Anti-nozizeptive Effekte und Wirkungsweisen aurikularer ... · klinischen und experimentellen...
67
Aus der Klinik und Poliklinik für Anästhesiologie – Anästhesie-, Intensiv-, Notfall- und Schmerzmedizin (Direktor Univ.- Prof. Dr. Klaus Hahnenkamp) der Universitätsmedizin der Universität Greifswald Thema: Anti-nozizeptive Effekte und Wirkungsweisen aurikularer transkutaner Vagusnervenstimulation Inaugural - Dissertation zur Erlangung des akademischen Grades Doktor der Wissenschaften in der Medizin (Dr. rer. med.) der Universitätsmedizin der Universität Greifswald 2018 vorgelegt von: Henriette Janner, geb. Hacker geb. am: 09.03.1991 in: Rostock
Transcript of Anti-nozizeptive Effekte und Wirkungsweisen aurikularer ... · klinischen und experimentellen...

Aus der Klinik und Poliklinik für Anästhesiologie – Anästhesie-, Intensiv-, Notfall- und
Schmerzmedizin
(Direktor Univ.- Prof. Dr. Klaus Hahnenkamp)�
der Universitätsmedizin der Universität Greifswald
Thema: Anti-nozizeptive Effekte und Wirkungsweisen aurikularer transkutaner
Vagusnervenstimulation
Inaugural - Dissertation
zur
Erlangung des akademischen
Grades
Doktor der Wissenschaften in der Medizin
(Dr. rer. med.)
der
Universitätsmedizin
der
Universität Greifswald�
2018
vorgelegt von:
Henriette Janner, geb. Hacker
geb. am: 09.03.1991
in: Rostock

2
Dekan: Prof. Dr. Max P. Baur
1. Gutachter: Prof. Dr. Taras I. Usichenko
2. Gutachter: Prof. Dr. Mathias Weymar
(3. Gutachter:)
Ort, Raum: Greifswald, Konferenzraum D 0.30 der Klinik für Neurologie/Neurochirurgie
Tag der Disputation: 17.06.2019

3
Inhaltsverzeichnis
Zusammenfassung 4
1 Einleitung 6
2 Invasive Vagusnervstimulation (VNS) 6
3 Aurikulare transkutane Vagusnervstimulation (tVNS) 7 3.1 Die aurikulare Akupunktur als tVNS 8 3.2 Die Wirkung aurikularer elektrischer tVNS auf die Schmerzwahrnehmung 10 3.3 Die Wirkung aurikularer tVNS auf Stimmung, Affekt und Kognition 13
4 Zusammenfassung und Ausblick 15
5 Literaturverzeichnis 17
Appendix A: Publikationen 20 Manuskript 1 21 Manuskript 2 31 Manuskript 3 39 Manuskript 4 49

4
Zusammenfassung
Die elektrische, transkutane aurikulare Stimulation des Vagusnervs (tVNS) erwies sich in
klinischen und experimentellen Studien als eine vielversprechende therapeutische Methode zur
Behandlung akuter und chronischer Schmerzen, Epilepsie sowie Stimmungs- und
Angststörungen. Afferente Ausläufer des Vagusnervs innervieren die Haut der menschlichen
Ohrmuscheln. Dadurch ist es möglich diese Nervenenden non-invasiv sowohl elektrisch durch
Elektroden als auch mechanisch z.B. durch die Applikation von Akupunkturnadeln zu
stimulieren. Der Kern des Vagusnervs befindet sich im Nucleus Tractus solitarius des
Hirnstamms, von dem ausgehend neuronale Bahnen zum Locus coeruleus, zu den Raphe-
Kernen, in verschiedene Areale des limbischen Systems sowie in den Neokortex projizieren.
Da diese neuronalen Strukturen mit der Wahrnehmung, Verarbeitung und Regulation von
emotionalen und nozizeptiven Reizen assoziiert sind, ist die tVNS von besonderem
therapeutischem Interesse. Thema dieser Arbeit sind die anti-nozizeptiven Effekte und
möglichen Wirkungsweisen der aurikularen tVNS.
In Studie 1 wurde die Stimulation von Vagusnerv-Afferenzen als möglicher
Wirkmechanismus der Ohrakupunktur postuliert. Zur Überprüfung dieser Hypothese wurde die
Lage von Akupunktur-Punkten, welche in kontrollierten Studien zur Behandlung von
Schmerzen mit Ohrakupunktur verwendetet wurden, hinsichtlich ihrer zugrundeliegenden
Innervationsgebiete in der Ohrmuschel deskriptiv analysiert. Dabei konnte gezeigt werden, dass
die Mehrzahl der Stimulationen an Innervationsgebieten des Vagusnervs erfolgten. In den
Kontrollbedingungen hingegen wurde in der Regel an Orten stimuliert, die ausschließlich von
zervikalen Nerven innerviert sind. Deshalb liegt es nahe, dass die Ohrakupunktur als
mechanische Form der aurikularen tVNS angesehen werden kann.
In Studie 2 wurde der Einfluss von elektrischer tVNS auf die Wahrnehmung von
wiederholten schmerzhaften Hitze-Reizen bei gesunden ProbandInnen untersucht. Dabei wurde
experimentell überprüft, ob tVNS im Vergleich mit aktiver Sham- und inaktiver Placebo-
Stimulation sowie keiner Intervention die wahrgenommene Schmerzintensität und die
Zunahme des Schmerzes durch wiederholte Reizung (temporale Summation von Schmerz als
experimentelle Form zentraler Sensibilisierungsprozesse) reduzieren kann. In der Studie wurde
die Schmerzintensität von allen Interventionen effektiv reduziert, jedoch waren die Effekte der
Interventionen vergleichbar. Nur in der Untergruppe der Männer konnte vor dem Beginn der
temporalen Summation eine Schmerzreduktion durch tVNS gefunden werden, welche größer
als die von Placebo und Sham war. Dahingegen konnte nur in der Untergruppe der Frauen eine
Reduktion der temporalen Summation von Schmerz durch tVNS festgestellt werden. Diese
Ergebnisse deuten auf Geschlechterunterschiede bei der Wirkung von tVNS hin, die
Gegenstand zukünftiger systematischer Untersuchungen sein sollten. Eine unbeabsichtigte
Stimulation vagaler Nervenenden in den Kontrollbedingungen konnte in unserer Studie nicht
ausgeschlossen werden und könnte auch einen Teil der Inkonsistenz hinsichtlich der Befunde

5
zur Wirksamkeit von tVNS in anderen Studien erklären. Darüber hinaus erscheint es möglich,
dass die Stimulation der Vagusnerv-Afferenzen weniger die sensorische, sondern eher die
affektive Verarbeitung der Schmerzreize verändert. Dafür sprechen Ergebnisse aus Studien zur
stimmungsaufhellenden und angstlösenden Wirkung von tVNS sowie Ohrakupunktur.
In Studie 3 wurde überprüft, ob Ohrakupunktur, appliziert an Innervationsgebieten des
Vagusnervs, Prüfungsangst bei Medizinstudierenden im Vergleich mit Placebo-Akupunktur
und keiner Intervention reduzieren kann. Dabei ergab sich, dass sowohl durch Placebo als auch
durch die Ohrakupunktur die situationale Angst vor einer Prüfung gesenkt werden konnte.
Direkt vor der Prüfung waren die Effekte der Ohrakupunktur denen der Placebo-Bedingung
jedoch überlegen. Dies spricht für eine affektive Wirkung von tVNS, welche möglichweise auf
eine Modulation der Aktivität limbischer Strukturen, mediiert durch eine erhöhte
Transmitterausschüttung im Locus coeruleus und den Raphe-Kernen, zurückzuführen sein
könnte.
In Studie 4 wurde die Methodologie der Ohrakupunktur aus Studie 3 zur Reduktion von
prä-operativer Angst untersucht, hinsichtlich ihrer Anwendbarkeit im klinischen Setting, zur
Vorbereitung auf eine randomisierte kontrollierte Studie. Dazu wurden 32 Patientinnen vor
einer ambulanten gynäkologischen Operation mit Ohrakupunktur behandelt und mit 30
Patientinnen ohne weitere Behandlung bezüglich des Ausmaßes an prä-operativer Angst
verglichen. Während bei den Patientinnen mit Ohrakupunktur die Angst vor der Operation
signifikant sank, konnte in der Vergleichsgruppe ein signifikanter Anstieg der Angst beobachtet
werden. Die in dieser Pilotstudie angewendete Methodik erwies sich als umsetzbar und
vielversprechend für die Untersuchung der Wirksamkeit von Ohrakupunktur zur Reduktion von
prä-operativer Angst in einer großen randomisierten kontrollierten klinischen Studie.
Unsere Ergebnisse sowie die anderer aktueller Studien deuten darauf hin, dass die
Stimulation vagal-innervierter Gebiete der Ohrmuschel als nicht-invasive Methode der
Neuromodulation wirksam ist. Dennoch sind die genauen Wirkungsweisen von tVNS bisher
nicht hinreichend belegt und bedürfen weiterer systematischer Untersuchungen. In Bezug auf
anti-nozizeptive Effekte aurikularer tVNS scheint es essentiell, zukünftig die Einflüsse der
tVNS auf die sensorische und affektive Komponente der Schmerzverarbeitung getrennt zu
untersuchen. Bildgebende Verfahren und pharmakologische Blockaden können ferner helfen,
weiteres Verständnis über die komplexen Wirkungsweisen von tVNS auf neuronaler Ebene zu
erlangen.

6
1 Einleitung
Die Stimulation des Vagusnervs ist eine vielversprechende therapeutische Methode der
Neuromodulation zur Behandlung von akuten und chronischen Schmerzen, epileptischen
Anfällen sowie Stimmungsstörungen und Angstzuständen (Menachem et al., 2015; Frangos et
al., 2017). Dabei kann die Stimulation elektrisch mit Hilfe invasiver Elektroden sowie non-
invasiv transkutan erfolgen (Ben-Groves & Brown, 2005; Menachem et al., 2015; Frangos et
al., 2017). Als Ort für eine nicht-invasive Stimulation des Vagus-Nervs eignet sich
insbesondere die Ohrmuschel, da dort die Haut unter anderem von vagalen Afferenzen
innerviert ist (Peuker & Filler, 2002). In der folgenden Arbeit sollen zunächst kurz die
Besonderheiten sowie die therapeutischen Anwendungen der Stimulation dieses Hirnnervs
beschrieben werden. Auf Grundlage von vier Publikationen unserer Arbeitsgruppe wird die
Vagusnervstimulation als möglicher Wirkmechanismus der Ohrakupunktur postuliert
(Manuskript 1). Anschließend werden die Ergebnisse unserer experimentellen Studie zur
Wirkung von tVNS auf die Wahrnehmung von wiederholten schmerzhaften Hitzereizen
vorgestellt und diskutiert (Manuskript 2). Im letzten Teil der Arbeit wird auf der Grundlage der
Ergebnisse zweier weiterer Untersuchungen zu den Effekten von Ohrakupunktur zur Reduktion
von Prüfungsangst (Manuskript 3) sowie prä-operativer Angst (Manuskript 4) ein alternativer
Wirkmechanismus der tVNS sowie dessen systematische Untersuchung in zukünftigen Studien
vorgeschlagen.
2 Invasive Vagusnervstimulation (VNS)
Der Vagusnerv innerviert als längster der Hirnnerven die Organe des Halses, des Thorax
und des Abdomens und besteht zu 20% aus parasympathischen efferent-motorischen Nerven,
welche an der Regulation und Kontrolle autonomer Funktionen, wie z.B. Herzrate, Blutdruck,
Verdauung und Atmung, beteiligt sind (Groves & Brown, 2005). 80% des Vagusnervs sind
afferent-sensorische Fasern, deren Kern sich im Nucleus tractus solitarius des Hirnstamms
befindet (Randich & Gebhart, 1992; Groves & Brown, 2005). Ausgehend von diesen
Hirnstrukturen projizieren Fasern in die ventromediale Medulla, den Locus coeruleus, in das
periäquadukatale Grau, den Hypothalamus und die Amygdala (Randich & Gebhart, 1992;
Groves & Brown, 2005). Diese Strukturen sind unter anderem mit der Transmission und
Verarbeitung nozizeptiver Reize sowie mit der Modulation von emotionaler Erregung und der
Schmerzwahrnehmung assoziiert (Ossipov et al., 2010; Lindquist et al., 2012). Aufgrund dieser

7
engen Verbindung der Vagus-Afferenzen mit den genannten Hirnstrukturen, ist die Stimulation
des Vagusnervs von vielfältigem therapeutischem Interesse.
Zunächst wurde die Vagusnervstimulation (VNS) zur Behandlung von fokaler Epilepsie
zugelassen (Groves & Brown, 2005). Dafür werden Elektroden direkt am Vagusnerv im Hals
implantiert, um die Nervenfasern über ein Stimulationsgerät mit geringer Stromstärke reizen zu
können. Da Patienten während dieser invasiven Behandlungsmethode oft eine Steigerung der
Stimmung berichteten, wurde die VNS auch zur Behandlung von therapieresistenten
Depressionen erforscht und mittlerweile für diese Anwendung zugelassen (Ben-Menachem et
al., 2015). Darüber hinaus ist die Behandlung von Angststörungen, Morbus Alzheimer und
chronischen Schmerzen mit invasiver VNS Gegenstand aktueller Forschung (Groves & Brown,
2005; Ben-Menachem et al., 2015; Frangos et al. 2017).
Die chirurgische Implantation von Vagusnerv-Stimulatoren ist jedoch mit einigen
Risiken verbunden. Sowohl bei der Operation, als auch beim Batteriewechsel oder bei einer
Fehlfunktion der Geräte können teilweise lebensgefährliche Komplikationen auftreten, wie z.B.
Infektionen, Bradykardie, ventrikulare Asystolen, Herzblock und Stimmbandlähmung (Ben-
Menachem et al., 2015). Um zudem mögliche unerwünschte Nebenwirkungen von invasiver
VNS wie Stimmveränderung, Husten, Kurzatmigkeit, Parästhesie und (Kopf)-schmerzen zu
vermeiden, wurde in den letzten Jahren zunehmend die Wirksamkeit von nicht-invasiver
elektrischer VNS erforscht (Ben-Menachem et al., 2015; Frangos et al., 2017).
3 Aurikulare transkutane Vagusnervstimulation (tVNS)
Methoden der nicht-invasiven VNS basieren auf anatomischen Daten der afferenten
Vagusnerven-Versorgung der Haut. Dabei sind insbesondere der äußere Gehörkanal und die
Conchae der Ohrmuschel von Interesse, da diese durch den Ramus auricularis, einem
afferenten Ausläufer des Vagusnervs, versorgt werden (Peuker & Filler, 2002). Bildgebende
Studien zeigten, dass die elektrische, transkutane Stimulation der Ohrmuschel bzw. des äußeren
Gehörgangs zum einen mit der Steigerung der Aktivität in Nucleus tractus solitarius, Locus
coeruleus, dorsalen Raphe Kernen, Insula, Nucleus accumbens, präzentrale Gyrus, Thalamus
und anterioren cingularen Kortex assoziiert ist. Zum anderen wird sie mit verminderter
Aktivität in limbischen Regionen wie der Amygdala, dem Hypothalamus, dem Hippocampus,
dem Parahippocampus, dem mittleren und superioren Gyrus temporalis und dem posterioren
cingularen Kortex in Verbindung gebracht. Diese Hirnareale stehen in Verbindung mit der
Verarbeitung und Regulation von emotionalen und nozizeptiven Reizen (Dietrich et al., 2008;
Kraus et al., 2013; Frangos et al., 2015; Usichenko et al., 2017a; Yakunina et al., 2016).

8
Untersucht wurde die tVNS bisher hauptsächlich zur Reduktion epileptischer Anfälle, zur
Verbesserung kognitiver Funktionen, zur Reduktion von situationaler Angst, zur
Stimmungsaufhellung und zur Schmerzlinderung (Ben-Menchanem et al., 2015; Frangos et al.
2017).
3.1 Die aurikulare Akupunktur als tVNS
Die aurikulare Akupunktur oder auch Ohrakupunktur ist eine komplementär-
medizinische Methode, die zur Behandlung von verschiedenen Krankheiten und Zuständen
angewandt wird (Usichenko & Anders, 2016). In ihrer differenziertesten Form geht sie als
therapeutische Methode auf den französischen Arzt Paul Nogier zurück. Dieser ersetzte um
1950 die bis dahin von „Heilern“ durchgeführte Kauterisierung bestimmter Punkte an den
Ohrmuscheln zur Behandlung von Krankheiten, wie z.B. Rückenschmerzen, durch die
mechanische Stimulation mittels Nadeln. In der Theorie von Nogier (1957) gehen
Dysfunktionen in Organen mit Veränderungen in bestimmten Arealen der Ohrmuschel einher,
wobei der gesamte menschliche Körper im externen Aurikel somatotop repräsentiert sei
(Nogier, 1957). Die Reizung dieser Areale, welche in Verbindung mit dem entsprechenden
Organ stünden, soll laut Nogier zur Verbesserung der Organfunktion führen bzw. Schmerz
lindern (Nogier, 1957; Usichenko & Anders, 2016). Tatsächlich konnte in zwei Studien erhöhte
Hautleitfähigkeit sowie reduzierte Gewebedichte an den von Nogier postulierten Punkten bei
Patienten mit Skelettmuskelschmerzen und koronaren Herzerkrankungen gefunden werden
(Oleson et al., 1980; Saku et al. 1993). Dennoch ist die genaue Art der Verbindung zwischen
den Arealen im Ohr und den Organen bisher nicht hinreichend in der Literatur beschrieben
worden (Usichenko & Anders, 2016; Usichenko et al., 2017b).
In randomisierten kontrollierten Studien konnte gezeigt werden, dass die
Ohrakupunktur im Vergleich mit Placebo- und Sham-Akupunktur insbesondere bei der
Behandlung von Schmerzen effektiv ist (Asher et al., 2010; Usichenko & Anders, 2016). Dabei
gibt es Befunde zur Senkung des post- und peri-operativen Opiod-Bedarfs sowie zur Linderung
akuter und chronische Schmerzen durch Ohrakupunktur (Asher et al., 2010). Als ein den
Effekten zugrundeliegender Wirkmechanismus kommt dabei die mechanische Stimulation
vagaler Nervenenden in der Ohrmuschel in Betracht. Zur Überprüfung dieser Hypothese haben
wir die Daten aus der bis zu diesem Zeitpunkt einzigen Meta-Analyse von ausreichender
wissenschaftlicher Qualität, veröffentlicht von Asher et al. (2010), hinsichtlich der
Innervationsgebiete der verwendeten Stimulationsorte analysiert (Usichenko et al., 2017b;
Manuskript 1). In die Meta-Analyse von Asher et al. (2010) wurden 17 randomisierte,

9
kontrollierte Studien über die Effekte von Ohrakupunktur zur Behandlung von akuten und
chronischen Schmerzen einbezogen (Asher et al., 2010).
Wir extrahierten aus dem Artikel von Asher et al. (2010) sowie den originalen Arbeiten
die spezifischen Ohrakupunktur-Punkte, welche zur Behandlung von Schmerzen untersucht
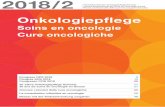
wurden sowie die verwendeten Orte der Kontroll-Stimulationen. Abbildung 1 zeigt die
Lokalisation der verwendeten Akupunktur- und Kontroll-Punkte auf der schematischen
Zeichnung einer Ohrmuschel sowie die Innervationsgebiete der Ohrmuschel nach Peuker und
Filler (Peuker & Filler, 2002).
Unsere Analyse ergab, dass mit 15 von 20 Akupunktur-Punkten Areale stimuliert wurden,
die entweder exklusiv von Vagusnerv-Afferenzen oder sowohl von kranialen als auch von
zervikalen Nerven innerviert waren. Sham-Stimulationen hingegen erfolgten an der Helix oder
den Ohrläppchen, welche zervikal innerviert sind.
Demnach erscheint es möglich, dass Ohrakupunktur als mechanische Form der tVNS
betrachtet werden kann, wobei der Wirkmechanismus auf der Stimulation kranialer Nerven und
assoziierter Hirnareale beruht.
Abbildung 1: In den Studien verwendete Ohrakupunkturpunkte (schwarze Kreise), Sham-Stimulationspunkte (Dreiecke) und Innervationsgebiete der Ohrmuschel durch Vagusnerv (VN), Plexus Cervicale (PC) und Trigeminusnerv (TN).

