Kanton Bern Was Medien wollen und was Behörden können 9. Herzberg-Tagung – 7. November 2007 - Basel.
Herzberg, G1., Hudson, B2., Mayne, P3., McFadzean, N4., McParland, B2., Mitrovic, A2., Schloeffel, R5. 1Bellingen Healing Centre, Bellingen, NSW; 2The University of Sydney, Sydney, NSW; 3Laurieton Medical Centre, Laurieton, NSW;
4RestorMedicine, San Diego CA, USA;5Pymble Grove Health Centre, Pymble NSW
Lyme borreliosis (LB), also known as Lyme disease;
• fastest growing arthropod borne infectious disease in the Northern
Hemisphere.
• caused by a spirochete bacterium and the pathogenic species are
collectively called Borrelia burgdorferi sensu lato (BBsl) and currently
includes 23 species.
• treated early with appropriate antimicrobials usually results in a full
recovery.
• if treatment delayed, disseminated LB can lead to a multi-systemic infection,
requiring complex treatment of longer duration and results in high morbidity
and mortality.
• clinical symptoms are broad including neurological, cardiac, arthralgia,
myalgia, fatigue, dermatological and psychiatric.
• initial symptoms can resemble a flu like illness.
• BBsl exist as spirochetes, cell wall deficient intracellular forms and dormant
cyst forms. This is important when treatment is considered in chronic LB.
• important to test for other arthropod borne infections as tick bite can deliver
multiple pathogens which can complicate clinical presentation and
treatment strategies.
In Australia; • LB diagnosis presumes the patient acquired LB overseas.
• NSW Ministry of Health states there is very little evidence of locally acquired
LB although it can’t be ruled out.
www.health.nsw.gov.au/factsheets/infectious/lyme_disease.html
• Preliminary data suggests Australian ticks carry Borrelia species,
presented in poster 72, and is consistent with a BBsl species.
• Very little research is being undertaken in Australia on arthropod borne
infections with fatal consequences (Senanayake et al., 2012).
Discussion- The way forward:
• Serology is only sensitive if the correct antigens are presented.
Igenex use 2 BBss strains so potentially LB patients infected with a
different BBsl species may not be detected.
• All Australian endemic BBsl species need to be identified and fully
characterised.
• Once BBsl species are isolated, serology tests can be developed.
• Endemic areas need to be identified
• Identify species of ticks that transmit BBsl and other infections.
• An Australian antigenic profile needs to be determined (Evans et al.,
2010) and how antigens correlate to symptomology to aid in diagnosis.
• PCR diagnostic tests need to be developed in combination with serology.
• A direct measure of infection such as PCR is far better than serology.
• PCR is highly specific and may not be applicable for general screening
until all BBsl species have been fully characterised.
• PCR is valuable in detection of LB in immune-compromised patients.
• IgG responses can take several weeks to develop and yet there is
only a small window of opportunity to treat LB up to 6-8 weeks before
the infection is disseminated.
• 4 weeks of doxycycline following a tick bite poses little risk to patient
as doxycycline has been used safely for decades, however, not treating
with doxycycline could lead to systemic infection causing chronic
illness of high morbidity and great cost to the community.
• Australia has a unique opportunity to develop appropriate
guidelines, guided by the European and American experience of LB.
• All arthropod borne infections need to be considered as highlighted by the
recent babesiosis fatality (Senanayake et al., 2012).
