




![AUGEN INFEKTIONEN, SPEZIALITÄTEN DER …elettan.eok.sote.hu/uploads/File/nemet/wahlkurs/Auge-Herz-ZNS.pdf · Hordeolum- „Gerstenkorn ... Microsoft PowerPoint - Ppt0000003 [Írásvédett]](https://static.fdokument.com/doc/165x107/5b81bf1a7f8b9ae87c8cfd31/augen-infektionen-spezialitaeten-der-hordeolum-gerstenkorn-microsoft.jpg)

Sprachen
Seiten
Rechtliche

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 1
Panton‐Valentine‐Leukozidin exprimierendeS. aureus: Infektionen und Epidemiologie
Leif G. Hanitsch1, Renate Krüger2, Rasmus Leistner3, Sylke Schneider‐Burrus4
* Interdisziplinäre Arbeitsgruppe ‚PVL+ S. aureus‘ aus Dermatologie, Pädiatrie, Immunologie/ Innere Medizin und Krankenhaushygiene

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 2
Was ist PVL?
Erstbeschreiber: Philip Noel Panton und Francis Valentine

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 3
Kobayashi et al., The American Journal of Pathology, 2015
Abszessbildung durch S. aureus

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 4Boyle‐Vavra et al., Laboratory Investigation 2007
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 5
Welche Krankheiten sind mit Panton‐Valentine‐Leukocidinpositiven S. aureus assoziiert?

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 6
Multiloculäre Hautabszesse ohne Vorerkrankungen
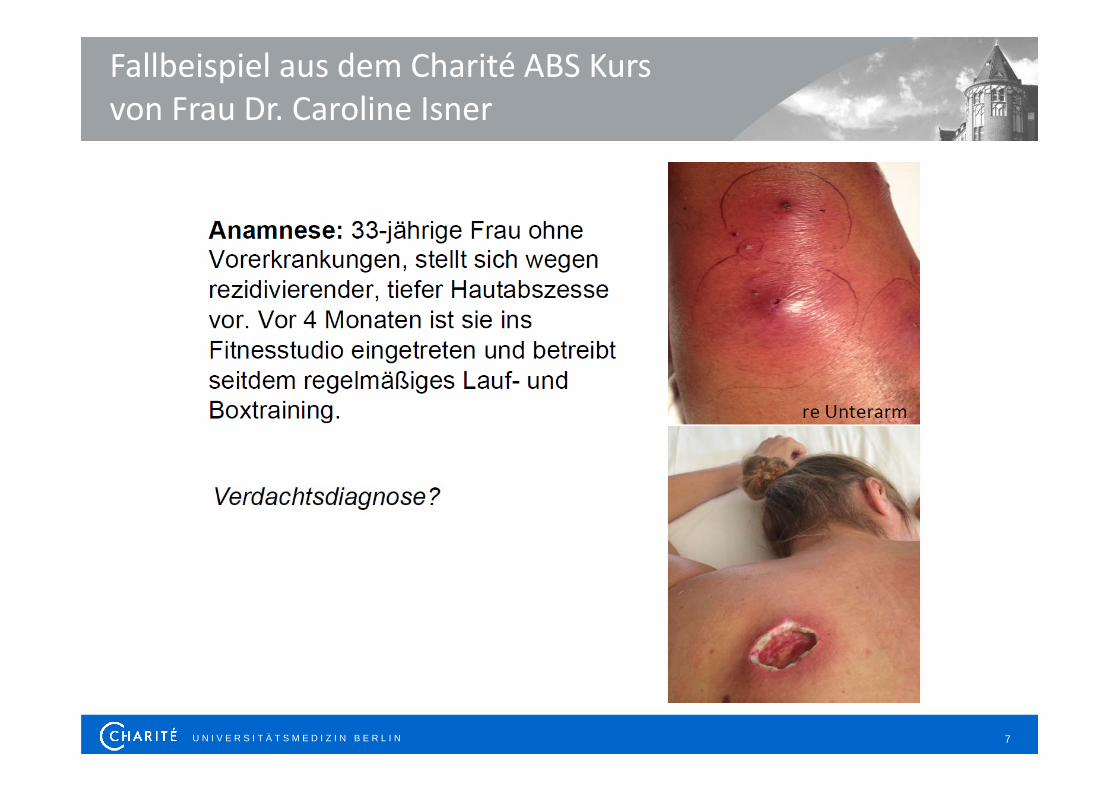
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 7
Fallbeispiel aus dem Charité ABS Kurs von Frau Dr. Caroline Isner