10
3.2 Die Wirkung aurikularer elektrischer tVNS auf die Schmerzwahrnehmung
Hinsichtlich der anti-nozizeptiven Effekte der tVNS wird angenommen, dass die
Stimulation der Vagusnerv-Afferenzen, durch deren Verbindungen zu den oben beschriebenen
Hirnarealen, zu einer Aktivierung des sogenannten endogenen absteigenden schmerz-
hemmenden Systems führt (Ossipov et al. 2010; Frangos et al., 2017; Usichenko et al., 2017a;
Usichenko et al., 2017b). Dieses beruht auf der Freisetzung von Monoaminen sowie einer „top-
down“ Inhibition der Weiterleitung nozizeptiver Reize auf Spinal-Ebene (Ossipov et al., 2010).
Elektrische tVNS erwies sich in klinischen Studien insbesondere bei der Behandlung
von Migräne und Cluster Kopfschmerz als wirksam (Silberstein et al, 2016a; Silberstein et al,
2016b; Frangos et al., 2017). Experimentelle Studien konnten zeigen, dass die elektrische
Stimulation der Conchae, Triangular fossa und des Tragus im Vergleich zur Stimulation der
Helix and Scapha des Ohrs Schmerzschwellen erhöhen bzw. wahrgenommene
Schmerzintensität während tonischer Schmerzstimulation senken konnte (Oliveri et al. 1985;
Simmons et al., 1991; Busch et al., 2013). Im Gegensatz dazu fanden Johnson et al. (1991)
keine Effekte von aurikularer elektrischer Stimulation auf die (elektrischen) Schmerzschwellen
(Johnson, 1991). Laqua et al. (2014) und Usichenko et al. (2017) fanden nur bei einem Teil der
untersuchten Probanden erhöhte Hitze-Schmerzschwellen unter tVNS (Laqua et al., 2014;
Usichenko et al., 2017a). Die inkonsistente Befundlage könnte auch dadurch begünstigt
werden, dass es herkömmlichen experimentellen Schmerz induzierenden Methoden oftmals an
Sensitivität und externer Validität mangelt, um moderate analgetische Effekte nachzuweisen
(Staahl et al., 2004).
Um klinische (chronische) Schmerzerfahrungen experimentell valider imitieren zu
können, ist die Untersuchung der Wahrnehmung von wiederholten schmerzhaften Reizen
besonders geeignet (Herrero, et al., 2000; Staahl et al., 2004). Wiederholte schmerzhafte
Reizung kann zu einer zunehmenden Schmerzintensität bei gleicher Reizstärke führen; ein
Phänomen, welches als temporale Summation von Schmerz bekannt ist (Herrero et al., 2000;
Granot et al., 2002). Temporale Summation von Schmerz gilt als perzeptives Korrelat zentraler
Sensibilisierung (Herrero et al., 2000; Granot et al. 2002; Anderson et al., 2013). Letztere ist
eine Voraussetzung für die Entwicklung chronischer Schmerzen (Herrero et al., 2000; Granot
et al. 2002; Anderson et al., 2013). Die experimentelle Untersuchung von zentraler
Sensibilisierung und dem Einfluss von hypo-/analgetischen Interventionen auf diese Prozesse
kann neue Aufschlüsse über biologische Schmerzmechanismen sowie die Behandlung von
chronischen Schmerzen geben. Herkömmliche Methoden zur Erzeugung dieses Phänomens
fallen jedoch durch große Variabilität hinsichtlich des Auftretens der temporalen Summation
von Schmerz auf (Anderson et al., 2013). Im vergangenen Jahr haben wir deshalb ein neues

11
Paradigma entwickelt und in einer methodologischen Studie getestet. Mit unserer Methode
gelingt es uns zuverlässig temporale Summation von Schmerz zu erzeugen, während wir eine
Erhöhung der externen Validität gegenüber anderen Schmerzmodellen erreichten (Möller et al.,
2017).
Um weiteres Verständnis über die Wirksamkeit und die Wirkungsweisen transkutaner
Vagusnervstimulation zu erlangen, untersuchten wir in einer randomisierten kontrollierten
Crossover-Studie den Einfluss von elektrischer tVNS auf die Wahrnehmung von wiederholten
schmerzhaften Hitze-Reizen bei gesunden Probanden und Probandinnen. Dabei überprüften
wir, ob die wahrgenommene Intensität von wiederholten schmerzhaften Hitze-Reizen unter
dem Einfluss von tVNS geringer ist verglichen mit dem Einfluss von Sham- und Placebo-
Stimulation sowie der Schmerzintensität ohne Intervention. Darüber hinaus untersuchten wir,
ob tVNS das Ausmaß von temporaler Summation von Schmerz durch wiederholte schmerzhafte
Hitze-Reizung im Vergleich mit Sham- oder Placebo-Stimulation sowie ohne Intervention
reduziert (Janner et al., 2018; Manuskript 2).
49 Probanden (25 Frauen) nahmen dafür an vier Untersuchungen teil, während derer jeweils
90 pulsierende Hitze-Reize mit Schmerztoleranztemperatur mittels einer Thermode (CHEPS,
Medoc Advanced Medical Systems, Ramat Yishai, Israel) am Unterarm appliziert wurden. Die
Probanden bewerteten die Schmerzintensität des ersten und jeden 10. Reizes auf einer
numerischen Skala (0=keine Empfindung bis 100=unerträglicher Schmerz). In der ersten
Untersuchung wurde die wahrgenommene Schmerzintensität ohne Intervention erfasst. In den
drei folgenden wurde in randomisierter Reihenfolge tVNS bzw. Placebo-Stimulation (inaktives
Gerät) in den Ohrmuscheln und Sham-Stimulation an den Ohrläppchen für 20 min vor sowie
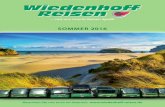
während der Hitze-Reizungen durchgeführt (Janner et al., 2018; Abbildung 2A).
Die wahrgenommene Schmerzintensität wurde durch alle Interventionen im Vergleich mit den
Werten ohne Intervention signifikant reduziert. Die hypoalgetischen Effekte von tVNS waren
in der Gesamtgruppe jedoch vergleichbar mit denen der Sham- und Placebo-Stimulationen. In
der Untergruppe der Männer war der Effekt der tVNS vor dem Beginn der temporalen
Summation des Schmerzes denen der Sham- und Placebo-Stimulation überlegen. Damit weisen
die Ergebnisse auf mögliche Geschlechterunterschiede hinsichtlich der Effekte von
Ohrstimulation hin, welche zukünftig Gegenstand systematischer Untersuchungen sein sollten.

12
Wie in Abbildung 2B dargestellt war der Verlauf der wahrgenommenen
Schmerzintensitäten über die Zeit in allen Bedingungen sehr ähnlich: nach einer initialen
Abnahme des Schmerzes, nahm die Schmerzintensität mit zunehmender Stimulus-Anzahl
wieder substantiell zu (temporale Summation). Dieses Muster könnte eine adaptive Reaktion
auf die wiederholte Stimulation mit Schmerzreizen reflektieren. Ein initiales „Warnsignal“,
gekennzeichnet durch hohe wahrgenommene Reizintensität, wird dabei von Schmerz
regulierenden Prozessen gefolgt, währenddessen die Person an die Stimulation habituiert, z.B.
durch die Adaptation der peripheren Nozizeptoren und/oder eine zentrale „top-down“
Suppression der Antwortraten im primären nozizeptiven Neuron im Rückenmark, (Andrew &
Greenspan, 1999; Herrero et al., 2000). Die anhaltende Reizung könnte dann zu einer zentralen
Sensibilisierung mit zunehmender Schmerzintensität führen (Herrero et al., 2000), welche die
Person dazu drängt, der schmerzhaften Reizung entgegenzuwirken, um Verletzungen des
Gewebes zu verhindern.
Die temporale Summation des Schmerzes wurde nur in der Untergruppe der Frauen,
signifikant durch die tVNS reduziert im Vergleich mit den Werten ohne Intervention (Janner et
al., 2018). Auch dieses Ergebnis deutet auf mögliche Geschlechterunterschiede bei der Wirkung
von tVNS hin.
Die deutlichen Effekte der Kontrollbedingungen auf die Schmerzwahrnehmung könnten
aufgrund von methodologischen Besonderheiten, welche im Manuskript 2 genauer beschrieben
Abbildung 1 A: Stimulationsorte der transkutanen Vagusnervenstimulation (TVNS), aktiver Sham- bzw. inaktiver Placebo-Stimulation am Ohr. B: Veränderungen der Schmerzintensität bei wiederholter Hitze-Reizung. Daten sind dargestellt als Mittelwerte ± Standardfehler. ***p < .001 für den Haupteffekt „Bedingung“ in der Varianzanalyse.

13
werden, auch auf eine unabsichtliche Stimulation vagaler Nervenenden (mechanisch durch
Druck der Elektroden oder elektrisch weitergeleitete Aktivierung benachbarter Nervenenden)
beruhen. Selbst eine unspezifische mechanische Stimulation vagaler Afferenzen könnte zur
Aktivierung bestimmter Hirnareale führen und eine veränderte Verarbeitung nozizeptiver oder
emotionaler Reize im Allgemeinen bewirken (Janner et al., 2018). Darüber hinaus ist es
möglich, dass tVNS eher die affektive und weniger die sensorische Komponente der
Schmerzwahrnehmung beeinflusst, wobei erstere in unserer Studie nicht isoliert erfasst wurde.
Für eine Beeinflussung der affektiven Komponente der Schmerzwahrnehmung durch tVNS
sprechen z.B. Befunde zu stimmungsaufhellender sowie angstreduzierender Wirkung von
elektrischer tVNS und Ohrakupunktur (Usichenko & Anders, 2016; Frangos et al., 2017).
3.3 Die Wirkung aurikularer tVNS auf Stimmung, Affekt und Kognition
Die stimmungsaufhellenden und angstlösenden Effekte von tVNS, welche sowohl bei
gesunden Probanden als auch Patienten mit depressiven Erkrankungen gefunden wurden,
werden mit einer durch tVNS aktivierten Steigerung der serotonergen und noradrenegen
Transmitterauschüttung im Locus coeruleus und den Raphe Kernen, welche durch deren enge
Verbindungen mit Strukturen des limbischen Systems maßgeblich an der Regulation
emotionaler Prozesse beteiligt sind, in Zusammenhang gebracht. Darüber hinaus wurden
Ergebnisse zum Einfluss von tVNS auf verschiedene kognitive Prozesse wie Aufmerksamkeit,
Gedächtnisleistung und Extinktionslernen veröffentlicht (Frangos et al., 2017).
Auch mechanische tVNS in Form von Ohrakupunktur erwies sich in verschiedenen
Studien als effektives Mittel zur Reduktion situationaler Angst in klinischen Settings z.B. bei
präoperativer Angst und Dentophobie (Wang et al., 2001; Karst et al., 2007; Michalek-Sauberer
et al., 2012). Darauf aufbauend untersuchten wir in einer weiteren randomisierten kontrollierten
Studie die Effektivität von Ohrakupunktur zur Reduktion von Prüfungsangst in gesunden
Medizinstudierenden (Klausenitz et al., 2016; Manuskript 3). Dafür erhielten 44
Medizinstudierende randomisiert Ohrakupunktur, Placebo-Akupunktur und keine Intervention
bevor sie drei aufeinander folgende, vergleichbare, mündliche Prüfungen absolvierten. So
genannte Ohrakupunktur-Dauernadeln wurden beidseitig an den nach WHO-Nomenklatur
bezeichneten Punkten MA-IC1, MA-TF1, MA-SC, MAAT1 und MA-TG (World Health
Organization, 1987; Abbildung 3) am Tag vor der Prüfung appliziert. Placebo-Nadeln wurden
als Kontrolle verwendet. Die Stärke der Angst wurde mittels visuellen Analogskala und State-
Anxiety Inventar vor und nach jeder Intervention sowie direkt vor der Prüfung erfasst
(KLausenitz et al., 2016). Im Vergleich mit den Werten ohne Intervention war die situationale
Angst sowohl nach der Ohrakupunktur als auch nach der Placebo-Akupunktur reduziert. Direkt

14
vor der mündlichen Prüfung war die Reduktion der Angst durch die Ohrakupunktur jedoch
signifikant größer als die der Placebo-Akupunktur. Diese Ergebnisse sprechen für eine
angstlösende Wirkung der Ohrakupunktur und rücken diese als mögliche alternative
Behandlung zu nebenwirkungsreichen angstlösenden Medikamenten in den Fokus.
In einer Pilot-Studie haben wir deshalb die Methodologie der Ohrakupunktur von
Klausenitz et al. (2016) zur Reduktion von prä-operativer Angst hinsichtlich ihrer
Anwendbarkeit im klinischen Setting in Vorbereitung auf eine randomisierte kontrollierte
klinische Studie untersucht (Klausenitz et al., 2016; Wunsch et al., 2018; Manuskript 4). Dazu
wurden 32 Patientinnen vor einer ambulanten gynäkologischen Operation mit der oben
beschriebenen Ohrakupunktur-Methodik behandelt und mit 30 Patienten ohne weitere
Behandlung bezüglich des Ausmaßes an prä-operativer Angst verglichen. Während bei den
Patienten mit Ohrakupunktur die Angst vor der Operation signifikant sank, konnte in der
Vergleichsgruppe ein signifikanter Anstieg der Angst beobachtet werden. Die in dieser
Pilotstudie angewendete Methodik erwies sich als umsetzbar und vielversprechend für die
Untersuchung der Wirksamkeit von Ohrakupunktur zur Reduktion von prä-operativer Angst in
einer großen randomisierten kontrollierten Studie (Wunsch et al., 2018).
Abbildung 3: Verwendete Ohrakupunktur-Punkte bezeichnet nach WHO-Nomenklatur (schwarze Kreise) und Placebo-Stimulationspunkte (Dreiecke).

15
4 Zusammenfassung und Ausblick
Thema dieser Arbeit waren die anti-nozizeptiven Effekte und möglichen
Wirkungsweisen der aurikularen transkutanen Vagusnervenstimulation. Dabei wurde die
Vagusnervenstimulation als ein möglicher Wirkmechanismus der Ohrakupunktur postuliert. Im
Rahmen unserer experimentellen Studie erwiesen sich sowohl tVNS als auch die Placebo- und
Sham-Stimulation als effektiv bei der Reduktion der Schmerzintensität, wobei die Effektstärken
der Interventionen vergleichbar waren. Weiter fanden wir Hinweise für mögliche
Geschlechterunterschiede bei der Wirkung von tVNS auf die Wahrnehmung von wiederholten
schmerzhaften Hitze-Reizen sowie die temporale Summation von Schmerz. Eine
unbeabsichtigte Stimulation vagaler Nervenenden in den Kontrollbedingungen konnte in
unserer Studie nicht ausgeschlossen werden und könnte auch einen Teil der Inkonsistenz
hinsichtlich der Befunde zur Wirksamkeit von tVNS in anderen Studien erklären. Deshalb ist
die Beachtung der methodologischen Besonderheiten bei aktiver Sham- und inaktiver Placebo-
Stimulation in zukünftigen Studien von zentraler Relevanz, um eine Verzerrung der Ergebnisse
zu verhindern. Darüber hinaus erscheint es möglich, dass die Stimulation der Vagusnerv-
Afferenzen keinen Einfluss auf die sensorischen Komponenten der neuronalen Verarbeitung
nozizeptiver Reize hat, sondern eher die affektive Verarbeitung der Schmerzreize verändert.
Diese Annahme wird unter anderem durch die Ergebnisse unserer Studien zu den Effekten von
mechanischer tVNS in Form von Ohrakupunktur zur Reduktion von Prüfungsangst sowie prä-
operativer Angst gestützt.
In zukünftigen Studien sollten demnach die schmerzlindernden Effekte von tVNS im
Vergleich zu einer aktiven Sham-Stimulation am Ohrläppchen jedoch mit sehr geringerer
Stromstärke durchgeführt werden, um eine ungewollte Stimulation kranialer Nerven zu
vermeiden. Zudem sollte in weiteren Studien darauf geachtet werden, die
Stimulationsparameter, wie z.B. den genauen Stimulationsort zu standardisieren, um die
Vergleichbarkeit zwischen den Studien zu erhöhen und möglicherweise Inkonsistenzen in den
Ergebnissen zu minimieren. Um die Stimulation zervikaler Nerven oder des Trigeminusnervs
zu vermeiden, bietet sich als Stimulationsort vor allem die Cymba Concha der Ohrmuschel an,
da diese laut Peuker und Filler (2002) ausschließlich vagal innerviert wird (Peuker & Filler,
2002). Einflüsse der tVNS auf die sensorische und affektive Komponente der
Schmerzverarbeitung sollten getrennt systematisch untersucht werden. Dabei sollten sowohl
Stichproben von gesunden Probanden als auch von Patienten mit z.B. chronischen
Schmerzerkrankungen untersucht werden, da sich Wirksamkeit und Wirkungsweisen der tVNS
in beiden Gruppen aufgrund von krankheits-assoziierten (neuronalen) Veränderungen
unterscheiden könnte.

16
Zusammenfassend lässt sich feststellen, dass die Ergebnisse einer Vielzahl von Studien
darauf hindeuten, dass die Stimulation vor allem vagal-innervierter Gebiete der Ohrmuschel als
nicht-invasive Methode der Neuromodulation wirksam ist. Dennoch sind die genauen
Wirkungsweisen von tVNS bisher nicht hinreichend belegt und bedürfen weiterer
systematischer Untersuchungen. Bildgebende Verfahren und pharmakologische Blockaden
z.B. muskarinerger Rezeptoren können ferner helfen, weiteres Verständnis über die komplexen
Wirkungsweisen von tVNS zu erlangen.

