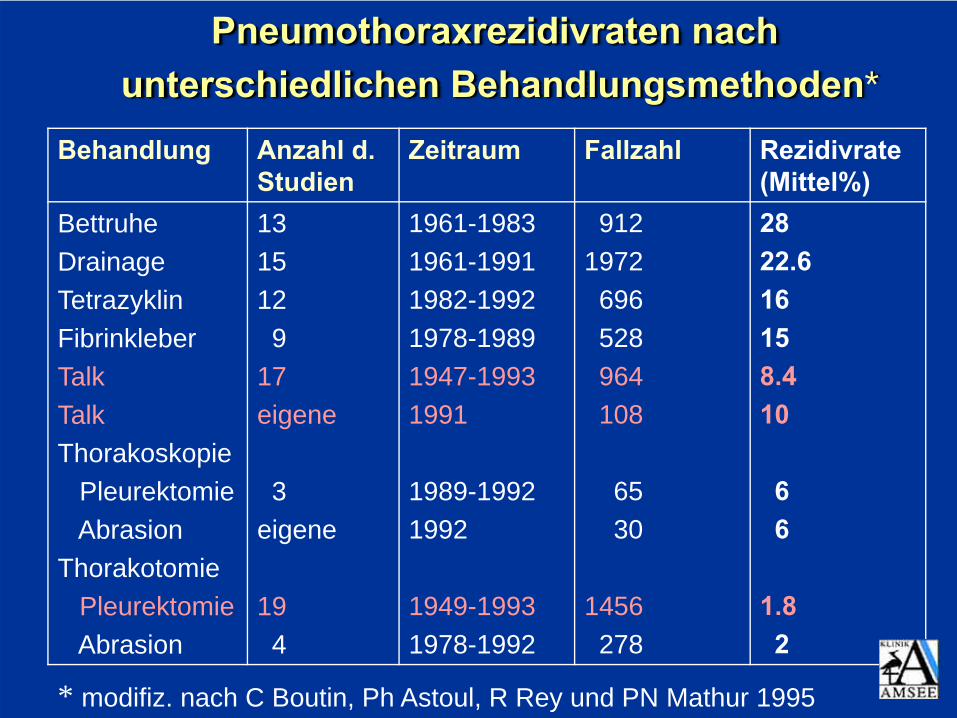
Pneumothoraxrezidivraten nachunterschiedlichen Behandlungsmethoden*
Behandlung Anzahl d. Studien
Zeitraum Fallzahl Rezidivrate (Mittel%)
BettruheDrainageTetrazyklinFibrinkleberTalkTalkThorakoskopie
PleurektomieAbrasion
ThorakotomiePleurektomieAbrasion
1315129
17eigene
3eigene
194
1961-19831961-19911982-19921978-19891947-19931991
1989-19921992
1949-19931978-1992
9121972696528964108
6530
1456278
2822.616158.410
66
1.82
* modifiz. nach C Boutin, Ph Astoul, R Rey und PN Mathur 1995

Thorakoskopische Talk-PoudragePleuraler Situs vor und nach Poudrage

VATS-Präparation bei der Bullaablation und der partiellen Pleurektomie

Thorakoskopisches Management des Pneumothorax
Akutmanagement/Prävention
Parameter
Prozedur
HospitalTage
Kosten€
Schmerzscore
Rezidiv-rate % Inst. 5 J
Drainage(n = 47)
7,4 + 3,9 10301081
5,0 - 1,8 21 34
Drainage +Talk (n= 61)
8,0 + 3,6 10691461
5,1 - 2,7 2 5
European Study on Medical Video-Assisted Thoracoscopy (ESMEVAT) in PSPTX: prospektiv, randomisiert, multizentrisch
Tschopp JM, Noppen M, Astoul P, Janssen et al. Eur Respir J, 2002,20:1003
Management des Spontanpneumothorax
Zwischenstatement
„Eine irgendwie geartete Prävention, i.d.R. die Durchführung der Pleurodese ist in den meisten Fällen des interventionspflichtigen SPTX eine
rationale, wenn nicht zwingende Option.“JM Tschopp 2002

Rolle der Thorakoskopie beim Pneumothorax (PTX) - Pro ?
….ist der thorakoskopische Befund in Relation zum
Aufwand relevant für das Management ?