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 8
Auch häufig : Hordeolum (Gerstenkorn)

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 9
Welche Infektionen werden häufig verursacht durch PVL‐positive S. aureus?
‐ Abszesse, Furunkel !!!!!!‐ Knochen‐, Muskel‐, Gelenk‐Infektionen ?‐ (Nekrotisierende) Pneumonien ?‐ Blutstrominfektionen ?
Shallgross et al., Lancet Infect Dis 2013; 13: 43–54

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 10
Shallgross et al., Lancet Infect Dis 2013; 13: 43–54
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 11
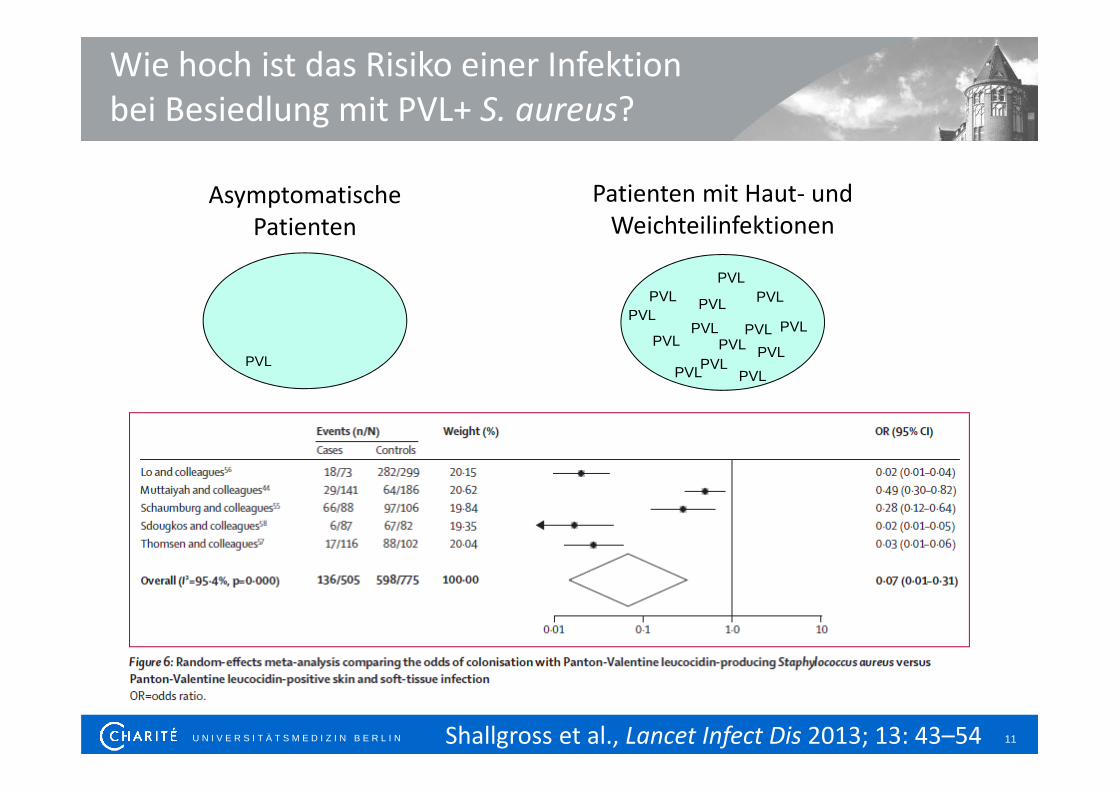
Wie hoch ist das Risiko einer Infektion bei Besiedlung mit PVL+ S. aureus?
Asymptomatische Patienten
Patienten mit Haut‐ und Weichteilinfektionen
PVLPVL
PVL
PVL
PVL
PVLPVL
PVLPVL
PVL
PVL
PVL
PVL
PVL
PVL
Shallgross et al., Lancet Infect Dis 2013; 13: 43–54