17
5 Literaturverzeichnis
• Anderson RJ, Craggs JG, Bialosky JE, Bishop MD, George SZ, Staud R, Robinson ME.
Temporal Summation of Second Pain: Variability in Responses to a Fixed Protocol. Eur J
Pain 2013;17:67–74.
• Andrew D, Greenspan JD. Peripheral coding of tonic mechanical cutaneous pain:
comparison of nociceptor activity in rat and human psychophysics. J Neurophysiol
1999;82:2641-8.
• Asher GN, Jonas DE, Coeytaux RR, Reilly AC, Loh YL, Motsinger-Reif AA, Winham SJ.
Auriculotherapy for pain management: a systematic review and meta-analysis of
randomized controlled trials. J Altern Complement Med 2010;16:1097-108.
• Ben-Menachem E, Revesz D, Simon BJ, Silberstein S. Surgically implanted and non-
invasive vagus nerve stimulation: a review of efficacy, safety and tolerability. Eur J Neurol
2015;22:1260-8.
• Busch V, Zeman F, Heckel A, Menne F, Ellrich J, Eichhammer P. The effect of
transcutaneous vagus nerve stimulation on pain perception – An experimental study. Brain
Stim 2013;6:202-9.
• Dietrich S, Smith J, Scherzinger C, Hofmann-Preiß K, Freitag T, Eisenkolb A, Ringler R.
A novel transcutaneous vagus nerve stimulation leads to brainstem and cerebral activations
measured by functional MRI. Biomed Engin 2008;53:104–11.
• Frangos E, Ellrich J, Komisaruk BR. Non-invasive Access to the Vagus Nerve Central
Projections via Electrical Stimulation of the External Ear: fMRI Evidence in Humans.
Brain Stim 2015;8:624-32.
• Frangos E, Richards EA, Bushnell C. Do psychological effects of vagus nerve stimulation
partially mediate vagal pain modulation? Neurobiol Pain. 2017;1:37-45.
• Granot M, Granovsky Y, Sprecher E, Nir RR, Yarnitsky D. Contact heat-evoked temporal
summation: Tonic versus repetitive-phasic stimulation. Pain 2006;122:295-305.
• Groves DA, Brown VJ. Vagal nerve stimulation: a review of its applications and potential
mechanisms that mediate its clinical effects. Neurosci Biobehav Rev 2005;29:493–500.
• Janner H, Klausenitz C, Gürtler N, Hahnenkamp K, Usichenko TI. Effects of Electrical
Transcutaneous Vagus Nerve Stimulation on the Perceived Intensity of Repetitive Painful
Heat Stimuli: A Blinded Placebo- and Sham-Controlled Randomized Crossover
Investigation. Anesth Anal 2018;126:2085-92.
• Herrero JF, Laird JMA, Lopez-Garcia JA. Wind-up of spinal cord neurones and pain
sensation: Much ado about something? Prog Neurobiol 2000;61:169–203.

18
• Johnson MI, Hajela VK, Ashton CH, Thompson JW. The effects of Auricular
Transcutaneous Electrical Nerve Stimulation (TENS) on experimental pain threshold and
autonomic function in healthy subjects. Pain 1991;46:337-42.
• Karst M, Winterhalter M, MuÈnte S, Francki B, Hondronikos A, Eckardt A, Hoy L, Buhck
H, Bernateck M, Fink M. Auricular acupuncture for dental anxiety: a randomized
controlled trial. Anesth Analg 2007;104:295-300.
• Kraus T, Kiess O, Hösl K, Terekhin P, Kornhuber J, Forster C. CNS BOLD fMRI Effects
of Sham-Controlled Transcutaneous Electrical Nerve Stimulation in the Left Outer
Auditory Canal – A Pilot Study. Brain Stim 2013;6:798-804.
• Klausenitz C, Hacker H, Hesse T, Kohlmann T, Endlich K, Hahnenkamp K, Usichenko
T. Auricular Acupuncture for Exam Anxiety in Medical Students-A Randomized
Crossover Investigation. Plos One 2016;11:e0168338 doi:10.1371/journal.pone.0168338. • Laqua R, Leutzow B, Wendt M, Usichenko T. Transcutaneous vagal nerve stimulation may
elicit anti- and pro-nociceptive effects under experimentally-induced pain - a crossover
placebo-controlled investigation. Auton Neurosci 2014;185:120-2.
• Lindquist KA, Wager TD, Kober H, Bliss-Moreau E, Barrett LF. The brain basis of
emotion: a meta-analytic review. Behav Brain Sci 2012;35:121-43.
• Michalek-Sauberer A, Gusenleitner E, Gleiss A, Tepper G, Deusch E. Auricular
acupuncture effectively reduces state anxiety before dental treatment: a randomised
controlled trial. Clin Oral Investig 2012;16:1517-22.
• Moeller N, Hacker H, Usichenko T. Search for optimal protocol of temporal summation
of experimental heat pain in healthy volunteers [abstract]. Clin Neurophysiol
2017;128:e158. doi:10.1016/j.clinph.2016.10.410.
• Nogier PMF. Über die Akupunktur der Ohrmuschel. Dt Ztschr Akup 1957;6:25-35.
• Oleson TD, Kroening RJ, Bresler DE. An experimental evaluation of auricular diagnosis:
the somatotopic mapping or musculoskeletal pain at ear acupuncture points. Pain
1980;8:217-29.
• Oliveri AC, Clelland JA, Jackson J, Knowles C. Effects of auricular transcutaneous
electrical nerve stimulation on experimental pain threshold. Phys Ther 1985;66:12-6.
• Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest
2010;120:3779–87.
• Peuker ET, Filler TJ. Nerve supply of the human auricle. Clin Anat 2002;15:35-7.
• Randich A, Gebhart GF. Vagal afferent modulation of nociception. Brain Res Rev
1992;17:77-99.
• Silberstein SD, Calhoun AH, Lipton RB, Grosberg BM, Cady RK, Dorlas S, Simmons KA,
Mullin C, Liebler EJ, Goadsby PJ, Saper JR. Chronic migraine headache prevention with
noninvasive vagus nerve stimulation. Neurology 2016a;87:529–38.

19
• Silberstein SD, Mechtle LL, Kudrow DB, Calhoun AH, McClure C, Saper JR, Liebler EJ,
Rubenstein-Engel E, Tepper SJ. Non–Invasive Vagus Nerve Stimulation for the ACute
Treatment of Cluster Headache: Findings From the Randomized, Double-Blind, Sham-
Controlled ACT1 Study. Headache 2016b;56:1317-32.
• Simmons MS, Oleson TD. Auricular electrical stimulation and dental pain threshold.
Anesth Prog 1993;40:14-9.
• Staahl C, Drewes AM. Experimental human pain models: a review of standardised methods
for preclinical testing of analgesics. Basic Clin Pharmacol Toxicol 2004;95:97-111.
• Saku K, Mukaino Y, Ying H, Arakawa K. Characteristics of reactive electropermeable
points on the auricles of coronary heart disease patients. Clin Cardiol 1993;16:415e9.
• Usichenko T, Anders E. Auricular acupuncture. In: Filshie White, Cummings, editors.
Medical acupuncture: a western scientific approach. second ed. Elsevier; 2016, p. 144-166.
• Usichenko T, Laqua R, Leutzow B, Lotze M. Preliminary findings of cerebral responses
on transcutaneous vagal nerve stimulation on experimental heat pain. Brain Imaging Behav
2017a;11:30-7.
• Usichenko T, Hacker H, Lotze M. Transcutaneous auricular vagal nerve stimulation
(taVNS) might be a mechanism behind the analgesic effects of auricular acupuncture. Brain
Stim 2017b;10:1042-44.
• Wang SM, Peloquin C, Kain ZN. The use of auricular acupuncture to reduce preoperative
anxiety. Anesth Analg 2001;93:1178-80. • World Health Organization, Regional Office of the Western Pacific. Third WHO Regional
Working Group on the Standardization of Acupuncture Nomenclature: report. Manila:
Regional Office of the Western Pacific; 1987.
• Wunsch J, Klausenitz C, Janner H, Hesse T, Mustea A, Hahnenkamp K, Petersmann A,
Usichenko T. Auricular acupuncture for treatment of preoperative anxiety in patients
scheduled for ambulatory gynaecological surgery - a prospective controlled investigation
with non-randomised arm. Acupunct Med Forthcoming 2018. doi: 10.1136/acupmed-2017-011456
• Yakunina N, Kim SS, Nam EC. Optimization of Transcutaneous Vagus Nerve Stimulation
Using Functional MRI. Neuromodulation 2017;20:290-300.

20
Appendix A: Publikationen
Manuskript 1:
Usichenko T, Hacker H, Lotze M. Transcutaneous auricular vagal nerve stimulation (taVNS)
might be a mechanism behind the analgesic effects of auricular acupuncture. Brain Stim
2017;10:1042-1044.
Manuskript 2:
Janner H, Klausenitz C, Gürtler N, Hahnenkamp K, Usichenko TI. Effects of Electrical
Transcutaneous Vagus Nerve Stimulation on the Perceived Intensity of Repetitive Painful
Heat Stimuli: A Blinded Placebo- and Sham-Controlled Randomized Crossover Investigation.
Anesth Anal 2018; 126:2085-2092.
Manuskript 3:
Klausenitz C, Hacker H, Hesse T, Kohlmann T, Endlich K, Hahnenkamp K, Usichenko T.
Auricular Acupuncture for Exam Anxiety in Medical Students-A Randomized Crossover
Investigation. Plos One 2016;11:e0168338 doi:10.1371/journal.pone.0168338.
Manuskript 4:
Wunsch J, Klausenitz C, Janner H, Hesse T, Mustea A, Hahnenkamp K, Petersmann A,
Usichenko T. Auricular acupuncture for treatment of preoperative anxiety in patients
scheduled for ambulatory gynaecological surgery - a prospective controlled investigation with
non-randomised arm. Acupunct Med Forthcoming 2018. doi: 10.1136/acupmed-2017-011456

21
Manuskript 1
Transcutaneous auricular vagal nerve stimulation (taVNS) might be a mechanism
behind the analgesic effects of auricular acupuncture
Taras Usichenko, Henriette Janner (geb. Hacker) & Martin Lotze
Veröffentlicht in Brain Stimulation 2017
TU, HJ und ML konzipierten das Studiendesign, analysierten die Daten. TU erstellte den
ersten Entwurf des Manuskripts. Alle Autoren waren an der Interpretation der Daten und
Revision des Manuskripts beteiligt.

22
Taras Usichenko, Henriette Hacker, Martin Lotze. Transcutaneous auricular vagal nerve
stimulation (taVNS) might be a mechanism behind the analgesic effects of auricular
acupuncture. Brain Stimulation (Volume 10, Issue 6), pp. 1042-1044 © 2017. This manuscript
version is made available under the CC-BY-NC-ND 4.0
license http://creativecommons.org/licenses/by-nc-nd/4.0/. DOI: 10.1016/j.brs.2017.07.013
Article title: Transcutaneous auricular vagal nerve stimulation (taVNS) might be a mechanism
behind the analgesic effects of auricular acupuncture
Authors: Taras Usichenko a, b, Henriette Hacker a, Martin Lotze c
Author affiliations:
a Department of Anesthesiology, University Medicine of Greifswald
b Department of Anesthesia, McMaster University, Hamilton, Canada
c Baltic Imaging Center, University Medicine of Greifswald
Corresponding author:
Taras I. Usichenko, MD, PhD
Department of Anesthesiology, University Medicine of Greifswald
Sauerbruchstrasse, 17475 Greifswald, Germany
Tel.: (49) 3834865893; e-mail: [email protected]
Running title: Auricular acupuncture and vagal nerve stimulation
Key words: auricular acupuncture; cranial nerves; non-invasive vagal nerve stimulation

23
Abstract
Background: Randomized clinical trials (RCT) demonstrated that auricular acupuncture (AA)
is effective in treatment of acute and chronic pain, although the mechanisms behind AA are not
elucidated.
Methods: The data concerning the localization of AA points, which are commonly used to treat
pain, were extracted from the meta-analysis of 17 RCTs and evaluated using the anatomical
map of auricular afferent nerve supply.
Results: Fifteen out of 20 specific AA points, used in the treatment of pain, are situated in areas
innervated mostly by the auricular branch of the vagal nerve (ABVN), whereas sham
stimulation was applied at the helix of the auricle, innervated by cervical nerves.
Conclusion: Considering the clinical data relating to the anatomy of neural pathways and
experimental findings of the mechanisms of transcutaneous auricular vagal nerve stimulation,
the analgesic effects of AA may be explained by stimulation of ABVN.

24
Introduction
Auricular acupuncture (AA) is a complementary medicine technique based on a
hypothesis that the entire human body is represented on the external auricle (1). Randomized
clinical trials (RCTs) have demonstrated that AA (including needling, acupressure and
electrical stimulation of AA points) can reduce opioid requirement during and after surgery as
well as pain intensity in acute and chronic pain conditions when compared to placebo and sham
control procedures (2,3). The mechanisms behind the analgesic effects of AA are not clearly
understood. The theory of AA postulates that the dysfunction of the organs of the human body
causes changes of the respective areas of the external auricle, which can be identified as painful
spots with decreased tissue density/resistance (on palpation) and reduced electrical impedance
of the skin (4,5). Stimulation of these areas, connected to an organ with “pathology” is believed
to improve the function of the organ or relieve the concomitant pain (1). Thus AA is based
rather on the theory of reflexotherapy than on the Chinese system of energy circulation along
the meridians, however no neuroanatomical pathways are known to connect the “diseased”
body organs with the external auricle and explain the analgesic effects of AA (1). In order to
clarify the potential mechanism of AA, we aimed to evaluate the localization of AA points,
which are commonly used to treat patients with acute and chronic pain with regard to
contemporary knowledge on neuroanatomy of the external auricle.
Methods
This was a re-analysis of the data from the systematic review of Asher et al. (3). This
investigation analyzed 17 RCTs on the effectiveness of AA in treatment of patients with acute
and chronic pain and remains the most comprehensive source of original research with
sufficient methodological quality on this research topic (6).
The data about the localization of AA points, which are commonly used to treat pain, were
extracted from the main Table 1 and the papers included in the meta-analysis of Asher et al.
(3). The choice of specific AA points was based on empirical recommendations, described in

25
detail in each RCT included in the meta-analysis. The choice of the areas for control procedures
(AA at non-acupuncture points – sham acupuncture) was recommended after methodological
investigation by an expert team (7). All specific AA as well as the sham points were plotted
over a schematic drawing of the pinna with an anatomical map of the auricular nerve supply
(Figure 1A & B). The data on the afferent nerve supply of the external auricle were taken from
the original investigation of Peuker and Filler, 2002, who traced the complete course of
auricular innervation using classical anatomic dissection of human cadavers under magnifying
glasses and dyeing of nerves (8).
Results and Discussion
Fifteen out of 20 AA points, which were used for treatment of pain in 17 RCTs, are
situated in the areas innervated by cranial nerves exclusively or receiving mixed innervation by
the auricular branch of the vagal nerve (ABVN) and cervical nerves (Table 1, Figure 1). The
AA points that were most frequently chosen to treat pain – Nr. 1 (Shenmen), Nr. 2 (Lung) and
Nr. 3 (Thalamus) - are located in the area of afferent mixed innervation of ABVN and cervical
nerves (Table 1, Figure 1). Whereas the specific AA points are situated in areas innervated by
cranial nerves only and in the areas of mixed innervation of ABVN and cervical nerves, sham
stimulation was mostly applied at the helix and lobulus of the auricle, innervated by cervical
nerves (Figure 1B).
The AVBN provides the cutaneous afferent innervation of the external acoustic meatus
and cymba conchae, whereas the peripheral regions of the auricle – helix and scapha are
innervated by the cervical nerves (8). According to Peuker and Filler (2002) the cavity of
conchae is supplied by ABVN in 45% of cases and by ABVN and the great auricular nerve
(GAN) in 55% (7). The afferent fibers of ABVN terminate in the brain stem nuclei of vagal and
trigeminal nerves, including mainly the ipsilateral nucleus solitarius, principal sensory and
spinal trigeminal nuclei (9).
Stimulation of the ABVN, but not cervical nerves of the external auricle, elicits

26
cardiovascular responses, which could be abolished using the antagonist of muscarinic
acetylcholine receptor atropine in experimental rodent investigation (10). Experimental human
investigations demonstrated anti-nociceptive effects of ABVN stimulation on experimentally
evoked pain in healthy volunteers and in patients with chronic pelvic pain (11-13). The
functional magnetic resonance imaging (fMRI) investigations on the mechanism of ABVN
stimulation in healthy volunteers confirmed the involvement of the neurons of the solitary tract
and the locus coeruleus in the brain stem (14,15). Moreover, decreases in fMRI signal in limbic
structures were demonstrated, including the amygdala, hippocampus, parahippocampal gyrus
and the cingulate cortex, suggesting that ABVN stimulation is targeting the regulation of
emotional and autonomic components in cerebral processing of pain (16,17).
On the other hand, transcutaneous electrical stimulation of the auricular branch of the
vagal nerve (ABVN), known as transcutaneous auricular vagal nerve stimulation (taVNS), is
being increasingly used as a non-invasive method for treatment of neurologic and psychiatric
disorders (18) but the clinical evidence of taVNS, based on few RCTs, is still too modest to
make any recommendations for clinical practice (19).
Conclusion
Almost all empirically described specific AA points, which were used in randomized
clinical trials to treat patients with acute and chronic pain, are situated in areas of the external
auricle that principally receive afferent innervation from cranial nerves. Regarding the clinical
data in connection with the anatomy of neural pathways of the external auricle and experimental
findings about the mechanisms of taVNS, we conclude that the analgesic effects of auricular
acupuncture can be explained by stimulation of ABVN.
Acknowledgement

27
We thank Dr. Mike Cummings for his critical comments and language editing of the
manuscript.

28
References
1. Usichenko T, Anders E. Auricular acupuncture. In: Filshie, White, Cummings (editors).
Medical Acupuncture: A Western Scientific Approach, 2nd edition, 2016 Elsevier.
2. Murakami M, Fox L, Dijkers MP. Ear Acupuncture for Immediate Pain Relief-A
Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Med
2017;18:551-64.
3. Asher GN, Jonas DE, Coeytaux RR, Reilly AC, Loh YL, Motsinger-Reif AA et al.
Auriculotherapy for pain management: a systematic review and meta-analysis of
randomized controlled trials. J Altern Complement Med 2010;16:1097-108.
4. Oleson TD, Kroening RJ, Bresler DE. An experimental evaluation of auricular
diagnosis: the somatotopic mapping or musculoskeletal pain at ear acupuncture points.
Pain 1980;8:217-29.
5. Saku K, Mukaino Y, Ying H, Arakawa K. Characteristics of reactive electropermeable
points on the auricles of coronary heart disease patients. Clin Cardiol 1993;16:415-9.
6. Asher GN, Motsinger-Reif AA, Jonas DE, Viera AJ. Quality of reporting on
randomised controlled trials of auriculotherapy for pain. Acupunct Med 2011;29:122-6.
7. Margolin A, Avants SK, Chang P, Birch S, Kosten TR. A single-blind investigation of
four auricular needle puncture configurations. Am J Chin Med 1995;23:105-14.
8. Peuker ET, Filler TJ. Nerve supply of the human auricle Clin Anat 2002;15:35-7.
9. Nomura S, Mizuno N. Central distribution of primary afferent fibers in the Arnold's
nerve (the auricular branch of the vagus nerve): a transganglionic HRP study in the cat.
Brain Res 1984; 292: 199-205.
10. Gao XY, Li YH, Liu K, Rong PJ, Ben H, Li L et al. Acupuncture-like stimulation at
auricular point Heart evokes cardiovascular inhibition via activating the cardiac-related
neurons in the nucleus tractus solitarius. Brain Res 2011;1397:19-27.
11. Busch V, Zeman F, Heckel A, Menne F, Ellrich J, Eichhammer P. The effect of
transcutaneous vagus nerve stimulation on pain perception - An experimental study.

