Albumintherapie bei Patienten mit LeberzirrhoseASCITES Schrier, Arroyo, et al. Hepatology (1988)...
42
Albumintherapie bei Patienten mit Leberzirrhose Alexander Zipprich Universitätsklinik und Poliklinik für Innere Medizin I Martin-Luther-Universität Halle-Wittenberg
Transcript of Albumintherapie bei Patienten mit LeberzirrhoseASCITES Schrier, Arroyo, et al. Hepatology (1988)...
-
Albumintherapie bei Patienten mit Leberzirrhose
Alexander ZipprichUniversitätsklinik und Poliklinik für Innere Medizin I
Martin-Luther-Universität Halle-Wittenberg
-
Transparenzerklärung
Hiermit lege ich offen, dass ich von folgenden Firmen finanzielle Unterstützung erhalten habe, die sich auf Vorträge, Beratertätigkeit, ungebundene Forschungsunterstützung oder sonstige medizinisch-wissenschaftliche Leistungen bezieht:
− Abbvie − Bayer Vital − Gilead − Grifols − OmniaMed − Norgine
Unentgeltliche Aktivitäten, z.B. für Non-Profit Organisationen: − Keine
Sonstige Interessen, die den Vortrag unangemessen beeinflussen könnten: − Keine
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
Natürlicher Verlauf Zirrhose
KompensierteZirrhose
DekompensierteZirrhose
Entwicklung der Zirrhose
Tod
Chronische Leber-
erkrankung
Entwicklung von Komplikationen OLT
Akute Leber-
erkrankung
• Aszites• Ösophagusvarizenblutung• Enzephalopathie• Ikterus
HCCZipprich et al. Liv Int 2012
-
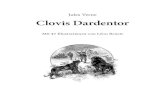
Häufigkeit der Dekompensationsereignisse
Tod 10%}
} Aszites 33%Blutung 10%}
}HCC 9%}
PSE 5%
Ikterus 3%
and in a decompensated stage 90 and 97% (P < 0.00001)(Figure 2d).
The cumulative incidence of encephalopathy and ofjaundice are shown in Figure 2e–f, together with mortal-ity after the development of each.
Prognostic stages of cirrhosisThe number of patients entering each of the five prog-nostic stages (at diagnosis or during the follow-up) isreported in Figure 3 together with 20-year incidence ofcompeting events per each stage. Five-year transitioning
intensity and mortality per each prognostic stage isreported in Table 6.
There were 202 patients with compensated cirrhosiswithout oesophageal varices (stage1). After 20 years, 163had disease progression, while 39 were still in this stage.Fourteen patients bled in this stage: 10 bled from variceswhich were not present at previous endoscopy (1 to3 years before); no varices were found in the remainingfour patients in whom portal hypertensive gastropathywas the most likely source of bleeding, althoughthere was no active bleeding at the time of endoscopy.
100
8060
4020
0
0251377
494 344 261 190 1445 41132117
309 186 14160 120 180 240
Decompensated
% surviving
CompensatedN = 377
N = 494
N = 117
Total
P < 0.00001
(a) 100
8060
4020
0
0 60 120 180 240377 274 203 146 109
Decompendationand death 4%
Death 10%
Decompensation 58%
% developing eventcompensated: 377 patientsCumulative event rate 72%
(b) 100
8060
4020
0
0203377 274 146 109
60 120 180 240
% first event occurring in compensatedpatients Cumulative incidence 71%
a death 10%b ascites 33%c bleeding 10%d hcc 9%e pse 5%f jaundice 3%
a
c
b
def
(c)
100
8060
4020
0
0 60 120 180 240243 152 89 74 52
Incidence of varices N = 243
53%
26%Death beforedeveloping varices
(d) 100
8060
4020
0
0132326 195 86 56
60 120 180 240
% surviving after development ofvarices, N = 326
(e)
100
8060
4020
0
0 60 120 180 240211 176 131 96 73136 78 55 39 28
Cumulative Incidenceof decompensation %
Varices N = 136
P < 0.0001
No varices 211
(f)
Cumulative incidence of event %
Figure 1 | Twenty-year survival and cumulative incidence of clinical events. Cumulative incidence is computed bycompeting risks analysis and each curve represents the probability of each specific outcome summed to the outcomeprobability represented in the next curve below. Survival curves are computed by the Kaplan–Meier method. The x-axis represents time in months and the numbers below the x-axis are patients at risk. (a) Survival of the whole seriesand, respectively, of compensated and decompensated patients at diagnosis. (b) Cumulative incidence ofdecompensation. Death and death at the time of first decompensation are shown as competing events. (c)Cumulative incidence of events presenting as a first event in 377 patients with compensated cirrhosis at thediagnosis. Twenty-year proportions of patients presenting each first event are reported in the box. (d) Cumulativeincidence of oesophageal varices. Death is shown as a competing event. Arrows indicate the 20-year incidence of thetwo competing events. (e) Survival of patients after development of varices. (f) Cumulative incidence ofdecompensation in patients with and without varices at diagnosis.
1186 Aliment Pharmacol Ther 2014; 39: 1180-1193ª 2014 John Wiley & Sons Ltd
G. D’Amico et al.
D’Amico G et al, APT, 2014
-
Häufigkeit der Dekompensationsereignisse
Tod 10%}
} Aszites 33%Blutung 10%}
}HCC 9%}
PSE 5%
Ikterus 3%
and in a decompensated stage 90 and 97% (P < 0.00001)(Figure 2d).
The cumulative incidence of encephalopathy and ofjaundice are shown in Figure 2e–f, together with mortal-ity after the development of each.
Prognostic stages of cirrhosisThe number of patients entering each of the five prog-nostic stages (at diagnosis or during the follow-up) isreported in Figure 3 together with 20-year incidence ofcompeting events per each stage. Five-year transitioning
intensity and mortality per each prognostic stage isreported in Table 6.
There were 202 patients with compensated cirrhosiswithout oesophageal varices (stage1). After 20 years, 163had disease progression, while 39 were still in this stage.Fourteen patients bled in this stage: 10 bled from variceswhich were not present at previous endoscopy (1 to3 years before); no varices were found in the remainingfour patients in whom portal hypertensive gastropathywas the most likely source of bleeding, althoughthere was no active bleeding at the time of endoscopy.
100
8060
4020
0
0251377
494 344 261 190 1445 41132117
309 186 14160 120 180 240
Decompensated
% surviving
CompensatedN = 377
N = 494
N = 117
Total
P < 0.00001
(a) 100
8060
4020
0
0 60 120 180 240377 274 203 146 109
Decompendationand death 4%
Death 10%
Decompensation 58%
% developing eventcompensated: 377 patientsCumulative event rate 72%
(b) 100
8060
4020
0
0203377 274 146 109
60 120 180 240
% first event occurring in compensatedpatients Cumulative incidence 71%
a death 10%b ascites 33%c bleeding 10%d hcc 9%e pse 5%f jaundice 3%
a
c
b
def
(c)
100
8060
4020
0
0 60 120 180 240243 152 89 74 52
Incidence of varices N = 243
53%
26%Death beforedeveloping varices
(d) 100
8060
4020
0
0132326 195 86 56
60 120 180 240
% surviving after development ofvarices, N = 326
(e)
100
8060
4020
0
0 60 120 180 240211 176 131 96 73136 78 55 39 28
Cumulative Incidenceof decompensation %
Varices N = 136
P < 0.0001
No varices 211
(f)
Cumulative incidence of event %
Figure 1 | Twenty-year survival and cumulative incidence of clinical events. Cumulative incidence is computed bycompeting risks analysis and each curve represents the probability of each specific outcome summed to the outcomeprobability represented in the next curve below. Survival curves are computed by the Kaplan–Meier method. The x-axis represents time in months and the numbers below the x-axis are patients at risk. (a) Survival of the whole seriesand, respectively, of compensated and decompensated patients at diagnosis. (b) Cumulative incidence ofdecompensation. Death and death at the time of first decompensation are shown as competing events. (c)Cumulative incidence of events presenting as a first event in 377 patients with compensated cirrhosis at thediagnosis. Twenty-year proportions of patients presenting each first event are reported in the box. (d) Cumulativeincidence of oesophageal varices. Death is shown as a competing event. Arrows indicate the 20-year incidence of thetwo competing events. (e) Survival of patients after development of varices. (f) Cumulative incidence ofdecompensation in patients with and without varices at diagnosis.