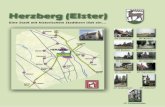
Figure 3: Comparison of BBsl positives by IGeneX criteria to CDC criteria. Bands represent different antigens-see figure 2 & 3. n=number tested
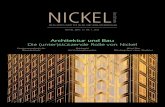
Figure 5: IgM &/or IgG IFA serology of arthropod borne infections Bartonella sp., Babesia sp., Ehrlichia sp., Anaplasma sp., and Rickettsia sp. n=number tested
Figure 6: Graph of IgM and IgG positive IFA to arthropod borne co-infections. n=number tested
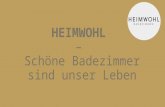
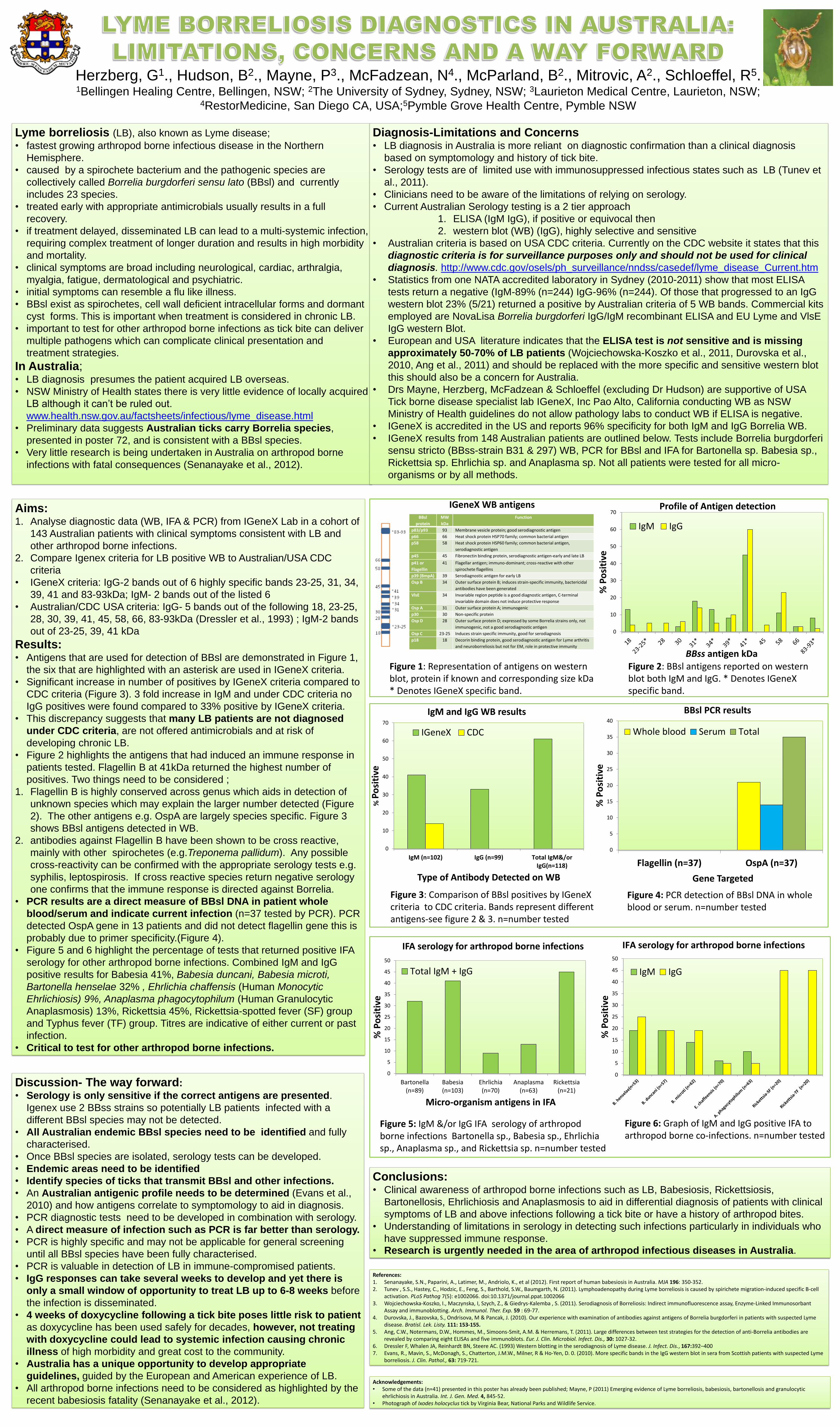
Figure 2: BBsl antigens reported on western blot both IgM and IgG. * Denotes IGeneX specific band.
Aims: 1. Analyse diagnostic data (WB, IFA & PCR) from IGeneX Lab in a cohort of
143 Australian patients with clinical symptoms consistent with LB and
other arthropod borne infections.
2. Compare Igenex criteria for LB positive WB to Australian/USA CDC
criteria
• IGeneX criteria: IgG-2 bands out of 6 highly specific bands 23-25, 31, 34,
39, 41 and 83-93kDa; IgM- 2 bands out of the listed 6
• Australian/CDC USA criteria: IgG- 5 bands out of the following 18, 23-25,
28, 30, 39, 41, 45, 58, 66, 83-93kDa (Dressler et al., 1993) ; IgM-2 bands
out of 23-25, 39, 41 kDa
Results: • Antigens that are used for detection of BBsl are demonstrated in Figure 1,
the six that are highlighted with an asterisk are used in IGeneX criteria.
• Significant increase in number of positives by IGeneX criteria compared to
CDC criteria (Figure 3). 3 fold increase in IgM and under CDC criteria no
IgG positives were found compared to 33% positive by IGeneX criteria.
• This discrepancy suggests that many LB patients are not diagnosed
under CDC criteria, are not offered antimicrobials and at risk of
developing chronic LB.