29
Brain Stimul 2013;6:202-9.
12. Frøkjaer JB, Bergmann S, Brock C, Madzak A, Farmer AD, Ellrich J, Drewes AM.
Modulation of vagal tone enhances gastroduodenal motility and reduces somatic pain
sensitivity. Neurogastroenterol Motil 2016;28:592-8.
13. Napadow V, Edwards RR, Cahalan CM, Mensing G, Greenbaum S, Valovska A et al.
Evoked pain analgesia in chronic pelvic pain patients using respiratory-gated auricular
vagal afferent nerve stimulation. Pain Med 2012;13:777-89.
14. Dietrich S, Smith J, Scherzinger C, Hofmann-Preiss K, Freitag T, Eisenkolb A et al. A
novel transcutaneous vagus nerve stimulation leads to brainstem and cerebral
activations measured by functional MRI. Biomed Tech (Berl) 2008;53:104-11.
15. Frangos E, Ellrich J, Komisaruk BR. Non-invasive Access to the Vagus Nerve Central
Projections via Electrical Stimulation of the External Ear: fMRI Evidence in Humans.
Brain Stimul 2015;8:624-36.
16. Kraus T, Kiess O, Hösl K, Terekhin P, Kornhuber J, Forster C. CNS BOLD fMRI
effects of sham-controlled transcutaneous electrical nerve stimulation in the left outer
auditory canal - a pilot study. Brain Stimul 2013;6:798-804.
17. Usichenko T, Laqua R, Leutzow B, Lotze M. Preliminary findings of cerebral responses
on transcutaneous vagal nerve stimulation on experimental heat pain. Brain Imaging
Behav 2017;11:30-7.
18. Straube A, Ellrich J, Eren O, Blum B, Ruscheweyh R. Treatment of chronic migraine
with transcutaneous stimulation of the auricular branch of the vagal nerve (auricular t-
VNS): a randomized, monocentric clinical trial. J Headache Pain 2015;16:543.
19. Carreno FR, Frazer A. The Allure of Transcutaneous Vagus Nerve Stimulation as a
Novel Therapeutic Modality. Biol Psychiatry 2016;79:260-1.

30
Legend to figure
Figure 1.
A: Auricular acupuncture (AA) points, used for treatment of patients with acute and chronic
pain in randomized controlled trials (RCTs) included into meta-analysis of Asher et al 2010
(reference 3). Black circles with numbers: various specific AA, the nomenclature is given in
Table 1; triangles: non-acupuncture points for sham acupuncture on the helix of the auricle as
a control condition in several RCTs from the meta-analysis.
B: Anatomic map of afferent nerve supply according to Peuker and Filler, 2002 (reference 7),
where cymba conchae is exclusively supplied by the auricular branch of the vagal nerve
(ABVN); cavity of conchae is exclusively supplied by ABVN in 45% of cases and by ABVN
and the great auricular nerve (GAN) from the cervical plexus in 55%; tail of helix is exclusively
supplied GAN; antihelix is exclusively supplied by ABVN in 73%, exclusively supplied by
GAN in 18%, and supplied by ABVN and GAN in 9%; the crura of antihelix are supplied by
GAN in 91% and ABVN in only 9%. ATN: auriculotemporal nerve (from trigeminal nerve).

31
Manuskript 2
Effects of Electrical Transcutaneous Vagus Nerve Stimulation on the Perceived
Intensity of Repetitive Painful Heat Stimuli: A Blinded Placebo- and Sham-
Controlled Randomized Crossover Investigation
Henriette Janner (geb. Hacker), Catharina Klausenitz, Nancy Gürtler, Klaus Hahnenkamp
& Taras Usichenko
Veröffentlicht in Anesthesia and Analgesia 2018
HJ, CK, KH und TU konzipierten das Studiendesign. HJ und NG erhoben die Daten. HJ
analysierte die Daten und erstellte den ersten Entwurf des Manuskripts. Alle Autoren waren an
der Interpretation der Daten und Revision des Manuskripts beteiligt.

'RZ
QORDGHGIURP
KWWSV���MRXUQDOV�OZZ�FRP
�DQHVWKHVLD�DQDOJHVLDE\
%K'0I�H3+
.DY�](RXP�W4
I1�D�N-/K(=JEV,+
R�;0L�K&
\Z&;�$:
Q<4S�,O4
U+'�-P
O�*+,NEZ
]��'L�(1
J.PSD8
I�4Q\[(1
DH�S*OV'
�%� RQ
����������
'RZQORDGHGIURPKWWSV���MRXUQDOV�OZZ�FRP�DQHVWKHVLD�DQDOJHVLDE\%K'0I�H3+.DY�](RXP�W4I1�D�N-/K(=JEV,+R�;0L�K&\Z&;�$:Q<4S�,O4U+'�-PO�*+,NEZ]��'L�(1J.PSD8I�4Q\[(1DH�S*OV'�%� RQ����������
Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.June 2018 • Volume 126 • Number 6 www.anesthesia-analgesia.org 2085
DOI: 10.1213/ANE.0000000000002820
Clinical data suggest that electrical and acupuncture stimulation of certain areas on the external auricle can diminish acute and chronic pain.1–4 Moreover, several
experimental studies have shown increased pain thresholds during electrical stimulation applied to auricular (acupunc-ture) points situated at the concha, triangular fossa, and anti-tragus in comparison with stimulation at the helix and scapha of the auricle.5–9 It has been assumed that these hypoalgesic effects are based on a transcutaneous stimulation of cranial nerves, especially the vagus nerve,5,10,11 whose auricular affer-ent branches supply the external acoustic meatus and auricu-lar conchae.12 These afferents terminate in cerebral structures as the nucleus tractus solitarii and the locus coeruleus in the brainstem that are known to be involved in the transmission and processing of nociceptive stimulation.13–15 Moreover, pro-jections of the solitary tract and locus coeruleus also reach the ventromedial medulla, periaqueductal gray, hypothalamus, and limbic forebrain, regions that are involved in the modu-lation of arousal and pain perception.11,16
Noninvasive electrical transcutaneous vagus nerve stimulation (TVNS) has been shown to be a promising
KEY POINTS• Question: Does transcutaneous vagus nerve stimulation (TVNS) reduce the perceived inten-
sity of repetitive painful heat stimuli and temporal summation of pain processes?• Findings: Pain intensity but not temporal summation of pain decreased during TVNS, as well
as control interventions, and TVNS exerted differential effects in men and women at certain time points.
• Meaning: TVNS was indistinguishable from sham and placebo in the reduction of experimental heat pain and suggested that gender effects should be verified in appropriate investigations.
BACKGROUND: Transcutaneous vagus nerve stimulation (TVNS) is a promising treatment for acute and chronic pain. However, experimental studies yielded controversial results. We exam-ined if TVNS reduces the perceived intensity of repetitive painful heat stimulation and temporal summation of pain (TSP) in healthy volunteers in comparison with placebo and sham stimula-tion, as well as no intervention.METHODS: In 4 sessions, 90 heat pulse stimuli at individual pain tolerance temperature were applied to the ventral forearm of 49 healthy volunteers (25 women) using a Contact Heat Evoked Potential Stimulator thermode (Medoc, Ramat Yishai, Israel). Pain intensity was assessed with verbal ratings on a numeric pain scale (0–100) at every tenth heat pulse. After the first session in which pain intensities without intervention were evaluated, participants completed 3 sessions in a single-blinded randomized crossover manner: (1) sham stimulation applied at the earlobes, (2) placebo stimulation (inactive device), or (3) TVNS applied at the cymbas conchae. Primary data were analyzed using analysis of variance for repeated measures and t test for paired samples.RESULTS: Pain intensity decreased during all interventions as compared to no intervention (ηp
2 = 0.22, P < .001; mean difference TVNS versus no intervention 9.5; 95% confidence interval [CI], 3.6–15.4; P < .001). Hypoalgesic effect of TVNS was better than that of placebo and sham in men before the onset of TSP (mean differences for TVNS versus placebo 6.2; 95% CI, 0.2–12.1; TVNS versus sham 6.2; 95% CI, 0.2–12.1; P < .05). In women, TSP response under TVNS was decreased if compared to no intervention (median difference, 7.5; 95% CI, 3.5–15.0; P = .003).CONCLUSIONS: TVNS, placebo, and sham stimulation exerted comparable effects under experi-mental heat pain stimulation. Only in male participants, TVNS was superior to sham and placebo conditions in the reduction of heat pain before the onset of TSP. (Anesth Analg 2018;126:2085–92)
Effects of Electrical Transcutaneous Vagus Nerve Stimulation on the Perceived Intensity of Repetitive Painful Heat Stimuli: A Blinded Placebo- and Sham-Controlled Randomized Crossover InvestigationHenriette Janner, MSc,* Catharina Klausenitz, MD,† Nancy Gürtler, BSc,* Klaus Hahnenkamp, MD, PhD,* and Taras I. Usichenko, MD, PhD*‡
From the *Department of Anesthesiology and †Institute of Diagnostic Radiology and Neuroradiology, University Medicine of Greifswald, Greifswald, Germany; and ‡Department of Anesthesia, McMaster University, Hamilton, Ontario, Canada.Accepted for publication December 13, 2017.Funding: This research has only been funded by resources of the Department of Anesthesiology of the University Medicine Greifswald and did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.The authors declare no conflicts of interest.Reprints will not be available from the authors.Address correspondence to Henriette Janner, MSc, Department of Anes-thesiology and Intensive Care Medicine, University Medicine of Greif-swald, Sauerbruchstrasse, 17475 Greifswald, Germany. Address e-mail to [email protected] © 2018 International Anesthesia Research Society
Chronic Pain MedicineSection Editor: Honorio T. Benzon

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.2086 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Transcutaneous Vagus Nerve Stimulation and Heat Pain
auricular stimulation treatment for acute and chronic pain conditions3,10,17; however, some experimental and clinical studies examining the pain-reducing effects of electrical auricular stimulation yielded controversial results.5,6,11,18,19 Furthermore, changes of experimental pain thresholds associated with auricular stimulation do not provide an explanatory model for the impact of auricular stimula-tion techniques on chronic pain conditions. Therefore, the examination of changes in pain perceptions over time using repetitive painful stimulation seems a more appropriate and convenient experimental method for this purpose.20 Repetitive noxious stimulation can lead to an increase of the perceived intensity of painful stimuli in humans, a phenomenon known as temporal summation of pain (TSP).21–25 TSP is suggested as a sensitive experi-mental human pain model for the measurement of mod-erate analgesic effects of nonopioid analgesic drugs or hypoalgesic neuromodulation.20 Moreover, it is claimed to be a perceptual correlate of (experimentally induced) central sensitization processes21,22,25–27 that are thought to play a crucial role in the development of chronic pain disorders.22,24,25
To find further evidence and understanding for hypo-algesic effects of electrical auricular stimulation in an experimental setting, we examined the impact of TVNS on perceived pain intensity and TSP in comparison with a pla-cebo and sham stimulation, as well as no intervention using a modified experimental heat stimulation protocol based on previously established methods.28 We expected TVNS to decrease the perceived intensity of painful stimulation and reduce TSP processes in comparison with no intervention and sham and placebo stimulation.
METHODSDesign of the Investigation and Participants’ Selection CriteriaThe local Institutional Review Board of the University Medicine of Greifswald approved the study protocol (No: BB 083/15), and written informed consent was obtained from each participant. The article adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
The prospective, single-blinded, crossover, placebo- and sham-controlled experimental investigation was performed in a laboratory room of the Department of Anesthesiology of the University Hospital Greifswald from July to December 2015. Fifty-one participants were recruited via an Internet announcement according to the following eligibility criteria: healthy volunteers (no physical or psychological disorders), ages 18–45 years, American Society of Anesthesiologists physical status score of I or II, no abnormal skin conditions (infection, scars, psoriasis, eczema) at the sites of stimula-tions, abstinence from analgesics (including over-the-coun-ter medications) or psychoactive substances for at least 3 days, and abstinence from caffeine for at least 3 hours before each visit. The subjects were paid for their participation.
The study consisted of 4 sessions, with an intersession interval of at least 48 hours to prevent carry-over effects. Each session lasted about 50 minutes and was performed at the same time of day.
In the first session, volunteers were acquainted to the environment, equipment, and study procedure to minimize the influence of fear or surprise on study outcomes. During the first visit, participants were informed about the study procedure. Subjects were told that the aim of the study was to test the influence of 3 different auricular stimula-tion methods on the perception of painful heat stimuli to blind them regarding the existence of an active treatment or placebo and sham condition. The investigator performing the stimulation procedures was aware of the allocation of conditions.
All participants signed the informed consent and completed the State-Trait-Anxiety-Inventory (STAI).29 Afterward, the heat stimulation procedure, described below, was performed without any auricular stimulation.
Thereafter, each subject participated in 3 randomly ordered sessions in a crossover manner, including TVNS, placebo, or sham stimulation (Figure 1). For randomiza-tion, the stimulation sides (left and right) and interven-tional conditions (TVNS, placebo, and sham) were coded with numbers. Random sequences of these numbers were created for each participant using an online random num-ber generator.30 Thus, 6 different sequences of 3 study
Heat-stimulation
(no intervention)
Heat-stimulation +
Placebo
Heat-stimulation +
TVNS
Heat-stimulation +
Sham
Assessed for eligibility (N = 51)
Final Analysis(N = 49 )
For each participant in randomized order
Discontinuedparticipation (n=1)
Session 1 Session 3Session 2 Session 4
Discontinuedparticipation (n=1)
Excluded from analysis due to
incomplete data sets
Figure 1. Flow of the study. Each par-ticipant underwent painful heat stimula-tion procedure without intervention (no intervention, session 1) and in random-ized order with transcutaneous vagus nerve stimulation (TVNS) at the cymbas conchae, placebo (inactive stimulation device), and sham stimulation (electri-cal stimulation at the earlobes) in a crossover manner (sessions 2–4).

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
June 2018 • Volume 126 • Number 6 www.anesthesia-analgesia.org 2087
interventions, which followed the first session with no intervention, were created.
Heat Stimulation ProcedureHeat stimulation was applied using a “Contact Heat Evoked Potential Stimulator” (Medoc Advanced Medical Systems, Ramat Yishai, Israel), described elsewhere in detail.11 The thermode was placed in a randomized order on the left or right ventral forearm, 45 mm below the elbow crease, and was fixed with a blood pressure cuff of 10 cm width, manually inflated to a pressure of 40 mm Hg, to enable a standardized pressure at the stimulated site throughout the investigation.
For determination of the individual stimulation tempera-ture, the contact surface of the thermode was automatically heated with a rate of 1°C/s from a baseline temperature (32°C) until participants determined their pain tolerance temperature (the temperature at which they felt intolerable pain) by pressing the button of a response unit that imme-diately cooled down the contact surface. Pain tolerances were measured with 6 trials with an interval of 3 seconds in between. The mean temperature of the last 5 trials was used as a maximum stimulation temperature for the further investigation. The first pain tolerance value was excluded due to influences of novelty and fear.31
Afterward, the stimulation side was changed to the alter-nate ventral forearm, and the thermode was fixed again as described above. Then repetitive heat pulses with a fre-quency of 0.4 Hz were applied. Within 8 pulses at the begin-ning, the pulse temperature was gently raised until the peak temperature was reached to mimic the rising skin tempera-ture seen during repetitive contacts with a preheated probe in previous studies.24 Subjects were stimulated with 90 brief heat stimuli of their individual pain tolerance temperature. For each pulse, the temperature was increased with a rate of 20°C/s from a baseline temperature (38°C), held for 800 mil-liseconds at the peak temperature, and then returned to the baseline temperature with a cooling rate of 40°C/s.
The stimulation and acquisition parameters were chosen according to methodology of previous investigations21,23,24 and our methodological investigation,28 whereas repetitive heat stimulation is the most commonly used and validated model to elicit the TSP phenomenon in humans.25
Intervention ProcedureAuricular electrical stimulation was applied bilaterally using self-manufactured electrodes, described elsewhere in detail,32 that were connected to a transcutaneous electri-cal nerve stimulation device PuntoBravo (Medizintechnik Rostock GmbH, Rostock, Germany). The electrodes’ con-tact surfaces, wrapped in wool, were moistened with 0.9% sodium chloride solution before each stimulation proce-dure, and the stimulation site was cleaned with alcohol to achieve optimal conductivity.
TVNS was applied at the cymbas conchae (Figure 2A) using electrical square impulses delivered in blocks of 9 impulses with a frequency of 100 Hz and a pulse width of 200 μseconds emitted twice per second, resulting in mixed frequency pattern of 100 Hz/2 Hz that was shown to elicit maximal analgesic effects and minimal habituation to elec-trical stimulation in animal and clinical studies.6,9,33 Current intensity was individually adjusted for each ear separately until participants described it as “clearly perceptible tin-gling sensation that was not uncomfortable or painful.”11 The electrodes were fixed using commercially available antinoise earplugs made of polyurethane foam, mull pads, adhesive tape, and an elastic headband to ensure a consis-tent contact of the electrodes with the skin.
For sham stimulation, the electrodes were attached with adhesive tape to the earlobes (Figure 2A) that receive affer-ent supply from cervical nerves,12 and the stimulation proce-dure was performed with the same parameters as described for the TVNS condition.
For the placebo condition, electrodes were attached at the cymbas conchae (Figure 2A), as described for the TVNS condition. The participants were told to choose a
Figure 2. A, Sites of bilateral auricular stimulations. Transcutaneous vagus nerve stimulation (TVNS): mixed frequency pattern of 100 Hz/2 Hz, duration: 25 min; placebo: inactive stimulation device declared as current intensity under perception threshold (duration: 25 min); sham: electrical stimulation at the earlobes (mixed frequency pattern of 100 Hz/2 Hz, duration: 25 min). B, Changes in pain intensity ratings in dif-ferent conditions. x-axis indicates number of heat stimuli (above) over time in seconds. No intervention: without any intervention ***P < .001, interventional conditions versus no intervention; main effect analysis of variance.

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.2088 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Transcutaneous Vagus Nerve Stimulation and Heat Pain
current intensity that was “directly under their perception threshold.” Once the current intensity was adjusted, the device was switched off without participants’ knowledge. During the adjustment of current intensity, impulses with a pulse width of 175 μseconds were applied with a fre-quency of 10 Hz.
Auricular stimulation was started 20 minutes before the repetitive heat stimulation procedure (Figure 3). Meanwhile, the participants sat comfortably in an armchair and were asked to solve conventional cognitive tasks that included questions of reasoning, numerical series, and common knowledge in the style of the German Intelligence-Structure-Test 2000 R34 to standardize participants’ behavioral states during the interventions as much as possible. The partici-pants were assured that these tasks were a method for stan-dardization of activity, and results were not the object of further investigation.
The auricular stimulation was continued during the repetitive painful heat stimulation and was terminated directly afterward (Figure 3). The total time of auricular stimulation was approximately 25 minutes.
Outcome MeasuresThe intensity of pain, reported by the participants during the repetitive heat pain stimulation, was the primary out-come measure. The subjects were asked to verbally rate the perceived intensity of pain at the first and every tenth heat stimulus, with pain tolerance temperature on a numeric pain scale ranging from 0 = no sensation to 100 = intoler-able pain, which was used and described in previous stud-ies.21,24,25,28 Every rating was immediately transcribed to a computer by the investigator, resulting in total number of 10 ratings per subject and session. TSP was calculated as the difference between the last and lowest pain intensity rating for each participant and condition.
As a secondary outcome measure, the STAI in German29 was assessed before the first session. At the beginning of each subsequent session, participants completed the state form of the STAI to quantify situational anxiety as a pos-sible confounding factor influencing the evaluation of pain-ful stimuli. Furthermore, heart rate and blood pressure were measured noninvasively using a SC 7000 patient monitor (Siemens Healthcare GmbH, Erlangen, Germany) at the beginning of each session (time point I) after completing the STAI, as well as before (time point II) and after (time point III) the repetitive painful heat stimulation (Figure 3).
After each interventional session, subjects were asked if the auricular stimulation had influenced their pain percep-tion and in what way. To test the quality of blinding, after
the last session, participants were asked which stimulation technique was most effective in influencing their pain per-ception and whether they realized that the auricular stimu-lation device was switched off during the placebo session.
Statistical AnalysisTo test our hypothesis that TVNS decreases perceived pain intensity in comparison with no intervention, placebo stim-ulation, and sham stimulation, at first 2 separate repeated measures analysis of variance (ANOVA) were performed to detect possible systematic differences among the conditions regarding pain tolerance temperature and STAI scores that could have influenced the primary outcome because the session with no intervention was not included in the ran-domization process. Afterward, primary outcome measures were analyzed using repeated measures ANOVA, with the within factors condition with 4 levels (no intervention, pla-cebo, TVNS, sham) and time with 10 levels (pain ratings), as well as the between-subject factors gender with 2 lev-els (men, women) and order with 6 levels (orders of inter-ventional applications). The gender and order levels were included to account for possible differences in perception/processing of pain between genders35 and to test for a differ-ential carry-over effect due to the nonrandomized session with no intervention. In the case of a significant interaction with a between-subject factor, subgroup analyses were per-formed. Mean ratings at certain time points of the condi-tions were compared using paired sample t test, and mean differences with 95% confidence intervals (CIs) were given as treatment effect estimates.
To test the hypothesis that TVNS reduces TSP response in comparison with no intervention, placebo stimulation, and sham stimulation, TSP responses were quantified as the difference between the last pain rating and the low-est pain rating for each individual and condition. Within a subgroup, skewed TSP responses of each condition were then compared with the Wilcoxon signed rank test, and the median of differences with 95% CIs were given as treatment effect estimates.
Data are presented as mean ± standard deviation unless otherwise stated. Two-sided P values are reported. P values of multiple pairwise comparisons in the subgroup analysis were corrected using the Holm-Bonferroni method. Data analysis was performed using the Statistical Package for the Social Sciences, Version 22.0 (SPSS, IBM Corporation, New York, NY).
Sample size calculation was performed using the pro-gram G*power 3.136 for ANOVA for repeated measures with the within factors condition (4 levels) and time (10 levels),
Heat-stimulatio n
TVNS / Placebo / Sham
10 min 2 0 min 4 min(I) (II) (III)
Start End
Figure 3. Flow of 1 study session with auricular stimulation in minutes. Assessment of State-Trait-Anxiety-Inventory at time point (I) and heart rate and blood pressure at time points (I)–(III). Rating of perceived pain intensities at the first and every tenth heat pulse during heat stimula-tion. Placebo indicates inactive device declared as under perception threshold stimulation at cymba conchae; sham: electrical stimulation at earlobes; TVNS, transcutaneous vagus nerve stimulation at cymba conchae.