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 12
Antikörper gegen PVL?
Hermos et al., CID 2010:51

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 13Thurlow et al., FEMS Immunol Med Microbiol. 2012
Dominanter USA300 Klon aus Ca‐MRSA: *Situation in den U.S.A

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 14
Beispiel eines Ausbruchs mit PVL+ S. aureus

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 15
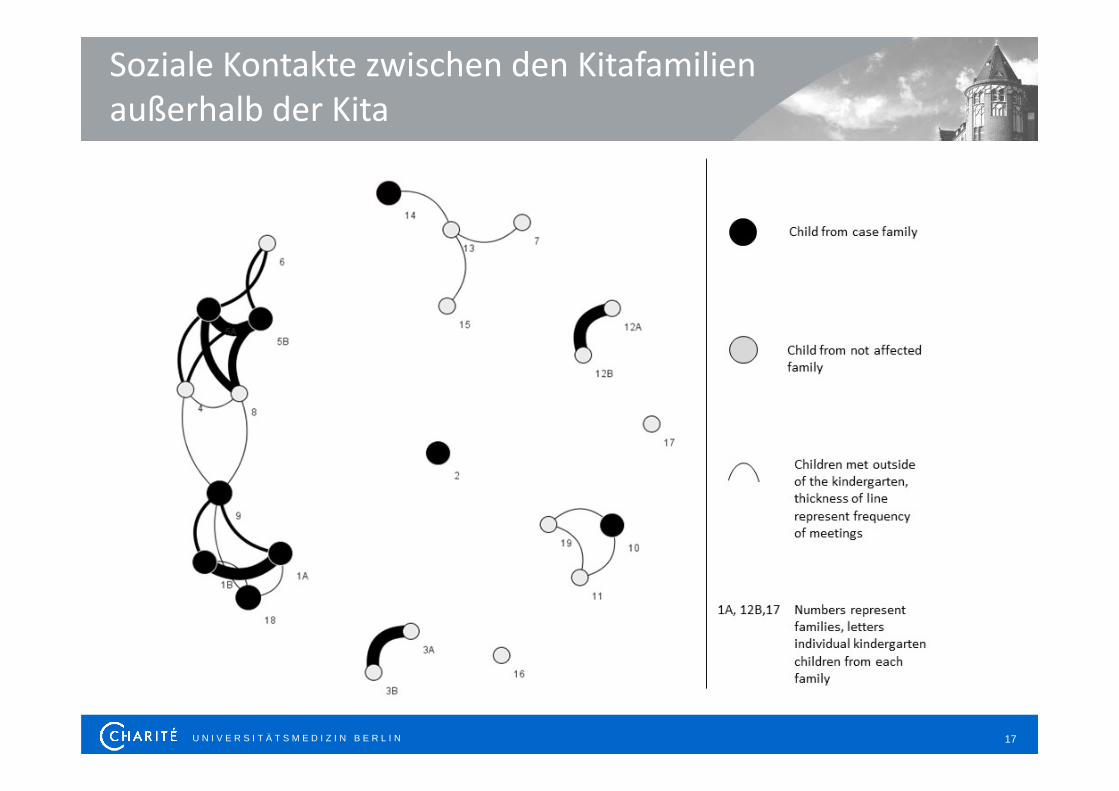
‐ 18 Familien
‐ 24 Kinder
‐ 4 Familien mit PVL Nachweis
‐ 5 Familien symptomatisch
‐ 2 Familien nur kolonisiert (9 Pers.)
‐ 2 Familien Nachweis & Symptome
PVL Ausbruch in Kitafamilien
Nachweis Erkrankung
KiTa