1186 Aliment Pharmacol Ther 2014; 39: 1180-1193ª 2014 John Wiley & Sons Ltd
G. D’Amico et al.
D’Amico G et al, APT, 2014
-
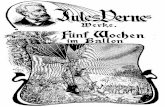
PORTAL HYPERTENSION
Splanchnic vasodilatation
Decrease in systemic vascular resistance
Activation vasoactive systems: RAAS, SNS, ADH
Increase in cardiac output
ASCITES
Schrier, Arroyo, et al. Hepatology (1988) Ripoll et al, GASL (2015)
Alcohol
Hepatitis B/C
Autoimmune
NASH
Hämodynamische Veränderungen bei Zirrhose
Hypoxia, Inflammation Fibrosis
Increase intrahepatic resistance
-
Mechanismen der splanchnischen Vasodilatation
Bernardi et al J Hep 2015
alcoholic steatosis, cholestatic and toxin-induced liver fibrosis[57,63]. Similarly, patients with pre-cirrhotic liver disease showa disrupted gut barrier [69–71]. However, translocation of viablebacteria is a hallmark of cirrhosis, in particular during decompen-sation [21].
In cirrhosis, impaired liver clearance contributes to an accu-mulation of PAMPs, and bacteria in the systemic circulation[47,72,73]. DAMPs originating from damaged liver tissue alsoincrease during acute and chronic liver diseases [23]. Microbialproducts and DAMPs activate receptors of the innate immunesystem contributing to liver disease progression and causing asystemic inflammatory response. Persistent stimulation ofcirculating immune cells increases plasma pro-inflammatorycytokines including IL-6, TNF-a and NO [74,75]. Several of thesemolecules, namely TNF-a, can disrupt intestinal tight junctionsaugmenting gut leakiness. During decompensated cirrhosis, a fur-ther increase in intestinal permeability could contribute toenhanced translocation of PAMPs and viable bacteria [21], possi-bly leading to overt infections. As antibiotic intestinal decontam-ination normalizes the number of activated immune cells andtheir production of pro-inflammatory cytokines in experimentaland human cirrhosis [76,77], the intestinal microbiota likelyrepresents a driving force for systemic inflammation. However,bacteria and bacterial products translocation is not exclusivelydetrimental. The commensal microbiota is protective in experi-mental liver fibrosis. Hepatotoxins cause more liver injury andfibrosis in germ-free than in wild-type mice [78]. Consistently,a mouse model of primary sclerosing cholangitis shows exacer-bated hepatobiliary damage under germ-free conditions [79].These results suggest that the intestinal microbiota has a benefi-cial role in chronic liver disease.
Cirrhosis as a systemic inflammatory multiorgan disease(Fig. 2)
Extrahepatic organ dysfunctions are common in advanced cirrho-sis. Although the underlying mechanisms have been only par-tially elucidated, inflammation and oxidative stress may beinvolved favoring cell death and tissue injury as in sepsis [80].
HRS-AKI, the new definition of type 1 HRS [81] in the settingof acute kidney injury (AKI) [82], is often precipitated by bacterialinfections [83–85], particularly when a severe inflammatoryresponse develops [86]. This suggests a more complex patho-physiology [87] than hypothesized by PAVH, which connectedHRS-AKI to intrarenal arterial vasoconstriction secondary to sev-ere effective hypovolemia. Indeed, both in clinical [88] and exper-imental [89] cirrhosis infection/inflammation leads to renaltubular TLR4 upregulation associated with tubular damage, sug-gesting that TLR4 mediates renal injury. The mechanism underly-ing these abnormalities is undefined, but likely results fromsustained exposure to PAMPs. Indeed, LPS-induced renaldysfunction in experimental cirrhosis is prevented by gutdecontamination with norfloxacin [90]. Thus, BT may upregulatetubular TLR4, increasing kidney susceptibility to inflammatoryinjury. TLR4 stimulation increases the transcription ofpro-inflammatory cytokines by upregulating nuclear factorjB-p65, ultimately leading to apoptotic tubular damage. There-fore, inflammation may represent an important pathogenic factorfor organ failures including AKI.
Systolic cardiac dysfunction, a feature of ‘‘cirrhotic cardiomy-opathy’’ [90], is also involved in the pathogenesis of HRS-AKI [10]
because it cannot sustain sufficient cardiac output to compensatethe extreme vasodilation characterizing this condition. Thepathophysiology of systolic dysfunction in cirrhosis iscomplex [90] and not well understood. Hyperdynamic circulationis involved, but there is growing experimental evidence high-lighting the role of inflammation. Oxidative stress- andTNFa-induced activation of the NF-jB-iNOS pathway and oxida-tive stress-induced alteration of b-receptor signaling accountedfor impaired left ventricular contractility [91]. Interestingly, suchmolecular abnormalities were reversed and contractility restoredby the anti-oxidant and scavenging effect of human albumin [91].However, other potential mechanisms should be investigated toexplain cardiac dysfunction in advanced cirrhosis, particularlyin sepsis. Enhanced expression of the C5a cardiomyocytes recep-tor is involved in experimental septic cardiomyopathy [92], butits role in cirrhosis is unknown.
Systemic inflammation could also be implicated in the patho-genesis of hepatopulmonary syndrome (HPS) caused by intrapul-monary vasodilatation (IPVD) and, less commonly, pleural andpulmonary arteriovenous communications resulting in functionaland anatomic shunts [93–95]. IPVD pathophysiology is likelymultifactorial, but the involvement of BT-induced systemicinflammation is supported by evidence that norfloxacin improvesHPS in rats with cirrhosis [96].
HPS is strongly related to increased NO release inpulmonary circulation [95]. BT-related endotoxemia and thepro-inflammatory response induce macrophage accumulation inlung microvasculature [97], where the activation of fractalkine(CX3CL1) chemokine enhances monocyte adherence [98].Monocytes express iNOS and produce heme oxygenase-1 that
PORTAL HYPERTENSION/LIVER FAILURE
BACTERIAL TRANSLOCATIONPathogen-associated molecular pattern release
ACTIVATION OF INNATE PATTERNRECOGNITION RECEPTORS
Other potential mechanisms? RELEASE OF PRO-INFLAMMATORY
MOLECULES (ROS/RNS)
ADRENAL DYSFUNCTION HE
KIDNEYDYSFUNCTION HPS
SPLANCHNIC ARTERIOLAR VASODILATION & CARDIOVASCULAR DYSFUNCTION
++
Fig. 2. Potential mechanisms leading to the major clinical manifestations ofadvanced cirrhosis. Along with the pathway promoting splanchnic arteriolarvasodilation and cardiovascular dysfunction secondary to portal hypertension,the sustained activation of innate host immunity brought about by abnormal guttranslocation of bacteria and bacterial products (known as pathogen-associatedmolecular patterns) is responsible for persistent activation of innate patternrecognition receptors (e.g., Toll-like receptors) and subsequent inflammation.Pro-inflammatory cytokines and oxidative/nitrosative stress impair effectivehypovolemia by enhancing arterial vasodilation (mainly mediated by NO) andpreventing cardiac output to fulfill the needs of peripheral circulation. Moreover,direct effects on kidney and other organs worsen their dysfunction. HE, hepaticencephalopathy; HPS, hepatopulmonary syndrome; ROS / RNS, reactive oxygen /nitrogen species.
