
Supportive Therapie & Lebensqualität in der GI-Onkologie ... · Urea/Lactic acid cream d Placebo...
28
Supportive Therapie & Lebensqualität in der GI-Onkologie 2010 Was muss man wissen ? Ralf-Dieter Hofheinz TagesTherapieZentrum am ITM & III. Medizinische Klinik Universitätsmedizin Mannheim
Transcript of Supportive Therapie & Lebensqualität in der GI-Onkologie ... · Urea/Lactic acid cream d Placebo...

Supportive Therapie & Lebensqualität in der GI-Onkologie 2010
Was muss man wissen ?
Ralf-Dieter Hofheinz
TagesTherapieZentrum am ITM & III. Medizinische Klinik
Universitätsmedizin Mannheim

Hand-Fuß-Syndrom
Hauttoxizität unter EGFR-Antagonisten
Studien
Lebensqualität und Hauttoxizität ?
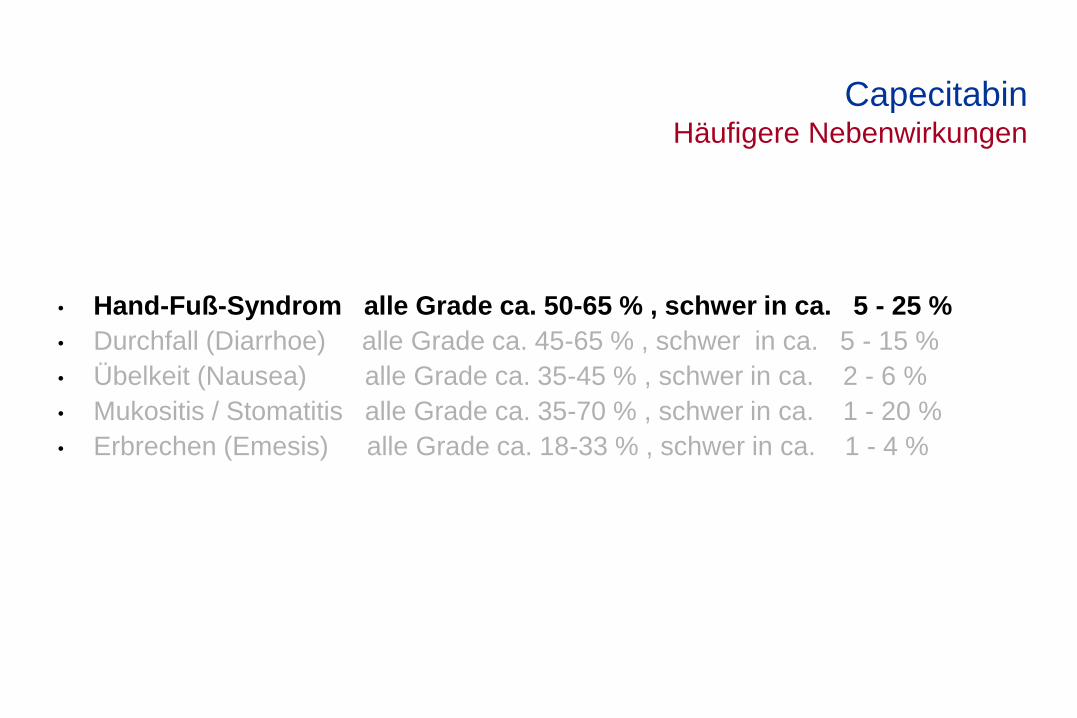
• Hand-Fuß-Syndrom alle Grade ca. 50-65 % , schwer in ca. 5 - 25 %
• Durchfall (Diarrhoe) alle Grade ca. 45-65 % , schwer in ca. 5 - 15 %
• Übelkeit (Nausea) alle Grade ca. 35-45 % , schwer in ca. 2 - 6 %
• Mukositis / Stomatitis alle Grade ca. 35-70 % , schwer in ca. 1 - 20 %
• Erbrechen (Emesis) alle Grade ca. 18-33 % , schwer in ca. 1 - 4 %
Capecitabin Häufigere Nebenwirkungen