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 16
MSSA mit Cotrimoxazol Resistenz
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 17
Soziale Kontakte zwischen den Kitafamilien außerhalb der Kita
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 18
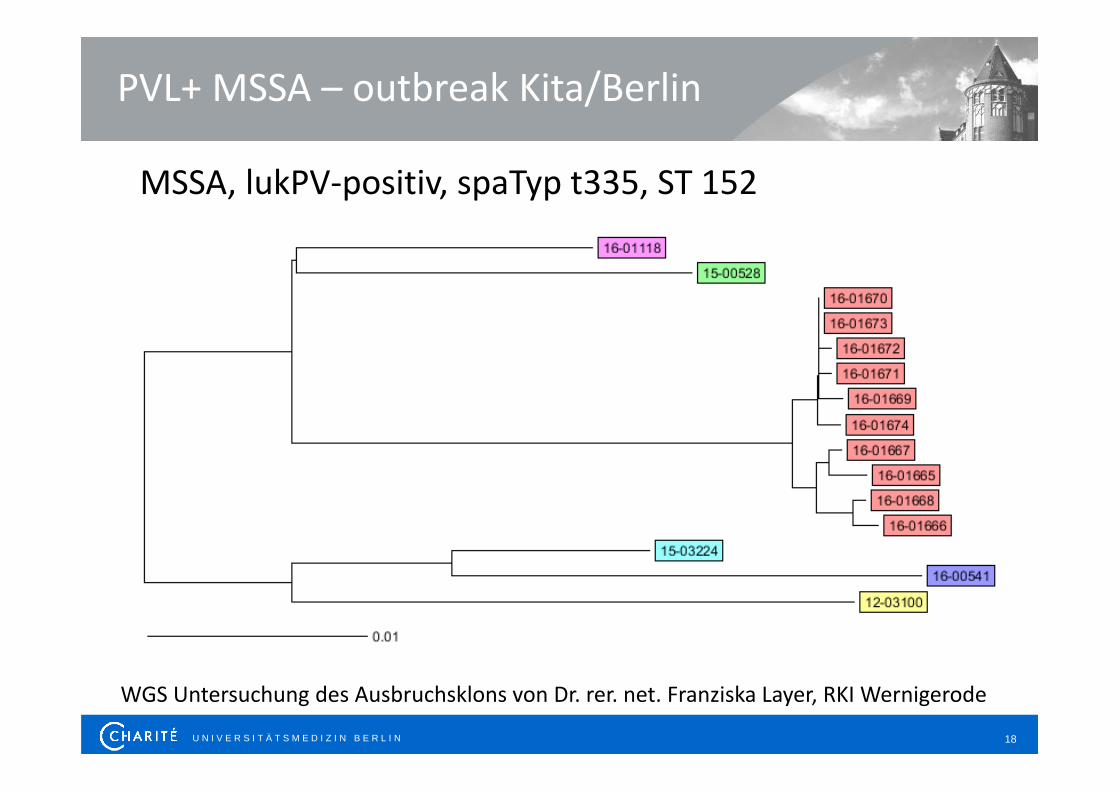
PVL+ MSSA – outbreak Kita/Berlin
WGS Untersuchung des Ausbruchsklons von Dr. rer. net. Franziska Layer, RKI Wernigerode
MSSA, lukPV‐positiv, spaTyp t335, ST 152

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 19
Wie: Kombination von Nasen‐, Rachen‐ , Haut‐dekolonisation und Desinfektion der Umgebung
Nase: Mupirocinsalbe (Kat IB) oder Octenidin‐Nasensalbe (Kat II) je 3mal täglich für 5 Tage
Rachen: Orales applizierbares Antiseptikum (Kat II) Chlorhexdin/ Octenidol
Haut: Antiseptische Waschungen (Kat II) Octenisan
Dekolonisation bei PVL grundsätzlich möglich

U N I V E R S I T Ä T S M E D I Z I N B E R L I N 20
Zum Download: Schema für ambulante Dekolonisation
3 Charité Ambulanzen (Dermatologie/Pädiatrie/Innere)
www.pvl‐abszess.de
U N I V E R S I T Ä T S M E D I Z I N B E R L I N 21
Bei rezidierenden, massiven Abszessen bei sonst gesunden Patienten: an PVL
denken!
www.pvl‐abszess.de
Vielen Dank!
Top Related