Hypothesis
Hypothesis
1278 Journal of Hepatology 2015 vol. 63 j 1272–1284
-
PORTAL HYPERTENSION
Splanchnic vasodilatation
Decrease in systemic vascular resistance
Activation vasoactive systems: RAAS, SNS, ADH
Increase in cardiac output
ASCITES
Schrier, Arroyo, et al. Hepatology (1988) Ripoll et al, GASL (2015)
Alcohol
Hepatitis B/C
Autoimmune
NASH
Hämodynamische Veränderungen bei Zirrhose
Hypoxia, Inflammation Fibrosis
Increase intrahepatic resistance
-
Wesentliche Komplikationen bei Patienten mit Aszites Therapie-refraktärer
Aszites
fehlendes Therapie-
ansprechen;vor allem auf diuretische Therapie
TIPSParacentese mit
AlbumingabeLeitlinie DGVS, EASL
Kom
plik
atio
n
Defin
ition
Beha
ndlu
ng
Spontan bakterielle Peritonitis
Entzündung des Aszites;
Nachweis von > 250/mm3
polymorpho-nukleären Zellen, d. h. neutrophilen
GranulozytenAntibose und Albumingabe
Hepato-renales
SyndromPotentiell
reversibles Nierenversagen bei
Patienten mit Leberzirrhose oder
Steatohepatitis
Vasopressin-analogagabe
und AlbumingabeTIPS
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
Aufbau von Albumin
Bernardi et al., J Clin Exp. Hepatol. 2014
• etwa 50% des Gesamtproteingehalts
• 585 Aminosäuren, 66 kDalton
• nur in Hepatozyten synthetisiert
• 10-15 g/Tag produziert, falls notwendig 3-4-fache
Zunahme möglich
• Halbwertszeit in der Zirkulation 16 - 18 h
• totale Halbwertszeit 12 - 18 Tage
-
Funktionen von Albumin
70-75% des onkotischen Drucks des PlasmasAntiinflammatorische Eigenschaften
domains are capable of folding into hydrophobic pockets,which can open and close, and accommodate large insol-uble anions as fatty acids. On the molecule surface therealso are cationic groups capable of forming ionic bondswith many ligands.2,3
Liver cells are the only site where albumin is synthesized.They produce about 10–15 g per day, but, if needed, albu-min production can increase upto 3–4 fold. The osmolarityand, subsequently, the oncotic pressure of the interstitialfluid in the hepatic parenchyma play a fundamental rolein the regulation of albumin synthesis. In health, its pro-duction is quite constant, so that only a small intracellulardeposit of the protein is required.
Approximately 30%–40% of the albumin pool is retainedin the blood stream, while the remaining is distributed inthe interstitium, where its concentration is low (1.4 g/dl),as well as inmuscles and skin. The exchange of albumin be-tween the plasma and the interstitium is a highly dynamicprocess: the protein leaves the vascular compartment at arate of 5% per hour, returning to it via the lymphatic sys-tem in an amount equaling the output. The circulatoryhalf-life of albumin, which is approximately 16–18 h, istherefore much lower than its total half-life, which variesfrom 12.7 to 18.2 days in a young healthy adult.
Albumin synthesis is stimulated by hormonal factorssuch as insulin, cortisol and growth hormone while,conversely, mediators of inflammation, such as cytokinesIL-6 and TNF-a, act as inhibitors. Albumin is mainlydegraded by the muscles, liver and kidneys, although itscatabolism is a widespread process involving many tissues,which is influenced by the plasma concentrations of atrialnatriuretic peptide.4,5
FunctionsAlbumin exerts important physiological roles. A mostprominent feature is that albumin is the main modulatorof fluid distribution in the various compartments of thebody. In fact, about 70–75% of the oncotic pressure ofthe plasma is determined by albumin due to its direct os-motic property. Moreover, binding of cations, such assodium, to the negative charges of the protein leads waterto move from interstitium to the intravascular compart-ment (Gibbs–Donnan effect).6
Albumin binds and carries a great variety of hydropho-bic molecules such as metals, fatty acids, metabolites anddrugs, with consequent implications on solubilization,transport and metabolism of many endogenous and exog-enous substances (Figure 1). Indeed, through the bindingwith albumin, many potentially toxic ligands are neutral-ized and definitively catabolized with the degradation ofthe protein.
Furthermore, albumin is the major source of extracel-lular reduced sulfhydryl groups (–SH), which act as potentscavengers of reactive oxygen species (ROS) derived fromoxidative stress, thus constituting the main circulatingantioxidant system in the body. In healthy adults, approx-imately 70–80% of albumin contains a free sulfhydrylgroup in Cys-34 position, the so called human mercaptal-bumin. About 25%, instead, presents the Cys-34 involved ina disulfide bond with plasma sulfhydryl compounds, suchas cysteine, homocysteine or glutathione. This form of al-bumin is called non-mercaptalbumin 1. Finally, only asmall percentage of albumin circulates in the form ofnon-mercaptalbumin 2, where the residue Cys-34 is
Figure 1 Albumin possesses functional domains with important properties, such as the free cysteine residue (SH) in position 34, which exerts potentanti-oxydant and scavenging activities, the aminoterminal (NH2) that binds to and removes highly toxic reactive metal species, and other domains thatbind a variety of endogenous and exogenous substances including endotoxins and various drugs (ROS: reactive oxygen species; LCFA: long-chainfatty acids; NSAIDs: non-steroideal anti-inflammatory drugs).
JOURNAL OF CLINICAL AND EXPERIMENTAL HEPATOLOGY
Journal of Clinical and Experimental Hepatology | December 2014 | Vol. 4 | No. 4 | 302–311 303
Live
rCirrho
sis
Bernardi et al., J Clin Exp. Hepatol. 2014
-
Albuminmodifikationen bei Zirrhose
• reduzierte Serumspiegel
• post-transkriptionale Veränderung
• Erhöhung des Anteils von oxidierten Albumin
• Albumin bei Zirrhose mit veränderter Funktion
• reduzierte Transportfunktion
• reduzierte anti-oxidative Funktion
• reduzierte Detoxifizierung
Bernardi et al., J Clin Exp. Hepatol. 2014
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
Wesentliche Komplikationen bei Patienten mit Aszites Therapie-refraktärer
Aszites
Spontan bakterielle Peritonitis
Hepato-renales
Syndrom
fehlendes Therapie-
ansprechen;vor allem auf diuretische Therapie
TIPSParacentese mit
AlbumingabeLeitlinie DGVS, EASL
Kom
plik
atio
n
Defin
ition
Beha
ndlu
ng
Entzündung des Aszites;
Nachweis von > 250/mm3
polymorpho-nukleären Zellen, d. h. neutrophilen
GranulozytenAntibose und Albumingabe
Potentiell reversibles
Nierenversagen bei Patienten mit
Leberzirrhose oder Steatohepatitis
Vasopressin-analogagabe
und AlbumingabeTIPS
-
LL- Indikation zur Albumingabe bei Patienten mit Zirrhose
Indikation Was sagt die Leitlinie? Dosis
ParacenteseBei Durchführung einer großvolumigen Parazentese (>5l) soll eine intravenöse
Albumingabe (6–8g/Liter Aszites) erfolgen.