Hand-Fuss-Syndrom
Hilft Pyridoxin (Vitamin B6) ?
GI-Tumoren
Strata
Cape mono
Cape / Cisplatin
Cape / Doce / Cisplatin
HFS ?
II oder III
Ran
do
mis
ati
on
Pyridoxin
200mg
Placebo
Ran
do
mis
ati
on
Pyridoxin
200mg
Placebo
Lee et al. ASCO 2007; abstr. 18S

Hand-Fuss-Syndrom
Hilft Pyridoxin (Vitamin B6) ?
GI-Tumoren
Strata
Cape mono
Cape / Cisplatin
Cape / Doce / Cisplatin
Pyridoxin
200mg
Placebo Ran
do
mis
ati
on
Lee et al. ASCO 2007; abstr. 18S
Pyridoxin Placebo
Patienten n = 180 n = 180
HFS II-III 32 % 31 %
Mediane Zyklen
bis HFS II-III
3 3
Mittlere Cape
Dosis bis HFS II-III
259.808
mg/m²
221.157
mg/m²

Hand-Fuss-Syndrom
Hilft Pyridoxin (Vitamin B6) ?
HFS ?
II oder III
Ran
do
mis
ati
on
Pyridoxin
200mg
Placebo
Lee et al. ASCO 2007; abstr. 18S
Pyridoxin-
naive
Patienten
Pyridoxin-naive mit
HFS II-III
n = 55
Randomisiert n = 44
Improvement
Verum vs Placebo
43 vs 48 %

Hand-Fuss-Syndrom
Hilft Urea-Handcreme ? Randomisierte, doppel-blinde Phase-III Studie
Tumoren
Kolonkarzinom
Mammakarzinom
Bronchialkarzinom
HFS ?
Moderat / severe CTC 3.0
(Primärer Endpunkt)
Urea/lactic acid
b.i.d.
Placebo
Ran
do
mis
ati
on
21 Tage
Wolf et al. ASCO 2010