Rolle der Thorakoskopie beim PTXWie groß ist der Aufwand?
Prämisseweitlumige Drainage = Therapieoptimum
• situative ad hoc Bereitstellung logistisch-personell möglich
• Trokarhülsentechnik erforderlich• 4-mm-Teleskop Minimalerfordernis• keine Prämedikation erforderlich• keine Bioptik erforderlich• kein chirurgischer Behandlungsraum erforderlich
Die Thorakoskopie beim PTX ist mit minimalem zusätzlichem Aufwand zur Drainagetherapie möglich = Minithorakoskopie
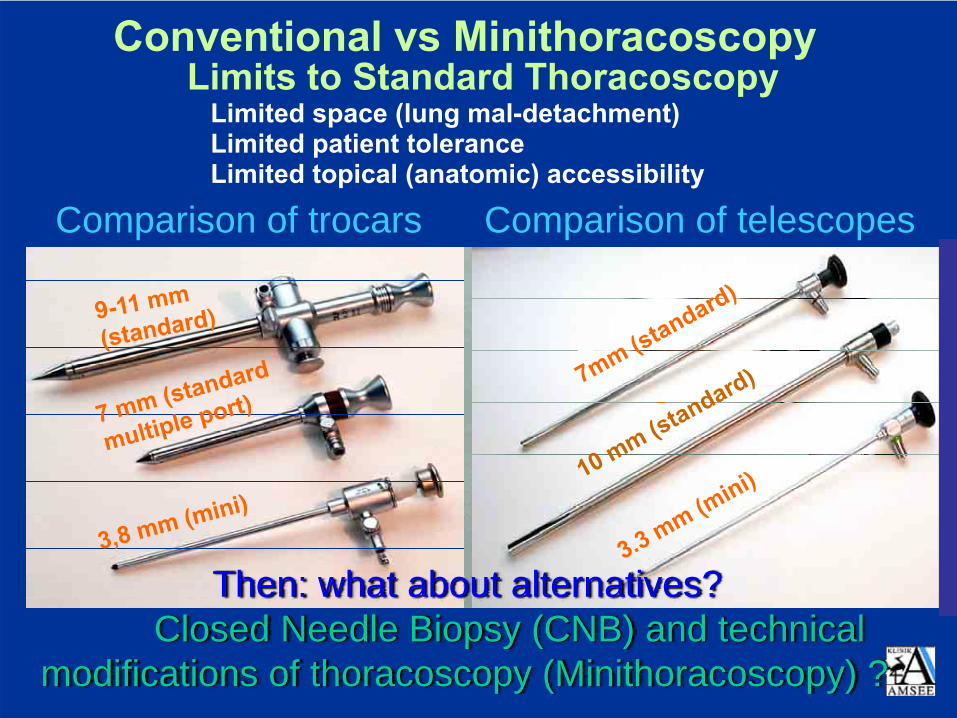
Conventional vs Minithoracoscopy
Comparison of trocars Comparison of telescopes
3 mm
Limits to Standard ThoracoscopyLimited space (lung mal-detachment)Limited patient toleranceLimited topical (anatomic) accessibility
Then: what about alternatives? Closed Needle Biopsy (CNB) and technical
modifications of thoracoscopy (Minithoracoscopy) ?

Rolle der Thorakoskopie beim PTX…….und was ist der Benefit?
• Lungenbeurteilung - prädisponierende Veränderungen? (primärer vs. sekundärer PTX)
• Lecksuche (Fluoreszin) und Leckbehandlung (Nd-YAG-Laser, Argonplasmabeamer)
• optimale Drainagepositionierung• Lösung von Adhäsionen• unmittelbare Überführung in Therapie („talcage“)• Indikationsstellung zur chirurgischen Therapie

Rolle der Thorakoskopie beim PTXMuster bzw. Klassifizierung endoskopischer
Befunde und ihre Häufigkeitsverteilung(Historische Stadieneinteilung)*
Muster (Typ) I
40%
Muster (Typ) II
12%
Muster (Typ) III
31%
Muster (Typ) IV
17%„idio-pathischer“ PTX, normal erscheinende Lunge („ELCs“)
pleurale Adhäsionen, dabei durch Einrisse gehäuft begleitender Hämatothorax
Blasen u. Bullae < 2 cm Ø
Bullae> 2cm Ø
* modifiziert nach SWIERENGA/VANDERSCHUEREN Lung (1990) Suppl. 1122