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
June 2018 • Volume 126 • Number 6 www.anesthesia-analgesia.org 2089
with a 2-sided level of significance of 5%, a power of 90%, and an estimated population effect size of f = 0.1, resulting in a suggested sample size of 44 subjects. Expecting a drop-out rate of 15%, the sample size was set to 51 participants.
RESULTSFifty-one participants were enrolled in the study. One woman refused to participate during the third session (pla-cebo condition) because of painful pressure in the ears after fixation of the electrodes. One male volunteer could not complete the third and fourth sessions due to a sport injury of his right arm. The data of 49 subjects (25 women), ages 24.8 ± 3.3 years, all Caucasians, were included for final anal-ysis (Table 1). Individual pain tolerance temperatures and STAI scores were comparable among the study conditions.
All interventional conditions reduced pain intensity in comparison with no intervention (main effect for condition
with F3,111 = 10.7; P < .001; ηp2 = 0.22), whereas Bonferroni-
adjusted pairwise comparisons showed comparable hypo-algesic effects, if compared to no intervention, for TVNS (mean difference 9.5; 95% CI, 3.6–15.4; P < .001), placebo (mean difference 9.1; 95% CI, 3.3–14.9; P = .001), and sham condition (mean difference 10.1; 95% CI, 4.3–16.0; P < .001). After an initial decrease of pain intensity (from the beginning of stimulation to approximately 93 seconds) (Figure 2B), the participants reacted with an increase of pain intensity (temporal summation [TSP]; main effect for factor time with F2.7100 = 20.8; P < .001; ηp
2= 0.36) during all 4 condi-tions. There was no effect of order on the primary outcome. Possible differences in responses between male and female subjects were indicated by small interaction effects of time and gender (F2.7100 = 5.3; P = .003; ηp
2 = 0.13) and condition and gender (F3,111 = 2.9; P = .04; ηp
2 = 0.07). Therefore, fur-ther subgroup analyses for male and female subjects were performed.
In male participants, pain intensity during TVNS at pulse 20 (after 70 seconds) was lower than during no intervention (mean difference 8.9; 95% CI, 0.5–17.2; t23 = 2.2; P = .039) and sham intervention (mean difference 5.2; 95% CI, 1.4–9.0; t23 = 2.8; P = .02). At pulse 30 (after 95 seconds), pain inten-sity under TVNS was lower in comparison with no inter-vention (mean difference 10.7; 95% CI, 3.1–18.3; t23 = 2.9; P = .024) and sham (mean difference 6.2; 95% CI, 1.8–10.5; t23 = 2.9; P = .027), as well as placebo condition (mean differ-ence 6.2; 95% CI, 0.2–12.1; t23 = 2.2; P = .04) (Figure 4). Other pain ratings under TVNS, sham stimulation, and placebo stimulation were comparable. In women, pain intensities under TVNS, placebo stimulation, and no intervention were also comparable.
Table 1. Study Subjects’ Characteristicsa
Total
(N = 49)Women (n = 25)
Men (n = 24)
Age (y) 24.8 ± 3.3 23.0 ± 3.1 26.6 ± 2.4Time between sessions (d) 7.1 ± 4.8 6.4 ± 4.0 7.9 ± 5.6STAI scoresb
Trait 36.1 ± 7.8 36.4 ± 8.1 35.8 ± 7.6 State 33.8 ± 4.6 34.1 ± 4.4 33.4 ± 4.9Pain tolerance temperature (°C) 47.1 ± 1.3 46.7 ± 1.5 47.5 ± 1.0Current intensity (mA) Left ear 6.8 ± 1.3 6.3 ± 1.1 7.2 ± 1.4 Right ear 8.3 ± 3.9 8.1 ± 3.5 8.5 ± 4.2
Abbreviation: STAI, State-Trait-Anxiety-Inventory.aData are presented as mean ± SD.bSTAI ranges from 20 to 80 points and quantifies anxiety as a state in a specific situation and as a general personal trait.
35
40
45
50
55
60
65
70
75TVNS Sham
Number of Heat Stimuli ov er Time in Seconds
Pain
Inte
nsity
(0-1
00)
35
40
45
50
55
60
65
70
75 Baseline Placebo
PainIntensity
(0-100)
Males
0 0
Females
*
22 95 170 245
9080706050403020101908070605040302010
Number of Heat Stimuli ov er Time in Seconds22 95 170 245
1
No Interv ention
A B
Figure 4. Changes in pain intensity ratings in different conditions for the male (A) and female (B) subgroups. x-axis indicates number of heat stimuli (above) over time in seconds. No intervention: without any intervention; transcutaneous vagus nerve stimulation (TVNS): with TVNS; sham: with electrical stimulation at the earlobes; placebo: with inactive stimulation device. *P < .05, Student t test revealed significantly reduced pain ratings at pulse 30 under TVNS compared with no intervention, placebo, and sham condition in the male but not in the female subgroup.

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.2090 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Transcutaneous Vagus Nerve Stimulation and Heat Pain
TSP responses were comparable among study condi-tions in male participants. In contrast, in women, TSP was decreased under TVNS (median difference = 7.5; 95% CI, 3.5–15.0; Z = 3.18; P = .003) and placebo condition (median difference = 8.0; 95% CI, 2.5–16.5; Z = 2.7; P = .012) (Table 2) in comparison with no intervention. However, no signifi-cant differences in TSP between TVNS, placebo, and sham condition were found.
Hemodynamic parameters were comparable among all conditions. No correlations between state or trait anxiety and TSP were found. None of the participants was aware that the device had been inactive in the placebo condi-tion, and there were no differences among the participants regarding their beliefs about the most effective intervention (χ2 = 3.6; P = .17), which indicates a successful blinding.
DISCUSSIONIn this randomized controlled single-blinded prospective crossover investigation, the effects of TVNS on the percep-tion of repetitive painful heat stimuli in comparison with no intervention, placebo stimulation, and sham stimulation were examined. TVNS and sham and placebo stimulation reduced the perceived intensity of the repetitive pain-ful stimulation about 15% if compared to no intervention. Busch et al5 also found reductions in pain ratings during the application of tonic heat for 5 minutes under TVNS and under sham stimulation if compared to baseline responses; in contrast, only the reduction under TVNS was signifi-cant in comparison with baseline (about 25%) and sham stimulation.
The pattern of pain intensity changes was similar in all conditions: after an initial decrease of pain, which is in line with findings of habituation of (first pain) experiences after repetitive stimulation,37 pain reincreased with a rising num-ber of applied heat stimuli. This increase indicates temporal summation processes that could be interpreted as an experi-mentally induced form of central sensitization.22–25,38
Furthermore, our results raise questions about possible differences in the impact of auricular stimulation in male and female subjects. In the male subgroup, TVNS was found to be more effective than placebo and sham stimula-tion, with a reduction of about 20% in perceived pain inten-sity compared to no intervention before the beginning of the
TSP. In women, no such difference was revealed, and the greatest pain-reducing effects were found under sham con-dition at all time points (Figure 4). However, TVNS reduced the TSP response substantially if compared to no interven-tion in female subjects.
Nahman-Averbuch et al39 demonstrated that higher para-sympathic activity was associated with higher efficiency of pain modulation in male but not in female subjects. The authors concluded that pain treatments that affect para-sympathetic activity (eg, via stimulation of the vagus nerve) may be more effective in male than in female subjects.39 Our findings could support this hypothesis. However, to the best of our knowledge, sex differences regarding the impact of TVNS on pain processing/modulation were not system-atically examined or discussed in previous studies.5,6,11,18
The interpretation of the data is limited due to several reasons: (1) our study was not a priori designed to detect gender differences in responses, and statistical analyses regarding these differences are underpowered; (2) the ses-sion without intervention was not randomized like the sub-sequent conditions; (3) despite the absence of the order effect on primary outcome, a potential differential carry-over effect cannot be completely excluded because the statistical analysis for this purpose was underpowered. Furthermore, even if the results of the STAI as a measurement instrument of situational anxiety did not indicate differences between anxiety levels among the conditions, influences of novelty or other confounding factors on the ratings of pain inten-sity cannot be entirely excluded. However, in contrast to the findings of Granot et al,21 neither state nor trait anxiety was associated with TSP responses in our study; (4) the fixation of electrodes for placebo condition exerted a mechanical pressure, which could have stimulated vagal nerve endings. Therefore, the substantial effects found in this condition may not only be based on a placebo effect. It would explain why perceived pain intensity was reduced during placebo condition without the clearly perceptible electrical stimula-tion, as in the TVNS and sham condition, which could have served as a distraction from the painful stimulation. Thus, our placebo condition might not have been a valid method for comparison that allows clear conclusions. (5) Because some participants reported the impression of their whole ear being electrically stimulated even in the sham condition, the intensity of current applied at the earlobes could have led to widespread neural activation, including cervical and cranial nerves. Regarding these uncertainties, at this point, we can-not differentiate whether or in which amount the reported hypoalgesic effects are based on distraction, expectations/beliefs of effectiveness, or genuine activation of vagal affer-ent fibers. Because the afferent fibers of the auricular branch of the vagal nerve (ABVN) terminate in the nuclei of the soli-tary tract, stimulation applied to ABVN could have led to an activation of the descending pain modulatory circuits.16 Indeed, the ascribed brainstem structures (eg, the nuclei of the solitary tract, which project to locus coeruleus [norad-renergic] and raphe [serotonergic] nuclei) are suggested to be part of the descending pain inhibitory system, exerting their antinociceptive effects through the (1) central release of monoamines, and (2) “top-down” inhibition of nociceptive transmission at the level of the spinal cord.16 The latter mech-anism may explain the expected antinociceptive effect of
Table 2. Temporal Summation of Pain Responses in Each Conditiona
ConditionTotal
(N = 49)Men
(n = 24)Women (n = 25)
No intervention 20 (10–30) 20 (7–27) 25 (10–34)TVNSb 15 (5–30) 15 (5–30) 7 (4–20)c
Placebod 10 (5–20) 15 (5–20) 10 (5–20)e
Shamf 12 (5–25) 15 (9.25–25) 10 (5–25)aTemporal summation of pain, defined as difference between the last and the lowest pain rating on a numeric rating scale (0–100) during repetitive pain stimulation. Data are presented as median (interquartile range).bTVNS: transcutaneous vagus nerve stimulation at cymbas conchae.cP = .003 for comparison of TVNS versus no intervention; Holm-Bonferroni–adjusted Wilcoxon test.dPlacebo: inactive stimulation device.eP = .012 for comparison of placebo versus no intervention; Holm-Bonferroni–adjusted Wilcoxon test.fSham: electrical stimulation at earlobes.

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
June 2018 • Volume 126 • Number 6 www.anesthesia-analgesia.org 2091
TVNS on TSP, which represents a perceptual correlate of the “wind-up” phenomenon (facilitation of neuronal responses in the dorsal horn of the spinal cord under direct repetitive stimulation of afferent unmyelinated C-fibers in experimen-tal animals).22,23,26 Moreover, in patients with chronic pain conditions, where descending pain inhibition may be weak-ened and descending pain facilitation enhanced,16 TVNS might reactivate the pain inhibitory pathways. This sug-gestion is supported by positive results from clinical stud-ies on auricular stimulation in patients with chronic pain and by findings from functional neuroimaging of TVNS effects, where decreased activation in limbic structures and hypothalamus (involved in regulation of emotional and autonomic components in cerebral processing of pain) was demonstrated.11,14,16 Because patients with chronic pain dem-onstrate enhanced TSP in comparison with healthy volun-teers,40 we expect TVNS to exert more pronounced effects in these patients, thus explaining the clinically relevant find-ings of auricular stimulation described previously in clini-cal trials.1–4,17 However, an involuntary stimulation of ABVN endings in sham and placebo conditions might be 1 explana-tion for controversial results in studies examining the pain-reducing effects of electrical auricular.5,6,11,18,19
However, this study also has some clear strengths because it was performed with a crossover design with 2 control conditions, whereas all interventional conditions and stimulation sides were randomized to prevent sys-tematic influences of the application order on primary out-comes. Possible confounding factors such as time of day and caffeine intake were controlled by standardization. Moreover, we used a different, complementing experi-mental heat stimulation paradigm developed to examine changes in perceived pain over time by applying a large number of pulsating heat stimuli, which results in a greater external validity. Because the course of changes in pain rat-ings was stable in all sessions, the method was shown to reliably induce TSP.
In future studies, the pain-reducing effects of TVNS should be examined in comparison with an active sham stimulation applied at the earlobes with lower current inten-sities, which is not likely to produce widespread neural acti-vation. Moreover, because verbal ratings can be biased due to an interaction with the investigator, subjects should rate their perceived pain on a continuous measurement device such as a computerized visual analog scale with a sliding controller. Intensity and unpleasantness of pain experience should be assessed. Female participants should be tested in standardized periods of their menstrual cycles to control influences of hormonal fluctuations.35 Equally, heart rate variability and skin conductance as indicators of activities in the autonomous system should be assessed in all partici-pants. An investigator who is not aware of the intervention allocation should analyze the data. Future studies should reveal the optimal parameters of TVNS that will exert the most specific effects on the parasympathetic nervous sys-tem and central pain inhibitory pathways. Finally, using improved methodology, the underlying effects of TVNS with regard to possible influences of gender and TVNS effects on TSP in patients with chronic pain conditions should be investigated.
CONCLUSIONSTVNS and sham and placebo stimulation exerted compa-rable effects in reducing the perceived pain intensity of repetitive painful heat stimulation. Evidence for the supe-rior effectiveness of TVNS in comparison with sham and placebo stimulation could only be found in male subjects before the beginning of TSP processes. These findings could be biased by involuntary stimulation of vagal nerve endings in the sham and placebo conditions. E
ACKNOWLEDGMENTSThe authors thank all volunteers for their participation; Dr James Paul, Department of Anesthesia, McMaster University, Canada, for carefully rechecking the article for spelling and grammar; and Mrs Nadin Möller, Department of Anesthesiology, University Medicine of Greifswald, Germany, for her support during the preparation of the study.
DISCLOSURESName: Henriette Janner, MSc.Contribution: This author helped with study design and concep-tion, data acquisition, data analysis, interpretation of data, drafting the article, and final approval of the article.Name: Catharina Klausenitz, MD.Contribution: This author helped with study design, interpretation of data, revising the article, and final approval of the article.Name: Nancy Gürtler, BSc.Contribution: This author helped with data acquisition, analysis of data, drafting the article, and final approval of the article.Name: Klaus Hahnenkamp, MD, PhD.Contribution: This author helped with study design and concep-tion, revising the article, and final approval of the article.Name: Taras I. Usichenko, MD, PhD.Contribution: This author helped with study design and concep-tion, data analysis, interpretation of the data, drafting the article, and final approval of the article.This manuscript was handled by: Honorio T. Benzon, MD.
REFERENCES 1. Asher GN, Jonas DE, Coeytaux RR, et al. Auriculotherapy
for pain management: a systematic review and meta-analy-sis of randomized controlled trials. J Altern Complement Med. 2010;16:1097–1108.
2. Sator-Katzenschlager SM, Scharbert G, Kozek-Langenecker SA, et al. The short- and long-term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupunc-ture. Anesth Analg. 2004;98:1359–1364.
3. Silberstein SD, Mechtler LL, Kudrow DB, et al; ACT1 Study Group. Non-invasive vagus nerve stimulation for the acute treatment of cluster headache: findings from the random-ized, double-blind, sham-controlled ACT1 study. Headache. 2016;56:1317–1332.
4. Usichenko TI, Lehmann Ch, Ernst E. Auricular acupuncture for postoperative pain control: a systematic review of randomised clinical trials. Anaesthesia. 2008;63:1343–1348.
5. Busch V, Zeman F, Heckel A, Menne F, Ellrich J, Eichhammer P. The effect of transcutaneous vagus nerve stimulation on pain perception–an experimental study. Brain Stimul. 2013;6:202–209.
6. Johnson MI, Hajela VK, Ashton CH, Thompson JW. The effects of auricular transcutaneous electrical nerve stimulation (TENS) on experimental pain threshold and autonomic function in healthy subjects. Pain. 1991;46:337–342.
7. Kitade T, Hyodo M. The effect of stimulation of ear acupunc-ture points on the body’s pain threshold. Am J Chin Med. 1987;3:241–252.
8. Oliveri AC, Clelland JA, Jackson J, Knowles C. Effects of auricu-lar transcutaneous electrical nerve stimulation on experimental pain threshold. Phys Ther. 1986;66:12–16.