0
5
10
15
20
25
30
35
40
Time (Days)
Urea/Lactic acid cream
Placebo
Pati
en
ts W
ith
Mil
d-S
evere
HF
S (
%)
1 7 14 21
Hand-Fuss-Syndrom (HFS) Patient-reported daily HFS during cycle 1 (days 1 – 21)
Wolf et al. ASCO 2010
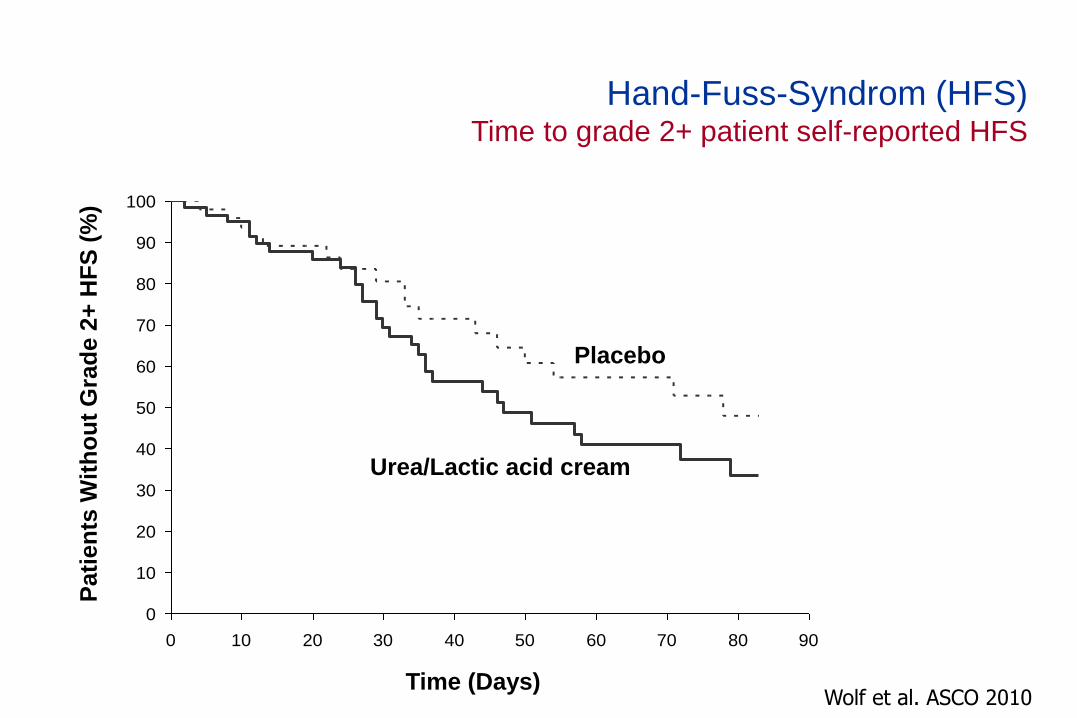
Hand-Fuss-Syndrom (HFS) Time to grade 2+ patient self-reported HFS
Wolf et al. ASCO 2010
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90
Time (Days)
Pati
en
ts W
ith
ou
t G
rad
e 2
+ H
FS
(%
)
Urea/Lactic acid cream
Placebo
1.0
0.8
0.6
0.4
0.2
0.0
Geschätzte Wahrscheinlichkeit
Monate
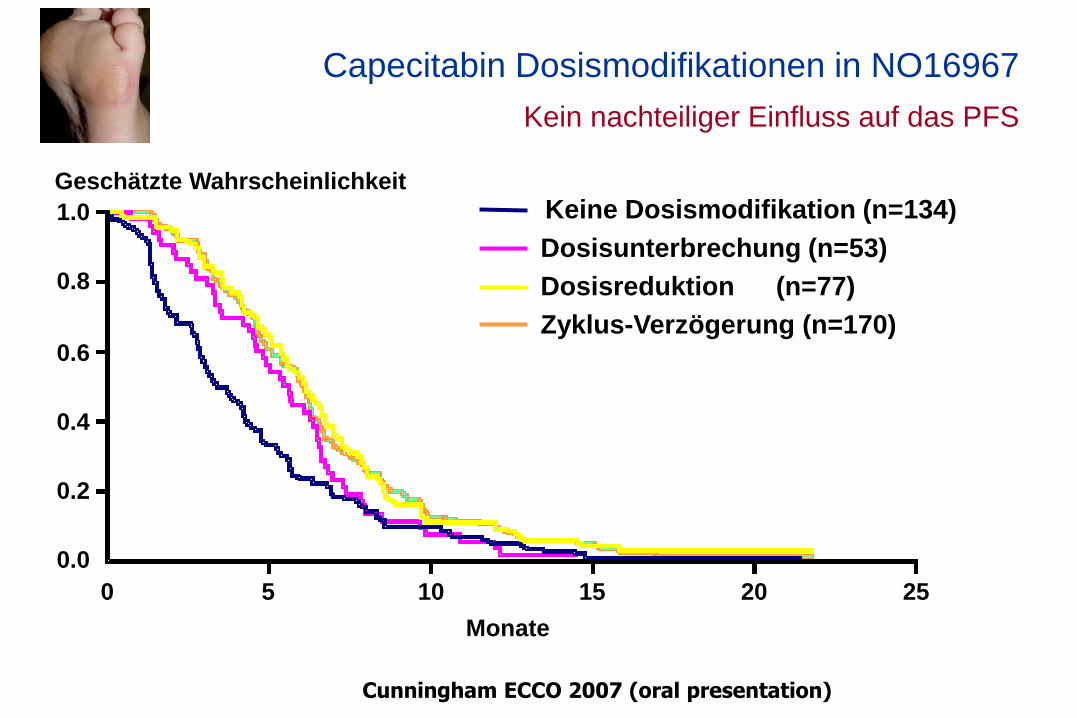
Dosisunterbrechung (n=53)
Dosisreduktion (n=77)
Zyklus-Verzögerung (n=170)
Keine Dosismodifikation (n=134)
0 5 10 15 20 25
Capecitabin Dosismodifikationen in NO16967
Kein nachteiliger Einfluss auf das PFS
Cunningham ECCO 2007 (oral presentation)