ELCs and microscopic inflammation in primary SPTX
Courtesy of JM Tschopp

Fluorescein Enhanced Autofluorescence Thoracoscopy (FEAT)
Noppen M. Am J Respir Care Med 2004;170:680-682
▪ True rupture of bullae/blebs/ELCs?• Pleural porosity?• Lung interstitium?
PSP: where is the air leak?

PTX Muster (Typ) IIausgedehnte Verwachsungsstränge

PTX Muster (Typ) III: „Blebs“ und Blasen < 2cm beim primären Spontanpneumothorax
(charakteristischerweise am Lappenrand)

PTX Muster (Typ) IV: zahlreiche Blasen > 2 cm und Bullae, vereinzelte Adhäsionen

Behandlung des komplizierten PTX mit einfacher Talkage in Lokalanästhesie
• PSP n=65; SSP n=28• Kurzzeiterfolgsrate 90/93 (97%)• Keine relevanten Komplikationen• Mittlere Beobachtungsdauer = 5.1 + 3.4(1.5 - 9.2) Jahre
• Langzeiterfolgsrate 80/84 (95%)
Tschopp et al, Thorax 1997; 52:329

Randomised controlled trial: simpletalcage under thoracoscopy (TT) versus
chest tube drainage (CTD)
• n = 108 -> 2 groups: CTD versus TT• no complication• failure rate 5% (TT) vs 27% (CTD): 5 yrs FU (p <.01)
• no difference in total costs• no difference in working capacity orresidual pain 1 month after leaving thehospital
Tschopp et al, Eur Respir J 2002;20:1003

Warum also keine simple Talkpoudrage in Lokalanästhesie ?

Präventive Interventionen bei SPTXBullektomie/Parenchymresektion oder
Pleurodese? Oder beides?• 6% RR in 72 pts mit allein VATS Bullektomievs 0% RR in 37 pts mit allein PleurodeseHatz, Ann Thor Surg 2000; 70: 253
• 16% RR in 50 pts mit Bullektomie allein vs1.9% RR in 53 pts mit VATS Bullektomie +PleurodeseHorio, Surg Endosc 2002; 16: 630
• 20% RR in 25 pts mit VATS Bullektomieallein vs 4% RR in 24 pts mit Bullektomie +PleurodeseLoubani, Respir Med 2000; 94: 888

Präventive Interventionen bei SPTXBullektomie/Parenchymresektion oder
Pleurodese? Oder beides?• In der Prävention ist die Pleurodese
(= Behandlung der ELCs) die entscheidende Intervention
• Die Bullektomie verbessert über die Pleurodese hinaus die Rückfallrate nicht signifikant und ist - außer bei großen Blasen (> 5 cm) - verzichtbar.
Eine diffuse Erkrankung braucht auch eine „diffuse“ Therapie!

Talkpoudrage beim Spontan-PTX

Treatment of PSP: preventionof recurrence: conclusions
• Simple talc pleurodesis by thoracoscopyis a safe, minimal invasive and cost-effectivetechnique to prevent recurrences of SP.
• It is not more painful than pleural drainageprovided adequate pain control byopioids.
• Patients should be given the choicebetween conservative treatment and talcpleurodesis by medical thoracoscopy
Baumann MH. Editorial Chest 2007;132:1110
ESMEVAT 2008