Copyright © 2018 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.2092 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Transcutaneous Vagus Nerve Stimulation and Heat Pain
9. Simmons MS, Oleson TD. Auricular electrical stimulation and dental pain threshold. Anesth Prog. 1993;40:14–19.
10. Ben-Menachem E, Revesz D, Simon BJ, Silberstein S. Surgically implanted and non-invasive vagus nerve stimula-tion: a review of efficacy, safety and tolerability. Eur J Neurol. 2015;22:1260–1268.
11. Usichenko T, Laqua R, Leutzow B, Lotze M. Preliminary find-ings of cerebral responses on transcutaneous vagal nerve stimulation on experimental heat pain. Brain Imaging Behav. 2017;11:30–37.
12. Peuker ET, Filler TJ. The nerve supply of the human auricle. Clin Anat. 2002;15:35–37.
13. Frangos E, Ellrich J, Komisaruk BR. Non-invasive access to the vagus nerve central projections via electrical stimulation of the external ear: fMRI evidence in humans. Brain Stimul. 2015;8:624–636.
14. Kraus T, Kiess O, Hösl K, Terekhin P, Kornhuber J, Forster C. CNS BOLD fMRI effects of sham-controlled transcutaneous electrical nerve stimulation in the left outer auditory canal: a pilot study. Brain Stimul. 2013;6:798–804.
15. Nomura S, Mizuno N. Central distribution of primary affer-ent fibers in the Arnold’s nerve (the auricular branch of the vagus nerve): a transganglionic HRP study in the cat. Brain Res. 1984;292:199–205.
16. Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest. 2010;120:3779–3787.
17. Straube A, Ellrich J, Eren O, Blum B, Ruscheweyh R. Treatment of chronic migraine with transcutaneous stimulation of the auricular branch of the vagal nerve (auricular t-VNS): a randomized, monocentric clinical trial. J Headache Pain. 2015;16:543.
18. Laqua R, Leutzow B, Wendt M, Usichenko T. Transcutaneous vagal nerve stimulation may elicit anti- and pro-nociceptive effects under experimentally-induced pain: a crossover placebo-controlled investigation. Auton Neurosci. 2014;185:120–122.
19. Michalek-Sauberer A, Heinzl H, Sator-Katzenschlager SM, Monov G, Knolle E, Kress HG. Perioperative auricular elec-troacupuncture has no effect on pain and analgesic con-sumption after third molar tooth extraction. Anesth Analg. 2007;104:542–547.
20. Staahl C, Drewes AM. Experimental human pain models: a review of standardised methods for preclinical testing of anal-gesics. Basic Clin Pharmacol Toxicol. 2004;95:97–111.
21. Granot M, Granovsky Y, Sprecher E, Nir RR, Yarnitsky D. Contact heat-evoked temporal summation: tonic versus repeti-tive-phasic stimulation. Pain. 2006;122:295–305.
22. Herrero JF, Laird JM, López-García JA. Wind-up of spinal cord neurones and pain sensation: much ado about something? Prog Neurobiol. 2000;61:169–203.
23. Price DD, Hu JW, Dubner R, Gracely RH. Peripheral suppres-sion of first pain and central summation of second pain evoked by noxious heat pulses. Pain. 1977;3:57–68.
24. Staud R, Price DD, Fillingim RB. Advanced continuous-contact heat pulse design for efficient temporal summation of second pain (windup). J Pain. 2006;7:575–582.
25. Anderson RJ, Craggs JG, Bialosky JE, et al. Temporal summa-tion of second pain: variability in responses to a fixed protocol. Eur J Pain. 2013;17:67–74.
26. Mendell LM, Wall PD. Responses of single dorsal cord cells to peripheral cutaneous unmyelinated fibres. Nature. 1965;206:97–99.
27. Schouenborg J. Functional and topographical properties of field potentials evoked in rat dorsal horn by cutaneous C-fibre stimulation. J Physiol. 1984;356:169–192.
28. Moeller N, Hacker H, Hahnenkamp K, Usichenko T. Search for optimal protocol of temporal summation of experimental heat pain in healthy volunteers [abstract]. Clin Neurophysiol. 2017;128:e158–e159.
29. Spielberger CD. Manual for the State-Trait Anxiety Inventory STAI (Form Y). Palo Alto, CA: Consulting Psychologists Press; 1983.
30. Urbaniak GC, Plous S. Research Randomizer 2013. Version 4.0 [software]. Available at: http://www.randomizer.org/. Accessed April 20, 2015.
31. Lautenbacher S, Kunz M, Strate P, Nielsen J, Arendt-Nielsen L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain. 2005;115:410–418.
32. Leutzow B, Lange J, Gibb A, et al. Vagal sensory evoked poten-tials disappear under the neuromuscular block: an experimen-tal study. Brain Stimul. 2013;6:812–816.
33. Han JS. Acupuncture: neuropeptide release produced by elec-trical stimulation of different frequencies. Trends Neurosci. 2003;26:17–22.
34 .Liepmann D, Beauducel A, Brocke B, Amthauer R. Intelligenz-Struktur-Test 2000 R (I-S-T 2000 R) Manual. 2nd ed. Göttingen: Hogrefe; 2007.
35. Mogil JS. Sex differences in pain and pain inhibition: multiple explanations of a controversial phenomenon. Nat Rev Neurosci. 2012;13:859–866.
36. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191.
37. Greffrath W, Baumgärtner U, Treede RD. Peripheral and central components of habituation of heat pain perception and evoked potentials in humans. Pain. 2007;132:301–311.
38. Andrew D, Greenspan JD. Peripheral coding of tonic mechani-cal cutaneous pain: comparison of nociceptor activity in rat and human psychophysics. J Neurophysiol. 1999;82:2641–2648.
39. Nahman-Averbuch H, Dayan L, Sprecher E, et al. Sex differ-ences in the relationships between parasympathetic activity and pain modulation. Physiol Behav. 2016;154:40–48.
40. Staud R, Craggs JG, Perlstein WM, Robinson ME, Price DD. Brain activity associated with slow temporal summation of C-fiber evoked pain in fibromyalgia patients and healthy con-trols. Eur J Pain. 2008;12:1078–1089.

39
Manuskript 3
Auricular Acupuncture for Exam Anxiety in Medical Students-A Randomized
Crossover Investigation
Catharina Klausenitz, Henriette Janner (geb. Hacker), Thomas Hesse, Thomas
Kohlmann, Karlhans Endlich, Klaus Hahnenkamp & Taras Usichenko
Veröffentlicht in Plos One 2016
CK, KH und TU konzipierten das Studiendesign. CK, TH, KHE und TU erhoben die Daten.
HJ, TK und TU analysierten die Daten. CK, KH und TU erstellten den ersten Entwurf des
Manuskripts. Alle Autoren waren an der Interpretation der Daten und Revision des Manuskripts
beteiligt.

RESEARCH ARTICLE
Auricular Acupuncture for Exam Anxiety inMedical Students—A Randomized CrossoverInvestigationCatharina Klausenitz1,2, Henriette Hacker1, Thomas Hesse1, Thomas Kohlmann3,Karlhans Endlich4, Klaus Hahnenkamp1, Taras Usichenko1,5
1 Department of Anesthesiology, University Medicine of Greifswald, Greifswald, Germany, 2 Institute ofDiagnostic Radiology and Neuroradiology, University Medicine of Greifswald, Greifswald, Germany,3 Institute of Community Medicine, University Medicine of Greifswald, Greifswald, Germany, 4 Institute ofAnatomy, University Medicine of Greifswald, Greifswald, Germany, 5 Department of Anesthesia, McMasterUniversity, Hamilton, Canada
Abstract
Auricular acupuncture (AA) is effective in the treatment of preoperative anxiety. The aim
was to investigate whether AA can reduce exam anxiety as compared to placebo and no
intervention. Forty-four medical students were randomized to receive AA, placebo, or no
intervention in a crossover manner and subsequently completed three comparable oral
anatomy exams with an interval of 1 month between the exams/interventions. AA was
applied using indwelling fixed needles bilaterally at points MA-IC1, MA-TF1, MA-SC, MA-
AT1 and MA-TG one day prior to each exam. Placebo needles were used as control. Levels
of anxiety were measured using a visual analogue scale before and after each intervention
as well as before each exam. Additional measures included the State-Trait-Anxiety Inven-
tory, duration of sleep at night, blood pressure, heart rate and the extent of participant blind-
ing. All included participants finished the study. Anxiety levels were reduced after AA and
placebo intervention compared to baseline and the no intervention condition (p � 0.003). AA
was better at reducing anxiety than placebo in the evening before the exam (p = 0.018). Par-
ticipants were able to distinguish between AA and placebo intervention. Both AA and pla-
cebo interventions reduced exam anxiety in medical students. The superiority of AA over
placebo may be due to insufficient blinding of participants.
Introduction
Exam (or test) anxiety is a type of situational anxiety and is reported to be a common problemamong university students [1,2]. Exam anxiety often leads to undesirable physiological andmental symptoms and may negatively influence academic performance [2,3]. Various mind-fulness-based behavioral interventions have been shown to be effective in reducing exam anxi-ety and stress among university students [4,5]. Some of these methods (e.g. expressive writing)have even been claimed to improve academic performance [6]. However, all of these methods
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 1 / 9
a1111111111a1111111111a1111111111a1111111111a1111111111
23(1$&&(66
Citation: Klausenitz C, Hacker H, Hesse T,Kohlmann T, Endlich K, Hahnenkamp K, et al.(2016) Auricular Acupuncture for Exam Anxiety inMedical Students—A Randomized CrossoverInvestigation. PLoS ONE 11(12): e0168338.doi:10.1371/journal.pone.0168338
Editor: Hong-Liang Zhang, National NaturalScience Foundation of China, CHINA
Received: September 30, 2016
Accepted: November 24, 2016
Published: December 29, 2016
Copyright: � 2016 Klausenitz et al. This is an openaccess article distributed under the terms of theCreative Commons Attribution License, whichpermits unrestricted use, distribution, andreproduction in any medium, provided the originalauthor and source are credited.
Data Availability Statement: All relevant data arewithin the paper and its Supporting Informationfiles. The raw data is given in SPSS table as S3 File.
Funding: The authors received no specific fundingfor this work.
Competing Interests: The authors have declaredthat no competing interests exist.

are time consuming, which makes the routine use of cognitive and behavioural interventionsin the treatment of anxiety immediately before an upcoming exam difficult [4,5].
Auricular acupuncture (AA) is a complementary medicine technique, which is physiologi-cally based on the mechanical stimulation of cranial nerves [7]. AA has already successfullybeen used to treat situational anxiety in clinical settings, such as dental and preoperative anxi-ety [8–10]. For exam anxiety, AA was studied in only one prospective observational study inmedical students without a control group [11]. Since this study did not provide sufficientinformation for further research, we tested the methodology of the AA intervention as well asthe outcome assessment in treatment of pre-exam anxiety using a preliminary pilot investiga-tion [12]. This pilot investigation informed the final study design and provided data to calcu-late the sample size for a subsequent randomized controlled study.
The aim of the present study was to investigate whether AA can reduce exam anxiety inmedical students in comparison with placebo and no intervention conditions in a randomizedcrossover investigation.
Methods
Study design and randomization
This prospective randomized, placebo controlled, single blinded crossover trial was performedbetween April and July 2012 at the University of Greifswald, Germany. The participants wererecruited via announcement in March 2012 before the first anatomy exam in April accordingto the following eligibility criteria: undergraduate medical students in their first year of studywith no fundamental knowledge about and experiences with acupuncture, undergoing threeoral anatomy exams within one month, without any history of alcohol abuse or use of opioidor psychotropic medication and with an American Society of Anesthesiologists physical statusscore of I-II. None of the students were taking any medications or recreational drugs at thetime of the study and all of them were paid for their participation. The follow-up was finishedon the day of the last anatomy exam in July 2012.
The research project was approved by the Institutional Ethics Committee of the UniversityMedicine of Greifswald (reference no. BB 49/12). The trial was registered at clinicaltrials.gov(registration number NCT02920164) after the enrollment of the participants was started sinceinitially the authors regarded the project as an experimental investigation. The authors con-firm that all ongoing and related trials for this drug/intervention are registered. The writteninformed consent was obtained from each participant after the nature of the study procedureswas explained. As all students took three comparable anatomy exams with an interval of onemonth, each of them was randomly assigned to the AA, placebo or no intervention conditionat the evening prior to a scheduled exam by drawing slips of paper with the numbers 1, 2 or 3out of a hat. Each number corresponded to an intervention, as determined a priori: 1 = AA,2 = placebo, 3 = no intervention before the first exam (Fig 1).
Before the second exam, participants were randomly assigned to one of the two remainingconditions by flipping a coin. The investigator, who performed the randomization, ensuredthat the participants could not have been randomized again to the condition they had before.Before the last exam, no further randomization was necessary. The investigator informed theacupuncturist about the assignment of the next participant immediately after the randomiza-tion procedure and prior to any intervention.
Study interventions
A licensed acupuncturist with more than five years of experience with this technique appliedAA at the acupuncture points MA-IC1 (Lung), MA-TF1 (ear Shenmen), MA-SC (Kidney),
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 2 / 9

MA-AT1 (Subcortex) and MA-TG (Adrenal gland) bilaterally according to the methodology,which was previously described in detail elsewhere [12]. Indwelling fixed ’New Pyonex’ nee-dles (length 1.5mm, diameter 0.22mm; Seirin Corp, Shizuoka City, Japan) embedded in askin-colored adhesive tape were used for AA. The participants were instructed by the acupunc-turist to stimulate the auricular needles for 3–5 minutes, if they felt anxious.
For the placebo procedure, ’New Pyonex’ placebo needles were attached to five sites on thehelix of the auricle bilaterally. ’New Pyonex’ placebo needles have the same appearance as AAneedles but consist of self-adhesive tape only [13]. In order to avoid potential physiologiceffects of acupressure, the participants were not instructed to stimulate the attached ’New Pyo-nex’ placebo needles. AA and placebo needles were left in situ until the next day and wereremoved out of sight of the participants after the exam by the investigator, who was notinvolved in acupuncture procedure (Fig 2).
If the participants were assigned to the no intervention condition, they remained seated inthe examination room for 10 to 15 min, which is the same amount of time an application ofthe needles would have taken. During that time, the investigator conducted a conversation
Fig 1. Flow of the study. First randomization (R1) was performed by drawing wrapped pieces of paper with hidden numbers ranging from 1to 3 before the first exam. Second randomization (R2) was performed before the second anatomy exam by flipping a coin; no furtherrandomization was necessary before the last exam in July. R: randomization; AA: auricular acupuncture; NI: no intervention.
doi:10.1371/journal.pone.0168338.g001
Fig 2. Timeline of the investigation with endpoint measurements. Time I: baseline; time II: evening of the day before exam; time 3:immediately before the anatomy exam; time IV: after exam. Auricular acupuncture (AA) was performed in the evening before the day ofexam (time I) using indwelling fixed needles, which remained in situ and were removed after the exam (time IV). Exam anxiety wasmeasured using the German version of Spielberger’s State-Trait-Anxiety Inventory (STAI) and 100 mm visual analogue scale (VAS-100) attimes I, II and III, as was heart rate and blood pressure. Duration and quality of sleep (over the course of the preceding 1 night, 1 week and 6months) were enquired about at time III. Immediately after the exam, at time point IV, exam performance (passed or failed) and the quality ofparticipants’ blinding were recorded.
doi:10.1371/journal.pone.0168338.g002
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 3 / 9

with the participants about leisure activities, place of birth, and opinions on the study facility,thereby, avoiding the topic of the upcoming exam.
For blinding purposes, participants were told that the study’s aim was to investigate two dif-ferent combinations of AA points as treatment methods for pre-exam anxiety in comparisonwith no intervention. Participants had no knowledge which condition they had been random-ized to, except for the no intervention condition.
Outcome measures
Pre-exam anxiety was measured in the evening prior to the exam; before the intervention(Time I); after the intervention (Time II); and immediately before the exam (Time III, Fig 2)using a 100 mm visual analogue scale (VAS-100; from 0 = no anxiety to 100 = maximum imag-inable anxiety) as primary outcome. Additionally state and trait anxiety levels assessed withthe German version of Spielberger’s State-Trait-Anxiety Inventory (STAI; ranging from20 = no anxiety to 80 = maximum imaginable anxiety; [14]) were registered at all three timepoints. In the morning of the exam the participants were asked to fill out a questionnaireabout the quality (6-point-scale ranging from 1 = excellent sleep to 6 = no sleep at all) andduration of sleep the night before as well as the duration of sleep in the preceding i) week andii) in the previous six months. Blood pressure and heart rate were measured before and aftereach intervention as well as before and after each exam (Time I-IV, Fig 2). Immediately afterthe exam, at Time IV, exam performance (passed or failed) and the quality of participantblinding were recorded.
Statistical analysis
The sample size was calculated based on a prospective pilot study [12] by determining the two-sided level of significance at 0.015 (three-period crossover investigation) and power at 85% fora paired sample t-test. Expecting to find a 25% difference in anxiety level between the differentstudy conditions and using the mean and standard deviation values measured in the pilotinvestigation using STAI State-anxiety, the number of participants needed was calculated to be43. Taking into account potential drop-out/withdrawal cases, the sample size was inflated to atotal of 46 volunteers.
Baseline characteristics as well as the differences between the study conditions at differenttime points were analyzed using paired sample t-tests, Holm-Bonferroni adjusted for multiplecomparisons. Fisher’s exact test was used to analyze the success of volunteer blinding. Dataanalysis was performed using IBM SPSS Statistics Software for Mac (Version 19.0.0, IBMCorp., New York, USA). All data are presented as mean (standard deviation) unless otherwisestated, two-sided Holm-Bonferroni-adjusted P-values < 0.05 were regarded as significant.
Results
46 students agreed to participate; two of them did not fulfill the inclusion criteria (Fig 1). 44students (all Caucasian, 35 females) aged 23 (3) were enrolled in the study. Four female partici-pants missed the third session because of illness (Fig 1), their data were treated as missed data.
The baseline anxiety levels (Time I) were comparable among all three trial conditions. Anx-iety levels measured with VAS 5 hours (2) after an intervention in the evening prior to theanatomy exam (Time II) decreased after AA in comparison with baseline values at Time I(mean difference (MD) = 10.5; 95% CI 5.3, 15.8; t40 = 4.0, P< 0.001, d = 0.6, 95% CI 0.3, 1.0;Table 1, Fig 3).
VAS-100 anxiety level at Time II was lower than after no intervention (MD = 13.4; 95% CI5.6, 21.1; t32 = 3.5; P = 0.003, d = 0.6) as well as lower after AA than after placebo (MD = 10.2;
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 4 / 9

Table 1. Outcome measures of the investigation presented as mean (SD).
Parameter Time of measurement Intervention
AA Placebo No intervention
Exam anxiety (VAS-100 mm) I (baseline) 50 (21) 49 (23) 47 (24)
II (after intervention) 39 (20) 49 (24)* 54 (25)**III (before exam) 49 (22) 58 (21)* 62 (23)**
Trait anxiety I 44 (11) 45 (12) 43 (11)
State anxiety I 55 (11) 53 (12) 54 (11)
II 47 (11) 52 (12)* 57 (13)**III 53 (11) 54 (10)* 60 (11)**
Duration of sleep (h) Preceding 6 months 7.7 (1) 7.7 (1) 7.7 (1)
Preceding week 6.9 (1) 7.0 (1) 7.0 (1)
Night before exam 7.0 (2) 7.3 (1) 6.8 (2)
Passed exam, N (%) After exam 34 (81) 32 (79) 33 (84)
Statistically significant differences between 3 study conditions (in bold letters) revealed with paired sample t-tests with Holm-Bonferroni-adjustment for
multiple comparisons. VAS-100: Visual Analogue Scale 100 mm.
* P 0.05 for comparisons of auricular acupuncture (AA) vs. placebo
** P � 0.01 for comparisons of AA vs. no intervention.
doi:10.1371/journal.pone.0168338.t001
Fig 3. Exam anxiety measured using Visual Analogue Scale 100mm. Time I: baseline; time II: evening of the day before exam;time 3: immediately before the anatomy exam. Holm-Bonferroni adjusted P = 0.018 for AA vs. placebo; ** Holm-Bonferroni adjustedP = 0.003 for AA vs. no intervention at time II and *** P � 0.003 for AA vs. no intervention at time III. Data given as mean (standarderror of mean).
doi:10.1371/journal.pone.0168338.g003
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 5 / 9