Data on file
Metaanalyse der Capecitabin Zulassungsstudien
Gesamtüberleben mit / ohne Hand-Fuss-Syndrom
Hand-Fuss-Syndrom
Kein Hand-Fuss-Syndrom
• Bei Patienten mit schmerzhaften Hand- oder Fußinnenflächen
(d.h. ab Grad 2 HFS ) sollte Behandlung sofort pausiert werden.
• Hände der Patienten immer zeigen lassen !
• Grad-2-Nebenwirkungen klingen in der Regel nach 3-6 Tagen ab.
• Pausen & Dosisreduktionen mindern nicht den Therapieerfolg.
Hand-Fuss-Syndrom
Management

Hand-Fuß-Syndrom
Hauttoxizität unter EGFR-Antagonisten
Studien
Lebensqualität und Hauttoxizität ?
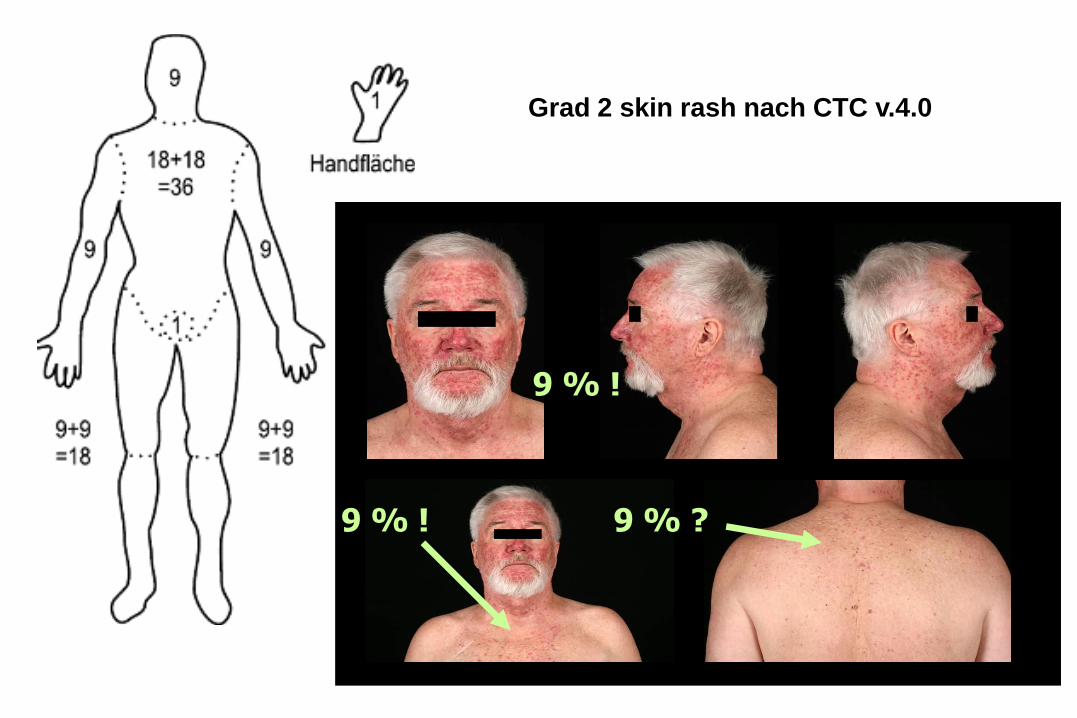
9 % !
9 % ! 9 % ?
Grad 2 skin rash nach CTC v.4.0

Hauttoxizität Umfrage (n=149); Gradierung des Ausschlags ?
Grad 1
Grad 2
Grad 3
10 %
59 %
31 %
Hassel et al. Onkologie 2010