• Figure 2 highlights the antigens that had induced an immune response in
patients tested. Flagellin B at 41kDa returned the highest number of
positives. Two things need to be considered ;
1. Flagellin B is highly conserved across genus which aids in detection of
unknown species which may explain the larger number detected (Figure
2). The other antigens e.g. OspA are largely species specific. Figure 3
shows BBsl antigens detected in WB.
2. antibodies against Flagellin B have been shown to be cross reactive,
mainly with other spirochetes (e.g.Treponema pallidum). Any possible
cross-reactivity can be confirmed with the appropriate serology tests e.g.
syphilis, leptospirosis. If cross reactive species return negative serology
one confirms that the immune response is directed against Borrelia.
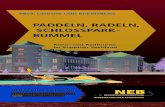
• PCR results are a direct measure of BBsl DNA in patient whole
blood/serum and indicate current infection (n=37 tested by PCR). PCR
detected OspA gene in 13 patients and did not detect flagellin gene this is
probably due to primer specificity.(Figure 4).
• Figure 5 and 6 highlight the percentage of tests that returned positive IFA
serology for other arthropod borne infections. Combined IgM and IgG
positive results for Babesia 41%, Babesia duncani, Babesia microti,
Bartonella henselae 32% , Ehrlichia chaffensis (Human Monocytic
Ehrlichiosis) 9%, Anaplasma phagocytophilum (Human Granulocytic
Anaplasmosis) 13%, Rickettsia 45%, Rickettsia-spotted fever (SF) group
and Typhus fever (TF) group. Titres are indicative of either current or past
infection.
• Critical to test for other arthropod borne infections.
Figure 1: Representation of antigens on western blot, protein if known and corresponding size kDa * Denotes IGeneX specific band.
0
5
10
15
20
25
30
35
40
45
50
Bartonella(n=89)
Babesia(n=103)
Ehrlichia(n=70)
Anaplasma(n=63)
Rickettsia(n=21)
% P
osi
tive
Micro-organism antigens in IFA
IFA serology for arthropod borne infections
Total IgM + IgG
0
10
20
30
40
50
60
70
% P
osi
tive
BBss antigen kDa
Profile of Antigen detection
IgM IgG
Figure 4: PCR detection of BBsl DNA in whole blood or serum. n=number tested
References: 1. Senanayake, S.N., Paparini, A., Latimer, M., Andriolo, K., et al (2012). First report of human babesiosis in Australia. MJA 196: 350-352. 2. Tunev , S.S., Hastey, C., Hodzic, E., Feng, S., Barthold, S.W., Baumgarth, N. (2011). Lymphoadenopathy during Lyme borreliosis is caused by spirichete migration-induced specific B-cell
activation. PLoS Pathog 7(5): e1002066. doi:10.1371/journal.ppat.1002066 3. Wojciechowska-Koszko, I., Maczynska, I, Szych, Z., & Giedrys-Kalemba , S. (2011). Serodiagnosis of Borreliosis: Indirect immunofluorescence assay, Enzyme-Linked Immunosorbant
Assay and immunoblotting. Arch. Immunol. Ther. Exp. 59 : 69-77. 4. Durovska, J., Bazovska, S., Ondrisova, M & Pancak, J. (2010). Our experience with examination of antibodies against antigens of Borrelia burgdorferi in patients with suspected Lyme
disease. Bratisl. Lek. Listy. 111: 153-155. 5. Ang, C.W., Notermans, D.W., Hommes, M., Simoons-Smit, A.M. & Herremans, T. (2011). Large differences between test strategies for the detection of anti-Borrelia antibodies are
revealed by comparing eight ELISAs and five immunoblots. Eur. J. Clin. Microbiol. Infect. Dis., 30: 1027-32. 6. Dressler F, Whalen JA, Reinhardt BN, Steere AC. (1993) Western blotting in the serodiagnosis of Lyme disease. J. Infect. Dis., 167:392–400 7. Evans, R., Mavin, S., McDonagh, S., Chatterton, J.M.W., Milner, R & Ho-Yen, D. 0. (2010). More specific bands in the IgG western blot in sera from Scottish patients with suspected Lyme
borreliosis. J. Clin. Pathol., 63: 719-721.
Acknowledgements: • Some of the data (n=41) presented in this poster has already been published; Mayne, P (2011) Emerging evidence of Lyme borreliosis, babesiosis, bartonellosis and granulocytic
ehrlichiosis in Australia. Int. J. Gen. Med. 4, 845-52. • Photograph of Ixodes holocyclus tick by Virginia Bear, National Parks and Wildlife Service.