-
Entwicklung eines PPCD mit Albumin und Plasmaexpander1008 GINÈS ET AL. GASTROENTEROLOGY Vol. 111, No. 4
natriuretic systems, the faster reaccumulation of ascitesin these patients was probably related to an accentuationof renal sodium retention. This contention is further sup-ported by the increased diuretic requirements in thisgroup of patients. The reason for the impaired prognosisis more difficult to ascertain. Perhaps postparacentesiscirculatory dysfunction developed in patients with moreadvanced disease. However, this possibility is unlikelybecause patients in whom circulatory dysfunction devel-oped after paracentesis did not differ from those in whomthe disturbance did not develop in the degree of impair-ment of liver and renal function or severity of alterationsin systemic hemodynamics. A more plausible explanationfor the impaired prognosis of patients developing post-paracentesis circulatory dysfunction is that changes in
Figure 4. Incidence of postparacentesis circulatory dysfunction ac- neurohumoral systems caused an acceleration of thecording to the plasma expander used (albumin, h; dextran 70 or course of the disease. Theoretical basis supports this pos-polygeline, ) and the volume of ascitic fluid drained. *P Å 0.04 and
sibility. First, it is well known that spontaneous impair-**P Å 0.02 with respect to the incidence in patients receiving albu-min. Figures represent patients developing postparacentesis circula- ment in systemic and renal circulatory function in cir-tory dysfunction and patients at risk, respectively. rhotic patients with ascites is associated with a poor
prognosis.29,30 Second, angiotensin II and other vasoactivesubstances released during postparacentesis circulatorydure.10,12,15,23,25 The recommendation of the use of albu-dysfunction, such as norepinephrine, are powerful renalmin as plasma expander after paracentesis is based onvasoconstrictors. On the other hand, plasma levels offindings showing that albumin maintains the initial im-atrial natriuretic peptide, a vasodilator hormone that par-provement in circulatory function after paracentesis andticipates in the maintenance of renal perfusion in cirrho-prevents the subsequent activation of vasoconstrictor sys-sis,31 decrease in patients developing circulatory dysfunc-tems and impairment in renal function.10,15 The mecha-tion after paracentesis.12,14,15 This imbalance betweennism of the circulatory dysfunction after paracentesis re-renal vasoactive systems may accelerate the impairmentmains incompletely understood. Plasma volume andof renal circulatory function and favor the developmenthematocrit do not change in patients developing circula-of renal dysfunction.32 Finally, angiotensin II and norepi-tory dysfunction after paracentesis, indicating that therenephrine increase intrahepatic vascular resistance and re-is no reduction in total intravascular volume.27 The exis-duce hepatic blood flow.33 The neurohormonal changestence of marked activation of vasoconstrictor systemsassociated with postparacentesis circulatory dysfunctionwithout changes in plasma volume therefore suggests amay therefore aggravate portal hypertension and impairreduction in effective intravascular volume after paracen-hepatic function. Nevertheless, because it is possible thattesis. The observation that these neurohumoral changesthe impaired prognosis in patients with postparacentesisare associated with a decrease in systemic vascular resis-circulatory dysfunction is related to some unrecognizedtance suggests that the circulatory dysfunction is causedfactor(s), further studies are clearly needed to investigateby an accentuation of the arterial vasodilatation of cir-this feature. Whatever the reason for the relationshiprhotic patients.28between postparacentesis circulatory dysfunction and im-The present study was designed to investigate whetherpaired survival, this observation is a very strong argu-circulatory dysfunction after paracentesis has any impactment for the use of measures to prevent this phenomenon.on the clinical course of the disease and assess the effec-
The development of circulatory dysfunction after para-tiveness of plasma expanders different from albumin incentesis was clinically silent. Neither changes in arterialthe prevention of this abnormality.pressure or laboratory parameters nor the developmentA major finding was that postparacentesis circulatoryof complications during hospitalization were useful todysfunction is not spontaneously reversible but persistsdiagnose the development of circulatory dysfunction (Ta-during follow-up. More importantly, this disorder is as-bles 4 and 5). Measurement of PRA 2 days after treat-sociated with faster reaccumulation of ascites and im-ment, although very specific, had a low sensitivity.paired prognosis. Because circulatory disturbance after
paracentesis is characterized by marked activation of anti- Another important observation of this study was that
/ 5e12$$0020 09-05-96 13:08:33 gasas WBS-Gastro
Gines 1996
-
LL- Indikation zur Albumingabe bei Patienten mit Zirrhose
Indikation Was sagt die Leitlinie? Dosis
ParacenteseBei Durchführung einer großvolumigen Parazentese (>5l) soll eine intravenöse
Albumingabe (6–8g/Liter Aszites) erfolgen. 8 g/l
Spontan-bakterielle Peritonitis
Begleitend zur antibiotischen Therapie soll die Gabe von Albumin intravenös am Tag der Diagnosestellung und am dritten Tag nach
Diagnosestellung durchgeführt werden.
-
Albumingabe bei spontan-bakterieller Peritonitis
INTRAVENOUS ALBUMIN IN PATIENTS WITH CIRRHOSIS AND SPONTANEOUS BACTERIAL PERITONITIS
Volume 341 Number 6
·
405
ime and albumin (6 of 63 [10 percent]) than amongthose treated with cefotaxime alone (21 of 63 [33percent], P=0.002) (Table 2). On days 3, 6, and 9,the blood urea nitrogen and serum creatinine levelswere lower and the serum sodium level was higherin the cefotaxime-plus-albumin group than in thecefotaxime group (Table 3). Renal impairment de-veloped in 27 patients, and in 23 of these patients,the worsening of renal function followed a progres-sive course characterized by oliguria or anuria, markedincreases in blood urea nitrogen and serum creati-nine levels (the peak values were 94±8 mg per dec-iliter [34±3 mmol per liter] and 3.4±1 mg per dec-iliter [301±88 µmol per liter], respectively), andsevere hyponatremia (124±1 mmol of sodium perliter). For the series of patients as a whole, inde-pendent predictors of the development of renal im-pairment included base-line serum bilirubin and cre-atinine levels (P
-
Albumingabe bei spontan-bakterieller Peritonitis
Salerno 2013
Treatment assignment was determined by computer-gener-ated sequence of random numbers in 3 trials11,18,19 and coin tossin 1 trial.17 In 3 trials, concealment of allocation to randomizedgroups was accomplished by using sealed envelopes.11,18,19 Allo-cation concealment method was unspecified for the fourthtrial.17 Thus, method of randomization was adequate for all 4included trials and of allocation concealment for 3 trials. Onthe other hand, only 1 of the 4 trials was blinded.11
In all trials, the patients of both groups received antibiotic(Table 1). Albumin was infused as a 20% solution in all trials.The treatment period with albumin was 3 days in 3 trials and 3weeks in the remaining trial. An albumin dose range of 0.5–1.5g/kg!1 was administered in 3 trials, whereas in the remainingtrial, 3 daily fixed dosages of 10 g (0.14 g/kg!1 for a 70-kgpatient) were given on the basis of National Health Insurancecoverage. Control treatment in 1 trial consisted of hydroxyethylstarch (HES) at the same dose as that of albumin. In the other3 trials, albumin was compared with no albumin. Length offollow-up was 90 days in 1 trial and unspecified in the others.
Renal ImpairmentIn 3 trials, renal impairment was defined according to
the presence or absence of renal insufficiency at baseline. Forpatients without preexisting renal insufficiency, renal impair-ment was defined as an increase from baseline in serum creat-
inine to "1.5 mg/dL!1 or, alternatively in 2 of the 3 trials, inblood urea nitrogen (BUN) to "30 mg/dL!1. In addition, in 2of the 3 trials the relative magnitude of serum creatinine orBUN increase must have been "50%. Only the "50% relativeincrease criterion was applied in cases of preexisting renal in-sufficiency. In the fourth trial, renal impairment was defined asa serum creatinine level "1.5 mg/dL!1 or BUN "25 mg/dL!1.
Across all 4 trials, 12 of 144 albumin recipients (8.3%) de-veloped renal impairment, compared with 44 of 144 controlgroup patients (30.6%). The odds ratios for renal impairment inthe 4 trials were highly consistent, ranging narrowly from 0.19 –0.30 (Figure 2). The pooled odds ratio was 0.21. There was noevidence of significant heterogeneity (P # .99; I2, 0%) or publi-cation bias (P # .11) with respect to the renal impairment endpoint.
The trials by Sort et al11 and Xue et al17 accounted for thepreponderance of meta-analytic weight. The pooled odds ratiofor renal impairment was 0.21 with 95% confidence interval (CI)of 0.08 – 0.54 after excluding the trial by Sort et al and 0.23 (CI,0.09 – 0.54) after excluding the trial by Xue et al. These resultsare the same as or closely similar to the pooled odds ratioshown in Figure 2 with no exclusion (0.21; CI, 0.11– 0.42).
For one included trial,11 outcomes were reported with strat-ification according to significant baseline predictors. Neverthe-less, in the report of that trial no formal analysis was presented
Table 1. Included Trials
Trial N Agea (SD), y Male, % Ethnicity Etiology Treatment regimen
Sort et al,11 1999 126 61.0 (7.9) 64.3 Caucasian 29.4% alcohol, 70.6%other
Cefotaxime intravenously dosed according tocreatinine without vs with 1.5g/kg!1 20%albumin within first 6 h plus 1.0 g/kg!1
on day 3Xue et al,17 2002 112 22–70b — Chinese — Ceftriaxone intravenously dosed according to
creatinine without vs with 0.5–1.0 g/kg!1
20% albumin within first 6 h and everythird day for 21 days
Fernández et al,18
200520 61.0 (9.5) 55.0 Caucasian 60.0% HCV, 40.0% other Ceftriaxone intravenously 2 g at diagnosis
and then 1 g/d plus 1.5 g/kg!1 atbaseline and 1.0g/kg!1 on day 3 of 20%albumin vs 6% HES 200/0.5
Chen et al,19
200930 56.5 (11.5) 60.0 Chinese 60.0% HBV, 23.3% HCV,
16.7% alcoholCephalosporins without vs with 50 mL 20%
albumin (0.14 g/kg!1 for a 70-kg patient)on days 1–3
HBV, hepatitis B virus; HCV, hepatitis C virus; SD, standard deviation.aMean, except as otherwise indicated.bAge range eligible for this trial; mean age not reported.