n
Watch & wait 3
Lokal
Hydrokortison
Metronidazol
Erythromycin
Nadifloxacin
Clindamycin
Pimecrolimus
135 (91%)
55
47
40
12
13
12
Systemisch
Doxycyclin
Minocyclin
Isotretionin
95 (64%)
50
47
3
Hauttoxizität Therapie (Mehrfachnennungen !) (n = 149)
Internistische Onkologen
22 % für präemptive Therapie
9 % Überweisung an Dermatologen
Dosisreduktion 3 % vs. 4 %
Therapie-Pause 15 % (IO) vs. 3 % (DO)
Hassel et al. Onkologie 2010
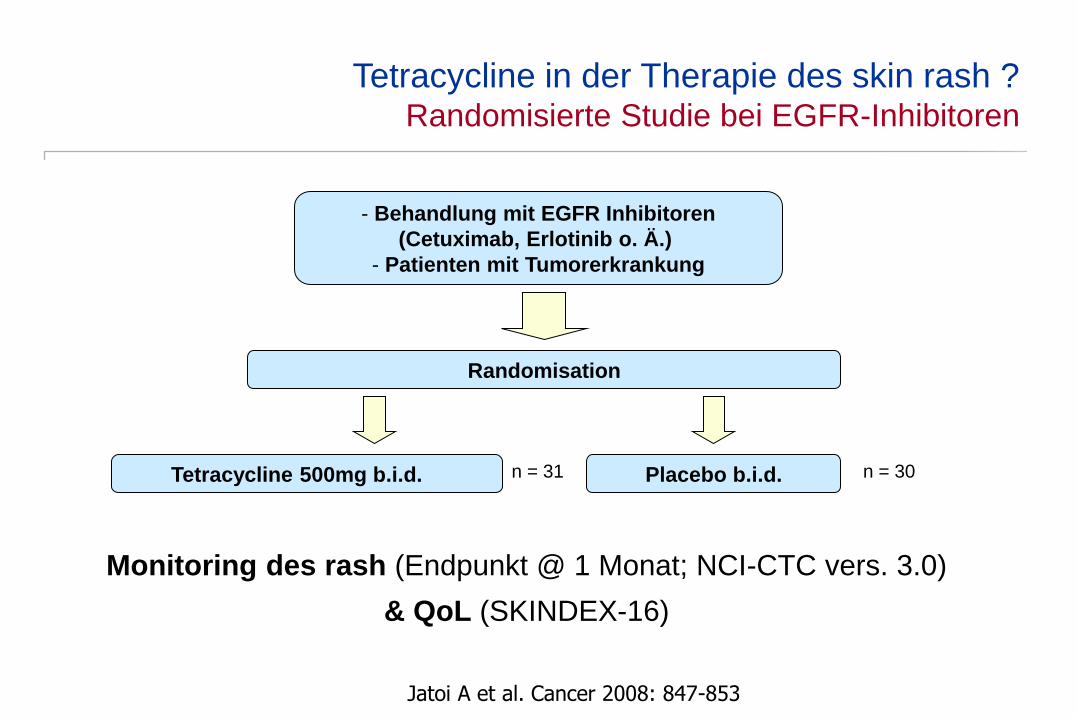
Tetracycline in der Therapie des skin rash ? Randomisierte Studie bei EGFR-Inhibitoren
Jatoi A et al. Cancer 2008: 847-853
Randomisation
Placebo b.i.d. Tetracycline 500mg b.i.d.
- Behandlung mit EGFR Inhibitoren
(Cetuximab, Erlotinib o. Ä.)
- Patienten mit Tumorerkrankung
n = 31 n = 30
Monitoring des rash (Endpunkt @ 1 Monat; NCI-CTC vers. 3.0)
& QoL (SKINDEX-16)

Tetracycline in der Therapie des skin rash ? Rash Inzidenz und Schweregrade
Jatoi A et al. Cancer 2008: 847-853
„Physician reported rash“
Zeitpunkt Tetracyclin Placebo p-Wert
4-Wochen
(alle Schwergrade)
15 (70%) 22 (76%) n.s.
4-Wochen (Grad 2
oder >50% BSA)
4 (17%) 16 (55%) 0,009
8-Wochen
(alle Schwergrade)
13 (87%) 16 (84%) n.s.
4-Wochen (Grad 2
oder >50% BSA)
4 (27%) 9 (47%) n.s.