95% CI 2.7, 17.7; t40 = 2.7; P = 0.018, d = 0.4). On the morning of the exam (Time III), VAS-100 anxiety level after AA was also lower than after no intervention (MD = 12.3; 95% CI5.8,18.8; t36 = 3.9; P< 0.003, d = 0.6) and in comparison with placebo (MD = 9.65; 95% CI1.3,18.0; t39 = 2.3; P = 0.05; d = 0.4).
In line with the findings of the primary outcome, state anxiety assessed with STAI at TimeII was also reduced after AA in comparison with placebo (MD = 4.4; 95% CI 0.7, 8.1; t40 = 2.4;P = 0.021, d = 0.4) and as compared to no intervention (MD = 9.9; 95% CI 6.0,13.9; t33 = 5.1;P = 0.003; d = 0.9). State Anxiety after placebo at Time II was also lowered if compared to nointervention (MD = 5.2; 95% CI 1.2, 9.2; t36 = 2.6; P = 0.024, d = 0.4). At Time III, state anxietyafter AA (MD = 6.7; 95% CI 3.5,9.9; t37 = 4.2; P = 0.003, d = 0.7) and after placebo (MD = 5.1;95% CI 1.9,8.2; t40 = 3.3; P = 0.004, d = 0.5) was reduced as compared to no intervention. Thetrait anxiety, assessed with STAI was 44 (11), which significantly exceeds the mean found inthe norm sample for the female population aged between 15 and 29 years (36 (10); t35 = 4.1;p< 0.001, d = 0.7; 14, Table 1).
The duration and quality of sleep, blood pressure, heart rate and exam performance werecomparable among the three study conditions (Table 1 and S1 Table). Being asked after theexam about their opinion on allocation to the study condition, the participants could distin-guish between AA and placebo intervention: for the AA condition, 34 participants thoughtthat they had received acupuncture vs. 7 for the placebo condition (P< 0.001; Table 2).
Conclusion
This randomized crossover trial demonstrated that both auricular acupuncture (AA) and pla-cebo reduced exam anxiety in comparison with no intervention in medical students, whereasAA yielded stronger effects than placebo procedure.
Without any intervention, the level of anxiety, measured with both STAI and VAS-100,increased constantly before the upcoming exam (Fig 3). These results are in line with the find-ings of Brockmeyer et al. [15]. Exam anxiety decreased by up to 20% from baseline after AA incomparison to placebo procedure and no intervention. The largest effect size of AA over pla-cebo procedure and no intervention was measured using VAS-100 in the evening after theintervention on the day before the exam. The effect size observed in the present study is com-parable to the findings of our pilot investigation [12] and other previous studies of AA and sit-uational anxiety [8–11]. For example, Karst et al. [9] reported that state anxiety scoresdecreased by about 18% from baseline to after AA treatment of dental anxiety in 19 patients.Likewise, Michalek-Sauberer et al [10] demonstrated a reduction in STAI state anxiety levelsby about 15% from baseline to after AA in 61 patients for dental procedures. However, bothinvestigations failed to find the difference between verum AA and placebo procedures.
In our investigation, placebo procedure was found to reduce exam anxiety in comparisonto no intervention in medical students as well, although this effect was not as strong as thereduction of pre-exam anxiety through AA. Even if the majority of participants could
Table 2. Participants’ opinion about the allocation to study condition/intervention.
Intervention
Auricular Acupuncture Placebo
It was verum 34 (77) 7 (15)
It was placebo 6 (14) 21 (48)
Do not know 1 (2) 8 (18)
Data is presented as number of participants (%).
doi:10.1371/journal.pone.0168338.t002
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 6 / 9

distinguish between verum and placebo procedure, we are hesitant to say that the differencebetween AA and placebo occurred due to a bias of potential “unblinding” because of twoaspects: i) due to “unblinding”, the placebo effect should have disappeared, however there wassustained effect of placebo over the no intervention condition, as measured by both VAS-100and STAI (Table 1, Fig 3); ii) questioning about the opinion on the allocation to the study con-dition took place at the end of the study after the exam, meaning that the exact time of poten-tial “unblinding” is unclear. We could not determine the time of “unblinding” in this studyand this fact remains the main limitation of our investigation. Moreover, since the participantswere instructed to stimulate the needles in case they start to feel anxious only before the AAcondition, this action could not be controlled in the placebo condition and may have dimin-ished the difference between AA and placebo due to the weak physiological effect of acupres-sure applied to ’New Pyonex’ placebo needles [16]. Furthermore, on the day before the exam, 3participants did not document their anxiety levels. They reported to have forgotten about itbecause of their high stress levels immediately before the exam.
As expected, STAI trait anxiety scores did not change during the course of the investigation.This is unsurprising as they are thought to reflect a stable personal characteristic that remainsconstant over time and between events [14]. The mean value of trait anxiety in the study groupsignificantly exceeded the mean found in the general female population aged between 15 and29 years [14]. This is in agreement with previous findings about increased anxiety levels andlower self-confidence among female medical students [17] and explains the “natural” selectionof predominantly anxious females that volunteered to participate in our study.
Despite the expectations based on previous results [6, 8–12], we could not observe the bene-ficial effect of AA or placebo on quality and duration of sleep as well as exam performance inparticipants of our study. The stability of hemodynamic parameters and the absence of sideeffects and complications confirm the respective findings of previous investigations [6, 8–13].
This trial followed the CONSORT guidelines for specific requirements of acupuncture stud-ies [18,19]. The randomized crossover design and the use of a formulaic auricular acupuncture(constant pattern of cranial nerves stimulation) rather than individualized acupuncture haveminimized potential biases. The dropout rate of 9% was low.
Regarding the above-mentioned limitations of the present investigation we suggest thatfuture studies should examine larger samples to compensate for dropout rates and incompletedata. The “parallel arms” approach might be considered in order to prevent any exchange ofparticipant experiences and intra-individual “carry-over” experience, which may have contrib-uted to the potential “unblinding” in our investigation. Also the number of participants, whohave stimulated the needles by pressing, if they felt anxious, should be verified in future inves-tigations, since the stimulation (or not stimulation of the needles) might have caused the effectbias. Furthermore, the measurement of non-invasive stress biomarkers as salivary cortisol, sali-vary ċ-amylase or catecholamines in urine might strengthen the findings of any future investi-gations, giving further insights into the biological mechanisms of AA.
In order to evaluate the clinical significance of the AA effect, this technique should be com-pared with methods that are commonly used for treatment of exam anxiety, such as relaxationtechniques, biofeedback and systematic desensitization [4–6, 20–22]. Moreover, after appro-priate investigations, AA might be used to treat pre-operative anxiety in surgical patients, con-stituting serious alternative for benzodiazepines, commonly used for this purpose in clinicalpractice [9,10,23].
In conclusion, both auricular acupuncture and placebo procedure were shown to be effec-tive in reducing levels of exam anxiety in medical students. The superiority of verum AA overplacebo AA and no intervention is considered to be due to stimulation of cranial nerves, butmay have been increased in effect by insufficient participant blinding.
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 7 / 9

Supporting Information
S1 Table. Blood pressure and heart rate during the study conditions given as mean (SD).(DOCX)
S1 File. Ethics commission application.(PDF)
S2 File. Pilot investigation.(PDF)
S3 File. Study Data.(SAV)
S4 File. Consort Checklist.(PDF)
Acknowledgments
The authors would like to thank Bianca Leutzow for her assistance in organization of thestudy, Franziska Miller for re-checking the manuscript for mistakes and the students who par-ticipated in this study.
Author Contributions
Conceptualization: CK TU.
Formal analysis: HH TK TU.
Investigation: CK TH KHE TU.
Methodology: CK HH TK TU.
Project administration: CK KH.
Resources: TK KHE KH.
Supervision: KHE KH.
Validation: HH TK.
Writing – original draft: CK KH TU.
Writing – review & editing: TH HH KHE.
References1. Eisenberg D, Hunt J, Speer N. Mental health in American colleges and universities: variation across stu-
dent subgroups and across campuses. J Nerv Ment Dis 2013; 201:60–7. doi: 10.1097/NMD.0b013e31827ab077 PMID: 23274298
2. Latas M, Pantic M, Obradovic D. Analysis of test-anxiety in medical students. Med Pregl 2010; 63:863–6. PMID: 21553469
3. Zhang Z, Su H, Peng Q. Exam anxiety induces significant blood pressure and heart rate increase in col-lege students. Clin Exp Hypertens 2011; 33: 281–6. doi: 10.3109/10641963.2010.531850 PMID:21787237
4. Neuderth S, Jabs B, Schmidtke A. Strategies for reducing test anxiety and optimizing exam preparationin German university students: a prevention-oriented pilot project of the University of Wurzburg. J Neu-ral Transm 2009 Jun; 116: 785–90. doi: 10.1007/s00702-008-0123-7 PMID: 18810305
5. Regehr C, Glancy D, Pitts A. Interventions to reduce stress in university students: a review and meta-analysis. J Affect Disord 2013; 148: 1–11. doi: 10.1016/j.jad.2012.11.026 PMID: 23246209
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 8 / 9

6. Ramirez G, Beilock SL. Writing about testing worries boosts exam performance in the classroom. Sci-ence 2011; 331: 211–3. doi: 10.1126/science.1199427 PMID: 21233387
7. Usichenko TI, Mustea A, Pavlovic D. On ears and Head. Acupunct Med 2010; 28: 165–6. doi: 10.1136/aim.2010.003244 PMID: 21148074
8. Wang SM, Peloquin C, Kain ZN. The use of auricular acupuncture to reduce preoperative anxiety.Anesth Analg 2001; 93: 1178–80. PMID: 11682391
9. Karst M, Winterhalter M, Munte S, Francki B, Hondronikos A, Eckardt A et al. Auricular acupuncture fordental anxiety: a randomized controlled trial. Anesth Analg 2007; 104: 295–300. doi: 10.1213/01.ane.0000242531.12722.fd PMID: 17242083
10. Michalek-Sauberer A, Gusenleitner E, Gleiss A, Tepper G, Deusch E. Auricular acupuncture effectivelyreduces state anxiety before dental treatment—a randomised controlled trial. Clin Oral Investig 2012;16: 1517–22. doi: 10.1007/s00784-011-0662-4 PMID: 22219023
11. Ogal H, Ogal M, Hafer J, Hennig J, Brockmeyer H, Kracht R et al. Beginn der Anxiolyse und Relaxationunter Ohrakupunktur. Deutsche Zeitschrift fur Akupunktur 2004; 47: 6–12.
12. Klausenitz C, Hesse T, Hacker H, Hahnenkamp K, Usichenko T. Auricular acupuncture for pre-examanxiety in medical students: a prospective observational pilot investigation. Acupunct Med 2016; 34:90–4. doi: 10.1136/acupmed-2015-010887 PMID: 26438557
13. Hesse T, Henkel B, Zygmunt M, Mustea A, Usichenko TI. Acupuncture for pain control after Caesareansection: a prospective observational pilot study. Acupunct Med 2016; 34: 14–9. doi: 10.1136/acupmed-2015-010852 PMID: 26307554
14. Spielberger CD. Manual for state-trait anxiety inventory (STAI: Form Y). Palo Alto, California: Consult-ing Psychologist Press, 1983.
15. Brockmeyer H. Prufungsangst: eine experimentelle Studie zur Wirkung der Ohrakupuntur auf Psycheund Hormone. Essen: KVC Verl., 2005; 79.
16. Lundeberg T, Lund I, Sing A, Naslund J. Is placebo acupuncture what it is intended to be? Evid BasedComplement Alternat Med 2011; 2011: 932407. doi: 10.1093/ecam/nep049 PMID: 19525330
17. Blanch DC, Hall JA, Roter DL, Frankel RM. Medical student gender and issues of confidence. PatientEduc Couns 2008; 72: 374–81. doi: 10.1016/j.pec.2008.05.021 PMID: 18656322
18. Moher D, Schulz KF, Altman DG, CONSORT GROUP (Consolidated Standards of Reporting Trials).The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Ann Intern Med 2001; 134: 657–62. PMID: 11304106
19. MacPherson H, White A, Cummings M, Jobst K, Rose K, Niemtzow R. Standards for reporting interven-tions in controlled trials of acupuncture: the STRICTA recommendations. Complement Ther Med 2001;9: 246–9. doi: 10.1054/ctim.2001.0488 PMID: 12184354
20. Dendato KM, Diener D. Effectiveness of cognitive/relaxation therapy and study-skills training in reduc-ing self-reported anxiety and improving the academic performance of test-anxious students. J CounsPsychol 1986; 33: 131–5.
21. Reed M, Saslow C. The effects of relaxation instructions and EMG biofeedback on test anxiety, generalanxiety, and locus of control. J Clin Psychol 1980; 36: 683–690. PMID: 6997335
22. Deffenbacher JL, Suinn RM. Systematic desensitization and the reduction of anxiety. Couns Psychol1988; 16: 9–30.
23. Maurice-Szamburski A, Auquier P, Viarre-Oreal V, Cuvillon P, Carles M, Ripart J et al. Effect of sedativepremedication on patient experience after general anesthesia: a randomized clinical trial. JAMA 2015;313:916–25. doi: 10.1001/jama.2015.1108 PMID: 25734733
Auricular Acupuncture for Exam Anxiety
PLOS ONE | DOI:10.1371/journal.pone.0168338 December 29, 2016 9 / 9

49
Manuskript 4
Auricular acupuncture for treatment of preoperative anxiety in patients scheduled for
ambulatory gynaecological surgery: a prospective controlled investigation with a non-
randomised arm
Jakub K. Wunsch, Catharina Klausenitz, Henriette Janner (geb. Hacker), Thomas Hesse,
Alexander Mustea, Klaus Hahnenkamp, Astrid Petersmann & Taras Usichenko
Akzeptiert zur Veröffentlichung in Acupuncture in Medicine am 31.12.2017
JW, CK und AM rekrutierten die Patienten. JW, TH, AP und TU erhoben die Daten. JW und
HJ analysierten die Daten. KH und TU interpretierten die Daten. Alle Autoren waren an der
Erstellung und Revision des Manuskripts beteiligt.

50
Jakub K. Wunsch, Catharina Klausenitz, Henriette Janner, Thomas Hesse, Alexander Mustea,
Klaus Hahnenkamp, Astrid Petersmann, Taras I. Usichenko, Auricular acupuncture for
treatment of preoperative anxiety in patients scheduled for ambulatory gynaecological surgery
- a prospective controlled investigation with non-randomised arm. Acupuncture in Medicine
(Volume 36, Issue 4) pp. 222-227. Copyright © [2018] (SAGE Publications).
DOI: [10.1136/acupmed-2017-011456].
Auricular acupuncture for treatment of preoperative anxiety in patients scheduled for
ambulatory gynaecological surgery - a prospective controlled investigation with non-
randomised arm
Authors: Jakub K. Wunsch1, Catharina Klausenitz2, Henriette Janner1, Thomas Hesse1,
Alexander Mustea3, Klaus Hahnenkamp1 Astrid Petersmann 4, Taras I. Usichenko1,5
Affiliations of the authors:
1. Department of Anaesthesiology, University Medicine of Greifswald, Germany
2. Institute of Diagnostic Radiology, University Medicine of Greifswald, Germany
3. Department of Gynaecology and Obstetrics, University Medicine of Greifswald, Germany
4. Institute of Clinical Chemistry, University Medicine of Greifswald, Germany
5. Department of Anesthesia, McMaster University, Hamilton, Canada1
Corresponding author:
Dr. Taras Usichenko, Department of Anaesthesiology, University Medicine of Greifswald
Sauerbruchstrasse, 17475 Greifswald; phone: 0049 3834 86 5893; Fax: 0049 3834 86 5802
Email: [email protected]
Key words: pre-operative anxiolysis; ambulatory surgery; auricular acupuncture

51
Word count: 2071
ABSTRACT
Objective Auricular acupuncture (AA) is a promising alternative treatment for situational
anxiety. This pilot investigation was aimed at testing the acceptability and feasibility of AA as
a treatment for preoperative anxiety (PA) in preparation for a subsequent randomized controlled
trial.
Methods AA was offered for treatment of PA to female patients, who were scheduled for
ambulatory gynaecological surgery. In patients who agreed, the indwelling fixed needles were
applied bilaterally at the points MA-IC1, MA-TF1, MA-SC, MA-AH7 and MA-T the day
before surgery. Patients who declined AA but agreed to be examined, constituted the control
group (no intervention). State anxiety (as primary outcome) was measured using State-Trait-
Anxiety Inventory (STAI) before AA (time I), the evening before surgery (time II) and
immediately before surgery (time III). Anxiety was measured with a 100 mm visual analogue
scale (VAS-100); heart rate, blood pressure and serum cortisol were also measured.
Results Data of 62 patients (32 with AA and 30 with no intervention) were analysed. Whereas
preoperative anxiety was reduced after AA the evening before surgery (P < 0.01), anxiety levels
in the control group increased from the first to the last measurement (P < 0.001). Secondary
outcomes were comparable among the patients from both groups.
Conclusions Auricular acupuncture methodology was acceptable and feasible as treatment for
preoperative anxiety. Results were used for sample size calculation of a subsequent randomised
controlled clinical trial.

52
INTRODUCTION
Patients undergoing surgery mostly experience acute psychological distress in the
preoperative period, including feelings of uncertainty, loss of control and decreased self-esteem,
anticipation of postoperative pain, as well as the fear of separation from their family [1]. All
these symptoms, known as preoperative anxiety syndrome, may have a profound effect on
patients, not only influencing their quality of life but also the course and outcome of the surgical
procedures [2-6]. However, pharmacological therapy of preoperative anxiety is associated with
numerous medico-biological and economical adverse effects [7,8]. Moreover, in patients
undergoing surgical procedures in ambulatory setting, the use of sedative drugs for
premedication should be critically discussed [9].
Auricular acupuncture (AA) is a complementary medicine technique, which has already
been used to treat situational anxiety in clinical settings [10-13]. In 1987, Lewis & Litt found
auricular acupressure and relaxation methods as effective as diazepam for premedication in 90
patients scheduled for surgery under general anaesthesia and those alternative treatments were
associated with a reduced autonomous stress reaction, as well as fewer side effects compared
with diazepam treatment [10]. Karst et al. (2007) confirmed these results using the same model
of situational anxiety in 67 patients scheduled for dental extractions. The authors compared AA
with intranasal midazolam, placebo acupuncture and no treatment [11]. Michalek-Sauberer et
al. (2012) reported AA to be more effective than sham acupuncture and no intervention
regarding the anxiolysis in a sample of 182 patients scheduled to undergo dental procedures
[12]. In a recently published randomised investigation, Luo et al (2015) found auricular
acupressure superior over placebo acupressure regarding the reduction of preoperative anxiety
in patients undergoing gynaecological surgery [13]. The data from experimental research
suggests that due to its unique neuroanatomical conditions, auricular stimulation exerts its
anxiolytic effects via the involvement of cranial nerves [14], which leads to the modulation of
the brain areas, involved in stress response like limbic system, locus coeruleus and
hypothalamus [15-17].