Figure 2. Renal impairment.CI is shown by error bars. Datapoints for individual trials sca-led according to meta-analyticweight.
February 2013 ALBUMIN IN SPONTANEOUS BACTERIAL PERITONITIS 125
on the comparative effectiveness of albumin in the subgroupsdefined by the baseline predictors. Such a subgroup analysis isshown in Table 2. The control group incidence of renal impair-ment was 14 of 29 (48%) when baseline serum bilirubin equaledor exceeded 4 mg/dL!1, as contrasted with 7 of 34 (21%) whenserum bilirubin was below 4 mg/dL!1 at baseline. The oddsratio for the prevention of renal impairment as the result ofalbumin treatment was 0.15 in patients with baseline serumbilirubin !4 mg/dL!1, compared with 0.32 in those with lowerbaseline serum bilirubin; however, this subgroup difference inthe effectiveness of albumin for averting renal impairment wasnot statistically significant (P " .47). With regard to renalimpairment, furthermore, the effectiveness of albumin was sim-ilar in the subgroup defined by either serum bilirubin !4
mg/dL!1 or serum creatinine !1 mg/dL!1 at baseline vs thesubgroup with lower values of those 2 parameters (Table 2).
MortalityTotal mortality was 23 of 144 patients allocated to
albumin treatment (16.0%) and 51 of 144 to the control regi-men (35.4%). Odds ratios for mortality in individual RCTs weresimilar, ranging from 0.16 – 0.55 (Figure 3). The pooled oddsratio was 0.34. There was no significant heterogeneity (P " .72;I2, 0%) or publication bias (P " .69) with respect to mortality.The pooled odds ratio for mortality with exclusion of either thetrial by Sort et al11 (0.28; CI, 0.12– 0.65) or by Xue et al17 (0.41;CI, 0.21– 0.80) was comparable to that with no exclusion shownin Figure 3 (0.34; CI, 0.19 – 0.60).
Table 2. Comparative Effectiveness of Albumin in Subgroupsa
Subgroup
Outcome
Odds ratio (CI) P valueb
Albumin Control
Event Total Event Total
Renal impairmentBilirubin !4 mg/dL!1 3 24 14 29 0.15 (0.04–0.63)Bilirubin #4 mg/dL!1 3 39 7 34 0.32 (0.08–1.36)Ratio of odds ratios (CI) 0.48 (0.06–3.58) .47Bilirubin !4 mg/dL!1 or creatinine !1 mg/dL!1 6 46 20 48 0.21 (0.07–0.59)Bilirubin #4 mg/dL!1 and creatinine #1 mg/dL!1 0 17 1 15 0.27 (0.01–7.28)Ratio of odds ratios (CI) 0.76 (0.02–23.8) .88
Hospital mortalityBilirubin !4 mg/dL!1 3 24 13 29 0.18 (0.04–0.72)Bilirubin #4 mg/dL!1 3 39 5 34 0.48 (0.11–2.19)Ratio of odds ratios (CI) 0.36 (0.05–2.88) .34BUN !30 mg/dL!1 6 23 13 28 0.41 (0.12–1.34)BUN #30 mg/dL!1 0 40 5 35 0.07 (0.00–1.28)Ratio of odds ratios (CI) 5.97 (0.25–142) .27Bilirubin !4 mg/dL!1 or BUN !30 mg/dL!1 6 39 18 43 0.25 (0.09–0.73)Bilirubin #4 mg/dL!1 and BUN #30 mg/dL!1 0 24 0 20 —c
Bilirubin !4 mg/dL!1 and BUN !30 mg/dL!1 3 8 8 14 0.45 (0.08–2.67)Bilirubin #4 mg/dL!1 or BUN #30 mg/dL!1 3 55 10 49 0.23 (0.06–0.87)Ratio of odds ratios (CI) 2.00 (0.21–18.7) .54
aData from included trial of Sort et al.11 Subgroups defined in terms of baseline levels for serum bilirubin, serum creatinine, or BUN. Inmultivariate analyses reported by Sort et al, independent predictors of renal impairment were baseline levels of serum bilirubin (P # .001) andserum creatinine (P " .01) and antibiotic treatment without albumin (P " .02). Independent predictors of hospital mortality included baselinelevels of serum bilirubin (P " .01) and BUN (P " .001) and antibiotic treatment without albumin (P " .05).bDifference in effectiveness of albumin between the subgroups by test of interaction.cOdds ratio inestimable for 0 events in both groups.
Figure 3. Mortality. CI is shownby error bars. Data points for in-dividual trials scaled accordingto meta-analytic weight.
126 SALERNO ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 2
-
LL- Indikation zur Albumingabe bei Patienten mit Zirrhose
Indikation Was sagt die Leitlinie? Dosis
ParacenteseBei Durchführung einer großvolumigen Parazentese (>5l) soll eine intravenöse
Albumingabe (6–8g/Liter Aszites) erfolgen. 8 g/l
Spontan-bakterielle Peritonitis
Begleitend zur antibiotischen Therapie soll die Gabe von Albumin intravenös am Tag der Diagnosestellung und am dritten Tag nach
Diagnosestellung durchgeführt werden.
1,5 g/kg KG am 1. Tag
1 g/kg KG am 3. Tag
Hepatorenales Syndrom
Die intravenöse Albumingabe zum Ausschluss eines Volumenmangels bzw. zur Sicherung der Diagnose
eines hepatorenalen Syndroms sollte erfolgen. Die Kombinationsbehandlung aus Albumininfusion und Vasokonstriktortherapie ist Therapie der ersten
Wahl bei hepatorenalem Syndrom Typ I.
-
decrease in SCr level by at least 30% by day 4 (13 terlip-ressin vs 23 placebo patients, P ! .037). Approximatelyone third of the subjects received less than 3 days oftherapy because of lack of response/dialysis, choice ofpalliative care, death, transplantation, early terminationbecause of adverse events, or other reasons, includingwithdrawal of consent and administrative reasons. Twopatients (1 terlipressin-treated patient and 1 placebo-treated patient) experienced a relapse of HRS type 1 afteran initial response and were retreated with the originallyassigned blinded study drug as defined in the protocol.
Changes in Renal FunctionAs shown in Table 2, the incidence of treatment
success at day 14 in the terlipressin group was doublethat of placebo, but this difference only trended towardstatistical significance (14/56, 25% vs 7/56, 12.5%, respec-tively, P ! .093). The results were similar when includinga surviving patient who was missing a day 14 SCr value(15/56, 26.8%, for terlipressin and 7/56, 12.5%, for pla-cebo, P ! .059). However, the results for HRS reversal,defined by a decrease in SCr level to !1.5 mg/dL, weresignificantly different between treatment groups (19/56,
33.9% for terlipressin and 7/56, 12.5% for placebo, P !.008) (Table 2). Figure 1 presents the cumulative inci-dence of HRS reversal. In the placebo/albumin arm, thebenefit of therapy was seen only within the first 96 hours.In contrast, in the terlipressin group, the incidence ofHRS reversal continued to increase throughout the 14days of therapy.