Tetracycline in der Therapie des skin rash ? Serieller SKINDEX-16 score
Jatoi A et al. Cancer 2008: 847-853
Tetracycline
Placebo

Skin rash – Stepp Studie Präemptive versus reaktive Theapie
Randomisation
Therapie reaktiv Therapie präemptiv (Tag –1)
Q2W: Panitumumab 6 mg/kg + FOLFIRI
Q3W: Panitumumab 9 mg/kg + Irinotecan
n = 48 n = 47
Lacouture et al. J Clin Oncol 2010

Primäres Zielkriterium
Inzidenzraten von Hauttoxizität ≥ Grade 2 bei Patienten mit präemptiver versus reaktiver Behandlung der Hauttoxizität innerhalb 6-Wochen-Periode
STEPP-Studie: Panitumumab +(Folf)Iri Präemptive oder reaktive Therapie der Hauttoxizität ?
Therapie
Skin moisturizer – Gesicht, Hände, Füsse, Hals, Rücken, Brust morgens
Sonnencreme (LSF ≥ 15, UVA/UVB Protektion) – exponierte Areale
Topisches Steroid (1% Hydrocortison-Creme) – abends
Doxycycline 100 mg BID
Lacouture et al. J Clin Oncol 2010

n (%) Wochen
Pre-emptive 14 (29) nr