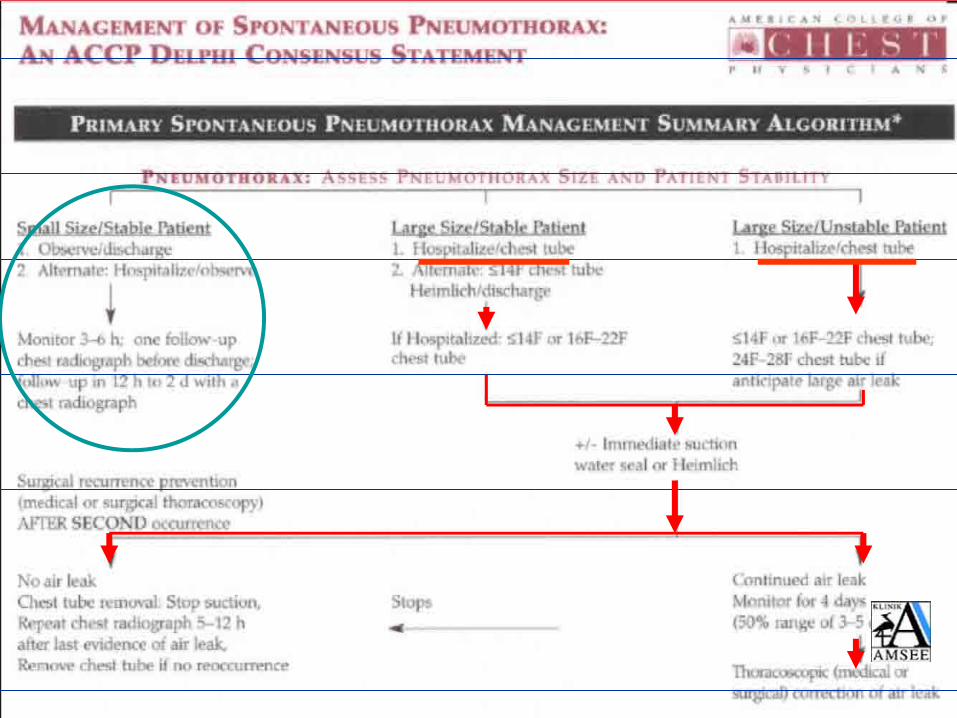
Derzeitige ACCP/BTS-Empfehlungen zum Management des SPTX-Erstereignis
Beobachtung +O2, Bettruhe
einfache Aspiration DLK WLK
primärer SPTX
sekundärerSPTX
RA-PTX und Spannungs-PTX
+ Thorako - skopie
Baumann et al. Chest 2001, 119:590
Davies RJO et al. Thorax 2003, 58, Suppl.11
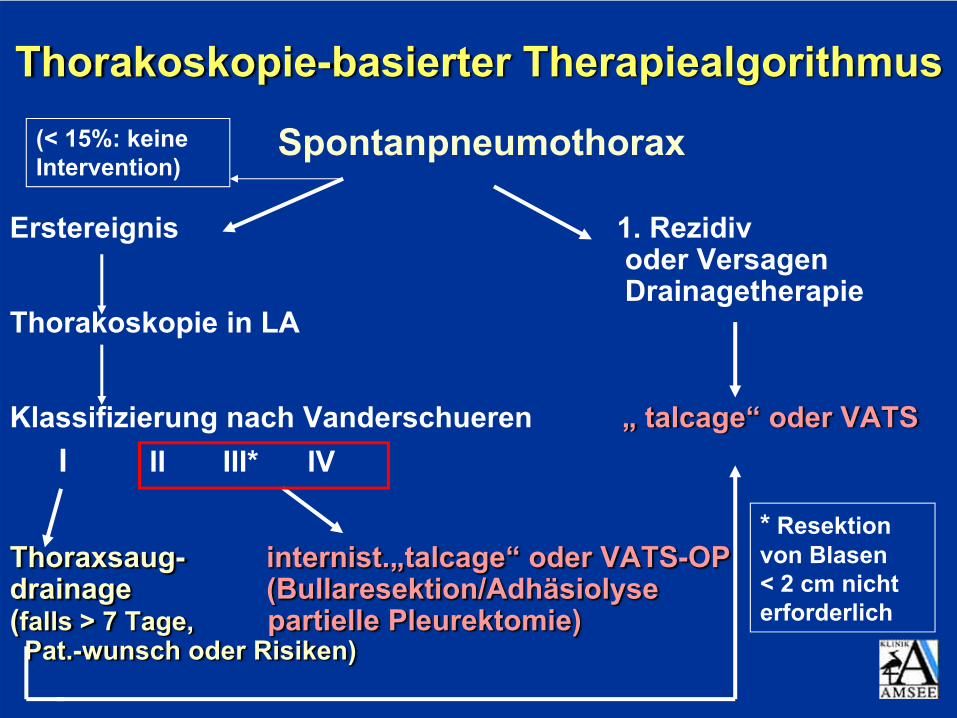
Thorakoskopie-basierter Therapiealgorithmus
Spontanpneumothorax
Erstereignis 1. Rezidivoder Versagen Drainagetherapie
Thorakoskopie in LA
Klassifizierung nach Vanderschueren „ talcage“ oder VATSI II III* IV
Thoraxsaug- internist.„talcage“ oder VATS-OPdrainage (Bullaresektion/Adhäsiolyse(falls > 7 Tage, partielle Pleurektomie)Pat.-wunsch oder Risiken)
* Resektion von Blasen < 2 cm nicht erforderlich
(< 15%: keine Intervention)