Published literature indicates that at least 3 days oftreatment with terlipressin is needed to improve renalfunction.14,16,27 Similarly in this trial, treatment success
Table 1. Summary of Key Demographic and Baseline Characteristics
Demographic measures Terlipressin n ! 56 Placebo n ! 56
Age, mean, y (SD) 50.6 (10.5) 52.9 (11.4)Sex, n (%) 41 (73.2) Male 39 (69.6) MaleEthnic origin, n (%) 51 (91.1) White 49 (87.5) WhiteChild–Pugh score, mean (SD) 11.7 (1.9) 11.2 (1.8)MELD score, mean (SD) 33.4 (6.0) 33.4 (6.3)Serum creatinine, mean, mg/dL (SD) 3.96 (2.19) 3.85 (1.17)Serum sodium, mean, mmol/L (SD) 130.6 (6.9) 132.4 (7.0)Albumin, mean, g/dL (SD) 2.6 (0.84) 2.9 (0.79)Bilirubin, mean, mg/dL (SD) 15.0 (13.6) 15.8 (15.1)INR, mean (SD) 2.3 (0.8) 2.3 (1.1)AST, mean, U/L (SD) 104.8 (111.9) 117.3 (143.2)ALT, mean, U/L (SD) 57.6 (76.4) 63.1 (91.3)Alcoholic hepatitis, n (%) 20 (35.7) 20 (35.7)Factors associated with HRS development, n (%) 30 (53.6) 31 (55.4)
Infection 14 (25.0) 9 (16.1)Gastrointestinal bleeding 2 (3.6) 3 (5.4)Prior diuretic treatment 12 (21.4) 15 (26.8)Large volume paracentesis 5 (8.9) 4 (7.1)
Cirrhosis, n (%) 51 (91.1) 51 (91.1)Etiology of liver disease, n (%)a
Alcohol 29 (51.8) 29 (51.8)Hepatitis C 22 (39.3) 19 (33.9)Hepatitis B 4 (7.1) 1 (1.8)Primary biliary cirrhosis 2 (3.6) 1 (1.8)Hepatocellular carcinoma 4 (7.1) 6 (10.7)Nonalcoholic steatohepatitis 2 (3.6) 5 (8.9)
History of esophageal variceal hemorrhage, n (%) 27 (48.2) 27 (48.2)Ascites, n (%) 54 (96.4) 54 (96.4)Diabetics, n (%) 13 (23.2) 13 (23.2)Mean arterial pressure, mean, mm Hg (SD) 75.5 (11.4) 77.2 (13.6)Prior octreotide, n (%) 10 (17.9) 11 (19.6)Prior midodrine, n (%) 11 (19.6) 12 (21.4)
INR, International normalized ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase.aIncludes patients with more than 1 etiology of liver disease.
Table 2. Treatment Outcomes
End pointTerlipressin
n (%) Placebo n (%) P value
All patients (n ! 56) (n ! 56)Treatment success at
day 1414 (25.0) 7 (12.5) .093
HRS reversal 19 (33.9) 7 (12.5) .008Patients who received "3
days of treatment(n ! 36) (n ! 39)
Treatment success atday 14
14 (38.9) 7 (17.9) .046
HRS reversal 19 (52.8) 7 (17.9) .002
CLIN
ICA
L–LI
VER
,PA
NCR
EAS,
AN
DBI
LIA
RYTR
ACT
May 2008 TERLIPRESSIN FOR TYPE 1 HEPATORENAL SYNDROME 1363
Albumininfusion zur Behandlung des
Hepatorenalen Syndroms
Sanyal 2008 Martin Lliahi 2008
-
decrease in SCr level by at least 30% by day 4 (13 terlip-ressin vs 23 placebo patients, P ! .037). Approximatelyone third of the subjects received less than 3 days oftherapy because of lack of response/dialysis, choice ofpalliative care, death, transplantation, early terminationbecause of adverse events, or other reasons, includingwithdrawal of consent and administrative reasons. Twopatients (1 terlipressin-treated patient and 1 placebo-treated patient) experienced a relapse of HRS type 1 afteran initial response and were retreated with the originallyassigned blinded study drug as defined in the protocol.
Changes in Renal FunctionAs shown in Table 2, the incidence of treatment
success at day 14 in the terlipressin group was doublethat of placebo, but this difference only trended towardstatistical significance (14/56, 25% vs 7/56, 12.5%, respec-tively, P ! .093). The results were similar when includinga surviving patient who was missing a day 14 SCr value(15/56, 26.8%, for terlipressin and 7/56, 12.5%, for pla-cebo, P ! .059). However, the results for HRS reversal,defined by a decrease in SCr level to !1.5 mg/dL, weresignificantly different between treatment groups (19/56,
33.9% for terlipressin and 7/56, 12.5% for placebo, P !.008) (Table 2). Figure 1 presents the cumulative inci-dence of HRS reversal. In the placebo/albumin arm, thebenefit of therapy was seen only within the first 96 hours.In contrast, in the terlipressin group, the incidence ofHRS reversal continued to increase throughout the 14days of therapy.
Published literature indicates that at least 3 days oftreatment with terlipressin is needed to improve renalfunction.14,16,27 Similarly in this trial, treatment success
Table 1. Summary of Key Demographic and Baseline Characteristics
Demographic measures Terlipressin n ! 56 Placebo n ! 56
Age, mean, y (SD) 50.6 (10.5) 52.9 (11.4)Sex, n (%) 41 (73.2) Male 39 (69.6) MaleEthnic origin, n (%) 51 (91.1) White 49 (87.5) WhiteChild–Pugh score, mean (SD) 11.7 (1.9) 11.2 (1.8)MELD score, mean (SD) 33.4 (6.0) 33.4 (6.3)Serum creatinine, mean, mg/dL (SD) 3.96 (2.19) 3.85 (1.17)Serum sodium, mean, mmol/L (SD) 130.6 (6.9) 132.4 (7.0)Albumin, mean, g/dL (SD) 2.6 (0.84) 2.9 (0.79)Bilirubin, mean, mg/dL (SD) 15.0 (13.6) 15.8 (15.1)INR, mean (SD) 2.3 (0.8) 2.3 (1.1)AST, mean, U/L (SD) 104.8 (111.9) 117.3 (143.2)ALT, mean, U/L (SD) 57.6 (76.4) 63.1 (91.3)Alcoholic hepatitis, n (%) 20 (35.7) 20 (35.7)Factors associated with HRS development, n (%) 30 (53.6) 31 (55.4)
Infection 14 (25.0) 9 (16.1)Gastrointestinal bleeding 2 (3.6) 3 (5.4)Prior diuretic treatment 12 (21.4) 15 (26.8)Large volume paracentesis 5 (8.9) 4 (7.1)
Cirrhosis, n (%) 51 (91.1) 51 (91.1)Etiology of liver disease, n (%)a
Alcohol 29 (51.8) 29 (51.8)Hepatitis C 22 (39.3) 19 (33.9)Hepatitis B 4 (7.1) 1 (1.8)Primary biliary cirrhosis 2 (3.6) 1 (1.8)Hepatocellular carcinoma 4 (7.1) 6 (10.7)Nonalcoholic steatohepatitis 2 (3.6) 5 (8.9)
History of esophageal variceal hemorrhage, n (%) 27 (48.2) 27 (48.2)Ascites, n (%) 54 (96.4) 54 (96.4)Diabetics, n (%) 13 (23.2) 13 (23.2)Mean arterial pressure, mean, mm Hg (SD) 75.5 (11.4) 77.2 (13.6)Prior octreotide, n (%) 10 (17.9) 11 (19.6)Prior midodrine, n (%) 11 (19.6) 12 (21.4)
INR, International normalized ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase.aIncludes patients with more than 1 etiology of liver disease.