53
Given these findings, it seems possible that auricular stimulation might serve as an
effective replacement of benzodiazepines, which are still widely used in Europe to treat
preoperative anxiety within standard premedication before surgery [7].
This pilot investigation was aimed at testing the acceptability and feasibility of outcome
measurements of the methodology of AA as a simple, non-pharmacological treatment of
preoperative anxiety in comparison with no intervention. Furthermore, results should provide
necessary data to calculate the adequate sample size for a subsequent randomised controlled
trial (RCT).
METHODS
Design and participants
This prospective open clinical study was conducted at the University Medicine of Greifswald
from December 2015 to April 2016. The local ethics committee approved the study protocol .
Patients were recruited according to the following eligible criteria: American Society of
Anaesthesiologists physical status of I to II, scheduled for elective ambulatory gynaecological
surgery under standardised general anaesthesia with a duration of surgery ≤ 60 min, aged
between 19 and 55 years, with the ability to fill in the chosen questionnaires, and without
previous opioid and psychotropic medication, current psychiatric disorders or local skin
infection at the sites of acupuncture. Patients were excluded when intraoperative complications
(bleeding, required blood transfusion more than 6 units of packed cells, cardiovascular
instability, required catecholamines) or failures by following the standardised schema of
general anaesthesia occurred, as well as if patients consumed opioid medication ≤ 6 months
before surgery or developed local auricular or systemic infection or a severe intercurrent disease
during the study.
During standard preoperative anaesthesiology examination, patients were informed, in
writing, about the aim and procedures of the study. Afterwards, patients were asked if they
wanted to participate and receive AA as treatment for preoperative anxiety before ambulatory

54
surgery. Patients who refused to receive AA were asked to take part in a routine internal audit
of perioperative anxiety without any intervention and without change in the scheme of clinical
routine for ambulatory patients. These patients of the non-randomised arm constituted the
control group with the “no intervention” in this investigation (Figure 1). Written informed
consent was obtained from each participant.
Auricular acupuncture
A licensed acupuncturist, with more than five years’ experience with auricular
acupuncture, applied indwelling fixed “New Pyonex” needles (length: 1.5 mm, diameter: 0.22
mm; Seirin Corp., Shizuoka City, Japan) bilaterally at five acupuncture points: MA-IC1 (Lung),
MA-TF1 (ear Shenmen), MA-SC (Kidney), MA-AT1 (Subcortex) and MA-TG (Adrenal gland,
Figure 2) according to the AA nomenclature of the World Health Organisation (WHO) [18] and
French classification [19]. The choice of acupuncture points was based on the methodology of
our randomised controlled study on treatment of situational (exam) anxiety in medical students
[20,21], as well as the AA patterns from previous investigations [10-13].
Before needle insertion, the skin was disinfected with alcohol swabs. Patients were
instructed by the acupuncturist to stimulate the auricular needles for 3 to 5 minutes if they feel
anxious. AA needles were placed the day before the surgery, immediately after the preoperative
anxiety level was assessed for the first time (Figure 3). The needles remained in situ until the
next day and were removed after the surgery, right before the discharge home.
General anaesthesia and postoperative analgesia
All study patients received standardised general anaesthesia. Anaesthesia was
performed using propofol 2-3 mg/kg, sufentanil 0.02 mcg/kg and mivacurium 0.2 mg/kg as
muscle-relaxing agents, if tracheal intubation was required. Lung ventilation was either
manually or mechanically controlled to keep end-tidal carbon dioxide at 4.5 to 5.3 kPa
throughout the surgery. Anaesthesia was maintained using either continuous infusion of

55
propofol 4-8 mg/kg/h or volatile anaesthetic sevoflurane with end-tidal concentration 1.5-2
volume % in a 40% oxygen-air mixture.
Perioperative PONV prevention was provided according to department-internal
standard using P6 acupuncture and dexamethason 0.01 mg/kg. Treatment of postoperative pain
included either acetaminophen 4 x 1 g or metamizol 4 x 1 g daily, supplemented by injections
of piritramide (opioid analgesic with 0.7 potency of morphine) 0.01-0.015 mg/kg if required.
Outcome measures
The primary outcome measure was preoperative anxiety, measured before AA
intervention or in the control group at a comparable time point (time I), in the evening of the
day before the surgery (time II) and immediately before the surgery (time III, Figure 3) using
the state form of the German version of the STAI, ranging from 20 (= no anxiety) to 80 (=
maximum imaginable anxiety) [22]. Secondary outcome measures were anxiety level,
measured using a 100 mm visual analogue scale (VAS-100; 0 = no anxiety and 100 = maximum
imaginable anxiety) at time points I, II and III as well as heart rate and blood pressure, which
were registered throughout the course of the study. Serum cortisol was measured at time point
II using a competitive immunoassay on the basis of ADVIA-Centaur chemoluminescence
technology (Siemens Healthcare Diagnostics, Eschborn, Germany) according to the Guideline
of the German Medical Association on Quality Assurance in Medical Laboratory Examinations
[23].
Statistical Analysis
This pilot investigation was aimed at generating data for sample size calculation of a
subsequent randomized controlled trial. Since data of state anxiety measured with STAI was
assumed to be nearly normally distributed from 30 subjects, the sample size was set to 30 for
each group (AA and “no intervention” group). Analysis of primary outcome was performed
using ANOVA for repeated measures with the between-subject factor GROUP (AA vs. no

56
intervention) and within-subject factor TIME (measurement time points I to III). Post-hoc
comparison, as well as the analysis of secondary outcome measures, was performed using
Student’s t-test (for normally distributed data) and Wilcoxon signed rank test (for skewed data)
within each group. IBM SPSS Statistics Software (Version 22.0) was used for data analysis. P-
values were corrected for multiple comparisons using Holm-Bonferroni procedure and adjusted
P-values < 0.05 were regarded as significant. All data are presented as mean ± SD unless
otherwise stated.
RESULTS
Out of 94 eligible patients, 63 agreed to participate and were included in the investigation.
One patient reacted with vasovagal faint during the AA intervention and was excluded (Figure
1). The time lapse between AA and the surgery on the next day consisted 22.5 ± 2.7 hours
(mean ± standard deviation). The demographic parameters and trait anxiety of 32 patients, who
wished to receive AA, were comparable to those of 30 participants, who consented only to the
audit for anxiety (Table 1).
There were no significant differences in preoperative anxiety between the study groups
at any of the three time points of outcome measurement, although the course of preoperative
anxiety differed with-in the groups, as indicated by the interaction effect of GROUP*TIME;
p<0.001 (Figure 4). In patients, who received no intervention, anxiety (STAI) increased through
the course of the study; at time III vs. time I; p = 0.002; and vs. time II (p < 0.001; Figure 4,
Table 2).
In participants who received AA, preoperative anxiety decreased after AA intervention
(time II) as compared to baseline (time I): p = 0.006; (Table 2 and Figure 4). On the next day
immediately before the surgery (time III), anxiety increased in comparison with time II: p =
0.013; Figure 4, Table 2).
Heart rate, blood pressure and serum cortisol were also comparable between the study
groups.

57
State anxiety, which will be the primary endpoint in our subsequent RCT (with 3 study
arms: verum, placebo and no intervention), was used to calculate the required sample size.
Assuming a variability in anxiety of 11 (standard deviation, Table 2), 60 patients per group are
needed to demonstrate an estimated minimal clinically important difference between groups of
20% at a significance level of 0.05 and power of 85%, taking into account a Bonferroni
adjustment for multiple comparisons between three anticipated experimental groups. In order
to compensate for the expected dropout rate of 10%, the size of these groups will be further
inflated to 67 patients each.
DISCUSSION
This open non-randomized pilot clinical investigation was aimed to test the acceptability
and feasibility of outcome measurements and the methodology of AA as a simple non-
pharmacological treatment of preoperative anxiety in comparison with no intervention.
All participants, except one patient, tolerated AA treatment well and wished to receive
it again before a surgery. The participant that reacted with a vasovagal syncope after AA
stimulation is one of the rare cases of hyperactive vagal responses that are documented in the
literature [24,25]. Since all patients received AA while being in supine position and applied by
a licensed MD, the occurrence of this adverse event was easily brought under control with no
further complication for the patient. However, the possibility of vasovagal reactions after
auricular stimulation should be kept in mind for all future AA treatments and the acupuncturist
should be always prepared to handle such situations properly.
The preoperative anxiety of patients that received AA was reduced about 14 % in the
evening before surgery, in comparison with anxiety levels before the AA intervention.
Preoperative anxiety immediately before the surgery nearly reached the anxiety level measured
before AA intervention. In the group with no intervention, however, preoperative anxiety levels
continuously increased from the first time point of measurement, through the evening before

58
the surgery, and remained increased about 20 % immediately before the surgery, if compared
to anxiety levels assessed at baseline.
These findings are in agreement with the results in previous investigations regarding
AA and situational anxiety [10-13,20,21]. For example, Karst et al. [11] reported that state
anxiety scores decreased by about 18% from baseline after AA treatment of dental anxiety.
Likewise, Michalek-Sauberer et al [12] demonstrated a reduction in STAI state anxiety levels
by about 15% from baseline after AA in 61 patients for dental procedures.
Trait anxiety scores were comparable in patients that received AA and patients with no
intervention. The mean value of trait anxiety in this sample was higher than the mean in the
general female population of this age (37 ± 11; p < 0.001, Table 2), but below the critical cut-
off for diagnosis of a specific phobia [22]. This finding is in line with results from Carr et al.
(2006) where almost half of the study sample of 80 women undergoing gynaecological surgery
reported trait anxiety scores of ≥ 45 [18]. This is probably due to the nature of gynaecological
conditions that are associated with high rates of psychological morbidity and vulnerability
[26,27].
The main limitation of the present investigation is that the patients were not randomly
allocated to receive either AA or no intervention. Moreover, effects of AA should be examined
in comparison with a comparable placebo treatment as in previous studies [11-13,21]. In
addition, future studies should assess stress-specific biomarkers such as cortisol,
catecholamines, and salivary alpha-amylase or continuous monitoring of heart rate variability
and electrodermal activity in order to support self-reports about anxiety. However, this study
was designed to test the acceptability and feasibility of our AA methodology and to yield
preliminary data to calculate the necessary sample size for further randomized controlled
investigations.
Conclusion

59
Auricular acupuncture was well accepted by patients as treatment for preoperative
anxiety, the chosen outcome measurements were feasible and have facilitated the calculation of
the sample size for a subsequent RCT.

60
Contributorship Statement:
J.W.: data collection, patients’ recruitment, analysis of data, writing the manuscript; C.K.:
patients’ recruitment, auricular acupuncture, writing the manuscript; H.H.: data collection,
writing the manuscript; T.H.: data collection; writing the manuscript; A.M.: patients’
recruitment, writing the manuscript; K.H.: data interpretation, writing the manuscript; A.P.:
data collection, writing the manuscript; T.I.U.: idea of publication, data collection, writing the
manuscript.
Funding statement:
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors.
Acknowledgement:
The authors would like to thank Maria Gagarine for re-checking the manuscript for mistakes,
the nurses from preoperative ward for recruiting the patients and the patients who participated
in this study.
Competing Interest: none declared
Ethics approval: The study was prospectively approved by the Institutional Ethics Committee
of University Medicine Greifswald (reference no. BB 158/15), the trial was registered at
clinicaltrials.gov (registration number NCT02656966) and was carried out in accordance with
the principles of the Declaration of Helsinki.

61
REFERENCES
1. Asilioglu K, Celik SS. The effect of preoperative education on anxiety of open cardiac
surgery patients. Patient Educ Couns 2004;53:65-70.
2. Markland D, Hardy L. Anxiety, relaxation and anaesthesia for day-case surgery. Br J Clin
Psychol 1993;32:493-504.
3. Pritchard MJ. Managing anxiety in the elective surgical patient. Br J Nurs 2009;18:416-
9.
4. Biddiss E, Knibbe TJ and McPherson A. The effectiveness of interventions aimed at
reducing anxiety in health care waiting spaces: a systematic review of randomized and
nonrandomized trials. Anesth Analg 2014;119:433-448.
5. Vaughn F, Wichowski H and Bosworth G. Does preoperative anxiety level predict
postoperative pain? AORN J 2007;85:589-604.
6. Van den Bosch JE, Moons KG, Bonsel GJ and Kalkman CJ. Does measurement of
preoperative anxiety have added values for predicting postoperative nausea and
vomiting? Anesth Analg 2005;100:1525-1532.
7. Maurice-Szamburski A, Auquier P, Viarre-Oreal V, Cuvillon P, Carles M, Ripart J,
Honore S, Triglia T, Loundou A, Leone M, Bruder N; PremedX Study Investigators.
Effect of sedative premedication on patient experience after general anesthesia: a
randomized clinical trial. JAMA 2015;313:916-25.
8. Patel T, Kurdi MS. A comparative study between oral melatonin and oral midazolam on
preoperative anxiety, cognitive, and psychomotor functions. J Anaesthesiol Clin
Pharmacol 2015;31:37-43.
9. White PF, Eng M. Fast-track anesthetic techniques for ambulatory surgery. Curr Opin
Anaesthesiol 2007;20:545-57.
10. Lewis GBH, Litt M. An alternative approach to premedication: comparing diazepam with
auriculotherapy and a relaxation method. Am J Acupunct 1987;15:205-

62
11. Karst et al. Auricular Acupuncture for Dental Anxiety: A Randomized Controlled Trial.
Anesth Analg 2007;104:295-300.
12. Michalek-Sauberer et al. Auricular acupuncture effectively reduces state anxiety before
dental treatment—a randomised controlled trial. Clin Oral Investig 2012;16:1517-22.
13. Luo L, Dai Q, Mo Y, Yan Y, Zhuang X, Hunag L et al. The effect of auricular acupressure
on preoperative anxiety in patients undergoing gynecological surgery. Int J Clin Exp Med
2016;9:4065-4070.
14. Usichenko T, Hacker H, Lotze M. Transcutaneous auricular vagal nerve stimulation
(taVNS) might be a mechanism behind the analgesic effects of auricular acupuncture.
Brain Stimul 2017;10:1042-4.
15. Kraus T, Hösl K, Kiess O, Schanze A, Kornhuber J, Forster C. BOLD fMRI deactivation
of limbic and temporal brain structures and mood enhancing effect by transcutaneous
vagus nerve stimulation. J Neural Transm 2007;114:1485-93.
16. Frangos E, Ellrich J, Komisaruk BR. Non-invasive Access to the Vagus Nerve Central
Projections via Electrical Stimulation of the External Ear: fMRI Evidence in Humans.
Brain Stimul 2015;8:624-36.
17. Chen J, Barrett DW, He Y, Gonzalez-Lima F. Anxiolytic-like behavioural effects of head
electroacupuncture in rats susceptible to stress. Acupunct Med 2016;34:235-40.
18. WHO. Third WHO Regional Working Group on Standardization of Acupuncture
Nomenclature. Seoul, 1987.
19. Nogier PFM. Traité d’auriculotherapie. Moulinlés-Metz: Maisonneuve,1972.
20. Klausenitz C, Hesse T, Hacker H, Hahnenkamp K, Usichenko T. Auricular acupuncture
for pre-exam anxiety in medical students: a prospective observational pilot investigation.
Acupunct Med 2016;34:90-4.
21. Klausenitz C, Hacker H, Hesse T, Kohlmann T, Endlich K, Hahnenkamp K, Usichenko
T. Auricular Acupuncture for Exam Anxiety in Medical Students - A Randomized
Crossover Investigation. PLoS ONE 2016;11:e0168338.

63
22. Spielberger CD. Manual for state-trait anxiety inventory (STAI: Form Y). Palo Alto,
California; Consulting Psychologist Press, 1983.
23. Richtlinie der Bundesärztekammer zur Qualitätssicherung laboratoriumsmedizinischer
Untersuchungen. Deutsches Ärzteblatt 2014;111:A1583-618.
24. Smith ML. Mechanisms of vasovagal syncope: relevance to postflight orthostatic
intolerance. J Clin Pharmacol 1994;34:460-5.
25. Thakar A, Deepak KK, Kumar SS. Auricular syncope. J Laryngol Otol 2008;122:1115-
7.
26. Carr E, Brockbank K, Allen S, Strike P. Patterns and frequency of anxiety in women
undergoing gynaecological surgery. J Clin Nurs 2006;15:341-352.
27. Lalinec MM, Engelsmann F. Anxiety, fears and depression related to hysterectomy. Can
J Psychiatry 1985;30:44 – 47.
Licence Statement: I, Taras Usichenko, the Corresponding Author of this article (the
“Contribution”) has the right to grant on behalf of all authors and does grant on behalf of all
authors, a licence to the BMJ Publishing Group Ltd and BMAS and its licensees, to permit this
Contribution (if accepted) to be published in Acupuncture in Medicine and any other BMJ
Group products and to exploit all subsidiary rights, as set out in our licence set out at:
(http://aim.bmj.com/acupuncturelicenceform.pdf)

64
Table 1. Patients’ characteristics.
Auricular Acupuncture
N=32
No Intervention
N=30
Age (years) 37 ± 10 36 ± 9
Body mass (kg) 71 ± 16 72 ± 17
Height (cm) 167 ± 7 168 ± 7
BMI (kg/m2) 24.4 ± 6.8 25.4 ± 5.8
Trait anxiety 44 ± 11 41 ± 10
BMI: Body-Mass-Index. Data is presented as mean ± standard deviation.

65
Table 2. Preoperative anxiety and serum cortisol concentration.
Time of outcome
measurement
Auricular acupuncture
N=32
No Intervention
N=30
State anxiety
I (before) 49 ± 15 44 ± 12
II (evening after
intervention) 42 ± 13 47 ± 11
III (before surgery) 47 ± 14 53 ± 12
VAS-100 (mm)
I 50 (13.75-75) 50 (10-57.5)
II 30 (15-50) 50 (30-65)
III 30 (15-70) 57.5 (30-80)
Serum cortisol
(ng/ml)
III 375 ± 153 390 ± 150
VAS-100: visual analogue scale 100 mm. Data is presented as mean ± standard deviation and
as median (interquartile range).

66
Figure Legends
Figure 1. Flow of study. Patients meeting the eligible criteria were asked for participation in
the study. Those who refused to receive auricular acupuncture (AA) as treatment for
preoperative anxiety, were asked to participate in a routine internal audit of perioperative
anxiety during standard clinical care (control group with no intervention).
Figure 2. Localisation of the auricular acupuncture points, used to treat preoperative anxiety:
MA-SC, Kidney; MA-TF1, Ear Shenmen; MA-IC1, Lung; MA-AT1, Subcortex and and MA-
TG, Adrenal gland.
Figure 3. Timeline of outcome measurement. I - afternoon of the day before surgery; II –
evening of the day before surgery; III – morning of the surgery day; IV – discharge home in
the afternoon. Auricular acupuncture was performed in the afternoon of the day before
surgery using indwelling fixed needles, which remained in situ and were removed after
surgery immediately before the discharge. Preoperative anxiety was measured using the
State-Trait-Anxiety Inventory (STAI) and a 100 mm visual analogue scale (VAS-100) at
time I, II, III. Serum cortisol was taken at time point III (immediately before the surgery).
Figure 4. Preoperative anxiety, measured in a patients that received auricular acupuncture (AA)
and untreated patients at the day before the surgery before AA or at a comparable time without
intervention (Time I); at the evening of the day before the surgery (Time II) and immediately
before the surgery (Time III) using the state form of the German version of the State-Trait-
Anxiety Inventory. * p < 0.01 for comparison of anxiety at Time I vs. Time II in Auricular
Acupuncture group. ** p < 0.001 for comparison at Time III vs. Time Point II and *** p < 0.01
for comparison at time III vs. time I in patients from No Intervention group; p values Holm-
Bonferroni corrected.
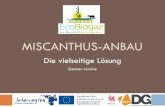











![Entwicklung einer Berechnungs-Methode für die Auslegung ...€¦ · Es gibt für den variablen Pitch bereits vielversprechende Ansätze, wie Paraschivoiu2009zeigt[22],bzw.bereits1995entwickelt[3].Jedochsind](https://static.fdokument.com/doc/165x107/60061a66b203207aa715c1b3/entwicklung-einer-berechnungs-methode-fr-die-auslegung-es-gibt-fr-den-variablen.jpg)