Reactive 29 (62) 2.7 (2.1, 6.3)
HR = 0.4 (95% CI: 0.2 - 0.7)
Wochen
Survival Distribution Function
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8
STEPP-Studie Primärer Endpunkt – Time to first occurence of Grade 2 skin toxicity
Lacouture et al. J Clin Oncol 2010
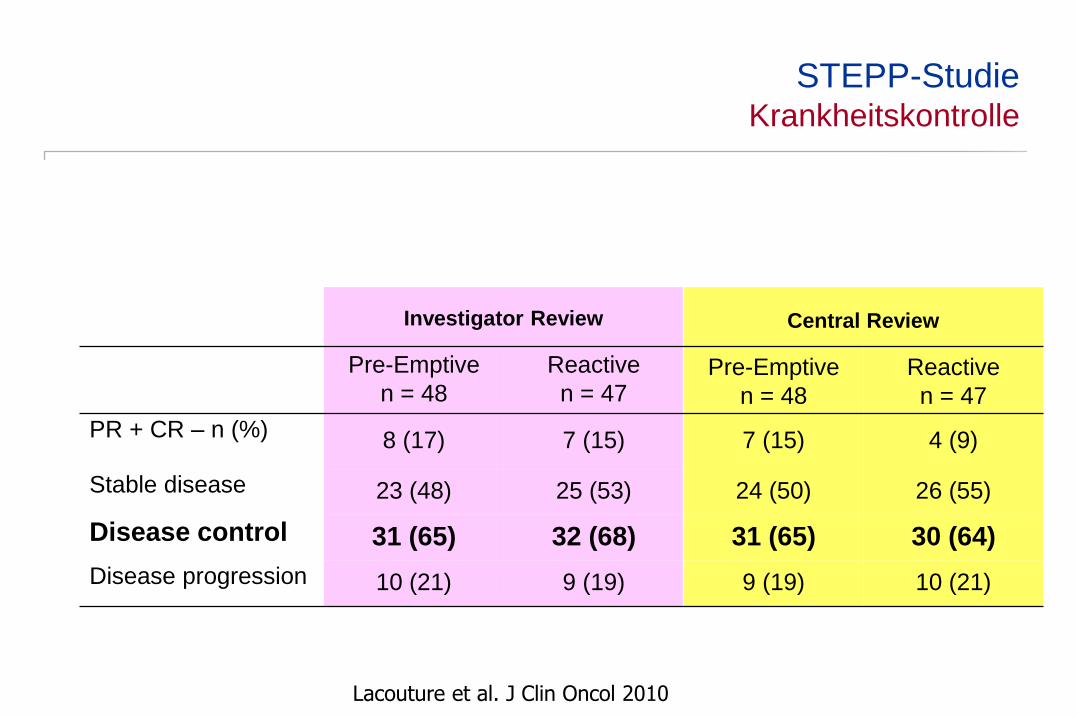
Investigator Review
Central Review
Pre-Emptive
n = 48
Reactive
n = 47 Pre-Emptive
n = 48
Reactive
n = 47
PR + CR – n (%) 8 (17) 7 (15) 7 (15) 4 (9)
Stable disease 23 (48) 25 (53) 24 (50) 26 (55)
Disease control 31 (65) 32 (68) 31 (65) 30 (64)
Disease progression 10 (21) 9 (19) 9 (19) 10 (21)
STEPP-Studie Krankheitskontrolle
Lacouture et al. J Clin Oncol 2010
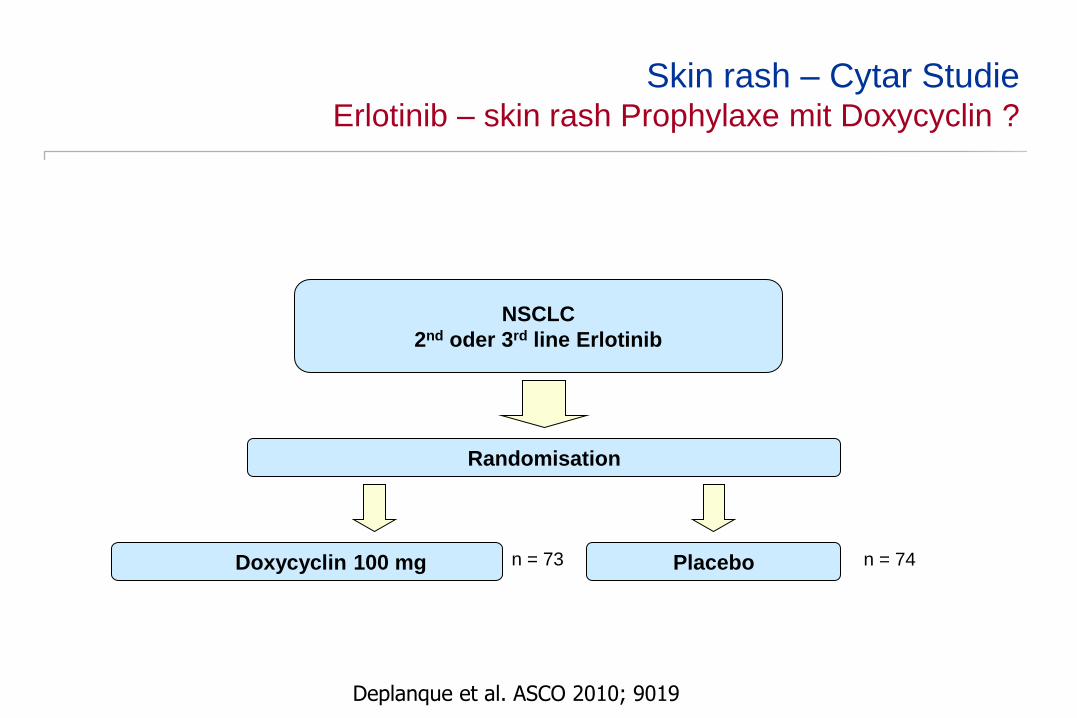
Skin rash – Cytar Studie Erlotinib – skin rash Prophylaxe mit Doxycyclin ?
Randomisation
Placebo Doxycyclin 100 mg
NSCLC
2nd oder 3rd line Erlotinib
n = 73 n = 74
Deplanque et al. ASCO 2010; 9019