Table 2. Treatment Outcomes
End pointTerlipressin
n (%) Placebo n (%) P value
All patients (n ! 56) (n ! 56)Treatment success at
day 1414 (25.0) 7 (12.5) .093
HRS reversal 19 (33.9) 7 (12.5) .008Patients who received "3
days of treatment(n ! 36) (n ! 39)
Treatment success atday 14
14 (38.9) 7 (17.9) .046
HRS reversal 19 (52.8) 7 (17.9) .002
CLIN
ICA
L–LI
VER
,PA
NCR
EAS,
AN
DBI
LIA
RYTR
ACT
May 2008 TERLIPRESSIN FOR TYPE 1 HEPATORENAL SYNDROME 1363
Figure 2 shows the probability of achieving improvementof renal function in patients from both groups. Out ofthe 10 patients who responded with terlipressin andalbumin, 7 had response with a dose of terlipressin of 1mg/4 hour and 3 patients with 2 mg/4 hour. In patientswho responded to treatment with terlipressin and albu-min, serum creatinine decreased from 256 ! 71 to 115 !18 !mol/L (P " .005) and mean arterial pressure in-creased from 75 ! 13 to 84 ! 18 mm Hg (P " .02). Nosignificant changes were observed in these parameters inpatients who did not respond to treatment with terlip-ressin and albumin (362 ! 195 vs 433 ! 248 !mol/L and68 ! 10 vs 69 ! 12 mm Hg, respectively; P " ns forboth). In the 2 patients who showed an improvement ofrenal function in the albumin group, serum creatininedecreased from 409 to 150 and 230 to 106 !mol/L,respectively. No significant changes in renal function orsystemic hemodynamic parameters were observed in pa-tients treated with albumin who did not respond totherapy. To assess whether the number of patients in-cluded by center could have had an influence on responseto therapy, the rate of response in centers that included5 or more patients (3 centers) was compared with that ofcenters that included less than 5 patients (6 centers). Rateof response to terlipressin and albumin was 43% (6 out of14 patients) and 44% (4 out of 9 patients) in both groupsof centers, respectively (P " 1.0). Corresponding values inthe albumin group were 8% (1 out of 13 patients) and10% (1 out of 10 patients), respectively (P " 1.0).
In the whole series of patients, predictive factors ofresponse to therapy were etiology of cirrhosis, baselineserum bilirubin, leukocyte count, serum creatinine andurine volume, and treatment assignment. In multivariate
analysis, the independent predictive factors of responseto therapy were baseline urine volume, serum creatinineand leukocyte count, and treatment assignment (Table2). Of the 10 patients who responded to terlipressin plusalbumin, only 1 patient (10%) had recurrence of renalfailure 18 days after terlipressin withdrawal. Eleven of the23 patients assigned to albumin received terlipressin aftertreatment with albumin, and 1 of them had improve-ment of renal function.
SurvivalThere were no significant differences between the
2 groups with respect to the number of patients whowere alive at 3 months, 6 in the terlipressin and albumingroup (27%) and 4 in the albumin group (19%) (P " .7).Causes of death were similar in the 2 groups. In patientsincluded in the terlipressin and albumin group, causes ofdeath were multiorgan failure (n " 11), liver failure (n "2), acute respiratory distress syndrome (n " 1), hepato-renal syndrome (n " 1), and unknown (n " 2). Inpatients in the albumin group, causes of death weremultiorgan failure (n " 7), liver failure (n " 6), sepsis (n" 2), hepatorenal syndrome (n " 1), and unknown (n "1). A univariate analysis of survival showed that baselineserum bilirubin, prothrombin time, serum creatinine,serum sodium, heart rate, leukocyte count, Child–Pughscore, and model for end-stage liver disease (MELD) scoreand response to therapy were associated with prognosis.In multivariate analysis, independent predictive factors of3-month survival were only baseline MELD score andresponse to therapy (Figure 3).
Adverse EventsTable 3 shows the adverse events observed in both
groups during randomized treatment. There was a simi-lar incidence of hepatic encephalopathy, bacterial infec-tions, and gastrointestinal bleeding in both groups. Onepatient in the terlipressin and albumin group developeda myocardial infarction, abdominal signs compatiblewith intestinal ischemia, and circulatory overload. Twopatients developed abdominal signs suggestive of intes-tinal ischemia, in 1 of them associated with circulatoryoverload. Two other patients developed transient ar-rhythmia: 1 patient bradycardia and another patient ven-
Figure 2. Inverse Kaplan–Meier curves estimating the cumulative inci-dence of improvement of renal function. The median time to improve-ment of renal function in patients treated with terlipressin and albuminwas 11 days (95% CI: 6.1–15.9). Improvement of renal function wasdefined either as reduction in serum creatinine below 133 !mol/L at theend of treatment (complete response) or reduction in serum creatinineof greater than 50% of the pretreatment value but with an end-of-treatment value equal to or greater than 133 !mol/L (partial response).
Table 2. Independent Predictive Factors of Response toTreatment
VariableResponders
(n " 12)Nonresponders
(n " 34)P
value
Assigned to terlipressin #albumin therapy (n)
10 (83%) 13 (38%) .005
Serum creatinine (!mol/L) 256.4 ! 70.7 369.4 ! 194.5 .000Urine volume (mL/day) 880 ! 440 496 ! 419 .005White cell (per mm3) 6649 ! 3556 10932 ! 8107 .001
NOTE. Plus-minus values are means ! SD.P values result from the multivariate analysis.
CLIN
ICA
L–LI
VER
,PA
NCR
EAS,
AN
DBI
LIA
RYTR
ACT
May 2008 TERLIPRESSIN IN HEPATORENAL SYNDROME 1355Albumininfusion zur Behandlung des
Hepatorenalen Syndroms
Sanyal 2008 Martin Lliahi 2008
-
Table 2. Treatment Outcomes
End pointTerlipressin
n (%) Placebo n (%) P value
All patients (n ! 56) (n ! 56)Treatment success at
day 1414 (25.0) 7 (12.5) .093
HRS reversal 19 (33.9) 7 (12.5) .008Patients who received "3
days of treatment(n ! 36) (n ! 39)
Treatment success atday 14
14 (38.9) 7 (17.9) .046
HRS reversal 19 (52.8) 7 (17.9) .002
Figure 2 shows the probability of achieving improvementof renal function in patients from both groups. Out ofthe 10 patients who responded with terlipressin andalbumin, 7 had response with a dose of terlipressin of 1mg/4 hour and 3 patients with 2 mg/4 hour. In patientswho responded to treatment with terlipressin and albu-min, serum creatinine decreased from 256 ! 71 to 115 !18 !mol/L (P " .005) and mean arterial pressure in-creased from 75 ! 13 to 84 ! 18 mm Hg (P " .02). Nosignificant changes were observed in these parameters inpatients who did not respond to treatment with terlip-ressin and albumin (362 ! 195 vs 433 ! 248 !mol/L and68 ! 10 vs 69 ! 12 mm Hg, respectively; P " ns forboth). In the 2 patients who showed an improvement ofrenal function in the albumin group, serum creatininedecreased from 409 to 150 and 230 to 106 !mol/L,respectively. No significant changes in renal function orsystemic hemodynamic parameters were observed in pa-tients treated with albumin who did not respond totherapy. To assess whether the number of patients in-cluded by center could have had an influence on responseto therapy, the rate of response in centers that included5 or more patients (3 centers) was compared with that ofcenters that included less than 5 patients (6 centers). Rateof response to terlipressin and albumin was 43% (6 out of14 patients) and 44% (4 out of 9 patients) in both groupsof centers, respectively (P " 1.0). Corresponding values inthe albumin group were 8% (1 out of 13 patients) and10% (1 out of 10 patients), respectively (P " 1.0).
In the whole series of patients, predictive factors ofresponse to therapy were etiology of cirrhosis, baselineserum bilirubin, leukocyte count, serum creatinine andurine volume, and treatment assignment. In multivariate
analysis, the independent predictive factors of responseto therapy were baseline urine volume, serum creatinineand leukocyte count, and treatment assignment (Table2). Of the 10 patients who responded to terlipressin plusalbumin, only 1 patient (10%) had recurrence of renalfailure 18 days after terlipressin withdrawal. Eleven of the23 patients assigned to albumin received terlipressin aftertreatment with albumin, and 1 of them had improve-ment of renal function.
SurvivalThere were no significant differences between the
2 groups with respect to the number of patients whowere alive at 3 months, 6 in the terlipressin and albumingroup (27%) and 4 in the albumin group (19%) (P " .7).Causes of death were similar in the 2 groups. In patientsincluded in the terlipressin and albumin group, causes ofdeath were multiorgan failure (n " 11), liver failure (n "2), acute respiratory distress syndrome (n " 1), hepato-renal syndrome (n " 1), and unknown (n " 2). Inpatients in the albumin group, causes of death weremultiorgan failure (n " 7), liver failure (n " 6), sepsis (n" 2), hepatorenal syndrome (n " 1), and unknown (n "1). A univariate analysis of survival showed that baselineserum bilirubin, prothrombin time, serum creatinine,serum sodium, heart rate, leukocyte count, Child–Pughscore, and model for end-stage liver disease (MELD) scoreand response to therapy were associated with prognosis.In multivariate analysis, independent predictive factors of3-month survival were only baseline MELD score andresponse to therapy (Figure 3).