Sekundärer Spontan PTX
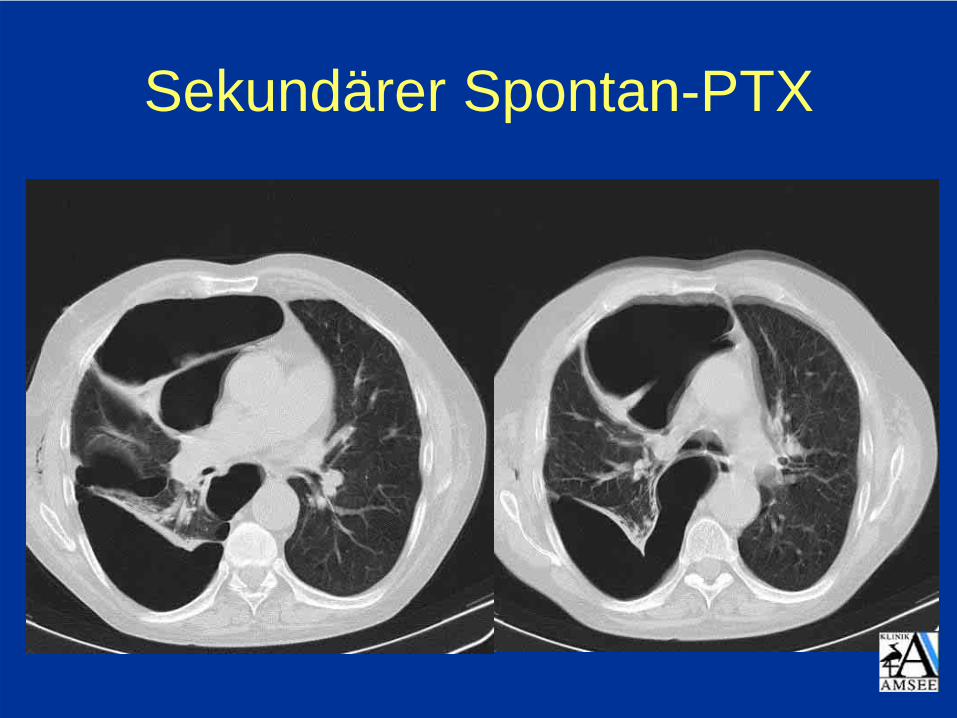
Sekundärer Spontan-PTX

ResüméeRolle der Thorakoskopie beim
Spontanpneumothorax….. beim interventionspflichtigen PTX
generell sinnvoll….. insbesondere in Verbindung mit
weitlumiger Drainageneinlage(identische Prozedur)
...... Grundlage der kostengünstigsten Präventivherapie („Talkage“)

Rolle der internistischen Thorakoskopiebeim PTX
Pro…aber Internist oder Chirurg ?(„Medical“ oder VATS) Wem „gehört“ der PTX ?
Bitte recht freundlich und jedem sein Teil!
WF








![Retrospektive Analyse zur Überprüfung der Wirksamkeit von ...¶ffentl.[1].pdf · Zentralvenöse Katheter (ZVK) kommen in der Hämatologie und internistischen Onkologie zur Infusion](https://static.fdokument.com/doc/165x107/5d47113e88c993066d8bae38/retrospektive-analyse-zur-ueberpruefung-der-wirksamkeit-von-ffentl1pdf.jpg)