Deplanque et al. ASCO 2010; 9019
Skin rash – Cytar Studie Inzidenz des skin rash während der ersten 4 Monate
61
18
35
62
4
18
0 2
0
10
20
30
40
50
60
70
Grad 1 Grad 2 Grad 3 Grad 4
Doxycyclin
Placebo
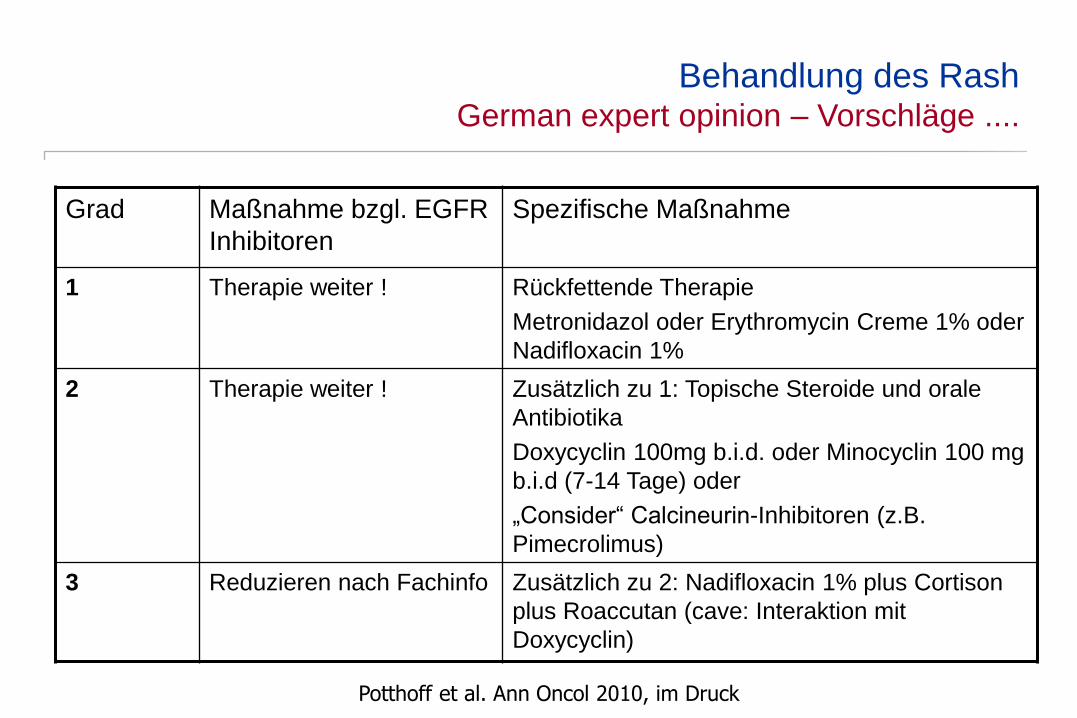
Behandlung des Rash German expert opinion – Vorschläge ....
Grad Maßnahme bzgl. EGFR
Inhibitoren
Spezifische Maßnahme
1 Therapie weiter ! Rückfettende Therapie
Metronidazol oder Erythromycin Creme 1% oder
Nadifloxacin 1%
2 Therapie weiter ! Zusätzlich zu 1: Topische Steroide und orale
Antibiotika
Doxycyclin 100mg b.i.d. oder Minocyclin 100 mg
b.i.d (7-14 Tage) oder
„Consider“ Calcineurin-Inhibitoren (z.B.
Pimecrolimus)
3 Reduzieren nach Fachinfo Zusätzlich zu 2: Nadifloxacin 1% plus Cortison
plus Roaccutan (cave: Interaktion mit
Doxycyclin)
Potthoff et al. Ann Oncol 2010, im Druck

Behandlung des skin rash AIO QoL 0110 – Studie (n = 100 geplant)
Randomisation
Erythromycin Creme 2% Doxycyclin 100mg 1-0-1
Behandlung mit Panitumumab im Label
Doxycyclin 100mg 1-0-1
QoL !!
Vergleich Scoring Systeme (CTC, WoMo, MESTT)
Nicht-Unterlegenheits-Design @ 8 Wochen

Behandlung des skin rash E-Vita – Studie (n = 120 geplant)
Doxycyclin etc. à la STEPP-Studie
Placebo (Reconval) Vitamin K1-Creme (Reconval K)
Behandlung mit FOLFIRI-Cetuximab im Label
Überlegenheitsdesign: Grad 2-3 Hauttoxizität von 30 auf 15%
QoL !!
Randomisation













![Nitrogen Quadrupole Coupling in Ethyl Isocyanide, C H NCzfn.mpdl.mpg.de/data/Reihe_A/40/ZNA-1985-40a-0043.pdfdrupole hyperfine structure (hfs) [1 3] because of the very narrow splittings.](https://static.fdokument.com/doc/165x107/607749a091cff529630f6f20/nitrogen-quadrupole-coupling-in-ethyl-isocyanide-c-h-nczfnmpdlmpgdedatareihea40zna-1985-40a-0043pdf.jpg)