Adverse EventsTable 3 shows the adverse events observed in both
groups during randomized treatment. There was a simi-lar incidence of hepatic encephalopathy, bacterial infec-tions, and gastrointestinal bleeding in both groups. Onepatient in the terlipressin and albumin group developeda myocardial infarction, abdominal signs compatiblewith intestinal ischemia, and circulatory overload. Twopatients developed abdominal signs suggestive of intes-tinal ischemia, in 1 of them associated with circulatoryoverload. Two other patients developed transient ar-rhythmia: 1 patient bradycardia and another patient ven-
Figure 2. Inverse Kaplan–Meier curves estimating the cumulative inci-dence of improvement of renal function. The median time to improve-ment of renal function in patients treated with terlipressin and albuminwas 11 days (95% CI: 6.1–15.9). Improvement of renal function wasdefined either as reduction in serum creatinine below 133 !mol/L at theend of treatment (complete response) or reduction in serum creatinineof greater than 50% of the pretreatment value but with an end-of-treatment value equal to or greater than 133 !mol/L (partial response).
Table 2. Independent Predictive Factors of Response toTreatment
VariableResponders
(n " 12)Nonresponders
(n " 34)P
value
Assigned to terlipressin #albumin therapy (n)
10 (83%) 13 (38%) .005
Serum creatinine (!mol/L) 256.4 ! 70.7 369.4 ! 194.5 .000Urine volume (mL/day) 880 ! 440 496 ! 419 .005White cell (per mm3) 6649 ! 3556 10932 ! 8107 .001
NOTE. Plus-minus values are means ! SD.P values result from the multivariate analysis.
CLIN
ICA
L–LI
VER
,PA
NCR
EAS,
AN
DBI
LIA
RYTR
ACT
May 2008 TERLIPRESSIN IN HEPATORENAL SYNDROME 1355
Sanyal 2008 Martin Lliahi 2008
Albumininfusion in Kombination mit Terlipressin zur Behandlung des
Hepatorenalen Syndroms
-
Albumininfusion in Kombination mit Terlipressin zur Behandlung des
Hepatorenalen Syndroms
and arterial hypertension (14% versus 0%; RR, 9.00; 95%CI, 2.14-37.85; I2, 0%). Twenty-one percent of patients inthe treatment group and 2% of patients in the control groupexperienced abdominal pain and diarrhea (RR, 6.82; 95%CI, 0.79-59.15; I2, 0%). There were no differences betweentreatment and control groups regarding any of the remainingadverse events: hepatic encephalopathy (70%), bacterial in-fections (46%), circulatory overload (24%), gastrointestinalbleeding (9%), respiratory distress or acidosis (3%), chestpain (5%), and livedo reticularis (1%).
Subgroup AnalysesType of Vasoconstrictor Drug. We repeated the pri-
mary meta-analysis on mortality with trials stratified by
the treatments assessed (Table 3). Subgroup analysesfound a beneficial effect of terlipressin alone or with albu-min (RR, 0.80; 95% CI, 0.66-0.97). As previously de-scribed, one of the included trials on terlipressin,administered albumin to 88% of patients in the treatmentand control group.19 There was a beneficial effect of ter-lipressin plus albumin irrespective of whether this trialwas included (RR, 0.81; 95% CI, 0.68-0.97) or excludedfrom the analysis (RR, 0.75; 95% CI, 0.61-0.93). Theremaining subgroup analyses included few patients andno differences were found for any of the remaining treat-ment comparisons (Table 3).
Type of Hepatorenal Syndrome. Three trials onlyincluded patients with type 1 HRS.16,18,19 A meta-analysis
Fig. 2. Forest plot of a random effects meta-analysis of randomized trials on vasoconstrictor drugs alone or with albumin versus no interventionor albumin for HRS. The outcome measure is all-cause mortality.
Fig. 3. Forest plots of random effects meta-analyses on terlipressin plus albumin versus albumin for patients with HRS. The outcome measuresare reversal of HRS and improved renal function. The included patients received terlipressin alone or with albumin versus no intervention or albumin.
580 GLUUD ET AL. HEPATOLOGY, February 2010
Gluud 2010
-
LL- Indikation zur Albumingabe bei Patienten mit Zirrhose
Indikation Was sagt die Leitlinie? Dosis
ParacenteseBei Durchführung einer großvolumigen Parazentese (>5l) soll eine intravenöse
Albumingabe (6–8g/Liter Aszites) erfolgen. 8 g/l
Spontan-bakterielle Peritonitis
Begleitend zur antibiotischen Therapie soll die Gabe von Albumin intravenös am Tag der Diagnosestellung und am dritten Tag nach
Diagnosestellung durchgeführt werden.
1,5 g/kg KG am 1. Tag
1 g/kg KG am 3. Tag
Hepatorenales Syndrom
Die intravenöse Albumingabe zum Ausschluss eines Volumenmangels bzw. zur Sicherung der Diagnose
eines hepatorenalen Syndroms sollte erfolgen. Die Kombinationsbehandlung aus Albumininfusion und Vasokonstriktortherapie ist Therapie der ersten
Wahl bei hepatorenalem Syndrom Typ I.
1 g/kg KGmax 100 g20-40 g/Tag
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
Kosten-Nutzen-Analysenfür Paracentese - Eingabewerte
Inputs for LVP
4
Kosten
Effektivität
Inputs for LVP
4
Runken, EASL Abstrakt 2018
Inputs for LVP
4
-
Detaillierte Kosten
Runken, EASL Abstrakt 2018
Cost Details for LVP
5
Cost Details for LVP
5
Cost Details for LVP
5
Kosten-Nutzen-Analysenfür Paracentese - Kosten
-
Therapiekosten
Runken, EASL Abstrakt 2018
Cost-Effectiveness in LVP
Cost-Effectiveness in LVP
Effektivität
Kosten-Nutzen-Analysenfür Paracentese - Ergebnisse
-
Therapiekosten
Runken, EASL Abstrakt 2018
Effektivität
Kosten-Nutzen-Analysenfür SBP - Ergebnisse
Cost-Effectiveness in SBP
Cost-Effectiveness in SBP
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
ANSWER-Studie
Caraceni etal, Lancet, 2018
• Patienten mit Zirrhose und unkomplizierten Aszites
• Behandlung mit Diuretika (Standard) und zusätzlich
Albumin (40 g/2xWochen, dann 40g/1xWoche)
• Ausschluß: LTX, TIPS, refraktärer Aszites/
Paracentese (mehr als 3)
• Primärer Endpunkt: Überleben
• Sekundärer Endpunkt: Komplikationen,
Paracentesen, Qualitiy-of-life, KH-Aufenthalte
-
ANSWER-StudiePatienteneinschluß
Caraceni etal, Lancet, 2018
-
ANSWER-StudieÜberlebensdaten
Caraceni etal, Lancet, 2018
-
ANSWER-StudieNotwendigkeit erste Parazentese
Caraceni etal, Lancet, 2018
-
ANSWER-StudieEntwicklung refraktärer Aszites
Caraceni etal, Lancet, 2018
-
ANSWER-StudieWeitere Ergebnisse/Limitationen
Caraceni etal, Lancet, 2018
• Inzidenzen
• SBP: 0,32, p
-
ÜbersichtLeberzirrhose und Komplikationen
Aufbau und Funktion von Albumin
Therapieempfehlungen der Komplikationen
Kosten-Nutzen-Analyse
ANSWER-Studie
Zusammenfassung
-
Zusammenfassung• Albumin bei Zirrhose ist vermindert und in der
Funktion eingeschränkt• Albumingabe ist wesentlicher Bestandteil der
Therapie bei Komplikationen der Zirrhose• Paracentese• Spontan-bakterielle Peritonitis• Hepato-renales Syndrom
• Regelmäßige Gabe von Albumin in der ANSWER Studie verbessert
• Überleben• Verhindert Entwicklung von Komplikationen
-
Vielen Dank!
Diese Fortbildung wird Ihnen auf cme.medlearning.de mit freundlicher Unterstützung von Grifols Deutschland GmbH angeboten (€ 7.250,00).