0
5
10
15
20
25
30
35
40
45
50
% P
osi
tive
IgM IgG
IFA serology for arthropod borne infections
Diagnosis-Limitations and Concerns • LB diagnosis in Australia is more reliant on diagnostic confirmation than a clinical diagnosis
based on symptomology and history of tick bite.
• Serology tests are of limited use with immunosuppressed infectious states such as LB (Tunev et
al., 2011).
• Clinicians need to be aware of the limitations of relying on serology.
• Current Australian Serology testing is a 2 tier approach
1. ELISA (IgM IgG), if positive or equivocal then
2. western blot (WB) (IgG), highly selective and sensitive
• Australian criteria is based on USA CDC criteria. Currently on the CDC website it states that this
diagnostic criteria is for surveillance purposes only and should not be used for clinical
diagnosis. http://www.cdc.gov/osels/ph_surveillance/nndss/casedef/lyme_disease_Current.htm
• Statistics from one NATA accredited laboratory in Sydney (2010-2011) show that most ELISA
tests return a negative (IgM-89% (n=244) IgG-96% (n=244). Of those that progressed to an IgG
western blot 23% (5/21) returned a positive by Australian criteria of 5 WB bands. Commercial kits
employed are NovaLisa Borrelia burgdorferi IgG/IgM recombinant ELISA and EU Lyme and VlsE
IgG western Blot.
• European and USA literature indicates that the ELISA test is not sensitive and is missing
approximately 50-70% of LB patients (Wojciechowska-Koszko et al., 2011, Durovska et al.,
2010, Ang et al., 2011) and should be replaced with the more specific and sensitive western blot
this should also be a concern for Australia.
• Drs Mayne, Herzberg, McFadzean & Schloeffel (excluding Dr Hudson) are supportive of USA
Tick borne disease specialist lab IGeneX, Inc Pao Alto, California conducting WB as NSW
Ministry of Health guidelines do not allow pathology labs to conduct WB if ELISA is negative.
• IGeneX is accredited in the US and reports 96% specificity for both IgM and IgG Borrelia WB.
• IGeneX results from 148 Australian patients are outlined below. Tests include Borrelia burgdorferi
sensu stricto (BBss-strain B31 & 297) WB, PCR for BBsl and IFA for Bartonella sp. Babesia sp.,
Rickettsia sp. Ehrlichia sp. and Anaplasma sp. Not all patients were tested for all micro-
organisms or by all methods.
0
5
10
15
20
25
30
35
40
Flagellin (n=37) OspA (n=37)
% P
osi
tive
Gene Targeted
Whole blood Serum Total
Conclusions: • Clinical awareness of arthropod borne infections such as LB, Babesiosis, Rickettsiosis,
Bartonellosis, Ehrlichiosis and Anaplasmosis to aid in differential diagnosis of patients with clinical
symptoms of LB and above infections following a tick bite or have a history of arthropod bites.
• Understanding of limitations in serology in detecting such infections particularly in individuals who
have suppressed immune response. • Research is urgently needed in the area of arthropod infectious diseases in Australia.
0
10
20
30
40
50
60
70
IgM (n=102) IgG (n=99) Total IgM&/orIgG(n=118)
% P
osi
tive
Type of Antibody Detected on WB
IgM and IgG WB results
IGeneX CDC
BBsl PCR results
IGeneX WB antigens BBsl
protein
MW
kDa
Function
p83/p93 93 Membrane vesicle protein; good serodiagnostic antigen
p66 66 Heat shock protein HSP70 family; common bacterial antigen
p58 58 Heat shock protein HSP60 family; common bacterial antigen,
serodiagnostic antigen
p45 45 Fibronectin binding protein, serodiagnostic antigen-early and late LB
p41 or
Flagellin
41 Flagellar antigen; immuno-dominant; cross-reactive with other
spirochete flagellins
p39 (BmpA) 39 Serodiagnostic antigen for early LB
Osp B 34 Outer surface protein B; induces strain-specific immunity, bactericidal
antibodies have been generated
VlsE 34 Invariable region peptide is a good diagnostic antigen, C-terminal
invariable domain does not induce protective response
Osp A 31 Outer surface protein A; immunogenic
p30 30 Non-specific protein
Osp D 28 Outer surface protein D; expressed by some Borrelia strains only, not
immunogenic, not a good serodiagnostic antigen
Osp C 23-25 Induces strain specific immunity, good for serodiagnosis
p18 18 Decorin binding protein, good serodiagnostic antigen for Lyme arthritis
and neuroborreliosis but not for EM, role in protective immunity